
www.wiser.pitt.edu
Simulating a Seamless Move.. Our Journey to Lawrenceville
Melinda F. Hamilton, MD, MSc, FAHA Assistant Professor of CCM & Pediatrics
Director, Pediatric Simulation Children’s Hospital of Pittsburgh of UPMC
Peter M. Winter Institute of Simulation ,Education, and Research
www.wiser.pitt.edu
Disclosures
• No conflicts of interest • Multiple people contributed to this talk!

www.wiser.pitt.edu
Overview
• Interesting information • How we utilized simulation in our move
– Plan our processes – Interrogate processes in place – Lessons learned
• Opportunities and surprises

www.wiser.pitt.edu
Early Simulation…
www.wiser.pitt.edu
INTERESTING STUFF…

www.wiser.pitt.edu
It takes a village…
• It takes a village to raise a child…. • African Proverb
• To move a tertiary care children’s hospital 2.5 miles, it takes – 300 staff – 40 CHP volunteers – 50 EMS/Police – 45 city ambulances – A whole lotta planning
www.wiser.pitt.edu
Let’s build it…
• Initial plans for new hospital began in 2001 • Team organized, met often
– Move coordinator – Medical equipment consultant – Nurse consultant – Data coordinator – Art consultant – Play/ Child Life consultant

www.wiser.pitt.edu
How do we do this?
• Actual move planning begins 2007 • Observation of other hospital moves
– Children’s Hospital of Denver – Adult facility in Los Angeles
• Consultant to move equipment • Simulation consultant for virtual move • Rental of beds, stretchers, ventilators • Organize ambulances, teams

www.wiser.pitt.edu
How do we keep track of patients?
• Patients with barcodes – Leaving unit in Oakland – Exiting building in Oakland – Entering building in Lawrenceville – Entering final destination
• Computer screen in command center with all patient locations via barcodes

www.wiser.pitt.edu
Let’s clear this place out!
• Empty the hospital… – Started with census of
250- panic! – Wednesday prior to
move, OR decreased by half
– Friday prior to move, only emergent OR
– Planned discharges day prior to move

www.wiser.pitt.edu
Up and Running… • New hospital
readiness… – OR in new facility ready
by 7am • Pump case and ECMO
ready
– ED open and fully staffed by 7am
– Beds in every room – Fully stocked hospital – Crisis team both sites

www.wiser.pitt.edu
Where did the hospital go? • One year prior to move start PR
– Office visits, letters sent
• 2 weeks prior to move – All patients and families admitted receive info – Community hospitals, maps, info to families – News and radio broadcasts
• Morning of move – Old signs covered and new ones uncovered – Police stationed at ED to direct
www.wiser.pitt.edu
What could go wrong?
• Things to consider… – Patients too sick to move? – Patient needing urgent OR? – Patient undergoing transplant?
• We have to make the move happen
www.wiser.pitt.edu
Children’s Hospital of Pittsburgh of UPMC-Oakland
www.wiser.pitt.edu
Children’s Hospital of Pittsburgh of UPMC-Lawrenceville

www.wiser.pitt.edu
SIMULATION

www.wiser.pitt.edu
Simulation Modeling • Complex
– Staff – Equipment- how many ventilators? – Patients – Ambulances – Elevators – Route
• How to evaluate the move strategies in advance?

www.wiser.pitt.edu
SIMUL8 • Simulation software company develops
computer modeling (www.simul8.com) • Prison System
– New sentencing system would cost taxpayers
• Manufacturing – Increase assembly line production
• Healthcare – Predict costs of treating obesity – Simulating a transplant center

www.wiser.pitt.edu
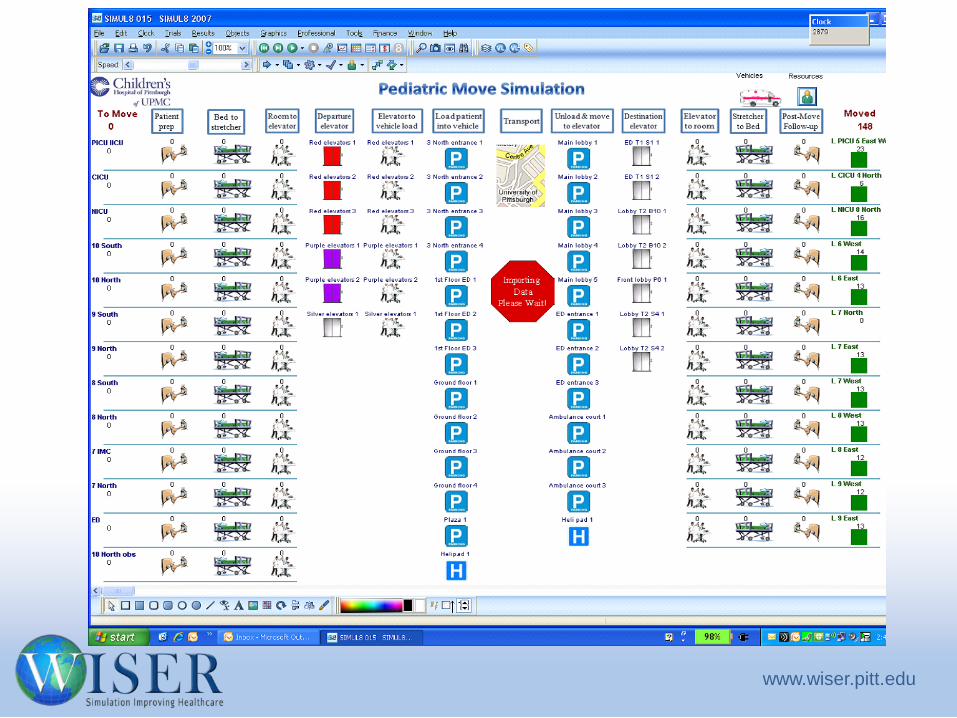
Simulation Modeling
• CHP Pediatric Move Simulation Project began 2 years in advance
• Mass evacuation model built for CHP • Allowed for extensive, interactive, move
analysis in advance • Multiple scenarios played out
– Time – Resources
www.wiser.pitt.edu

