The Present and Future of Hepatitis B, C & E
Eyob L. Feyssa, MD, MPH, FACP, Dipl. ABOMDirector, Viral Hepatitis Program
Einstein Healthcare Network
Advances in Liver Disease 2018: A Year in Review
Disclosure of Conflicts of Interest
• Eyob L. Feyssa, MD, MPH, FACP, Dipl. ABOM has affiliations with Gilead Sciences, Merck, Abbvie, Salix Dova, and Conatus.
• I have included discussion on unlabeled uses of a commercial product or an investigational use of a product not yet approved for this purpose

Learning Objectives
Interpret current evidence for individualizing antiviral therapy choices in chronic hepatitis B and C infections
Review data on available evidence of benefits of antiviral therapy in unique at risk population
• Summarize the benefits of Hepatitis C therapy beyond virologic cure
Updates: Natural History and treatment of chronic HBV infection
Slide 2
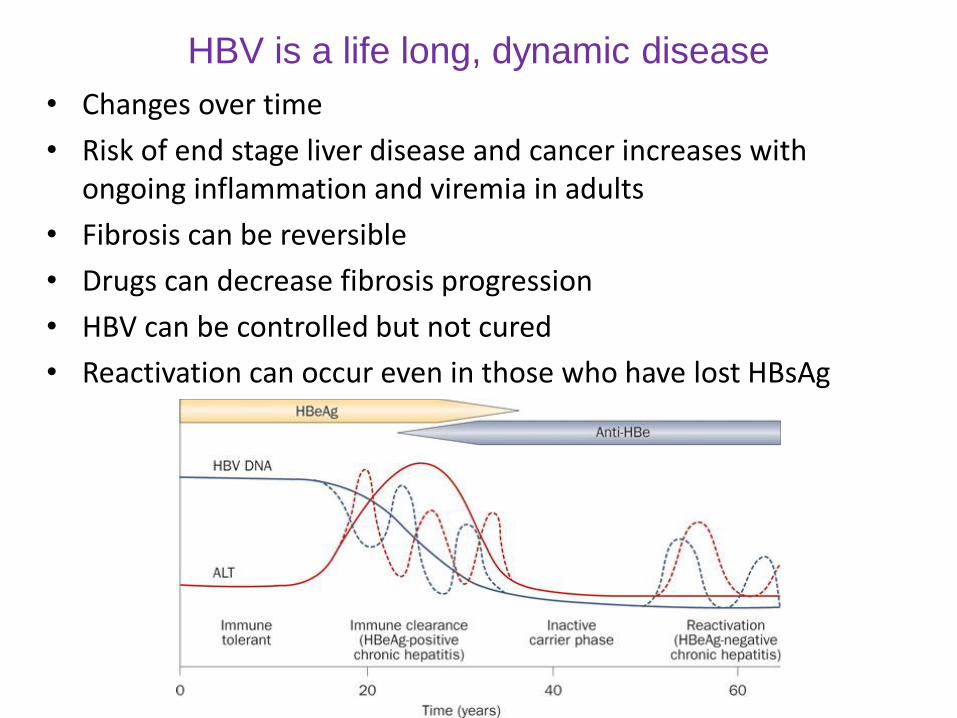
HBV is a life long, dynamic disease
• Changes over time
• Risk of end stage liver disease and cancer increases with ongoing inflammation and viremia in adults
• Fibrosis can be reversible
• Drugs can decrease fibrosis progression
• HBV can be controlled but not cured
• Reactivation can occur even in those who have lost HBsAg
Slide 13
Approved HBV treatments
Interferon alfa-2b – 1991 Lamivudine – 1998 Adefovir – 2002 Entecavir – 2005 Peginterferon alfa-2a – 2005 Telbivudine – 2006 Tenofovir - 2008
For HIV: Emtricitabine Tenofovir + emtricitabine (single pill co-
formulation) Tenofovir alafenamide (TAF) 2016
Novel, Targeted prodrug of Tenefovir 25 mg daily dosing vs TDF 300 mg daily
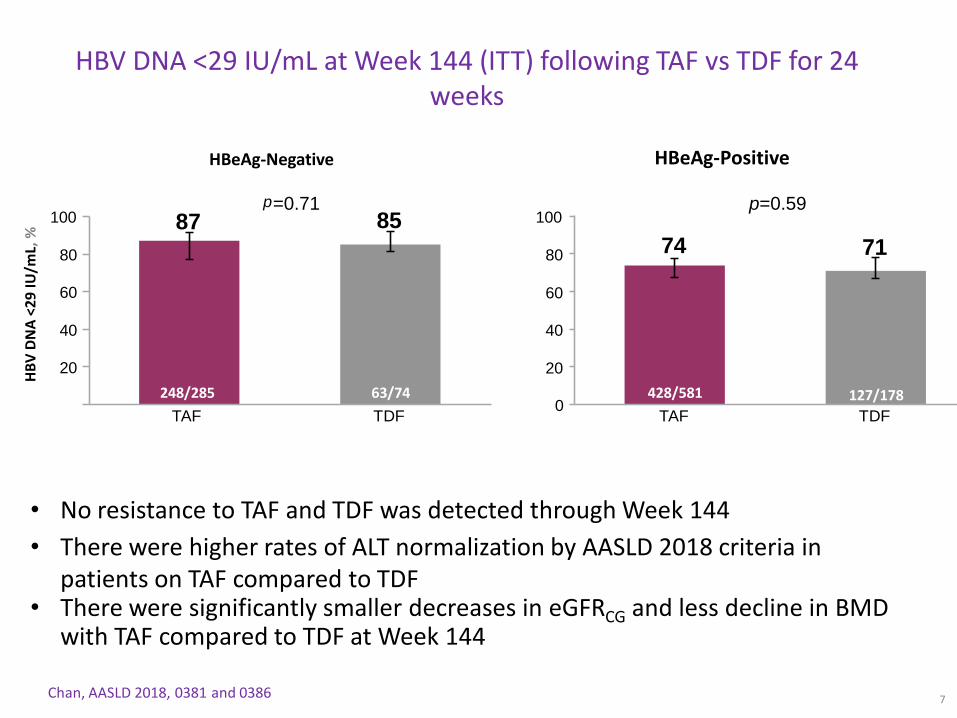
HBV DNA <29 IU/mL at Week 144 (ITT) following TAF vs TDF for 24 weeks
Chan, AASLD 2018, 0381 and 0386
• No resistance to TAF and TDF was detected through Week 144
• There were higher rates of ALT normalization by AASLD 2018 criteria in patients on TAF compared to TDF
• There were significantly smaller decreases in eGFRCG and less decline in BMD with TAF compared to TDF at Week 144
7
p=0.7187 85
20
40
60
80
100
TAF TDF
74 71
0
20
40
60
80
100
TAF TDF
p=0.59
HBeAg-Negative HBeAg-Positive
HB
V D
NA
<2
9 IU
/mL,
%
248/285 63/74 428/581 127/178
Slide 10
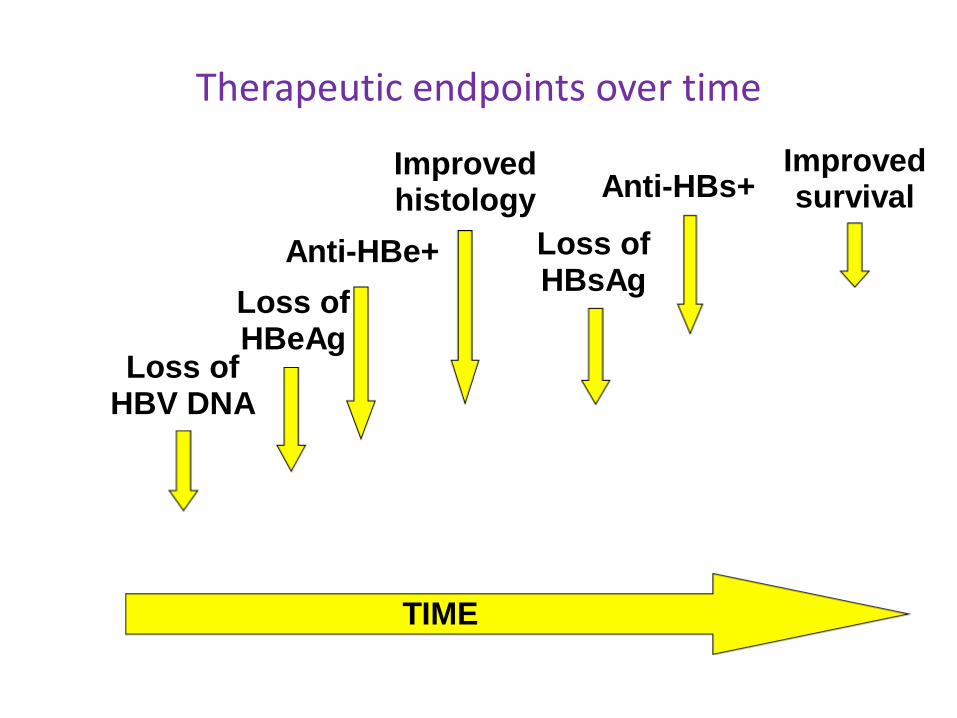
Therapeutic endpoints over time
TIME
Loss of HBeAg
Loss of HBV DNA
Anti-HBe+ Loss ofHBsAg
Anti-HBs+Improvedsurvival
Improvedhistology

