Embed Size (px)
Citation preview
Airway pressure release ventilation (APRV)
in PICU: Current evidence
Chor Yek Kee
Sarawak General Hospital

Outline
• Brief introduction of APRV
• History of APRV
• Common confusion in APRV
• Features of APRV and how it works
• Evidences of APRV
• Future of APRV


Natural High Frequency Ventilation

Natural APRV Blowhole of dolphin
Natural APRV



. .. . . . . , . , . ; ‘ . - . . ‘ “ .
. . . . . . . . . . . .
APRV open up lung at FRC Intrinsic lung pathology reduced FRC
Extrinsic compressing factor reduced FRC
Healthy lung at normal FRC
APRV maintained FRC by counter extrinsic pressure
High level CPAP
High level CPAP

Constant Vs Intermitent Recruitment
Open the lung and keep it open
Never let the lung collapse
Lachmann B : Intensive Care Medicine 1992 Joshua Satalin : Ann Transl Med 2016


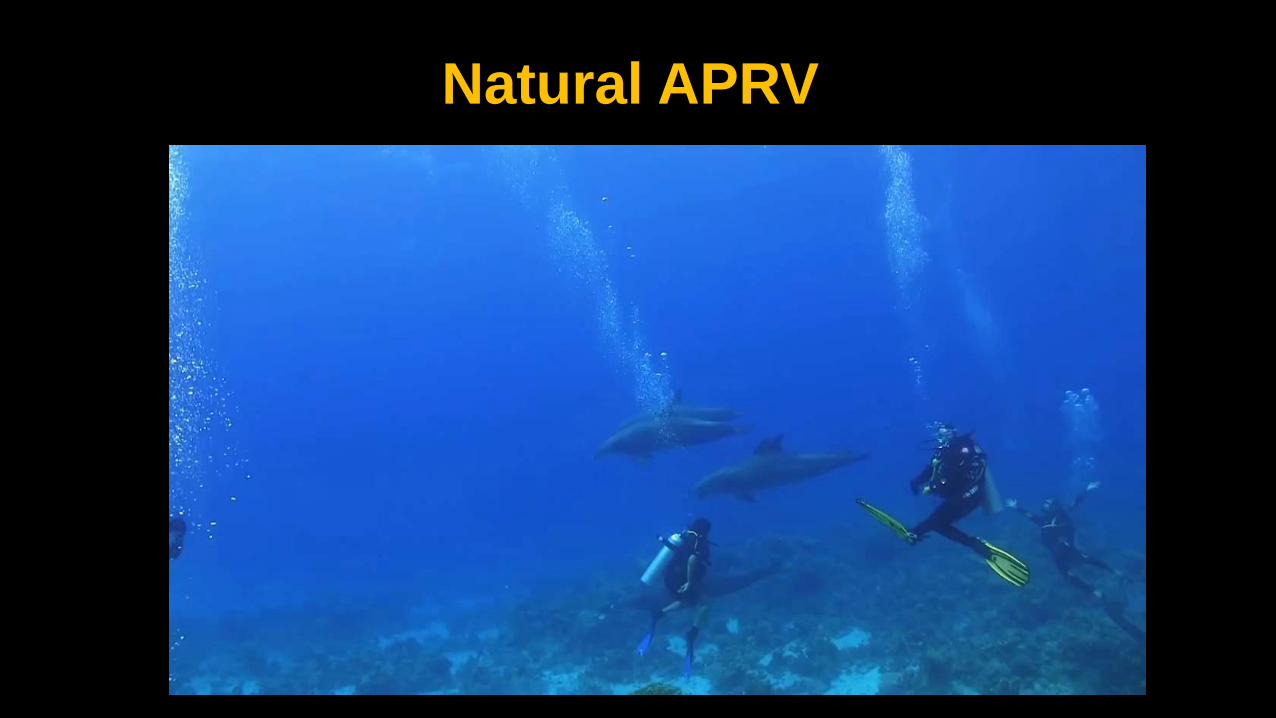
Mode of ventilation Percentage
APRV 1.6%
Conventional 75.2%
HFPV 16.4%
Non-invasive 8.5%
59 PICU from North America and Europe, Cross sectional study 2007

2013 email survey • 88 respiratory
therapist • 4 countries
• United State • Canada • Saudi Arabia • United Arab
Emirates

History of APRV
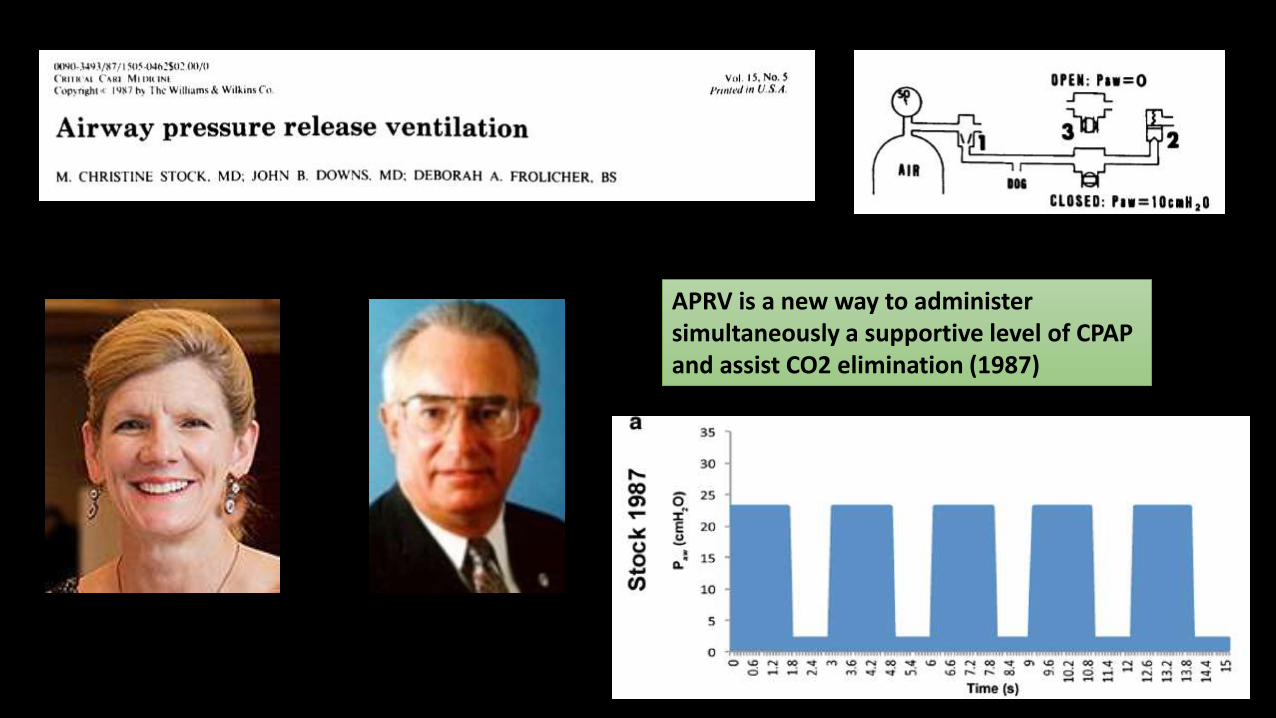
APRV is a new way to administer simultaneously a supportive level of CPAP and assist CO2 elimination (1987)

