
22/11/2017
1
PERIOPERATIVE MEDICINE IN
PRIVATE PRACTICE
“A LOCAL RESPONSE TO A
LOCAL NEED”
Dr Prakash NayagamMBBS (Hons), MRCP (UK), FRACP.
Physician
Gunnamatta Beach, VictoriaGunnamatta Beach, VictoriaGunnamatta Beach, VictoriaGunnamatta Beach, Victoria
22/11/2017
2
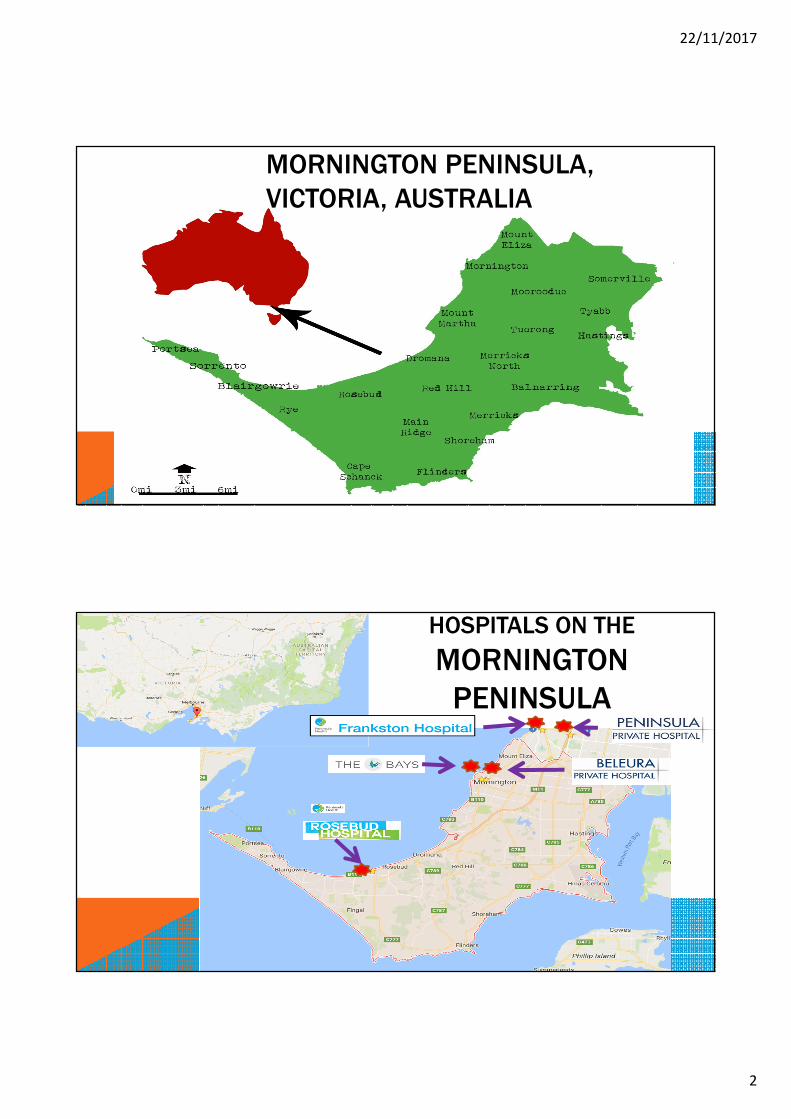
MORNINGTON PENINSULA,
VICTORIA, AUSTRALIA
HOSPITALS ON THE
MORNINGTON
PENINSULA

22/11/2017
3
2011 census2011 census2011 census2011 census
Cardiovascular Cardiovascular Cardiovascular Cardiovascular diseasediseasediseasedisease
�AF/CCF/PPM/ICD
�CAGS
GORD, OSAGORD, OSAGORD, OSAGORD, OSA
StrokeStrokeStrokeStroke
Renal FailureRenal FailureRenal FailureRenal Failure
DiabetesDiabetesDiabetesDiabetes
DementiaDementiaDementiaDementia
PolypharmacyPolypharmacyPolypharmacyPolypharmacy
CancerCancerCancerCancer
CO MORBIDITIES WITH AGEING

