Embed Size (px)
DESCRIPTION
benign aggressive bone tumors
Citation preview

Benign aggressive bone tumors

INTRODUCTION● aggressiveness of these lesions is between
purely benign and frankly malignant.● Today in this seminar brief dicussion of such benign
aggressive tumors would be done● GIANT CELL TUMOR● CHONDROBLASTOMA● OSTEOBLASTOMA● CHONDROMYXOID FIBROMA● LANGERHANS CYST HISTOCYTOSIS

Giant Cell Tumor● Sir Astley Cooper first describe in 1818 emphasizing its
benign nature. ● Dr Paget called it “brown or Myeloid tumour” in 1853.● WHO- ‘’An aggressive , potentially malignant lesion’’
Its an aggressive lesion characterised by well- vascularised tissue composed of spindle cells and multinucleated giant cells uniformly dispersed throughout the tumour.

Incidence
● acc to mayo clinic series 5% of neoplasms of bone.
● common in some parts of andhra pradesh in india.

Age groups involved.
● Usually after epiphyseal closure.● Hence age group involved is 20 to 40
years(70%) with slight female predominance (3:2 ).
● Gradual Decrease in after fifth decade.

Site of Involvement
Situated mostly at epiphyseo-metaphyseal region of long bones.
AROUND KNEE JOINT 55 %
DISTAL END OF RADIUS 10-12 %
UPPER END OF HUMERUS 7%
LOWER END OF TIBIA 3-4 %
SMALL BONES OF HAND AND FEET 2%
SPINE ,SKULL AND PELVIS 15-17%

CLINICAL PRESENTATION
● complains of vague persistent pain over the swelling at end of long bones…swelling present from few weeks to several months.
● Note- This pain could have increased after pathological fracture which may bring the patient to surgeon for first time.

Clinical PictureOverlying skin is stretched , shiny with no engorged veins.
● PALPATION- The swelling is warm , smooth with variable consistency, predominantly bony and tenderness is present on firm palpation.● EGG SHELL CRACKLING-ELICITABLE WHEN THERE
IS PATHOLOGICAL FRACTURE OR TOO MUCH THINNING OF CORTEX.

ROM at adjacent joint can be restricted due to mechanical block.

Radiological featuresPlain Radiograph-● Tumour will show large , sharply
circumscribed area of reduced density asymmetrically located in the epiphysis, begining subcortically and extending towards metaphysis.
● SOAP BUBBLE APPEARANCE- multilocular and trabeculated appearance of tumor.
● Geographical destruction type of osteolysis. ● cortical thinning.● no sclerotic rim and new bone formation.

Computed Tomography● Helps in confirming the integrity
of cortex and outlining the tumour extent.
● Subcortical destruction can be well appreciated with a ct scan.
● Limitation- soft tissue extension of tumour and its relationship with adjacent structures cannot be seen .

M.R.I● With mri the morphologic analysis
and extent of disease into surrounding soft tissue can be assessed .
● As in CT SCAN, sub cortical destruction can be well appreciated by multiplanar mri.
● Intramedullary tumors best appreciated in T1 weighted images.
● Extraosseous Tumors best appreciated in T2 weighted images.

ANGIOGRAPHY
● to check Relationship of major vessles to large tumors.
● Does not correlate with grading of tumor.

RADIONUCLIDE SCINTIGRAPHY
● GCT takes up increased uptake of technetium 99.
● Again does not have any correlation with grading of tumor.

BiopsyThis is the final diagnostic tool for diagnosis of gct.Sample can be taken by● OPEN INCISIONAL BIOPSY ● FINE NEEDLE ASPIRATION ● CORE NEEDLE BIOPSY

GROSS APPEARANCE● Epiphyseal end of long bone will be expanded with
thining of periosteum and cortex, being easily broken by handling.
● Composed of ragged , very friable, readily bleeding tissue containing variously sized cavitations and small cysts.
● colour -varies from reddish brown to chocolate color in which vascular tissue predominates , to greyish or mottled where connective tissue is major component.
● no evidence of periosteal new bone formation.● the inner wall of tumor is lined by a fibrous capsule
from which the septae extend inwards to partition the tumor.

