Embed Size (px)
Citation preview
Radiotherapy Techniques In Carcinoma Cervix
Presented by : Dr. Isha JaiswalGuided by: Dr Ritusha Mishra
Date: -5th May 2015

RT plays an important role in management high dose can be delivered by combined technique of EBRT &
Brachytherapy
• The cervical cancer has two components
• Central component –• disease confined to cervix , vagina & medial parametria• best treated by brachytherapy
• Peripheral component – • disease involving lateral parametria & regional lymph nodes• best treated by EBRT& brachytherapy as boost

External-beam pelvic irradiation is delivered before Intracavitary insertions in patients with
• Bulky cervical lesions/tumors beyond stage IIA to improve the geometry of the intracavitary application;
• Exophytic, easily bleeding tumors• Tumors with necrosis or infection• Parametrial involvement.
Perez & Brady's Principles and Practice of Radiation Oncology;6thedition,pg 1373
Indications of EBRT
• As definitive RT• As adjuvant RT in post operative settings• As palliative RT
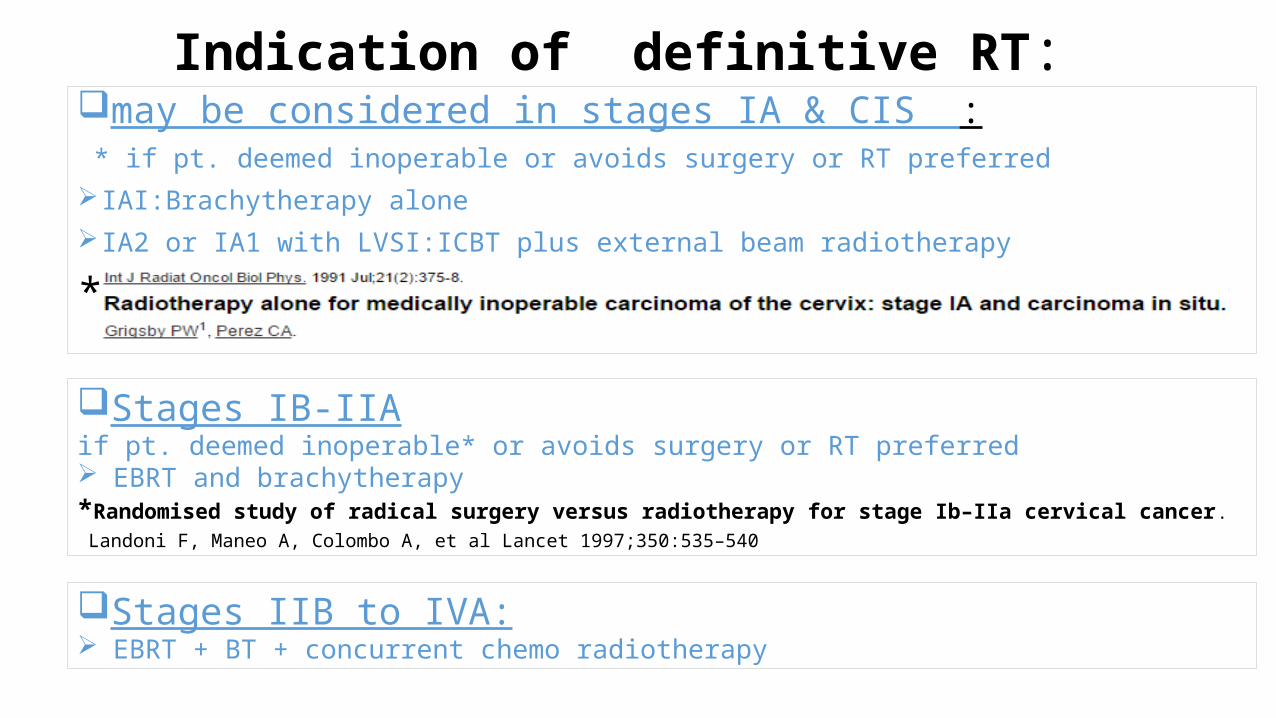
Indication of definitive RT:may be considered in stages IA & CIS : * if pt. deemed inoperable or avoids surgery or RT preferred
IAI:Brachytherapy alone
IA2 or IA1 with LVSI:ICBT plus external beam radiotherapy
*
Stages IB-IIAif pt. deemed inoperable* or avoids surgery or RT preferred EBRT and brachytherapy*Randomised study of radical surgery versus radiotherapy for stage Ib–IIa cervical cancer.
Landoni F, Maneo A, Colombo A, et al Lancet 1997;350:535–540
Stages IIB to IVA: EBRT + BT + concurrent chemo radiotherapy
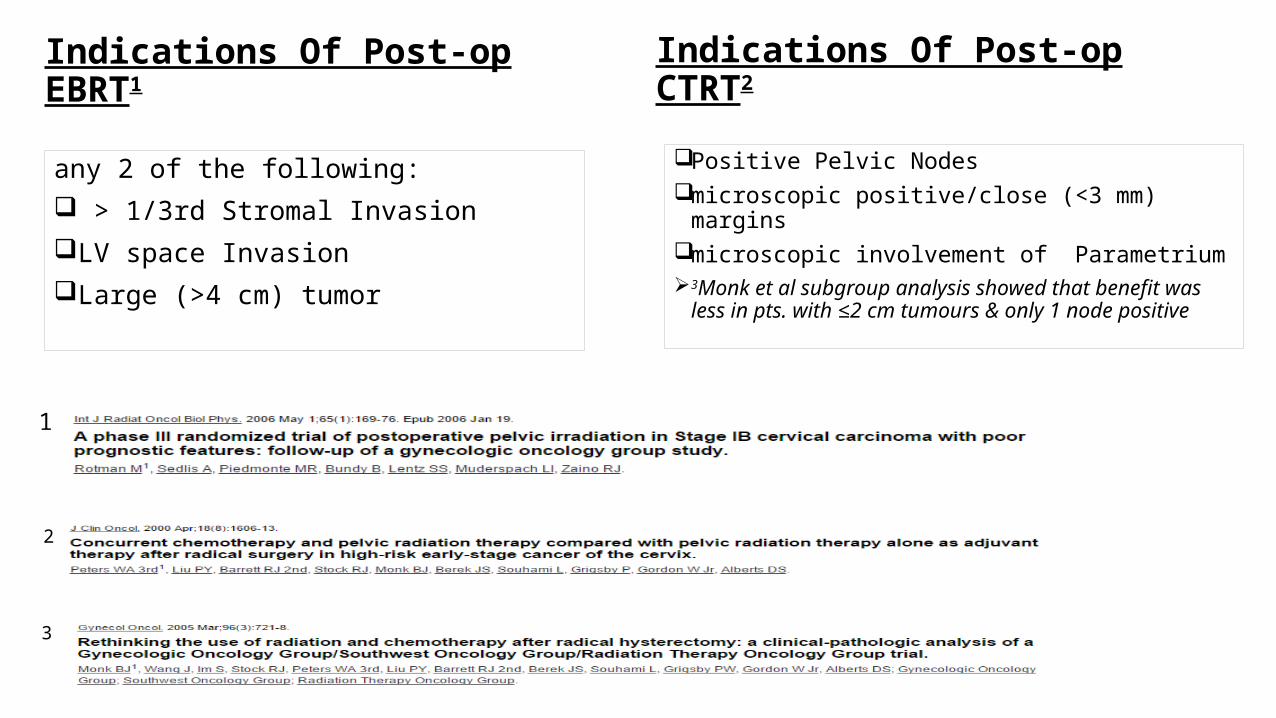
Indications Of Post-op EBRT1
any 2 of the following: > 1/3rd Stromal InvasionLV space InvasionLarge (>4 cm) tumor
Indications Of Post-op CTRT2
Positive Pelvic Nodesmicroscopic positive/close (<3 mm) margins microscopic involvement of Parametrium 3Monk et al subgroup analysis showed that benefit
was less in pts. with ≤2 cm tumours & only 1 node positive
2
1
3

