1
FINAL VERSION – 20th of April 2004 - PDV accepted for publication in Social Science and Medicine- May 2004
planned publication: first trimester 2005
Shifting the Demand for Emergency Care in Cuba’s Health System Author Pol De Vos Department of Public Health - Institute of Tropical Medicine - Antwerp - Belgium Co-authors Pedro Murlá National Institute for Hygiene, Epidemiology & Microbiology - La Habana - Cuba Armando Rodriguez National Institute for Hygiene, Epidemiology & Microbiology - La Habana - Cuba
Mariano Bonet National Institute for Hygiene, Epidemiology & Microbiology - La Habana - Cuba Pedro Màs National Institute for Hygiene, Epidemiology & Microbiology - La Habana - Cuba Patrick Van der Stuyft Department of Public Health - Institute of Tropical Medicine - Antwerp - Belgium Department of Public Health - Institute of Tropical Medicine Nationalestraat 155 - 2000 Antwerp - Belgium tel : 32 3 247 62 85 – fax : 32 3 247 62 58 - email : [email protected] Instituto Nacional de Higiene, Epidemiología y Microbiología Infanta n° 1158 e/ Llinas y Clavel 10300 Ciudad de la Habana – CUBA tel : 537 78 14 79 – fax : 537 66 24 04 – email : [email protected]
Formatted: Width: 595,35pt, Height: 842 pt
2
Abstract
Cuba developed a programme of quality improvement of its health services, which included
an extra muros emergency care system in which policlinics and general practitioner networks
play an important role. Using routine health information from the decentralised first line
emergency units (FLES) and from the hospital emergency service (HES) for the period 1995-
2000, we evaluated the effects of the emergency care subsystem reform on the utilisation rates
of first line and hospital services in Baracoa and Cerro, a rural and a metropolitan
municipality respectively.
In the self-contained health system of Baracoa, the reform of the emergency subsystem
resulted in a first phase of increased utilisation of the FLES, followed by a second phase of
gradual decrease, during which there was an increased utilisation of general practitioners. In
contrast, the overall results of the reform in Cerro were unclear. Proximity of a hospital seems
to be the most important element in the patient’s decision on which entry point to the Cerro
health system to use. A potential adverse effect of the reform is an increased emergency
services utilisation in situations where GP care remains below patients’ expectations. Given
the current world-wide trends in health care reform, the organisational alternatives developed
in the Cuban health system might remain specific to the local contextual setting.

3
Key words
Cuba
Health-service-organisation
Health-sector-reform
Emergency-care
Decentralisation
First-line-health-services
4
Shifting the Demand for Emergency Care in Cuba’s Health System
Introduction
In many countries the historical function of hospital emergency departments was to care for
patients who did not have the financial means to consult private physicians (Blackwell &
Cantab, 1962). Once social security systems and financially accessible first line health
services were developed, the function of emergency departments shifted towards ensuring
adequate response to accidents and legitimate medical emergencies. However, many patients
continue to visit emergency departments for problems that could have been solved at the level
of a family doctor or health care centre. Extensive literature documents the inappropriate use
or even the abuse of emergency services (Davidson, Hildrey & Floyer, 1983; Davies, 1986;
Foster, Dale & Jessopp, 2001; Fouroughi & Chadwick, 1989; Murphy, 1998; Myers, 1982).
Proposals to improve emergency systems traditionally focused on either effectiveness
(improve the quality of human resources, physical structure and technical capacity) or
efficiency (decrease workload by separating ‘real’ emergencies from ‘inappropriate’ demand)
(Olesen & Jolleys, 1994). It is well recognised that direct involvement of emergency medical
specialists is one of the most critical determinants of effectiveness (Bickell, 1994; Falk,
1993). Likewise, infrastructure, medical supplies and transport facilities are essential.
Unfortunately, even after introducing a broad array of initiatives to canalise non-emergent
patients to a corresponding level of care, inappropriate use of emergency services continues to
be a problem (Hull, Jones, Moser & Fisher, 1998; Rund, Nemer, Robertson, Moeschberger &
Garraway, 1992). Cuba’s national health system is also confronted with this problem.
At the beginning of the 90’s, radical changes in the terms of trade with the former Soviet
Union and the tightening of the USA embargo drastically reduced the national income.
5
(PAHO, 1998) Health care spending dropped and scarce resources were concentrated
(Kirkpatrick, 1996). This resulted in patients, who could have been appropriately attended by
family physicians, overcrowding hospital emergency units, perusing scarce resources and
receiving sub-optimal care (Bolibar, Balanzo, Armada, Fernandez, Foz, Sanz et al., 1996).
Despite the economic crisis, the authorities did not turn to privatisation of health care services
nor cost recovery schemes. The Cuban health care system continued to offer free preventive,
curative and rehabilitation services at the different levels of care (Delgado, 1998; Feinsilver,
1993). It developed plans for rationing health care and increasing efficiency, while ratifying
the principles of state responsibility, equity and universal coverage.
The Ministry of Health set up a programme of quality improvement, strengthened family and
preventive medicine, and introduced decentralisation, inter-sectorial action and community
participation. Emphasis was put on maternal and child health, chronic non-communicable
diseases, communicable diseases, and care of the elderly (PAHO, 1998; Rojas & López, 1997;
Van der Stuyft, De Vos & Hilderbrand, 1997; Veeken, 1995).
