Embed Size (px)
Citation preview
Perioperative Cardiac Evaluation &
Management for Noncardiac Surgery:
2014 ACC/AHA Guidelines
Steven L. Cohn, MD, FACP, SFHM Medical Director - UHealth Preoperative Assessment Center
Director – Medical Consultation Service
University of Miami Hospital
Professor of Clinical Medicine
University of Miami Miller School of Medicine
Disclosures
No relevant COI for this topic except:
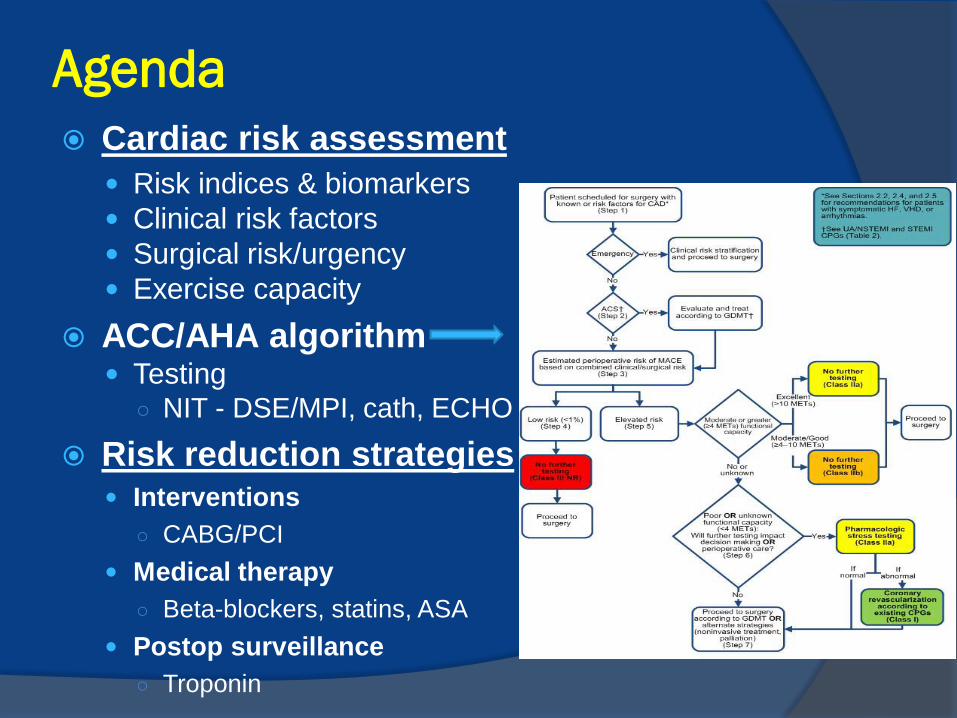
Agenda
Cardiac risk assessment
Risk indices & biomarkers
Clinical risk factors
Surgical risk/urgency
Exercise capacity
ACC/AHA algorithm Testing
○ NIT - DSE/MPI, cath, ECHO
Risk reduction strategies Interventions
○ CABG/PCI
Medical therapy
○ Beta-blockers, statins, ASA
Postop surveillance
○ Troponin
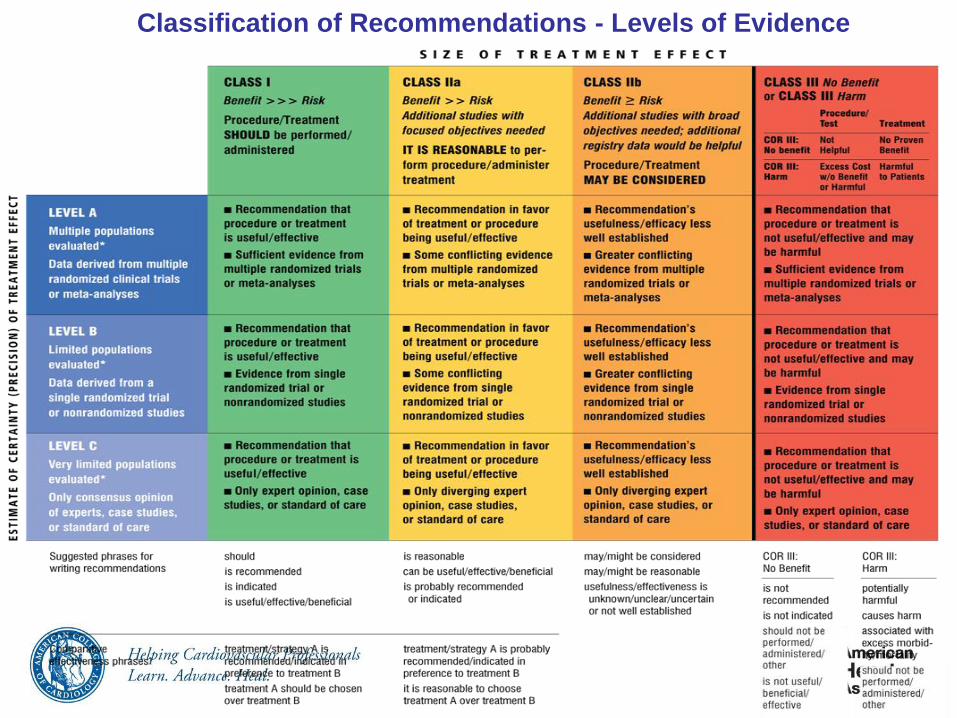
Classification of Recommendations - Levels of Evidence
Purpose of Preop Medical Consultation
Identify risk factors and assess severity & stability
Provide a clinical risk profile for informed and shared decision-making
Make recommendations for any management changes, need for further testing, or specialty consultation
NOT to CLEAR FOR SURGERY!
Pt is in his/her OPTIMAL MEDICAL CONDITION for surgery.
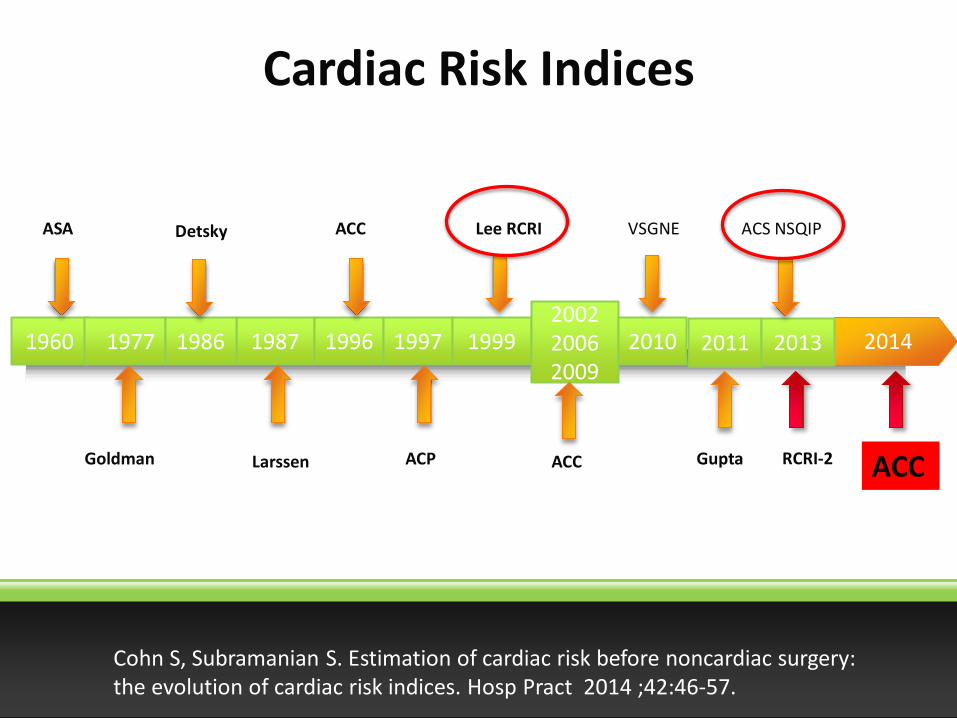
2014 1987 1996 1997 1999 2002 2006 2009
2010 1960 1977 1986
Detsky
Cardiac Risk Indices
ACC Lee RCRI VSGNE
Gupta ACC ACP Goldman Larssen
ASA
2011 2013
ACS NSQIP
RCRI-2 ACC
Cohn S, Subramanian S. Estimation of cardiac risk before noncardiac surgery: the evolution of cardiac risk indices. Hosp Pract 2014 ;42:46-57.