Indications of Palliative radiation
• In stage IVB :• for indications such as • vaginal bleeding, • pain• urethral obstruction
Paraaortic L.N irradiation: indications
• Definitive: • in radiologically/histologically positive paraaortic L.N
• Prophylactic: in pt. with high risk of paraaortic L.N involvement: pt with positive pelvic nodal ds and not receiving CTRT
• Evidences:
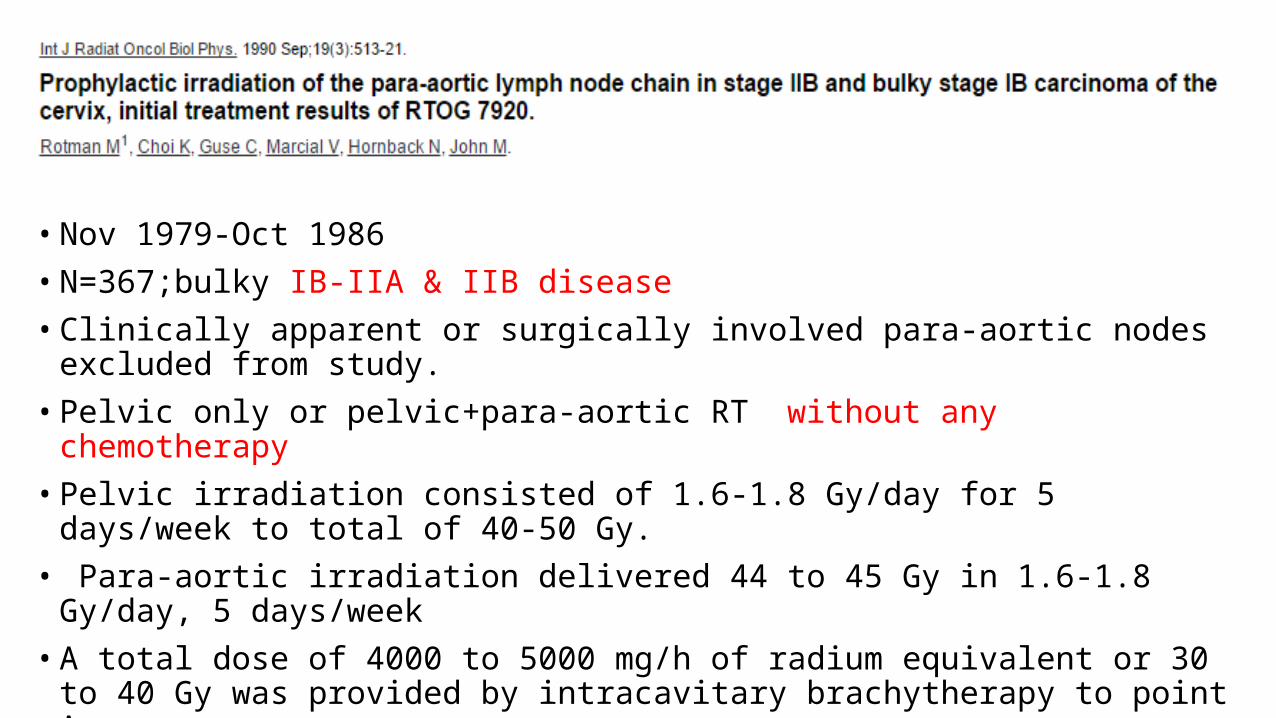
• Nov 1979-Oct 1986
• N=367;bulky IB-IIA & IIB disease
• Clinically apparent or surgically involved para-aortic nodes excluded from study.
• Pelvic only or pelvic+para-aortic RT without any chemotherapy
• Pelvic irradiation consisted of 1.6-1.8 Gy/day for 5 days/week to total of 40-50 Gy.
• Para-aortic irradiation delivered 44 to 45 Gy in 1.6-1.8 Gy/day, 5 days/week
• A total dose of 4000 to 5000 mg/h of radium equivalent or 30 to 40 Gy was provided by intracavitary brachytherapy to point A.
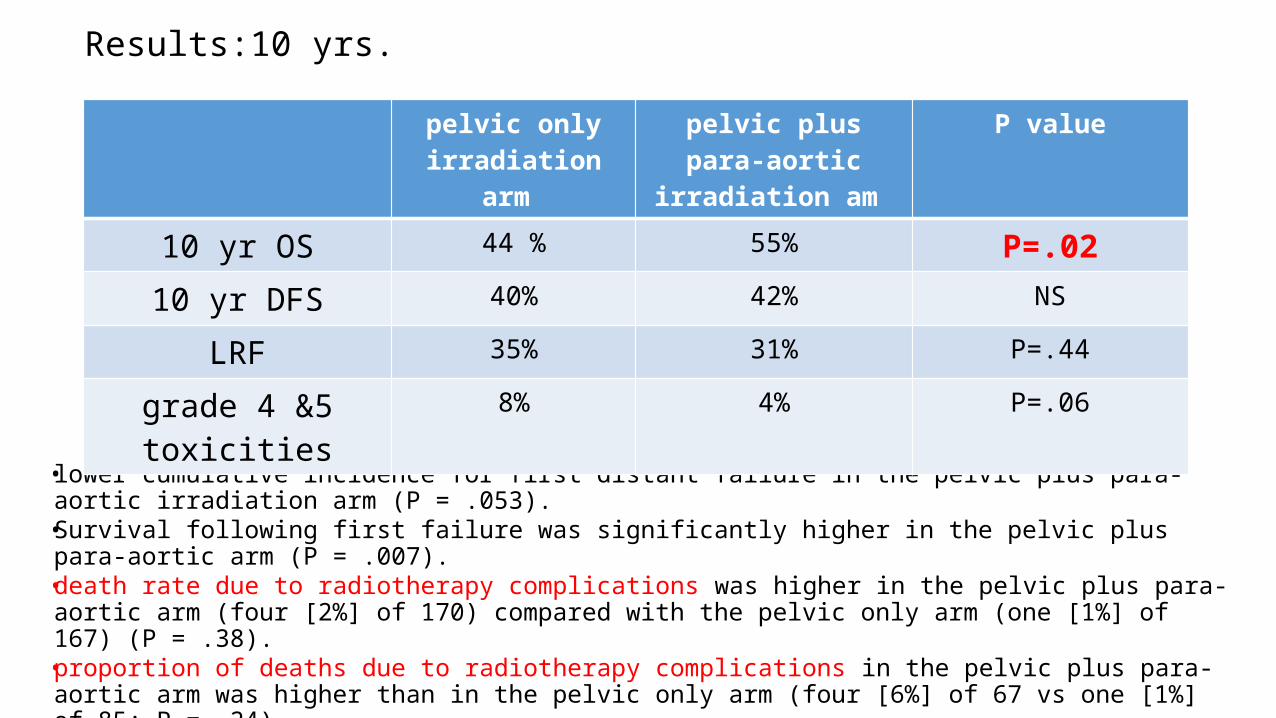
Results:10 yrs.
• lower cumulative incidence for first distant failure in the pelvic plus para-aortic irradiation arm (P = .053).
• Survival following first failure was significantly higher in the pelvic plus para-aortic arm (P = .007).
• death rate due to radiotherapy complications was higher in the pelvic plus para-aortic arm (four [2%] of 170) compared with the pelvic only arm (one [1%] of 167) (P = .38).
• proportion of deaths due to radiotherapy complications in the pelvic plus para-aortic arm was higher than in the pelvic only arm (four [6%] of 67 vs one [1%] of 85; P = .24).
pelvic only irradiation arm
pelvic plus para-aortic irradiation am
P value
10 yr OS 44 % 55% P=.02
10 yr DFS 40% 42% NS
LRF 35% 31% P=.44
grade 4 &5 toxicities 8% 4% P=.06
CONCLUSIONS OF RTOG 79-20:
• The statistically significant difference in overall survival at 10 years for the pelvic plus para-aortic irradiation arm, without a difference in disease-free survival, can be explained by the following two factors:
• (1) a lower incidence of distant failure in complete responders
• (2) a better salvage in the complete responders who later failed locally
• A higher percentage of local failures were salvaged long-term on the pelvic plus para-aortic arm compared with the pelvic only arm (25% vs 8%).
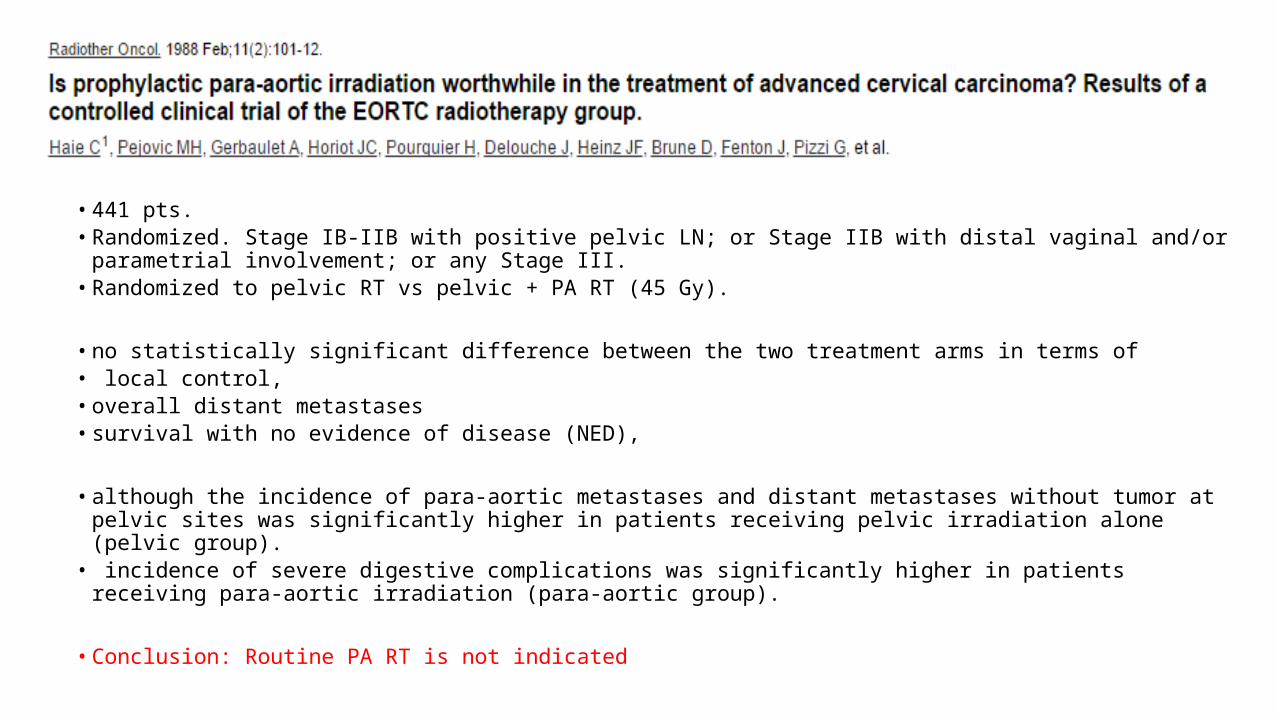
• 441 pts. • Randomized. Stage IB-IIB with positive pelvic LN; or Stage IIB with distal vaginal and/or
parametrial involvement; or any Stage III. • Randomized to pelvic RT vs pelvic + PA RT (45 Gy).
• no statistically significant difference between the two treatment arms in terms of• local control, • overall distant metastases• survival with no evidence of disease (NED),
• although the incidence of para-aortic metastases and distant metastases without tumor at pelvic sites was significantly higher in patients receiving pelvic irradiation alone (pelvic group).
• incidence of severe digestive complications was significantly higher in patients receiving para-aortic irradiation (para-aortic group).
• Conclusion: Routine PA RT is not indicated
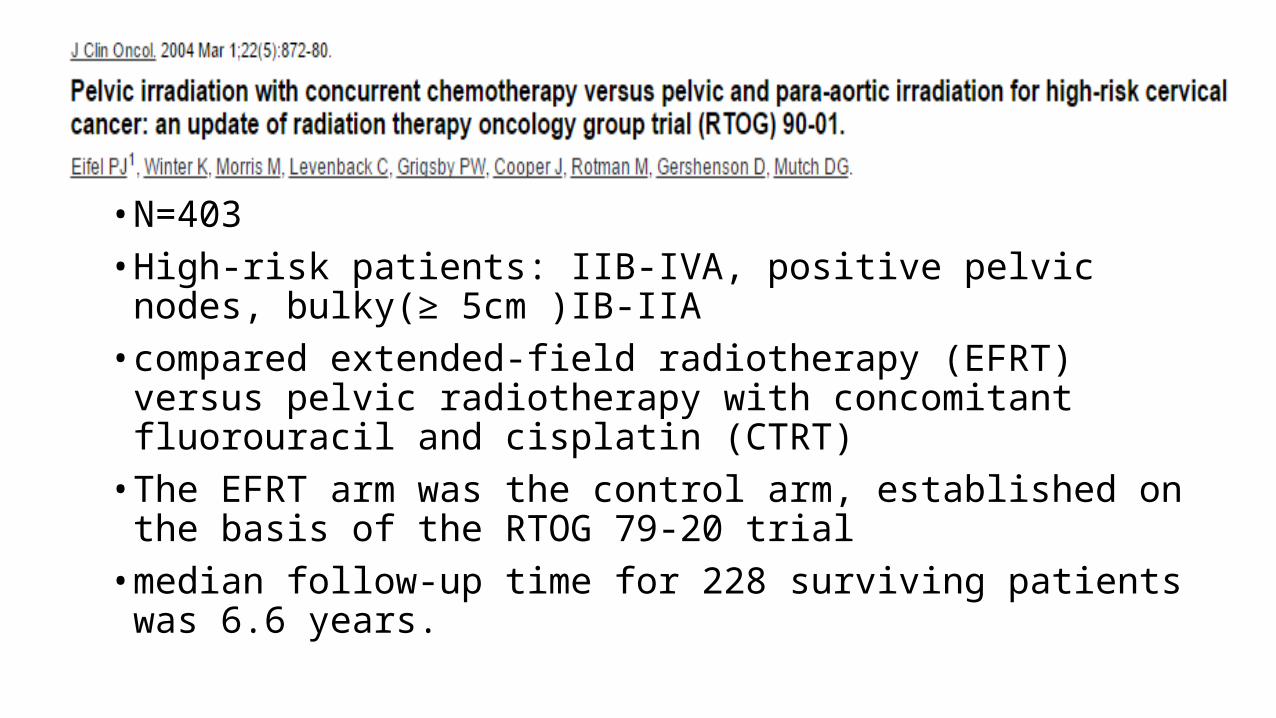
• N=403• High-risk patients: IIB-IVA, positive pelvic nodes, bulky(≥ 5cm )IB-IIA• compared extended-field radiotherapy (EFRT) versus pelvic
radiotherapy with concomitant fluorouracil and cisplatin (CTRT) • The EFRT arm was the control arm, established on the basis of the
RTOG 79-20 trial• median follow-up time for 228 surviving patients was 6.6 years.
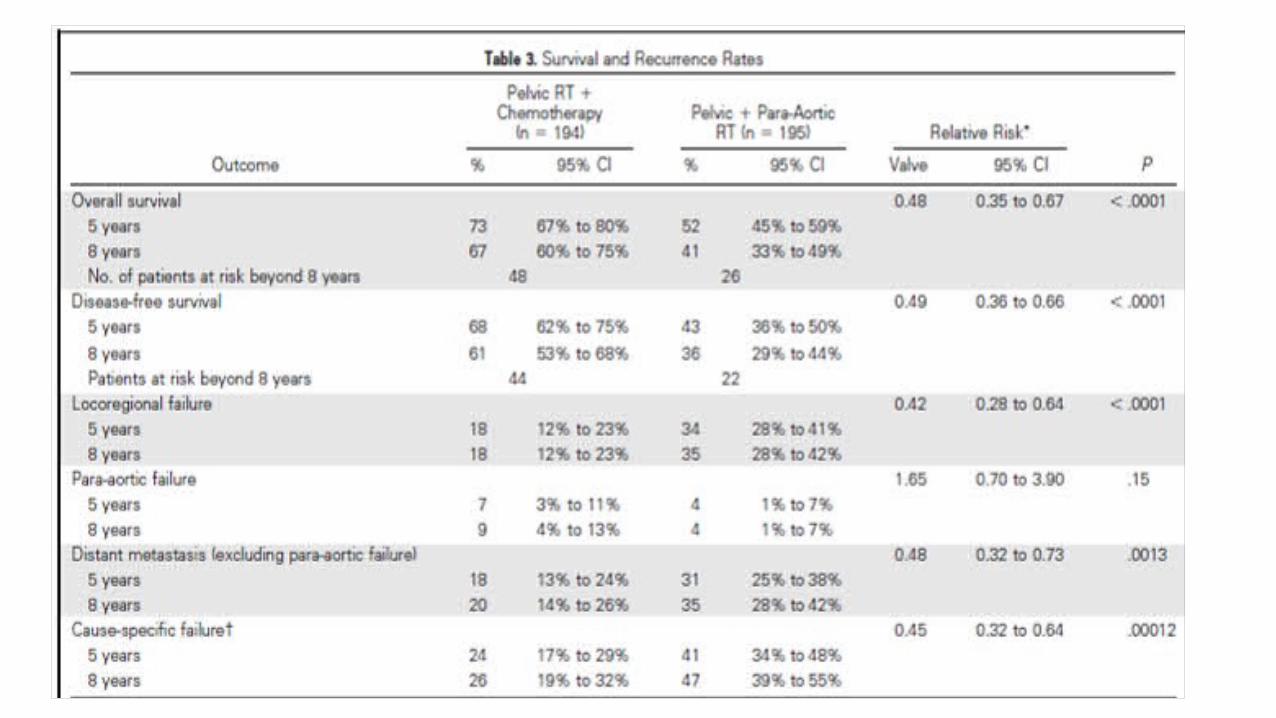
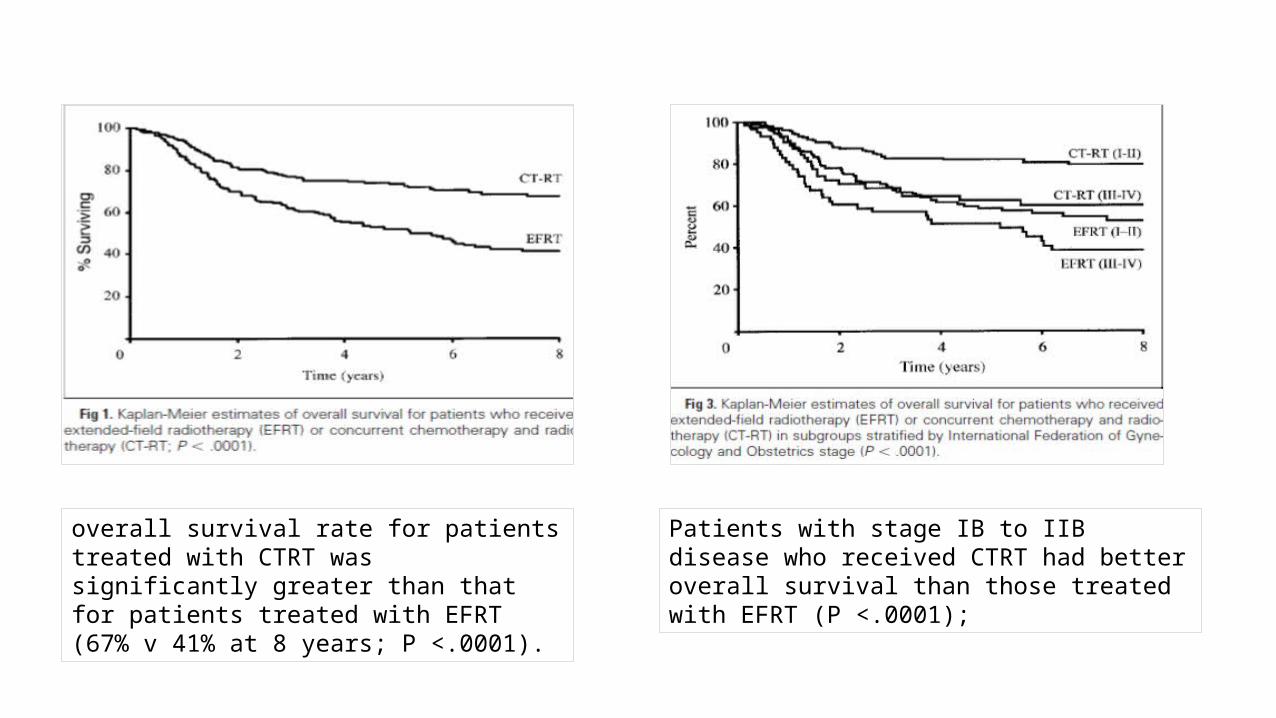
overall survival rate for patients treated with CTRT was significantly greater than that for patients treated with EFRT (67% v 41% at 8 years; P <.0001).
Patients with stage IB to IIB disease who received CTRT had better overall survival than those treated with EFRT (P <.0001);
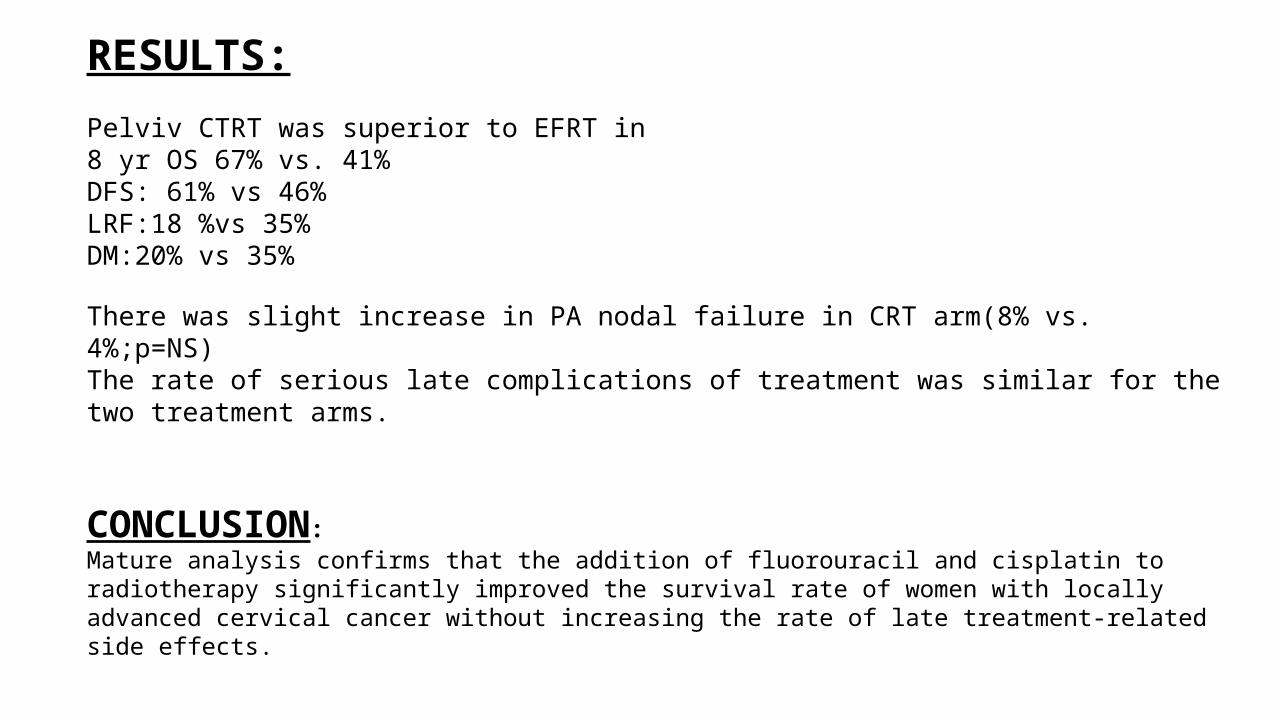
RESULTS:
Pelviv CTRT was superior to EFRT in8 yr OS 67% vs. 41%DFS: 61% vs 46%LRF:18 %vs 35%DM:20% vs 35%
There was slight increase in PA nodal failure in CRT arm(8% vs. 4%;p=NS)The rate of serious late complications of treatment was similar for the two treatment arms.
CONCLUSION:Mature analysis confirms that the addition of fluorouracil and cisplatin to radiotherapy significantly improved the survival rate of women with locally advanced cervical cancer without increasing the rate of late treatment-related side effects.

