Screening and Best Practices in Screening and Best Practices in Treatment for Gambling DisorderTreatment for Gambling Disorder
Henry R. Lesieur, Ph.D., Psy.D.
Consultant
Pawtucket, Rhode Island
© 2014, Henry Lesieur, Ph.D.

TopicsTopics
Screening for Gambling and Gambling Disorder
Types of Gamblers and Problem GamblersBest Practices in Screening for GamblingScreening for Cognitive DistortionsBest Practices in Treatment for Gambling
Problems

Best Practices in ScreeningBest Practices in Screening
Need to use validated, reliable measure that have been validated by at least two different research groups
Short measures, while convenient, are less reliable than longer ones
Best screens have been translated into other languages and are used internationally
I searched PsychInfo and PubMed 2000-Jan.2014

Different Screens for Different Different Screens for Different PurposesPurposes
Not all screens are appropriate or accurate
What is gambling? – often assumed but there is a wide range
Best practice screens would define gambling for the person filling out the screen

Types of Gambling – LotteryTypes of Gambling – Lottery Lottery – (legal in colonial US and after civil war,
then illegal because of scandals in 1890; legal in1964 New Hampshire)
Weekly & daily lottery (numbers) – 1967-71 NY & NJ
Scratch tickets – 1974 Massachusetts Keno – 1988 New York Video lottery – 1989 South Dakota

Types of Gambling -- Types of Gambling -- Charitable Gambling Charitable Gambling Legal in colonial USSome outlawed after scandals but increased
after 1930sBingo – 1940sPull Tabs; scratch tickets; raffles; punch
boardsLas Vegas nites; carnival games

Types of Gambling – Types of Gambling – Pari-Mutuel WageringPari-Mutuel Wagering
Race tracks – big after civil war but corruption lead to outlaw (but legal in NY 1863 to today)
Wagering on greyhounds – 1922 FloridaPari-mutuel wagering – 1927 IllinoisJai Alai wagering – 1934 IllinoisRacetracks legal in only 6 states in 1930; 46
states in 2014

Types of Gambling – Pari-Types of Gambling – Pari-Mutuel Wagering (cont’d)Mutuel Wagering (cont’d)
Off-track wagering – 1971 New York Inter-track wagering – 1982 Colorado Racino – VLTs at race tracks – 1990 West
Virginia & Minnesota

Types of Gambling -- Types of Gambling -- CasinoCasino
Table games (banking games) – 1931 Nevada
Blackjack Roulette Craps Baccarat Wheel of fortune Keno
Pai Gow poker Caribbean, etc. poker Poker (non-banking)
Sports wagering – 1931 Nevada
Bookmakers predominate in US
Banking game = any gambling game in which bets are laid against the gambling house or the dealer

Cards and Competitive Cards and Competitive GamesGames
PokerGin RummyCrapsPool, Golf, Bowling, etc. for money

Types of GamblingTypes of Gambling Illegal gambling venues (illegal casinos and card
rooms) Numbers runners Bookmaker Illegally Appended Enterprises e.g. card rooms in clubs; bookmaker operates out
of bar; numbers in stores & bodegas; illegal gambling in bingo halls; grey machines in clubs & stores

Gambling in other VenuesGambling in other Venues
Stick dice & peach pits (historic Native American games)
Cockfights (legal in Puerto Rico)
Dog fights Pachinko (Japan)
Camel races (Turkey) Two-up (Australia) Mah-jong Con games (e.g. two
card monte) Stock speculation


Best Practice for Translation Best Practice for Translation of Screensof Screens
Translated and back-translated by an independent party
Different forms of gambling used in other culture are included in the screen (e.g. camel racing included in Turkish SOGS and pachinko included in Japanese version of SOGS)

Best Practices would take Best Practices would take Types Types of Gamblersof Gamblers into Account* into Account*
Casual Social gambler Serious Social gamblerProfessional gambler -- entrepreneur (bookmaker; casino, etc.) -- percentage player (poker) -- card counter (Blackjack) -- handicapper (horses, dogs, sports)
*Custer & Milt (1985); Lesieur & Custer, 1984)

Types of Gamblers Types of Gamblers (cont’d)(cont’d)
Antisocial Gambler – hustler; cheat; mechanic
Problem gambler – some problemsCompulsive, pathological, disordered
gambler (overlaps with professional and antisocial)
PGs show greater impulsivity and DSM disorders than professional gamblers.

Best Practices for Identifying Best Practices for Identifying Types of GamblersTypes of Gamblers
Current surveys do not identify antisocial or professional gamblers (may desire to do so in treatment)
Surveys look at “Non-problem,” “at risk,” and “problem gamblers”
Definitions of “at risk” and “problem” have not been standardized.
Best practice use standardized instruments or DSM criteria

InstrumentsInstruments South Oaks Gambling Screen (SOGS) DSM based instruments (e.g. NODS; DIS) Canadian Problem Gambling Index Problem Gambling Severity Index (PGSI) Lie/bet questionnaire GA-20 Questions

Adolescent ScreensAdolescent Screens
South Oaks Gambling Screen-RADSM-IV-J (Fisher)GA 20 QuestionsLie/Bet has been used with adolescents also

South Oaks Gambling Screen South Oaks Gambling Screen ((SOGSSOGS))
An easy to use paper and pencil screenScore of 0-2 = no problemScore of 3-4 = “Problem Gambler”Score of 5+ = “Probable Pathological
Gambler”Range = 0-20 – easy to scoreMost PG’s will score double digits.

