
International Journal of
Science, Engineering and Innovative Research Volume 6, December 2015
ISSN: 2412-513X
1
STATISTICAL ANALYSIS ON HOUSEHOLD FACTORS INFLUENCING ANNUAL
EPISODES OF MALARIA
K.O. Obisesan
Department of Statistics
University of Nigeria
A.S. Adelanwa
Total Quality Management Department
University College Hospital, Ibadan
Abstract
Malaria is responsible for about 66 per cent of all clinic visits in Nigeria. It accounts for 25%
of under-5 mortality, 30% childhood mortality and 11% maternal mortality. At least 50% of
the population will have at least one episode of malaria annually. Moreover, environment
dictates the incidence and prevalence of diseases all over the world and if timely action is not
taken, it may lead to diseases. Three (3) out of six (6) major towns in Ido local government
area are considered and accumulated one hundred and ninety one (191) individuals as
respondents using haphazard non probability sampling technique for selection. The obtained
data through questionnaire was presented on frequency table and charts while inferential
statistics were analysed using dummy variables in regression. It was revealed that majority of
the respondents suffered from one or more incidences of malaria in a year, where female had
the higher percentage of the incidence and there was high incidence of malaria among the adult
ages 30years and above. The qualitative predictor variable in regression analysis revealed
significant relationship between annual episode of malaria and number of members of
household, toilet type, absent ceiling, building type, disposable site and source of domestic
water. The ANOVA, F – test was significant for all predicted factors. Conclusively, in the view
of the discovery, it was therefore recommended that people need awareness on densely
populated area / household are more prone to experience more episodes of malaria incidence
than sparsely populated one, encouragement on utilization of closed domestic water system
instead of open system to avoid reservoir for mosquito, enlightenment on type toilet used and
avoid absence ceiling to prevent being a breeding site for mosquitoes, government to stage
more campaign against malaria especially for adult not for children under 5year alone and
International Journal of
Science, Engineering and Innovative Research Volume 6, December 2015
ISSN: 2412-513X
2
create a task force officer/ sanitary inspectors to checkmate sanitation of our environment to
avoid unkempt toilet habit which serves as breeding site for mosquitoes.
1 Introduction
Malaria is a disease caused by a parasite that is transmitted by an Anopheles mosquito.
The symptoms include fever, chills, headaches, muscle aches and general malaise (similar to
flu symptoms). This disease is prevalent in tropical or sub-tropical climates [8]. In Nigeria,
malaria causes the deaths of an estimated 250,000 children under the age of five every year.
Malaria is responsible for about 66 per cent of all clinic visits in Nigeria. Health workers are
sometimes forced to work overtime, and doctors and nurses can be on duty for over 12 hours a
day [21].
Malaria transmission can be reduced by preventing mosquito bites by distribution of
inexpensive mosquito nets and insect repellents, or by mosquito-control measures such as
spraying insecticides inside houses and draining standing water where mosquitoes lay their
eggs [15]. Mosquito nets help keep mosquitoes away from people and greatly reduce the
infection and transmission of malaria [22]. However, the inexpensive mosquito nets are not a
perfect barrier. Insecticides Treated Nets(ITNs) have been shown to be the most cost-effective
prevention method against malaria and are part of WHO’s Millennium Development Goals
(MDGs), but less than 2% of children in urban areas in Sub-Saharan Africa are protected by
ITNs and this process poses a significant logistical problem in rural environment [10].
In Nigeria, the burden of malaria is well documented and has been shown to be a big
contributor to the economic burden of disease in communities where it is endemic and is
responsible for annual economic loss of 132 billion Naira [19], [5] and [13]. It is estimated that
300, 000 deaths occurring each year, 60% of outpatient visits and 30% hospitalizations are all
attributable to malaria [6] and [18]. The disease is particularly virulent among pregnant women
and children under 5 years of age, due to their low levels of immunity. Also [20] indicated a
strong correlation between malaria and poverty has also long been recognized. Not only does
malaria thrive in poverty but it also impedes economic growth and keeps households in poverty.
This study aimed to investigate household factors influencing the annual episodes of malaria
among people living in Ido local governments Area, Oyo State. Specifically, the study is to
investigate the prevalence of malaria in Ido local government area of Oyo State, examine the

International Journal of
Science, Engineering and Innovative Research Volume 6, December 2015
ISSN: 2412-513X
3
sex and age group with high incidence of the malaria, and household components with
significant relationship with annual episodes of malaria.
WHO, (2014) [24] reported that commonly, the disease is transmitted by the bite of an
infected female Anopheles mosquito. This bite introduces the parasites from the mosquito's
saliva into a person's blood. The parasites then travel to the liver where they mature and
reproduce. Five species of Plasmodium can infect and be spread by humans. Most deaths are
caused by P. falciparum because P. vivax, P. ovale, and P. malariae generally cause a milder
form of malaria. The species P. knowlesi rarely causes disease in humans. Carabolla, (2013)
[2] opined that malaria is typically diagnosed by the microscopic examination of blood using
blood films, or with antigen-based rapid diagnostic tests. Methods that use the polymerase
chain reaction to detect the parasite's DNA have been developed, but are not widely used in
areas where malaria is common due to their cost and complexity.
Malaria occurs mostly in poor tropical and subtropical areas of the world. In many of
the countries affected by malaria, it is a leading cause of illness and death. In 2010, [4] reported
that 3.4 billion people live in areas at risk of malaria transmission in 106 countries and
territories. An estimated 91% of deaths in 2010 were in the African Region. In 2012, an
estimated 627,000 people died of malaria and it caused 207 million clinical episodes - most
were young children in sub-Saharan Africa. Within the last decade, increasing numbers of
partners and resources have rapidly increased malaria control efforts [23].