EBRT: treat the whole pelvis (WPRT)
Target volume includesuterus and cervixtumor bed, in postoperative casesvagina: depending on extent of involvementparametrial tissuelymph nodes. paracervical, parametrial,obturator,presacral L.N
internal iliac, external iliac, common iliac L.Npara-aortic L.N in selected cases(clinical or radiological positive)
EBRT techniques
• Conventional• 3DCRT• IMRT/IGRT
Planning technique
• Positioning & Immobilization• Simulation• Field design• Beam energy• Dose & fractionation
Positioning & Immobilization
Patients may be positioned in • Supine position• Prone position with belly board
supine position is preferred because• Most comfortable• Reproducible position• Stabilizes pelvis• Can be combined with immobilization devices
knee rest can be used • Relaxes lower back making pt. more comfortable• Minimize rotation of pelvis• Knee rest with indexing limits superior-inferior and lateral motion
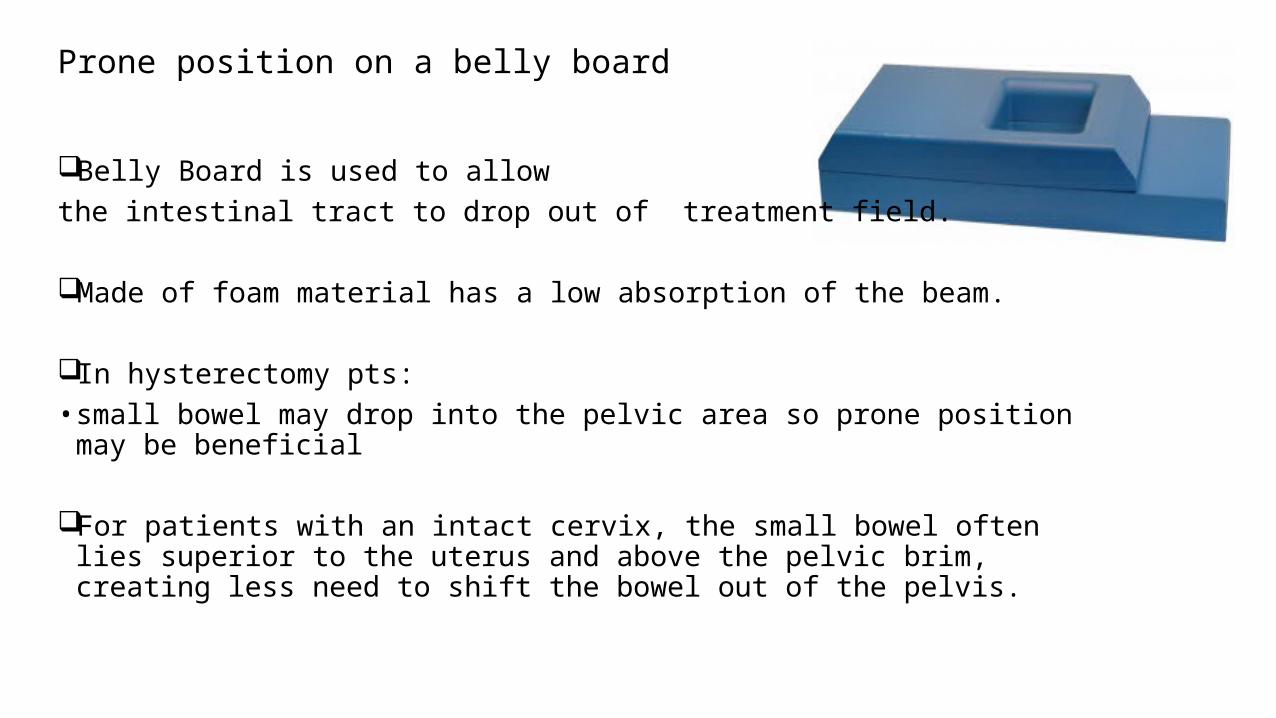
Prone position on a belly board
Belly Board is used to allow the intestinal tract to drop out of treatment field.
Made of foam material has a low absorption of the beam.
In hysterectomy pts: • small bowel may drop into the pelvic area so prone position may be beneficial
For patients with an intact cervix, the small bowel often lies superior to the uterus and above the pelvic brim, creating less need to shift the bowel out of the pelvis.
Immobilization
Several types of immobilization options available in radiotherapyNeeds to be:
Comfortable Reproducible Minimal beam attenuating Affordable
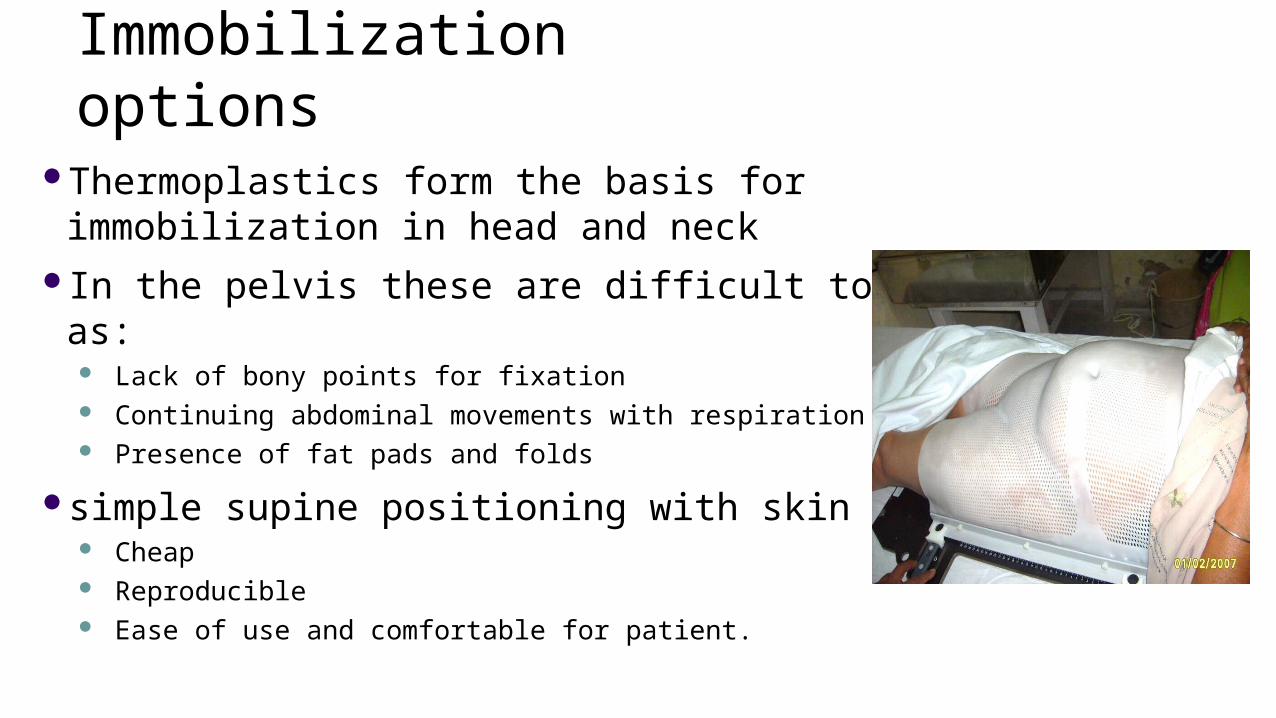
Immobilization options
Thermoplastics form the basis for immobilization in head and neckIn the pelvis these are difficult to be used as:
Lack of bony points for fixation Continuing abdominal movements with respiration Presence of fat pads and folds
simple supine positioning with skin markings: Cheap Reproducible Ease of use and comfortable for patient.
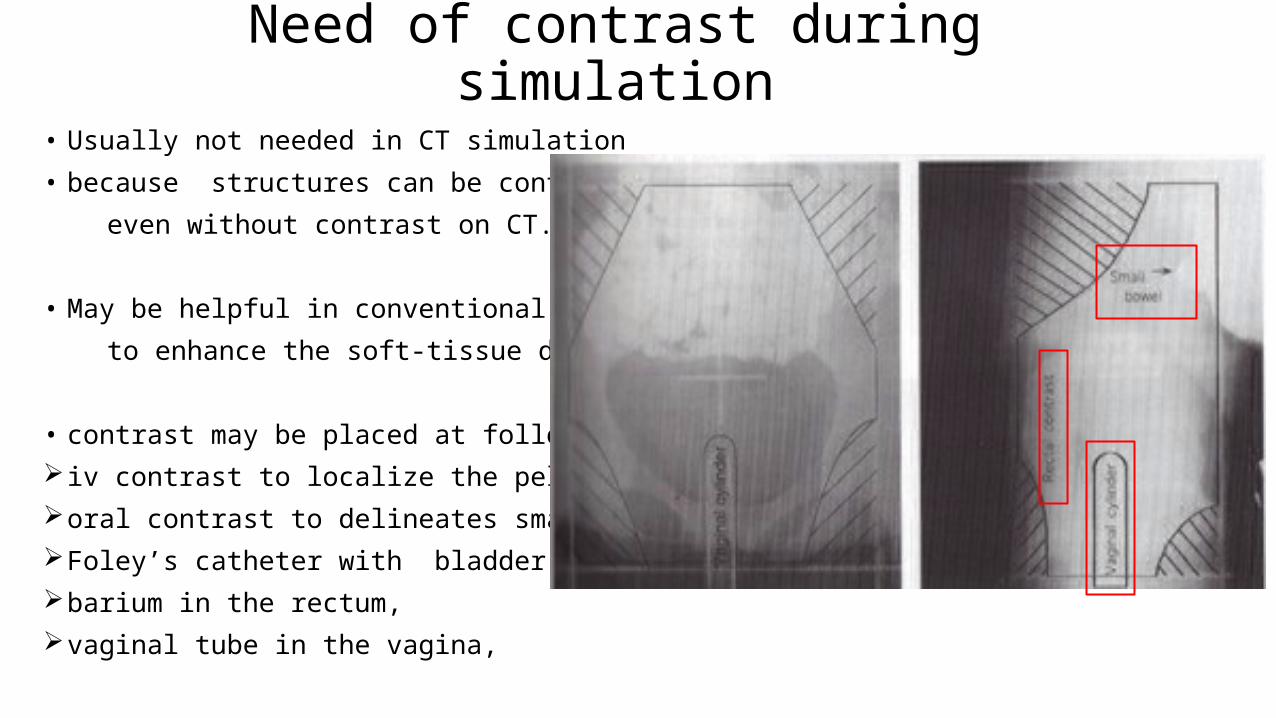
Need of contrast during simulation
• Usually not needed in CT simulation
• because structures can be contoured
even without contrast on CT.
• May be helpful in conventional simulation
to enhance the soft-tissue detail
• contrast may be placed at following sites iv contrast to localize the pelvic vesselsoral contrast to delineates small bowel. Foley’s catheter with bladder contrastbarium in the rectum, vaginal tube in the vagina,
X-Ray SimulationConventional simulator can be used to acquire patient data Patient position: supine with arms on the chest, knee and lower leg immobilisation or alpha cradles may
be used to prevent pelvic rotationOrthogonal laser beams aligned with anterior and lateral tattoos marked with radio-opaque material. For obese patients, a prone belly board may be used to allow small bowel to fall anteriorlyInferior border of tumor marked with radio-opaque material.Bladder protocol is used to maintain a constant bladder filling – ‘comfortably full’ AP and lateral simulator films are taken. Standard field borders decided using bony anatomical landmarks.
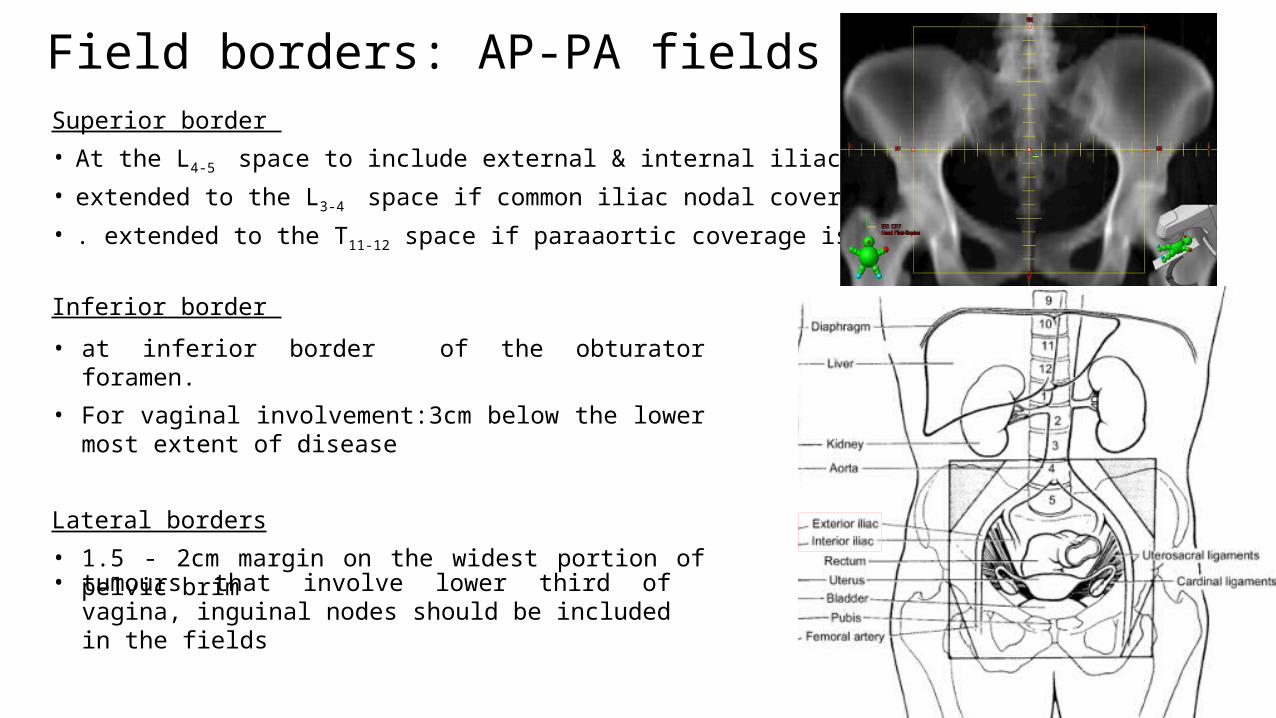
Field borders: AP-PA fieldsSuperior border
• At the L4-5 space to include external & internal iliac L.N.
• extended to the L3-4 space if common iliac nodal coverage is indicated
• . extended to the T11-12 space if paraaortic coverage is indicated
Inferior border
• at inferior border of the obturator foramen.
• For vaginal involvement:3cm below the lower most extent of disease
Lateral borders
• 1.5 - 2cm margin on the widest portion of pelvic brim
• tumours that involve lower third of vagina, inguinal nodes should be included in the fields
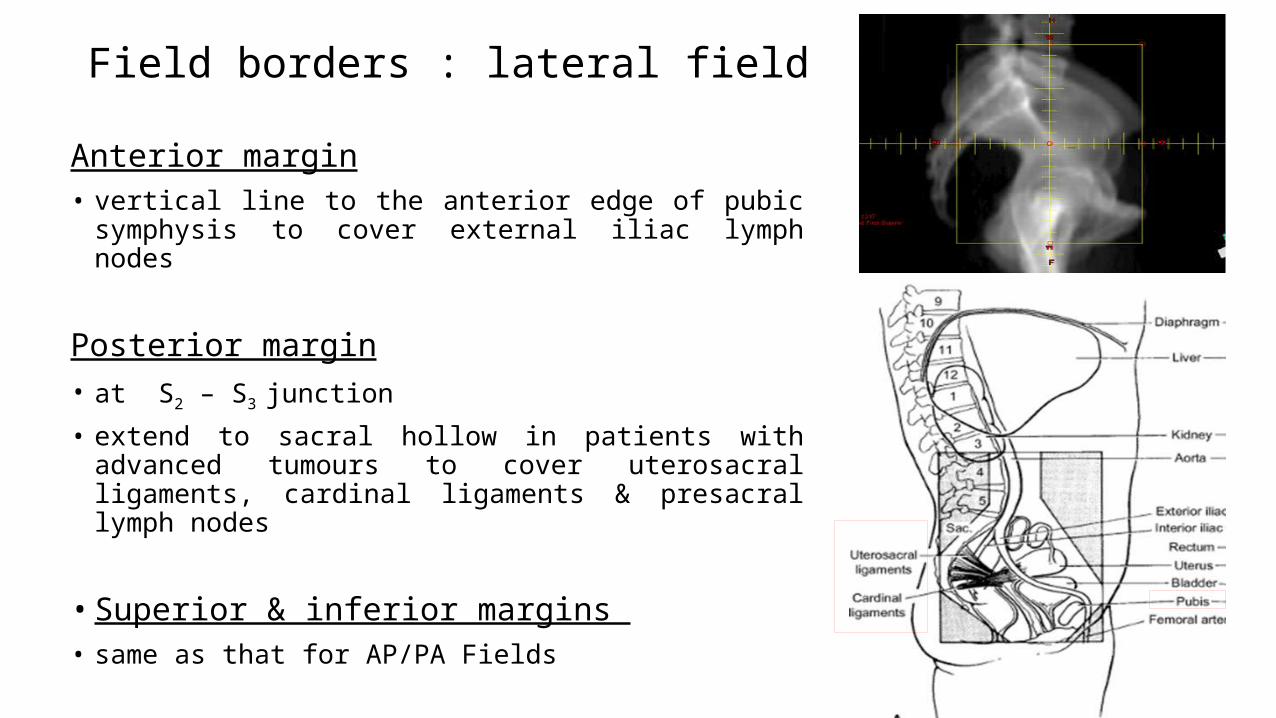
Field borders : lateral field
Anterior margin• vertical line to the anterior edge of pubic symphysis to cover
external iliac lymph nodes
Posterior margin• at S2 – S3 junction
• extend to sacral hollow in patients with advanced tumours to cover uterosacral ligaments, cardinal ligaments & presacral lymph nodes
• Superior & inferior margins • same as that for AP/PA Fields
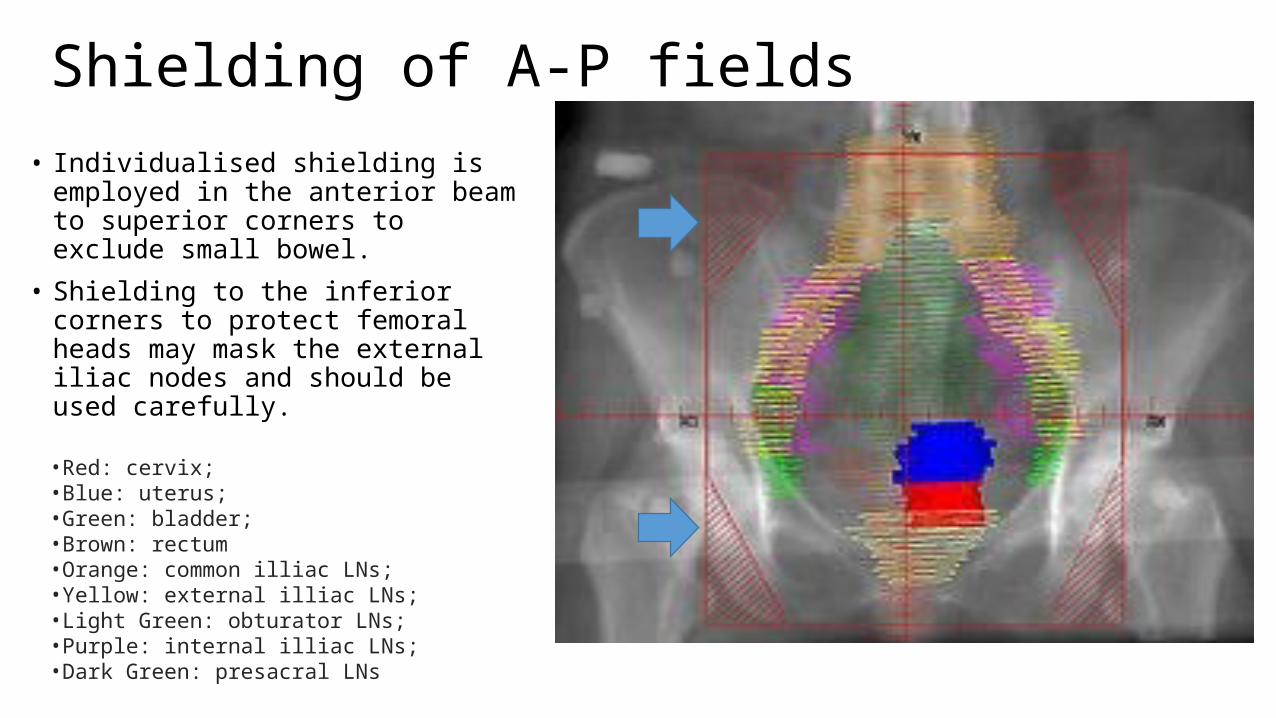
Shielding of A-P fields• Individualised shielding is employed in
the anterior beam to superior corners to exclude small bowel.
• Shielding to the inferior corners to protect femoral heads may mask the external iliac nodes and should be used carefully.
•Red: cervix;•Blue: uterus; •Green: bladder; •Brown: rectum•Orange: common illiac LNs; •Yellow: external illiac LNs; •Light Green: obturator LNs; •Purple: internal illiac LNs; •Dark Green: presacral LNs
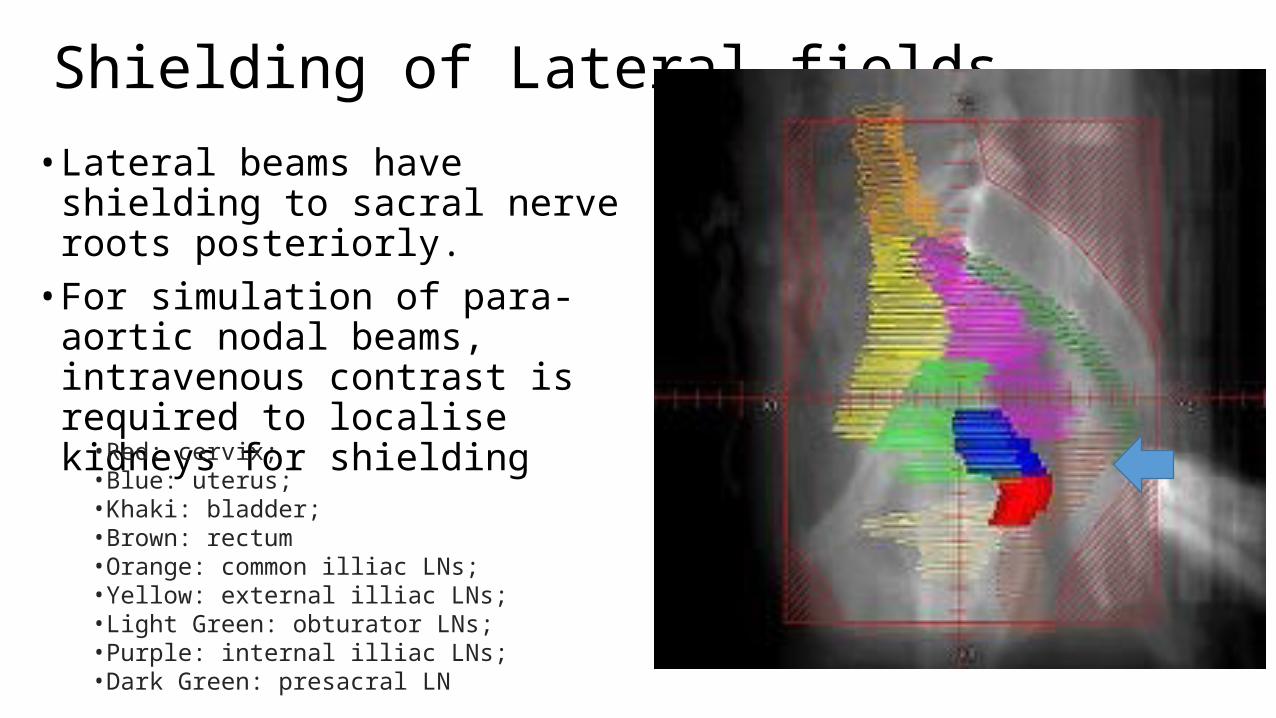
• Lateral beams have shielding to sacral nerve roots posteriorly.
• For simulation of para-aortic nodal beams, intravenous contrast is required to localise kidneys for shielding
Shielding of Lateral fields
•Red: cervix; •Blue: uterus; •Khaki: bladder; •Brown: rectum•Orange: common illiac LNs; •Yellow: external illiac LNs; •Light Green: obturator LNs; •Purple: internal illiac LNs; •Dark Green: presacral LN
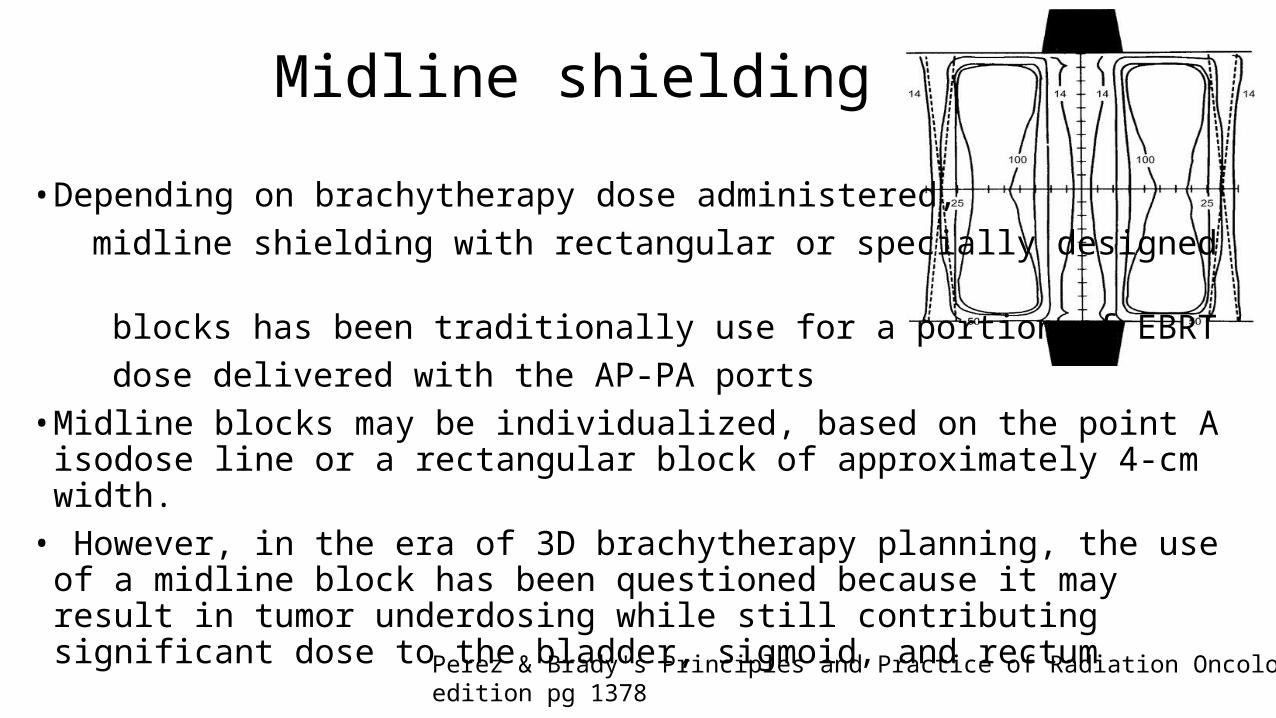
Midline shielding
• Depending on brachytherapy dose administered, midline shielding with rectangular or specially designed blocks has been traditionally use for a portion of EBRT dose delivered with the AP-PA ports• Midline blocks may be individualized, based on the point A isodose line or a