APRV Setting
P High Pressure during CPAP phase
P Low Pressure during release phase
T High Time during CPAP phase
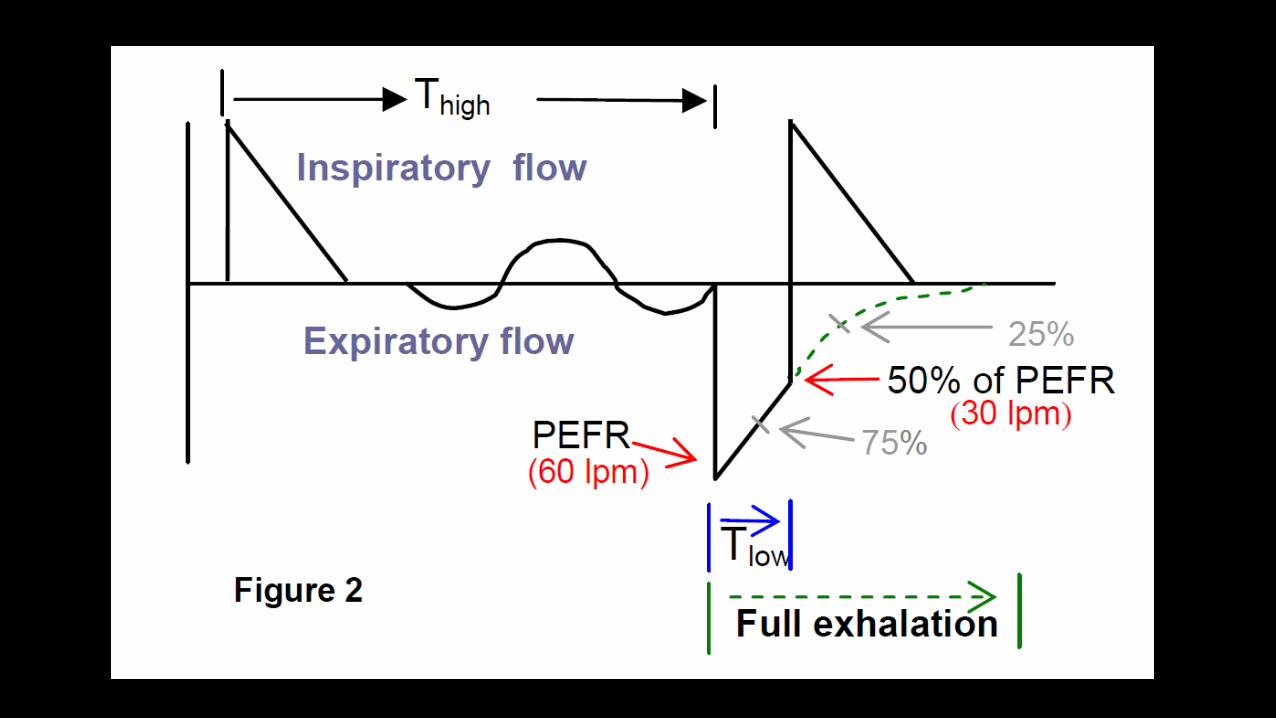
T Low Time during Release Phase
% CPAP Percent CPAP
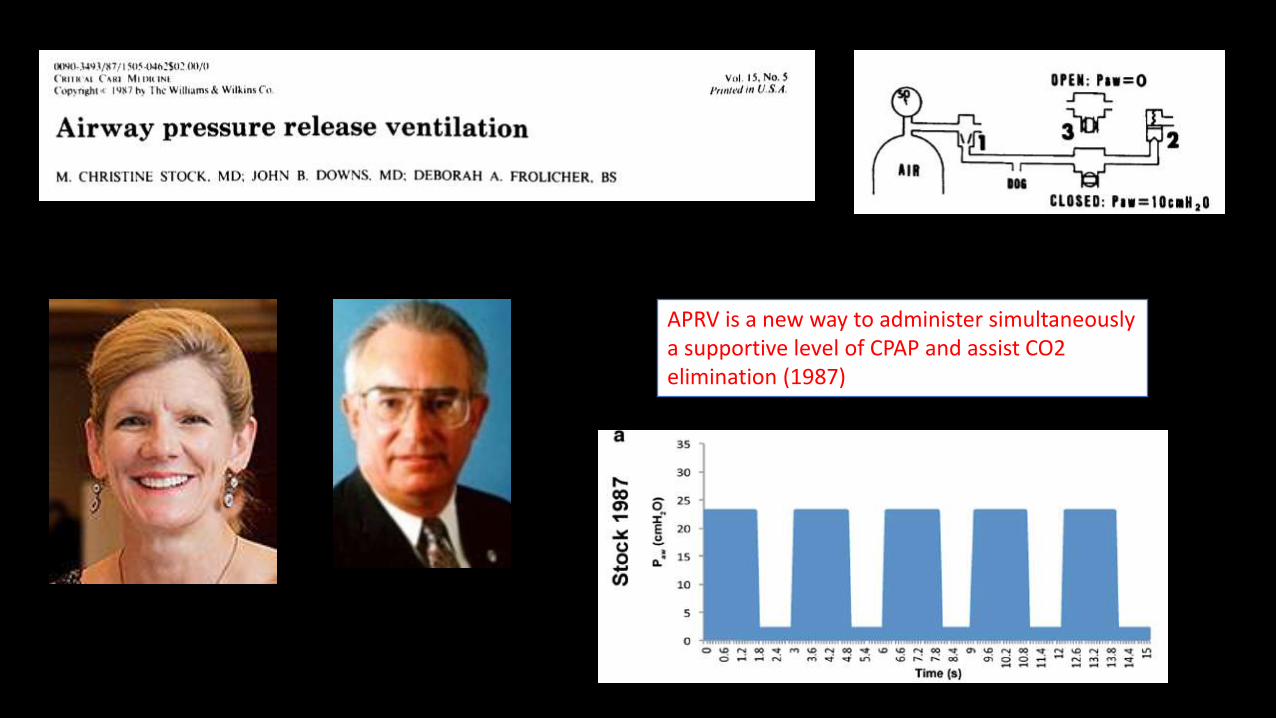
APRV is a new way to administer simultaneously a supportive level of CPAP and assist CO2 elimination (1987)

• Tremendous variation in setting of APRV
• Impossible to assess efficacy of a single strategy since almost none of the APRV setting were identical

Fixed ( F-APRV)
T High CPAP < 90% of total cycle time.
T Low Fixed T Low , not base on changing of lung mechanic
P Low P low is set > 0 cmH2O
Personalised P-APRV
T High CPAP > 90% of total cycle time
T Low T low is set by the changes in the lung mechanic by analysing the slope of the expiratory flow curve
P Low P low is set at 0 cmH2O
APRV Strategies

APRV BIPAP
Baum M et al : BIPAP- a new form of augmented ventilation. Anaesthetist : 1989
Christine and Down et al. Airway Pressure Release Ventilation. CCM 1987

Superficially similar BUT Fundamentally different
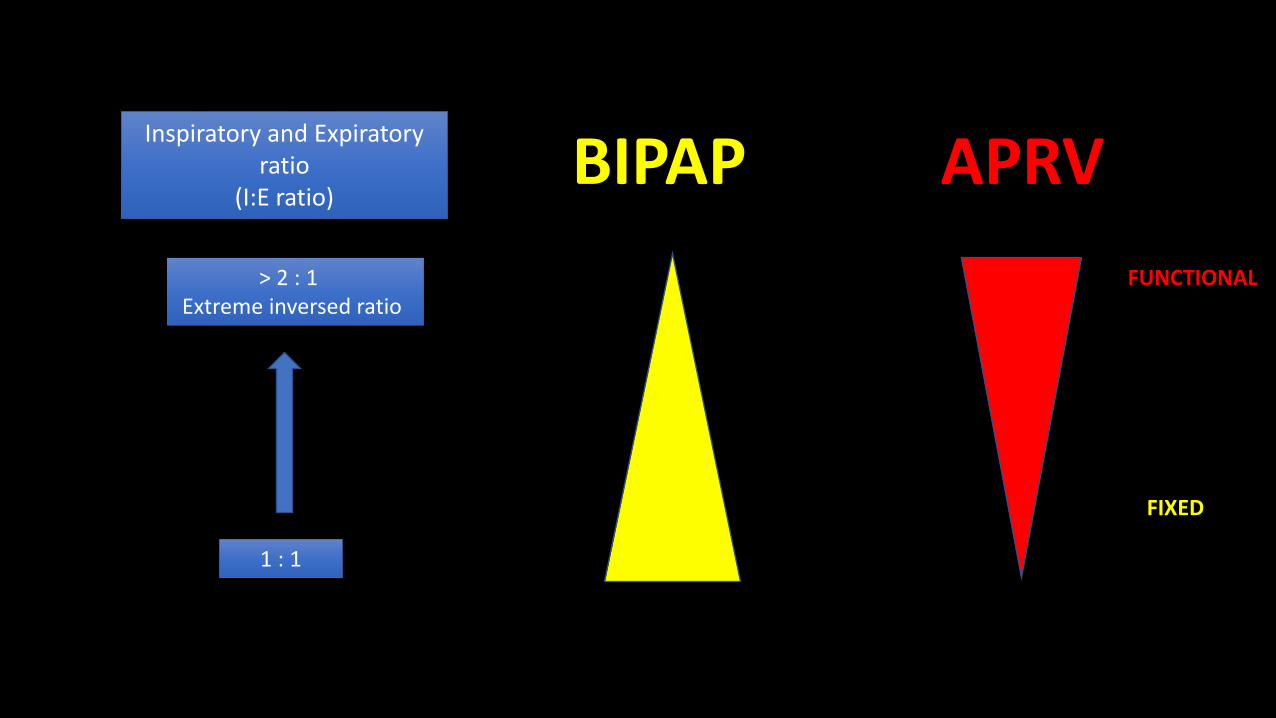
Inspiratory and Expiratory ratio
(I:E ratio)
> 2 : 1 Extreme inversed ratio
1 : 1
BIPAP APRV
FIXED
FUNCTIONAL