22/11/2017
4
HOSPITAL DEMOGRAPHICSHospitalHospitalHospitalHospital BedsBedsBedsBeds Operating Operating Operating Operating
TheatreTheatreTheatreTheatre
Emergency Emergency Emergency Emergency
DeptDeptDeptDept
ICU BedsICU BedsICU BedsICU Beds HDU BedsHDU BedsHDU BedsHDU Beds
Public-
Frankston
454 5 34 10
Public- Rosebud 60 1 9
Private
Ramsay-
Peninsula
253 6+1 Cath Lab 14 10 4
Private
Ramsay-
Beleura
157 4 + 1 Cath Lab 6
Private –
The Bays
109 5 5
PRIVATE SECTOR PROFILE
Number of Operations Per yearNumber of Operations Per yearNumber of Operations Per yearNumber of Operations Per year
Peninsula Private 12,000
Beleura 6,000
The Bays 9,800

22/11/2017
5
GeneralGeneralGeneralGeneral
OrthopaedicsOrthopaedicsOrthopaedicsOrthopaedics
UrologyUrologyUrologyUrology
VascularVascularVascularVascular
BreastBreastBreastBreast
ENTENTENTENT
DentalDentalDentalDental
OroOroOroOro----MaxillaryMaxillaryMaxillaryMaxillary
OGD/ColonoscopyOGD/ColonoscopyOGD/ColonoscopyOGD/Colonoscopy
BronchoscopyBronchoscopyBronchoscopyBronchoscopy
PlasticsPlasticsPlasticsPlastics
TYPES OF SURGERY
PERIOPERATIVE MORBIDITY“Near Misses” due to inadequate pre“Near Misses” due to inadequate pre“Near Misses” due to inadequate pre“Near Misses” due to inadequate pre----op op op op assessment and poor postassessment and poor postassessment and poor postassessment and poor post----op op op op cocococo----ordination.ordination.ordination.ordination.
Highlighted by HDU Nursing Staff initiallyHighlighted by HDU Nursing Staff initiallyHighlighted by HDU Nursing Staff initiallyHighlighted by HDU Nursing Staff initially
Led to………………..Led to………………..Led to………………..Led to………………..

22/11/2017
6
SurgeonsSurgeonsSurgeonsSurgeons
AnaesthetistsAnaesthetistsAnaesthetistsAnaesthetists
PhysiciansPhysiciansPhysiciansPhysicians
Nursing StaffNursing StaffNursing StaffNursing Staff
Hospital AdminHospital AdminHospital AdminHospital Admin
Well attended Well attended Well attended Well attended
----weekday eveningweekday eveningweekday eveningweekday evening
hosted by one of the hosted by one of the hosted by one of the hosted by one of the
private hospitalsprivate hospitalsprivate hospitalsprivate hospitals
Attendance over 50Attendance over 50Attendance over 50Attendance over 50
From this group of 50…..From this group of 50…..From this group of 50…..From this group of 50…..
CONVENING OF A GENERAL MEETING
Chairman (Physician)Chairman (Physician)Chairman (Physician)Chairman (Physician)
SurgeonSurgeonSurgeonSurgeon�Orthopaedic (1)� Vascular (1)�General (1)�Plastic (1)�Urology (1)�Gynaecology (1)
Anaesthetist (2)Anaesthetist (2)Anaesthetist (2)Anaesthetist (2)
Cardiologist (1)Cardiologist (1)Cardiologist (1)Cardiologist (1)
Gastroenterologist (1)Gastroenterologist (1)Gastroenterologist (1)Gastroenterologist (1)
CEO (3)CEO (3)CEO (3)CEO (3)
DON (3)DON (3)DON (3)DON (3)
WORKING PARTY ESTABLISHED
3x two hour meetings
17 attendees in all

22/11/2017
7
WHERE TO NOW?
Seaford Seaford Seaford Seaford Pier, Pier, Pier, Pier, VictoriaVictoriaVictoriaVictoria
ENHANCING PERI-OPERATIVE
CARE IN THE PRIVATE HOSPITALS ON THE
MORNINGTON PENINSULA, VICTORIA
A Working Party A Working Party A Working Party A Working Party
DocumentDocumentDocumentDocument
May 2011May 2011May 2011May 2011

