Embed Size (px)
Citation preview

Sean Tierney,
Consultant Vascular Surgeon
Adelaide & Meath National Children’s Hospital,
Tallaght
Issues Issues in in
AAA managementAAA management20132013
http://www.perfuse.netVascular surgery @ Tallaght
AAA - Issues for discussionAAA - Issues for discussion
• Screening• Surveillance• Predicting Operative Risk
– Reducing operative risk
• Choosing operative option
• Perioperative issues
• Technical – Open repair– EVAR
• Complex anatomy– Fenestrated– Branched

http://www.perfuse.netVascular surgery @ Tallaght
ScreeningScreening
“Multicentre Aneurysm Screening Study” Thompson S G et al. BMJ 2009

http://www.perfuse.netVascular surgery @ Tallaght
ScreeningScreening
• £7600 after 10 years (per DALY gained)
• Impact of EVAR unknown
“Multicentre Aneurysm Screening Study” Thompson S G et al. BMJ 2009
http://www.perfuse.netVascular surgery @ Tallaght
ScreeningScreening
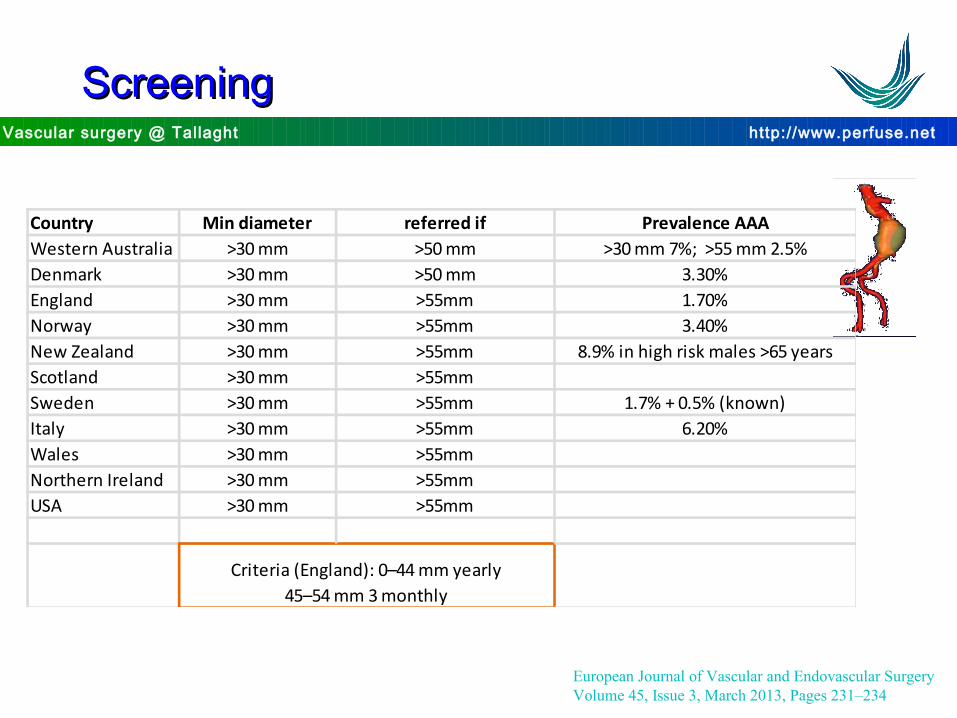
Country Min diameter referred if Prevalence AAAWestern Australia >30 mm >50 mm >30 mm 7%; >55 mm 2.5%Denmark >30 mm >50 mm 3.30%England >30 mm >55mm 1.70%Norway >30 mm >55mm 3.40%New Zealand >30 mm >55mm 8.9% in high risk males >65 yearsScotland >30 mm >55mmSweden >30 mm >55mm 1.7% + 0.5% (known)Italy >30 mm >55mm 6.20%Wales >30 mm >55mmNorthern Ireland >30 mm >55mmUSA >30 mm >55mm
Criteria (England): 0–44 mm yearly45–54 mm 3 monthly
European Journal of Vascular and Endovascular SurgeryVolume 45, Issue 3, March 2013, Pages 231–234

