Embed Size (px)
Citation preview

RHEUMATIC RHEUMATIC HEART DISEASE WITH HEART DISEASE WITH MYOCARDIAL INFARCTIONMYOCARDIAL INFARCTION
DR.A.VIJAYALAKSHMI.DR.A.VIJAYALAKSHMI.Prof.P.VIJAYARAGAVAN UNIT.Prof.P.VIJAYARAGAVAN UNIT.
UNIT M6.UNIT M6.

Mr.Shankar 37yrs male PainterMr.Shankar 37yrs male Painter
Admitted with complaints of Breathlessness, cough for Admitted with complaints of Breathlessness, cough for one week durationone week duration..
History of present illnessHistory of present illness::
A known case of RHD for 8 yrs. On regular treatment A known case of RHD for 8 yrs. On regular treatment discontinued his medicine for 1 week had dyspnea of discontinued his medicine for 1 week had dyspnea of grade IV associated with cough was brought to SMCgrade IV associated with cough was brought to SMC..

• There was no h/o chest pain, syncope, palpitations.There was no h/o chest pain, syncope, palpitations.
• No h/o fever and sputum expectoration.No h/o fever and sputum expectoration.
..• No h/o rhematic fever and no evidence of infective No h/o rhematic fever and no evidence of infective
endocarditisendocarditis..

Past history:Past history:
Known RHD. No D.M, H.T, Epilepsy, NoT.BKnown RHD. No D.M, H.T, Epilepsy, NoT.B..
Personal historyPersonal history::
Nil relevantNil relevant..
Family historyFamily history::
Nil relevantNil relevant..
Treatment historyTreatment history::
He was on T.Digoxin 0.25mg ½ ODHe was on T.Digoxin 0.25mg ½ OD
T.Frusemide40mg ½ ODT.Frusemide40mg ½ OD
Syp.KCL 10 ml tds.Syp.KCL 10 ml tds.
T.Aspirin 150 mg ½ ODT.Aspirin 150 mg ½ OD
T.Penicillin 250mg 1BD.T.Penicillin 250mg 1BD.
T.Enalapril 2.5 mg 1 BD. He discontinued these drugs for 1 T.Enalapril 2.5 mg 1 BD. He discontinued these drugs for 1 week as he went away from native place for his job purpose.week as he went away from native place for his job purpose.

GENERAL EXAMINATIONGENERAL EXAMINATION
• Conscious, oriented . Afebrile.Conscious, oriented . Afebrile.• No cyanosis, no clubbing, no pedal edema,No cyanosis, no clubbing, no pedal edema,• Not icteric, no generalised lymphaadenopathy.Not icteric, no generalised lymphaadenopathy.• JVP raised.JVP raised.• Pulse ;178/min.irreularly irregular.Felt equaly in all Pulse ;178/min.irreularly irregular.Felt equaly in all
limbs.limbs.• Pulse deficit 40/min.Pulse deficit 40/min.• BP:140/70 mmof Hg.BP:140/70 mmof Hg.

Cardiovascular examination:Cardiovascular examination:• First and second heart sound heard in all the area.First and second heart sound heard in all the area.• First sound heard with varying intensity.First sound heard with varying intensity.• Pan systolic murmur present in the mitral area conducted Pan systolic murmur present in the mitral area conducted
to axilla and MDM present in the mitral region. to axilla and MDM present in the mitral region. • Loud P2 present in the pulmonary areaLoud P2 present in the pulmonary area..

Respiratory system:Respiratory system:• Normal vesicular breath sounds heardNormal vesicular breath sounds heard..
Abdomen:Abdomen:• Soft , mild Hepatomegaly presentSoft , mild Hepatomegaly present..
Central nervous systemCentral nervous system::• No focal neurological deficitNo focal neurological deficit..

