Embed Size (px)
Citation preview

NEOPLASIA
Melbia Shiny First MDS

contents Definition classification Difference between benign & malignant Metastasis Carcinogens & carcinogenesis
Definition A mass of tissue formed as a result of
abnormal ,excessive , uncoordinated , autonomous , & purposeless proliferation of cells.
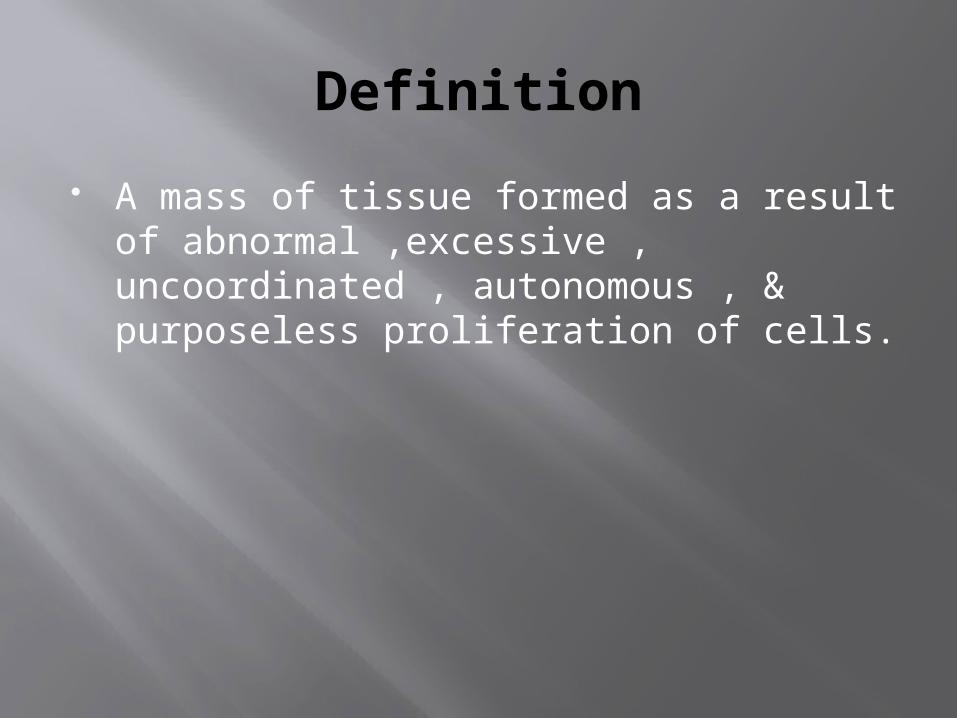
Classification
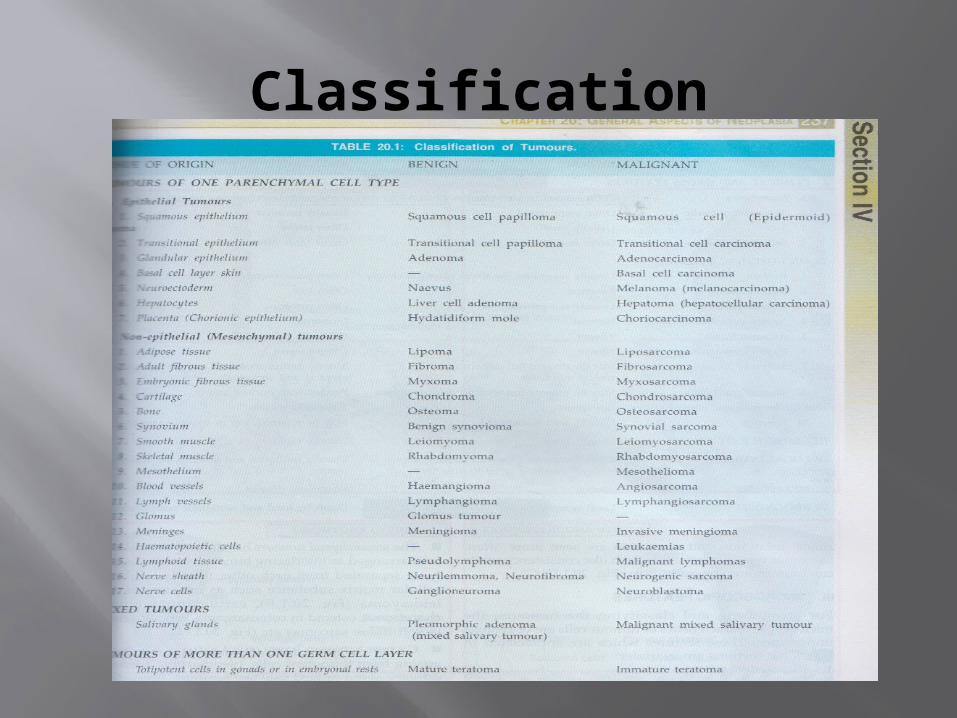
Difference between benign & malignant
metastasis Spread of tumour by invasion in such a
way that discontinuous secondary tumour mass/masses are formed at site of lodgement.
Routes of metastasis Lymphatic spread Haematogenous spread Other routes- transcoelomic
spread,implantation ,spread through CSF,epithelium lined surface,
Lymphatic spread Carcinomas – metastasise by lymphatics Sarcomas - metastasise by
hamatogeneous route. Two forms: Lymphatic permeation-walls of
lymphatics invaded by cancer cells & form continuous growth

