Embed Size (px)
Citation preview

WELCOME
• History suggests, during 20thcentury, significant increase of women's involvement in workplace outside the home setting had made breast-feeding less popular and a burden. Urbanization and advances in technology had contributed further. With the rapid growth of industries and their competition in the twentieth century, industrial food products were developed along with the production of breast milk substitutes.

• Decrease in breastfeeding prevalence was found to increase the morbidity and mortality among children. This situation received the worldwide attention and to address the issue, Baby Friendly Hospital Initiative (BFHI) was initiated by WHO and UNICEF in 1991.

• The Baby Friendly Hospital Initiatives launched in 1991, is an effort by UNICEF and WHO to ensure that all maternities , whether free standing or in a hospital, become center of breastfeeding support
Key dates in the history of breast feeding and BFHI
• 1979- Joint WHO/UNICEF meeting on Infant and Young Child Feeding Geneva
• 1981- Adoption of the International Code of Marketing of Breast- Milk Substitute
• 1989- Protecting, promoting and supporting breast feeding . The special role of maternity services
- Convention on the child right• 1990- Innocenti Declaration
• 1991- Launching of BFHI• 2000- Who expert Consultant on HIV and infant
Feeding • 2001- WHO consultation on the optimal duration
of exclusive breast feeding • 2002- Endorsement of the global strategy for
infant and young child feeding • 2005 Innocenti Declaration 2005• 2007- Revision of BFHI documents

• In 2002, Global Strategy for Infant and Young Child Feeding was developed by WHO and UNICEF which was based on the Innocenti Declaration and BHFI and addresses the needs of all children, including those living in difficult circumstances, such as mothers living with HIV, low birth-weight infants and infants in emergency situations.

• In the process of development and expansion of the BFHI, several regional and national level meetings were organized for effective networking and providing feedback and recommendations. These meetings updated the global criteria, assessment tools and the training courses.
• Inclusion of mother friendly care within the initiative was one of the important recommendations. Although the revision was done in 2004-2005, the final version of the materials was completed in 2007.
Summary of main point of international code
• No advertising of breast milk substitute and other products to the public
• No donation of breast milk substitute and supplies to maternity hospital
• No free samples to mother• No promotion in the health services

• Since the launch of initiative, more than 20,000 hospitals in 156 countries in the world have adopted it over the last 15 years
Global and Regional Scenario
• A significant progress has been observed in improving infant and young child feeding practices worldwide after the adoption of original Innocenti Declaration in 1990. However, inappropriate feeding practices, sub-optimal or no breastfeeding and inadequate complementary feeding has still remained the greatest threat to child health and survival globally.

• Studies showed that improved breastfeeding alone could save the lives of more than 3,500 children every day, more than any other preventive intervention. Promotion of breastfeeding has been identified as one of the important 45 evidence based interventions to address under-nutrition in children (Unicef.com.:http:/ /www.unicef.org/programme/breastfeeding/baby.htm.
• According to UNICEF, till 2002, 14,994 hospitals throughout the world were declared as baby friendly with highest number 8747 in the East and Pacific Region followed by South Asia Region. China is the country with largest numbers of baby friendly hospitals [6312] while India has the second largest number [1250].

• There are some success stories of implementation of BFHI in different parts of the globe. Cuba, China, Gabon, Chile etc. have such examples. In Cuba, the rate of exclusive breastfeeding was increased almost three times from 25% to 72% in the six years’ duration (1990-1996) where 49 out of 56 hospitals were identified as baby friendly.

• In China which has more than 6,000 baby-friendly hospitals, exclusive breastfeeding in rural and urban areas rose significantly. It raised from 29 per cent in 1992 to 68 per cent in 1994 in rural areas while in urban areas; the increase was from 10 per cent to 48 percent.

• Similarly, data from Central Hospital of Libreville in Gabon showed that cases of neonatal diarrhea fell by 15 per cent, diarrheal dehydration declined by 14 per cent and mortality fell by 8 per cent after successful implementation of BFHI.

National Scenario
• In Nepal BFHI activities were started in 1994 with the training of health workers from 22 hospitals all over the country till 1996.
• After training, these hospitals were assessed by external and internal assessors in 1997-98 through Nepal Pediatric Society and seven of the hospitals were certified as Baby Friendly Hospitals.

• These seven hospitals are: Tribhuvan University Teaching Hospital, Maharajgunj, Kathmandu, Maternity Hospital, Thapathali, Kathmandu, Patan Hospital, Lalitpur, Bhaktapur Hospital, Bhaktapur, Hetauda Hospital, Makawanpur, BP Koirala Institute of Health Science, Dharan and Koshi Zonal Hospital, Bitratnagar.