1.1 Malaria in Nigeria
Jimoh et al., (2007) [13] reported that malaria is the 3rd leading cause of death for
children under five years worldwide, after pneumonia and diarrheal disease. Nigeria bears up
to 25 percent of the malarial disease burden in Africa, hence contributing significantly to the
one million lives lost per year in the region, which mostly consists of children and pregnant
women. Malaria in Nigeria is endemic and constitutes a major public health problem despite
the curable nature of the disease. Malaria-related deaths account for up to 11 percent of
maternal mortality. Additionally, they contribute up to 25 percent of infant mortality and 30
percent of under-5 mortality, resulting in about 300,000 childhood deaths annually. The disease
overburdens the already-weakened health system: nearly 110 million clinical cases of malaria
are diagnosed each year, and malaria contributes up to 60 percent of outpatient visits and 30

International Journal of
Science, Engineering and Innovative Research Volume 6, December 2015
ISSN: 2412-513X
4
percent of admissions. Malaria also exerts a huge social and economic burden on families,
communities, and the country at large, causing an annual loss of about 132 billion naira in
payments for treatment and prevention as well as hours not worked.
Malaria is a major public health problem in Nigeria where it accounts for more cases
and deaths than any other country in the world. Malaria is a risk for 97% of Nigeria’s
population. The remaining 3% of the population live in the malaria free highlands. There are
an estimated 100 million malaria cases with over 300,000 deaths per year in Nigeria. This
compares with 215,000 deaths per year in Nigeria from HIV/AIDS. Malaria contributes to an
estimated 11% of maternal mortality
1.2 Malaria Transmission in Nigeria
The seasonality, intensity, and duration of the malaria transmission season vary
according to the five ecological strata that extend from the South to the North. These include
mangrove swamps, rain forest, guinea-savannah, Sudan-savannah, and Sahel-savannah. The
duration of the season decreases as one moves from the South to the North, being perennial in
duration in most of the South but lasting three months or less in the northeastern region
bordering Chad. The geographic location of Nigeria makes the climate suitable for malaria
transmission throughout the country. It is estimated that up to 97 percent of the country’s more
than 150 million people risk getting the disease. The remaining 3 percent of the population who
live in the mountains in southern Jos (the Plateau State) at an altitude ranging from 1,200 to
1,400 metres, are at relatively low risk for malaria.
1.3 Malaria in Oyo State
Gbadegesin (2013) [9] in Oyo State, the state’s Commissioner for Health at the
inauguration of the 2013 World Malaria Day Celebration said, ‘NO fewer than six million
attacks of malaria occur yearly’. Furthermore, he said malaria had serious health and socio-
economic impact, reiterated that six out of every 10 cases of patients attended to at the state
hospitals were as result of malaria. Children from age zero to four years have at least two to
four attacks in a year, while half of the adult population have at least one attack in a year.
To curb deaths from malaria, there is need for individuals to seek appropriate medical
attention and embark on self-help activities such as use of insecticide-treated nets and keep
International Journal of
Science, Engineering and Innovative Research Volume 6, December 2015
ISSN: 2412-513X
5
their environment clean to prevent mosquitoes. The government was committed to reducing
the malaria prevalence by 50 per cent yearly and so exceed the Millennium Development Goal
target. To achieve this, the state was in collaboration with its malaria implementing partners,
distributed 890,000 long-lasting insecticide-treated nets (LLIN); supplied malaria-designated
health care facilities with 300,000 doses of antimalarial drugs and 80,000 rapid diagnostic
tools, as well as 100 per cent malaria coverage for pregnant women.
1.4 Household Components
1.4.1 Drains, Ditches and Gutters
While agriculture provides the most productive urban vector breeding sites, drains and
ditches may provide more common habitats. [3] reported in a study in Dar es Salaam, Tanzania,
there were three times more anopheline-positive drains and ditches compared to agricultural
breeding sites, and anopheline presence was much more likely in drains that were blocked. [1]
reported that blockages are often due to poor sanitation and lead to reduced water flow and
accumulation of stagnant water pools which are ideal for mosquito breeding. Gutters provide
a similar breeding site for mosquitoes in both the wet and dry seasons and were specifically
noted by a recent study in Abeokuta, Nigeria.
1.4.2 Tyre Tracks
Tyre tracks were the second most-cited artificial vector breeding site. In Malindi,
Kenya, they accounted for as much as 29% of all water bodies that were positive for mosquitoes
[12]. Tyre tracks are more common in areas of high socioeconomic status, which tend to house
more vehicle owners while still having roads of sufficiently poor quality to lead to the
formation of potholes, tyre tracks, and other artificial breeding sites.
1.4.3 Swimming Pools
In another study in Malindi, unused swimming pools were found to provide a
particularly productive habitat for Anopheles immature stages [12]. Of the 250 habitats
identified in the study, 66 were swimming pools, and these were found to have the highest
abundance of Anopheles mosquitoes. Hotel workers, tourists, and domestic workers may be at
heightened risk of malaria transmission in areas with an abundance of unused pools.
1.4.4 Water Pipes

International Journal of
Science, Engineering and Innovative Research Volume 6, December 2015
ISSN: 2412-513X
6
Klinkenberg et al. (2008) [16] reported that water pipes can lead to breeding site
formation in a variety of ways, most frequently when they are broken and pools of water collect.
