Embed Size (px)
DESCRIPTION
Citation preview

Motor System Examination
By:
Vibhushit Kaul69/09

Outline•Anatomy•Inspection and Palpation•Posture and abnormal movements•Tone and Power•Reflexes•Coordination•Stance and gait

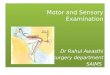
MOTOR PATHWAYS
Corticobulbar (corticonuclear) fibers: originate in the region of the sensorimotor cortex, where the face is represented. They pass through the posterior limb of the internal capsule and the middle portion of the crus cerebri to their targets, the somatic and brachial efferent nuclei in the brain stem.

Corticospinal tract: originates in the remainder of the sensorimotor cortex and other cortical areas. It follows a similar trajectory through the brain stem and then passes through the pyramids of the medulla (hence, the name pyramidal tract), decussates, and descends in the lateral column of the spinal cord.




Inspection and Palpation
Look for:•any asymmetry, inspecting both proximally and distally. •any deformities such as clawing of the hands or pes cavus.•wasting or hypertrophy, fasciculation and involuntary movements. •Palpate muscles to assess their bulk.


Causes of Muscle wasting
•Lower motor neurone lesions, peripheral nerve section•Longstanding or developmental upper motor neurone damage disuse atrophy of muscle groups•Muscle disorders •Rheumatoid arthritis•Cachexia

Posture and Abnormal Movements
Ask the patient to hold the arms outstretched with the eyes closed:
•Pyramidal drift describes a tendency for the hand to move upward and supinate if the hands are held outstretched in a pronated position (palms downward), or to pronate downward if the hands are held in supination.
•Cerebellar drift is generally upward, with excessive rebound movements if the hand is suddenly displaced downward by the examiner.
•Parietal drift is an outward movement on displacing the ulnar border of the supinated hand.

Abnormal movements
•Fasciculations•Tremors: Rest tremors, Postural tremors, Action tremors, Hysterical tremors, Rubral tremors•Myoclonic jerks •Athetosis•Chorea•Ballism or Hemiballismus

•Pseudoathetosis
•Dystonia
•Tics
•Tetany
•Cramps

TONE
•Muscular tone refers to the state of muscle tension or contraction
•For clinical purposes, it is the resistance felt by the examiner when moving a joint passively through its range of movement.

Examination sequence
•Ask the patient to lie supine on the examination couch, relax and 'go floppy'. •Passive movements of the joints should be through as full a range as possible and both slowly and quickly. •In the upper limb hold the patient's hand as if shaking hands, using your other hand to support the patient's elbow. Then rotate the forearm, flex and extend the wrist, elbow and shoulder, varying the speed and direction.•With the lower limb begin by rolling or rotating the leg from side to side, then briskly lift the knee into a flexed position.•Knee clonus: with the patient relaxed and the knee extended, sharply push with your thumb and forefinger above the patella towards the foot, sustaining the pressure for a few seconds. •Ankle clonus: support the patient's leg with both the knee and ankle resting in 90° flexion. Briskly dorsiflex and partially evert the foot and sustain the pressure

Common abnormalities
•Hypotonia: decreased muscle tone•Hypertonia: increased muscle tone.There are two principal types of hypertonia:
spasticity rigidity

Power•Muscle power is tested for groups of muscles moving various joints.•Strength of individual muscle groups is tested by comparing them with examiner’s own strength•Before testing power always look for tenderness and contracture of muscles and joints•Fix the proximal joints to avoid movements by uninvolved muscles.

MRC Scale for grading muscle power
Grade 0 Complete paralysis
Grade 1 A flicker of contraction only
Grade 2 Power detectable only when gravity is excluded by postural adjustment
Grade 3 Limb can be held against gravity but not resistance
Grade 4 Limb can be held against gravity and some resistance
Grade 5 Normal power

Examination sequence
•Test the power of individual muscle groups in both limbs alternately to compare.•Ask the patient to contract a group of muscles to maintain a position and resist your attempt to displace the limb (isometric testing).•Ask the patient to put the joint through a movement while you try to oppose the action (isotonic testing).

