Embed Size (px)
Citation preview

Developmental disorders of teeth
By : Dr.hanan ahmad
abumnaizel

Developmental disorders of teeth, soft tissues, and craniofacial malformations e.g. cleft lip and palate.
Developmental disorders :-1-Teeth.2- oral soft tissues 3- craniofacial Defects e.g. cleft lip and palate.
(1)Teeth :-1- Number 2- size 3- from (abnormalities of morophodiffrentiation.4- Defects in tooth structure : Defects in histodiffrentiation.(2)Number :-(A) Hypodontia: when one or several teeth are missing . _ Anodontia : when there is complete absence of one or both dentitions. _ Hypodontia : is more common in permanent than deciduous dentition .
_ more common in females .

_ may be symmetrical or habhazourd .
_ primary teeth are unusual to be missing, but when tooth is missing usually permanent successor is also missing .
_3rd molars, max lat incisors, mandibular 2nd pemolars are most frequently associated with symmetrical hypodontia .
_max . Late. Incisor loss usually associated with hereditary trait.
_ mutations in regulatory genes may result in tooth agenesis (e.g.: MSX1).

_ Severe hypodontia\ Anodontion is associated most frequently with :{hypohidrotic ectodermal dysplasia}.
_ it is characterized by congenital absence of ectodermal structures.
_ usually X-linked recessive trait .
_ patients have smooth dry skin with fine scanty hairs and partial or total loss of sweat glands which lead to hyperthermia . Some patients have few deformed teeth with conical crowns .

(B) Hyperdontia :- (supernumerary teeth)
_ more common in anterior and molar region of the maxilla followed by premolar region in the mandible .
_ occasionally associated with other defect .
_ more common in females .
_relatively uncommon in primary dentition .
_ mesiodense:- the most common supernumerary teeth between maxillary central incisors, the majority have conical crown and short roots.

Paramolar :- alongside max molars usually buccaly erupted.Distomolar :- develops distal to a third molar .
Supernumerary teeth which resemble those of the normal series are called supplemental teeth but more are reduced in size .
(2) Size :-Macrodontia $ microdontia :_ size of teeth $ jaws is influenced by genetic $environmental factors.terms macro and microdontia are used to describe teeth which are larger or smaller than normal. _ microdontia of the whole dentition may be associated with other defects e.g down syndrome, congenital heart disease .

Abnormalities in size $ number of teeth may occur together e.g one missing permanent max lat.incisor in which case the contralateral tooth is frequently peg_shaped .
(3) Disturbance in form of teeth;disturbances in tooth form may involve crown ,root ,or both. the most frequent variation affects max permenant lat. Incisor which may be peg shaped or show accentuated cingulm .Premolars and molars with increased or decreased number of cusps are also frequently seen .1- dilaceration :-_The crown of the teeth is displaced from its normal alignment with the root ,so that the tooth is severely bent at its long axis _usually due to acute mechanical trauma_most frequently max incisors.

Taurodantism :-(bull-like) tooth , pulp chamber has greater apicoocclusal height than normal teeth. no constriction at CEJ. affects multirooted teeth may be caused by failure of hertawigs sheath to invaginate at proper horizontal level.
Either accidental or associated with other abnormalities such as no. of sex chromosme,such as in klinefelter and poly-X syndrome Rare in primary dentition.
(3) Double tooth ._The anomaly when 2 teeth appear joined together _ The union my involve crown, roots or both. _The union usually through dentin, pulp chamber not only enamel .

Previously the terms were :-_fusion; union Between dentin $\or enamel of two or more separate developing teeth._gemintion :- partial development of 2 teeth from a single tooth bud following incomplete division .
But the etiology remain unclear so the term now is double-tooth .common in primary .The incisors are most frequently affected. _In primary mostly mandibular ant teeth
(4) Concrescence :_roots of teeth are united by cementum, acquired anomaly. _union by cementum alone following hypercementosis._more common in permanent than Primary dentition .

Disturbances in sturcture :-(A)Enamel :-_enamel hypoplasia : deficient matrix production ._hypomineralised enamel :defective maturation-mineralisation.Clinicaly :*Hypoplasia\ pits or grooves in enamel structure or general reduction in
thickness of the whole enamel. the defective enamel have few prisms*hypemineralised enamel :-Appear white opaque it may be pigmented buff,orange,$brown and be
quickly chipped $worned away .Hypoplasia and hypomineralisation may affects single ,multiple or all
teeth . The structure of formed enamel depend on severity , duration ,nature of
the disturbances. usually the disturbances produce both hypoplasia $hypomineralisation but clinically one type usually predominate in a particular patient .