22/11/2017
8
RECOMMENDATIONS OF
WORKING PARTYApproved by MAC’sApproved by MAC’sApproved by MAC’sApproved by MAC’s
& widely distributed & widely distributed & widely distributed & widely distributed
to to to to Medical, Nursing, Allied Health Medical, Nursing, Allied Health Medical, Nursing, Allied Health Medical, Nursing, Allied Health and Hospital Administrations and Hospital Administrations and Hospital Administrations and Hospital Administrations of all 3 private hospitalsof all 3 private hospitalsof all 3 private hospitalsof all 3 private hospitals
PRE-OPERATIVE RECOMMENDATIONSPreamblePreamblePreamblePreamble�Inadequate pre op assessment of elderly, multiple co-morbidities
�Early recognition ensures comprehensive assessment prior to surgery
�Optimize unstable medical condition�Decision re private vs public, ICU back up etc.
22/11/2017
9
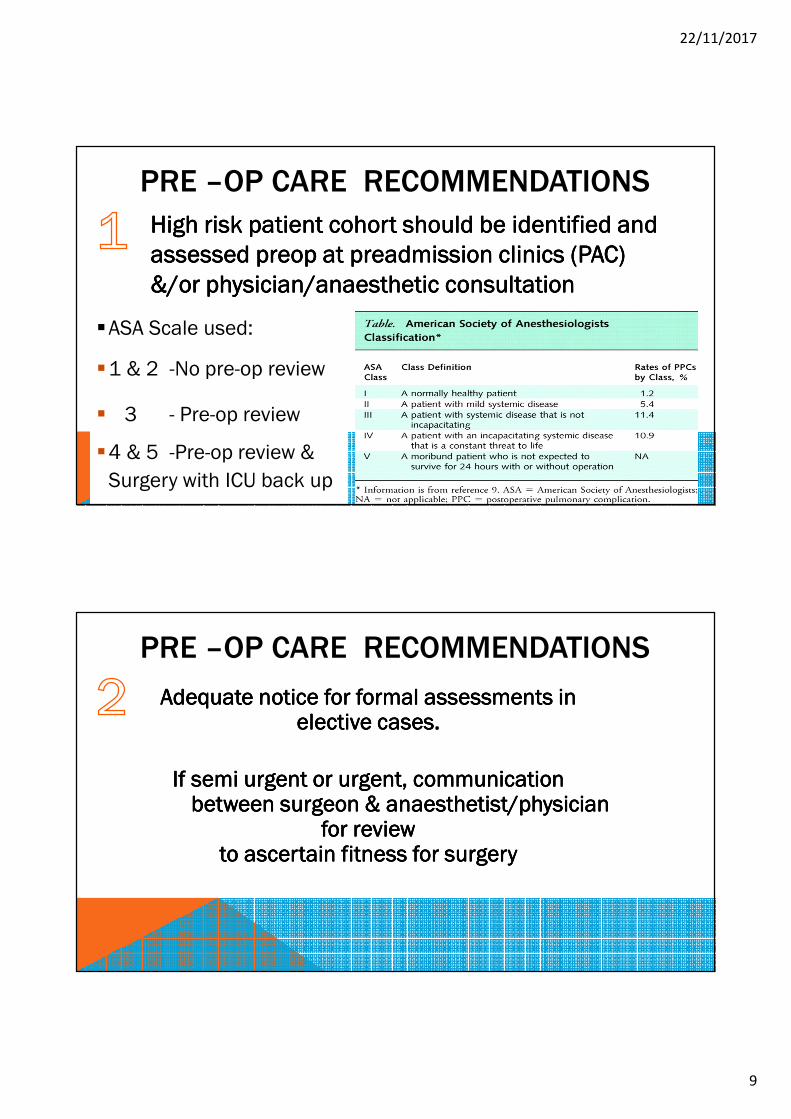
PRE –OP CARE RECOMMENDATIONS
High risk patient cohort should be identified and High risk patient cohort should be identified and High risk patient cohort should be identified and High risk patient cohort should be identified and
assessed preop at preadmission clinics (PAC) assessed preop at preadmission clinics (PAC) assessed preop at preadmission clinics (PAC) assessed preop at preadmission clinics (PAC)
&/or physician/anaesthetic consultation&/or physician/anaesthetic consultation&/or physician/anaesthetic consultation&/or physician/anaesthetic consultation
�ASA Scale used:
�1 & 2 -No pre-op review
� 3 - Pre-op review
�4 & 5 -Pre-op review &
Surgery with ICU back up
Adequate notice for formal assessments in Adequate notice for formal assessments in Adequate notice for formal assessments in Adequate notice for formal assessments in elective cases. elective cases. elective cases. elective cases.
If semi urgent or urgent, communication If semi urgent or urgent, communication If semi urgent or urgent, communication If semi urgent or urgent, communication between surgeon & anaesthetist/physician between surgeon & anaesthetist/physician between surgeon & anaesthetist/physician between surgeon & anaesthetist/physician
for review for review for review for review to ascertain fitness for surgeryto ascertain fitness for surgeryto ascertain fitness for surgeryto ascertain fitness for surgery
PRE –OP CARE RECOMMENDATIONS