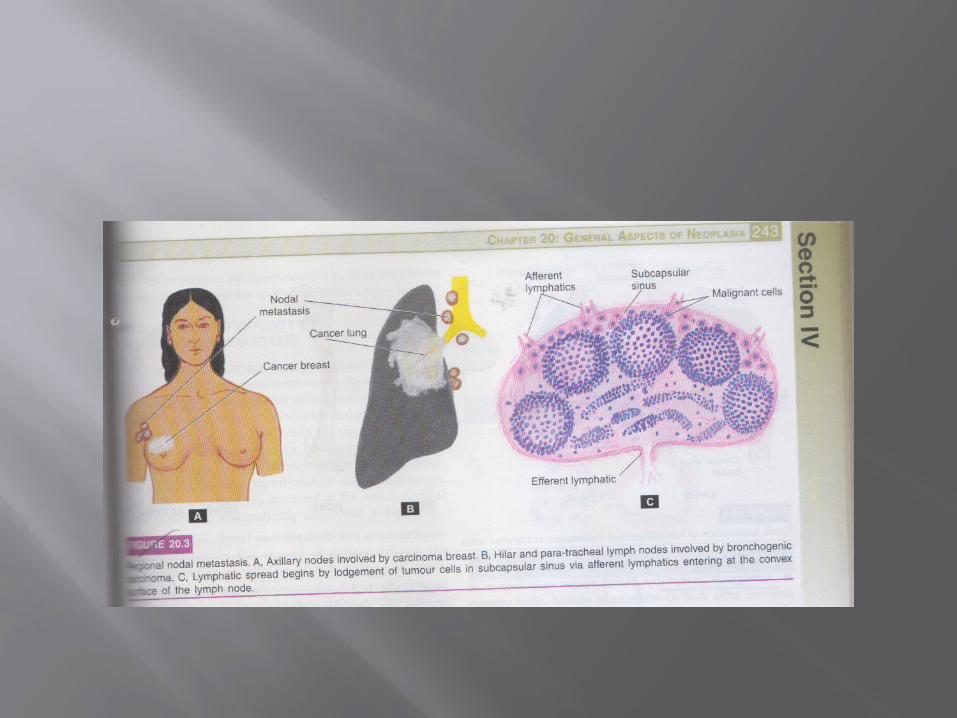
Lymphatic emboli - malignant cell detach to form tumour emboli & are carried along lymph to next lymph node & get lodged in subcapsular sinus.
Regional nodal metastasis seen in: Carcinoma breast – to axillary lymph
nodes Carcinoma thyroid – to lateral cervical
lymph node
Skip metastasis – due to venous lymphatic anastomosis/ due to obliteration of lymphatics by inflammation or radiation lymphatic metastasis do not occur in nearest node.
Retrograde metastasis – due to obstruction of lymphatics by tumour cells lymph flow is disturbed & tumour cell spread against flow of lymph.
Virchow’s lymph node – nodal metastasis to supraclavicular lymph node from cancer of abdominal organs.
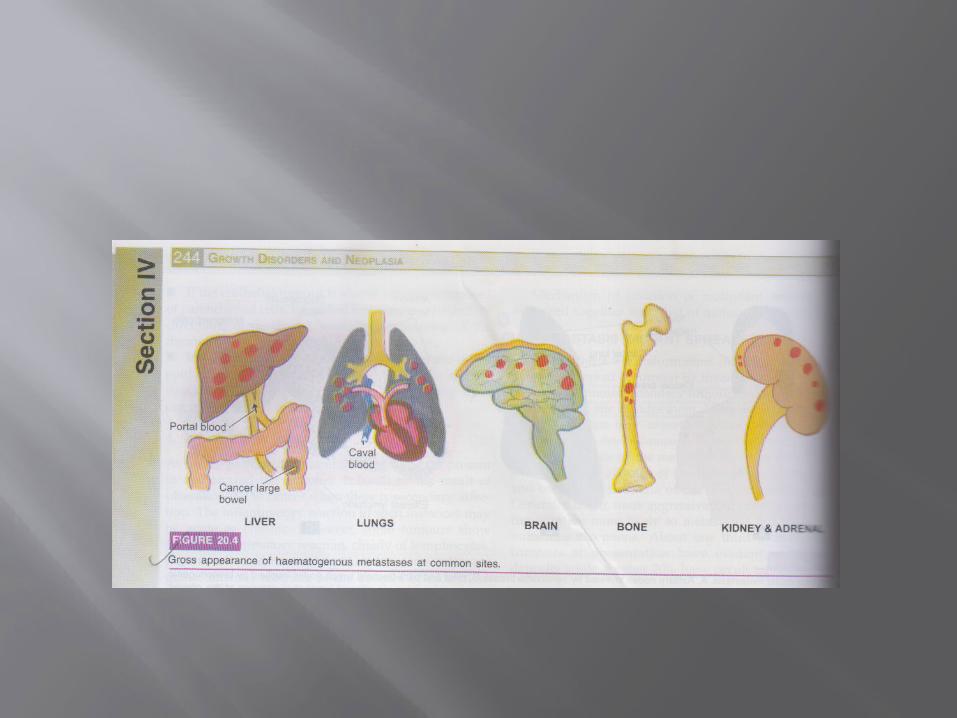
Haematogenous spread Common sites are – liver ,lung ,brain,
bone,kidney, & adrenals These provide good soil for growth of
good seed - Seed soil theory Do not allow metastasis to grow – heart ,
spleen , skeletal muscle. Arterial spread is less likely because of
thick wall & elastic tissue.

