Embed Size (px)
Citation preview
SAMIR EL ANSARY
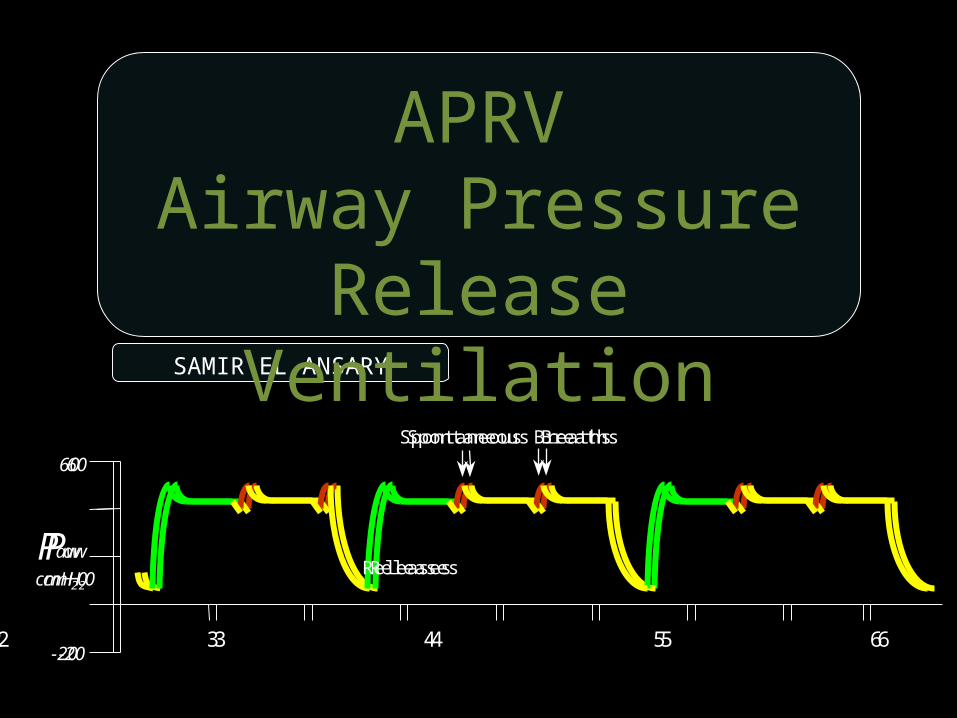
APRVAirway Pressure Release
Ventilation
Paw
cmH20
60
-201 2 3 4 5 6 7 8
Spontaneous Breaths
ReleasesPaw
cmH20
60
-201 2 3 4 5 6 7 8
Spontaneous Breaths
Releases

https://www.facebook.com/groups/1451610115129555/#!/groups/1451610115129555/
Wellcome in our new group ..... Dr.SAMIR EL ANSARY
APRVAirway Pressure Release
Ventilation
SAMIR EL ANSARYICU PROFESSOR
AIN SHAMSCAIRO

Spontaneous breaths
CPAP Level
CPAP Level 2
CPAP Level 1
CPAP Released CPAP Restored
Time
Airw
ay P
ress
ure
APRV(Airway Pressure Release Ventilation)

Is a form of Bi level ventilation that utilises a very short expiratory time
for pressure release
All spontaneous breathing is done at upper pressure level
to promote lung recruitment of collapsed and poorly ventilated alveoli

The CPAP is released periodically for brief period This short release along with spontaneous
breathing promotes CO2 elimination
The release time is short to prevent the peak expiratory flow
from returning to a zero baseline

Control Trigger Limit Cycle
Pressure Time Pressure Time
Time Triggered Time-cycled Ventilation
Airway Pressure Release Ventilation

The ventilator cycles from high CPAP to low CPAP
{high lung volume to lower lung volume}
Patient can breathspontaneously at either level
The presence of a dynamic expirtatory valve in these ventilators
Allows spontaneous breathing at high lung volumes
APRV should be seen as full tidal volume ventilation
The patient is ventilated on the expiratory limb of the volume
pressure curve
These breaths can beUnsupported, pressure supported
or supported by automatic tube compensation