[11] stated that pipes often break as a result of poor installation or quality, clay soil expansion
and contraction, construction work, and as an opportunity to procure free water for sale or
consumption. Water sources that are further away from pipes are more likely to be anopheline
positive because water flow from nearby pipes may disturb the water surface, reducing the
breeding site quality [12]. Artificial water storage containers can also serve as breeding sites,
and car washing has been found to provide excellent habitats for larval development [14].
1.4.5 Other household factors
Better-quality housing decreases the risk of malaria as it minimizes entry points for
mosquitoes during the night. To illustrate this, a study in Gambia showed that houses with
malaria-infected children are more likely to have mud walls, open eaves, and absent ceilings
than those with uninfected children. Floors comprised of earth bricks are also associated with
lower malaria risk as inhabitants are more likely to sleep on raised beds to avoid ground
moisture, in turn eluding bites from An. gambiae mosquitoes which search for blood close to
the ground. Interestingly, a study in Burkina Faso found that electricity use was associated with
increased malaria risk, as the alternative of biomass fuel burning produces smoke that is
thought to deter mosquitoes from entering houses; however, electricity use in better-quality
housing would presumably not show this trend [25].
Fobil et al. (2011) opined hygiene, sanitation, and waste collection are key determinants
of malaria transmission which, while household responsibilities, have a community-level effect
on disease transmission. As an example, the more the households dispose of waste properly,
the lower the risk of liquid waste collecting in pools of stagnant water and forming vector
breeding sites. [17] stated that in Accra, Ghana, being connected to a toilet was found to be
even more important than waste removal in reducing community malaria mortality; however,
toilets are also potential areas of mosquito activity, and septic tanks within communities are a
potential source of vector breeding sites.
2. Materials and Methodology
A self-developed and well structured empirically related questionnaire was used. The
text items were twenty seven in number. It has three sections: A – Contain text item to elicit
International Journal of
Science, Engineering and Innovative Research Volume 6, December 2015
ISSN: 2412-513X
7
information on respondent’s socio-demographic variables. B– have items to elicit information
on respondent’s household components and C– have items to elicit information on respondent’s
malaria preventive measures. In order to ensure that the research instrument maintain
consistency in measuring what it intends to measure, a pilot study of 10% of the sample size
was carried out using 20 people from Akinyele local government area. Cronbach alpha
reliability coefficient was used to analyse data collected. For effective collection of data for
this study, the researcher employed the help of six (6) research assistants who were trained and
assessed for data collection process. A questionnaire was administered to the identified willing
and available members of household selected. The questionnaire was retrieved immediately
after duly and correctly filled. Exploratory data analysis was carried out on the collected data
to explore the salient features of the data and clean-up the error it contained. Descriptively,
qualitative data were presented on tables and charts, continuous data as mean and standard
deviations.
Inferentially, dummy variables in regression was employed whereby the episode of
incidence of malaria on individual is the response variable (Y) and the predictor variables are
age (X1), sex (X2), family income (X3), Disposable site (X4), Water drainage system (X5), Mud
wall (X6), Absent Ceiling (X7), Drinking water (X8), Domestic water (X9), toilet type (X10) and
building type (X11).
Regression Model is given by:
Y = 0 + 1X1 + 2X2 + 3X3 + 4X4 + 5X5 + 6X6 + 7X7 + 8X8 + 9X9 + ....+Ui (i)
Tool Model X1 X2 X3 X4 X5 X6 X7 X8 X9 ... X11
M1 Xi1 1 0 0 0 0 0 0 0 0
M2 Xi2 0 1 0 0 0 0 0 0 0
M3 Xi3 0 0 1 0 0 0 0 0 0
M4 Xi4 0 0 0 1 0 0 0 0 0
M5 Xi5 0 0 0 0 1 0 0 0 0
M11 Xi5 0 0 0 0 0 0 0 0 1
E(Y) for equation (i)
E(Y) = 0 + 1X1 + 2X2 + 3X3 + 4X4 + 5X5 + 6X6 + 7X7 + 8X8 + 9X9 + .... (ii)
For M1; X2 = 1, X3 =X4 =X5 =X6 =X7 =X8 =X9 =X10 =X11 = 0.
E(Y) = 0 + 1X1 + 2X2

International Journal of
Science, Engineering and Innovative Research Volume 6, December 2015
ISSN: 2412-513X
8
= 0 + 1X1 + 2(1)
= (0 + 2) + 1X1
For M2; X3 = 1, X2 = X4 =X5 =X6 =X7 =X8 =X9 =X10 =X11 = 0.
E(Y) = 0 + 1X1 + 3X3
= 0 + 1X1 + 3(1)
= (0 + 3) + 1X1
3. Analysis and Result
3.1 Data Visualization
Table 1 reveals that out of 191 respondents, 56 (29.3%) were residing at Apata, 60(31.4%)
were residing at Ido town and 75(39.3%) were residing at Apete area. The proportion was in
line with the population of the area. In Apata, Ido local government area covers only a sectional
part, Ido is a town but more rural than urban because majority of the land were used as
farmland. Apete is a settlement with more enlightening personnel including students than
illiterate due to its nearness to high institution of learning. 171 (89.5%) of the respondents are
Yoruba indicating Yoruba ethnic dominated area. Fifty six percent were Muslims among whom
53.9% polygamous home. Slightly above half of the respondents 50.8 percent had between
N10,000 and N30,000 as their family average monthly income. There were 53.4% female in
the study. The mean age of the respondents was 24years (S.D = 17), the minimum was 1 year
and maximum 70years.