Incidence and predictors of HBsAg Seroclerance
• Retrospective Study 1 North American and 8 Asian centers
– 10,614 CHB patients treatment Naïve
– two undetectable HBsAg results six months apart.
Yee Hui Yeo et al; AASLD 2018: #212
• Low seroclearance rate • annual rate of 1.33%
(95% CI: 1.26-1.40)• 20-year cumulative
incidence rate 25.49%• Improved therapy is Needed
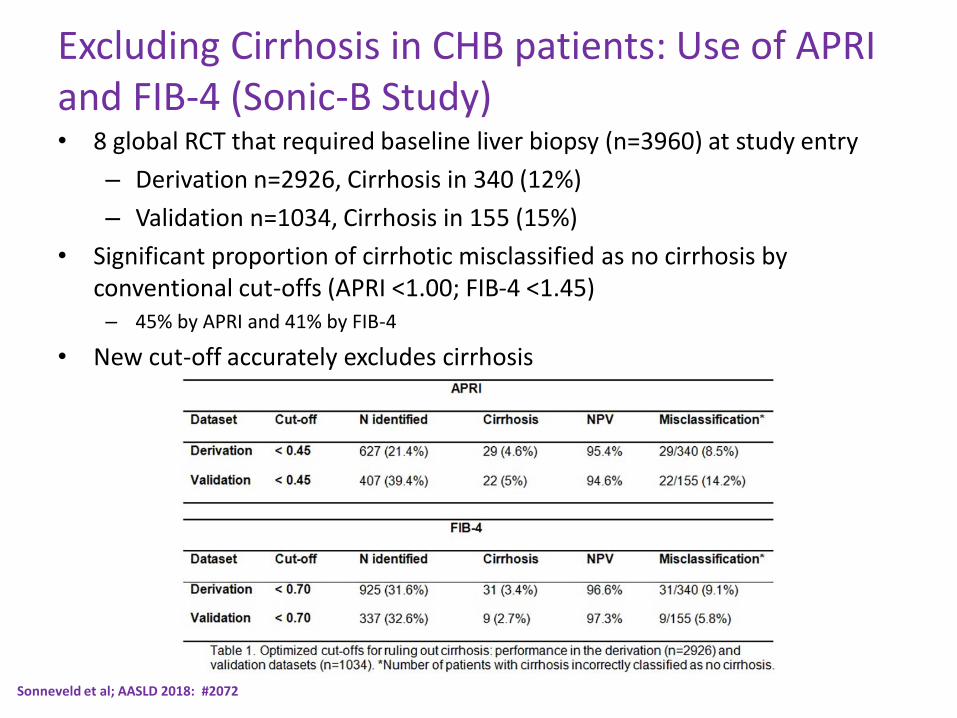
Sonneveld et al; AASLD 2018: #2072
Excluding Cirrhosis in CHB patients: Use of APRI and FIB-4 (Sonic-B Study)• 8 global RCT that required baseline liver biopsy (n=3960) at study entry
– Derivation n=2926, Cirrhosis in 340 (12%)
– Validation n=1034, Cirrhosis in 155 (15%)
• Significant proportion of cirrhotic misclassified as no cirrhosis by conventional cut-offs (APRI <1.00; FIB-4 <1.45) – 45% by APRI and 41% by FIB-4
• New cut-off accurately excludes cirrhosis