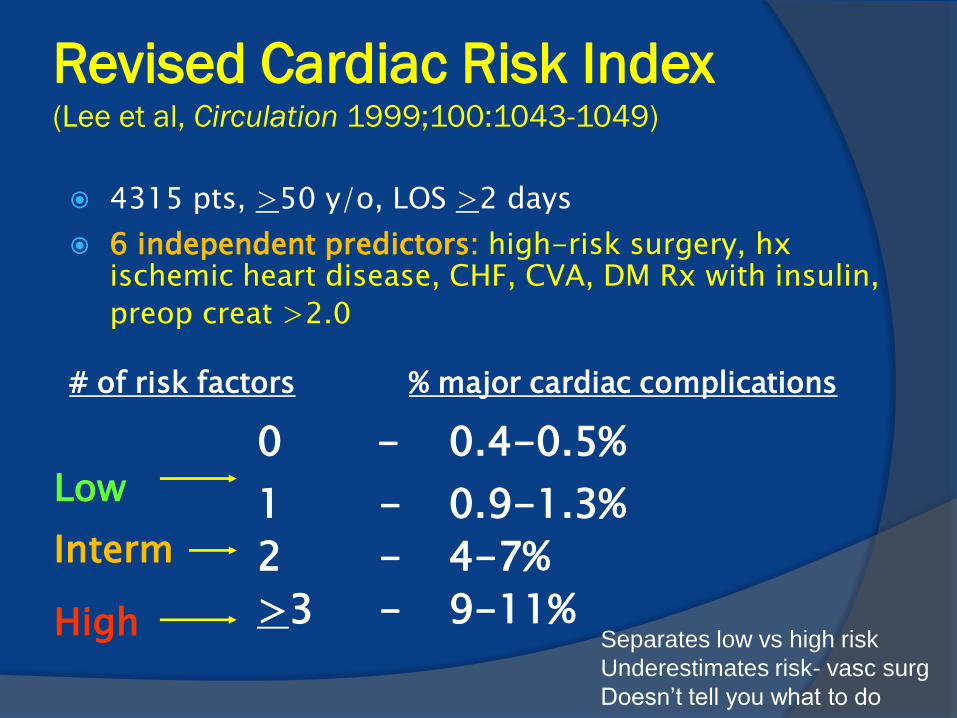
Revised Cardiac Risk Index (Lee et al, Circulation 1999;100:1043-1049)
4315 pts, >50 y/o, LOS >2 days
6 independent predictors: high-risk surgery, hx ischemic heart disease, CHF, CVA, DM Rx with insulin,
preop creat >2.0 # of risk factors % major cardiac complications
0 - 0.4-0.5%
1 - 0.9-1.3%
2 - 4-7%
>3 - 9-11%
Low Interm High
Separates low vs high risk
Underestimates risk- vasc surg
Doesn’t tell you what to do
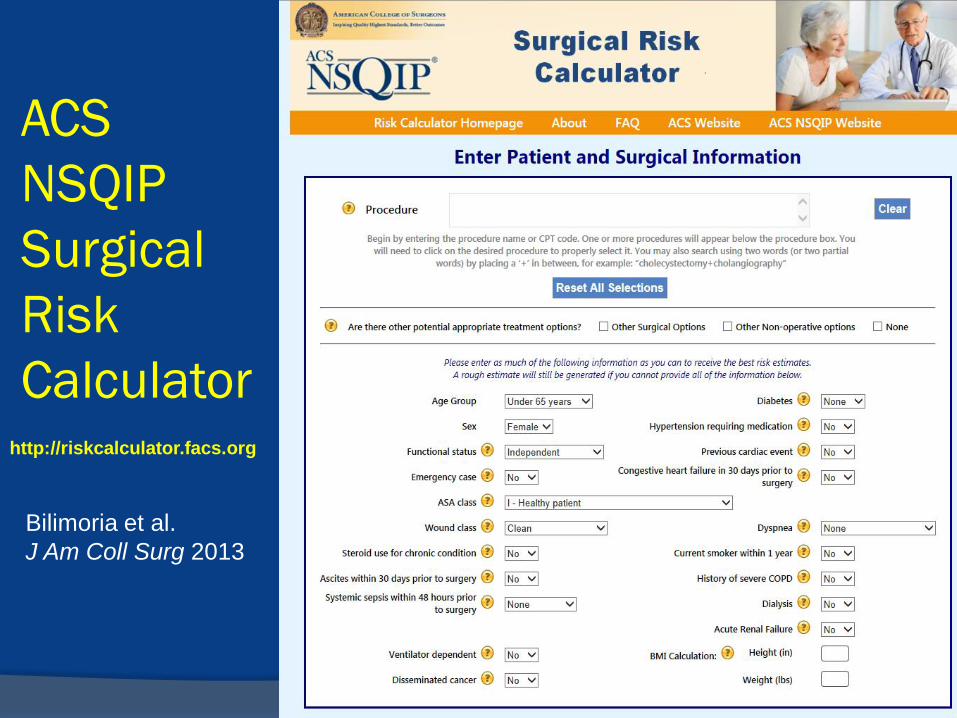
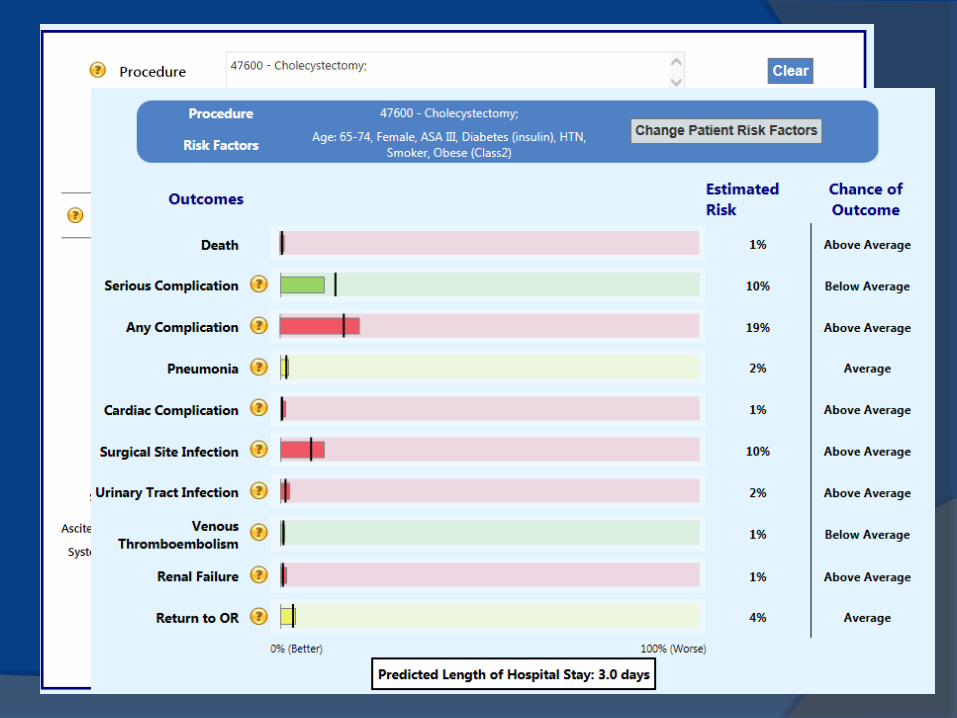
ACS
NSQIP
Surgical
Risk
Calculator
http://riskcalculator.facs.org
Bilimoria et al.
J Am Coll Surg 2013
Definitions of Urgency & Risk
Urgency
Emergency: <6 hours
Urgent: 6-24 hours
Time sensitive: can delay 1-6 weeks
Elective: can delay up to 1 year
Risk (combined surg & pt characteristics)
Low risk: <1% MACE
Elevated: >1% MACE
Clinical Risk Factors
CAD Isch Sx/NYHA, prior MI/timing, CABG/PCI,
elevated biomarkers
HF Decompensated + depressed LV funct worst;
Sx > asympt; syst (EF<30-40%) > diastolic
Valvular disease Type (stenotic>regurg), severity, symptoms
Arrhythmias Hemodynamic effects, underlying structural heart
disease
Evaluation of Valvular Heart Disease
Echocardiography (I-C) is recommended in patients
with suspected moderate to severe stenotic or
regurgitant lesions if:
worsening in clinical condition
not done within the past year
If indicated, valvular intervention to reduce risk. (I-C)
Asymptomatic severe AS, AR, or MR: (IIa-C)
reasonable to perform elevated risk noncardiac surgery
using appropriate perioperative hemodynamic monitoring
Asymptomatic severe MS: (IIb-C)
may be reasonable if not a candidate for repair
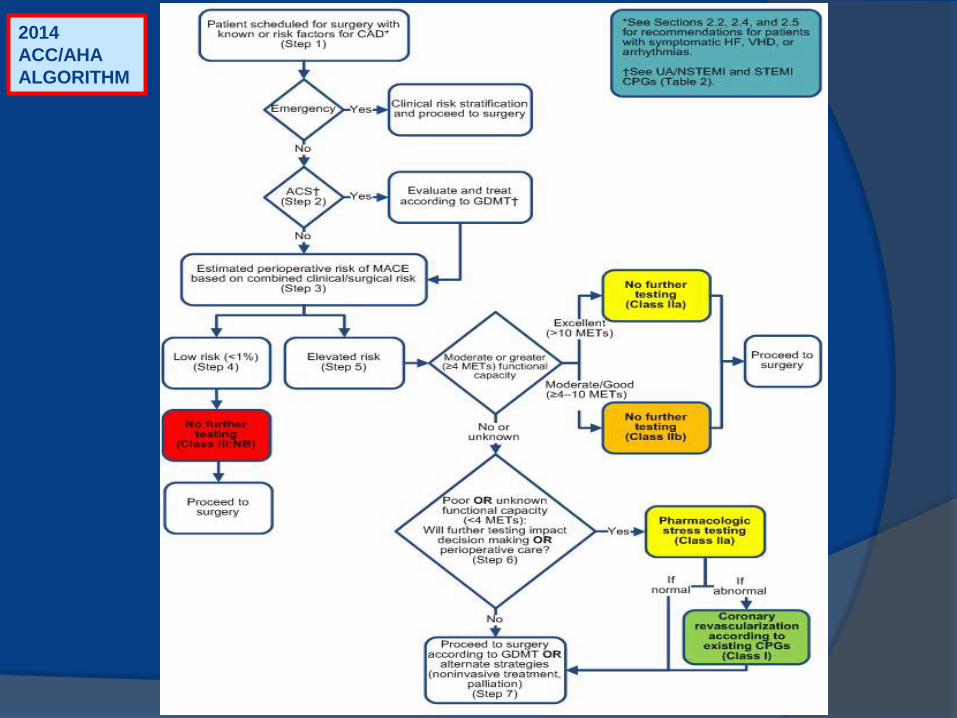
2014
ACC/AHA
ALGORITHM
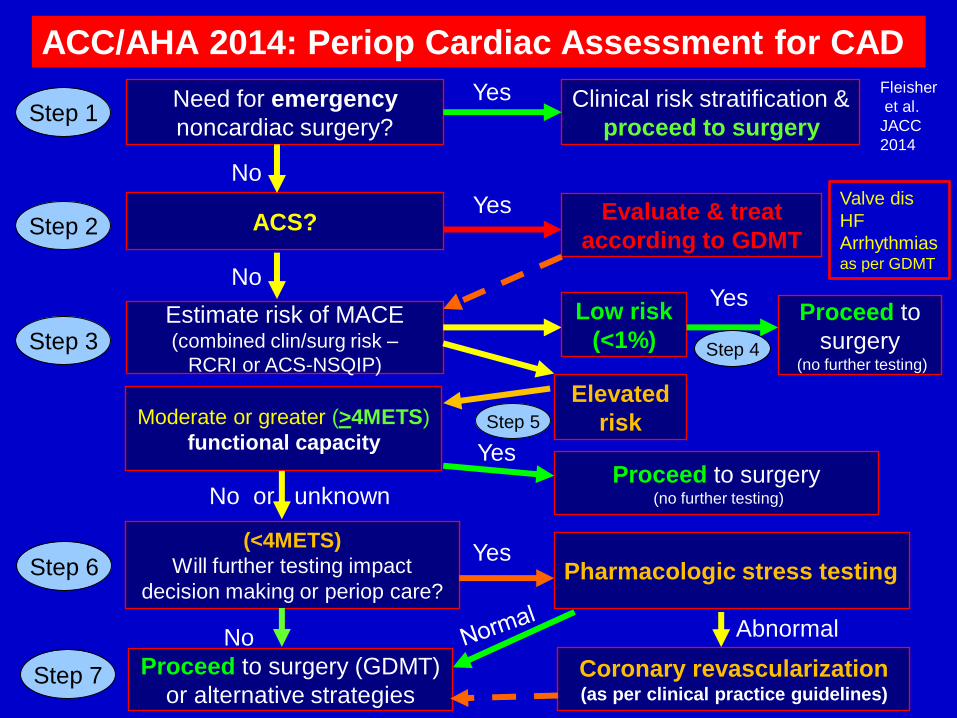
ACC/AHA 2014: Periop Cardiac Assessment for CAD
Step 1
Step 2
Step 3
Step 6
Need for emergency
noncardiac surgery?
ACS?
Estimate risk of MACE (combined clin/surg risk –
RCRI or ACS-NSQIP)
Moderate or greater (>4METS)
functional capacity
(<4METS)
Will further testing impact
decision making or periop care?
Clinical risk stratification &
proceed to surgery
Evaluate & treat
according to GDMT
Proceed to
surgery (no further testing)
Proceed to surgery (no further testing)
No
No
No or unknown
Yes
Yes
Yes
Yes
Pharmacologic stress testing
Fleisher
et al.