APRV is named in various way and can be set in machine with BIPAP mode
1. APRV ( Dragger Evita, Savina and V series, Hamilton G5 )
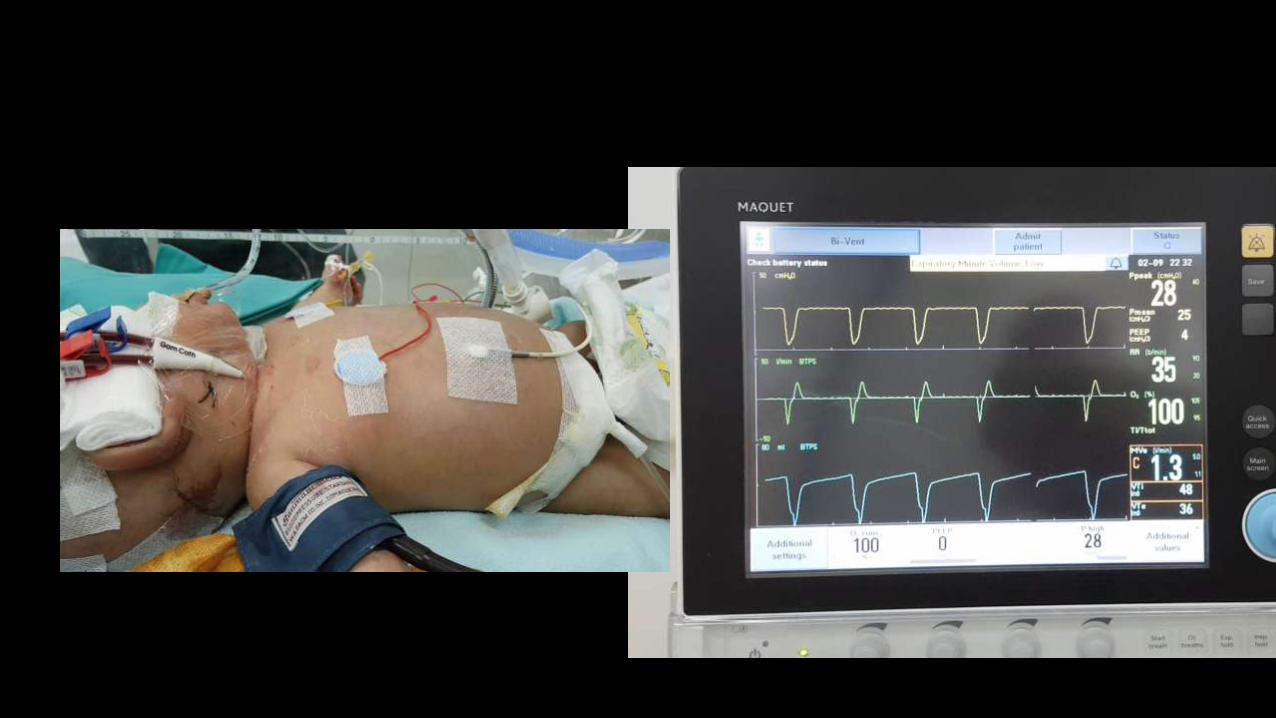
2. Bi-Vent ( Maquet Servo-I )
3. BiLevel ( Engstrom carestation, Puriton Bennett 840 & 980, Covidien)
4. APRV/BiPhasic ( Viasys Avea )
5. DuoPAP ( Hamilton )

WHY APRV ?

Features of APRV
Elevated CPAP Level
Time Pressure Release
Spontaneous breathing

High Level CPAP in APRV
Open the lung and keep it open
Prolonged CPAP ( P High )--- recruiting the lung
Never let the lung collapse
Minimal release duration ( T Low ) preventing lung collapse
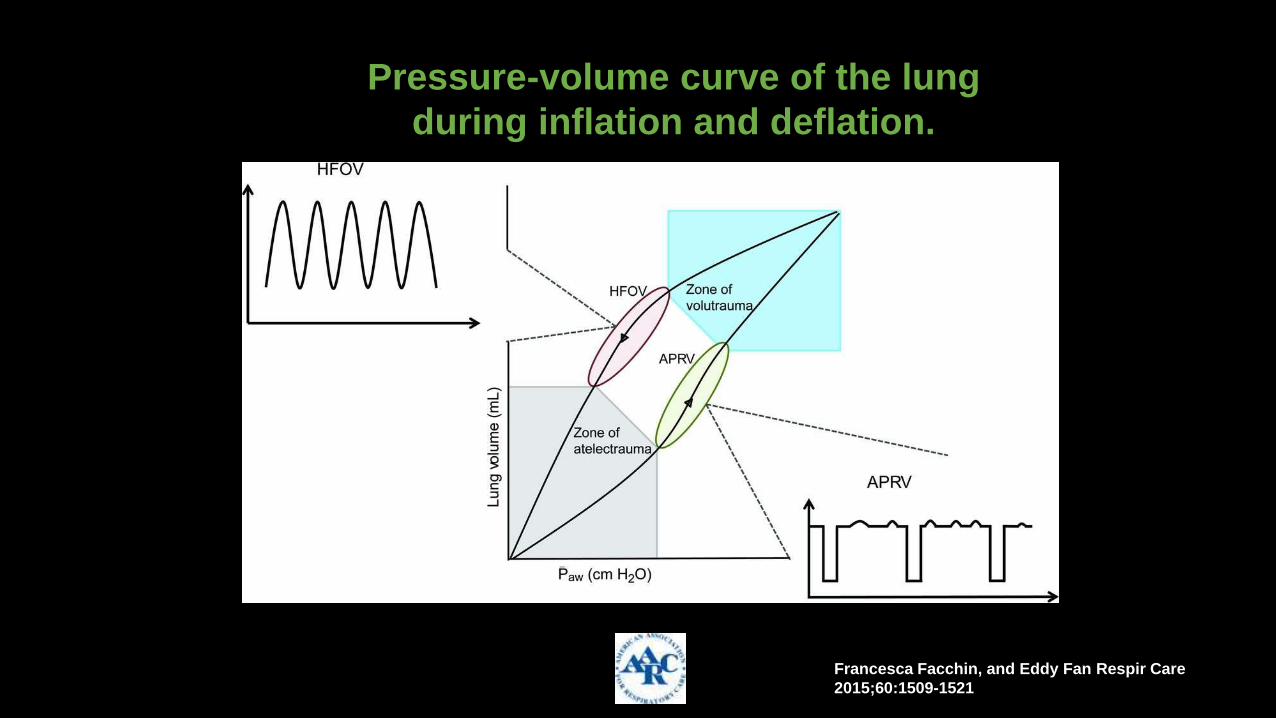
Pressure-volume curve of the lung during inflation and deflation.
Francesca Facchin, and Eddy Fan Respir Care
2015;60:1509-1521
(c) 2012 by Daedalus Enterprises, Inc.
Francesca Facchin, and Eddy Fan Respir Care
2015;60:1509-1521
Pressure-volume curve of the lung
during inflation and deflation.

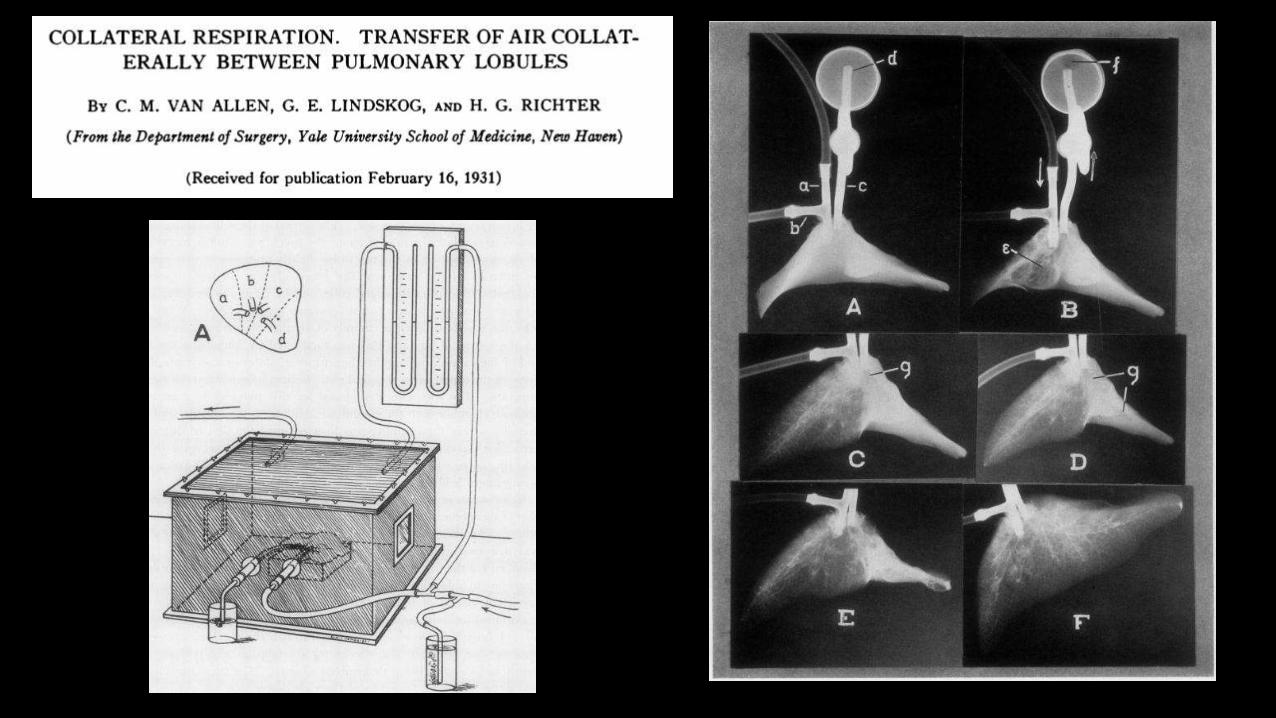
How does elevated CPAP recruit the lung in
APRV?
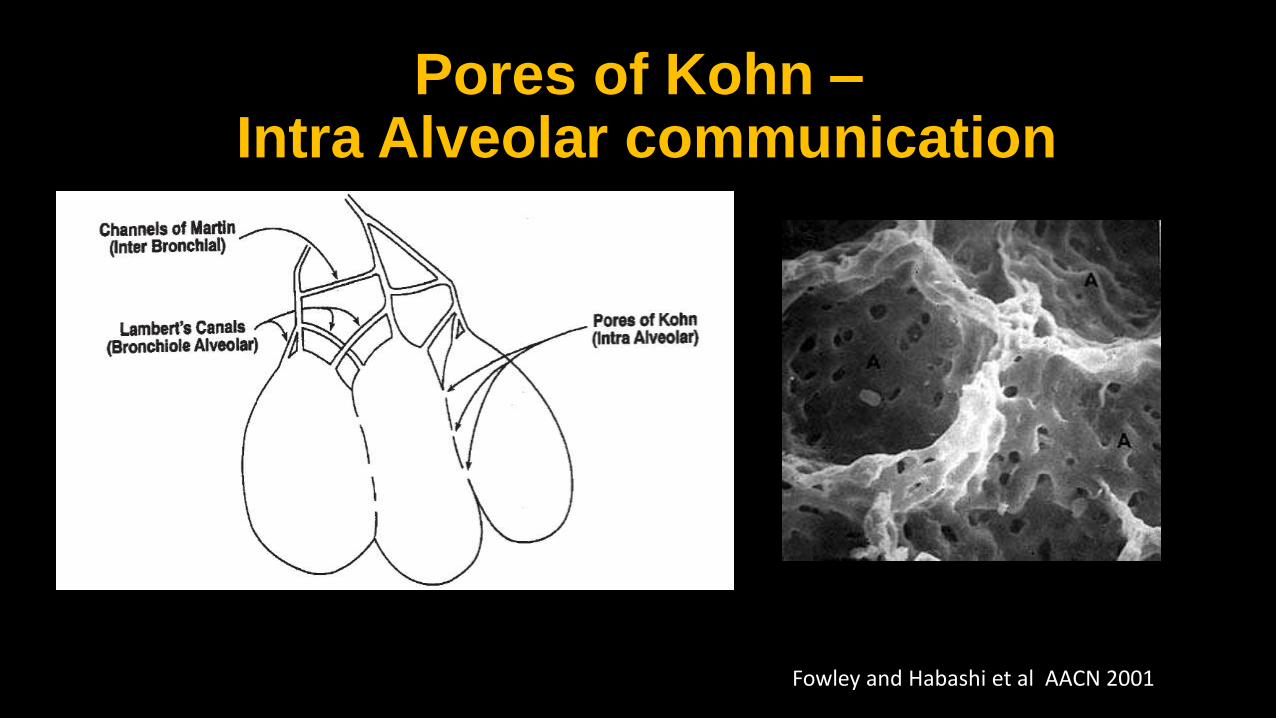
Pores of Kohn – Intra Alveolar communication
Fowley and Habashi et al AACN 2001

