Embed Size (px)
Citation preview
Dr. José Antonio García Erce Hematología y HemoterapiaHospital de San Jorge, Huesca (España)[email protected]
IV Curso Medicina Transfusional Ahorro de sangre en cirugía
ANEMIA. EVALUACIÓN PREOPERATORIA Y TRATAMIENTO. HIERRO IV
AUMENTO DE MASA ERITROCITARIA. ERITROPOYETINA
José Antonio García-Erce Servicio de Hematología y Hemoterapia
Hospital “San Jorge”, Huesca.

José Antonio García-Erce Servicio de Hematología y Hemoterapia
Hospital “San Jorge”, Huesca.
www.awge.org
Declaración de Conflicto de intereses
Asesor externo - AMGEN Oncología 2010- Roche Anemia 2009- Ditassa-Ferrer 2004
Charlas, estudios investigación y ayudas a congresos-Vifor-Uriach/Ferralinze-Janssen-Cilag-Astra-Tech de Aztra Zeneca-Sanofi Aventis/Esteve-Cobe-Caridian/Roche OncologíaMiembro del CAT 2002-2005Miembro del Documento de Sevilla “Alternativas a la Transfusión”Miembro del Documento LatinoAmericano de la AnemiaMiembro de GIEMSA/ Secretario AWGE/Socio SETS/AEHH/NATAEditor Asociado Revista ANEMIA www.revistaanemia.orgMiembro Comité Científico NATA y TATM
Documentos de Consensos

Agradecimientos
Prof. Manolo Muñoz GómezGIEMSA. Facultad de Medicina. Universidad de Málaga
Dr. Jorge Cuenca EspiérrezDepartment of Orthopaedic SurgeryUniversity Hospital Miguel Servet, Zaragoza
Prof. Antonio Herrera RodríguezCátedra Department of Orthopaedic SurgeryUniversity Hospital Miguel Servet, Zaragoza
Dra. Elvira BisbeDepartment of Anaesthesiology. University Hospital Mar-Esperança, Barcelona
www.awge.org
www.awgla.com
www.revistanemia.org
ANEMIA. EVALUACIÓN PREOPERATORIA Y
TRATAMIENTO.
www.awge.org
¿QUÉ ES LA ANEMIA?
AUMENTO DE MASA ERITROCITARIA

Anemia yenfermedad
Primer signo de una enfermedad más grave
LA ANEMIA LA ANEMIA PUEDE SER EL PRIMER PUEDE SER EL PRIMER
SIGNO de un paciente conSIGNO de un paciente con::
- ÚLCERA- MIOMA- CELAQUIA- CÁNCER- INSUFICIENCIA RENAL- INSUFICIENCIA CARDÍACA- APLASIA MÉDULA- INFECCIÓN- INTOXICACIÓN
Anemia y peorpronóstico de muchas enfermedades
Anemia del paciente con:
- CÁNCER- INSUFICIENCIA CARDÍACA - CIRUGÍA TRAUMATOLÓGICA- CIRUGÍA CARDÍACA- DIABETES- INSUFICIENCIA RENAL- TRANSPLANTE RENAL
Errores, falacias y otras leyendas urbanas
ANEMIA. EVALUACIÓN PREOPERATORIA Y
TRATAMIENTO.
www.awge.org
¿ES FRECUENTE LA ANEMIA?
AUMENTO DE MASA ERITROCITARIA

Prevalencia de anemia
Errores, falacias y otras leyendas urbanas

Prevalencia de anemia
Errores, falacias y otras leyendas urbanas
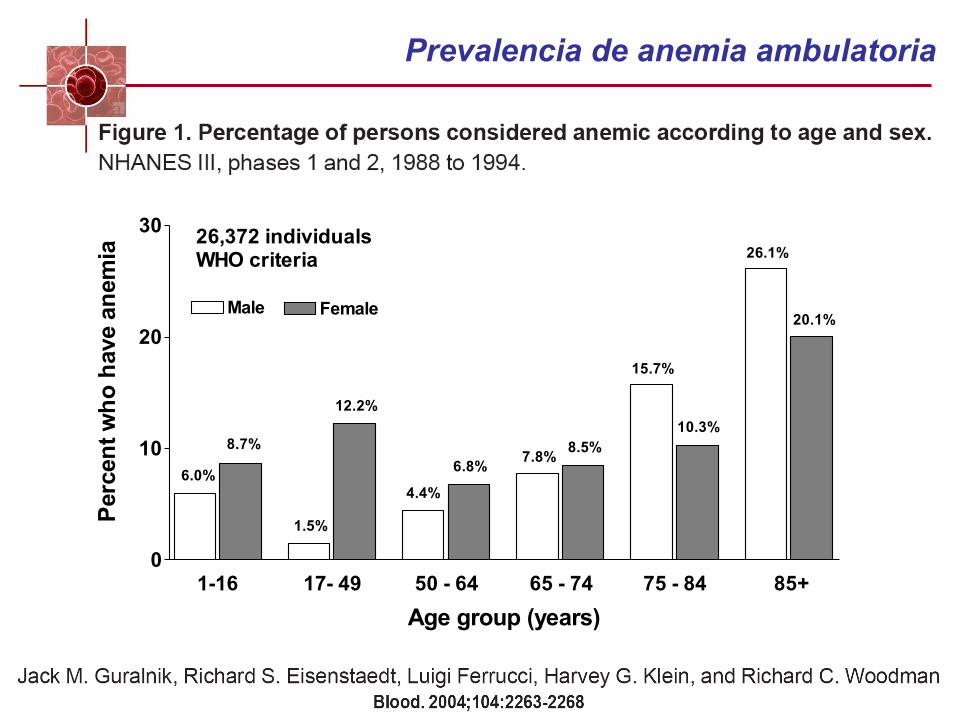
1.0 2.0 3.0 4.0 5.0 6.00
10
20
30
Male Female
6.0%
8.7%
1.5%
12.2%
4.4%
6.8%7.8%
8.5%
15.7%
10.3%
26.1%
20.1%
1-16 17- 49 50 - 64 65 - 74 75 - 84 85+
Age group (years)
Per
cen
t w
ho
hav
e an
emia
26,372 individualsWHO criteria
Prevalencia de anemia ambulatoria
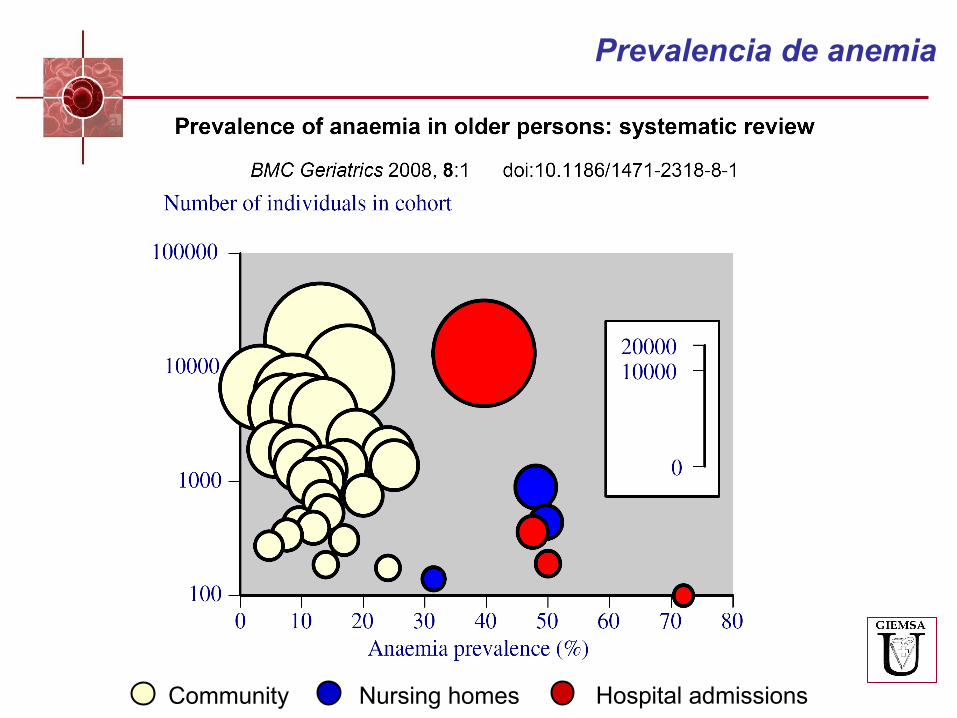
Community Nursing homes Hospital admissions
Prevalencia de anemia

Wen-Chih Wu et al. JAMA 2007; 297: 2481 – 2488
Haematocrit < 39% Procedure Patients (n) n % General surgery 106 340 45 478 42.8 Urology 59 157 21 408 36.2 Orthopaedics 57 636 25 131 43.6 Periferic vascular 47 734 24 865 52.1 Thoracic 14 051 6 780 48.3 Others 25 393 9 308 36.7 Overall 310 311 132 970 42.8
Incidencia de la anemia perioperatoria

Prevalencia de anemia en cáncer
N = 14 912*Hb <12 g/dL al reclutamiento
Ludwig et al. Eur J Cancer 2004;40:2293-306.
Patients with anaemia* (%)
Lymphoma/ myeloma
Head and neck
0 20 40 60
Urogenital
Leukaemia
Gynaecological
GI-colorectal
Lung
Breast 30%
38%
39%
25%
49%
53%
53%
29%
EUROPEAN CANCER ANAEMIA SURVEY (ECAS)

Prevalencia de anemia preoperatoria
Puntos clave:
• Entre el 20% y el 75% de los pacientes quirúrgicos pueden presentar anemia preoperatoria debido a su patología quirúrgica o a otras patologías.

