
STRATEGIC CLINICAL DECISION-MAKING AFTER
ACL INJURY AND RECONSTRUCTION:
PATIENT REPORTED OUTCOME MEASURES,
RETURN TO SPORT, SECOND INJURY PREVENTION,
AND PREDICTORS OF OSTEOARTHRITIS
by
Jessica L Johnson
A dissertation submitted to the Faculty of the University of Delaware in partial fulfillment of the requirements for the degree of Doctor of Philosophy in Biomechanics and Movement Science
Spring 2020
© 2020 Jessica L Johnson All Rights Reserved
STRATEGIC CLINICAL DECISION-MAKING AFTER
ACL INJURY AND RECONSTRUCTION:
PATIENT REPORTED OUTCOME MEASURES,
RETURN TO SPORT, SECOND INJURY PREVENTION,
AND PREDICTORS OF OSTEOARTHRITIS
by
Jessica L Johnson
Approved: __________________________________________________________ Samuel C.K. Lee, Ph.D. Director of the Interdisciplinary Graduate Program in Biomechanics and
Movement Science Approved: __________________________________________________________ Kathleen S Matt, Ph.D. Dean of the College of Health Sciences Approved: __________________________________________________________ Douglas J. Doren, Ph.D. Interim Vice Provost for Graduate and Professional Education and
Dean of the Graduate College
I certify that I have read this dissertation and that in my opinion it meets the academic and professional standard required by the University as a dissertation for the degree of Doctor of Philosophy.
Signed: __________________________________________________________ Lynn Snyder-Mackler, Sc.D., FAPTA Professor in charge of dissertation I certify that I have read this dissertation and that in my opinion it meets
the academic and professional standard required by the University as a dissertation for the degree of Doctor of Philosophy.
Signed: __________________________________________________________ May Arna Risberg, Ph.D. Member of dissertation committee I certify that I have read this dissertation and that in my opinion it meets
the academic and professional standard required by the University as a dissertation for the degree of Doctor of Philosophy.
Signed: __________________________________________________________ Thomas S Buchanan, Ph.D. Member of dissertation committee I certify that I have read this dissertation and that in my opinion it meets
the academic and professional standard required by the University as a dissertation for the degree of Doctor of Philosophy.
Signed: __________________________________________________________ Elizabeth Wellsandt, Ph.D. Member of dissertation committee

I certify that I have read this dissertation and that in my opinion it meets the academic and professional standard required by the University as a dissertation for the degree of Doctor of Philosophy.
Signed: __________________________________________________________ James J Irrgang, Ph.D., FAPTA Member of dissertation committee

Trials teach us what we are; they dig up the soil and let us see what we are made of. -Charles Spurgeon You can’t do anything about the length of your life, but you can do something about
it’s width and depth. -Evan Esar
vi
To my advisor, Lynn Snyder-Mackler. From our first meeting in the
Wilmington Amtrak Station, your absolute no-nonsense, get-to-the-point attitude
convinced me that I could get this done. I would not be languishing in my sixth year of
writing with no dissertation in sight. Your commitment to my growth as a researcher
and scientist is invaluable and I will carry the lessons with me forever. Thank you.
To my committee. Thank you for your passion and excellence. Thank you for
your willingness to read, edit, and debate this work. Your combined expertise has
made me a better researcher, writer, and scientist.
To Martha Callahan and the staff at the Delaware Research Institute. Thank
you for taking care of our participants and all of your assistance with scheduling and
data management.
To the SmackLab, both past and present, I could not have managed this
without your support and guidance. To Jessica Galgiani, thank you for the listening ear
and the Trader Joe’s runs. To my fellow PhD students, which is too many to possibly
list, thank you. And lunch is still at noon.
And always, always, to my family. To my sister, Liz, your cards, letters, late
night texts, and constant cheering have made all the difference. To my brother-in-law,
Adam, your crazy questions and curiosity are always appreciated. To Mira, Malachi,
and Vivienne. I started this journey two weeks before Malachi was born and defended
three weeks after Vivienne. Your funny stories and smiling faces have been a bright
light in the rough times. And to my parents. Your unwavering faith in my abilities and
ACKNOWLEDGMENTS
vii
your constant encouragement has been my sustaining force. I could not ask for better
parents. Thank you.
This work is dedicated to all of the participants who volunteered for these
studies. This work would not be possible without all 380 of you. Thank you for your
time and willingness to participate.
This research was supported by the National Institutes of Health and the
National Institute of Arthritis and Musculoskeletal and Skin Diseases (R01-
AR048242) and the Eunice Kennedy Shriver National Institute of Child Health and
human Development (937-HD037985). Thank you to the University of Delaware for
the support of a summer Dissertation Award.
viii
LIST OF TABLES ....................................................................................................... xii LIST OF FIGURES ..................................................................................................... xiii ABSTRACT ................................................................................................................ xiv Chapter
1 INTRODUCTION, RATIONAL, AND SPECIFIC AIMS ............................... 1
1.1 Introduction ............................................................................................... 1 1.2 Overall Scientific Premise ......................................................................... 2
1.2.1 Scientific Premise for Aim 1: Can we stop asking so many questions? Selection of patient reported outcome measures. ........ 3
1.2.2 Scientific premise for Aim 2: Secondary injury prevention for female athletes. .............................................................................. 4
1.2.3 Scientific premise of Aim 3: Timing of specialized intervention and the impact on rates of return to sport, competitive level, and second ACL injuries. ................................ 6
1.2.4 Scientific premise of Aim 4: Using gait biomechanics five years after ACL injury/reconstruction to predict joint space width 10 years after injury. ........................................................... 7
1.3 Significance ............................................................................................... 8 1.4 Innovation ................................................................................................. 9 1.5 Specific Aims .......................................................................................... 10 1.6 Summary ................................................................................................. 11
2 CAN WE STOP ASKING SO MANY QUESTIONS? COMPARING THE RESPONSIVENESS OF THE GLOBAL RATING SCALE TO LEGACY KNEE OUTCOME SCORES: A DELAWARE-OSLO COHORT STUDY .. 13
2.1 Introduction ............................................................................................. 13 2.2 Methods ................................................................................................... 16
2.2.1 Participants .................................................................................. 17 2.2.2 Study design ................................................................................ 17
TABLE OF CONTENTS
ix
2.2.3 Global Rating Score .................................................................... 18 2.2.4 Knee Outcome Survey-Activities of Daily Living Scale ............ 18 2.2.5 International Knee Documentation Committee-Subjective
Knee Form ................................................................................... 18 2.2.6 Knee injury and Osteoarthritis Outcome Score .......................... 19 2.2.7 Statistics ...................................................................................... 19
2.3 Results ..................................................................................................... 20
2.3.1 Effect Sizes .................................................................................. 20 2.3.2 Ceiling Effect .............................................................................. 21 2.3.3 Validity ........................................................................................ 21 2.3.4 Minimally Important Change ...................................................... 21
2.4 Discussion ............................................................................................... 23 2.5 Strengths and Limitations ....................................................................... 26 2.6 Conclusions ............................................................................................. 28
3 SECONDARY INJURY PREVENTION PROGRAM MAY DECREASE CONTRALATERAL ACL INJURIES IN FEMALE ATHLETES: 2-YEAR INJURY RATES IN THE ACL-SPORTS RANDOMIZED CONTROL TRIAL .............................................................................................................. 31
3.1 Introduction ............................................................................................. 31 3.2 Methods ................................................................................................... 33
3.2.1 Participants .................................................................................. 34 3.2.2 Training ....................................................................................... 35 3.2.3 Age .............................................................................................. 36 3.2.4 Statistics ...................................................................................... 36
3.3 Results ..................................................................................................... 37
3.3.1 Second ACL injury ..................................................................... 38 3.3.2 Age .............................................................................................. 39
3.4 Discussion ............................................................................................... 41
3.4.1 Graft Rupture .............................................................................. 41 3.4.2 Contralateral ACL Injury ............................................................ 42 3.4.3 Return to Sport ............................................................................ 43 3.4.4 Post-surgical follow-up ............................................................... 43 3.4.5 RTS criteria ................................................................................. 44
x
3.5 Clinical Implications ............................................................................... 44 3.6 Strengths and Limitations ....................................................................... 45 3.7 Conclusions ............................................................................................. 46
4 HIGH RATES OF RETURN TO SPORT AND COMPETITIVE LEVEL WITH A SPECIALIZED INTERVENTION REGARDLESS OF TIMING OF INTERVENTION ...................................................................................... 48
4.1 Introduction ............................................................................................. 48 4.2 Methods ................................................................................................... 50
4.2.1 Participants .................................................................................. 50 4.2.2 Intervention ................................................................................. 51 4.2.3 Surveys ........................................................................................ 52
4.3 Results ..................................................................................................... 52 4.4 Discussion ............................................................................................... 55 4.5 Strengths and Limitations ....................................................................... 58 4.6 Conclusion ............................................................................................... 58
5 LOW LOADING OF THE MEDIAL TIBIOFEMORAL COMPARTMENT DURING GAIT FIVE YEARS AFTER ACL INJURY IS PREDICTIVE OF SMALLER JOINT SPACE WIDTH AT TEN YEARS ............................ 59
5.1 Introduction ............................................................................................. 59 5.2 Methods ................................................................................................... 61
5.2.1 Subjects ....................................................................................... 61 5.2.2 Modeling ..................................................................................... 61 5.2.3 Radiographs ................................................................................. 62 5.2.4 Statistics ...................................................................................... 63
5.3 Results ..................................................................................................... 63 5.4 Discussion ............................................................................................... 66 5.5 Conclusions ............................................................................................. 69
6 SUMMARY ..................................................................................................... 70
6.1 Overview of the aims .............................................................................. 70 6.2 Aim 1 Purpose ......................................................................................... 70
6.2.1 Hypothesis 1.1: ............................................................................ 70 6.2.2 Hypothesis 1.2: ............................................................................ 71 6.2.3 Conclusion ................................................................................... 71
xi
6.3 Aim 2 Purpose: ........................................................................................ 71
6.3.1 Hypothesis 2.1: ............................................................................ 71 6.3.2 Conclusion ................................................................................... 71
6.4 Aim 3 Purpose: ........................................................................................ 72
6.4.1 Hypothesis 3.1: ............................................................................ 72 6.4.2 Hypothesis 3.2: ............................................................................ 72 6.4.3 Hypothesis 3.3: ............................................................................ 72 6.4.4 Conclusion ................................................................................... 72
6.5 Aim 4 Purpose: ........................................................................................ 73
6.5.1 Hypothesis 4.1: ............................................................................ 73 6.5.2 Hypothesis 4.2: ............................................................................ 73 6.5.3 Conclusion ................................................................................... 73
6.6 Summary of Work ................................................................................... 74
REFERENCES ............................................................................................................. 75 Appendix
A IRB DOCUMENTATION ............................................................................... 93 B LIST OF ABBREVIATIONS .......................................................................... 95 C PROGNOSTIC FACTORS FOR PATIENT-REPORTED OUTCOME
MEASURES AND PHYSICAL ACTIVITY TWO TO TEN YEARS AFTER ACL INJURY OR RECONSTRUCTION: SYSTEMATIC REVIEW .......................................................................................................... 96
xii
Table 2.1: Demographics of participants at enrollment ............................................... 20
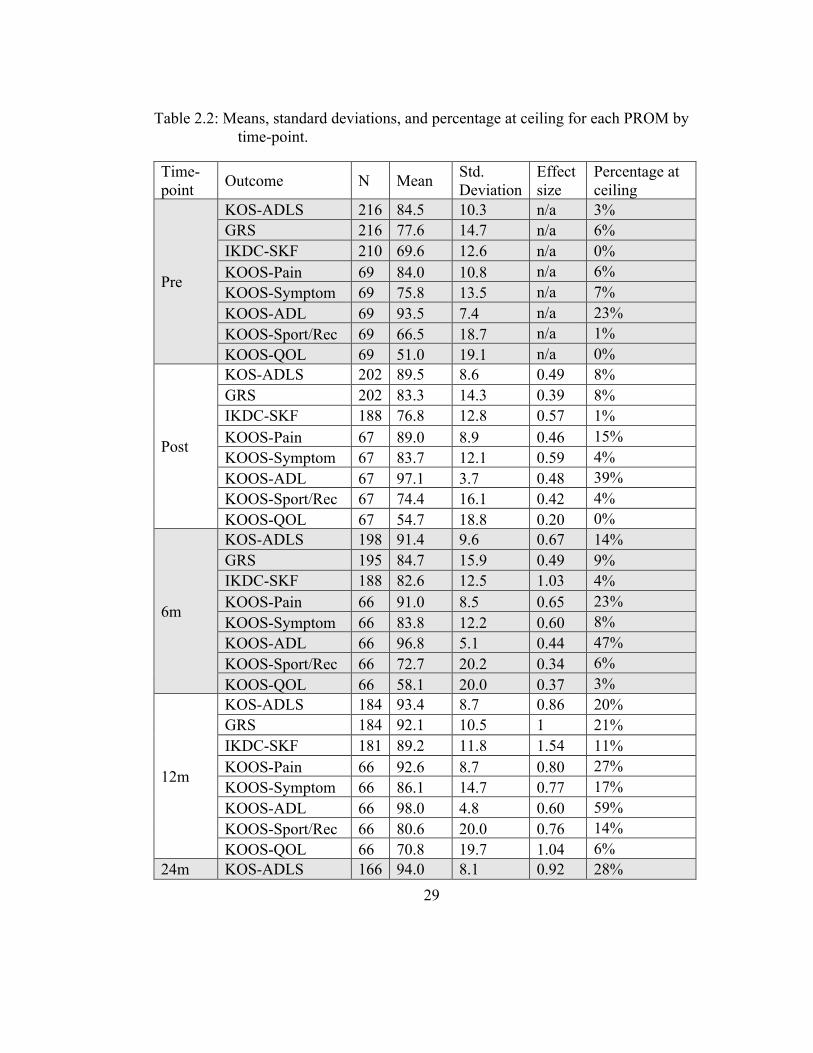
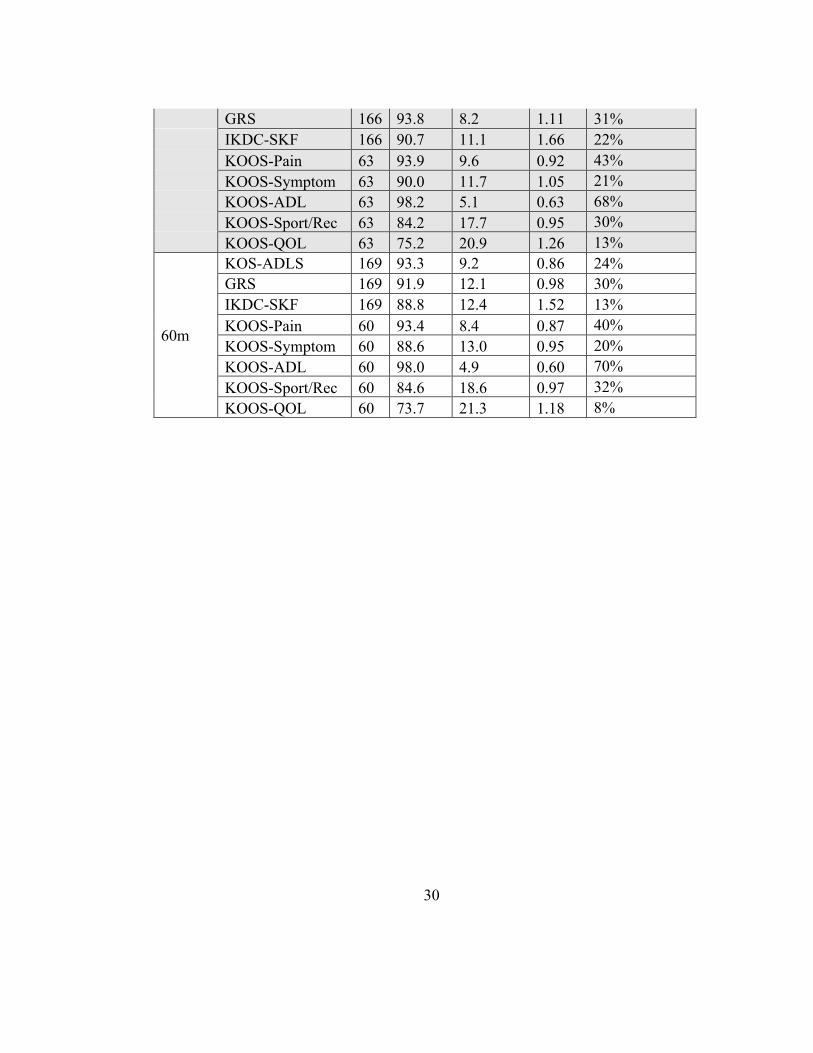
Table 2.2: Means, standard deviations, and percentage at ceiling for each PROM by time-point. ............................................................................................... 29
Table 3.1 Demographics of participants at enrollment by group. ................................ 37
Table 3.2 By group comparisons for SAPP versus SAPP+PERT ............................... 39
Table 3.3 Rates of second ACL injury by age. ............................................................ 40
Table 3.4: Comparison between rates of second injury for female athletes of the ACL-SPORTS trial matched by age to previous literature ..................... 40
Table 4.1: Demographics at enrollment ....................................................................... 53
Table 4.2: Rates of same sport and same competitive level 2 years after ACLR ........ 53
Table 4.3: Rates and side of second ACL injury two years after ACLR ..................... 55
TABLE C.1. PubMed search ..................................................................................... 130
TABLE C.2: Characteristics of included studies (n=20) ........................................... 131
TABLE C.3: Risk of bias assessment (n=20) ............................................................ 136
LIST OF TABLES
xiii
Figure 2.1 Effect sizes. ................................................................................................. 22
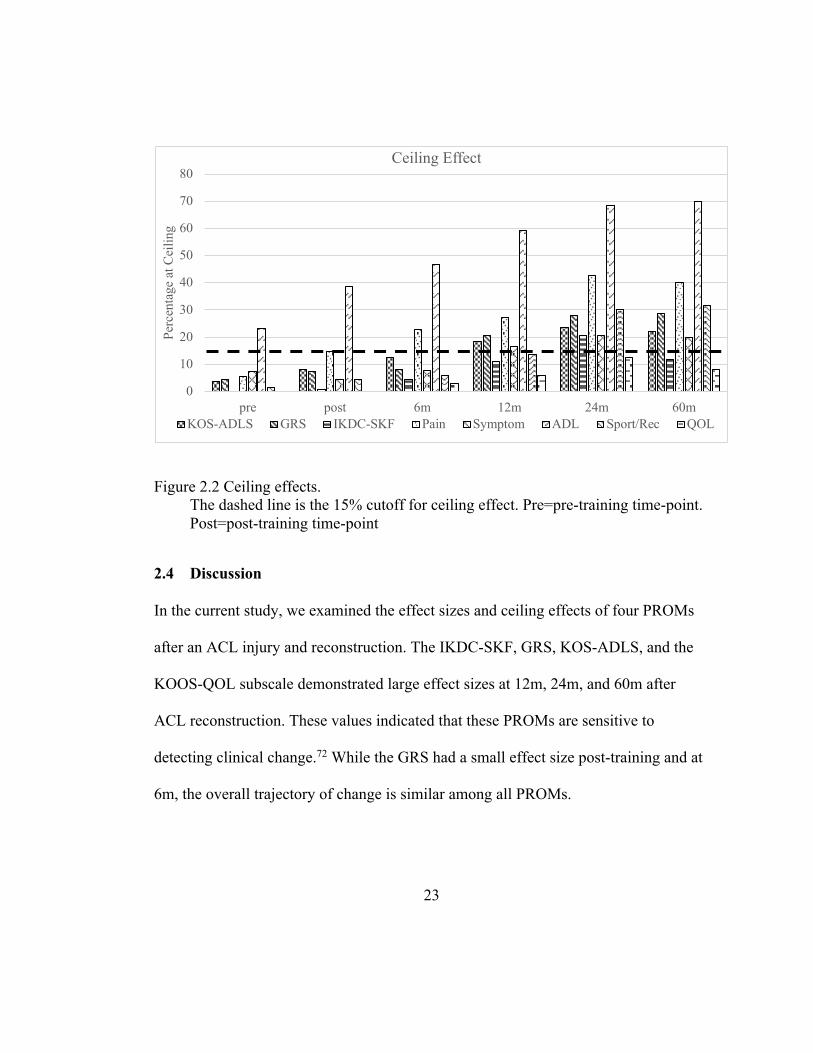
Figure 2.2 Ceiling effects. ............................................................................................ 23
Figure 3.1 Perturbation exercises performed by the SAPP+PERT group ................... 36
Figure 3.2 CONSORT flow diagram for ACL-SPORTS female athletes ................... 47
Figure 4.1: Rates of return to pre-injury sport ............................................................. 54
Figure 4.2: Rates of return to pre-injury competitive level .......................................... 54
Figure 4.3: Rates and sides of second ACL injuries .................................................... 55
Figure 5.1: Predicting medial compartment JSW at ten years with loading at ten years ........................................................................................................ 64
Figure 5.2: Predicting medial compartment JSW at ten years with loading symmetry at five years ............................................................................ 65
Figure 5.3 Predicting medial compartment JSW at ten years with loading at five year by surgical status ............................................................................. 66
Figure C.1. Flow chart ............................................................................................... 138
LIST OF FIGURES

xiv
Anterior cruciate ligament (ACL) reconstruction (ACLR) is the common treatment
recommendation after ACL injury,102 however, outcomes after surgery are not
uniformly good. Only about 55% of athletes return to previous levels of competition
after ACLR8 and among those who do return, up to 30% have a second ACL injury.58
Additionally, patients with ACL injury have higher rates of osteoarthritis,84,14 some as
early as one year after injury.32,74 ACL injury is a common sport injury2 with
increasing incidence,80,81,126 and a peak age between 15-25 years old,16,117,126,162 so
these injuries have devastating consequences to both activities of daily living and
sports participation in young active individuals.104,105,135
The long-term objective of this work is to improve clinical decision-making to
increase return to sport rate, reduce second injuries, and reduce incidence of early OA
after ACL injury. This project will measure responsiveness of four commonly used
PROMs (Aim 1), identify biomechanical risk factors for loss of medial compartment
tibiofemoral joint space width (Aim 2), evaluate the effect of a specialized
intervention on second injury rate (Aim 3), and the timing of intervention on second
injury and return to sport rates (Aim 4) to achieve this goal,. The goal of this work is
to inform clinical decision-making regarding outcome measures, timing of visits,
ABSTRACT
xv
second injury risk, and identification for progression of radiographic knee
osteoarthritis in patients after an ACL injury/reconstruction.
1
INTRODUCTION, RATIONAL, AND SPECIFIC AIMS
1.1 Introduction
The rates of primary anterior cruciate ligament (ACL) injury are on the rise,22 with the
highest incidence of ACL injury occurring between the ages of 15 and 25 years
old.117,126,162 These young athletes have very high expectations after ACL injury and
reconstruction that are not currently being met. While 91% expect to return to their
previous sports,44 a recent systematic review found only about 55% actually return to
their previous competitive levels, with younger age, male sex, and elite sport
participation all increasing the odds of returning to sport.8
Athletes who successfully return to a level I sport (jumping, hard cutting, and
pivoting)33 are approximately 15 times more likely to sustain a second injury than
matched uninjured controls,109 nearly half of the injuries occur within two months of
returning to sport.58 Again, age is important, with younger athletes at higher risk for
second ACL injuries,130,148,150 most in the first year after return to sport.150 However,
with a strong association between age and returning to cutting/pivoting sports,19,130,150
Chapter 1
2
younger age may be a proxy for returning to high risk sports and not an independent
risk.57
Long-term, 98% of patients expect no or only slightly higher risk of osteoarthritis
(OA) after their injury and ACL reconstruction (ACLR),44 but most have signs of
radiographic knee OA ten to twenty years after ACLR.84,85
Taken together, the impact of not returning to a sport, returning only to have a second
ACL injury, and the high rate of OA, suggest we are not meeting the expectations of
our patients. There are considerable and devastating effects of ACL injury on both
activities of daily living and sports participation104,105,135 we need to address.
1.2 Overall Scientific Premise
This dissertation aimed to improve clinical decision-making regarding outcome
measures, timing of visits, second injury risk, rate of return to sport, and identification
of potentially modifiable risk factors of radiographic knee OA in patients after an ACL
injury/reconstruction.
3
1.2.1 Scientific Premise for Aim 1: Can we stop asking so many questions? Selection of patient reported outcome measures.
Patient reported outcome measures (PROMs) are designed to measure the patient’s
perspective on symptoms, function, and health related quality of life.17 The selection
of PROMs is essential for obtaining meaningful information to determine a plan of
care37 and make clinical decisions,145 but even within a specific diagnosis such as
ACL injury and reconstruction, there are multiple recommended outcome
measures,68,88,92,93 and no consensus among providers.87 Surveys are often
administered concurrently,87 which may burden providers and patients leading to
mistakes and missing data.63 While the number of questions or length of time to
complete PROMs that patients will accept varies,121 longer PROMs place more strain
on respondents and administrators and may lead to errors in responding to items and
missing data,63 as well as lower response rates.121 Additionally, there may be higher
burden if multiple surveys with similar concepts are administered at the same time.121
In a survey of health care providers regarding markers of successful outcomes after
ACL injury and reconstruction, Lynch et al reported the highest scoring PROM was
the Global Rating Scale (GRS) with 45% of respondents reporting it as an important
measure; the Knee Outcome Survey-Activities of Daily Living (KOS-ADLS ),
International Knee Documentation Committee-Subjective Knee Form (IKDC-SKF),
and the Knee injury and Osteoarthritis Outcome Score (KOOS) were rated as

4
important by 41%, 38%, and 37% of healthcare providers respectively, none reaching
consensus.87
A valid measure must be able to detect a clinically-important change136 and construct
validity may be accessed with correlations to other measures of the construct.70,138
Responsiveness is an instrument’s ability to detect real changes in the construct that it
is intended to measure136 and may be measured with effect size,137 a standardized
measure of change in a group72 and the presence of a ceiling effect, the percentage of
patients with the maximum score.144 With no consensus, and the most frequently used
PROMs appropriate at different stages of recovery, having one simple measure that
can be used effectively throughout the rehabilitation timeline would improve plan of
care decision-making as well as monitor progress across the continuum of care.
We assessed the construct validity of the single-item GRS with the IKCD-SKF as well
as determined the minimal important difference for the GRS. We also assessed the
responsiveness of the four highest rated PROMs (GRS, IKDC-SKF, KOS-ADLs, and
the KOOS) in the 5 years after ACL injury and reconstruction
1.2.2 Scientific premise for Aim 2: Secondary injury prevention for female athletes.
Athletes who return to Level I sport (jumping, hard cutting, and pivoting)33 after an
ACLR are approximately 15 times more likely to sustain a second injury than matched
controls,109 most in the first year after return to sport150 and nearly half of those within
5
the first two months.58 The risks are highest for female athletes,90 with reported risk of
a second injury as high as six times that of male athletes.109 The type of second injury
is also different between sexes, with a higher contralateral injury rate in females
compared to males.109,113,149
And while the use of and enforcement of stringent RTS criteria have been shown to
reduce second injury risk,58 specialized secondary injury prevention programs are also
effective in reducing this risk, and current recommendations include quadriceps
strengthening and neuromuscular training for 9-12 months after ACLR.54,77,98 One
specific type of neuromuscular training, perturbation training, improves knee stability
through adaptations in neuromuscular control with potential destabilizing activities
about the knee.48 Perturbation training is designed to induce compensatory changes in
muscle activation patterns and facilitate dynamic joint stability.119 Perturbation
training improved self-reported knee function more than strength training alone in the
first six months after ACLR118.
Arundale et al. found a 2.5% second injury rate in the male participants of the ACL-
SPORTS randomized control trial using progressive strengthening, agilities,
plyometrics and prevention exercises; the injury rate was so low they were unable to
analyze the impact of perturbation training in these athletes.12 In this aim we assessed
how female athletes responded to this intervention and its effectiveness in reducing the
6
rate of second injuries. Specifically, this work determined the effectiveness of
reducing second ACL injuries with the addition of perturbation training to a secondary
injury prevention compared to the prevention program alone.
1.2.3 Scientific premise of Aim 3: Timing of specialized intervention and the impact on rates of return to sport, competitive level, and second ACL injuries.
Current recommendations after ACL injury include a phase of pre-operative
rehabilitation, with a systematic review finding pre-operative rehabilitation was
effective in improving post-operative outcomes in patients waiting for ACLR.4 A
clinical practice guideline update in 2016 also recommended a phase of pre-operative
rehabilitation.98 Additionally, the most effective post-operative training programs for
returning to pre-injury level of function and reducing the risk of reinjury include
quadriceps strengthening and neuromuscular training for 9-12 months.54,77,98
Limited resources and increasing healthcare costs may render extended pre-operative
and post-operative interventions difficult to implement. Currently, we do not know
how the timing of specialized interventions may impact risk factors and patient goals
if there are a limited number of visits available.
This work analyzed the impact of the timing of a specialized intervention (either pre-
operatively or in the return to sports phase of rehabilitation) on rates of return to sport,
competitive level, and rates of second ACL injury.
7
1.2.4 Scientific premise of Aim 4: Using gait biomechanics five years after ACL injury/reconstruction to predict joint space width 10 years after injury.
Athletes with ACL injuries experience high rates of radiographic OA 14,107 within a
decade of injury.96 Current best recommendations for the treatment of OA include
physical therapy, education, pain control, and surgery.106,163 These secondary and
tertiary level treatments address symptoms but are unable to reverse the damage to the
joint.106,122 With peak age of ACL injury at between 15-25 years old16,117,126,162 and
roughly 50% developing radiographic OA within twenty years of ACL
injury/reconstruction,84 identification of modifiable risk factors to intervene before the
initiation of cartilage degradation are critical.
One possible risk factor is gait biomechanics, which vary after ACL
injury.40,51,60,61,124,131,135 Even small changes in the load bearing position of the
tibiofemoral joint may be significant contributors to the development of premature
OA,39 and under-loading of the medial tibiofemoral compartment was associated with
ROA changes 5 years after ACLR.153 Since healthy cartilage responds positively to
load,5 this under-loading of normally loaded tissue may be responsible for the high
rate of radiographic knee OA in ACL injured athletes.
We assessed medial compartment tibiofemoral joint contact forces during gait 5 years
after injury/reconstruction with a previously validated EMG driven musculoskeletal
8
model20 to predict fixed location medial compartment tibiofemoral joint space width
using the International Knee Documentation Committee (IKDC) objective criteria to
classify narrowing of the tibiofemoral compartment64,97 10 years after ACL
injury/reconstruction.
1.3 Significance
While anterior cruciate ligament (ACL) reconstruction (ACLR) is the common
recommendation after ACL injury,102 outcomes after surgery are not uniformly good.
Only an average of 55% return to previous level of competition,8 up to 30% have a
second ACL injury after returning,58 and as many as 90% develop signs and symptoms
of OA after ACLR.14 Since ACL injury is a common sport injury2 with increasing
incidence,80,81,126 these injuries have devastating consequences to both activities of
daily living and sports participation.104,105,135 The long-term objective of this work is to
improve clinical decision-making to increase return to sport rate, reduce second
injuries, and reduce incidence of early OA after ACL injury. To achieve this goal, this
project measured responsiveness of four commonly used PROMs (Aim 1), evaluated
the effect of a specialized intervention on second injury rate (Aim 2) and timing of
specialized intervention on second injury and return to sport rates (Aim 3), and
identified risk factors for loss of JSW (Aim 4), and Thus, this work will inform future
work in developing interventions to reduce provider and patient burden with a valid
and responsive single-item PROMs used across time-points by any provider, identify
9
modifiable risk factors of for radiographic OA, reduce second injury rates, and
improve rates of return to sport and competitive level.
1.4 Innovation
This work is the first to assess responsiveness of PROMs through five years of ACLR
recovery. This work will decrease provider and patient burden, as well as improve
continuity of care among providers and ensure patient and provider goals are being
met. Additionally, this work is the first to assess the effect of perturbation training on
female athletes after ACLR. If effective, this intervention could reduce the rate of
second ACL injuries in female athletes. This work assessed the impact of the timing of
ten sessions of specialized training on rate of return to sports and competitive level
and rate of second ACL injuries. Lastly, we are the first to assess change in joint space
width as a marker of radiographic OA along with predictive factors of that change.
This assessment of long-term outcomes after ACL injury may inform future clinical
interventions and decision-making. These combined aims inform clinical decision
making to the best utilization of rehabilitation resources, improving outcomes and
decreasing costs associated with ACL injury.
Together, these innovations allow for the development of targeted treatments and
recommendations for prevention of second injuries, prevention of OA, and improved
sports participation.
10
1.5 Specific Aims
• Aim 1 Purpose: Determine the construct validity of the GRS and determine the
responsiveness of the GRS, the IKDC-SKF, the KOS-ADLS, and the KOOS
subscales with effect sizes and ceiling effects after ACL injury and reconstruction.
o Hypothesis 1.1: We hypothesized that the GRS would have good construct
validity when compared with the IKDC-SKF.
o Hypothesis 1.2: We hypothesized there would be no difference in
responsiveness between the GRS, the IKDC-SKF, the KOS-ADLS, and the
KOOS subscales as measured by effect size and ceiling effects.
