Embed Size (px)
Citation preview

Welcome

INTRODUCTION TO PATHOLOGY.JOMIN GEORGE
LECTURER
FACULTY OF HEALTH INFORMATION MANAGEMENT
Email: [email protected]

• Learning Objectives
• Upon completing this chapter students should be able to:
• 1. Define pathology and branches
• 2. Know the diagnostic techniques used in pathology
• 3.Discuss the core aspects of disease in pathology

What is Pathology?
• Pathology is the study of disease by scientific methods.
• The word pathology came from the Latin words “patho” & “logy”.
• ‘Patho’ means disease and ‘logy’ means study, therefore pathology is a scientific study of disease.
• It focuses on the structural, biochemical, and functional changes in cells, tissues, and organs in disease.
Branches of pathology
• General Pathology
• Systemic pathology.
• General pathology is concerned with the basic reactions of cells and tissues to abnormal stimuli that underlie all diseases.
• Systemic (organ and organ system) pathology examines the specific responses of specialized organs and tissues to more or less well-defined stimuli.

Techniques
• Explain the whys and wherefores of the signs and symptomsMicrobiologicMolecular
Immunologic Morphologic
Is it your Fault ?? Getting Sick
• The patient's own fault (for having sinned) or the effects of outside agents, such as bad smells, cold, evil spirits,
• two major classes of etiologic factors:
• Genetic and Acquired

Disease process
Etiology
Pathogenesis
Clinical manifestations
Molecular and morphologic changes
EP MC
Etiology
• Etiology of a disease means the cause of the disease. If the cause of a disease is known it is called
• primary etiology.
• If the cause of the disease is unknown it is called• idiopathic.
• There are two major classes of etiologic factors: Genetic and Acquired (infectious, nutritional, chemical, physical, etc).

Pathogenesis
• Pathogenesis means the mechanism through which the cause operates to produce the pathological and clinical manifestations or structural and functional abnormalities.
The incubation period, the time between exposure to the virus and the appearance of symptoms.
Morphologic Changes.
• The morphologic changes refer to the structural alterations in cells or tissues that occur following the pathogenetic mechanisms.
• The structural changes in the organ can be seen with the naked eye or they may only be seen under the microscope.
• GROSS MORPHOLOGIC CHANGES & MICROSCOPIC CHANGES.
Clinical Manifestations.
• The morphologic changes in the organ influence the normal function of the organ.
• By doing so, they determine the clinical features (symptoms and signs), course, and prognosis of the disease.
• In summary, pathology studies:-
Cellular responseto stress and toxins:

Cell Injury & Cell Death

Objectives
• Upon completion of this lecture you will be able to:
• be a guide to cell injury and cell death• Explain the difference between reversible and irreversible cell injury.
• List 7 common causes of cell injury.
• describe the morphological changes of cell injury/death
• Explain the difference between necrosis and apoptosis.
• Describe patterns of necrosis In tissues or organs.

Cell Injury.
• If the cells fail to adapt under stress,
they undergo certain changes called
cell injury.
Reversible and irreversible cell injury
• The affected cells may recover from the injury (reversible) or may die (irreversible).
Adapt or die!

Objectives
• Upon completion of this lecture you will be able to:
• be a guide to cell injury and cell death• Explain the difference between reversible and irreversible cell injury.
• List 7 common causes of cell injury.
• describe the morphological changes of cell injury/death• Explain the difference between necrosis and apoptosis.
• Describe patterns of necrosis In tissues or organs.
Causes of cell Injury
Cell Injury Acquired
Genetic

Physical Agents
O2 Deprivatio
n
Chemical Agents
Infectious
Genetic Derangements
Immunologic
reactions
Genetic
Developmental
Cytogenetic
Single gene
Acquired Causes
Nutritional imbalance

O2 Deprivation
• Hypoxia is a deficiency of oxygen, which causes cell injury by reducing aerobic oxidative respiration.
• Hypoxia is an extremely important and common cause of cell injury and cell death.
• Causes of hypoxia include reduced blood flow (celled ischemia)
• Inadequate oxygenation
due to cardiorespiratory failure.
decreased oxygen-carrying capacity of the blood
as in anemia after severe blood loss

Physical Agents.
• Physical agents capable of causing cell injury include
mechanical trauma extremes of temperature radiation

Chemical Agents and Drugs.
• Poisons, such as arsenic, cyanide, or mercuric salts, may destroy sufficient numbers of cells within minutes or hours to cause death.
• Other potentially injurious substances as air pollutants, insecticides, and herbicides; industrial and occupational hazards, such as carbon monoxide and asbestos.
• Drugs ,alcohol and the ever-increasing variety of therapeutic drugs.

Infectious Agents.
• The rickettsiae, bacteria, fungi, and higher forms of parasites.

Immunologic Reactions.
1.Autoimmunity 2.Hypersensitivity
Alopecia areata

Genetic Derangements.
• Disease may result from
abnormal mutated genes
or chromosomal
abnormalities.
46

Nutritional Imbalances.
•Nutritional Deficiencies
•Nutritional excesses
• In summary, cell injury:-

Morphologic Alterations in Cell Injury
• Swelling of the cell and its organelles
• Blebbing of the plasma membrane
• Detachment of ribosomes from the
ER
• Clumping of nuclear chromatin.
• Loss of cell membrane integrity,
defects in protein synthesis,
cytoskeletal Damage
• DNA damage.
Reversible cell injury
Cellular swelling
Acute and mid
Fatty changes
Hypoxia
Fatty liver

Cell Death
For every cell, there is a time to live and a time to die.
How many times you die?

