Embed Size (px)
Citation preview

Master Degree in Medical Biotechnologies
INTERNAL MEDECINE
DIABETES: THE BIOLOGICAL BASES OF TREATMENT

DIABETES
DEFINITION: heterogeneous group of metabolic disorders that share the phenotype of hyperglycemia
EPIDEMIOLOGY: diabetes prevalence is increasing worldwide, it is similar in males and females and it is related with age:
• age < 20 years prevalence 0.19%
• age > 20 years prevalence 8.6%
• age > 65 years prevalence 20.1%
HEALTHCARE IMPACT: diabetes is the main cause of renal failure, limbs amputation and blindness in adults (USA epidemiologic data)

CLASSIFICATION
Type 1 Diabetes is characterized by insufficient insulin secretion due to the loss of beta cells in Langherans Islets
• autoimmune (tipo IA)
• idiopathic (tipo IB)
Type 2 Diabetes is characterized by insulin resistence
• congenital (very uncommon)
• idiopathic (common, adult-onset, related with obesity and metabolic syndrome).
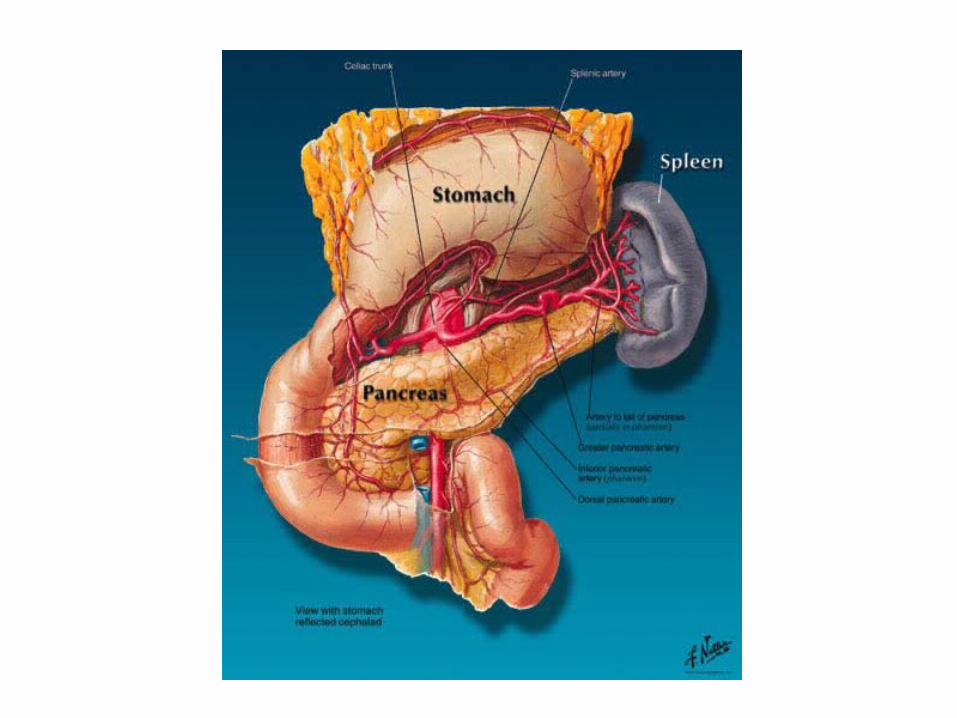



