Why Are We Invloved in the Detection and Treatment of Peripheral Artery
Disease?
HU Dayi

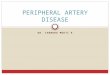
Major Clinical Manifestations of Atherothrombosis
Adapted from: Drouet L. Cerebrovasc Dis 2002; 13(suppl 1): 1–6.
Transient ischemic attack
Angina
Ischemicstroke
Myocardial infarction
Peripheral arterialdisease:• Intermittent claudication• Rest Pain• Gangrene• Necrosis
Renal artery stenosis
Atherosclerotic nephrology


NCEP ATP III: Evaluation—CAD Risk Equivalents
• Diabetes
Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA. 2001;285:2486.
• Atherosclerotic disease– Peripheral artery disease
– Abdominal aortic aneurysm
– Symptomatic carotid artery disease
• CAD 10-year risk >20%

1. Adult Treatment Panel II. Circulation 1994; 89:1333–63. 2. Kannel WB. J Cardiovasc Risk 1994; 1: 333–9. 3. Wilterdink JI, Easton JD. Arch Neurol1992; 49: 857–63. 4. Criqui MH et al. N Engl J Med 1992; 326: 381–6.
*Sudden death defined as death documented within 1 hour and attributed to coronary heart disease (CHD)†Includes only fatal MI and other CHD death; does not include non-fatal MI
Increased risk vs general population (%)
Original event Myocardial infarction Stroke
Myocardial infarction
Stroke
Peripheral arterial disease
5–7 x greater risk1
(includes death)3–4 x greater risk2
(includes TIA)
2–3 x greater risk2
(includes angina and sudden death*)
9 x greater risk3
4 x greater risk4
(includes only fatal MI and other CHD death†)
2–3 x greater risk3
(includes TIA)
Risk of a Second Vascular Event


Why A PAD Guideline?
• To enhance the quality of patient care• Increasing recognition of the importance of
atherosclerotic lower extremity PAD:– High prevalence– High cardiovascular risk– Poor quality of life
• Improved ability to detect and treat renal artery disease
• Improved ability to detect and treat AAA• The evidence base has become increasingly robust,
so that a data-driven care guideline is now possible


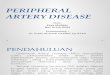
Natural History of PADAge > 50 years
Limb
Morbidity
Cardiovascular Morbidity / Mortality
Worsening Claudication
10-20%
Critical Limb
Ischemia
1-2%
Nonfatal CV Events
20%
Mortality 15-30%
Stable Claudication
70-80%
CV Causes75%
Non CV Causes25%

Quality of Life in Patients with PAD
• Individuals with asymptomatic lower extremity PAD have a worse quality of life and limb function than an age-matched cohort
• The quality of life for patients with severe CLI can be worse than that of patients with terminal cancer
McDermott MM, J Am Geriatr Soc 2002;50:238-46.
Dormandy JA, J Vasc Surg 2000;31(1 pt 2):S1-S296.

Defining a Population “At Risk” for Lower Extremity PAD
• Age less than 50 years with diabetes, and one additional risk factor (e.g., smoking, dyslipidemia, hypertension, or hyperhomocysteinemia)
• Age 50 to 69 years and history of smoking or diabetes
• Age 70 years and older
• Leg symptoms with exertion (suggestive of claudication) or ischemic rest pain
• Abnormal lower extremity pulse examination
• Known atherosclerotic coronary, carotid, or renal artery disease

Only 1 in 10 patients with PAD has classical symptoms of intermittent claudication
Only 1 in 10 of these patients has classical symptoms of
intermittent claudication (IC)
1 in 5 people over 65
has PAD†
† ABI<0.9
Diehm C et al. Atherosclerosis 2004; 172; 95-105.


Lower extremity systolic pressureBrachial artery systolic pressure ABI =
• The ankle-brachial index is 95% sensitive and 99% specific for PAD
• Establishes the PAD diagnosis
• Identifies a population at high risk of CV ischemic events
• “Population at risk” can be clinically & epidemiologically defined:
The Ankle-Brachial Index
Exertional leg symptoms, non-healing wounds, age > 70, age > 50 years with a history of smoking or diabetes.
• Toe-brachial index (TBI) useful in individuals with non-compressible pedal pulses
Lijmer JG. Ultrasound Med Biol 1996;22:391-8; Feigelson HS. Am J Epidemiol 1994;140:526-34; Baker JD. Surgery 1981;89:134-7; Ouriel K. Arch Surg 1982;117:1297-13; Carter SA. J Vasc Surg 2001;33:708-14

Lipid Lowering and Antihypertensive Therapy
Treatment with an HMG coenzyme-A reductase inhibitor
(statin) medication is indicated for all patients with
peripheral arterial disease to achieve a target LDL
cholesterol of less than 100 mg/dl.
Antihypertensive therapy should be administered to
hypertensive patients with lower extremity PAD to a goal of
less than 140/90 mmHg (non-diabetics) or less than 130/80
mm/Hg (diabetics and individuals with chronic renal
disease) to reduce the risk of myocardial infarction, stroke,
congestive heart failure, and cardiovascular death.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII

Antihypertensive Drug
Beta-adrenergic blocking drugs are effective antihypertensive agents and are not contraindicated in patients with PAD.
The use of angiotensin-converting enzyme inhibitors is reasonable for symptomatic patients with lower extremity PAD to reduce the risk of adverse cardiovascular events
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII

Antiplatelet Therapy
Antiplatelet therapy is indicated to reduce the risk of myocardial infarction, stroke, or vascular death in individuals with atherosclerotic lower extremity PAD.
Aspirin, in daily doses of 75 to 325 mg, is recommended as safe and effective antiplatelet therapy to reduce the risk of myocardial infarction, stroke, or vascular death in individuals with atherosclerotic lower extremity PAD.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
Clopidogrel (75 mg per day) is recommended as an effective alternative antiplatelet therapy to aspirin to reduce the risk of myocardial infarction, stroke, or vascular death in individuals with atherosclerotic lower extremity PAD.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII

Recommended