• Aim 2 Purpose: We compared the rate and side of second ACL injuries in female
athletes who received post-operative strength, agility, plyometric and prevention
training (SAPP) compared to those who receive post-operative training plus
specialized perturbation (SAAP+PERT) training.
o Hypothesis 2.1: We hypothesized that SAPP+PERT athletes would have
fewer second ACL injuries than those who received SAPP training alone.
• Aim 3 Purpose: We analyzed the impact of timing of a specialized intervention (pre-
operatively versus return to sport phase) on rates of return to sport and competitive
level and rates of second ACL injury.
o Hypothesis 3.1 We hypothesized that those who received post-operative
training would have a higher rate of return to their pre-injury sports than
those who had pre-operative training.
11
o Hypothesis 3.2: We hypothesized that those who received post-operative
training would have a higher rate of return to their pre-injury competitive
levels of sport than those who had pre-operative training.
o Hypothesis 3.3: We hypothesized that there would be no difference in rates
of second ACL injury between those who received pre-operative training
and those who had post-operative training.
• Aim 4 Purpose: Using medial compartment joint contact forces collected during
gait at 5 years and tibiofemoral JSW from radiographs at five and ten years, we
will analyze predictive factors of joint space narrowing.
o Hypothesis 4.1: We hypothesized that under-loading in the medial
compartment of the knee during gait five years after ACL
injury/reconstruction would predict smaller JSW in the medial tibiofemoral
compartment ten years after ACL injury/reconstruction.
o Hypothesis 4.2: We hypothesized that lower loading in the medial
compartment of the knee during gait five years after ACL
injury/reconstruction would predict smaller JSW in the medial tibiofemoral
compartment ten years after ACL injury/reconstruction.
1.6 Summary Clinicians are faced with high patient expectations, low rates of return to sport, and
high rates of second injury and OA for patients after ACL injury and reconstruction.
12
This work improves clinical decision making by identifying the validity and
responsiveness of a single-item patient reported outcome measure to improve provider
communication and decrease provider and patient burden, by identifying possibly
modifiable risk factors for development of radiographic knee OA, by analyzing the
impact of specialized intervention on second ACL injury rates in female athletes, and
evaluating the impact of the timing of that intervention on rates of return to
sport/competitive level and second injury.
Taken together, these aims address the unmet high expectations of our patients and our
clinical decision-making to address common limitations and risks after ACL injury
and reconstruction.
13
CAN WE STOP ASKING SO MANY QUESTIONS? COMPARING THE RESPONSIVENESS OF THE GLOBAL RATING SCALE TO LEGACY KNEE
OUTCOME SCORES: A DELAWARE-OSLO COHORT STUDY
2.1 Introduction While originally designed for use in research, patient-reported outcome measures
(PROMs) are now also used by healthcare providers to assess the effects of clinical
care and are designed to measure the patient’s perspective on their symptoms,
function, and health-related quality of life.17 The selection of PROMs is essential for
obtaining meaningful information to manage a patient, determine a plan of care37 and
make clinical decisions,145 however, the process for selection of PROMs for clinical
care is not easy. The relevance to the patient, psychometric properties, including
reliability, validity, and responsiveness, as well as provider and patient burden are all
important factors to consider in selection of a PROM.
A 2010 systematic review by Wang et al. identified and evaluated 24 separate PROMs
for the knee and recommended different measures depending on diagnosis; while the
International Knee Documentation Committee-Subjective Knee Form (IKDC-SKF)
was the most generalizable, no measure was applicable across the spectrum of
Chapter 2
14
diagnoses or patient group.146 Even within a diagnosis such as anterior cruciate
ligament (ACL) injury and reconstruction, there are multiple recommended outcome
measures.68,88,92,93 While having multiple PROMs allows clinicians and researchers
flexibility in selecting the appropriate measure for their patient, this variation makes it
difficult to compare data across providers and studies.68
While the number of questions or length of time to complete PROMs that patients will
accept varies,121 longer PROMs place more strain on respondents and administrators
and may lead to errors in responding to items and missing data,63 as well as lower
response rates.121 Additionally, there may be higher burden if multiple surveys with
similar concepts are administered at the same time,121 as is often the case in research
studies and at initial clinical visits.
Previous work on other single-item scales has found they are valid in those with knee
injuries.129,157 The single assessment numeric evaluation (SANE) asks respondents: On
a scale from zero to 100, how would you rate your knee today (with 100 being
normal)? In comparison, the Global Rating Scale (GRS) asks respondents: Rate your
current knee function from 0% to 100%, with 100% equaling preinjury function.
The critical properties of outcome measures are patient-relevancy, user-friendliness,
reliability, validity, and responsiveness to clinical change.59 Kirshner & Guyatt
15
describe three applications of patient-reported measures; discriminative, used to
distinguish between individuals on an underlying dimension, predictive, used as a
screening or diagnostic instrument, and evaluative, used to quantitate treatment benefit
and must be able to detect a clinically meaningful difference over time.75 This work
falls into the last category, assessing the ability to detect real changes in functional
impairments and quality of life. Within the context of assessing change, a valid
measure must be able to detect a clinically-important change136 and responsiveness is
an instrument’s ability to detect real changes in the construct that it is intended to
measure.136 Construct validity may be accessed with correlations other measures of the
construct.70.138 Responsiveness may be measured with effect size,137 a standardized
measure of change in a group,72 (mean change score in baseline standard deviation
units; with pre-training as baseline)72 and the presence of a ceiling effect (percentage
of patients with the maximum score).144 A measure that has a ceiling effect is unable
to identify a further improvement in a high functioning individual.144
In a survey of health care providers regarding markers of a successful outcome after
ACL injury and reconstruction, Lynch et al. found a consensus (≥80%) that PROMs
are an important marker of success, but they did not find a consensus for the preferred
use of any individual measure.87 The highest consensus PROM was for the Global
Rating Scale (GRS) with 45% of respondents reporting it as an important measure.
The Knee Outcome Survey-Activities of Daily Living Scale (KOS-ADLS), the IKDC-
16
SKF, and the Knee injury and Osteoarthritis Outcome Score (KOOS) were rated as
important by 41%, 38%, and 37% of respondents respectively.87 This lack of
consensus among providers makes the selection of an appropriate outcome measure
increasingly difficult.
Regardless, having one simple measure that can be used effectively throughout the
rehabilitation timeline could improve plan of care decision-making as well as monitor
progress across the continuum of care. If GRS has similar effect size and ceiling effect
to longer measures, its use in isolation could decrease burden on patients and
providers.
The objective of this study was to assess the validity of the GRS compared to the
IKDC, determine the minimally important change (MIC) for the GRS, and to
determine the responsiveness of four PROMs as identified by Lynch et al87 via effect
size and the presence of a ceiling effect in a prospective cohort of ACL reconstructed
followed for 5 years. We hypothesized that the GRS would have similar effect size
and ceiling effect to the most commonly use legacy PROMs.
2.2 Methods This is a secondary analysis of an ongoing prospective observational study.36,56 The
study was approved by the ethical/human subjects committees at the Regional Ethics
17
Committee for South-Eastern Norway and the University of Delaware and all patients
provided written informed consent, or parental consent with written assent if under 18
years old at enrollment. Participants were enrolled at both centers between 2007 and
2012. The Delaware-Oslo ACL Cohort Study is supported by grant R37 HD037985
from the National Institutes of Health.
2.2.1 Participants
At enrollment, all participants had a complete unilateral ACL rupture confirmed by 3-
mm or greater difference in anterior tibial excursion with instrumented arthrometry33
(KT1000; MEDmetric Corporation, San Diego, CO) within the previous seven
months. Patients were athletes 13 to 55 years of age and regular participants in cutting
and pivoting activities for at least 50 hours per year before their injury. Exclusion
criteria included a repairable meniscus, symptomatic grade III injury to other knee
ligaments, or greater than 1-cm2 full-thickness articular cartilage lesion.
2.2.2 Study design
Following study enrollment, participants completed ten pre-operative rehabilitation
sessions. Of the 300 participants, 218 chose to have an ACLR, completed post-
operative progressive criterion-based rehabilitation early after surgery, and were
followed for five years. We collected the GRS, KOS-ADLS, IKDC-SKF, and KOOS
at pre- and post-training, and at 6, 12, 24, and 60 months after ACLR.
18
2.2.3 Global Rating Score
The GRS is a single item designed to assess current knee functional performance;
patients are asked to rate their current knee function from 0% to 100%, with 100%
equaling preinjury function.
2.2.4 Knee Outcome Survey-Activities of Daily Living Scale
The KOS-ADLS consists of 14 questions and was designed to determine symptoms
and functional limitations in usual daily activities caused by various knee
pathologies.68 The KOS contains activities such as walking, stair climbing, and
kneeling, and symptoms rated on their impact on these activities. It has questions
related to recreational or sporting activities. Scores range between 0-100%, a greater
symptoms and lower level of function resulting in a lower score.68
2.2.5 International Knee Documentation Committee-Subjective Knee Form
The IKDC-SKF has 18 items and was designed to detect improvement or deterioration
in symptoms, function, and sports activities in a variety of knee conditions.69 It is
reliable and valid for use in ligament and meniscal injuries, articular cartilage lesions,
arthritis, and patellofemoral populations.69 Scores range between 0-100%, with higher
19
scores representing lower levels of symptoms and higher levels of function and sports
activity.69
2.2.6 Knee injury and Osteoarthritis Outcome Score
The KOOS has 42 questions arranged in five subscales: Symptoms, Pain, Activities of
Daily Living (KOOS-ADL), Sport and Recreation function (Sport/Rec), and knee-
related Quality of Life (KOOS-QOL) with scores ranging between 0-100%, with
100% equaling no difficulties.123
2.2.7 Statistics
We used Excel (Microsoft, Seattle WA) to calculate effect sizes as: (mean score at
time-point minus the mean score at baseline, divided by baseline standard deviation;
pre-training as baseline)72 and the presence of a ceiling effect as a percentage of
patients with the maximum score. Effect size and ceiling effects cut-offs were set a
priori: 0.5 for medium effect size and 0.8 for large effect size,30 and ≥15% of
participants having a maximum score for the presence of a ceiling effect.95 We
correlated with GRS with the IKDC-SKF with a Pearson correlation. We calculated
the MDC for the GRS, IKDC-SKF, KOS-ADLS, and KOOS subscales as the values
associated with 20%125 and 33%160 of the standard deviation of the measure at
baseline. Power for the clinical trial was calculated a priori.
20
2.3 Results Of the 300 total participants, 218 (100 women) completed training and chose to have
an ACLR (106 hamstring grafts, 42 patellar tendon grafts, and 62 allografts);
demographics at enrollment are in Table 2.1. Results shown are for all available data
(Table 2.2); there was no change when the analysis used only those participants with a
complete data set (n=114). We did not begin collecting KOOS responses from study
participants until midway through enrollment, thus the analysis of the KOOS
subscales included only the 69 participants with baseline KOOS scores.
Table 2.1: Demographics of participants at enrollment
Mean (range) Age (years) 25.0 (13-52) Height (cm) 174.5 (148-195) Weight (kg) 75.7 (43.3-139) Body Mass Index (BMI) (kg/m2) 24.7 (18.6-40.2) Time from injury to enrollment (weeks)
8.3 (1-38)
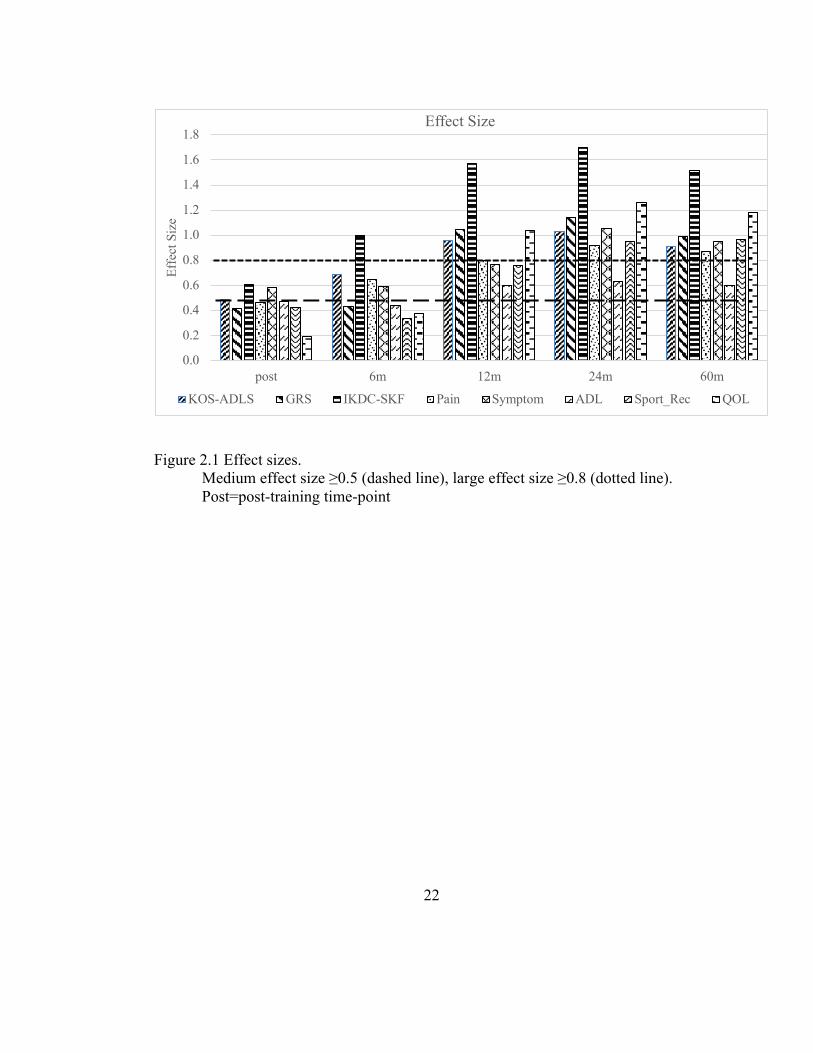
2.3.1 Effect Sizes
Effect sizes for all PROMs peaked at the 24-month time-point, with minimal
differences observed between 12m, 24m, and 60m (Figure 2.1, Table 2.2). The IKDC-
SKF had the largest effect sizes at all time-points (Figure 2.1). The GRS had a similar
effect size and change in effect size compared to the longer PROMs.
21
2.3.2 Ceiling Effect
The KOOS-QOL subscale did not demonstrate a ceiling effect at any time-point and
the IKDC-SKF only showed a ceiling effect at the 24m time-point (Figure 2.2, Table
2.2). All other measures had a ceiling effect at at least one time-point (most at 12m,
24m, and 60m) while the KOOS-ADL subscale had a ceiling effect at all time-points,
and the KOOS-Pain subscale had ceiling effects at all but pre-training. The GRS had a
similar effect size and change in ceiling effect compared to the longer PROMs.
2.3.3 Validity
The Pearson correlation coefficient between the GRS and the IKDC-SKF was 0.72
(p<0.001) when data were pooled across all time-points.
2.3.4 Minimally Important Change
The MDC for the GRS was 2.9 when using an 20%125 and 4.9 at 30%160 of the
standard deviation of the scores, which correspond to a small and small to medium
effect. The MDC for the IKDC-SKF was 2.5 and 4.1 respectively.
22
Figure 2.1 Effect sizes. Medium effect size ≥0.5 (dashed line), large effect size ≥0.8 (dotted line). Post=post-training time-point
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1.6
1.8
post 6m 12m 24m 60m
Effe
ct S
ize
Effect Size
KOS-ADLS GRS IKDC-SKF Pain Symptom ADL Sport_Rec QOL
23
Figure 2.2 Ceiling effects. The dashed line is the 15% cutoff for ceiling effect. Pre=pre-training time-point. Post=post-training time-point
2.4 Discussion In the current study, we examined the effect sizes and ceiling effects of four PROMs
after an ACL injury and reconstruction. The IKDC-SKF, GRS, KOS-ADLS, and the
KOOS-QOL subscale demonstrated large effect sizes at 12m, 24m, and 60m after
ACL reconstruction. These values indicated that these PROMs are sensitive to
detecting clinical change.72 While the GRS had a small effect size post-training and at
6m, the overall trajectory of change is similar among all PROMs.
0
10
20
30
40
50
60
70
80
pre post 6m 12m 24m 60m
Perc
enta
ge a
t Cei
ling
Ceiling Effect
KOS-ADLS GRS IKDC-SKF Pain Symptom ADL Sport/Rec QOL

24
Gangel et al. correlated the SANE with the Lysholm knee score in 130 college-age
patients after ACL reconstruction and found a good correlation (0.75, p<0.001).157
Shelbourne et al. correlated the same SANE to the IKDC-SKF after ACL
reconstruction and found an ICC of 0.66 and that the precision of agreement
(calculated as the mean difference ±1 standard deviation), was met for 81% of
respondents and limits of agreement (calculated as the mean difference ±2 SD) met for
94%.129 In this study, the correlation between GRS and IKDC-SKF was 0.72 (0.69-
0.75), p<0.001, which is a moderately strong relationship that provides some evidence
of construct validity for the GRS in this population.
As may be expected, the large effect sizes at the later time-points correspond to the
time-points with ceiling effects. All measures except the KOOS QOL had a ceiling
effect at at least one time-point (most at 12m, 24m, and 60m) while the KOOS-ADL
subscale had a ceiling effect at all time-points, and the KOOS-Pain subscale had
ceiling effects at all but pre-training. The GRS had a similar size and change in ceiling
effect compared to the longer PROMs. However, it is worth debating if the GRS can
truly have a ceiling effect. The GRS asks a respondent to rate their current knee
functional performance compared to pre-injury performance, so a score of 100%
indicates the full resolution of any impairments or limitations relevant to that
respondent. This may mean that, regardless of the percentage of respondents with a
score of 100%, the GRS does not have a ceiling effect, but a performance asymptote,
25
or the greatest true value that can be demonstrated147. In a measure with a ceiling
effect, a true score can only be observed if it is less than or equal to the ceiling
threshold. So a patient may score 100% on the IKDC-SKF or the KOOS but still have
functional limitations because not every activity or symptoms is covered on those
PROM. In contrast, we would not expect there to be a score above the 100% scored on
the GRS, this is an asymptote and not a ceiling, which differentiates it from the other
measures.
Clinical decision making requires that health care providers choose the best tool for
patient evaluation121 and previous authors have suggested a combination of PROMs
may be necessary to assess functional success.37,87 In practice, a clinician could
administer the GRS frequently, with the IKDC-SKF (or other measure as desired)
given at the initial visit, then at 3 month (initiation of running116/return to
participation)6 6 months (return to sport activities)6, 9 months (return to sport58/return
to performance)6, and at 12 and 24 months after ACLR. Based on our estimation of the
MDC of 2.8/4.9, if a participant reports GRS scores of 60, 65, 65, and 70, a therapist
should continue to progress treatment as indicated by stage of healing and objective
criteria. If, however, a patient reports weekly scores of 60, 65, 65, and then 40, it
would be appropriate to administer other tests/measures to identify causes for an
unexpected change in status. While single-item measures are reliable and valid,129,157
their simplicity comes at the cost of detail.132 To gain this detail, clinicians could use
26
outcome measures related to ADLs and functional limitations (KOS-ADLS68 or
IKDC-SKF69), fear (Tampa Scale of Kinesiophobia159 or the ACL-Return to Sports
after Injury151) or activity participation (Tegner143 or Marx94) as appropriate for the
stage of recovery and goals of rehabilitation. Additionally, no PROM alone is
sufficient to base all clinical decisions upon. Quadriceps strength, performance
measures, and biological healing are all important factors to consider after an ACL
injury.6,37,45,58
Additionally, when a patient is nearing return to sport/performance, current
recommendations suggest both objective and subjective criteria for clearance to
return.45,58 At the 12m time-point, the GRS had a large effect size, indicating it is
responsive to a clinically meaningful change from baseline to the time of return-to-
sport decision-making. Achieving a GRS of 9058 may indicate that the patient is ready
for objective criteria testing.45,58 As previously discussed, no one PROM is applicable
to all patients at all time-points.146 Clinicians can use the GRS for repeated, frequent
assessment of change and reserve longer, more burdensome PROM for significant
milestones during recovery.
2.5 Strengths and Limitations The study population was active athletes after ACL injury and subsequent ACLR.
These patients were not enrolled immediately after their ACL injury, but at a “quiet
27
knee” stage of recovery (8.3±5 weeks, range 1-38 weeks after injury). We, therefore,
do not have data from the patient’s initial encounter with a health professional, nor do
we have immediate post-operative data and so are unable to assess effect sizes with an
early post-operative baseline. Additionally, previous research comparing this cohort to
a comparable subgroup of the MOON cohort found our participants had statistically
and clinically significantly higher baseline and two-year IKDC-SKF and KOOS
scores42.
We assessed validity, responsiveness, and determined the MDC of the GRS in this
study. Future research should establish test-retest reliability, standard error of the
measurement. Also, while none of our measures are ACL specific, we only analyzed
patients with ACL rupture and subsequent ACLR. We do not know the validity,
responsiveness or MDC in patients with other knee injuries/surgeries.
Also, because we did not begin using the KOOS until midway through enrollment,
analysis of the KOOS was only done in the 69 participants who had baseline KOOS
scores.
We were unable to directly assess response burden in our participants. The difference
in the length and thus the time needed to complete each PROMs is however much
shorter in the GRS than the other three measures. The simplicity of administering the
28
GRS may decrease burden on respondents and administrators while still providing
responsive and valid information regarding patient status.
2.6 Conclusions
The IKDC-SKF has the largest effects sizes while the KOOS-QOL had the
smallest ceiling effects. The GRS, however, responds similarly to the IKDC-SKF,
KOS-ADLS, and KOOS measures and is responsive to patient change, with evidence
of construct validity and a small MDC. The ease of use and patient-specific nature of
the question means that, for clinical practice, it may be appropriate to use the GRS as a
frequent measure throughout the course of rehabilitation, with different measures used
at the beginning of treatment and other measures used at the later stages, or specific
scales based on patient’s deficits or goals.
29
Table 2.2: Means, standard deviations, and percentage at ceiling for each PROM by time-point.
Time- point Outcome N Mean Std.
Deviation Effect size
Percentage at ceiling
Pre
KOS-ADLS 216 84.5 10.3 n/a 3% GRS 216 77.6 14.7 n/a 6% IKDC-SKF 210 69.6 12.6 n/a 0% KOOS-Pain 69 84.0 10.8 n/a 6% KOOS-Symptom 69 75.8 13.5 n/a 7% KOOS-ADL 69 93.5 7.4 n/a 23% KOOS-Sport/Rec 69 66.5 18.7 n/a 1% KOOS-QOL 69 51.0 19.1 n/a 0%
Post
KOS-ADLS 202 89.5 8.6 0.49 8% GRS 202 83.3 14.3 0.39 8% IKDC-SKF 188 76.8 12.8 0.57 1% KOOS-Pain 67 89.0 8.9 0.46 15% KOOS-Symptom 67 83.7 12.1 0.59 4% KOOS-ADL 67 97.1 3.7 0.48 39% KOOS-Sport/Rec 67 74.4 16.1 0.42 4% KOOS-QOL 67 54.7 18.8 0.20 0%
6m
KOS-ADLS 198 91.4 9.6 0.67 14% GRS 195 84.7 15.9 0.49 9% IKDC-SKF 188 82.6 12.5 1.03 4% KOOS-Pain 66 91.0 8.5 0.65 23% KOOS-Symptom 66 83.8 12.2 0.60 8% KOOS-ADL 66 96.8 5.1 0.44 47% KOOS-Sport/Rec 66 72.7 20.2 0.34 6% KOOS-QOL 66 58.1 20.0 0.37 3%
12m
KOS-ADLS 184 93.4 8.7 0.86 20% GRS 184 92.1 10.5 1 21% IKDC-SKF 181 89.2 11.8 1.54 11% KOOS-Pain 66 92.6 8.7 0.80 27% KOOS-Symptom 66 86.1 14.7 0.77 17% KOOS-ADL 66 98.0 4.8 0.60 59% KOOS-Sport/Rec 66 80.6 20.0 0.76 14% KOOS-QOL 66 70.8 19.7 1.04 6%
24m KOS-ADLS 166 94.0 8.1 0.92 28%
30
GRS 166 93.8 8.2 1.11 31% IKDC-SKF 166 90.7 11.1 1.66 22% KOOS-Pain 63 93.9 9.6 0.92 43% KOOS-Symptom 63 90.0 11.7 1.05 21% KOOS-ADL 63 98.2 5.1 0.63 68% KOOS-Sport/Rec 63 84.2 17.7 0.95 30% KOOS-QOL 63 75.2 20.9 1.26 13%
60m
KOS-ADLS 169 93.3 9.2 0.86 24% GRS 169 91.9 12.1 0.98 30% IKDC-SKF 169 88.8 12.4 1.52 13% KOOS-Pain 60 93.4 8.4 0.87 40% KOOS-Symptom 60 88.6 13.0 0.95 20% KOOS-ADL 60 98.0 4.9 0.60 70% KOOS-Sport/Rec 60 84.6 18.6 0.97 32% KOOS-QOL 60 73.7 21.3 1.18 8%
31
SECONDARY INJURY PREVENTION PROGRAM MAY DECREASE CONTRALATERAL ACL INJURIES IN FEMALE ATHLETES: 2-YEAR
INJURY RATES IN THE ACL-SPORTS RANDOMIZED CONTROL TRIAL
3.1 Introduction The incidence of primary ACL reconstruction (ACLR) is on the rise, with a 77%
increase for women and 19% increase for men over a twelve year period.22 Female
athletes have a higher incidence of ACL injuries in the comparable sports of
basketball, soccer, and lacrosse2 compared to male athletes. Athletes who return to
cutting and pivoting sports after ACLR have increased odds of graft rupture and
contralateral injury compared to those who return to less strenuous sports.150 Up to one
in three athletes who return to sport may sustain a second ACL injury, nearly half of
those within two months of returning to sport58. Female athletes have a higher
contralateral injury rate compared to males109,113,149, with the reported risk of a
contralateral ACL injury as high as six times more likely compared to male athletes
(26% versus 5% respectively)109.
While younger athletes are more likely to return to their pre-injury levels of
sport8,71,150, athletes under 20 years-old have six times increased odds for a graft
Chapter 3
32
rupture and three times increased odds for a contralateral tear compared to older
athletes.150 A systematic review of athletes aged 6-19 years undergoing ACLR found
an overall second ACL injury rate of 27%71. Young female athletes have an even
higher rate of second ACL injury130, up to 32%149.
When an important marker of success (return to their previous level of sport) is also a
key risk factor for second ACL injury, clearly there is a need for targeted secondary
ACL injury prevention and return to sport (RTS) training. Current clinical practice
guidelines for primary prevention of knee and ACL injuries10 recommend preventative
training programs include a combination of neuromuscular training, strengthening,
balance, and proximal control exercises141. The most effective post-operative training
programs for returning to pre-injury level of function and reducing the risk of reinjury
include quadriceps strengthening and neuromuscular training for 9-12 months54,77,98.
Neuromuscular training techniques, such as perturbation training, designed to induce
compensatory changes in muscle activation patterns and facilitate dynamic joint
stability119, improve self-reported knee function more than strength training alone in
the first six months after ACLR118. Perturbation training improves knee stability
through adaptations in neuromuscular control with potential destabilizing activities
about the knee48. It is unclear how female athletes respond to post-operative
perturbation training.
33
The Anterior Cruciate Ligament-Specialized Post-Operative Return to Sports (ACL-
SPORTS) training program is a sport-specific secondary ACL injury prevention
program.155 ACL-SPORTS included progressive strengthening, agility, plyometric,
and prevention (SAPP) exercises. The program is effective for preventing secondary
ACL injury in men, with only one graft rupture in 40 male athletes12. However, the
second ACL injury prevention effects in women have yet to be explored.
The purpose of this study was to determine if adding perturbation training to a second
injury prevention program was more effective than the prevention program alone in
reducing second ACL injury rates in female athletes after ACLR. We hypothesized
that female athletes who received perturbation training in addition to the second injury
prevention program would have fewer graft ruptures and fewer contralateral ACL
injuries compared to those who received the prevention program alone.
3.2 Methods White et al155 previously published the methods of the ACL-SPORTS single-blinded
randomized controlled trial which was approved by the University of Delaware
Institutional Review Board and registered at clinicaltrials.gov (NCT01773317), with
funding provided by the National Institute of Child Health and Human Development
(NICHD) AR048212. This analysis is part of the a priori secondary outcomes for this
trial. Prior to enrollment, all athletes gave written consent (assent if under 18 years
34
with parent/guardian consent). The CONSORT diagram is in Figure 3.2. This analysis
achieves objective (a) in patient/athlete/public partner involvement in the research:
addressing outcomes deemed important by patients.
3.2.1 Participants
Participants were recruited from the local community through physician and physical
therapist referral, newspaper and flyer advertisements, and word of mouth, with 40
female athletes enrolled from December 2011 through January 2017 from 17
surgeons. Selection criteria were: age 13-55 years, participated in and planning to
return to a cutting/pivoting/jumping sport more than 50 hours per year, no previous
ACL injury, and no history of other major lower extremity injury/surgery. Participants
must have had a unilateral ACLR with no grade III concomitant ligament injuries or
cartilage defects larger than 1cm2.
Surgical technique, graft choice, and rehabilitation prior to enrollment were not
controlled. At enrollment, participants were screened by a physical therapist, and had
no knee pain, minimal to no knee effusion, and full knee range of motion. They were
less than nine months after ACLR, had ≥80% quadriceps index (QI), initiated a
running progression, and not yet returned to Level I/II sport. Athletes were
randomized to SAPP or SAPP plus perturbation (SAPP+PERT) using a random
35
number generator by a research coordinator (MC). All researchers performing data
collection were blinded.
All participants completed training. However, the researchers received information
that one athlete (SAPP+PERT group) may not have had an intact ACL graft at
enrollment. Therefore, we excluded her data from all analyses. All participants were
required to pass objective return to sport criteria58,154. Participants returned to the
clinic at 1- and 2-years after surgery for functional and clinical testing and patient
reported outcomes. Those who were unable to return in person at two years (n=3)
were contacted by phone. Self-reported second ACL injury status was collected for all
39 participants, as well as time from surgery to RTS, time from surgery to second
ACL injury, and time from RTS to second ACL injury. Additionally, 100% of
participants returned to sport by two years, 87% at their pre-injury level of sport.24
3.2.2 Training
Training occurred twice a week for five weeks under the supervision of a physical
therapist at the University of Delaware Physical Therapy Clinic. Perturbation exercises
used a platform/roller board combination, unilateral stance on a roller board, and
unilateral stance on a tilt board, each with therapist perturbations in multiple planes
(Figure 3.1); a full list and description of all training exercises can be found in White
et al155. Training also included education and cuing for correct technique of all

36
exercises especially avoiding valgus collapse during landings; progression was
determined according to soreness and effusion guidelines1,43,155. All participants were
required to pass the following RTS criteria before beginning return to sport: ≥90% QI
and four single legged hop limb symmetry index (LSI), ≥90% scores on the Knee
Outcomes Survey-Activities of Daily Living Subscale (KOS-ADLS) and a single item
global gating of perceived knee function (GRS), and obtain surgeon approval.
Figure 3.1 Perturbation exercises performed by the SAPP+PERT group A: Platform and roller board, B: Unilateral roller board, C: Unilateral tilt board
3.2.3 Age
Since younger age at primary ACL injury increases the risk of a second
injury71,130,149,150, we divided our athletes as those under 25, those under 20, and those
under 18.
3.2.4 Statistics
We compared rate and side of second ACL injury between the two groups using chi-
square tests of proportions and time from primary surgery to second ACL injury using
37
independent t-tests (alpha = 0.05) with SPSS (IBM Corp, Armonk NY). To compare
to previously published literature, we categorized the rate and side of second ACL
injury by age, independent of group assignment and calculated chi-squared tests of
proportions for each age category. Power was calculated a priori for the primary
outcomes of the trial (biomechanical and clinical and functional outcomes), and the
study was adequately powered155.