INSULIN
• Insulin is syntetized by b cells into the Langerhans islets (endocrine pancreas); from the polypeptidic precursor, consisting of a single chain of 86 aa, the preproinsulin, through a proteolytic process, we obtain the proinsulin and from this, for detachment of an internal peptide of 31 aa, called C-peptide, insulin is obtained. The active hormone is formed by two amino acid chains of 21 and 30 aa, called A and B chain respectively, joined together by disulfide bridges
• Insulin is a small protein (PM 6 kDa) that is stored in the cytoplasm of b cells within secretory vescicles
• Insulin secretion is stimulated by: plasma glucose concentration, gastrin, GP-1, VIP, aa, vagus nerve.
• Insulin secretion is Ca2+ dependent and it is strictly dependent also by ATP intracellular concentration
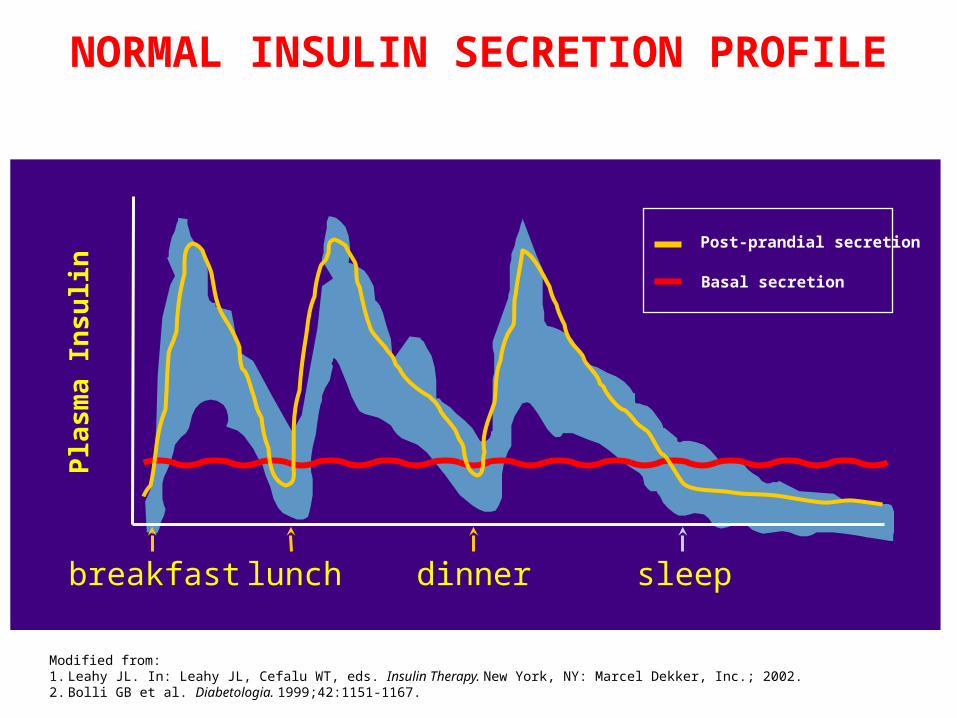
• Insulin secretion shows a pulsatile profile with small peaks, that occur every 10 minutes, and large peaks, lasting 2-3 hours, induced by meals.
COUNTER-REGULATION OF INSULIN SECRETION
Insulin secretion is inhibited when plasma glucose concentration is lower than 70 mg/dL
In addition to direct control exerted by plasma glucose there are several hormones that antagonize insulin:
• GLUCAGON (secreted by alpha cells in pancreas islet)
• CATECHOLAMINES
• CORTISOL
breakfast dinnerlunch sleep
Pla
sma
Insu
lin
Modified from:1. Leahy JL. In: Leahy JL, Cefalu WT, eds. Insulin Therapy. New York, NY: Marcel Dekker, Inc.; 2002.2. Bolli GB et al. Diabetologia. 1999;42:1151-1167.
Basal secretion
Post-prandial secretion
NORMAL INSULIN SECRETION PROFILE

INSULIN BIOSYNTESIS

INSULIN STRUCTURE
A-chain
B-chain

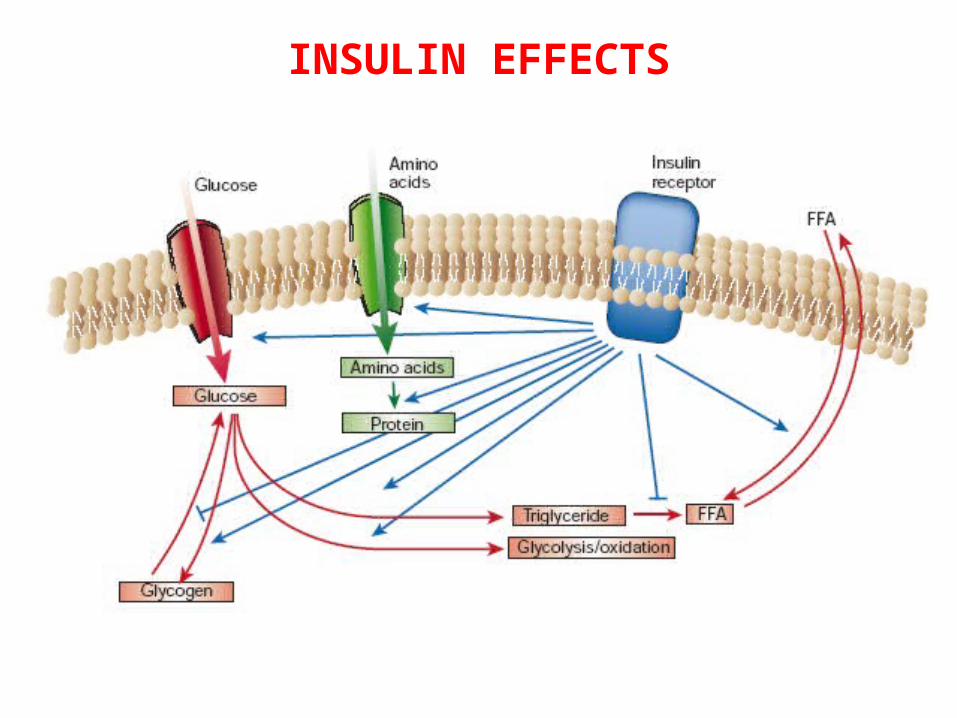
INSULIN EFFECTS
ANABOLIC EFFECT: Insulin determines internalization into cells of glucose, FFA and aa, it activates enzymes involved in glycogen synthesis, TG and proteins. Finally insulin inhibits enzymes that degrade themLIVER: Insulin increases glycogen, inhibits gluconeogenesis, glycogenolysis, b-oxidation of fatty acids and ketogenesisMUSCLE: Insulin increases the synthesis of insulin-dependent glucose transporters (Glut-4) and induces its translocation to the cell membrane, induces glycogen synthesis, inhibits glycogenolysis.ADIPOSE TISSUE: stimulates the storage of FFA in the form of triglycerides, inhibits the hormone-sensitive lipase causing block of hydrolysis of TG and fall of glycerol and FFA plasma concentrations.
INSULIN EFFECTS

