
10/1/2008
1
What’s New in LipidWhat s New in Lipid Therapy?
Brooke Hudspeth, PharmDBrooke Hudspeth, PharmD
Diabetes CareDiabetes Care
Kroger PharmacyKroger Pharmacy
Disclosure Statement
In accordance with policies set forth by the Accreditation Council for In accordance with policies set forth by the Accreditation Council for p yp yContinuing Medical Education (ACCME) and American Council for Continuing Medical Education (ACCME) and American Council for Pharmacy Education (ACPE), accrediting bodies, the University of Pharmacy Education (ACPE), accrediting bodies, the University of Kentucky Colleges of Pharmacy and Medicine Continuing Education Kentucky Colleges of Pharmacy and Medicine Continuing Education Program (UKCPMCE) requires all faculty members who participate in Program (UKCPMCE) requires all faculty members who participate in an activity designed for accreditation to disclose any financial interest, an activity designed for accreditation to disclose any financial interest, or other relationship, he/she has with any manufacturer(s) of or other relationship, he/she has with any manufacturer(s) of commercial product(s). These affiliations include, but are not limited commercial product(s). These affiliations include, but are not limited to grants research support consultation fees speaker’s bureaus andto grants research support consultation fees speaker’s bureaus andto grants, research support, consultation fees, speaker s bureaus and to grants, research support, consultation fees, speaker s bureaus and directly purchased stock.directly purchased stock.
Brooke Hudspeth, Brooke Hudspeth, PharmDPharmD, , has nothing to disclose.has nothing to disclose.

10/1/2008
2
Objectives
Review current dyslipidemia managementReview current dyslipidemia management Review current dyslipidemia management Review current dyslipidemia management strategies and discuss the role of lipoprotein strategies and discuss the role of lipoprotein parameters other than LDL or nonparameters other than LDL or non--HDL in lipid HDL in lipid managementmanagement
Discuss the results of the ENHANCE trial and Discuss the results of the ENHANCE trial and how this will effect therapy decisionshow this will effect therapy decisionspypy
Examine new therapies for treating dyslipidemia Examine new therapies for treating dyslipidemia that are under active developmentthat are under active development
Background
Coronary heart disease (CHD) is the single largestCoronary heart disease (CHD) is the single largest Coronary heart disease (CHD) is the single largest Coronary heart disease (CHD) is the single largest killer of both men and women in the killer of both men and women in the USUS
DyslipidemiaDyslipidemia (specifically elevated LDL) = major (specifically elevated LDL) = major modifiable risk factor for the development and modifiable risk factor for the development and progression of CHD. progression of CHD. Thus, Thus, LDLLDL--lowering therapy lowering therapy reduces risk for CHD.reduces risk for CHD.
Estimated that > 65 million Americans eligible for Estimated that > 65 million Americans eligible for lipid modificationlipid modification
APhA. Pharmacy-Based Lipid Management. 2005: 1-2.
10/1/2008
3
Pharmacists’ Role in Lipid Management
PharmacyPharmacy--based lipid management services:based lipid management services: PharmacyPharmacy--based lipid management services:based lipid management services:
60%60%--70% of patients at lipid goal70% of patients at lipid goal
*National average ~20%*National average ~20%--30%30%
>90% compliance with lipid>90% compliance with lipid--lowering lowering therapytherapytherapytherapy
*National average ~30%*National average ~30%--40%40%
Bluml BM, McKenney JM, Cziraky MJ. Pharmaceutical care services and results in Project ImPACT: Hyperlipidemia. J Am Pharm Assoc 2000;40:157-165.
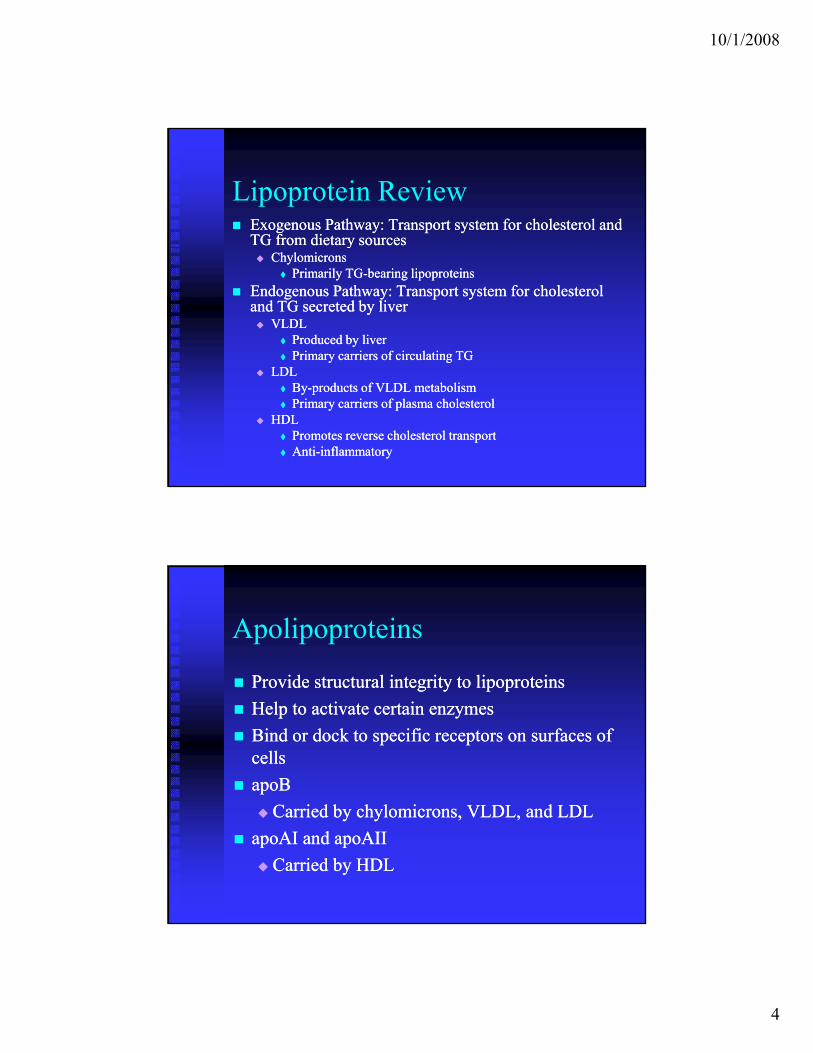
Lipoprotein Review
Lipids derived from dietary Lipids derived from dietary th i d b b dth i d b b dsources or synthesized by bodysources or synthesized by body
Cholesterol: Primarily Cholesterol: Primarily synthesized in liversynthesized in liver
Triglycerides (TG): Dietary Triglycerides (TG): Dietary triglycerides account for triglycerides account for >75% of total>75% of total
These lipids transported to sites These lipids transported to sites of use or storage via of use or storage via LipoproteinsLipoproteins ((chylomicronschylomicrons, , p pp p (( yy ,,VLDL, IDL, LDL, and HDL)VLDL, IDL, LDL, and HDL)
Derived from
10/1/2008
4
Lipoprotein Review Exogenous Pathway: Exogenous Pathway: Transport Transport system for cholesterol and system for cholesterol and
TG from dietary sourcesTG from dietary sourcesyy ChylomicronsChylomicrons
Primarily TGPrimarily TG--bearing lipoproteinsbearing lipoproteins
Endogenous Endogenous PathwayPathway: : Transport Transport system for cholesterol system for cholesterol and TG secreted by liverand TG secreted by liver VLDL VLDL
Produced by liverProduced by liver Primary carriers of circulating TGPrimary carriers of circulating TG
LDLLDL LDLLDL ByBy--products of VLDL metabolismproducts of VLDL metabolism Primary carriers of plasma cholesterolPrimary carriers of plasma cholesterol
HDLHDL Promotes reverse cholesterol transport Promotes reverse cholesterol transport AntiAnti--inflammatory inflammatory
Apolipoproteins
Provide structuralProvide structural integrityintegrity to lipoproteinsto lipoproteins Provide structural Provide structural integrity integrity to lipoproteinsto lipoproteins
Help to activate certain enzymesHelp to activate certain enzymes
Bind or dock to specific receptors on surfaces of Bind or dock to specific receptors on surfaces of cellscells
apoBapoB
C i d bC i d b h l ih l i dd Carried by Carried by chylomicronschylomicrons, VLDL, and LDL, VLDL, and LDL
apoAIapoAI and and apoAIIapoAII
Carried by HDLCarried by HDL