Table1.2 Aetiology of developmental abnormalities of enamel :
Local causes Infection Trauma Radiotherapy Idiopathic (enamel opacities )
General causes(a) Environmental systemic (chronological hypoplasias)(1) Prenatal _infections, e . g . Rubella , syphilis _maternal disease _excess fluoride ions (2) Neonatal _haemolytic disease of the newborn _hypocalcaemia _ _premature birth/prolonged labour

(3) Postnatal _ severe childhood infections, especially the viral exanthemata _chronic diseases , gastrointestinal and endocrine diseases _nutritional deficiencies , e . g. vitamin D _cancer chemotherapy _excess fluoride ions
(b) Genetic (1) Teeth only affected _amelogenesis imperfecta (2) Teeth affected in association with generalized defects _ectodermal dysplasia syndromes _Down syndrome (trisomy 21)

Aetiology of developmental abnormalities of enamel;
localized causes :--infection _trauma_radiotherapy_idiopathic enamel opacities
Local infection or trauma : if single tooth is only involved it is seen in max incisors, max or mandibular premolar .Turner tooth; infection or trauma of the deciduous Predecessor results in damage of the permanent successor .
Clinically :-the defect range from yellowish or brownish pigmentation the enamel to extensive Pitting and irregularity of the surface, the crowns often being smaller than normal .Yellow color is sometimes due to deposition of cementum on enamel
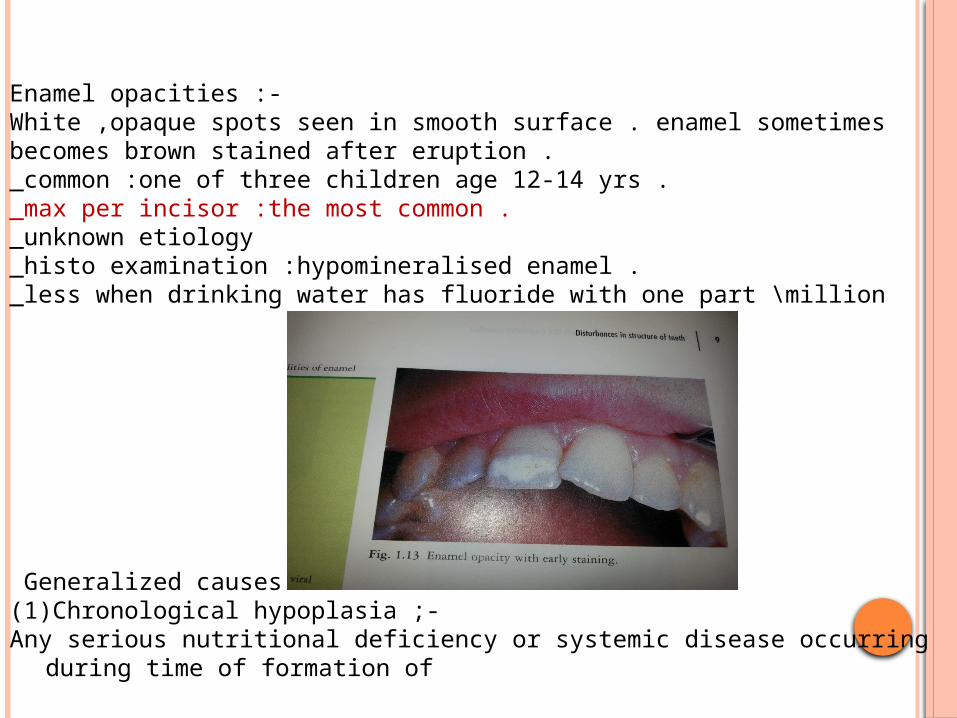
Enamel opacities :-White ,opaque spots seen in smooth surface . enamel sometimes becomes brown stained after eruption ._common :one of three children age 12-14 yrs ._max per incisor :the most common ._unknown etiology _histo examination :hypomineralised enamel ._less when drinking water has fluoride with one part \million
Generalized causes :-(1)Chronological hypoplasia ;-Any serious nutritional deficiency or systemic disease occurring during time
of formation of