Validated versions of Validated versions of SOGSSOGS
SOGS-R –past year SOGS-6 – past six months SOGS-3 – past 3 months SOGS has been validated in other languages
including multiple versions of Spanish, French (France & Canada), Portuguese (Portugal & Brazil, Chinese (US & China), Turkish, Vietnamese, Cambodian, Slovenian)

SOGSSOGS Translations Translations 46 languages so far (not all validated)46 languages so far (not all validated)
Africaans Arabic Bosnian Cambodian Chinese Croatian Czech Danish Dari Dutch English Estonian Farsi Finnish French German Greek Hebrew Hindi Hmong Hungarian Icelandic Inuktitut (Canadian North)
Italian Japanese Korean Laotian Lithuanian Macedonian Maori Norwegian Polish Portuguese Russian Samoan Sesotho Slovenian Somali Spanish Swedish Tagalog Thai Tongan Turkish Urdu Vietnamese Xhosa Zulu

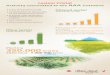
Avg. Lost, Borrowed & Stolen Avg. Lost, Borrowed & Stolen Lifetime by Lifetime by SOGSSOGS Score Score
176,170
89,76380,944
251,481
147,500
23,333
0
50,000
100,000
150,000
200,000
250,000
300,000
$$ Lost Debts Stolen
SOGS 10+
SOGS 5-9

Job Related Impacts by Job Related Impacts by SOGSSOGS Score (Percents) Score (Percents)
76
43
191220
36
614
01020304050607080
Lost Job Missedtime
# HrsMissed/
Mo.
Stole
SOGS 10+
SOGS 5-9

Suicidal Ideation of Pathological Suicidal Ideation of Pathological Gamblers by Gamblers by SOGSSOGS Score (Pct) Score (Pct)
76
1925
49
85
6
4444
0102030405060708090
SOGS 10+
SOGS 5-9

Concurrent validity
DSM-IV based measures – from US, Canada, New Zealand, UK, Spain
DSM5 Identifies 89 to 95% of
people in treatment for PG (higher than DSM-IV based measures)
Gambling frequency Hours gambled/month Hours gambled per
session Number of games
played Number of games
played weekly Time spent gambling

Correlates*Correlates* Gender M>F MS single>married Age under 30>over Earlier age of onset Minority group
member Not all studies: lower
income & education
Parental gambling & alcohol problems
SUD clients Prisoners Illegal activities Arrests High risk sex Impulsivity
*SOGS; DSM-based measures; and PGSI also correlated

Correlates - 2Correlates - 2
Impulsivity Irrational beliefs Depression Anxiety Poor coping skills
(avoidant & impulsive)
Psychiatric disorders Genetic risk factors
(studies based on SOGS & DSM-IV-based measures)
SOGS & DSM-IV (also DSM5) typically correlated with same measures

SOGSSOGS Modifications Modifications
Gambling type specific (e.g. Poker machines)
Brief SOGS
Short SOGS (SSOGS)
Cuestionario Breve de Juego Patologica (a short Spanish SOGS)
Best Practice is to use SOGS-lifetime; SOGS-R (past year); SOGS-6 (past 6 months); and SOGS-3 (past 3 months – used in evaluation research)

Clinical Barriers to Using the Clinical Barriers to Using the SOGSSOGS – Staff Non-Compliance – Staff Non-Compliance
Staff think gambling not consequential See Lottery ticket purchase as not possibly
problematic Think clients do not gamble that much Think it is too much work to screen Do not know what to do with gambler No clinical supervision SOGS scores higher among treatment staff

Critiques of the Critiques of the SOGSSOGS
Lifetime Measure is too inclusive – individuals with problems in the past but not the present are included
Solutions use current measuresSOGS-R (Volberg); SOGS-6; SOGS-3
(New Zealand) answer this criticism each has been validated internationally

Critiques of the Critiques of the SOGSSOGS - - 22
SOGS produces higher estimates of gambling problem than DSM-IV-based measures
A low false positive rate (e.g. 2-3% can be a problem in studies of large populations)
2% false positive can mean 200 out of 10,000 people in a survey.
DSM-IV – used a cutoff of 5+ DSM5 uses a cutoff of 4+ DSM5 will probably have rates that are closer to the
SOGS

Critiques of the Critiques of the SOGSSOGS - - 33
Some Australians would have us raise the cutoff for SOGS from 5+ to 10+ to reduce false positives
90% of individuals in gambling treatment in Ontario score 5+
Only 48.7% score 10+ The Australian strategy would be a serious error at
least in North American Australian Productivity Commission agreed Chinese researchers use SOGS-8

Critiques of the Critiques of the SOGSSOGS -- -- 44
SOGS overemphasizes borrowing – true but Critics solution is to replace specific forms of
borrowing with global borrowing questions – this is an error
Global borrowing questions fail to understand the context of gambling
Friends borrow from each other while gambling Bookmakers and casinos issue credit widely

Alternative MeasuresAlternative Measures
DSM-IV based measures DIS (DSM-IV based) NODS [NORC] CPGI + PGSI GA 20 Questions Lie/Bet Questionnaire Behavioral Markers
URICA IGS Cognitive Distortion
Measures Gambling Urge and
Cravings measures