ANEMIA. EVALUACIÓN PREOPERATORIA Y
TRATAMIENTO.
www.awge.org
¿CÓMO SE PRODUCE LA ANEMIA?
AUMENTO DE MASA ERITROCITARIA
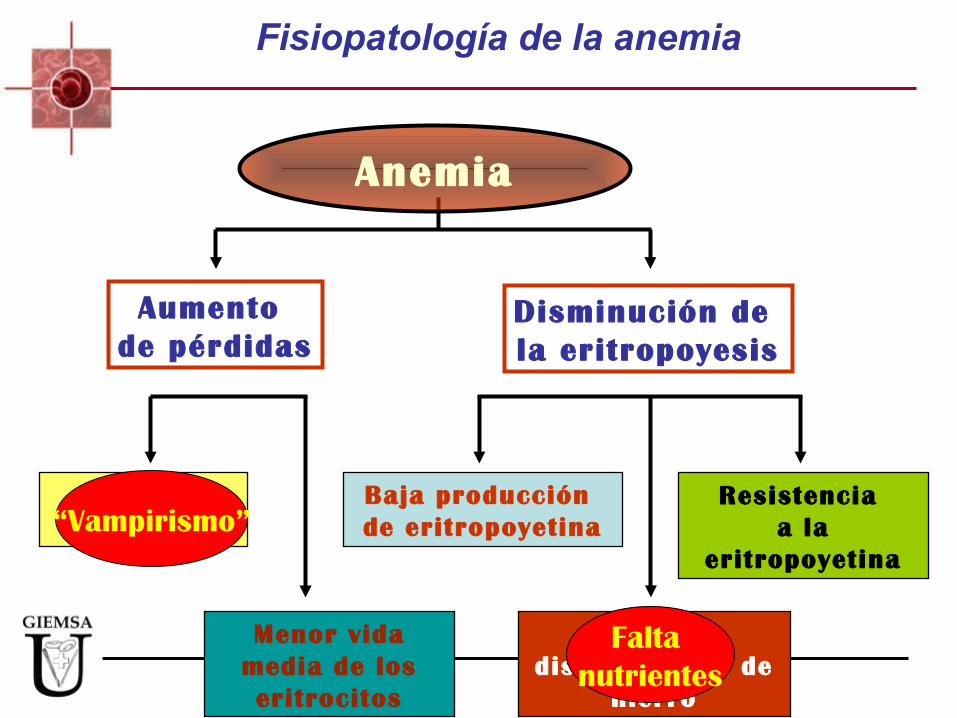
Anemia
Pérdidasde sangre
Menor vida media de los eritrocitos
Baja producción de eritropoyetina
Resistencia a la
eritropoyetina
Baja disponibilidad de
hierro
Aumento de pérdidas
Disminución de la eritropoyesis
“Vampirismo”
Falta nutrientes
Fisiopatología de la anemia

20-30mg/día
Músculo(250 mg)
Médula ósea(300 mg)
Eritrocitos(2.000 mg)
Macrófagos SRE(500 mg)
Hígado(1000 mg)
Absorción intestinal de hierro(1-2 mg/día)
Transferrina(3 mg)
Pérdidas de hierro(1-2 mg/día)
Fisiopatología de la anemia ferropénica

Definición de AnemiaDiagnóstico de la anemia
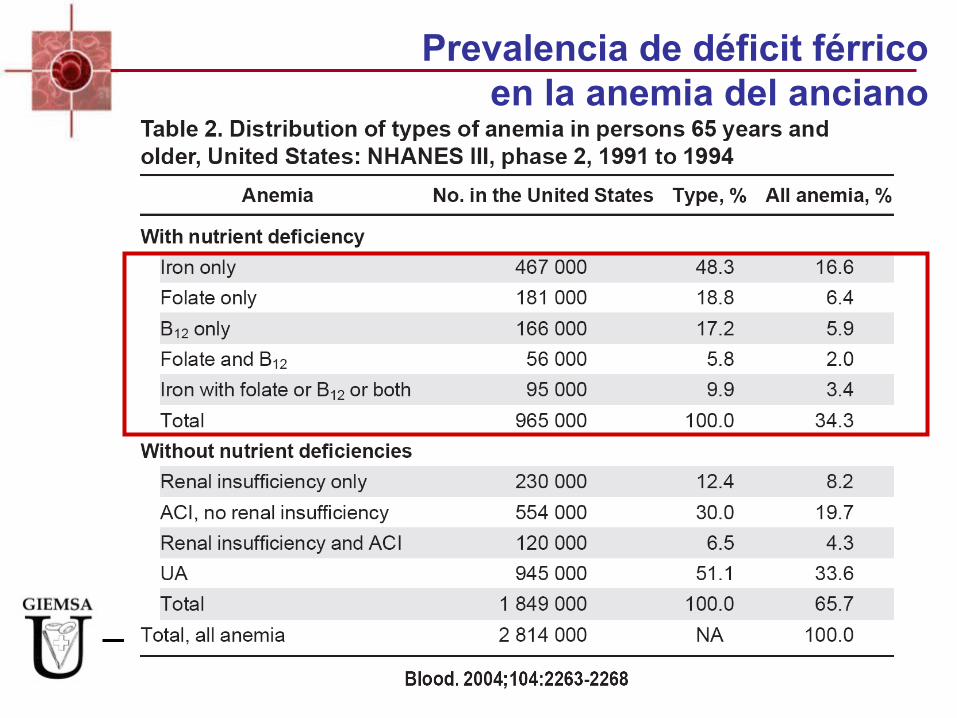
Prevalencia de déficit férricoen la anemia del anciano
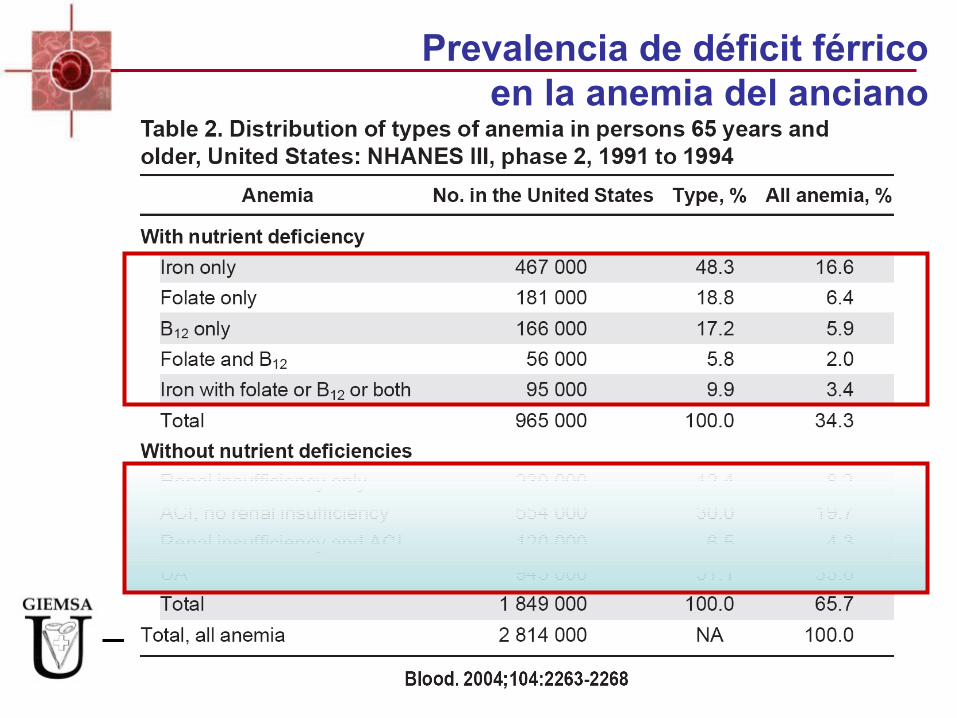
Prevalencia de déficit férricoen la anemia del anciano
ANEMIA. EVALUACIÓN PREOPERATORIA Y
TRATAMIENTO.
www.awge.org
ANEMIA Y/O FERROPENIA
AUMENTO DE MASA ERITROCITARIA
Anemia ferropénicaDatos epidemiológicos
• Prevalencia: – Anemia ferropénica: ¼ población mundial (2.000 millones en todo mundo)– Déficit de hierro: 1/3 población mundial– 2-5 % chicas adolescentes en EEUU anemia ferropénica.
– > 10% mujeres españolas (Cataluña) con ferropenia
• Etiología de la anemia ferropénica– Mujer fértil causa más frecuente: ginecológica.– Causa más frecuente global: pérdida hemática digestiva.
** Hasta 1/3 de pacientes con Enfermedad de Crohn, tienen anemia (mala tolerancia a hierro oral).
www.awge.org
Errores, falacias y otras leyendas urbanas
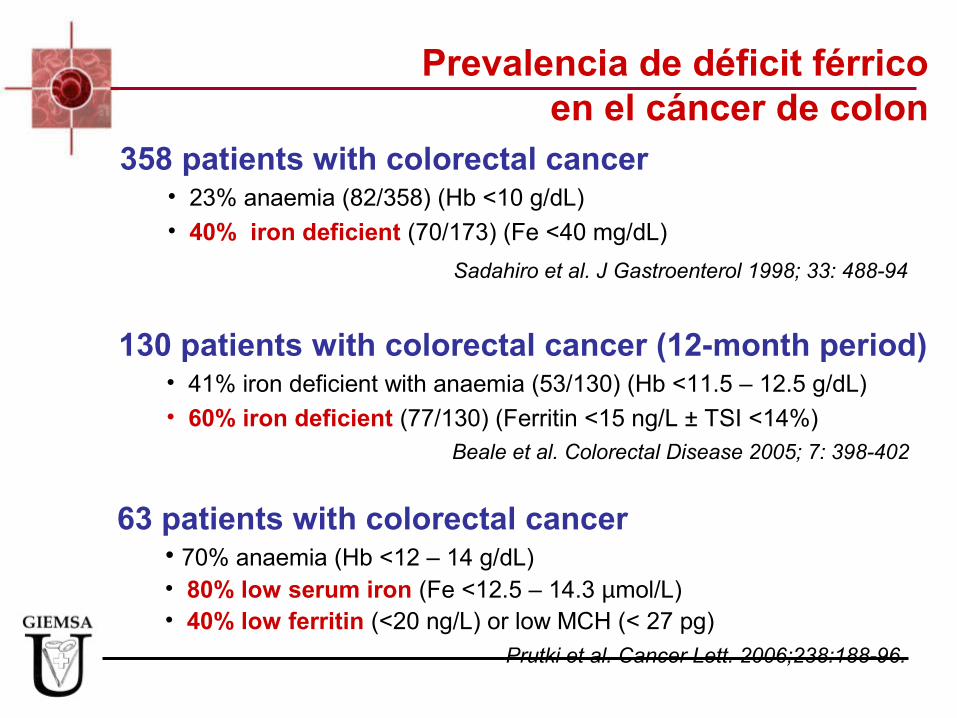
Prevalencia de déficit férricoen el cáncer de colon
130 patients with colorectal cancer (12-month period)• 41% iron deficient with anaemia (53/130) (Hb <11.5 – 12.5 g/dL)• 60% iron deficient (77/130) (Ferritin <15 ng/L ± TSI <14%)
Beale et al. Colorectal Disease 2005; 7: 398-402
358 patients with colorectal cancer • 23% anaemia (82/358) (Hb <10 g/dL)• 40% iron deficient (70/173) (Fe <40 mg/dL)
Sadahiro et al. J Gastroenterol 1998; 33: 488-94
63 patients with colorectal cancer• 70% anaemia (Hb <12 – 14 g/dL)• 80% low serum iron (Fe <12.5 – 14.3 µmol/L)• 40% low ferritin (<20 ng/L) or low MCH (< 27 pg)
Prutki et al. Cancer Lett. 2006;238:188-96.
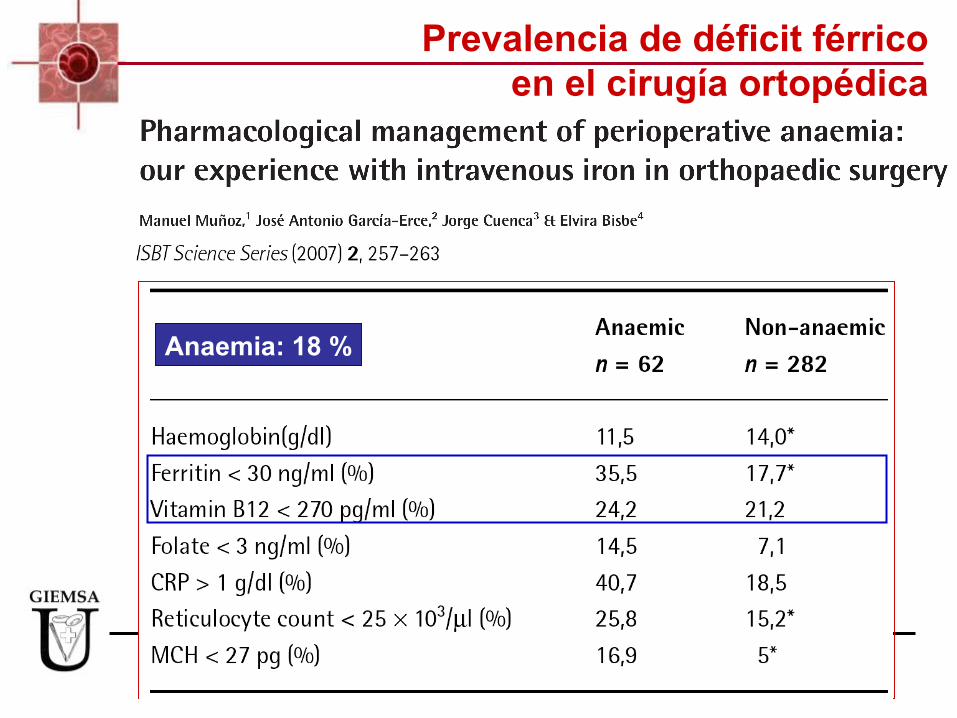
Anaemia: 18 %
Prevalencia de déficit férricoen el cirugía ortopédica
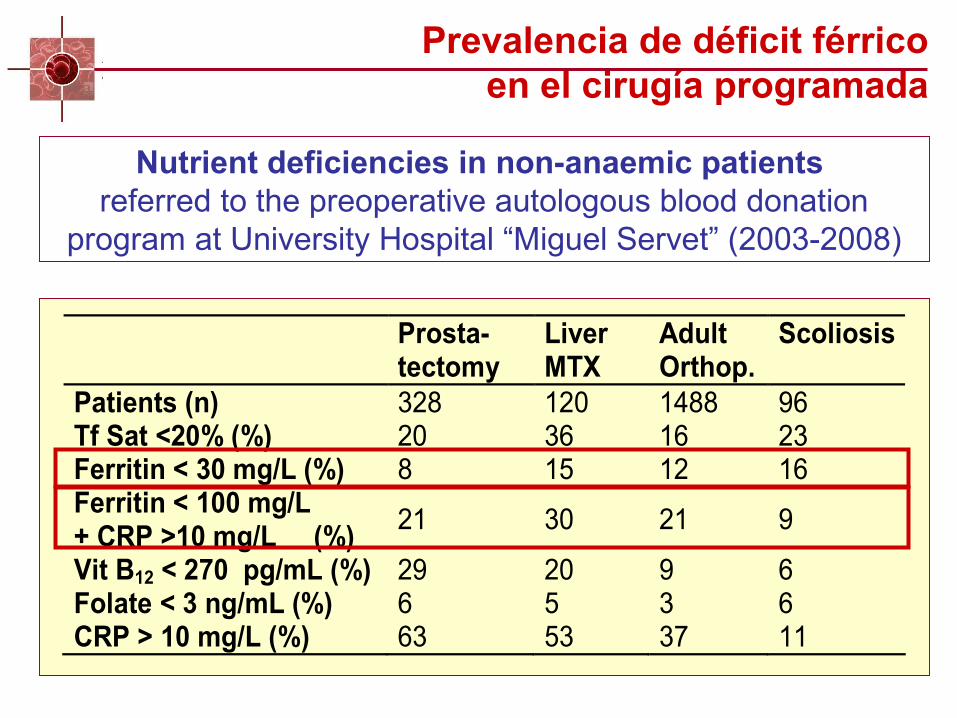
Nutrient deficiencies in non-anaemic patients referred to the preoperative autologous blood donation
program at University Hospital “Miguel Servet” (2003-2008)
Prosta-tectomy
Liver MTX
Adult Orthop.
Scoliosis
Patients (n) 328 120 1488 96 Tf Sat <20% (%) 20 36 16 23 Ferritin < 30 mg/L (%) 8 15 12 16 Ferritin < 100 mg/L + CRP >10 mg/L (%)
21 30 21 9
Vit B12 < 270 pg/mL (%) 29 20 9 6 Folate < 3 ng/mL (%) 6 5 3 6 CRP > 10 mg/L (%) 63 53 37 11
Prevalencia de déficit férricoen el cirugía programada