Measures implemented to strengthen family medicine included improving drug availability
and follow up of patients. A programme of home hospitalisation was reinforced, and an extra
muros emergency care system was set up, in which first line policlinics and general
practitioner networks played a central role (MINSAP, 1996; PAHO, 2002).
In the framework of an inter-institutional collaboration between Belgian and Cuban research
institutes, the authors have been studying Cuba’s first line health care reform since the mid-
nineties. They researched the effects of this reform of the emergency care system on the
utilisation rates of first line and hospital level services. (MINSAP, 1996).
Material and methods
6
The emergency system reform
Cuban municipalities are divided into health areas, in which a policlinic organises the first
line health care for about 30.000 inhabitants (MINSAP, 1996; PAHO, 1998). It covers the
whole population with a family doctor ( general practitioner – GP) Program (one family
doctor and one nurse per 700-800 inhabitants), and ensures the necessary diagnostic support
and specialist backstopping.
Until 1996, only hospital emergency services (HES), covering about 150.000 inhabitants,
offered an acceptable quality of emergency care. From then onwards, adequately equipped
and supplied first line emergency services (FLES), with well trained personnel, were
gradually set up. Each municipality had an associated principal emergency policlinic (a
central first line emergency service), combined with a variable number of emergency centres
(smaller and more peripheral care centers) (Chang, Alemán, García & Miranda, 2000;
MINSAP, 2002).
Selected study sites
Baracoa and Cerro, a rural and a metropolitan municipality respectively, were selected to
evaluate the effects of the reform. Baracoa is situated on the northern coast of the
Guantánamo province of Cuba. This municipality has a population of 85.000 inhabitants. It is
composed of an urban, peri-urban and rural, mostly mountainous zone, of which some parts
have difficult accessibility. In Baracoa, roughly 190 physicians are working in three health
areas. The municipal hospital is located near the principal emergency policlinic. Baracoa is
geographically isolated from the rest of the province and from the provincial reference
hospital situated in Guantánamo, the provincial capital. An ambulance takes two and a half
hours to cover the distance of 170 km between the two towns.
7
Cerro is one of the central municipalities of Havana, Cuba’s capital. The municipality is
densely populated with a total of about 122.000 inhabitants. It is divided into four health
areas, covered by an estimated 185 general practitioners. Cerro is characterised by a complex
and open metropolitan health services network comprising of two hospitals, and three others
situated just across the municipal boundaries. Hence the majority of its inhabitants live within
walking distance from a hospital. The principal emergency policlinic is in Maceo, the health
area most distant from the aforementioned hospitals.
Data collection
For the period 1995-2000 we established the number of patient contacts with first line
services (general practitioners), decentralised FLES and HES. The research team extracted the
raw data from the routine health information system, acknowledged by UNDP to be of good
quality (UNDP, 2002). Utilisation rates were calculated with yearly-adjusted population
figures provided by the Ministry of Health (MINSAP, 1995-2000).
In 1998 the definition of ‘real emergencies’ was standardised and a training programme was
developed for all doctors working in emergency services. At the FLES, ‘real emergencies’
include all health problems that are either immediately or potentially life-threatening or acute
(MINSAP, 2002). From July 1999 onwards, information on the emergency status of patients
was collected on a specially designed form by the physicians who attended the patients. The
research team ensured adequate supervision of the data collection process, through revising a
sample of the forms with the health staff during the monthly site visits and by systematic
checks for inconsistencies after data entry. The complex geographical distribution of HES and
FLES in Cerro, described above, made us collect patient-origin specific utilisation figures for
the HES from Cerro and neighbouring municipalities. The research team performed a
8
secondary analysis of routine hospital data, differentiating between inhabitants of Cerro and
other users of the hospitals in this municipality to calculate correct utilisation rates. For three
other hospitals in neighbouring municipalities that attract patients from Cerro, we also
collected specific HES utilisation data and calculated patient origin specific utilisation rates.
Since this detailed information was not available through the routine health information
system, the collection of these data was limited to 1999.