rectangular block of approximately 4-cm width.• However, in the era of 3D brachytherapy planning, the use of a midline block
has been questioned because it may result in tumor underdosing while still contributing significant dose to the bladder, sigmoid, and rectum
Perez & Brady's Principles and Practice of Radiation Oncology,6th edition pg 1378
PARAAROTIC L.N. IRRADIATION
• Extended field RT:• pelvis & para-aortic L.N. should be treated as contiguous extended field portal
• Separate field:• Para-aortic L.N. and the pelvis are irradiated through separate portals • In this case, a gap calculation b/w the pelvic and para-aortic portals must be
done to avoid overlap and excessive dose to the small intestines.
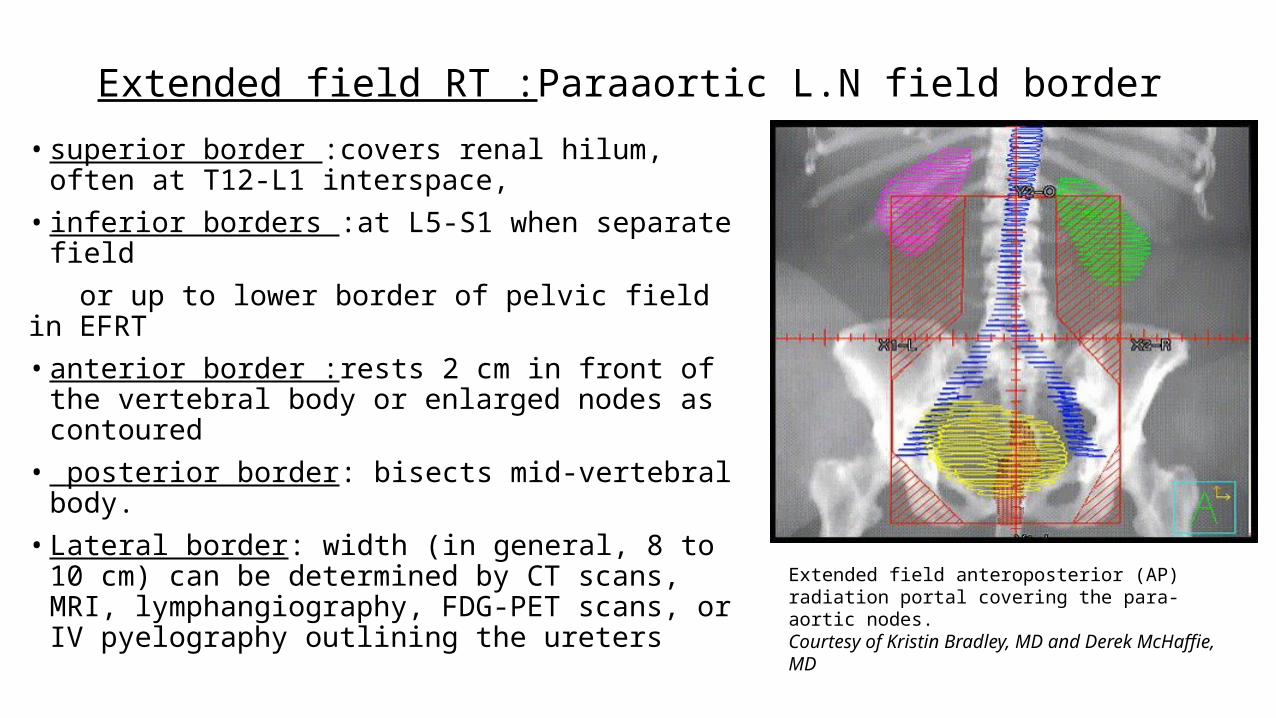
Extended field RT :Paraaortic L.N field border• superior border :covers renal hilum, often at T12-L1
interspace,• inferior borders :at L5-S1 when separate field or up to lower border of pelvic field in EFRT• anterior border :rests 2 cm in front of the vertebral
body or enlarged nodes as contoured• posterior border: bisects mid-vertebral body. • Lateral border: width (in general, 8 to 10 cm) can be
determined by CT scans, MRI, lymphangiography, FDG-PET scans, or IV pyelography outlining the ureters Extended field anteroposterior (AP) radiation portal
covering the para-aortic nodes.Courtesy of Kristin Bradley, MD and Derek McHaffie, MD
Para-aortic field: 2 field vs. 4 field
• AP-PA treatments to the para-aortic nodal chain may overdose the kidneys, spinal cord, and small bowel.
• The spinal cord dose (T12 to L2–3) should be kept to <45 Gy• This can be done by• interposing a 2-cm-wide 5–half-value-layer shield on the posterior portal (usually after
40-Gy tumor dose) • or using lateral ports and limiting the kidney dose to <18 Gy• The use of four fields, including AP-PA and two lateral fields, is implemented as
an alternative to AP-PA alone as a way to reduce some of the dose to the anterior small bowel, kidney S.C
Midline Shielding in AP-PA Portals and Use of a Parametrial Boost
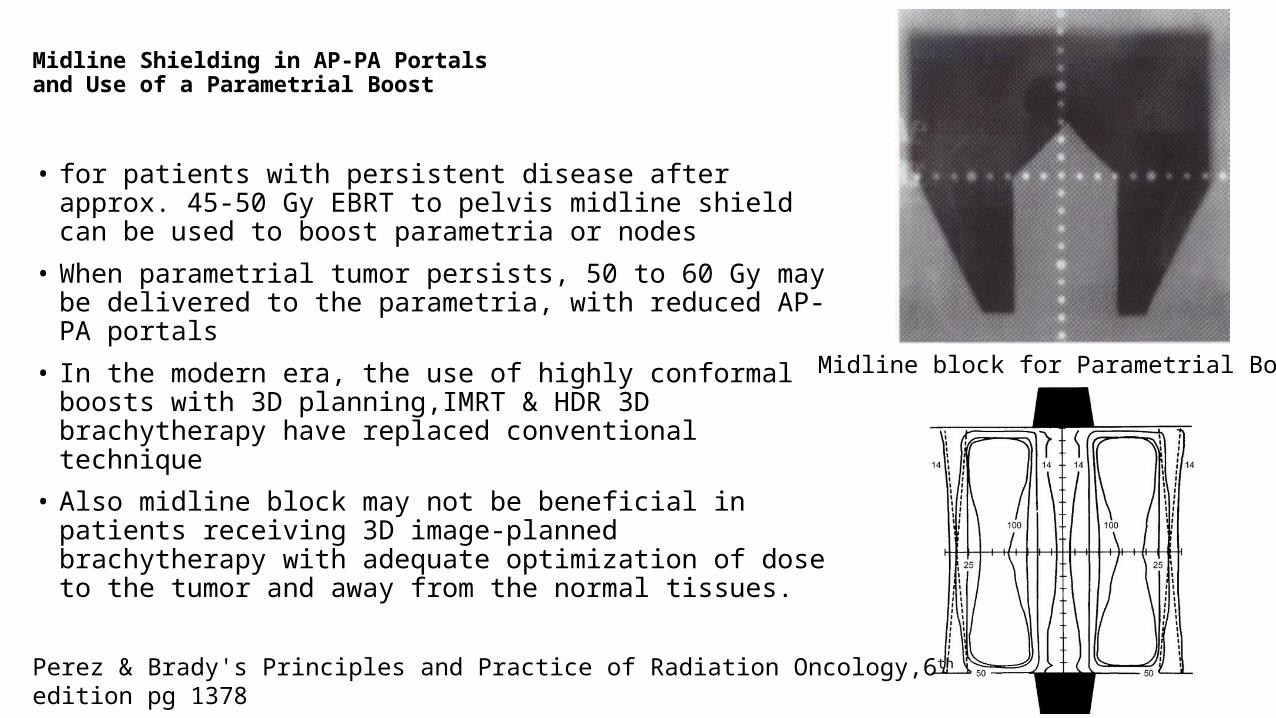
• for patients with persistent disease after approx. 45-50 Gy EBRT to pelvis midline shield can be used to boost parametria or nodes
• When parametrial tumor persists, 50 to 60 Gy may be delivered to the parametria, with reduced AP-PA portals
• In the modern era, the use of highly conformal boosts with 3D planning,IMRT & HDR 3D brachytherapy have replaced conventional technique
• Also midline block may not be beneficial in patients receiving 3D image-planned brachytherapy with adequate optimization of dose to the tumor and away from the normal tissues.
Midline block for Parametrial Boost
Perez & Brady's Principles and Practice of Radiation Oncology,6th edition pg 1378
Treatment technique: SSD Vs SAD
• SSD treatments:• Setup possible without
requiring expensive aids e.g. Laser
• SAD treatments:• Ease of setup reproducibility• Impact of setup inaccuracies is
minimized
The principal advantage of isocentric technique over SSD technique is that the patient is not moved between fields. Once the isocenter is positioned accurately within the patient, the remaining fields are arranged simply by gantry rotation or couch movement, not by displacing the patient relative to the couch.
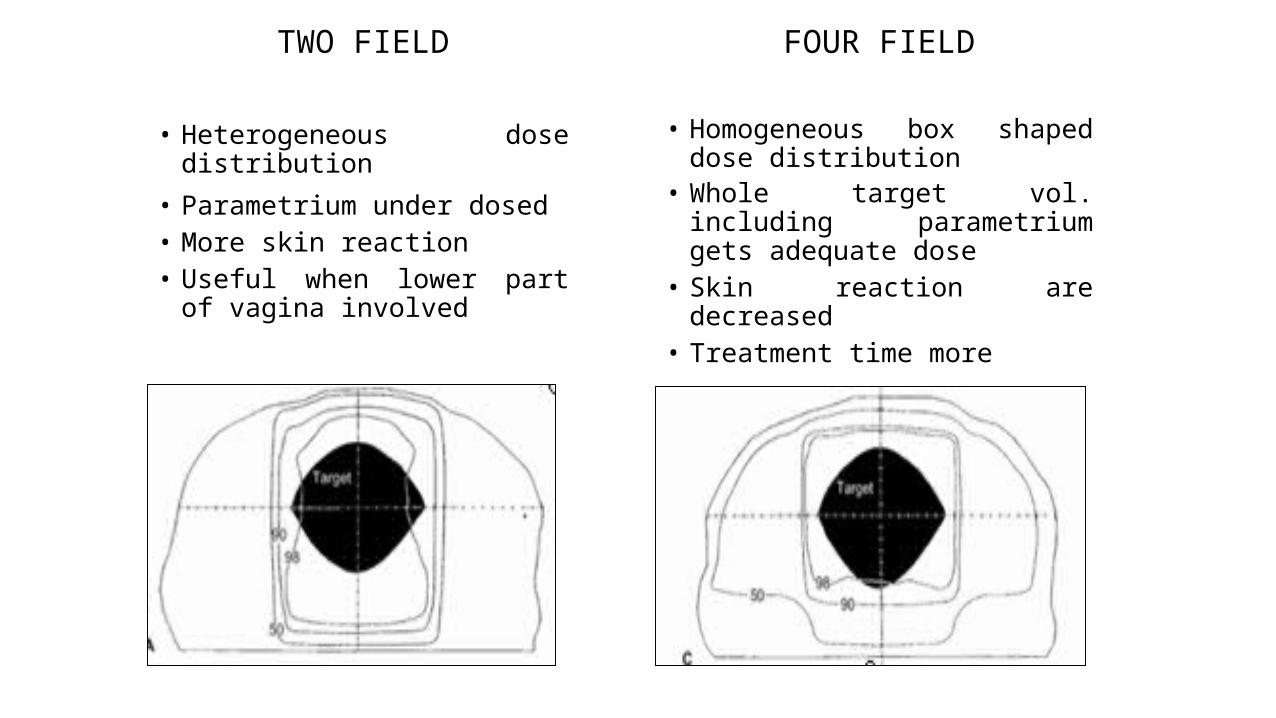
TWO FIELD
• Heterogeneous dose distribution
• Parametrium under dosed• More skin reaction• Useful when lower part of vagina
involved
FOUR FIELD
• Homogeneous box shaped dose distribution
• Whole target vol. including parametrium gets adequate dose
• Skin reaction are decreased• Treatment time more
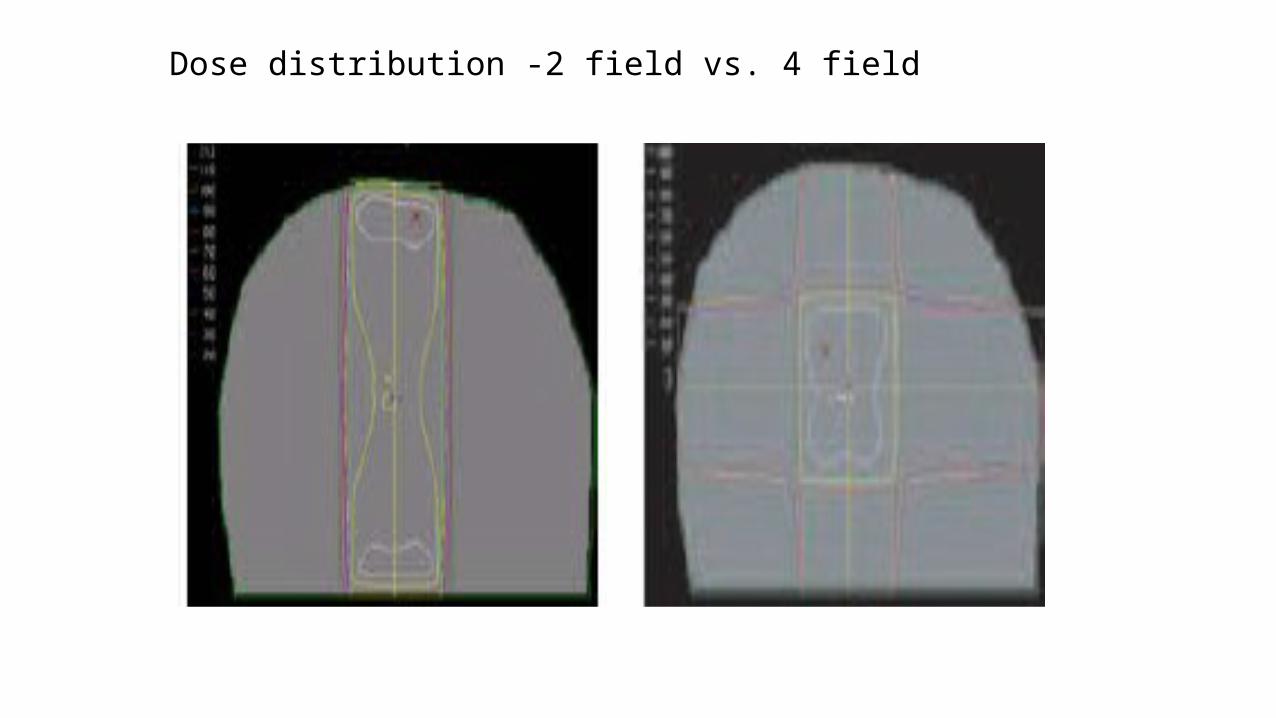
Dose distribution -2 field vs. 4 field
BEAM ENERGY• Because of the thickness of the pelvis, high-energy photon beams (10 MV or higher) are
especially suited for this treatment.
• They decrease the dose of radiation delivered to the peripheral normal tissues (particularly bladder and rectum)
• provide a more homogeneous dose distribution in the central pelvis.• avoid subcutaneous fibrosis
Dose & fractionationPrimary radiotherapy
Stage IB2 and IIA
• 45 Gy in 25 daily fractions of 1.8 Gy given in 5 weeks followed by Intracavitary brachytherapy.
Stage IIB or above
• 50.4 Gy in 28 daily fractions of 1.8 Gy given in 51⁄2 weeks followed by Intracavitary brachytherapy.
Persistant /bulky parametrial tumor: boost upto 60 Gy
Adjuvant radiotherapy
• 45 Gy in 25 daily fractions of 1.8 Gy given in 5 weeks.
• 50.4 Gy in 28 daily fractions of 1.8 Gy in 51⁄2 weeks if macroscopic residual disease.
Para-aortic node radiotherapy
• Adjuvant radiotherapy:45 Gy in 25 daily fractions of 1.8 Gy given in 5 weeks.
Palliative treatment
• Whole pelvis or para-aortic nodes
• 20–30 Gy in 5–10 daily fractions given in 1–2 weeks.
• 8–10 Gy in 1 fraction for haemostasis.
Practical Radiotherapy Planning; Jane Dobbs;pg 392
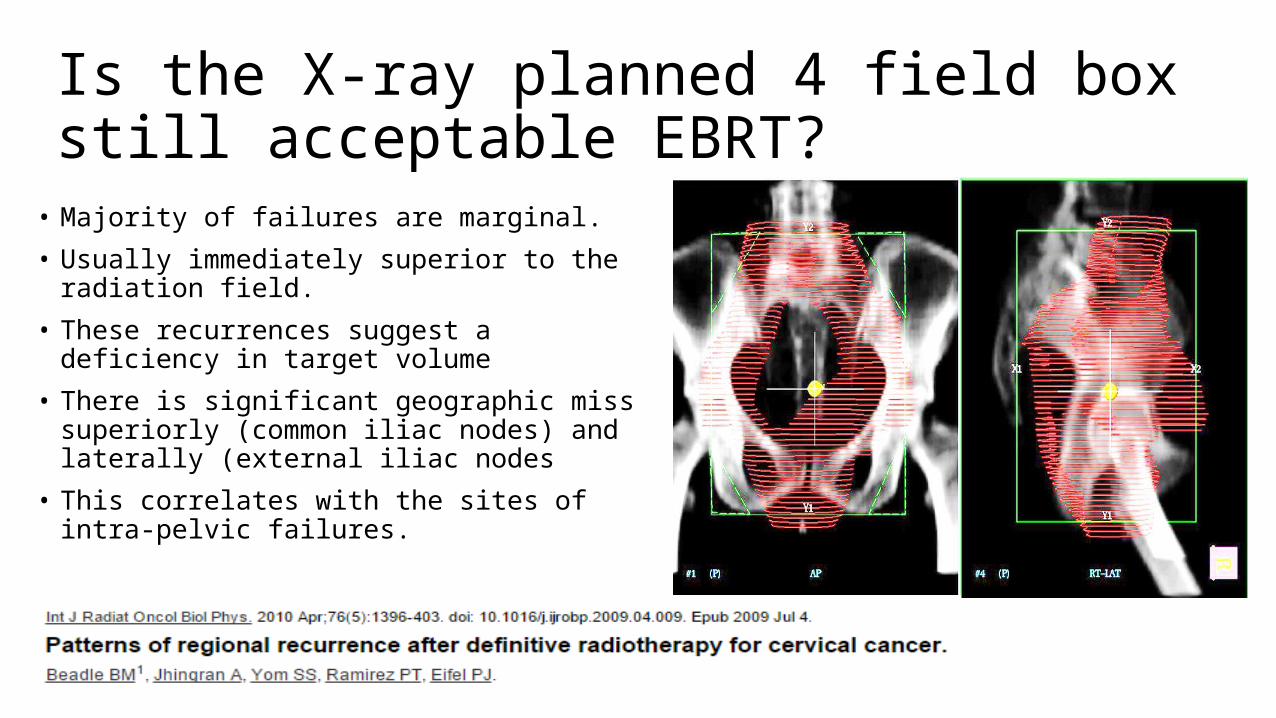
Is the X-ray planned 4 field box still acceptable EBRT?
• Majority of failures are marginal.
• Usually immediately superior to the radiation field.
• These recurrences suggest a deficiency in target volume
• There is significant geographic miss superiorly (common iliac nodes) and laterally (external iliac nodes
• This correlates with the sites of intra-pelvic failures.