Systemic vein drain into vena cava from limbs ,head ,neck & pelvis.- metastasis to lungs
Portal vein drain from bowel , spleen, & pancreas – secondaries in lungs
Retrograde spread due to venous obstruction ,seen in vertebral metastases in cancer of thyroid & prostrate.
Spread along body cavity & natural passage
Transcoelomic spread Cancers invade serosal wall of coelomic
cavity so tumour fragments break & are carried in coelomic fluid & get implanted in body cavity.
Peritoneal cavity mostly involved Carcinoma of stomach into ovary Carcinoma of ovary into peritoneal cavity Carcinoma of bronchus & breast into
pleura & peritoneum
Along epithelium lined surfaces Unusual because intact epithelium are
resistant to penetration by tumour cell Fallopian tube from endometrium to
ovaries & vice versa Through bronchus into alveoli Through ureters from kidney into lower
urinary tract
Spread via CSF Malignant tumours of leptomeninges
spread by releasing tumour cells into CSF to produce metastasis
Implantation Due to implantation by needles , sutures,
or transfer from lower lip to upper lip.

Mechanism & biology of invasion & metastasis
steps a involved at cell molecular level: 1)aggressive clonal proliferation and angiogenesis rapidly proliferating clone of cancer cells
based on tumour heterogenicity.Tumour angiogenesis (new blood vessels are formed from pre existing ones) plays a important role,which provide nourishment to growing tumours.The morphologic features are:
i)microvascular density –the new capillaries add to vascular density of tumour.
ii)central necrosis –if tumour outgrows its blood supply tumour angiogenesis fail & core undergoes ischaemic necrosis.
2)Tumour cell loosening Normally cell adhesion is due to
CAMs,E(epithelial)-cadherin.in carcinomas there is loss or inactivation of E-cadherin & other CAMs.
3)tumour cell ECM interaction Loosened cancer cells are
attached to ECM proteins laminin & fibronectin.