Clinical & biologic death
• Clinical death is the reversible transmission
between life and biologic death. Clinical
death is defined as the period of respiratory,
circulatory and brain arrest during which
initiation of resuscitation can lead to
recovery.

• Signs indicating clinical death are
• The patient is without pulse or blood pressure and is completely unresponsive to
the most painful stimulus.
• The pupils are widely dilated
• Some reflex reactions to external stimulation are preserved. For example, during
intubations, respiration may be restored in response to stimulation of the
receptors of the superior laryngeal nerve, the nucleus of which is located in the
medulla oblongata near the respiratory center.
• Recovery can occur with resuscitation.

Biological Death
• Biological death (sure sign of death), which sets in after clinical death,
is an irreversible state of cellular destruction.
• It manifests with irreversible cessation of circulatory and respiratory
functions, or irreversible cessation of all functions of the entire brain,
including brain stem.

Irreversible cell injury
Persistent or excessive injury“point of no
return”
Necrosis Apoptosis
NecrosisNecrosis = Death / premature death of cells in living tissue.
In necrosis, excess fluid enters the cell, swells it, & ruptures its membrane which kills it. After the cell has died, intracellular degradative reactions occur within a living organism.
Narcosis???

• In an average adult human, between 50 billion and 70 billion cells die
off and are replaced every day, but necrosis refers to cell death that is
unprogrammed and results from atypical body conditions,
such as infections, cancer, serious injury, the presence of venom,
severe inflammation, and a variety of diseases.
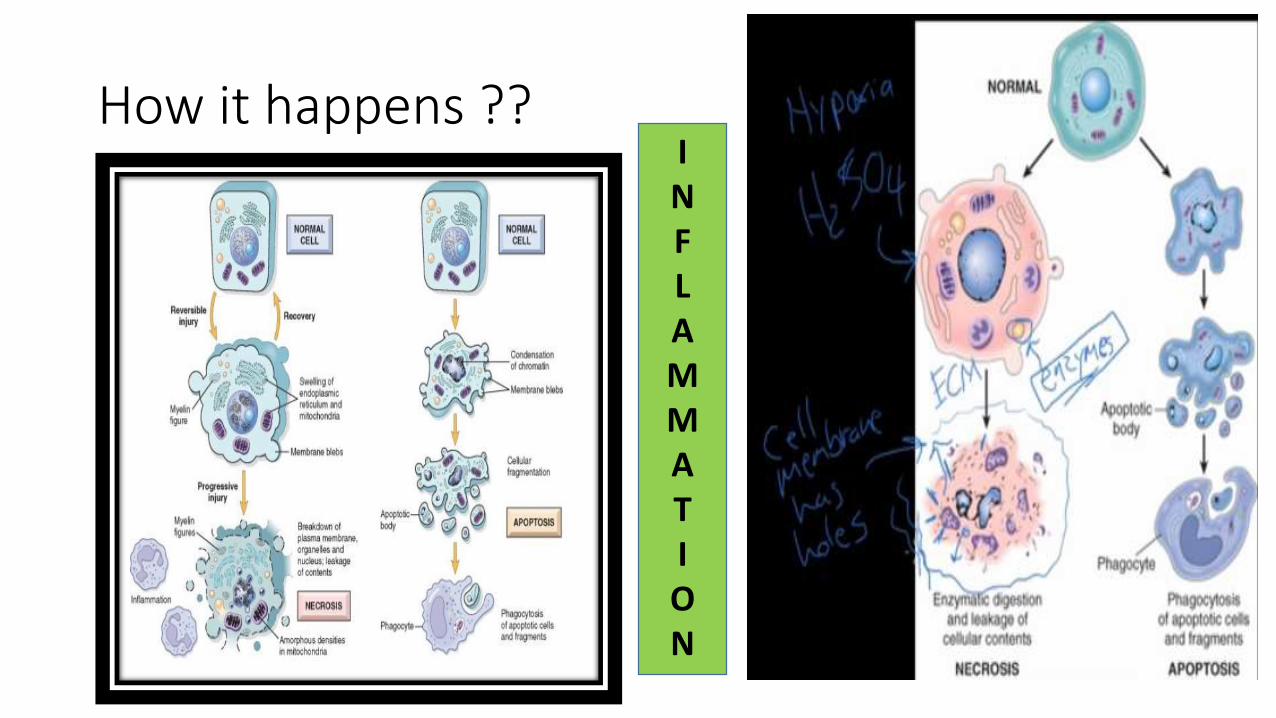
How it happens ??INFLAMMATION
Necrosisdoes not occur in dead organisms. In dead organisms, autolysis & heterolysis take place
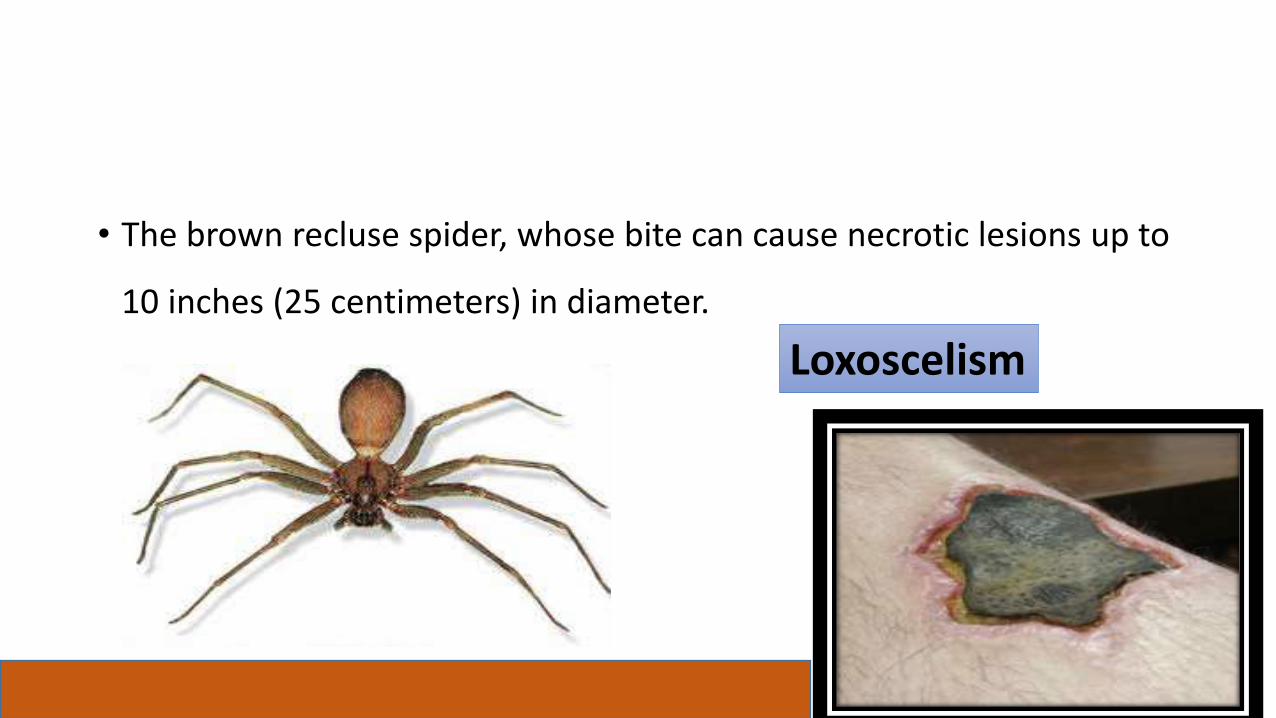
• The brown recluse spider, whose bite can cause necrotic lesions up to
10 inches (25 centimeters) in diameter.
Loxoscelism