ANEMIA. EVALUACIÓN PREOPERATORIA Y
TRATAMIENTO.
www.awge.org
RIESGOS DE LA ANEMIA
AUMENTO DE MASA ERITROCITARIA

0%10%20%30%40%50%60%70%80%90%
TRANSFUSIÓN
Hb<120 G/L Hb 120-140 G/L Hb> 140 G/L
García-Erce JA, Solano VM, Cuenca J, Ortega P. “LA HEMOGLOBINA PREOPERATORIA COMO ÚNICO FACTOR PREDICTOR DE LAS NECESIDADES TRANSFUSIONALES EN LA ARTROPLASTIA DE RODILLA”. Rev Esp Anestesiol Reanim 2002; 49: 131-5
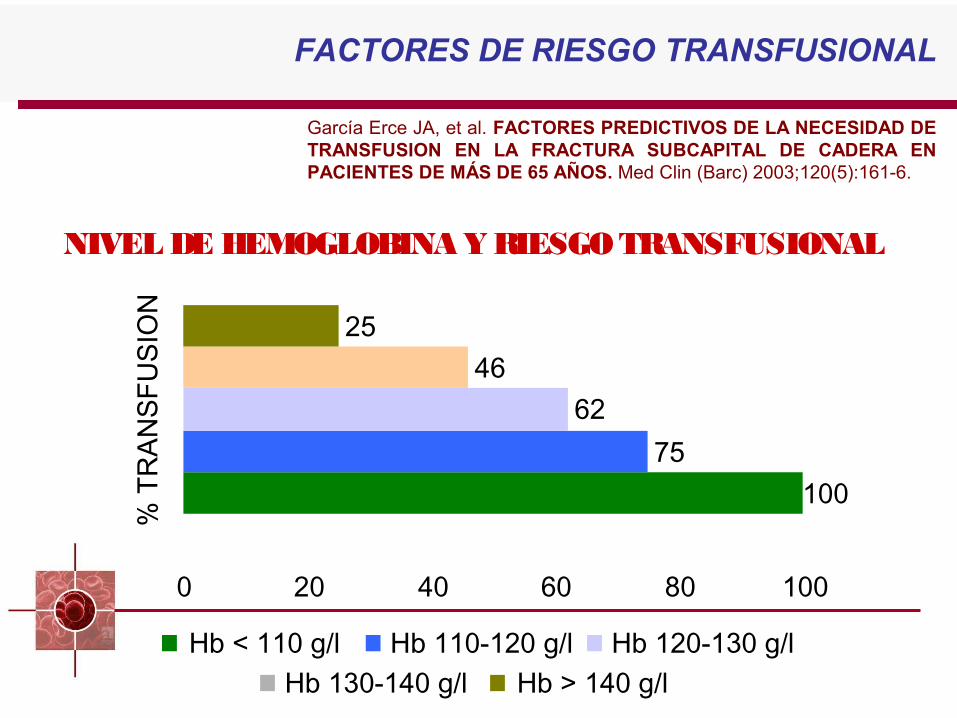
NIVEL DE HEMOGLOBINA Y RIESGO TRANSFUSIONAL
FACTORES DE RIESGO TRANSFUSIONAL
Hb 130-140 g/l
10075
6246
25
0 20 40 60 80 100
% T
RA
NSF
USI
ON
Hb < 110 g/l Hb 110-120 g/l Hb 120-130 g/lHb > 140 g/l
García Erce JA, et al. FACTORES PREDICTIVOS DE LA NECESIDAD DE TRANSFUSION EN LA FRACTURA SUBCAPITAL DE CADERA EN PACIENTES DE MÁS DE 65 AÑOS. Med Clin (Barc) 2003;120(5):161-6.
NIVEL DE HEMOGLOBINA Y RIESGO TRANSFUSIONAL
FACTORES DE RIESGO TRANSFUSIONAL
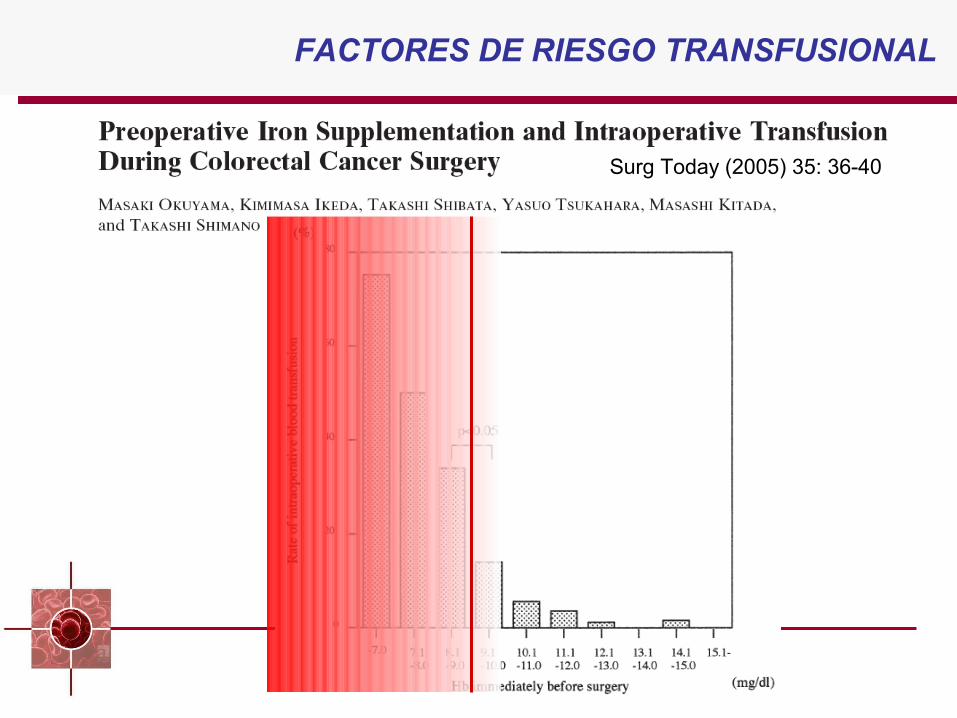
Surg Today (2005) 35: 36-40
FACTORES DE RIESGO TRANSFUSIONAL
Hem
og
lob
ina
(g/d
L)
10
13
16
7
4
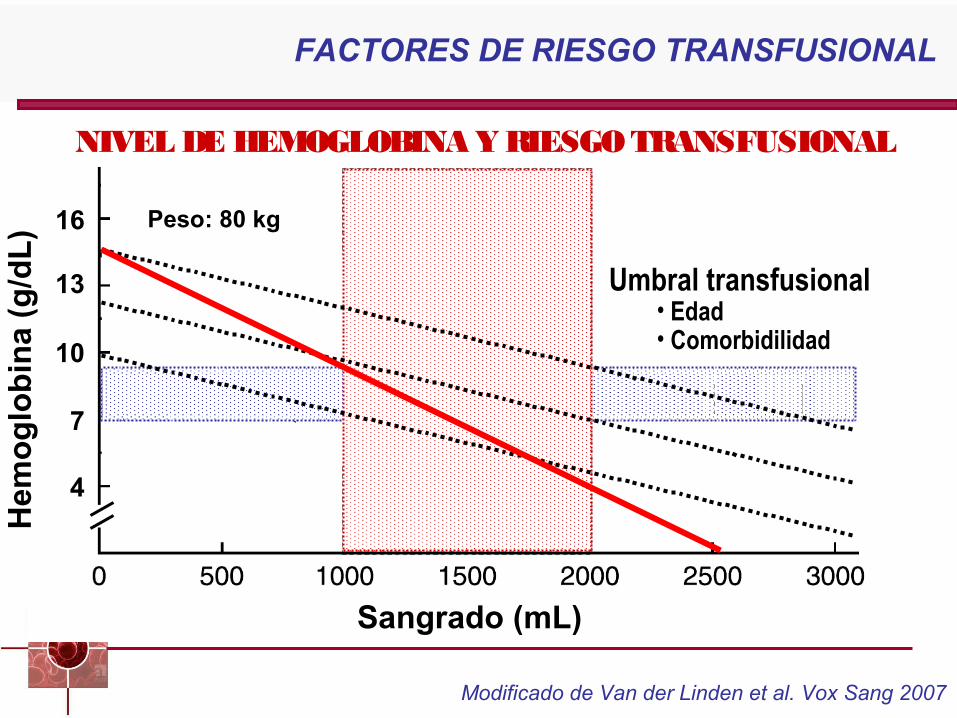
Sangrado (mL)
Umbral transfusional• Edad• Comorbidilidad
Peso: 80 kg
Modificado de Van der Linden et al. Vox Sang 2007
NIVEL DE HEMOGLOBINA Y RIESGO TRANSFUSIONAL
FACTORES DE RIESGO TRANSFUSIONAL