4)degradation of ECM Tumour cells overexpress proteases and
matrix degrading enzymes ,cathepsind metalloproteinases(collagenase,gelatinase). (dissolution of ECM).
5)entry of tumour cells into capillary lumen This is by these mechanism: Autocrine motility factor (AMF)-this stimulate
receptor mediated motility of tumours cells Cleavage products of matrix components-these
promote chemotaxis,growth promotion & angiogenesis.
6)thrombus formation The protruding tumour cells are covered
with circulating blood and form thrombus.Thrombus provide nourishment and protect from immune attack.
7)extravasation of tumour cells Tumour cells block these vascular
channels and attach to vascular endothelium. 8)survival and growth of metastatic deposit The extravasated malignant cell on
lodgement grow further under growth factors(PDGF, FGF, TGF-B & VEGF.

Grading of cancer Grading is defined as macroscopic &
microscopic degree of differentiation of tumour
Based on : Degree of anaplasia Rate ofgrowth

Borders grading Grade I – well differentiated (<25%
anaplastic) Grade II – moderately differentiated (25-
50% anaplastic cells) Grade III – moderately differentiated(50-
75% anaplastic cells) Grade IV – poorly differentiated /
anaplastic (>75% anaplastic cells)
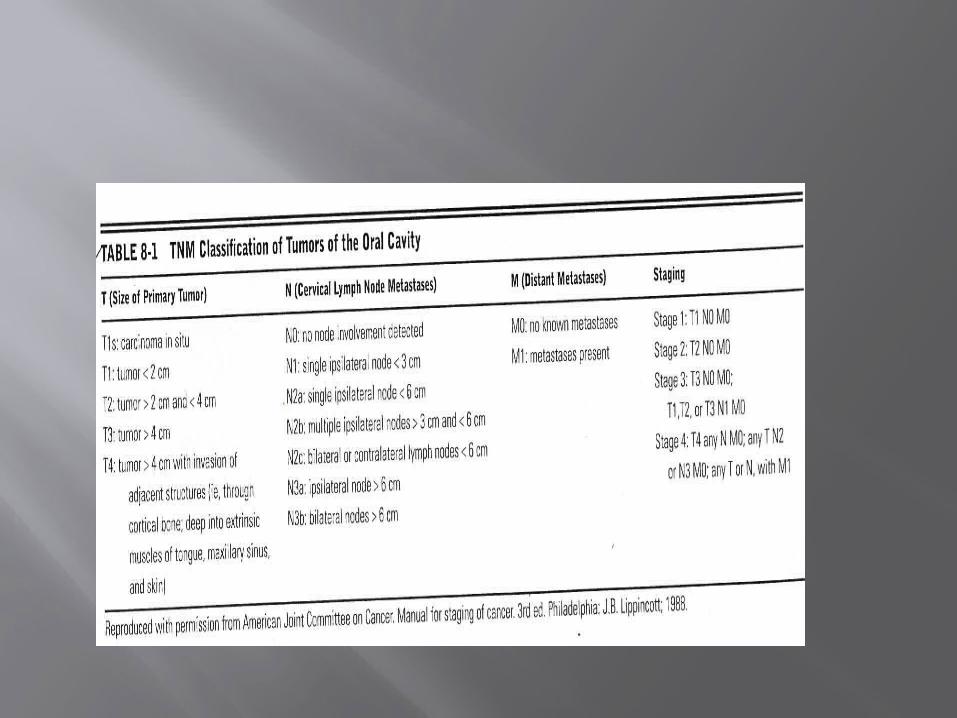
Staging of cancer Means extent of spread of tumour within
the patient TNM staging: T- primary tumour N- regional nodal involvement M- distant metastasis

CARCINOGENESIS AND CARCINOGENS
Carcinogenesis /oncogenesis/tumorigenesis means mechanism of induction of tumours.
Agents inducing tumours are called carcinogens The etiology & pathogenesis are discussed under 1)molecular pathogenesis of cancer(genes &
cancer) 2)chemical carcinogens & chemical
carcinogenesis 3)physical carcinogens & physical carcinogenesis 4)biologic carcinogens & viral oncogenesis.

