Abstracts 355
46% in Triglycerides, and a mean percent increase in HDL-C of 40%.
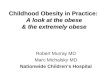
Figure 1 Correlation coefficients for the associations between1-year changes in circulating 25(OH)D and 1-year changes in vari-ables reflecting adiposity and plasma glucose-insulin homeostasis.The dashed line represents the r value threshold above which as-sociations are significant at p,0.05. ***p,0.005. TAT: total adi-pose tissue.
Figure 2 One-year changes in circulating 25(OH)D accordingto quartiles of 1-year changes in variables reflecting adiposity.
Visceral Obesity, Metabolic Syndrome andAtherosclerosis
178
Targeting Visceral Adiposity Loss as a Mean to OptimizeVitamin D Levels? Results From a Lifestyle InterventionStudy in Viscerally Obese Men*
Anne Gangloff, MD, Jessica Smith, PhD, Jean-Pierre Despres, PhD, Jean Bergeron, MD,Isabelle Lemieux, PhD, Emilie Pelletier-Beaumont, MSc,Paul Poirier, MD, Natalie Almeras, PhD, Angelo Tremblay,PhD, Anne-Laure Borel, MD, Julie-Anne Nazare, PhD,(Sainte–Foy, Qu)
Author’s Financial Disclosures: NoneStudy Funding: YesFunding Sources: This study was funded by the Cana-dian Institutes of Health Research.
Background/Synopsis: Vitamin D deficiency has beenassociated to obesity while both obesity and vitamin Ddeficiency have been linked to diabetes. The contributionsof adiposity vs. vitamin D levels to glucose-insulin homeo-stasis remain unclear.
Objective/Purpose: The objective of the study was toinvestigate the effects of a 1-year lifestyle intervention onplasma 25-hydroxyvitamin D (25(OH)D) levels and theirrelationships with adiposity indices and glucose-insulinhomeostasis markers.
Methods: Design and Setting: Intervention study (SYN-ERGIE study) performed between 2004 and 2006 withparticipants recruited from the general community. Partic-ipants: Sedentary, abdominally obese and dyslipidemic men(n5103) involved in a 1-year lifestyle modification pro-gram compared to 20 men who received standard clinicalevaluation/care (control group). Intervention: Subjects wereindividually counselled by a kinesiologist and a nutritionistonce every 2 weeks during the first 4 months with subse-quent monthly visits in order to elicit a 500 kcal dailyenergy deficit and to increase physical activity/exercisehabits. Main Outcome Measures: Cardiometabolic riskprofile and adiposity mapping by computed-tomography,to which a plasma vitamin D measurement was added.
Results: The 1-year intervention resulted in a 26%increase in plasma 25(OH)D (from 4862 nmol/L to5862 (6SEM) nmol/L, p,0.0001) whereas levels re-mained stable in the control group (from 5565 nmol/L to5065 nmol/L, p50.07). One-year increases in 25(OH)Dlevels correlated inversely with changes in all adiposityindices, especially 1-year changes in visceral (r5-0.36,p,0.005) and total abdominal (r5 0.37, p,0.0005) adi-pose tissue volumes. Association between changes in25(OH)D and the response of plasma glucose-insulin
homeostasis markers (basal glucose, basal insulin, 2h-glucose, 2h-insulin and HOMA-IR) was observed onlyfor basal glucose (r5-0.28, p,0.005). One-year vitamin Dincrease was associated with the 1-year decrease in heartrate assessed at a standardized submaximal treadmillworkload as an index of cardiorespiratory fitness(r5-0.24; p,0.05). Exception made of the one-year changein triglycerides (r5-0.26, p50.0091), one-year changes inlipid profile (total cholesterol, HDL-C, LDL-C, apo B) andinflammation markers (TNF-alpha, PAI-1, CRP) were notassociated to changes in 25(OH)D. Changes in triglycerideswere no longer associated with changes in 25(OH)D oncechanges in visceral adiposity were taken into account.
Conclusion: These results suggest that vitamin Ddeficiency is one of the many metabolic disturbances dueto excess visceral adiposity and therefore support a role ofvisceral adiposity reduction in the management of obesity-associated vitamin D insufficiency.
Recommended