MICROSCOPIC APPEARANCE● Multinucleated giant cells and spindle
cells are the main component .
● GIANT CELLS in this tumor are characteristic and specific having size of 10 to 100 microns with centrally placed uniform sized nuclei numbering 15 to 150 max.
● SPINDLE CELLS- They are oval ,elongated and contain relatively large chromatinized nucleus and small acidophilic cytoplasm

● The appearance of spindle cells indicates the malignant potential of tumor.
POINT TO BE NOTED-● Appearance of giant cells is not diagnostic. Giant cells are
also seen in lesions like aneurysmal, unicameral cyst, non ossifying fibroma, chondroblastoma and brown tumor of hyperparathyroidism
● appearance of spindle cells is important.(main neoplastic component)

GRADING OF GCT

CAMPANACCI RADIOGRAPHIC GRADING
● Grade 1- tumor has well marinated border of a thin rim of mature bone, and the cortex is intact or slightly thinned but not deformed.

● Grade 2- tumor has relatively well defined margins, but no radio opaque rim, cortex is thin and expanded but is present.

Grade 3- cortex is perforated with extension of tumor into soft tissue.

Enneking staging of Giant cell tumorBased on clinical radiological and histopathological featuresStage 1- LATENT(10 - 15%)● Patient is asymptomatic, discovered incidentally.● May be associated with pathological fractures.● Radiologically-tumor is intracapsular, with well defined margins and sclerotic rim.
no cortical destruction.Stage 2- ACTIVE ( 70-75 %)● Patient is symptomatic.● Often associated with pathological fracture.● Radiologically- intracapsular, has expanded or thinned out cortex ,but there is no
breakthrough the cortex.

Stage 3 (aggressive) : 10 - 15 %● Symptomatic ● Rapidly growing mass ● Radiologically- Extracapsular, has cortical
perforation ● Will show intense vascularity on angioram

Note-
TNM Classification system is not applicable to GCT because anatomically it remains intracompartmental for a long time within well formed capsule of the periosteum and soft tissue.

Giant Cell Variants
1. Aneurysmal bone cyst2. Brown tumor of hyperparathyroidism3. non ossifying fibroma4. Unicameral bone cyst5. Fibrous dysplasia6. Chondroblastoma7. Giant cell reparative granuloma8. ossifying fibroma9. osteogenic sarcoma

MANAGEMENT AND COMPLICATIONS OF GCT

INTRODUCTION
● Majority of tumors are benign, have 30 to 40 % recurrence and has tendency to metastasize.

AIM OF TREATMENT
● To eradicate the growth completely at initial operation
● to avoid ablation of limb
● to maintain possible function

● Traditionally
: intralesional curettage/resection with bone graft
:recurrence 35-42 %
● En Bloc resection : recurrence 10% : multiple complications

● HISTORICALLY TREATMENT CONSISTED OF SIMPLE CURETTAGE
● BUT RECURRENCE RATES > 50%
● FOR DEFECTS AFTER RESECTION OR CURETTAGE,EITHER ALLOGRAFT OR BONE CEMENT USED AS FILLING AGENTS
EXTENDED CURETTAGE –USE OF A POWER BURR TO ENLARGE THE CAVITY 1-2 CM IN ALL DIRECTIONS IS NOW CONSIDERED STANDARD

ADJUNCT Tx
●PMMA, Liquid N2, Phenol, l,electrocautery.
–Local extension of margin
–Kill residual foci and remaining tumour cell
● ASSOCIATED WITH PATHOLOGIC FRACTURES & WOUND HEALING PROBLEMS

Bone graft
ADVANTAGE:
• RESTORING NORMAL BIOMECHANICS TO JOINT SURFACE
•PREVENT FUTURE DEGENERATIVE JOINT DISEASES
•RESTORING BONE STOCK

•DISADVANTAGES
: JOINT MUST BE PROTECTED FOR AN EXTENDED PERIOD OF TIME TO PREVENT A PATHOLOGICAL FRACTURES.
● TUMOUR RECURRENCE IS DIFFICULT TO DISTINGUISH FROM GRAFT RESORPTION.

Bone cement•THE ABOVE DISADVANTAGES OVERCOME BY USE OF BONE
CEMENT
•PROVIDES IMMEDIATE STABILITY-HENCE QUICKER REHABILITATION
•EASIER DETECTION OF RECURRENCE SEEN AS EXPANDING RADIOLUCENCY ADJ TO CEMENT
•KILLS RESIDUAL TMR CELLS THROUGH POLYMERISATION HEAT.
● CYTOTOXIC AGENTS- METHOTREXATE AND ADRIAMYCIN CAN BE INCORPORATED IN BONE CEMENT.
.