MOLECULAR PATHOGENESIS OF CANCER
The general concept of molecular mechanism of cancer is below;
1)monoclonality of tumours arise from single clone of cells by
genetic transformation or mutation. In multiple myeloma(malignant disorder of
plasma cell)there is production of single type of immunoglobulin.
benign uterine tumours contain either A or B genotype,while normal myometrium is mosaic
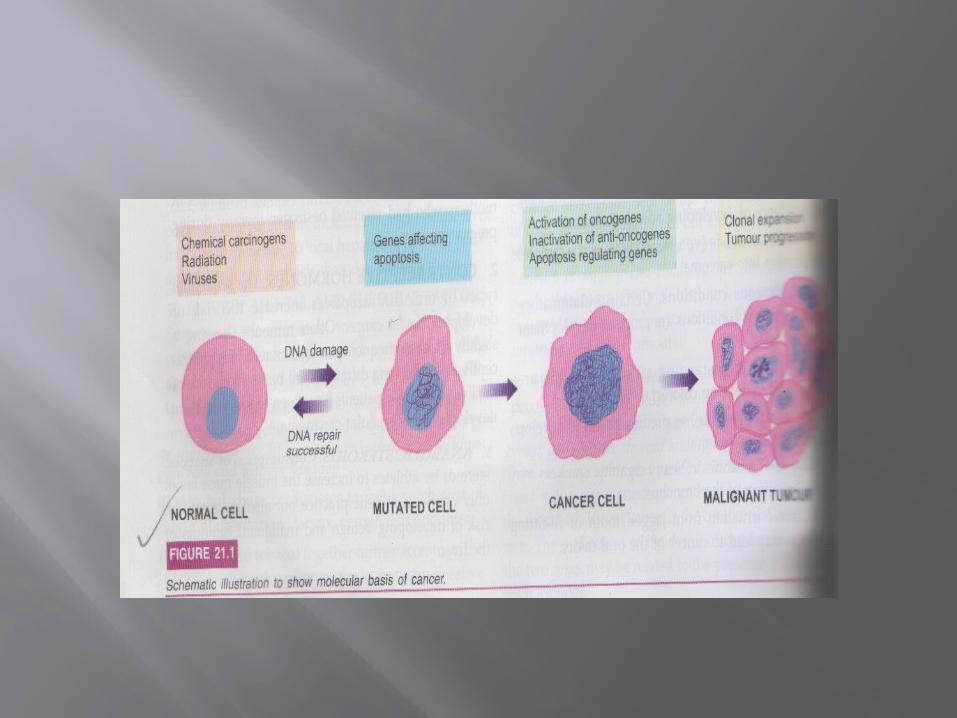

2)Genetic theory of cancer There is either abnormality in genes of cell or
normal genes with abnormal expression.3)genetic regulators of normal & abnormal mitosis In normal cell growth four regulatory genes Proto oncogenes Anti oncogene Apoptosis regulatory genes DNA repair genes In cancer transformed cells are produced by activation of growth promoting oncogene
Inactivation of cancer suppressor gene Abnormal apoptosis regulatory genes Failure of DNA repair4)multi step processof cancer growth &
progression