International Journal of
Science, Engineering and Innovative Research Volume 6, December 2015
ISSN: 2412-513X
9
Table 1: Demographic Characteristics of the Respondents (N = 191)
Variable Response Frequency (n) Percentage (%)
Location Apata 56 29.3
Ido 60 31.4
Apete 75 39.3
Tribe Yoruba 171 89.5
Igbo 20 10.5
Religion Christianity 84 44.0
Islam 107 56.0
Family Type Monogamy 88 46.1
Polygamy 103 53.9
Amount of family
income (Monthly
average)
Below 10,000 7 3.7
10,000 – 30,000 97 50.8
31,000 – 50,000 29 15.2
51,000 – 70,000 19 9.9
71,000 – 90,000 2 1.0
Above 90,000 37 19.4
Sex Male 89 46.6
Female 102 53.4
Age group (yrs) 1 – 5 21 11.0
6 – 10 25 13.1
11 – 15 29 15.2
16 – 20 22 11.5
21 – 25 22 11.5
26 – 30 11 5.0
Above 30 61 31.9
Episode of Malaria
in a year
None 13 6.8
1 46 24.1
International Journal of
Science, Engineering and Innovative Research Volume 6, December 2015
ISSN: 2412-513X
10
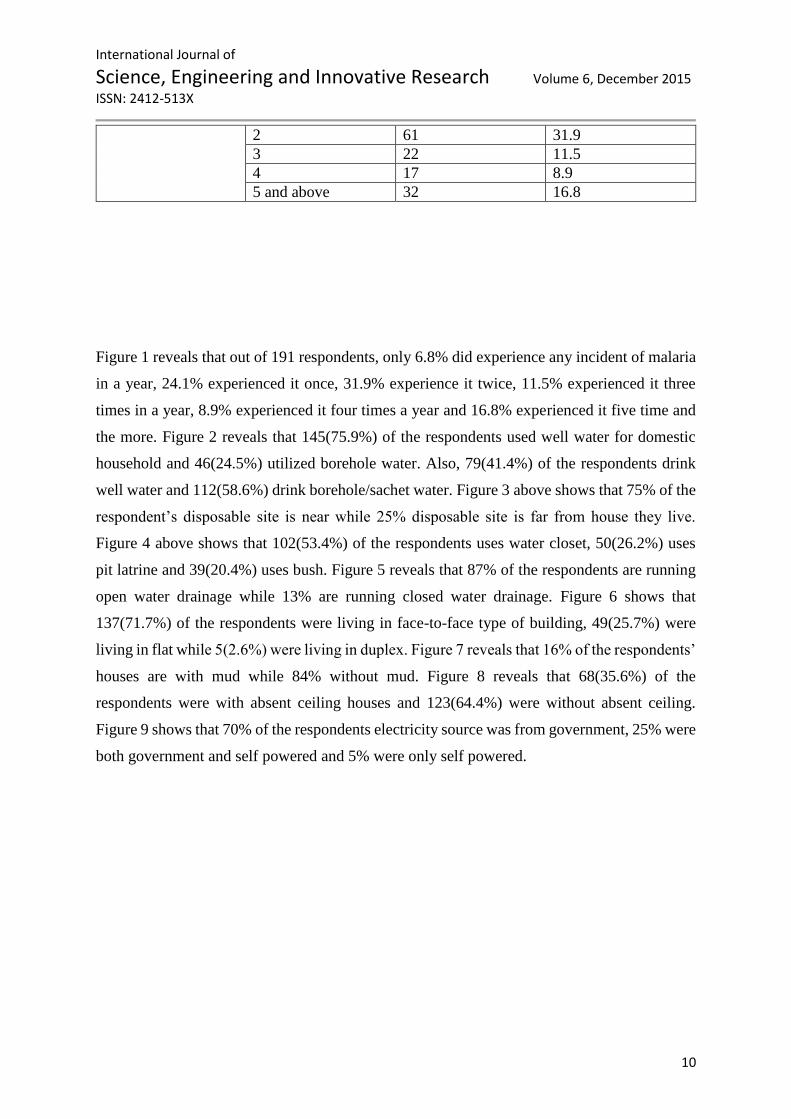
2 61 31.9
3 22 11.5
4 17 8.9
5 and above 32 16.8
Figure 1 reveals that out of 191 respondents, only 6.8% did experience any incident of malaria
in a year, 24.1% experienced it once, 31.9% experience it twice, 11.5% experienced it three
times in a year, 8.9% experienced it four times a year and 16.8% experienced it five time and
the more. Figure 2 reveals that 145(75.9%) of the respondents used well water for domestic
household and 46(24.5%) utilized borehole water. Also, 79(41.4%) of the respondents drink
well water and 112(58.6%) drink borehole/sachet water. Figure 3 above shows that 75% of the
respondent’s disposable site is near while 25% disposable site is far from house they live.