http://www.perfuse.netVascular surgery @ Tallaght
PrognosisPrognosis
Szilagyi 1966
% 5 year survival
6cm
http://www.perfuse.netVascular surgery @ Tallaght
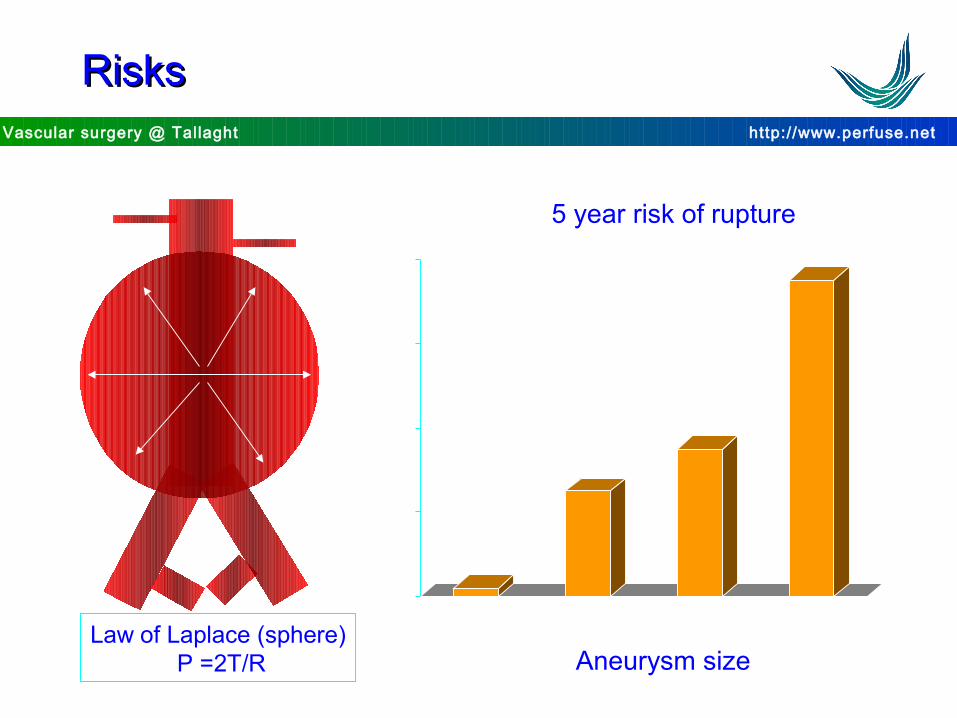
Law of Laplace (sphere) P =2T/R
0
20
40
60
80
<5cm 5.0-5.9cm >6.0-6.0cm >7.0cm
5 year risk of rupture
Aneurysm size
RisksRisks

http://www.perfuse.netVascular surgery @ Tallaght
Operative mortality (open repair)Operative mortality (open repair)
Brady et al. BJS 2000 (Small AAA trial)