3. Results
During the 5 years after the decentralisation of emergency services (January 1996 in both
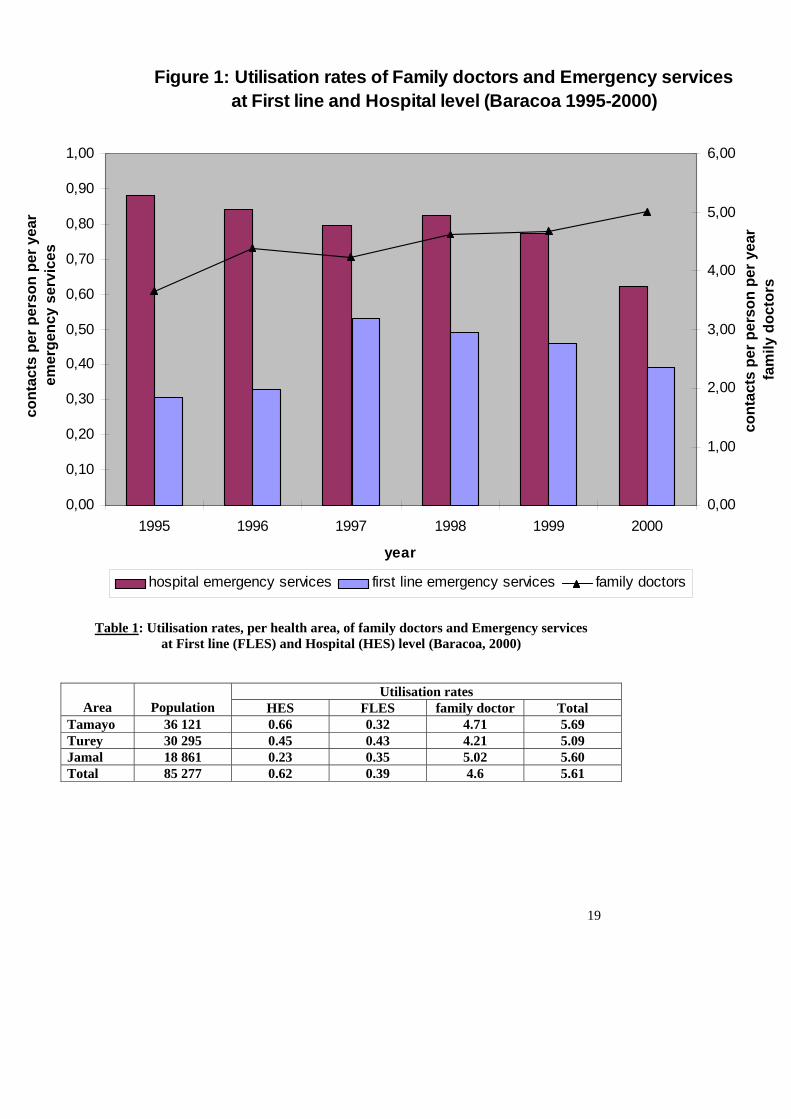
municipalities), the utilisation of the HES in Baracoa gradually decreased 30% from 0,88
contacts per person and per year (cpy) to 0,62 cpy (Figure 1). The utilisation rate of the FLES
increased 70% from 0,31 cpy to 0,53 cpy between 1995 and 1997, and then again decreased to
0,39 cpy during the following years. The total emergency utilisation rate, after a temporary
rise, decreased 18% from 1.23 cpy in 1996 to 1.01 cpy in 2000. Over the same time span, the
utilisation rate of family doctors or gradually rised 39% from 3,6 cpy to 5 cpy.
The ratio of emergency services / family doctors fell from 0,33 in 1995 to 0,20 in 2000. Over
the same period, the total number of patient contacts (family doctors, HES and FLES) raised
from 4.83 cpy in 1995 to 6 cpy in 2000.
The emergency status of the patients was analysed for a 2 year period (July 1999 to June
2001). The decreased utilisation rates of FLES over that period was mainly due to a 27%
reduction of non-emergencies (from 4944 to 3597 contacts per trimester), while the number of
cases defined as “real emergencies” remained stable around 3750 contacts per trimester. The
proportion of contacts evaluated by the medical staff as “real emergencies” hence increased
from 42% in the third trimester of 1999 to more than 50% in the second trimester of 2001.
9
While the total utilisation rate for the different health care entry points was similar in all three
areas of Baracoa (between 5.1 and 5.7 cpy), there was a difference in the specific utilisation
rates (Table 1). In Tamayo, the area where the hospital is situated, we calculated a hospital
emergency care utilisation rate of 0.66 cpy, while that figure was 0.45 cpy in the nearby Turey
area and 0.23 cpy in the mountainous area of Jamal. This is compensated in Turey by a higher
use of FLES, while in the mountainous Jamal area with more difficult access to emergency
services, the family doctor utilisation rate was higher.
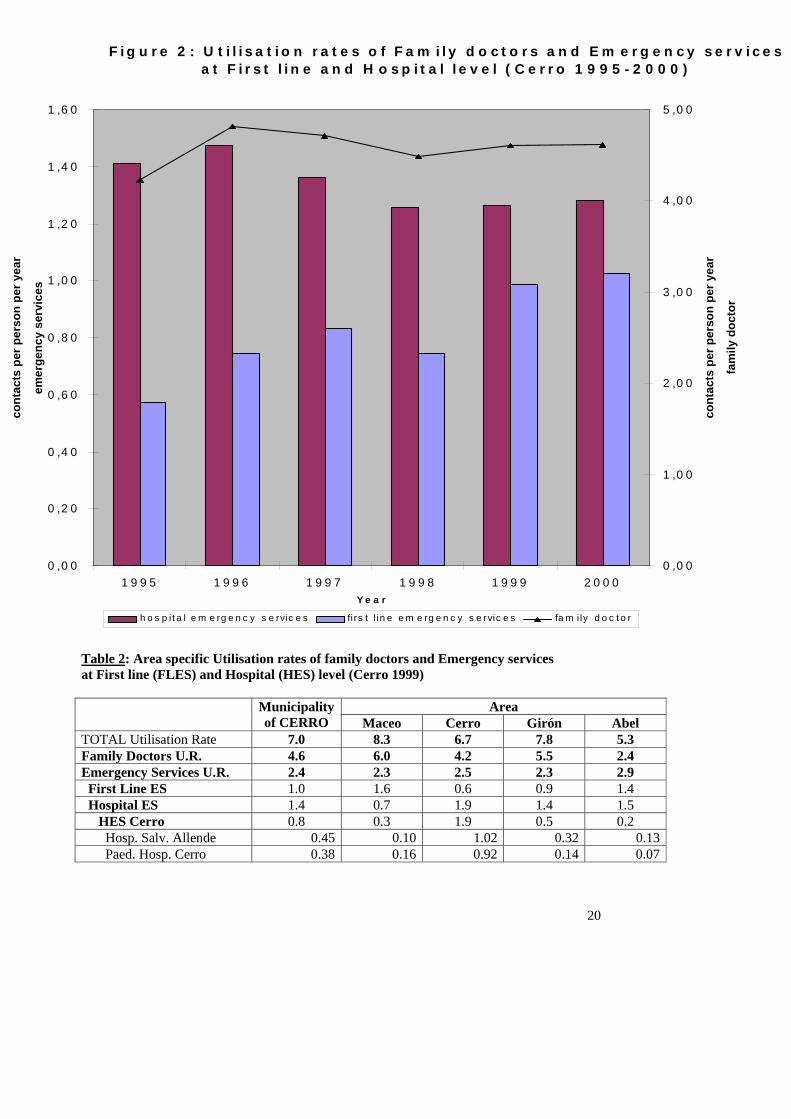
In the metropolitan Cerro municipality, the HES utilisation rates only slightly decreased by
8% (from 1.4 cpy to 1.3 cpy) after the introduction of the decentralised emergency system in
1996. The FLES utilisation rates increased more than 55%, from 0.6 cpy to 1.0 cpy, and the
family doctor utilisation increased with about 10% from 4.2 to 4.6 cpy. The total utilisation
rate varied between 6.2 and 7 cpy (Figure 2).