10/1/2008
5
Atherosclerosis
LDL accumulates in subendothelial space of LDL accumulates in subendothelial space of artery and initiates inflammatory responseartery and initiates inflammatory responseartery and initiates inflammatory response. artery and initiates inflammatory response.
Eventually leads to the formation of foam Eventually leads to the formation of foam cells which turn into fatty streaks (initial cells which turn into fatty streaks (initial lesion of atherosclerosis) covered by fibrous lesion of atherosclerosis) covered by fibrous caps. caps.
When the fibrous cap becomes unstable and When the fibrous cap becomes unstable and ruptures, a thrombus develops which leads ruptures, a thrombus develops which leads p , pp , pto CHD.to CHD.
Derived from http://www.nutrizone.co.za/slides/100/images/ss2s3_JPG.jpg
Comprehensive Evaluation
ObjectivesObjectives ObjectivesObjectives
1.1. Determine the magnitude of the future Determine the magnitude of the future risk of CVD eventsrisk of CVD events
2.2. Identify the presence of possible Identify the presence of possible modifiable prognostic factors modifiable prognostic factors p gp g
3.3. Establish a treatment planEstablish a treatment plan
Consensus statement from the American Diabetes Association and the American College of Consensus statement from the American Diabetes Association and the American College of Cardiology Foundation. Diabetes Care 2008;31(4):811Cardiology Foundation. Diabetes Care 2008;31(4):811--822.822.
10/1/2008
6
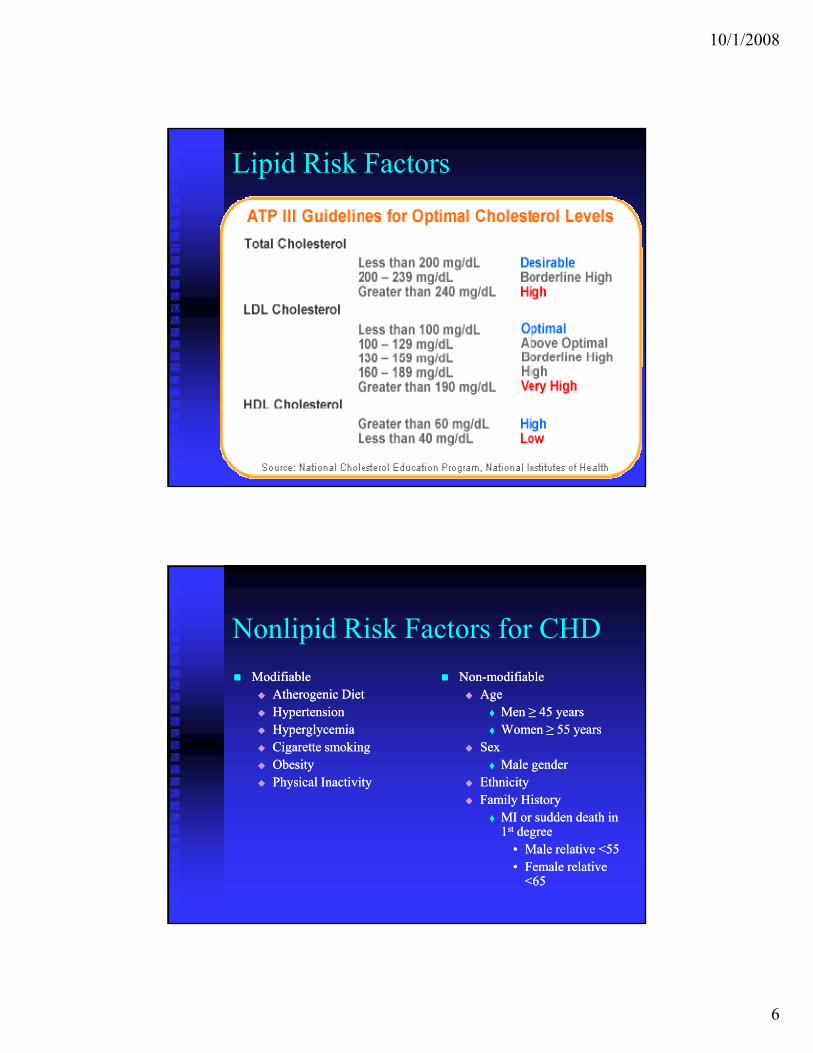
Lipid Risk Factors
Nonlipid Risk Factors for CHD
ModifiableModifiable NonNon--modifiablemodifiable Atherogenic DietAtherogenic Diet HypertensionHypertension HyperglycemiaHyperglycemia Cigarette smokingCigarette smoking Obesity Obesity Physical InactivityPhysical Inactivity
AgeAge Men Men ≥ 45 years≥ 45 years Women ≥ 55 yearsWomen ≥ 55 years
SexSex Male genderMale gender
EthnicityEthnicity Family HistoryFamily Historyy yy y
MI or sudden death in MI or sudden death in 11stst degreedegree
•• Male Male relative <55relative <55•• Female Female relative relative
<65<65