GLUCOSE HOMEOSTASIS

Date of download: 3/5/2015 Copyright © 2015 McGraw-Hill Education. All rights reserved.
Mechanisms of glucose-stimulated insulin secretion and abnormalities in diabetes. Glucose and other nutrients regulate insulin secretion by the pancreatic beta cell. Glucose is transported by a glucose transporter (GLUT1 in humans, GLUT2 in rodents); subsequent glucose metabolism by the beta cell alters ion channel activity, leading to insulin secretion. The SUR receptor is the binding site for some drugs that act as insulin secretagogues. Mutations in the events or proteins underlined are a cause of maturity-onset diabetes of the young (MODY) or other forms of diabetes. SUR, sulfonylurea receptor; ATP, adenosine triphosphate; ADP, adenosine diphosphate, cAMP, cyclic adenosine monophosphate. IAPP, islet amyloid polypeptide or amylin.
Legend:
INSULIN SECRETION
From: Chapter 344. Diabetes Mellitus
Harrison's Principles of Internal Medicine, 18e, 2012
From: Chapter 344. Diabetes Mellitus
Harrison's Principles of Internal Medicine, 18e, 2012
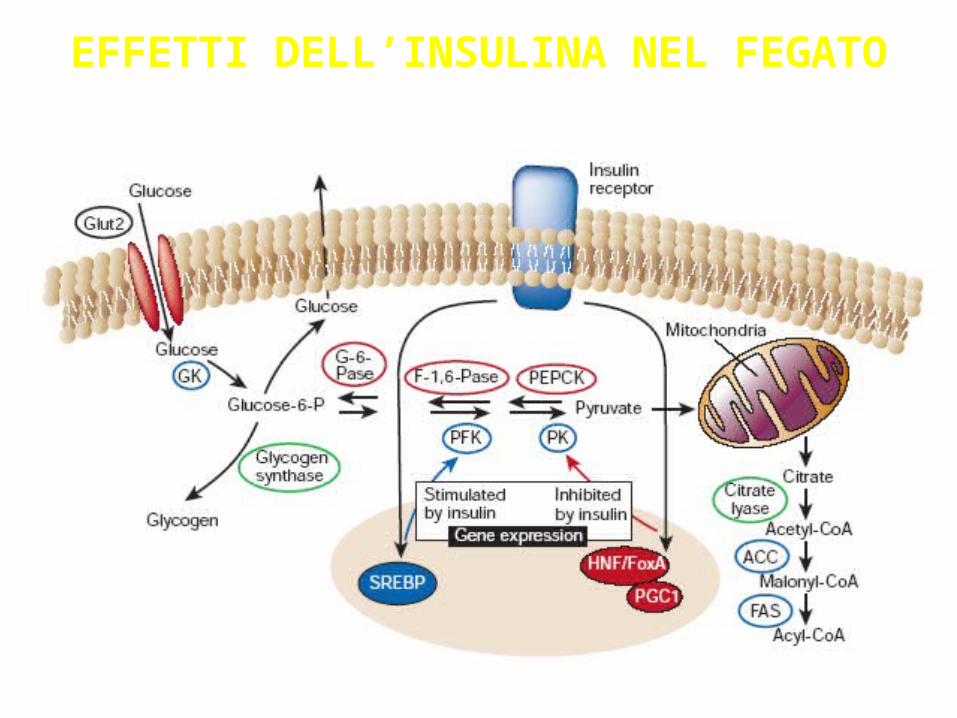
EFFETTI DELL’INSULINA NEL FEGATO
Date of download: 3/5/2015 Copyright © 2015 McGraw-Hill Education. All rights reserved.
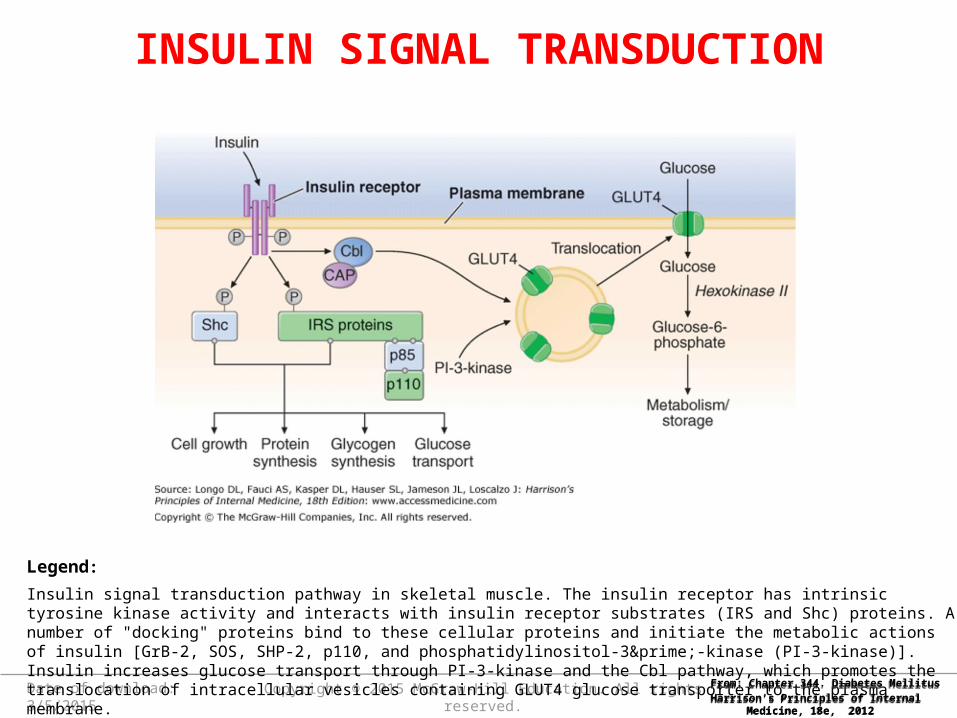
Insulin signal transduction pathway in skeletal muscle. The insulin receptor has intrinsic tyrosine kinase activity and interacts with insulin receptor substrates (IRS and Shc) proteins. A number of "docking" proteins bind to these cellular proteins and initiate the metabolic actions of insulin [GrB-2, SOS, SHP-2, p110, and phosphatidylinositol-3′-kinase (PI-3-kinase)]. Insulin increases glucose transport through PI-3-kinase and the Cbl pathway, which promotes the translocation of intracellular vesicles containing GLUT4 glucose transporter to the plasma membrane.