JACC
2014
Low risk
(<1%)
Elevated
risk
Step 4
Step 5
No
Proceed to surgery (GDMT)
or alternative strategies
Yes
Coronary revascularization (as per clinical practice guidelines)
Abnormal
Step 7
Valve dis
HF
Arrhythmias
as per GDMT
Supplemental Testing
ECG
ECHO
Stress testing
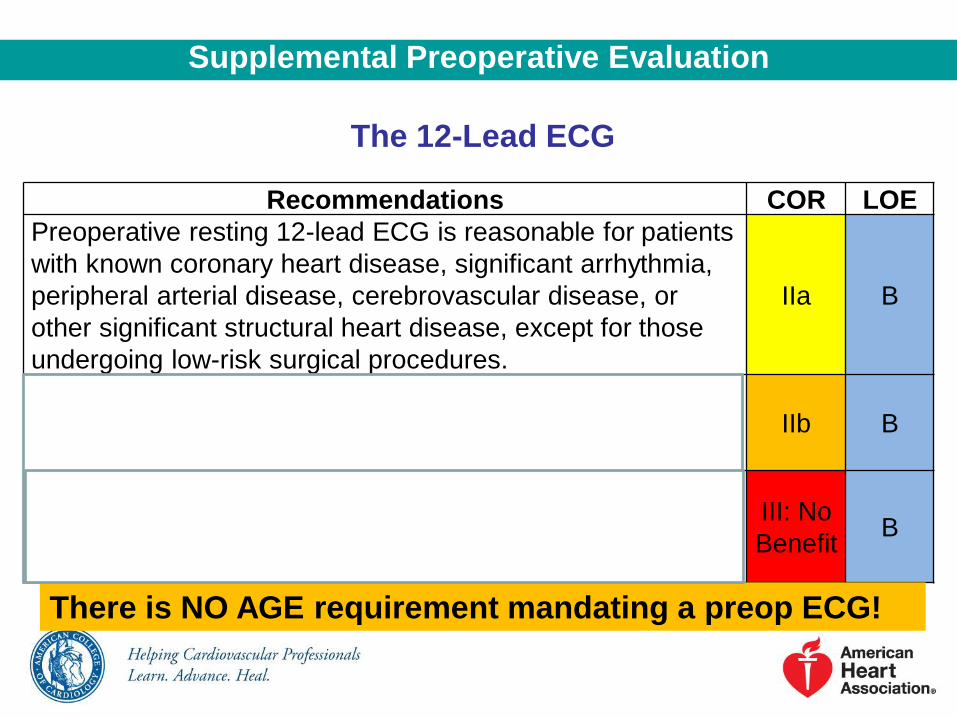
The 12-Lead ECG
Supplemental Preoperative Evaluation
Recommendations COR LOE
Preoperative resting 12-lead ECG is reasonable for patients
with known coronary heart disease, significant arrhythmia,
peripheral arterial disease, cerebrovascular disease, or
other significant structural heart disease, except for those
undergoing low-risk surgical procedures.
IIa B
Preoperative resting 12-lead ECG may be considered for
asymptomatic patients without known coronary heart
disease, except for those undergoing low-risk surgery.
IIb B
Routine preoperative resting 12-lead ECG is not useful for
asymptomatic patients undergoing low-risk surgical
procedures.
III: No
Benefit B
There is NO AGE requirement mandating a preop ECG!
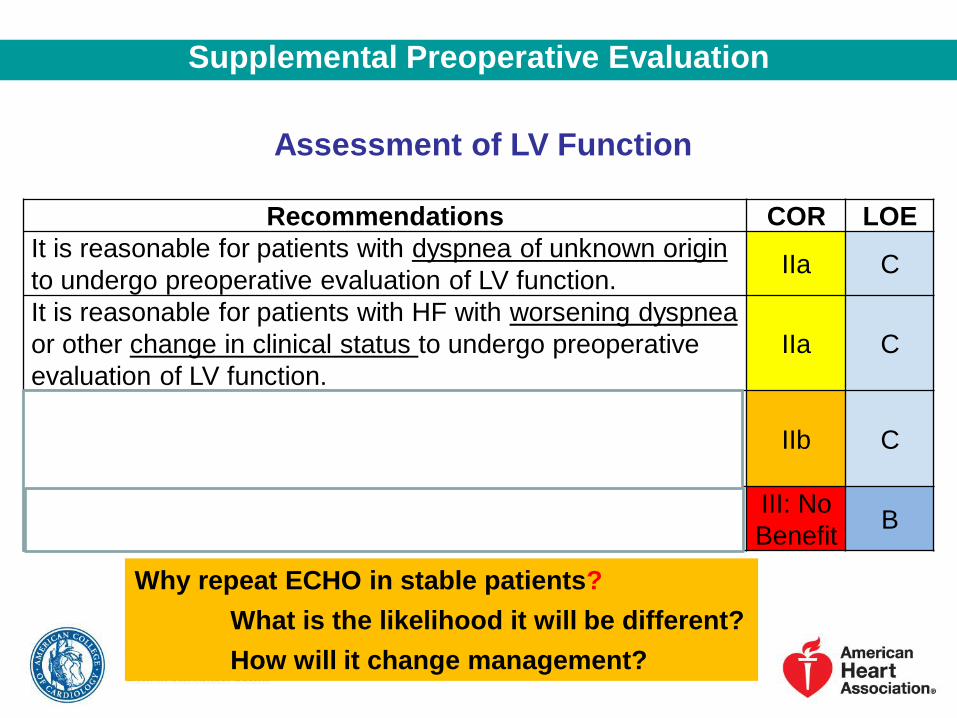
Assessment of LV Function
Supplemental Preoperative Evaluation
Recommendations COR LOE
It is reasonable for patients with dyspnea of unknown origin
to undergo preoperative evaluation of LV function. IIa C
It is reasonable for patients with HF with worsening dyspnea
or other change in clinical status to undergo preoperative
evaluation of LV function.
IIa C
Reassessment of LV function in clinically stable patients
with previously documented LV dysfunction may be
considered if there has been no assessment within a year.
IIb C
Routine preoperative evaluation of LV function is not
recommended.
III: No
Benefit B
Why repeat ECHO in stable patients?
What is the likelihood it will be different?
How will it change management?
?
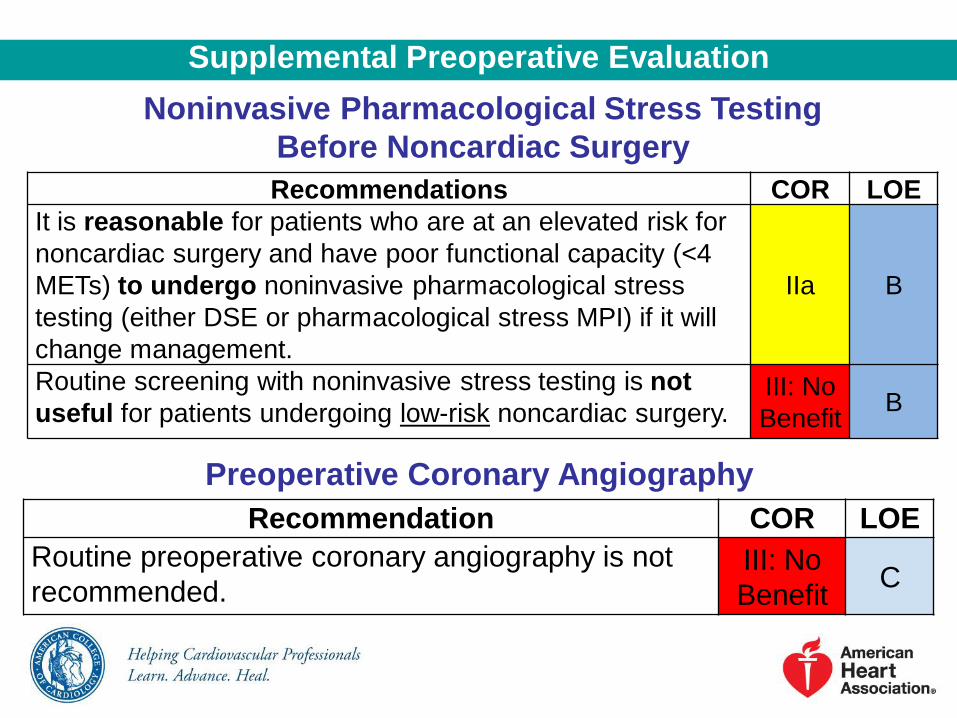
Noninvasive Pharmacological Stress Testing
Before Noncardiac Surgery
Supplemental Preoperative Evaluation
Recommendations COR LOE
It is reasonable for patients who are at an elevated risk for
noncardiac surgery and have poor functional capacity (<4
METs) to undergo noninvasive pharmacological stress
testing (either DSE or pharmacological stress MPI) if it will
change management.
IIa B
Routine screening with noninvasive stress testing is not
useful for patients undergoing low-risk noncardiac surgery. III: No
Benefit B
Recommendation COR LOE
Routine preoperative coronary angiography is not
recommended. III: No
Benefit C
Preoperative Coronary Angiography
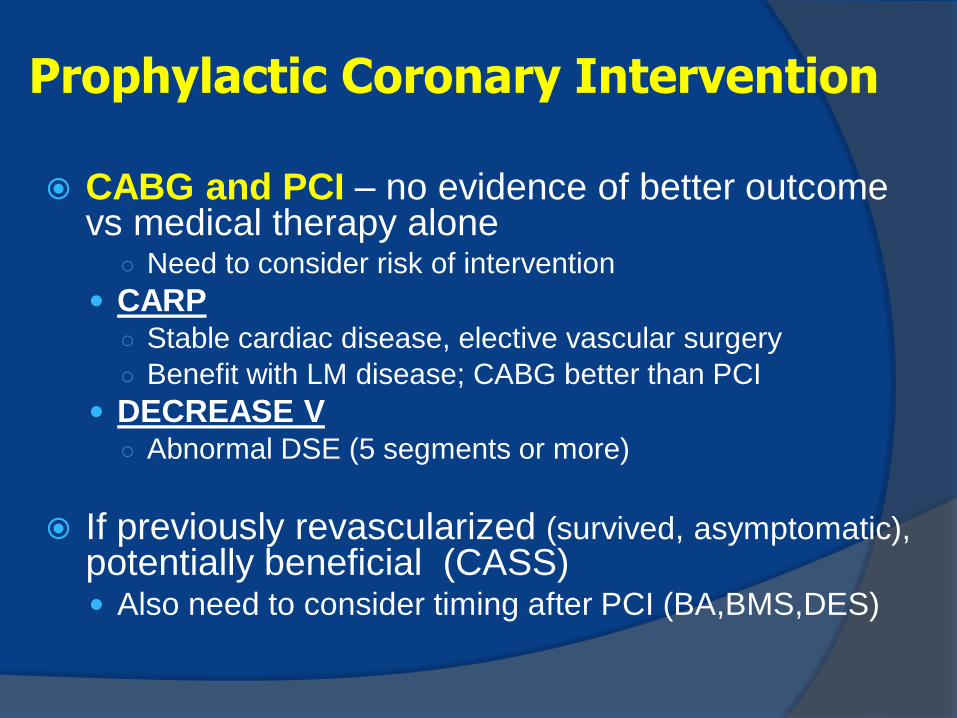
CABG and PCI – no evidence of better outcome vs medical therapy alone
○ Need to consider risk of intervention
CARP ○ Stable cardiac disease, elective vascular surgery
○ Benefit with LM disease; CABG better than PCI
DECREASE V ○ Abnormal DSE (5 segments or more)
If previously revascularized (survived, asymptomatic), potentially beneficial (CASS) Also need to consider timing after PCI (BA,BMS,DES)
Prophylactic Coronary Intervention
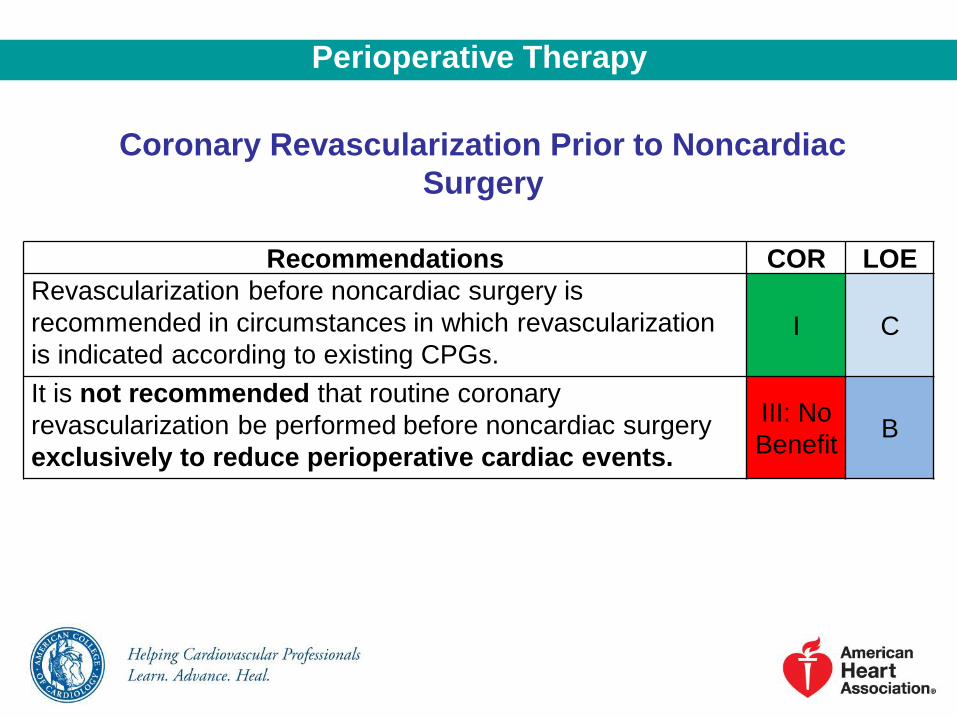
Coronary Revascularization Prior to Noncardiac
Surgery
Perioperative Therapy
Recommendations COR LOE
Revascularization before noncardiac surgery is
recommended in circumstances in which revascularization
is indicated according to existing CPGs. I C
It is not recommended that routine coronary
revascularization be performed before noncardiac surgery
exclusively to reduce perioperative cardiac events.