TREATMENTTREATMENT
• He was continued digoxin ,lasix, He was continued digoxin ,lasix, enalapril,aspirin,syp.KCL.enalapril,aspirin,syp.KCL.
• He was sent for ECHO and cardiology opinionHe was sent for ECHO and cardiology opinion . .
Cardiology opinionCardiology opinion : :• Advised to start T.Metoprolol 50mg ½ OD., T. Advised to start T.Metoprolol 50mg ½ OD., T.
Aldactone 25mg 1OD.Aldactone 25mg 1OD.• T.Enalapril2.5mg1BD.T.Enalapril2.5mg1BD.• ECHO was done.ECHO was done.
ECHOCARDIGRAPHY on 3. 5 10ECHOCARDIGRAPHY on 3. 5 10..• Small LA appendage clot present.Small LA appendage clot present.• LA size 5 cm.LA size 5 cm.• Aorta3.3cm.Aorta3.3cm.• AV opening17mm.AV opening17mm.• LA/LV dilated.LA/LV dilated.• MS moderate 1.4cmMS moderate 1.4cm• MPC 80mm 0f Hg.MPC 80mm 0f Hg.• MR mild.MR mild.• AR moderate, Severe LV dysfunction EF 30%AR moderate, Severe LV dysfunction EF 30%

• He was started on Inj. Heparin 5000U I.V Q.I.D. He was started on Inj. Heparin 5000U I.V Q.I.D. • The course of Heparin was over and we planned for The course of Heparin was over and we planned for
discharge since the patient is doing his day today activities discharge since the patient is doing his day today activities well and good .well and good .
• On 8.5.10 patient developed chest pain and also had On 8.5.10 patient developed chest pain and also had sweating . Possibility of Aspirin-induced Gastritis was sweating . Possibility of Aspirin-induced Gastritis was considered.considered.

• He was given Inj.25% dextrose and inj.Ranitidine He was given Inj.25% dextrose and inj.Ranitidine 50mg.50mg.
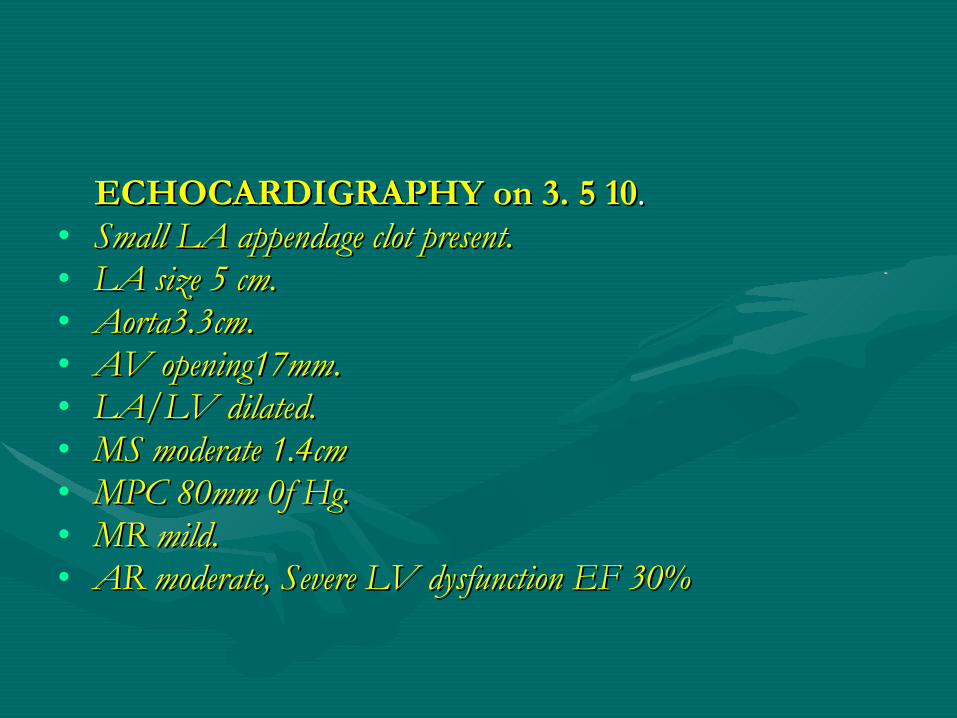
• The chest pain not controlled. ECG was taken - showed The chest pain not controlled. ECG was taken - showed Hyper-Acute Anterior wall MI.Hyper-Acute Anterior wall MI.
• Patient was shifted to ICCU.Patient was shifted to ICCU.

