Embed Size (px)
DESCRIPTION
A COMPLEX HEALTH CHALLENGE
Citation preview

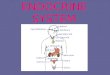
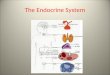
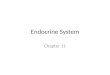
The Endocrine SystemEndocrine System• The endocrine system includes all the
endocrine cells and the tissues of the body that produce hormones or paracrine factors with effects beyond their tissue origin.
• Endocrine cells are glandular secretory cells that release their secretions into the extracellular fluid.
• The organs that produce endocrine secretions main function is to secrete hormones while some organs have other functions.
Organs of the Endocrine System are: • Hypothalamus, pituitary gland, thyroid
gland, thymus, adrenal glands, pineal gland, parathyroid glands, heart, kidney, adipose tissue, pancreatic islets, digestive tract, and gonads

John Smith, a 18-year-old man presented to the emergency department with nausea and headache for one day at 1020. He has recently moved to Burk’s Fall and does not have a physician. He was in town visiting friends for a few days. John was assigned a triage level of 4 based on his baseline vitals of (37.1°C, 80bpm, 20rr, 90/50mmHg, 95% O2 sats) and sent back out into the waiting room.
On a busy day in the North Bay General Hospital’s Emergency room department:

A COMPLEX HEALTH CHALLENGE

The Endocrine System: Pancreas
• Functions as an endocrine organ, where the islets of Langerhans secrete various types of hormones, primarily:
• Glucagon: secreted by A cells
• Insulin: secreted by B cells
• The pancreas controls serum glucose by regulating the rate at which glucose is synthesized, stored and moved to and from the bloodstream through the actions of glucagon and insulin

Hormones:
Insulin:- Controlled by chemical, hormonal and neural mechanisms
- Acts as a storage hormone to lower blood glucose by permitting glucose to enter the cells of the liver, muscles and tissues
- Glucose within the cells is then stored as glycogen or used for energy
- Insulin signals the liver to stop the release of glucose into the blood
- In the absence of insulin, glucose cannot enter the body resulting in higher serum osmolarity, hyperglycemia and glucosuria


Hormones:
Glucagon:- Hormone produced by the pancreas
- Is the antagonist to insulin: Increases blood glucose levels by:- Breaking down glycogen (glucogenolysis)- Breaking down amino acids and lipids to form glucose (gluconeogenesis)
- Glucagon is released by the pancreas in response to decreased levels of blood glucose
- Epinephrine, adrenocorticosteroids, growth hormone and thyroid hormones have the same hypoglycemic effects

Euglycemia:
- Homeostasis between insulin and glucagon secretions
-Capillary blood glucose reading falls between 4-8mmol/L
- As glucose in the blood rises, insulin is released, which allows glucose to be transported across the cell membranes, and to be used or stored as energy
- Insulin signals the liver to cease breaking down glycogen or amino acid reserves, and instead utilizes glucose, provided by insulin secretion.
- Blood glucose levels decrease, reaching euglycemia levels

Diabetes Insipidus:- The body is unable to produce a therapeutic amount of antidiruetic hormone (ADH)- Decreased ADH concentrations lead to vast water loss through the kidneys
- Polyruia (>12L/d)- secondary hypotension- enlarged bladder- glucosuria
Clinical Manifestations:
- Insatiable polydipsia- Dehydration- Unexplainable weight loss- Electrolyte imbalances: lethargy, headache, irritability and muscle pains Treatment:
- Pharmacological intervention (vasopressin)- Fluid replacement therapy with electrolyte supplements

Type I Diabetes Mellitus: - Rare: accounts for 10% of diabetes mellitus
- Two types:- Immune
- autoantibodies attack B cells causing destruction
- Non-Immune- pancreatic destruction due to infection, medications and viruses
- Causes insulin deficiency

Type I Diabetes Mellitus:
1. The stomach changes food into glucose
2. Glucose enters the bloodstream
3. The pancreas makes little or no insulin
4. Little or no insulin enters the bloodstream
5. Glucose builds up in the bloodstream resulting in hyperglycemia and the buildup of ketones in the blood
Type I Diabetes
- When serum glucose levels increase past 9.9mmol/L the renal threshold is surpassed causing glucosuria
- Ketone bodies are produced due to the uninhibited breakdown of fats and amino acids
Clinical Manifestations:
- Glucosuria
- Hyperglycemia
- Ketoacidosis if untreated- ketones (acids) buildup in the blood due to the breakdown of lipids that are needed to provide energy for the body. Metabolic acidosis results, leading to DKA.
Treatment:
- Resolve underlying factors
- Pharmacological intervention
- Pancreatic transplant