http://www.perfuse.netVascular surgery @ Tallaght
Predictors of mortalityPredictors of mortality
0.04 0.01
0.01
Brady et al. BJS 2000 (Small AAA trial)
http://www.perfuse.netVascular surgery @ Tallaght
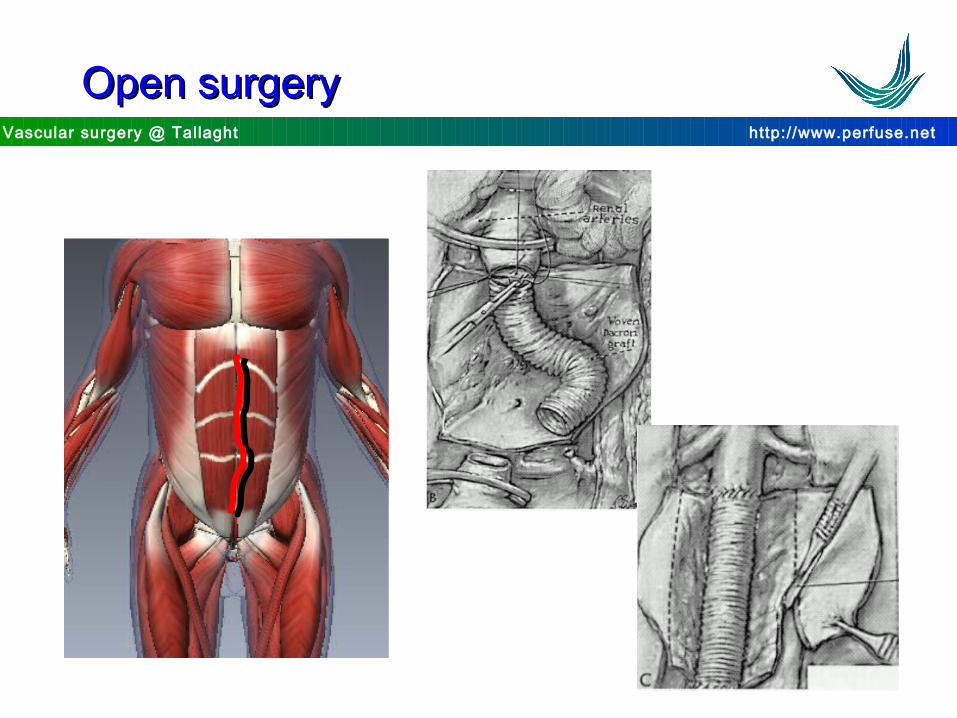
Open surgeryOpen surgery

http://www.perfuse.netVascular surgery @ Tallaght
New technologyNew technology
Parodi et al Ann Vasc 1991
http://www.perfuse.netVascular surgery @ Tallaght
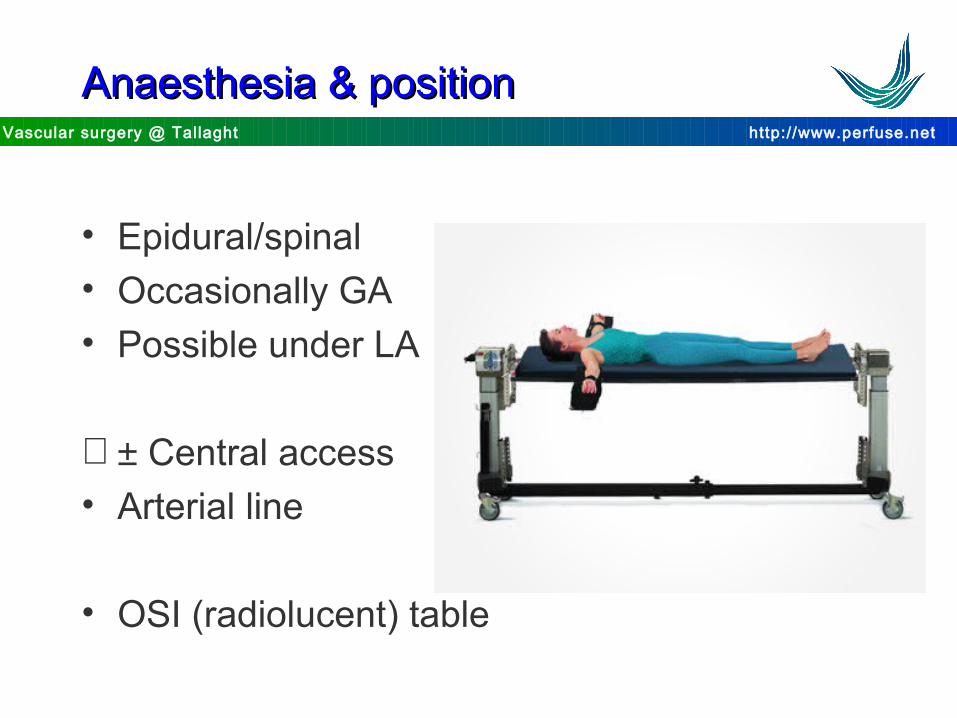
Anaesthesia & positionAnaesthesia & position
• Epidural/spinal• Occasionally GA• Possible under LA
∀ ± Central access• Arterial line
• OSI (radiolucent) table
http://www.perfuse.netVascular surgery @ Tallaght
PositionPosition
• Arms tucked in by sides
• Contrast pressure injector (angio)
• C Arm
• 2 tables – open/endo