National Opinion Research Center DSM-IV National Opinion Research Center DSM-IV
Screen for Gambling Problems Screen for Gambling Problems ((NODSNODS))
Developed for the US national survey Uses DSM-IV criteria Independently validated and reliable Validated in different languages Being used in epidemiological surveys and some
other gambling research Meets best practices criteria for use in
epidemiological surveys

Canadian Problem Gambling IndexCanadian Problem Gambling Index& Problem Gambling Severity Index& Problem Gambling Severity Index
CPGI – 31 questionsPGSI – 9 questions (part of the CPGI) Validated and reliable PGSI translations validated in at least 6 languages
in other countries Being used in epidemiological studies and some
other research Meets best practice criteria

20 Questions20 Questions
In use in Gamblers Anonymous since 1957 Available on many web sites (including
www.GamblersAnonymous.org) Validated against the SOGS and DSM-IV Score of 7 or more is indicative of a serious
gambling problem Translated into many languages and validated in
Spanish Meets Best Practice criteria

Lie/BetLie/Bet QuestionnaireQuestionnaire
Have you ever felt the need to bet more and more money? Have you ever had to lie to people important to you about
how much you gambled?
Validated by independent groups Translated and validated in other languages (e.g.
Portuguese and Norwegian) Best practice would be to use the Lie/Bet for quick
screening in doctor’s offices

Behavioral Markers at Behavioral Markers at https://bwin.comhttps://bwin.com
multiple platform gamblers who were identified by bwin.party’s Responsible Gambling (RG) program compared with randomly selected controls studied over a 30 day period
two high-risk groups (i.e., groups in which 90% of the members were identified by bwin.party’s RG program)

Behavioral MarkersBehavioral Markers1. engaged in three or more gambling
activities and evidenced high wager variability on casino-type games
2. Group 2 engaged in two different gambling activities and evidenced high variability for live action wagers
Behavioral Markers show promise in identifying PGs on Internet sites

Behavioral Markers – Behavioral Markers – Player Tracking CardsPlayer Tracking Cards
In use in Nova Scotia, Sweden, Norway & Australia Play Activity report Time & dollar limit setting Timeouts Current session feedback – time & dollars spent Risk Assessment BEST PRACTICE would make this available to
players on a voluntary basis

Adolescent Gambling ScreensAdolescent Gambling Screens
SOGS-RA Validated and reliable Validated by
Independent groups Translated into other
languages Validated in other
languages
DSM-IV-J Validated and reliable Validated by
independent groups Translated into other
languages Validated in other
languages
Both seem to meet Best Practice criteria; other screens need more research

Measures that Need Further TestingMeasures that Need Further Testing
3 validated measures MAGS – not indep.
validated Victorian Gambling
Screen – limited use; not translated
Eight Screen (NZ) –Not indep. validated; not translated
Behavioral Markers in casino settings

Measures Used During TreatmentMeasures Used During Treatment
Time Line follow back methodURICA for GamblingInventory of Gambling Situations (IGS)Measures of Cognitive DistortionsUrge and Cravings Measures

Time-line Follow-Back MethodTime-line Follow-Back Method
Use 1, 3 or 6-month calendarNote important dates (birthdays,
anniversaries, job changes, etc.)Ask about types of gambling on each dayEstimate $ lost

URICA for URICA for Gambling (Petry)Gambling (Petry)
32 items reflecting the four stages of change proposed by DiClemente and Prochaska
Validated by independent groupsNot translatedMore research need to meet Best Practice
criteria

Inventory of Gambling Inventory of Gambling Situations (IGS)Situations (IGS)
Used to find out potential sources of relapse in clients (may be useful for those less familiar with gambling)
Three different versionsLimited use in the literatureNot translatedNeeds further research to meet best practice
criteria

Measures of Cognitive Measures of Cognitive DistortionsDistortions
Gambling Related Cognitions Scale (GRCS)Gamblers’ Belief Questionnaire (GBQ)Gambling Attitude and Belief Survey (GABS)Other measures are too narrow (e.g. limited to
video machines)

What Cognitive Distortions are Measured?
Gambler’s Fallacy (the belief that after a string of one event, such as a coin landing heads, an alternative event, such as the coin landing tails, becomes more likely).
Illusion of control (perceiving more personal control over events than is warranted)
Beyond these two errors, there is scant consensus on relevant errors, and a wide variety has been studied
All measures are correlated with PG measures Sub-scales judged to assess gambler’s fallacy show
evidence of more robust effects sizes than those that assess illusion of control

Gambling Related Cognitions Scale (GRCS)Gambling Related Cognitions Scale (GRCS)
23 items on a 7 point scale Validated and reliable by independent research
groups Translated and validated in French, Chinese and
Spanish 5 subscales: Gambling expectancies; Illusion of control; Predictive control Inability to stop gambling; Interpretive bias The most widely used scale; meets Best Practice

Gamblers’ Belief Questionnaire (GBQ)Gamblers’ Belief Questionnaire (GBQ)
21 items measured on a 7 point scale
Validated and reliableValidated in Chinese by different research
groupPossibly meets Best Practice criteria but not
widely adopted

Gambling Attitude and Gambling Attitude and Belief Survey (GABSBelief Survey (GABS))
35 items on 4 point scale (3 items reverse scored)
Validated and reliableShorter version validated by independent
groupNot translatedNeeds more research to meet best practice
criteria

Measures of Gambling Measures of Gambling CravingsCravings
None meet Best Practice criteriaGambling Urge ScaleGambling Craving ScaleGambling Passion ScaleTemptations for Gambling QuestionnaireOther measures have been reported but
psychometrics not reported or poor

