Embed Size (px)
DESCRIPTION
Citation preview

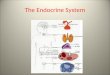
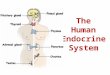
The Endocrine System

Endocrine SystemEndocrine vs. ExocrineOrgans are not physically connectedAlters activities of target organs/cellsPurpose: Growth/Development
ReproductionRegulationStress Reactions

Hormones are Activated By
Hormonal
Humoral
Neural

Gland/Hormone FunctionsSome glands produce >1 hormone
Some hormones produced by >1 gland
Some organs have >1 function
Some hormones have >1 function

Functions of Endocrine Glands
Endocrine Functions onlyProductionSecretion
Contained within other organs which have other functions

Categories of GlandsCentral: Pituitary
Hypothalamus
Peripheral: Thyroid PinealAdrenals GonadsParathyroids PancreasThymus Others

HypothalamusFound on floor of diencephalonNeural and endocrine functionsBiofeedback mechanism for:Osmotic pressuresTemperature regulationsMetabolic functions

PituitaryExtends from Hypothalamus-behind sphenoid bone“Master Gland” of bodyAnterior- Portal networkPosterior- Neural-contains axons of
Hypothalamus neurons

Anterior PituitaryGH- Growth HormoneProlactinTSH- Thyroid Stimulating HormoneACTH- AdrenocorticotropicFSH- Follicle Stimulating HormoneLH- Luteinizing Hormone

Posterior Pituitary
ADH- Anti-Diuretic Hormone
Oxytocin

Pituitary Disorders Acromegaly- Hypersecretion of GH
Dwarfism- Hyposecretion of GH

ThyroidInferior to larynx2 LobesT3- Triiodothyronine
T4- Thyroxine
Calcitonin

Thyroid DisordersHypothyroidism- Hyposecretion
Hyperthyroidism- HypersecretionGraves Disease
Goiters- iron deficiencies

Parathyroids4 small glands posterior surface of thyroidParathyroid hormoneResponsible for osteoclast of boneDecreases blood phosphate levels(By way of kidneys)Enhances activation of Vitamin D

Parathyroid Disorders Hyperparathyroidism
“Moan and groan, stones and bones”

Pineal GlandForms part of diencephalonMelatoninInhibits hypothalamus release of gonadotropinsMelatonin-decreases in light/increase in dark (circadian rhythm)

Thymus GlandPosterior to sternum, around great vesselsThymosinBoth lymphatic and endocrineLymphatic- produces T-lymphocytesEndocrine- ‘programs’ T-cells

The AdrenalsLocated on superior end of each kidney
Medulla- inner gland
Cortex- outer gland

Adrenal MedullaSympathetic preganglionic fibers synapse on cells in medulla
Release of epinephrine/norepinephrine into general circulation

Adrenal CortexProduce over 30 steroid hormones
Three main cortical hormonesMineralocorticoidsGlucocorticoidsSex hormones

MineralocorticoidsRegulate levels of electrolytes and water in extracellular fluid
95% are aldosteroneSodium reabsorption Potassium excretion

GlucocorticoidsInfluence carbohydrate metabolismImportant in body’s response to stress95% cortisol (hydrocortisone)
stimulates gluconeogenesissecretion is regulated by ACTH

Sex HormonesAndrogens (testosterone)
Estrogens
Both are secreted in greater numbers by gonads

Adrenal Disorders Cushing’s disease-
cortisol over-production secondary to
increased ACTH
Addison’s Disease-cortisol/aldosterone deficiencies

GonadsTestes- males
TestosteroneOvaries- females
EstrogensProgesterone
Both produce hormones/gametes

PancreasRetroperitoneal-posterior to stomachExocrine & EndocrineEndocrine- islets of Langerhans
AlphaBetaDelta

Alpha cells20% of islets
Hormone glucagon
Stimulates breakdown of glycogen in liver- raises glucose levels in blood(glycogenolysis & glyconeogenesis)