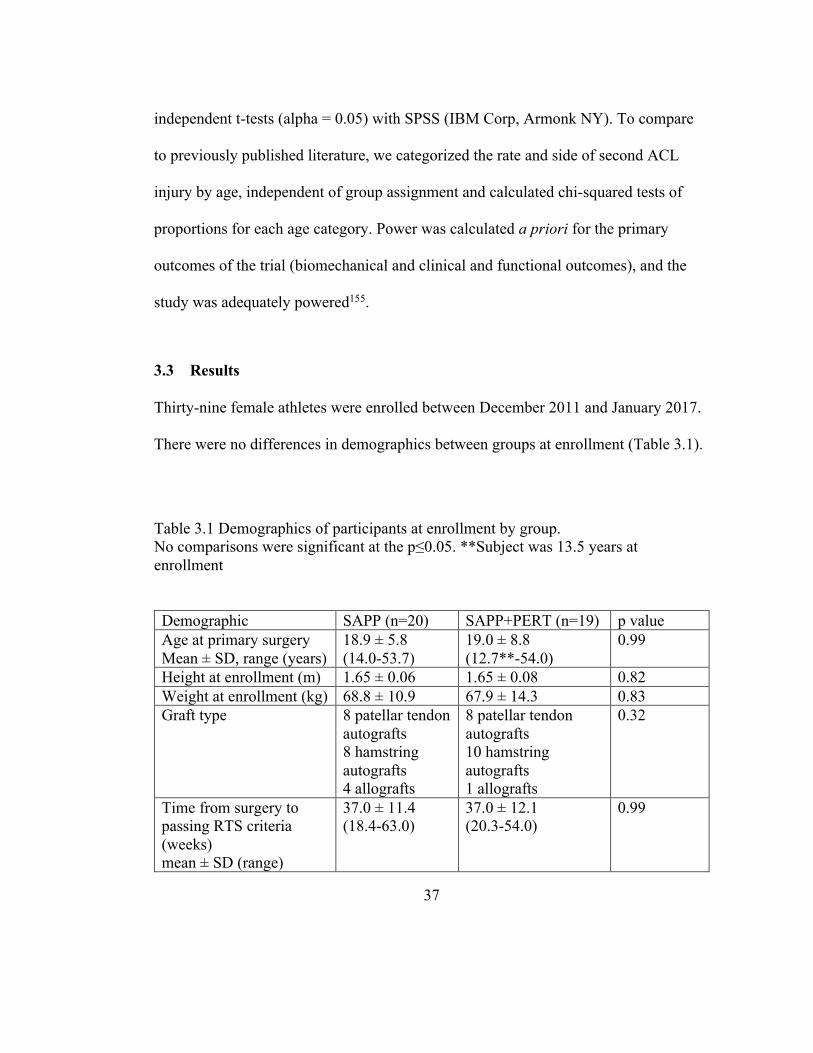
3.3 Results Thirty-nine female athletes were enrolled between December 2011 and January 2017.
There were no differences in demographics between groups at enrollment (Table 3.1).
Table 3.1 Demographics of participants at enrollment by group. No comparisons were significant at the p≤0.05. **Subject was 13.5 years at enrollment
Demographic SAPP (n=20) SAPP+PERT (n=19) p value Age at primary surgery Mean ± SD, range (years)
18.9 ± 5.8 (14.0-53.7)
19.0 ± 8.8 (12.7**-54.0)
0.99
Height at enrollment (m) 1.65 ± 0.06 1.65 ± 0.08 0.82 Weight at enrollment (kg) 68.8 ± 10.9 67.9 ± 14.3 0.83 Graft type 8 patellar tendon
autografts 8 hamstring autografts 4 allografts
8 patellar tendon autografts 10 hamstring autografts 1 allografts
0.32
Time from surgery to passing RTS criteria (weeks) mean ± SD (range)
37.0 ± 11.4 (18.4-63.0)
37.0 ± 12.1 (20.3-54.0)
0.99
38
3.3.1 Second ACL injury
There were 9 second ACL injuries within two years of ACLR in the women of the
ACL-SPORTS trial: 4 graft ruptures and 5 contralateral injuries, for an overall second
ACL injury rate of 23% (Table 3.2). All second ACL injuries occurred in athletes with
a hamstring autograft. There were no group differences in rate (p=0.77) or side
(p=0.25) of second ACL injury, thus the groups were collapsed for additional
comparisons. Post-hoc analysis revealed an effect size of w=0.047 for power of (1-
β)=0.059.
39
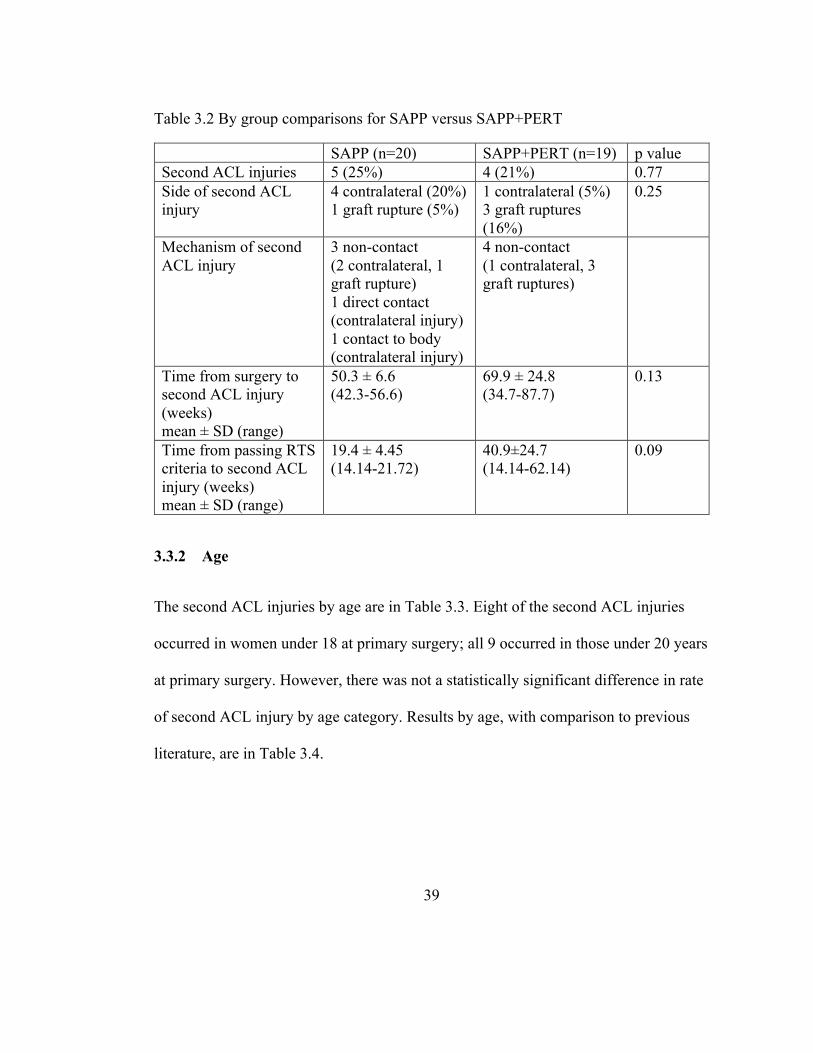
Table 3.2 By group comparisons for SAPP versus SAPP+PERT
SAPP (n=20) SAPP+PERT (n=19) p value Second ACL injuries 5 (25%) 4 (21%) 0.77 Side of second ACL injury
4 contralateral (20%) 1 graft rupture (5%)
1 contralateral (5%) 3 graft ruptures (16%)
0.25
Mechanism of second ACL injury
3 non-contact (2 contralateral, 1 graft rupture) 1 direct contact (contralateral injury) 1 contact to body (contralateral injury)
4 non-contact (1 contralateral, 3 graft ruptures)
Time from surgery to second ACL injury (weeks) mean ± SD (range)
50.3 ± 6.6 (42.3-56.6)
69.9 ± 24.8 (34.7-87.7)
0.13
Time from passing RTS criteria to second ACL injury (weeks) mean ± SD (range)
19.4 ± 4.45 (14.14-21.72)
40.9±24.7 (14.14-62.14)
0.09
3.3.2 Age
The second ACL injuries by age are in Table 3.3. Eight of the second ACL injuries
occurred in women under 18 at primary surgery; all 9 occurred in those under 20 years
at primary surgery. However, there was not a statistically significant difference in rate
of second ACL injury by age category. Results by age, with comparison to previous
literature, are in Table 3.4.
40
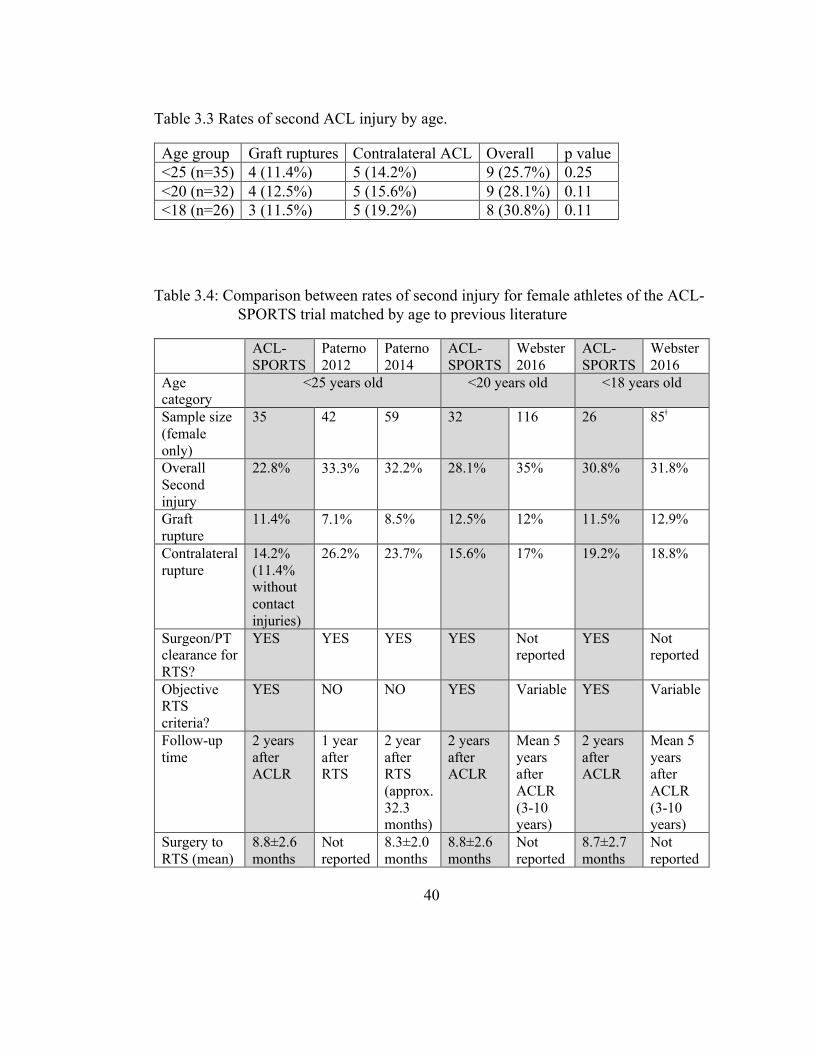
Table 3.3 Rates of second ACL injury by age.
Age group Graft ruptures Contralateral ACL Overall p value <25 (n=35) 4 (11.4%) 5 (14.2%) 9 (25.7%) 0.25 <20 (n=32) 4 (12.5%) 5 (15.6%) 9 (28.1%) 0.11 <18 (n=26) 3 (11.5%) 5 (19.2%) 8 (30.8%) 0.11
Table 3.4: Comparison between rates of second injury for female athletes of the ACL-SPORTS trial matched by age to previous literature
ACL-SPORTS
Paterno 2012
Paterno 2014
ACL-SPORTS
Webster 2016
ACL-SPORTS
Webster 2016
Age category
<25 years old <20 years old <18 years old
Sample size (female only)
35 42 59 32 116 26 85ǂ
Overall Second injury
22.8% 33.3% 32.2% 28.1% 35% 30.8% 31.8%
Graft rupture
11.4% 7.1% 8.5% 12.5% 12% 11.5% 12.9%
Contralateral rupture
14.2% (11.4% without contact injuries)
26.2% 23.7% 15.6% 17% 19.2% 18.8%
Surgeon/PT clearance for RTS?
YES YES YES YES Not reported
YES Not reported
Objective RTS criteria?
YES NO NO YES Variable YES Variable
Follow-up time
2 years after ACLR
1 year after RTS
2 year after RTS (approx. 32.3 months)
2 years after ACLR
Mean 5 years after ACLR (3-10 years)
2 years after ACLR
Mean 5 years after ACLR (3-10 years)
Surgery to RTS (mean)
8.8±2.6 months
Not reported
8.3±2.0 months
8.8±2.6 months
Not reported
8.7±2.7 months
Not reported
41
3.4 Discussion The purpose of this secondary outcomes analysis was to determine if adding
perturbation training to a second injury prevention program was more effective than
the prevention program alone in reducing second ACL injury rates in female athletes
after ACLR. There was not a statistically significant difference in rate or side of
second ACL injury between those who received SAPP+PERT and those who received
SAPP alone, so we collapsed the groups to determine any differences in outcomes
with our injury prevention program compared to the existing literature.
3.4.1 Graft Rupture
The graft rupture rate in our study is comparable, or slightly higher than previous
research (see Table 3.4 for comparisons). There are many risk factors for graft rupture,
including younger age at primary injury71,130,149,150, return to a
cutting/pivoting/jumping sport142,150, and graft type89,103,114. Almost half the athletes in
our study had a hamstring autograft, and all graft ruptures occurred in those with a
hamstring graft; Paterno et al did not report graft types109,113. Hamstring grafts have
slightly higher rates of failure than bone-patellar tendon-bone (BPTB) grafts114,115,128.
Athletes who had ACLR with hamstring autografts achieved impairment resolution
earlier and returned to sports on average 4 months earlier than those with BPTB
autografts. Therefore, biological healing may have played a role in the graft failure133.
42
Because age, time to return to sport, and rate of return to cutting/pivoting sports were
comparable, possible differences in graft selection may account for the differences
between our athletes and those reported by Paterno et al.
3.4.2 Contralateral ACL Injury
The contralateral ACL injury rate in our study is lower or comparable to previous
research (see Table 3.4 for comparisons). The lower rates of contralateral ACL
injuries may be due to the bilateral training in the ACL-SPORTS training program: all
agility drills and a majority of the plyometric and strengthening activities were
performed in both limbs. With similar altered movement patterns and impairments
predicting primary and secondary ACL injuries18,66,110, if poor mechanics and
movement patterns were at fault in primary ACL injury, similar mechanics and
movement patterns may exist in the contralateral limb. Additionally, the uninvolved
limb may also develop altered mechanics as compensation for the injured limb23,111,156.
Neuromuscular training can improve impairments15,119 and movement patterns28,101.
The ACL-SPORTS training emphasis on proper landing technique and movement
patterns during agilities, plyometric and performance activities bilaterally155 may
explain the lower contralateral injury rate in our study.
43
3.4.3 Return to Sport
Because athletes in our study had the highest rate of return to sport (100% returned to
sport, 87% to preinjury level24) reported in the literature8,150, they also had greater
sports exposure and subsequently, higher risk of any second ACL injury142,150. Yet, the
rate of second ACL injury in our study was not higher than previous research149,150.
Webster et al did not report the rate of returning to cutting/pivoting sports149,150 and
neither Paterno et al109,113 nor Webster et al149,150 reported any control of their
participants’ rehabilitation. Thus, the similarities in injury rates across different studies
may reflect a positive effect of our intervention.
3.4.4 Post-surgical follow-up
We registered new injuries in the first 2 years after ACL reconstruction. Over half of
all second injuries occur in the first year after ACLR149,150, and more than three
quarters occur within 2 years of surgery149. There were minimal differences in rates of
second injuries from 1- to 2-years after return to sport109,113, with a mean time from
RTS to second injury of 7.0 months113. In the female athletes of the ACL-SPORTS
trial, average time from surgery to RTS was 8.5 months, giving an average follow-up
of 15.5 months after RTS. Therefore, our 2-year registration period should be
sufficient to capture most second ACL injuries in our cohort.
44
3.4.5 RTS criteria
Passing RTS criteria can reduce risk of second ACL injuries47,58,79, but there is
conflicting evidence about the efficacy and impact of these criteria86,108. All athletes in
the ACL-SPORTS trial were required to pass objective criteria and have surgeon
approval for RTS: ≥90% QI and four single legged hop limb symmetry index (LSI),
≥90% scores on the Knee Outcomes Survey-Activities of Daily Living Subscale
(KOS-ADLS) and a single item global gating of perceived knee function (GRS). In the
cohorts reported by Paterno et al, athletes were required to have surgeon and physical
therapist approval for RTS but did not have to meet any objective criteria before
release109,113. The study cohort by Webster et al reported criteria including running and
squatting, but did not provide objective thresholds for passing149.
While we cannot separate the impact of our RTS criteria on rate of second ACL injury
from the impact of the training program, these findings suggest that the ACL-SPORTS
training program with objective RTS criteria may reduce risk of second ACL injury in
female athletes, however, it is not enough to reduce the risk of second ACL injury in
our youngest female athletes.
3.5 Clinical Implications The reduction in contralateral ACL injury rate in our female athletes compared to
other published research is promising, especially with an easy to implement training
45
program. However, our overall second injury rate of 26% is still much too high to
believe we have addressed the needs of our athletes. While the ACL-SPORTS training
was highly effective in reducing second ACL injury rates in male athletes (1 second
injury in 40 athletes)12, it was not as effective in female athletes. Current rehabilitation
programs are not meeting all the needs of female athletes, particularly those under 18
years. High compliance to a neuromuscular training program is associated with a
lower rate of ACL injuries in female athletes139. Higher volume and more frequent,
longer duration sessions are effective for primary knee injury prevention140. However,
ten sessions over five weeks, as in our study, may not maximize the benefits of
training for female athletes. Additional, research on longer, higher intensity, more
frequent secondary prevention programs for female athletes are needed, as well as
research on the influence of types of feedback52,53 and psychological readiness to
return to sport7,78,151.
3.6 Strengths and Limitations A strength of this study is our sample. We recruited from a variety of surgeons and
participants had post-operative rehabilitation at multiple physical therapy clinics,
making our results generalizable. Reasonable enrollment criteria ensured that all
participants entered the study at an appropriate point to begin the return to sport
progression but were not overly burdensome.
46
Athletes self-reported return to sport and level of participation and we did not assess
number of athletic exposures (practice/games). Because all athletes were required to
meet RTS criteria, we are unable to separate the effects of the training program from
the RTS criteria. Additionally, while a majority of second ACL injuries occur within
two years of ACLR, 2 years may not be sufficient follow-up to capture the true rate of
contralateral ACL injuries, which may occur later after ACLR.
While our sample of n=39 is small, Type II error is unlikely. Post-hoc analysis
revealed an effect size of w=0.047 for power of (1-β)=0.059. We would have needed
more than 3000 participants to be adequately powered to detect a between group
difference.
3.7 Conclusions While the addition of perturbation training to a secondary injury prevention program
does not seem to have benefits for female athletes, the participants in the ACL-
SPORTS training program report fewer contralateral injuries compared to previously
published results.
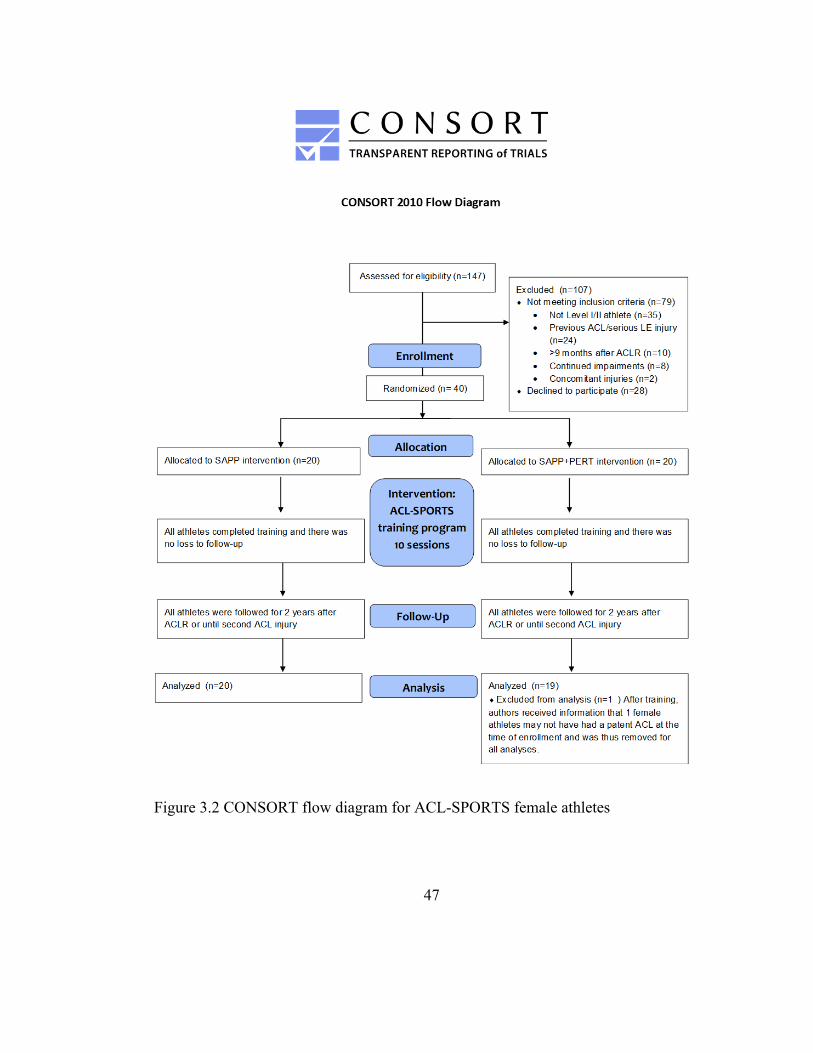
47
Figure 3.2 CONSORT flow diagram for ACL-SPORTS female athletes
48
HIGH RATES OF RETURN TO SPORT AND COMPETITIVE LEVEL WITH A SPECIALIZED INTERVENTION REGARDLESS OF TIMING OF
INTERVENTION
4.1 Introduction Anterior cruciate ligament (ACL) injury is a common sports injury2 with considerable
lasting effects on both activities of daily living and sports participation.104,105,135 While
91% of athletes expect to return to their previous levels of sport participation after an
anterior cruciate ligament reconstruction (ACLR), a 2014 meta-analysis found only
55% are able to return to their pre-injury levels of competition and only 80% return to
any sport activity after their ACLR.8
A successful return to sport is not the end of the journey. Athletes who do successfully
return to cutting and pivoting sports have a higher risk for a second ACL injury (both
graft rupture and contralateral ACL injury) compared to those who return to less
strenuous sports.150 Approximately one-third experience an second ACL injury, with
nearly half of those second injuries occurring within two months of their return.58
Objective return to sport (RTS) criteria can reduce these rates,12,58 with quadriceps
strength and performance measure symmetry currently recommended.1,6,58,79,112
Chapter 4
49
A recent clinical practice guideline recommends a phase of pre-operative
rehabilitation, with a systematic review of eight studies finding pre-operative
rehabilitation was effective in improving post-operative outcomes in patients waiting
for ACLR.4 Current post-operative recommendations include 9-12 months of
quadriceps strengthening and neuromuscular retraining.10,54,77,98,141 Previous work
from our lab has shown improved patient-reported outcomes, improved quadriceps
strength symmetry, and improved hop performance symmetry after a ten-session
progressive intervention in both ACL-deficient and reconstructed athletes.11,83,134 It
may not be possible, however, to have both extended pre-operative and post-operative
intervention due to financial limitations or insurance visit restrictions. We do not
currently know if the timing of this intervention impacts the rates of second injuries or
return to sport/competitive level, nor do we know the best recommendation for an
athlete if there are a limited number of physical therapy visits available.
The purpose of this work is to compare the rates of return to sport, return to
competitive level, and second ACL injuries in the two years after ACLR between a
group who received a ten-session intervention before reconstruction and a group who
received the intervention in the return to sports phase of rehabilitation after ACLR.
50
4.2 Methods This is a secondary analysis of an ongoing longitudinal prospective cohort study and a
randomized control trial.
4.2.1 Participants
The Delaware-Oslo Cohort (DOC) is a prospective cohort study of 13- to 55-year-
olds, participated in and planning to return to a cutting/pivoting/jumping sport more
than 50 hours per year. They were enrolled with a complete unilateral ACL rupture,
confirmed by 3-mm or greater difference in anterior tibial excursion with instrumented
arthrometry33 (KT1000; MEDmetric Corporation, San Diego, CO). They had a ten-
session intervention and then self-selected operative or non-operative management.
Exclusion criteria included a repairable meniscus, symptomatic grade III injury to
other knee ligaments, or greater than 1-cm2 full-thickness articular cartilage lesion.
This analysis uses only those in Delaware who self-selected ACLR (n=62). The study
was approved by the University of Delaware Institutional Review Board and all
patients provided written informed consent, or parental consent with written assent if
under 18 years old at enrollment. The Delaware-Oslo Cohort Study is supported by
grant R37-HD037985 from the National Institutes of Health.
The Anterior Cruciate Ligament-Specialized Post-Operative Return to Sports (ACL-
SPORTS) randomized control trial enrolled athletes 13-55 years old, who participated
51
in and planned to return to a cutting/pivoting/jumping sport for more than 50 hours per
year (n=70). Patients were enrolled 3-9 months after ACLR and had a ten-session
intervention. Exclusion criteria included a repairable meniscus, symptomatic grade III
injury to other knee ligaments, or greater than 1-cm2 full-thickness articular cartilage
lesion. The study was approved by the University of Delaware Institutional Review
Board and all patients provided written informed consent, or parental consent with
written assent if under 18 years old at enrollment. The ACL-SPORTS trial is
registered at clinicaltrials.gov (NCT01773317) and is supported by grant R01-
AR048212 from the Eunice Kennedy Shriver National Institute of Child Health and
Human Development.
4.2.2 Intervention
All participants in the DOC had ten sessions of progressive strengthening, agilities,
plyometrics, performance, and perturbation training.38 The athletes in the ACL-
SPORTS study were randomized, with all athletes receiving progressive strength,
agilities, plyometrics, and performance training and half also participating in the
perturbation exercises.154 However, no differences in strength, performance, return to
sport,11,13,24 or second injury12 were found between those who did and did not have
perturbation training, so the groups for ACL-SPORTS have been collapsed for this
analysis.
52
4.2.3 Surveys
We used the Tampa Scale of Kinseophobia (TSK-11) to assess fear of movement after
both surgery and intervention (6 months after ACLR for the DOC and post-
intervention for ACL-SPORTS). We administered the TSK-11 again two years after
ACLR. Also at the two-year time-point, participants were asked if they had had a
second ACL injury (yes/no, and if yes, side), returned to their pre-injury sport (yes/no,
if no was it because of knee related issues or lifestyle reasons), and if they had
returned to their pre-injury level of competition (yes/no, if no was it because of knee
related issues or lifestyle reasons). We used independent t-tests to compare age,
height, weight, TSK-11 and time to second ACL injury, and a Pearson chi-square to
compare sex, rate of returning to the same sport, rate of returning to the previous
competitive level, and rate of second injury.
4.3 Results Demographics for the two groups at enrollment are presented in Table 4.1. Only age
was statistically different between groups.
Rates of return to the same sport, competitive level are shown in Table 4.2 and Figures
4.1 and 4.2. There were no statistically significant differences between groups.
Rates of second injury are shown in Table 4.3 and Figure 4.3. We had two subjects
from the DOC cohort with missing second injury data (n=60). There was no
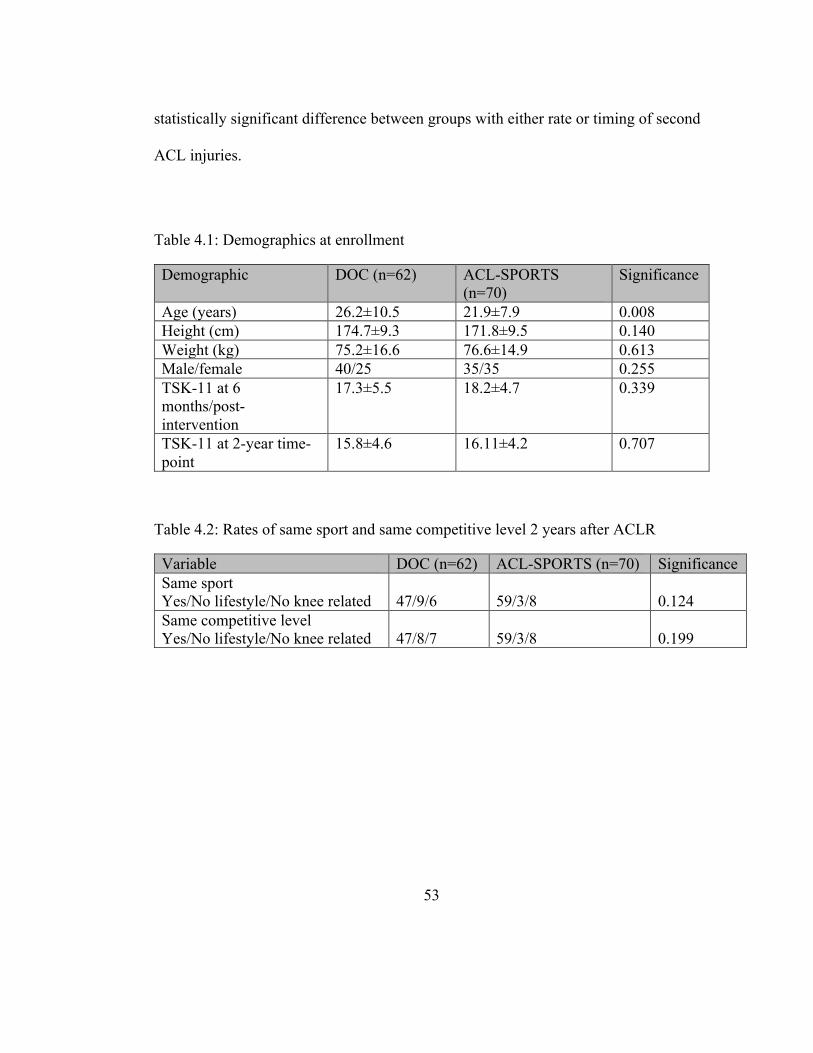
53
statistically significant difference between groups with either rate or timing of second
ACL injuries.