• According to the last two Demographic Health Surveys (DHS 2006 & 2011) there has not been any change in the neonatal mortality which is constant at 33/1000 live births. Practice of initiation of breastfeeding within one hour of birth was only 35% and exclusive breastfeeding for six months was 53% in 2006,

• but there has been some increment in both the indicators in 2011. Early initiation of breastfeeding rose to 45% and exclusive breastfeeding to 70%. The reasons of such increment could be due to increase in literacy and awareness among the women.
• Although there is a need of continuous monitoring and supervision of BFHI activities to ensure proper implementation, it was about 13 years that no any monitoring and assessment activities were carried out in Nepal. In 2011, an assessment was carried out in all of the 7 BFHI hospitals initiated by Child Health Division, Department of Health Services which used the revised tools developed by WHO/ UNICEF.
• For the assessment, interview was done with Head of the institutions, hospital staffs, pregnant women and lactating mothers and observation in different units of the hospitals, followed by a market survey.

• The study drew some interesting findings. All the hospitals certified as BFHI were found not fulfilling all the 10 steps of BFHI activities. There was no display of policy on BFHI in the hospitals, health workers were very limited or were not trained, demand feeding was not strictly followed and mother support group or mother friendly care did not exist in any of these hospitals but these hospitals had good practice of rooming-in and pacifier and teats were not provided to newborns.

• There could be many reasons for not fulfilling the ten steps of BFHI by hospitals in Nepal. The main reason could be lack of monitoring and supervision activities since a long time, from the time the hospitals were certified. Transfer of almost all the trained staffs and lack of training to the new ones could be the other reason
• At present, Child Health Division, DoHS is in the process of finalization/ finalized the strategy on Infant and Young Child Feeding. Although nutrition section of the division has some programs on breastfeeding it is not enough to promote breastfeeding as desired because the programs are limited only to creating awareness and most of the times they are limited to breastfeeding week (August 1-7) only.

• The internationally defined term Baby Friendly may be used only by maternity services that have passed external assessment according to the Global criteria for the BFHI

• A maternity facility can be designated ‘baby friendly’ when it does not accept Free or low cost breast milk substitute, feeding bottles or teats and has implemented 10 specific steps to support successful breast feeding
• The process currently controlled by national breast feeding authorities, using Global Criteria that can be applied to maternity Care in every country. Implementing guides for the BFHI have been developed by WHO and UNICEF

Goals of the BFHI
1.To transform hospitals and maternity facilities through implementation of the “ten steps”
2.To end the practice of distribution of free and low cost supplies of breast - milk substitutes to maternity wards hospitals

10 steps
• Step 1- Have a written breast feeding policy that is routinely communicated to all health care staff

Why breast feeding policy?• Requires a course of action and provides guidance• Helps establish consistent care for mothers and babies• Provides a standards that can be evaluated • Breast feeding policy should coverAt a minimum it should include:• 10 steps• An institutional ban on acceptance of free or low cost supplies
of breast milk substitutes, bottles and teats and its distribution• A frame work for assisting HIV positive mothers to make
informed infant feeding decisions that their individual Circumstances and then support for this decision

How should be it presented ?
• It should be written in the most common languages understood by patient and staff
• Available to all staff caring for mothers and babies
• posted or displayed in areas where mothers and babies are cares for

STEP 2- Train all health care staff in skill necessary to implement this policy

Area of Knowledge
• Advantage of breastfeeding • Risks of artificial feeding• Mechanism of lactation and sucking • How to help mothers initiate and sustain
breastfeeding
• How to resolve breast feeding difficulties• How to assess a breastfeed• Hospital breast feeding policies and practices• Focus on changing negative attitudes which
set up barriers
• STEP 3- Inform all pregnant women about the benefits and management of breastfeeding
Antenatal education should be
• Antenatal education should include• Benefits of breastfeeding • Early initiation importance of rooming in• Importance of feeding on demand• Importance of exclusive breast feeding • How to assure enough breast milk

• STEP – 4Help mothers initiate breast feeding within a half hour of birth

• Place babies in skin- to skin contact with their mothers immediately following birth
• For at least an hour and encourage mothers to recognize when their babies are ready to breastfed, offering help if needed

• STEP 5Show mothers how to breastfed and how o maintain lactation, even if they should be separated from their infants
• “contrary to popular beliefs, attaching the baby on breast”
• Is not an ability with which a mother is ( born) rather it is a learned skill which she must acquire by observation and experience