To restore FRC through recruitment and to maintain FRC by creating intrinsic PEEP
APRVProvide lung protective ventilation
support while minimising alveolar distension
And avoidingrepeated alveoli collapse and re-expansion.
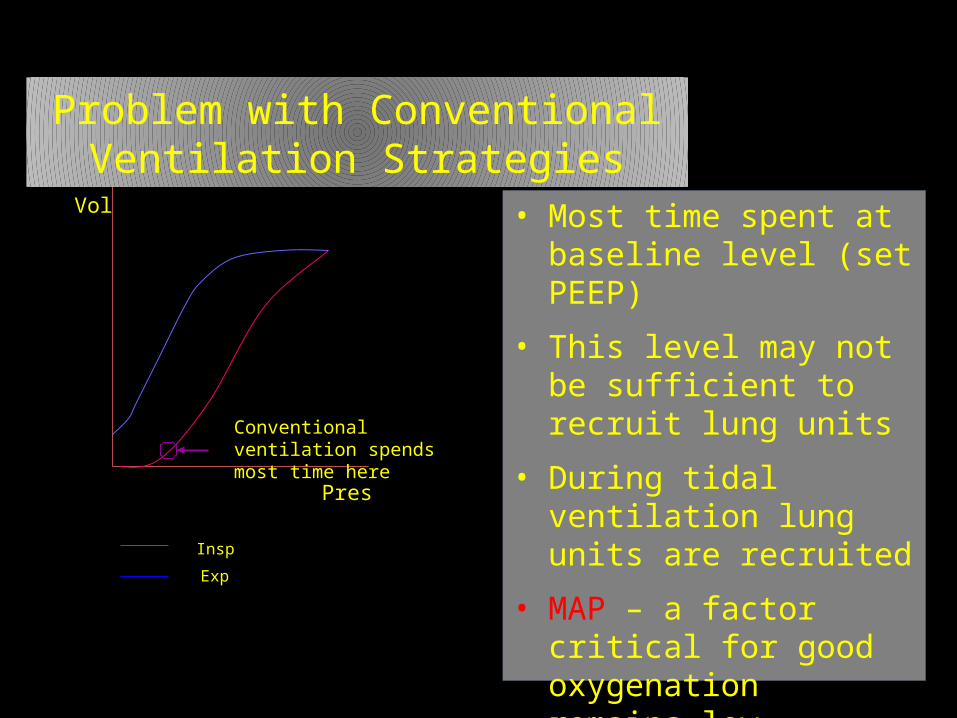
Vol
Pres
Conventional ventilation spends most time here
Insp
Exp
Problem with Conventional Ventilation Strategies
• Most time spent at baseline level (set PEEP)
• This level may not be sufficient to recruit lung units
• During tidal ventilation lung units are recruited
• MAP – a factor critical for good oxygenation remains low

Vol
Pres
Conventional ventilation spends most time here
APRV spends most time here
Insp
Exp
Airway Pressure Release
Ventilation StrategyFundamental concept of
APRV• Maintain optimal V/Q
by optimising MAP• Ventilates from point
much higher on PV curve
• Maximizes the recruitable surface of
the lung

They become important In diseased states
APRV takes advantage of the collateral channels of ventilation that are barely used at the FRC level in normal,
healthy lungs
Kohn
Lambert
Martin
•The CPAP level drives oxygenation
• The timed releases aid in CO2
clearance

ACUTE LUNG INJURIES AND ARDS
Paw
cmH20
60
-201 2 3 4 5 6 7 8
Spontaneous Breaths
Releases
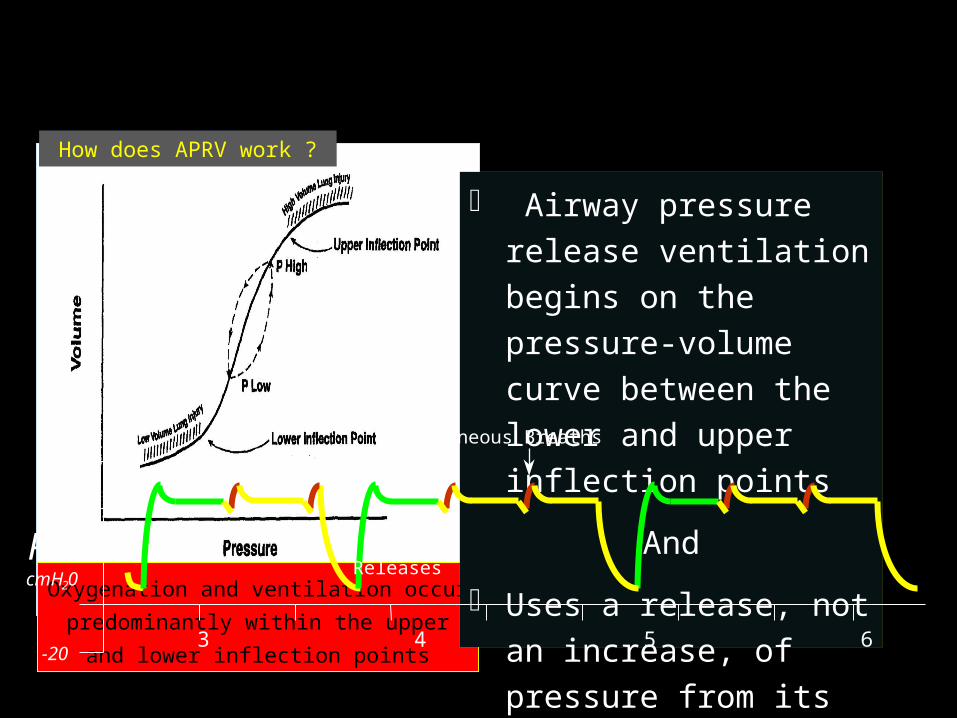
Oxygenation and ventilation occur
predominantly within the upper and
lower inflection points
How does APRV work ?
Airway pressure release ventilation begins on the pressure-volume curve between the lower and upper inflection points
And
Uses a release, not an increase, of pressure from its baseline.
Paw
cmH20
60
-201 2 3 4 5 6 7 8
Spontaneous Breaths
Releases