10/1/2008
7
Emerging Risk Factors
BiomarkersBiomarkers BiomarkersBiomarkers
CC--reactive protein (CRP)reactive protein (CRP)
HomocysteineHomocysteine
FibrinogenFibrinogen
Lipoprotein(a)Lipoprotein(a)Lipoprotein(a)Lipoprotein(a)
Classification
PrimaryPrimary GeneticGenetic GeneticGenetic
SecondarySecondary Drugs (i.e. Drugs (i.e. progestinsprogestins, steroids, protease , steroids, protease
inhibitors)inhibitors) Diet (i.e. excessive alcohol, saturated fats)Diet (i.e. excessive alcohol, saturated fats) Metabolic Disorders (i.e. diabetes, weight gain, Metabolic Disorders (i.e. diabetes, weight gain,
anorexia hypothyroidism)anorexia hypothyroidism)anorexia, hypothyroidism)anorexia, hypothyroidism) Disease States (i.e. Disease States (i.e. nephroticnephrotic syndrome, chronic syndrome, chronic
liver disease)liver disease)
Stone NJ. Med Clin North Am.1994;78:120
Stone and Blum. Management of Lipids in Clinical Practice. 6th edition. 2006
10/1/2008
8
Risk Assessment and Strategies
American Diabetes AssociationAmerican Diabetes Association DiabetesPHDDiabetesPHD (Personal Health Decisions)(Personal Health Decisions) http://www.diabetes.org/diabetesphd/default.jsphttp://www.diabetes.org/diabetesphd/default.jsp Calculates current risk for diabetes and complications Calculates current risk for diabetes and complications
(i.e. heart attack, stroke, kidney failure, eye and foot (i.e. heart attack, stroke, kidney failure, eye and foot complications) based on patient health complications) based on patient health history history and how and how making healthy changes could making healthy changes could affect affect future healthfuture health
ATP III Guidelines AtATP III Guidelines At--AA--Glance Quick Desk referenceGlance Quick Desk referenceQQ http://www.nhlbi.nih.gov/guidelines/cholesterol/atglanchttp://www.nhlbi.nih.gov/guidelines/cholesterol/atglanc
e.pdfe.pdf Treatment algorithm for treating lipid disordersTreatment algorithm for treating lipid disorders 9 step process9 step process
Step 1
Determine lipoprotein levelsDetermine lipoprotein levelsDetermine lipoprotein levelsDetermine lipoprotein levels

10/1/2008
9
ATP III Guidelines
Obtain complete lipoprotein profile afterObtain complete lipoprotein profile after 99-- Obtain complete lipoprotein profile after Obtain complete lipoprotein profile after 99--to 12to 12--hour hour fastfast
ATP III recommends that all Americans ATP III recommends that all Americans ≥ ≥ 20 have fasting lipid panel performed every 20 have fasting lipid panel performed every 5 years5 years
More frequent measurements in people with More frequent measurements in people with multiple CHD risk factorsmultiple CHD risk factors
Step 2
Identify presence of CHD or CHD riskIdentify presence of CHD or CHD riskIdentify presence of CHD or CHD risk Identify presence of CHD or CHD risk equivalentsequivalents
10/1/2008
10
CHD and CHD Risk Equivalents
Established CHDEstablished CHD Established CHDEstablished CHD
Abdominal Aortic AneurysmAbdominal Aortic Aneurysm
Peripheral Arterial DiseasePeripheral Arterial Disease
Carotid Artery DiseaseCarotid Artery Disease
DiabetesDiabetes DiabetesDiabetes
Step 3
Determine the presence of major riskDetermine the presence of major riskDetermine the presence of major risk Determine the presence of major risk factorsfactors