www.wiser.pitt.edu
Simulation
• All hospital staff had a 4 hr general orientation – Tour of hospital – Tour of “your space”
• Department specific orientation – Physicians handled via department – More in depth for those intimately involved in
move day

www.wiser.pitt.edu
Simulation
• Day in the Life Simulation Scenarios – Planned for all nursing, HUC, PCT staff in hospital – 12-16 hours in the new facility – Planned by nurse educators, advanced practice
nurses – Education Plan – Day in the Life Scenarios
www.wiser.pitt.edu
Day in the Life- PICU
• Education plan – Phone training
• New, with monitors alarming to phones
– Seek and find • Equipment, supplies
– Way finding • Where is radiation oncology?

www.wiser.pitt.edu
PICU- Day in the Life
• Your trauma patient is in cardiac arrest – Use wall button to call
for help – First nurse to locate
crash cart and bring to room
– Nurse 2 locate O neg blood and bring to room
– Meds from new cart
www.wiser.pitt.edu
Lessons learned
• This is a big ICU… – Can’t yell anymore…
• Alarm system was confusing • Within one month we had screens posted at all corners
of unit
– We needed 6 code carts, multiple airway bags, new line carts
– Maneuver around booms in room… – Lights were not bright enough…

www.wiser.pitt.edu
Day in the Life- PICU
• Your patient needs to go to MRI… – Find transport
equipment – Call staff for trip (doc,
RT) – Find correct elevator – Find MRI….

www.wiser.pitt.edu
Lessons Learned
• MRI not conducive to ICU monitoring – Miles of IV tubing – Arterial line monitoring “iffy” at best
• PICU and code team badges won’t work to enter MRI suite… – Tech has to open door and pull patient out of
scanner into back hallway

www.wiser.pitt.edu
Day in the Life – SDS and PACU
• Education Plan – Find your way around! – Phones – Monitors – Equipment

www.wiser.pitt.edu
Day in the Life-SDS and PACU
• Patient in recovery with respiratory distress – Alert anesthesia – Find BVM and airway
cart – Administer neb tx – Call PICU and arrange for
bed – Find transport monitor
and pack up pt
www.wiser.pitt.edu
Lessons Learned
• Locations of code carts, emergency equipment • Pyxis location, new phone numbers • OR was further away, more time for
anesthesia response

www.wiser.pitt.edu
Day in the Life- SDS
• 14 year old post-op from ACL repair – Ordered a post-op x-ray – Patient requires crutch
training- call physical therapy to arrange
– Patient with pain-request medication by calling CRNP
– Find med in pyxis and administer…

www.wiser.pitt.edu
Lessons Learned
• This is a really big place – Usual workload takes much more time… – Consider how to arrange equipment and supplies
for ease and efficiency – Routes (where is x-ray)
• Way finding • Maps, guides
www.wiser.pitt.edu
Day in the Life- Crisis Team
• Simulated mocks in every patient care area – Acute care – Intensive care units – Clinic areas – Non-clinical areas (cafeteria) – Not cardiac arrest or high fidelity
• Hypotension • Seizure
www.wiser.pitt.edu
Lessons Learned
• Much more space to cover – 25 to 52 code carts (and growing) – BVM in every room, hallways
• What are we going to do with adults? – Develop a process – Medications in code cart – Paperwork

www.wiser.pitt.edu
Lessons Learned
• Placement of carts and defibrillators • Emergency buttons on walls • Elevators and stairwells • Names of clinics- Alligator and Bear • Creation of the Super Cart • Standardize restocking and expiration process
for carts

www.wiser.pitt.edu
Opportunities
• Brand new code carts – Top two drawers locked – Medications alphabetically – Fluids added to cart – Airway bag implemented thruout hospital – Push-pull system assembly – Quick connect in all carts
• Equipment for education

www.wiser.pitt.edu
Simulation- just prior to move
• Table top move – Involved parties met in a
room – Role playing- simulated
the move through discussion
– Laid some ground rules • Those in t-shirts… leave
them be… • Only 2 people can stop
the move… • Once started, we have to
finish – Safety…

www.wiser.pitt.edu
Simulation-trial run • Simulated patient
moves – 2 simulated moves – 6 patients each – Ambulances, stretchers,
equipment – Elevators, routes
• Discoveries – Communication problem – Rented seat belts for
stretchers…

www.wiser.pitt.edu
How did it go? • Moved 152 patients in 6 hours and 19
minutes- SAFELY! – 2 patients transported on ECMO – 3rd ECMO pt cannulated 2 hrs after move – First OR pts 2 hours after move
• No adverse events… – Patient lost….just for a little bit – Trauma on helipad- delay red team move

www.wiser.pitt.edu
Happy Endings..
• Building of relationships within hospital – Pride – Teamwork – Responsibility – For our patients/families
• With our families – Pride
• Part of the move
– Family centered facility

www.wiser.pitt.edu
Thank you and Questions…

www.wiser.pitt.edu
Acknowledgments
• Jen Iagnemma, RN • Marnie Burkett, RN • Educators and staff of
SDS and PACU • Condition A/C Task
Force • Hundreds who made
the move happen
• WISER – Paul Phrampus, MD – Tom Dongilli – Jon Lutz – Jim Christman – Kevin Miracle, Max
Leake – John, Larry, Janell,
Marisa – Jen and Dan
Recommended

