• Sustained plateau pressurepromotes alveolar recruitment
Rational for APRV
while being maintained at an acceptable level
• The number of respiratory cycles is minimized
prevents both the repetitive opening of alveoli and alveolar stretch, that may
result in lung injury
Rational for APRV

APRV can unload inspiratory muscles–Decrease the work of breathing associated with chronic obstructive
pulmonary disease
Rational for APRV

The end-inspiratory pressure
which equates to P High or plateau pressure should be kept
< 35 cmH20
Rational for APRV

https://www.facebook.com/groups/1451610115129555/#!/groups/1451610115129555/
Wellcome in our new group ..... Dr.SAMIR EL ANSARY

The preset pressure limit
prevents or limits, over-distension of alveoli and high-volume lung injury
APRV affects tidal ventilation by decreasing rather than increasing airway pressure
Rational for APRV
Decreasing lung volume for ventilation
Limits air space over-distension
Limits low-volume lung injuryby avoiding the repetitious opening of alveoli
Rational for APRV
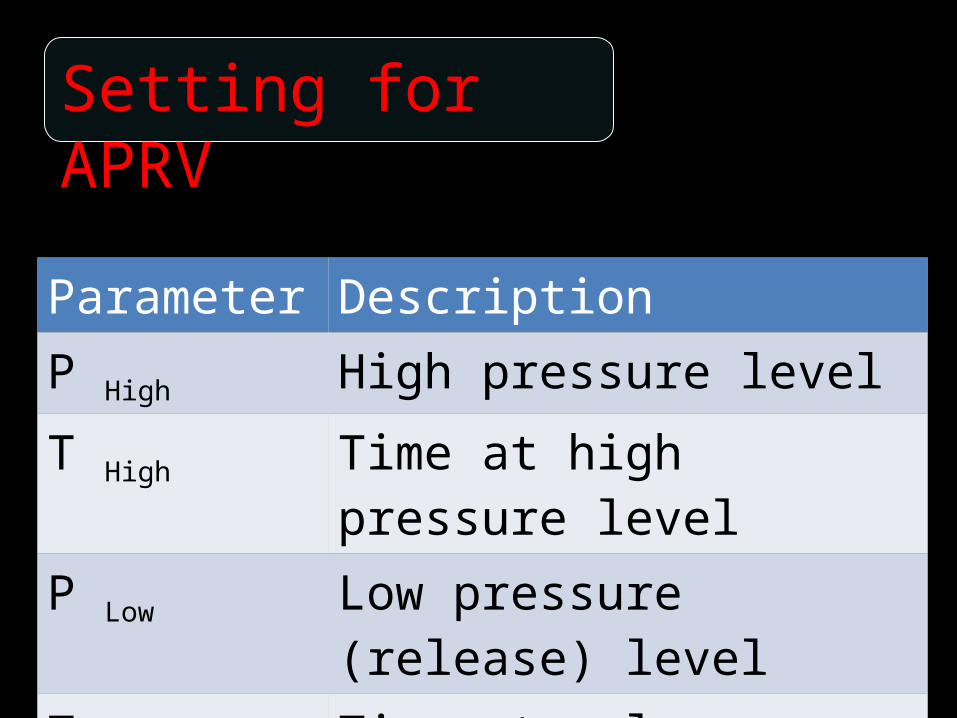
Parameter DescriptionP High High pressure levelT High Time at high pressure levelP Low Low pressure (release) levelT Low Time at release level
Setting for APRV

P High The upper CPAP level
Similar to MAP (mean airway pressure ) and thus
affects oxygenation.P Low
(Also referred to as PEEP)The lower pressure setting
Terminology

Terminology
T HighInspiratory time phase for the high CPAP
T Low
Release time allowing CO2 elimination
(T high plus T low is the total time of one cycle)

TerminologyI:E ratio in APRV becomes irrelevant
because APRV is really best thought of as CPAP with occasional release
Inverse ratio ventilation
Initial Setting
P highMean airway pressure
20-25cm H2Oor
MAP the patient is on conventional ventilation.

