Embed Size (px)
Citation preview

Get Homework/Assignment Done
Homeworkping.com
Homework Help
https://www.homeworkping.com/
Research Paper help
https://www.homeworkping.com/
Online Tutoring
https://www.homeworkping.com/
click here for freelancing tutoring sites

SUBMITTED BY: SUBMITTED TO: BSN 3 GROUP 2 Mrs.MARIBEL MURILLO
JANE MICHELLE CESARIO
A. GENERAL DATA
1. PATIENT NAME: IE.DR
DENGUE

2. ADDRESS: Laoac, Pangasinan
3. AGE: 4 years old
4. SEX:Male
5. BIRTH DATE: April 20, 2009
6. RANK IN THE FAMILY: 2nd child
7. NATIONALITY: Filipino
8: CIVIL STATUS: Single
9 .DATE OF ADMISSION: July 22,2013
10. ORDER OF ADMISSION:
Admit to pedia ward
Secure consent
TPR q4 every shift
Diagnostics: CBC, platelet, urinalysis
11. ATTENDING PHYSICIAN: Dr. Viduya
12. ADMITTING DIAGNOSIS: Fever for 3days
B.CHIEF COMPLAINT
Intermitent fever for 3days
C.HISTORY OF PRESENT ILLNESS
a day prior to admission the patient experienced hyperthermia.
D.PAST HEALTH HISTORY/STATUS

He didn’t have any operations, surgeries or any allergies to food or drugs . He had measles, mumps and common colds. He has been immunized and
completed vaccinations for Bacillus Calmette Guerin (BCG), Oral Polio Virus (OPV), Diphtheria, Pertusis, andTetanus (DPT), Hepatitis B and MMR.
E.FAMILY ASSESSMENT
NAME
RELATION
AGE
SEX
OCCUPATION
EDUCATIONAL
ATTAINMENT
J.DR
Mother
32
Female
OFW
College graduate
J.DR
Sister
7
Female
Student
F.SYSTEM TO REVIEW-Gordon’s 11 Functional Health Patterns Assessment
1.HEALTH PERCEPTION-HEALTH MAINTENANCE PATTERN
-‘’Health is only physical it is a wholeness of a person’’as verbalized by the patient.
2.NUTRITIONAL-METABOLIC PATTERN
BEFORE HOSPITALIZATION:The patient eats 3 times a day and with afternoon snacks. According to the SO of the patient, he eats meat, fish and also
vegetables. He doesn’t have any allergies on foods and drugs. His appetite is moderate and usually depends on the food being served. He didn’t
complain any difficulty in swallowing.
DURING HOSPITALIZATION:The patient has loss his appetite and hasn’t eaten a lot. He is on a DAT (Diet asTolerated) EDCF (Except Dark Colored
Foods).
3.ELIMINATION PATTERN
BEFORE HOSPITALIZATION:The patient does not have any problem on her elimination pattern. He usuallyurinates 4-5 timesa day without any
difficulty. He added that the color of her urine is light yellow. He didn’t feel any pain in urination. The patient defecates once a day usuallyearly in the
morning with yellow to brown color. He verbalizedthat sometimes however, it is hard in consistency with dark color, which generallydepends on what he
eats.
DURING HOSPITALIZATION: The patient urinates 2-3 times a day. The color of his urine is yellow. The patientdefecates once every two days.
4.ACTIVITY EXERCISE PATTERN
BEFORE HOSPITALIZATION:He could perform activities of her daily living.