ON admission ECG dated 1.5 10ON admission ECG dated 1.5 10
On the day of MI on 8.5.10On the day of MI on 8.5.10
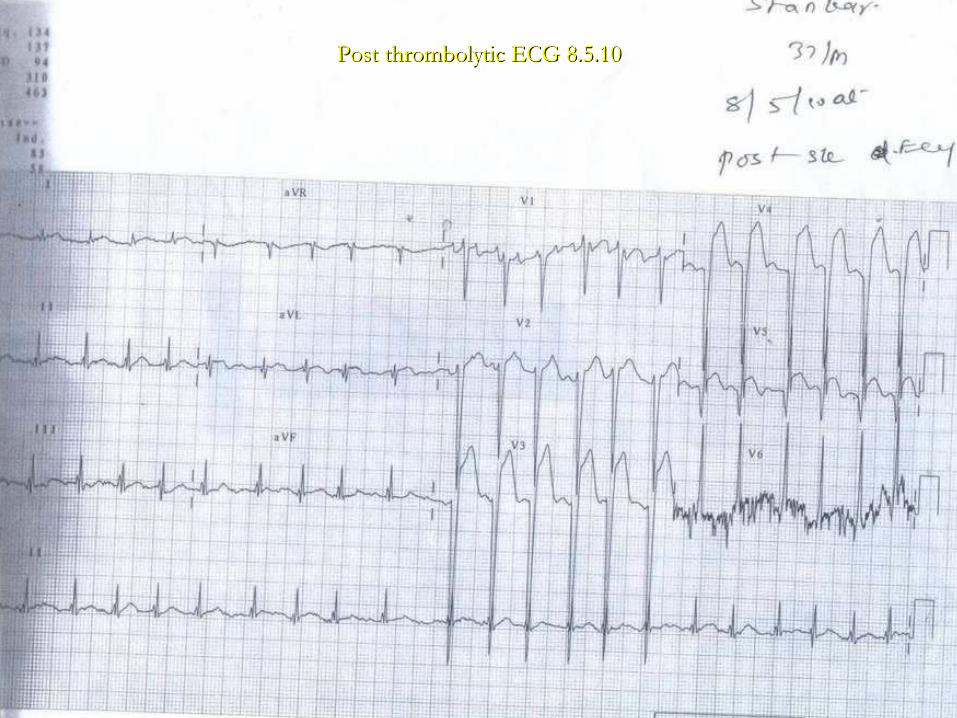
Post thrombolytic ECG 8.5.10Post thrombolytic ECG 8.5.10


FINAL DIAGNOSISFINAL DIAGNOSIS
• Rheumatic MS, MR , AR with AF with LA Rheumatic MS, MR , AR with AF with LA thrombus with coronary embolism .thrombus with coronary embolism .
Thromboembolism in RHD with AFThromboembolism in RHD with AF
• RHD with AF is the second most common cause of embolic RHD with AF is the second most common cause of embolic myocardial infarction.myocardial infarction.
• In AF the lack of an organized atrial contraction can result in In AF the lack of an organized atrial contraction can result in stagnant blood in the LA or Left atrial appendage and thus can stagnant blood in the LA or Left atrial appendage and thus can lead to a thromboembolismlead to a thromboembolism..
• Patients with AF and heart valve disease are at a higher risk for Patients with AF and heart valve disease are at a higher risk for developing embolism.developing embolism.
• The incidence of thromboembolism in AF is not affected by age, The incidence of thromboembolism in AF is not affected by age, sex, heart failure, chest pain, heart disease associated with high sex, heart failure, chest pain, heart disease associated with high BP, smoking, volume of heart and size of Left atriumBP, smoking, volume of heart and size of Left atrium..
• In AF the fast ventricular rate due to AF may cause In AF the fast ventricular rate due to AF may cause angina, leading to cardiac ischemia and heart failure.angina, leading to cardiac ischemia and heart failure.
Has poor prognosis with increased mortalityHas poor prognosis with increased mortality..
In addition thrmboembolism also causes cardiac ischemia In addition thrmboembolism also causes cardiac ischemia leading to myocadial infarctionleading to myocadial infarction..

DiscussionDiscussion
Antithrombotic therapy for valvular heart Antithrombotic therapy for valvular heart diseases.diseases.
For native valve disease require antithrombotic therapy For native valve disease require antithrombotic therapy only in the presence of an associated risk factors. The 2 only in the presence of an associated risk factors. The 2 most risk factors are AF and left ventricular LV systolic most risk factors are AF and left ventricular LV systolic dysfunction.dysfunction.
Atrial fibrillation:Atrial fibrillation:• Warfarin is recommended in the setting of prior systemic Warfarin is recommended in the setting of prior systemic
embolus or or if a patient has 2 or more of the embolus or or if a patient has 2 or more of the following-1.DM , H.T., CCF., age more than 75 following-1.DM , H.T., CCF., age more than 75 yrs.Those with none or only one of the risk factor can yrs.Those with none or only one of the risk factor can reasonably be given Aspirin 325mg/day.reasonably be given Aspirin 325mg/day.
LV dysfunctionLV dysfunction• Warfarin may be used if the LV EF<30%, or Warfarin may be used if the LV EF<30%, or
Aspirin 325mg may be used if warfarin is associated Aspirin 325mg may be used if warfarin is associated with risk.with risk.
• Prior thromboemboliPrior thromboemboli::• Life long warfarin should be consideredLife long warfarin should be considered..