22/11/2017
10
PRE –OP CARE RECOMMENDATIONS
Avoid Sunday Admissions for review before Avoid Sunday Admissions for review before Avoid Sunday Admissions for review before Avoid Sunday Admissions for review before
Monday surgery if in ASA 3Monday surgery if in ASA 3Monday surgery if in ASA 3Monday surgery if in ASA 3----5555
PRE –OP CARE RECOMMENDATIONS
Pre Pre Pre Pre Admission Admission Admission Admission clinicsclinicsclinicsclinics
Surgeons encouraged to refer to PACs when Surgeons encouraged to refer to PACs when Surgeons encouraged to refer to PACs when Surgeons encouraged to refer to PACs when feasible; feasible; feasible; feasible;
or provide results of investigations/previous or provide results of investigations/previous or provide results of investigations/previous or provide results of investigations/previous assessments so that they are available at time of assessments so that they are available at time of assessments so that they are available at time of assessments so that they are available at time of
surgerysurgerysurgerysurgery
22/11/2017
11
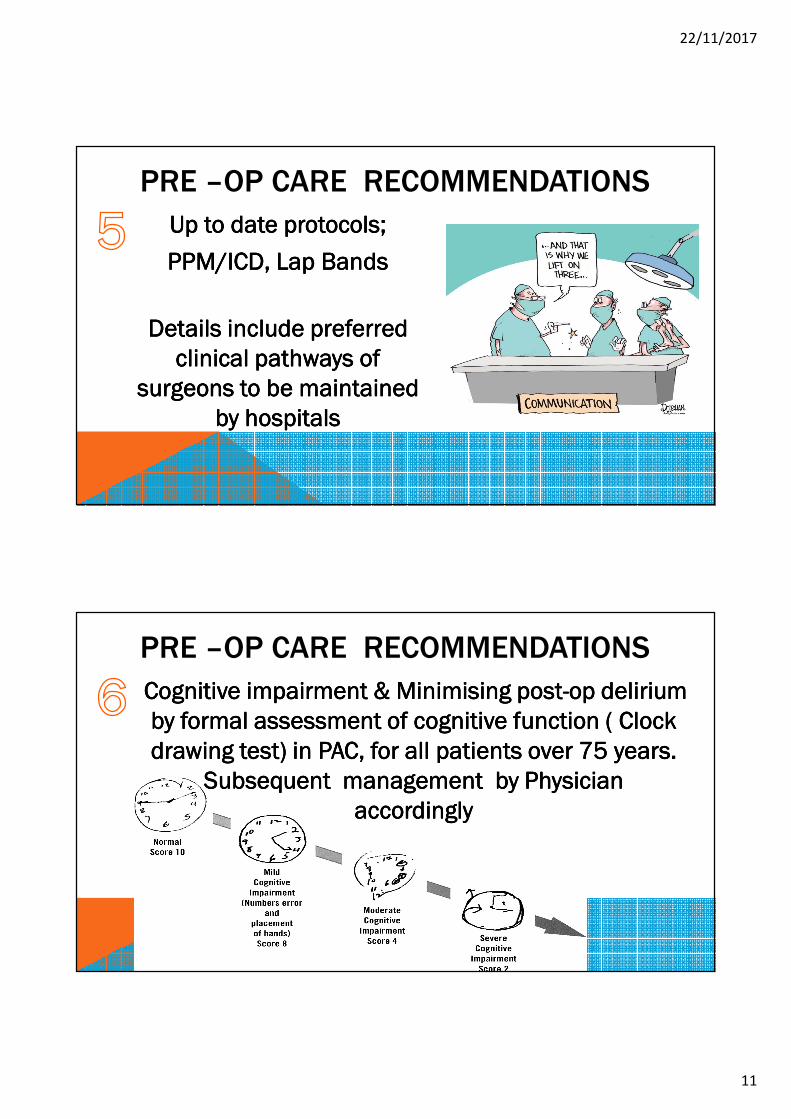
PRE –OP CARE RECOMMENDATIONS
Up Up Up Up to date to date to date to date protocols;protocols;protocols;protocols;
PPM/ICD, Lap BandsPPM/ICD, Lap BandsPPM/ICD, Lap BandsPPM/ICD, Lap Bands
Details Details Details Details include preferred include preferred include preferred include preferred
clinical pathways of clinical pathways of clinical pathways of clinical pathways of
surgeons to be maintained surgeons to be maintained surgeons to be maintained surgeons to be maintained
by by by by hospitalshospitalshospitalshospitals
PRE –OP CARE RECOMMENDATIONS
Cognitive impairment & Minimising postCognitive impairment & Minimising postCognitive impairment & Minimising postCognitive impairment & Minimising post----op delirium op delirium op delirium op delirium
by formal assessment of cognitive function ( Clock by formal assessment of cognitive function ( Clock by formal assessment of cognitive function ( Clock by formal assessment of cognitive function ( Clock
drawing test) in PAC, for all patients over 75 drawing test) in PAC, for all patients over 75 drawing test) in PAC, for all patients over 75 drawing test) in PAC, for all patients over 75 years.years.years.years.
Subsequent management by Subsequent management by Subsequent management by Subsequent management by Physician Physician Physician Physician
accordinglyaccordinglyaccordinglyaccordingly