The teeth can lead to hypoplasia or hypomineralisation,because ameloblasts are amongst the most sensitive cells in the body in terms of metobolic requirements .Pitting type usually results ,but ridging and grooving may also be seen _a horizontal band of hypoplsia may result , reflecting chronology of tooth development .
_ if the disturbance happen at or soon after birth . it may affects the incisal edges of the permanent central incisors and occlusal surfaces of the first permanent molars in addition to the deciduous teeth .(2) Congenital syphilis :-This produces characteristic hypoplastic change in the enamel of permanent

Incisors and first molars due to infection of tooth germ by spirochaetes .Mesial and distal surfaces of incisors taper toward incisal edges rather than toward cervical margin given a screwdriver appearance,and incisal edges usually have a central notch ; Hutchinsons incisors Most obvious of max central incisors .Occlusal surfaces Of the crowns of the lst molars are covered by small globular masses of enamel ;moon molar or. mulberry molar
Fluoride lons: - _excess ingestion of fluoride can produce : hypoplastic or hypominemlized enamel
_ early maturation stage is more sensitive than secretory stage.

Clinicaly ;_ faint white flecking of enamel, white patches, in severe cases yellow or brownish _black discoloration , particularly in teeth most exposed to light .Mottling ;- the term used to describe the appearance of dental fluorosis _mainly in permenant but deciduous teeth may be involved in severe cases or in areas of endemic fluorosis .
(4)Amelogenesis imperfecta : Is a group of hereditary conditions affecting enamel formation. Two types : 1- hypoplastic type. 2-hypomineralised \ hypomaturation type .Inherited as :autosomal dominant,autosomal resessive or x_linked form .Most cases are : autosomal dominant and less frequently x_linked traits .

The patterns of inheritence are not related to particular variations in the clinical manifestations (phenotype) All types of amelogenesis imperfecta affect deciduous and permanent dentitions and most of the enamel on all of the teeth involved _ X- linked forms associated with mutations in amelogenin (AMELX) gene ._Mutations in genes coding for other enamel proteins linked to autosomal patterns of inheritence .•Hypomineralisation from :_ The most common from ._Normal tooth morphology when first erupts._Soft chalky enamel easily lost exposing dentine ._teeth prone to attrition ,sometimes severe being worn down to gum level _Because of deficient mineralization the enamel has a similar density to dentine on radiographs.

Hypoplastic Type :-_enamal of normal hardness but variable appearances ._variable pitting | vertical grooving |generalized thinning .
-teeth may appear small ,show abnormal cuspal morphology : teeth may have needle –like cusps
Disturbances of structure of dentin :Local Causes :- Trauma e.g Turner teeth, radio therapy .Dentinogenesis imperfecta :- Type 1- associated with osteogenesis imporfecta .Type 11- only teeth are affected (including shell teeth) Type 111-Brsndy wine isolate (rare racial isolate in USA)

Dentin dysplasia :-Type 1-radicular dentine dysplasia (rootless teeth ) Type 11-coronal dentine dysplasia .Environmental \systemic:-Vit-D dependent rickets .-vit-D resistant rickets (hypophosphataemia)-haypophosphatasia .-juvenile hypoparathyoidism .-other mineral deficiencies .-Drugs e.g chemotherapeutic agents.
•Dentinogenesis imperfecta (hereditary opalescent dentine).Type 1--associated with osteogenesis imperfecta .-genetically distinct from type 11-primary dentition more affected than permanent .-appearance of primary dentition as for type 11.-the involvement of permanent dentition is very variable from type 11, tooth discoloration and attrition don’t occur to the same extent.

Type 11;- _autosomal dominant ._the most common dental genetic disease._affects both primary and secondary dentition._on eruption teeth have normal color but opalescent amber-like appearance, subsequently they may have normal color, then they become translucent , and finally grey or brownish with bluish reflection from enamel –although in most cases enamel is normal it is rapidly lost and teeth show marked attrition ._Radiographicaly ; short , blunt “stunted” roots with partial or total obliteration of pulp chambers And root canals by dentine. _abnormal dentine structure and composition ._Dentin shows an increased water and decreased mineral content ._caries is unusual but if happens it is confined to superficial layers ._pulp chamber of primary teeth may not be obliterated , dentine may remain thin and pulp may be exposed by attrition shell-teeth

Dentin dysplasia : _rare, autosomal dominant (1)Atype 1 : (rootles teeth )_ permenant teeth have normal crowns, root canals are obliterated ,roots stunted._due to defect in hertwig root sheath ._The first sign may be premature exfoliation either spontaneously or with minor trauma .(2) Type 11-Coronal dentine dysplasia .Permenant teeth are of normal colour and root length .
*metabolic disturbances affecting dentinogenesis:-_Rickets : areas of interglobular dentine corresponding to the period of illness may be seen ._vit D resistent rickets (hypophosphataemia);_ pronounced interglobular dentine and large pulp chambers and large pulp horn .overlying enamel may be cracked resulting in pulpitis.

