Embed Size (px)
Citation preview
Biochemistry Assignment
Name:Muhammad Ramzan Ul Rehman
Roll no:246
Metabolic Changes in Liver Failure
Carbohydrate Metabolism
The hepatocyte actively stores glucose by converting it to the longchain starch, glycogen. Glycogen can then be later broken down to release glucose into the general circulation. The factors that control thisinsulin, epinephrine, growth hormone (STH), glucagon and the thyroid hormonestend to counterbalance each other so that the hepatocytes store glycogen as the blood sugar rises and break it back down into glucose as blood sugar level falls. Again, this is a critical function, an impairment of which produces some of
the more serious manifestations of liver disease hyperglycemia and hypoglycemia. In fact, patients with severe liver disease often have glucose tolerance curves very much like those seen in diabetes mellitus. That is to say, with food ingestion, they tend to become hyperglycemic because the hepatocytes cannot store glycogen while, as dietary intake is decreased or absent, the hepatocytes are not well able to mobilize glucose from what little stored glycogen there is, and so these patients have episodes of hypoglycemia. This phenomenon is sometimes called "hepatic diabetes."
Defects in Lipid Metabolism
The liver has an extremely complex role in lipid metabolism, In the diseased liver, there are two prime manifestations of liver failure with regard to lipid metabolism.
The first of these is the deposition of triglycerides within the organ itself. This is the basic mechanism of socalled "fatty liver," which develops most often as a result of chronic alcoholism.
The second prime feature of disordered hepatic lipid metabolism is a diminution in the rate of synthesis of cholesterol. In fact, a decrease below the normal level of serum cholesterol is often found in advanced diffuse liver disease or in severe acute liver disease.
Defects in Amino Acid Metabolism
Amino acids are delivered to the liver either from the gut or from the general circulation. In the liver there are two major processes in the metabolism of amino acids:
oxydative deamination
transamination.
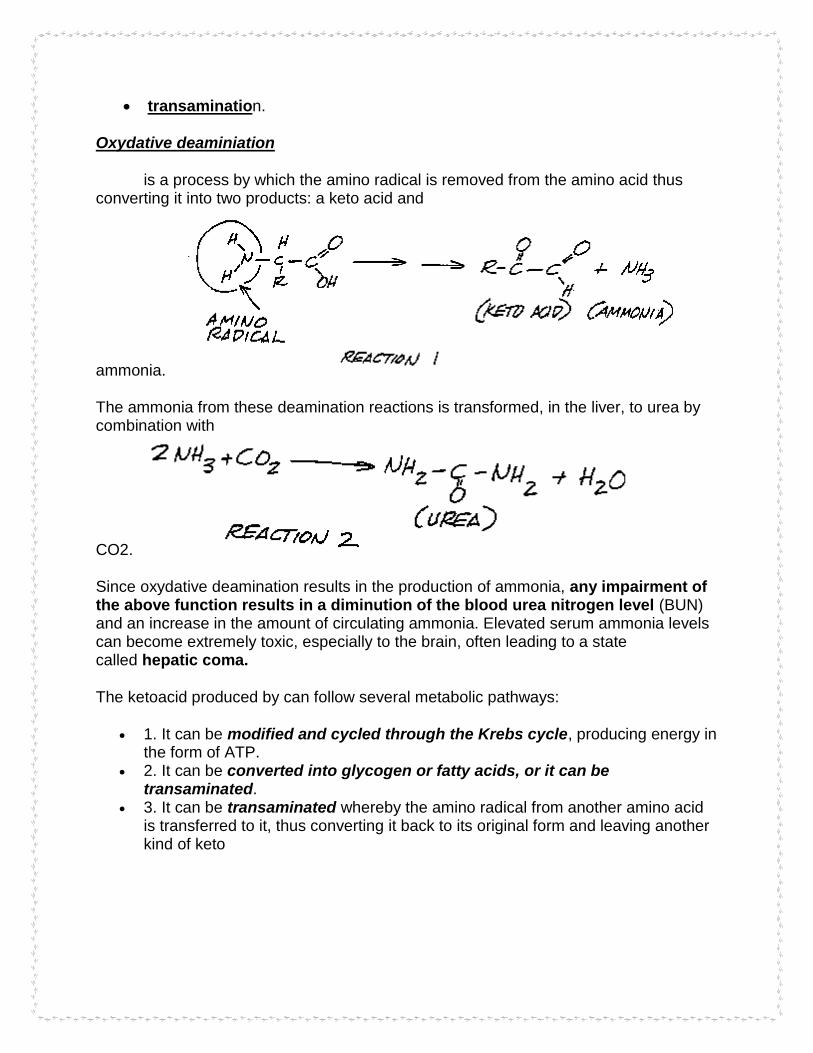
Oxydative deaminiation
is a process by which the amino radical is removed from the amino acid thus converting it into two products: a keto acid and
ammonia.
The ammonia from these deamination reactions is transformed, in the liver, to urea by combination with
CO2.
Since oxydative deamination results in the production of ammonia, any impairment of the above function results in a diminution of the blood urea nitrogen level (BUN) and an increase in the amount of circulating ammonia. Elevated serum ammonia levels can become extremely toxic, especially to the brain, often leading to a state called hepatic coma.
The ketoacid produced by can follow several metabolic pathways:
1. It can be modified and cycled through the Krebs cycle, producing energy in the form of ATP.
2. It can be converted into glycogen or fatty acids, or it can be transaminated.
3. It can be transaminated whereby the amino radical from another amino acid is transferred to it, thus converting it back to its original form and leaving another kind of keto