Gambling Urge Gambling Urge Scale (GUS)Scale (GUS)
6 item scale based on Alcohol Urge ScaleIndependently validatedTranslated into Chinese by the original
authorsNeeds further international research to meet
Best Practices criteria

Gambling Craving Gambling Craving Scale (GACS)Scale (GACS)
Several versions (e.g. Lori Rugle)One is validated (Young & Wohl, 2009) but
not by an independent groupNot translatedNeed more research to meet Best Practices
criteria

Gambling Passion ScaleGambling Passion Scale
10 items with 2 subscales Obsessive Passions; Harmonious Passions Valid and reliable Independently validated (but harmonious passion
positively r with PG rather than neg. in one study) Not translated Needs more research to meet Best Practices
criteria

Temptations for Gambling Temptations for Gambling QuestionnaireQuestionnaire
21 items with 4 subscales Negative Affect; Positive Mood/ Impulsivity;
Seeking wins or Money; Social Factors Valid and reliable Not independently validated and not translated Need more research to meet Best Practices
criteria

Gambling Self-Efficacy QuestionnaireGambling Self-Efficacy Questionnaire
Valid and reliableTranslated and validated in Spanish, Italian
but with at least one of the authors from the same group
Needs further research and totally independent validation to meet Best Practices criteria

Best Practices with Best Practices with Outcome MeasuresOutcome Measures
Need to use validated, reliable measure that has been validated by at least two different research groups
Best screens have been translated into other languages and are used internationally
Use Objective criteria to reduce therapist bias Best measures should be multidimensional (not
just abstinence but also includes a range)

The The Banff Alberta Consensus Banff Alberta Consensus for for Measuring Outcome – at minimum Measuring Outcome – at minimum
measures of gambling behavior - the net expenditure each month, the frequency (in days per month) with which gambling takes place, and the time spent thinking about or engaged in the pursuit of gambling each month
measures of the problems caused by gambling - especially problems in the areas of personal health, relationships, financial, and legal; these measures can be complemented by additional measures of quality of life
measures of the processes of change - whatever mechanisms of change are assumed to occur (e.g. changes in cognition)

Outcome MeasuresOutcome Measures Number of DSM criteria met (e.g. NODS) SOGS-6 month; SOGS-3 month PG-CGI (clinical global impression) PG-YBOCS (Yale-Brown Obsessive-
Compulsive Scale) G-SAS (Gambling Symptom Assessment Scale) 2 measures that are Multi-dimensional ASI-G (also called GSI) used with ASI GAMTOMS

PG-CGI (clinical global PG-CGI (clinical global impression)impression)
Widely used in Pharmacological research and research by MDs
Highly subjectiveNot possible to validate even though it is
used internationallyNot best practice

Yale-Brown Obsessive-Compulsive Scale – Gambling (PG-YBOCS)
YBOCS (internationally used measure for OCD) was modified for gambling
Used in many pharmacological studies and a few studies of psychological assessments by MDs
Validated and reliable Not validated by independent group Not translated Needs further research to meet best practice
criteria

PG-YBOCSPG-YBOCS10 items with 2 subscales: thoughts/urges and behavior10 items with 2 subscales: thoughts/urges and behavior
Gambling thoughts/Urges
1. Time occupied
2. Interference
3. Degree of Distress
4. Resistance
5. Degree of Control
Gambling Behavior
6. Time occupied
7. Interference
8. Degree of Distress
9. Resistance
10. Degree of Control

Gambling Symptom Gambling Symptom Assessment Scale (G-SAS)Assessment Scale (G-SAS)
Validated and reliableTranslated into other languagesUsed in drug treatment outcome studies
(not by psychologists); limited to past weekNot independently validatedNeeds further research to meet best practice

Gambling Symptom Assessment Gambling Symptom Assessment Scale (G-SAS) – past weekScale (G-SAS) – past week
Items 1-4: Focus on Urges
- strength
- frequency
- preoccupation
- degree of control
Items 5-7: Focus on thoughts about gambling
- frequency
- degree of control
Items 8 –12: Focus on Behaviors
- time spent on gambling
- excitement or pleasure before and after gambling
- emotional distress
- personal problems

Gambling Severity Index
Addition to the Addiction Severity Index Used with the ASI – multidimensional (medical;
employment/support; alcohol; drug use; legal; family/social; psychiatric
Independently developed and validated by two research groups
Used by other researchers but not translated Needs further research to meet best practice

Gambling Severity Index Gambling Severity Index in Past 30 Daysin Past 30 Days
Gambled more than could affordAny gambling at all$ spent per week on gambling# days experienced gambling problemsTroubled/bothered by gamblingHow important is gambling treatment at
present time

Multidimensional Batteries (e.g. used by Multidimensional Batteries (e.g. used by Minnesota group)Minnesota group)
abstinence rates (definition needs to be clear) gambling frequency (# days gambled in past 30 days) largest amount of money bet in one day gambling debt gambling-related financial problems work absenteeism arrests and legal status gambling problem recognition scale psychosocial functioning substance use frequency recovery attitude scale satisfaction with treatment post-treatment service utilization