http://www.perfuse.netVascular surgery @ Tallaght
Set up & equipmentSet up & equipment
1
2
Scrub/N 1
C-arm
Monitors
Injector
Scrub/N 2
http://www.perfuse.netVascular surgery @ Tallaght
Draping & incisionDraping & incision

http://www.perfuse.netVascular surgery @ Tallaght
ExposureExposure

http://www.perfuse.netVascular surgery @ Tallaght
AnimationAnimation
Tri Fab design
http://www.perfuse.netVascular surgery @ Tallaght
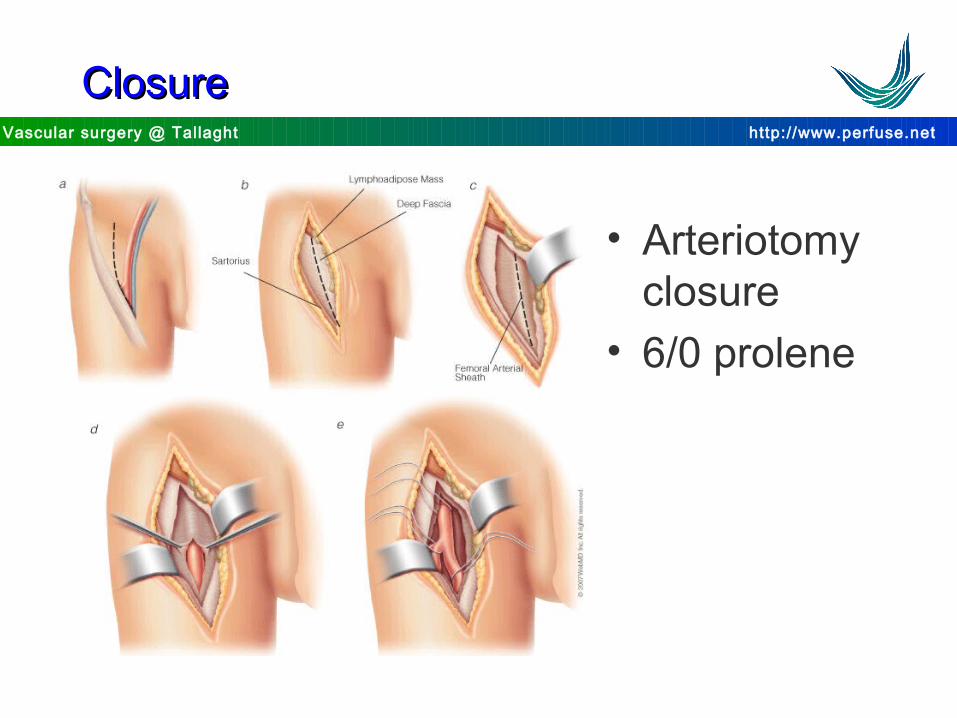
ClosureClosure
• Arteriotomy closure
• 6/0 prolene
http://www.perfuse.netVascular surgery @ Tallaght
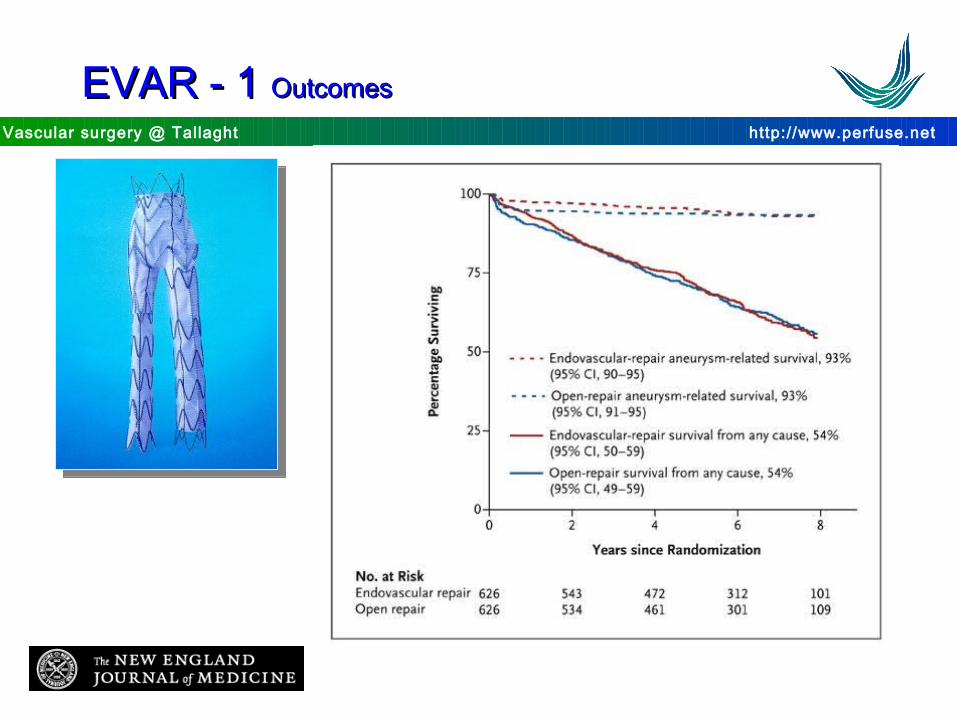
EVAR - 1 EVAR - 1 OutcomesOutcomes