CANCER RELATED GENES AND CELL GROWTH
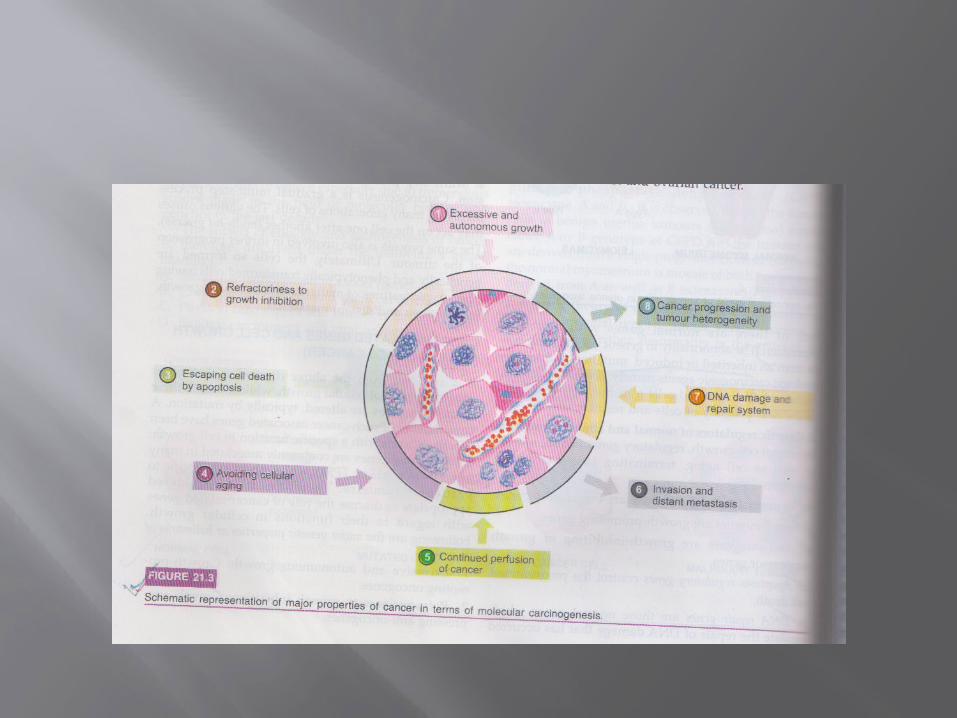
i)excessive & autonomous growth –growth promoting oncogenes.
ii)refractoriness to growth inhibition- growth suppressing anti oncogenes.
iii)escaping cell death by apoptosis – genes regulating apoptosis and cancer.
iv)avoiding cellular aging – telomeres & telomerase.v)continued perfusion of cancer – cancer angiogenesis.vi)invasion & distant metastasis- cancer dissemination vii)DNA damage & repair system- mutator gene& cancer viii)cancer progression & tumour heterogeneity.- clonal
aggressiveness.

Growth promoting oncogene

Growth supressing oncogene
3)Gene regulating apoptosis & cancer:
In cancer cells apoptosis is interfered due to mutation in the gene.eg are
BCL2 gene seen in B cell lymphoma removes the apoptosis –inhibitary control on cancer cells.
CD95 receptors are depleted in hepatocellular carcinoma.
4)Telomereses & telomerase in cancer
Telomerase is RNA enzyme that help in repair of damage to DNA and maintain normal telomere length in successive cell division.
After repetitive mitosis telomeres are lost in normal cell & cease mitosis.Cancer cell have upregulated telomerase enzyme ,hence avoid aging & mitosis does not slow down.
5)Tumour angiogenesis The stimulus is provided by Promoters of tumour angiogenesis-
vascular endothelial growth factors(VEGF)& basic fibroblast growth factors(bFGF)
Antiangiogenesis factors – thrombospondin 1,angiostatin ,endostatin & vasculostatin.
6)Mutated genes & cancerThe example mutated gene present are ;Hereditary nonpolyposis colon cancer(lynch syndrome)Ataxia telangiectasia(ATM)Xeroderma pigmentosumBloom syndromeHereditary breast cancer

7)Clonal aggressiveness With passage of time tumour cells
acquire more heterogenecity & leads to tumour progression.