Prevalencia de anemia preoperatoria
Puntos clave:
• Entre el 20% y el 75% de los pacientes quirúrgicos pueden presentar anemia preoperatoria debido a su patología quirúrgica o a otras patologías.
• En el paciente quirúrgico, la anemia preoperatoria se asocia con un mayor riesgo de TSA (La Hb es el principal factor predictor de la necesidad de TSA)
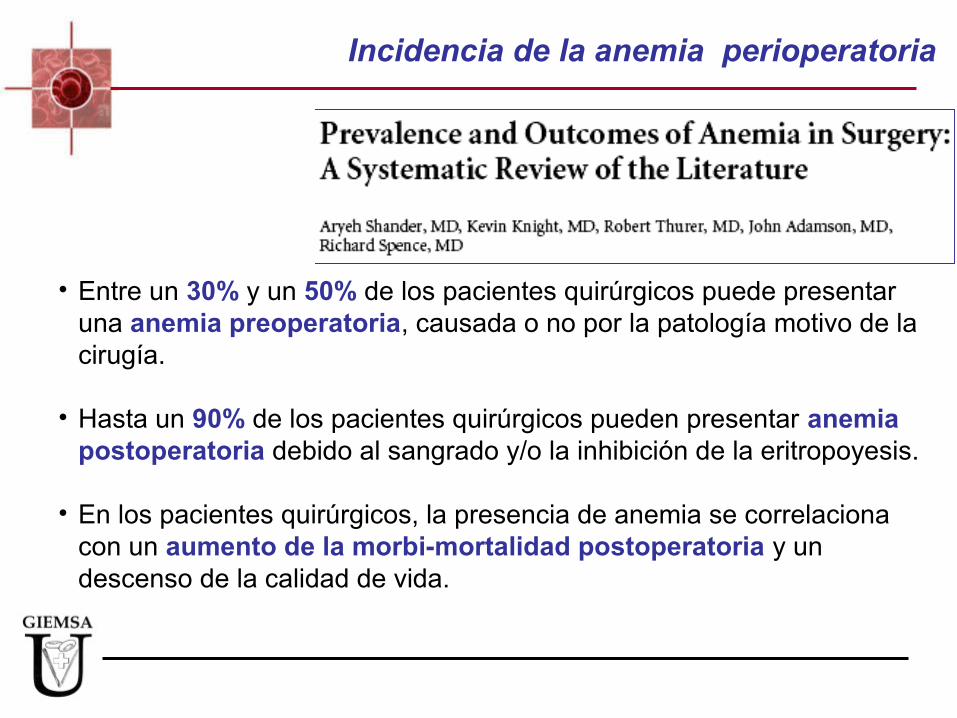
• Entre un 30% y un 50% de los pacientes quirúrgicos puede presentar una anemia preoperatoria, causada o no por la patología motivo de la cirugía.
• Hasta un 90% de los pacientes quirúrgicos pueden presentar anemia postoperatoria debido al sangrado y/o la inhibición de la eritropoyesis.
• En los pacientes quirúrgicos, la presencia de anemia se correlaciona con un aumento de la morbi-mortalidad postoperatoria y un descenso de la calidad de vida.
Incidencia de la anemia perioperatoria
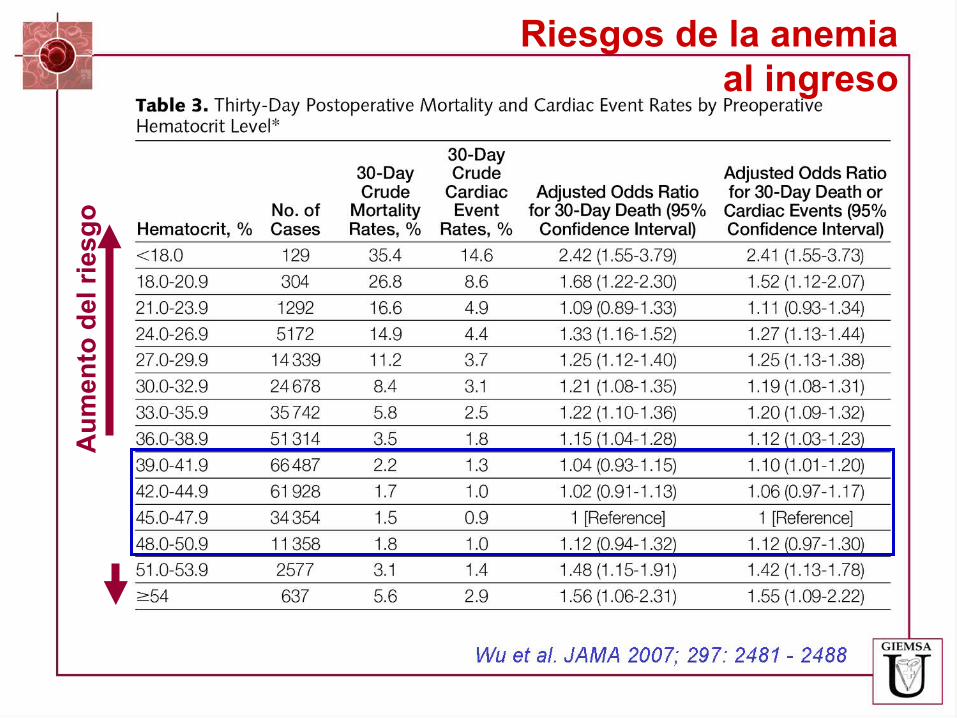
Au
men
to d
el r
ies
go
Riesgos de la anemiaal ingreso
Prevalencia de anemia preoperatoria
Puntos clave:
• Entre el 20% y el 75% de los pacientes quirúrgicos pueden presentar anemia preoperatoria debido a su patología quirúrgica o a otras patologías.
• En el paciente quirúrgico, la anemia preoperatrioa se asocia con un mayor riesgo de TSA (La Hb es el principal factor predictor de la necesidad de TSA)
• Además, en estos pacientes la anemia se asocia con un mayor tasa de morbimortalidad postoperatoria y con un descenso en la calidad de vida.
www.awge.org
¿CÓMO TRATAR LA ANEMIA?
La transfusión como tratamiento estándar de la
hemorragia grave
AUMENTO DE MASA ERITROCITARIA
Compromisodel aporte de
oxígeno
TransfusionalInstaurar
tratamiento
ANEMIA
Tratamiento de la anemia
www.awge.org
¿POR QUÉ SE TRANSFUNDE?
¿POR QUÉ SE DEBERÍA TRANSFUNDIR?
La transfusión como tratamiento estándar de la
hemorragia grave
AUMENTO DE MASA ERITROCITARIA
CRITERIOS TRANSFUSIONALESAABT
John S. Lundy, MD. Anesthesiologist who set upthe Mayo Clinic Blood Bank in 1935
Lund with an anesthesia colleague, R Charles Adams at Mayo Clinic, advocated the use of a hemoglobin trigger of 8 to 10 g% for patients considered to be of poor surgical risk.
Adams RC, Lundy JS: Anesthesia in cases of poor surgical risk. Some suggestions for decreasing the risk. Surg Gynecol Obstet 64:1011- 1019, 1942
Objetivo:•Corregir la hipoxia tisular
Medio:•Aumentar la capacidad de transporte de oxígeno de la sangre
Cuestiones a valorar:•Indicación de la tansfusión (riesgo/beneficio)•Cantidad a transfundir•Alternativas
Tratamiento transfusional

Criterios generales de indicación
Uso adecuado:•Presencia de signos o síntomas de hipoxia tisular•Ausencia de tratamiento específico de la anemia•Refractariedad al tratamiento específico•La situación clínica del paciente precisa una reposición inmediata de la masa eritrocitaria
Tratamiento transfusional
Criterios generales de indicación
Uso adecuado:•Presencia de signos o síntomas de hipoxia tisular•Ausencia de tratamiento específico de la anemia•Refractariedad al tratamiento específico•La situación clínica del paciente precisa una reposición inmediata de la masa eritrocitaria
Tratamiento transfusional
Compromisodel aporte de
oxígeno
TransfusionalInstaurar
tratamiento
ANEMIA
Tratamiento de la anemia
Transfusional
Problemas de la TSA
Regan y Taylor, BMJ 2002Shander, Semin Hematol 2004
Muñoz, 2007
Costes de producción elevados
Sangre humana: un recurso limitado
TSA no está libre de riesgos:
Errores de identificación
TRALI
Sobrecarga de fluidos (TACO)
Infección postoperatoria (TRIM)
Recidiva de cáncer (TRIM)
Legislación vigente
AUMENTO DE MASA ERITROCITARIA
Problemas de la TSA
Legislación vigente