Hsu et al; AASLD 2018: #264
Treatment benefit in minimal disease HBV infected patients
• Double Blind RCT of TDF vs Placebo in CHB HBV DNA >2,000IU/ml and ALT 1-2XULN with paired liver Bx at 0 and 3 years. (Taiwan)
– 132 paired liver biopsy data (65 TDF and 67 placebo)
• TDF treatment associated with
– Less progression of fibrosis and progression to cirrhosis
– Reduced inflammation score, HBV DNA and ALT. Clarify whether tenofovir disoproxil fumarate (TDF) could prevent disease progression in CHB patients with minimally raised ALT.
Liem et al; AASLD 2018: #268
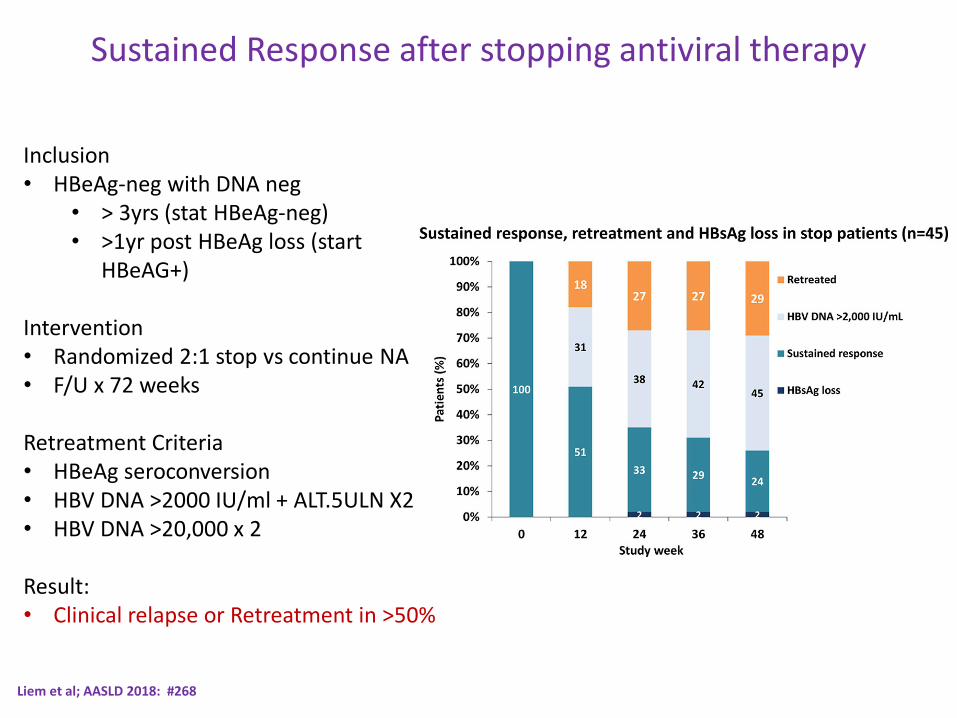
Sustained Response after stopping antiviral therapy
Inclusion• HBeAg-neg with DNA neg
• > 3yrs (stat HBeAg-neg)• >1yr post HBeAg loss (start
HBeAG+)
Intervention• Randomized 2:1 stop vs continue NA• F/U x 72 weeks
Retreatment Criteria• HBeAg seroconversion• HBV DNA >2000 IU/ml + ALT.5ULN X2• HBV DNA >20,000 x 2
Result:• Clinical relapse or Retreatment in >50%

Papatheodoridis et al; AASLD 2018: #17
HCC risk after the First 5 Years of ETV or TDF Therapy in Caucasian Chronic Hepatitis B (CHB) Patients of the PAGE-B Cohort
• 1951 adult Caucasians with CHB±compensated cirrhosis
• 1427 (73%) have completed followup >5 years without HCC until year 5 (age at year 5:57±13 years, males:70%, baseline cirrhosis:26%).
– After year 5, HCC developed exclusively in patients older than 50 years.
– HCC surveillance should continue in all patients >50 years old and probably in the few cirrhotics ≤50 years old.