Muscles of Shoulder Girdle & Scapula
Supraspinatus:
•Main Segmental Supply
–
C5, C6
•Nerve supply-
Suprascapular
Nerve
•Action: Shoulder
abduction•Test: The patient rests the
arm down by the side. Grip at the elbow and resist abduction

Deltoid
•Main Segmental Supply - C5
•Peripheral Nerve – Circumflex
•Action: Shoulder abduction, extension
•Test: The patient abducts arms with elbows
bent. Press down on the upper arms

Deltoid

Infraspinatus(C5, Suprascapular)
•Action: Shoulder External rotation•Test: The patient rests the arm down by his side with the forearm pointing anteriorly at 90° to the arm. Resist external rotation of the shoulder

Pectoralis major(sternocostal head)
•Nerve supply: Medial and lateral pectoral; C6, C7, C8
•Causes shoulder adduction•Test: The patient brings the arm just a little away from the side. Hold at th elbow and resist shoulder adduction. Observe the musclecontract on the anterior chest wall

Pectoralis major(Clavicular head)
•Nerve Supply: Lateral pectoral N.; C5, C6•Shoulder flexion•The patient brings the arm up laterally with the forearm pointing superiorly. Hold at the elbow and resist shoulder flexion forwards.

Rhomboids
•Nerve Supply: Dorsal scapular N.; C4, C5•Shoulder internal rotation•Test: The patient brings the hand to the small of the back with the palm facing posteriorly. Press against the palm of the patient's hand to resist movement of the hand posteriorly.

Serratus anterior
•Long thoracic C5, C6, C7•Stabilization of scapula•Test: The patient brings the hands anteriorly to push against a vertical wall. In paralysis, the free medial edge of the scapula 'wings‘ posteriorly away from the rib cage
Winging of scapula

Latissimus dorsi
•Thoracodorsal N.; C6, C7, C8•Shoulder adduction•The patient brings the arm up laterally to horizontal. Hold at the elbow and resist shoulder adduction. Observe the muscle contract on the side of the chest wall

Elbow
Biceps brachii•Musculocutaneous N.; C5, C6•Elbow flexion•The patient flexes the elbow with the forearm supinated. Hold the wrist, stabilize at the elbow and resist flexion

Triceps
•Radial N.; C6, C7, C8•Elbow extension•The patient holds the arm out with the elbow half-extended. Hold at the wrist, stabilize at the elbow and resist extension
Testing Long head
Testing whole muscle

Brachioradialis
•Radial N.; C5, C6•Elbow flexion•The patient flexes the elbow with the forearm mid-pronated. Hold the wrist, stabilize at the elbow and resist flexion. Observe the muscle belly along forearm.

Forearm: Supinator
•Radial N.; C6, C7•Forearm supination•Grasp the patient in a handshake with the patient's elbow extended and resist supination.

Pronator teres
• Median N.; C6, C7 • Forearm pronation• Grasp patient in a
handshake with his elbow extended and resist pronation.

Wrist and Hand
Extensor carpi radialis longus•Radial N.; C5, C6•Wrist extension and abduction•The patient cocks the wrist up. Press over the dorsum of the hand at the second metacarpal head and resist extension and abduction of the wrist. Stabilize with the other hand at the base of the forearm near the wrist

Extensor carpi ulnaris
•Posterior interosseous N.; C7, C8•Wrist extension and adduction•The patient cocks the wrist up. Press over the dorsum of the hand at the fifth metacarpal head and resist extension and adduction of the wrist. Stabilize with your other hand at the base of the forearm near the wrist.

Flexor carpi radialis
•Median N.; C6, C7•Wrist flexion and abduction•Hold the fingers of your hand against the upturned palmar aspect of the patient's second metacarpal head and resist wrist flexion and abduction, stabilizing at the dorsal forearm with your other hand. Observe the flexor tendon at the wrist

Flexor carpi ulnaris
•Ulnar N.; C7, C8, T1•Wrist flexion and adduction•Hold the fingers of your hand against the patient's upturned hand at the hypothenar eminence and resist wrist flexion and adduction, stabilizing at the dorsal forearm. Observe the tendon over the ulnar border of the wrist.

Flexor digitorum longus
•Median N; C7, C8, T1•Causes Finger flexion•Stabilize the patient's proximal phalanx between your thumb and finger and use a finger of your other hand to resist flexion of the proximal inter-phalangeal joint

Flexor digitorum profundus I, II
•Anterior interosseous N.; C7, C8•Finger flexion•Stabilize the patient's index middle phalanx between your thumb and finger and resist finger flexion by pulling against the flexed distal phalanx.

Flexor digitorum profundus III, IV
•Ulnar N.; C7, C8 •Finger flexion•As for Flexor digitorum profundus I, II, but with the patient's little finger

Flexor pollicis longus
•Anterior interosseous N.; C7, C8•Thumb flexion•The patient flexes the thumb at the inter-phalangeal joint. Press against the distal phalanx and resist flexion at this joint.

Abductor pollicis brevis
•Median N.; C8, T1•Thumb abduction•The patient holds the palm upward and brings his thumb away from his hand at 90° to the palm. Hold your thumb against the side of the patient's thumb and resist abduction. Observe the thenar eminence.

