Tracking Expenditure for HIV and AIDS in Africa ~
Cross-Country Comparisons
Guthrie, T., Kioko, U.Inaugural Conference of the African Health Economics and Policy Association
Accra - Ghana, 10th - 12th March 2009PS 04/8

Objectives•Determine the total flows of financing and
expenditures for HIV/AIDS, from all international and public (domestic) sources of financing
•To identify the flow of expenditures by sources, agent, providers of services activities, and target population
•To make recommendations for improved efficiency and prioritization of HIV and AIDS spending, and for improved financial information systems.

Methodology• Review of UNGASS Indicator 1 for SSA countries
(Source: UNAIDS Global Report 2008 Annex2)• Review of Country NASA Reports for further detail:
Ghana, Botswana, Zambia, Swaziland• National AIDS Spending Assessment is an approach to
comprehensively measure:▫All spending for HIV/AIDS▫From all sources, through agents, providers, activities to
beneficiaries▫From a multi-sectoral perspective▫According to interventions reflected in the NSPs▫Allows countries to monitor their own progress towards
the national and international commitments.• Acknowledgements to UNAIDS, the NACs and NASA
team members for access to their data

Comparison of UNGASS Indicator1 - Sources of Financing for HIV/AIDS
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
SSA Low Income Countries Public and International Contributions to Spending on HIV/AIDS 2006
Internat. (av 75%)Public (av 25%)
% o
f Pu
blic
+ I
nter
nati
onal
Source: UNAIDS Global Report 2008 Annex 2

Comparison of UNGASS Indicator1 - Sources of Financing for HIV/AIDS
Cameroon Lesotho Swaziland Mauritius South Africa
Botswana0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%SSA Middle Income Countries Public and International Con-
tributions to Spending on HIV/AIDS 2006
Internat. (av 48%)Public (av 52%)
% o
f Pub
lic +
Inte
rnat
iona
l
Source: UNAIDS Global Report 2008 Annex 2
Low Middle Income Upper Middle Income

SSA Low Income Countries HIV Prevalence (%) and Spending per Capita on HIV/AIDS (2006, in current US$)
Nigeria DRC
Sene
gal
Ghana
Sierra
Leon
e
Eritre
aNige
rTo
go
Cote d'
Ivoire Mali
Burkin
a Fas
o
C.Afri
can R
epub
lic
Mozam
bique
Rwanda
Zimba
bwe
Zambia
0.00
2.00
4.00
6.00
8.00
10.00
12.00
14.00
16.00
18.00
20.00
Per Capita Spending on HIV/AIDS (US$) HIV prevalence (%)

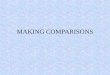
Per Capita HIV/AIDS Spending (current US$) & HIV Prevalence (%) in Middle Income SSA Countries (2006)
Mauritius Cameroon South Africa Lesotho Swaziland Botswana
$1 $2 $13 $14
$51
$87
18.3 23.0 26.0 24.0
Per capita HIV/AIDS Spending (US$) HIV prevalence (%)
Source: UNAIDS Global Report 2008 Annex 2 (own calcs)

Using Detailed NASA dataFrom Botswana, Zambia, Swaziland, Ghana

Levels & Sources of Financing (US$m, 2006)
Botswana Swaziland Zambia Ghana -
50,000,000
100,000,000
150,000,000
200,000,000
250,000,000
Internat. Contrib. (av 58.8%)Public contrib. (av 41.2%)

Agents of HIV/AIDS Spending (US$m, 2006)
Botswan
a
Swaz
iland
Zambia
Ghana
-
50,000,000
100,000,000
150,000,000
200,000,000
250,000,000
Local (NGO / pvt) AgentsExternal AgentsPublic Agents
US$

Providers of HIV/AIDS Services (US$m, 2006)
Swaziland Zambia -
50,000,000
100,000,000
150,000,000
200,000,000
250,000,000
LNGO & other providersExternal ProvidersPublic providers
US$

AIDS Spending Activities ~ Priorities (US$m, 2006)
Ghana Botswana Zambia Swaziland0
50,000,000
100,000,000
150,000,000
200,000,000
250,000,000
Research (HIV- and AIDS-Related) Community Development & Enhanced Environment Social mitigationHuman Resource IncentivesProgrm. Devmt & Strengthen HCSOrphans and Vulnerable Children (OVC) Treatment and care components Prevention Programmes

Public Spending Categories (2003-2005)
0
100,000,000
200,000,000
300,000,000
400,000,000
500,000,000
600,000,000
700,000,000
800,000,000
900,000,000
1,000,000,000
2003 2004 2005
Pula
FN 8..HIV- and AIDS-Related Research
FN 7..Community Development &Enhanced Environment
FN 6..Social mitigation
FN 5..Human Resources for HIV andAIDS activities
FN 4..Prog.Devmt & HSS strengthening
FN 3..Orphans and Vulnerable Children(OVC)
FN 2..Treatment and care components Total
FN 1..Prevention Programmes
Botswana ~ Public Trends (Pula, 2003-2005)

Swaziland ~ HIV/AIDS Priorities by Source of Funds (SZL, 2006)
-
50,000,000
100,000,000
150,000,000
200,000,000
250,000,000
300,000,000
350,000,000
400,000,000
Public funds Internationalfunds
Total
Sources of funds
SZL
HIV and AIDS realatedresearch(Excluding operationalresearch)Enabling Environment and CommunityDevelopment
Social Protection and Social Services(EXCLUDING OVC)
Human Resources' recruitments andRetention Incentive - Human Capital
ProgrammeManagement andadministration strengthening
OVC
Care and Treatments
Prevention