III: No
Benefit B
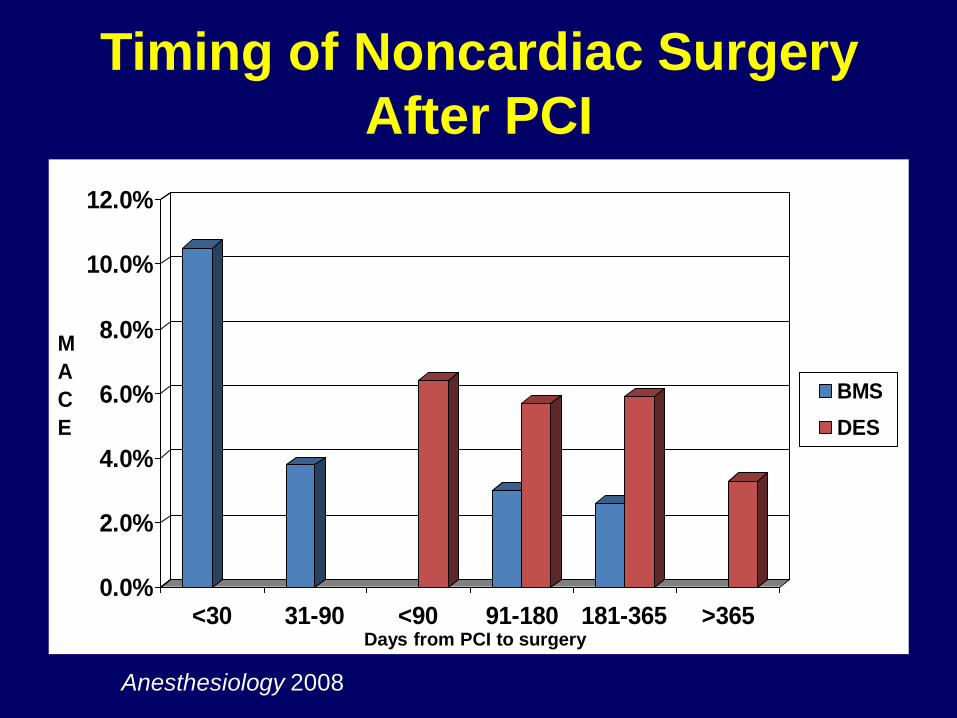
Timing of Noncardiac Surgery
After PCI
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
<30 31-90 <90 91-180 181-365 >365
BMS
DES
M
A
C
E
Anesthesiology 2008
Days from PCI to surgery
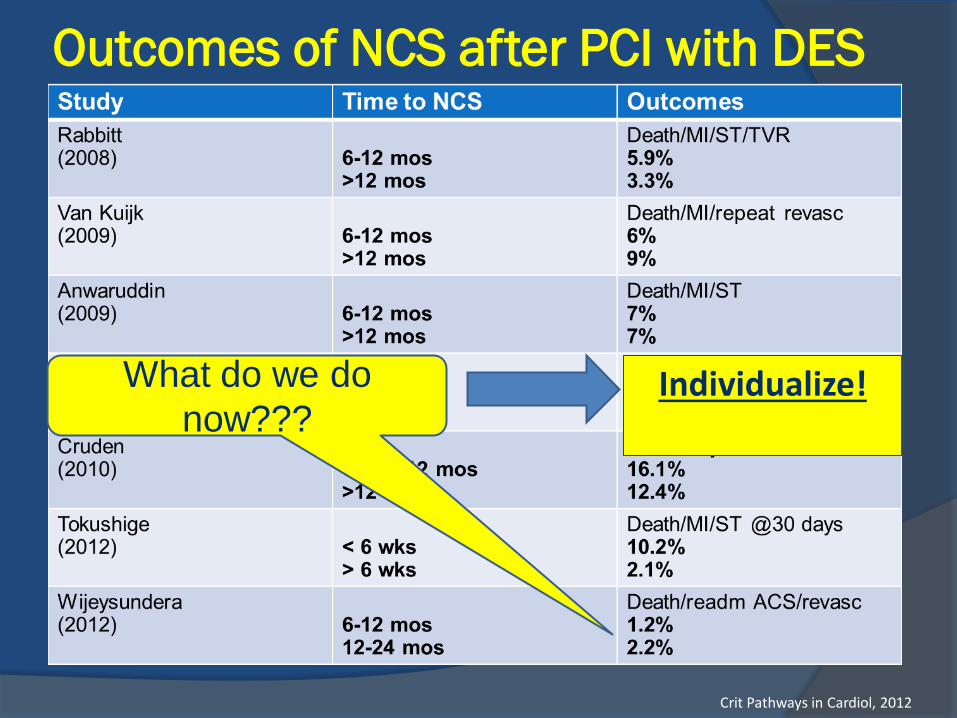
Outcomes of NCS after PCI with DES
Crit Pathways in Cardiol, 2012
What do we do
now??? Individualize!
Urgency of surgery
Type of surgery
Patient clinical risk factors
Risk factors for stent thrombosis
○ Patient (ACS, low EF, DM, age)
○ Procedure (LAD/LM, multiple stents/vessels)
○ Lesion (bifurcation, length, diameter, multiple)
Management of antiplatelet therapy
○ Continue both, stop one, stop both
Individualize
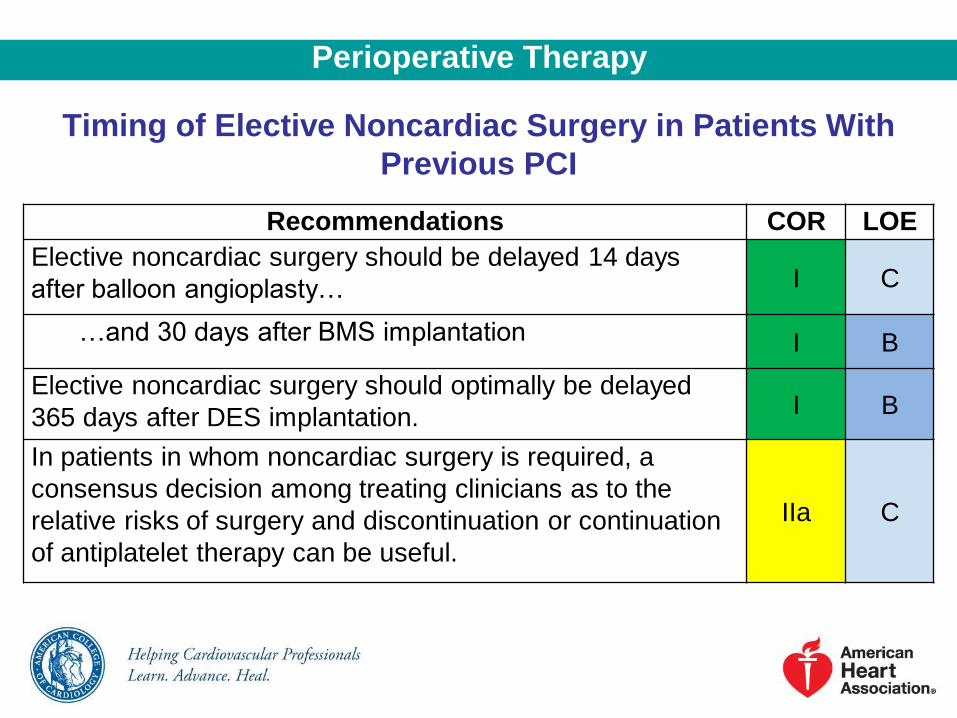
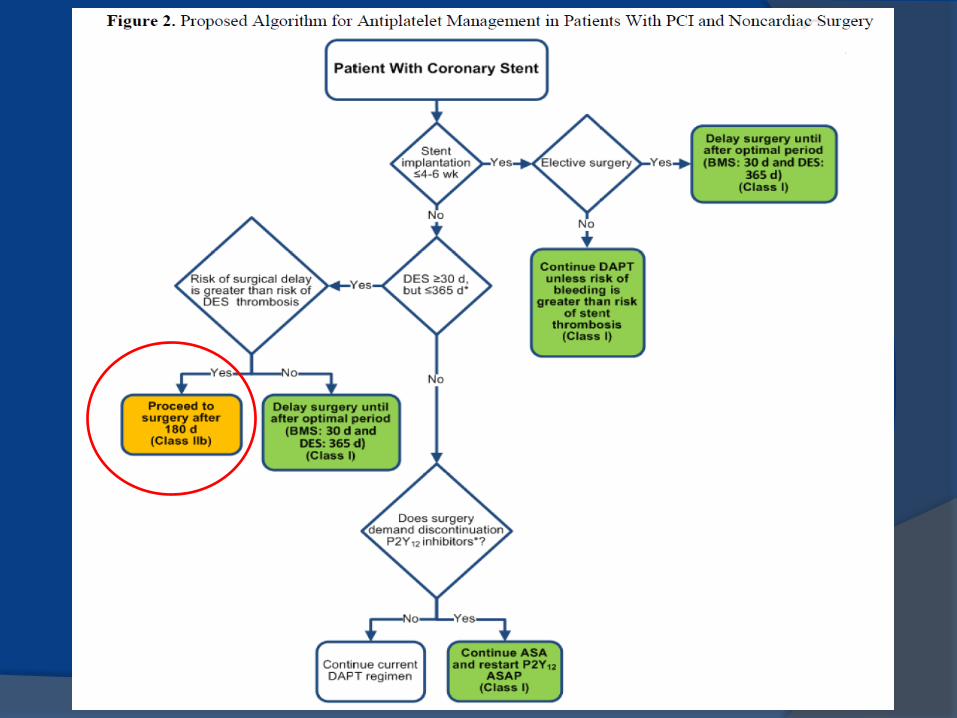
Timing of Elective Noncardiac Surgery in Patients With
Previous PCI
Recommendations COR LOE
Elective noncardiac surgery should be delayed 14 days
after balloon angioplasty… I C
…and 30 days after BMS implantation I B
Elective noncardiac surgery should optimally be delayed
365 days after DES implantation. I B
In patients in whom noncardiac surgery is required, a
consensus decision among treating clinicians as to the
relative risks of surgery and discontinuation or continuation
of antiplatelet therapy can be useful.