GAMTOMS (Minnesota Group)GAMTOMS (Minnesota Group) (a) Gambling Treatment Admission
Questionnaire/Interview (GTAQ/GTAI) (b) Gambling Treatment Discharge
Questionnaire/Interview (GTDQ/ GTDI) (c) Gambling Treatment Services Questionnaire (GTSQ) (d) Gambling Treatment Follow-up
Questionnaire/Interview (GTFQ/GTFI). Has been validated and is reliable; Not validated by another research group Not translated

Best Practices will Take Known Facts Best Practices will Take Known Facts about Problem Gambling into Accountabout Problem Gambling into Account
Problem gambling is highest among minority groups (esp. Blacks, Hispanics, Asians, and Native Americans in the USA; immigrants in Europe)
Problem gambling is high among individuals employed in the gaming industry
Problem gambling is highest among arrested and incarcerated populations
Problem gambling rates are high among SUD and others with psychiatric diagnoses

Known Facts about Problem Gambling Known Facts about Problem Gambling (cont’d)(cont’d)
Rates of problem gambling are higher among youth and young adults than among older adults
Homeless (including homeless veterans) have higher rates than other adults

Predictors of Problem Predictors of Problem GamblingGambling
Impulsivity and ADHDGambling to relieve depression or anxietyPlaying multiple gamesGoing “on tilt” and lack of emotional
controlHigh levels of gambling-related cognitive
distortions

Natural RecoveryNatural Recovery Most problem gamblers recover on their own – numerous
surveys find that 33-82% of people with gambling problems do NOT have problems at the next survey
Twin registry survey in Australia – 82% who recovered did so without treatment
2 surveys: Among individuals with a lifetime history of DSM-IV pathological gambling, 36%-39% did not experience any gambling-related problems in the past year
2 surveys: only 7%-12% of PGs had ever sought treatment or attended GA

Natural RecoveryNatural Recovery Five long terms prospective studies in different
countries – rates are relatively stable but the people identified change
problem gambling appeared to be more transitory and episodic than enduring and chronic at the individual level; studies show instability and multidirectional courses in disordered gambling
Best Practice acknowledges that a combination of Progression, Reduction, Consistency and Non-linearity are found in the careers of people with gambling problems

Natural RecoveryNatural Recovery
Studies comparing Naturally Recovered (NR) gamblers with tx. seekers find NR quit by weighing pros and cons while tx seekers seek help because of consequences
Naturally recovered gamblers have less severe problems than those who go into treatment
BEST PRACTICE would address Natural Recovery

Why Not Seek Why Not Seek Treatment?Treatment?
Stigma (embarassment) – higher with older adults
Denial; Social factorsI can do it myself respondents who had numerous gambling
problems were more concerned about treatment costs, and the availability and effectiveness of treatment

Why Not Seek Treatment?Why Not Seek Treatment?
Study of Help-seekers (from helpline) and Non-help-seekers (from NZ survey)
pride (78% of HS participants, 84% of NHS participants), shame (73% of HS participants, 84% of NHS
participants) denial (87% of NHS participants) were most frequently
reported No other barrier was mentioned by >10% Another survey (in Ontario) found 49% of those with
serious PGSI identified PGs denied having a problem

Self-exclusionSelf-exclusion
Global Cash Access (casino cash machine self-exclusion)
http://www.gcainc.com/responsible-gaming/programs/
Exclusion from Internet Gambling siteshttp://www.betfilter.com/http://www.gamblock.com/index.html

Self-exclusion StudiesSelf-exclusion Studies N=161 (Quebec) followed at 6, 12, 18 and 24-months. 73% of the participants were DSM-IV pathological
gamblers urge to gamble, DSM score + negative consequences
reduced perception of control increased significantly for all
participants.
German study n=152 12 month follow-up Sig. improvement in psychosocial function
Similar but less systematic studies have been done on Internet self-exclusion

Self-exclusion – Part of Responsible Gaming Programs Self-exclusion programs are used by only a few
problem gamblers motivated by harms, evaluation/decision-making
(weighing pros & cons) and a wish to regain control
Some self-excluders reenter casinos However, self-exclusion is effective at reducing
harm

Problems with Self-exclusionProblems with Self-exclusion
Low publicityCan gamble in other venues unless
multiple venue banning on one application occurs
Inadequate venue monitoring for breaches of self-banning orders
Ideally should be able to ban without going to casino as well as in the casino

More successful Self-More successful Self-ExclusionExclusion
Linked self-excluder to treatment programs and provided other information
Improved programs include an initial voluntary evaluation, phone support, and a mandatory meeting if they wish to be taken off the list

Other Gambling-Based Other Gambling-Based Harm ReductionHarm Reduction
Use of Player tracking cards for self-monitoring; self-imposed limits on play (pre-commitment); few people use the cards
Changing machines to reduce PG Reduction of maximum bet levels has
been found to be the only modification likely to be effective as a harm minimization strategy for problem gamblers

Cooper’s Chat Room Cooper’s Chat Room StudyStudy
Studied 50 people going to GAwebAverage SOGS score was 1472% used the web site to avoid face-to-face
contact – STIGMA paramount80% eventually went to GACGHub had links to female gamblers’
rooms, local area sites, etc.

