Embed Size (px)
Citation preview
A critical analysis of purchasing arrangements operating under the tax-funded health system in South Africa
Ayako HondaHealth Economics Unit, University of Cape TowniHEA, Milan; Tuesday 14 July, 2015
South African tax-funded health services
• Mainly used by those without medical scheme coverage, including low-income formal sector workers, informal sector workers, the unemployed and the poor; the combination of which account for approximately 83% of the population
• Tax funds are centrally collected by the South African Revenue Services (SARS), generated mainly from personal income tax, Value Added Tax, company tax
• The government allocates funds to provinces (for all sectors) using a needs-based formula (Provincial Equitable Share)
• Each province has the autonomy to decide on how funds are allocated to individual sectors

South African tax-funded health services
• Provincial Departments of Health (PDoHs) receive budget from Provincial Treasuries and allocate funds to health providers
• PDoHs also receive NDoH Conditional Grants to fund work focussed on specific national government policy objectives
• Public sector health facilities are allocated line-item budgets and staff are paid salaries to work at facilities
• Public facilities offer a relatively comprehensive range of service benefits but quality challenges

Actors in purchasing in the South African tax-funded health services
• PurchaseroProvincial Department of Health (PDoH)
• GovernmentoNational Department of Health (NDoH) develops norms
and standards for health care service provisionoProvincial Treasury (P Treasury) allocates health sector
budget to PDoH and monitors PDoH financial management
Actors in purchasing in the South African tax-funded health services
• Providerso Public sector health providers, including community health
centres and clinics, district hospitals and regional and other tertiary hospitals
o Private sector health providers supply specific types of health services
• Citizenso People in the province/countryo Community Health Centre Committee (CHCCs) and Hospital
Boards as community accountability mechanisms o Community-based organisations (CBOs)
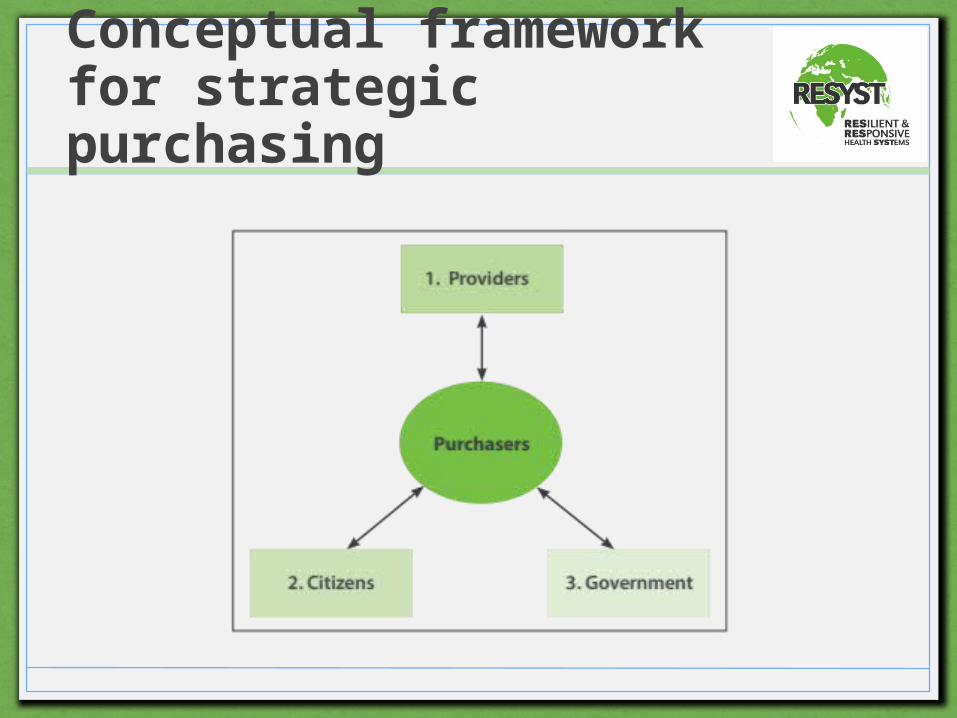
Conceptual framework for strategic purchasing
Overview of results: Purchaser-Government relationship• The ability of NDoH to enforce national public health
priorities to be reflected in purchasing decision-making is limited due to federal mechanisms that provide strong decision-making authority to PDoH, and PDoH decision-making that reflects its own political and local context
• The National Treasury, through Provincial Treasuries, uses a number of monitoring / communication strategies to ensure PDoH adherence with the Public Finance Management Framework in spending the provincial equitable share
• PDoH undertake strict management of their budget so that they can secure a large proportion of the provincial budget for use in the health sector
Overview of results: Purchaser-Provider relationship
• PDoH considers the socio-economic situation of communities when allocating budget
• PDoH provides line-item budget, salaries, guidance, support, and monitoring to health providers for health care service provision
• Although these mechanisms can be considered as tools for the public purchaser to use in strategic purchasing, they are embedded in existing public sector health systems and do not send specific signals for efficiency, equity and quality improvement
Overview of results: Purchaser-Citizen relationship
• While formal mechanisms exist to determine people’s needs, preferences and values, many of the mechanisms (e.g. community health centre committees (CHCCs) and hospital boards) do not function as government policy intends in terms of serving as accountability and communication intermediaries between communities and health facilities
• Implementation gaps result from: o inadequacies in (and/or absence of) policy design o local political contexts o lack of the required skills/time by health facility managerso lack of appropriate knowledge/skills in health facility board
memberso lack of community awareness

Key policy implications
• Whether a centralised or de-centralised purchasing mechanism provides environment that is more enabling for public purchasers and other key actors to undertake strategic purchasing needs to be established
• Strong awareness of strategic purchasing by PDoH and the introduction of strategic purchasing elements in the purchaser-provider relationship are necessary if the tools are to function effectively
• Public purchasers must provide clear guidance, frequent communication, technical support and resources to implementation-level actors and the community if true community participation and accountability mechanisms are to be realised
www.wpro.who.int/asia_pacific_observatoryhttp://resyst.lshtm.ac.uk@RESYSTresearch
The research is a collaboration between RESYST and the Asia Pacific Observatory on Health Systems and Policies.
RESYST is funded by UK aid from the UK Department for International Development (DFID). However, the views expressed do not necessarily reflect the Department’s official policies.
More information: http://resyst.lshtm.ac.uk/research-projects/multi-country-purchasing-study