How does high CPAP level changes lung volume
? Changing in alveolar volume
? changing alveolar numbers

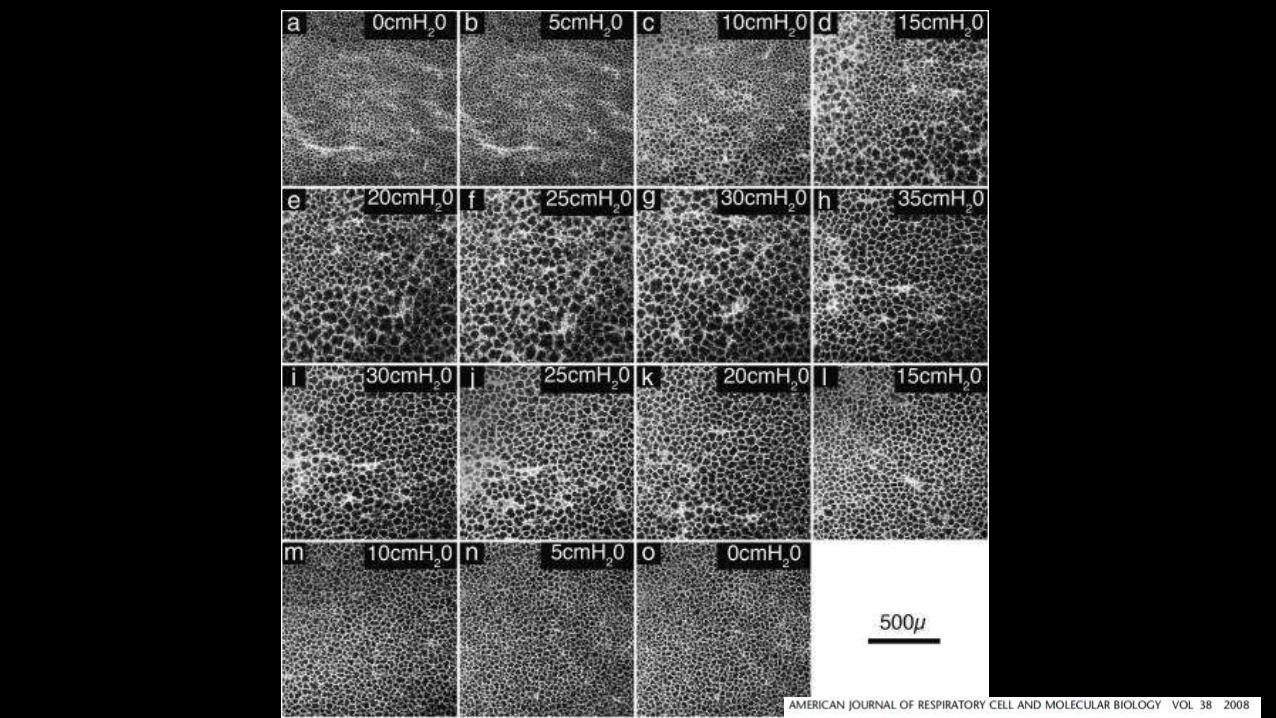


Numbers of alveoli
Size of the alveoli Alveoli wall
length/ microstrain
inflate

Mother and Daughter hypothesis Increasing the numbers of
( less strained) alveoli

Group A -- Sham Group B -- LTV Group C --APRV
Tidal volume 10 ml/Kg PEEP 5 cmH2O Rate 12 bpm FiO2 = 21%
Low tidal volume group Tidal volume 4 to 6 ml/Kg PEEP according to PEEP/FiO2 table
APRV with tidal volume of 10 ml/Kg
Group C Group B