Summary of HBV in 2018
• HBV is a lifelong and dynamic disease
• Spontaneous HBsAg clearance (functional cure) rate is low
• Virologic suppression with TAF is comparable with TDF
– offering lower effect / changes in eGFR and bone mineral density.
• New threshold for excluding cirrhosis using APRI and FIB-4
• Earlier antiviral intervention during the intermediate phase before ALT elevation may prevent unnecessary clinical events.
• Rate of sustained response is low after stopping therapy and warrants continuation of antiviral therapy.
• HCC occurs even with NA therapy. Surveillance recommended.
Present and Future considerations on HCV care
• HCV in US
– Deadliest infectious disease
– 3.5 million Americans affected
– Multiple effective DAA therapies with SVR > 95%
– AASLD/IDSA recommends all patient with HCV be offered therapy (www.HCVguidelines.org)
• HCV in 2018 and at the liver meeting– Challenges in treating high-risk population
– Data on benefits of HCV therapy beyond SVR
– HCV, DAA therapy and HCC risk
Introduction
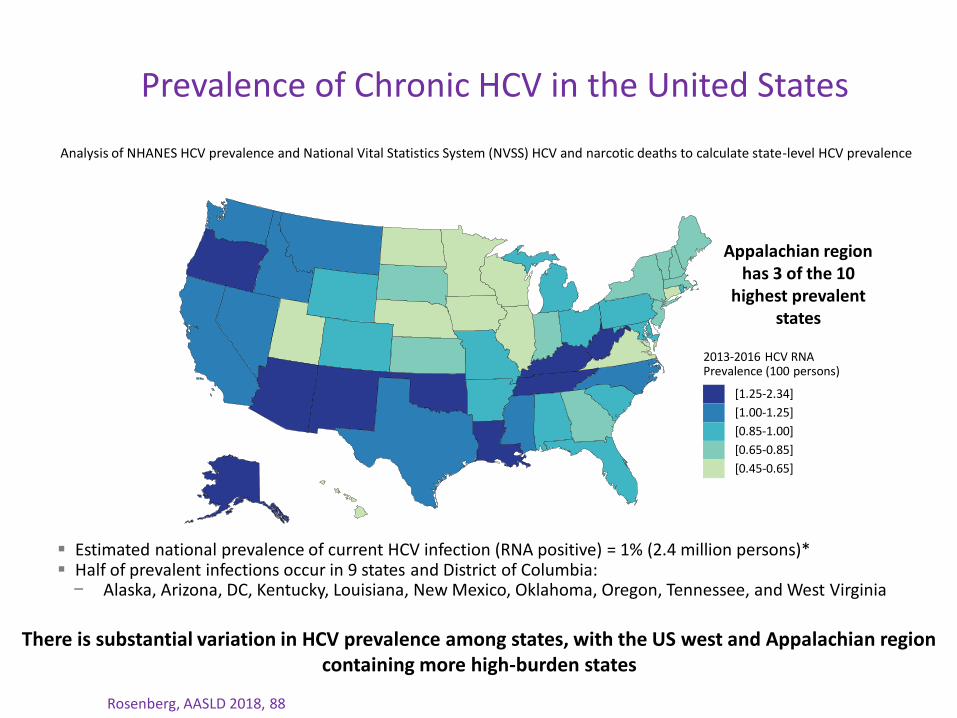
Prevalence of Chronic HCV in the United States
Analysis of NHANES HCV prevalence and National Vital Statistics System (NVSS) HCV and narcotic deaths to calculate state-level HCV prevalence
Rosenberg, AASLD 2018, 88
There is substantial variation in HCV prevalence among states, with the US west and Appalachian region containing more high-burden states
Estimated national prevalence of current HCV infection (RNA positive) = 1% (2.4 million persons)* Half of prevalent infections occur in 9 states and District of Columbia:− Alaska, Arizona, DC, Kentucky, Louisiana, New Mexico, Oklahoma, Oregon, Tennessee, and West Virginia
Appalachian region has 3 of the 10
highest prevalent states
2013-2016 HCV RNAPrevalence (100 persons)
[1.25-2.34]
[1.00-1.25]
[0.85-1.00]
[0.65-0.85]
[0.45-0.65]
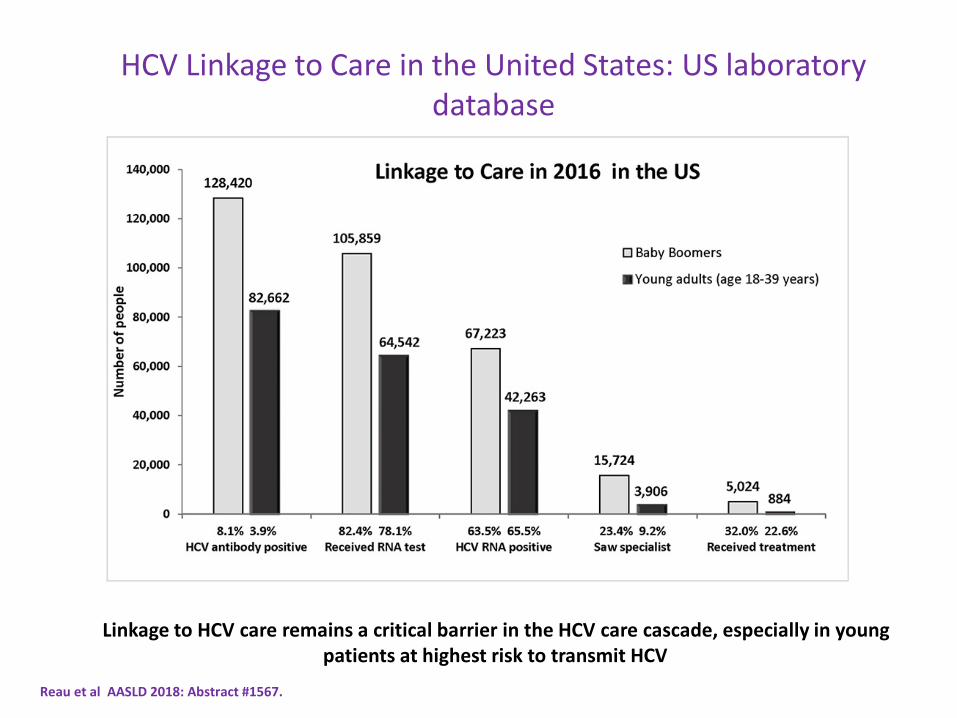
Reau et al AASLD 2018: Abstract #1567.
Linkage to HCV care remains a critical barrier in the HCV care cascade, especially in young patients at highest risk to transmit HCV
HCV Linkage to Care in the United States: US laboratory database