http://www.perfuse.netVascular surgery @ Tallaght
ReinterventionsReinterventions
Trial Year N AAA Reinterventions P valueEVAR Open
EVAR 2010 1252 > 5.5 cm 10% 28% <0.001
DREAM 2010 351 > 5 cm 30% 18% 0.03
ACE 2011 316 > 5 cm 24% 14% <0.01
OVER 2012 881 > 5 cm 22.1%b 17.8%b 0.12
European Journal of Vascular and Endovascular SurgeryVolume 45, Issue 4, April 2013, Pages 313–314

http://www.perfuse.netVascular surgery @ Tallaght
EVAR - 2 EVAR - 2 OutcomesOutcomes
Lancet 2005; 365: 2187–92
http://www.perfuse.netVascular surgery @ Tallaght
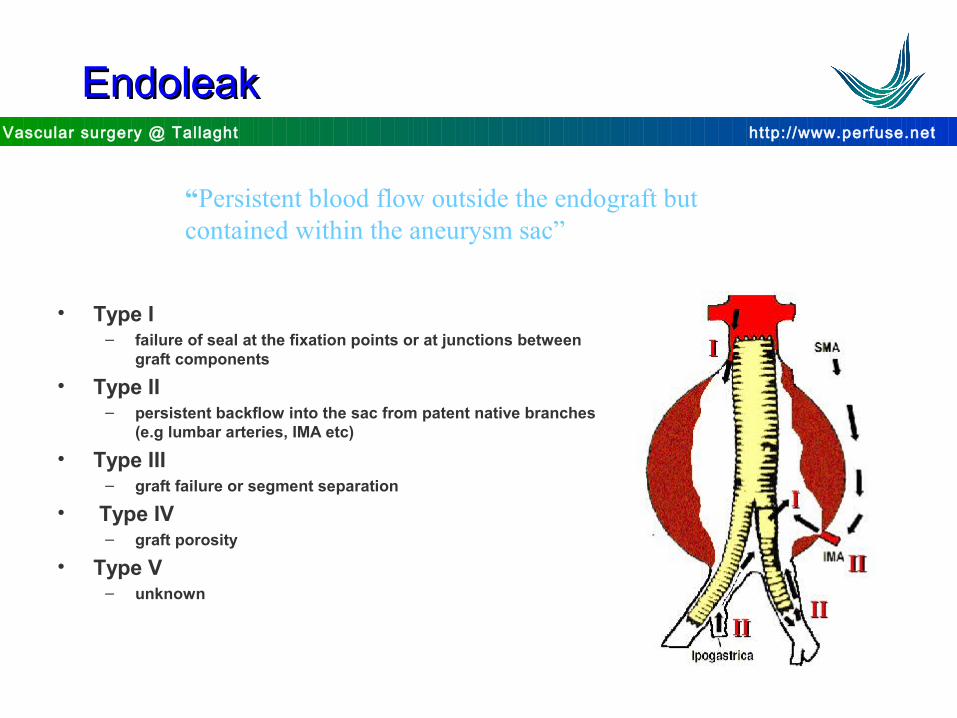
EndoleakEndoleak
“Persistent blood flow outside the endograft but contained within the aneurysm sac”
• Type I– failure of seal at the fixation points or at junctions between
graft components
• Type II– persistent backflow into the sac from patent native branches
(e.g lumbar arteries, IMA etc)
• Type III– graft failure or segment separation
• Type IV– graft porosity
• Type V– unknown