Safe Harbor Safe Harbor http://www.sfcghub.comhttp://www.sfcghub.com
http://compulsivegamblers.gotop100.com/

Chat Rooms with Chat Rooms with CounselorsCounselors
Australian study of email & chat rooms with professional counselors
Almost 70 % of people accessing these programs were seeking treatment for the first time
Email contacts significantly more likely to be new treatment seekers (78.0 %) compared with chat clients (68.1 %)

Values of Internet Treatment*Values of Internet Treatment*
Clients can use online programs when considering seeking help
while waiting for help services to be available as an adjunct to face-to-face therapy or following therapy for relapse prevention and ongoing
maintenance and support. The anonymous nature of online care enables clients to
test the service and come back at any stage or time without experience shame or guilt at previous failed attempts
* Monaghan & Blasczcynski (2009)

Criteria for Best Practices Criteria for Best Practices in Treatmentin Treatment
Pre-post test measurement; 6-months; 1 year or more follow-up
Experimental and control groups with randomized assignment
Independently validated results (need to have standardized treatment for this)
Treatment is used internationally

Empirically Validated Therapy Empirically Validated Therapy for Problem Gamblersfor Problem Gamblers
Self-Help ManualsMotivational InterviewingCognitive Behavioral TherapyRelapse PreventionGamblers Anonymous

Self-Help ManualsSelf-Help ManualsAustralia, New Zealand & CanadaAustralia, New Zealand & Canada

Self-Help ManualsSelf-Help Manuals
Typically include: self-assessment (e.g. SOGS, GA 20 questions)
Gambling Diary Goal Setting Triggers/High Risk Situations Gambling Cognitions Alternatives to Gambling Resources for further help (GA/treatment)

Self-Help Manual & InterviewSelf-Help Manual & Interview
In the first study done (Dickerson et al, 1990): 29 adults who responded to advertisements for help with
problem gambling received the manual with or without an initial in-depth interview
No difference between groups Both groups reduced the freq of gambling sessions, freq.
of overspending, and amount spent per week in the 6 mo after initial contact, but expenditure per session remained largely unchanged

Motivational InterviewingMotivational Interviewing
Numerous international studies (US, Canada, Sweden, have validated MI treatment for PG
Validated in randomized, control trialsTreatment effects are good at 24 monthsOne session of MI less gambling; money
spent; distress

Motivational Interviewing & Self-Motivational Interviewing & Self-HelpHelp (Hodgins, Currie & el-Guebaly)(Hodgins, Currie & el-Guebaly)
3 groups: wait-list control
self-help manual
manual & telephone motivational
interview 3 & 6 month – manual & MI better 12 month manual & MI -- 30% abstinent (59% improved) Manual only -- 21% abstinent (59% improved)

Empirically Validated Self-Help Empirically Validated Self-Help ManualsManuals
Your First Step To Change: Gambling N=315 (from newspaper & public ads) randomly assigned to: (a) a printed toolkit, (b) the toolkit and a brief guide to the toolkit’s content, or
(c) assignment to a wait‐list condition After 3 months sig. more toolkit recipients reported reduced
gambling and abstinence than controls
Online self-help guides (use CBT as guide)

Ontario Gambling Ontario Gambling Decisions (Robson et al)Decisions (Robson et al)Not abstinence oriented Uses Prochaska & DiClemente readiness to
change model with nurse practitioners Also used Social Learning theory, Motivational
Interviewing, & Social-Cognitive Model Severe PGs & those needing MH services not
included in the study 70-80% of mild-moderate problem gamblers
improved (26% abstinent)

Peersonalized normative feedback over the phone (comparing person with others who gamble)
no more effective than feedback on gambling

Brief Motivational InterviewingBrief Motivational Interviewing
Brief Motivational telephone interview plus self-help manual more effective than self-help manual alone (not sig. after 12 months but …
After 24 months, motivational intervention group gambled fewer days, lost less money, and had lower South Oaks Gambling Screen scores. They were more likely to be categorized as improved compared with the self-help workbook only group
However, both groups improved

Some Data to Use in MISome Data to Use in MI
Estimated readiness for change Less than 2% of the US adult population scores 5 or more
on the SOGS in their lifetime Money and escape are more common motivations among
problem gamblers than among non-PGs Increase in frequency of gambling associated with PG Increased in cognitive distortions associated with PG (can
use GABS or GBQ) Go over scored SOGS questions answered in PG direction
and note that non-PG answer “No.”

Varieties of CBTVarieties of CBT
Imaginal DesensitizationExposure & Response Prevention (either in
vivo or to triggers [cue exposure])Cognitive Therapy (focus on changing
thinking only)Cognitive Behavioral Therapy (combines
cognitive and behavioral change)

Imaginal DesensitizationImaginal Desensitization
Relaxation is taught firstExposure to gambling images is continued
until saturation and relaxation inducedExposure to triggers and arousal to scenes of
gamblingEffective after long follow-up (2 to 9 yrs)Recording of the procedure designed for
home use also found effective

Imaginal Desensitization (ID)Imaginal Desensitization (ID)
EMDR and Hypnosis have been used with ID but have not been experimentally evaluated
Needs research

Exposure & Response Prevention Exposure & Response Prevention (ERP)(ERP)
Included in international treatment programs (esp. Australia & Spain)
Positive results in both individual and group settings but can have high dropout rate
Brief exposure increases cravings so exposure need to be longer than single session
Caution but meets Best Practice

Cognitive TreatmentCognitive Treatment
Ladouceur & Colleagues (2001)A focus on randomness is very effective
when compared to controlsErroneous beliefs about chance, luck, skill
and randomness were challenged
Petry – CBT > GA alone but effectiveness increases when GA added

CBT (Ladouceur)CBT (Ladouceur) (a) cognitive correction of erroneous perceptions
about gambling (b) problem-solving training (c) social skills training (d) relapse prevention Successful but almost half dropped out of
treatment Effective with adolescents (small sample)