To fully understand the health services utilisation patterns in Cerro, we differentiated between
inhabitants of Cerro and other users of the hospital emergency services. While the uncorrected
emergency services utilisation rate of both hospitals in Cerro is 1.26 cpy in 1999, the area
specific utilisation rates of the ‘General Hospital Salvador Allende’ and the ‘Paediatric
Hospital of Cerro’ is 0.83 cpy (Table 2). Over the same year, the inhabitants of Cerro had 0.58
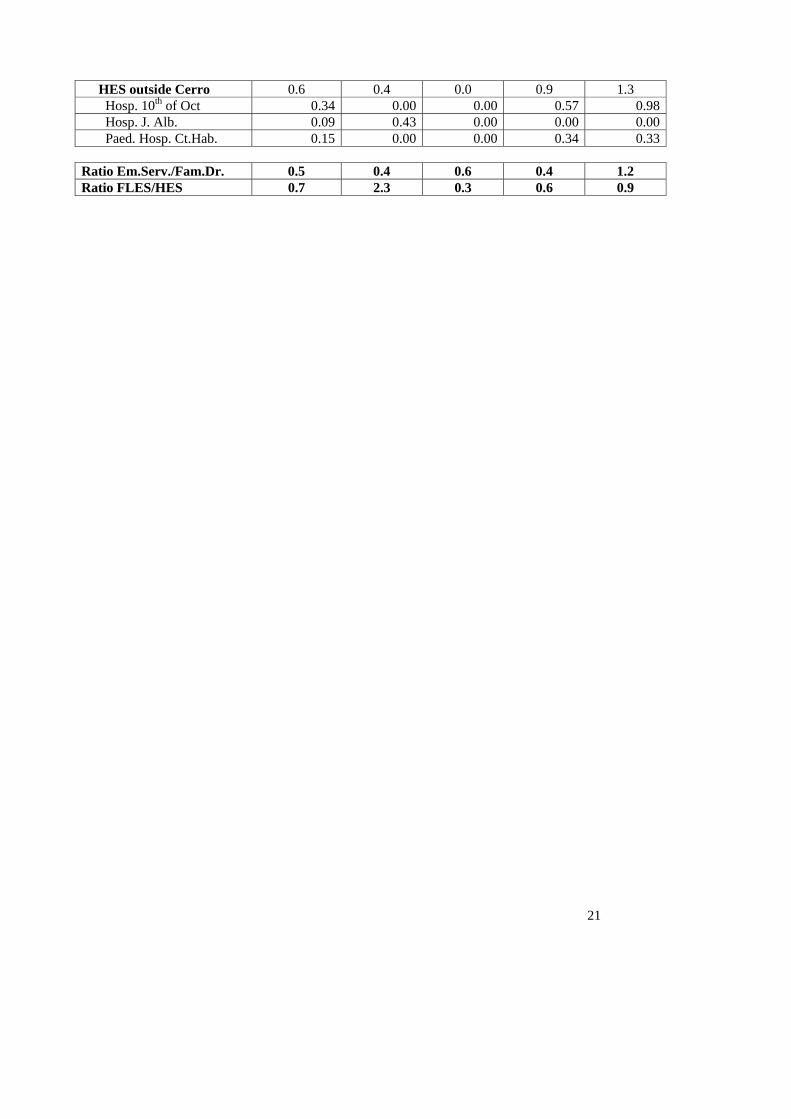
cpy in two general hospitals and one paediatric hospital, located near Cerro. A geographical
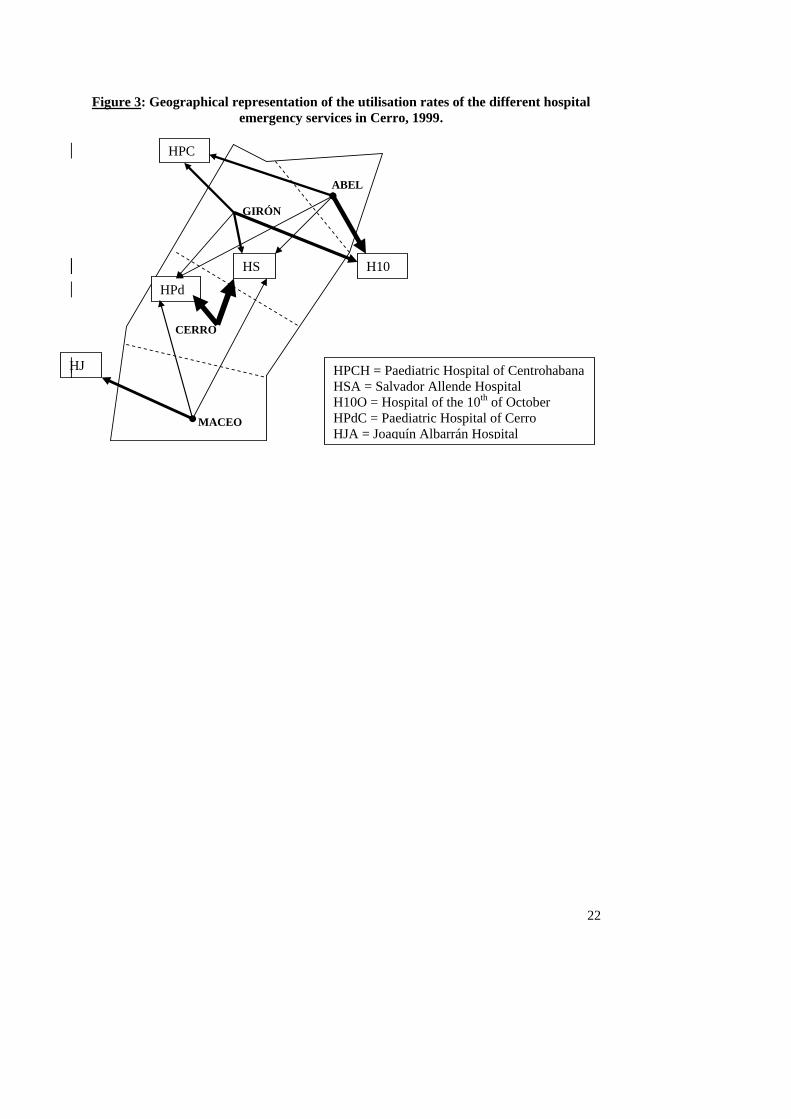
analysis of the patient flow showed a quite diverse utilisation pattern by area (Figure 3). The
total utilisation rates of the different entry points into the health care system varied from 5.3
cpy in Abel to 8.3 cpy in Maceo. While the family doctor contacts per person and per year
varied from 2.4 in Abel to 6.0 in Maceo, the emergency services (ES) utilisation rates varied
only slightly between 2.3 cpy in Maceo or Girón and 2.9 cpy in Abel. On the other hand, the
FLES / HES-ratio showed a clear variation, from 0.3 in Cerro to 2.3 in Maceo. The
10
emergency services / family doctor-ratio was between 0.4 and 0.6, except in Abel where the
low family doctor utilisation rate pushed the ratio to 1.2.
4. Discussion
The political priority given to health in Cuba, in the form of good quality services free of
charge at the point of delivery, explains the high utilisation rates found at all levels of the
system. Due to its specific socio-political context, Cuba is thus not confronted with the
essential problem that most developing countries are facing: ensuring accessible health
services of acceptable quality for all (Segall & Gryseels, 2003). Today, the country’s priority
is to consolidate these accomplishments in a difficult international economic and political
environment. To that objective, structural reorientation of patient demand to the adequate
level of care is central to improving the efficiency of the system.