Figure 4 above shows that 102(53.4%) of the respondents uses water closet, 50(26.2%) uses
pit latrine and 39(20.4%) uses bush. Figure 5 reveals that 87% of the respondents are running
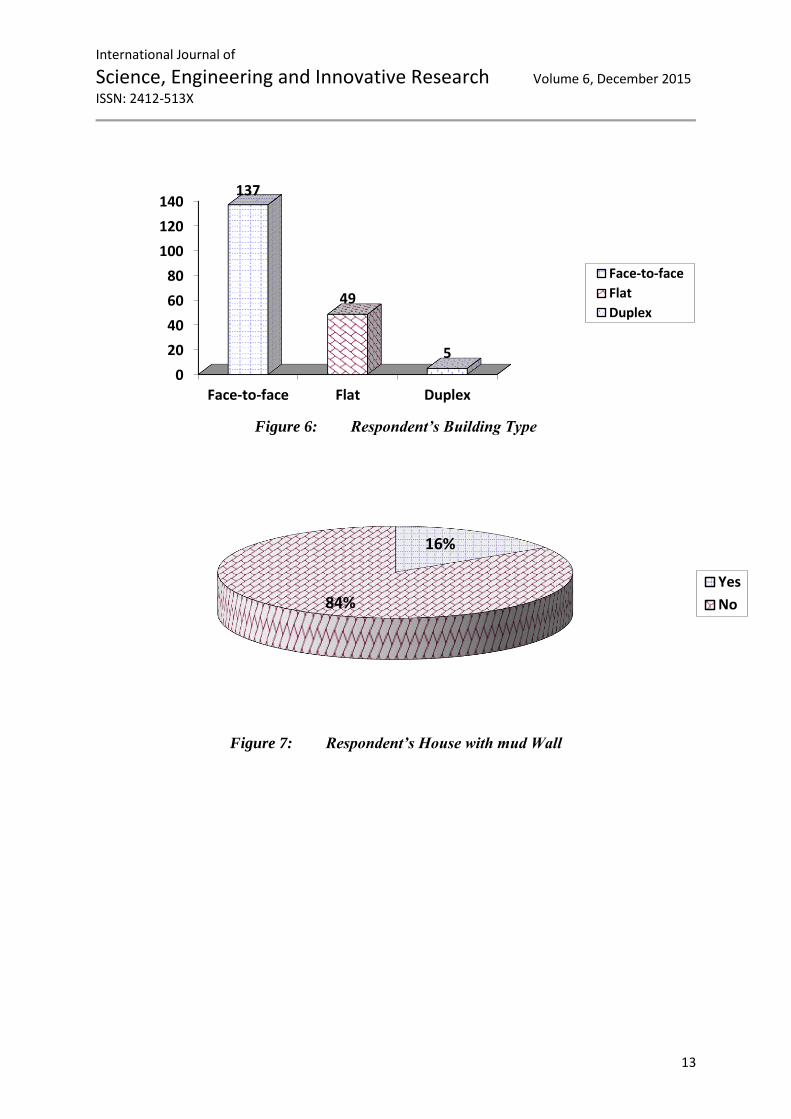
open water drainage while 13% are running closed water drainage. Figure 6 shows that
137(71.7%) of the respondents were living in face-to-face type of building, 49(25.7%) were
living in flat while 5(2.6%) were living in duplex. Figure 7 reveals that 16% of the respondents’
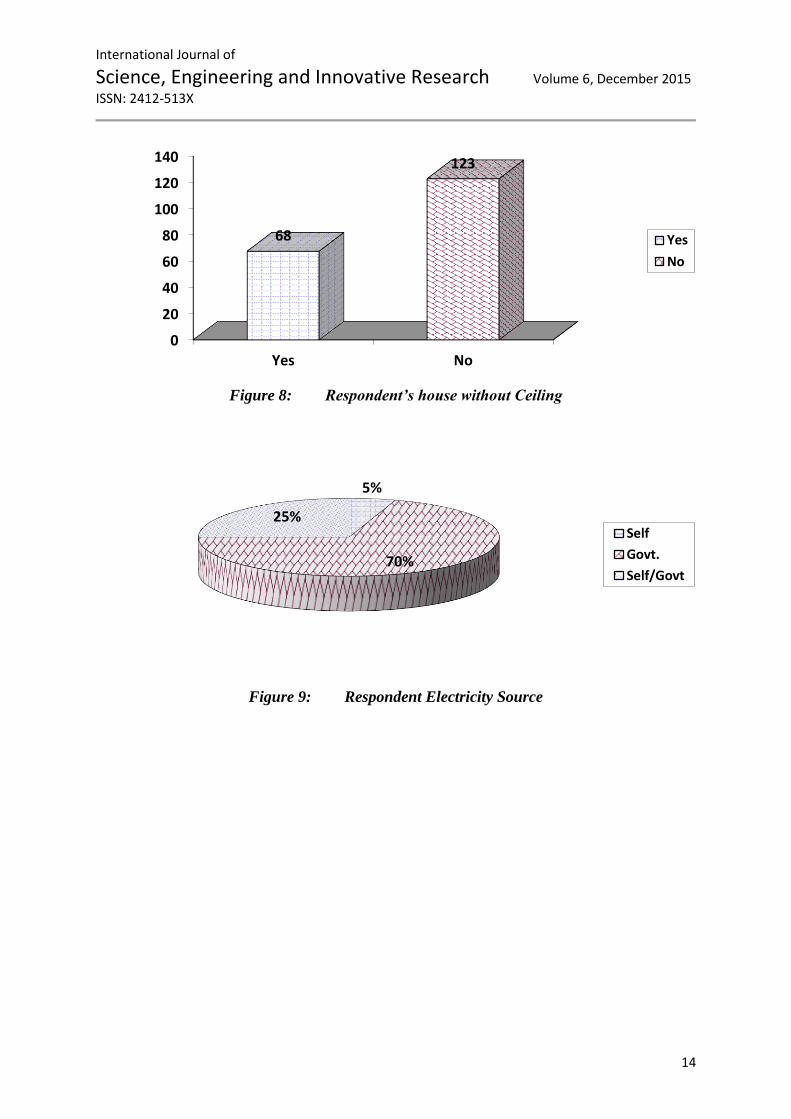
houses are with mud while 84% without mud. Figure 8 reveals that 68(35.6%) of the
respondents were with absent ceiling houses and 123(64.4%) were without absent ceiling.