Morphology changes
• Necrotic cells show increased eosinophilia.
• Have a more glassy homogeneous appearance than do normal cells,
mainly as a result of the loss of glycogen particles.
• the cytoplasm becomes vacuolated and appears moth-eaten.
• Dead cells may be replaced by large, myelin figures.
• the dead cells may ultimately become calcified.

Types of necrosis
• The types of necrosis include:
1. Coagulative necrosis
2. Liquefactive necrosis
3. Fat necrosis
4. Caseous necrosis
5. Gangrenous necrosis
Morphological patterns of Necrosis
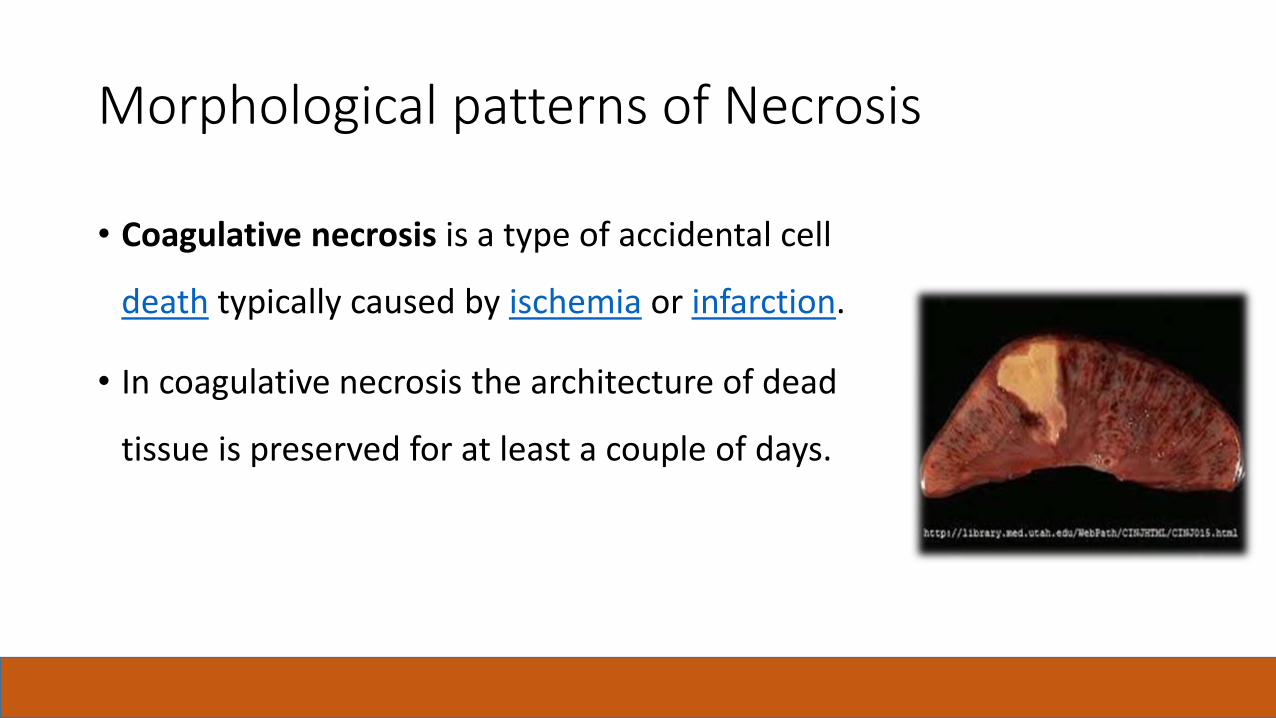
• Coagulative necrosis is a type of accidental cell
death typically caused by ischemia or infarction.
• In coagulative necrosis the architecture of dead
tissue is preserved for at least a couple of days.