http://www.perfuse.netVascular surgery @ Tallaght
OptionsOptions
??


http://www.perfuse.netVascular surgery @ Tallaght
Fenestrated graftFenestrated graft


http://www.perfuse.netVascular surgery @ Tallaght
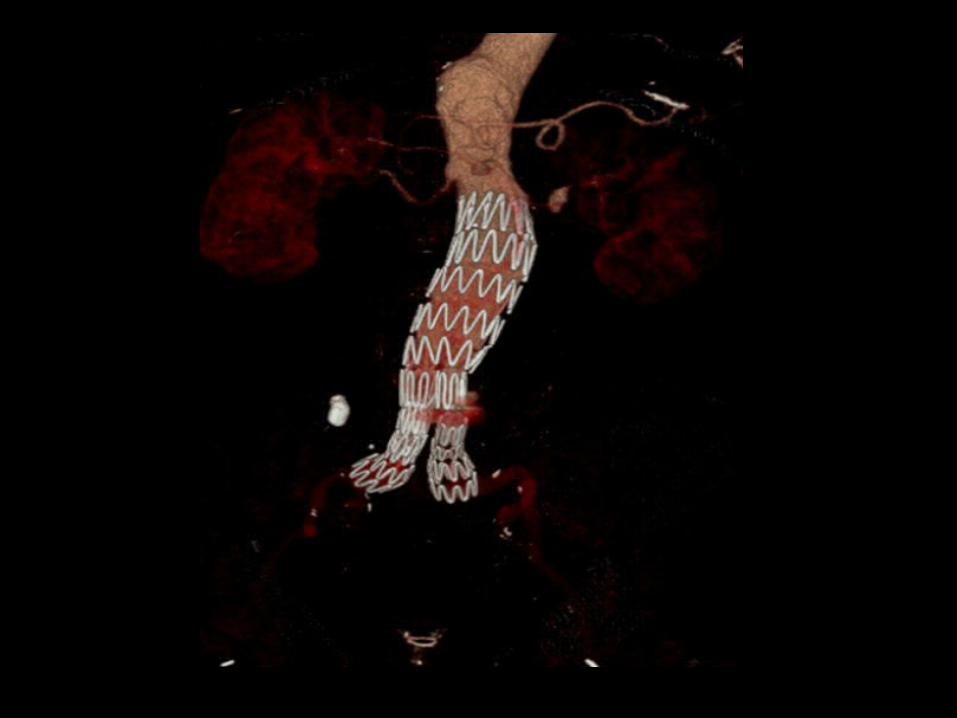
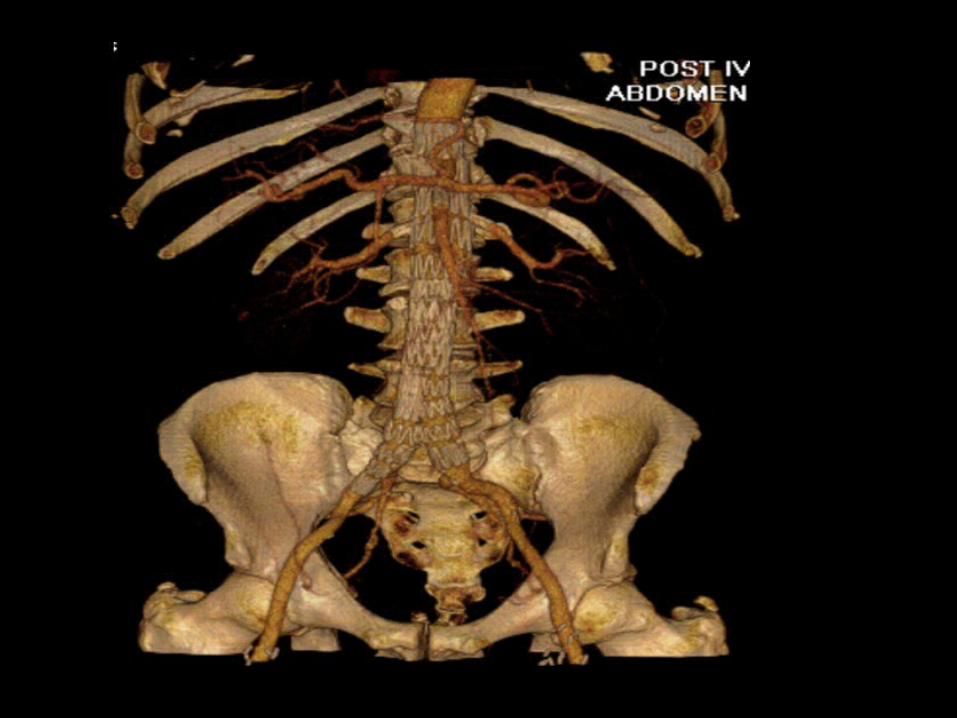
Iliac branch graftIliac branch graft
http://www.perfuse.netVascular surgery @ Tallaght