Mechanical valvesMechanical valves • Require warfarin therapy. The INR between 2to3.If Require warfarin therapy. The INR between 2to3.If
risk factors present the INR may be to 2.5 to 3.5. with risk factors present the INR may be to 2.5 to 3.5. with addition of low dose aspirinaddition of low dose aspirin..
Biological valvesBiological valves• For 1For 1stst 3 months after implantation of the valve 3 months after implantation of the valve
warfarin is indicated ,after that it is treated as native warfarin is indicated ,after that it is treated as native valves. Associated LV dysfunction and AF are the valves. Associated LV dysfunction and AF are the situation for life long warfarinsituation for life long warfarin. .

Special situationSpecial situation
Surgery and dental care:Surgery and dental care:• For procedure in which bleeding is less likely For procedure in which bleeding is less likely
antithrombotic therapy should not be stopped.antithrombotic therapy should not be stopped.• If bleeding is likely If patient is on Aspirin it should be If bleeding is likely If patient is on Aspirin it should be
discontinued 1 week before the procedure.discontinued 1 week before the procedure.• And for pts. On warfarin , it should be stopped 72 And for pts. On warfarin , it should be stopped 72
hours before the procedure to achieve INR <1.5. unless hours before the procedure to achieve INR <1.5. unless postop hemorrahge occurs , warfarin can be restarted postop hemorrahge occurs , warfarin can be restarted within 24 hours of surgery.within 24 hours of surgery.

Pregnancy Pregnancy • For 1For 1stst 3 months Heparin to be given ,then switch over to 3 months Heparin to be given ,then switch over to
warfarin. At 1 to 3 weeks before labor and delivery, switch back warfarin. At 1 to 3 weeks before labor and delivery, switch back to Heparin.to Heparin.
Cardiac catheterization and AngiographyCardiac catheterization and Angiography• Neither antiplatelet therapy nor heparin is stopped. Preferably the Neither antiplatelet therapy nor heparin is stopped. Preferably the
warfarin can be stopped 72 hours before the procedure and warfarin can be stopped 72 hours before the procedure and restarted after the procedure on the same day. If the pt. is having restarted after the procedure on the same day. If the pt. is having risk of thromboembolism Heparin should be started 48 hours risk of thromboembolism Heparin should be started 48 hours before the procedure and continued until warfarin is startedbefore the procedure and continued until warfarin is started..

THERAPY AT THE TIME OF THERAPY AT THE TIME OF THROMBOEMBOLIC EVENTTHROMBOEMBOLIC EVENT
• If the embolic event occurs when a patient is off If the embolic event occurs when a patient is off antithrombotic therapy , long term warfarin is required. antithrombotic therapy , long term warfarin is required. If embolic events occurs while on antithrombotic therapy If embolic events occurs while on antithrombotic therapy the treatment should be altered as follows,the treatment should be altered as follows,

• If on warfarin, with an INR of 2to 3 increase the dose to If on warfarin, with an INR of 2to 3 increase the dose to achieve an INR of2.5 to 3.5.achieve an INR of2.5 to 3.5.
• If on warfarin ,with an INRof 2.5 to 3.5; add If on warfarin ,with an INRof 2.5 to 3.5; add aspirin50 to 100mg/d.aspirin50 to 100mg/d.
• If on warfarin ,with an INR of 2.5 to 3.5 ,plus If on warfarin ,with an INR of 2.5 to 3.5 ,plus aspirin100mg ;aspirin may be raised to 325mg/d.aspirin100mg ;aspirin may be raised to 325mg/d.
• Embolism occuring after this medical approach should Embolism occuring after this medical approach should lead to consideration of valve surgery if the valve is the lead to consideration of valve surgery if the valve is the likely source of the embolism.likely source of the embolism.

• THANK UTHANK U