Current therapy: Real world data
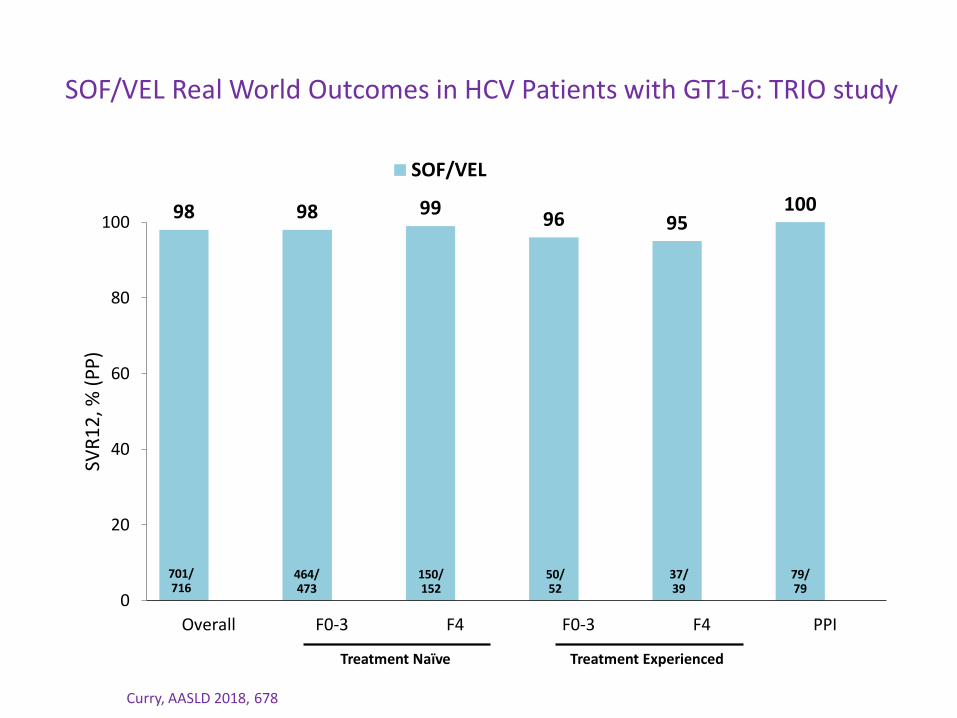
SOF/VEL Real World Outcomes in HCV Patients with GT1-6: TRIO study
Curry, AASLD 2018, 678
98 98 9996 95
100
0
20
40
60
80
100
Overall F0-3 F4 F0-3 F4 PPI
SVR
12
, % (
PP
)
SOF/VEL
Treatment Naïve Treatment Experienced
701/716
464/473
150/152
50/52
37/39
79/79
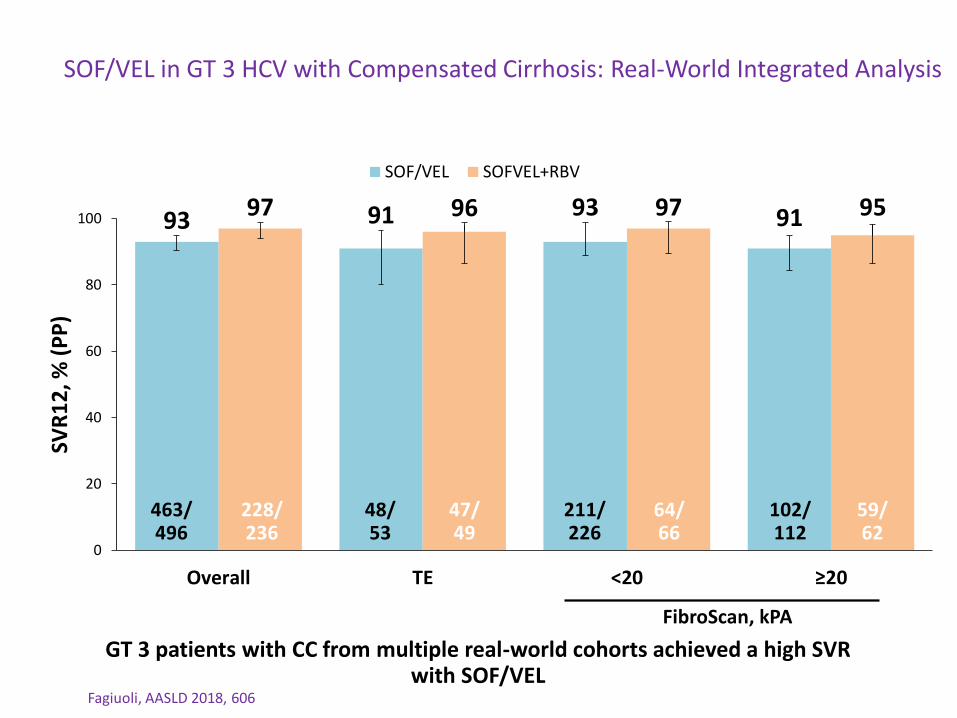
SOF/VEL in GT 3 HCV with Compensated Cirrhosis: Real-World Integrated Analysis
Fagiuoli, AASLD 2018, 606
GT 3 patients with CC from multiple real-world cohorts achieved a high SVR with SOF/VEL
93 91 93 9197 96 97 95
0
20
40
60
80
100
Overall TE <20 ≥20
SVR
12
, % (
PP
)
SOF/VEL SOFVEL+RBV
FibroScan, kPA
463/496
228/236
48/53
47/49
211/226
64/66
102/112
59/62

Efficacy of Glecaprevir/Pibrentasvir 8 weeks therapy in TN NC: US TRIO Real World Experience.