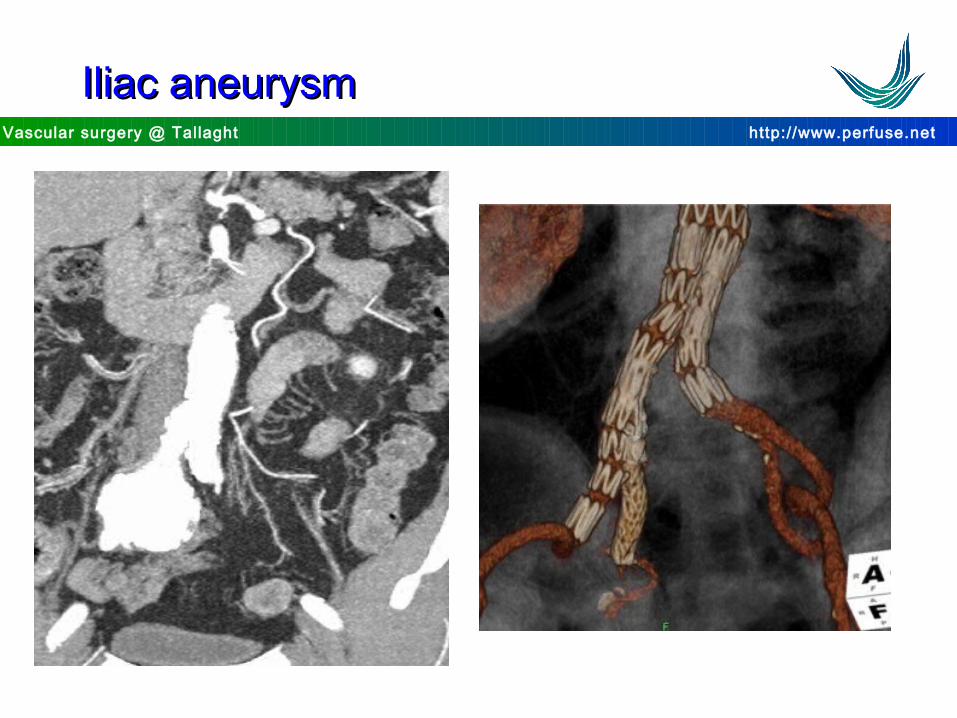
Iliac aneurysmIliac aneurysm


http://www.perfuse.netVascular surgery @ Tallaght
Place for EVARPlace for EVAR
IndicationsIndications• still unresolved issues• anatomical suitability• older vs younger• ? high risk patient• significant costs
• Complement rather than replaces open surgery