Pressure-volume curve of the lung during inflation and deflation.
Francesca Facchin, and Eddy Fan Respir Care
2015;60:1509-1521
(c) 2012 by Daedalus Enterprises, Inc.
Francesca Facchin, and Eddy Fan Respir Care
2015;60:1509-1521
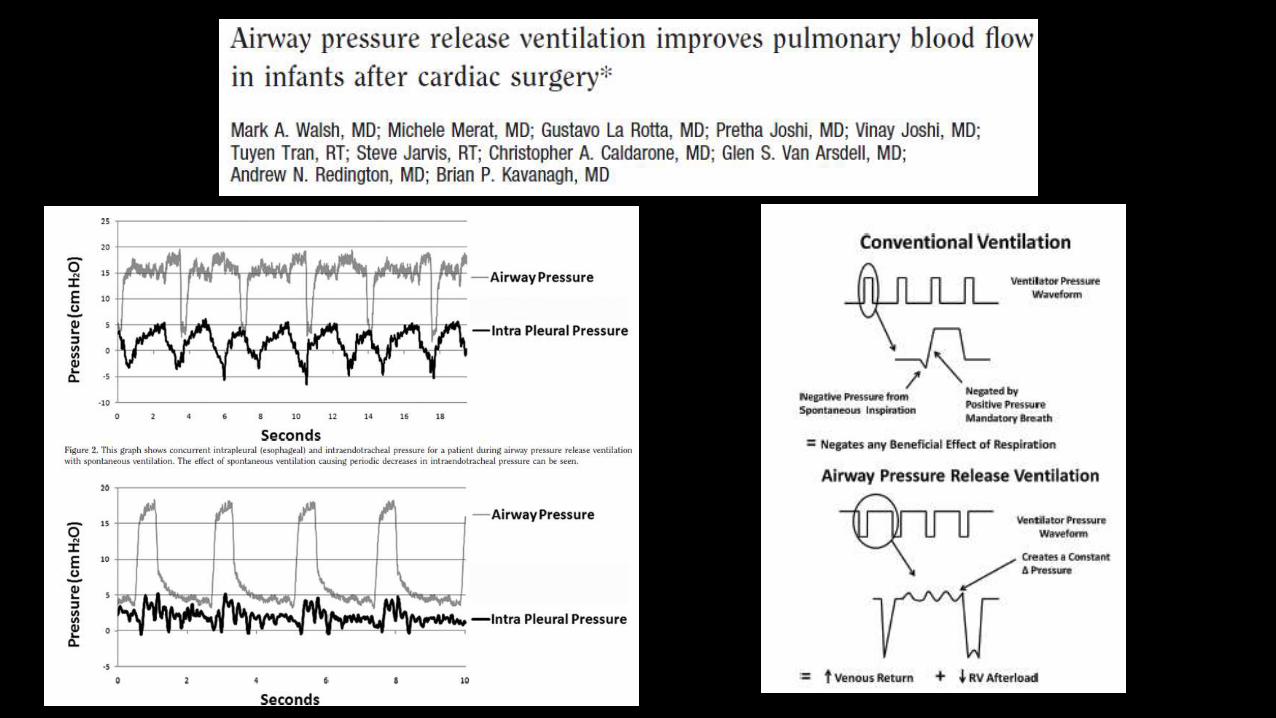
APRV and Pulmonary vascular resistance
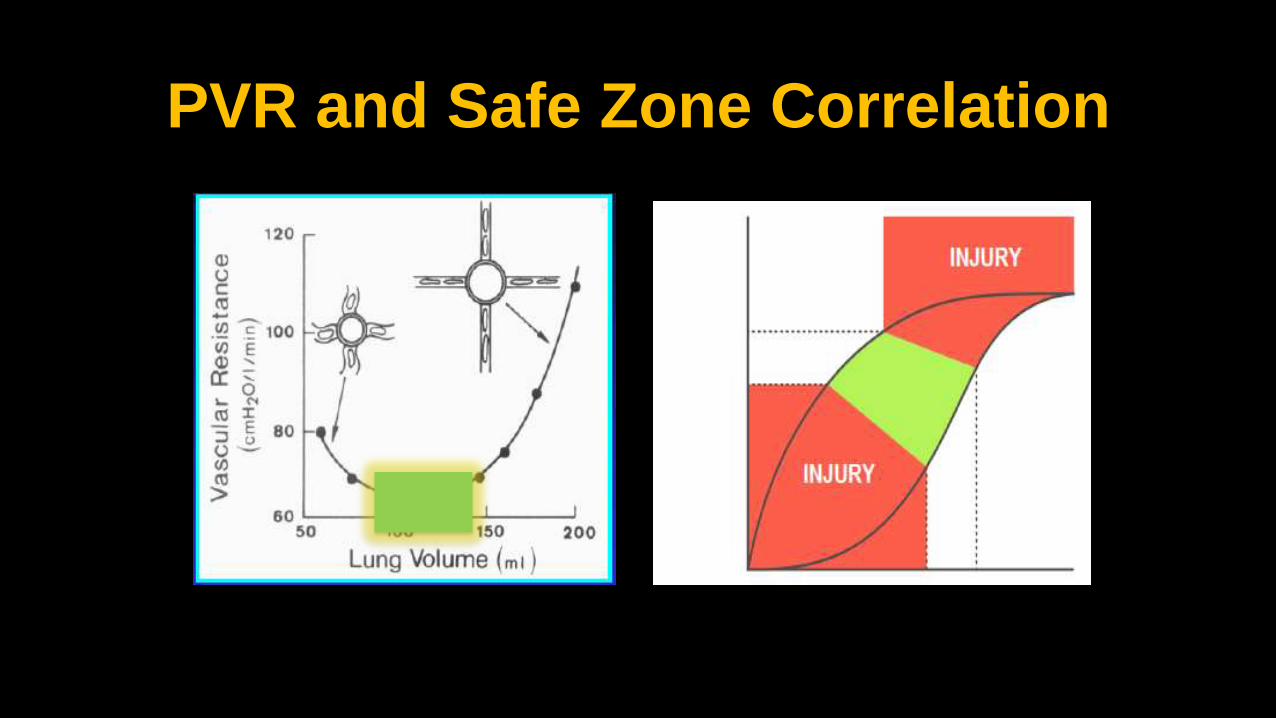
PVR and Safe Zone Correlation
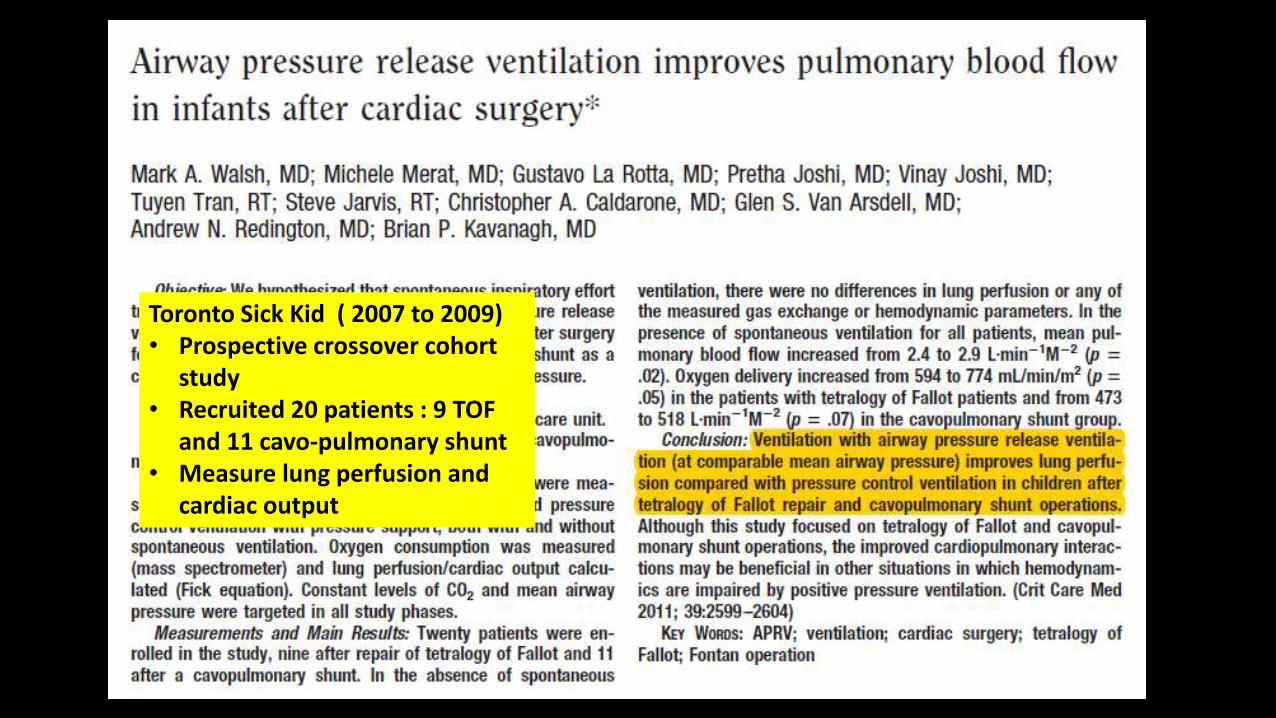
Toronto Sick Kid ( 2007 to 2009) • Prospective crossover cohort
study • Recruited 20 patients : 9 TOF
and 11 cavo-pulmonary shunt • Measure lung perfusion and
cardiac output


Elevated CPAP Level
• Gradually recruit lung to achieve FRC via collateral respiration
• Reduction of micro-strain to the alveoli that prevent ventilator induced lung injury
• At FRC, improve pulmonary perfusion and oxygen delivery