With regard to adequate use of emergency services, the definitions of ‘minor problems’ and of
the category of ‘inappropriate user’ in emergency care continue to be controversial (Smith,
Lattimer & George, 2001). While a body of literature on the subject claims that the majority
of these patients would be better off by consulting a competent general practitioner instead of
emergency services, explicit objective criteria for ‘inappropriate’ use are frequently lacking
(Walsh, 1995). Besides, the patients’ perception should be included to define what constitutes
an ‘inappropriate’ visit to the emergency department (Hewstone & Antaki 1988; Sbaih, 1993).
The ‘health belief model’ takes into account that patients perform a personal cost-benefit
analysis when deciding to utilise a particular service (Jones, Jones & Katz, 1991; Rosenstock,
1974). When financial considerations are of marginal importance, as is the case in Cuba, the
decision to visit a family doctor might depend on the perception of the problem or disease
experienced (Irwin & Jessop, 1993; Knaus, Draper, Wagner & Zimmerman, 1993), the
11
personality of the patient and his confidence in the physician, and the perceived technical
ability of the physician, his accessibility and the existing material conditions in which he
works (Singh, 1988; Wood & Cliff, 1986). The patient’s decision is also largely influenced by
his personal expectations and preferences. From this point of view, “inappropriate use” is the
result of a rational process that requires adequate evaluation by family doctors and hospital
emergency departments (Andersen & Gaudry, 1984; Dale, Green, Reid & Glucksman, 1995;
Lang, Davido, Diakite, Agay, Viel & Flicoteaux, 1996; Mallon, Cullen, Keenan, Kiberd &
Matthews, 1997; Murphy, 1998; Siddiqui & Ogbeide, 2002). Restructuring to promote
patients’ use of adequate entry points to the health system should therefore be based on the
integration of hospital and first line health care, optimal care quality and accessibility, better
communication, and health promotion (Anonymous, 1979; Hadfield, Yates & Berry, 1994;
Swerissen, 2002).