• A localized area of coagulative necrosis is called an infarct.

Liquefactive necrosis
• Liquefactive necrosis (or colliquative necrosis) is a type of necrosis which results
in a transformation of the tissue into a liquid viscous mass..
• It is seen in focal bacterial or, occasionally, fungal infections.
• The necrotic material is frequently creamy yellow because of the presence of
dead leukocytes and is called pus.
• For unknown reasons, hypoxic death of cells within the central nervous system
often manifests as liquefactive necrosis
Gangrenous necrosis
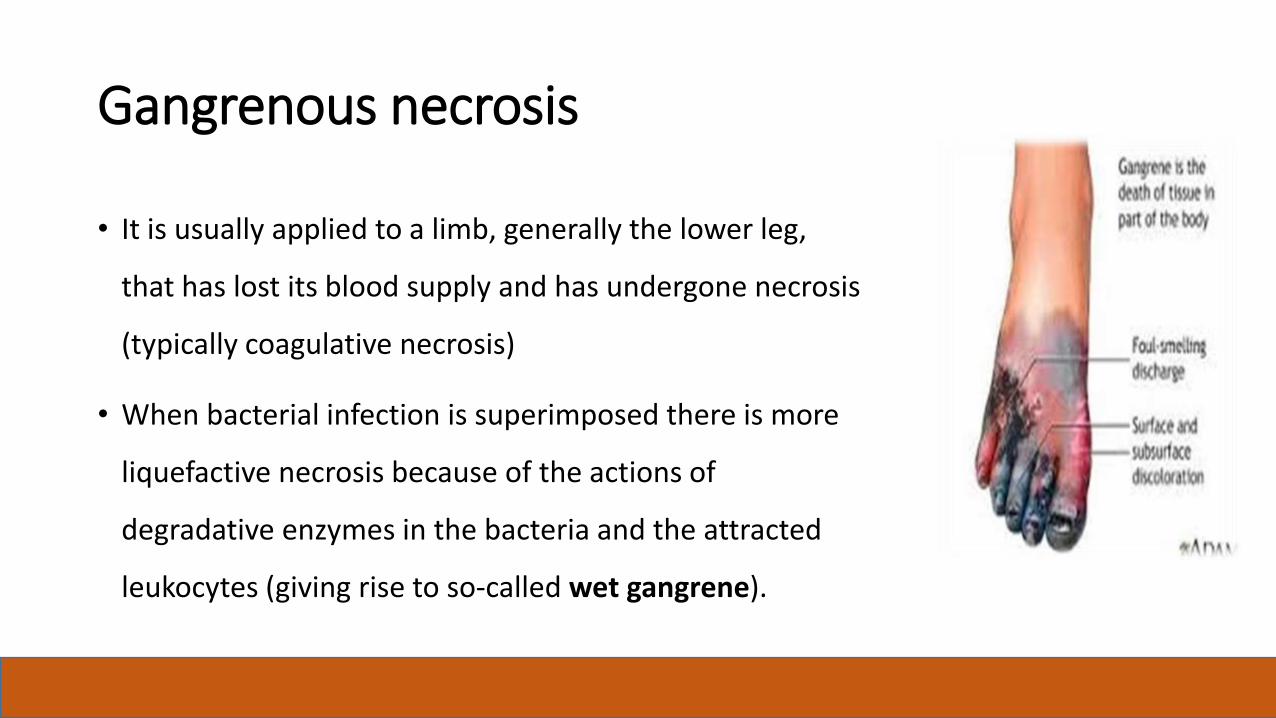
• It is usually applied to a limb, generally the lower leg,