Features of APRV
Elevated CPAP Level
Time Pressure Release
Spontaneous breathing

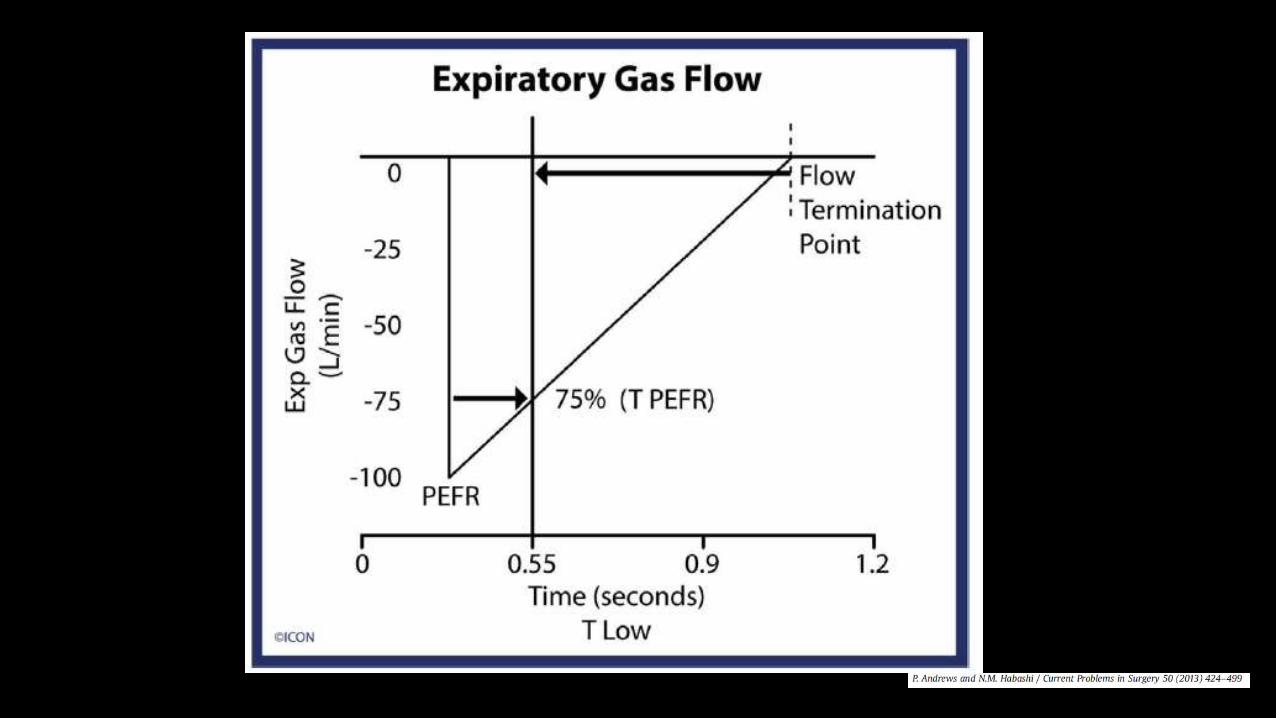
Intermitent release ( T low )
•Setting T PEFR ( EEFR/PEFR ) 50 to 75% with P Low of 0 cmH20 •Determine the amount of end expiratory lung volume ( EELV) that is retained.
•Maintained alveolar stability
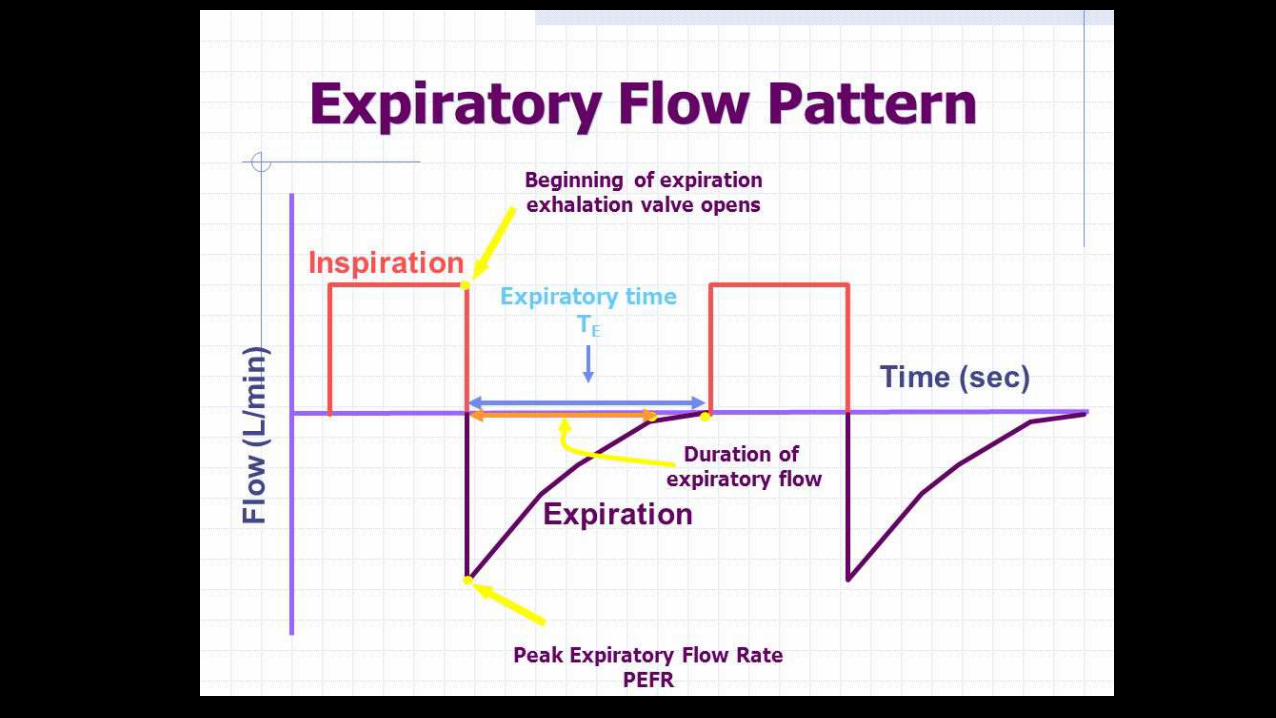
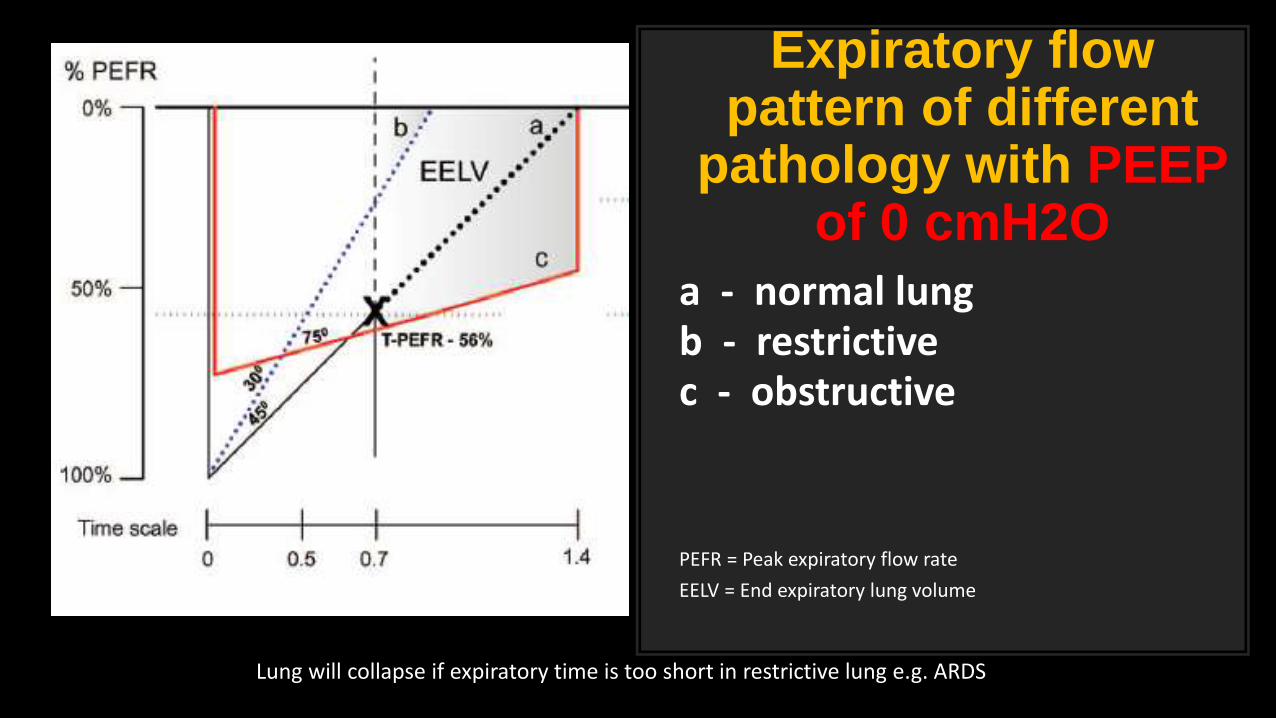
Expiratory flow pattern of different
pathology with PEEP of 0 cmH2O
a - normal lung b - restrictive c - obstructive
PEFR = Peak expiratory flow rate
EELV = End expiratory lung volume
Lung will collapse if expiratory time is too short in restrictive lung e.g. ARDS

More restrictive lung shorter T Low

Despite P low is 0 cm H2O Actual tracheal pressure never reach 0 cmH2O (Green line)
AutoPEEP which maintain alveolar stability

APRV ventilation at T-PEFR 75% There is only 10% of variation of alveolar volume between end inspiration and
release phase at injured animal lung model

Normal alveoli
No stain Alveoli duct and alveoli sac
Alveolus

Injured rat model

Time Pressure Release
• Titration based on lung mechanic that maintained stability of lung
• At T-PEFR of 75%, there is significant reduce in conducting airway microstrain
Features of APRV
Elevated CPAP Level
Time Pressure Release
Spontaneous breathing

Spontaneous breathing at APRV
• Spontaneous breathing enhance cardiopulmonary and organ perfusion benefit.
• Spontaneous breathing without pressure support favor gas distribution to dependent area

APRV


60
PubMed Search 1987 to 2015 Excluding NIV, review, editorials and case studies
(52 articles)
32 animal studies
28 human studies
Wide variety of APRV setting have all been used in literature making comparison between studies difficult
Study designs are mainly • Cossover • Randomized prospective • Retrospective case control • Retrospective review

1. None of the studies reviewed showed a worse outcome using APRV as compared with CPPV
2. Many studies showing significant benefits in cardiopulmonary variables
3. P-APRV personalized, adaptive mechanical breath may prove more efficacious at treating and preventing ARDS than the current standard of care
4. More studies are needed using consistent and well-defined settings to identify the optimal APRV breath necessary to maximize lung protection