10/1/2008
11
Major Risk Factors (Exclusive of LDL Cholesterol) That Modify LDL Goals
Risk FactorRisk Factor DefinitionDefinition
Cigarette smoking Cigarette smoking Any cigarette smoking in the past Any cigarette smoking in the past monthmonth
HypertensionHypertension BPBP≥≥ 140/90 mmHg or on 140/90 mmHg or on antihypertensive medicationantihypertensive medication
Low HDL cholesterolLow HDL cholesterol <40 mg/dl<40 mg/dl
Family history of premature CHDFamily history of premature CHD CHD in male first degree relative <55 CHD in male first degree relative <55 years; CHD in female first degree years; CHD in female first degree y ; gy ; grelative <65 yearsrelative <65 years
AgeAge men men ≥≥ 45 years; women 45 years; women ≥≥ 55 years55 years
Negative Risk FactorNegative Risk Factor
High HDL cholesterolHigh HDL cholesterol ≥ 60 mg/dl≥ 60 mg/dl
Step 4
Assess ShortAssess Short Term CHD riskTerm CHD riskAssess ShortAssess Short--Term CHD riskTerm CHD risk
10/1/2008
12
Framingham Point Scores
If person has If person has ≥ 2 risk factors (from Step 3) ≥ 2 risk factors (from Step 3) pp ( p )( p )without CHD risk equivalents, perform 10without CHD risk equivalents, perform 10--year year risk assessment using Framingham point scoresrisk assessment using Framingham point scores
Scores based on age, total cholesterol, systolic Scores based on age, total cholesterol, systolic BP, treatment of BP, treatment of hypertension hypertension and smoking and smoking statusstatus
3 levels of 103 levels of 10--yr risk:yr risk: High: High: >>20% 20% ---- CHD risk equivalentCHD risk equivalent Moderate: Moderate: 1010--2020%% Low: Low: <<10%10%
Step 5
Determine Risk CategoryDetermine Risk CategoryDetermine Risk CategoryDetermine Risk Category
10/1/2008
13
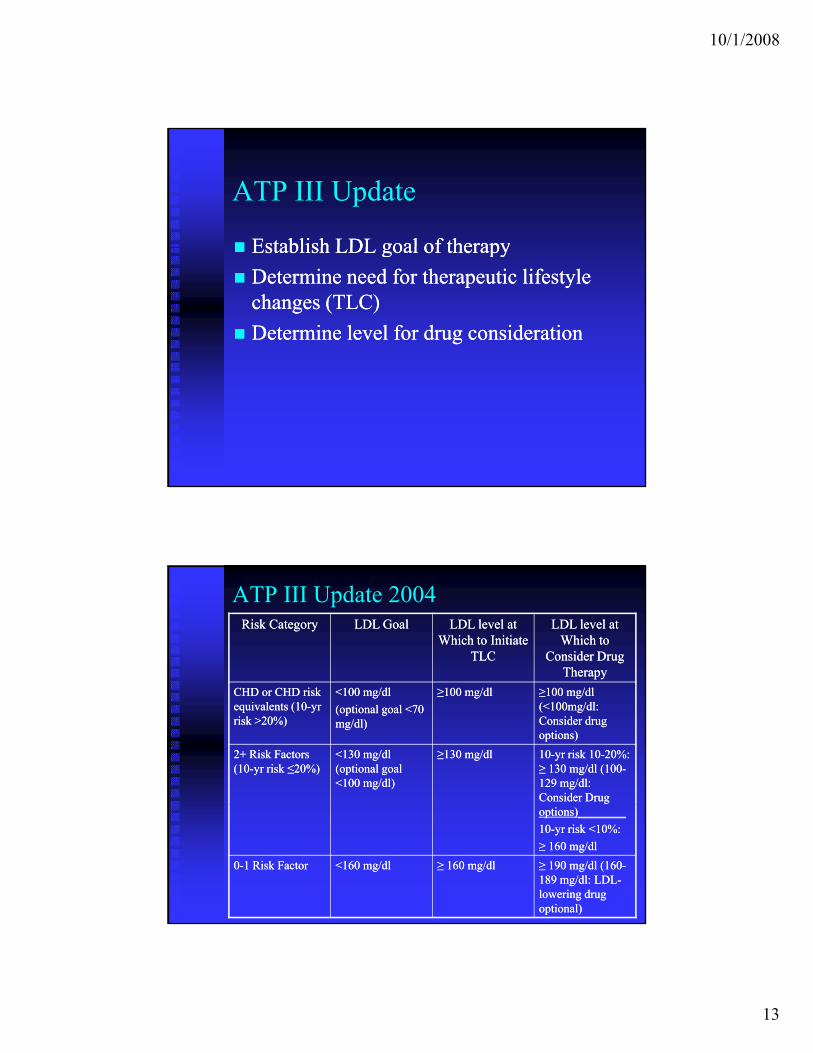
ATP III Update
Establish LDL goal of therapyEstablish LDL goal of therapy Establish LDL goal of therapyEstablish LDL goal of therapy
Determine need for therapeutic lifestyle Determine need for therapeutic lifestyle changes (TLC)changes (TLC)
Determine level for drug considerationDetermine level for drug consideration
ATP III Update 2004Risk CategoryRisk Category LDL GoalLDL Goal LDL level at LDL level at
Which to Initiate Which to Initiate TLCTLC
LDL level at LDL level at Which to Which to
Consider Drug Consider Drug TherapyTherapy
CHD or CHD risk CHD or CHD risk equivalents (10equivalents (10--yr yr risk >20%)risk >20%)
<100 mg/dl<100 mg/dl
(optional goal <70 (optional goal <70 mg/dl)mg/dl)
≥100 mg/dl≥100 mg/dl ≥100 mg/dl ≥100 mg/dl (<100mg/dl: (<100mg/dl: Consider drug Consider drug options)options)
2+ Risk Factors 2+ Risk Factors (10(10--yr risk yr risk ≤20%)≤20%)
<130 mg/dl <130 mg/dl (optional goal (optional goal <100 mg/dl)<100 mg/dl)
≥130 mg/dl≥130 mg/dl 1010--yr risk 10yr risk 10--20%: 20%: ≥ 130 mg/dl (100≥ 130 mg/dl (100--129 mg/dl: 129 mg/dl: Consider DrugConsider Drugoptions)________options)________
1010--yr risk <10%:yr risk <10%:
≥ 160 mg/dl≥ 160 mg/dl
00--1 Risk Factor1 Risk Factor <160 mg/dl<160 mg/dl ≥ 160 mg/dl≥ 160 mg/dl ≥ 190 mg/dl (160≥ 190 mg/dl (160--189 mg/dl: LDL189 mg/dl: LDL--lowering drug lowering drug optional)optional)

10/1/2008
14
ATP III Update 2004
Based upon information from 5 recentBased upon information from 5 recent Based upon information from 5 recent Based upon information from 5 recent clinical trials (PROSPER, ALLHATclinical trials (PROSPER, ALLHAT--LLT, LLT, ASCOTASCOT--LLA, PROVE IT, HPS), a LLA, PROVE IT, HPS), a modified scheme of LDL cholesterol goals modified scheme of LDL cholesterol goals and treatment cutpoints were proposedand treatment cutpoints were proposed
No modifications in lowNo modifications in low--risk patientsrisk patients No modifications in lowNo modifications in low risk patientsrisk patients Most recommendations pertaining Most recommendations pertaining
specifically to patients in highspecifically to patients in high--risk categoryrisk category
Key Changes
High Risk High Risk LDL cholesterol goal <70 mg/dl therapeutic option, especially in LDL cholesterol goal <70 mg/dl therapeutic option, especially in
very high risk patientsvery high risk patients If baseline LDL >100 mg/dl, an LDLIf baseline LDL >100 mg/dl, an LDL--lowering drug is indicated lowering drug is indicated If baseline LDL <100 mg/dl, LDLIf baseline LDL <100 mg/dl, LDL--lowering drug is therapeutic lowering drug is therapeutic
optionoption
Moderately High RiskModerately High Risk LDL goal <100mg/dl therapeutic optionLDL goal <100mg/dl therapeutic option LDL 100LDL 100 129mg/dl LDL129mg/dl LDL lowering drug is therapeutic optionlowering drug is therapeutic option LDL 100LDL 100--129mg/dl, LDL129mg/dl, LDL--lowering drug is therapeutic optionlowering drug is therapeutic option
High Risk and Moderately High RiskHigh Risk and Moderately High Risk Intensity of LDLIntensity of LDL--lowering drug therapy sufficient to achieve at lowering drug therapy sufficient to achieve at
least 30% reduction in LDL cholesterolleast 30% reduction in LDL cholesterol