Opponens pollicis
•Median N•Opposition of the thumb•The patient should try to touch the tip of the little finger with the thumb, against your resistance.

First dorsal interosseous
•Ulnar N.; C8, T1•Index finger abduction•The patient holds the hand out palm downwards with the fingers apart. Hold your finger against the side of the index finger and resist abduction

Testing the grip
•C7, C8, T1•Ask the patient to squeeze two of your fingers as hard as possible and not let them go. You should normally have difficulty removing your fingers from the patient's grip. Test both grips simultaneously with arms extended or in the lap.

Lumbricals
•Lateral median and medial ulnar, C8, T1•Phalanges extension•Stabilize the patient's metacarpophalangeal joint in hyperextension by pressing your finger against the palmar surface of the middle phalanx so that the long extensors cannot act, and resist extension of the distal phalanx

Hip
Iliopsoas•Spinal branches and femoral N.; L1, L2, L3•Hip flexion•The patient flexes the thigh at the hip near 90°. Resist this by pressing on the anterior aspect of the thigh just proximal to the knee.

Gluteus maximus
•Inferior gluteal N.; L5, S1, S2•Hip extension•The patient lies supine with legs extended. Slightly flex the hip by placing your hand under the knee. Ask the patient to extend the hip to support the weight of the pelvis off the couch.

Hip adductors
•Oburator N.; L2, L3, L4•Hip adduction•The patient lies supine with legs extended. Resist adduction of the hip by pressing against the medial surface of the knee, stabilizing with your other hand against the side of the pelvis.

Gluteus medius and tensor fasciae latae
•Superior gluteal N.; L4, L5, S1•Hip abduction•The patient lies supine with legs extended. Resist abduction of the hip by pressing against the lateral surface of the knee, stabilizing with your hand against the opposite side of the pelvis.

Knee-Quadriceps
•Femoral N.; L2, L3, L4•Knee extension•The patient lies supine with legs extended. Use one hand to lift the patient's leg from underneath the knee to about 20°knee flexion and ask the patient to extend the knee, resisting with your other hand over the patient's lower shin.

Hamstrings
•Knee flexion•Sciatic N.; L5, S1, S2•The patient lies supine with the knee flexed at 90°. Hold the leg at the ankle and resist pulling of the heel in towards the buttock.

Ankle and foot
Gastrocnemius•Tibial N.; S1, S2•Ankle extension•The patient lies supine with legs extended and plantar-flexing the foot. Hold the foot at the metatarsal heads and resist plantar-flexion.

Tibialis anterior
•Deep peroneal N.; L4, L5•Ankle dorsiflexion•The patient lies supine with legs extended and the foot dorsi-flexed. Hold the foot over the dorsal surface and resist dorsi-flexion.

Tibialis posterior
•Tibial N.; L4, L5•Ankle inversion•Hold the patient's foot medially at the first metatarsal and resist inversion.

Peronei (longus and brevis)
•Superficial peroneal N.; L5, S1•Ankle eversion•Hold the patient's foot laterally at the fifth metatarsal and resist eversion

Extensor hallucis longus
•Deep peroneal N.; L5, S1•Great toe extension•The patient dorsiflexes the distal phalanx of the great toe. Press against the dorsal surface of the distal phalanx to resist dorsiflexion.

Extensor digitorum brevis
•Deep peroneal N.; L5, S1•Toe extension•The patient dorsiflexes the proximal phalanges of the toes and attempts to 'spread' the toes. Alternatively, press against the dorsal surfaces of the middle phalanges. Observe and palpate the muscle belly 4 cm distal to the lateral malleolus.

Flexor digitorum longus
•Tibial N.; L5, S1, S2•Toe flexion•Hold the patient's toes with your fingers over the plantar surfaces and resist flexion.

DEEP TENDON REFLEXES

General Instructions•Encourage the patient to relax, then position the limbs properly and symmetrically.•Hold the reflex hammer loosely between your thumb and index finger so that it swings freely in an arc within the limits set by your palm and other fingers.•With your wrist relaxed, strike the tendon briskly using a rapid wrist movement. Your strike should be quick and direct, not glancing.•Note the speed, force, and amplitude of the reflex response and grade the response using the scale below. Always compare the response of one side with the other.

Scale For Grading Reflexes

Reinforcement
•A technique involving isometric contraction of other muscles for up to 10 seconds that may increase reflex activity.•Tell the patient to pull just before you strike the tendon.