acid which itself can then undergo any of the above three steps.
in severe acute hepatitis of any form, this particular hepatocyte failure results in a severe derangement of amino acid metabolism and thus of ammonia and urea levels.
Defects in Protein Synthesis
Two of the liver's cell types, are responsible for synthesizing many kinds of proteins.
o the hepatocyte o the Kupffer cell,
The hepatocyte o synthesizes albumin and some immune globulins.
The Kupffer cells, o which line the hepatic sinusoids, and which are a part of the socalled
reticuloendothelial system, synthesize several kinds of immune globulins.
the functions of both of these kinds of cells can be impaired in either chronic diffuse liver disease or in severe acute liver disease, a diminution of the levels of circulating albumin and of the immune globulins often appears in liver

disease.
Metabolic Changes in Renal Failure
Carbohydrate metabolism
non-diabetic Renal Failure patients often also have glucose intolerance because of peripheral insulin resistance. Reduced insulin-mediated
non-oxidative glucose disposal is the most evident defect of glucose metabolism.
Insulin resistance may be related to arterial hypertension and may contribute to high cardiovascular morbidity and mortality in patients with CKF
Lipid metabolism
Serum triglycerides (TG) are elevated in Renal Failure
because of o enhanced production of TG-rich lipoproteins such as very-low-
density lipoproteins (VLDL) in the liver.