Table 4.1: Demographics at enrollment
Demographic DOC (n=62) ACL-SPORTS (n=70)
Significance
Age (years) 26.2±10.5 21.9±7.9 0.008 Height (cm) 174.7±9.3 171.8±9.5 0.140 Weight (kg) 75.2±16.6 76.6±14.9 0.613 Male/female 40/25 35/35 0.255 TSK-11 at 6 months/post-intervention
17.3±5.5 18.2±4.7 0.339
TSK-11 at 2-year time-point
15.8±4.6 16.11±4.2 0.707
Table 4.2: Rates of same sport and same competitive level 2 years after ACLR
Variable DOC (n=62) ACL-SPORTS (n=70) Significance Same sport Yes/No lifestyle/No knee related
47/9/6
59/3/8
0.124
Same competitive level Yes/No lifestyle/No knee related
47/8/7
59/3/8
0.199
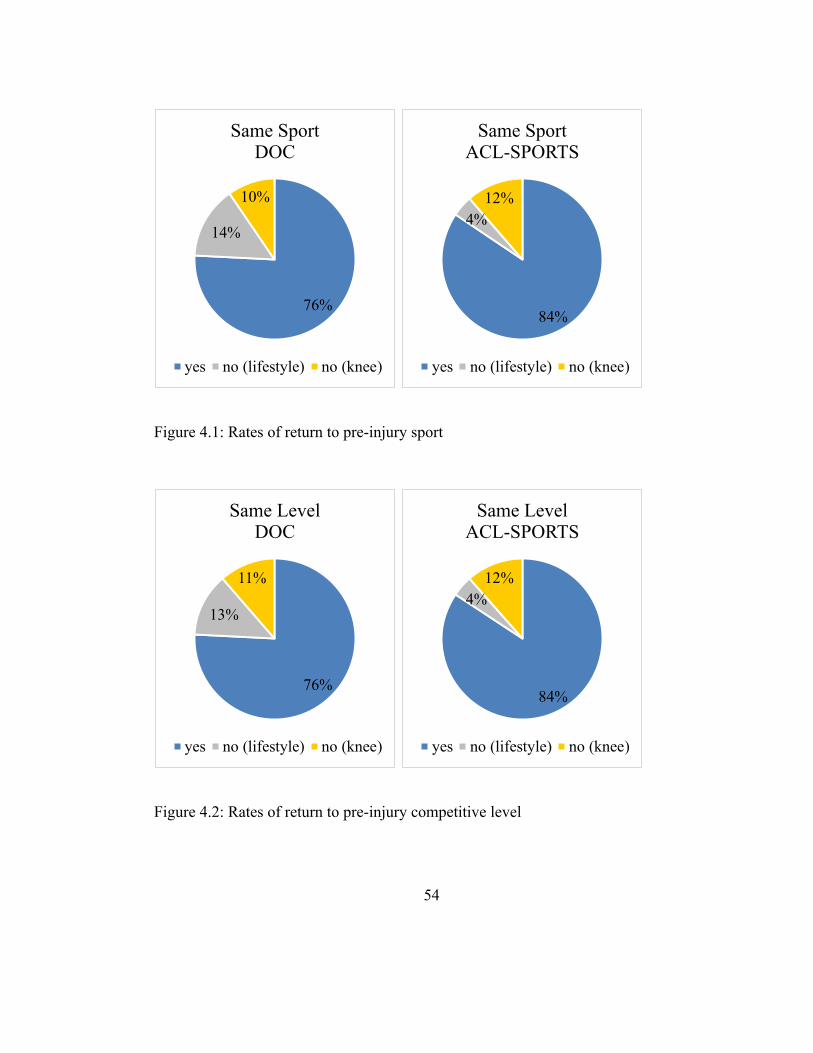
54
Figure 4.1: Rates of return to pre-injury sport
Figure 4.2: Rates of return to pre-injury competitive level
76%
14%
10%
Same SportDOC
yes no (lifestyle) no (knee)
84%
4%12%
Same SportACL-SPORTS
yes no (lifestyle) no (knee)
76%
13%
11%
Same LevelDOC
yes no (lifestyle) no (knee)
84%
4%12%
Same LevelACL-SPORTS
yes no (lifestyle) no (knee)
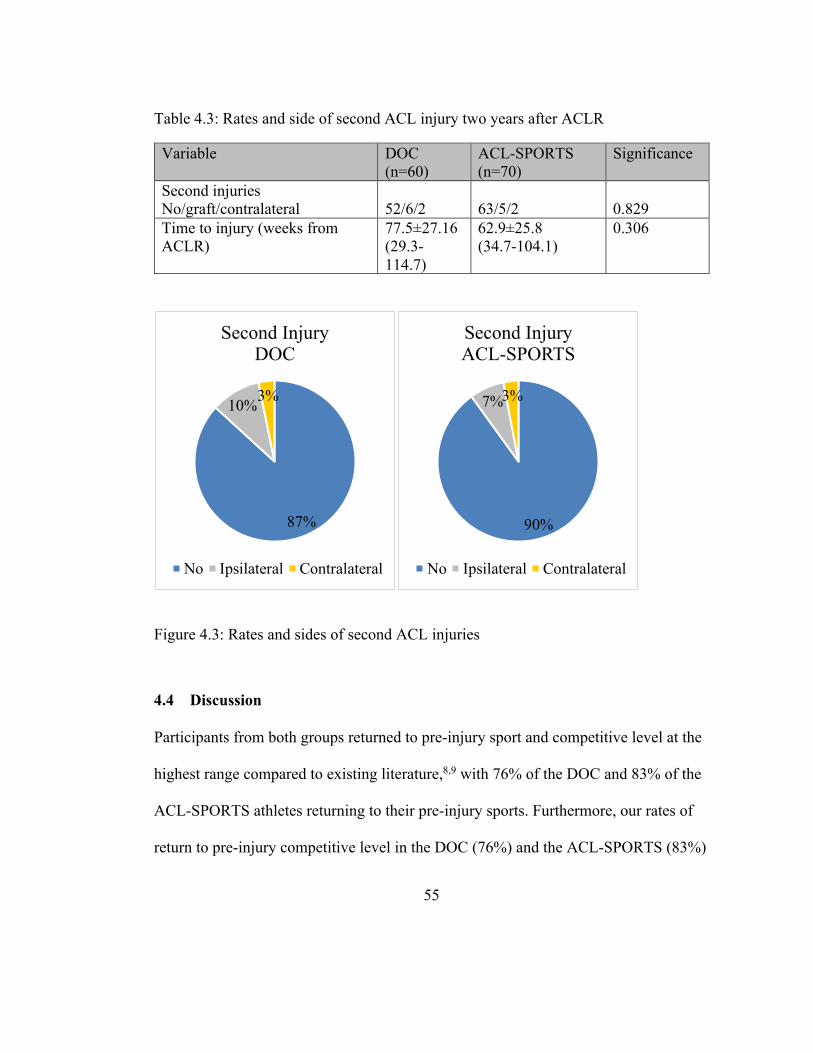
55
Table 4.3: Rates and side of second ACL injury two years after ACLR
Variable DOC (n=60)
ACL-SPORTS (n=70)
Significance
Second injuries No/graft/contralateral
52/6/2
63/5/2
0.829
Time to injury (weeks from ACLR)
77.5±27.16 (29.3-114.7)
62.9±25.8 (34.7-104.1)
0.306
Figure 4.3: Rates and sides of second ACL injuries
4.4 Discussion Participants from both groups returned to pre-injury sport and competitive level at the
highest range compared to existing literature,8,9 with 76% of the DOC and 83% of the
ACL-SPORTS athletes returning to their pre-injury sports. Furthermore, our rates of
return to pre-injury competitive level in the DOC (76%) and the ACL-SPORTS (83%)
87%
10%3%
Second InjuryDOC
No Ipsilateral Contralateral
90%
7%3%
Second InjuryACL-SPORTS
No Ipsilateral Contralateral
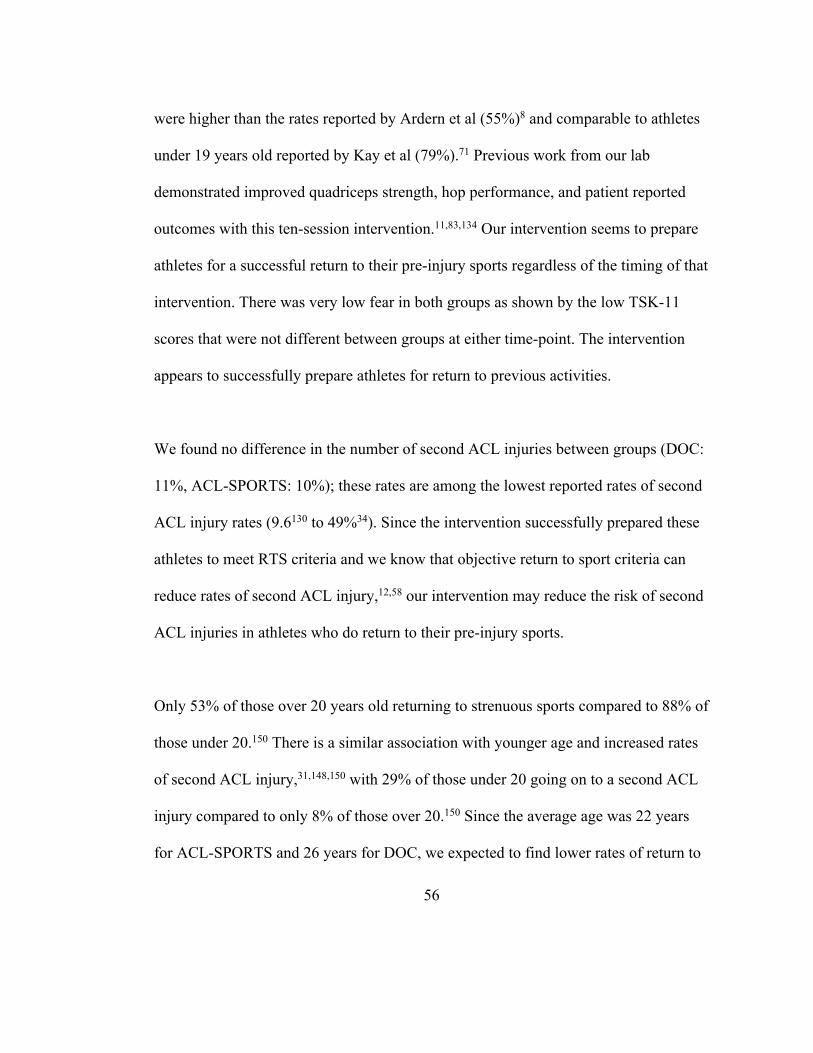
56
were higher than the rates reported by Ardern et al (55%)8 and comparable to athletes
under 19 years old reported by Kay et al (79%).71 Previous work from our lab
demonstrated improved quadriceps strength, hop performance, and patient reported
outcomes with this ten-session intervention.11,83,134 Our intervention seems to prepare
athletes for a successful return to their pre-injury sports regardless of the timing of that
intervention. There was very low fear in both groups as shown by the low TSK-11
scores that were not different between groups at either time-point. The intervention
appears to successfully prepare athletes for return to previous activities.
We found no difference in the number of second ACL injuries between groups (DOC:
11%, ACL-SPORTS: 10%); these rates are among the lowest reported rates of second
ACL injury rates (9.6130 to 49%34). Since the intervention successfully prepared these
athletes to meet RTS criteria and we know that objective return to sport criteria can
reduce rates of second ACL injury,12,58 our intervention may reduce the risk of second
ACL injuries in athletes who do return to their pre-injury sports.
Only 53% of those over 20 years old returning to strenuous sports compared to 88% of
those under 20.150 There is a similar association with younger age and increased rates
of second ACL injury,31,148,150 with 29% of those under 20 going on to a second ACL
injury compared to only 8% of those over 20.150 Since the average age was 22 years
for ACL-SPORTS and 26 years for DOC, we expected to find lower rates of return to
57
sport and second ACL injuries in the DOC group.31,148,150 While there is a strong
association between age and returning to cutting/pivoting sports,19,130,150 , recent work
from our cohort showed that activity and functional readiness, not age, were the
critical factors for second anterior cruciate ligament injury and that age is a proxy for
returning to high risk sports.57 The similar rate of return to sport and competitive level
for the DOC group compared to the younger ACL-SPORTS group may therefore
explain why there was not a difference in second ACL injury rates between groups.
Our neuromuscular and strength training intervention may be addressing the needs of
older athletes, increasing their rate of return to pre-injury sports/competitive level.
Since the group who had the intervention pre-operatively showed excellent post-
surgical outcomes, both in this analysis and in other studies,28,38,62,100 it is further
evidence that delaying surgery for pre-operative rehabilitation positively impacts long
term clinical outcomes41 and that individualized decision-making regarding timing of
ACLR is appropriate.46,55 Since previous studies found no extra benefit from the
addition of perturbation training,11,13,24,27 progressive pre-operative rehabilitation that
addresses strength, range of motion, and control of swelling may not need multiple
visits of skilled physical therapy intervention. For patients with limited resources
(financial or insurance-based), participating a progressive pre-operative home program
to save physical therapy visits for the end of rehabilitation may be beneficial to
address patient-specific impairments and sport-specific return to sports training.
58
4.5 Strengths and Limitations While there were obvious differences in part of the enrollment criteria (ACL-deficient
versus return to sports phase after reconstruction), age range, sport participation,
intention to return, and all exclusion criteria were the identical for both groups. All
interventions for both DOC and ACL-SPORTS were provided by physical therapists
at the University of Delaware Physical Therapy Clinic. The participants in the DOC
were not asked about a return to any sport (versus return to pre-injury sport), so we
cannot assess that rate in the DOC; athletes in the ACL-SPORTS study had a 97%
return to any sport rate (95% for men12, 100% for women24).
4.6 Conclusion Both those who received the intervention pre-operatively and those who received the
intervention in the return to sports phase of rehabilitation after ACLR reported among
the highest rates of return to their pre-injury sport and competitive level compared to
previously published literature, while timing of intervention did not have a statistically
significant impact on rates of return to sport, competitive level, or second ACL injury.
A ten-session intervention may prepare athletes for a successful return to their pre-
injury sport and level of competition and reduce the rate of second ACL injuries.
59
LOW LOADING OF THE MEDIAL TIBIOFEMORAL COMPARTMENT DURING GAIT FIVE YEARS AFTER ACL INJURY IS PREDICTIVE OF
SMALLER JOINT SPACE WIDTH AT TEN YEARS
5.1 Introduction Anterior cruciate ligament (ACL) injuries have devastating consequences to both
activities of daily living and sport participation.104,105,135 Patient expectations do not
match actual outcomes. 98% of patients expect no or only a slightly higher risk of
osteoarthritis (OA) after injury and ACL reconstruction (ACLR),44 yet up to 50% of
ACL injured individuals develop radiographic OA within 20 years.14,32,74,84
Current best recommendations for the treatment of OA include physical therapy,
education, pain control, medication, and surgery.106,163 These secondary and tertiary
level treatments address symptoms but are unable to reverse extant joint damage.106,122
The peak age of ACL injury between 15-25 years old16,117,126,162 and roughly 50%
developing radiographic OA within ten to twenty years of ACL
injury/reconstruction.84 Thus, identification of modifiable risk factors for primary level
treatment before the initiation of cartilage degradation is critical.
Chapter 5
60
One possible risk factor for the development of OA is gait biomechanics, which are
altered after ACL injury/reconstruction.29,51,60–62,110,111,120,124,131 Gait biomechanics
continue to normalized from up to eight years after ACLR,40,51 suggesting a continued
long-term recovery of function and joint loading. These gait changes shift loading to
regions of cartilage not adapted to joint loading39 which may result in cartilage
degradation. The medial compart of the tibiofemoral joint carries the majority of the
tibiofemoral load127,158 and under-loading of the medial tibiofemoral compartment was
associated with radiographic OA changes five years after ACLR.152 Since healthy
cartilage responds positively to cyclic load,5 unloading normally loaded cartilage may
result in “deconditioned” cartilage, which if reloaded as gait biomechanics improve,
may account for the higher rates of radiographic knee OA after ACLR.
The purpose of this study was to analyze gait biomechanics five years after ACL
injury/reconstruction and to quantify its effect on medial tibiofemoral compartment
joint space width (JSW) five and ten years after ACL injury/reconstruction. We
hypothesized that low loading in the medial tibiofemoral compartment five years after
ACL injury would predict smaller medial compartment JSW at ten years. We
hypothesized that under-loading in the medial tibiofemoral compartment five years
after ACL injury/reconstruction would predict smaller JSW and a larger change in
JSW from five to ten years.
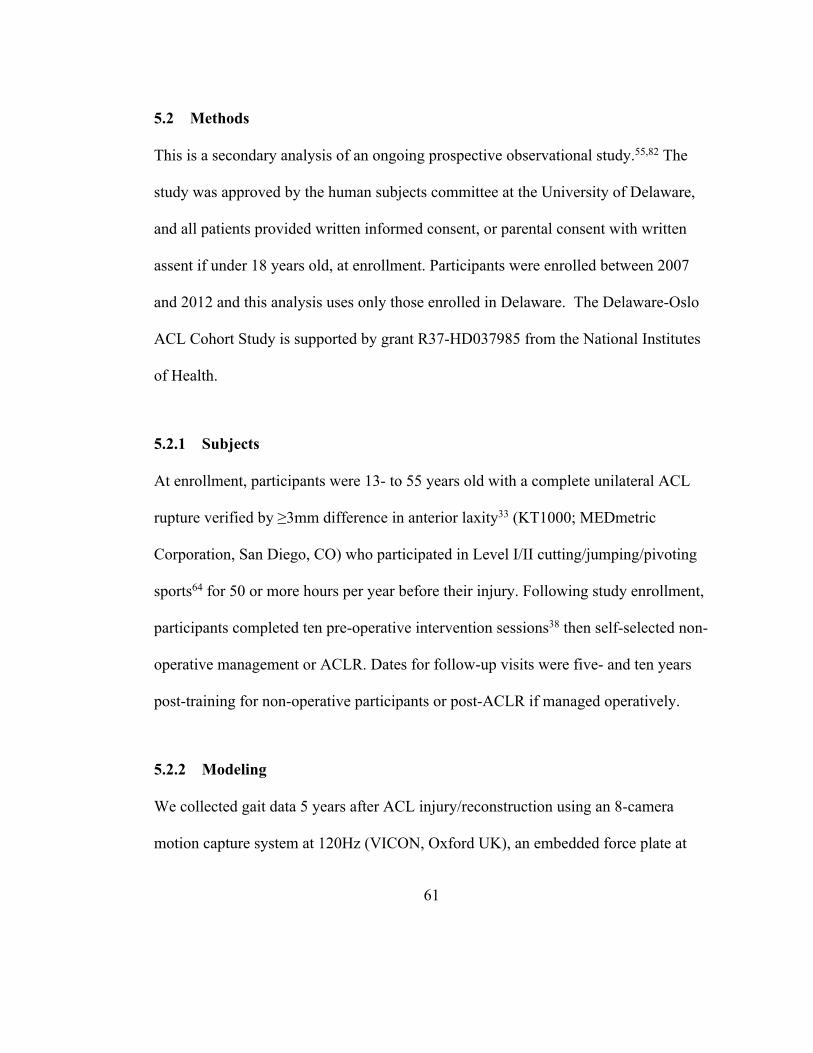
61
5.2 Methods This is a secondary analysis of an ongoing prospective observational study.55,82 The
study was approved by the human subjects committee at the University of Delaware,
and all patients provided written informed consent, or parental consent with written
assent if under 18 years old, at enrollment. Participants were enrolled between 2007
and 2012 and this analysis uses only those enrolled in Delaware. The Delaware-Oslo
ACL Cohort Study is supported by grant R37-HD037985 from the National Institutes
of Health.
5.2.1 Subjects At enrollment, participants were 13- to 55 years old with a complete unilateral ACL
rupture verified by ≥3mm difference in anterior laxity33 (KT1000; MEDmetric
Corporation, San Diego, CO) who participated in Level I/II cutting/jumping/pivoting
sports64 for 50 or more hours per year before their injury. Following study enrollment,
participants completed ten pre-operative intervention sessions38 then self-selected non-
operative management or ACLR. Dates for follow-up visits were five- and ten years
post-training for non-operative participants or post-ACLR if managed operatively.
5.2.2 Modeling We collected gait data 5 years after ACL injury/reconstruction using an 8-camera
motion capture system at 120Hz (VICON, Oxford UK), an embedded force plate at
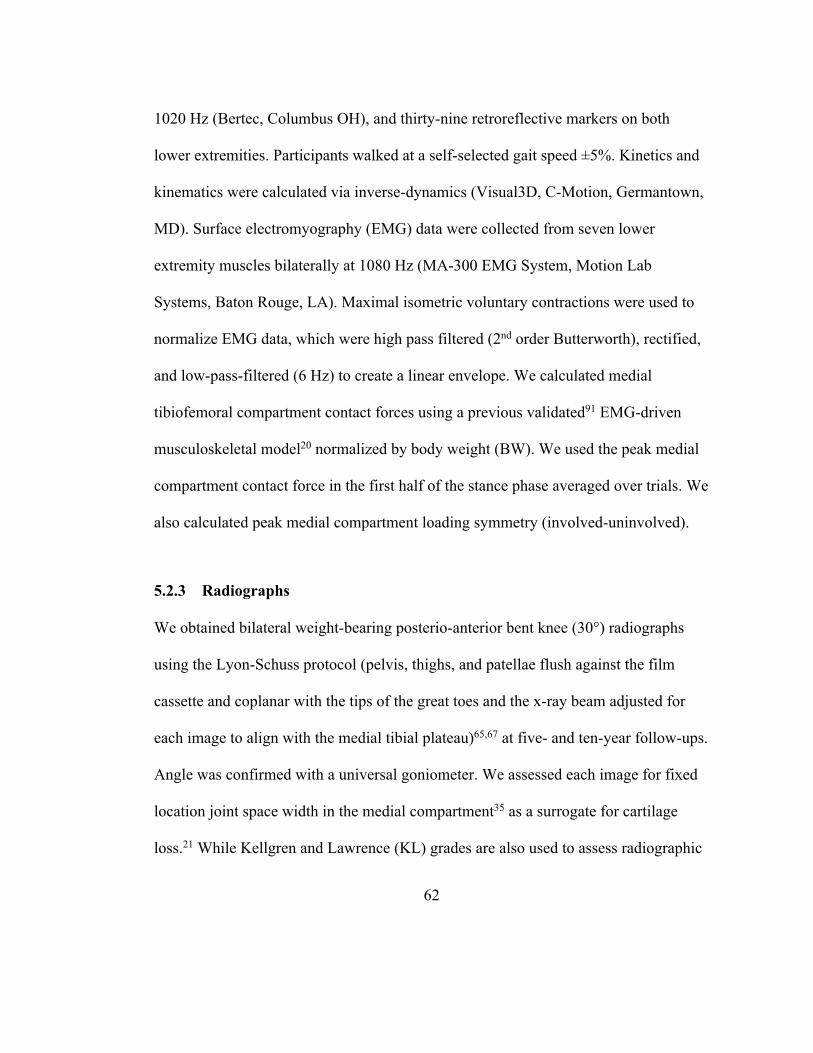
62
1020 Hz (Bertec, Columbus OH), and thirty-nine retroreflective markers on both
lower extremities. Participants walked at a self-selected gait speed ±5%. Kinetics and
kinematics were calculated via inverse-dynamics (Visual3D, C-Motion, Germantown,
MD). Surface electromyography (EMG) data were collected from seven lower
extremity muscles bilaterally at 1080 Hz (MA-300 EMG System, Motion Lab
Systems, Baton Rouge, LA). Maximal isometric voluntary contractions were used to
normalize EMG data, which were high pass filtered (2nd order Butterworth), rectified,
and low-pass-filtered (6 Hz) to create a linear envelope. We calculated medial
tibiofemoral compartment contact forces using a previous validated91 EMG-driven
musculoskeletal model20 normalized by body weight (BW). We used the peak medial
compartment contact force in the first half of the stance phase averaged over trials. We
also calculated peak medial compartment loading symmetry (involved-uninvolved).
5.2.3 Radiographs We obtained bilateral weight-bearing posterio-anterior bent knee (30°) radiographs
using the Lyon-Schuss protocol (pelvis, thighs, and patellae flush against the film
cassette and coplanar with the tips of the great toes and the x-ray beam adjusted for
each image to align with the medial tibial plateau)65,67 at five- and ten-year follow-ups.
Angle was confirmed with a universal goniometer. We assessed each image for fixed
location joint space width in the medial compartment35 as a surrogate for cartilage
loss.21 While Kellgren and Lawrence (KL) grades are also used to assess radiographic

63
OA,73 tibiofemoral joint space width (JSW) may be measured on plain film
radiographs as a surrogate for cartilage loss.21 The International Knee Documentation
Committee (IKDC) has published objective criteria for JSW to classify narrowing of
the tibiofemoral compartment.64,97 JSW was measured by a single rater (JLJ,
ICC=0.959) (SigmaView, AGFA HealthCare, Mortsel, Belgium).
5.2.4 Statistics We used linear regression to assess effect of medial compartment loading five years
after ACL injury/reconstruction on medial compartment JSW at ten years, loading
symmetry five years after ACL injury/reconstruction. on medial compartment JSW at
ten years and loading symmetry five years after ACL injury/reconstruction on change
in JSW from five to ten years. Statistical significance was set at p ≤0.05 a priori.
5.3 Results Sixteen participants (6 female) had complete data sets, 6 had self-selected to manage
non-operatively (3 female), 1 subject had a medial meniscus repair at ACLR. The
average age was 38.0±11.8 years (range 21.5-58.6 years) and body mass index (BMI)
was 28.1±4.8 kg/m2 at the time of the five-year follow-up. None of our participants
had medial compartment radiographic OA five years after ACL injury/reconstruction
based on IKDC objective criteria of <4mm of JSW.64,97
64
Involved medial compartment loading at five years predicted involved medial
compartment JSW at ten years (R2=0.61, p<0.001, Figure 5.1). Loading symmetry
(involved-uninvolved) predicted JSW at ten years (R2=0.32, p=0.024, Figure 5.2).
Loading symmetry did not predict change in JSW from five- to ten years (R2=0.06,
p=0.379, no figure). Results varied by surgical status; all participants with
radiographic OA at ten years had chosen ACLR as their management (Figure 5.3).
Figure 5.1: Predicting medial compartment JSW at ten years with loading at ten years The black dashed line represents R2=0.61. The red vertical dashed line represents the mean compartment loading, 2.7 BW. The red horizontal dashed line represents 4.0mm, the IKDC cut-off for the presence of radiographic OA.
0.01.02.03.04.05.06.07.08.09.0
10.0
0 0.5 1 1.5 2 2.5 3 3.5 4 4.5
Invo
lved
med
ial J
SW (m
m)
Involved medial compartment joint loading (BW)
Predicting medial JSW at 10 years from medial compartment loading at 5 years
65
Figure 5.2: Predicting medial compartment JSW at ten years with loading symmetry at five years
The black dashed line represents R2=0.32. The red vertical dashed lines represent 0.3 BW, the MDC for contact force, used to define symmetry and under- and over-loading. The red horizontal dashed line represents 4.0mm, the IKDC cut-off for the presence of radiographic OA.
0.01.02.03.04.05.06.07.08.09.0
10.0
-1.5 -1 -0.5 0 0.5 1 1.5 2
Invo
lved
med
ial J
SW (m
m)
loading symmetry (BW)
Predicting medial JSW at 10 years from loading symmetry at 5 years
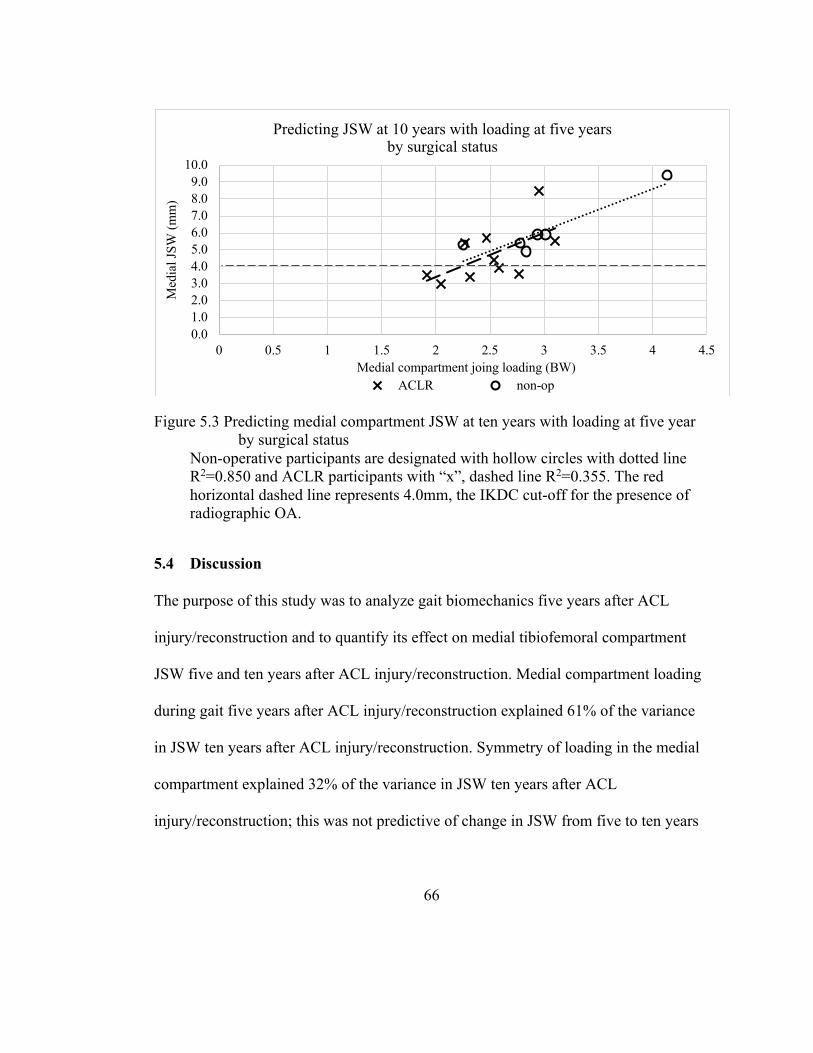
66
Figure 5.3 Predicting medial compartment JSW at ten years with loading at five year by surgical status
Non-operative participants are designated with hollow circles with dotted line R2=0.850 and ACLR participants with “x”, dashed line R2=0.355. The red horizontal dashed line represents 4.0mm, the IKDC cut-off for the presence of radiographic OA.
5.4 Discussion The purpose of this study was to analyze gait biomechanics five years after ACL
injury/reconstruction and to quantify its effect on medial tibiofemoral compartment
JSW five and ten years after ACL injury/reconstruction. Medial compartment loading
during gait five years after ACL injury/reconstruction explained 61% of the variance
in JSW ten years after ACL injury/reconstruction. Symmetry of loading in the medial
compartment explained 32% of the variance in JSW ten years after ACL
injury/reconstruction; this was not predictive of change in JSW from five to ten years
0.01.02.03.04.05.06.07.08.09.0
10.0
0 0.5 1 1.5 2 2.5 3 3.5 4 4.5
Med
ial J
SW (m
m)
Medial compartment joing loading (BW)
Predicting JSW at 10 years with loading at five yearsby surgical status
ACLR non-op
67
after ACL injury/reconstruction. Additionally, all participants with radiographic OA
changes ten years after ACL injury/reconstruction chose ACLR.
None of our participants had medial compartment radiographic OA five years after
ACL injury/reconstruction based on the IKDC objective criteria of >4mm. Ten years
after ACL injury/reconstruction, five participants had JSW between 3.0 and 3.9mm,
indicating mild radiographic OA.64,97 When we compare symmetry of medial
compartment loading using the previously established minimal detectable change
(MDC) of 0.3 BW50 in those classified with radiographic OA at ten years, three were
under-loaders, one was symmetrical, and one was an over-loader. For the eleven
participants without radiographic OA at ten years, one was an under-loader, five were
symmetrical, and five were over-loaders. When we analyze totally medial tibiofemoral
compartment load, four of the participants with radiographic OA at ten years were
below the mean compartment load of 2.7 BW with one just above; for those without
radiographic OA, four loaded below the mean of 2.7 BW, and seven were above.
Previous research has suggested that under-loading, and not overloading, of the
tibiofemoral joint may be the underlying cause of degenerative changes after ACL
injury.5,76,153,161 We found not only the symmetry of loading but the amount of load
was predictive of JSW at ten years after ACL injury/reconstruction. Gait biomechanics
are modifiable with a ten-session pre-operative intervention,62,111,153 but did not change
when the intervention was in the return to sports phase of rehabilitation after ACLR.25–
68
27 Thus, rehabilitation and intervention to restore both normal symmetry and quantity
of medial tibiofemoral compartment loading early after ACL injury/reconstruction
may be a primary treatment for those at high risk for developing OA after ACL
injury/reconstruction.
Even though ACLR is the most common recommendation after an ACL injury,102
there is growing evidence that non-operative management of ACL injuries is
successful, with no difference in patient reported function49,55,99 clinical outcomes,56,99
or OA progression49 between non-operative and operative managed participants. A
2014 meta-analysis of six studies found a higher relative risk for developing any
radiographic OA in the non-operatively managed patients but a lower relative risk of
moderate or severe radiographic OA compared to the operatively managed patients3,
however, all five of the participants with radiographic OA changes in this analysis
were operatively managed. The results of this study add to the evidence that those who
choose to manage non-operatively after ACL injury should not assume poorer
outcomes than those who select reconstruction.
In our participants, those who demonstrated low loading in the medial tibiofemoral
compartment during gait at five years had less joint space at ten years after ACL
injury/reconstruction. Since healthy cartilage responds positively to cyclic load,5 not
only the symmetry of loading but the amount of load may influence the maintenance
69
of JSW after ACL injury/ACLR. Additionally, only those who chose ACLR went on
to develop radiographic OA. The identification of these potentially modifiable risk
factors may drive future research into rehabilitation interventions to address low and
asymmetrical loading of the medial compartment of the tibiofemoral joint which may
reduce the rates of radiographic knee OA after ACL injury/reconstruction.
5.5 Conclusions We were able to predict 61% of the variance in JSW at ten years with medial
compartment loading at five years: the more loading that occurred in the medial
compartment at five years, the more JSW at ten years. Loading symmetry was
predictive of JSW at ten years but not predictive of change in joint space width from
five- to ten years after ACLR. All participants with radiographic OA changes were
operatively managed. These potentially modifiable risk factors may allow for the
development of interventions to target those at high risk of developing radiographic
OA before measurable joint degradation occurs.
70
SUMMARY
6.1 Overview of the aims
This dissertation aimed to improve clinical decision-making regarding patient-reported
outcome measures, second ACL injury risk, rate of return to sport and competitive
level, the timing of intervention, and identification of potentially modifiable risk
factors of radiographic knee OA in patients after an ACL injury/reconstruction.
This work aimed to address the high, unmet expectations of our patients and improve
our clinical decision-making to address common limitations and risks after ACL injury
and reconstruction.
6.2 Aim 1 Purpose
We determined the construct validity of the GRS and assessed the responsiveness of
the GRS, the IKDC-SKF, the KOS-ADLS, and the KOOS subscales with effect sizes
and ceiling effects in the five years after ACL injury and reconstruction.
6.2.1 Hypothesis 1.1:
We hypothesized that the GRS would have good construct validity when compared
with the IKDC-SKF.
Chapter 6
71
6.2.2 Hypothesis 1.2:
We hypothesized there would be no difference in responsiveness between the GRS,
the IKDC-SKF, the KOS-ADLS, and the KOOS subscales as measured by effect size
and ceiling effects.
6.2.3 Conclusion
The GRS had good construct validity, a small MDC, and responded similarly to the
IKDC-SKF, KOS-ADLS, and KOOS measures and was responsive to patient change.
The ease of use and patient-specific nature of the single item GRS means that, for
clinical practice, it may be appropriate to use as a frequent measure throughout
rehabilitation with other measures used as needed at specific milestones or for
additional details.
6.3 Aim 2 Purpose:
We compared the rate and side of second ACL injuries in female athletes who
received post-operative strength, agility, plyometrics, and prevention training (SAPP)
compared to those who received post-operative training plus specialized perturbation
(SAAP+PERT) training.
6.3.1 Hypothesis 2.1:
We hypothesized that SAPP+PERT athletes would have fewer second ACL injuries
than those who received SAPP training alone.
6.3.2 Conclusion
The addition of perturbation training to a secondary injury prevention program did not
have additional preventative benefits for female athletes. However, the participants in
72
the ACL-SPORTS training program reported fewer contralateral ACL injuries
compared to previously published results.
6.4 Aim 3 Purpose:
We analyzed the impact of the timing of a specialized intervention (pre-operatively
versus the return to sport phase) on rates of return to sport and competitive level and
rates of second ACL injury.
6.4.1 Hypothesis 3.1:
We hypothesized that those who received post-operative training would have a higher
rate of return to their pre-injury sports than those who had pre-operative training.
6.4.2 Hypothesis 3.2:
We hypothesized that those who received post-operative training would have a higher
rate of return to their pre-injury competitive levels of sport than those who had pre-
operative training.
6.4.3 Hypothesis 3.3:
We hypothesized that there would be no difference in rates of second ACL injury
between those who received pre-operative training and those who had post-operative
training.