The evolution of the utilisation rates between 1995 and 2000 can not be explained by
economic change, evolutions in disease patterns, epidemics or natural disaster. In the closed
and self-contained health system of Baracoa, the reform of the emergency subsystem initially
resulted in increased utilisation of the decentralised emergency units. This was followed by a
gradual decrease of this FLES utilisation rate, with a concomitant increased utilisation of the
general practitioners. Measures taken to reinforce the first level of care, and in particular the
decentralisation of emergency services, seem to have resulted in a ‘two-step’ channelling of
demand for non-urgent health care towards family doctors. Our findings suggest that the
decentralisation of the emergency services is, at least in a closed setting, a useful strategy to
diminish the pressure on the HES and to improve the use of the first line services as entry
point.
12
The overall results of the reform in Cerro, a complex metropolitan health system, are, in
contrast, unclear. The total emergency utilisation rate (HES + FLES) remains high, and on top
of this the decentralised emergency service in the Maceo area seems to function as a ‘small
hospital’. Furthermore, the family doctor utilisation rates differ sharply from one area to the
other. The proximity of a hospital appears to be the most important element in the patient’s
decision on which entry point to the health system to use.
Only a contextual analysis, taking into account the specific features of the Cuban social and
health system, can lead to a full understanding of the local impact of the Cuban emergency
care system reform, and create opportunities to further adapt the system to the patients’
problems and needs. In Baracoa a well functioning family doctor programme has been in
place for more than 15 years in both the urban and rural parts of the municipality. The family
doctors mostly live in the community they serve. This may be essential to ensure a gradual
shift of the patient flow from emergency services to family doctors. Also, a systematic and
well-organised GP-involvement in the emergency network may ensure a growing confidence
of the FLES-patients towards ‘their’ family doctor and his technical skills. Together with a
sufficient technical and an adequate drug provision, this may enhance the attractiveness and
utilisation of this level of care. In the metropolitan setting of Cerro, however, the family
doctor programme has been implemented more recently. It has also suffered from the lack of
stability of family doctors. Furthermore, because of lack of adequate facilities, most family
doctors practise in the premises of polyclinics, not necessarily located in the neighbourhoods
they serve. This can compromise the quality of the relationship with the population. More
importantly, the introduction of a decentralised emergency service can result in an adverse
effect of increased ‘emergency’-contacts in situations where the first line care remains below
the patients’ expectations.
13
The Cuban experience with decentralising emergency services in direct collaboration with the
first line health services, could be useful for other countries seeking a strategy to alleviate the
pressure on overcrowded hospital emergency services and to reinforce the first line health
services. However, given current world-wide trends in health sector reform, the organisational
alternatives developed in the Cuban health sector may be specific to the local context. First,
the Cuban authorities had no recourse to financial barriers to deter patients from non-
appropriate health care seeking behaviour at the level of the emergency services. Furthermore,
the existence of a unified public health system, without parallel insurance and/or private
service delivery, facilitates government stewardship in planning and restructuring (Murphy,
Leonard, Plunkett, Bury, Lynam, Smith et al, 1997; Rojas & López, 1997).
Finally, while in many countries health care and social services are affected by the
introduction of cost recovery schemes and privatisation (Estrada, Barilari, Sepulveda & Soto,
1998; Iriart, Merhy & Waitzkin, 2001; Stocker, Waitzkin & Iriart, 1999), Cuban health
services remain public and free at the point of delivery. Cuba also continues to rely on the
state as ‘organiser’ and not just as ‘regulator’ of comprehensive and integrated health care.
In a world where scarce economic resources are increasingly constraining the development of
social policies, the results of Cuba’s alternative health system reform should contribute to the
international debate on health sector policies.
14
Acknowledgements
We thank the health personnel of the research areas and the Ministry of Health in Havana for
their invaluable support. This research was financially supported by INCO-DEV programme
of the European Commission (contract n° IC18-CT98-0348).
15
References
Andersen, N.A., & Gaudry, P.L. (1984). Patients attending an accident and emergency department for primary medical care. Family Practice 1(2), 79-85. Anonymous (1979). What are accident and emergency departments for? Report by a special correspondent. British Medical Journal 2, 837-839. Bickell, W.H. (1994). Emergency Medical Services: Factors Associated With Poor Survival (letter). Journal of the American Medical Association 272, 1573. Blackwell, B., & Cantab, M.B. (1962). Why patients come to a casualty department. Lancet 1962, 369-371. Bolibar, I., Balanzo, X., Armada, A., Fernandez, J.L., Foz, G., Sanz, E., et al. (1996). El impacto de la reforma de la atención primaria en la utilización de servicios de urgencias hospitalarios. Medicina Clínica (Barcelona) 107(8), 289-295. Chang, M., Alemán, M.C., García, R., & Miranda, R.J. (2000). Evaluación de la calidad de la atención médica en el subsistema de urgencias del municipio 10 de Octubre, 1997. Revista Cubana de Salud Pública 24(2), 110-116. Dale, J., Green J., Reid F., & Glucksman E. (1995). Primary care in the accident and emergency department: I. Prospective identification of patients. British Medical Journal 311, 423-426. Davidson, A.C., Hildrey, A.C., & Floyer, M.A. (1983). Use and misuse of an accident and emergency department in the east end of London. Journal of the Royal Society of Medicine 76, 37-40. Davies, T. (1986). Accident Department or general practice? British Medical Journal (Clinical Research Edition) 292, (6515), 241-243. Delgado, G. (1998). Desarrollo histórico de la salud pública en Cuba. Revista Cubana de Salud Pública 24(2), 110-118. De Vos, P. (2002). Cuba’s Geneeskunde voor het volk. In: Globalisering en gezondheidszorg. EPO/MS: Brussels, Belgium. Estrada, A., Barilari, E., Sepulveda, J., & Soto, M. (1998). Atención gerenciada en Chile: Centro de investigación y Capacitación de Salud (Santiago de Chile). Falk, J.L. (1993). Medical direction of emergency medical service systems: A full-time commitment whose time has come. Critical Care Medicine 21(9), 1259-1260. Feinsilver, J.M. (1993) Healing the Masses. Cuban Health Politics at Home and Abroad. Berkerley, Los Angeles, London: University of California Press. Foster, J., Dale, J., & Jessopp, L. (2001). A qualitative study of older people’s view of out-of-hours services. British Journal of General Practice 51(470), 719-723.