Legend:
INSULIN SIGNAL TRANSDUCTION
From: Chapter 344. Diabetes Mellitus
Harrison's Principles of Internal Medicine, 18e, 2012
From: Chapter 344. Diabetes Mellitus
Harrison's Principles of Internal Medicine, 18e, 2012
INSULIN RESISTANCE
• is defined as the decreased ability of insulin to act effectively on target tissues (especially muscle, liver, and fat)
• is a prominent feature of type 2 DM and results from a combination of genetic susceptibility and obesity.
• Insulin resistance may remain silent for a long time, since supranormal levels of circulating insulin will normalize the plasma glucose.
• Insulin resistance impairs glucose utilization by insulin-sensitive tissues and increases hepatic glucose output; both effects contribute to the hyperglycemia
• Insulin resistance and abnormal insulin secretion are central to the development of type 2 DM.
• Insulin resistance precedes an insulin secretory defect but diabetes develops only when insulin secretion becomes inadequate.
• Type 2 DM is polygenic and multifactorial, since in addition to genetic susceptibility, environmental factors modulate the phenotype.
• The genes that predispose to type 2 DM are incompletely identified, but recent genome-wide association studies have identified a large number of genes involved; the most prominent is a variant of the transcription factor 7–like 2 gene
• Genetic polymorphisms associated with type 2 diabetes have also been found in the genes encoding the peroxisome proliferators–activated receptor-γ, potassium channel, zinc transporter, IRS, and calpain 10.
TYPE 2 DIABETES MELLITUS
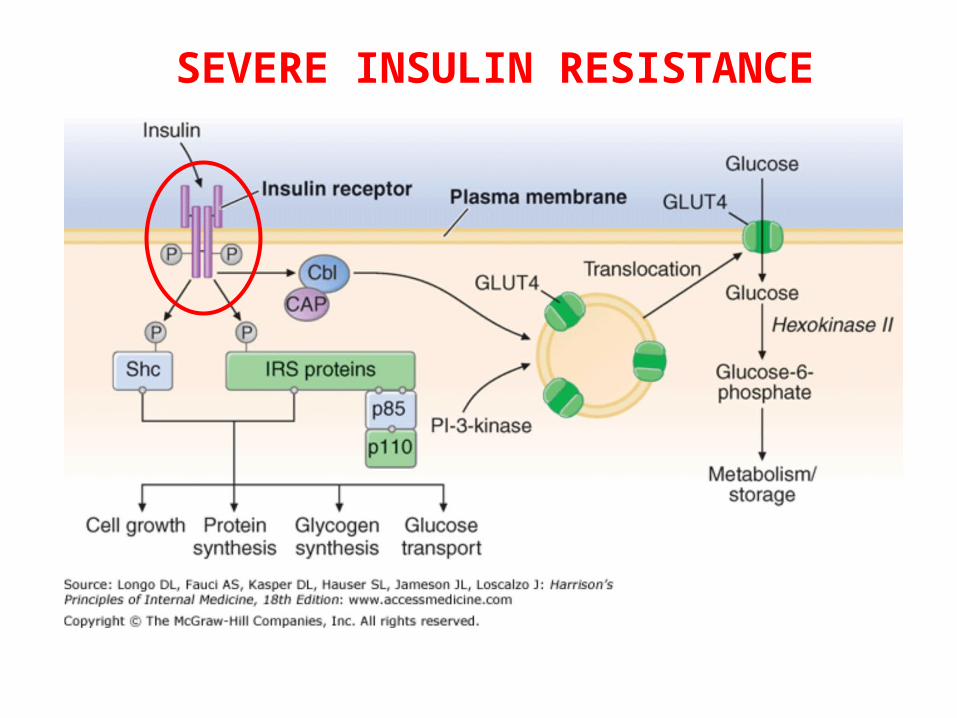
SEVERE INSULIN RESISTANCE