6.4.4 Conclusion
Both the group that received the intervention pre-operatively and the group that
received the intervention in the return to sports phase of rehabilitation reported among
the highest rates of return to the same sport and competitive level reported in

73
published literature, but the timing of the intervention did not have a statistically
significant impact on rates of return to sport, competitive level, or second ACL injury.
6.5 Aim 4 Purpose:
Using medial compartment joint contact forces collected during gait at five years and
tibiofemoral JSW from radiographs at five and ten years after ACL
injury/reconstruction, we analyzed predictive factors of joint space narrowing.
6.5.1 Hypothesis 4.1:
We hypothesized that under-loading in the medial compartment of the knee during
gait five years after ACL injury/reconstruction would predict smaller JSW in the
medial tibiofemoral compartment ten years after ACL injury/reconstruction.
6.5.2 Hypothesis 4.2:
We hypothesized that lower loading in the medial compartment of the knee during gait
five years after ACL injury/reconstruction would predict smaller JSW in the medial
tibiofemoral compartment ten years after ACL injury/reconstruction.
6.5.3 Conclusion
We were able to predict 60% of the variance in JSW at ten years with medial
compartment loading at five years: the more loading that occurred in the medial
compartment at five years, the more JSW at ten years. Loading symmetry was
predictive of JSW at ten years but not predictive of change in joint space width from
five- to ten years after ACL injury/ reconstruction. The five participants with
radiographic OA at ten years were all operatively managed. These potentially
modifiable risk factors may allow for the development of interventions to target those
74
at high risk of developing radiographic OA before measurable joint degradation
occurs.
6.6 Summary of Work
Clinicians are faced with high patient expectations and low rates of return to sport and
high rates of second injury and OA. This work aimed to inform clinical decision-
making by analyzing the validity and responsiveness of a single-item patient-reported
outcome measure to improve provider communication and decrease provider and
patient burden, by analyzing the impact of specialized intervention on second ACL
injury rates in female athletes, by evaluating the impact of the timing of that
intervention on rates of return to sport/competitive level and second ACL injury, and
by identifying possibly modifiable risk factors for development of radiographic knee
OA.
75
1. Adams D, Logerstedt DS, Hunter-Giordano A, Axe MJ, Snyder-Mackler L. Current Concepts for Anterior Cruciate Ligament Reconstruction: A Criterion-Based Rehabilitation Progression. J Orthop Sport Phys Ther. 2012;42(7):601-614. doi:10.2519/jospt.2012.3871.
2. Agel J, Rockwood T, Klossner D. Collegiate ACL Injury Rates Across 15 Sports: National Collegiate Athletic Association Injury Surveillance System Data Update. Clin J Sport Med. 2016;26:518-523. http://insights.ovid.com/pubmed?pmid=27315457. Accessed May 15, 2017.
3. Ajuied A, Wong F, Smith C, et al. Anterior cruciate ligament injury and radiologic progression of knee osteoarthritis: A systematic review and meta-analysis. Am J Sports Med. 2014;42(9):2242-2252. doi:10.1177/0363546513508376.
4. Alshewaier S, Yeowell G, Fatoye F. The effectiveness of pre-operative exercise physiotherapy rehabilitation on the outcomes of treatment following anterior cruciate ligament injury: A systematic review. Clin Rehabil. 2017;31(1):34-44. doi:10.1177/0269215516628617.
5. Andriacchi TP, Koo S, Scanlan SF. Gait Mechanics Influence Healthy Cartilage Morphology and Osteoarthritis of the Knee. J Bone Jt Surg. 2009;91(Supplement 1):95-101. doi:10.2106/JBJS.H.01408.
6. Ardern CL, Glasgow P, Schneiders A, et al. 2016 Consensus statement on return to sport from the First World Congress in Sports Physical Therapy, Bern. Br J Sports Med. 2016;50(14):853-864. doi:10.1136/bjsports-2016-096278.
7. Ardern CL, Sonesson S, Forssblad M, Kvist J. Comparison of patient-reported outcomes among those who chose ACL reconstruction or non-surgical treatment. Scand J Med Sci Sports. 2017;27(5):535-544. doi:10.1111/sms.12707.
8. Ardern CL, Taylor NF, Feller JA, Webster KE. Fifty-five per cent return to competitive sport following anterior cruciate ligament reconstruction surgery:
REFERENCES
76
an updated systematic review and meta-analysis including aspects of physical functioning and contextual factors. Br J Sports Med. 2014;48(21):1543-1552. doi:10.1136/bjsports-2013-093398.
9. Ardern CL, Webster KE, Taylor NF, Feller JA. Return to the Preinjury Level of Competitive Sport After Anterior Cruciate Ligament Reconstruction Surgery. Am J Sports Med. 2011;39(3):538-543. doi:10.1177/0363546510384798.
10. Arundale AJH, Bizzini M, Giordano A, et al. Exercise-Based Knee and Anterior Cruciate Ligament Injury Prevention. J Orthop Sport Phys Ther. 2018;48(9):A1-A42. doi:10.2519/jospt.2018.0303.
11. Arundale AJH, Capin JJ, Zarzycki R, Smith A, Snyder-Mackler L. Functional and Patient-Reported Outcomes Improve Over the Course of Rehabilitation: A Secondary Analysis of the ACL-SPORTS Trial. Sports Health. 2018;10(5):441-452. doi:10.1177/1941738118779023.
12. Arundale AJH, Capin JJ, Zarzycki R, Smith AH, Snyder-Mackler L. Two Year ACL Reinjury Rate of 2.5%: Outcomes Reports of the Men in a Secondary ACL Injury Prevention Program (ACL-SPORTS). Int J Sports Phys Ther. 2018;13(3):422-431. doi:10.26603/ijspt20180422.
13. Arundale AJH, Cummer K, Capin JJ, Zarzycki R, Snyder-Mackler L. Report of the Clinical and Functional Primary Outcomes in Men of the ACL-SPORTS Trial: Similar Outcomes in Men Receiving Secondary Prevention With and Without Perturbation Training 1 and 2 Years After ACL Reconstruction. Clin Orthop Relat Res. 2017;475(10):2523-2534. doi:10.1007/s11999-017-5280-2.
14. Barenius B, Ponzer S, Shalabi A, Bujak R, Norlén L, Eriksson K. Increased risk of osteoarthritis after anterior cruciate ligament reconstruction: A 14-year follow-up study of a randomized controlled trial. Am J Sports Med. 2014;42(5):1049-1057. doi:10.1177/0363546514526139.
15. Beard DJ, Dodd CA, Trundle HR, Simpson AH. Proprioception enhancement for anterior cruciate ligament deficiency. A prospective randomised trial of two physiotherapy regimes. J Bone Joint Surg Br. 1994;76(4):654-659. http://www.ncbi.nlm.nih.gov/pubmed/8027158. Accessed October 10, 2019.
16. Beck NA, Lawrence JTR, Nordin JD, DeFor TA, Tompkins M. ACL Tears in School-Aged Children and Adolescents Over 20 Years. Pediatrics. 2017;139(3):e20161877. doi:10.1542/peds.2016-1877.
17. Black N. Patient reported outcome measures could help transform healthcare.
77
BMJ. 2013;346:f167. doi:10.1136/bmj.f167.
18. Boden BP, Dean GS, Feagin JA, Garrett WE. Mechanisms of anterior cruciate ligament injury. Orthopedics. 2000;23(6):573-578. http://www.ncbi.nlm.nih.gov/pubmed/10875418. Accessed December 3, 2018.
19. Brophy RH, Schmitz L, Wright RW, et al. Return to play and future ACL injury risk after ACL reconstruction in soccer athletes from the multicenter orthopaedic outcomes network (MOON) group. Am J Sports Med. 2012;40(11):2517-2522. doi:10.1177/0363546512459476.
20. Buchanan TS, Lloyd DG, Manal K, Besier TF. Neuromusculoskeletal modeling: Estimation of muscle forces and joint moments and movements from measurements of neural command. J Appl Biomech. 2004;20(4):367-395. doi:10.1123/jab.20.4.367.
21. Buckland-Wright JC, Macfarlane DG, Lynch JA, Jasani MK, Bradshaw CR. Joint space width measures cartilage thickness in osteoarthritis of the knee: high resolution plain film and double contrast macroradiographic investigation. Ann Rheum Dis. 1995;54:263-268. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1005571/pdf/annrheumd00504-0029.pdf. Accessed November 17, 2017.
22. Buller LT, Best MJ, Baraga MG, Kaplan LD. Trends in Anterior Cruciate Ligament Reconstruction in the United States. Orthop J Sport Med. 2015;3(1):2325967114563664. doi:10.1177/2325967114563664.
23. Butler RJ, Dai B, Garrett WE, Queen RM. Changes in landing mechanics in patients following anterior cruciate ligament reconstruction when wearing an extension constraint knee brace. Sports Health. 2014;6(3):203-209. doi:10.1177/1941738114524910.
24. Capin JJ, Failla MJ, Zarzycki R, et al. Superior 2-Year Functional Outcomes Among Young Female Athletes After ACL Reconstruction in Just 10 Return-to-Sport Training Sessions: Comparison of ACL-SPORTS Randomized Control Trial to Delaware-Oslo and MOON Cohorts. Orthop J Sport Med. 2019;(8):2325967119861311. doi:10.1177/2325967119861311.
25. Capin JJ, Khandha A, Zarzycki R, et al. Gait mechanics and tibiofemoral loading in men of the ACL-SPORTS randomized control trial. J Orthop Res. 2018;36(9):2364-2372. doi:10.1002/jor.23895.
26. Capin JJ, Zarzycki R, Arundale A, Cummer K, Snyder-Mackler L. Report of
78
the Primary Outcomes for Gait Mechanics in Men of the ACL-SPORTS Trial: Secondary Prevention With and Without Perturbation Training Does Not Restore Gait Symmetry in Men 1 or 2 Years After ACL Reconstruction. 2017;475(10):2513-2522. doi:10.1007/s11999-017-5279-8.
27. Capin JJ, Zarzycki R, Ito N, et al. Gait Mechanics in Women of the ACL‐SPORTS Randomized Control Trial: Interlimb Symmetry Improves Over Time Regardless of Treatment Group. J Orthop Res. 2019;37(8):jor.24314. doi:10.1002/jor.24314.
28. Chmielewski TL, Hurd WJ, Rudolph KS, Axe MJ, Snyder-Mackler L. Perturbation training improves knee kinematics and reduces muscle co-contraction after complete unilateral anterior cruciate ligament rupture. Phys Ther. 2005;85(8):740-749; discussion 750-4. http://www.ncbi.nlm.nih.gov/pubmed/16048422. Accessed December 12, 2018.
29. Chmielewski TL, Rudolph KS, Fitzgerald GK, Axe MJ, Snyder-Mackler L. Biomechanical evidence supporting a differential response to acute ACL injury. Clin Biomech. 2001;16(7):586-591. doi:10.1016/S0268-0033(01)00050-X.
30. Cohen J. Statistical Power Analysis for the Behavioral Sciences.; 1988.
31. Cordasco FA, Black SR, Price M, et al. Return to Sport and Reoperation Rates in Patients Under the Age of 20 After Primary Anterior Cruciate Ligament Reconstruction: Risk Profile Comparing 3 Patient Groups Predicated Upon Skeletal Age. Am J Sports Med. 2019;47(3):628-639. doi:10.1177/0363546518819217.
32. Culvenor AG, Collins NJ, Guermazi A, et al. Early Knee Osteoarthritis Is Evident One Year Following Anterior Cruciate Ligament Reconstruction: A Magnetic Resonance Imaging Evaluation. Arthritis Rheumatol. 2015;67(4):946-955. doi:10.1002/art.39005.
33. Daniel DM, Stone M Lou, Dobson BE, Fithian DC, Rossman DJ, Kaufman KR. Fate of the ACL-injured Patient. Am J Sports Med. 1994;22(5):632-644. doi:10.1177/036354659402200511.
34. Drogset JO, Grøntvedt T, Robak OR, Mølster A, Viset AT, Engebretsen L. A sixteen-year follow-up of three operative techniques for the treatment of acute ruptures of the anterior cruciate ligament. J Bone Jt Surg - Ser A. 2006;88(5):944-952. doi:10.2106/JBJS.D.02876.
35. Duryea J, Neumann G, Niu J, et al. Comparison of radiographic joint space
79
width with magnetic resonance imaging cartilage morphometry: analysis of longitudinal data from the Osteoarthritis Initiative. Arthritis Care Res (Hoboken). 2010;62(7):932-937. doi:10.1002/acr.20148.
36. Eitzen I, Eitzen TJ, Holm I, Snyder-Mackler L, Risberg MA. Anterior cruciate ligament-deficient potential copers and noncopers reveal different isokinetic quadriceps strength profiles in the early stage after injury. Am J Sports Med. 2010;38(3):586-593. doi:10.1177/0363546509349492.
37. Eitzen I, Moksnes H, Snyder-Mackler L, Engebretsen L, Risberg MA. Functional tests should be accentuated more in the decision for ACL reconstruction. Knee Surg Sports Traumatol Arthrosc. 2010;18(11):1517-1525. doi:10.1007/s00167-010-1113-5.
38. Eitzen I, Moksnes H, Snyder-Mackler L, Risberg MA. A progressive 5-week exercise therapy program leads to significant improvement in knee function early after anterior cruciate ligament injury. J Orthop Sports Phys Ther. 2010;40(11):705-721. doi:10.2519/jospt.2010.3345.
39. Erhart-Hledik JC, Chu CR, Asay JL, Andriacchi TP. Gait mechanics 2 years after anterior cruciate ligament reconstruction are associated with longer-term changes in patient-reported outcomes. J Orthop Res. 2016:30-32. doi:10.1002/jor.23317.
40. Erhart-Hledik JC, Chu CR, Asay JL, Andriacchi TP. Longitudinal changes in knee gait mechanics between 2 and 8 years after anterior cruciate ligament reconstruction. J Orthop Res. 2018;36(5):1478-1486. doi:10.1002/jor.23770.
41. von Essen C, McCallum S, Barenius B, Eriksson K. Acute reconstruction results in less sick-leave days and as such fewer indirect costs to the individual and society compared to delayed reconstruction for ACL injuries. Knee Surgery, Sport Traumatol Arthrosc. February 2019. doi:10.1007/s00167-019-05397-3.
42. Failla MJ, Logerstedt DS, Grindem H, et al. Does Extended Preoperative Rehabilitation Influence Outcomes 2 Years After ACL Reconstruction? Am J Sports Med. 2016;44(10):2608-2614. doi:10.1177/0363546516652594.
43. Fees M, Decker T, Snyder-Mackler L, Axe MJ. Upper Extremity Weight-Training Modifications for the Injured Athlete. Am J Sports Med. 1998;26(5):732-742. doi:10.1177/03635465980260052301.
44. Feucht MJ, Cotic M, Saier T, et al. Patient expectations of primary and revision
80
anterior cruciate ligament reconstruction. Knee Surgery, Sport Traumatol Arthrosc. 2016;24(1):201-207. doi:10.1007/s00167-014-3364-z.
45. Filbay SR, Grindem H. Evidence-based recommendations for the management of anterior cruciate ligament (ACL) rupture. Best Pract Res Clin Rheumatol. 2019;33(1):33-47. doi:10.1016/j.berh.2019.01.018.
46. Filbay SR, Roos EM, Frobell RB, Roemer F, Ranstam J, Lohmander LS. Delaying ACL reconstruction and treating with exercise therapy alone may alter prognostic factors for 5-year outcome: an exploratory analysis of the KANON trial. Br J Sport Med. 2017;51:1622-1629. doi:10.1136/bjsports-2016-097124.
47. Fitzgerald GK, Axe MJ, Snyder-mackler L. A decision-making scheme for returning patients to high-level activity with nonoperative treatment after anterior cruciate ligament rupture. Knee Surg Sport Traumatol Arthrosc. 2000;8(2):76-82. doi:10.1007/s001670050190.
48. Fitzgerald GK, Axe MJ, Snyder-Mackler L. The Efficacy of Perturbation Training in Nonoperative Anterior Cruciate Ligament Rehabilitation Programs for Physically Active Individuals. Phys Ther. 2000;80(2):128-140. doi:10.1093/ptj/80.2.128.
49. Frobell RB, Roos HP, Roos EM, Roemer FW, Ranstam J, Lohmander LS. Treatment for acute anterior cruciate ligament tear: five year outcome of randomised trial. BMJ. 2013;346(jan24 1):f232-f232. doi:10.1136/bmj.f232.
50. Gardinier ES, Manal K, Buchanan TS, Snyder-Mackler L. Minimum detectable change for knee joint contact force estimates using an EMG-driven model. Gait Posture. 2013;38(4):1051-1053. doi:10.1016/j.gaitpost.2013.03.014.
51. Gokeler A, Benjaminse A, van Eck CF, Webster KE, Schot L, Otten E. Return of normal gait as an outcome measurement in acl reconstructed patients. A systematic review. Int J Sports Phys Ther. 2013;8(4):441-451. http://www.ncbi.nlm.nih.gov/pubmed/24175130. Accessed February 17, 2020.
52. Gokeler A, Benjaminse A, Hewett TE, et al. Feedback techniques to target functional deficits following anterior cruciate ligament reconstruction: implications for motor control and reduction of second injury risk. Sports Med. 2013;43(11):1065-1074. doi:10.1007/s40279-013-0095-0.
53. Gokeler A, Benjaminse A, Welling W, Alferink M, Eppinga P, Otten B. The effects of attentional focus on jump performance and knee joint kinematics in patients after ACL reconstruction. Phys Ther Sport. 2015;16(2):114-120.
81
https://www.sciencedirect.com/science/article/pii/S1466853X1400039X?via%3Dihub. Accessed October 25, 2018.
54. Gokeler A, Bisschop M, Benjaminse A, Myer GD, Eppinga P, Otten E. Quadriceps function following ACL reconstruction and rehabilitation: Implications for optimisation of current practices. Knee Surgery, Sport Traumatol Arthrosc. 2014;22(5). doi:10.1007/s00167-013-2577-x.
55. Grindem H, Eitzen I, Engebretsen L, Snyder-Mackler L, Risberg MA. Nonsurgical or Surgical Treatment of ACL Injuries: Knee Function, Sports Participation, and Knee Reinjury: The Delaware-Oslo ACL Cohort Study. J Bone Joint Surg Am. 2014;96(15):1233-1241. doi:10.2106/JBJS.M.01054.
56. Grindem H, Eitzen I, Engebretsen L, Snyder-Mackler L, Risberg MA. Nonsurgical or Surgical Treatment of ACL Injuries. J Bone Jt Surg. 2014;96(15):1233-1241. doi:10.2106/JBJS.M.01054.
57. Grindem H, Engebretsen L, Axe M, Snyder-Mackler L, Risberg MA. Activity and functional readiness, not age, are the critical factors for second anterior cruciate ligament injury — the Delaware-Oslo ACL cohort study. Br J Sports Med. February 2020:bjsports-2019-100623. doi:10.1136/bjsports-2019-100623.
58. Grindem H, Snyder-Mackler L, Moksnes H, Engebretsen L, Risberg MA. Simple decision rules can reduce reinjury risk by 84% after ACL reconstruction: the Delaware-Oslo ACL cohort study. Br J Sports Med. 2016. doi:10.1136/bjsports-2016-096031.
59. H Liang M, M Jette A. Measuring functional ability in chronic arthritis. a critical review. Arthritis Rheum. 1981;24(1):80-86. doi:10.1002/art.1780240113.
60. Hart HF, Culvenor AG, Collins NJ, et al. Knee kinematics and joint moments during gait following anterior cruciate ligament reconstruction: a systematic review and meta-analysis. Br J Sports Med. 2015;(0):1-17. doi:10.1136/bjsports-2015-094797.
61. Hart JM, Ko JWK, Konold T, Pietrosimione B. Sagittal plane knee joint moments following anterior cruciate ligament injury and reconstruction: A systematic review. Clin Biomech. 2010;25(4):277-283. doi:10.1016/j.clinbiomech.2009.12.004.
62. Hartigan E, Axe MJ, Snyder-Mackler L. Perturbation training prior to ACL reconstruction improves gait asymmetries in non-copers. J Orthop Res.
82
2009;27(6):724-729. doi:10.1002/jor.20754.
63. Hays RDRD, Reeve BBB. Measurement and Modeling of Health-Related Quality of Life. Int Encycl Public Heal. January 2008:241-252. https://www.sciencedirect.com/science/article/pii/B9780123739605003361. Accessed November 27, 2018.
64. Hefti F, Müller W, Jakob RP, Stäubli HU. Evaluation of knee ligament injuries with the IKDC form. Knee Surg Sports Traumatol Arthrosc. 1993;1(3-4):226-234. http://www.ncbi.nlm.nih.gov/pubmed/8536037. Accessed March 28, 2019.
65. Hellio Le Graverand MP, Vignon EP, Brandt KD, et al. Head-to-head comparison of the Lyon Schuss and fixed flexion radiographic techniques. Long-term reproducibility in normal knees and sensitivity to change in osteoarthritic knees. Ann Rheum Dis. 2008;67(11):1562-1566. doi:10.1136/ard.2007.077834.
66. Hewett TE, Myer GD, Ford KR, et al. Biomechanical Measures of Neuromuscular Control and Valgus Loading of the Knee Predict Anterior Cruciate Ligament Injury Risk in Female Athletes: A Prospective Study. Am J Sports Med. 2005;33(4):492-501. doi:10.1177/0363546504269591.
67. Hunter DJ, Le Graverand M-PH, Eckstein F. Radiologic markers of osteoarthritis progression. Curr Opin Rheumatol. 2009;21(2):110-117. doi:10.1097/BOR.0b013e3283235add.
68. Irrgang J, Snyder-Mackler L, Wainner RS, et al. Development of a Patient-Reported Measure of Function of the Knee. Vol 6058.; 1998. https://insights.ovid.com/pubmed?pmid=9730122. Accessed September 5, 2018.
69. Irrgang JJ, Anderson AF, Boland AL, et al. Development and validation of the International Knee Documentation Committee Subjective Knee Form. Am J Sports Med. 2001;29(5):600-613. doi:10.1177/03635465010290051301.
70. Irrgang JJ, Snyder-Mackler L, Wainner RS, Fu FH, Harner CD. Development of a Patient-Reported Measure of Function of the Knee. J Bone Jt Surg. 1998;80(8):1132-1145. https://insights.ovid.com/crossref?an=00004623-199808000-00006. Accessed March 29, 2019.
71. Kay J, Memon M, Marx RG, Peterson D, Simunovic N, Ayeni OR. Over 90 % of children and adolescents return to sport after anterior cruciate ligament reconstruction: a systematic review and meta-analysis. Knee Surgery, Sport
83
Traumatol Arthrosc. 2018;26(4):1019-1036. doi:10.1007/s00167-018-4830-9.
72. Kazis LE, Anderson JJ, Meenan RF. Effect sizes for interpreting changes in health status. Med Care. 1989;27(3 Suppl):S178-89. http://www.ncbi.nlm.nih.gov/pubmed/2646488. Accessed September 6, 2018.
73. Kellren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis. 1957;16(4):494-502. doi:10.1136/ARD.16.4.494.
74. Khan T, Alvand A, Prieto-Alhambra D, et al. ACL and meniscal injuries increase the risk of primary total knee replacement for osteoarthritis: a matched case-control study using the Clinical Practice Research Datalink (CPRD). Br J Sports Med. January 2018:bjsports-2017-097762. doi:10.1136/bjsports-2017-097762.
75. Kirshner B, Guyatt G. A methodological framework for assessing health indices. J Chronic Dis. 1985;38(1):27-36. doi:10.1016/0021-9681(85)90005-0.
76. Koo S, Andriacchi TP. A comparison of the influence of global functional loads vs. local contact anatomy on articular cartilage thickness at the knee. J Biomech. 2007;40(13):2961-2966. doi:10.1016/j.jbiomech.2007.02.005.
77. Kruse LMM, Gray B, Wright RWW. Rehabilitation after anterior cruciate ligament reconstruction: a systematic review. J Bone Jt Surg. 2012;94(19):1737-1748. doi:10.2106/JBJS.K.01246.
78. Kvist J, Ek A, Sporrstedt K, Good L. Fear of re-injury: a hindrance for returning to sports after anterior cruciate ligament reconstruction. Knee Surgery, Sport Traumatol Arthrosc. 2005;13(5):393-397. doi:10.1007/s00167-004-0591-8.
79. Kyritsis P, Bahr R, Landreau P, Miladi R, Witvrouw E. Likelihood of ACL graft rupture: not meeting six clinical discharge criteria before return to sport is associated with a four times greater risk of rupture. Br J Sports Med. 2016. doi:10.1136/bjsports-2015-095908.
80. LaBella CR, Hennrikus W, Hewett TE, Council on Sports Medicine and Fitness, and Section on Orthopaedics. Anterior Cruciate Ligament Injuries: Diagnosis, Treatment, and Prevention. Pediatrics. 2014;133(5):e1437-e1450. doi:10.1542/peds.2014-0623.
81. Leathers M, Merz A, Wong J, Scott T, Wang J, Hame S. Trends and Demographics in Anterior Cruciate Ligament Reconstruction in the United
84
States. J Knee Surg. 2015;28(05):390-394. doi:10.1055/s-0035-1544193.
82. Logerstedt D, Grindem H, Lynch A, et al. Single-legged hop tests as predictors of self-reported knee function after anterior cruciate ligament reconstruction: the Delaware-Oslo ACL cohort study. Am J Sports Med. 2012;40(10):2348-2356. doi:10.1177/0363546512457551.
83. Logerstedt D, Lynch A, Axe MJ, Snyder-Mackler L. Symmetry Restoration and Functional Recovery before and after Anterior Cruciate Ligament Reconstruction. Knee Surg Sport Traumatol Arthrosc. 2013;21(4):859-868. doi:10.1007/s00167-012-1929-2.
84. Lohmander LS, Englund PM, Dahl LL, Roos EM. The Long-term Consequence of Anterior Cruciate Ligament and Meniscus Injuries. Am J Sports Med. 2007;35(10):1756-1769. doi:10.1177/0363546507307396.
85. Lohmander LS, Östenberg A, Englund M, Roos H. High prevalence of knee osteoarthritis, pain, and functional limitations in female soccer players twelve years after anterior cruciate ligament injury. Arthritis Rheum. 2004;50(10):3145-3152. doi:10.1002/art.20589.
86. Losciale JM, Zdeb RM, Ledbetter L, Reiman MP, Sell TC. The Association Between Passing Return-to-Sport Criteria and Second Anterior Cruciate Ligament Injury Risk: A Systematic Review With Meta-Analysis. J Orthop Sport Phys Ther. November 2018:1-52. doi:10.2519/jospt.2019.8190.
87. Lynch AD, Logerstedt DS, Grindem H, et al. Consensus criteria for defining “successful outcome” after ACL injury and reconstruction: A Delaware-Oslo ACL cohort investigation. Br J Sports Med. 2015;49(5):335-342. doi:10.1136/bjsports-2013-092299.
88. Lysholm J, Tegner Y. Knee injury rating scales. Acta Orthop. 2007;78(4):445-453. doi:10.1080/17453670710014068.
89. Maletis GB, Inacio MCS, Desmond JL, Funahashi TT. Reconstruction of the anterior cruciate ligament. Bone Joint J. 2013;95-B(5):623-628. doi:10.1302/0301-620X.95B5.30872.
90. Maletis GB, Inacio MCS, Funahashi TT. Risk factors associated with revision and contralateral anterior cruciate ligament reconstructions in the Kaiser Permanente ACLR registry. Am J Sports Med. 2015;43(3):641-647. doi:10.1177/0363546514561745.

85
91. Manal K, Buchanan TS. An electromyogram-driven musculoskeletal model of the knee to predict in vivo joint contact forces during normal and novel gait patterns. J Biomech Eng. 2013;135(2):021014. doi:10.1115/1.4023457.
92. Marx RG. Knee rating scales. Arthrosc J Arthrosc Relat Surg. 2003;19(10):1103-1108. https://www.sciencedirect.com/science/article/pii/S0749806303009721?via%3Dihub. Accessed February 21, 2019.
93. Marx RG, Jones EC, Allen AA, et al. Reliability, Validity, and Responsiveness of Four Knee Outcome Scales for Athletic Patients.; 2001. https://insights.ovid.com/pubmed?pmid=11679594. Accessed September 5, 2018.
94. Marx RG, Stump TJ, Jones EC, Wickiewicz TL, Warren RF. Development and Evaluation of an Activity Rating Scale for Disorders of the Knee. Am J Sports Med. 2001;29(2):213-218. doi:10.1177/03635465010290021601.
95. McHorney CA, Tarlov AR. Individual-patient monitoring in clinical practice: are available health status surveys adequate? Qual Life Res. 1995;4(4):293-307. doi:10.1007/BF01593882.
96. van Meer BL, Oei EHG, Meuffels DE, et al. Degenerative Changes in the Knee 2 Years After Anterior Cruciate Ligament Rupture and Related Risk Factors. Am J Sports Med. 2016;44(6):1524-1533. doi:10.1177/0363546516631936.
97. Mehta VM, Paxton LW, Fornalski SX, Csintalan RP, Fithian DC. Reliability of the International Knee Documentation Committee Radiographic Grading System. Am J Sports Med. 2007;35(6):933-935. doi:10.1177/0363546507299742.
98. van Melick N, van Cingel REH, Brooijmans F, et al. Evidence-based clinical practice update: practice guidelines for anterior cruciate ligament rehabilitation based on a systematic review and multidisciplinary consensus. Br J Sports Med. 2016;50(24):1506-1515. doi:10.1136/bjsports-2015-095898.
99. Meuffels DE, Favejee MM, Vissers MM, Heijboer MP, Reijman M, Verhaar JAN. Ten year follow-up study comparing conservative versus operative treatment of anterior cruciate ligament ruptures. A matched-pair analysis of high level athletes. Br J Sports Med. 2009;43(5):347-351. doi:10.1136/bjsm.2008.049403.
100. Michael D. Lewek TLCMARLS. Dynamic Knee Stability After Anterior
86
Cruciate Ligament Rupture. Exerc Sport Sci Rev. 2003;31(4):195-200. https://insights.ovid.com/pubmed?pmid=14571959. Accessed December 11, 2018.
101. Myer GD, Ford KR, Palumbo JP, Hewett TE. Neuromuscular Training Improves Performance and Lower-Extremity Biomechanics in Female Athletes. J Strength Cond Res. 2005;19(1):51. doi:10.1519/13643.1.
102. Myklebust G, Bahr R, Bohr R, Bahr R. Return to play guidelines after anterior cruciate ligament surgery. Br J Sports Med. 2005;39(3):127-131. doi:10.1136/bjsm.2004.010900.
103. Nawasreh Z, Adams G, Pryzbylkowski O, Logerstedt D. INFLUENCE OF PATIENT DEMOGRAPHICS AND GRAFT TYPES ON ACL SECOND INJURY RATES IN IPSILATERAL VERSUS CONTRALATERAL KNEES: A SYSTEMATIC REVIEW AND META-ANALYSIS. Int J Sports Phys Ther. 2018;13(4):561-574. http://www.ncbi.nlm.nih.gov/pubmed/30140550. Accessed October 14, 2019.
104. NCAA. Mens Soccer Injuries. Sport Inj Fact Sheet. 2009.
105. NCAA. Women’s Soccer Injuries. Sport Inj Fact Sheet. 2009.
106. OARSI. Osteoarthritis : A Serious Disease. Osteoarthr Cartil. 2016.
107. Øiestad BE, Engebretsen L, Storheim K, Risberg MA. Knee osteoarthritis after anterior cruciate ligament injury: A systematic review. Am J Sports Med. 2009;37(7):1434-1443. doi:10.1177/0363546509338827.
108. Paterno M V., Rauh M, Thomas S, Hewett TE, Schmitt L. Current Return to Sport Criteria after ACL Reconstruction Fail to Identify Increased Risk of Second ACL Injury in Young Athletes. Orthop J Sport Med. 2018;6(7_suppl4):2325967118S0006. doi:10.1177/2325967118S00060.
109. Paterno M V., Rauh MJ, Schmitt LC, Ford KR, Hewett TE. Incidence of Contralateral and Ipsilateral Anterior Cruciate Ligament (ACL) Injury After Primary ACL Reconstruction and Return to Sport. Clin J Sport Med. 2012;22(2):116-121. doi:10.1097/JSM.0b013e318246ef9e.
110. Paterno M V., Schmitt LC, Ford KR, et al. Biomechanical Measures During Landing and Postural Stability Predict Second Anterior Cruciate Ligament Injury After Anterior Cruciate Ligament Reconstruction and Return to Sport. Am J Sports Med. 2010;38(10):1968-1978. doi:10.1177/0363546510376053.
87
111. Paterno M V, Ford KR, Myer GD, Heyl R, Hewett TE. Limb Asymmetries in Landing and Jumping 2 Years Following Anterior Cruciate Ligament Reconstruction. Clin J Sport Med. 2007;17(4):258-262. doi:10.1097/JSM.0b013e31804c77ea.
112. Paterno M V, Huang B, Thomas S, Hewett TE, Schmitt LC. Clinical Factors That Predict a Second ACL Injury After ACL Reconstruction and Return to Sport: Preliminary Development of a Clinical Decision Algorithm. Orthop J Sport Med. 2017;5(12). doi:10.1177/2325967117745279.