16
Fouroughi, D., & Chadwick, L. (1989). Accident and emergency abusers. The Practitioner 233, 657-659. Hadfield, J.M., Yates, D.W., & Berry, A. (1994). The emergency department and the community: a model for improved cooperation. Journal of the Royal Society of Medicine 87, 663-665. Hewstone, M., & Antaki, C. (1988). Attribution theory and social explanations. In Hewstone, M. Introduction to Social Psychology (pp. 111-141). Oxford: Blackwell Scientific. Hull, S., Jones, I.R., Moser, K., & Fisher, J. (1998). The use and overlap of AED and general practice services by patients registered at two inner London general practices. British Journal of General Practice 48(434), 1575-1579. Iriart, C., Merhy, E., & Waitzkin, H. (2001). Managed Care in Latin America: the new common sense in health policy reform. Social Science & Medicine 52, 1243-1253. Irwin, D., & Jessop, E.G. (1993). Severity of Sickness at Admission to Hospital in Colchester 1985 and 1990. Public Health 107, 171-175. Jones, S., Jones, P., & Katz, J. (1991). Compliance in acute and chronic patients receiving a health belief model intervention in the emergency department. Social Science & Medicine 32(10), 1183-1189. Kirkpatrick, A.F. (1996). Role of the USA in shortage of food and medicine in Cuba. Lancet 348, 1489-1491. Knaus, W.A., Draper, E.A., Wagner, D.P., & Zimmerman, J.E. (1985). APACHE II: a severity of disease classification system. Critical Care Medicine 13, 818-829. Lang, T., Davido, A., Diakite, B., Agay, E., Viel, J.F., & Flicoteaux, B. (1996). Non-urgent care in the hospital medical emergency department in France: how much and which health needs does it reflect? Journal of Epidemiology and Community Health 50, 456-462. Mallon, B., Cullen, A., Keenan, P., Kiberd, B., & Matthews, T. (1997). A profile of attenders at the A&E Department of the Children’s Hospital, Temple Street, Dublin. Irish Medical Journal 90(7), 266-267. MINSAP - Ministerio de Salud Pública (1996). Presentación del desarrollo de las estrategias para1996. La Habana, Cuba. MINSAP - Ministerio de Salud Pública (1999). Indicadores Bàsicos 1999. La Habana, Cuba. MINSAP - Ministerio de Salud Pública (2002). Carpeta metodológica. La Habana, Cuba. MINSAP - Ministerio de Salud Pública (1995-2000) Anuario Estadístico. 1995-1996-1997-1998-1999-2000. La Habana, Cuba.
17
Murphy, A.W., Leonard, C., Plunkett, P.K., Bury, G., Lynam, F., Smith, M., & Gibney, D. (1997). Effect of the introduction of a financial incentive for fee-paying A&E attenders to consult their general practitioner before attending the A&E department. Family Practice 14(5), 407-410. Murphy, A.W. (1998). ‘Inappropriate’ attenders at accident and emergency departments I : definition, incidence and reasons for attendance. Family Practice 15(1), 23-32. Myers, P. (1982). Management of minor medical problems and trauma; general practice or hospital? Journal of the Royal Society of Medicine 75, 879-883. Olesen, F., & Jolleys, J.V. (1994). Out of hours service: the Danish solution examined. British Medical Journal 309, 1624-1626. PAHO (1998). Cuba. In: Health in the Americas (pp. 206-219). Washington. PAHO (2002). Cuba. In: Health in the Americas (pp. 198-212). Washington. Rojas, F., & López, C. (1997). Report from Cuba: Economy, politics and health status in Cuba. International Journal of Health Services 27(4), 791-807. Rosenstock, I. (1974). Historical origins of the health belief model. Health Education Monographs 2, 328-335. Rund, D.A., Nemer, J., Robertson, C., Moeschberger, M., & Garraway, M. (1992). Uses of the accident and emergency department in Scotland: Patient characteristics and expectations. Public Health 106, 351-356. Sbaih, L. (1993). Accident and emergency work; a review of some of the literature. Journal of Advanced Nursing 18, 957-962. Segall, M., & Gryseels, B. (2003). Essential health care for the poor: promoting health systems (Editorial). International Journal of Health Planning and Management 18, S1-S4. Siddiqui, S., & Ogbeide, D.O. (2002). Utilisation of emergency services in a community hospital. Saudi Medical Journal 23(1), 69-72. Singh, S. (1988). Self referral to accident and emergency department: patients’ perception. . British Medical Journal 297, 1179-1180. Smith, H., Lattimer, V., & George, S. (2001). General practitioners’ perception of the appropriateness an inappropriateness of out-of-hours calls. British Journal of General Practice 51(465), 270-275. Stocker, K., Waitzkin, H., & Iriart, C. (1999). The Exportation of Managed Care to Latin America. New England Journal of Medicine 340(14), 1131-1136. Swerissen, H. (2002) Toward greater integration of the health system. Australian health review 25(5), 88-93.