OTHER MECHANISMS OF INSULIN RESISTANCE

OBESITY AND INSULIN RESISTANCE
• Adipocytes secrete a number of biologic products (nonesterified free fatty acids, retinol-binding protein 4, leptin, TNF-α, resistin, and adiponectin)
• Adipokines modulate insulin sensitivity.
• The increased production of free fatty acids and some adipokines may cause insulin resistance in skeletal muscle and liver.
• Free fatty acids impair glucose utilization in skeletal muscle, promote glucose production by the liver, and impair beta cell function.
• In contrast, the production by adipocytes of adiponectin, an insulin-sensitizing peptide, is reduced in obesity.and this may contribute to hepatic insulin resistance.
• Adipocyte products and adipokines also produce an inflammatory state and may explain why markers of inflammation such as IL-6 and C-reactive protein are often elevated in type 2 DM.
• In addition, inflammatory cells have been found infiltrating
adipose tissue. Inhibition of inflammatory signaling pathways such as the nuclear factor κB (NF-κB) pathway appears to reduce insulin resistance and improve hyper-glycemia in animal models.
OBESITY AND INFLAMMATION
DEVELOPMENT OF DRUGS FOR THE TREATMENT OF DIABETES
MELLITUS
1. Drugs that sensitize the body to insulin and/or control hepatic glucose production
2. Drugs that stimulate the pancreas to make more insulin
3. Drugs that slow the absorption of starches
ThiazolidinedionesBiguanides
SulfonylureasMeglitinides
Alpha-glucosidase inhibitors
MAJOR CLASSES OF MEDICATIONS
NEW DRUGS
• INCRETINS

SULFONYLUREAS

THIAZOLIDINEDIONES
• PPAR- g nuclear receptor agonists (peroxisome proliferator-activated receptor )g
They increase the FFA storage in adipose tissue reducing their circulating concentration
induce expression on the cell membrane and translocation of Glut-4
reduce the adipocytes TNF- a release

In healthy subjects an oral glucose load stimulates an higher insulin release (3-4 fold) with respect to iv administration of the same amount of glucose. This “incretin effect” is impaired in patients with Type 2 diabetes.
INCRETIN EFFECT

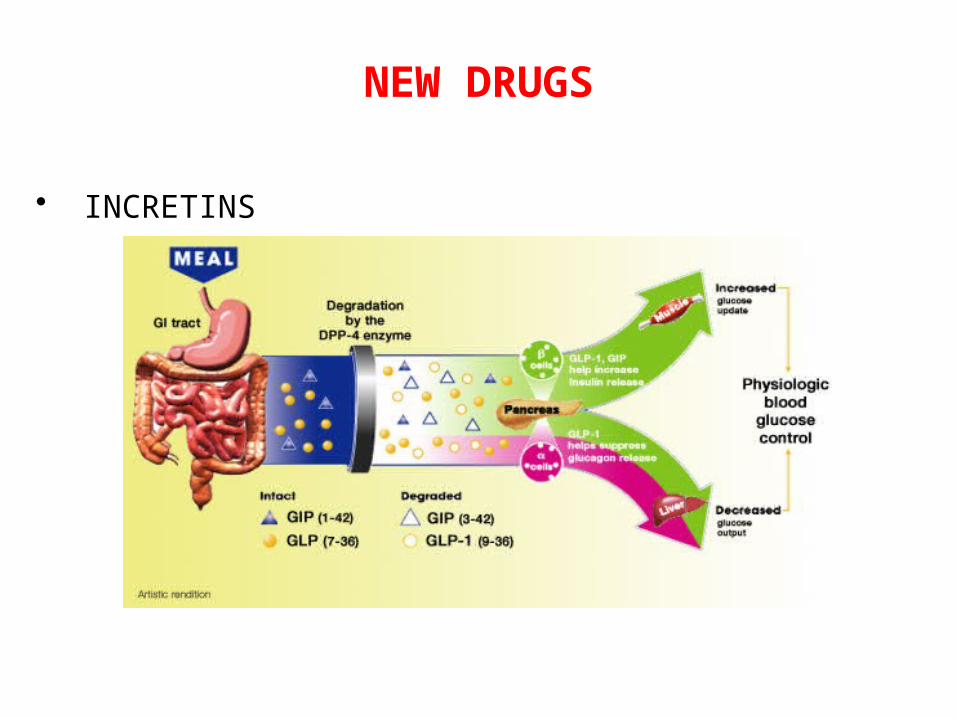
GLP-1 and GIP are the two major incretin hormones found in humans.These incretins are released from the gut in response to ingestion of food and collectively contribute to glucose control by: Stimulating glucose-dependent insulin release from
pancreatic beta cells (GLP-1 and GIP); insulin increases glucose uptake in peripheral tissues (mainly muscle and fat) and suppresses glucose production from the liver.
Decreasing glucagon production from pancreatic alpha cells (GLP-1) when glucose levels are elevated.
INCRETINS