113. Paterno M V, Rauh MJ, Schmitt LC, Ford KR, Hewett TE. Incidence of second ACL injuries 2 years after primary ACL reconstruction and return to sport. Am J Sports Med. 2014;42(7):1567-1573. doi:10.1177/0363546514530088.
114. Persson A, Fjeldsgaard K, Gjertsen J-EE, et al. Increased risk of revision with hamstring tendon grafts compared with patellar tendon grafts after anterior cruciate ligament reconstruction: A study of 12,643 patients from the norwegian cruciate ligament registry, 2004-2012. Am J Sports Med. 2014;42(2):285-291. doi:10.1177/0363546513511419.
115. Rahr-Wagner L, Thillemann TM, Pedersen AB, Lind M. Comparison of Hamstring Tendon and Patellar Tendon Grafts in Anterior Cruciate Ligament Reconstruction in a Nationwide Population-Based Cohort Study. Am J Sports Med. 2014;42(2):278-284. doi:10.1177/0363546513509220.
116. Rambaud AJM, Ardern CL, Thoreux P, Regnaux JP, Edouard P. Criteria for return to running after anterior cruciate ligament reconstruction: A scoping review. Br J Sports Med. 2018;52(22):1437-1444. doi:10.1136/bjsports-2017-098602.
117. Renstrom P, Ljungqvist A, Arendt E, et al. Non-contact ACL injuries in female athletes: an International Olympic Committee current concepts statement. Br J Sports Med. 2008;42(6):394-412. doi:10.1136/bjsm.2008.048934.
118. Risberg MA, Holm I, Myklebust G, Engebretsen L. Neuromuscular Training Versus Strength Training During First 6 Months After Anterior Cruciate Ligament Reconstruction: A Randomized Clinical Trial. Phys Ther. 2007;87(6):737-750. doi:10.2522/ptj.20060041.
119. Risberg MA, Mørk M, Jenssen HK, Holm I. Design and Implementation of a Neuromuscular Training Program Following Anterior Cruciate Ligament Reconstruction. J Orthop Sport Phys Ther. 2001;31(11):620-631. doi:10.2519/jospt.2001.31.11.620.
88
120. Roewer BD, Di Stasi SL, Snyder-Mackler L. Quadriceps strength and weight acceptance strategies continue to improve two years after anterior cruciate ligament reconstruction. J Biomech. 2011;44(10):1948-1953. doi:10.1016/j.jbiomech.2011.04.037.
121. Rolstad S, Adler J, Rydén A. Response Burden and Questionnaire Length: Is Shorter Better? A Review and Meta-analysis. Value Heal. 2011;14(8):1101-1108. doi:10.1016/J.JVAL.2011.06.003.
122. Roos EM, Arden NK. Strategies for the prevention of knee osteoarthritis. Nat Rev Rheumatol. 2016;12(2):92-101. doi:10.1038/nrrheum.2015.135.
123. Roos EM, Roos HP, Lohmander LS, Ekdahl C, Beynnon BD. Knee Injury and Osteoarthritis Outcome Score (KOOS)—Development of a Self-Administered Outcome Measure. J Orthop Sport Phys Ther. 1998;28(2):88-96. doi:10.2519/jospt.1998.28.2.88.
124. Rudolph KS, Eastlack ME, Axe MJ, Snyder-Mackler L. 1998 Basmajian Student Award Paper: Movement patterns after anterior cruciate ligament injury: a comparison of patients who compensate well for the injury and those who require operative stabilization. J Electromyogr Kinesiol. 1998;8(6):349-362. doi:10.1016/S1050-6411(97)00042-4.
125. Samsa G, Edelman D, Rothman ML, Williams GR, Lipscomb J, Matchar D. Determining Clinically Important Differences in Health Status Measures. Pharmacoeconomics. 1999;15(2):141-155. doi:10.2165/00019053-199915020-00003.
126. Sanders TL, Maradit Kremers H, Bryan AJ, et al. Incidence of Anterior Cruciate Ligament Tears and Reconstruction. Am J Sports Med. 2016;44(6):1502-1507. doi:10.1177/0363546516629944.
127. Saxby DJ, Modenese L, Bryant AL, et al. Tibiofemoral contact forces during walking, running and sidestepping. Gait Posture. 2016;49:78-85. doi:10.1016/J.GAITPOST.2016.06.014.
128. Shakked R, Weinberg M, Capo J, Jazrawi L, Strauss E. Autograft Choice in Young Female Patients: Patella Tendon versus Hamstring. J Knee Surg. 2016;30(03):258-263. doi:10.1055/s-0036-1584561.
129. Shelbourne KD, Barnes AF, Gray T. Correlation of a Single Assessment Numeric Evaluation (SANE) Rating With Modified Cincinnati Knee Rating System and IKDC Subjective Total Scores for Patients After ACL

89
Reconstruction or Knee Arthroscopy. Am J Sports Med. 2012;40(11):2487-2491. doi:10.1177/0363546512458576.
130. Shelbourne KD, Gray T, Haro M. Incidence of subsequent injury to either knee within 5 years after anterior cruciate ligament reconstruction with patellar tendon autograft. Am J Sports Med. 2009;37(2):246-251. doi:10.1177/0363546508325665.
131. Shi DL, Wang Y Bin, Ai ZS. Effect of anterior cruciate ligament reconstruction on biomechanical features of knee in level walking: A meta-analysis. Chin Med J (Engl). 2010;123(21):3137-3142. doi:10.3760/cma.j.issn.0366-6999.2010.21.034.
132. Sloan JA, Aaronson N, Cappelleri JC, et al. Assessing the clinical significance of single items relative to summated scores. In: Mayo Clinic Proceedings. Vol 77. Elsevier Ltd; 2002:479-487. doi:10.4065/77.5.479.
133. Smith AH, Capin J, Zarzycki R, Snyder-Mackler L. Athletes With Bone-Patellar Tendon Bone Autograft for ACL Reconstruction Were Months Slower to Meet Rehabilitation Milestones and Return to Sport Criteria Than Athletes With Hamstring Tendon Autograft or Soft Tissue Allograft: Secondary Analysis From the ACL-SPORTS Trial. J Orthop Sport Phys Ther. November 2019:1-28. doi:10.2519/jospt.2020.9111.
134. Di Stasi S, Hartigan EH, Snyder-Mackler L. Sex-specific gait adaptations prior to and up to 6 months after anterior cruciate ligament reconstruction. J Orthop Sport Phys Ther. 2015;45(3):207-214. doi:10.2519/jospt.2015.5062.
135. Di Stasi SL, Logerstedt D, Gardinier ES, Snyder-Mackler L. Gait patterns differ between ACL-reconstructed athletes who pass return-to-sport criteria and those who fail. Am J Sports Med. 2013;41(6):1310-1318. doi:10.1177/0363546513482718.
136. Stratford PW, Binkley JM, Riddle DL. Health Status Measures: Strategies and Analytic Methods for Assessing Change Scores. Phys Ther. 1996;76(10):1109-1123.
137. Streiner DL, Norman GR, Cairney J. Oxford Medicine Online Health Measurement Scales : A practical guide to their development and use ( 5 ed .) Chapter : Selecting the items. 2019:1-27. doi:10.1093/med/9780199685219.001.0001.
138. Stucki G, Liang MH, Fossel AH, Katz JN. Relative responsiveness of
90
condition-specific and generic health status measures in degenerative lumbar spinal stenosis. J Clin Epidemiol. 1995;48(11):1369-1378. doi:10.1016/0895-4356(95)00054-2.
139. Sugimoto D, Myer GD, Bush HM, Klugman MF, Medina McKeon JM, Hewett TE. Compliance with neuromuscular training and anterior cruciate ligament injury risk reduction in female athletes: a meta-analysis. J Athl Train. 2012;47(6):714-723. doi:10.4085/1062-6050-47.6.10.
140. Sugimoto D, Myer GD, Foss KDB, Hewett TE. Dosage effects of neuromuscular training intervention to reduce anterior cruciate ligament injuries in female athletes: meta- and sub-group analyses. Sports Med. 2014;44(4):551-562. doi:10.1007/s40279-013-0135-9.
141. Sugimoto D, Myer GD, Foss KDB, Hewett TE. Specific exercise effects of preventive neuromuscular training intervention on anterior cruciate ligament injury risk reduction in young females: meta-analysis and subgroup analysis. Br J Sports Med. 2015;49(5):282-289. doi:10.1136/bjsports-2014-093461.
142. Swärd P, Kostogiannis I, Roos H. Risk factors for a contralateral anterior cruciate ligament injury. Knee Surgery, Sport Traumatol Arthrosc. 2010;18(3):277-291. doi:10.1007/s00167-009-1026-3.
143. Tegner Y, Lysholm J, Odensten M, Gillquist J. Evaluation of cruciate ligament injuries A review. Acta Orthop Scand. 1988;59(3):336-341. doi:10.3109/17453678809149379.
144. Uttl B. Measurement of individual differences: lessons from memory assessment in research and clinical practice. Psychol Sci. 2005;16(6):460-467. http://www.ncbi.nlm.nih.gov/pubmed/15943672. Accessed January 22, 2019.
145. Valier AR, Lam KC. Beyond the Basics of Clinical Outcomes Assessment: Selecting Appropriate Patient-Rated Outcomes Instruments for Patient Care. Athl Train Educ J. 2015;10(1):91-100. doi:10.4085/100191.
146. Wang D, Jones MH, Khair MM, Miniaci A. Patient-reported outcome measures for the knee. J Knee Surg. 2010;23(3):137-151. http://www.ncbi.nlm.nih.gov/pubmed/21329255. Accessed August 17, 2018.
147. Wang L, Zhang Z, McArdle JJ, Salthouse TA. Investigating Ceiling Effects in Longitudinal Data Analysis. Multivariate Behav Res. 2009;43(3):476-496. doi:10.1080/00273170802285941.
91
148. Webster KE, Feller JA. Exploring the High Reinjury Rate in Younger Patients Undergoing Anterior Cruciate Ligament Reconstruction. Am J Sports Med. 2016;44(11):2827-2832. doi:10.1177/0363546516651845.
149. Webster KE, Feller JA. Exploring the High Reinjury Rate in Younger Patients Undergoing Anterior Cruciate Ligament Reconstruction. Am J Sports Med. 2016;44(11):2827-2832. doi:10.1177/0363546516651845.
150. Webster KE, Feller JA, Fracs yz, Leigh WB, Richmond AK. Younger Patients Are at Increased Risk for Graft Rupture and Contralateral Injury After Anterior Cruciate Ligament Reconstruction. Am J Sports Med. 2014;42(3):641-647. doi:10.1177/0363546513517540.
151. Webster KE, Feller JA, Lambros C. Development and preliminary validation of a scale to measure the psychological impact of returning to sport following anterior cruciate ligament reconstruction surgery. Phys Ther Sport. 2008;9(1):9-15. doi:10.1016/J.PTSP.2007.09.003.
152. Wellsandt E, Gardinier ES, Manal K, Axe MJ, Buchanan TS, Snyder-Mackler L. Decreased Knee Joint Loading Associated With Early Knee Osteoarthritis After Anterior Cruciate Ligament Injury. Am J Sports Med. 2016;44(1):143-151. doi:10.1177/0363546515608475.
153. Wellsandt E, Gardinier ES, Manal K, Axe MJ, Buchanan TS, Snyder-Mackler L. Decreased Knee Joint Loading Associated with Early Knee Osteoarthritis after Anterior Cruciate Ligament Injury. Am J Sports Med. 2016;44(1):143-151. doi:10.1177/0363546515608475.
154. White K, Stasi SL Di, Smith AH, Snyder-mackler L. Anterior cruciate ligament- specialized training : a randomized control trial. BMC Musculoskelet Disord. 2013;14:1-10. doi:10.1186/1471-2474-14-108.
155. White K, Di Stasi SL, Smith AH, Snyder-Mackler L. Anterior cruciate ligament- specialized post-operative return-to-sports (ACL-SPORTS) training: a randomized control trial. BMC Musculoskelet Disord. 2013;14(1):108. doi:10.1186/1471-2474-14-108.
156. Wiggins AJ, Grandhi RK, Schneider DK, Stanfield D, Webster KE, Myer GD. Risk of Secondary Injury in Younger Athletes After Anterior Cruciate Ligament Reconstruction: A Systematic Review and Meta-analysis. Am J Sports Med. 2016;44(7):1861-1876. doi:10.1177/0363546515621554.
157. Williams GN, Taylor DC, Gangel TJ, et al. Comparison of the Single
92
Assessment Numeric Evaluation Method and the Lysholm Score. Clin Orthop Relat Res. 2000;373:184-192. doi:10.1097/00003086-200004000-00022.
158. Winby CR, Lloyd DG, Besier TF, Kirk TB. Muscle and external load contribution to knee joint contact loads during normal gait. J Biomech. 2009;42(14):2294-2300. doi:10.1016/J.JBIOMECH.2009.06.019.
159. Woby SR, Roach NK, Urmston M, Watson PJ. Psychometric properties of the TSK-11: A shortened version of the Tampa Scale for Kinesiophobia. Pain. 2005;117(1-2):137-144. doi:10.1016/j.pain.2005.05.029.
160. Yost KJ, Eton DT. Combining distribution- and anchor-based approaches to determine minimally important differences: The FACIT Experience. Eval Heal Prof. 2005;28(2):172-191. doi:10.1177/0163278705275340.
161. Zabala ME, Favre J, Scanlan SF, Donahue J, Andriacchi TP. Three-dimensional knee moments of ACL reconstructed and control subjects during gait, stair ascent, and stair descent. J Biomech. 2013;46(3):515-520. doi:10.1016/j.jbiomech.2012.10.010.
162. Zbrojkiewicz D, Vertullo C, Grayson JE. Increasing rates of anterior cruciate ligament reconstruction in young Australians, 2000-2015. Med J Aust. 2018;208(8):354-358. doi:10.5694/mja17.00974.
163. Zhang W, Moskowitz RW, Nuki G, et al. OARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines. Osteoarthr Cartil. 2008;16(2):137-162. doi:10.1016/j.joca.2007.12.013.
93
IRB DOCUMENTATION
Appendix A
94
95
LIST OF ABBREVIATIONS
ACL Anterior Cruciate Ligament ACLR Anterior Cruciate Ligament Reconstruction ACL-SPORTS Anterior Cruciate Ligament-Specialized Post-Operative Return
To Sports ADL Activities of Daily Living BMI Body Mass Index BPTB Bone-Patellar Tendon-Bone Graft BW Body Weight DOC Delaware-Oslo Cohort EMG Electromyography ES Effect Size GRS Global Rating Scale IKDC International Knee Documentation Committee IKDC-SKF International Knee Documentation Committee-Subjective Knee
Form JSW Joint Space Width Kg Kilogram KOOS Knee injury and Osteoarthritis Outcome Score KOS-ADLS Knee Outcome Survey-Activities of Daily Living Scale LSI Limb Symmetry Index MIC Minimal Important Change mm Millimeter OA Osteoarthritis PERT Perturbation PROMs Patient Reported Outcome Measures QI Quadriceps Index QOL Quality Of Life RTS Return To Sports SANE Single Assessment Numeric Evaluation SAPP Strength, Agility, Plyometric, and Performance SAPP+PERT Strength, Agility, Plyometric, and Performance + Perturbation TSK-11 Tampa Scale of Kinesiophobia
Appendix B
96
PROGNOSTIC FACTORS FOR PATIENT-REPORTED OUTCOME MEASURES AND PHYSICAL ACTIVITY TWO TO TEN YEARS AFTER
ACL INJURY OR RECONSTRUCTION: SYSTEMATIC REVIEW
Marie Pedersen, PT, MS1, Jessica L. Johnson, PT, DPT2, Hege Grindem, PT, PhD1, Karin Magnusson PT, PhD3,4, Lynn Snyder-Mackler, PT, ScD2,5, May Arna Risberg, PT, PhD1,6 1 Department of Sports Medicine, Norwegian School of Sport Sciences, Oslo, Norway 2 Graduate Program in Biomechanics and Movement Science, University of Delaware, Newark, DE, United States 3 Lund University, Faculty of Medicine, Department of Clinical Sciences Lund, Orthopaedics, Clinical Epidemiology Unit, Lund, Sweden 4 Diakonhjemmet Hospital, Department of Rheumatology, National Advisory Unit on Rehabilitation in Rheumatology, Oslo, Norway 5 Department of Physical Therapy, University of Delaware, Newark, DE, United States 6 Division of Orthopedic Surgery, Oslo University Hospital, Oslo, Norway Corresponding author: Marie Pedersen Department of Sports Medicine Norwegian School of Sport Sciences PB 4014 Ullevaal stadion 0806 Oslo Norway [email protected]
Appendix C
97
Word count (excluding title page, abstract, references, figures and tables): 4845. Funding: The project is funded by the National Institutes of Health through grant R37HD37985. Public trials registry: Our study protocol was published in the International Prospective Register of Systematic Reviews (PROSPERO: CRD42018095602) on June 7th 2018.
AKNOWLEDGEMENTS We would like to acknowledge librarians Anne Grethe Gabrielsen, Karianne
Hasledalen and Elin Hecker at the Norwegian School of Sport Sciences and Marte
Ødegaard at the University of Oslo for assistance and reviewing of systematic
searches.
98
ABSTRACT
OBJECTIVE: (1) Assess prognostic factors for patient-reported outcome measures
(PROMs) and physical activity (PA) two to ten years after anterior cruciate ligament
reconstruction (ACLR) or injury. (2) Assess differences in prognostic factors between
patients treated with ACLR and with rehabilitation alone.
DESIGN: Prognosis systematic review.
LITERATURE SEARCH: Systematic searches in PubMed, Web of science and
SPORTDiscus.
STUDY SELECTION CRITERIA: We selected prospective cohort studies and
randomised clinical trials that included adults/adolescents undergoing either ACLR or
rehabilitation alone after ACL rupture. Studies had to assess for a statistical
association between potential prognostic factors (factors related to patient
characteristics, injury or knee symptoms/function measured at baseline or within one
year) and outcomes (PROMS and PA).
DATA SYNTHESIS: Our search yielded 1008 references. Twenty studies met
inclusion criteria. Seven studies with low or moderate risk of bias remained for data
synthesis.
RESULTS: Concomitant meniscus and cartilage injuries were prognostic factors
with moderate certainty for worse PROMs two to ten years after ACLR, while BMI,
smoking and baseline PROMs were factors with very low certainty. Female sex and
worse baseline Marx Activity Rating Scale (Marx) were prognostic factors for worse
99
Marx two to ten years after ACLR with very low certainty. There was a lack of studies
on prognostic factors after rehabilitation alone.
CONCLUSION: Concomitant meniscus and cartilage injuries are prognostic factors
for worse long-term PROMs after ACLR. The certainty is low/very low for other
prognostic factors. We were unable to assess differences in prognostic factors between
treatment groups.
KEY WORDS: Prognosis, Ligament, Knee surgery, Sporting injuries
100
INTRODUCTION
Anterior cruciate ligament (ACL) injuries have serious negative long-term
consequences such as lower extremity dysfunction, low levels of physical activity
(PA), poor quality of life, and early development of knee osteoarthritis (OA) (1-7).
Resolving impairments and returning to sport are often the main short-term goals for
patients (1, 8). But as clinicians, we need to incorporate long-term consequences of
ACL injury into our patient education and allow them to inform our interventions
early after injury or reconstruction (9). Hence, high quality studies on prognostic
factors for important long-term outcomes such as patient reported outcome measures
(PROMs), levels of PA and OA are valuable.
A prognostic study can aim to predict the total individual risk given all available
information in a prediction model, or to estimate a population average causal effect of
an exposure or treatment on an outcome given adjustment for relevant confounders.
Both approaches may provide important information on prognostic factors, as a
prognostic factor can be either causally or non-causally related to an outcome variable
(10-12). Many systematic reviews have evaluated prognostic factors for developing
knee OA after ACL injury (5, 13-17). A few systematic reviews have reported
prognostic factors for long-term PROMs and level of PA (15, 16, 18-21), but most of
them are of poor quality due to lack of risk of bias assessments (15, 16, 18). Also,
patients treated with rehabilitation alone have not been included in these previous
systematic reviews.
101
Consequently, we need a high-quality systematic review on prognostic factors for
PROMs and level of PA two to ten years after ACL injury or ACLR, with an
appropriate and thorough risk of bias assessment. Such a study may provide
information about prognostic factors that can be targeted with early treatment, and can
thereby help to improve outcomes for patients with ACL injury.
Current evidence suggests similar clinical courses following rehabilitation alone and
ACLR (3, 22-26), but we do not know if prognostic factors differ in the two treatment
groups. There is great clinical interest to identify early prognostic factors associated
with better outcome after both ACLR and rehabilitation alone. This knowledge can
help inform treatment choices. No systematic review has previously addressed this
topic.
Therefore, the aims of our systematic review were (1) To assess prognostic factors for
patient-reported outcome measures (PROMs) and physical activity (PA) two to ten
years after anterior cruciate ligament reconstruction (ACLR) or injury. (2) To assess
differences in prognostic factors between patients treated with ACLR and with
rehabilitation alone.
METHODS
This systematic review was conducted in accordance with the Preferred Reporting
Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (27). Our
102
study protocol was published in the International Prospective Register of Systematic
Reviews (PROSPERO: CRD42018095602) on June 7th 2018.
Eligibility criteria
Studies were included using the following criteria: (1) Prospective cohort studies and
randomised clinical trials (RCT), that (2) report prognostic factors for PROMs or level
of PA, at (3) a mean of ≥ two and <10 years, in (4) adults and adolescents (mean
age > 13 years), (5) undergoing either ACLR or rehabilitation alone after complete
ACL rupture. (6) Studies had to assess the association between exposure and outcome
with regression analyses. Studies only on revision ACLR, knee dislocations, partial
tears or bilateral injury were excluded. We included studies where a subset of patients
had these conditions. Prognostic factors were defined as either patient characteristics
(all factors that describes a patient, eg age, sex, psychological factors), factors related
to the injury (eg concomitant injury) or knee symptoms and function (eg functional
performance, patient reported outcome measures) that were assessed ≤ one year after
injury or ACLR.
The following PROMs were selected; Knee injury and Osteoarthritis Outcome Score
(KOOS), International Knee Documentation Committee Subjective Knee Form
(IKDC-SKF) and Knee Outcome Survey Activities of Daily Living Scale (KOS-
ADLS). These PROMs were chosen based on their frequent use as stand-alone
PROMs for long-term outcomes during the last decade and because they have good
103
measurement properties (28-34). The KOOS consists of five subscales: pain, other
symptoms, function in daily living (ADL), function in sport and recreation (S/R), and
knee-related quality of life (QoL) (32). KOOS can be reported as individual subscales
or as KOOS4 which is an average score of four subscales (ADL excluded). The IKDC-
SKF measures symptoms, function and sports activity in patients with different types
of knee problems (34). The KOS-ADLS assesses the impact of symptoms on subjects'
ability to perform daily activities (28). All three questionnaires are scored from 0
(worst) to 100 (best). We included all outcomes that reflect type and level of PA,
including the three components defining physical activity: frequency, intensity and
duration (35) (eg objective measures such as accelerometers, patient-reported PA
questionnaires and return to sports). An example of a patient-reported outcome
measure of PA for ACL injured individuals is The Marx Activity Rating Scale (Marx).
Marx is a brief survey on the frequency of participation in sports involving running,
pivoting, cutting, and deceleration (36).
Data sources and searches
We systematically searched PubMed, Web of science and SPORTDiscus for articles
published from database inception to 20th September 2018. See search strategy for
PubMed in TABLE 1. Filters on “Humans” and “English language” were used and all
104
free text words/terms were searched on "Title/abstract". Relevant systematic reviews
were identified with the same search terms in PubMed. Reference lists from
systematic reviews and included studies were hand searched for relevant material to
supplement electronic database searches. To identify additional literature, the
following simplified search was performed in Google Scholar: "Anterior cruciate
ligament"|ACL Prognosis|"Prognostic factors"|Predict|Associations "Return to
sports"|Participation|"Activity level"|"Physical activity"|Tegner|Marx|KOOS
|IKDC|KOS "Prospective study"|"Observational study"|"Cohort study"|RCT”. The 100
first (and most relevant) results from Google Scholar were screened. The searches
were performed with assistance from and reviewed by librarians at the Norwegian
School of Sport Sciences and the University of Oslo.
Study selection and data extraction
Two independent researchers (MP and JLJ) screened for eligibility and extracted data
with customized data extraction forms. Covidence systematic review software (Veritas
Health Innovation, Melbourne, Australia, available at www.covidence.org) was used
to assist this process. Calibration exercises were performed to ensure consistency
between reviewers, but without testing agreement. Discrepancies were resolved by
discussion or a third reviewer (HG or MAR). We contacted study authors to resolve
uncertainties when necessary. Titles and abstracts were screened to identify potentially
relevant studies for full text eligibility assessment. The reasons for exclusion were
105
recorded. When several exclusion criteria were fulfilled, the first reason on a
predefined list was chosen.
Risk of bias assessment
Risk of bias was assessed with the Quality in Prognosis Study (QUIPS) risk of bias
tool (37). We chose this tool because it is developed specifically for the
methodological assessment of prognostic studies. QUIPS is a reliable tool for
systematically assessing risk of bias in the following six domains: study participation,
study attrition, prognostic factor measurement, outcome measurement, study
confounding and statistical analysis and reporting (37). Three independent reviewers
(MP, JLJ and KM) performed the scoring of the different domains. Our
operationalization of the QUIPS items is described in APPENDIX 1. For studies
where the objective was prediction and not etiology, the confounding domain was
classified as irrelevant (because the goal of a prediction model is to predict the total
individual risk given all information, for example independent of the covariates’
influence on each other) (11, 12). The overall risk of bias for each study was
classified: (1) low, if there was low risk of bias in all domains, (2) moderate, if there
was moderate risk of bias for ≥one domain and (3) high, if there was high risk of bias
for ≥one domain (38). For all domains, high risk of bias was defined as a level where
the results of the study should not be trusted, and/or it was impossible to interpret due
to research methodology and/or inadequate description of methodology. This was an
106
overall assessment and decision, hence, no study was classified as high risk of bias in
any domain based on only one question.
Data synthesis and analysis
Results from all included studies (n=20) are presented in APPENDIX 2 and 3. We
included only studies with low or moderate risk of bias in the data synthesis. The
purpose was to ensure conclusions and recommendations to clinicians and patients
were not based on results that should not be trusted, and to make the results easier to
interpret and, hence, easier to translate into practice. When data from the same patients
were used in publications on the same prognostic factors and outcomes at different
time points, we included the most recent publication. Results were presented
separately for the outcomes PROMs and level of PA and for patients undergoing
ACLR and rehabilitation alone. When possible, results from studies on each treatment
group were extracted separately. Results from adjusted analyses were preferred. It was
not possible to perform a meta-analysis due to methodological diversity in outcome
measures and follow-up time.
Quality of evidence for each prognostic factor was judged as high, moderate, low or
very low with the "Grading of Recommendations Assessment, Development and
Evaluation" (GRADE) approach. The GRADEpro software (39) was applied and
adjusted according to recommendations for prognostic factor research (40, 41).
107
RESULTS
Search results
A total of 974 references were identified through database searching. Additional 23
references were identified through bibliographies (n=2), Google Scholar (n=3) and
reference lists (n=18). After removing duplicates, 561 references remained. All were
screened for eligibility and 431 were ineligible due to objectives, outcome or follow-
up time. The remaining 130 articles were read in full text and 20 met all eligibility
criteria (FIGURE 1). Seventeen of the included studies were identified through the
systematic search, while three were identified through other sources. Due to more
recent publications on the same prognostic factors and outcomes, we excluded the
results on concomitant cartilage lesions, but not meniscus lesions from Røtterud et al.
(42) and all results from the study by Magnussen et al. (43) from 2016. Seven studies
with low or moderate risk of bias remained for data synthesis (42, 44-49).
Study characteristics
Characteristics of the included studies (n=20) are presented in TABLE 2. Most of the
cohort studies were based on data from the Multicenter Orthopedic Outcomes
Network (MOON) cohort (n= 8) (43, 47, 48, 50-54) and the Swedish and/or
Norwegian Knee Ligament Registries (SKLR/NKLR) (n= 5) (42, 44, 46, 49, 55). In
the included RCTs, both treatment groups were treated as one cohort for the
assessment of prognostic factors (45, 56-58). Three of the RCT publications were
based on the Knee Anterior Cruciate Ligament, Nonsurgical versus Surgical
108
Treatment (KANON) trial (45, 57, 58). The studies included median (Q1-Q3) 495
(121-2333) patients. Due to several publications on the same patients in the large
registry studies, it was challenging to estimate the total number of unique patients
included in this systematic review. Most studies included patients undergoing primary
ACLR only, and no study included only patients treated with rehabilitation alone.
Patients with substantial concomitant injuries (43, 45-47, 51, 53, 55-61) and/or
contralateral ACL injury (42, 46, 48, 49, 51-54, 56) were frequently excluded from the
included studies. The median age at inclusion was 26 years (range 18-27). The median
percentage of females was 44% (range 26-77%). Preinjury activity level was reported
in seven studies, where four (52, 59-61) included patients active in pivoting sports
preinjury and three (45, 57, 58) included patients with Tegner Activity Scale between
6 and 9 (6=recreational pivoting sports, 9=competitive sports).
Sixteen studies were etiological (42-47, 49-53, 56-59, 61) and four were predictive
(48, 54, 55, 60). Among the studies included in our data synthesis, only Spindler et al.
(48) was a predictive study.
Risk of bias
Risk of bias for the six QUIPS-domains and an overall rating is shown in TABLE 3.
Studies generally received poor scores on the domains "Study confounding" and
"Analysis and reporting" because they did not explicitly state what covariates were
109
adjusted for and why, did not separate between confounders, mediators and colliders
(and subsequently did not treat these covariates in accordance with existing rules for
adjustment), or had mixed predictive and etiological statistical approaches, which led
to uninterpretable results (10, 12, 62).
Data synthesis of studies with low or moderate risk of bias (n=7)
Prognostic factors for PROMs in patients treated with ACLR
Prognostic factors for PROMs in patients treated with ACLR were assessed in seven
studies from four cohorts. The IKDC-SKF was an outcome in two studies (47, 48) and
the KOOS was an outcome in seven studies (42, 44-49). The following 13 factors
were assessed by ≥1 study with low or moderate risk of bias: sex, age, body mass
index (BMI), smoking, ethnicity, type of sport, concomitant injury on medial or lateral
concomitant ligaments (MCL/LCL), meniscus or cartilage, hearing a pop at injury,
knee laxity, extension range of motion deficit and baseline PROMs. These factors
were measured at baseline, preoperatively or during ACLR.
Patient characteristics
One predictive study reported higher baseline BMI as a prognostic factor for worse
six-year IKDC-SKF and KOOS S/R outcomes and smoking for worse IKDC-SKF
(48). The same study found no association between higher BMI and KOOS QoL, or
between smoking and KOOS QoL and KOOS S/R.
110
There were no statistically significant association between the factors sex, age,
ethnicity and type of sport and the outcomes two- and six-year IKDC-SKF and KOOS
(44, 48).
Factors related to the injury
Concomitant meniscus injury was reported as a prognostic factor in some studies, but
not in others. Three studies (two etiological and one predictive) of three different
cohorts, found a statistically significant negative association between concomitant
meniscus injury and two-year patient-reported success (KOOS4 ≥80th percentile) (46)
and five- and six-year KOOS S/R and QoL outcomes (45, 48). The mean difference
between those with and without concomitant meniscus injury was 10-14.4 points for
KOOS S/R (45, 48) and 8.9 points for KOOS QoL (48). These values are of
questionable clinical relevance as the minimal perceptible clinical
improvement/minimal important difference are 8-12,1 points for KOOS S/R and 8-
18,3 points for KOOS QoL (63, 64). The same studies found, however, no statistically
significant associations between meniscus injury and the other KOOS subscales and
IKDC-SKF (45, 48). In one etiological study, concomitant meniscus injury was not a
prognostic factor for any two-year KOOS subscale (42).
Concomitant cartilage injury was assessed in four studies from four different cohorts
(45, 46, 48, 49). Two etiological studies found a statistically significant association
between concomitant cartilage lesions and five-year KOOS (all subscales),
111
particularly for the full-thickness lesions (45, 49). The mean difference between those
with and without concomitant cartilage injury was 8.1 points for KOOS S/R (49) and
8-12.3 points for KOOS QoL (45, 49). These values are also of questionable clinical
relevance (63, 64). The results of Filbay et al. (45) applied only for the five-year
KOOS QoL in patients with early (not delayed) ACLR. In a third etiological study, the
absence of concomitant cartilage injury predicted two-year patient-reported success
(as previously defined) while having a concomitant cartilage injury predicted failure
(KOOS4 ≤ 20th percentile) (46). One predictive study found no association between
concomitant cartilage injury and six-year KOOS S/R and QoL and IKDC-SKF (48).
There were no statistically significant associations between concomitant MCL/LCL
injury or hearing a pop at injury and the outcomes two-year patient-reported success or
failure (46) and six-year IKDC-SKF, KOOS QoL and KOOS S/R (48).
Knee symptoms/function
In one etiological study, baseline KOOS4 predicted five-year KOOS Symptoms,
KOOS S/R and KOOS QoL, but not KOOS pain, in patients with early ACLR (45). In
those with delayed ACLR, KOOS4 did not predict any of the five-year KOOS
subscales (45). A predictive study found conflicting results for the association between
baseline and five-year KOOS scores (48).