The Biceps Reflex (C5, C6)
•The patient's arm should be partially flexed at the elbow with palm down.• Place your thumb or finger firmly on the biceps tendon. •Strike with the reflex hammer so that the blow is aimed directly through your digit towards the tendon.•Observe flexion at the elbow, and watch for and feel the contraction of the biceps muscle.


The Triceps Reflex (C6, C7)
•The patient may be sitting or supine. Flex the patient's arm at the elbow, with palm toward the body, and pull it slightly across the chest.• Strike the triceps tendon above the elbow. Use a direct blow from directly behind it. •Watch for contraction of the triceps muscle and extension at the elbow.

If you have difficulty getting the patient to relax, try supporting the upper arm as illustrated. Ask the patient to let the arm go limp, as if it were “hung up to dry.” Then strike the triceps tendon.

The Supinator or Brachioradialis Reflex (C5, C6)
•The patient's hand should rest on the abdomen or the lap, with the forearm partly pronated.•Strike the radius with the point or flat edge of the reflex hammer, about 1 to 2 inches above the wrist.•Watch for flexion and supination of the forearm.

The Knee Reflex (L2, L3, L4)
•The patient may be either sitting or lying down as long as the knee is flexed.•Briskly tap the patellar tendon just below the patella.•Note contraction of the quadriceps with extension at the knee.


The Ankle Reflex (primarily S1)
•If the patient is sitting, dorsiflex the foot at the ankle. Persuade the patient to relax.•Strike the Achilles tendon.•Watch and feel for plantar flexion at the ankle. Note also the speed of relaxation after muscular contraction.


Ankle clonus
•Support the knee in a partly flexed position. With your other hand, dorsiflex and plantar flex the foot a few times while encouraging the patient to relax, and then sharply dorsiflex the foot and maintain it in dorsiflexion.Look and feel for rhythmic oscillations between dorsiflexion and plantar flexion.• In most normal people, the ankle does not react to this stimulus.

Superficial spinal reflexes

Abdominal Reflexes
•Lightly but briskly stroke each side of the abdomen, above (T8, T9, T10) and below (T10, T11, T12) the umbilicus.•Note the contraction of the abdominal muscles and deviation of the umbilicus toward the stimulus.

The plantar reflex (L5, S1)
•With an object such as a key or the wooden end of an applicator stick, stroke the lateral aspect of the sole from the heel to the ball of the foot, curving medially across the ball.•Note movement of the big toe, normally plantar flexion.•Babinski response: Instead of the normal flexor response, dorsiflexion of the great toe precedes all other movement. This is followed by spreading and extension of the other toes, by marked dorsiflexion of the ankle, and by flexion withdrawal of the hip and knee. It is pathognomonic of an UMN lesion.


Coordination
To assess coordination, observe the patient's performance in:
•Rapid alternating movements
•Point-to-point movements
•Gait and other related body movements
•Standing in specified ways

Rapid Alternating Movements
•Ask the patient to tap your palm with the tips of the fingers of one hand, alternately in pronation and supination, as fast as possible.•In cerebellar disease, one movement cannot be followed quickly by its opposite and movements are slow, irregular, and clumsy. This abnormality is called dysdiadochokinesis.

Point-to-Point MovementsFinger-to-nose Test
•Ask the patient to touch the point of the nose and then the tip of your finger, held at arm's length in front of the
patient's face, using their index finger.•Ask the patient to repeat the test with the eyes closed.

Heel-shin testAsk the patient to place one heel on the opposite knee, and then run it down the shin to the big toe. Note the smoothness and accuracy of the movements. Repetition with the patient's eyes closed tests for position sense. Repeat on the other side.

Gait
Ask the patient to:•Walk across the room or down the hall, then turn, and come back. Observe posture, balance, swinging of the arms, and movements of the legs.•Walk heel-to-toe in a straight line (tandem walking).•Walk on the toes, then on the heels•Hop in place on each foot in turn •Do a shallow knee bend, first on one leg, then on the other.•Rising from a sitting position without arm support and stepping up on a sturdy stool.

Tandem walking Hopping

Stance
The Romberg Test:This is mainly a test of position sense. The patient should first stand with feet together and eyes open and then close both eyes for 30 to 60 seconds without support. Note the patient's ability to maintain an upright posture. Normally only minimal swaying occurs.

Test For Pronator Drift
•The patient should stand for 20 to 30 seconds with both arms straight forward, palms up, and with eyes closed. A person who cannot stand may be tested for a pronator drift in the sitting position.•Now, instructing the patient to keep the arms up and eyes shut, tap the arms briskly downward. The arms normally return smoothly to the horizontal position.

Vibhushit Kaul
Acknowledgements:Dr. H.S. Pannu
26/4/2013