GLP-1 (glucagon-like peptide 1)
• Produced by L cells in ileum and in colon
GIP (glucose-dependent insulinotropic polypeptide)
• Produced by K cells in duodenum and proximal jejunum
INCRETINS
dipeptidyl peptidase-4 (DPP-4)• Enzyme that rapidly inactivates endogenous
GLP-1 and GIP• Its inhibition enhances and prolongs the actions
of both GLP-1 and GIP.
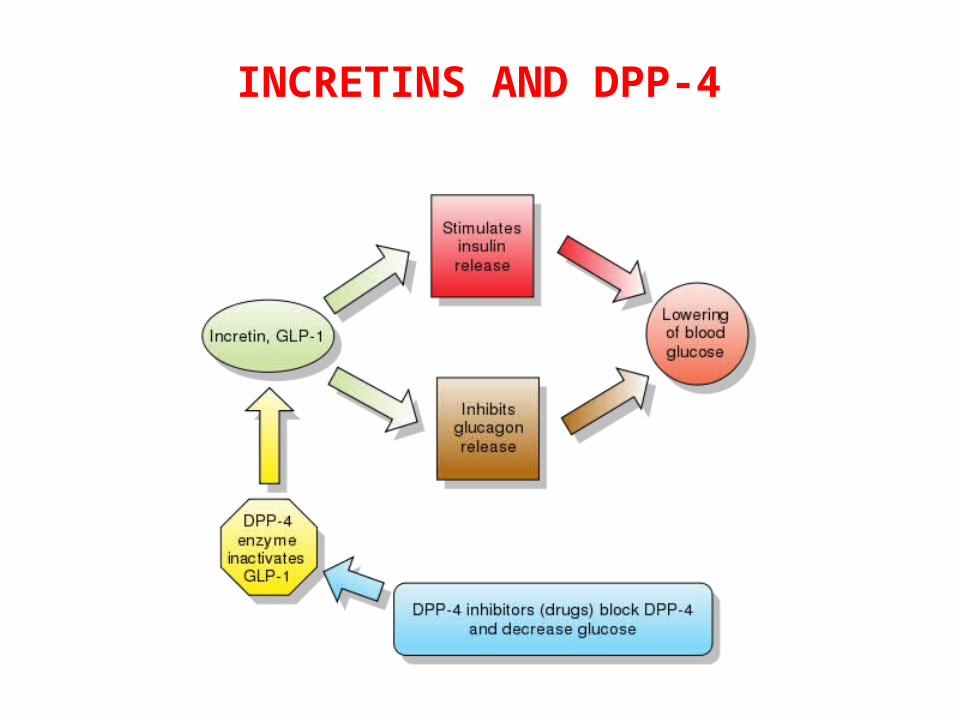
INCRETINS AND DPP-4

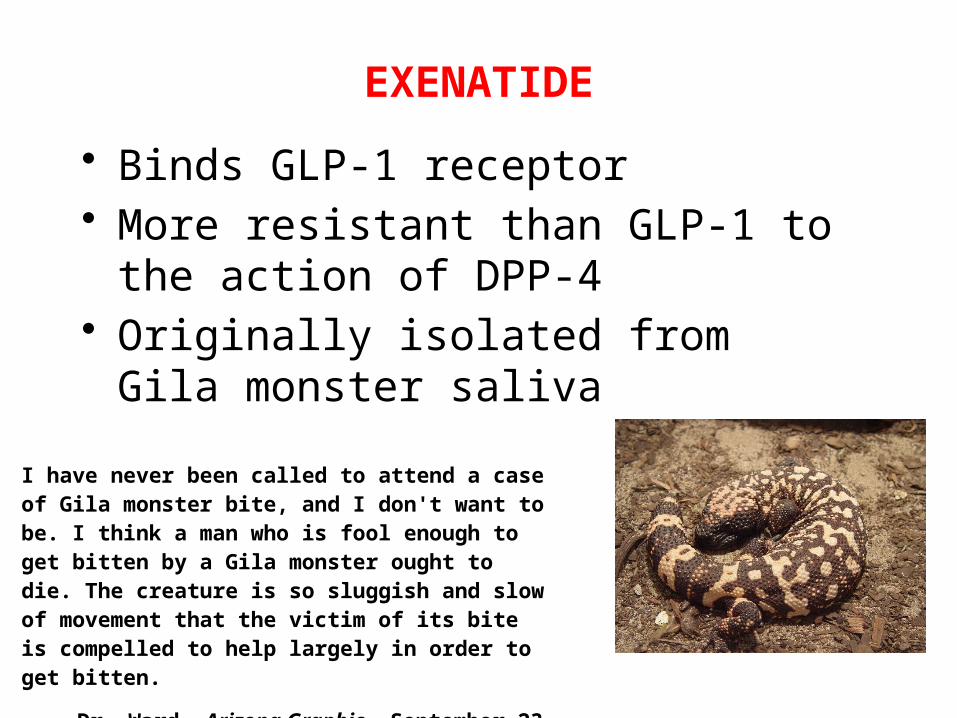
• Binds GLP-1 receptor• More resistant than GLP-1 to the action of
DPP-4• Originally isolated from Gila monster
saliva
I have never been called to attend a case of Gila monster bite, and I don't want to be. I think a man who is fool enough to get bitten by a Gila monster ought to die. The creature is so sluggish and slow of movement that the victim of its bite is compelled to help largely in order to get bitten.
—Dr. Ward, Arizona Graphic, September 23, 1899
EXENATIDE