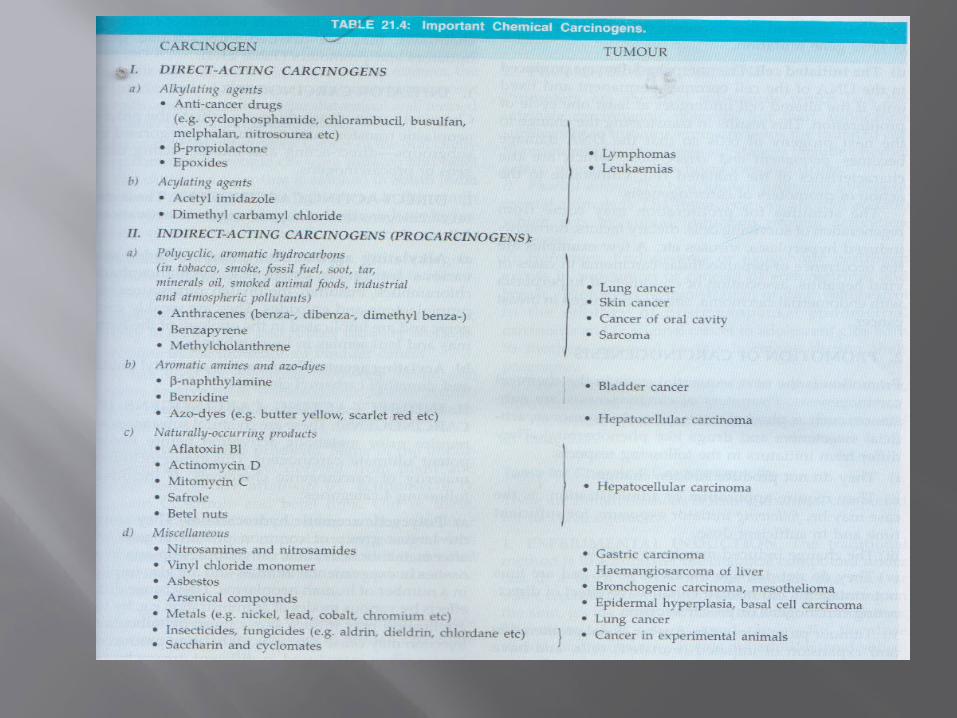
CHEMICAL CARCINOGENESIS
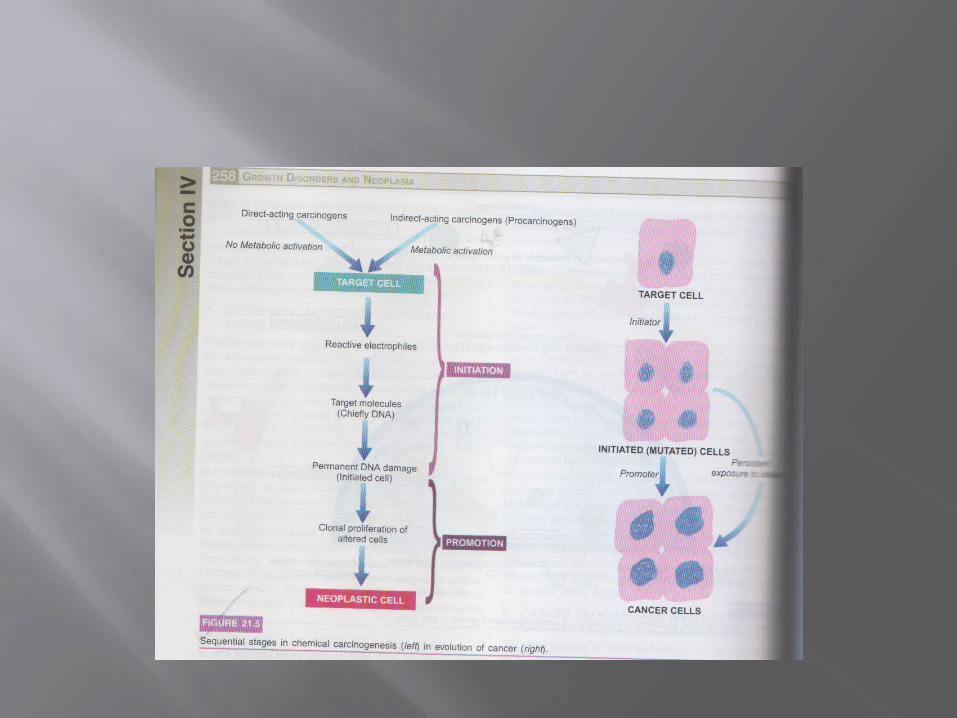
The stages of chemical carcinogenesis is : i)Initiation of carcinogenesis there are two (direct acting & indirect
acting). The steps are involved to transform target
cell to initiated cell a)Metabolic activation procarcinogens needs activation & are
activated in liver by monooxygenase of cytochrome& P-450 system in endoplasmic reticulum
b)Reactive electrophiles these bind to electron rich portions
such as DNA, RNA, other proteins. c)Target molecules the primary target is DNA
producing mutagenesis d)Initiated cell the changes produced in DNA
become fixed only if the altered cell undergoes one cell cycle

ii)Promotion of carcinogenesis they are not mutagenic need repeated dose exposure for long
time produce slow response the change may be reversible applied after exposure to initiators is not effective alone there is a clonal expansion of mutated
gene eg- hormones , phorbol esters

PHYSICAL CARCINOGENESIS
They are of two types; Radiation & nonradiation i)Radiation carcinogenesis UV & ionizing radiation the UV radiation produce pyrimidine dimmers
in DNA which remains unrepaired in exceesively exposed individuals.
Ionizing radiation are X rays ,alpha ,beta,gamma rays radioactive isotopes ,protons & neutrons can cause cancer.
ii)Non radiation carcinogenesis these include mechanical injury
from stones in gallbladder, urinary tract, healed scars from burns /trauma,implant materials like plastic ,glass, or foreign bodies.