DURING HOSPITALIZATION: His activity was limited lying on bed but the patient is given her bathroom privileges.
5.SLEEP-REST PATTERN
BEFORE HOSPITALIZATION:He has the normal 6-8 hours of sleep. He also has his nap time for 1-2 hours a day.Sleeping and watching the
television are his form of rest.
DURING HOSPITALIZATION:He doesn’t have the adequate time of sleep since he is disturbed with the nursesthat enter the room every now
and then, and because of the environmental changes of his surroundings. He also has inadequate time to rest since she doesn’t have enough time
to sleep.
6.COGNITIVE-PERCEPTUAL PATTERN
He sees herself as a person with a good personality. She has been a good brother and daughter. He said he has to be a good person in order not to hurt
others.
7.ROLE-RELATIONSHIP PATTERN
BEFORE HOSPITALIZATION:He has a close relationship with her family. They were two siblings in their family. He was the youngest. I was also able to
ask his mother about his being a son andshe confessed that he is a good son but at times he doesn’t obey her.
DURING HOSPITALIZATION:He had more time to bond with her family.
8.SEXUALITY-REPRODUCTIVE PATTERN
-none-
9.COPING STRESS TOLERANCE
He does not fully identify her situations having stress but she always tell her parents when something is wrong.
10.VALUE-BELIEF PATTERN
He is a Roman Catholic devotee. She always goes with her family every Sunday to go tomass. He was taught by his family to believe and have fear to
GOD. They usually believe inquack doctors.

G. HEREDO-FAMILIAL ILLNESS
Maternal PATERNAL
(Deceased)
Asthma
IE.DR
(patient)
dengue
None

H. DEVELOPMENT HISTORY (according to Erickson, Freud, Piaget, Kohlberg, Fowler)
THEORIST
AGE
SEX
PATIENT DESCRIPTION
Erickson
Fidelity: Identity vs. Role Confusion (Adolescence, 13-19
years)
FEMALE
Existential Question: Who Am I and What Can I Be? The adolescent is newly concerned with how they appear to others. Superego identity is the accrued confidence that the outer sameness and
continuity prepared in the future are matched by the sameness and continuity of one's meaning for oneself, as evidenced in the promise of a career. The ability to settle on a school or occupational identity is
pleasant. In later stages of Adolescence, the child develops a sense of sexual identity. As they make the transition from childhood to adulthood, adolescents ponder the roles they will play in the adult world.
Initially, they are apt to experience some role confusion—mixed ideas and feelings about the specific ways in which they will fit into society—and may experiment with a variety of behaviors and activities (e.g. tinkering
with cars, baby-sitting for neighbors, affiliating with certain political or religious groups). Eventually, Erikson proposed, most adolescents achieve a sense of identity regarding who they are and where their lives
are headed.
Piaget’s theory of cognitive
development
Formal operations (beginning at ages 11-
15)
FEMALE
Cognition reaches its final form. By this stage, the person no longer requires concrete objects to make rational judgments. He or she is
capable of deductive and hypothetical reasoning. His or her ability for abstract thinking is very similar to an adult.
FREUD Genital stage
12 – 20 y/o
FEMALE
The genital stage affords the person the ability to confront and resolve his or her remaining psychosexual childhood conflicts. The ego is established
in the latter. The person’ s concern shifts from primary-drive gratification (instinct) to applying secondary process-thinking to gratify desire symbolically and intellectually by means of friendships, a love
relationship, family and adult responsibilities