IIa C
Perioperative Therapy
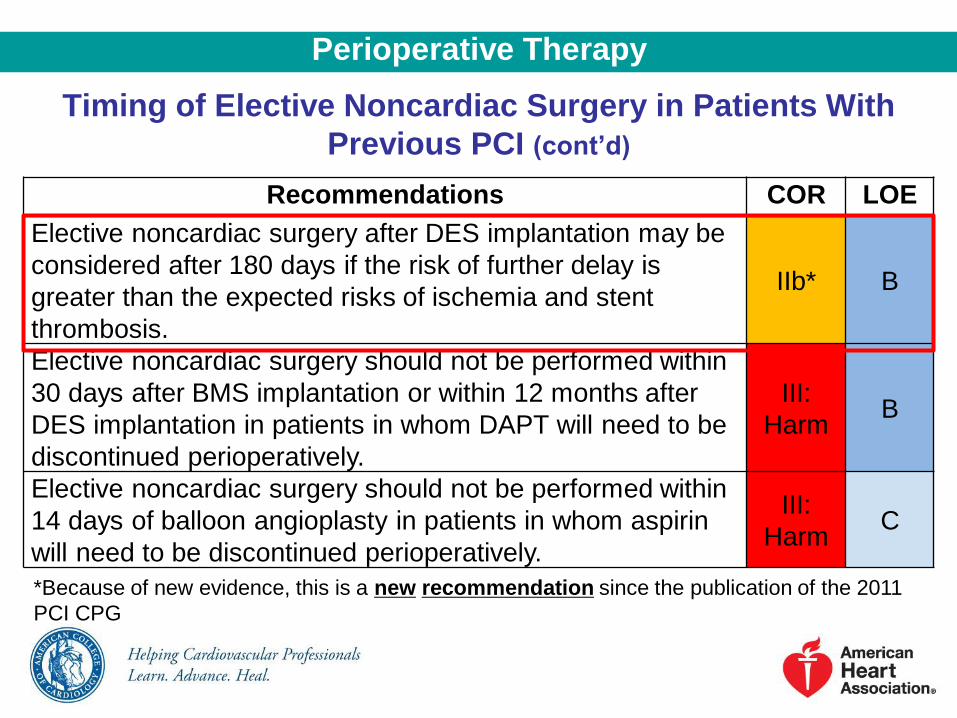
Timing of Elective Noncardiac Surgery in Patients With
Previous PCI (cont’d)
Recommendations COR LOE
Elective noncardiac surgery after DES implantation may be
considered after 180 days if the risk of further delay is
greater than the expected risks of ischemia and stent
thrombosis.
IIb* B
Elective noncardiac surgery should not be performed within
30 days after BMS implantation or within 12 months after
DES implantation in patients in whom DAPT will need to be
discontinued perioperatively.
III:
Harm B
Elective noncardiac surgery should not be performed within
14 days of balloon angioplasty in patients in whom aspirin
will need to be discontinued perioperatively.
III:
Harm C
*Because of new evidence, this is a new recommendation since the publication of the 2011
PCI CPG
Perioperative Therapy
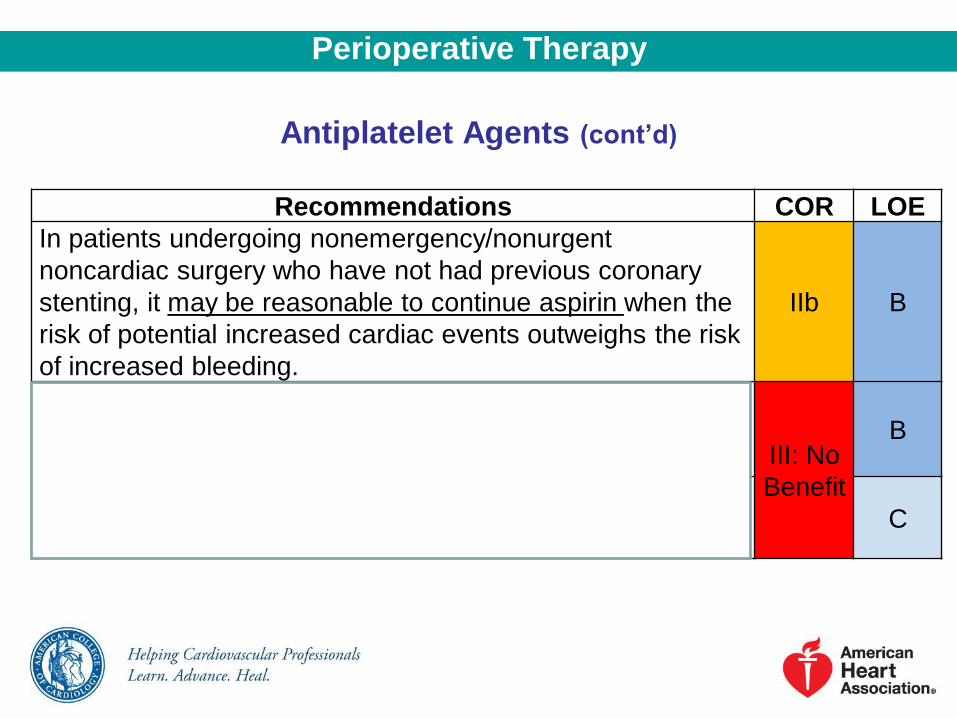
Antiplatelet Agents (cont’d)
Recommendations COR LOE
In patients undergoing nonemergency/nonurgent
noncardiac surgery who have not had previous coronary
stenting, it may be reasonable to continue aspirin when the
risk of potential increased cardiac events outweighs the risk
of increased bleeding.
IIb B
Initiation of aspirin is not beneficial in patients undergoing
elective noncardiac noncarotid surgery who have not had
previous coronary stenting,… III: No
Benefit
B
…unless the risk of ischemic events outweighs the risk
of surgical bleeding. C
Perioperative Therapy
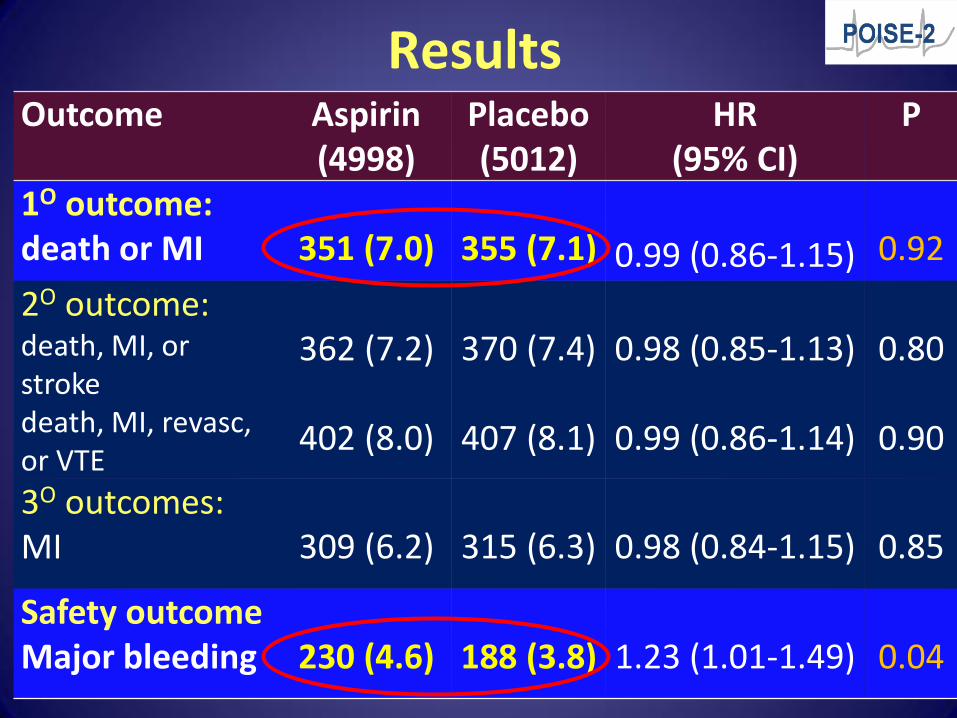
Results
28
Outcome
Aspirin (4998)
Placebo (5012)
HR (95% CI)
P
1O outcome: death or MI
351 (7.0)
355 (7.1)
0.99 (0.86-1.15)
0.92
2O outcome: death, MI, or stroke death, MI, revasc, or VTE
362 (7.2)
402 (8.0)
370 (7.4)
407 (8.1)
0.98 (0.85-1.13)
0.99 (0.86-1.14)
0.80
0.90
3O outcomes: MI
309 (6.2)
315 (6.3)
0.98 (0.84-1.15)
0.85
Safety outcome Major bleeding
230 (4.6)
188 (3.8)
1.23 (1.01-1.49)
0.04
Impact on Practice
• Should stop ASA preop for primary prevention
• Should postpone restarting ASA early postop
• Unanswered questions: subgroups
• Recent stents (were excluded)
• Recent cardiovascular events (within 1 yr)
• Primary vs secondary prevention
• High-bleeding risk surgery vs other procedures
BETA-BLOCKERS
CONTROVERSY: - Poldermans – question about scientific integrity of DECREASE trials
- POISE – question regarding dosing of metoprolol
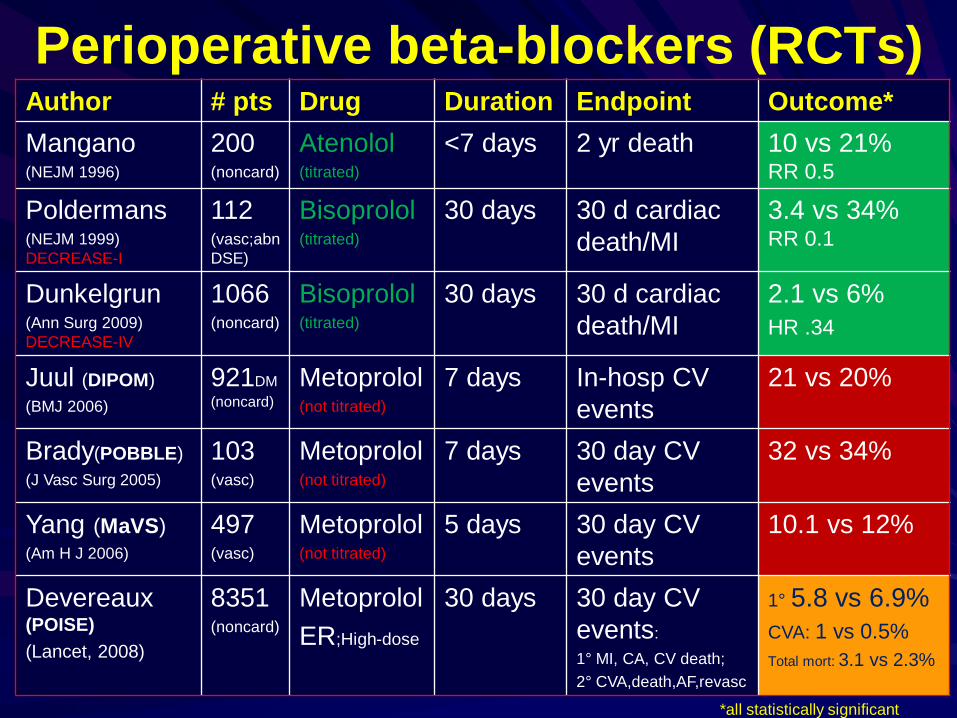
Perioperative beta-blockers (RCTs) Author # pts Drug Duration Endpoint Outcome*
Mangano (NEJM 1996)
200 (noncard)
Atenolol (titrated)
<7 days 2 yr death 10 vs 21% RR 0.5
Poldermans (NEJM 1999)
DECREASE-I
112 (vasc;abn
DSE)
Bisoprolol (titrated)
30 days 30 d cardiac
death/MI
3.4 vs 34% RR 0.1
Dunkelgrun (Ann Surg 2009)
DECREASE-IV