that has lost its blood supply and has undergone necrosis
(typically coagulative necrosis)
• When bacterial infection is superimposed there is more
liquefactive necrosis because of the actions of
degradative enzymes in the bacteria and the attracted
leukocytes (giving rise to so-called wet gangrene).
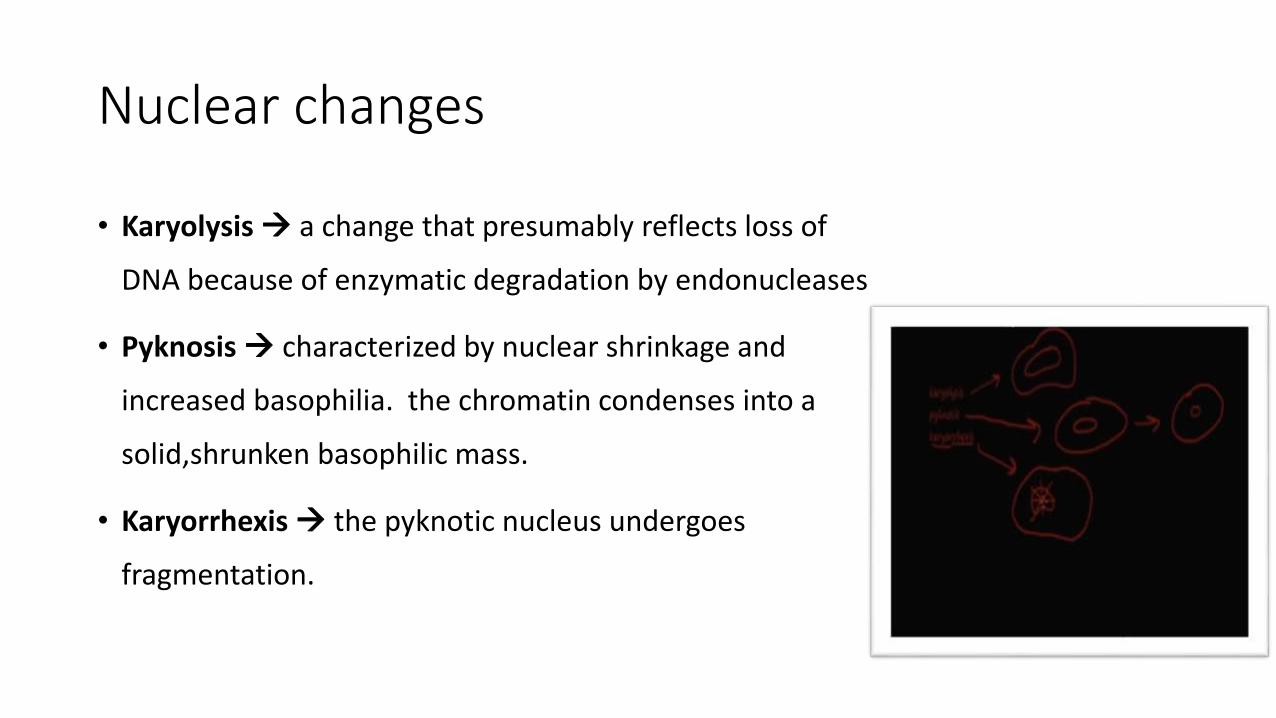
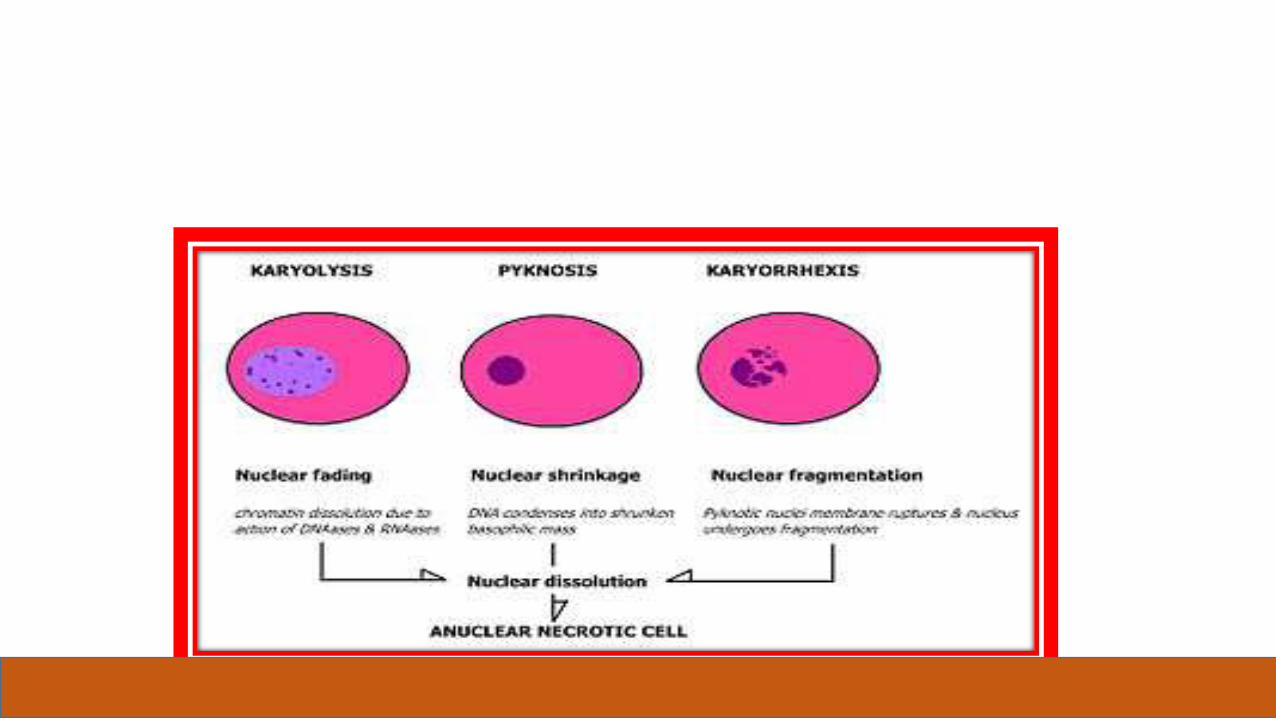
Nuclear changes
• Karyolysis a change that presumably reflects loss of
DNA because of enzymatic degradation by endonucleases
• Pyknosis characterized by nuclear shrinkage and
increased basophilia. the chromatin condenses into a
solid,shrunken basophilic mass.
• Karyorrhexis the pyknotic nucleus undergoes
fragmentation.