10/1/2008
15
Step 6
Initiate Therapeutic Lifestyle ChangesInitiate Therapeutic Lifestyle ChangesInitiate Therapeutic Lifestyle Changes Initiate Therapeutic Lifestyle Changes (TLC)(TLC)
TLC
Weight ManagementWeight Management Weight ManagementWeight Management TLC DietTLC Diet
Saturated fat <7% of calories, cholesterol Saturated fat <7% of calories, cholesterol <200mg/day<200mg/day
Increase soluble fiber (10Increase soluble fiber (10--25g/day) and 25g/day) and ll ll / l (2 /d )/ l (2 /d )plant plant stanolsstanols/sterols (2g/day)/sterols (2g/day)
Increased Physical ActivityIncreased Physical Activity Smoking CessationSmoking Cessation

10/1/2008
16
Consider Adding Drug TherapyConsider Adding Drug TherapyConsider Adding Drug TherapyConsider Adding Drug Therapy
Drugs That Affect Lipoprotein Metabolism
ChartChart ChartChart
10/1/2008
17
HMG-CoA Reductase Inhibitors (Statins)
Most effective class of drugs for loweringMost effective class of drugs for lowering Most effective class of drugs for lowering Most effective class of drugs for lowering LDLLDL--cholesterolcholesterol
Mainstay of lipidMainstay of lipid--modifying therapy (in modifying therapy (in combination with TLC)combination with TLC)
MOA: MOA: catalyze catalyze the rate limiting step in the rate limiting step in yy g pg pcholesterol synthesischolesterol synthesis
Also have ability to decrease CRPAlso have ability to decrease CRP
Bile Acid Sequestrants
22ndnd most effective class of drugs for lowering LDLmost effective class of drugs for lowering LDL22 most effective class of drugs for lowering LDLmost effective class of drugs for lowering LDL Add to the LDLAdd to the LDL--lowering effects of other drugs lowering effects of other drugs
((statinsstatins)) MOA: MOA: lead lead to conversion of cholesterol to bile to conversion of cholesterol to bile
acids in the liveracids in the liver Not absorbed by the GI tract; do not act Not absorbed by the GI tract; do not act
systemicallysystemically Caution: Caution: May May increase TGincrease TG Space other medications Space other medications

10/1/2008
18
Nicotinic Acid (Niacin)
Oldest known lipidOldest known lipid--lowering agent still in uselowering agent still in use Usually secondary agent in combination with other drugs Usually secondary agent in combination with other drugs
due to intolerabilitydue to intolerability MOA: MOA: Exact Exact mechanism not known. mechanism not known. Appears Appears to decrease to decrease
hepatic synthesis of VLDL particles by inhibition of hepatic synthesis of VLDL particles by inhibition of mobilization of free fatty acids from peripheral tissues. mobilization of free fatty acids from peripheral tissues. Also causes a shift in LDL particles from small, dense Also causes a shift in LDL particles from small, dense particles to larger particles.particles to larger particles.A il bl i 2 f l iA il bl i 2 f l i Available in 2 formulations: Available in 2 formulations: Immediate Release (crystalline) preparations Immediate Release (crystalline) preparations Extended Release tablets Extended Release tablets
Only agent known to reduce levels of lipoprotein A Only agent known to reduce levels of lipoprotein A
Fibric Acids
Primarily used asPrimarily used as monotherapymonotherapy oror Primarily used as Primarily used as monotherapymonotherapy or or combination therapy to decrease combination therapy to decrease triglycerides and increase HDL triglycerides and increase HDL
MOA: MOA: Enhance Enhance the catabolism of the catabolism of triglyceridetriglyceride--rich remnant lipoproteins and rich remnant lipoproteins and decrease hepatic synthesis of VLDL decrease hepatic synthesis of VLDL particles particles

10/1/2008
19
Cholesterol Absorption Inhibitors
EzetimibeEzetimibe ((ZetiaZetia®®)) first member of thisfirst member of this EzetimibeEzetimibe ((ZetiaZetia ) ) first member of this first member of this class of medicationsclass of medications
MOA: MOA: Selectively Selectively inhibits the intestinal inhibits the intestinal absorption of dietary and absorption of dietary and biliarybiliary cholesterol cholesterol at the brush border of the small intestine at the brush border of the small intestine
Primary use asPrimary use as combinationcombination therapy withtherapy with Primary use as Primary use as combinationcombination therapy with therapy with statinsstatins for LDLfor LDL--lowering (lowering (monotherapymonotherapy for for selected patients)selected patients)
ENHANCE Trial
Effect of Combination Effect of Combination EzetimibeEzetimibe and Highand High--Dose Dose ggSimvastatinSimvastatin vs. vs. SimvastatinSimvastatin Alone on the Atherosclerotic Alone on the Atherosclerotic Process in Patients with Heterozygous Familial Process in Patients with Heterozygous Familial Hypercholesterolemia Hypercholesterolemia
Study evaluated carotid Study evaluated carotid intimalintimal thickness in patients with thickness in patients with familial hypercholesterolemia who were taking familial hypercholesterolemia who were taking VytorinVytorin®®
10/80 mg vs. 10/80 mg vs. simvastatinsimvastatin 80 mg alone 80 mg alone No difference in two groups in regard toNo difference in two groups in regard to intimalintimal thicknessthickness No difference in two groups in regard to No difference in two groups in regard to intimalintimal thicknessthickness 1818--20% greater decrease in LDL in patients taking 20% greater decrease in LDL in patients taking
VytorinVytorin® ® vs. vs. simvastatinsimvastatin alonealone
Kastelein JP, Akdim F, et al. Simvastatin with or without Ezetimibe in Kastelein JP, Akdim F, et al. Simvastatin with or without Ezetimibe in Familial Hypercholesterolemia. NEJM 2008;358(18):1977.Familial Hypercholesterolemia. NEJM 2008;358(18):1977.