Real-World Efficacy of SOF/VEL/VOX: TRIO data
Bacon, AASLD 2018, 706
183/186
19/19
163/165
88/89
19/20
43/ 43
Baseline Demographics
TotalN=196
Male, n (%) 144 (73)
Mean Age, year(range)
61 (26–82)
TE, n (%) 173 (88)
Cirrhosis, n (%) 82 (42)
Hypertension, n (%)
81 (41)
CKD stage 1–3, n (%)
77 (43)
Prior regimens, n (%)LDV/SOF±RBVSOF/VEL±RBVEBR/GZR±RBVOther SOFOther regimens
92/173 (53)20/173 (12)19/173 (11)17/173 (10)23/173 (13)
98 100 99 9995
0
20
40
60
80
100
Overall TN TE LDV/SOF±RBV
SOF/VEL±RBV
Prior treatment
183/186
19/19
163/165
88/89
19/20
SVR
12
, % (
PP
)
SOF/VEL/VOX for 12 weeks resulted in high real world efficacy, irrespective of genotype
and prior treatment regimen

Current therapy: New data / application

8 Weeks therapy with G/P in Compensated cirrhotic patients: Expedition-8 study
Brown et al; AASLD 2018: LB7
• 5 no SVR 12• 1 DC
• No virological failures• No Safety concerns
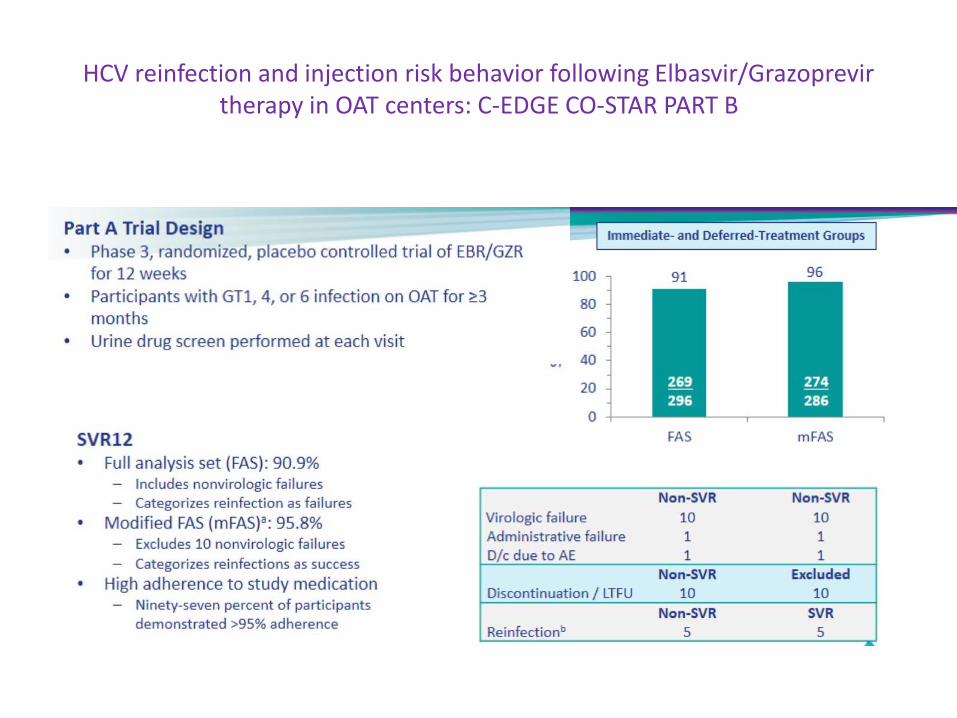
HCV reinfection and injection risk behavior following Elbasvir/Grazoprevir therapy in OAT centers: C-EDGE CO-STAR PART B
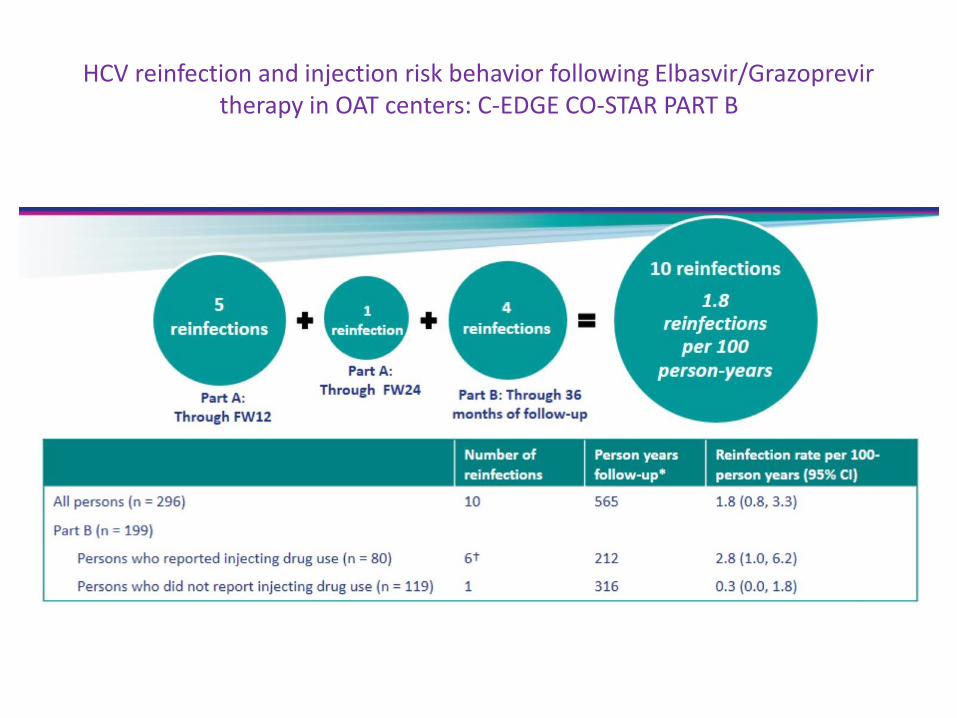
HCV reinfection and injection risk behavior following Elbasvir/Grazoprevir therapy in OAT centers: C-EDGE CO-STAR PART B
Benefits of HCV therapy beyond SVR