Preoperative knee laxity, defined as severely abnormal either Lachman, anterior
drawer or pivot-shift test, was assessed in one etiological study (47). There was a
statistically significant association between preoperative knee laxity and six-year
112
IKDC-SKF and KOOS QoL. The mean difference in IKDC-SKF and KOOS QoL
between those with and without preoperative laxity was small (2.3 and 2.7 points) and
therefore not clinically relevant (47).
There were no statistically significant associations between baseline Short-Form 36
and knee extension deficit >10 degrees and five-year KOOS outcomes (45).
GRADE evaluation for prognostic factors for PROMs in patients treated with ACLR
TABLE 4 shows the quality of evidence for each potential prognostic factor. The
evidence for concomitant meniscus and cartilage injuries was moderate, while for the
other factors it was low or very low. Our conclusions did not differ when all 20
eligible studies were included in a GRADE evaluation (APPENDIX 4)
Prognostic factors for PA in patients treated with ACLR
Prognostic factors for level of PA in patients treated with ACLR was assessed in two
studies from the same cohort, both using the Marx questionnaire as the outcome (47,
48). The following 13 factors were assessed by ≥1 study with moderate risk of bias:
sex, age, BMI, smoking, marital status, ethnicity, type of preinjury sport, baseline
PROMs, concomitant injury to the LCL/ MCL, meniscus or cartilage, knee laxity and
hearing a pop at injury (TABLE 2).
113
Patient characteristics
One predictive study assessed several demographic factors as possible prognostic
factors for six-year Marx (48). Female sex and worse baseline Marx were prognostic
factors for worse six-year Marx, while age, BMI, smoking, marital status, ethnicity
and type of preinjury sport were not (48).
Factors related to the injury
None of the following factors were prognostic factors for six-year Marx score:
concomitant MCL/LCL, meniscus or cartilage injuries and hearing a pop at injury
(48). One etiological study found a statistically significant association between
preoperative laxity (as previously defined) and six-year Marx (47). The mean
difference between those with and without preoperative laxity was small (0.5 points)
and not clinically relevant (47).
GRADE evaluation for prognostic factors for level of PA in patients treated with
ACLR
Quality of evidence was judged as very low for all the prognostic factors for level of
PA in patients treated with ACLR. Serious limitations in several GRADE domains
occurred because evidence for all factors was based on only one study with moderate
risk of bias.
114
Prognostic factors for PROMs and PA in patients treated with rehabilitation
alone
One etiological study assessed prognostic factors for five-year KOOS4 for a group of
patients treated with rehabilitation alone separately (45). None of the following factors
were prognostic factors: baseline cartilage defect, meniscus damage, osteochondral
lesion, extension deficit, SF-36 and KOOS4 (45). Quality of evidence was judged as
very low due to few studies. No study assessed prognostic factors for PA in this
patient group.
Differences in prognostic factors between treatment groups
One etiological study with low risk of bias assessed differences in prognostic factors
between those treated with rehabilitation alone and with ACLR (45). Based on
differences in prognostic factors for five-year KOOS4 between the treatment groups,
the authors suggested that patients with concomitant meniscus injury and those with
worse KOOS symptoms, S/R and QoL in the early phase may benefit most from
exercise therapy before choosing treatment (45).
DISCUSSION
Concomitant meniscus and cartilage injuries were, with moderate degree of certainty,
prognostic factors for worse PROMs two to ten years after ACLR. Smoking, BMI and
baseline PROMs were prognostic factors for two to ten-year PROMs with very low
certainty. For level of PA two to ten years after ACLR, we concluded with very low
certainty that female sex and worse baseline Marx were prognostic factors for worse
115
long-term Marx. The other factors assessed in this systematic review were not
associated with the outcomes. No studies included only patients treated with
rehabilitation alone. One study assessed differences in prognostic factors between
patients treated with rehabilitation alone and with ACLR. They suggested that patients
with certain concomitant injuries and lower KOOS scores in the acute phase may
benefit most from an initial non-surgical treatment choice, but further research on the
topic is needed to draw conclusions. Hence, we could not answer the second aim of
this systematic review.
Comparison with other studies
To our knowledge, the current study is the first systematic review to assess prognostic
factors for PROMs and level of PA after ACL injury both in patients treated with
ACLR and with rehabilitation alone. Although the paucity of studies on patients
treated with rehabilitation alone made it impossible to answer our review questions
regarding prognostic factors for PROMs and level of PAs for this treatment group, or
to assess differences in prognostic factors between treatment groups. We used a high-
quality search strategy, a well-suited tool for risk of bias assessment and included only
studies with low or moderate risk of bias in the data synthesis which ensured that
conclusions and recommendations to clinicians and patients were not based on results
that should not be trusted.
116
Our results highlighted the importance of risk of bias assessments in systematic
reviews as 12 of 20 included studies (60%) were rated as having high risk of bias. Bias
was suspected especially in the domains "Study confounding" and "Statistical analysis
and reporting". Lack of clarity in aims and methods about whether studies were
predictive or etiological was a recurring limitation. Effect estimates calculated from
one model, often a prediction model, which is presented in one table may give a wrong
interpretation because the underlying associations between covariates are not taken
into account (table 2 fallacy) (10). Even when study aims were clearly of an
etiological nature, because of a statistically driven rather than theoretically driven
approach, it was unclear in many of the papers if the estimate of the effect was
adjusted for all relevant confounders and whether it should have been interpreted as a
total or direct causal effect (11). Epidemiological research methodology has developed
over time, and the distinction between explanatory and predictive aims was less clear
at the time when the included studies were performed. As an example, our systematic
review included relatively recent articles (median publication year 2015, range 2005 to
2018), while studies excluded due to statistical analysis had a median publishing year
of 2007 (range 1999-2018).
Because of the systematic risk of bias assessment and inclusion of only studies with
low or moderate risk of bias in the data synthesis, our study could not reproduce some
of the conclusions of previous systematic reviews. For example, de Valk et al. (19)
concluded that male patients and patients aged <30 years had better functional
117
outcomes after ACLR and that quadriceps weakness and range-of-motion deficits have
a negative effect on outcomes.
Also, the systematic review of Everhart et al. (21) drew conclusions based on studies
that found an association between psychological factors and the outcomes KOOS and
return to sport (65-67). These studies were not included in our review due to a longer
follow-up time and exclusion of studies with inappropriate statistical analysis.
We found that concomitant meniscus and cartilage injuries were negative prognostic
factors for outcomes (PROMs) which is supported by two previous systematic reviews
(16, 18). We also found similar results as Tan et al. (15) that there were no sex
differences in IKDC-SKF and KOOS after ACLR, while women had worse Tegner
scores and return to sport rates.
Limitations
As significant findings from observational studies are more likely to be published (68),
publication bias may be a serious limitation in our GRADE evidence profile, and
limits the ability to draw conclusions. We found no information about published study
protocols for the included studies, limiting our ability to assess this factor.
An important limitation in the literature was the likely between-study overlap of
patients within the different publications from the MOON cohort and the
SKLR/NKLR. This overlap can possibly have led to a correlation between study
118
results that we could not account for. To minimize this problem, we only included the
most recent publication of data from the same patients and on the same prognostic
factors. Further, our strict inclusion criteria might have led us to miss high quality
research where other PROMs than IKDC-SKF, KOOS and KOS-ADLS were used,
such as Lysholm, ACL Return to Sport after Injury scale (ACL-RSI) and Short Form-
36 (SF-36). The included studies did not differentiate between types of meniscus
injuries, and we therefore lack knowledge on the prognosis after different injury types
(eg. dislocated bucket-handle tears versus stable, horizontal tears).
It is also important to bear in mind that the etiological and predictive studies in our
review should be interpreted differently. From the one prediction study in our data
synthesis (48), a prognostic factor cannot be interpreted as independent from the other
prognostic factors that are included in the prediction model, because the total risk
given all included prognostic factors is estimated (12).
Our results apply to individuals with first time complete unilateral ACL-injury, not
including knee dislocations. The prognostic factors are also only applicable to the
outcomes PROMs and level of PAs ≥ two and <10 years after ACLR. Important
outcomes such as psychological, overall health or quality of life outcomes was not
assessed in our study.
Implications for clinical practice
119
Our work has important implications for future clinical practice. When planning future
physical activities and discussing patient expectations, it is useful for both patients,
physical therapists, orthopaedic surgeons and athletic trainers to be aware that
concomitant meniscus or cartilage injuries may lead to worse knee function two to ten
years after ACLR. As concomitant meniscus injuries are also the most frequently
reported prognostic factor for knee OA after ACL injury (5, 13), these patients should
be informed about preventive measures for knee OA such as optimal knee extensor
muscle strength and maintaining a healthy body weight (69-75). Although with very
low certainty, higher BMI was a prognostic factor for worse PROMs after ACLR. Due
to the relation to both knee function and development of knee OA, BMI as a
prognostic factor is important and needs to be incorporated in the early patient
education. We also found that smoking is a negative prognostic factor for PROMs. As
this factor is modifiable, patients should be informed that avoiding smoking might
contribute to better long-term outcomes.
Implications for future research on prognostic factors after ACL injury and
ACLR
The current study has several implications for future research. Future studies should
better clarify whether their aims and methods are mainly predictive or etiological. If
the aim is etiological, they should carefully state their hypothesis with background and
run an informed causal effect analysis, ensuring that rules for adjustment for different
120
types of covariates (confounders, mediators and colliders) are followed (11, 76). If the
aim is predictive, studies should systematically build a prediction model based on all
available predictors and study the model’s discriminative ability and calibration and
subsequently internally and externally validate findings (77, 78). Pre-registration of
study protocols for observational studies on prognostic factors might enable
researchers to assess if selective reporting and publication bias occur within this field.
Future high-quality prognosis studies should include patients treated with
rehabilitation alone. This patient group is important as it represents between 26% and
77% of the ACL-injured population (79-81). New studies should also compare
prognostic factors between patients treated with rehabilitation alone and with ACLR in
order to help clinicians determine who will have the best prognosis with ACLR and
who will succeed with rehabilitation alone.
Our systematic review also uncovered a lack of studies on level of PAs long-term after
ACL injury. Most studies had high risk of bias and the study outcomes were only
activity rating scale (Marx) and the prevalence of return to sport, neither of which are
fully in line with the most common definition of level of PA (35) as they only measure
participation in specific type of sports. Future studies should therefore include more
general level of PA as outcomes (eg accelerometery, International Physical Activity
Questionnaire).
121
Future studies should also assess modifiable prognostic factors which can be targeted
in early rehabilitation, such as muscle strength, range of motion and hop performance.
CONCLUSION
Concomitant meniscus and cartilage injuries were prognostic factors for worse
PROMs two to ten years after ACLR. In addition, prognostic factors with very low
certainty included BMI, smoking and baseline PROMs. Marx score was the only
outcome measure used for physical activity. Female sex and worse baseline Marx
score were prognostic factors with very low certainty for worse Marx score two to ten
years after ACLR. A high proportion of the included studies had a high risk of bias.
Due to a lack of studies on prognostic factors in patients treated with rehabilitation
alone, we were unable to assess differences in prognostic factors between treatment
groups.
KEY POINTS
FINDINGS: We have moderate confidence that concomitant meniscus and cartilage
injuries are prognostic factors for worse long-term PROMs after ACLR. The certainty
is low/very low for other prognostic factors.
IMPLICATIONS: When planning future activities and discussing patient
expectations, it is useful for both patients, physical therapists, orthopaedic surgeons
122
and athletic trainers to consider that concomitant meniscus or cartilage injuries may
lead to worse knee function two to ten years after ACLR.
CAUTION: A large proportion (60%) of included studies in this systematic review
had high risk of bias and there is a lack of studies on prognostic factors in patients
treated with rehabilitation alone.
123
References
1. Ardern CL, Taylor NF, Feller JA, Webster KE. Fifty-five per cent return to competitive sport following anterior cruciate ligament reconstruction surgery: an updated systematic review and meta-analysis including aspects of physical functioning and contextual factors. British journal of sports medicine. 2014;48(21):1543-52. 2. Filbay SR, Ackerman IN, Russell TG, Macri EM, Crossley KM. Health-related quality of life after anterior cruciate ligament reconstruction: a systematic review. The American journal of sports medicine. 2014;42(5):1247-55. 3. Grindem H, Eitzen I, Engebretsen L, Snyder-Mackler L, Risberg MA. Nonsurgical or Surgical Treatment of ACL Injuries: Knee Function, Sports Participation, and Knee Reinjury: The Delaware-Oslo ACL Cohort Study. The Journal of bone and joint surgery American volume. 2014;96(15):1233-41. 4. Moksnes H, Risberg MA. Performance-based functional evaluation of non-operative and operative treatment after anterior cruciate ligament injury. Scandinavian journal of medicine & science in sports. 2009;19(3):345-55. 5. Oiestad BE, Engebretsen L, Storheim K, Risberg MA. Knee osteoarthritis after anterior cruciate ligament injury: a systematic review. The American journal of sports medicine. 2009;37(7):1434-43. 6. Culvenor AG, Collins NJ, Guermazi A, Cook JL, Vicenzino B, Khan KM, et al. Early knee osteoarthritis is evident one year following anterior cruciate ligament reconstruction: a magnetic resonance imaging evaluation. Arthritis & rheumatology (Hoboken, NJ). 2015;67(4):946-55. 7. Ajuied A, Wong F, Smith C, Norris M, Earnshaw P, Back D, et al. Anterior cruciate ligament injury and radiologic progression of knee osteoarthritis: a systematic review and meta-analysis. The American journal of sports medicine. 2014;42(9):2242-52. 8. Ardern CL, Osterberg A, Sonesson S, Gauffin H, Webster KE, Kvist J. Satisfaction With Knee Function After Primary Anterior Cruciate Ligament Reconstruction Is Associated With Self-Efficacy, Quality of Life, and Returning to the Preinjury Physical Activity. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2016;32(8):1631-8.e3. 9. Risberg MA, Grindem H, Oiestad BE. We Need to Implement Current Evidence in Early Rehabilitation Programs to Improve Long-Term Outcome After Anterior Cruciate Ligament Injury. The Journal of orthopaedic and sports physical therapy. 2016;46(9):710-3. 10. Westreich D, Greenland S. The table 2 fallacy: presenting and interpreting confounder and modifier coefficients. American journal of epidemiology. 2013;177(4):292-8. 11. Hernan MA, Robins JM. Estimating causal effects from epidemiological data. Journal of epidemiology and community health. 2006;60(7):578-86.
124
12. Shmueli G. To Explain or To Predict? Statistical Science. 2010;25(3):289-310. 13. van Meer BL, Meuffels DE, van Eijsden WA, Verhaar JA, Bierma-Zeinstra SM, Reijman M. Which determinants predict tibiofemoral and patellofemoral osteoarthritis after anterior cruciate ligament injury? A systematic review. British journal of sports medicine. 2015;49(15):975-83. 14. Magnussen RA, Mansour AA, Carey JL, Spindler KP. Meniscus status at anterior cruciate ligament reconstruction associated with radiographic signs of osteoarthritis at 5- to 10-year follow-up: a systematic review. The journal of knee surgery. 2009;22(4):347-57. 15. Tan SH, Lau BP, Khin LW, Lingaraj K. The Importance of Patient Sex in the Outcomes of Anterior Cruciate Ligament Reconstructions: A Systematic Review and Meta-analysis. The American journal of sports medicine. 2016;44(1):242-54. 16. Magnussen RA, Spindler KP. The effect of patient and injury factors on long-term outcome after anterior cruciate ligament reconstruction. Current orthopaedic practice. 2011;22(1):90-103. 17. Van Ginckel A, Verdonk P, Witvrouw E. Cartilage adaptation after anterior cruciate ligament injury and reconstruction: implications for clinical management and research? A systematic review of longitudinal MRI studies. Osteoarthritis and cartilage. 2013;21(8):1009-24. 18. Magnussen RA, Verlage M, Flanigan DC, Kaeding CC, Spindler KP. Patient-Reported Outcomes and Their Predictors at Minimum 10 Years After Anterior Cruciate Ligament Reconstruction: A Systematic Review of Prospectively Collected Data. Orthopaedic journal of sports medicine. 2015;3(3):2325967115573706. 19. de Valk EJ, Moen MH, Winters M, Bakker EW, Tamminga R, van der Hoeven H. Preoperative patient and injury factors of successful rehabilitation after anterior cruciate ligament reconstruction with single-bundle techniques. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2013;29(11):1879-95. 20. An VV, Scholes C, Mhaskar VA, Hadden W, Parker D. Limitations in predicting outcome following primary ACL reconstruction with single-bundle hamstring autograft - A systematic review. Knee. 2017;24(2):170-8. 21. Everhart JS, Best TM, Flanigan DC. Psychological predictors of anterior cruciate ligament reconstruction outcomes: a systematic review. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA. 2015;23(3):752-62. 22. Grindem H, Eitzen I, Moksnes H, Snyder-Mackler L, Risberg MA. A pair-matched comparison of return to pivoting sports at 1 year in anterior cruciate ligament-injured patients after a nonoperative versus an operative treatment course. The American journal of sports medicine. 2012;40(11):2509-16. 23. Frobell RB, Roos HP, Roos EM, Roemer FW, Ranstam J, Lohmander LS. Treatment for acute anterior cruciate ligament tear: five year outcome of randomised trial. British journal of sports medicine. 2015;49(10):700.
125
24. Frobell RB, Roos EM, Roos HP, Ranstam J, Lohmander LS. A randomized trial of treatment for acute anterior cruciate ligament tears. The New England journal of medicine. 2010;363(4):331-42. 25. Meuffels DE, Favejee MM, Vissers MM, Heijboer MP, Reijman M, Verhaar JA. Ten year follow-up study comparing conservative versus operative treatment of anterior cruciate ligament ruptures. A matched-pair analysis of high level athletes. British journal of sports medicine. 2009;43(5):347-51. 26. Ageberg E, Thomee R, Neeter C, Silbernagel KG, Roos EM. Muscle strength and functional performance in patients with anterior cruciate ligament injury treated with training and surgical reconstruction or training only: a two to five-year followup. Arthritis Rheum. 2008;59(12):1773-9. 27. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ (Clinical research ed). 2009;339:b2535. 28. Irrgang JJ, Snyder-Mackler L, Wainner RS, Fu FH, Harner CD. Development of a patient-reported measure of function of the knee. The Journal of bone and joint surgery American volume. 1998;80(8):1132-45. 29. Irrgang JJ, Anderson AF, Boland AL, Harner CD, Neyret P, Richmond JC, et al. Responsiveness of the International Knee Documentation Committee Subjective Knee Form. The American journal of sports medicine. 2006;34(10):1567-73. 30. van Meer BL, Meuffels DE, Vissers MM, Bierma-Zeinstra SM, Verhaar JA, Terwee CB, et al. Knee injury and Osteoarthritis Outcome Score or International Knee Documentation Committee Subjective Knee Form: which questionnaire is most useful to monitor patients with an anterior cruciate ligament rupture in the short term? Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2013;29(4):701-15. 31. Anderson AF, Irrgang JJ, Kocher MS, Mann BJ, Harrast JJ. The International Knee Documentation Committee Subjective Knee Evaluation Form: normative data. The American journal of sports medicine. 2006;34(1):128-35. 32. Roos EM, Roos HP, Lohmander LS, Ekdahl C, Beynnon BD. Knee Injury and Osteoarthritis Outcome Score (KOOS)--development of a self-administered outcome measure. The Journal of orthopaedic and sports physical therapy. 1998;28(2):88-96. 33. Collins NJ, Misra D, Felson DT, Crossley KM, Roos EM. Measures of knee function: International Knee Documentation Committee (IKDC) Subjective Knee Evaluation Form, Knee Injury and Osteoarthritis Outcome Score (KOOS), Knee Injury and Osteoarthritis Outcome Score Physical Function Short Form (KOOS-PS), Knee Outcome Survey Activities of Daily Living Scale (KOS-ADL), Lysholm Knee Scoring Scale, Oxford Knee Score (OKS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), Activity Rating Scale (ARS), and Tegner Activity Score (TAS). Arthritis care & research. 2011;63(S11):S208-S28.
126
34. Irrgang JJ, Anderson AF, Boland AL, Harner CD, Kurosaka M, Neyret P, et al. Development and validation of the international knee documentation committee subjective knee form. The American journal of sports medicine. 2001;29(5):600-13. 35. Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public health reports (Washington, DC : 1974). 1985;100(2):126-31. 36. Marx RG, Stump TJ, Jones EC, Wickiewicz TL, Warren RF. Development and evaluation of an activity rating scale for disorders of the knee. The American journal of sports medicine. 2001;29(2):213-8. 37. Hayden JA, van der Windt DA, Cartwright JL, Cote P, Bombardier C. Assessing bias in studies of prognostic factors. Annals of internal medicine. 2013;158(4):280-6. 38. Higgins J, Green Se. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Table 8.7.a. 2011 [updated 2018.11.16. Available from: www.handbook.cochrane.org. 39. GRADEpro GDT: GRADEpro Guideline Development Tool [Software]. McMaster University dbEP, Inc.). Available from gradepro.org. [ 40. Iorio A, Spencer FA, Falavigna M, Alba C, Lang E, Burnand B, et al. Use of GRADE for assessment of evidence about prognosis: rating confidence in estimates of event rates in broad categories of patients. BMJ (Clinical research ed). 2015;350:h870. 41. Huguet A, Hayden JA, Stinson J, McGrath PJ, Chambers CT, Tougas ME, et al. Judging the quality of evidence in reviews of prognostic factor research: adapting the GRADE framework. Systematic Reviews. 2013;2(1):71. 42. Røtterud JH, Sivertsen EA, Forssblad M, Engebretsen L, Årøen A. Effect of Meniscal and Focal Cartilage Lesions on Patient-Reported Outcome After Anterior Cruciate Ligament Reconstruction: A Nationwide Cohort Study From Norway and Sweden of 8476 Patients With 2-Year Follow-up. American Journal of Sports Medicine. 2013;41(3):535-43. 43. Magnussen RA, Reinke EK, Huston LJ, Hewett TE, Spindler KP. Effect of High-Grade Preoperative Knee Laxity on Anterior Cruciate Ligament Reconstruction Outcomes. The American journal of sports medicine. 2016;44(12):3077-82. 44. Ageberg E, Forssblad M, Herbertsson P, Roos EM. Sex differences in patient-reported outcomes after anterior cruciate ligament reconstruction: data from the Swedish knee ligament register. The American journal of sports medicine. 2010;38(7):1334-42. 45. Filbay SR, Roos EM, Frobell RB, Roemer F, Ranstam J, Lohmander LS. Delaying ACL reconstruction and treating with exercise therapy alone may alter prognostic factors for 5-year outcome: an exploratory analysis of the KANON trial. British journal of sports medicine. 2017;51(22):1622-9. 46. Hamrin Senorski E, Alentorn-Geli E, Musahl V, Fu F, Krupic F, Desai N, et al. Increased odds of patient-reported success at 2 years after anterior cruciate ligament reconstruction in patients without cartilage lesions: a cohort study from the Swedish
127
National Knee Ligament Register. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA. 2018;26(4):1086-95. 47. Magnussen RA, Reinke EK, Huston LJ, Hewett TE, Spindler KP, Amendola A, et al. Effect of High-Grade Preoperative Knee Laxity on 6-Year Anterior Cruciate Ligament Reconstruction Outcomes. The American journal of sports medicine. 2018:363546518793881. 48. Spindler KP, Huston LJ, Wright RW, Kaeding CC, Marx RG, Amendola A, et al. The prognosis and predictors of sports function and activity at minimum 6 years after anterior cruciate ligament reconstruction: a population cohort study. The American journal of sports medicine. 2011;39(2):348-59. 49. Ulstein S, Aroen A, Engebretsen L, Forssblad M, Lygre SHL, Rotterud JH. Effect of Concomitant Cartilage Lesions on Patient-Reported Outcomes After Anterior Cruciate Ligament Reconstruction A Nationwide Cohort Study From Norway and Sweden of 8470 Patients With 5-Year Follow-up. Orthopaedic journal of sports medicine. 2018;6(7). 50. Brophy RH, Huston LJ, Wright RW, Nwosu SK, Kaeding CC, Parker RD, et al. Outcomes of ACL Reconstruction in Patients with Diabetes. Medicine and science in sports and exercise. 2016;48(6):969-73. 51. Cox CL, Huston LJ, Dunn WR, Reinke EK, Nwosu SK, Parker RD, et al. Are articular cartilage lesions and meniscus tears predictive of IKDC, KOOS, and Marx activity level outcomes after anterior cruciate ligament reconstruction? A 6-year multicenter cohort study. The American journal of sports medicine. 2014;42(5):1058-67. 52. Dunn WR, Spindler KP. Predictors of activity level 2 years after anterior cruciate ligament reconstruction (ACLR): a Multicenter Orthopaedic Outcomes Network (MOON) ACLR cohort study. The American journal of sports medicine. 2010;38(10):2040-50. 53. Spindler KP, Warren TA, Callison JC, Jr., Secic M, Fleisch SB, Wright RW. Clinical outcome at a minimum of five years after reconstruction of the anterior cruciate ligament. The Journal of bone and joint surgery American volume. 2005;87(8):1673-9. 54. Wasserstein D, Huston LJ, Nwosu S, Kaeding CC, Parker RD, Wright RW, et al. KOOS pain as a marker for significant knee pain two and six years after primary ACL reconstruction: a Multicenter Orthopaedic Outcomes Network (MOON) prospective longitudinal cohort study. Osteoarthritis and cartilage. 2015;23(10):1674-84. 55. Barenius B, Forssblad M, Engstrom B, Eriksson K. Functional recovery after anterior cruciate ligament reconstruction, a study of health-related quality of life based on the Swedish National Knee Ligament Register. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA. 2013;21(4):914-27. 56. Sasaki S, Tsuda E, Hiraga Y, Yamamoto Y, Maeda S, Sasaki E, et al. Prospective Randomized Study of Objective and Subjective Clinical Results Between
128
Double-Bundle and Single-Bundle Anterior Cruciate Ligament Reconstruction. The American journal of sports medicine. 2016;44(4):855-64. 57. Ericsson YB, Roos EM, Frobell RB. Lower extremity performance following ACL rehabilitation in the KANON-trial: impact of reconstruction and predictive value at 2 and 5 years. British journal of sports medicine. 2013;47(15):980-5. 58. Roessler KK, Andersen TE, Lohmander S, Roos EM. Motives for sports participation as predictions of self-reported outcomes after anterior cruciate ligament injury of the knee. Scandinavian Journal of Medicine & Science in Sports. 2015;25(3):435-40. 59. Ithurburn MP, Paterno MV, Ford KR, Hewett TE, Schmitt LC. Young Athletes After Anterior Cruciate Ligament Reconstruction With Single-Leg Landing Asymmetries at the Time of Return to Sport Demonstrate Decreased Knee Function 2 Years Later. The American journal of sports medicine. 2017;45(11):2604-13. 60. Nawasreh Z, Logerstedt D, Cummer K, Axe M, Risberg MA, Snyder-Mackler L. Functional performance 6 months after ACL reconstruction can predict return to participation in the same preinjury activity level 12 and 24 months after surgery. British journal of sports medicine. 2018;52(6):375. 61. Sonnery-Cottet B, Saithna A, Cavalier M, Kajetanek C, Temponi EF, Daggett M, et al. Anterolateral Ligament Reconstruction Is Associated With Significantly Reduced ACL Graft Rupture Rates at a Minimum Follow-up of 2 Years: A Prospective Comparative Study of 502 Patients From the SANTI Study Group. The American journal of sports medicine. 2017;45(7):1547-57. 62. Hernán M, Robins J. Causal Inference: Boca Raton: Chapman & Hall/CRC, forthcoming; 2019. 63. Ingelsrud LH, Terwee CB, Terluin B, Granan LP, Engebretsen L, Mills KAG, et al. Meaningful Change Scores in the Knee Injury and Osteoarthritis Outcome Score in Patients Undergoing Anterior Cruciate Ligament Reconstruction. The American journal of sports medicine. 2018;46(5):1120-8. 64. Roos EM, Lohmander LS. The Knee injury and Osteoarthritis Outcome Score (KOOS): from joint injury to osteoarthritis. Health and quality of life outcomes. 2003;1:64. 65. Swirtun LR, Renstrom P. Factors affecting outcome after anterior cruciate ligament injury: a prospective study with a six-year follow-up. Scandinavian journal of medicine & science in sports. 2008;18(3):318-24. 66. Gobbi A, Francisco R. Factors affecting return to sports after anterior cruciate ligament reconstruction with patellar tendon and hamstring graft: a prospective clinical investigation. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA. 2006;14(10):1021-8. 67. Thomee P, Wahrborg P, Borjesson M, Thomee R, Eriksson BI, Karlsson J. Self-efficacy of knee function as a pre-operative predictor of outcome 1 year after anterior cruciate ligament reconstruction. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA. 2008;16(2):118-27.
129
68. Easterbrook PJ, Berlin JA, Gopalan R, Matthews DR. Publication bias in clinical research. Lancet (London, England). 1991;337(8746):867-72. 69. Oiestad BE, Juhl CB, Eitzen I, Thorlund JB. Knee extensor muscle weakness is a risk factor for development of knee osteoarthritis. A systematic review and meta-analysis. Osteoarthritis and cartilage. 2015;23(2):171-7. 70. Roos EM, Arden NK. Strategies for the prevention of knee osteoarthritis. Nat Rev Rheumatol. 2016;12(2):92-101. 71. Hart HF, Barton CJ, Khan KM, Riel H, Crossley KM. Is body mass index associated with patellofemoral pain and patellofemoral osteoarthritis? A systematic review and meta-regression and analysis. British journal of sports medicine. 2017;51(10):781-90. 72. Jiang L, Tian W, Wang Y, Rong J, Bao C, Liu Y, et al. Body mass index and susceptibility to knee osteoarthritis: a systematic review and meta-analysis. Joint, bone, spine : revue du rhumatisme. 2012;79(3):291-7. 73. Zhou Z-Y, Liu Y-K, Chen H-L, Liu F. Body mass index and knee osteoarthritis risk: A dose-response meta-analysis. Obesity. 2014;22(10):2180-5. 74. Zheng H, Chen C. Body mass index and risk of knee osteoarthritis: systematic review and meta-analysis of prospective studies. BMJ Open. 2015;5(12):e007568. 75. Fernandes L, Hagen KB, Bijlsma JW, Andreassen O, Christensen P, Conaghan PG, et al. EULAR recommendations for the non-pharmacological core management of hip and knee osteoarthritis. Ann Rheum Dis. 2013;72(7):1125-35. 76. Hernan MA. A definition of causal effect for epidemiological research. Journal of epidemiology and community health. 2004;58(4):265-71. 77. Collins GS, Reitsma JB, Altman DG, Moons KG. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): the TRIPOD statement. BMJ (Clinical research ed). 2015;350:g7594. 78. Steyerberg EW, Vickers AJ, Cook NR, Gerds T, Gonen M, Obuchowski N, et al. Assessing the performance of prediction models: a framework for traditional and novel measures. Epidemiology (Cambridge, Mass). 2010;21(1):128-38. 79. Nordenvall R, Bahmanyar S, Adami J, Stenros C, Wredmark T, Fellander-Tsai L. A population-based nationwide study of cruciate ligament injury in Sweden, 2001-2009: incidence, treatment, and sex differences. The American journal of sports medicine. 2012;40(8):1808-13. 80. Collins JE, Katz JN, Donnell-Fink LA, Martin SD, Losina E. Cumulative incidence of ACL reconstruction after ACL injury in adults: role of age, sex, and race. The American journal of sports medicine. 2013;41(3):544-9. 81. Sanders TL, Maradit Kremers H, Bryan AJ, Kremers WK, Levy BA, Dahm DL, et al. Incidence of and Factors Associated With the Decision to Undergo Anterior Cruciate Ligament Reconstruction 1 to 10 Years After Injury. The American journal of sports medicine. 2016;44(6):1558-64.