• Orally active DPP-4 inhibitor• Prolungues and enhances the action
of endogenous GLP-1 and GIP.
SITAGLIPTIN

BRIEF INSULIN HISTORY
• Langerhans described pancreatic islets in the second half of the nineteenth century
• after a few years it has been observed that dogs developed a syndrome similar to DM after pancreatectomy
• in the early '900 has been observed that the administration of hydroalcoholic extracts of pancreas was able to determine the reduction of glycosuria in diabetic dogs
• in 1922 Banting and Best (Toronto) treated the first DM patient with pancreatic islets extract
• Banting and Macleod, an expert in chemical extraction techniques, began to develop a method that was used to obtain stable extracts of insulin and this led them to win the Nobel Prize for Medicine in 1923

INSULIN TREATMENT• after insulin discovery patients were treated with insulin preparations from porcine
or bovine pancreatic extracts for >70 years; these hormones were characterized by immunogenicity because they present some differences in aa sequences with respect to human insulin (1 and 3 aa respectively)
• with the advent of human insulin, beef and pork insulin are no longer produced
• Human insulin is produced by recombinant DNA technology
• In 1978 insulin became the first human protein to be manufactured through biotechnology. A team of researchers from the City of Hope National Medical Center and the biotechnology company Genentech managed to synthesize human insulin in the laboratory using a process that could produce large amounts.The team inserted the gene for human insulin into bacterial DNA, and used the bacteria as miniature factories to make the A and B chains of the protein separately. In a second step, a chemical process combined them. The result was human insulin, without the problems animal insulin sometimes causes.
• Humulin, as the commercial product was called, revolutionized diabetes treatment when it became widely available in the early 1980s. Today, almost all diabetic people use recombinant human insulin instead of animal insulin.
Two approaches are used to modify the absorption and pharmacokinetic profile of insulin. • The first approach, which has been used for >70 years to alter
the absorption profile of native insulin, is based on formulations that slow the absorption following subcutaneous injection.
• The other approach is to alter the amino acid sequence or protein structure of human insulin so that it retains its ability to bind the insulin receptor, but its behavior in solution or following injection is either accelerated or prolonged in comparison to native or regular insulin
INSULIN FORMULATION

INSULIN ABSORPTION: FROM SUBCUTANEOUS TISSUE TO BLOODSTREAM

CHEMICAL MANIPULATION
• Slow insulin NPH (neutral protamine Hagedorn) o isophane insulin suspension: zinc and protamine complexed insulin suspension in phosphate buffer
• Because of this formulation, the insulin dissolves more gradually when injected subcutaneously and thus its duration of action is prolonged. NPH insulin is usually given either once a day (at bedtime) or twice a day in combination with short-acting insulin.