Petry CBT units (modeled after Petry CBT units (modeled after SUD CBT treatment)SUD CBT treatment)
Start with Triggers Functional analysis (thoughts, feelings & situations gambling) Increase pleasant activities Self-management planning Coping with cravings and urges to gamble Assertive Skills and Gambling Refusal Training Correcting Irrational Thinking Planning for Emergencies and Coping with Lapses Financial Planning and Dealing with Creditors Termination

Varieties of CBT Varieties of CBT
Randomized control studies (Cochrane Reviews) CBT is Effective in both individual and group therapy (research conducted in Canada, US, Australia, Spain & Norway)
CBT is effective in treating both men & women “Node-link mapping” CBT effective Short term CBT is effective at reducing problems
(small effect) Meets Best Practice criteria

MI and CBT combinedMI and CBT combined
Effective in both individual and group formats MI & Imaginal desensitization Study of Brief (1 session) MI or Brief MI & 3
sessions of CBT; vs. 10 min. brief advice Brief advice assoc. with reduced gambling but
surpassed after 6 weeks by MI plus CBT in effect Study of Brief MI (1 session) vs. CBT (3-4
sessions) – both reduced DSM criteria and gambling consequences

Imaginal Desensitization and Imaginal Desensitization and Motivational InterviewingMotivational Interviewing
68 PG assigned to either IDMI or GAPeople who failed to respond to GA were
given IDMIHigh rate of abstinence following tx.Some reduction in effect but significant
reductions in PG-YBOCS maintained after 6 months

Combined CBTCombined CBT
Manualized treatment combined CBT, MI and Imaginal Exposure in South Africa
Significant reductions in PG-YBOCS andSheehan Disability Scale (SDS) after
treatment ended

Combined CBTCombined CBT(study of 56 females)(study of 56 females)
Compared Individual and Group Therapy financial limit setting, alternative activity planning cognitive correction, problem solving communication training relapse prevention imaginal desensitisation
Individual therapy (92% no longer met DSM criteria) more effective than group (60% no longer met DSM criteria) at 6 month follow-up

Combined CBT & ERPCombined CBT & ERP
CBT alone was as effective as combination of CBT & ERP in one study but not in another
Dropout rate was higher with CBT + ERP (Spain) Combined approach is in use in Australia where
dropout rate is lower than Spain

Gamblers AnonymousGamblers Anonymous
Eight sessions of CBT compared with eight sessions of twelve-step facilitation (TSF) based on the first five steps of GA – both equally effective
“Node-linked” CBT & TSF equally effective IDMI more effective than GA (IDMI effective
after GA failure) When GA added to CBT, effect improves (several
studies)

Help to Significant OthersHelp to Significant Others
Community Reinforcement and Family Therapy (CRAFT) model modified PG sig. others workbook
3 groups: (1) workbook only; (2) workbook plus telephone support; (3) control--treatment resource book
Groups 1 & 2 reduced days gambling, inc. satisfaction with the program, and number who had their needs met; no dif. in % seeking treatment

Help to Significant Help to Significant Others 2Others 2
Second study reported on Coping Skills Training for sig others
CST vs. wait list controls CST improved coping skills and large significant
reduction in depression and anxiety Partner gambling reduced for both groups However, other studies point to beneficial effect of
social support in treatment outcome for PGs

Predictors of Dropout and Predictors of Dropout and RelapseRelapse
Dropout Impulsivity (not all
studies) Self-regulatory
impairments Sensation seeking
traits Cluster B personality
disorder
Relapse lack of social support* Psych. Distress Problem severity* Gambling urges& Cluster B personality
disorder* Stress reactivity
*Supported by more than one study

Introduce the TurtleIntroduce the Turtle
Stop BreatheThinkDecideresisting urge to gamble: delay 15
minutes (think of a turtle) think of eight alternative options

Some Differences in the Basic Some Differences in the Basic CBT ModelCBT Model
Motivational interviewing -- Join with the patient – Discuss stages of change and find ambivalence
Costs-Benefits Triggers Experience Cycle Leisure Activities

Differences in Basic Differences in Basic CBT Model (cont’d)CBT Model (cont’d)
Randomness, randomness, randomness Safe@Play (for slots players and as relapse
prevention) Gambling specific cognitive distortions – use
GABS, T-BAGS, etc. (zero in on their gambling preferences)
Relapse prevention– Planning, planning, planning
Schema questionnaire and schema focused therapy

Relapse Relapse PreventionPrevention
Review triggersEmphasize cues to potential relapseDiscuss high risk situationsDevelop specific means to deal with each
situationErect Barriers to relapse

Imaginal Desensitization Imaginal Desensitization to Gambling Triggersto Gambling Triggers
Teach person progessive muscle relaxation Have person imagine cues to gambling Suggest that time has passed and that s/he should
notice changes in the body; record arousal on a scale from 1 to 10
Continue this until the person notices an increase and then a reduction in arousal
Keep going until arousal has ceased or reduced considerably

Addiction-Based Addiction-Based TreatmentTreatment
Abstinence FocusedNo control trialsMethod of treatment ranges widelyOften involve individual and group therapy-- Need systematic evaluation of indiv. vs.
group vs. combination-- Need evaluation of Modules