Durability of SVR Following Treatment with DAAs
3-year registry of patients treated in Gilead-sponsored trials who achieved SVR
Schwabe, AASLD 2018, 595
Treatment Regimens (%)99
0
20
40
60
80
100
Du
rab
ility
of
SVR
%
6577/6607
30 patients had detectable HCV RNA during their participation in the SVR registry 8 (0.1%) had virologic evidence of relapse 15 (0.2%) had virologic evidence of reinfection with phylogenetically distinct virus of same
genotype 7 (0.1%) had reinfection with different genotype
SVR is durable and late relapses (beyond SVR12) are rare
26
33
21
9
10
SOF+RBV±PegIFN
LDV/SOF±RBV
SOF/VEL±RBV
SOF/VEL/VOX
Other

Benefits of SVR
• Liver-related and All-cause mortality is lower in patients with SVR vs patients who failed therapy
• SVR associated with substantial reduction in the incidence of extrahepatic manifestations– Mood disorders (21%), CKD (53%), HTN, osteoporosis, HIV infection
– Mental health, Fatigue and substance use
• Reduced incidence rate of Type-2 DM following completion of DAA therapy
• Reduced Cardiovascular event after HCV therapy
Janjua et al; AASLD 2018: #145, Rossi et al; AASLD 2018: #148, Butt et al; AASLD 2018: #1566, Singer et al; AASLD 2018: #589

Reduction in Cardiovascular Events After HCV Treatment: ERCHIVES VA HCV Database
Butt, AASLD 2018, 1566
Treatedn=17,103
Untreatedn=17,103
Age, median 59 58
Race, %WhiteBlack
5624
5624
Male, % 96 96
Alcohol abuse/ dependence, %
37 41
Drug abuse/ dependence, %
36 40
BMI, % >30 kg/m2 35 29
FIB-4 >3.25, % 21 17
Median total cholesterol, mg/dL
165 170
Diabetes, % 8 9
Hypertension, % 51 54
SVR, % 76 -
Baseline Characteristics
Exclude If CVD at baselinen=151,593
PegIFN+RBV treated per study criteria n=4,436
Untreated, matched controlsn=4,436
DAA treated per study criteria n=12,667
Untreated, matched controlsn=12,667
n=13,536
Study Flow
CV Events: acute myocardial infarction, angina, cardiac failure, peripheral vascular disease, bypass, angioplasty,
stroke
Atherosclerotic Cardiovascular Disease
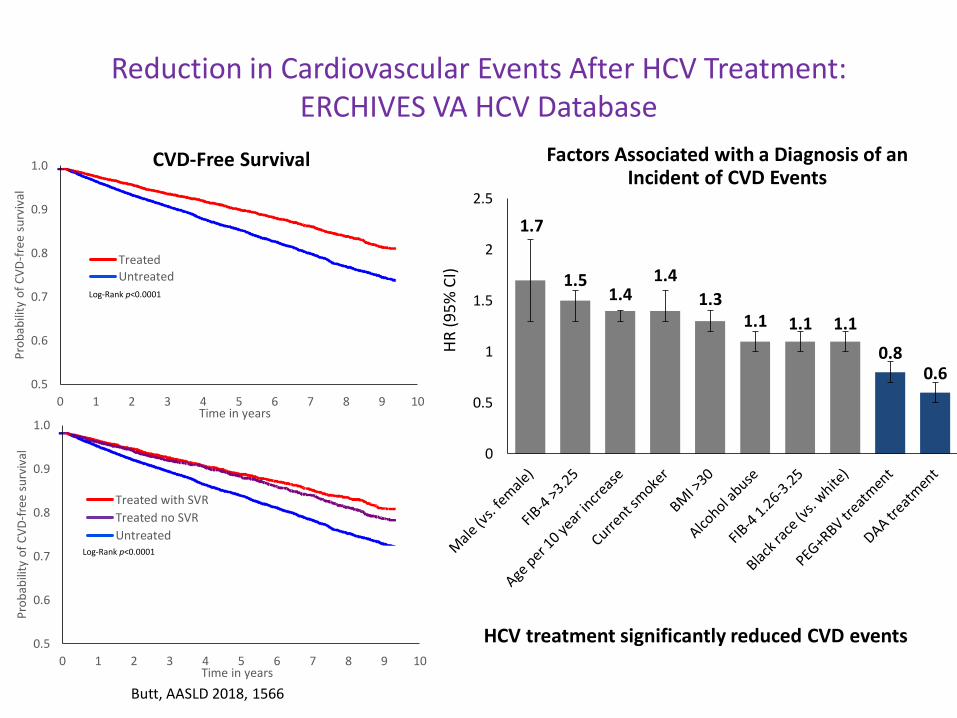
HCV treatment significantly reduced CVD events
1.7
1.51.4
1.4
1.31.1 1.1 1.1
0.80.6
0
0.5
1
1.5
2
2.5
HR
(9
5%
CI)
Factors Associated with a Diagnosis of an Incident of CVD Events
Butt, AASLD 2018, 1566
0.5
0.6
0.7
0.8
0.9
1.0
0 1 2 3 4 5 6 7 8 9 10
Pro
bab
ility
of
CV
D-f
ree
su
rviv
al
Time in years
Treated
Untreated
0.5
0.6
0.7
0.8
0.9
1.0
0 1 2 3 4 5 6 7 8 9 10
Pro
bab
ility
of
CV
D-f
ree
su
rviv
al
Time in years
Treated with SVR
Treated no SVR
Untreated
CVD-Free Survival
Log-Rank p<0.0001
Log-Rank p<0.0001
Reduction in Cardiovascular Events After HCV Treatment: ERCHIVES VA HCV Database