At 1120 in the waiting room others noticed he had become increasingly lethargic,confused, and hyperventilating with breath smelling like Juicy Fruit and dry-heavevomiting.
On secondary assessment he was drowsy and dehydrated with tachypnea (24rr),tachycardia (100), and a temperature of 37.1°C. On admission the athletically built young man weighed 100 kg. There were no localizing clinical signs of infection.A urine dipstick test detected ketones, and bedside capillary testing with a glucometershowed "high" glucose concentrations at 28.
Blood samples were sent to the laboratory.
Back to John, who is waiting anxiously in the busy ER waiting room:

More thorough history includes that he is a diabetic and over the last 24 hours hehad felt increasingly tired, lethargic, polyuric, and thirsty. As he was unable to keep any food down, but continued to drink alcohol with his friends the previous night. He also had omitted two insulin injections, including one on the morning of admission because he had left his insulin back in Burk’s Fall. He has no history of chest pain.He has been recently diagnosed with type-1 diabetes and was injecting Humulin U once a day, and Humulin R sliding scale insulin three times a day with meals. He has not been in contact with any hospital clinic and has no known complications of diabetes.
The arterial blood gas analysis indicated metabolic acidosis (pH 7.16, carbon dioxide partial pressure 1.8 kPa, oxygen partial pressure 15.9 kPa, bicarbonate concentration 12 mmol/l). His other indicative lab values include plasma glucose level 28 mmol/L, positive for serum ketones, effective serum osmolarity of 315, anion gap of 15 mmol/L, BUN of 30 mg/dl, and electrolytes have increasepotassium 6 mEq/L, and decreased sodium of 125 mEq/L.

HbA1c
• Glucose sticks to the haemoglobin to make a ‘glycosylated haemoglobin’ molecule, called haemoglobin A1c or HbA1c.
• The more glucose in the blood, the more haemoglobin A1c or HbA1c will be present in the blood.
• Red cells live 120 days before they are replaced. By measuring the HbA1C it can tell you how high your blood glucose has been on average over the last 8-12 weeks. A normal non-diabetic HbA1C is 3.5-5.5%. In diabetes about 6.5% is good.
• The HbA1C test is currently one of the best ways to check diabetes is under control; the HbA1C is not the same as the glucose level.

Type I Diabetes Mellitus:
Diabetic KetoacidosisCauses:
-Inadequate insulin production as seen in type I diabetes-Infection-Trauma-Myocardial infarction-Insulin interruption for type I diabetics
Pathophysiology:-Due to the decrease of insulin supply, and as a result of circulating antagonistichormones such as epinephrine, glucagoncatecholamines, growth hormone and cortisol, hyperglycemia develops
-Lipids and amino acids are catabolized to provide energy for the body, and produce ketone acids within the body
-Body is sent into metabolic acidosis, with bicarbonate reserves being quickly depleted- fruity-smelling breath

Type I Diabetes Mellitus:
Diabetic Ketoacidosis-If not treated, hyperglycemia leads to diabetic ketoacidosis (DKA) due to the accumulation of ketones produced by lipids
Clinical Manifestations:
- Hyperglycemia Signs & Symptoms
-Polydipsia-Polyphagia-Polyuria-Dehydration-Nausea & vomiting-Weakness-Fatigue-Altered mental status-Tachycardia-Hypotension
- Unique DKA Signs & Symptoms
-Tachypnea-Kussmaul’s breathing-Electrolyte imbalances
-Hypokalemia-Hyopnatremia
-Seizures-Ketonuria-Acetone breath-Coma

Laboratory Tests:

John is now diagnosed diabetic ketoacidosis(DKA is a triad of hyperglycemia, ketonemia and acidemia) which criteria for conclusion are included in table 2.
TABLE 2Diagnostic Criteria for Diabetic Ketoacidosis
Mild DKA Moderate DKA Severe DKA
Plasma glucose (mg per dL [mmol per L])
> 250 (13.9) > 250 > 250
Arterial pH 7.25 to 7.30 7.00 to 7.24 < 7.00
Serum bicarbonate (mEq per L)
15 to 18 10 to < 15 < 10
Urine ketones Positive Positive Positive
Serum ketones Positive Positive Positive
Beta-hydroxybutyrate
High High High
Effective serum osmolality (mOsm per kg)*
Variable Variable Variable
Anion gap† > 10 > 12 > 12
Alteration in sensoria or mental obtundation
Alert Alert/drowsy Stupor/coma
DKA = diabetic ketoacidosis*-Effective serum osmolality = 2 3 measured Na (mEq per L) + (glucose [mg per dL] ÷ 18).†-Anion gap = Na+ - (Cl- + HCO3- [mEq per L]).Adapted with permission from Kitabchi AE, Umpierrez GE, Murphy MB, Barrett EJ, Kreisberg RA, Malone JI, et al. Hyperglycemic crises in diabetes. Diabetes Care 2004;27(suppl 1):S95, with additional information from
SO:

John was placed, as per physician’s orders, on the NBGH Pre-printed orders for Treatment protocol: Adult Diabetic Ketoacidosis
He was started on fluid replacement with 0.9% saline at 150 ml/hr and a secondary line of intravenous soluble insulin at 10 units/hour. The patient was transferred to the Critical Care Unit.
At 1220 Secondary CBG is 20 mmol/L.
The nurse’s main concern was his electrolyte balance and dehydration.Nurses there also watched for other complications that could occur, which include:myocardial infarction(MI), acute gastric dilation, erosive gastritis, late hypoglycemia, respiratory distress, infection, hypophosphatemia, mucormycosis (inhaled fungal infection).

Type I Diabetes Mellitus:
Diabetic Ketoacidosis
Nursing Interventions:
- Prevention of hyperglycemia
- Insulin administration: bolus dose calculated 0.1-0.15U/kg
- Administration 1L isotonic solution within the first hour
- Monitor lab values, and replace lost electrolytes: Na, K, Ph, bicarbonate etc.
- Maintenance dose of insulin, typically 5-7u SC (sliding scale) to maintain euglycemia
- Close monitoring is crucial to assess for rebound hypoglycemia, fluid overload, pulmonary edema, cerebrovascular changes, and renal complications
- Vital signs q1h, I&O, mental status and neurological impairment
- Check urine for glucose and ketones periodically with a urine dip test

Predisposing Factors
Type II Diabetes Mellitus: - Characterized by insulin resistance of peripheral cells
- Insulin cannot adequately bind to cell receptor sites, thereby rendering insulin less effective at stimulating glucose uptake
Heredity
Advancing Age
Overweight
Poor Diet
Sedentary Lifestyle

Predisposing Factors
Type II Diabetes Mellitus: - Characterized by insulin resistance of peripheral cells
- Insulin cannot adequately bind to cell receptor sites, thereby rendering insulin less effective at stimulating glucose uptake
Heredity
Advancing Age
Overweight
Poor Diet
Sedentary Lifestyle
Clinical Manifestations:
- Signs and symptoms of hyperglycemia

Type II Diabetes Mellitus:
Hyperglycemic Symptoms
- Lab values may indicate dyslipidemia and hyperinsulinemia
- History of recurrent infections
Clinical Manifestations:
- Controlled type-II diabetics usually will not progress to ketoacidosis because there is enough insulin within circulation to control the breakdown of fat and amino acids- Uncontrolled type II diabetics will lead to another acute complication: Hyperglycemic Hyperosmolar Nonketotic Syndrome

Type II Diabetes Mellitus:
Treatment:
- Attempt to restore euglycemia
- Pharmacological interventions
- Dietary measures
- Exercise

Type II Diabetes Mellitus:
Hyperglycemic Hyperosmolar Nonketotic Syndrome
Pathophysiology:- Severe condition of hyperglycemia and hyperosmolarity due to insulin resistance but with no ketone production
- Endogenous insulin is able to regulate catabolism of amino acids, however this leads to heightened hyperglycemia
- Hyperglycemia surpasses the renal threshold, allowing for glucose and electrolytes to be lost in polyuria. Severe dehydration, cerebro-vascular edema and seizures can occur, and finally hypovolemic shock
Causes:-Occurs during periods of stress and more commonly in the elderly
-Individuals with HHNS do not exhibit abdominal S/S that are associated with DKA: therefore there is a greater degree of dehydration and a higher mortality rate of 15%