Apoptosis
• It is type of cell death which helps to
eliminate unwanted cells--an internally
SUICIDE PROGRAM series of events
effected by dedicated gene products
• Apoptosis is the death of single cells
within clusters of other cells.
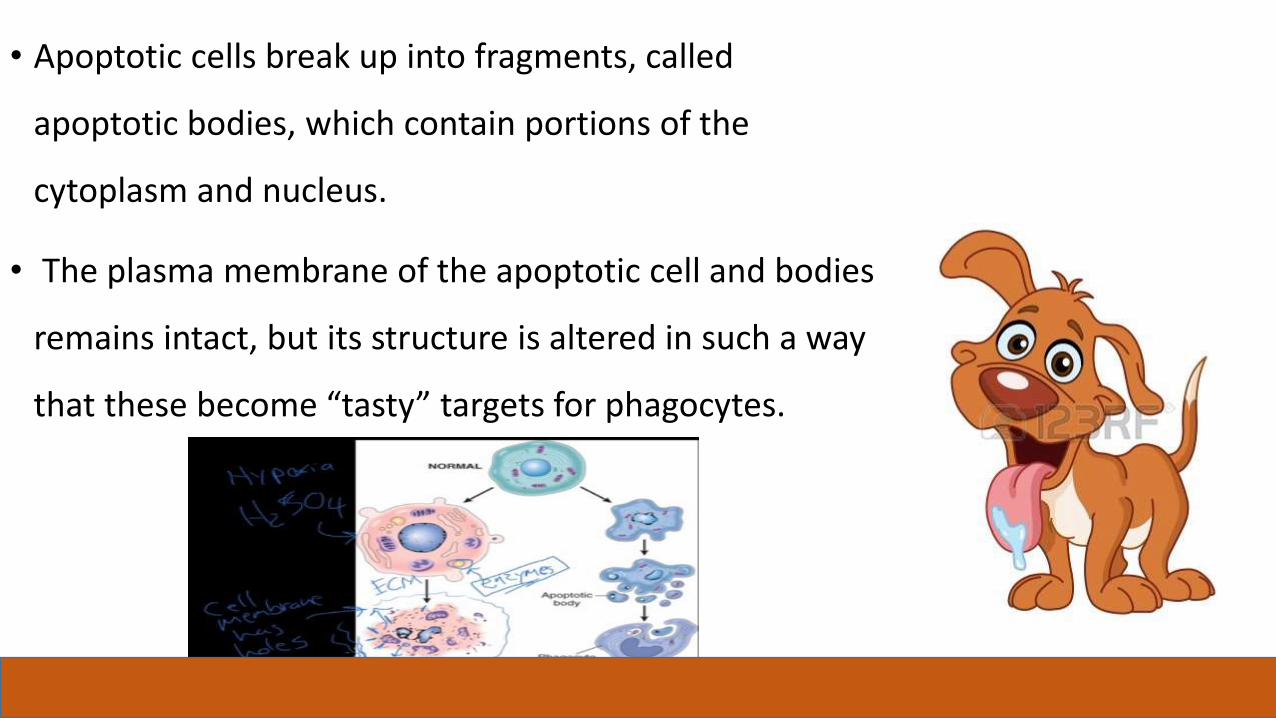
• Apoptotic cells break up into fragments, called
apoptotic bodies, which contain portions of the
cytoplasm and nucleus.
• The plasma membrane of the apoptotic cell and bodies
remains intact, but its structure is altered in such a way
that these become “tasty” targets for phagocytes.
• When a cell is compelled to commit suicide , proteins called
caspases go into action. They break down the cellular
components needed for survival.