Problemas de la TSA
12. Patients should be informed of the known risks and benefits of blood transfusion and/or alternative therapies and have the right to accept or refuse the procedure. Any valid advance directive should be respected.
Principle of patient’s autonomy
15. Genuine clinical need should be the only basis for transfusion therapy.
Ethical principles of beneficence and justice
Legislación vigente
Problemas de la TSA
Regan y Taylor, BMJ 2002Shander, Semin Hematol 2004
Muñoz, 2007
Costes de producción elevados
Sangre humana: un recurso limitado
TSA no está libre de riesgos:
Errores de identificación
TRALI
Sobrecarga de fluidos (TACO)
Infección postoperatoria (TRIM)
Recidiva de cáncer (TRIM)
Legislación vigente
Variabilidad
AUMENTO DE MASA ERITROCITARIA

www.awge.org
AUMENTO DE MASA ERITROCITARIA

Compromisodel aporte de
oxígeno
TransfusionalInstaurar
tratamiento
Farmacológico
Enfermedad
ANEMIA
Tratamiento de la anemia
Sustitutos
Transfusional

INTRODUCCIÓNFACTORES DE RIESGO TRANSFUSIONALANEMIA PREOPERATORIAMANEJO DE LA ANEMIA PREOPERATORIA
AUMENTO DE MASA ERITROCITARIA
“Lo primero que debemos hacer con un paciente quirúrgico es detectar la presencia de anemia y
determinar su causas con la suficiente antelación como para poder hacer algo con ella”
Goodnough LT et al . Anesth Analg 2005; 101: 1858-61
El tratamiento de la anemia preoperatoria ha demostrado ser eficaz para reducir los requerimientos transfusionales y mejorar la evolución postoperatoria y la calidad de vida de los pacientes quirúrgicos.
Shander A et al. Am J Med 2004; 116 (suppl 7A): 58S-69S.
Manejo de la anemia preoperatoria
NATA Expert Panel on Intravenous Iron
ANAEMIA MANAGEMENT IN SURGERY – CONSENSUS STATEMENT ON THE ROLE OF INTRAVENOUS IRON
Photis Beris, Manuel Muñoz, José A. García-Erce, Dafydd Thomas, Alice Maniatis & Philippe Van der Linden.
Modificado de Van der Linden et al. Vox Sang 2007
“Siempre que sea clínicamente factible, en los pacientes programados
para una cirugía con alto riesgo de desarrollar anemia postoperatoria
grave, se debería determinar la hemoglobina y el status férrico, al
menos 30 días antes de la intervención. En los pacientes >60 años,
se deberían determinar también los niveles de vitamina B12 y folatos”.
Manejo de la anemia preoperatoria
La correción de estas deficiencias es de capital importancia para:
• Optimizar los niveles preoperatorios de Hb, especialmente en los pacientes en tratamiento con agentes estimuladores de la eritropoyesis.
• Acelerar la recuperación de la anemia postoperatoria.
Manejo de la anemia preoperatoria
INTRODUCCIÓNFACTORES DE RIESGO TRANSFUSIONALANEMIA PREOPERATORIAMANEJO DE LA ANEMIA PREOPERATORIAALTERNATIVAS A LA TRANSFUSIÓN ALOGÉNICA
AUMENTO DE MASA ERITROCITARIA

AABTAlternativas a la
Transfusión Alogénica
Spanish Consensus Statement onAlternatives to Allogeneic Blood Transfusions
“An update of Seville’s Document”
11th Annual SymposiumBarcelone, Spain. April 8 - 9 , 2010
HS EH HS EH HS EH
AABT
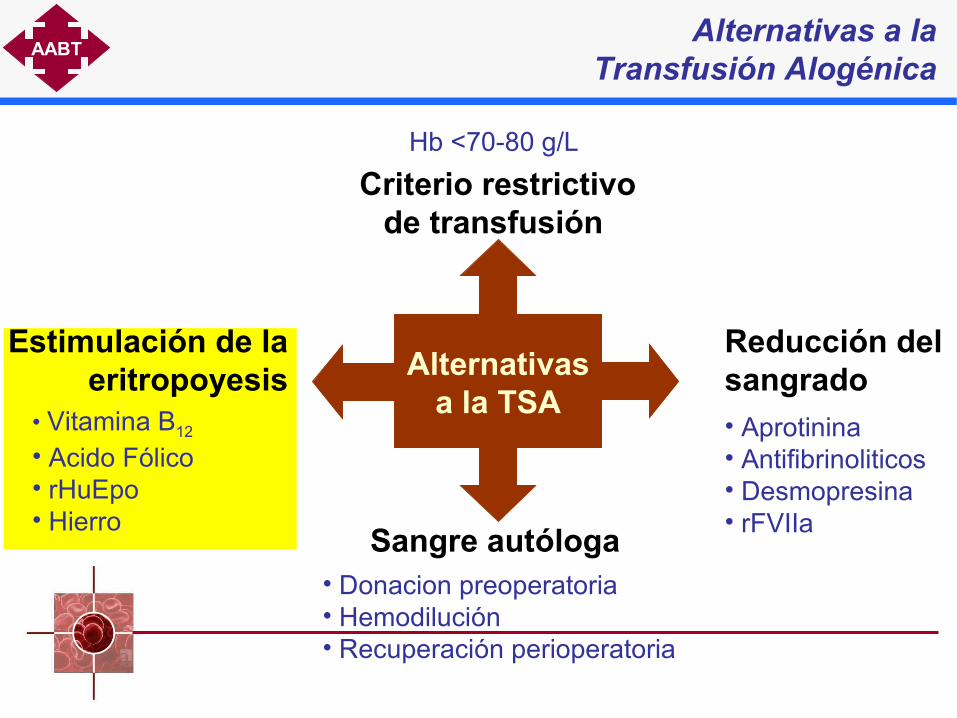
Sangre autóloga• Donacion preoperatoria• Hemodilución• Recuperación perioperatoria
Criterio restrictivode transfusión
Hb <70-80 g/L
Reducción del sangrado• Aprotinina• Antifibrinoliticos• Desmopresina• rFVIIa
Estimulación de la eritropoyesis
• Vitamina B12 • Acido Fólico• rHuEpo• Hierro
Alternativasa la TSA
Alternativas a la Transfusión Alogénica

Estimulación de la eritropoyesis
- Hierro (enteral o parenteral)(oral y ev)- Agentes Estimulantes de la Eritropoyesis (rHuEpo y darbopetina) (ESAs)- Vitamina B12 - Acido Fólico - Otras vitaminas- Andrógenos
AUMENTO DE MASA ERITROCITARIA
Estimulación de la eritropoyesis
- Hierro (enteral o parenteral)(oral y ev)- Agentes Estimulantes de la Eritropoyesis (rHuEpo y darbopetina) (ESAs)- Vitamina B12 - Acido Fólico - Otras vitaminas- Andrógenos
AUMENTO DE MASA ERITROCITARIA
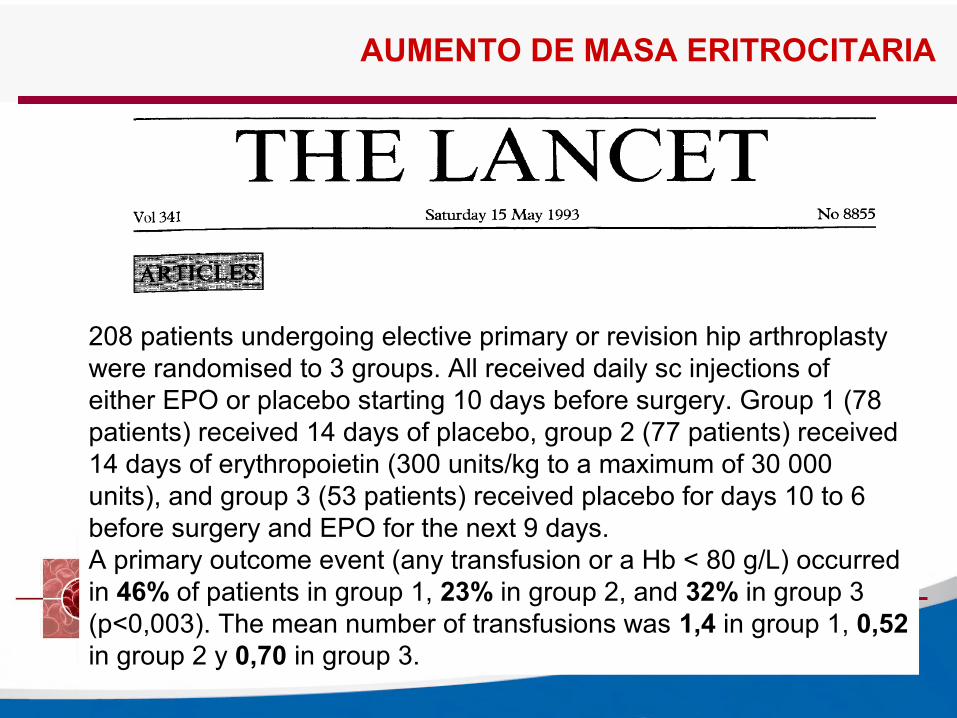
208 patients undergoing elective primary or revision hip arthroplasty were randomised to 3 groups. All received daily sc injections ofeither EPO or placebo starting 10 days before surgery. Group 1 (78 patients) received 14 days of placebo, group 2 (77 patients) received 14 days of erythropoietin (300 units/kg to a maximum of 30 000 units), and group 3 (53 patients) received placebo for days 10 to 6 before surgery and EPO for the next 9 days. A primary outcome event (any transfusion or a Hb < 80 g/L) occurred in 46% of patients in group 1, 23% in group 2, and 32% in group 3 (p<0,003). The mean number of transfusions was 1,4 in group 1, 0,52 in group 2 y 0,70 in group 3.
AUMENTO DE MASA ERITROCITARIA