GENETIC MANIPULATION
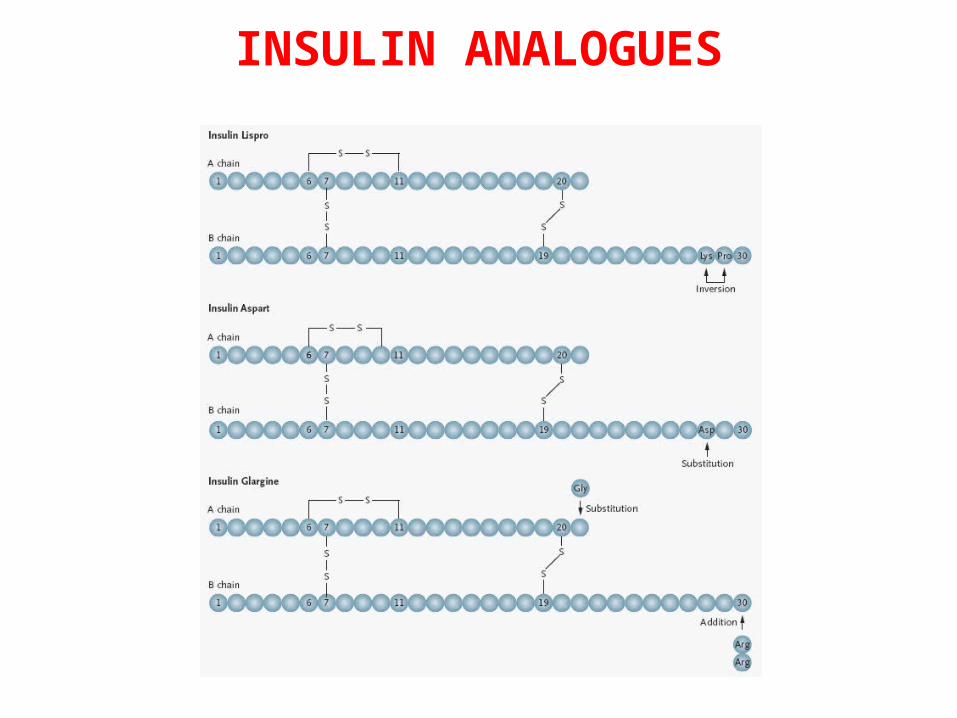
• Short-acting insulin analogs (lispro, aspart, glulisine) dissociates into monomers almost instantaneously following injection. This property results in the characteristic rapid absorption and shorter duration of action compared with regular insulin. Two therapeutic advantages have emerged with these analogs as compared with regular insulin: the prevalence of hypoglycemia is reduced and glucose control is modestly but significantly improved.
• Slow-acting insulin analog (glargine or LANTUS) is a long-acting analog of human insulin that is produced following two alterations of human insulin. Two arginine residues are added to the C terminus of the B chain, and an asparagine molecule in position 21 on the A chain is replaced with glycine. Insulin glargine is a clear solution with a pH of 4.0, which stabilizes the insulin hexamer. When injected into the neutral pH of the subcutaneous space, aggregations occurs, resulting in prolonged, but predictable, absorption from the injection site. In clinical studies glargine has a sustained peakless absorption profile, and provides a better once-daily 24-hour insulin coverage than NPH insulin.
Date of download: 3/6/2015 Copyright © 2015 McGraw-Hill Education. All rights reserved.
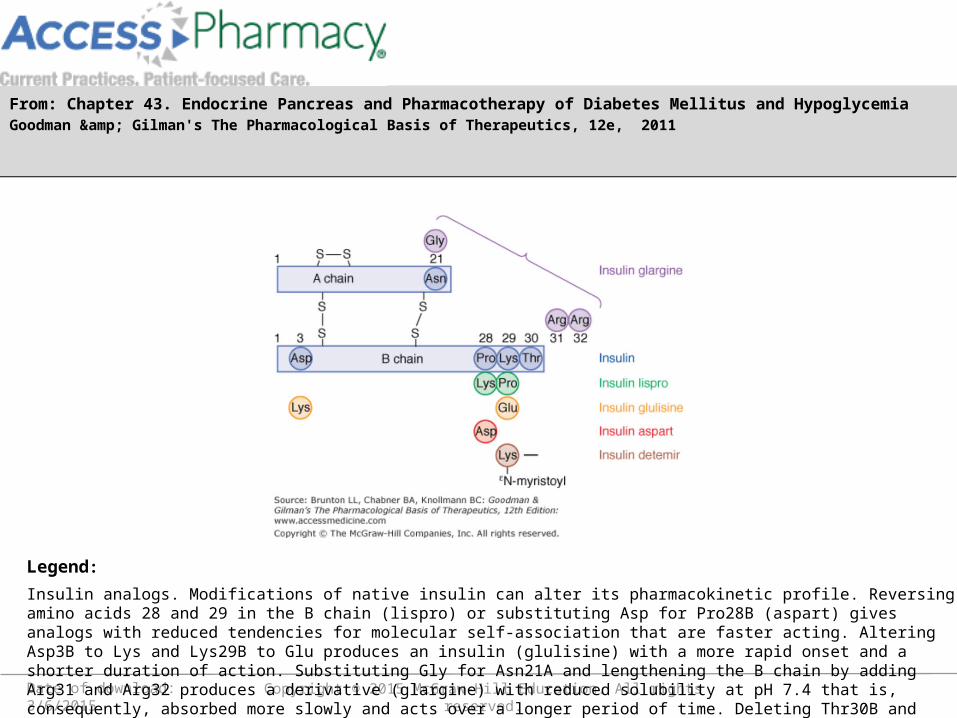
Insulin analogs. Modifications of native insulin can alter its pharmacokinetic profile. Reversing amino acids 28 and 29 in the B chain (lispro) or substituting Asp for Pro28B (aspart) gives analogs with reduced tendencies for molecular self-association that are faster acting. Altering Asp3B to Lys and Lys29B to Glu produces an insulin (glulisine) with a more rapid onset and a shorter duration of action. Substituting Gly for Asn21A and lengthening the B chain by adding Arg31 and Arg32 produces a derivative (glargine) with reduced solubility at pH 7.4 that is, consequently, absorbed more slowly and acts over a longer period of time. Deleting Thr30B and adding a myristoyl group to the ε-amino group of Lys29B (detemir) enhances reversible binding to albumin, thereby slowing transport across vascular endothelium to tissues and providing prolonged action.
Legend:
From: Chapter 43. Endocrine Pancreas and Pharmacotherapy of Diabetes Mellitus and HypoglycemiaGoodman & Gilman's The Pharmacological Basis of Therapeutics, 12e, 2011
From: Chapter 43. Endocrine Pancreas and Pharmacotherapy of Diabetes Mellitus and HypoglycemiaGoodman & Gilman's The Pharmacological Basis of Therapeutics, 12e, 2011
INSULIN ANALOGUES

PHARMACOKINETIC

breakfast dinnerlunch sleep
Pla
sma
Insu
lin
Modified from:1. Leahy JL. In: Leahy JL, Cefalu WT, eds. Insulin Therapy. New York, NY: Marcel Dekker, Inc.; 2002.2. Bolli GB et al. Diabetologia. 1999;42:1151-1167.
Basal secretion
Post-prandial secretion
DO YOU REMEMBRE THE NORMAL INSULIN SECRETION PROFILE?
Short-acting analog
Slow-acting analog

OTHER TREATMENT OPTIONS
• Continuous subcutaneous insulin infusion (CSII) pumps
• Pancreas islets transplantation
• Stem cells





