Let’s see

APRV in Neonate
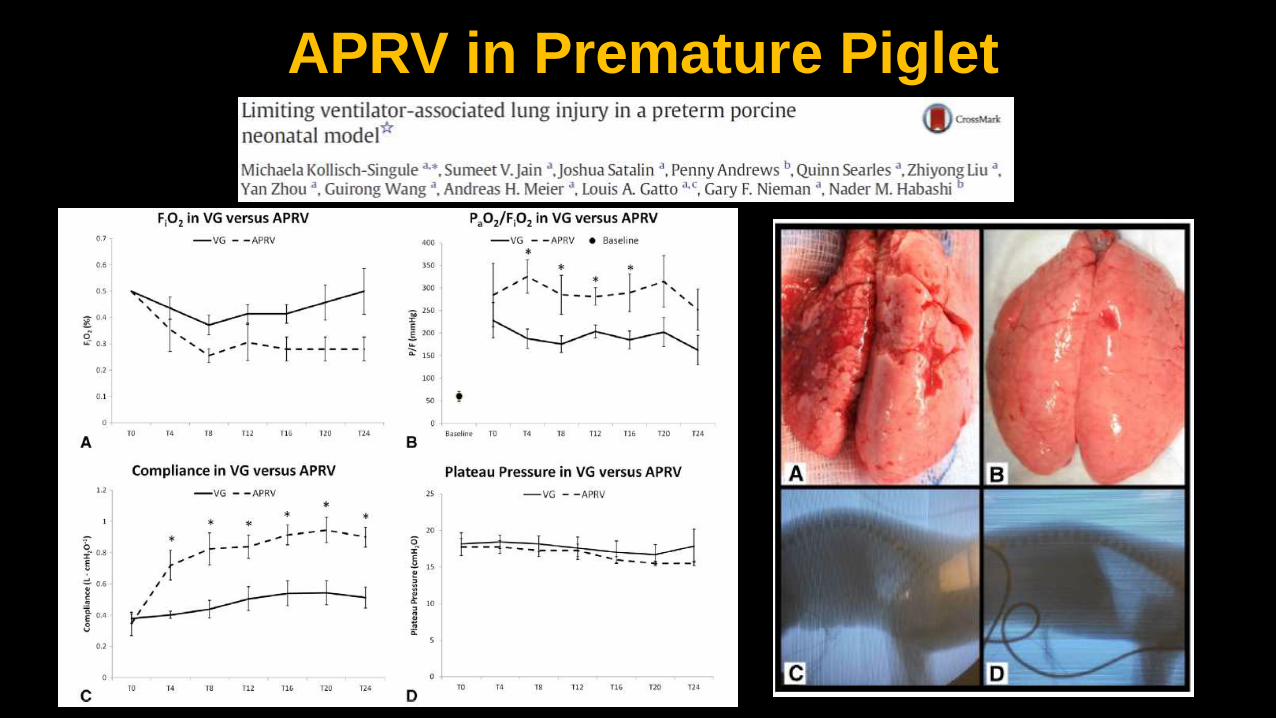
APRV in Premature Piglet
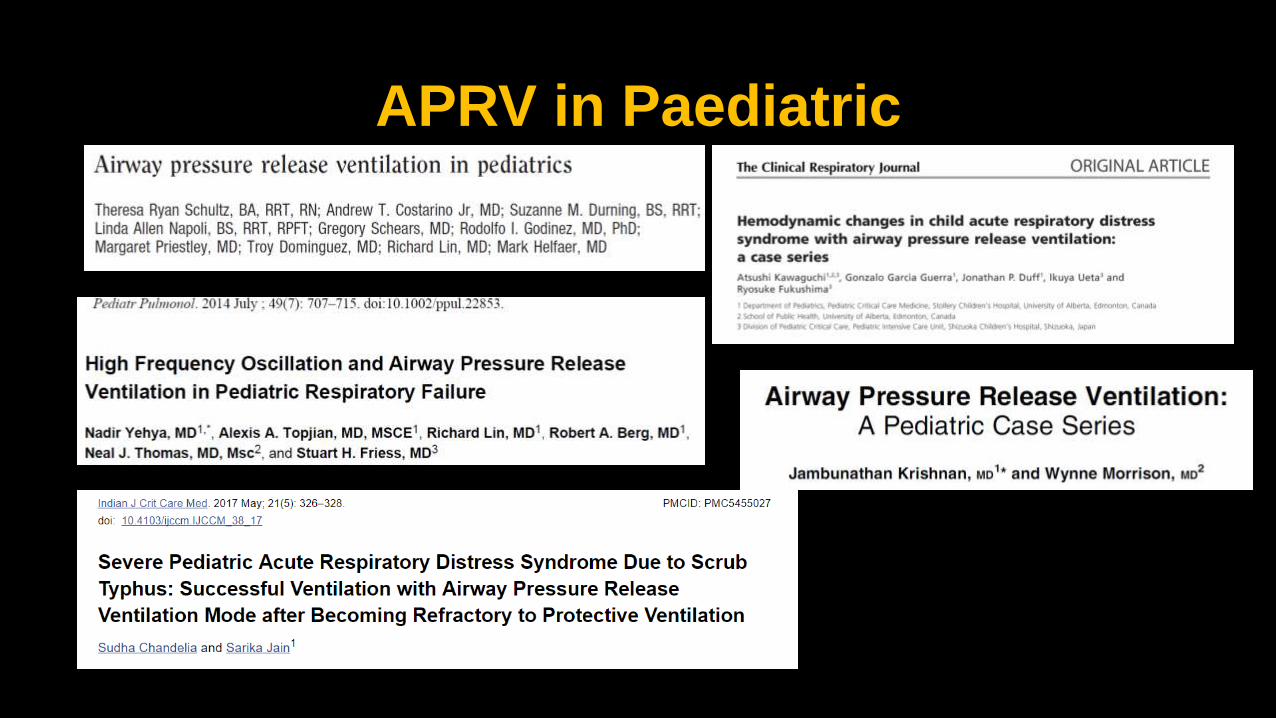
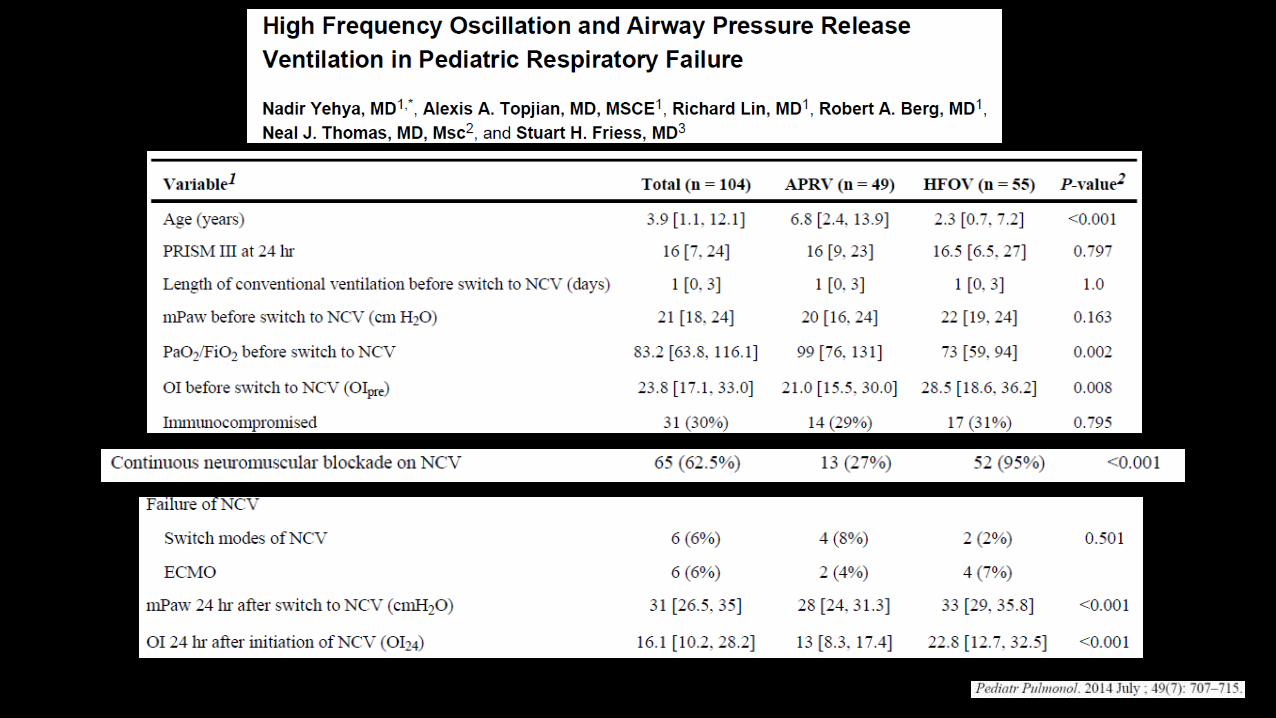
APRV in Paediatric
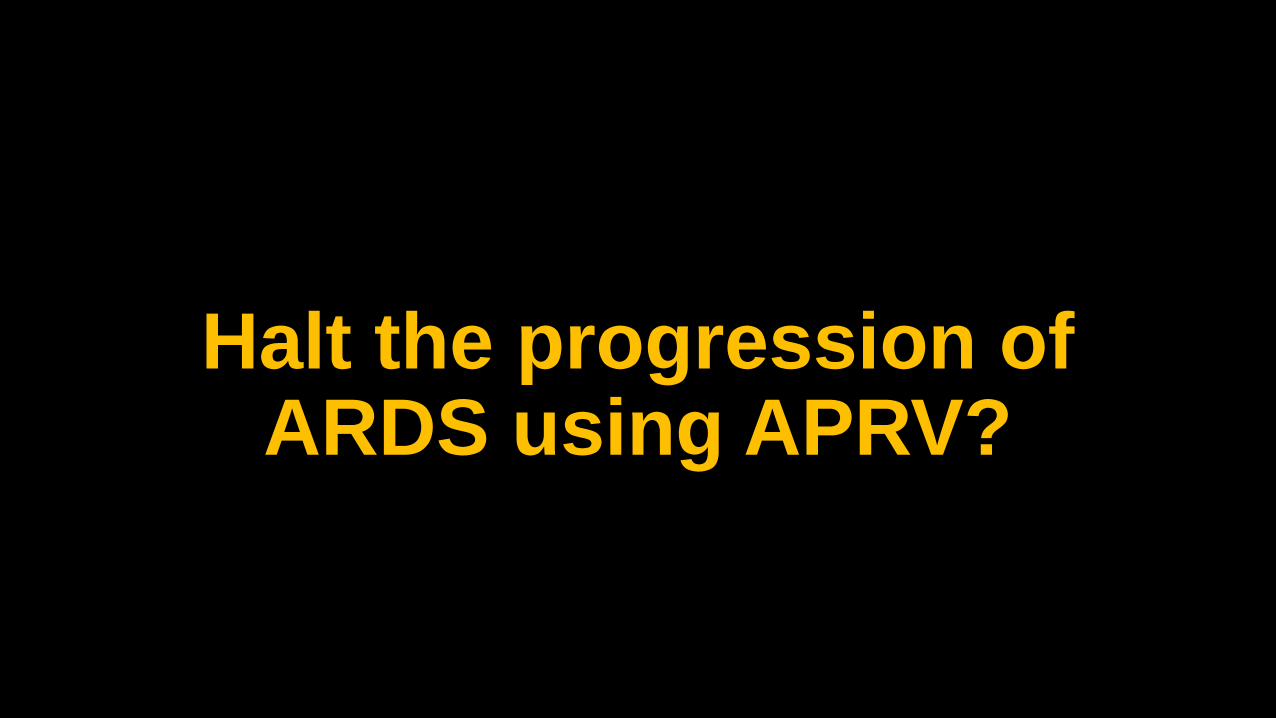
Halt the progression of ARDS using APRV?