• Apoptosis is not followed by inflammation or calcification.
•Examples: The resorption of the tadpole tail at
the time of its metamorphosis into a frog
occurs by apoptosis.
•The formation of the fingers and toes of the
fetus requires the removal, by apoptosis, of the
tissue between them.
•The sloughing off of the inner lining of the
uterus (the endometrium) at the start of
menstruation occurs by apoptosis
CAUSES OF APOPTOSIS
Apoptosis occurs normally both during development and throughout
adulthood, and serves to eliminate unwanted, aged or potentially harmful
cells. It is also a pathologic event when diseased cells become damaged
beyond repair and are eliminated.
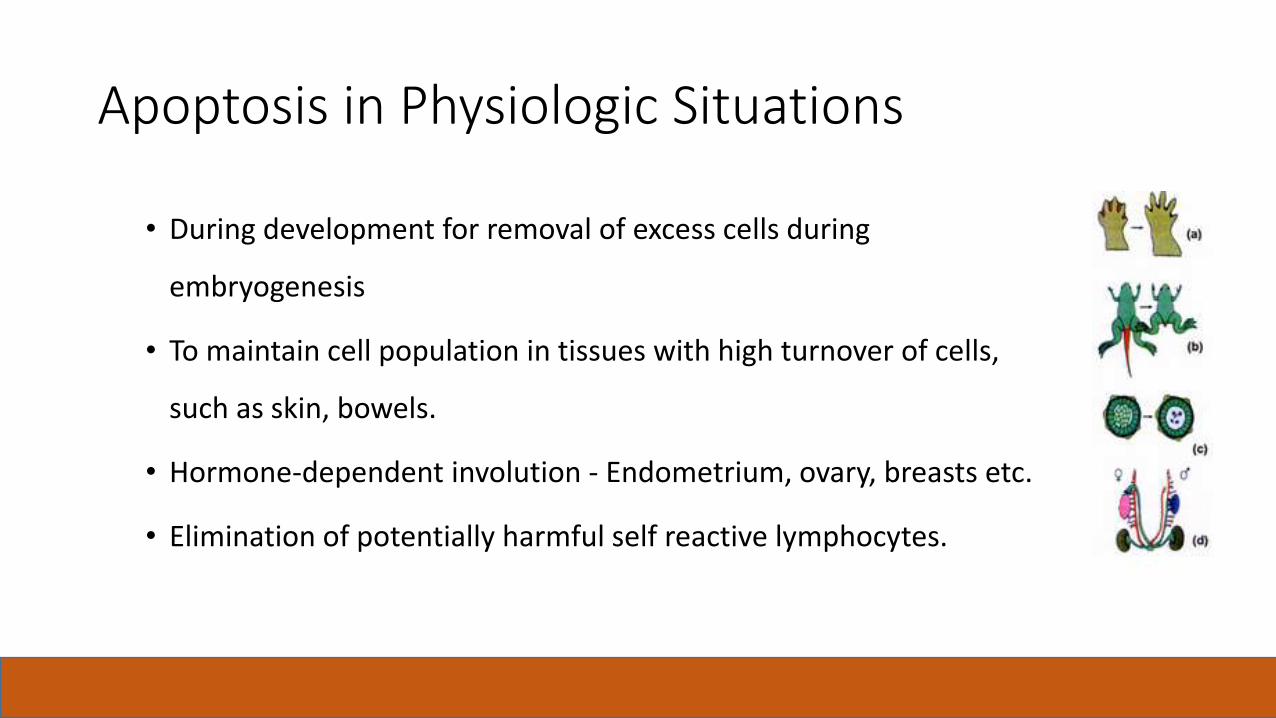
Apoptosis in Physiologic Situations
• During development for removal of excess cells during
embryogenesis
• To maintain cell population in tissues with high turnover of cells,
such as skin, bowels.
• Hormone-dependent involution - Endometrium, ovary, breasts etc.
• Elimination of potentially harmful self reactive lymphocytes.

• To remove damaged cells by virus
• To eliminate cells with DNA damage by radiation, cytotoxic agents etc.
• Cell death in tumours
Apoptosis in Pathologic Situations

Features of Necrosis and Apoptosis
• Table – 12 . Refer it.
• In summary, cell Death:-
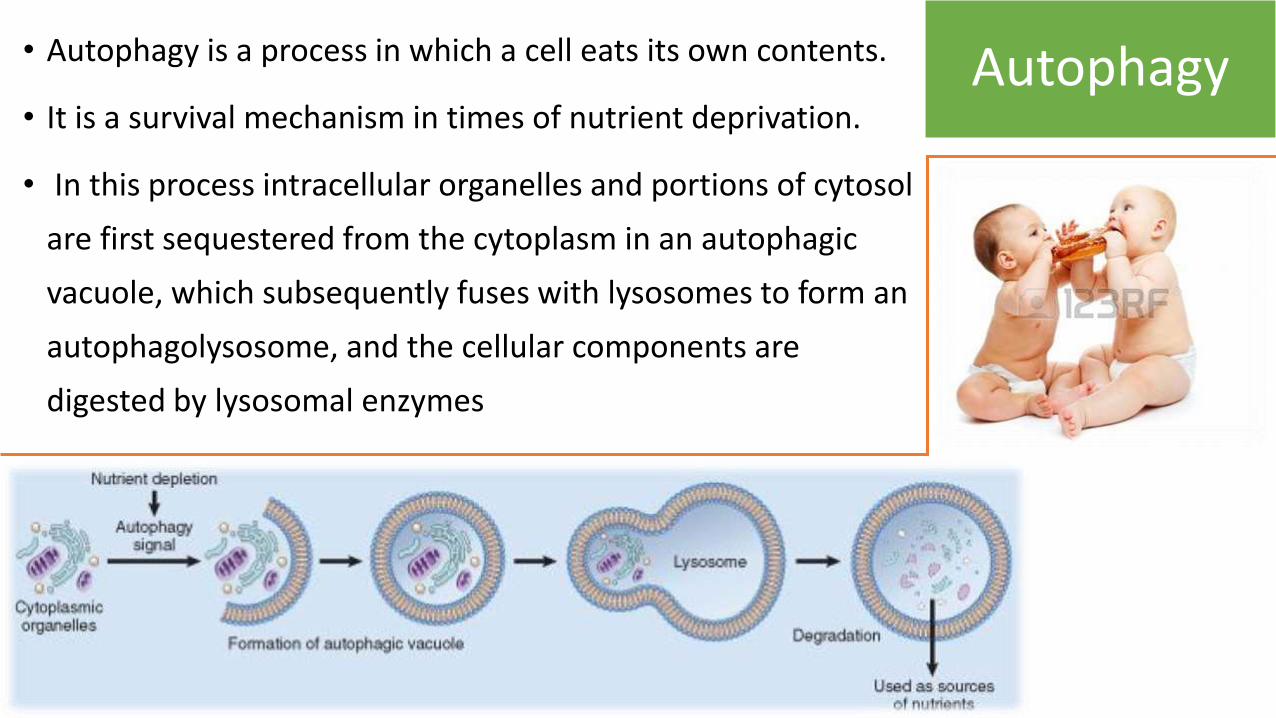
Autophagy• Autophagy is a process in which a cell eats its own contents.
• It is a survival mechanism in times of nutrient deprivation.
• In this process intracellular organelles and portions of cytosol
are first sequestered from the cytoplasm in an autophagic
vacuole, which subsequently fuses with lysosomes to form an
autophagolysosome, and the cellular components are
digested by lysosomal enzymes