Figure 9 shows that 70% of the respondents electricity source was from government, 25% were
both government and self powered and 5% were only self powered.

International Journal of
Science, Engineering and Innovative Research Volume 6, December 2015
ISSN: 2412-513X
11
Figure 1: Annual Episode of Malaria Attack
Figure 2: Type of Domestic and Drinkable water used by the respondents
0
10
20
30
40
50
60
70
None 1 time 2 times 3 times 4 times 5 times and above
Fre
qu
en
cy
0
20
40
60
80
100
120
140
160
Domestic Water Drinkable Water
WellBorehole

International Journal of
Science, Engineering and Innovative Research Volume 6, December 2015
ISSN: 2412-513X
12
Figure 4: Respondent’s Toilet Type
Figure 5: Respondent’s Water Drainage
75%
25%
Near
Far
0
20
40
60
80
100
120
Water Closet Pit Latrine Bush
102
5039
Water Closet
Pit Latrine
Bush
87%
13%
Open
Closed
Figure 3: Nearness of Respondent’s Disposable Site
International Journal of
Science, Engineering and Innovative Research Volume 6, December 2015
ISSN: 2412-513X
13
Figure 6: Respondent’s Building Type
Figure 7: Respondent’s House with mud Wall
0
20
40
60
80
100
120
140
Face-to-face Flat Duplex
137
49
5
Face-to-face
Flat
Duplex
16%
84%Yes
No
International Journal of
Science, Engineering and Innovative Research Volume 6, December 2015
ISSN: 2412-513X
14
Figure 8: Respondent’s house without Ceiling
Figure 9: Respondent Electricity Source
0
20
40
60
80
100
120
140
Yes No
68
123
Yes
No
5%
70%
25%Self
Govt.
Self/Govt
International Journal of
Science, Engineering and Innovative Research Volume 6, December 2015
ISSN: 2412-513X
15
Model Summary
Model R
R
Square
Adjusted R
Square
Std. Error of
the Estimate
Change Statistics
R Square Change F Change df1 df2 Sig. F Change
1 .571a .326 .277 2.163 .326 6.589 13 177 .000
a. Predictors: (Constant), Abse_Ceil_Yes, Age, Fem, Well1, Tiolet, Near, Mono, Open, Mud_No, Well2, No_HH,
Fam_Inc, Building
ANOVAb
Model Sum of Squares df Mean Square F Sig.
1 Regression 400.840 13 30.834 6.589 .000a
Residual 828.343 177 4.680
Total 1229.183 190
a. Predictors: (Constant), Abse_Ceil_Yes, Age, Fem, Well1, Tiolet, Near, Mono, Open, Mud_No, Well2, No_HH, Fam_Inc, Building
b. Dependent Variable: Episode
Coefficientsa
Model
Unstandardized Coefficients Standardized Coefficients
t Sig. B Std. Error Beta
1 (Constant) -1.792 1.499 -1.195 .234
Poly -.605 .494 -.119 -1.224 .223
Fam_Inc -.143 .161 -.090 -.890 .375
No_HH .238 .114 .191 2.094 .038
Male .009 .319 .002 .028 .978
Age .007 .009 .047 .739 .461
Far .968 .433 .165 2.233 .027
Toilet 1.165 .294 .364 3.966 .000
Closed -1.018 .816 -.135 -1.247 .214
Building 1.040 .300 .391 3.471 .001
Mud_Yes .590 .638 .085 .925 .356
Abse_Ceil_No 2.044 .415 .386 4.924 .000
Borehole2 -.103 .431 -.020 -.239 .811
Borehole1 -1.153 .445 -.194 -2.590 .010
a. Dependent Variable: Episode
3.2 Findings
International Journal of
Science, Engineering and Innovative Research Volume 6, December 2015
ISSN: 2412-513X
16
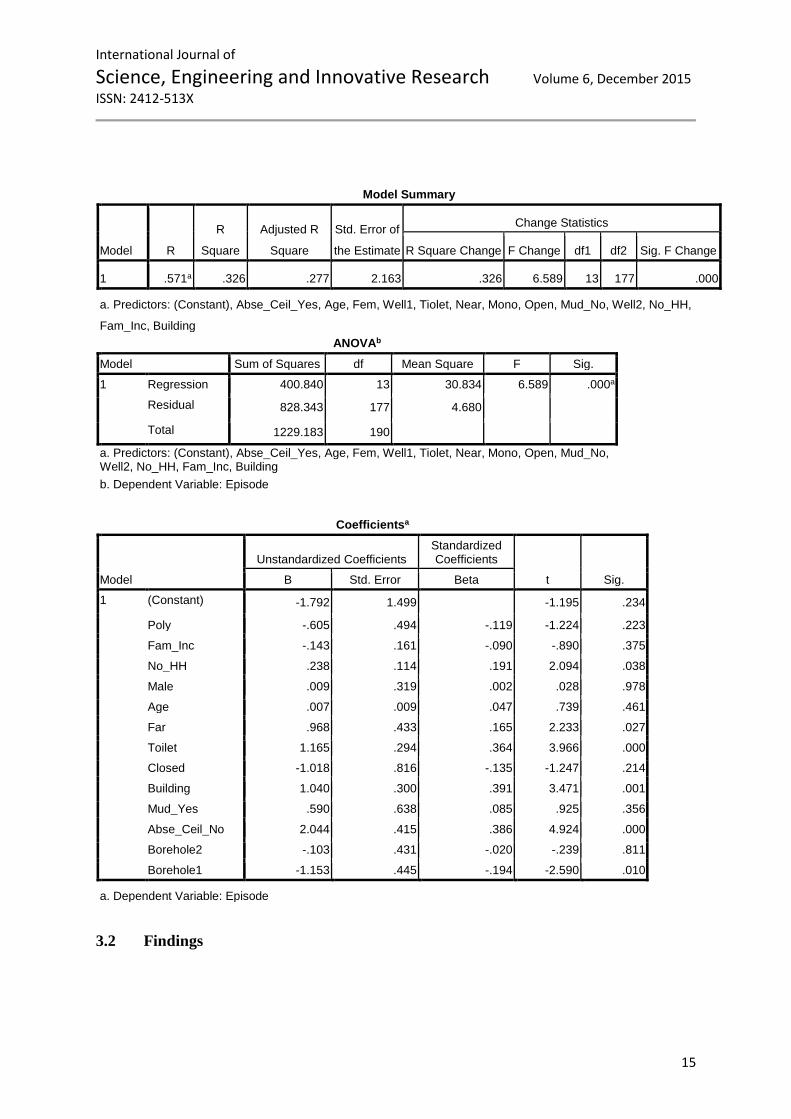
The R-squared is (0.326) indicating the factors considered could only explain 32.6% of the
causes of annual episode of malaria. The ANOVA indicating the combination of the factors
with F-value (6.589) was significant having p-value (0.0001).
The factors that were significantly influencing the annual episode of malaria include:
- Number of household member
- Disposable site
- Toilet type
- Building type
- Absence ceiling
- Source of domestic water
4 Discussion and Conclusion
The number of the household living together in the same house thus constitute high rate
of malaria for the members may be due to the fact that the belongs of the dwellers will be much
and that will serves as hidden place for the mosquitoes that gained access into the room.