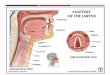
Curettage with bone cementing

En bloc excision
•INITIAL PROCEDURE OF CHOICE AND HERE 2 CM OF NORMAL
BONE IS ALSO EXCISED
•
•DEFECTS ARE FILLED WITH CANCELLOUS BONE GRAFTS,FREEZE DRIED ALLOGRAFT OR PROSTHESIS

resection of tumor in lesions of sacrificable part● lower end ulna● upper end of fibula● phalanges● metatarsal rays
RECURRENCE IS ALMOST NILL

Resection and reconstruction with Autograft

•AROUND THE KNEE,A HEMI CONDYLAR OSTEOARTICULAR
ALLOGRAFT RECONSTRUCTION OR A ROTATING HINGE ENDOPROSTHESIS MAY BE NECESSARY
•FOR AGGRESSIVE LESION OF DISTAL RADIUS,PRIMARY RESECTION AND RECONSTRUCTION WITH A PROXIMAL FIBULAR AUTOGRAFT INDICATED

EXCISION AND RECONSTRUCTION
•FOR GCT AFFECTING LOWER END OF FEMUR OR UPPER END OF TIBIA
• AFTER EN BLOCK EXCISION RECONSTRUCTION CAN BE DONE BY
1.TURN-O-PLASTY TECHNIQUE
2.ARTHRODESIS
3.ARTHROPLASTY

RADIOTHERAPY- Disappointing recurrence rate of 50-70%. ● malignant sarcomatous transformation ocuured in 7-10 %
cases
CHEMOTHERAPY- NO EFFECTIVE CHEMOTHERAPEUTIC AGENTS AVAILAIBLE FOR MANAGEMENT OF GCT.

RECURRENCE OF LESIONS● Most local recurrences and pulmonary metastases occur within 3
years or even upto 20 years.
● Patient should have radiograph of primary tumor site and of the chest at
>> 3 MONTHS INTERVAL FOR 1YR
>> 6 MONTHS INTERVAL FOR NEXT 2 YRS
>>AND ANNUALLY THEREAFTER

•treatment is same as for primary lesions.
•after biopsy shows that tumor is still benign,repeat curretage or resection is performed.

CHONDROBLASTOMA

INTRODUCTION
● Codman in 1931 first described..”Codmans tumor”
● It is a rare , benign bone tumor of immature cartilage cells derivation arising in epiphysis consisting of polygonal chondroblast, foci of chondroid, osteoclast like giant cells and small foci of calcifications.

● INCIDENCE- less than 1 % of primary bone tumors.
● AGE Ranges - 3 to 73 years.Usually teenagers, before obliteration of epiphyseal plate.90% Reported in 5 to 25 years.● SEX Male:female 2:1

● SITEEpiphyseal region of long bone, occasionally extends to adjacent metaphysis. ● COMMON OCCURRENCElower extremity(72%)...in which 50 % cases have been reported knee
Proximal humerus 18%
Proximal Tibia 17 %
Distal Femur 16 %
Proximal femur 16%
Ankle bones 9%

SIZE - 1 to 6 cm
CLINICAL FEATURES-. >Pain & swelling – several months.
>May be referred to nearest joint
>Some loss of joint function & muscle wasting. >Joint effusion esp. around knee. >Pathological fractures – rare.

RADIOLOGICAL FEATURES
X – RAYS: >Lytic area –
>Oval or round
< ½ of epiphyseal area.
>Thin rim of sclerosis
>Punctate or streaky calcification.

● In metaphyseal extension, i.e tumor crossing growth plate results in – Eccentric location & bulging expansion of cortex

PATHOLOGY Gross:
● Usually well demarcated lesions.
● Capsule – thin, easily disruptable
● Cut section- Soft, reddish –purple, friable, focally fritty tissue.
● Cystic spaces and haemorrhages may be seen.

MICROSCOPIC:-
● Islands of chondroblasts with uniform polyhedral closely packed cells.
● Background of fibrous stroma cells within the islands – PAVING STONE APPEARANCE.

● Cells – round, plump and active little immature matrix is present.
● Pericellular lattice-like fine calcification – “CHICKEN WIRE” or “PICKET FENCE” pattern are seen.
● Small granular purplish areas of microcalcification.
● Multinucleated Giant cells – scattered in stroma.
● Often prominent, dilated blood vessels at centre & periphery are present.