Dosimetric comparison between conventional and conformal radiotherapy for carcinoma cervix
• Three-dimensional conformal radiotherapy gives significantly better target coverage, which may translate into better local control and survival.
• On the other hand, it also requires significantly larger field sizes though doses to the OARs are not significantly increased.

Aims: To estimate inadequacies in target volume coverage when using conventional planning based on bony landmarks.
Materials and Methods: 50 patients. biopsy proven patients of locally advanced uterine cervix cancer stage II-III‑32 patients (64%) belonged to Stage IIB and 18 (36%) to Stage IIIB.
All patients were planned for radical radiation of 46Gy/23 fractions over 4.5 weeks and 78% patients received concomitant chemotherapy with weekly cisplatin at a dose of 40 mg/m2 followed by two sessions of HDR intracavitary brachytherapy, with a dose of 9 Gy per fraction.
In all patients, the treatment was completed within 56 days of starting external radiation
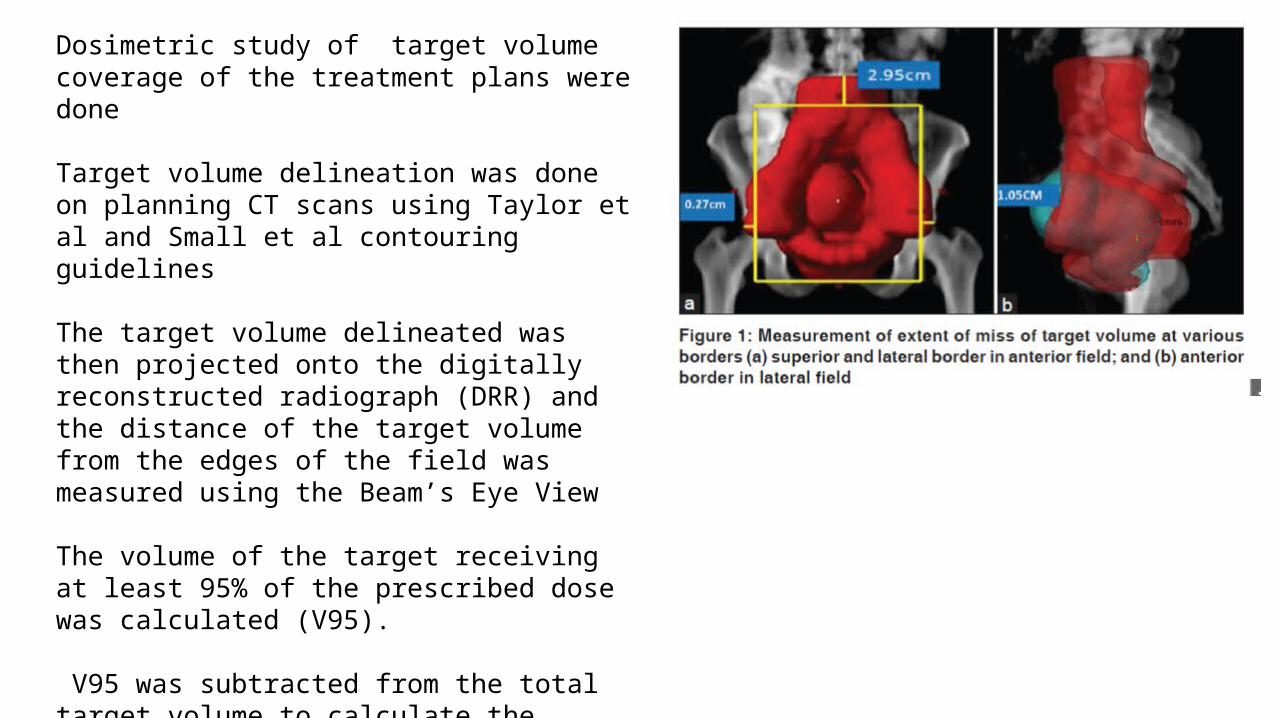
Dosimetric study of target volume coverage of the treatment plans were done
Target volume delineation was done on planning CT scans using Taylor et al and Small et al contouring guidelines
The target volume delineated was then projected onto the digitally reconstructed radiograph (DRR) and the distance of the target volume from the edges of the field was measured using the Beam’s Eye View
The volume of the target receiving at least 95% of the prescribed dose was calculated (V95).
V95 was subtracted from the total target volume to calculate the volume that would have been missed in conventional planning based on bony landmarks
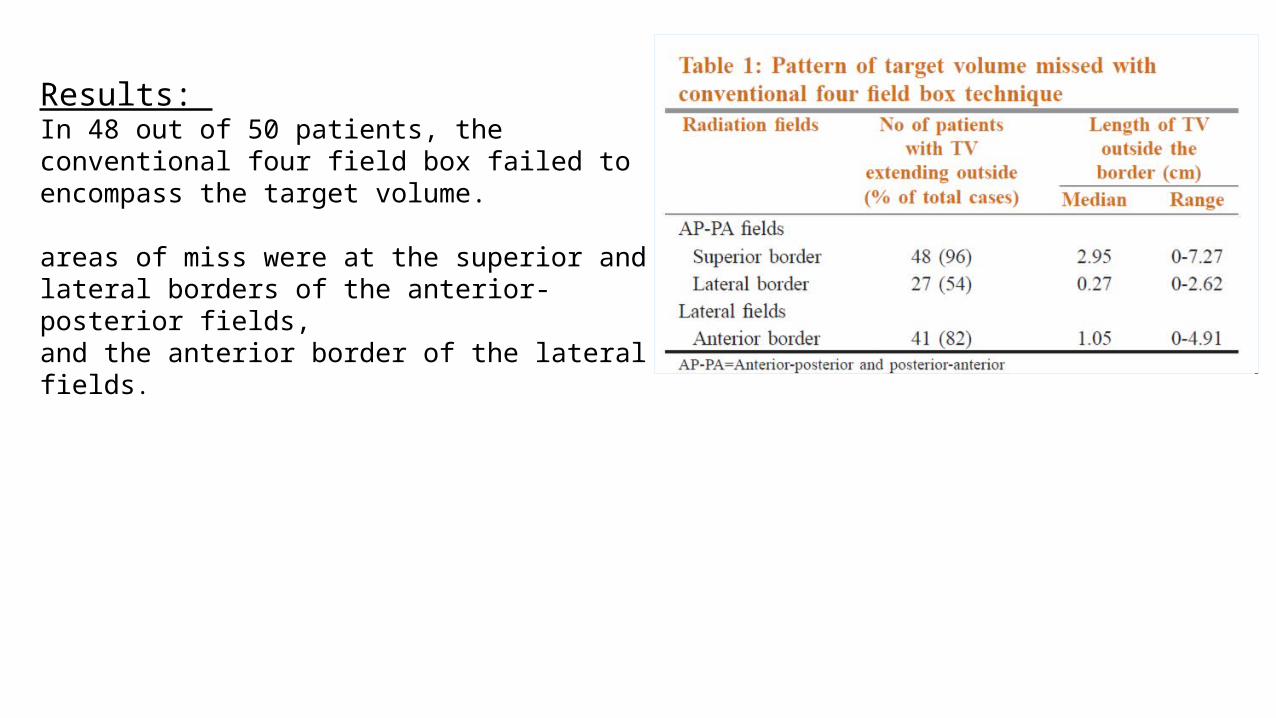
Results: In 48 out of 50 patients, the conventional four field box failed to encompass the target volume. areas of miss were at the superior and lateral borders of the anterior-posterior fields, and the anterior border of the lateral fields.
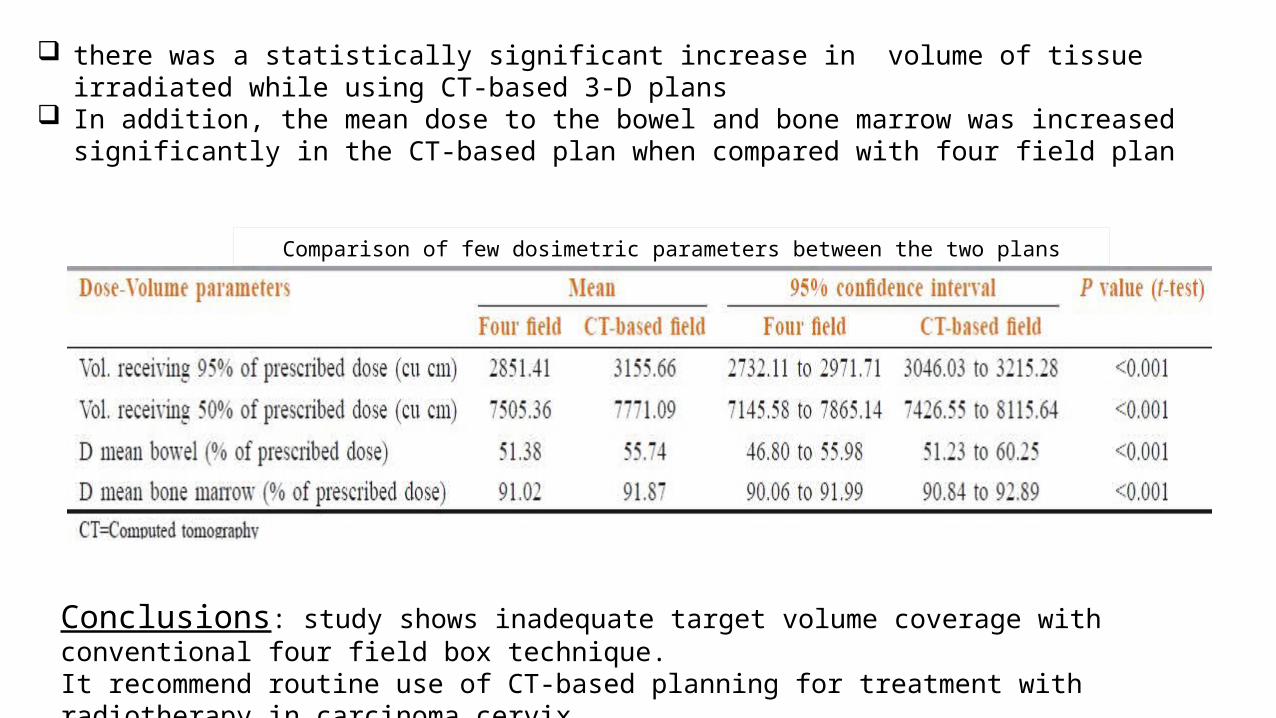
there was a statistically significant increase in volume of tissue irradiated while using CT based 3 D plans ‑ ‑ In addition, the mean dose to the bowel and bone marrow was increased significantly in the CT based plan ‑
when compared with four field plan
Comparison of few dosimetric parameters between the two plans
Conclusions: study shows inadequate target volume coverage with conventional four field box technique. It recommend routine use of CT based planning for treatment with radiotherapy in carcinoma cervix‑
3D CRT Planning
• Patient position and immobilization• Volumetric data acquisition• Image transfer to the TPS• Target volume delineation• Planning• Dose distribution analysis• Treatment QA & delivery
CT SIMULATION CT scanning is recommended for data acquisition.
Patients are usually scanned in supine position, arms overhead , knees immobilised with knee rest For obese pts. prone belly board may be used A vaginal marker is placed at the lower extent of disease when it extends into vagina to determine the
length of vagina involved Or the marker can also be placed at the external os and the lower extent of disease individually
determined based on findings of clinical examinations
Intravenous contrast is used to outline pelvic blood vessels to be used as surrogates for pelvic node Oral and rectal contrast may be given for delineation of critical structures
CT scan is obtained from T10-T11 interspace to upper third of femur, slice thickness may vary from 3-5 mm depending upon institutional protocol These images are transferred to treatment planning system (TPS) and contouring is done
In pelvic malignancies bladder filling status has largely been the matter of debate. George et al.,[1] and Pinkawa et al.,[2] recommended a full bladder for treatment of gynecological
malignancies, as the dose-volume-load to bladder and cranially displaced sigmoid colon/small bowel loops can be reduced significantly.
However; Pinkawa in another study[3] found that bladder wall displacements are reduced significantly (P < 0.01) at superior and anterior border while treating empty bladder compared to full bladder and also there is less variability in bladder volume in an empty bladder state.
the ideal bladder filling status has not been ensured by any study so far. The bladder protocols may vary from institution however most institute follow a consistent bladder
filling protocol of voiding urine 15 min prior to both imaging and treatment
Bladder Protocol for Simulation
1:Georg P, Georg D,et al. Factors influencing bowel sparing in intensity modulated whole pelvic radiotherapy for gynaecological malignancies. Radiother Oncol 2006;80:19-26. 2:Pinkawa Met al. Dose-volume histogram evaluation of prone and supine patient position in external beam radiotherapy for cervical and endometrial cancer. Radiother Oncol 2003;69:99-105. 3.:Pinkawa M,, et al. Bladder extension variability during pelvic external beam radiotherapy with a full or empty bladder. Radiother Oncol 2007;83:163-7.

Target Volume delineation
For definitive treatment of carcinoma cervix with conformal radiation techniques, accurate target delineation is vitally important,
Various guidelines for CTV delineation are published in the literature yet a consensus definition of clinical target volume (CTV) remains variable
Clinical judgement remains the most important aspect of determining the target volumes

ContouringSeveral contouring guidelines available for CTVTaylor et al pelvic nodal delineation (CT based)Toita et al for CTV delineation in intact cervix EBRT (CT based)Lim et al for CTV delineation in intact cervix IMRT (MRI based)Small et al for CTV delineation in post operative IMRT (CT based)PGI literature review & guidelines for delineation of CTV for intact carcinoma cervix (CT based)
Guidelines for organ at riskPelvic Normal Tissue Contouring Guidelines for Radiation Therapy: A Radiation Therapy Oncology
Group Consensus Panel Atlas (CT based)
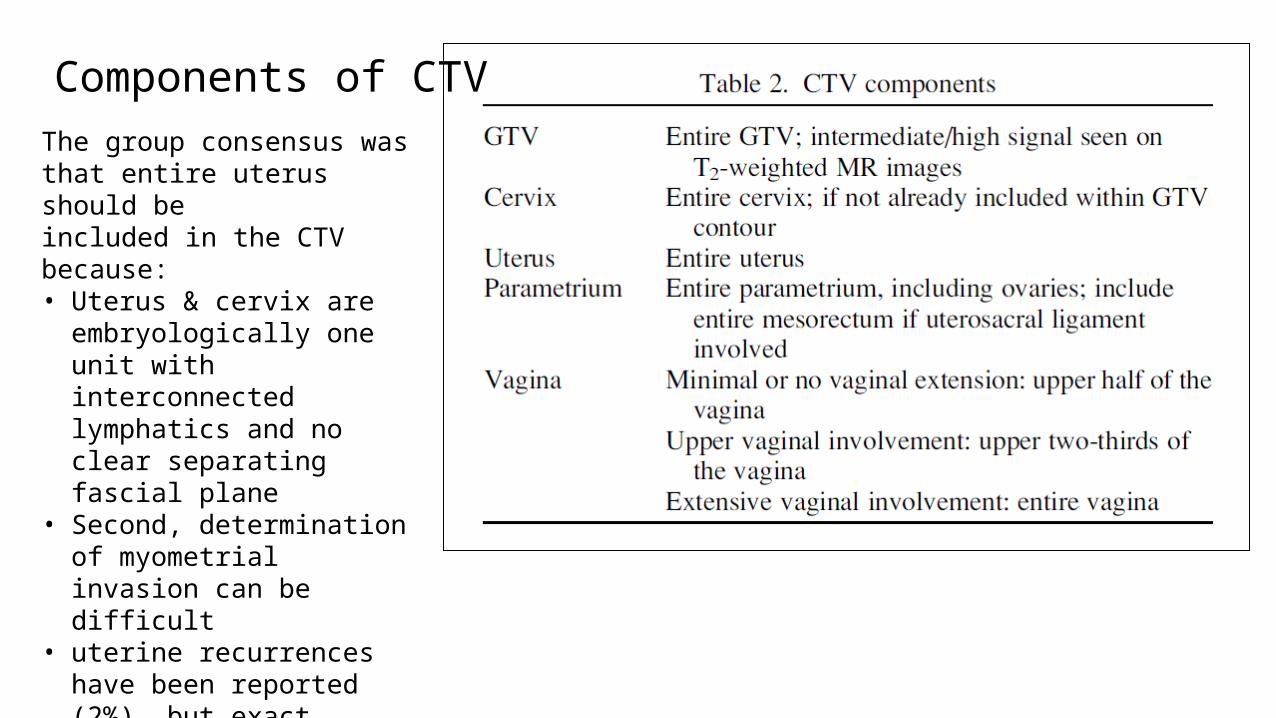
Components of CTVThe group consensus was that entire uterus should beincluded in the CTV because:• Uterus & cervix are
embryologically one unit with interconnected lymphatics and no clear separating fascial plane
• Second, determination of myometrial invasion can be difficult
• uterine recurrences have been reported (2%), but exact location of these recurrences(fundal vs. corpus) have not been stated