Type II Diabetes Mellitus: Hyperglycemic Hyperosmolar Nonketotic SyndromeClinical Manifestations:
- CBG level can reach >33.3mmol/L
- Extreme glucosuria and proteinuria
- Hypotension related to profound dehydration
- Altered neurological state combined with edema and seizure activity
Diagnostic Tests:
- Lab tests - Blood glucose: 600-1200mg/d
- Electrolytes- osmotic diureses causes severe dehydration- BUN- CBC- Serum osmolarity: exceeds 350mOsm/kg- Arterial blood gas analysis
Treatment- Fluid replacement with electrolyte replacement
- Insulin administration and close monitoring related to rebound effects

Acute Complications of Diabetes:
Hypoglycemia:
- Referred to as insulin reactions, or insulin shock- Defined as CBG of 2.7-3.3mmol/L
- Caused by:- over-administration of insulin- too little food intake or excessive exercise

Acute Complications of Diabetes:
Hypoglycemia:
Hypoglycemic Symptoms
Clinical Manifestations:

Acute Complications of Diabetes:
Hypoglycemia:Treatment:
- Must give some form of glucose, otherwise death will ensue
- Follow with a snack containing protein and starch
- Patient teaching

Chronic Complications of Diabetes: - Long-term complications of diabetes affects nearly every organ system
- Three categories:
Macrovascular Complications
Microvascular Complications
Neuropathy

Chronic Complications of Diabetes: Macrovascular Complications:
- Hyperglycemia causes atherosclerosis which causes other cardiovascular complications
- Coronary Artery Disease: 60% of diabetics die related to CAD
- Peripheral Vascular Disease: Diabetics are 2-3 times more likely to develop thrombi- In the lower extremities, arterial occlusion is responsible for gangrene
Cerebral Vascular Disease: •MI is more 2 times more likely to occur in
diabetic men, three times in woman•Silent ‘ischemic attacks’- due to neuropathies
- CVAs are common due to atherosclerotic changes

Chronic Complications of Diabetes: Microvascular Complications: - hyperglycemia and hypertension causes capillary membrane thickening throughout the body
- Increased wall thickness causes decrease perfusion across the membrane
- Edema and scarification occurs due to cellular necrosis
- New blood vessels attempt to perfuse the retina, which lead to clouding of the vitreus, and block light from reaching the retina
- New blood vessels dislodge the retina, leading to blindness
Diabetic Retinopathy

Chronic Complications of Diabetes: Microvascular Complications:
Diabetic Retinopathy
Clinical Manifestations:
- Painless process
- Blurry Vision Cobweb’s Complete loss of vision
Assessment:
- Direct assessment with an opthalmascope
Treatment:
- Maintenance of euglycemia
- Photocoagulation and surgery

Chronic Complications of Diabetes: Microvascular Complications:
Diabetic Nephropathy: - Renal disease due to microvascular changes in the kidneys
- Changed capillary basement membrane thickness affects the kidney’s ability to filter blood
- Results in albuminurea with simultaneous necrosis of renal tissue
- When the kidney’s have lost 85% of their function = end stage renal failure

Chronic Complications of Diabetes: Microvascular Complications:
Diabetic Nephropathy: Clinical Manifestations of End-Stage Renal Failure:
- Uremia
- Aggravated hypertension, heart failure, and pulmonary edema due to fluid overload
- Gastrointestinal symptoms
-Neurological changes- altered mental status- change in consciousness- muscle twitching- seizures
- Electrolyte and fluid imbalances due to acidosis
End-Stage Renal Failure ultimately results in multiple-system organ failure

Chronic Complications of Diabetes: Microvascular Complications:
Diabetic Nephropathy:
Assessment:
- Lab values to highlight albumin leakage in urine
- BUN/creatinine assessment
Treatment:
- Control of hyperglycemia from ACE-inhibitors
- Low sodium/low protein diet
- Dialysis

Chronic Complications of Diabetes: Diabetic Neuropathies:
- Group of diseases that affect peripheral, autonomic and spinal nerve innervations
- Results in clinically diverse disorders
- Prevalence increases with age and length of disease
- Caused by hyperglycemia due to its vascular and metabolic effects on the cell, and due to its demylenization of nerve fibers
Two Types:
1. Peripheral Neuropathy
2. Autonomic Neuropathy

Chronic Complications of Diabetes: Diabetic Neuropathies:
Peripheral Neuropathy
- Parenthesis and burning sensation of the lower extremities
Decreased proprioception
Decreased sensation of pain and temperature
Clinical Manifestations & Complications:
- Charcot joints
- Increased risk for tissue damage
- Unsteady and altered gait