I.PHYSICAL ASSESSMENT
A. GENERAL SURVEY
Body proportions are normal. Posture is erect but slightly not comfortable when standing straight. Gait is rhythmic and coordinated with arms
swinging at side when walking. Wears ordinary clothes such as shirt and shorts. He weighs 14.5 kilograms. There is slight body odor and breath
odor. Interacts and communicates in an appropriate manner with others. He is alert and oriented with time, place and person. His speech is clear
and can comprehend with instructions when asked.
B. VITAL SIGN
BP: 70/80mmHg
PR: 93 beats per minute
RR: 26 breaths per minute
TEMP: 38 degree Celsius
C. REGIONAL EXAM
1. Hair, head and face:Head is normal cephalic, no lesions, and no complaints of pain when palpated. Can puff out cheeks, and can feel sharp and dull
objects.
2. Eyes are symmetric to each other, eye bags noted due to lack of sleep, no swelling, lesions, and no complaints of eye pain; eyelashes are evenly
distributed, curled outward; skin intact, no discoloration, symmetric eyelids and eyeballs; able to blink involuntarily; bulbar conjunctiva transparent, no
lesions; palpebral conjunctiva, smooth, pink, no edema.
3. Nose: shape and size are symmetric; no lesions; as the client breaths normally; mucosa is pink and no lesions, intact nasal septum between the nasal
chambers.
4. Ears: the color is light which is symmetric to her facial skin; firm, not tender and pinna recoils after it was folded; cerumen is sticky wet, no skin
lesions, pus and blood.
5. Mouth and Throat: There are no lesions and or swelling noted on the mouth. Presence of tartar and cavities are seen on the front teeth. The tongue is
reddish and in normal size. No inflammation of the throat.
6. Neck and Lymph Nodes: No pain when palpated. No swelling or inflammation.
7. Skin: fair complexion, no edema, no birthmark, no lesions, moisture in skin folds and ax illae.
8. Nails: pinkish, intact epidermis improper grooming, no markings and capillary refill 1-3 second.
9. Thorax and Lungs: No signs of distressed when breathing, not using accessory muscle, and no pain when palpated. It is also symmetrical to each
other.

10. Cardiovascular:No distension of Jugular veins. The pulse rate is palpated with 93 beats per minute rate and regular pattern.
11. Breast and Axilla: Breast are symmetrical to each other, there is no visible vein and no retraction and dimpling. No presence of mass and nodules
with foul odor and no lesions. No enlarge lymph nodes.
12. Abdomen: Characterized as rounded, no lesions. No bruit sound.
13. Extremities: Both arms and legs are same with the skin tone of the body. Skin is warm to touch. No lesions and excoriations noted.
14. Genitals: not performed.
15. Rectum and Anus: not performed
II. PERSONAL / SOCIAL HISTORY
a. Habits/ Vices: watching television, playing.
a. Caffeine: not drinking coffee
b. Smoking: not smoking
c. Alcohol: not drinking alcohol
d. Tea: not drinking tea.
E. drugs –none
b. Lifestyle
When staying in house he watches television or playing with toys.
c. Social Affiliation
He doesn’t participate in any affiliations.
d. Rank in the family
He is youngest among two siblings
e. Travel (within 6 months)
He didn’t travel.
f. Educational Attainment
Still not going to school
I. Environment History (Living/ Neighborhood/Circumstances)
Their house is bungalow and made of cement, they have their own comfort room and faucet as their source of water. They sell different kinds of candies
as their source of living. They have their own tricycle as their transportation and they also use it as their service in their rolling store.
V.INTRODUCTION