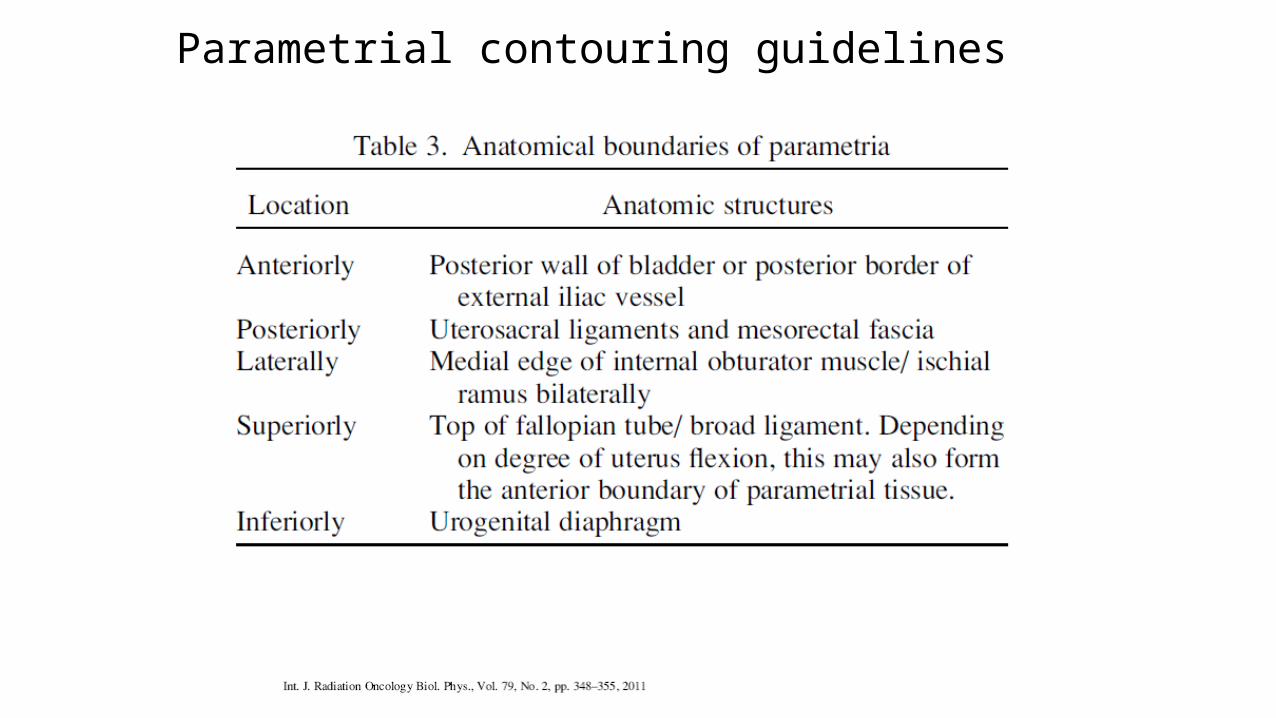
Parametrial contouring guidelines
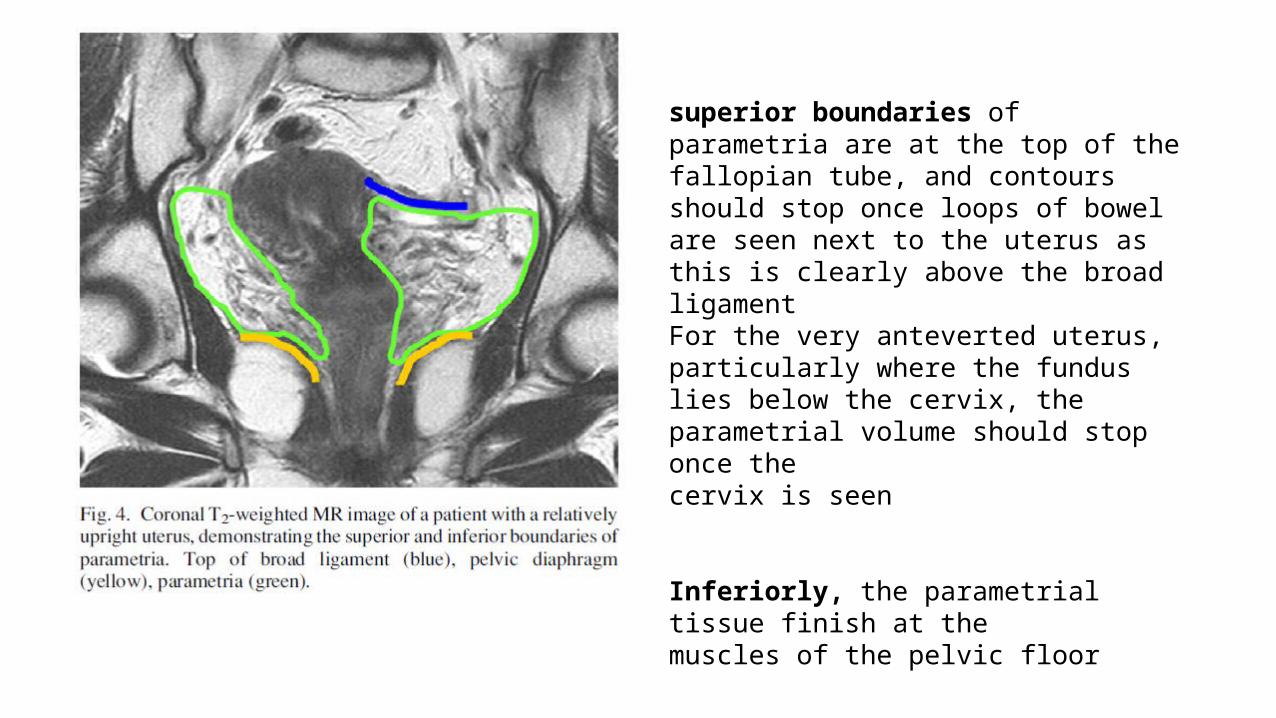
superior boundaries of parametria are at the top of the fallopian tube, and contoursshould stop once loops of bowel are seen next to the uterus as this is clearly above the broad ligamentFor the very anteverted uterus, particularly where the fundus lies below the cervix, the parametrial volume should stop once thecervix is seen
Inferiorly, the parametrial tissue finish at themuscles of the pelvic floor
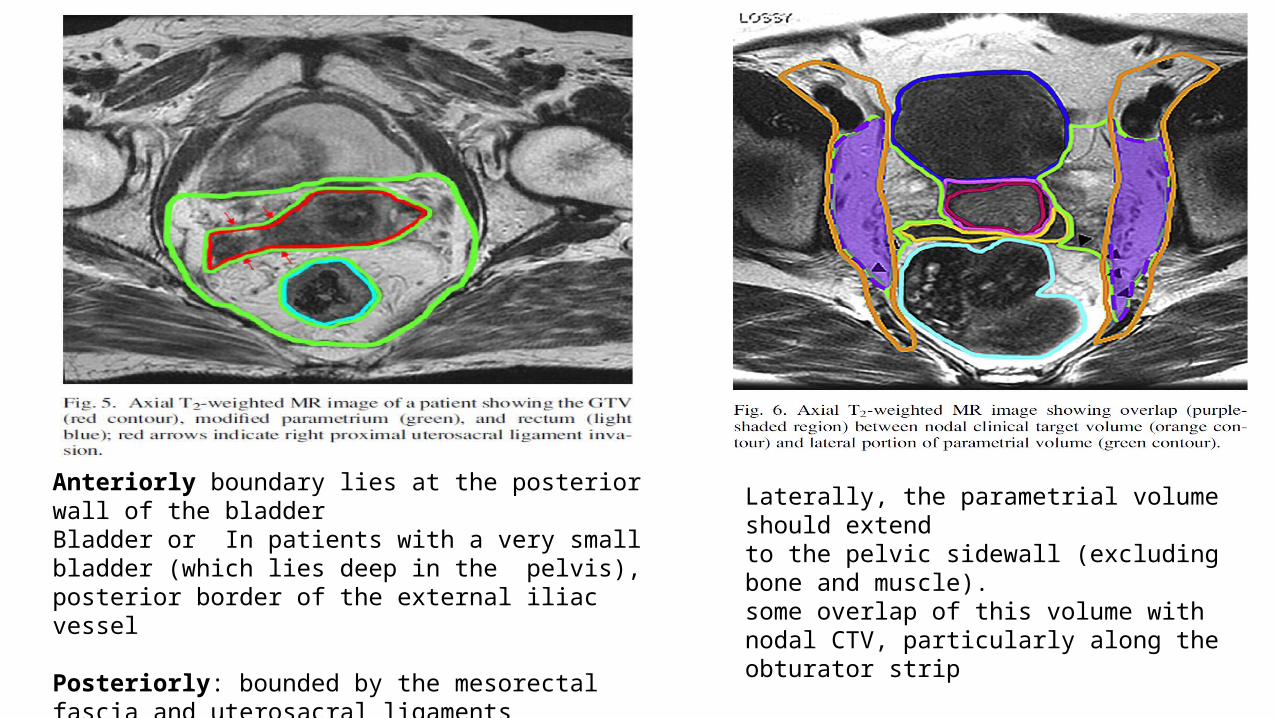
Anteriorly boundary lies at the posterior wall of the bladderBladder or In patients with a very small bladder (which lies deep in the pelvis), posterior border of the external iliac vessel
Posteriorly: bounded by the mesorectal fascia and uterosacral ligamentsparametrial volumes would extend up to the rectal contour in advances stages
Laterally, the parametrial volume should extendto the pelvic sidewall (excluding bone and muscle).some overlap of this volume with nodal CTV, particularly along the obturator strip
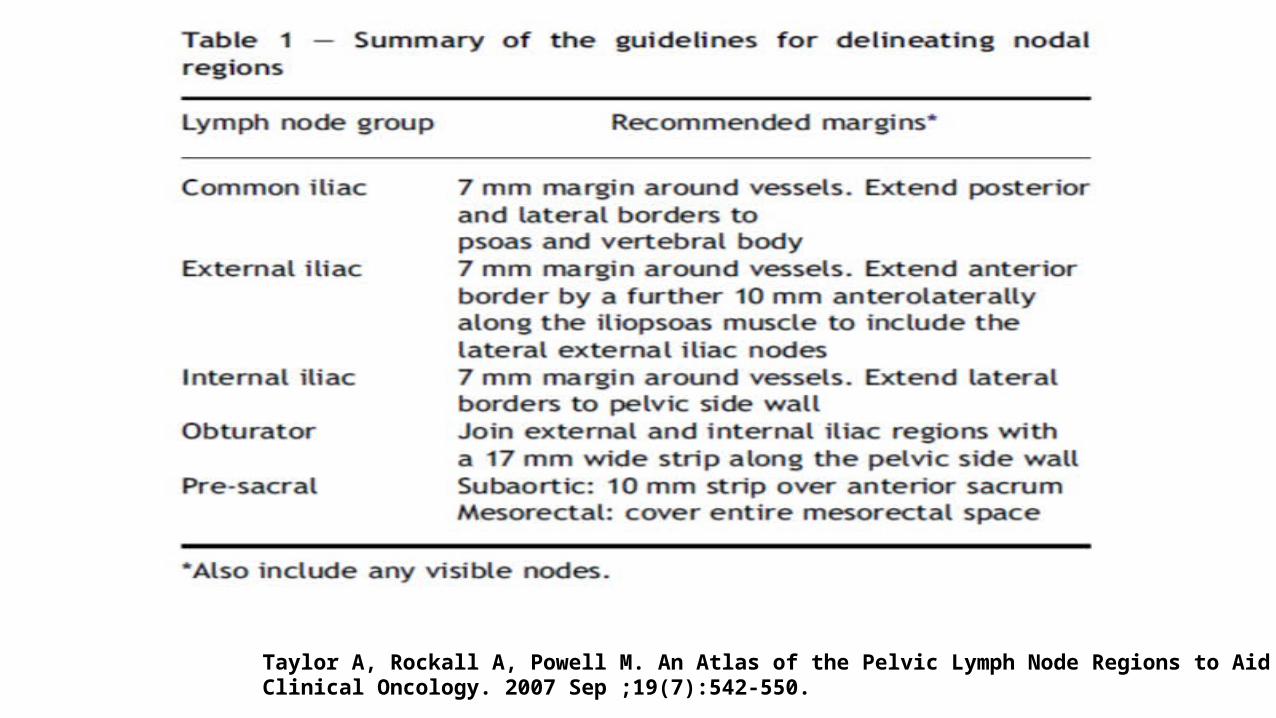
Taylor A, Rockall A, Powell M. An Atlas of the Pelvic Lymph Node Regions to Aid Radiotherapy Target Volume Definition. Clinical Oncology. 2007 Sep ;19(7):542-550.
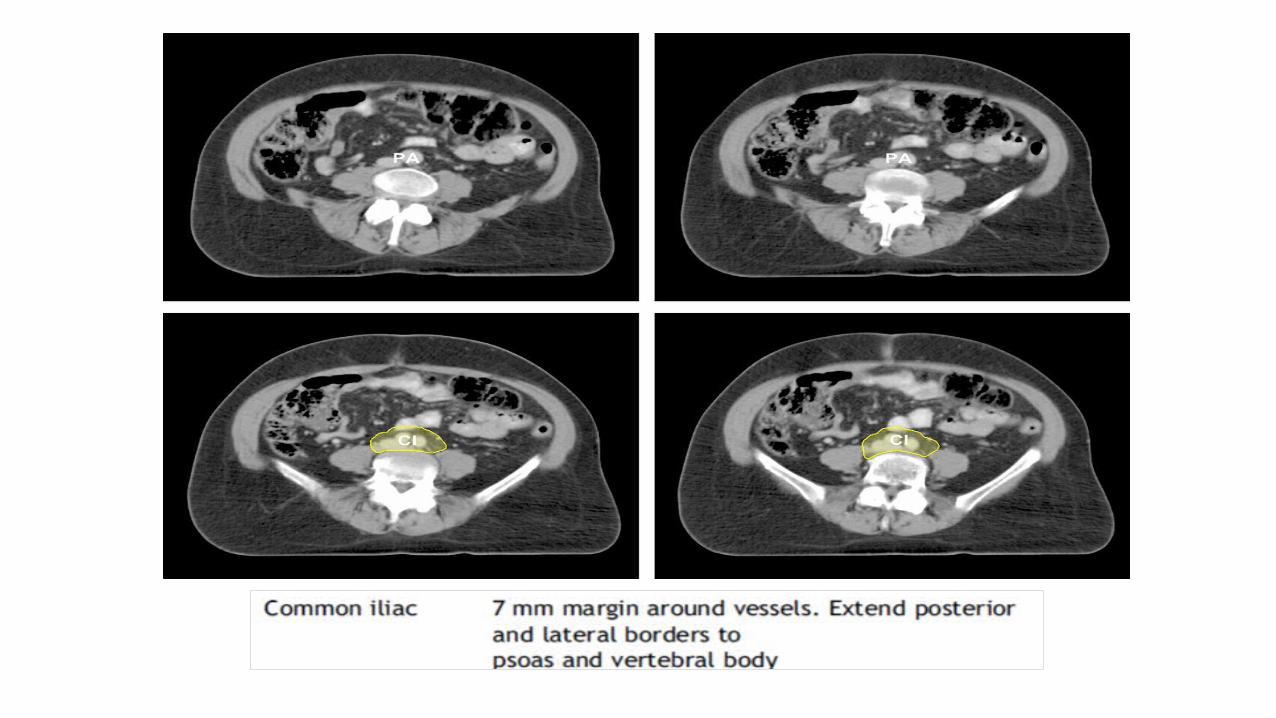
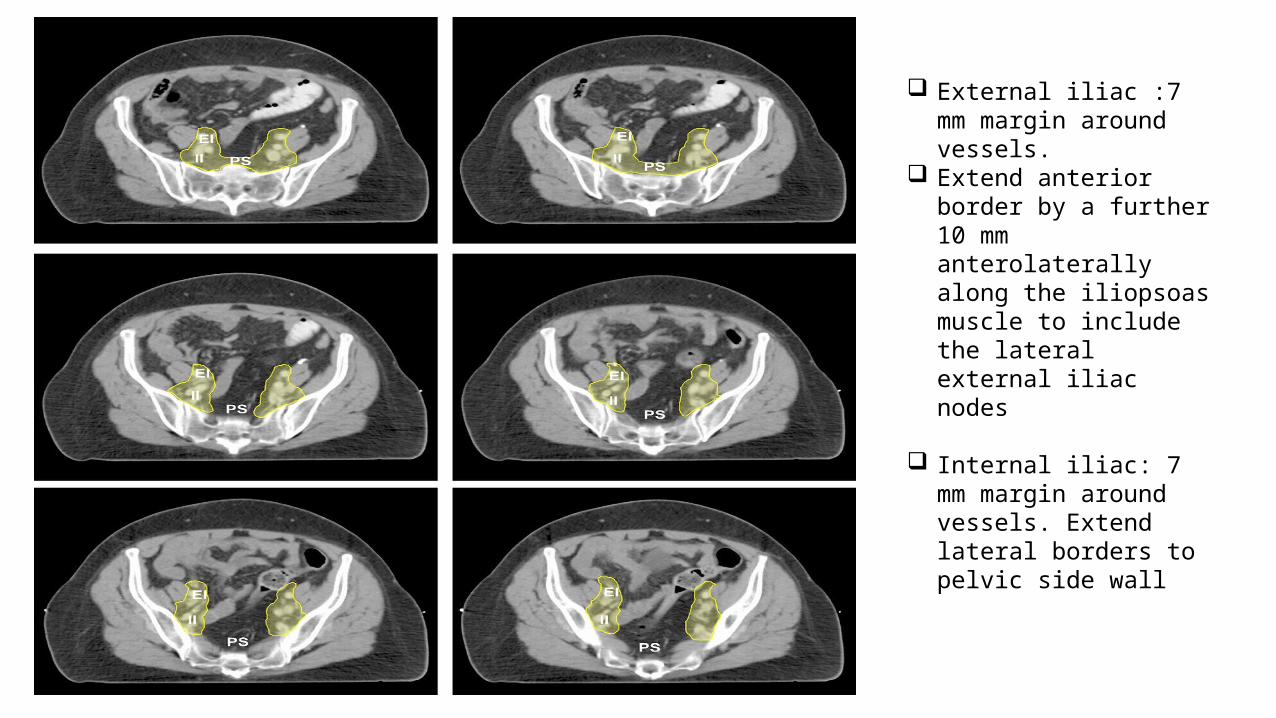
External iliac :7 mm margin around vessels.
Extend anterior border by a further 10 mm anterolaterally along the iliopsoas muscle to include the lateral external iliac nodes
Internal iliac: 7 mm margin around vessels. Extend lateral borders to pelvic side wall