1066 (noncard)
Bisoprolol (titrated)
30 days 30 d cardiac
death/MI
2.1 vs 6%
HR .34
Juul (DIPOM)
(BMJ 2006)
921DM
(noncard)
Metoprolol (not titrated)
7 days In-hosp CV
events
21 vs 20%
Brady(POBBLE)
(J Vasc Surg 2005)
103 (vasc)
Metoprolol (not titrated)
7 days 30 day CV
events
32 vs 34%
Yang (MaVS)
(Am H J 2006)
497 (vasc)
Metoprolol (not titrated)
5 days 30 day CV
events
10.1 vs 12%
Devereaux
(POISE)
(Lancet, 2008)
8351 (noncard)
Metoprolol
ER;High-dose
30 days 30 day CV
events:
1° MI, CA, CV death;
2° CVA,death,AF,revasc
1° 5.8 vs 6.9%
CVA: 1 vs 0.5%
Total mort: 3.1 vs 2.3%
*all statistically significant
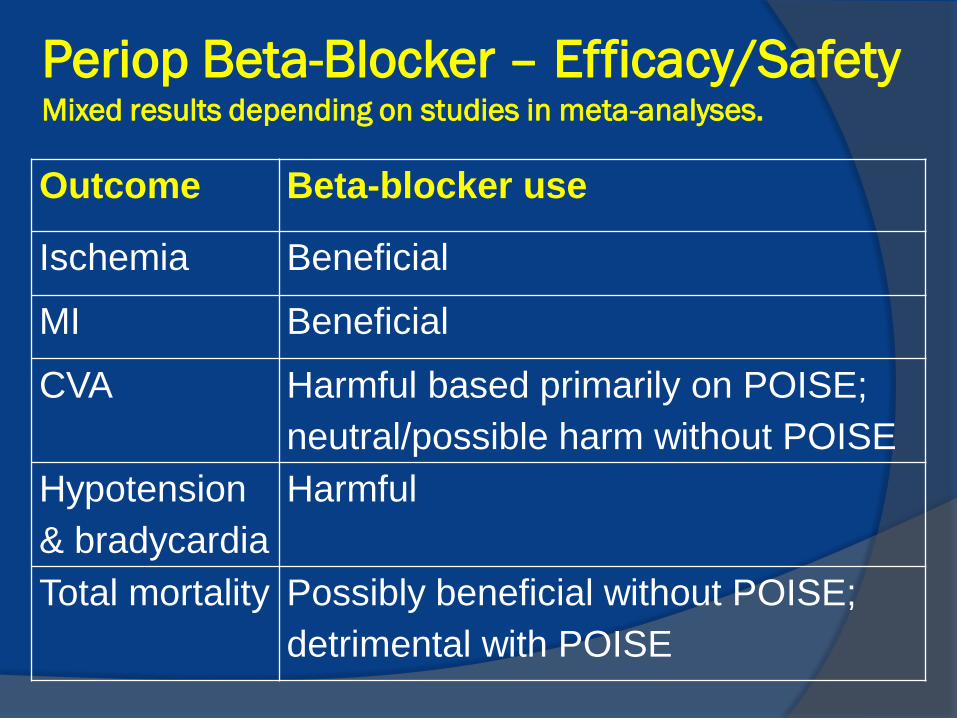
Periop Beta-Blocker – Efficacy/Safety Mixed results depending on studies in meta-analyses.
Outcome Beta-blocker use
Ischemia Beneficial
MI Beneficial
CVA Harmful based primarily on POISE;
neutral/possible harm without POISE
Hypotension
& bradycardia
Harmful
Total mortality Possibly beneficial without POISE;
detrimental with POISE
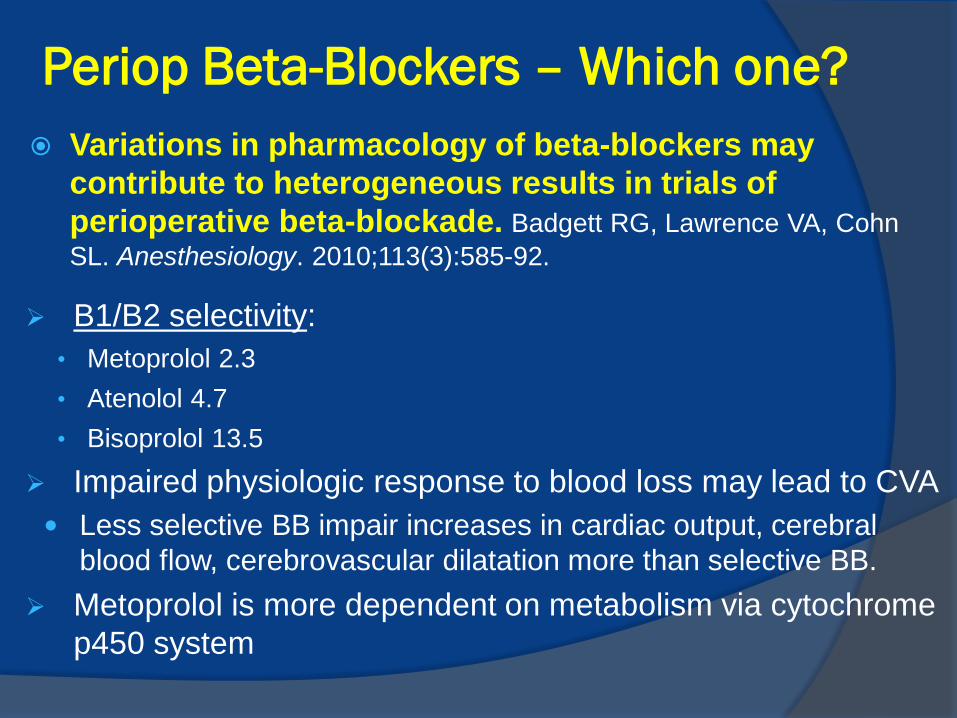
Periop Beta-Blockers – Which one?
Variations in pharmacology of beta-blockers may
contribute to heterogeneous results in trials of
perioperative beta-blockade. Badgett RG, Lawrence VA, Cohn
SL. Anesthesiology. 2010;113(3):585-92.
B1/B2 selectivity:
• Metoprolol 2.3
• Atenolol 4.7
• Bisoprolol 13.5
Impaired physiologic response to blood loss may lead to CVA
Less selective BB impair increases in cardiac output, cerebral
blood flow, cerebrovascular dilatation more than selective BB.
Metoprolol is more dependent on metabolism via cytochrome
p450 system
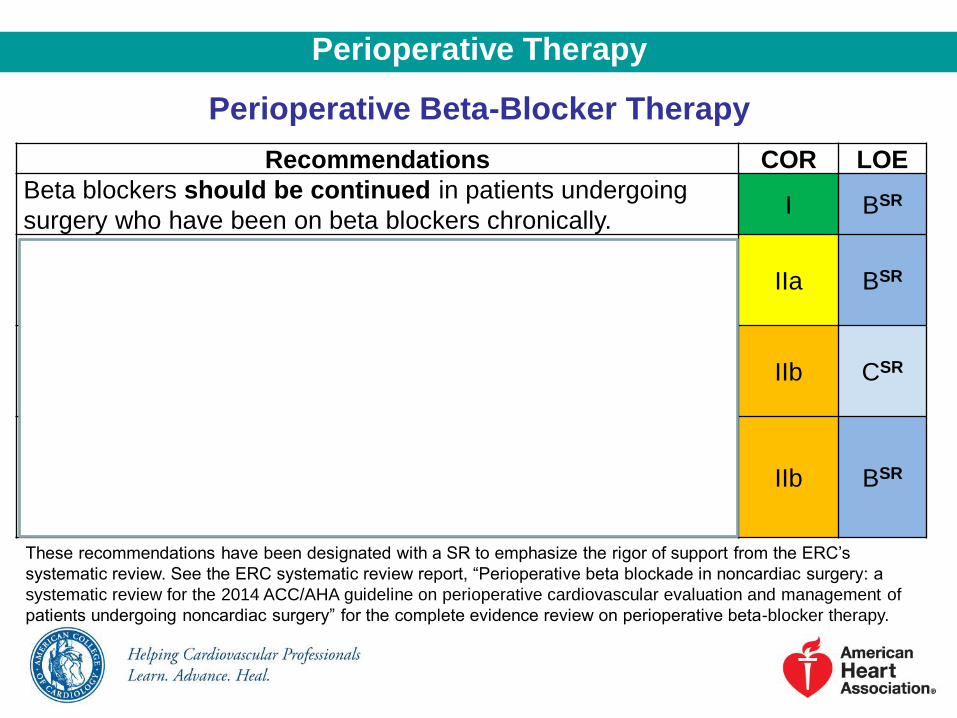
Perioperative Therapy
Perioperative Beta-Blocker Therapy
Recommendations COR LOE
Beta blockers should be continued in patients undergoing
surgery who have been on beta blockers chronically. I BSR
It is reasonable for the management of beta blockers after
surgery to be guided by clinical circumstances, independent of
when the agent was started.
IIa BSR
In patients with intermediate- or high-risk myocardial ischemia
noted in preoperative risk stratification tests, it may be
reasonable to begin perioperative beta blockers.
IIb CSR
In patients with 3 or more RCRI risk factors (e.g., diabetes
mellitus, HF, CAD, renal insufficiency, cerebrovascular
accident), it may be reasonable to begin beta blockers before
surgery.
IIb BSR
These recommendations have been designated with a SR to emphasize the rigor of support from the ERC’s
systematic review. See the ERC systematic review report, “Perioperative beta blockade in noncardiac surgery: a
systematic review for the 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of
patients undergoing noncardiac surgery” for the complete evidence review on perioperative beta-blocker therapy.