Disposable site is another influencing factor which could be as a result in being near
the house. It will contribute towards high risk of insects leading to unhygienic environment.
The insects such mosquitoes will find their reservoir for surviving and breeding their new ones.
This is in line with Fobil et al. (2011) opined that hygiene, sanitation, and waste collection are
key determinants of malaria transmission which, while household responsibilities, have a
community-level effect on disease transmission. As an example, the more the households
dispose of waste properly, the lower the risk of liquid waste collecting in pools of stagnant
water and forming vector breeding sites. Another finding of Adeleke et al (2008) reported that
blockages are often due to poor sanitation and lead to reduced water flow and accumulation of
stagnant water pools which are ideal for mosquito breeding.
Toilet type was significantly associated with annual episode of malaria. This may be as
a result of dampness of the toilet facility available without being covered which can serve as a
reservoir/breeding site for mosquitoes causing malaria. This supported the finding of
Impoinvil, et al., (2008) reported that unused swimming pools were found to provide a
particularly productive habitat for Anopheles immature stages. Mourou et al. (2010) stated that
in Accra, Ghana, being connected to a toilet was found to be even more important than waste
removal in reducing community malaria mortality; however, toilets are also potential areas of

International Journal of
Science, Engineering and Innovative Research Volume 6, December 2015
ISSN: 2412-513X
17
mosquito activity, and septic tanks within communities are a potential source of vector
breeding sites.
Building type is an influencing factor of annual episode of malaria which shared the
same view with number of members of household.
Absence ceiling in a building is an affluence of annual episode of malaria. It
consequently create abode for mosquitoes in the house. Yamamoto et al. (2010) report that
houses with malaria-infected children are more likely to have mud walls, open eaves, and
absent ceilings.
Source of domestic water is an influencing factor of annual episode of malaria. The
study showed that the majority of the respondents depend on borehole which is not owned by
the household and this warrant them having more containers to reserve the water for domestic
use and consequently, it serves as mosquitoes reservoir. This finding supported report of
Keating et al., (2003) that artificial water storage containers can also serve as breeding sites,
and car washing has been found to provide excellent habitats for larval development.
Conclusively, study aimed at investigating significant factors influencing annual
episodes of malaria. Therefore, it concluded that female were prone to more episode of malaria
than male. Malaria episode was on increase among age 30years and above. Specifically, the
study discovered that factors like number of household member, Disposable site, Toilet type,
Building type, Absence ceiling and Source of domestic water are factors influencing factors of
annual episode of malaria which the stakeholder needs to work on.

International Journal of
Science, Engineering and Innovative Research Volume 6, December 2015
ISSN: 2412-513X
18
References
[1] Adeleke, M. A. Mafiana, C. F. Idowu, A. B. Adekunle, M. F.and Sam-Wobo S. O.,
(2008). “Mosquito larval habitats and public health implications in Abeokuta, Ogun
State, Nigeria,” Tanzania Journal of Health Research, vol. 10, no. 2, pp. 103–107
[2] Caraballo H (2013). "Emergency department management of mosquito-borne illness:
Malaria, dengue, and west nile virus". Emergency Medicine Practice 16 (5).