Dengue Fever is caused by one of the four closely related, but antigenically distinct, virusserotypes Dengue type 1, Dengue t ype 2, Dengue type
3, and Dengue type 4 of the genus Flavivirus and Chikungunya virus. Infection with one of these serotype provides immunity toonly that serotype of life, to
a person living in a Dengue-endemic area can have more than oneDengue infection during their lifetime. Dengue fever through the four different Dengue
serotypesare maintained in the cycle which involves humans and Aedes aegypti or Aedes albopictusmosquito through the transmission of the viruses to
humans by the bite of an infected mosquito.The mosquito becomes infected with the Dengue virus when it bites a person who has Dengueand after a
week it can transmit the virus while biting a healthy person. Dengue cannot betransmitted or directly spread from person to person. Aedes aegypti is
the most common aedesspecie which is a domestic, day-biting mosquito that prefers to feed on humans.
INTUBATION PERIOD: Uncertain. Probably 6 days to 10 days
PERIOD OF COMMUNICABILITY: Unknown. Presumed to be on the 1st week of illness when virus is still present in the blood
CLINICAL MANIFESTATIONS:
First 4 days:
>febrile or invasive stage --- starts abruptly as high fever, abdominal pain and headache; later flushing which may be accompanied by vomiting,
conjunctival infection and epistaxis
4th to 7th day:
>toxic or hemorrhagic stage --- lowering of temperature, severe abdominal pain, vomiting and frequent bleeding from GIT in the form of melena;
unstable BP, narrow pulse pressure and shock; death may occur; vasomotor collapse
7th to 10th day:
>convalescent or recovery stage --- generalized flushing with intervening areas of blanching appetite regained and blood pressure already
stable
MODE OF TRANSMISSION:
Dengue viruses are transmitted to humans through the infective bites of female Aedesmosquito. Mosquitoes generally acquire vi rus while
feeding on the blood of an infected person. After virus incubation of 8-10 days, an infected mosquito is capable, during probing and blood feeding of
transmitting the virus to susceptible individuals for the rest of its life. Infected female
mosquitoes may also transmit the virus to their offspring by transovarial (via the eggs)transmission.
Humans are the main amplifying host of the virus. The virus circulates in the blood of infected humans for two to seven days, at approximately
the same time as they have fever. Aedesmosquito may have acquired the virus when they fed on an individual during this period. Dengue cannot be
transmitted through person to person mode.
CLASSIFICATION:
1. Severe, frank type

>flushing, sudden high fever, severe hemorrhage, followed by sudden drop of temperature, shock and terminating in recovery or death
2. Moderate
>with high fever but less hemorrhage, no shock present
3. Mild
>with slight fever, with or without petichial hemorrhage but epidemiologically related to typical cases usually discovered in the course of invest or
typical cases
GRADING THE SEVERITY OF DENGUE FEVER:
Grade 1:
>fever
>non-specific constitutional symptoms such as anorexia, vomiting and abdominal pain
>absence of spontaneous bleeding>positive tourniquet test
Grade 2:
>signs and symptoms of Grade 1: plus
>presence of spontaneous bleeding: mucocutaneous, gastrointestinal
Grade 3:
>signs and symptoms of Grade 2 with more severe bleeding: plus>evidence of circulatory failure: cold, clammy skin, irritability,
weak tocompressible pulses, narrowing of pulse pressure to 20 mmhg or less, coldextremities, mental confusion
Grade 4:
>signs and symptoms of Grade 3, declared shock, massive bleeding, pulse lessand arterial blood Pressure = 1 mmhg (Dengue Syndrome/DS)
SUSCEPTABILITY, RESISTANCE, AND OCCURRENCE:
>all persons are susceptible
>both sexes are equally affected>age groups predominantly affected are the pre-school age and school age>adults and infants are not
exempted
>peak age affected: 5-9 years old
DF is sporadic throughout the year. Epidemic usually occurs during rainy seasons (June – November). Peak months are September – October. It occurs
wherever vector mosquito exists.
DIAGNOSTIC TEST:
Tourniquet tes
>Inflate the blood pressure cuff on the upper arm to a point midway between thesystolic and diastolic pressure for 5 minutes.
>Release cuff and make an imaginary 2.5 cm square or 1 inch square just belowthe cuff, at the antecubital fossa.
>Count the number of petechiae inside the box. A test is positive when 20 or more petechiae per suare are observed.

Dengue haemorrhagic fever (DHF), a potentially lethal complication, was firstrecognized in the 1950s during the dengue epidemics in the
Philippines and Thailand, but todayDHF affects most Asian countries and has become a leading cause of hospitalization and deathamong children in
several of them.
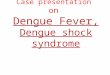
VI. ANATOMY AND PHYSIOLOGY
The Immune System
A second line of defense is housedwithin the body: a finely tuned
immunesystem that recognizes and destroysforeign substances and
organisms thatenter the body. The immune system
candistinguish between the body's owntissues and outside substances c
alledantigens. This allows cells of theimmune army to identify and destro
yonly those enemy antigens. The abilityto identify an antigen also permits
theimmune system to "remember" antigensthe body has been exposed
to in thepast; so that the body can mount abetter and faster immune
response thenext time any of these antigens appear.The immune system
also includes
other proteins and chemicals that assistantibodies and T cells in their wor
k.Among them are chemicals that alertphagocytes to the site of the
infection.The complement system, a group of proteins that normally float
freely in the blood, move toward infections, where theycombine
to help destroy microorganisms and foreign
particles. They do this bychanging the surface of bacteria or other
microorganisms, causing them to die.