DIFFERENTIAL DIAGNOSIS● Enchondroma
Hand, diaphysis.
● G.C.T.
Eccentrical, soap bubble or trabecular pattern
No calcifications
Often after closure of growth plate.
● Central chondrosarcoma Slow growth, severe pain & margins not demarcated on xrays.

● Chondromyxoid fibroma
Site- Metadiaphysis
Septae are present.

TREATMENT AND PROGNOSIS● Curettage and autologous bone grafting – high recurrence rate (10 –
35%).● Close follow up & observation for all till skeletal maturity – in
patients , whose potential growth is remaining and lesions abuts the epiphyseal plate, lesions should be followed up and observed, instead of premature or aggressive treatment
● Marginal extra capsular excision – when growth plate not at all at risk, curettage and excision is done.
Defect can be obliterated with Autogenous bone graft.

● Methacrylate adjunct – when excision impractical & intracapsular curettage is of high risk of recurrence due to surgical inaccessibility.
● Curettage followed by cryosurgery:
>In case of recurrence or when associated with ABC.
>Yields consistent good results with a high cure rate when entire tumor is adequately frozen by liquid nitrogen.

Radiosensitivity:● Radiosensitive tumor● Not used for uncomplicated cases – potential hazards
of irradiation induced malignant transformation.

OSTEOBLASTOMA

INTRODUCTION● Jaffe and lichtenstein first described it in 1956.● Rare bone tumor, ● 1 % of all primary bone tumors● 3 % of benign bone tumors. It is a Solitary benign progressively growing bone tumor histologically similar to osteoid osteoma , size, clinical and radiological features differentiate it.

AGE● Young person 10 to 30 years (80%)
SEX● Males: female -3:1.

SITE
Vertebral Column 34 %
Extremities 30%
Hands and feet 14%
Skull and facial bones 15 %

● In long bones it occurs in medullary portion of metaphysis. Rarely juxtacortical or periosteal osteoblastomas are reported.
● In Spine- spinous and transverse process are frequently involved. lesions in body are rare.

Clinical features● Pain- Dull , aching, persistent and localized.● Slight local tenderness and palpable swelling of increasing
size.● spinal location > radiculopathy(50%).
>rarely produce neurological symptoms . >scoliosis and muscle spasm may appear.
● lesions of extremities may present with wasting and limp.

RADIOLOGICAL FEATURES
● lesion is well circumscribed, radiolucent, eccentric and with an intact surrounding shell of bone .
● centrally there is lytic area >2cm with surrounding sclerosis.

● In vertebrae it is seen as definitely expansile radiolucent growth containing granular radiopacities
● ct scans are better appreciated for vertebral lesions

CT SCAN.
● it can show cotton wool appearance when calcification of tumor tissue has occured...if cotton wool appearance is seen in lesion...it is diagnostic.

PATHOLOGYGROSS● well circumscribed, 2-10 cm.● surrounded by shell of cortical bone or thickened
periosteum.● Haemorrhagic, granular , friable and calcified
lesions.

HISTOPATHOLOGY•Vascular spindle-cell stroma with abundant irregular spicules of mineralized bone and Osteoid

DIFFERENTIAL DIAGNOSISOSTEOBLASTOMA OSTEOID OSTEOMA
1. INCIDENCE one fifth as common as osteoid osteoma
10% of benign bone tumor
2. COMMONEST LOCATION Vertebral column, often posterior element
Proximal femur
3.CLINICAL PRESENTATION Pain inconsistent pain persistent , nocturnal
4. RADIOGRAPHY Size > 2 cm no or minimal perifocal osseous reaction
size < 2cm, perifocal osseous reaction is marked.
5.HISTOLOGY>Osteoid trabeculae with discontinuous and irregular bone formation,> abundant fibrous stromal reaction,>many multinucleated osteoblastic giant cells
>osteoid trabaculae with continuous and regular bone formation.>Scanty stromal reaction>multinucleated osteoblastic giant cells are rare.

● OSTEOSARCOMANo ALP rise in osteoblastoma, stromal cells are not large, but are relatively uniform.
● GCT>>more than half are located near knee, or distal radius.>>soap bubble appearance.