22/11/2017
12
PRE –OP CARE RECOMMENDATIONS
PrePrePrePre----operative weight loss operative weight loss operative weight loss operative weight loss
programmes for selected cases programmes for selected cases programmes for selected cases programmes for selected cases
E.g. E.g. E.g. E.g. Radical Prostatectomy,Radical Prostatectomy,Radical Prostatectomy,Radical Prostatectomy,
CholecystectomyCholecystectomyCholecystectomyCholecystectomy
PRE –OP CARE RECOMMENDATIONS
Current Current Current Current Medication lists and/or medications Medication lists and/or medications Medication lists and/or medications Medication lists and/or medications
brought by patient when admitted for surgery brought by patient when admitted for surgery brought by patient when admitted for surgery brought by patient when admitted for surgery ––––
part of hospital admission protocol part of hospital admission protocol part of hospital admission protocol part of hospital admission protocol packagepackagepackagepackage

22/11/2017
13
Rye Ocean Rye Ocean Rye Ocean Rye Ocean Beach, Beach, Beach, Beach, Victoria Victoria Victoria Victoria (“A birds eye(“A birds eye(“A birds eye(“A birds eye----view”)view”)view”)view”)
POST–OPERATIVE CARE RECOMMENDATIONS
Poor lines of communication when multiple doctors are Poor lines of communication when multiple doctors are Poor lines of communication when multiple doctors are Poor lines of communication when multiple doctors are involvedinvolvedinvolvedinvolved---- “No one takes ultimate responsibility”“No one takes ultimate responsibility”“No one takes ultimate responsibility”“No one takes ultimate responsibility”
Confusion as to WHO Confusion as to WHO Confusion as to WHO Confusion as to WHO is responsible especially is responsible especially is responsible especially is responsible especially first 24 hoursfirst 24 hoursfirst 24 hoursfirst 24 hours
Medication and fluid orders Medication and fluid orders Medication and fluid orders Medication and fluid orders not written up or verbal ordersnot written up or verbal ordersnot written up or verbal ordersnot written up or verbal ordersnot signed leading to nurses not signed leading to nurses not signed leading to nurses not signed leading to nurses doing this “de facto”……= illegal! doing this “de facto”……= illegal! doing this “de facto”……= illegal! doing this “de facto”……= illegal!
Preamble