VII. PATHOPHYSIOLOGY
Medical Diagnosis
T/C Dengue Hemorrhagic Fever/ Pleural Effusion, T/C Liver Pathology
Definition
Dengue Hemorrhagic Fever -
is a severe, potentially deadly infection spread by certain species of mosquitoes (Aedesaegypti).
Pleural Effusion -
is excess fluid that accumulates in the pleural cavity, the fluid-filled space that surrounds the lungs.Excessive amounts of such fluid can impair breathing
by limiting the expansion of the lungs during inhalation.
Liver Pathology –
a condition characterized by any liver diseases or condition
Predisposing
Geographicacl area – tropical islands
in thePacific (Philippines) and Asia
Precipitating
Environmental conditions (open spaces with water pots, and
plants)Immunocompromise Mosquito carrying dengue virus
soldier sweaty skin
Aedesaegypti (dengue virus carrier) 8-
12 days of viral replication on
mosquito’s salivary glands

Bite from mosquito (portal of entry in
the skin)
Allowing dengue virus to be inoculated
towards the circulation/blood
(incubation days 3-14 days)
Antibodies attach to the viralantigens, and
thenmonocytes/macrophages willperform
phagocytosis through Fcreceptor (FcR) within
the cells anddengue virus replicates in the
cells
Virus disseminated rapidly into the blood and stimulates WBCs including B-lymphocytes that produces and secretes immunoglobulin (antibodies), and monocytes, macrophages and neutrophils monocyte.
Redness and itchiness in the area
Entry to the
bone marrow
Entry to the
spleen

Recognition of dengue viral antigen on
infected monocyte.
Release of cytokines which consist of
vasoactive agent such as interleukens, tumor
necrosis factor, urokinase and platelet
activating factor which stimulate WBC and
pyrogen release
Dengue
Cellular direct destruction of red bone
marrow precursor cell as well as
immunological shortened platelet
Virus ultimately targets liver and spleen
parynchemal cells where infection
produces cell death
Hepatosplenomegaly Thrombocytopenia
Dengue Hemorrhagic

VIII. NURSING CARE PLAN
FOCUS: Increased body temperature
ASSESSMENT
DIAGNOSIS
PLANNING
INTERVENTION
RATIONALE
EVALUATION
Subjective:
“ apat na araw na po ako nilalagnat, di pa
po ako guagaling,”as verbalized by
the patient.
Objective: Flushed skin Weak in
appearance Teary eyes Increase in vital
signs PR: 93 bpm T: 38° C
R:26 BP:100/80mmHg
Hyperthermia
related to increased metabolic rate as
evidenced by increase in body temperature
(38°C).
Short term
objective: After 30 minutes of rendering
appropriate nursing intervention, the
patient’s temperature will be decreased
from 38°C to 37.5°C or lower(within
normal range).
Diagnostics: Note presence or
absence of sweating as body attempts to increase heat loss by
evaporation, conduction, and diffusion.
Monitor and record all sources of fluid loss such as urine.
Monitor vital signs especially temperature.
Therapeutics: Dependent: Administer
medications as indicated or ordered by the physician.
Administer
replacement of fluids
and electrolytes. Independent: Perform tepid sponge
bath.
Evaporation is
decreased by environmental factors of high humidity and high
ambient temperature.
Oliguria and/or renal failure may occur due to hypotension,
dehydration, shock, and tissue necrosis.
To evaluate effects or degree of hyperthermia.
To treat underlying
cause.
To support circulating volume and tissue perfusion.
Heat loss by
evaporation and
conduction.
Goal met. Patient’s temperature subsided from
38°C to 37.5°C.