BIOLOGIC CARCINOGENESIS THEY ARE Parasites- schistosoma haematobium
cause carcinoma of urinary tract Fungus – aspergillus flavus cause
hepatocellular carcinoma Bacteria – helicobacter pylori cause
gastric lymphoma

VIRAL CARCINOGENESIS
Oncogenic viruses is transmitted byVertical transmission-from parent to
offspring Horizontal transmission- one to another
by direct contact Two types of oncogenic viruses are DNA
oncogenic viruses & RNA oncogenic viruses

DNA ONCOGENIC VIRUSES
1)Papova virus Human papilloma virus Papilloma virus Polyoma virus2)Herpes virus EB virus Human herpesvirus 83)Adeno virus4)Pox virus 5)Hepadnavirus HB virus
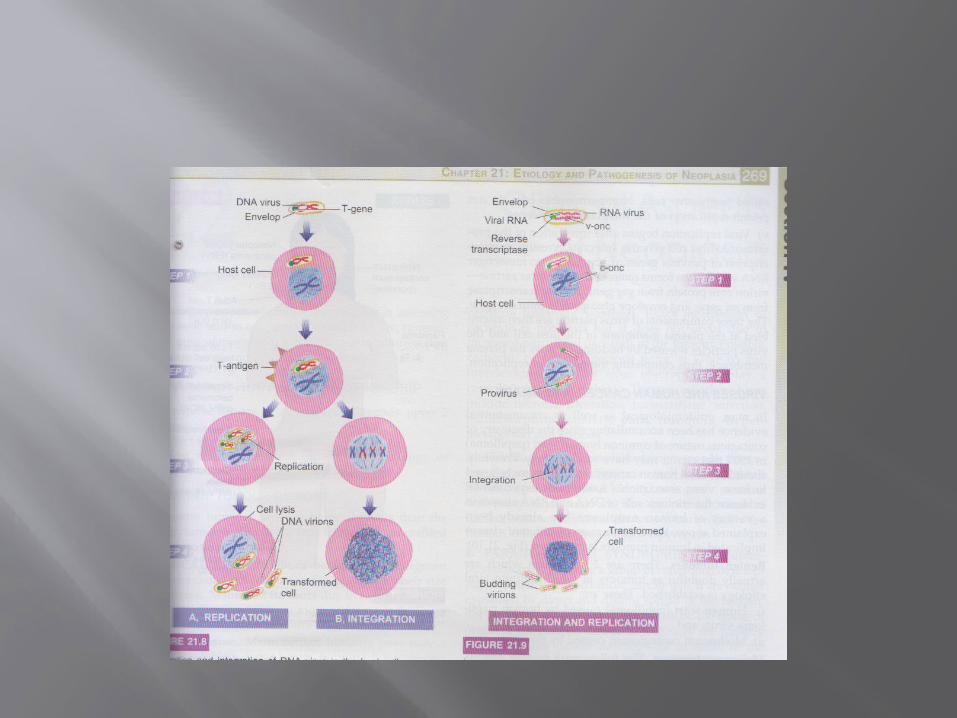
Mechanism
1)Mode of DNA viral oncogenesis Replication The DNA virus invade the host cell & is
incorporated into host nucleus & T antigen is expressed.
Virions are formed in cell nucleus.The new virions released are accompanied by host cell lysis.
Integration Integration of viral genome into host
cell genome occurs which requires essential presence of functional T antigen.
2)Mode of RNA viral oncogenesis a)RNA virus invade the host cell ,the viral
envelope fuses with plasma membrane of host cell,viral RNA genome as well as reverse transcriptase are released into cytosol
b)Reverse transcriptase act as template to synthesise single strand of matching viral DNA which is copied to form complementary DNA resulting in double stranded viral DNA(proviruses)
c)The provirus is integrated into host cell genome d)Finally brings about replication of viral
components.
DIAGNOSIS OF CANCER
1)histological methods 2)cytological methods Exfoliative cytology FNAC 3)histochemistry & cytochemistry 4)immunohistochemistry 5)electron microscopy 6)tumour markers 7)modern aids Flow cytometry In situ hybridization Molecular diagnostic techniques DNA micro assay analysis of tumours
Thank you