Initial Setting
P lowZero cm H2O
This provides
Rapid drop in pressureMaximum delta p
It also avoids collapse during T low

Initial Setting
T HighThe inspiratory time
4.0 seconds
It is progressively increased as the patient is weaned

Initial Setting
T Low0.2 to 0.6 seconds
Too long a release time would interfere with oxygenation and allow alveolar collapse and
atelectasis can develop quickly

Control Settings for CO2
{ PHigh - P Low}
Determines the volume exchange therefore affecting PCO2 clearance as TV
would
Optimising spontaneous ventilation will also help clear CO2

To decrease PCO2
Decrease T-high
Increase P High
Increase T Low to allow more time for “exhalation.”

To increase PCO2
Increase T HighDecrease P High to lower the MAP
(Monitor oxygenation and avoid derecruitment)
It may be better to accept hypercapnia than to reduce P High so much that
oxygenation decreases

To increase PaO2
Increase FiO2 Increase MAP
by increasing P High slowly(by increments of 2cm H2o at a time)
Increase T High slowlyUse recruitment manoeuvres

Weaning From APRV
FiO2 should be weaned first Reduce P high
Increase T High gradually
The patient essentially transits to CPAP with very few releases

Weaning From APRV
Patient should increasing his spontaneous rate to compensate
During weaning closely monitorMAP - O2 Sat
Exhaled Minute VolumeEnd Tidal CO2
Weaning From APRV
Always reduce FiO2 before P High!
If PHigh > or = 30cmH2OReduce FiO2 to 50% before
decreasing P High

Weaning From APRV
“Drop and Stretch”PHigh is dropped and the Thigh is stretched
out sequentially

https://www.facebook.com/groups/1451610115129555/#!/groups/1451610115129555/
Wellcome in our new group ..... Dr.SAMIR EL ANSARY

Weaning From APRV
The “drop and stretch technique” is continued until
PHigh is at 10 – 15 cmH2O and the T High is at 10 -15 seconds.
At this point the patient is effectively on CPAP

“Mandatory rules“ in APRV
The expiratory timeshould be short enough to prevent
derecruitment
And long enough to obtain a suitable tidal volume

“Mandatory rules“ in APRV
The expiratory time 0.4 to 0.6 seconds
The tidal volume is your target(between 4 and 6ml/kg)
“Mandatory rules“ in APRV
If the tidal volume is inadequate
the expiratory time is lengthened
If it is too high ( > 6ml/kg) the expiratory time is shortened

“Mandatory rules“ in APRV
If you are starting off with APRV then start high (28cmH2O of less) and work your way
down
Higher transalveolar pressures recruit the lungs

“Mandatory rules“ in APRV
Low PEEP is set at 0 cmH2O The large pressure ramp allows for tidal ventilation in very short expiratory times
The inspiratory time is set at 4-6 seconds
(the respiratory rate should be 8 to 12 breaths per minute - never more)

“Mandatory rules“ in APRV
There are two different ways to wean patients from APRV
If lung mechanics rapidly return to normal the patient should be weaned to
Pressure support

“Mandatory rules“ in APRV
If ARDs is prolonged, then the high CPAP level is gradually weaned
down to 10 cmH2Oand then the patient is converted to a
standard vent wean

The pressure support {High CPAP- Low CPAP}
Paw
cmH20
60
-201 2 3 4 5 6 7 8
Spontaneous Breaths
Releases
“Mandatory rules“ in APRV

BiLevel Ventilation
PEEPH
PEEPL
Pressure SupportPEEPHigh + PS
Paw
cmH20
60
-201 2 3 4 5 6 7

Thigh
Tlow
Plow
Phigh
Time
Time
Pres
sure
Pres
sure
Psupp

Thigh
Tlow
Plow
Phigh
Time
Time
Pres
sure
Pres
sure
Phigh
Psupp

Thigh
Tlow
Plow
Phigh
Time
Time
Pres
sure
Pres
sure
PhighPsupp
Psupp

GOOD LUCK
SAMIR EL ANSARYICU PROFESSOR
AIN SHAMSCAIRO
https://www.facebook.com/groups/1451610115129555/#!/groups/1451610115129555/
Wellcome in our new group ..... Dr.SAMIR EL ANSARY