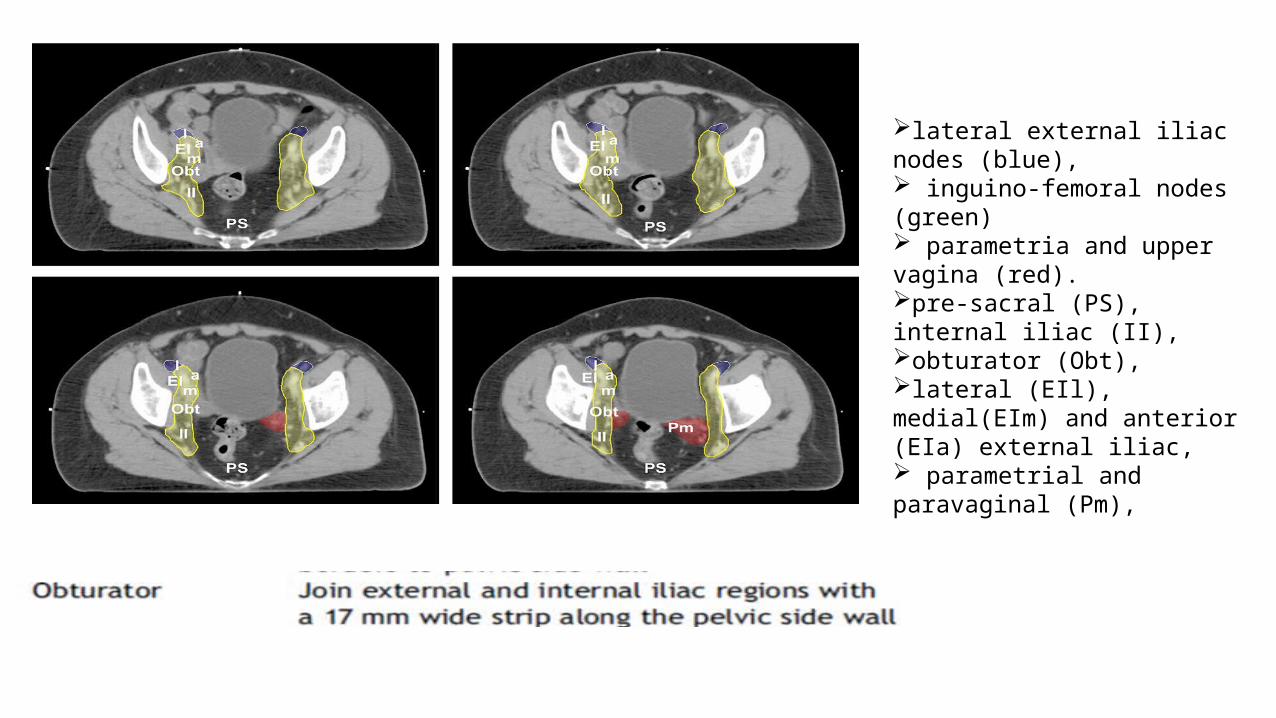
lateral external iliac nodes (blue), inguino-femoral nodes (green) parametria and upper vagina (red).pre-sacral (PS), internal iliac (II), obturator (Obt), lateral (EIl), medial(EIm) and anterior (EIa) external iliac, parametrial and paravaginal (Pm),
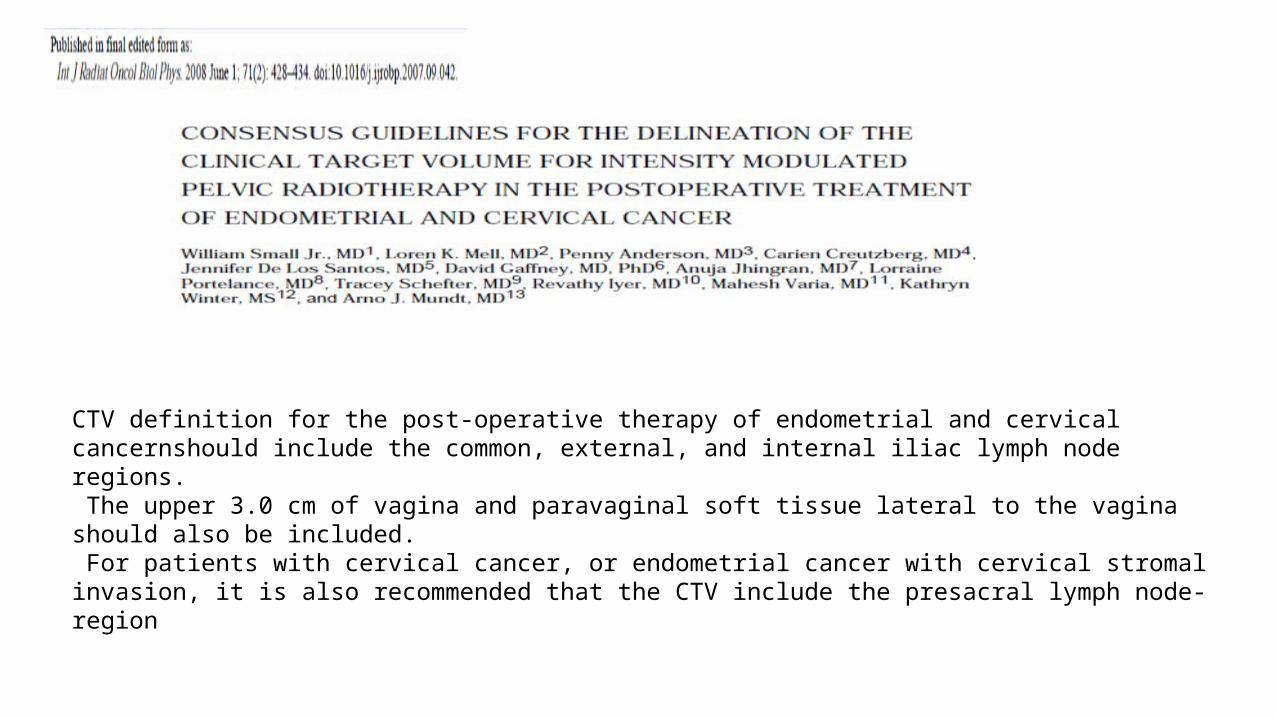
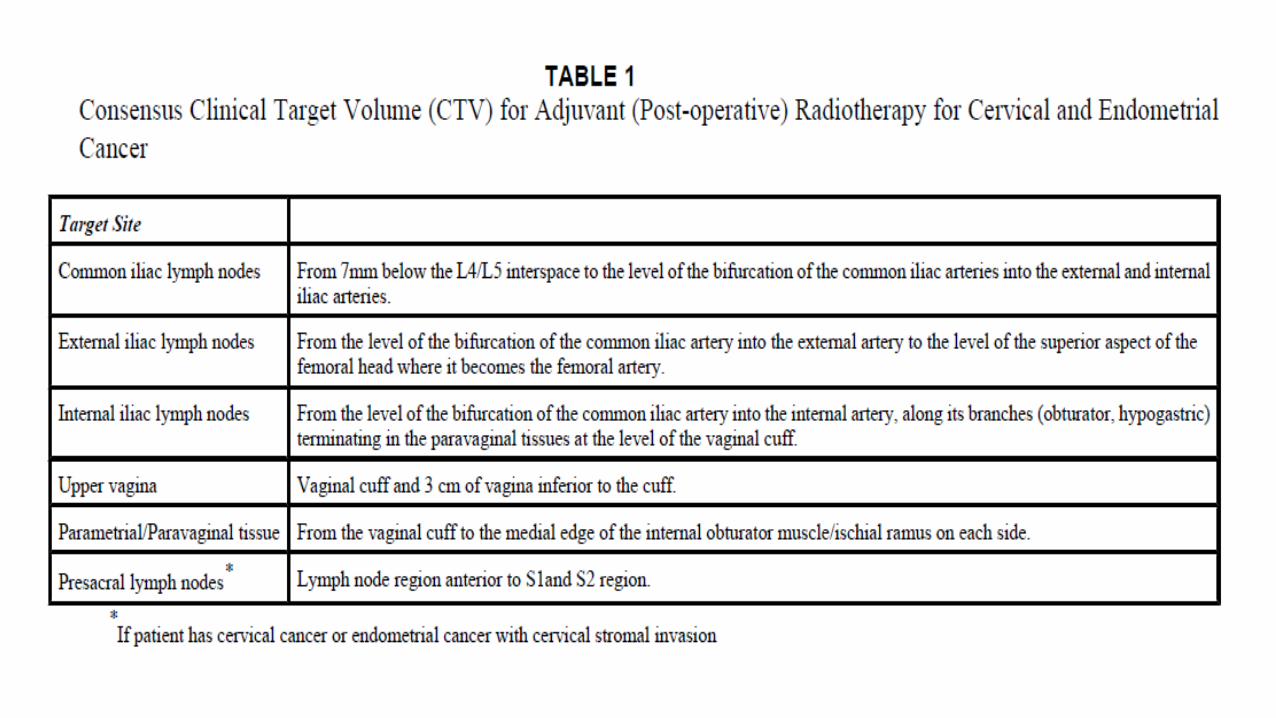
CTV definition for the post-operative therapy of endometrial and cervical cancernshould include the common, external, and internal iliac lymph node regions. The upper 3.0 cm of vagina and paravaginal soft tissue lateral to the vagina should also be included. For patients with cervical cancer, or endometrial cancer with cervical stromal invasion, it is also recommended that the CTV include the presacral lymph node-region

• Upper Common Iliac CTV • Mid CI (red) , Pre-sacral CTV (blue) • Lower C.I (red) ,Pre-sacral CTV (blue)
• Upper El and II (red) PS blue • Parametrial/Vaginal (green) CTV Vaginal CTV
The aim of the article was to review the guidelines for CTV delineation published in the literature and to present the guidelines practiced at their institute
6 articles : 2 articles from Taylor et al and Toita et al and 1 from Small et al., Lim et al., were reviewed
The CTV in cervical cancer consists of the CTV nodal and CTV primary. CTV nodal consists of common iliac, external iliac, internal iliac, pre-sacral and obturator group of lymph nodes, and CTV primary consists of the gross tumor volume, uterine cervix, uterine
corpus, parametrium, upper third of vagina and uterosacral ligaments. Pelvic LN CTV is contoured in accordance with the latest Taylor’s guidelines with some modifications This was the first report to provide the complete set of guidelines for delineating both the CTV
primary and CTV nodal in combination
Normal Tissue Delineation (RTOG)• Bowel: The small and large bowel can be contoured together as a Bowel-Bag.
• Inferiorly, the bowel bag should begin with the first small or large bowel loop or above the ano-rectum, whichever is most inferior.
• The contours should end 1 cm. above the PTV .
• Ano-Rectum: Ano-Rectum should be contoured from the level of the anus to the sigmoid flexure. It should extend from the anal verge (marked by a radiopaque marker at simulation) to superiorly where it loses its round shape in the axial plane and connects anteriorly with the sigmoid.
• Bladder: Contoured inferiorly from its base, and superiorly to the dome.
• Femoral Heads:The ball of the femur, trochanters, and proximal shaft to the level of the bottom of ischial tuberosities
Gay HA, Barthold HJ, O′Meara E, Bosch WR, El Naqa I, Al-Lozi R, et al. Pelvic normal tissue contouring guidelines for radiation therapy: A Radiation Therapy Oncology Group consensus panel atlas. Int J Radiat Oncol Biol Phys 2012;83:e353-62.
Problems with contouring for gynaec cancer
on CT images
• The GTV itself may/ may not be well seen• The parametrial disease is usually not visualized• Though pelvic nodal contouring is systematic, but we still tend to end up
replicating the traditional cranio-caudal boundaries of a 4-field box• MR based guidelines are difficult to implement on CT• It is expensive to do routine MR-based planning• Problems with the availability of MR-based TPS
IMRT in Ca Cervix
• required inverse planning. • modulates the intensity of the beam using the motion of multileaf
collimators.• Computerized software used to conform the dose to the shape of the
target in 3D
Rationale
• Improved delivery of conventional doses• ↓Dose to normal tissues: small bowel, bladder, rectum, marrow• Dose escalation in high risk patients: node positive/gross residual disease• Replacement or integration with Brachytherapy
Potentials of IMRT: as suggested by Dosimetric and small phase 2 studies
For Whole Pelvic Treatments: Reduction in acute small bowel morbidity. Roeske JC, Bonta D, Mell LK, et al. A dosimetric analysis of acute gastrointestinal toxicity in women receiving intensity modulated whole-
pelvic radiation therapy. Radiother Oncol 2003;69:201-207
Prevention of late term anorectal/ GI and GU dysfunction. Mundt AJ, Mell LK, Roeske JC, et al. Preliminary analysis of chronic gastrointestinal toxicity in gynecology patients treated with
intensitymodulated whole pelvic radiation therapyIJROBP 2003;56:1354-1360.
Reduction in acute hematological toxicity with bone marrow sparing. Lujan AE, Mundt AJ, Yamada SD, et al. Intensity-modulated radiotherapy as a means of reducing dose to bone marrow in gynecologic
patients receiving whole pelvic radiotherapy. IJROBP 2003;57:516-521.
For simultaneous extended field irradiation (± CCT). Salama JK, Mundt AJ, Roeske J, Mehta N. Preliminary outcome and toxicity report of extended-field, intensity-modulated radiation therapy
for gynecologic malignancies. International Journal of Radiation Oncology*Biology*Physics. 2006 Jul 15;65(4):1170-1176.
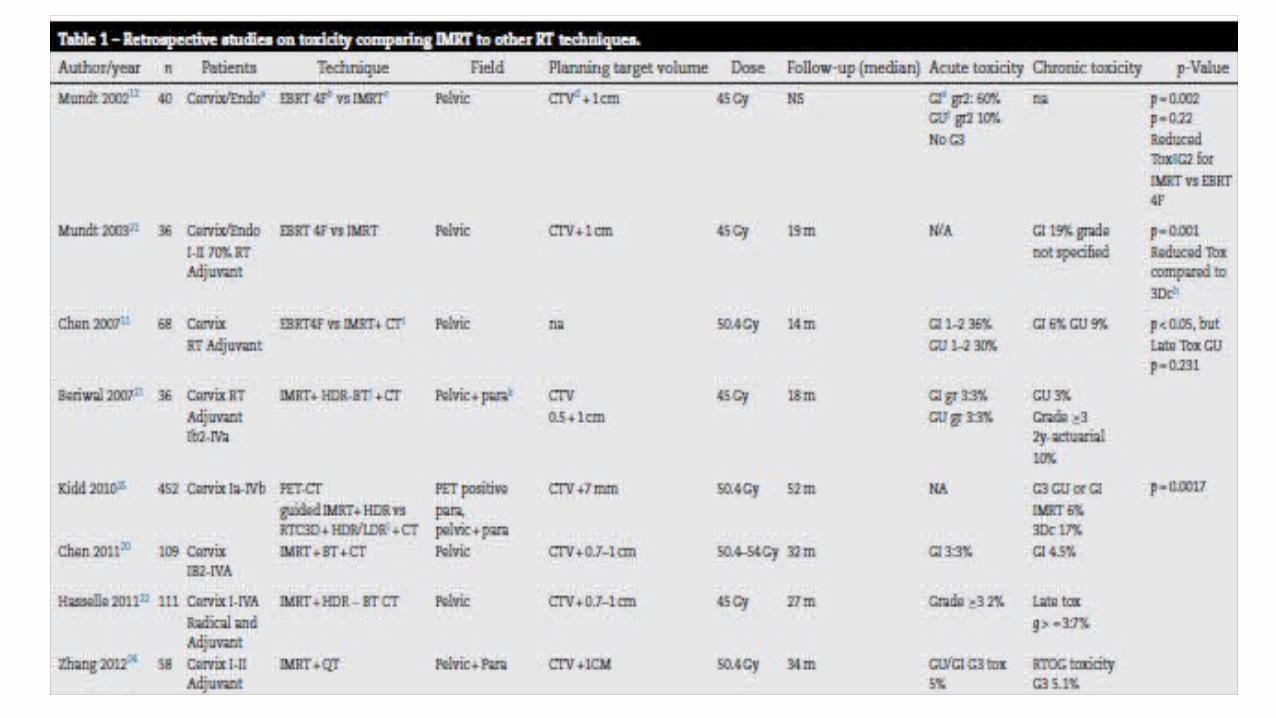
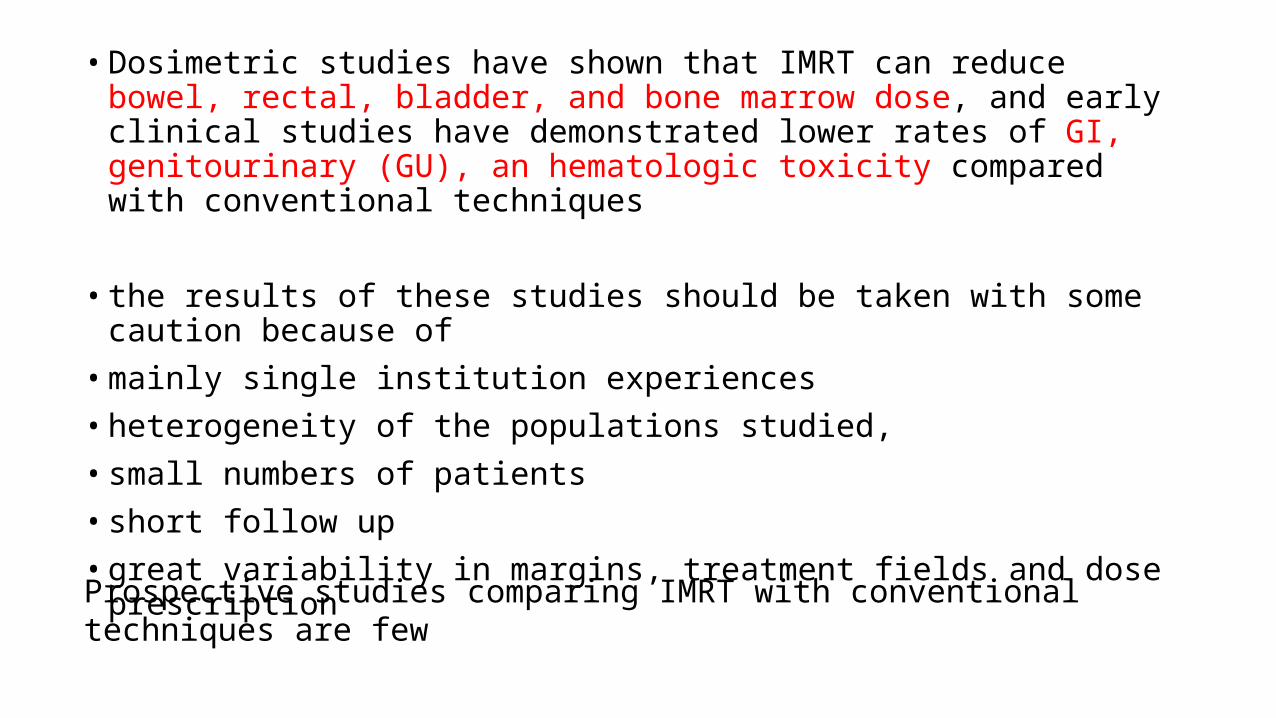
• Dosimetric studies have shown that IMRT can reduce bowel, rectal, bladder, and bone marrow dose, and early clinical studies have demonstrated lower rates of GI, genitourinary (GU), an hematologic toxicity compared with conventional techniques
• the results of these studies should be taken with some caution because of• mainly single institution experiences• heterogeneity of the populations studied, • small numbers of patients• short follow up• great variability in margins, treatment fields and dose prescription
Prospective studies comparing IMRT with conventional techniques are few
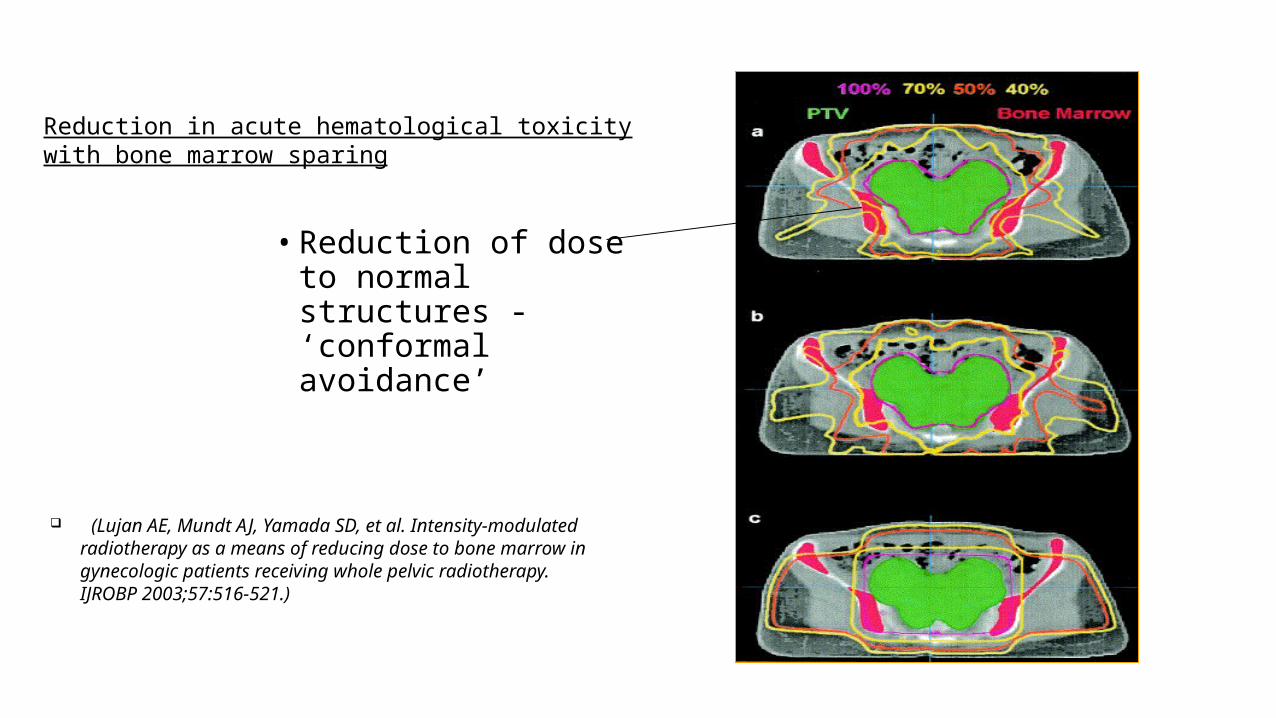
• Reduction of dose to normal structures - ‘conformal avoidance’
(Lujan AE, Mundt AJ, Yamada SD, et al. Intensity-modulated radiotherapy as a means of reducing dose to bone marrow in gynecologic patients receiving whole pelvic radiotherapy. IJROBP 2003;57:516-521.)
Reduction in acute hematological toxicity with bone marrow sparing
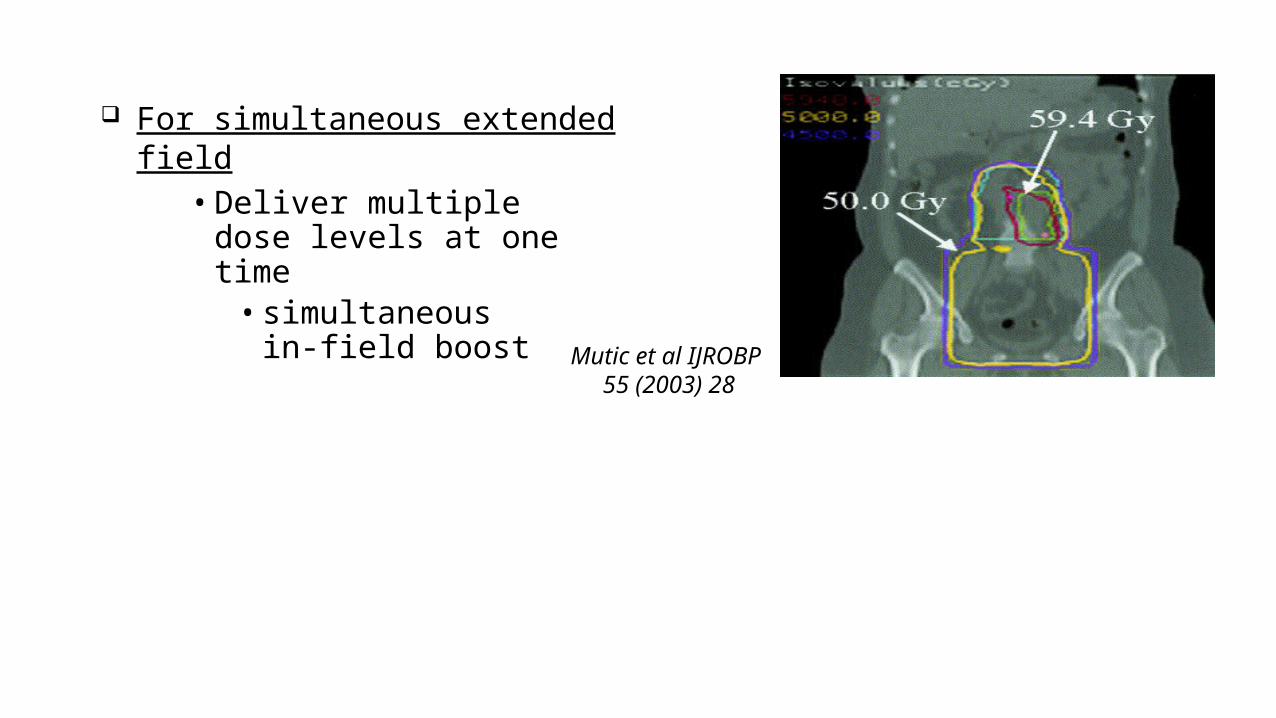
• Deliver multiple dose levels at one time
• simultaneous in-field boost
Mutic et al IJROBP 55 (2003) 28
For simultaneous extended field
As an alternative to brachytherapy: In distorted anatomy to circumvent limitations of brachytherapy. To give higher dose to pelvic nodes present In postoperative patients with residual central disease instead of interstitial
brachytherapy.
Suggested Potentials of IMRT
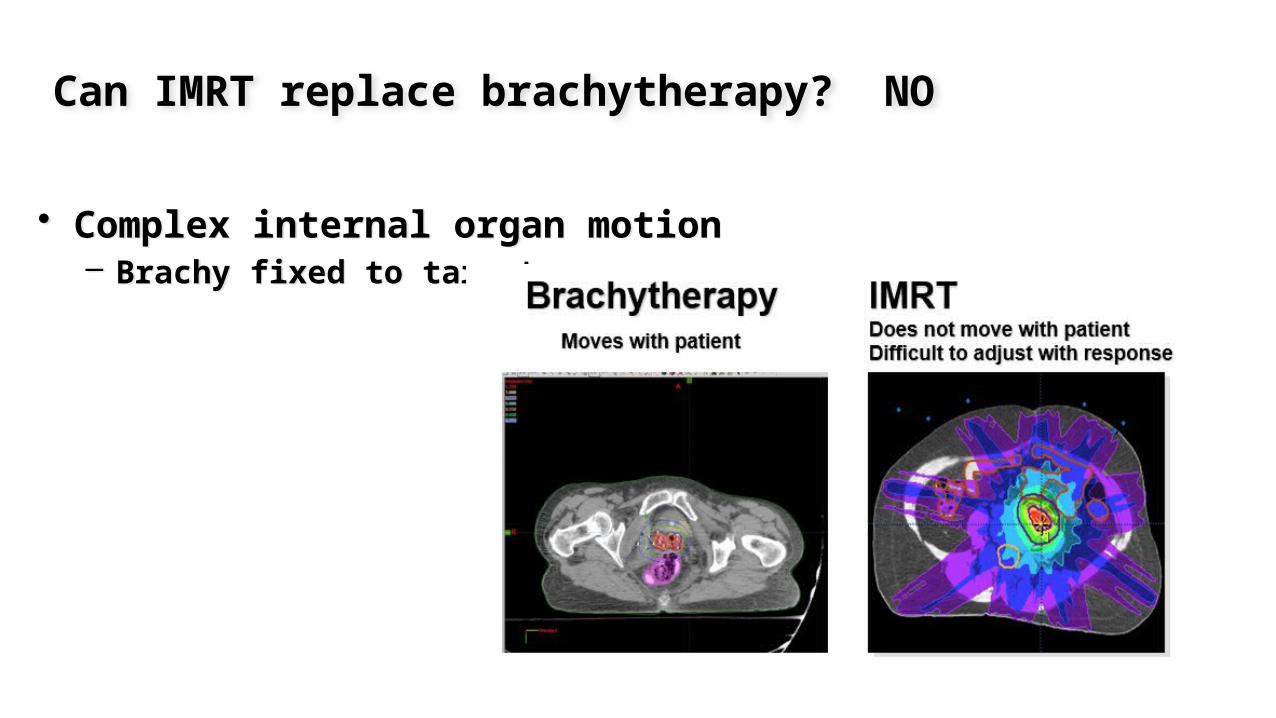
Can IMRT replace brachytherapy? NO
• Complex internal organ motion– Brachy fixed to target
• Complex internal organ motion– Brachy fixed to target
After 45 Gy EBRT