Promote surface
cooling by means of
undressing/reducing clothes and removing excess blankets.
Maintain Bed rest.
Educative:
Discuss importance of adequate fluid intake from 1,500-
2000 ml per day. Instruct to increase
intake of Vitamin C-
rich foods.
To assist with measures to reduce body temperature/restore
normal body/organ function.
To reduce metabolic demands and oxygen consumption.
To prevent dehydration.
To boost the immune
system.

FOCUS: Nose bleeding
ASSESSMENT
DIAGNOSIS
PLANNING
INTERVENTION
RATIONALE
EVALUATION
Subjective: “bigla nalang
pong dumugo itong ilong ko”, verbalized by
the patient. Objective: Irritability
Epistaxis Weak in
appearance
pallor
Risk for injury hemorrhage
related to alter clotting factor.
Short term objective: After an
hour of nursing interventions, the patient will be able
to demonstrate behaviors that reduce the risk for
bleeding.
Diagnostics: Assess vital signs
including BP, pulse, and respiration.
Assess skin color and
moisture, urinary output, level of consciousness or
mentation.
Review laboratory data
(CBC) result Assess for signs and
symptoms of G.I
bleeding. Check for secretions; observe color and consistency
of stools or vomitus. Therapeutics:
Dependent: Assist with treatment
of underlying
conditions causing or contributing to blood loss.
Educative: Need to inform health
care providers when
taking aspirin and other anti-coagulant-type agents.
Instruct at risk patient
and family regarding:
To determine if
intravascular fluid deficit exists.
Changes in these signs maybe indicative of blood loss affecting
systemic circulation or local organ function such as kidneys or
brain.
Note for alterations on
blood. The G.I.
tract(esophagus and
rectum) is the most usual source of bleeding of its mucosal
rigidity.
To prevent
bleeding/correct
potential causes of excessive blood loss.
These agents will most
likely be held for a
period of time prior to elective procedures to reduce potential for
excessive blood loss. To prevent bleeding /
correct potential causes
Goal me. Patient is able to
demonstrate behaviors that reduce risk for bleeding.

- Specific signs of
bleeding requiring health care provider
notification such as prolonged epistaxis.
of excessive blood loss.

IX. DRUG STUDY Generic name: ceftriaxone sodium
Brand name: Rocephin Drug Classification: Antibiotic, Cephalosporin (third generation) Dosage: 1 amp IV q 12 h, ANST (-)
Indication: Urinary tract infection
MECHANISM OF
ACTION
SIDE EFFECT CONTAINDICATIONS ADVERSE REACTION NURSING
CONSIDERATIONS
Bactericidal: Inhibits
synthesis of cell wall
causing cell death
Nausea, vomiting,
diarrhea, anorexia,
abdominal pain,
flatulence
Ranging from rash
to fever
Pain, phlebitis
Super infections,
desulfiram-like
reaction with
alcohol
Contraindicated
with allergy to cephalosporins or penicillins.Use
cautiously with renal failure.
CNS: headache, dizziness, lethargy,
paresthesias
GI: Nausea, vomiting, diarrhea,
anorexia, abdominal pain, flatulence,
pseudomembranous colitis, liver
toxicity
GU: nephrotoxicity
Hematologic: Bone marrow
depression – decreased WBC,
decreased platelets, decreased Hct.
Hypersensitivity: Ranging from rash
to fever to anaphylaxis; serum
sickness reaction
Local: Pain, abscess at injection site;
phlebitis, inflammation at IV site
Other: Super infections, desulfiram-
like reaction with alcohol.
Teaching points:
You may experience
these side effects:
stomach upset or
diarrhea
Report severe
diarrhea, difficulty
breathing, unusual
tiredness or fatigue,
pain at injection site.
Discontinue if
hypersensitivity reaction
occurs.