o dysfunction of TG degradation resulting from insufficient mitochondrial betaoxidation of fatty acids
low levels of high-densitylipoprotein (HDL) cholesterol. Low-density lipoprotein (LDL) cholesterol levels are often normal
Cause oxidative stress and insulin resistance may mediate the lipid-induced renal damage
Protein metabolism
Disorders in protein metabolism in the dialysis period are usually caused by
combined (protein and energy) malnutrition that can be termed uremic malnutrition
o It is characterized by insidious loss of somatic protein stores (reflected in lean body mass and serum creatinine) and visceral protein concentrations (reflected in serum albumin and prealbumin concentrations)
Urinary losses of protein and losses of amino acid. Metabolic acidosis is an important factor that markedly contributes to
negative nitrogen and total body protein balance in Renal Failure
Metabolic Changes in Ischemic Heart Disease.
Carbohydrate metabolism
Modest fall in coronary flow (mild ischemia) increases glucose uptake, more major fall (severe ischemia) decreases uptake.
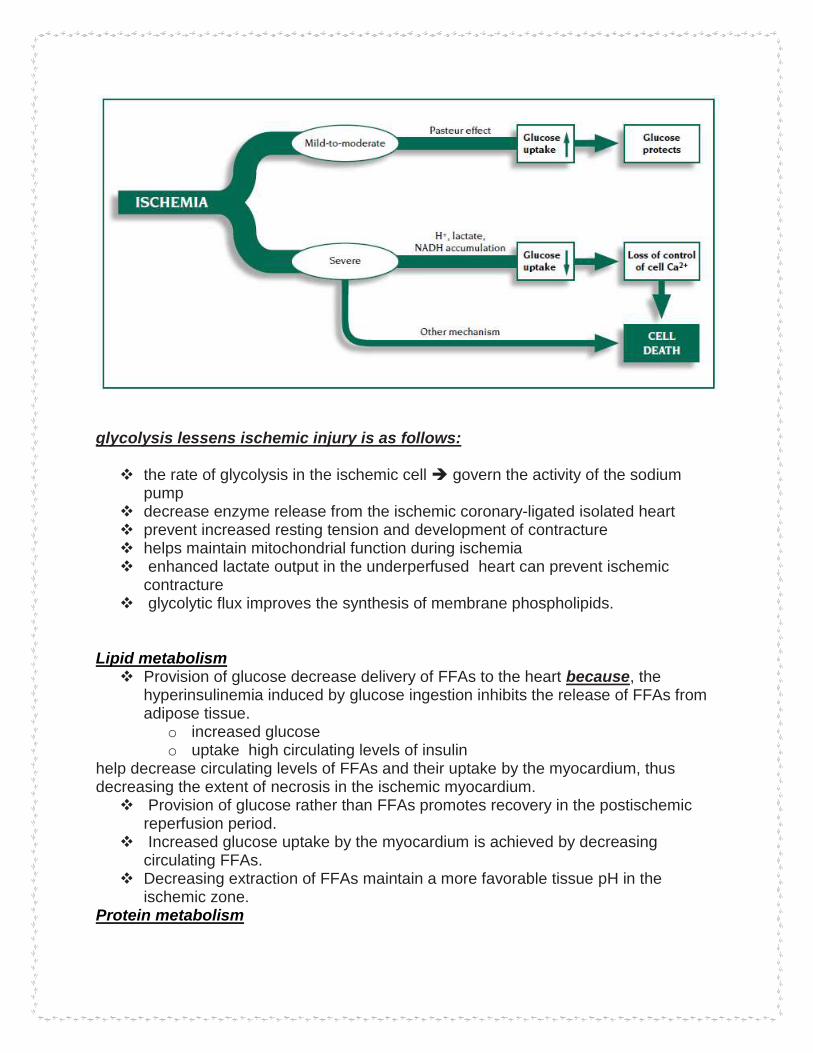
glycolysis lessens ischemic injury is as follows: the rate of glycolysis in the ischemic cell govern the activity of the sodium
pump decrease enzyme release from the ischemic coronary-ligated isolated heart prevent increased resting tension and development of contracture helps maintain mitochondrial function during ischemia enhanced lactate output in the underperfused heart can prevent ischemic
contracture glycolytic flux improves the synthesis of membrane phospholipids.
Lipid metabolism Provision of glucose decrease delivery of FFAs to the heart because, the
hyperinsulinemia induced by glucose ingestion inhibits the release of FFAs from adipose tissue.
o increased glucose o uptake high circulating levels of insulin
help decrease circulating levels of FFAs and their uptake by the myocardium, thus decreasing the extent of necrosis in the ischemic myocardium. Provision of glucose rather than FFAs promotes recovery in the postischemic
reperfusion period. Increased glucose uptake by the myocardium is achieved by decreasing
circulating FFAs. Decreasing extraction of FFAs maintain a more favorable tissue pH in the
ischemic zone. Protein metabolism

The effect on protein turnover and on the myocardial balance of amino acids and branched chain ketoacids (BCKA) in these patients were
o Net release of phenylalanine reflecting protein degradation o Net myocardial protein catabolism. o Protein synthesis increased to equal the degradation rate o The phenylalanine balance shifted from negative to neutral o The myocardial uptake of both BCAA and their ketoacid conjugates was
increased. o Net uptake of the BCAA greatly exceeded that of other essential amino
acids.
Metabolic Changes in Edema and Dehydration.
Edema Effects
Metabolic changes that occurs in edema are :
1. increased hydrostatic pressure;
2. reduced oncotic pressure within blood vessels;
3. increased tissue oncotic pressure;
4. increased blood vessel wall permeability e.g. inflammation;
5. obstruction of fluid clearance in the lymphatic system;
6. changes in the water retaining properties of the tissues themselves. Raised
hydrostatic pressure often reflects retention of water and sodium by the kidney
Dehydration Effects
During dehydration organ water content was defended with no change in water content in skeletal muscle
Dehydration stimulated a rapid and massive increase in liver glucose production. liver glucose rise also in other organs increased Glucose synthesis was supported by glycogenolysis in liver. Liver energy status (ATP, total adenylates, energy charge) was maintained even
after the loss of 35% of total body water but at 50% dehydration all parameters showed a sharp decline;
for example, o energy charge fall
accumulation of lactate in four organs, probably hypoxia-induced the to impaired circulation.
Standard Medical Education.
Definition 'Standard' refers to "something set up and established by authority, custom or general consent as a model, example or rule for the measure of quantity, weight, extent, value, or quality". The function of any standard is a transmission of information from those who have
the knowledge to those who need and can use that knowledge. In the educational system, standards tell students what is expected of them to succeed in the College and professional life.
Criteria for Slandered Medical Education Only general aspects of medical education and training should be covered. Standards should be concerned with broad categories of the content, process,
educational environment and outcome of postgraduate medical education. Standards should function as a lever for change and reform. Standards are intended not only to set minimal global requirements but also to
encourage quality development beyond the levels specified. Standards should be formulated in such a way that, in addition to respecting
global core requirements, they will acknowledge necessary regional and national differences in the educational programme, and allow for different local, national and regional profiles and developments.
Standards should recognise the dynamic nature of programme development.Standards are formulated as a tool which authorities, organisations and institutions responsible for postgraduate medical education can use as a basis and a model for their own programme development. The value of the standards must be tested in evaluation studies in each.Standards must be clearly defined, and be meaningful,
Present Status of Medical Education
In the past few years medical education has undergone considerable change,
particularly at the graduate and postgraduate levels