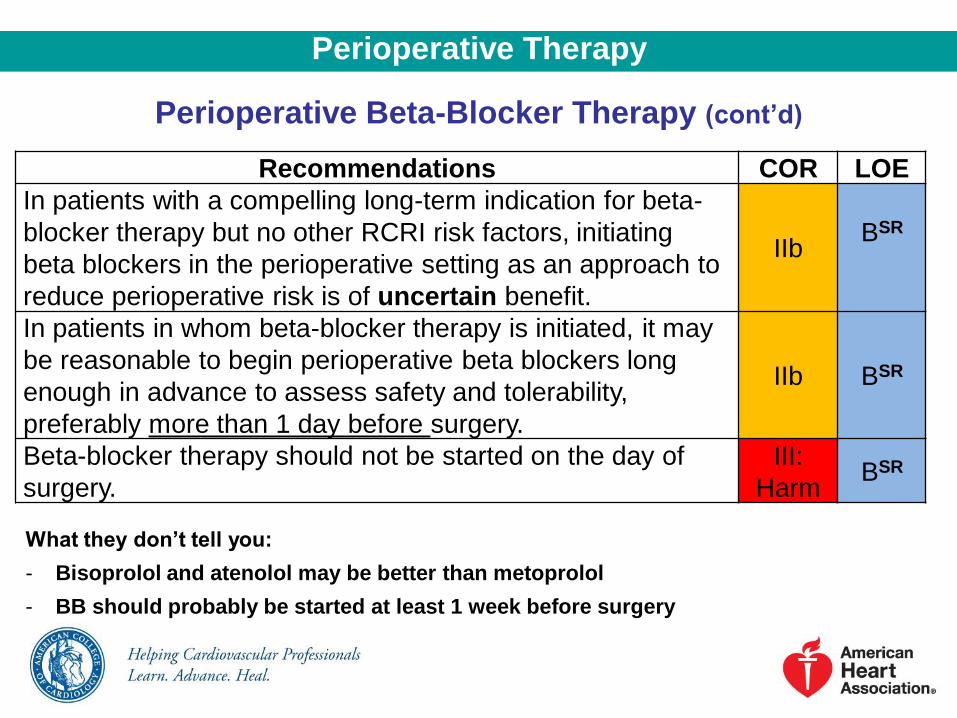
Perioperative Beta-Blocker Therapy (cont’d)
Recommendations COR LOE
In patients with a compelling long-term indication for beta-
blocker therapy but no other RCRI risk factors, initiating
beta blockers in the perioperative setting as an approach to
reduce perioperative risk is of uncertain benefit.
IIb BSR
In patients in whom beta-blocker therapy is initiated, it may
be reasonable to begin perioperative beta blockers long
enough in advance to assess safety and tolerability,
preferably more than 1 day before surgery.
IIb BSR
Beta-blocker therapy should not be started on the day of
surgery.
III:
Harm BSR
What they don’t tell you:
- Bisoprolol and atenolol may be better than metoprolol
- BB should probably be started at least 1 week before surgery
Perioperative Therapy
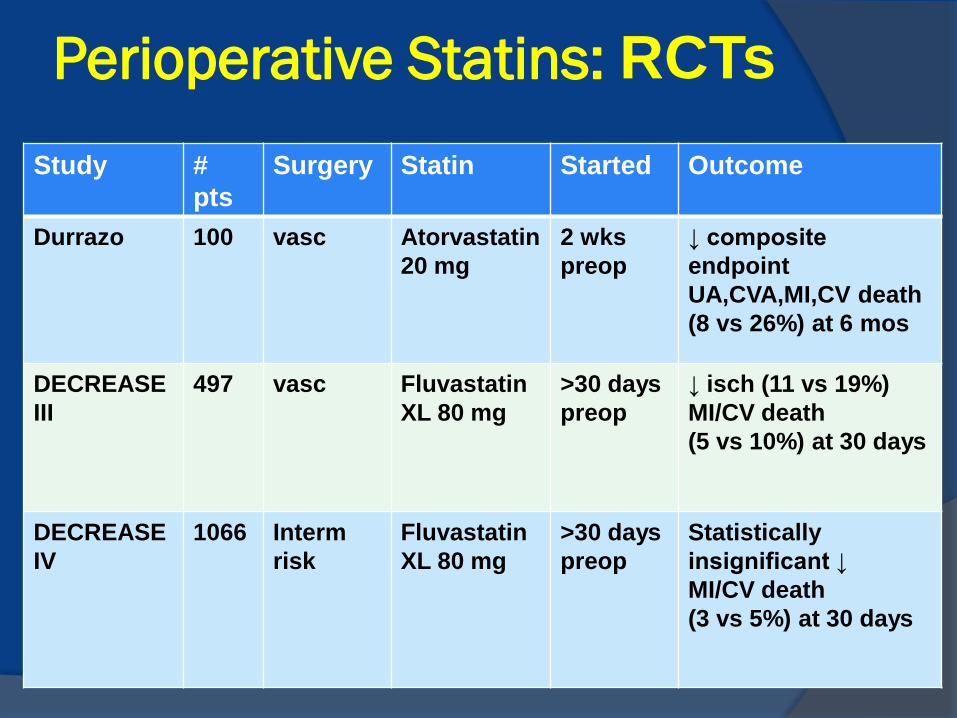
Perioperative Statins: RCTs
Study #
pts
Surgery Statin Started Outcome
Durrazo 100 vasc Atorvastatin
20 mg
2 wks
preop
↓ composite
endpoint
UA,CVA,MI,CV death
(8 vs 26%) at 6 mos
DECREASE
III
497 vasc Fluvastatin
XL 80 mg
>30 days
preop
↓ isch (11 vs 19%)
MI/CV death
(5 vs 10%) at 30 days
DECREASE
IV
1066 Interm
risk
Fluvastatin
XL 80 mg
>30 days
preop
Statistically
insignificant ↓
MI/CV death
(3 vs 5%) at 30 days
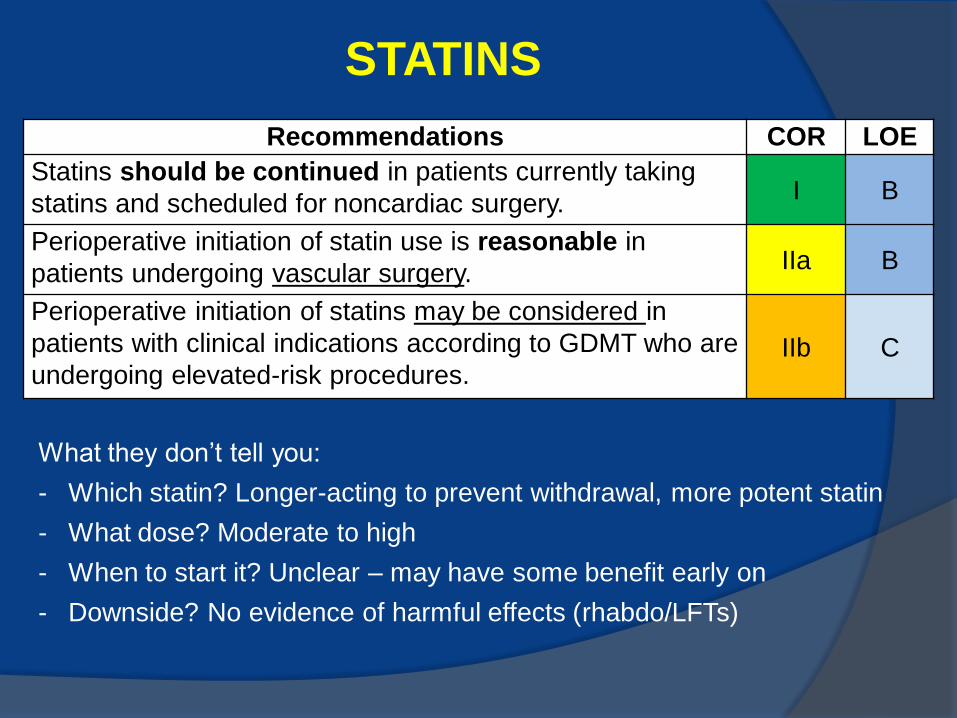
STATINS
What they don’t tell you:
- Which statin? Longer-acting to prevent withdrawal, more potent statin
- What dose? Moderate to high
- When to start it? Unclear – may have some benefit early on
- Downside? No evidence of harmful effects (rhabdo/LFTs)
Recommendations COR LOE
Statins should be continued in patients currently taking
statins and scheduled for noncardiac surgery. I B
Perioperative initiation of statin use is reasonable in
patients undergoing vascular surgery. IIa B
Perioperative initiation of statins may be considered in
patients with clinical indications according to GDMT who are
undergoing elevated-risk procedures. IIb C
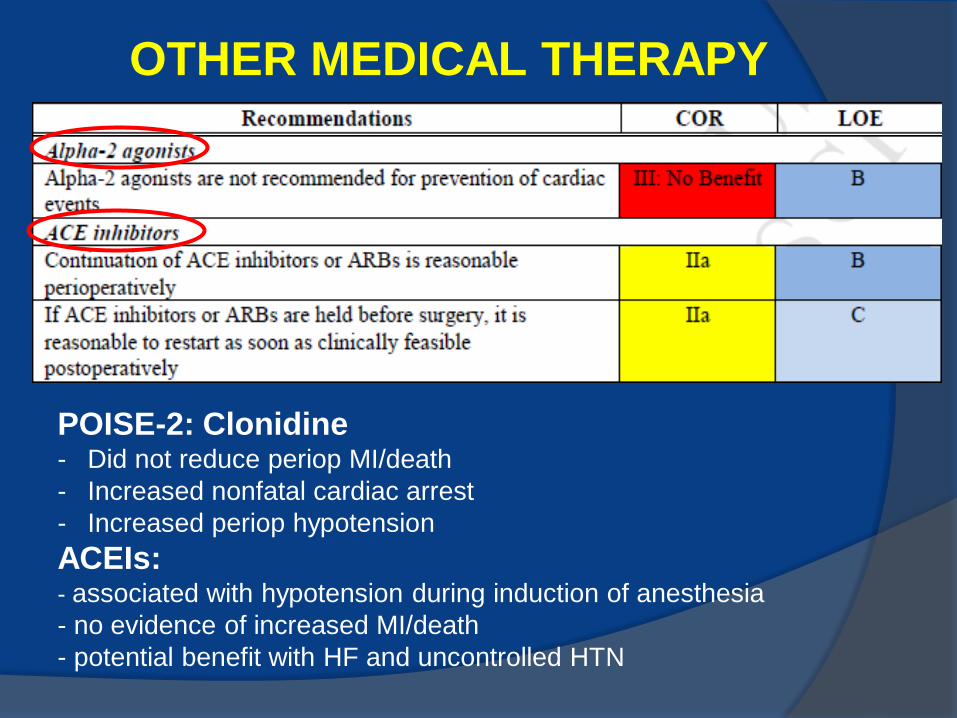
OTHER MEDICAL THERAPY
POISE-2: Clonidine - Did not reduce periop MI/death
- Increased nonfatal cardiac arrest
- Increased periop hypotension
ACEIs: - associated with hypotension during induction of anesthesia
- no evidence of increased MI/death
- potential benefit with HF and uncontrolled HTN
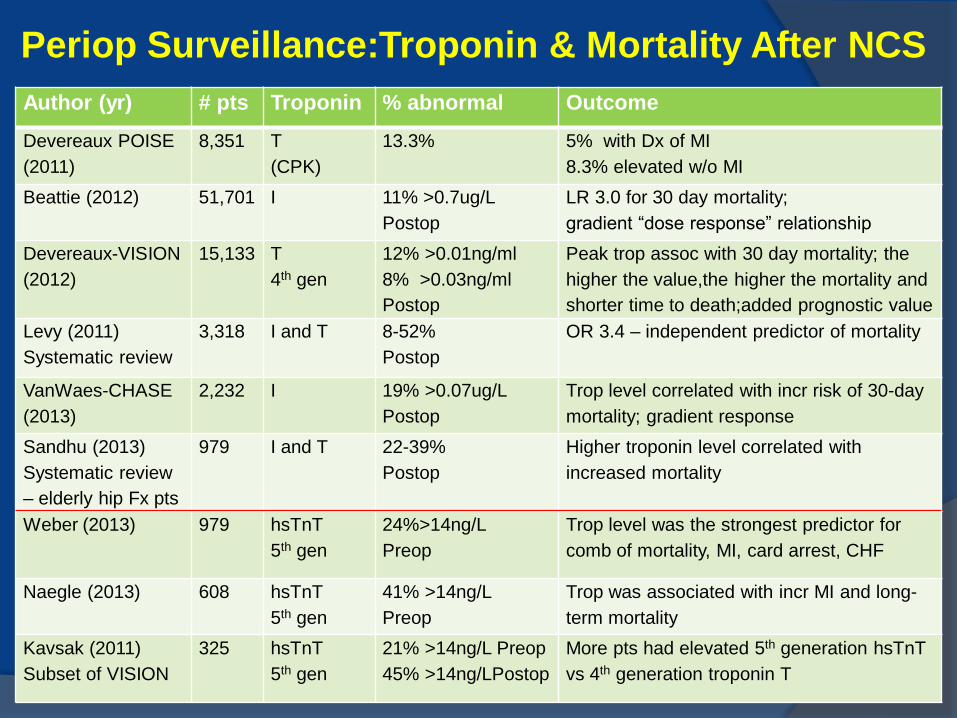
Periop Surveillance:Troponin & Mortality After NCS
Author (yr) # pts Troponin % abnormal Outcome
Devereaux POISE
(2011)
8,351 T
(CPK)
13.3% 5% with Dx of MI
8.3% elevated w/o MI