18
UNDP (2002). Cuba's health network wins Stockholm Challenge award. (Press Report 19/12/2002). (http://www.health.fgov.be/WHI3/krant/krantarch2002/kranttekstdec2/021219m01undp.htm) Van der Stuyf P., De Vos P., & Hilderbrand K. (1997). USA and shortage of food and medicine in Cuba (Letter). Lancet 349, 363. Veeken, H. (1995). Cuba: plenty of care, few condoms, no corruption. British Medical Journal 311, 935-937. Walsh, M. (1995). The health belief model and use of accident and emergency services by the general public. Journal of Advanced Nursing 22, 694-699. Wood, T.C.A., & Cliff, K.S. (1986). Accident and emergency departments - Why people attend with minor injuries and ailments. Public Health 100, 15-20.
19
Table 1: Utilisation rates, per health area, of family doctors and Emergency services
at First line (FLES) and Hospital (HES) level (Baracoa, 2000)
Utilisation rates
Area
Population HES FLES family doctor Total Tamayo 36 121 0.66 0.32 4.71 5.69 Turey 30 295 0.45 0.43 4.21 5.09 Jamal 18 861 0.23 0.35 5.02 5.60 Total 85 277 0.62 0.39 4.6 5.61
Figure 1: Utilisation rates of Family doctors and Emergency services at First line and Hospital level (Baracoa 1995-2000)
0,00
0,10
0,20
0,30
0,40
0,50
0,60
0,70
0,80
0,90
1,00
1995 1996 1997 1998 1999 2000
year
cont
acts
per
per
son
per y
ear
emer
genc
y se
rvic
es
0,00
1,00
2,00
3,00
4,00
5,00
6,00
cont
acts
per
per
son
per y
ear
fam
ily d
octo
rs
hospital emergency services first line emergency services family doctors
20
Table 2: Area specific Utilisation rates of family doctors and Emergency services at First line (FLES) and Hospital (HES) level (Cerro 1999)
Area Municipalityof CERRO Maceo Cerro Girón Abel
TOTAL Utilisation Rate 7.0 8.3 6.7 7.8 5.3 Family Doctors U.R. 4.6 6.0 4.2 5.5 2.4 Emergency Services U.R. 2.4 2.3 2.5 2.3 2.9 First Line ES 1.0 1.6 0.6 0.9 1.4 Hospital ES 1.4 0.7 1.9 1.4 1.5 HES Cerro 0.8 0.3 1.9 0.5 0.2 Hosp. Salv. Allende 0.45 0.10 1.02 0.32 0.13 Paed. Hosp. Cerro 0.38 0.16 0.92 0.14 0.07
F ig u r e 2 : U t i l i s a t io n r a t e s o f F a m i ly d o c t o r s a n d E m e r g e n c y s e r v i c e s a t F i r s t l i n e a n d H o s p i t a l l e v e l ( C e r r o 1 9 9 5 - 2 0 0 0 )
0 ,0 0
0 ,2 0
0 ,4 0
0 ,6 0
0 ,8 0
1 ,0 0
1 ,2 0
1 ,4 0
1 ,6 0
1 9 9 5 1 9 9 6 1 9 9 7 1 9 9 8 1 9 9 9 2 0 0 0Y e a r
cont
acts
per
per
son
per y
ear
emer
genc
y se
rvic
es
0 ,0 0
1 ,0 0
2 ,0 0
3 ,0 0
4 ,0 0
5 ,0 0
cont
acts
per
per
son
per y
ear
fam
ily d
octo
r
h o s p i t a l e m e rg e n c y s e rvic e s fi rs t l in e e m e rg e n c y s e rvic e s fa m i ly d o c t o r
21
HES outside Cerro 0.6 0.4 0.0 0.9 1.3 Hosp. 10th of Oct 0.34 0.00 0.00 0.57 0.98 Hosp. J. Alb. 0.09 0.43 0.00 0.00 0.00 Paed. Hosp. Ct.Hab. 0.15 0.00 0.00 0.34 0.33 Ratio Em.Serv./Fam.Dr. 0.5 0.4 0.6 0.4 1.2 Ratio FLES/HES 0.7 2.3 0.3 0.6 0.9
22
Figure 3: Geographical representation of the utilisation rates of the different hospital
emergency services in Cerro, 1999. ABEL GIRÓN CERRO MACEO
HPC
HS H10
HPd
HJ HPCH = Paediatric Hospital of Centrohabana HSA = Salvador Allende Hospital H10O = Hospital of the 10th of October HPdC = Paediatric Hospital of Cerro HJA = Joaquín Albarrán Hospital
Recommended

