Chronic Complications of Diabetes: Diabetic Neuropathies:
Autonomic Neuropathy
Results in a broad range of dysfunctions that affect almost everyorgan system
Gastrointestinal complications: -delayed gastric emptying, nausea, vomiting, constipation, and early satiety
Cardiovascular complications: -tachycardia, orthostatic hypotension, silent symptoms for MI
Renal complications: -urinary retention due to decreased sensation leads to bladder distention and increased risk for UTIs
Hypoglycemia Unawareness: -Autonomic neuropathy masks adrenergic symptoms of diaphoresisshaking, tachycardia and palpitations -Can lead to DKA

Chronic Complications of Diabetes: Foot and Leg Complications
- 50-70% of lower extremity amputations are performed on diabetics
- Complications that increase the risk for foot and leg complications include:
Peripheral Neuropathy Complications:- Loss of pain and pressure sensation and Charcot joints increases the risk for the development of wounds
Autonomic Neuropathy Complications:- Dryness and fissuring of the skin due to decreased sweating increases the risk for infection and skin breakdown
Macrovascular Complications:- Altered blood flow impairs the ability for disease-fighting cells to reach wound sites
Immunocompromised :- Hyperglycemia decreases the potency of WBCs, thus there is a lowered resistance to infection

Chronic Complications of Diabetes: Foot and Leg ComplicationsPrevention
1. Never go barefoot, even indoors.
2. Wear shoes that fit properly and are supportive.
3. Wash, dry and moisturize your feet daily. Wipe off excess lotion.
4. Wear fresh clean socks every day. Do not wear tight socks, garters or elastics.
5. Inspect your feet daily: Check for blisters, scrapes, cuts, sores or cracks.
6. Clean cuts and scrapes with mild soap and water.
7. Do not attempt to treat foot complications yourself. Do not have manicures by non-professionals.
8. Trim toenails straight across.
9. Ask your physician to check your feet every visit, and to check for neuropathy at least once a year.
10. Seek medical attention if you notice redness, swelling or warmth in your legs and feet, or if you notice signs of infection concurrent with abrasions.

4. Thiazolidinediones (e.g. Avandia-improved insulin responsiveness in skeletal muscle, facilitate glucose uptake and utilization
MEDICATIONS FOR DIABETES: ORAL MEDICATIONS
Five types of oral medications for diabetes to control insulin:
1. Sulfonylureas (e.g. Diabeta)- Stimulates insulin secretion by attaching to the sulfonylurea receptor on the beta cells of the pancreas
Sulfonylureas
Meglitinides
[Alpha]-GlucosidaseInhibitors
Thiazolidinediones
Biguanides
2. Meglitinides (e.g. Prandin)- stimulate insulin secretion by attaching to a different receptor on the beta cells of the pancreas.
3. [Alpha]-Glucosidase Inhibitors (e.g. Precose)-inhibits enzymes in the intestines to retard the entry of glucoseinto systemic circulation.
5. Biguanides (e.g. Metformin) -multiple effects that are not completely understood. Reduces liver glucose output, boost glucose uptake by insulin sensitive cells, and decrease glucose absorption by the small intestine

MEDICATIONS FOR DIABETES: INSULIN
Type Trade names Onset of Action
Peak Action Duration of Action
Rapid acting(Clear)
Humalog (insulin lispro)
NovoRapid (insulin aspart)10-15min 60-90 min 4-5 hours
Fast acting(clear)
Humulin-RNovolin ge
Toronto
30-60 min 2-4 hours 5-8 hours
Intermediate acting
(cloudy)
Novolin ge NPHHumulin- LHumulin- N
1-3 hours 5-8 hours up to 18 hours
Long acting(cloudy)
Humulin -U 3-4 hours 8-15 hours 22-26 hours
Extended long acting analogue
Lantus (insulin glargine) approved, but not yet available in Canada
90 min - 24 hours
Premixed(cloudy)
Humalog mix 25 TMHumulin (20/80, 30/70)
Novolin ge (10/90, 20/80, 30/70, 40/60, 50/50)

MEDICATIONS FOR DIABETES: INSULIN
Five methods to deliver insulin:
1. Intravenous
2. Syringes
3. Pens
4. Jet Injectors
5. Insulin Pumps

MEDICATIONS FOR DIABETES: SODIUM BICARBONATE
- Alkalizing agent used for the treatment and reversal of metabolic acidosis
- At NBGH it is given IV as per the diabetic protocol:
- if pH is less than 7.0 add 50mmol NaHCO3 to 200ml of 4.5% saline, infuse at 200ml/h
- if pH is less than 6.9 add 100mmol NaHCO3 to 400ml of 4.5% saline, infuse at 200ml/h
- if pH is greater than 7.0- do not give NaHCO3