Supply and demand
• Milk removal stimulates milk production• The amount of breast milk removed at each
feed determines the of milk production in the next few hours
• Milk removal must be continued during separation to maintain supply

• STEP 6Give newborn infants no food or drink other than breast milk unless medically indicated

• Decreased frequency of effectiveness of suckling
decreased amount of milk removed from breasts
Delayed milk production or reduced milk supplySome infants have difficulty attaching to breast if formula given by bottle

Acceptable medical reasons for supplementation or replacement
Infant condition• Infants who cannot be BF but an receive BM include those who are
very weak• Have sucking difficulties or oral abnormalities or are separated from
their mothers • Infant who may need other other nutrition in addition to BM include
VLBW or pre-term infants are risk of hypoglycemia, or those who are dehydrated or malnourished, when BM alone is not enough
• Infants with galactosemia should not receive BM or the usual BMS. They will need a galactose free formula
• Infants with PKU may be BF and receive some phenylalanine free formula
Maternal condition • Should stop during therapy, if mother is taking anti- metabolites,
radioactive iodine, or thyroid medication• Some medications may cause drowsiness or other side effects in
infants and should be substituted during BF• BF remains the feeding choices for the majority of infants even with
tobacco, alcohol and drug use. If the mother is an intravenous drug user BF is not indicated
• Avoidance of all BF by HIV + mothers is recommended when replacement feeding is acceptable, feasible, affordable, sustainable and safe. Otherwise EBF is recommended during the 1st months, with BF discontinued when condition are met. Mixed feeding is not recommended
• If a mother is weak, she may be assisted to position her baby so she can BF
• BF is not recommended when a mother has a breast abscess, but BM should be expressed and BF resumed once the breast is drained and antibodies have commenced
• Mothers with herpes lesion on their breasts should refrain from BF until active have been resolved
• BF is not encouraged for mothers with Human T-cell Leukemia Virus, if safe and feasible options are available
• BF can be continued when mothers have hepatitis B, TB and Mastitis, with appropriate treatment undertaken
• STEP 7 Practice rooming in- allows mothers and newborn to remain together 24 hours a day Rooming –in A hospital arrangement where a mother/ baby pair stay in the same room day and night, allowing unlimited contact between mother and infant
Why rooming in ?• Reduces costs• Requires minimal equipment• Require no additional personnel• Reduces infection• Help establish and maintain breastfeeding
• STEP 8 Encourage breastfeeding on demand WHY?• Earlier passage of meconium• Lower maximal weight loss• Breast milk flow established sooner• Larger volume of milk intake on day 3• Less incidence of jaundice

• STEP9Give no artificial teats or pacifiers ( also called dummies and soothers) to breastfeeding infants

• STEP 10Foster the establishment of breast feeding support group and refer mothers to them on discharge from hospital or clinicSupports can include• Early postnatal or clinic checkup• Home visits• Telephone calls• Community services• Mother support group• community support group
Breastfeeding
• The feeding of an infant or young child with breast milk directly from females human breasts
• Rather than from a baby bottle or other container

Benefits to the baby
• Perfect nutrition• Higher IQ• Complete food for the 1st six month• Prevent infections• Prevent chronic diseases easily digested