Brachytherapy 12 (2013) 311e316
aimed to compare the dosimetry achieved by IBT and IMRT in patients not suitable for ICRT
Results of study have shown that IBT provides superior dosimetry as compared with IMRT; and, therefore, IBT,as of now, remains the standard treatment for patients with cervical carcinoma who are not suitable for ICRT
MATERIALS: The CT imaging data, previously used for IBT planning of12 patients with cervical carcinoma, were transferred to IMRT planning system to generate parallelIMRT plans. Prescribed dose to the planning target volume (PTV) was 20 Gy delivered in 2-weekly high-dose-rate fractions of 10 Gy each with IBT (biologically equivalent dose [BED10] 40 Gy) and 33 Gy/13 fractions/2.5 wk with IMRT (BED10 41 Gy.
RESULTS: For PTV, the meanD95 (dose received by 95% of PTV) was better with IBT (57.16 Gy vs. 41.47 Gy, p50.003). The mean conformity index was 0.94 and 0.90 with IBT and IMRT, respectively ( p50.034). IBT delivered significantly reduced doses to bladder and rectal volume as compared with IMRT.
Imrt in post op setting: need for small bowel dose reduction
Conventional 4 field technique exposes most of the contents of the true pelvis to the prescribed dose (usually 45-50 Gy in 25-28 fractions).
This is of concern in post-op pts. since after hysterectomy, small bowel tends to fall into the vacated space in the true pelvis, increasing the amount of bowel treated to high dose.
It increases the risk of acute and late small bowel complications The major potential advantage of IMRT in the postoperative setting, is the ability to
shape a dose distribution that delivers a lower dose to intraperitoneal pelvic contents (i.e., small and large bowel) than to the surrounding pelvic lymph nodes.
This should make it possible to reduce the acute and late side effects of treatment
• IMRT reduces small bowel dose by 50–67% as compared with conventional WPRT• Prospective studies evaluating IMRT have demonstrated 30% reduction in acute
grade II toxicity and upto 30% reduction in the prescription of antidiarrhoeals Portelance L, et al. Post-operative pelvic IMRT with chemotherapy for patients with cervical carcinoma/RTOG 0418 phase II study.
IJROBP 2009;75:S640–1.
Schwarz JK, Wahab S, Grigsby PW. Prospective phase I/II trial of helical tomotherapy with or without chemotherapy for postoperative cervical cancer patients IJROBP2009;81:1258–63.
Kabarriti R, Thawani N, Gao W, et al. Feasibility and acute toxicity of intensity modulated radiation therapy with CDDP chemotherapy for postoperative pelvic radiation in patients with cervical cancer. IJROBP 2009;75:S376–7.
Vandecasteele K, Tummers P, Makar A, et al. Postoperative intensity modulated arc therapy for cervical and endometrial cancers: a prospective report on toxicity. IJROBP 2012;84:408–14.
Mundt AJ, Roeske JC. Can intensity-modulated radiation therapy replace brachytherapy in the management of cervical cancer? Counterpoint. Brachytherapy 2002;1:192–4.
phase II studies have reported favourable outcomes with the use of IMRTResults of RTOG 0418 and study from TMH Mumbai awaited
IMRT in intact cervix: problems
• adequate margins in the intact cervix setting is debatable given significant organ motion during treatment.
• Uncertainties in the definition of target volumes arise using 3D techniques.
• Bladder-filling and rectal-filling changes require accurate definition of margins for the PTV.
• With IMRT, there is a need for continual replanning (at least every other week), given rapid tumor regression and internal-organ motion.
• To evaluate the toxicity and clinical outcome in patients with LACC treated with WP-CRT versus WP-IMRT
• METHODS AND MATERIALS:• Between January 2010 and January 2012, • 44 patients with (FIGO 2009) stage IIB-IIIB SCC cervix randomized to receive 50.4 Gy in 28 fractions delivered
via either WP-CRT or WP-IMRT with concurrent weekly cisplatin 40 mg/m2 followed by high-dose-rate HDR) IICRT, 7 Gy to point A in 3 once-weekly sessions
• In patients deemed unsuitable for ICRT, interstitial brachytherapy (IBT) 10 Gy in 2 once-weekly sessions based on our previous experience
• Acute toxicity : graded according to the CTCAE version 3.0• Late toxicity: graded according to RTOG• Primary end point :acute gastrointestinal toxicity• secondary endpoints: disease-free survival
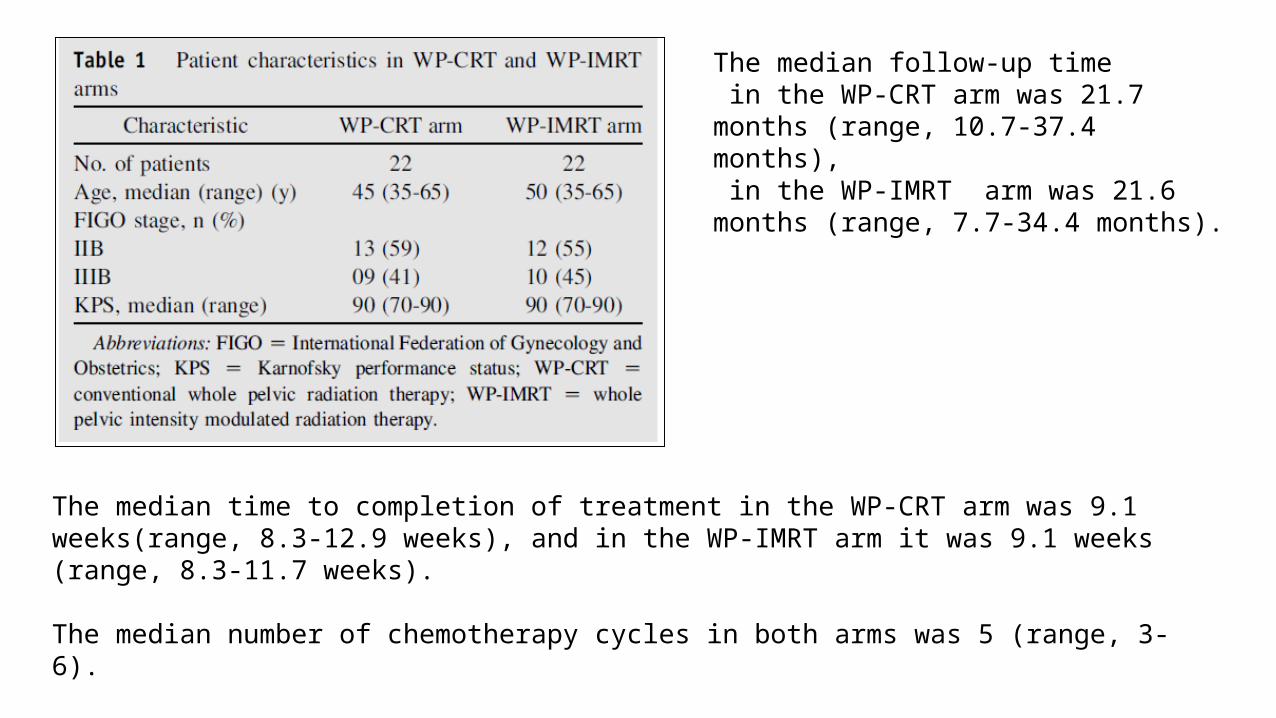
The median time to completion of treatment in the WP-CRT arm was 9.1 weeks(range, 8.3-12.9 weeks), and in the WP-IMRT arm it was 9.1 weeks (range, 8.3-11.7 weeks).
The median number of chemotherapy cycles in both arms was 5 (range, 3-6).
The median follow-up time in the WP-CRT arm was 21.7 months (range, 10.7-37.4 months), in the WP-IMRT arm was 21.6 months (range, 7.7-34.4 months).

RESULTS
Patients in the WP-IMRT arm experienced significantly fewer grade ≥2 acute gastrointestinal toxicities (31.8% vs 63.6%, P=.034) and grade ≥3 gastrointestinal toxicities (4.5% vs 27.3%, P=.047) than did patients receiving WP-CRT

RESULTS:
At 27 months, disease-free survival was 79.4% in the WP-CRT group versus 60% in the WP-IMRT group (P=.651)overall survival was 76% in the WP-CRT group versus 85.7% in the WP-IMRT group (P=.645).
CONCLUSION:
WP-IMRT is associated with significantly less toxicity compared with WP-CRT and has a comparable clinical outcome.
LIMITATION: small sample sizes and short follow-up times.no use of image guidance
Caveats of IMRTSignificantly increased expenditure:
Machine with treatment capability Imaging equipment: Planning and Verification Software and Computer hardware
Extensive physics manpower and time required.
Immobilization: Patient setup must be accurate and reproducibleContouring: Need accurate contouring to avoid misses.Knowledge of Internal Motion: Margins could vary greatly depending on organ motion
Concerns with integral dose and secondary malignancy
RADIATION SIDE EFFECTS
•Acute Side Effects:
Acute gastrointestinal side effects: include diarrhea, abdominal cramping, rectal discomfort, and occasionally, rectal bleeding, which may be caused by transient enteroproctitis.
• Genitourinary symptoms:secondary to cystourethritis, are dysuria, frequency, and nocturia,microscopic or even gross hematuria..
• Skin reactions: erythema and dry or moist desquamation may develop in the perineum or intergluteal fold.
• acute radiation vaginitis, superficial ulceration of the vagina, and vagianl stenosis can also occur

• Late Side Effects:
Late radiation effects are closely related to total doses given to the pelvic organs.• Retrovaginal or vesicovaginal fistula and proctitis or cystitis can occur but in small
percentages.• Injury to the gastrointestinal tract usually appears within 2 years of radiation
therapy• Complications of the urinary tract more frequently are seen 3- 4 years after
treatment.• Vaginal stenosis is associated with dyspareunia• Anal incontinence is observed occasionally
Thank you




![Unusual Metastasis from Carcinoma Cervix · Carcinoma cervix is the most prevalent malignancy in Indian women with incidence of about 19–44 per 100,000 women [3]. The standard treatment](https://img.dokumen.tips/doc/110x75/5f704683f3e5dc1d486aa6c3/unusual-metastasis-from-carcinoma-cervix-carcinoma-cervix-is-the-most-prevalent.jpg)