10/1/2008
20
ENHANCE Trial (cont’d)
No difference in the incidence of cardiovascular mortality, No difference in the incidence of cardiovascular mortality, nonnon--fatal MI, nonfatal MI, non--fatal fatal stroke stroke or need for revascularization or need for revascularization This This trial not adequately powered to study these clinical trial not adequately powered to study these clinical
outcomes outcomes Overall incidence of treatmentOverall incidence of treatment--related adverse events was related adverse events was
similar between the two groups similar between the two groups Impact on Impact on Therapy Therapy
Clinical decisions to stop Clinical decisions to stop VytorinVytorin®® should not be made should not be made pp yyon the ENHANCE trial alone and should still be on the ENHANCE trial alone and should still be considered a treatment option considered a treatment option
See College of Cardiology’s (ACC) Statement on the See College of Cardiology’s (ACC) Statement on the ENHANCE trialENHANCE trial
http://www.acc.org/enhance.htm
Omega-3-Acid Ethyl Esters
LovazaLovaza®® (previously(previously OmicorOmicor®®)) LovazaLovaza (previously (previously OmicorOmicor ))
Used as an adjunct to reduce very high TG Used as an adjunct to reduce very high TG levels (>500 mg/dl) in adult patientslevels (>500 mg/dl) in adult patients
MOA: MOA: May May reduce synthesis of reduce synthesis of triglycerides in the liver triglycerides in the liver g yg y
10/1/2008
21
New Therapies - Cholesteryl Ester Transfer Protein (CETP) Inhibitor
Increase HDLIncrease HDL Phase 3 clinical trial of Phase 3 clinical trial of torcetrapibtorcetrapib (ILLUMINATE) terminated (ILLUMINATE) terminated
early due to excess CV eventsearly due to excess CV events Question of safety of drug itself vs. safety of target of Question of safety of drug itself vs. safety of target of
therapy (CETP inhibition)therapy (CETP inhibition) Newer CETP inhibitors have different chemical structuresNewer CETP inhibitors have different chemical structures
RO4607381 RO4607381 Phase 2 safety data positivePhase 2 safety data positive
C l b i l d i Ph 3 li i l i lC l b i l d i Ph 3 li i l i l Currently being evaluated in Phase 3 clinical trialCurrently being evaluated in Phase 3 clinical trial AnacetrapibAnacetrapib
Studied in phase 2 clinical trialsStudied in phase 2 clinical trials
ACC 2008: The Future of managing dyslipidemia.
New Therapies - Phospholipase A2
(PLA2) Inhibitors PhospholipasePhospholipase AA2 2 (PLA(PLA22) Inhibitors) Inhibitors
PLAPLA22 modifies LDL particles in vitromodifies LDL particles in vitro22 pp Hydrolyze phospholipidsHydrolyze phospholipids Enhanced uptake by macrophagesEnhanced uptake by macrophages Reaction products lead to activation of Reaction products lead to activation of
immunoinflammatoryimmunoinflammatory processes related to the processes related to the pathogenesis and complications of atherosclerosispathogenesis and complications of atherosclerosis
LipoproteinLipoprotein--associated (associated (LpLp))--PLAPLA2 2 and and SecretorySecretory(s)PLA(s)PLA22(s)PLA(s)PLA2 2
High plasma levels of LpHigh plasma levels of Lp--PLAPLA2 2 associated with associated with increased CV riskincreased CV risk
Inhibition of PLAInhibition of PLA22
AntiAnti--inflammatory effectsinflammatory effects Reduction of CV eventsReduction of CV events
ACC 2008: The Future of managing dyslipidemia.

10/1/2008
22
New Therapies - Phospholipase A2
(PLA2) Inhibitors
DarapladibDarapladib Selective LpPLASelective LpPLA22 InhibitorInhibitor In Phase 2/3 development with GlaxoSmithKlineIn Phase 2/3 development with GlaxoSmithKline
•• No major safety concernsNo major safety concerns•• Did not modify levels of LDL, HDL, Did not modify levels of LDL, HDL, TC TC or TGor TG•• Significant reductions in inflammatory Significant reductions in inflammatory
biomarkersbiomarkers IBISIBIS 2 study2 study IBISIBIS--2 study2 study
•• Designed to assess impact of Designed to assess impact of darapladibdarapladib on on arterial plaque compositionarterial plaque composition
•• Decision on whether to advance to Phase 3 trials Decision on whether to advance to Phase 3 trials will be madewill be made
ACC 2008: The Future of managing dyslipidemia.
New Therapies - Phospholipase A2
(PLA2) Inhibitors
VarespladibVarespladib
Potent inhibitor of sPotent inhibitor of sPLAPLA2 2
Phase 2 PLASMA trialPhase 2 PLASMA trial Marked reduction sPLAMarked reduction sPLA2 2 mass and reduced LDLmass and reduced LDL Treatment Treatment with with statinstatin: : significantly significantly greater greater
reductions in LDLreductions in LDL Twice daily administrationTwice daily administration
Phase 2b clinical trialPhase 2b clinical trial Phase 2b clinical trialPhase 2b clinical trial Reduction in sPLAReduction in sPLA2 2 and LDLand LDL Once daily administration Once daily administration
ACC 2008: The Future of managing dyslipidemia.