Intracellular Accumulations
DEFINITION:
Accumulation of abnormal amounts of various substances due to manifestations of metabolic derangements in the cell.
• CATEGORIES:
• 1. Normal cellular constituents
e.g., water, lipids, CHO.
2. Abnormal substances
a) Exogenous Substance accumulate because the cell can neither
degrade the substance nor the ability to transport it to other sites.
e.g., mineral or products of infectious agents
• b) Endogenous Substance that cannot be metabolized because of
deficiency or defect of the enzyme and accumulate in cells.
e.g., products of abnormal synthesis or metabolism
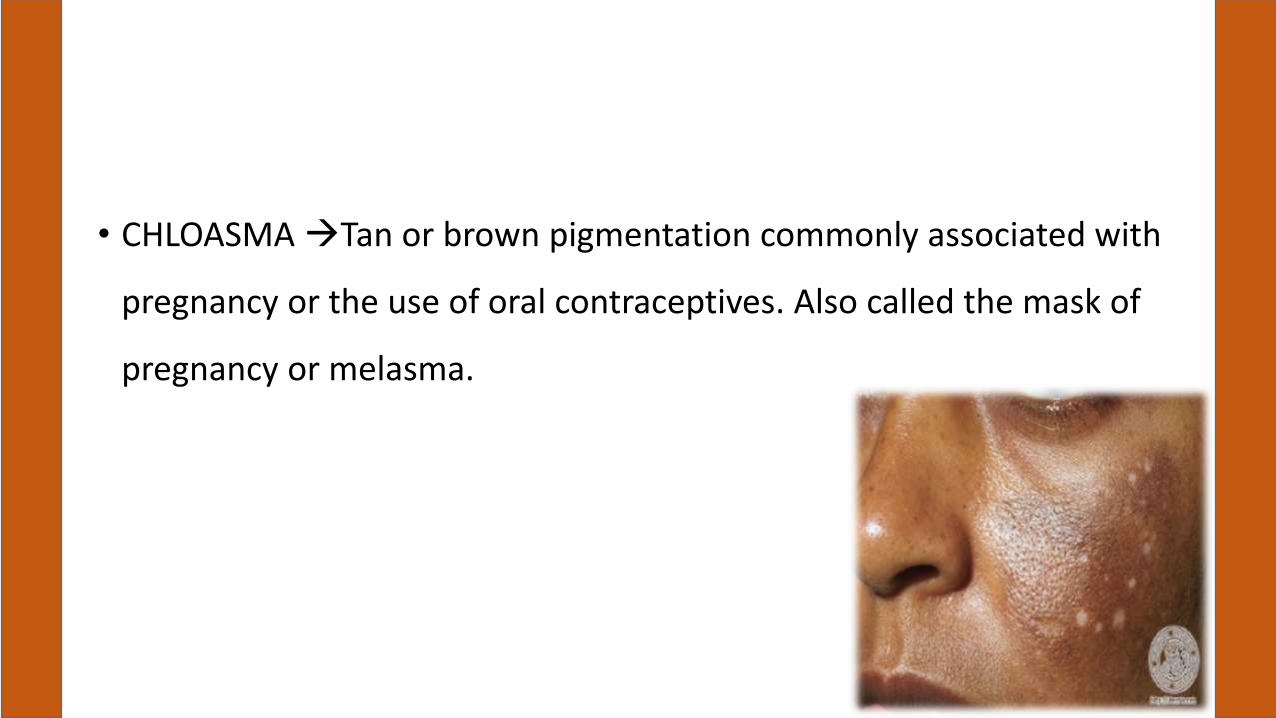
• CHLOASMA Tan or brown pigmentation commonly associated with
pregnancy or the use of oral contraceptives. Also called the mask of
pregnancy or melasma.


Steatosis ( Fatty Changes)
• The terms steatosis and fatty change describe abnormal accumulations
of triglycerides within parenchymal cells.

Organs Involved & Causes
• Fatty change is often seen in the liver because it is the major organ
involved in fat metabolism, but it also occurs in heart, muscle, and kidney.
• Disorder with heoatocyte damage.
• The causes of steatosis include toxins, protein malnutrition, alcohol and
anoxia
• Disorder with Hyperlipidemia.
• diabetes mellitus and obesity.
Assignment.
• proteins, Glycogen, Pigments ,Hyaline Change
• Endogenous and Exogenous Constituents





