Benefits to the mother
• Reduces post delivery bleeding and anemia• Help delay next pregnancy• Protective effects against breast and ovarian
cancer• Helps to loose weight• Emotional bonding • Needing no preparation
Immunologic specificity
• Protection against pathogens and allergens• Kills pathogenic organism or modifies their growth• Stimulates epithelial maturation for future defense• First immunization• Protection against common respiratory and intestinal
disease Colostrum = baby’s 1st vaccination• Less risk to illness such as: Ear infection, pneumonia,
crohn’s disease and other bowel illness Childhood cancer, DM, arthritis, allergies, asthma and eczema
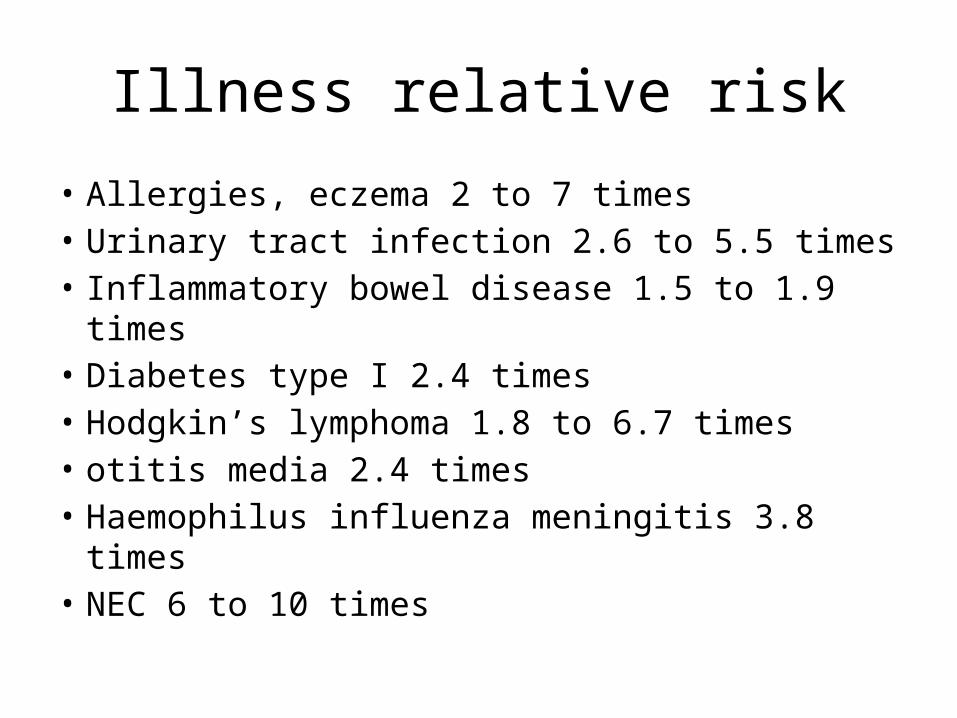
Illness relative risk
• Allergies, eczema 2 to 7 times• Urinary tract infection 2.6 to 5.5 times• Inflammatory bowel disease 1.5 to 1.9 times• Diabetes type I 2.4 times• Hodgkin’s lymphoma 1.8 to 6.7 times• otitis media 2.4 times• Haemophilus influenza meningitis 3.8 times• NEC 6 to 10 times
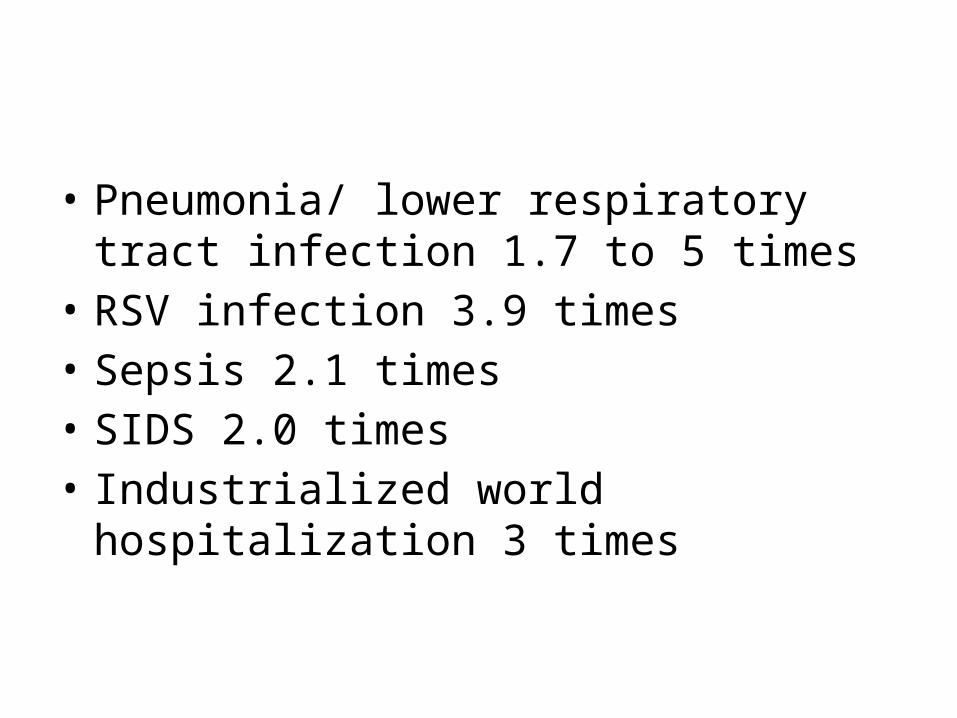
• Pneumonia/ lower respiratory tract infection 1.7 to 5 times
• RSV infection 3.9 times• Sepsis 2.1 times• SIDS 2.0 times• Industrialized world hospitalization 3 times

THANK YOU





