Hypophosphatosia and nutritional deficiencies :_inter globular dentine ._Cytotoxic agents :-Produce incremental lines coincident with drug administration ._Juvenile hyperparathyroidism : Teeth are small with hypoplastic enamel , roots stunted .•Regional odontodysplasia (ghost teeth ) •_unknown etiology ._ abnormalities in pulp, dentine, enamel ,and dental follicle ._ mostly in anterior part of maxilla unilateral ._radiological examination: Reduced radioopacity of teeth and loss of distinction between enamel and dentin (ghost appearance )Disturbances in structure of cementum :--acellular (primary) cementum :-cover coronal 1/3 of root .-cellural (secondary) cementum; cover apical 2/3 and continues to be formed throughout life, its thickness increase with age to compensate for occlusal wear.

Hypercementosis : -
_ idiopathic or due to general or local disorders. _may be associated with ankylosis .Causes :-(1)Periapical inflammation :Although resorption of cementum occur close to the center of
inflammatory focus apposition may be stimulated alittle further away. This produces generalized thickening or localised konb-like enlargement .
(2) Mechanical stimulation :- Excessive forces applied to tooth may produce resorption, but
mechanical stimulus below threshold may stimulate apposition .
(3)Functionless and unerupted teeth :-
Such teeth may show cementum resorption or excessive apposition .(4)paget disease of bane :-_hypercementosis is common ._mosaic appearance of thickened cementum ._ankylosis is common.

HYPOCEMENTOSIS :-_Hypoplasia and aplasia of cementum is uncommon .cleidocranial dysplasia; there is lack of cellular cementum ._hypophosphatasia :- charectterised by :-_aplasia of cementum._recessive autosomal disease ._reduced serum alkaline phosphatase level and skeletal abnormalities ._premature loss of some or all deciduous and permanent teeth ._Dentin also may be abnormal .
(B) Soft tissues :- 1-oral mucosa. 2-gingiva and periodontium.3-Tongue _Oral mucosa :-1-white spongue nevus : _autosomal dominent ._superficial layer of epithelium are soft and of uneven thickness producing a shaggy or folded thickness _may be apparent in infancy or early child hood or may not be evident until adolescence .

Fordyces granule :-Sebaceous glands of oral mucosa are known as fordyces granules, separate, small, yellowish bodies, although on occasions may be numerous to from slightly raised confluent plaques, commonly in upper lip, cheeks, rarely in lower lip. (B)Gingiva and periodontium :-1- hereditary gingival fibromatosis :-_rare hereditary condition._mainly autosomal dominant but might be recessive ._Generalised or occasionaly localised fibrous enlargement of the gingiva which usualy begins with the eruption of permanent or occasionaly decidous teeth._may be associated with epilepsy, mental retardation .( C)Tongue :- 1-macroglossia 11- cleft tongue 111-ankyloglossia

(1)Macroglossia _may be caused by congenital or acquired conditions._the most common cause are :- _vascular malformations (lymphangioma and haemangioma)._muscle hyper trophy .In edentulous patients lack of teeth makes larger room of tongue
causing pseudomacroglossia .(11) Bifid Tongue : Congenital lingual structural defect in which its anterior part is
divided longitudinally.
(111) Ankyloglossia Tongue- Tie ) Congenital oral anomaly may decrease the mobility of the
tongue._may be mild characterized by mucous membrane , or complete
ankyloglssia .

Craniofacial anomalies :-Majority has genetic basis .May be associated with developmental genes e.G; cleidocranial dysplasia :-_mutation of master control genes of osteoblast function (11) Crouzon syndrome := Mutation of fibroblast growth factor receptor gene .*orofacial clefts :- (cleft of the lip and\or palate)_have multifactorial etiology involving the inter play of genetic and environmental factors._orofacial clefts are amongst the commonest of all congenital structural birth defects and may occur alone or in combination with over 300 Syndromes, although 70% are non-syndromic._the prevalence varies in different parts of the world but range from (1 in 500) or (1 in 1000) births usually ._ higher incidence of cleft lip and palate compared to clefts of palate alone there is familial history in about 30% of the former and 15% of the later .

20 possible genes have been suggestedClefts have also been associated with environmental factors;1-smoking.2-alcohol.3-folic acid deficiency.