Beta Cells75% of islets
Hormone- insulin
Decreases glucose levels

Glucose MetabolismOrganic components of food:Carbohydrates (instant-energy)GlucoseFatsFatty acids/glycerolsProteinsAmino acids

Carbohydrate Metabolism Insulin is released by humoral, hormonal, neural means
Increased glucoseParasympathetic stimulationGastrointestinal hormones

Carbohydrate Metabolism 60% of carbohydrates are stored as
glycogen in liver
If muscles are not exercised after eating-stored as muscle glycogen

Glycolysis Glucose is broken down into pyruvate
and lactate- releasing 2ATPs
(Anaerobic metabolism)
Krebs Cycle

Fat Metabolism A third of any glucose passing through liver is converted to fatty acids
Fatty acids are converted to triglycerides and stored in adipose tissue

Fat Metabolism Without insulin, fat is broken back down into triglycerides/cholesterol CAD
Fatty acids are also broken down into ketone bodies

Protein Metabolism In absence of insulin- protein storage stops and breakdown begins (muscle)
Amino acid breakdown for energy leads to increased urea in urine organ dysfunction

Pancreas Disorders Diabetes-
Type 1- Juvenile onsetType 2- Mature onset Gestational diabetes

Type 1 Diabetes Insulin dependant
S/S:polyuriapolydipsiapolyphagiablurred visionweight loss

Type 2 DiabetesGenerally non-insulin dependant
Has ability to make small amounts of insulin
Can develop into insulin dependant

Gestational DiabetesDevelops during pregnancy
Deficiencies in insulin leads to inability to metabolize carbohydrates
Generally disappears after delivery

Insulin AgentsEarly- porcine, bovineRecent- genetic engineered human insulinProteinRapid, intermediate and long-termCombination of long-term, rapid each day

Insulin TypesRegular- Fast acting0.5-1 hour onset6-8 hour duration
NPH- Intermediate1-1.5 hour onset24 hour duration

Insulin TypesUltralente- Long acting
4-6 hour onset36 hour duration
Oral agents:Diabinese (chlorpropamide)Orinase (tolbutamide)Micronase (glyburide)Glucotrol

Diabetic EmergenciesHypoglycemiaHyperglycemiaDiabetic Ketoacidosis (DKA)Hyperosmolar Hyperglycemic Nonketotic Coma (HHNK)

HypoglycemiaRapid on-set< 60 mg/dlCauses: too much insulin
decreased intake salicylatesexcessive activity beta blockersemotional stress hypothermiachronic alcoholism sepsis

S/S of HypoglycemiaAltered LOCs- irritability, nervousness,
confusion, combativeCool, clammyWeak, rapid pulseSnoring, salivationNormal BP

Diabetic KetoacidosisFat metabolism leads to ketoacidsAcidosis leads to K+ in circulation &
hyperkaluria K+ deficiencyOsmotic diuresis dehydration,
electrolyte imbalances

S/S of DKAWarm, dry skinDry mucous membranesTachycardia, thready pulsePostural hypotensionWeight loss‘Polys’

S/S of DKAAbdominal painAnorexia, nausea/vomitingAcetone breathKussmaulsDecreased LOC

Hyperosmolar Hyperglycemic Nonketotic
ComaGenerally Type II diabeticOsmotic diuresis secondary to sugarsNot acidotic as in DKAFactors: Geriatric
Preexisting diseasesIncreased insulin requirementsMedication use- thiazide, diureticsParenteral/enteral feedings

S/S of HHNKWeaknessThirstPolyuriaWeight LossExtreme dehydration

Treatment of Diabetic Emergencies
Hypoglycemia- ABCsIV- NSMonitor ECGOral, IV DextrosePoss. Glucagon IMPoss. Thiamine
Monitor glucose!

Treatment of Diabetic Emergencies
Hyperglycemia (DKA, HHNK)-
ABCsO2
IV- NSMonitor ECG for abnormalities