TREATMENT● Curettage and resection.● bone grafting of defect.● In spine- if resection causes instability,
instrumented fusion can be necessary.● Radiation- some authors have recommended,
adjuvant radiation therapy for spinal lesions, as revision surgery is difficult.

CHONDROMYXOID FIBROMA

INTRODUCTION
● Rare tumour, least common benign cartilaginous tumors.
● Can be misdiagnosed as chondrosarcoma...as it is composed of similar cytological features, however radiological and clinical findings are of benign tumor .

AGE● 2nd and 3rd decade, rare in children.SEX● No predominance.LOCATION● metaphyseal region of large tubular bones.
(eccentric)● can also involve thin tubular bones- fibula,
phalanx and calcaneus.(usually entire width)

CLINICAL PICTURE● In young adults tumor causes mild or no pain,
slowly increasing local swelling and palpable tender tumor.
● Rarely metastasizes
● In less than 10 years age group- symptoms are more pronounced.

RADIOLOGICAL FINDINGSXRAY
● in long bones
>>Lesion -translucent mass of variable sizes , located eccentrically in metaphysis
>> on medullary aspect of lesion- margin is scalloped and sclerosed.
>>Cortex - Expanded and thinned out, may appear interrupted.

● in case narrow tubular bone (fibula) or small tubular bone (phalanx)- generally entire width of bone is involved
● fusiform expansion and thinning of both cortices.

PATHOLOGY GROSS
● Outer surface- covered by thin shell of newly formed periosteal bone.
● Cut Surface-solid tumor mass of greyish white or bluish grey color,resembles cartilage and sometimes contain cavities of mucoid tissue
● consistency - usually firm.● Calcified areas are unusual.● no bony septa traverse the tumor.

MICROSCOPIC•Tumor is composed of lobulated and pseudo lobulated areas of stellate cells with indistinct cytoplasmic borders,lying within the central portion of lobule and widely separated by mucin like material.

TREATMENT● Curettage is not sufficient, as tumor may recur.● En Bloc excision and filling cavity with
autogenous bone results in high rate of cure.● Despite Wide excision , if tumor recurs then
additional studies should be done to rule out malignant transformation.

Curettage and Bone cementing

LANGERHANS CELL HISTIOCYTOSIS

● Previously called HISTIOCYTOSIS X
● Characterised by widespread dissemination of reticuloendothelial system.
● Syndrome constitutes following clinical conditions 1. Eosinophilic Granuloma
2. Hand -Schuller -Christian disease
3. Letterer -Siwe disease.

Orthopaedic surgeon is primarily concerned with EOSINOPHILIC GRANULOMA OF BONE

EOSINOPHILIC GRANULOMA
● Self limited benign bone destructive lesion characterised by histocytic and eosinophilic leucocyte infiltration.
Incidence● Usually in first two decades with peak incidence in 5 to 10 years group.● solitary lesion usually seen in ribs vertebrae, skull, flat bones and long
tubular bones.● multiple lesions are rare - ocurrance in skull and femur● diaphysis and metaphysis are commonly involved.

Clinical Picture
● Acute onset● complains of dull aching pain in a limited local area of bone.● local tenderness , warmth and swelling over the affected bone.● pathological fracture of long bone or vertebral collabs can be
seen.● Disease usually progress for few weeks to few months , and
recovery is usually spontaneous

RADIOGRAPHY● Rapidly destructive lytic process
producing punched out appearance

● In diaphysis of long bones lesions may have aggressive permeative appearance with periosteal reactive bone formation.

● Eosinophilic granuloma of vertebral body
● showing marked flattening of vertebral body or vertebral plana

Histopathology
•Diagnosis is made by identification of langerhans cell.
•Mixture of eosinophils, plasma cells, histiocytes along with peculiar large mononuclear giant cells (Langerhans cells) with abundant pale cytoplasm and cleaved nuclei.
•Necrosis, fibrosis and reactive cells are evident

TREATMENT
● Microscopically diagnosis is made by identification of langerhans cell.
● Recommended treatments incd- >> corticosteroid infiltrations >> radiation therapy >> Curettage with or without bone grafting.

Hand schuller - christian disease

REFRENCES
1. ORTHOPAEDICS PRINCIPLES AND THEI APPLICATION: SAMUEL L TURES
2. CAMPBELLS OPERATIVE ORTHOPAEDICS
3. TEXTBOOK OF ORTHOPAEDICS AND TRAUMA - GS KULKARNI
4. J.B.JS.