Swaziland ~ funds for Programme Management by NERCHA (SZL, 2006)
-
5,000,000
10,000,000
15,000,000
20,000,000
25,000,000
30,000,000
35,000,000
40,000,000
45,000,000
50,000,000
Other sources toNERCHA
GFATM toNERCHA
TOTAL
SOURCES OF FUNDS
SZL
Upgrading and construction ofinfrastructure not elsewhereclassified (n.e.c)
Upgrading laboratoryinfrastructure and new equipment
Serological-surveillance(Serosurveillance)
Monitoring and evaluation
Planning and coordination
Transaction costs
Programme Administration

Swaziland Prevention Spending (SZL, 05/06-06/07)
-
10,000,000
20,000,000
30,000,000
40,000,000
50,000,000
60,000,000
70,000,000
2005/ 2006 2006/ 2007
YEAR
SZL
Prevention activities not elsewhere classified (n.e.c.)
Post-exposure prophylaxis (PEP)
Blood safety
Prevention of mother-to-child transmission(PMTCT)
Prevention, diagnosis and treatment of sexuallytransmitted infections (STI) (Improving managementof STI) Public and commercial sector condom provision
Prevention programmes in the workplace
Prevention of HIV transmission aimed at personsliving with HIV (PLHA)
Prevention - Youth out-of-school
Prevention - Youth in school
Risk-reduction for vulnerable and specialpopulations (Programmes for vulnerable and specialpopulations)Voluntary counselling and testing
Community mobilization
Communication for social and behavioral change
Preventio
n
CommMob
l
VCT
CondomsPMTCTBlood Safety

Swaziland ~ Social Protection spending (SZL, 05/06-06/07)
-
5,000,000
10,000,000
15,000,000
20,000,000
25,000,000
2005/ 2006 2006/ 2007
YEAR
SZL
Social protection services and social servicesnot elsewhere classified (n.e.c)
HIV-specific income generation projects
Social protection through provision of socialservices
Social protection through in-kind benefits
Social protection through monetary benefits

Swazi~ environment and community development spending (SZL, 2006/07)
-
1,000,000
2,000,000
3,000,000
4,000,000
5,000,000
6,000,000
7,000,000
Public Funds International funds Total
SOURCES OF FUNDS
SZL
Enabling environment and communitydevelopment not elsewhere classified(n.e.c)
AIDS-specific programmes focused onwomen
AIDS-specific Institutional Development
Human rights
Advocacy and strategic communication

Beneficiaries of HIV/AIDS Spending(%, 2006)
Botswana Swaziland Zambia Ghana0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
General PopulationAccessibleVulnerableMARPSPLWHA

To what Degree Does HIV/AIDS Spending Contribute to
General health systems strengthening?

Botswana HIV Spending that may Contribute to general HSS (9.83% of THAE)
Blood safety 5%
Opportunistic infection (OI) prophylaxis
80%
Opportunistic infections’ (OI)
treatment 3%
Monitoring and evaluation
9%
Upgrading laboratory in-frastructure and new
equipment 4%

HIV/AIDS Spending on HSS & General Health:Zambia 2007, 15% of THAE Swaziland, 11% of THAE
Blood safety 11%
Lab. monitorg
1%OI
treatmt 20%
M&E16%
Operatn research
2%
Upgrade lab. In-frast.&
new equipmt
32%
Other infrast.
devpmt
17%
Blood safety 1%
Safe medical inject
1% Lab.
moni-torg
14%
OVC Basic health care 17%
M&E18%
Drug
supply systems 45%

Recommendations•Need for more sustainable predictable
financing for HIV/AIDS and health•Need for increasing public agents ie. Control
of funds ~ through common funds, DBS, IHPs.•LNGOs playing important role in delivery of
HIV/AIDS services ~ need to be supported through efficient funding mechanisms
•Treatment requiring increasing share of financing, prevention and other interventions requiring increasing, especially mitigation and social protection activities

Recommendations cont.•Increase public funds for enabling
environment esp. Promotion and protection of human rights
•Improve output indicators to enable beneficiary incidence analysis
•Increase funds for MARPs and vulnerable groups
•Increase HSS funding and mechanisms (eg.IHPs) and increase allocations to HIV/AIDS activities that contribute to general HSS (eg. Blood safety, laboratories, upgrading facilities)

Recommendations cont.• Increasing alignment with NSPs, but some
donors still have own agenda, own systems ~ need harmonisation
• Increase absorptive capacity:▫Reduce donor ‘dumping’ of funds at the end of the
financial year▫Improve predictability of donor commitments, over
longer period▫Increase speed of disbursements, reduce tedious
systems, while improving public accountability systems
▫ Improve public programmatic and human resource capacity to deliver services

Recommendations cont.•Improve public financial reporting &
information systems•Routine resource tracking ~ institutionalise
NASA in M&E systems•Harmonise to 1 national system for reporting
on commitments, disbursements & spending•Civil society play greater role in monitoring
public spending & in sharing their own spending activities
•Critical to have good financial monitoring systems in place before implementing IHPs etc.

Thank YouTeresa GuthrieCentre for Economic Governance and AIDS in Africa Email: [email protected]: +27-21-425-2852Cell: +27-82-872-4694
Recommended