Administración de EPO
EPOControl
Reducción del 73% en la tasa de transfusión
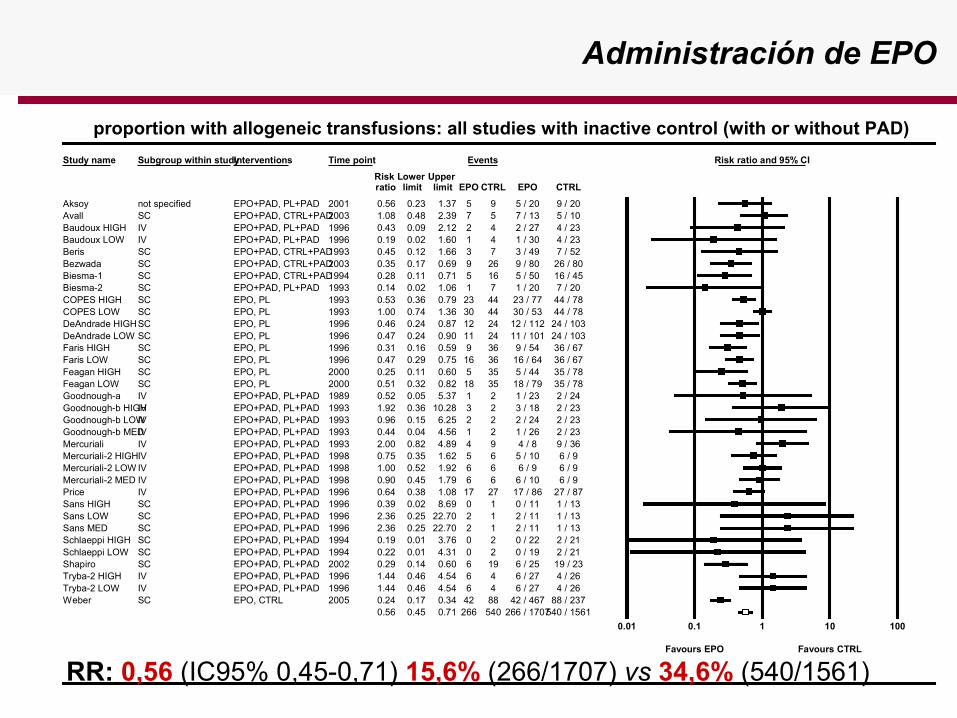
Study name Subgroup within studyInterventions Time point Events Risk ratio and 95% CI
Risk Lower Upper ratio limit limit EPO CTRL EPO CTRL
Aksoy not specified EPO+PAD, PL+PAD 2001 0.56 0.23 1.37 5 9 5 / 20 9 / 20Avall SC EPO+PAD, CTRL+PAD2003 1.08 0.48 2.39 7 5 7 / 13 5 / 10Baudoux HIGH IV EPO+PAD, PL+PAD 1996 0.43 0.09 2.12 2 4 2 / 27 4 / 23Baudoux LOW IV EPO+PAD, PL+PAD 1996 0.19 0.02 1.60 1 4 1 / 30 4 / 23Beris SC EPO+PAD, CTRL+PAD1993 0.45 0.12 1.66 3 7 3 / 49 7 / 52Bezwada SC EPO+PAD, CTRL+PAD2003 0.35 0.17 0.69 9 26 9 / 80 26 / 80Biesma-1 SC EPO+PAD, CTRL+PAD1994 0.28 0.11 0.71 5 16 5 / 50 16 / 45Biesma-2 SC EPO+PAD, PL+PAD 1993 0.14 0.02 1.06 1 7 1 / 20 7 / 20COPES HIGH SC EPO, PL 1993 0.53 0.36 0.79 23 44 23 / 77 44 / 78COPES LOW SC EPO, PL 1993 1.00 0.74 1.36 30 44 30 / 53 44 / 78DeAndrade HIGHSC EPO, PL 1996 0.46 0.24 0.87 12 24 12 / 112 24 / 103DeAndrade LOW SC EPO, PL 1996 0.47 0.24 0.90 11 24 11 / 101 24 / 103Faris HIGH SC EPO, PL 1996 0.31 0.16 0.59 9 36 9 / 54 36 / 67Faris LOW SC EPO, PL 1996 0.47 0.29 0.75 16 36 16 / 64 36 / 67Feagan HIGH SC EPO, PL 2000 0.25 0.11 0.60 5 35 5 / 44 35 / 78Feagan LOW SC EPO, PL 2000 0.51 0.32 0.82 18 35 18 / 79 35 / 78Goodnough-a IV EPO+PAD, PL+PAD 1989 0.52 0.05 5.37 1 2 1 / 23 2 / 24Goodnough-b HIGHIV EPO+PAD, PL+PAD 1993 1.92 0.36 10.28 3 2 3 / 18 2 / 23Goodnough-b LOWIV EPO+PAD, PL+PAD 1993 0.96 0.15 6.25 2 2 2 / 24 2 / 23Goodnough-b MEDIV EPO+PAD, PL+PAD 1993 0.44 0.04 4.56 1 2 1 / 26 2 / 23Mercuriali IV EPO+PAD, PL+PAD 1993 2.00 0.82 4.89 4 9 4 / 8 9 / 36Mercuriali-2 HIGHIV EPO+PAD, PL+PAD 1998 0.75 0.35 1.62 5 6 5 / 10 6 / 9Mercuriali-2 LOW IV EPO+PAD, PL+PAD 1998 1.00 0.52 1.92 6 6 6 / 9 6 / 9Mercuriali-2 MED IV EPO+PAD, PL+PAD 1998 0.90 0.45 1.79 6 6 6 / 10 6 / 9Price IV EPO+PAD, PL+PAD 1996 0.64 0.38 1.08 17 27 17 / 86 27 / 87Sans HIGH SC EPO+PAD, PL+PAD 1996 0.39 0.02 8.69 0 1 0 / 11 1 / 13Sans LOW SC EPO+PAD, PL+PAD 1996 2.36 0.25 22.70 2 1 2 / 11 1 / 13Sans MED SC EPO+PAD, PL+PAD 1996 2.36 0.25 22.70 2 1 2 / 11 1 / 13Schlaeppi HIGH SC EPO+PAD, PL+PAD 1994 0.19 0.01 3.76 0 2 0 / 22 2 / 21Schlaeppi LOW SC EPO+PAD, PL+PAD 1994 0.22 0.01 4.31 0 2 0 / 19 2 / 21Shapiro SC EPO+PAD, PL+PAD 2002 0.29 0.14 0.60 6 19 6 / 25 19 / 23Tryba-2 HIGH IV EPO+PAD, PL+PAD 1996 1.44 0.46 4.54 6 4 6 / 27 4 / 26Tryba-2 LOW IV EPO+PAD, PL+PAD 1996 1.44 0.46 4.54 6 4 6 / 27 4 / 26Weber SC EPO, CTRL 2005 0.24 0.17 0.34 42 88 42 / 467 88 / 237
0.56 0.45 0.71 266 540 266 / 1707540 / 1561
0.01 0.1 1 10 100
Favours EPO Favours CTRL
proportion with allogeneic transfusions: all studies with inactive control (with or without PAD)
Administración de EPO
RR: 0,56 (IC95% 0,45-0,71) 15,6% (266/1707) vs 34,6% (540/1561)
AABT
Seville’s document update
Estimulation of erythropoiesis
Erythropoiesis Stimulating Agents (ESAs)
We recommend the preoperative use of ESAs plus iron in anemic patients scheduled for major elective orthopedic surgery for decreasing perioperative needs for ABT.
- Elective orthopedic surgery
1A
• The efficacy of perioperative administration of rHuEPO plus oral or IV iron in anemic patients undergoing hip, knee or spine surgery has been documented in several large RCTs.
• However, the minimum effective rHuEPO dose to attain a blood sparing effect in this patient population is largely unknown, especially when used with IV iron.
• In patients undergoing complex or revision surgery, rHuEPO may be enhanced the efficacy of PCS or PABD (combination of techniques)
PROVISIONAL (presentado en NATA 2010, Barcelona)

Administración de EPO
Hierro y EPO perioperatorio en cirugía cardíaca
Estudio, ańo + rHuEPO Placebo HierroTipo, dosis, dias
rHuEPO (U/kg)n %ABT n %ABT
Sowade, 97 36 11 36 53* Oral, 300 mg,14d 2.500 IV
D’Ambra, 97 63 32 56 48 Oral, 975 mg, >8d 2.400 SC
D’Ambra, 97 63 28 56 48 Oral, 975 mg, >8d 1.200 SC
Shimpo, 97 21a 0 16b 31* aIV, 4d 1.200 IV
Shimpo, 97 11 a 9 16b 31 bOral, 4s 600 IV
Yazicioglu, 01 25 ? 28 ?** No hierro 100 IV
* Reducción de la tasa (%) y el índice de transfusión (U/pt)** Reducción del índice de transfusión solamente.
AABT
Seville’s document update
Estimulation of erythropoiesis
For anemic patients scheduled for cardiac surgery with cardiopulmonary bypass we suggest preoperative ESAs use plus iron for reducing perioperative ABT rate.
- Cardiac surgery
2B
• Several small RCTs have documented the efficacy of perioperative administration of rHuEPO plus oral or IV iron for reducing ABT in anemic patients undergoing on-pump cardiac procedures.
• However, there is no evidence supporting the use of rHuEPO in off-pump surgery, whereas the evidence supporting a role for rHuEPO in hastening the recovery from postoperative anemia in this patient population is inconclusive.
• It must be borne in mind that this is an “off-label” use of rHuEPO.
Erythropoiesis Stimulating Agents (ESAs)PROVISIONAL (presentado en NATA 2010, Barcelona)
Administración de EPO
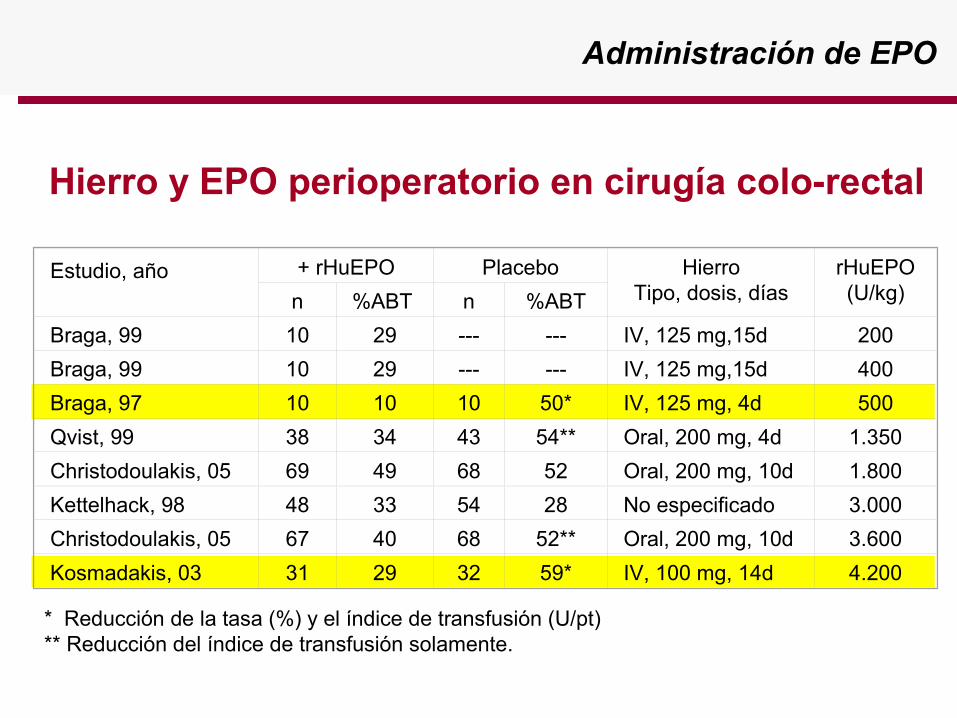
Estudio, año + rHuEPO Placebo HierroTipo, dosis, días
rHuEPO (U/kg)n %ABT n %ABT
Braga, 99 10 29 --- --- IV, 125 mg,15d 200
Braga, 99 10 29 --- --- IV, 125 mg,15d 400
Braga, 97 10 10 10 50* IV, 125 mg, 4d 500
Qvist, 99 38 34 43 54** Oral, 200 mg, 4d 1.350
Christodoulakis, 05 69 49 68 52 Oral, 200 mg, 10d 1.800
Kettelhack, 98 48 33 54 28 No especificado 3.000
Christodoulakis, 05 67 40 68 52** Oral, 200 mg, 10d 3.600
Kosmadakis, 03 31 29 32 59* IV, 100 mg, 14d 4.200
Hierro y EPO perioperatorio en cirugía colo-rectal
* Reducción de la tasa (%) y el índice de transfusión (U/pt)** Reducción del índice de transfusión solamente.
AABT
Seville’s document update
Estimulation of erythropoiesis
We suggest that preoperative ESAs use in anemic patients scheduled for neoplasic colorectal surgery could decrease the perioperative needs for allogeneic blood transfusions.
- Colorectal cancer surgery
2B
• This recommendation derives from several RCTs and Obs of gastrointestinal cancer patients (mostly colorectal cancer) with different rHuEPO doses and treatment duration.
• rHuEPO efficacy was increased by adjuvant IV iron therapy.
• Again, it must be remembered that this is an “off-label” use of rHuEPO and that there are safety concerns in despite of being a short-term therapy.
Erythropoiesis Stimulating Agents (ESAs)PROVISIONAL (presentado en NATA 2010, Barcelona)
Administración de EPO
Administración de EPO