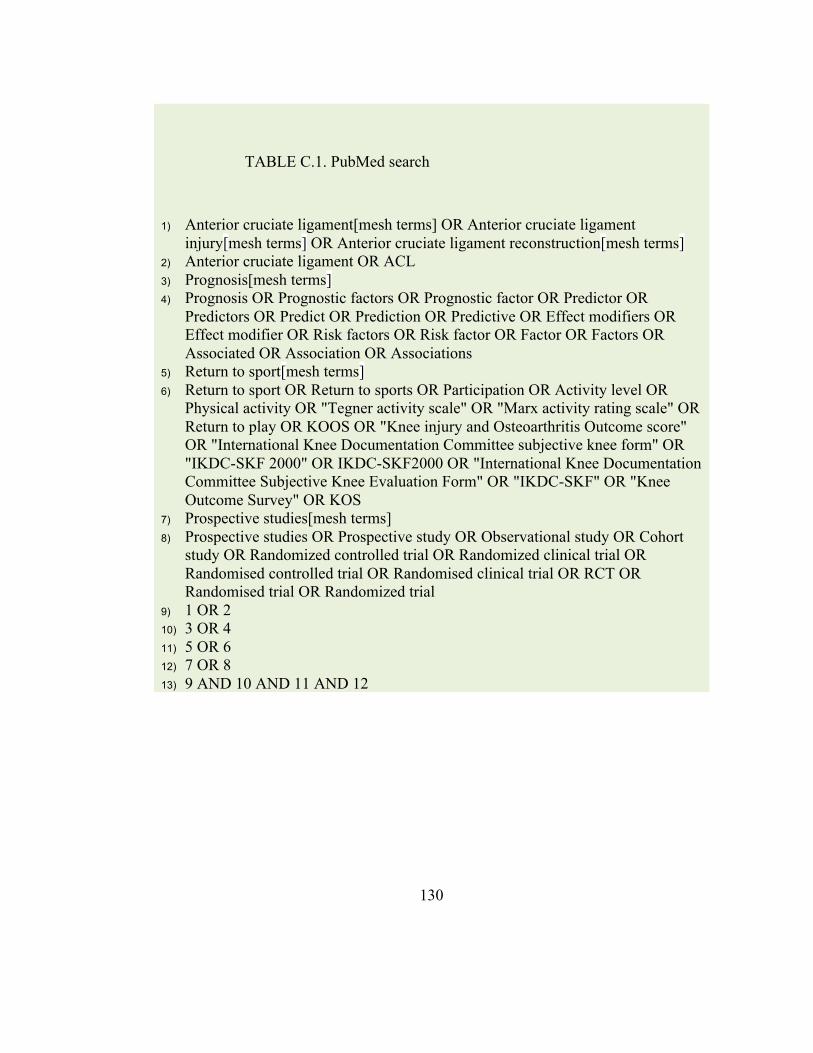
130
TABLE C.1. PubMed search
1) Anterior cruciate ligament[mesh terms] OR Anterior cruciate ligament injury[mesh terms] OR Anterior cruciate ligament reconstruction[mesh terms]
2) Anterior cruciate ligament OR ACL 3) Prognosis[mesh terms] 4) Prognosis OR Prognostic factors OR Prognostic factor OR Predictor OR
Predictors OR Predict OR Prediction OR Predictive OR Effect modifiers OR Effect modifier OR Risk factors OR Risk factor OR Factor OR Factors OR Associated OR Association OR Associations
5) Return to sport[mesh terms] 6) Return to sport OR Return to sports OR Participation OR Activity level OR
Physical activity OR "Tegner activity scale" OR "Marx activity rating scale" OR Return to play OR KOOS OR "Knee injury and Osteoarthritis Outcome score" OR "International Knee Documentation Committee subjective knee form" OR "IKDC-SKF 2000" OR IKDC-SKF2000 OR "International Knee Documentation Committee Subjective Knee Evaluation Form" OR "IKDC-SKF" OR "Knee Outcome Survey" OR KOS
7) Prospective studies[mesh terms] 8) Prospective studies OR Prospective study OR Observational study OR Cohort
study OR Randomized controlled trial OR Randomized clinical trial OR Randomised controlled trial OR Randomised clinical trial OR RCT OR Randomised trial OR Randomized trial
9) 1 OR 2 10) 3 OR 4 11) 5 OR 6 12) 7 OR 8 13) 9 AND 10 AND 11 AND 12
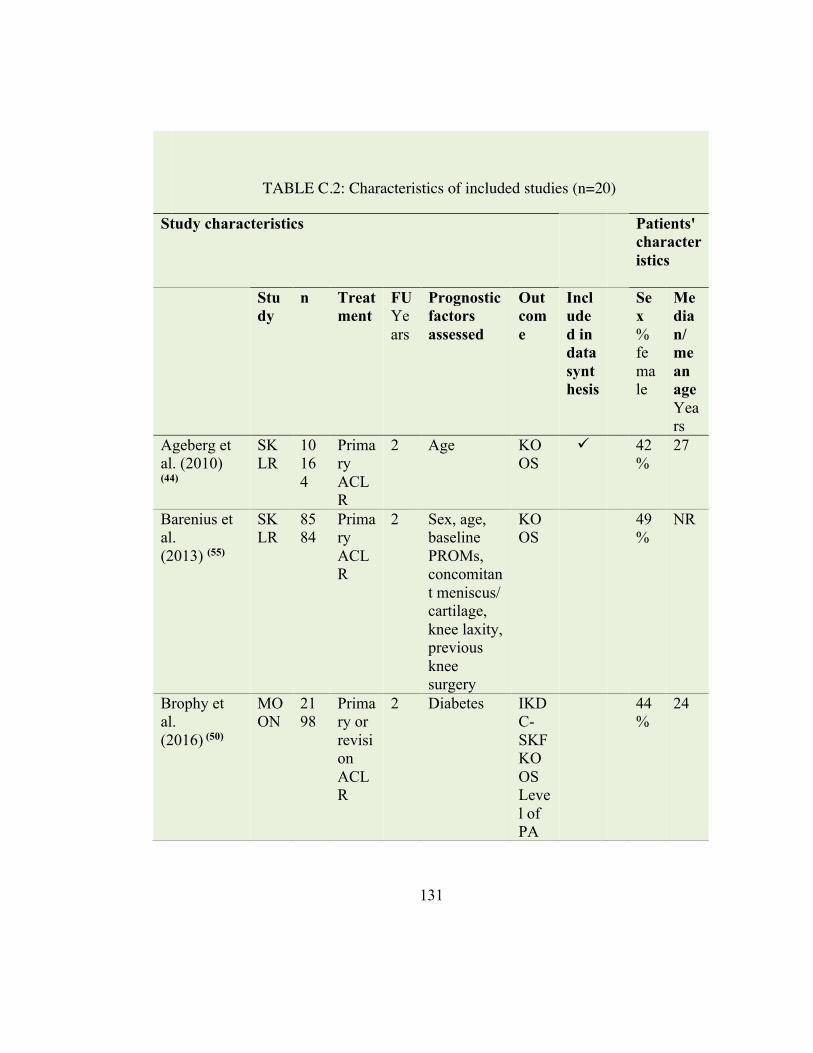
131
TABLE C.2: Characteristics of included studies (n=20)
Study characteristics Patients' characteristics
Study
n Treatment
FU Years
Prognostic factors assessed
Outcome
Included in data synthesis
Sex % female
Median/ mean age Years
Ageberg et al. (2010) (44)
SKLR
10164
Primary ACLR
2 Age KOOS
ü 42%
27
Barenius et al. (2013) (55)
SKLR
8584
Primary ACLR
2 Sex, age, baseline PROMs, concomitant meniscus/ cartilage, knee laxity, previous knee surgery
KOOS
49%
NR
Brophy et al. (2016) (50)
MOON
2198
Primary or revision ACLR
2 Diabetes IKDC-SKF KOOS Level of PA
44%
24
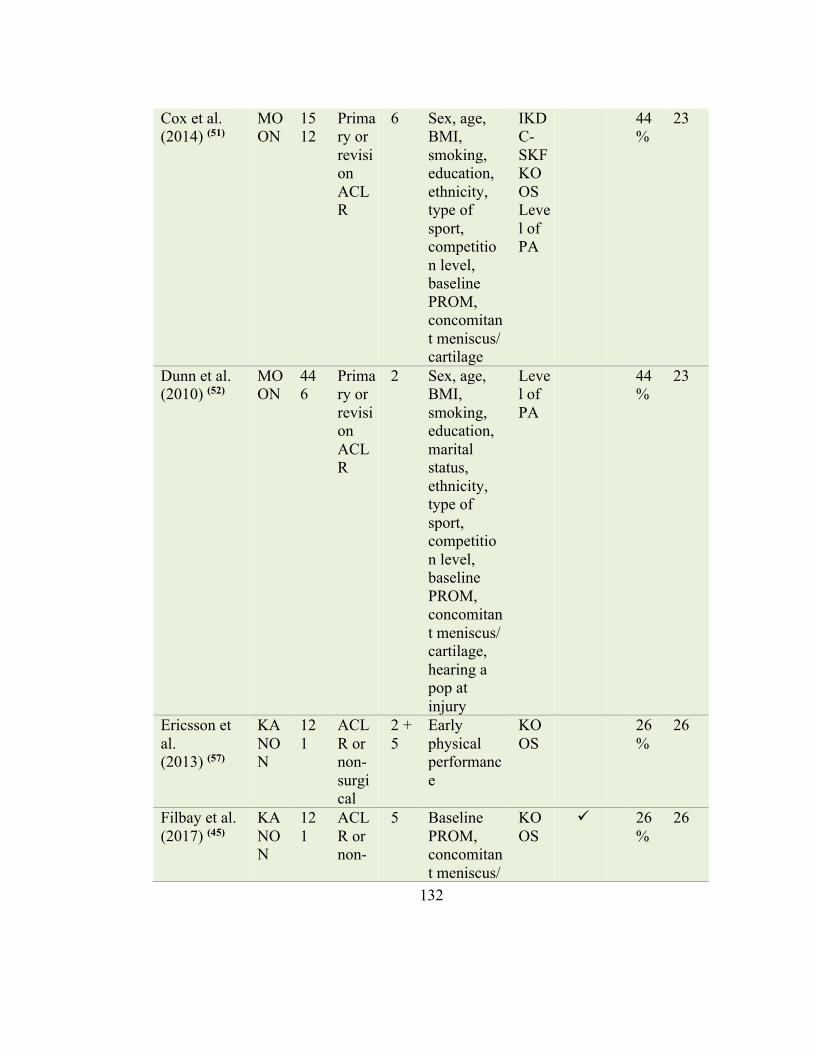
132
Cox et al. (2014) (51)
MOON
1512
Primary or revision ACLR
6 Sex, age, BMI, smoking, education, ethnicity, type of sport, competition level, baseline PROM, concomitant meniscus/ cartilage
IKDC-SKF KOOS Level of PA
44%
23
Dunn et al. (2010) (52)
MOON
446
Primary or revision ACLR
2 Sex, age, BMI, smoking, education, marital status, ethnicity, type of sport, competition level, baseline PROM, concomitant meniscus/ cartilage, hearing a pop at injury
Level of PA
44%
23
Ericsson et al. (2013) (57)
KANON
121
ACLR or non-surgical
2 + 5
Early physical performance
KOOS
26%
26
Filbay et al. (2017) (45)
KANON
121
ACLR or non-
5 Baseline PROM, concomitant meniscus/
KOOS
ü 26%
26
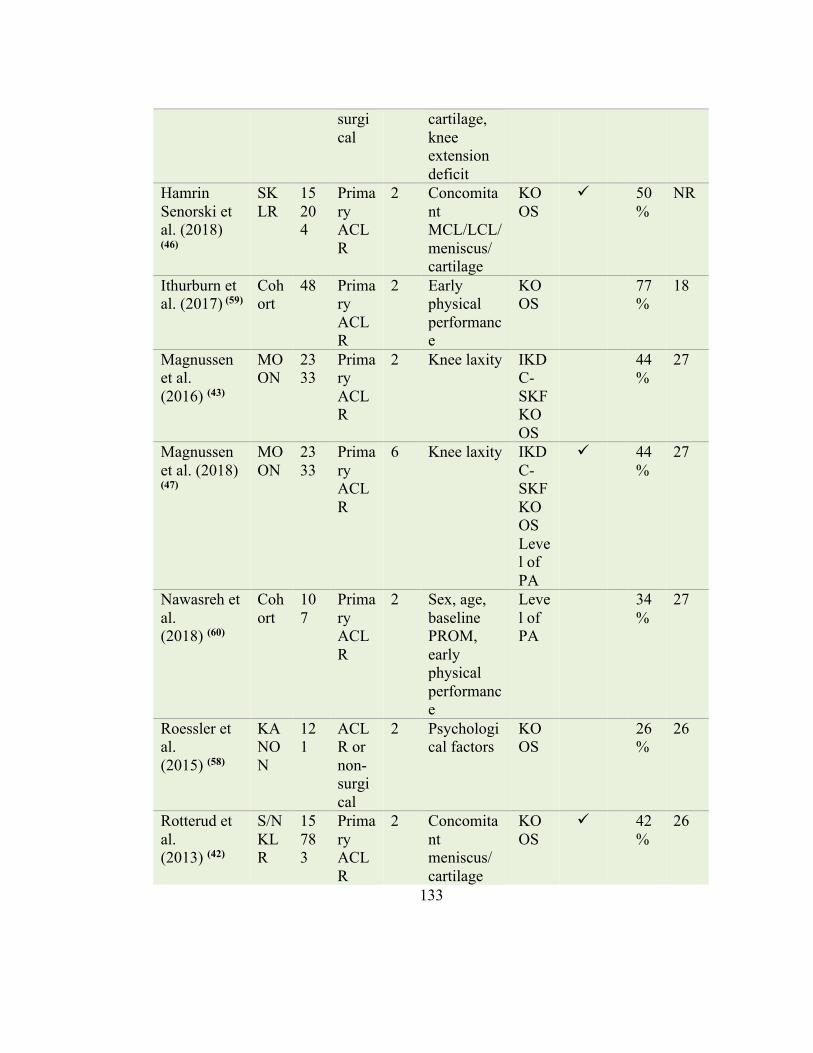
133
surgical
cartilage, knee extension deficit
Hamrin Senorski et al. (2018) (46)
SKLR
15204
Primary ACLR
2 Concomitant MCL/LCL/ meniscus/ cartilage
KOOS
ü 50%
NR
Ithurburn et al. (2017) (59)
Cohort
48 Primary ACLR
2 Early physical performance
KOOS
77%
18
Magnussen et al. (2016) (43)
MOON
2333
Primary ACLR
2 Knee laxity IKDC-SKF KOOS
44%
27
Magnussen et al. (2018) (47)
MOON
2333
Primary ACLR
6 Knee laxity IKDC-SKF KOOS Level of PA
ü 44%
27
Nawasreh et al. (2018) (60)
Cohort
107
Primary ACLR
2 Sex, age, baseline PROM, early physical performance
Level of PA
34%
27
Roessler et al. (2015) (58)
KANON
121
ACLR or non-surgical
2 Psychological factors
KOOS
26%
26
Rotterud et al. (2013) (42)
S/N KLR
15783
Primary ACLR
2 Concomitant meniscus/ cartilage
KOOS
ü 42%
26
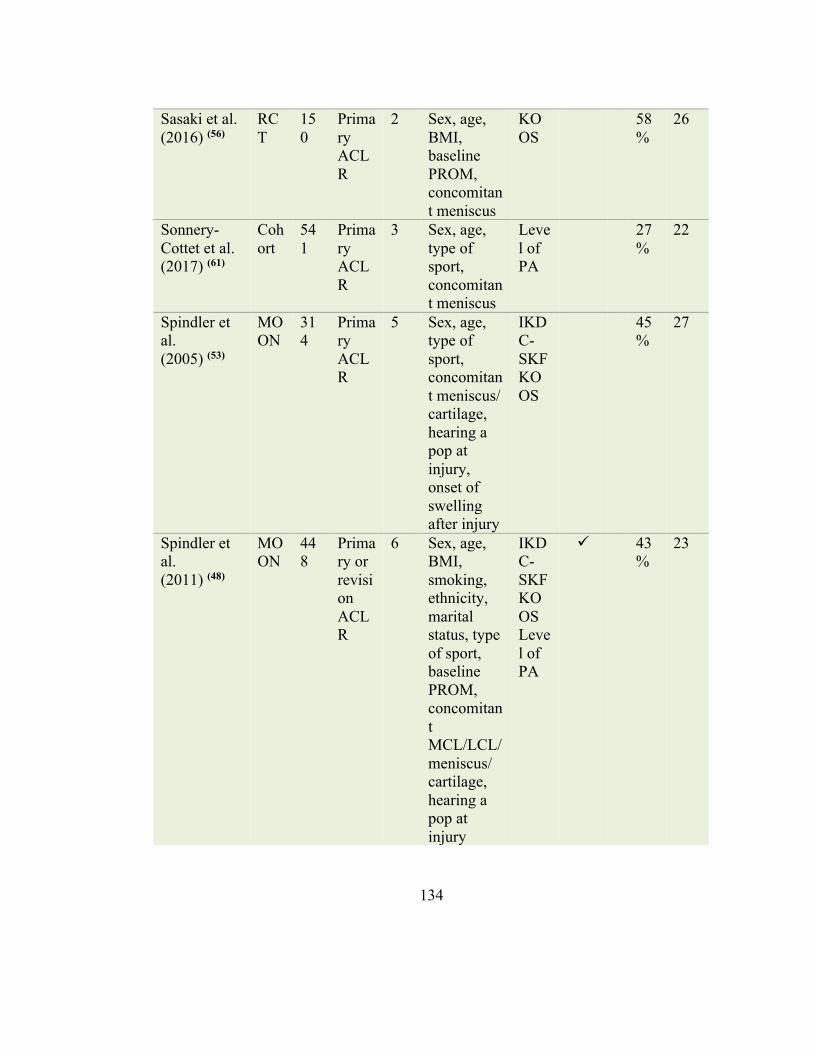
134
Sasaki et al. (2016) (56)
RCT
150
Primary ACLR
2 Sex, age, BMI, baseline PROM, concomitant meniscus
KOOS
58%
26
Sonnery-Cottet et al. (2017) (61)
Cohort
541
Primary ACLR
3 Sex, age, type of sport, concomitant meniscus
Level of PA
27%
22
Spindler et al. (2005) (53)
MOON
314
Primary ACLR
5 Sex, age, type of sport, concomitant meniscus/ cartilage, hearing a pop at injury, onset of swelling after injury
IKDC-SKF KOOS
45%
27
Spindler et al. (2011) (48)
MOON
448
Primary or revision ACLR
6 Sex, age, BMI, smoking, ethnicity, marital status, type of sport, baseline PROM, concomitant MCL/LCL/ meniscus/ cartilage, hearing a pop at injury
IKDC-SKF KOOS Level of PA
ü 43%
23
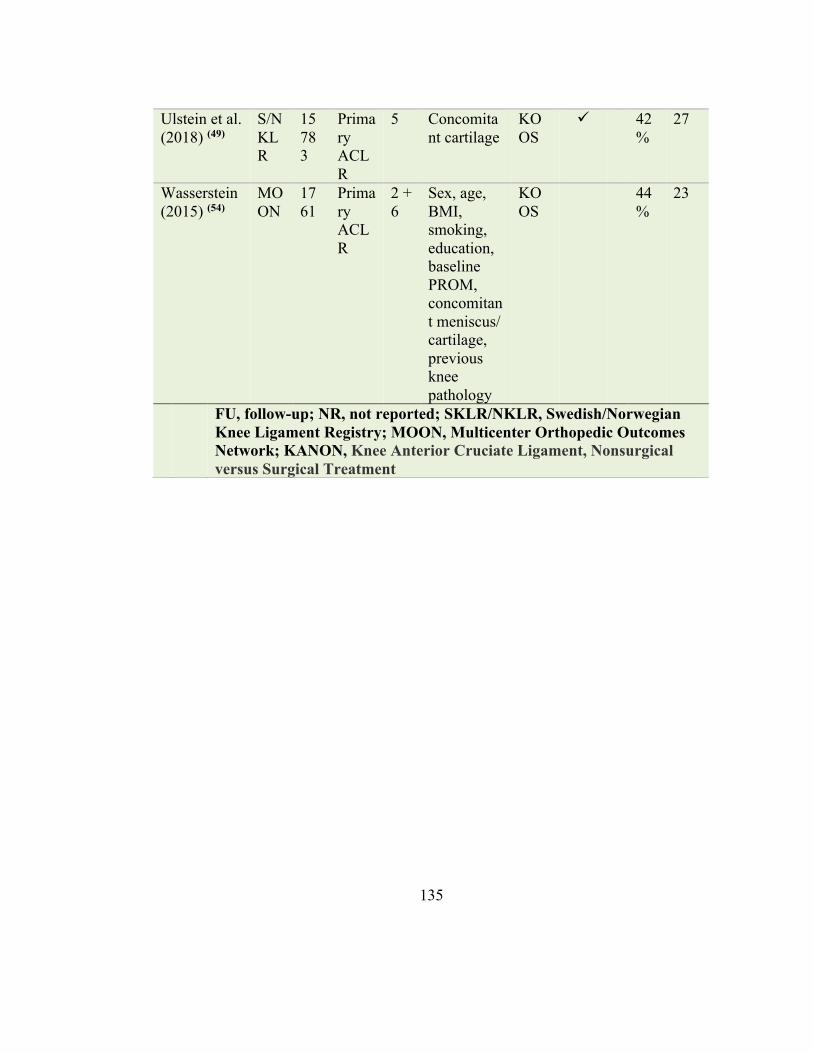
135
Ulstein et al. (2018) (49)
S/N KLR
15783
Primary ACLR
5 Concomitant cartilage
KOOS
ü 42%
27
Wasserstein (2015) (54)
MOON
1761
Primary ACLR
2 + 6
Sex, age, BMI, smoking, education, baseline PROM, concomitant meniscus/ cartilage, previous knee pathology
KOOS
44%
23
FU, follow-up; NR, not reported; SKLR/NKLR, Swedish/Norwegian Knee Ligament Registry; MOON, Multicenter Orthopedic Outcomes Network; KANON, Knee Anterior Cruciate Ligament, Nonsurgical versus Surgical Treatment
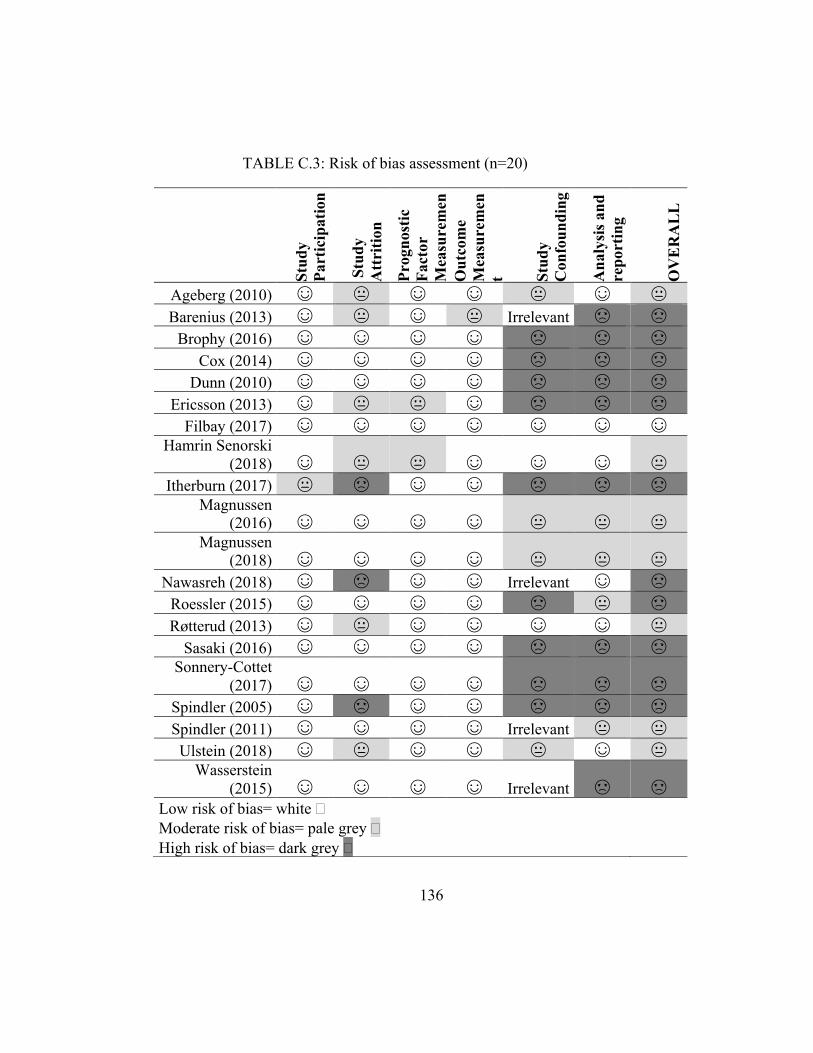
136
TABLE C.3: Risk of bias assessment (n=20)
Stud
y Pa
rtic
ipat
ion
Stu
dy
Att
ritio
n Pr
ogno
stic
Fa
ctor
M
easu
rem
ent O
utco
me
Mea
sure
men
t Stud
y C
onfo
undi
ng
Ana
lysi
s and
re
port
ing
OV
ER
AL
L
Ageberg (2010) ☺ 😐 ☺ ☺ 😐 ☺ 😐 Barenius (2013) ☺ 😐 ☺ 😐 Irrelevant ☹ ☹
Brophy (2016) ☺ ☺ ☺ ☺ ☹ ☹ ☹ Cox (2014) ☺ ☺ ☺ ☺ ☹ ☹ ☹
Dunn (2010) ☺ ☺ ☺ ☺ ☹ ☹ ☹ Ericsson (2013) ☺ 😐 😐 ☺ ☹ ☹ ☹
Filbay (2017) ☺ ☺ ☺ ☺ ☺ ☺ ☺ Hamrin Senorski
(2018) ☺ 😐 😐 ☺ ☺ ☺ 😐 Itherburn (2017) 😐 ☹ ☺ ☺ ☹ ☹ ☹
Magnussen (2016) ☺ ☺ ☺ ☺ 😐 😐 😐
Magnussen (2018) ☺ ☺ ☺ ☺ 😐 😐 😐
Nawasreh (2018) ☺ ☹ ☺ ☺ Irrelevant ☺ ☹ Roessler (2015) ☺ ☺ ☺ ☺ ☹ 😐 ☹ Røtterud (2013) ☺ 😐 ☺ ☺ ☺ ☺ 😐
Sasaki (2016) ☺ ☺ ☺ ☺ ☹ ☹ ☹ Sonnery-Cottet
(2017) ☺ ☺ ☺ ☺ ☹ ☹ ☹ Spindler (2005) ☺ ☹ ☺ ☺ ☹ ☹ ☹ Spindler (2011) ☺ ☺ ☺ ☺ Irrelevant 😐 😐 Ulstein (2018) ☺ 😐 ☺ ☺ 😐 ☺ 😐
Wasserstein (2015) ☺ ☺ ☺ ☺ Irrelevant ☹ ☹
Low risk of bias= white � Moderate risk of bias= pale grey � High risk of bias= dark grey �
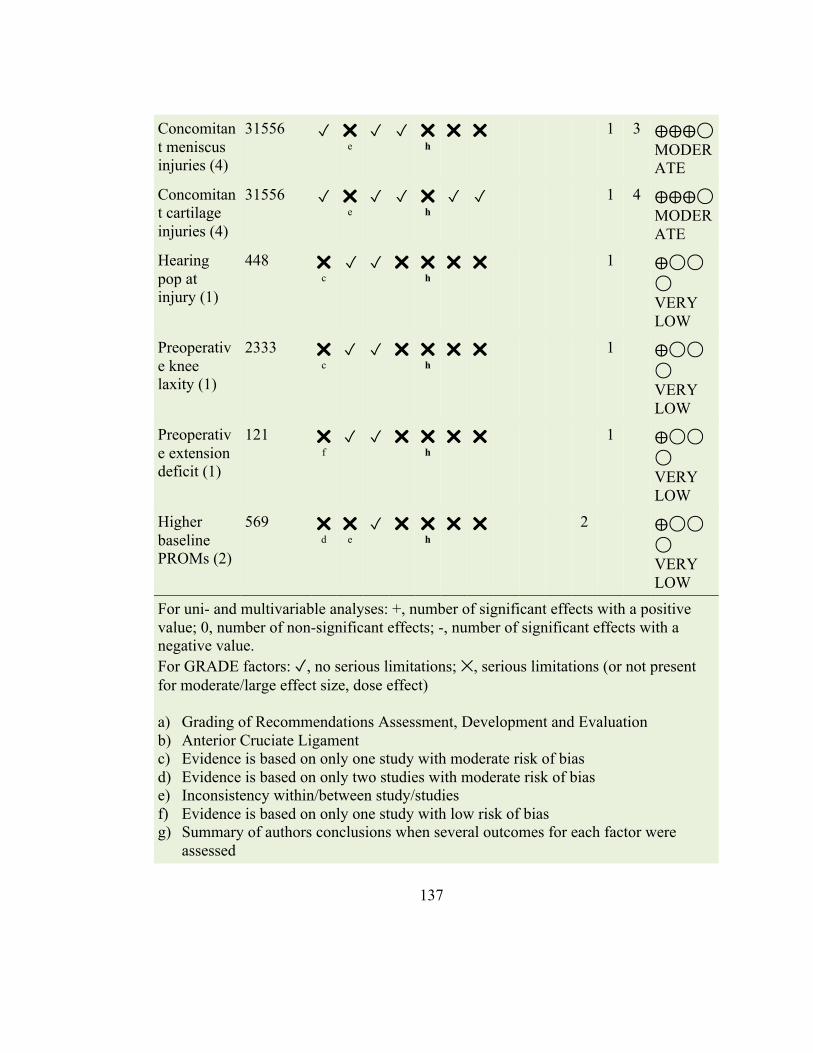
137
Concomitant meniscus injuries (4)
31556 ✓ ✕
e ✓ ✓ ✕
h ✕ ✕ 1 3 ⨁⨁⨁◯
MODERATE
Concomitant cartilage injuries (4)
31556 ✓ ✕
e ✓ ✓ ✕
h ✓ ✓ 1 4 ⨁⨁⨁◯
MODERATE
Hearing pop at injury (1)
448 ✕
c ✓ ✓ ✕ ✕
h ✕ ✕ 1 ⨁◯◯
◯ VERY LOW
Preoperative knee laxity (1)
2333 ✕
c ✓ ✓ ✕ ✕
h ✕ ✕ 1 ⨁◯◯
◯ VERY LOW
Preoperative extension deficit (1)
121 ✕
f ✓ ✓ ✕ ✕
h ✕ ✕ 1 ⨁◯◯
◯ VERY LOW
Higher baseline PROMs (2)
569 ✕
d ✕
e ✓ ✕ ✕
h ✕ ✕ 2 ⨁◯◯
◯ VERY LOW
For uni- and multivariable analyses: +, number of significant effects with a positive value; 0, number of non-significant effects; -, number of significant effects with a negative value. For GRADE factors: ✓, no serious limitations; ✕, serious limitations (or not present for moderate/large effect size, dose effect) a) Grading of Recommendations Assessment, Development and Evaluation b) Anterior Cruciate Ligament c) Evidence is based on only one study with moderate risk of bias d) Evidence is based on only two studies with moderate risk of bias e) Inconsistency within/between study/studies f) Evidence is based on only one study with low risk of bias g) Summary of authors conclusions when several outcomes for each factor were
assessed
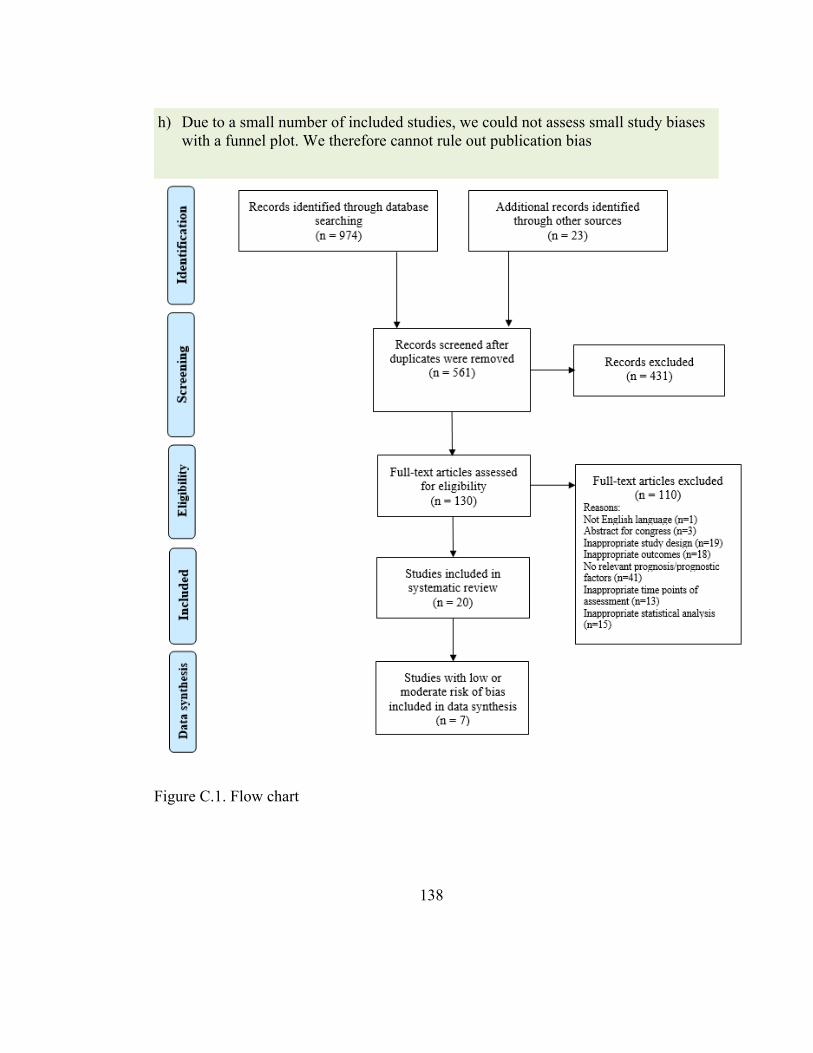
138
Figure C.1. Flow chart
h) Due to a small number of included studies, we could not assess small study biases with a funnel plot. We therefore cannot rule out publication bias
139
Recommended

