Education
Nurse’s Role for Clients with Diabetes
One of the biggest challenges in recent years regarding diabetic management is takingresponsibility for your own care. It’s not just the doctor, or the nurse that takes care ofyour diabetes. Now it is a collaborative approach with the client. (Canadian Diabetes Association, 2006)
Nursing Role:
-To slow progression of diabetes, and to minimize the complications of the disease, the nurse works with the client to enhance wellness and health.
-Informing the client regarding signs and symptoms of complications, adherence to medication regimes, as well as diet, food choices and exercise
-Linking the client to multiple resources in the community that provide counseling, information sessions, as well as a variety of other programs that will be beneficial to the client
-Depression affects 15% of diabetics due to complications resulting from the condition. The nurse should educate clients and family members about this heightened risk factor, and acknowledge the steps clients can take to minimize this complication.

Nurse’s Role for Clients with DiabetesTeaching Regarding Nutrition
-What, when and how much you eat all play an important role in regulating bloodglucose levels.
-The amount of food you need to eat daily depends on:
-Age-Body size-Activity level-Gender-Pregnancy or breastfeeding
-Diabetics are urged to follow the Glycemic Index for foods-Scale that ranks carbohydrate-rich food by how much they raise blood glucose levels-Adherence to the Glycemic Index can help control blood cholesterol levels control appetite cravings, lower the risk for cardiovascular disease and slow the progression of type II diabetes by controlling blood glucose levels

Nurse’s Role for Clients with DiabetesTeaching Regarding Nutrition
Glycemic Index:
-Postprandial blood glucose rises in response to the type and amount of food that is ingested -The degree that food elevates blood glucose is called it’s glycemic response
-The glycemic response is influenced by what type of food it is, how the food is processed, and how much is eaten:
-Canada’s Food Guide states that 55% of calories consumed per day should originate from carbohydrates
- But, not all carbohydrates have the same glycemic response - Many can drastically elevate blood glucose quickly, putting the client at risk for complications of diabetes

Skim milkPlain YogurtSoy beverageApple/plum/orangeSweet potatoOat bran breadOatmeal (slow cook oats)All-Bran™Converted or Parboiled ricePumpernickel breadAl dente (firm) pastaLentils/kidney/baked beansChick peas
BananaPineappleRaisinsNew potatoesPopcornSplit pea or green pea soupBrown riceCouscousBasmati riceShredded wheat cerealWhole wheat breadRye bread
WatermelonDried datesInstant mashed potatoesBaked white potatoParsnipsRutabagaInstant riceCorn Flakes™Rice Krispies™Cheerios™Bagel, whiteSoda crackersJellybeansFrench friesIce creamDigestive cookiesTable sugar (sucrose)
Low Glycemic Response Medium Glycemic Response High Glycemic Response
Glycemic Index:
Nurse’s Role for Clients with Diabetes
Benefits of low glycemic index foods are not limited to the minimal effect on blood glucoseThey tend to be healthier, lower in fat, and high in fiber, nutrients, and antioxidants.

Nurse’s Role for Clients with DiabetesTeaching Regarding Exercise
- Regular physical activity helps your body lower blood glucose levels, promotes weight loss, reduces stress and enhances overall fitness
-The benefits of exercise include:
Lower rates of illness and deathHigher rates of weight lossBetter heart and lung healthBetter blood pressure controlEnhanced lipid controlStronger bones and optimal balanceReduced levels of stress and depressionImproved mental skillsLower rates of heart disease, stroke, cancer and depressionMore energyHigher self-esteem

Nurse’s Role for Clients with DiabetesTeaching Regarding Exercise
Type I Diabetics:
-Blood glucose levels fluctuate due to the type, duration, and intensity of the exercise and the timing of the last insulin administration and carbohydrate intake
What do you think is important in educating type I diabetics about exercise?
-Low to moderate intensity exercise lowers blood glucose levels and can lead to hypoglycemia
-High intensity exercise can lead to hyperglycemia due to increased stress placed upon the muscles and cardiovascular system
Nursing Interventions: -Educate clients to take CBG before exercising, along with a meal rich in low glycemic carbohydrates to normalize blood glucose levels throughout exercising-Keep a source of emergency glucose reserves on hand