Administración de EPO

Administración de EPO

Administración de EPO

Administración de EPO
Tratamiento de la anemia post-traumatismo/cirugía
rHuEPO en paciente crítico
Tratamiento de la anemia post-traumatismo/cirugía
rHuEPO en paciente crítico
AABT
Seville’s document update
Estimulation of erythropoiesis
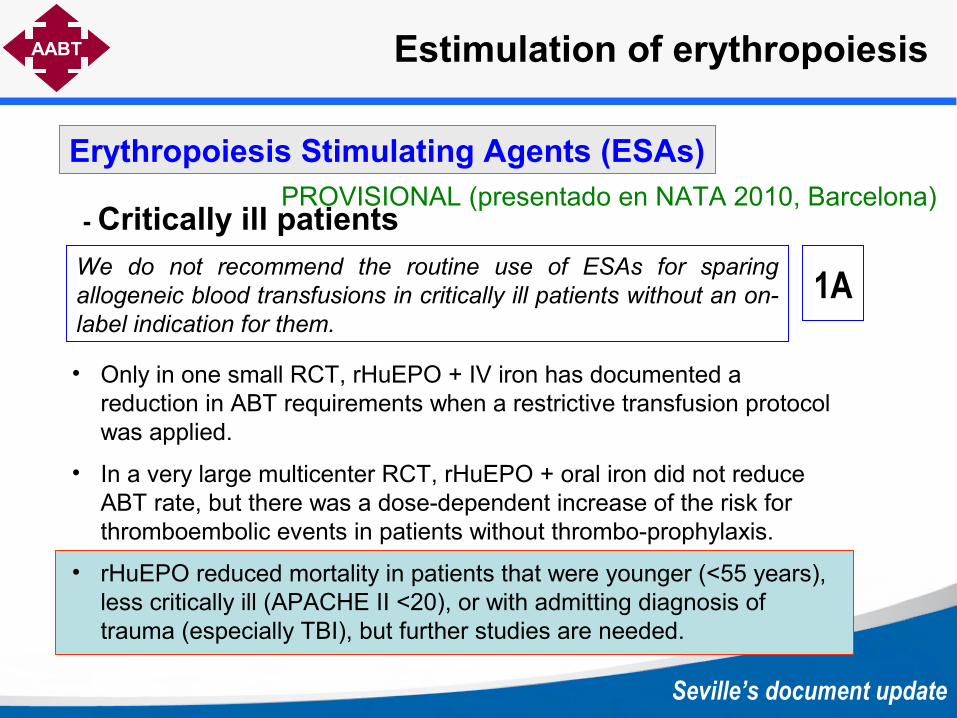
We do not recommend the routine use of ESAs for sparing allogeneic blood transfusions in critically ill patients without an on-label indication for them.
- Critically ill patients
1A
• Only in one small RCT, rHuEPO + IV iron has documented a reduction in ABT requirements when a restrictive transfusion protocol was applied.
• In a very large multicenter RCT, rHuEPO + oral iron did not reduce ABT rate, but there was a dose-dependent increase of the risk for thromboembolic events in patients without thrombo-prophylaxis.
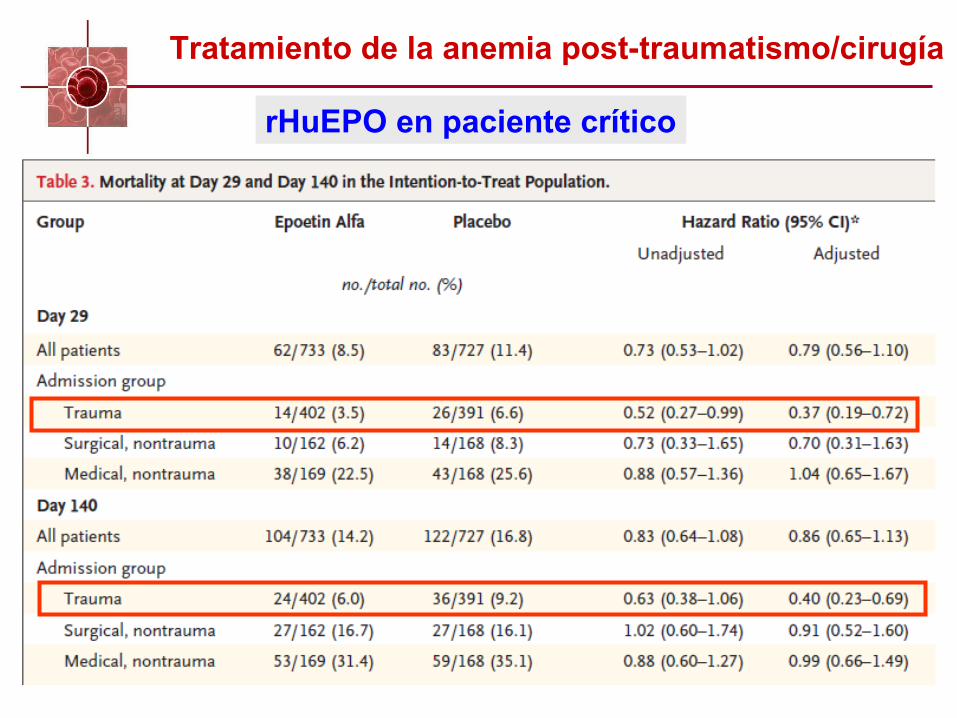
• rHuEPO reduced mortality in patients that were younger (<55 years), less critically ill (APACHE II <20), or with admitting diagnosis of trauma (especially TBI), but further studies are needed.
Erythropoiesis Stimulating Agents (ESAs)PROVISIONAL (presentado en NATA 2010, Barcelona)


HIERROHIERRO
AUMENTO DE MASA ERITROCITARIA

20-30mg/día
Músculo(250 mg)
Médula ósea(300 mg)
Eritrocitos(2.000 mg)
Macrófagos SRE(500 mg)
Hígado(1000 mg)
Absorción intestinal de hierro(1-2 mg/día)
Transferrina(3 mg)
Pérdidas de hierro(1-2 mg/día)
Hierro EV
Administración de FE EV

Esta indicación tiene en cuenta varios factores, como:
Intolerancia ó contraindicación al hierro oral (eg, EII).
Poco tiempo antes de la cirugía.
Anemia preoperatoria grave.
Uso de estimuladores de la eritropoyesis
Estado inflamatorio del paciente.
Sangrado perioperatorio estimado.
¿Cúal es el papel del hierro EV?
Administración de FE EV

Tratamiento perioperatorio Administración de FE EV
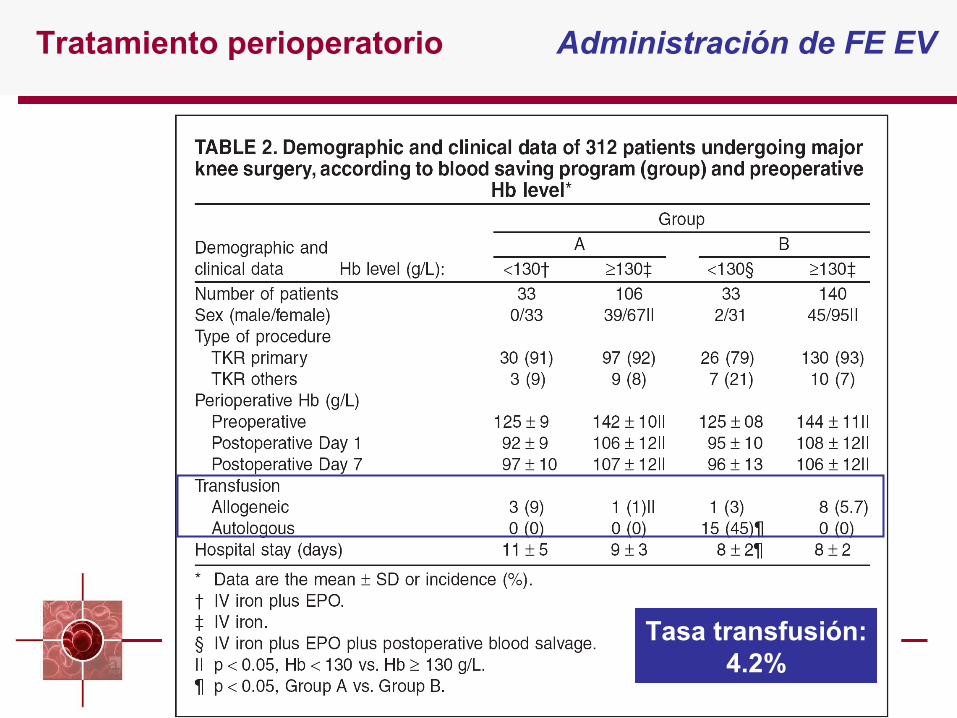
Tasa transfusión:4.2%
Tratamiento perioperatorio Administración de FE EV
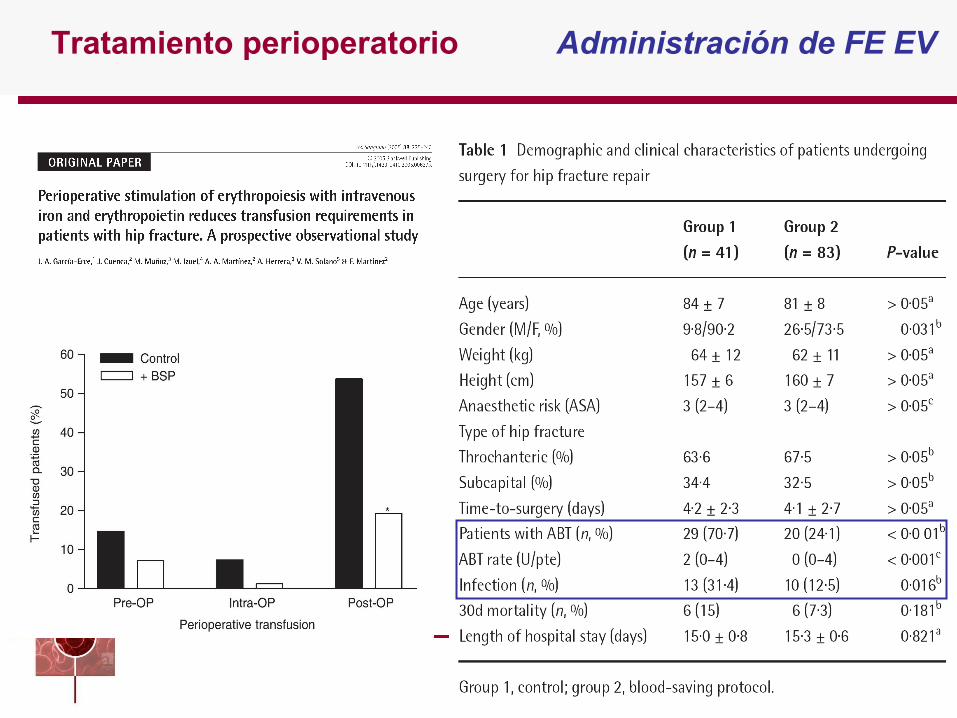
Tratamiento perioperatorio Administración de FE EV