Systemic review • 16 articles • 66,199 patients


What is actually happening out there?

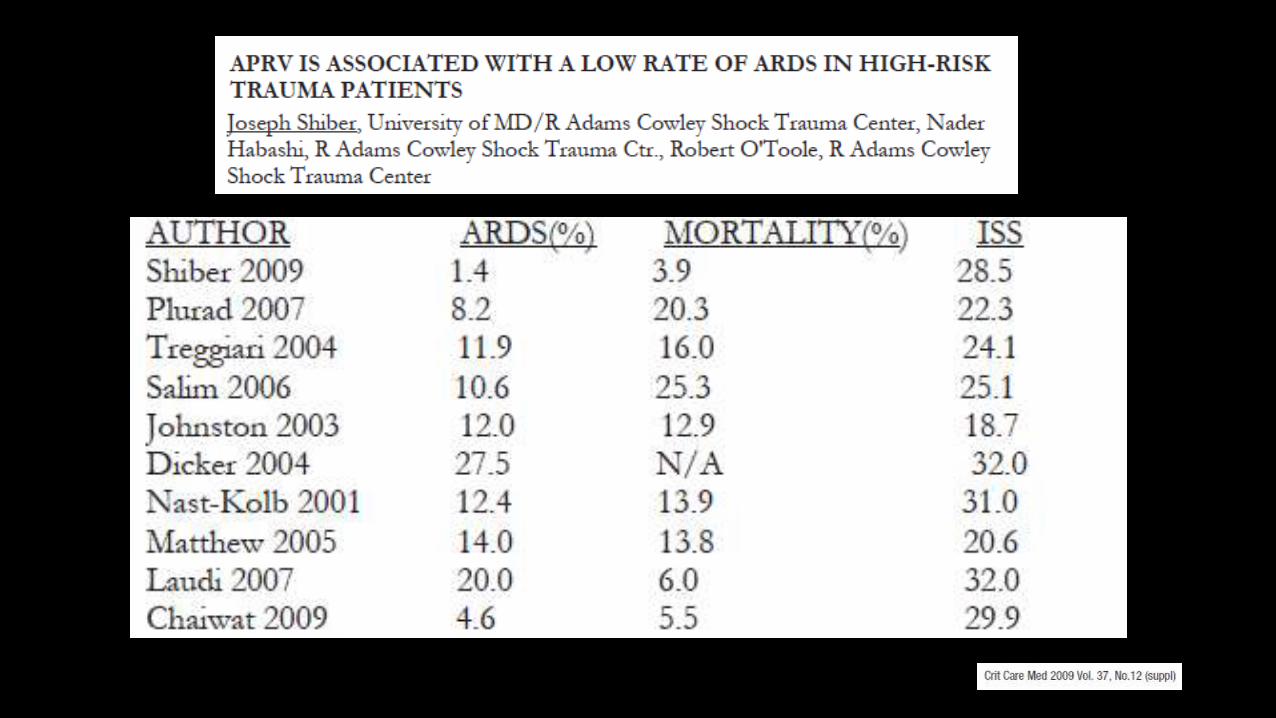
Respiratory Care June 2017
15 questions survey regarding clinical management strategies with APRV • Started January 4 , 2016 • Total 60 respondent from 60
different hospital. • 74% of these hospital use APRV
as initial rescue strategy for patient failing conventional ventilator .

Respiratory Care June 2017, respcare.05494
Respiratory Care June 2017, respcare.05494

Respiratory Care June 2017, respcare.05494

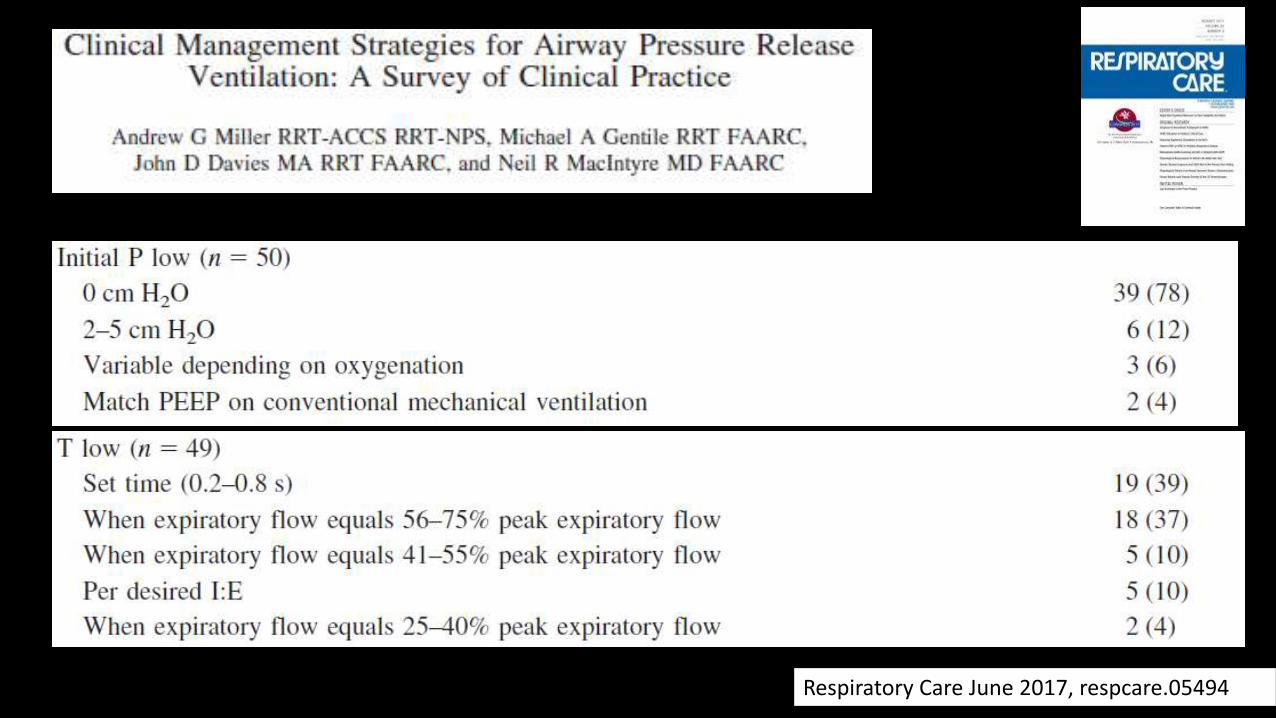
Amato et NEJM 2015
Amato et NEJM 2015

Conclusion from current evidence
1. Tremendous variation in setting of APRV, most of the study regarding the setting were physiology concept, animal data and small clinical trial
2. Impossible to assess efficacy of a single strategy since almost none of the APRV setting were identical.
3. Studies compare between APRV and CPPV did not show worse outcome but showing significant benefit in cardiopulmonary variables.
4. Personalized APRV (P-APRV) may prove more efficacious at treating and preventing ARDS.
5. APRV reduces sedation and neuromuscular blocker requirements

Thank you

![Relationship between Acute Lung Injury and the …UIP) from pressure-volume curves [3]. In recent years, airway pressure release ventilation (APRV) based on the Open-Lung Concept (OLC)](https://img.dokumen.tips/doc/110x75/5fb68c67ea1e206cf65ee588/relationship-between-acute-lung-injury-and-the-uip-from-pressure-volume-curves.jpg)