Things that can be done to improve present status of Medical Education There is an urgent need for the profession as whole and the faculties of medical colleges in particular to develop a consensus on: (i) Outcomes that will prepare graduates to meet the growing challenges posed to health profession globally and locally. (ii) Deriving learning objectives that lead towards achieving the desired outcomes. (iii) Accepting the challenge of exponential growth of information by designing a curriculum based on integration of basic and clinical sciences. (iv) A curriculum that focuses on health promotion and preventive aspects (v) Student-centered learning methods that are based on adult learning theory and will produce life long learners. (vi) Adequate and balanced training of medical students in primary, secondary and tertiary care settings. (vii) Training students for holistic care that focus on continuity of care to individuals and families in primary care settings. (viii) Creating a conducive environment that will foster life long self- learning skills. (ix) Fostering empathy and ethical values.
How to Know
The Slandered medical education not only involves the educationing but also the learning of the behavior how to deal with patients The Concepts of A medical students, the command over the diagnosis and other factors reported by patients that tells about slandered medical Education are
Confident: "The doctor's confidence gives me confidence." Empathetic: "The doctor tries to understand what I am feeling and experiencing,
physically and emotionally, and communicates that understanding to me." Humane: "The doctor is caring, compassionate, and kind." Personal: "The doctor is interested in me more than just as a patient, interacts with me,
and remembers me as an individual." Forthright: "The doctor tells me what I need to know in plain language and in a forthright
manner." Respectful: "The doctor takes my input seriously and works with me." Thorough: "The doctor is conscientious and persistent."
Standards The Standards for Medical Education are divided into core values of medical educators and five domains.

Learning and teaching principles Make shure that
Student Is aware of different ways of learning and teaching Student Is aware of the need to define what is to be learned Student Is aware of a range of learning methods, experiences and resources and how they may be used effectively Student Responds appropriately to feedback and evaluation of educational interventions
learning and teaching principles in the design of a unit, module or subject area
Matches course design to support different ways of learning and teaching
Gathers and interprets basic information on the needs of learners
Constructs appropriate learning outcomes that can be measured or judged
Matches learning methods,experiences and resources to intended outcomes Develops learning resources for planned courses
Evaluates and improves educational interventions

Future Professional Goal Career goals are goals that you set for your career path. They can be anything from your career choice to where you want to be in your career in a certain number of years. A career defines how you want to spend a large part of your life, so career goal setting is something that everyone should be doing regardless of what career they choose. Targets
The competent, effective, and compassionate care of patients and the advancement of knowledge about disease, its prevention and treatment require that physicians in training be introduced to a lifelong educational process in the practice of medicine.
Basis to Slect Goal
1. What is your Motivation to Pursue a Healthcare Career? 2. How are You Going to Obtain the Education and Training Needed for Your Career? 3. Are your Skills and Strengths a Fit for the Healthcare Industry? 4. What Specific Role within the Healthcare Field is Most Suitable for You? 5. Where Do You Want to Work? 6. How Will Your Healthcare Career Impact Your Family and Personal Life Long-term? **********************************************************************
![Research Paper EBV(LMP1)-induced metabolic …EBV(LMP1) changes the cellular metabolic profile and plays an important part in cancer cell metabolic reprogramming [13, 16, 17]. Therefore,](https://img.dokumen.tips/doc/110x75/60dd05f4ec70eb601e176813/research-paper-ebvlmp1-induced-metabolic-ebvlmp1-changes-the-cellular-metabolic.jpg)










![Metabolic Changes of Phomopsis longicolla Fermentation … Metabolic Changes of Phomopsis longicolla Fermentation and Its Effect on ... [12]. In the last few ... PLS-DA extracts as](https://img.dokumen.tips/doc/110x75/5b6e00b07f8b9a3b388db09e/metabolic-changes-of-phomopsis-longicolla-fermentation-metabolic-changes-of-phomopsis.jpg)

