Generic name: paracetamol Brand name:Flugard
Drug classification: antipyretic, analgesic (non opioid) Dosage: IV 1 amp now then PRN fer fever Indications: for fever
MECHANISM OF ACTION SIDE EFFECT CONTAINDICATIONS ADVERSE REACTION NURSING
CONSIDERATIONS
Antipyretic: reduces fever by acting directly on the hypothalamic
heat-regulating center to cause vasodilation and sweating, which helps
dissipate heat. Analgesic: site and
mechanism action unclear.
none Contraindicated
with allergy to acetaminophen.
Use cautiously with impaired hepatic function, chronic
alcoholism, pregnancy, lactation.
CNS: headache CV: chest pain, dyspnea,
myocardial damage when doses of 5-8 g/day are ingested daily for several
weeks or when doses of 4 g/day are ingested for 1 year.
GI: Hepatic toxicity and failure, jaundice
GU: acute renal failure, renal tubular necrosis.
Hematologic: methemoglobinemia – cyanosis; hemolytic anemia –
hematuria; anuria; neutropenia, leukopenia,thrombocytopenia,
hypoglycemia Hypersensitivity: rash, fever
Assessment:
History: allergy to acetaminophen,
impaired hepatic function.
Physical: skin
color, lesions, T; liver evaluation; CBC, LFT’s, renal
function tests.

X. DIAGNOSTIC TESTS/LABORATORY RESULTS:
TESTS RESULT NORMAL VALUES REMARKS
RBC Count
4.55
M=4.69-6.13x10 12/L F=4.04-5.48x10 12/L
normal
Hemoglobin
103
M=140-180g/L F=120-160g/L
normal
Hematocrit
.30
M=0.40-0.54
F=0.37-0.47
normal
WBC
3.8
5-10x10 9/L
Normal
DIFFERENT COUNT :
Segment
.49
0.50-0.70
Normal
Lymphocytes
.46
0.20-0.40
Monocytes
.5
0.0-0.07
URINALYSIS
RESULTS NORMAL VALUES SIGNIFICANCE

PHYSICAL: Color
Transparency CHEMICAL:
Specific Gravity
Urobilinogen
Red Blood Cells
Protein
pH
Blood cells
MICROSCOPIC: RBC
Epithelial Cells
A Urates/Phosphates
Dark Yellow
Slightly turbid
1.010
Normal
1-2
(-)
6.0
(-)
1-2
Few
Few
Straw yellow to amber
Clear
1.010 – 1.030
0 – 2
(-)
4.8-8
(-)
Normal
Indicates abnormality
Normal
Normal
Normal
Normal
Normal
Normal

XI. ONGOING APPRAISAL
The patient is responding well to both medical and nursing intervention.
XIII. DISCHARGE PLAN (HEALTH TEACHING)
Medication: Instruct IE.DR to take all the necessary medicines that the doctors prescribed.
Treatment: Instruct to follow all prescribed therapeutic regimens.
Clinical follow up: Instruct the patient to come back on scheduled follow up check.
Diet: Advise to eat dark green leafy vegetables, rich in iron and vitamin C diet to regain strength and boost his immune system
Danger Signs: Instruct the patient to seek medical advice if he is experiencing excessive nose bleeding and high-grade fever and appearance of rashes.

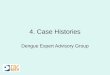
I. PATHOPHYSIOLOGY ( in diagram )
Dengue infection
Antibody formation
Reinfection
Augmentation of virus multiplication
Increased vascular permeability Reduce Platelets
Plasma Leakage Coagulopathy
Hypovolemia Disseminated intravascular coagulation
Shock Severe Bleeding
Death