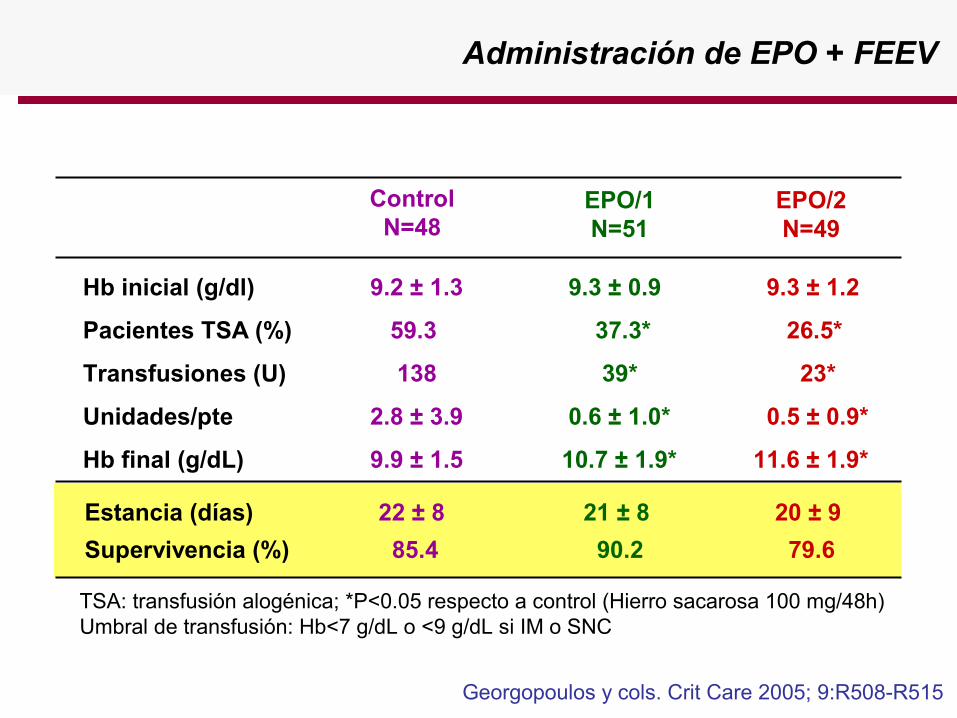
Administración de EPO + FEEV
Administración de EPO + FEEV
Georgopoulos y cols. Crit Care 2005; 9:R508-R515
EPO/1N=51
ControlN=48
EPO/2N=49
Hb inicial (g/dl) 9.2 ± 1.3 9.3 ± 0.9 9.3 ± 1.2
Pacientes TSA (%) 59.3 37.3* 26.5*
Transfusiones (U) 138 39* 23*
Unidades/pte 2.8 ± 3.9 0.6 ± 1.0* 0.5 ± 0.9*
Hb final (g/dL) 9.9 ± 1.5 10.7 ± 1.9* 11.6 ± 1.9*
Estancia (días) 22 ± 8 21 ± 8 20 ± 9
Supervivencia (%) 85.4 90.2 79.6
TSA: transfusión alogénica; *P<0.05 respecto a control (Hierro sacarosa 100 mg/48h)Umbral de transfusión: Hb<7 g/dL o <9 g/dL si IM o SNC
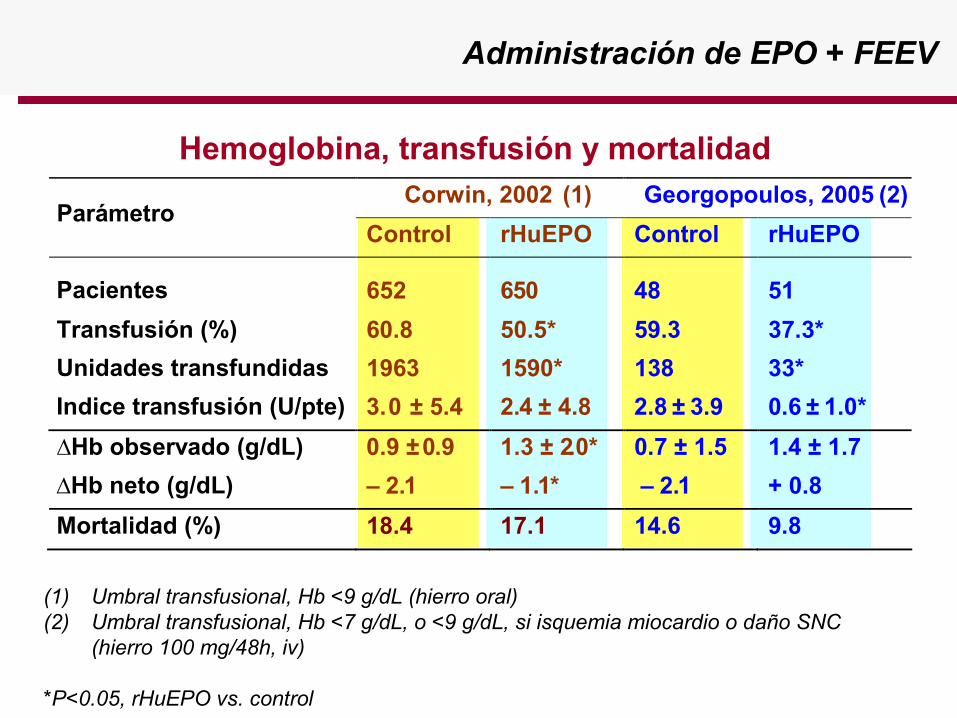
Administración de EPO + FEEV
Hemoglobina, transfusión y mortalidad
(1) Umbral transfusional, Hb <9 g/dL (hierro oral)(2) Umbral transfusional, Hb <7 g/dL, o <9 g/dL, si isquemia miocardio o daño SNC
(hierro 100 mg/48h, iv)
*P<0.05, rHuEPO vs. control
Corwin, 2002 (1) Georgopoulos, 2005 (2) Parámetro
Control rHuEPO Control rHuEPO Pacientes 652 650 48 51
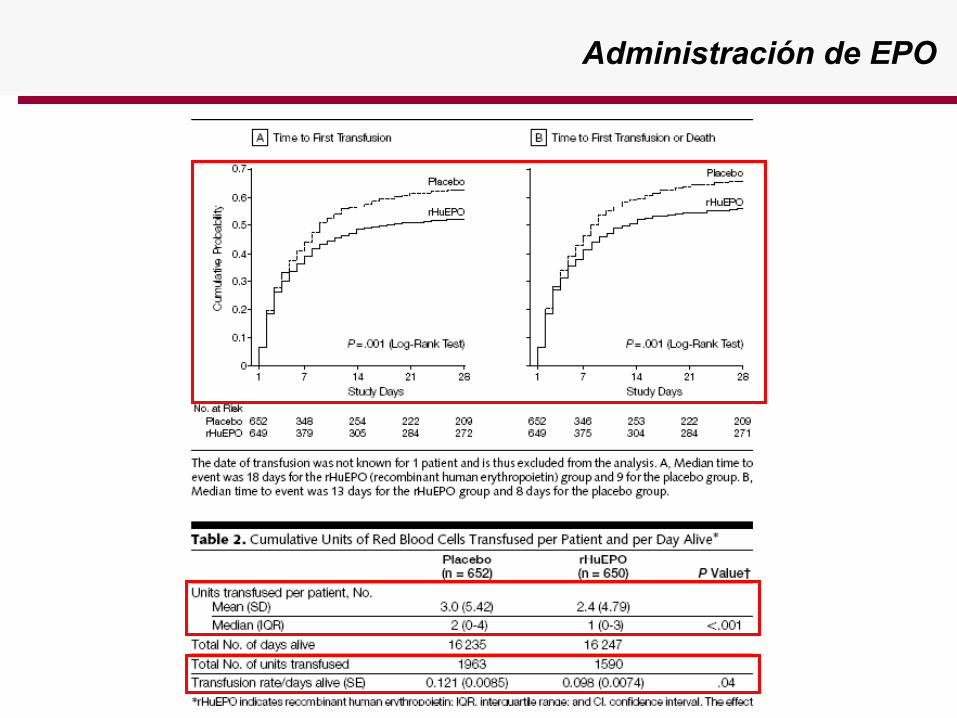
Transfusión (%) 60.8 50.5* 59.3 37.3*
Unidades transfundidas 1963 1590* 138 33*
Indice transfusión (U/pte) 3.0 ± 5.4 2.4 ± 4.8 2.8 ± 3.9 0.6 ± 1.0*
∆Hb observado (g/dL) 0.9 ± 0.9 1.3 ± 2.0* 0.7 ± 1.5 1.4 ± 1.7
∆Hb neto (g/dL) – 2.1 – 1.1* – 2.1 + 0.8
Mortalidad (%) 18.4 17.1 14.6 9.8
Dr. José Antonio García Erce Hematología y HemoterapiaHospital de San Jorge, Huesca (España)[email protected]
Alternativas a la transfusión alogénica en cirugía.
Gracias por su atención