
UW HEALTH PRIMARY CARE / BEHAVIORAL
HEALTH INTEGRATION
UNITED WAY FORUM
September 22, 2014
1

UW Health Overview

UW Health Enterprise Facts and Figures• UW Health Healthcare Entities
– UW Hospital and Clinics (566 beds)– American Family Children’s Hospital (61
beds)– UW Medical Foundation (1 of 10 largest
medical groups in nation)
• Facts and Figures– 26,797 Inpatient Admissions– 2,317,332 Outpatient Visits– 43,806 Emergency Visits– 1,200+ Physicians; 10,000+ Employees– Level 1 Adult and Pediatric Trauma
Center– Comprehensive Cancer Center– 48 Primary Care & Specialty Clinics – Outreach sites in 50+ communities

UW Health Primary Care
• 38 Primary Care Clinics*– Family Medicine = 21– General Internal Medicine = 9– Pediatrics = 8
• 194 Primary Care Physicians
• 266,000 medically homed patients– 35,600 with behavioral health diagnoses
• Top diagnoses: depression, anxiety, alcohol
• *8 clinics with on-site Behavioral Health provider

5
Family Medicine
General Internal Medicine
Pediatrics
Dept of Psychiatry LocationsBehavioral Health Provider Embedded in Clinic
ΨΨ
Ψ
Ψ

Impetus for Primary Care / Behavioral Health Integration • In pursuit of the Triple AIM
– Improve health of populations– Improve experience of care– Reduce per capita cost
• Primary Care Redesign launched 2008– Patient Centered Medical Home Recognition
• Behavioral Health Analysis 2013– Demand exceeds capacity
• 46% of behavioral health care is managed by UW Health PCPs• 85% of PCPs not satisfied with access to behavioral health services
– Depression is #1 outpatient and inpatient diagnosis– Poor access and follow-up for behavioral health services– Poor continuity of care and communication between providers– Insurance barriers– Led to system-wide initiative to improve behavioral health services
Institute for Healthcare Improvement
Primary Care / Behavioral Health Integration Model Development
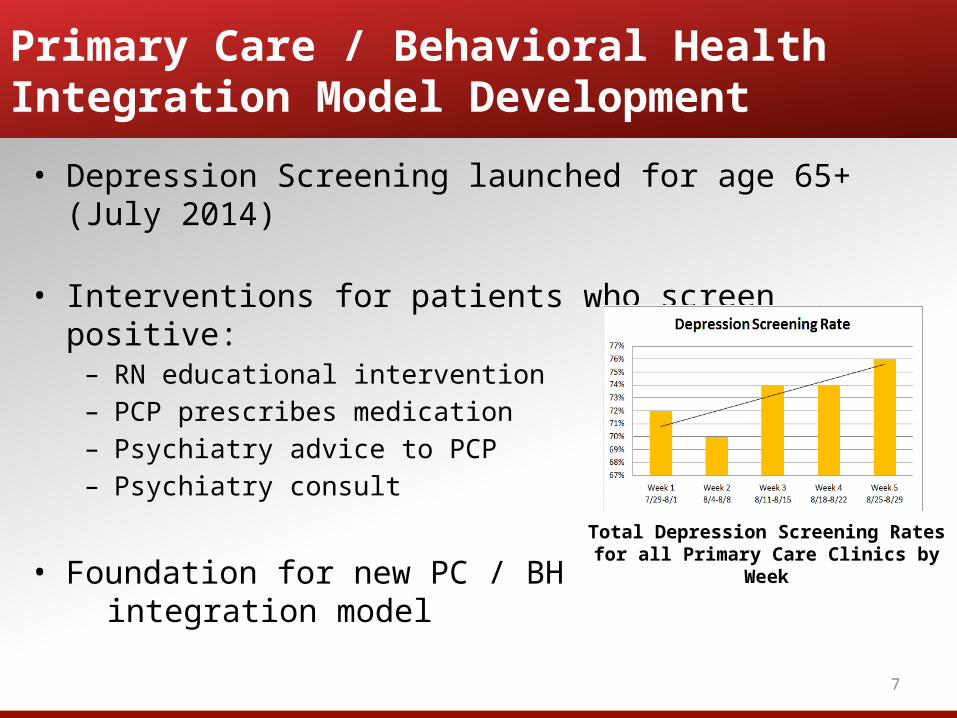
• Depression Screening launched for age 65+ (July 2014)
• Interventions for patients who screen positive:– RN educational intervention– PCP prescribes medication – Psychiatry advice to PCP – Psychiatry consult
• Foundation for new PC / BH integration model
7
Total Depression Screening Rates for all Primary Care Clinics by Week

• Team-based and patient-centered• Co-location is not Collaborative Care. Team members learn to work differently.
Collaboration
• Treat-to-target• Treatments are actively changed until the clinical goals are achieved
• Evidenced-based care
Stepped Care
• All patients tracked in a registry• No one falls through the cracks• Population-based approach
Close follow-up
8
Primary Care / Behavioral Health Integration Model Development: Collaborative Care

9
DRAFT UW Health Collaborative Care Model
BH Complex Case Management
Specialty/Org Resources
Specialty BH CarePsychiatrist MS TherapistPsychologist
PC Clinic Resources
PCP
PatientCare Manager (RN Care Coordinator
Dep, DM, HTN)
Adapted from University of Washington, 2013
ConsultingPsychiatrist

• September 2014– Endorsed by Primary Care and Behavioral Health
leadership
• October 2014 – January 2015– Model design and build
• February – March 2015– Test model in five Primary Care Clinic locations
10
Primary Care / Behavioral Health Integration Model Development

• Strengths– Patient-centered – Evidence-based model– Proven cost-savings– Aligned with UW Health Primary Care Redesign and other
organizational imperatives
• Challenges– Paradigm shift for key roles – Investment in time and resources– Adapting model to variation in UW Health Primary Care clinics
11
Primary Care / Behavioral Health IntegrationModel Strengths and Challenges
Recommended


