Summary of HCV in 2018
• DAA therapy option available for all group HCV infected individuals
• HCV treatment rate is low vs number of patients diagnosed
• Available data support that high risk population can be treated with low risk of relapse or reinfection rates
• SVR is associated with reduced rates of liver related and all-cause morbidity

Few points on Hepatitis E (HEV)
• HEV common cause of acute viral hepatitis but least diagnosed– RNA virus member of the genus
Hepevirus
• Variability in reported prevalence – By geography – high in developing
world– Also reported variability in sensitivity
and specificity of different serologic tests
– Genotype 1 – 4
• Transmission: – contaminated food and water– blood transfusions– through mother-to-child
transmission.
Purcell and Emerson J Hepatol 2008Donnelly et al,. Aliment Pharmacol Ther. 2017; 1-6.
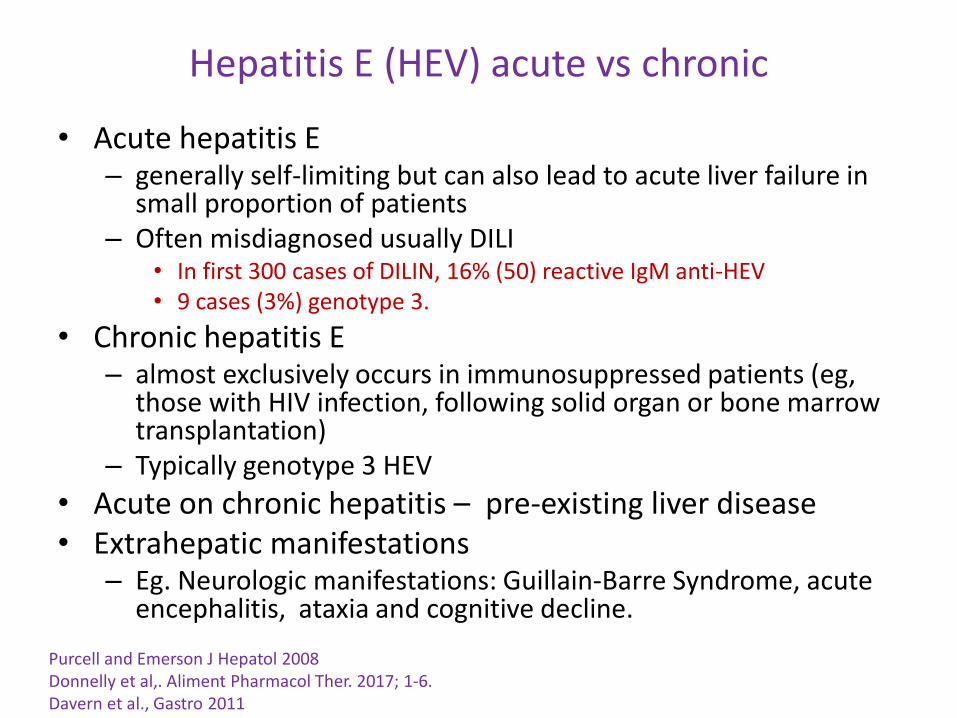
Hepatitis E (HEV) acute vs chronic
• Acute hepatitis E – generally self-limiting but can also lead to acute liver failure in
small proportion of patients– Often misdiagnosed usually DILI
• In first 300 cases of DILIN, 16% (50) reactive IgM anti-HEV• 9 cases (3%) genotype 3.
• Chronic hepatitis E– almost exclusively occurs in immunosuppressed patients (eg,
those with HIV infection, following solid organ or bone marrow transplantation)
– Typically genotype 3 HEV
• Acute on chronic hepatitis – pre-existing liver disease• Extrahepatic manifestations
– Eg. Neurologic manifestations: Guillain-Barre Syndrome, acute encephalitis, ataxia and cognitive decline.
Purcell and Emerson J Hepatol 2008Donnelly et al,. Aliment Pharmacol Ther. 2017; 1-6.Davern et al., Gastro 2011
Hepatitis E (HEV) – diagnosis and therapy
• Consider HEV infection in – Possible DILI, ACLF or seronegative acute / chronic
hepatitis– Reliable testing available
• DVH laboratory at CDC – contact Amanda Poe email: [email protected] ; phone: 404-639-0722
• If anti-HEV IgM reactive, check HEV RNA by PCR in serum or stool
• Therapy– RBV 600 – 800mg alone for 3 months– PegInterferon alfa2b– SVR 66-75%

Thank You!
Recommended

