10/1/2008
23
New Therapies – New Formulation of Fenofibric Acid CholineCholine fenofibratefenofibrate (ABT(ABT--335):335): activeactive CholineCholine fenofibratefenofibrate (ABT(ABT 335): 335): active active
metabolite of metabolite of fenofibricfenofibric acidacidPharmacokinteticPharmacokintetic profile differs from profile differs from
fenofibratefenofibrateCombo therapy with Combo therapy with statinstatin has shown has shown
improved lipid levels compared withimproved lipid levels compared withimproved lipid levels compared with improved lipid levels compared with corresponding corresponding monotherapiesmonotherapies
If approved, will be marketed as If approved, will be marketed as TriLipixTriLipix™™
ACC 2008: The Future of managing dyslipidemia.
Step 8
Identify and Treat Metabolic SyndromeIdentify and Treat Metabolic SyndromeIdentify and Treat Metabolic SyndromeIdentify and Treat Metabolic Syndrome
10/1/2008
24
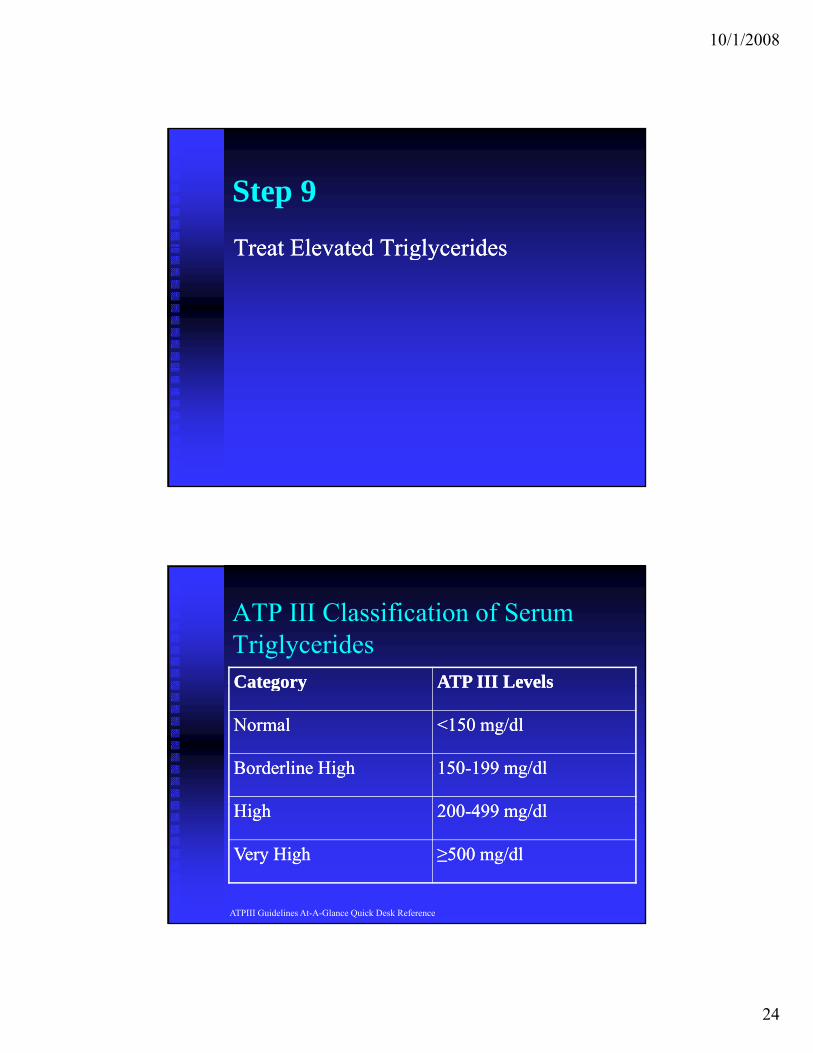
Step 9
Treat Elevated TriglyceridesTreat Elevated TriglyceridesTreat Elevated TriglyceridesTreat Elevated Triglycerides
ATP III Classification of Serum TriglyceridesCategoryCategory ATP III LevelsATP III LevelsCategoryCategory ATP III LevelsATP III Levels
NormalNormal <150 mg/dl<150 mg/dl
Borderline HighBorderline High 150150--199 mg/dl199 mg/dl
Hi hHi h 200200 499 /dl499 /dlHighHigh 200200--499 mg/dl499 mg/dl
Very HighVery High ≥500 mg/dl≥500 mg/dl
ATPIII Guidelines At-A-Glance Quick Desk Reference
10/1/2008
25
Non-HDL as Secondary Target
NonNon--HDL = Total HDL = Total Cholesterol Cholesterol –– HDLHDL Reflects the concentration of cholesterol within Reflects the concentration of cholesterol within
atherogenicatherogenic lipoprotein particleslipoprotein particles i.ei.e represents represents apoapo B carrying lipoproteinsB carrying lipoproteins VLDL, VLDL, chylomicronchylomicron remnants, VLDL remnants, IDL, remnants, VLDL remnants, IDL,
LDLLDL Used as secondary target (after targeting LDL) in patients Used as secondary target (after targeting LDL) in patients y g ( g g ) py g ( g g ) p
with elevated TGwith elevated TG If LDL goals met and TG If LDL goals met and TG ≥ ≥ 200, 200, calculate noncalculate non--HDLHDL Set nonSet non--HDL goal at 30 points higher than LDL goalHDL goal at 30 points higher than LDL goal
APhA. PharmacyAPhA. Pharmacy--Based Lipid Management. 2005Based Lipid Management. 2005
Non-HDL as Secondary Target
May be a better predictor of CVD risk thanMay be a better predictor of CVD risk than May be a better predictor of CVD risk than May be a better predictor of CVD risk than is LDL cholesterol is LDL cholesterol
Especially in statinEspecially in statin--treated patientstreated patients
Lack of additional expense in patients Lack of additional expense in patients already getting lipid panel measurementsalready getting lipid panel measurementsy g g p py g g p p
Diabetes Care 2003;26:16-23Diabetes Care 2005;28:1916Diabetes Care 2005;28:1916--19211921Circulation 2005;112:3375Circulation 2005;112:3375--33833383

10/1/2008
26
Other targets—LDL Particle Number and Size LDL particle concentration and size important predictors of CVDLDL particle concentration and size important predictors of CVD
ConcentrationConcentration Direct measure of the # of LDL particles using nuclear Direct measure of the # of LDL particles using nuclear
magnetic resonance (NMR)magnetic resonance (NMR) SizeSize
LDL particle size can also be measuredLDL particle size can also be measured AtherogenicAtherogenic properties of small dense LDL particlesproperties of small dense LDL particles Unclear if particle size measurement of valueUnclear if particle size measurement of value
Limitations of NMR measurementLimitations of NMR measurement Technique not widely availableTechnique not widely available Relatively expensiveRelatively expensive Need for more data confirming the accuracy of the methodNeed for more data confirming the accuracy of the method
Consensus statement from the American Diabetes Association and the American Consensus statement from the American Diabetes Association and the American College of Cardiology Foundation. Diabetes Care 2008;31(4):811College of Cardiology Foundation. Diabetes Care 2008;31(4):811--822.822.
Other Targets—ApoB-100
Represent total burden of particles considered Represent total burden of particles considered p pp pmost atherogenicmost atherogenic Chylomicrons, VLDL, IDL, LDL, Lp(a) Chylomicrons, VLDL, IDL, LDL, Lp(a)
particles each contain a single apoB moleculeparticles each contain a single apoB molecule Some studies suggest that once LDL lowered, Some studies suggest that once LDL lowered,
apoB may be more effective way to assess residual apoB may be more effective way to assess residual CVD risk and determine therapy adjustmentsCVD risk and determine therapy adjustments
ApoB measurementsApoB measurements Do not require fasting sampleDo not require fasting sample Standardized but not widely availableStandardized but not widely available
Consensus statement from the American Diabetes Association and the American College of Consensus statement from the American Diabetes Association and the American College of Cardiology Foundation. Diabetes Care 2008;31(4):811Cardiology Foundation. Diabetes Care 2008;31(4):811--822.822.
10/1/2008
27
Lipoprotein Management in Patients With
C di t b li Ri kCardiometabolic Risk:
Consensus Statement from the American Diabetes AssociationAmerican Diabetes Association
and the American College of Cardiology Foundation
Residual Risk on Statin Therapy
Proven evidence that Proven evidence that statinstatin therapy reduces therapy reduces pypycardiovascular riskcardiovascular risk However, residual risk remains in treated However, residual risk remains in treated
patientspatients Studies neededStudies needed
To determine whether residual risk can be To determine whether residual risk can be decreased by interventions effecting other decreased by interventions effecting other y gy glipoproteins (i.e. HDL, small dense LDL)lipoproteins (i.e. HDL, small dense LDL)
To directly determine if other therapeutic To directly determine if other therapeutic targets (i.e. targets (i.e. apoBapoB, other lipoproteins) , other lipoproteins) are are superior to LDLsuperior to LDL
Consensus statement from the American Diabetes Association and the American College of Consensus statement from the American Diabetes Association and the American College of Cardiology Foundation. Diabetes Care 2008;31(4):811Cardiology Foundation. Diabetes Care 2008;31(4):811--822.822.