Face-to-Face Face-to-Face Treatment PathwayTreatment Pathway
Psychodynamic Therapy has been examined in 6 different trials and found effective but there were no control groups
Needs further research to meet Best Practice criteria

Face-to-Face vs.TelephoneFace-to-Face vs.Telephone
Face-to-Face vs. Telephone – no sig. difference between them in total hours, money and proportion of income spent on gambling, and the gambling attitudes and beliefs scores (no controls)
No controlled studies; internationally done but studies not the same
Probably useful for those without access to face-to-face tx. (e.g. rural areas)

Telephone TreatmentTelephone Treatment
Six 1-hr long telephone-delivered sessions conducted by a mental health provider using a translated version (Chinese) of the Freedom from Problem Gambling Self-Help Workbook (California)
majority of clients who enrolled into the program did not report any gambling behavior after baseline and improved on self-reported measures of overall life satisfaction, gambling urges, and self-control

Internet TreatmentInternet Treatment Accessibile, Convenient, Cost-effective,
Anonymous and Private Useful for: online gamblers, rural populations,
disabled populations, socially phobic populations “Internet is an effective medium for the delivery
of health-related information, self-assessment, counseling, peer-based support and other therapeutic interventions”
No control group
* Gainsbury & Blaszczynski International Gambling Studies, Vol 11(3), Dec 2011

Internet Based TreatmentInternet Based Treatment Internet & Telephone MI and CBT (Sweden) –
n=66 pre-post but no control showed moderate or large improvements in gambling, anxiety and depression after 36 months
Internet & telephone (Norway) – pre-post but no control; significant reductions in the scores of pathological gambling, anxiety, and depression maintained over 36 months (n= 284 no control group)
CBT (Finnish study) N=224 treatment completers; Reduced gambling urge, impaired control, cognitive distortions, alcohol use, and depression
Online self-guided treatments are also available

Swedish ICBT components
Four MI sessions based on manualized treatment from Ladouceur and others
Includes decisions about gambling; open-ended questions evoking talk of change; suggestions to get input from relatives
Readings and completed assignments posted and looked at online
Weekly 15 minute telephone contacts (4 weeks)

Norwegian study ICBT components
There are nine assignments that include: - Motivation / goals - Readiness to change (the stages) - Analyzing gambling situations - High-risk situations / identifying automatic erroneous
thoughts - Flashcard & notebook (self-help tools used in
treatment) - Financial situation and challenges - Relationship, trust/honesty

Pharmacological Treatment – Pharmacological Treatment – Placebo control studiesPlacebo control studies
Naltrexone & nalmefene (opioid agonists) – controlled studies (higher doses had intolerable side effects)
mostly supportive but not all studies; one study found positive family history of alcoholism predicted favorable response to agonists; one study found no effect for nalmefene
Paroxetine (Paxil) controlled study -- results not significant in two studies; sig in one but 2-month outcome measure
There is a strong placebo effect especially in the first 8-12 weeks

Pharmacological Treatment – Pharmacological Treatment – Placebo control studiesPlacebo control studies
Buproprion (Wellbutrin) –results not significant in one study sig. in another
Olanzepine –negative results Topirate (Topamax) anticonvulsant –
randomized, double-blind comparison with fluvoxamine (Luvox) – both effective at 3 months; not effective in another study
Fluvoxamine (Luvox) – not significant

Pharmacological TreatmentPharmacological Treatment
Nefazodone (Serzone) – open label Escitalopram (Lexapro) – open label N-acetyl cysteine (amino acid) open label Carbamazepine – open label Tocalpone (a COMT inhibitor) – open label enzyme catechol-O-methyltransferase (COMT)
is responsible for degradation of dopamine No controls

Pharmacological TreatmentPharmacological Treatment
Meta-analysis (Pallesen et al., 2007) 16 studies. A total of 597 subjects were included pharmacological interventions were more effective than no
treatment/placebo
Meta-Analysis (Bartley & Bloch, 2013) concluded that there is not enough data to support pharmacological treatments for PG
Meta-analysis included 14 rigorously conducted trials involving 1024 participants

Pharmacological TreatmentPharmacological Treatment
Review of 18 double-blind, placebo-controlled pharmacotherapy studies (Grant et al, 2012)
Opioid antagonists and glutaminergic agents effective in reducing cravings in PGs
Other reviewers agree on efficacy of opioid antagonists for PG
Studies of dual diagnosis will be discussed in another presentation

Pharm. vs. CBT
Meta-analysis of randomized control group studies
Pharm high effect sizes at end of intervention (no data for long term)
CBT high effect sizes after long term (M=14 months) followup
CBT more effective than pharm. treatment

Combined Treatments
CBT plus SSRI vs. CBT + placebo vs. SSRI aloneCombination patients improved faster
than CBT or SSRI aloneNot independently validated

Promising Therapies Needing Promising Therapies Needing Further ValidationFurther Validation
Self-exclusionInternet based CBT and minimal
telephone based treatmentInternet based CBTDBT with treatment resistant PGs

Best Practice in Treating PGsBest Practice in Treating PGs

Further InformationFurther Information
Henry R. Lesieur, Psy.D., Ph.D.Pawtucket, RI
Tel: (401) 727-4748Cell: (347) 410-2902
Copyright, 2014, Henry R. Lesieur. No part of this Copyright, 2014, Henry R. Lesieur. No part of this presentation can be copied without expressed presentation can be copied without expressed permission of Dr. Lesieur.permission of Dr. Lesieur.
Recommended