22/11/2017
14
When condition deteriorates, nurses asked to “contact a physician”, who has no knowledge of the patient
Medical documentationvaries from comprehensiveto None! Medico –Legal implications
POST–OPERATIVE CARE RECOMMENDATIONS
PreamblePreamblePreamblePreamble
(a) Surgeon (a) Surgeon (a) Surgeon (a) Surgeon �Unexplained hypotension
�Haemorrhage
�Fluid Balance
� Ileus
Treating Surgeon ultimately ResponsibleTreating Surgeon ultimately ResponsibleTreating Surgeon ultimately ResponsibleTreating Surgeon ultimately Responsible
POST OP CARE RECOMMENDATIONS

22/11/2017
15
POST OP CARE RECOMMENDATIONS
(b) Anaesthetist(b) Anaesthetist(b) Anaesthetist(b) Anaesthetist�Post op Nausea and Vomiting
�Post Op Respiratory Complications
�Analgesic regimes e.g. Ketamine, Epidurals
�Airways/Pressure care & positioning issues
� (ANZCA guidelines re 24 hr post op cover)
Treating Surgeon ultimately ResponsibleTreating Surgeon ultimately ResponsibleTreating Surgeon ultimately ResponsibleTreating Surgeon ultimately Responsible
Treating Surgeon ultimately ResponsibleTreating Surgeon ultimately ResponsibleTreating Surgeon ultimately ResponsibleTreating Surgeon ultimately Responsible
POST OP CARE RECOMMENDATIONS
(c) Physician(c) Physician(c) Physician(c) Physician�Cardiac arrhythmias/APO
�Suspected AMI/PE
�Acute Renal Impairment
�Sepsis/Pneumonia
�Stroke/TIA
�TPN
�Unstable Diabetes

22/11/2017
16
Medication & Fluid orders written up in theatreMedication & Fluid orders written up in theatreMedication & Fluid orders written up in theatreMedication & Fluid orders written up in theatre
Nursing staff to use the ISBAR tool to communicateNursing staff to use the ISBAR tool to communicateNursing staff to use the ISBAR tool to communicateNursing staff to use the ISBAR tool to communicate
with medical staffwith medical staffwith medical staffwith medical staff
Paper documentation in notes by all Medical/Nursing Paper documentation in notes by all Medical/Nursing Paper documentation in notes by all Medical/Nursing Paper documentation in notes by all Medical/Nursing
staff involved in care. staff involved in care. staff involved in care. staff involved in care.
Can be brief but should Can be brief but should Can be brief but should Can be brief but should
occuroccuroccuroccur
POST OP CARE RECOMMENDATIONS
Communication between surgeons, physicians and anaesthetists must be done person to person, rather than through nursing staff
POST OP CARE RECOMMENDATIONS
Communication issues
Surgeon plays the liaison role (not the nurse) in
cases with post op uncertainty