10/1/2008
28
Summary of Recommendations
Statin therapy for the majority of dyslipoproteinemic adult Statin therapy for the majority of dyslipoproteinemic adult py j y y p ppy j y y p ppatients with cardiometabolic risk (CMR)patients with cardiometabolic risk (CMR)
In patients with CMR on statin therapy, therapy should be In patients with CMR on statin therapy, therapy should be guided with apoB measurements and treatment to apoB guided with apoB measurements and treatment to apoB goals as well as LDL cholesterol and nongoals as well as LDL cholesterol and non--HDL cholesterol HDL cholesterol assessmentsassessments
Treatment goals that address high lifetime risk of patients Treatment goals that address high lifetime risk of patients with dyslipoproteinemia and CMR (see table)with dyslipoproteinemia and CMR (see table)with dyslipoproteinemia and CMR (see table)with dyslipoproteinemia and CMR (see table)
Clinical trials to determine whether pharmacologic therapy Clinical trials to determine whether pharmacologic therapy required to achieve very low levels of atherogenic required to achieve very low levels of atherogenic lipoproteins is safe and costlipoproteins is safe and cost--effectiveeffective
Consensus statement from the American Diabetes Association and the American Consensus statement from the American Diabetes Association and the American College of Cardiology Foundation. Diabetes Care 2008;31(4):811College of Cardiology Foundation. Diabetes Care 2008;31(4):811--822.822.
Suggested Treatment Goals in Patients with CMR and Lipoprotein Abnormalities
AALDL LDL Goal Goal (mg/dl)(mg/dl)
NonNon--HDL HDL Goal Goal (mg/dl)(mg/dl)
ApoB ApoB Goal Goal (mg/dl)(mg/dl)
HighestHighest--risk patientsrisk patients11 <70<70 <100<100 <80<80
HighHigh--risk patientsrisk patients22 <100<100 <130<130 <90<901Including those with: 1) known CVD or 2) diabetes plus ≥ 1 additional major CVD risk factors*
2Including those with: 1) no diabetes or known clinical CVD but ≥ 2 additional major CVD risk factors or 2) diabetes but no other major CVD risk factors
*Other major risk factors = smoking, HTN, family history of premature CAD

10/1/2008
29
Questions?
References
APhAAPhA. . PharmacyPharmacy--Based Based Lipid Management. Lipid Management. 20052005 BlumlBluml BM, BM, McKenneyMcKenney JM, JM, CzirakyCziraky MJ. Pharmaceutical care services MJ. Pharmaceutical care services
and results in Project and results in Project ImPACTImPACT: : HyperlipidemiaHyperlipidemia. J Am . J Am PharmPharm Assoc Assoc 2000;40:1572000;40:157--165. 165.
BrunzellBrunzell JD, Davidson M, et al. JD, Davidson M, et al. Lipoprotein Lipoprotein Management in Patients Management in Patients With With CardiometabolicCardiometabolic Risk: Risk: Consensus Consensus statement from the American statement from the American Diabetes Association and the American College of Cardiology Diabetes Association and the American College of Cardiology Foundation. Foundation. Diabetes Diabetes Care 2008;31(4):811Care 2008;31(4):811--822.822.
Stone and Blum. Management of Lipids in Clinical Practice. 6th edition. 2006
ATPIII Guidelines At-A-Glance Quick Desk Reference (http://www.nhlbi.nih.gov/guidelines/cholesterol/atglance.pdfhttp://www.nhlbi.nih.gov/guidelines/cholesterol/atglance.pdf))
KasteleinKastelein JP, JP, AkdimAkdim F, et al. F, et al. SimvastatinSimvastatin with or without with or without EzetimibeEzetimibe in in Familial Hypercholesterolemia. NEJM 2008;358(18):1977.Familial Hypercholesterolemia. NEJM 2008;358(18):1977.

10/1/2008
30
References
http://www.acc.org/enhance.htmhttp://www.acc.org/enhance.htm Davidson MH and Brookes L. What to Add to a Statin: New Lipid-
Regulating Therapies Continue in Development. ACC 2008: The Future of managing dyslipidemia.
Lu W, Resnick HE, et al. Non-HDL cholesterol as a predictor of cardiovascular disease in type 2 diabetes: the Strong Heart Study. Diabetes Care 2003;26:16-23.
Liu J, Sempos C, et al. Joint distribution of nonLiu J, Sempos C, et al. Joint distribution of non--HDL and LDL HDL and LDL cholesterol and coronary heart disease risk prediction among cholesterol and coronary heart disease risk prediction among individuals with and without diabetes. Diabetes Care 2005;28:1916individuals with and without diabetes. Diabetes Care 2005;28:1916--;;1921.1921.
Pischon T, Girman CJ, et al. NonPischon T, Girman CJ, et al. Non--high density lipoprotein cholesterol high density lipoprotein cholesterol and apolipoproein B in the prediction of coronary heart disease in men. and apolipoproein B in the prediction of coronary heart disease in men. Circulation 2005;112:3375Circulation 2005;112:3375--3383.3383.
Recommended

