Table 1.1 Example of craniofacial anomalies and developmental syndromesassociated with abnormalities in the number of teeth
Syndrome/anomaly Associated features
A . Hypodontia Cleft lip/palate .
Crouzon syndrome. Down syndrome (trisomy 21 ).
Hypohidrotic ectodermal dysplasia.
Ellis-van Creveld syndrome (chondroectodermal dysplasia).
Oral-facial-digital syndrome .
B. Hyperdontia.
Cleft lip/palate.
Cleidocranial dysplasia .
Gardner syndrome .
Oral-facial-digital syndrome
Possible deafness and other cranial and skeletal abnoramalities. Craniosynostosis , maxillary hypoplasia , hypertelorism. Multiple, e. g. mental retardation, maxillary hypoplasia, macroglossia.
Hypotrichosis, hypohidrosis, saddle-nose. Dwarfism , polydactyly , cardiac malformations.
Cleft palate , hypoplasia of the nose , digital malformations.
Possible deafness and other cranial and skeletal abnormalities.
Aplasia of clavicles, delayd ossification of fontanelles, enlargement of cranium . Multiple osteomas of jaws, skin cysts and fibromas.intestinal polyposis. Cleft palate , hypoplsia of the nose , digital malformations.

hyperdontia



Discoloration of teeth :- *Incorporation of pigments into the dental hard tissues during their formation . (1)Congenital hyperbilirubenemia: ( Neonatal Jaundice ) _in severe cases of Jaundice of neonates bile pigments
may be deposited in calcifying dentine and enamel along
neonatal incremental line. Mainly in dentine, the affected tooth discoloured green
to yellowish –brown. Enamel hypoplasia may also accur .(2) Congenital porphyria : Rare , autosomal recessive, in born error of porphyrin
metabolism , excretion of red prophyrin pigments in the blood . Being deposited in bone and dental hard tissues.

Affected teeth show pinkish-brown discoloration and red fluorescence under ultraviolet light .(3) Tetracycline pigmentation : Systemic administration of tetracycline during the period of tooth devebpment results in their deposition in dental hard tissues as well as in bone . Dentine is more heavily stained than enamel ._Yellow bands related to incremental lines in dentine can be seen._The pigmented bands fluoresce a bright yellow under ultraviolet light. _The severity of discoloration in depends on ;_Type of tetracycline preparation,_Dose._Age of patient._Time of drug administration. Tetracycline cross placenta and can affect deciduous teeth if given anytime from 29 weeks to full term. It is also important to avoid tetracycline from 4 months to about 7 years.

Disorders of eruption and shedding teeth ._premature eruption natal and neonatal teeth ._Natal teeth : teeth erupted at birth._Neonatal teeth , erupts within the first 30 days of life .
_1/3000 births._Mainly mandibular incisors._Arise from normal tooth germs developing in a superficial position in the Jaw. _May be lost spontaneously or have to be extracted if there is risk of dislocation or inhalation ,or if they interfere with feeding._Generalized early eruption of the permanent dentition may also be seen in children with endocrine abnormalities associated with excess secretion of grwoth hormone or with hyperthyroidism.

Retarded eruption :-Endocrinopathies (e,g hypothyroidism ),prematurity nutritional deficiencies . And chromosome abnormalities such as down syndrome may be associated with retarded eruption.Idiopathic migration , traumatic displacement of tooth germs or abnormally large crowns may also be associated with retarded eruption .
Premature loss :- Occasionally it is associated with hyophosphatasia . Hereditary palmer- planter hyperkeratosis.

Persistence of deciduous teeth :-Associated with the failure of eruption of the permanent succors because it is missing or displaced ._persistence of the entire deciduas dentition is uncommon and has systemic background such as cleidocranial dysplasia .
* Impaction of teeth :- Impacted tooth is the one which remain unerrupted in the jaw beyond the time when it should normally be fully erupted ._Rarely seen in primary dentition ._Most frequently :-3rd molars , mand . Premolars Max canines ._Local causes :-1-abnormal position of tooth germ.2-lock of space for the teeth in the jaws.3-supernumerary teeth.
Reimpaction of tteeth The term describes the situation in which i previously erupted tooth becomes submerged in tissues .
Alternative terms are infraocclusion and submerged teeth. The deciduous second molar is most commonly affected and reimpaction occurs twice as frequently in the mandible than in the maxilla .the cause is unknown , but it is likely that the root first became ankylosed and this is followed by alack of growth of the alveolar process .





