22/11/2017
17
IF Inability to Contact a treating IF Inability to Contact a treating IF Inability to Contact a treating IF Inability to Contact a treating specialist this specialist this specialist this specialist this is communicated to is communicated to is communicated to is communicated to
the surgeon who is ultimately responsiblethe surgeon who is ultimately responsiblethe surgeon who is ultimately responsiblethe surgeon who is ultimately responsible
IF Surgeon is uncontactable, then a surgical peer is called.IF Surgeon is uncontactable, then a surgical peer is called.IF Surgeon is uncontactable, then a surgical peer is called.IF Surgeon is uncontactable, then a surgical peer is called.
IF NEITHER are IF NEITHER are IF NEITHER are IF NEITHER are contactable: contactable: contactable: contactable: the hospital the hospital the hospital the hospital
supervisor notified and patient is transferred supervisor notified and patient is transferred supervisor notified and patient is transferred supervisor notified and patient is transferred outoutoutout
Incident Report sent to relevant Incident Report sent to relevant Incident Report sent to relevant Incident Report sent to relevant committee/scommittee/scommittee/scommittee/s
POST OP CARE RECOMMENDATIONS
Communication issues
Admitting Doctor should never besurprised to receive a call at any hour of the day or night,regarding their patients
Inappropriate comments to nursing staff triggers an incident report
If necessary Chair of the MAC has a “quiet word” with doctor concerned
POST OP CARE RECOMMENDATIONS Communication issues

22/11/2017
18
Blairgowrie Back Blairgowrie Back Blairgowrie Back Blairgowrie Back BachBachBachBachVictoriaVictoriaVictoriaVictoria
BENEFITS OF PROJECT
TO CURRENT SITUATION• New Specialists seeking accreditation are sent a copy of the
working party document, to raise awareness of standards
expected
• Resident cover in private hospitals enhanced by CMOs
• Triggered incident reports in periop care discussed at
Internal medicine and MACs
• More general physicians attracted to area & periop medicine

22/11/2017
19
PLANS FOR THE FUTURECentralised repository of all pathology & imaging in conjunction with local providers, private rooms, which is easily accessible by all stake holders (avoids duplication)
GP involvement in PAC’sGP involvement in PAC’sGP involvement in PAC’sGP involvement in PAC’s
KPIs to be formulatedKPIs to be formulatedKPIs to be formulatedKPIs to be formulated� -e.g. booked patients cancelled on day of surgery� -% patients cancelled due to medical conditions� -Unexpected transfers out of post surgical patients� -Undiagnosed dementia identified at PACs
PERI-OPERATIVE PARAMETERS USED
AT PHYSICIAN ASSESSMENT
• NSQIP Index (NSQIP Index (NSQIP Index (NSQIP Index (Gupta)Gupta)Gupta)Gupta)• Estimated risk probability for Periop MI
or Cardiac arrest (iphone app)
• ASA ClassASA ClassASA ClassASA Class
• Predictors of Pulmonary complicationsPredictors of Pulmonary complicationsPredictors of Pulmonary complicationsPredictors of Pulmonary complications
• PONVPONVPONVPONV
Appendix

22/11/2017
20
PERI-OPERATIVE PARAMETERS USED
AT PHYSICIAN ASSESSMENT
Appendix
• OSA ScreeningOSA ScreeningOSA ScreeningOSA Screening
• Obesity/Waist Obesity/Waist Obesity/Waist Obesity/Waist Circumference /BMICircumference /BMICircumference /BMICircumference /BMI
• Aortic StenosisAortic StenosisAortic StenosisAortic Stenosis
• NYHA Class for Heart NYHA Class for Heart NYHA Class for Heart NYHA Class for Heart FailureFailureFailureFailure
• Clock Drawing (>75 Clock Drawing (>75 Clock Drawing (>75 Clock Drawing (>75 ysysysys old)old)old)old)
• Stent management Stent management Stent management Stent management
/Warfarin//Warfarin//Warfarin//Warfarin/AntiplateletsAntiplateletsAntiplateletsAntiplatelets
/PPM/ICD’s/NOAC’s/PPM/ICD’s/NOAC’s/PPM/ICD’s/NOAC’s/PPM/ICD’s/NOAC’s
• Respiratory Failure Respiratory Failure Respiratory Failure Respiratory Failure
indexindexindexindex
WWW.ROMYNAYAGAMPHOTOGRAPHY.COM
Mothers Beach, Mornington, VictoriaMothers Beach, Mornington, VictoriaMothers Beach, Mornington, VictoriaMothers Beach, Mornington, Victoria
Recommended












![Perioperative Medicine[1]](https://img.dokumen.tips/doc/110x75/577d38e31a28ab3a6b98b058/perioperative-medicine1.jpg)