[3] Castro MC, Kanamori S, Kannady K, Mkude S, Killeen GF and Fillinger U (2010).
“The importance of drains for the larval development of lymphatic filariasis and malaria
vectors in dares salaam, United Republic of Tanzania,” PLoS Neglected Tropical
Diseases, vol. 4, no. 5, article e693
[4] Centre for Disease Control (CDC, 2010) Centers for Disease Control and Prevention
1600 Clifton Rd, MS A-06, Atlanta, GA 30333
[5] Federal Ministry of Health (FMOH, 2005). National Antimalarial Treatment Policy.
FMOH, National malaria and Vector Control Division, Abuja, Nigeria 2005
[6] Federal Ministry of Health (FMOH, 2009). Strategic Plan 2009-2013 "A Road Map for
Malaria Control in Nigeria. Nigeria and National Malaria Control Programme (NMCP).
Abuja, Nigeria. 2009.
[7] Fobil JN, Kraemer A, Meyer CG, et al. (2011). “Neighborhood urban environmental
quality conditions are likely to drive malaria and diarrhea mortality in Accra, Ghana,”
Journal of Environmental and Public Health, vol. 2011, Article ID 484010, 10 pages
[8] Freudenrich Craig, (2011). Mosquito Bites, Diseases and Protection. Discovery
Communication. http://www.animals.howstuffworks.com//
[9] Gbadegesin (2013) © Copyright 2004-2014 African Newspapers of Nigeria Plc | All
Rights Reserved | Site Designed by Tribune Web Team
[10] Hawley WA, Philips-Howard PA, ter Kuile FO (2003). “Community-wide effects of
permethrin-treated bed nets on child mortality and malaria morbidity in western
Kenya”. Amj. Trop. Med. Hyg. 68 (4 Suppl): 121-7, April.
[11] Himeidan YE and Rayah, E. E. A. (2008) “Role of some environmental factors on the
breeding activity of Anopheles arabiensis in New Halfa town, eastern Sudan,” Eastern
Mediterranean Health Journal, vol. 14, no. 2, pp. 252–259
[12] Impoinvil DE, Keating J, Mbogo CM, Potts MD, Chowdhury RR, and Beier JC, (2008).
“Abundance of immature Anopheles and culicines (Diptera: Culicidae) in different

International Journal of
Science, Engineering and Innovative Research Volume 6, December 2015
ISSN: 2412-513X
19
water body types in the urban environment of Malindi, Kenya,” Journal of Vector
Ecology, vol. 33, no. 1, pp. 107–116
[13] Jimoh A., Sofola O., Petu A., Okorosobo T. (2007). Quantifying the Economic Burden
of Malaria in Nigeria Using the Willingness to Pay Approach, Cost Effectiveness and
Resource Allocation 2007, 5:6doi:10.1186/1478-7547-5-6
[14] Keating J, Macintyre K, Mbogo C, et al. (2003). “A geographic sampling strategy for
studying relationships between human activity and malaria vectors in urban Africa,”
American Journal of Tropical Medicine and Hygiene, vol. 68, no. 3, pp. 357–365
[15] Kilama W., Ntoumi F. (2009). “Malaria: a research agenda for the eradication era”.
Lancet 374 (9700): 1480-2. http/linkinghub.elsevier.com. October.
[16] Klinkenberg, E. McCall, P. J Wilson, M. D. Amerasinghe, F. P. and Donnelly, M. J.
(2008). “Impact of urban agriculture on malaria vectors in Accra, Ghana,” Malaria
Journal, vol. 7, article 151.
[17] Mourou JR, Coffinet T, Jarjaval F, et al. (2010). “Malaria transmission and insecticide
resistance of Anopheles gambiae in Libreville and Port-Gentil, Gabon,” Malaria
Journal, vol. 9, no. 1, article 321.
[18] National Population Commission. Nigeria demographic and health survey. Federal
Republic of Nigeria Abuja, Nigeria. 2008
[19] Onwujekwe O., Chima R., Okonkwo P. (2000). Economic burden of malaria illness on
households versus that of all other illness episodes: a study in five malaria holo-endemic
Nigerian communities. Health Policy, 54 : 143-159
[20] Teklehaimanot A., Mejia P. Malaria and Poverty. Ann. N.Y. Acad. Sci. (2008). 1136:
32-37 New York Academy of Sciences. doi: 10.1196/annals.1425.037
[21] UNICEF, Nigeria (2009). Partnering to roll back malaria in Nigeria’s Bauchi State.
UNICEF At a glance: Nigeria.
[22] WHO (2004). Development of laboratory testing methods for malaria rapid diagnostic
tests. Report of the WHO informal consultation on laboratory methods for quality
assurance of malaria rapid diagnostic tests. Manila, World Organization Regional
Office for the Western Pacific, VOA News, July.
[23] WHO (2013). "World Malaria Report 2013". World Health Organization. Retrieved 13
February 2014.
[24] WHO (2014): "Executive summary and key points". World Malaria Report 2013.
World Health Organization. Retrieved 13 February 2013.
[25] Yamamoto S, Louis VR, Sié V and Sauerborn R (2010). “Household risk factors for
clinical malaria in a semi-urban area of Burkina Faso: a case-control study,”

International Journal of
Science, Engineering and Innovative Research Volume 6, December 2015
ISSN: 2412-513X
20
Transactions of the Royal Society of Tropical Medicine and Hygiene, vol. 104, no. 1,
pp. 61–65
Recommended

