Beattie (2012) 51,701 I 11% >0.7ug/L
Postop
LR 3.0 for 30 day mortality;
gradient “dose response” relationship
Devereaux-VISION
(2012)
15,133 T
4th gen
12% >0.01ng/ml
8% >0.03ng/ml
Postop
Peak trop assoc with 30 day mortality; the
higher the value,the higher the mortality and
shorter time to death;added prognostic value
Levy (2011)
Systematic review
3,318 I and T 8-52%
Postop
OR 3.4 – independent predictor of mortality
VanWaes-CHASE
(2013)
2,232 I 19% >0.07ug/L
Postop
Trop level correlated with incr risk of 30-day
mortality; gradient response
Sandhu (2013)
Systematic review
– elderly hip Fx pts
979 I and T 22-39%
Postop
Higher troponin level correlated with
increased mortality
Weber (2013) 979 hsTnT
5th gen
24%>14ng/L
Preop
Trop level was the strongest predictor for
comb of mortality, MI, card arrest, CHF
Naegle (2013) 608 hsTnT
5th gen
41% >14ng/L
Preop
Trop was associated with incr MI and long-
term mortality
Kavsak (2011)
Subset of VISION
325 hsTnT
5th gen
21% >14ng/L Preop
45% >14ng/LPostop
More pts had elevated 5th generation hsTnT
vs 4th generation troponin T
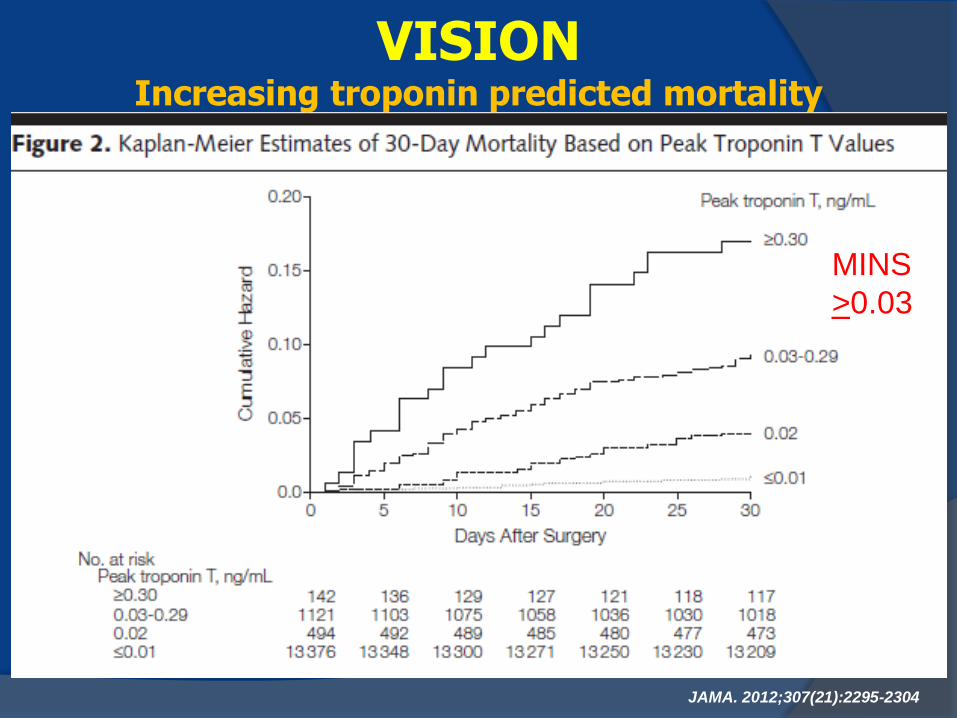
VISION Increasing troponin predicted mortality
JAMA. 2012;307(21):2295-2304
MINS
>0.03
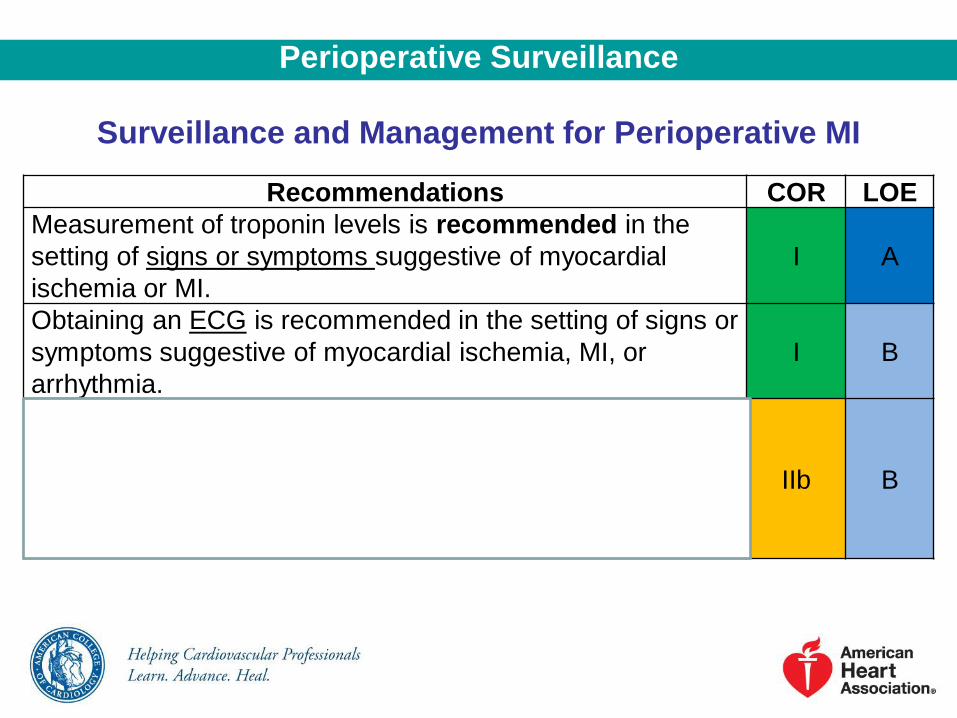
Perioperative Surveillance
Surveillance and Management for Perioperative MI
Recommendations COR LOE
Measurement of troponin levels is recommended in the
setting of signs or symptoms suggestive of myocardial
ischemia or MI.
I A
Obtaining an ECG is recommended in the setting of signs or
symptoms suggestive of myocardial ischemia, MI, or
arrhythmia.
I B
The usefulness of postoperative screening with troponin
levels in patients at high risk for perioperative MI, but
without signs or symptoms suggestive of myocardial
ischemia or MI, is uncertain in the absence of established
risks and benefits of a defined management strategy.
IIb B
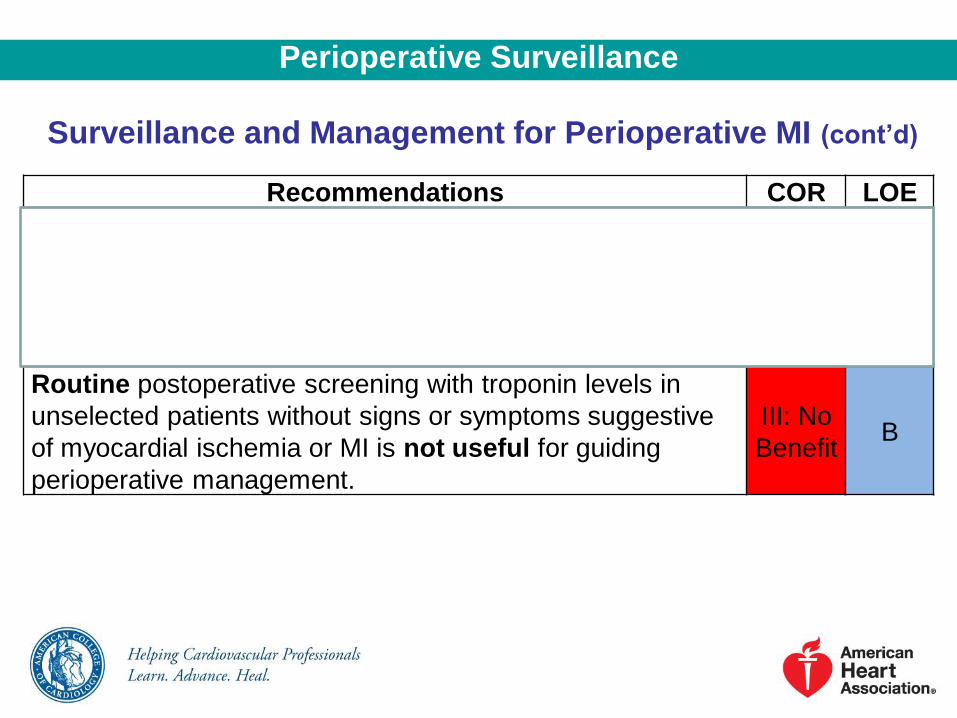
Surveillance and Management for Perioperative MI (cont’d)
Recommendations COR LOE
The usefulness of postoperative screening with ECGs in
patients at high risk for perioperative MI, but without signs
or symptoms suggestive of myocardial ischemia, MI, or
arrhythmia, is uncertain in the absence of established risks
and benefits of a defined management strategy.
IIb B
Routine postoperative screening with troponin levels in
unselected patients without signs or symptoms suggestive
of myocardial ischemia or MI is not useful for guiding
perioperative management.
III: No
Benefit B
Perioperative Surveillance
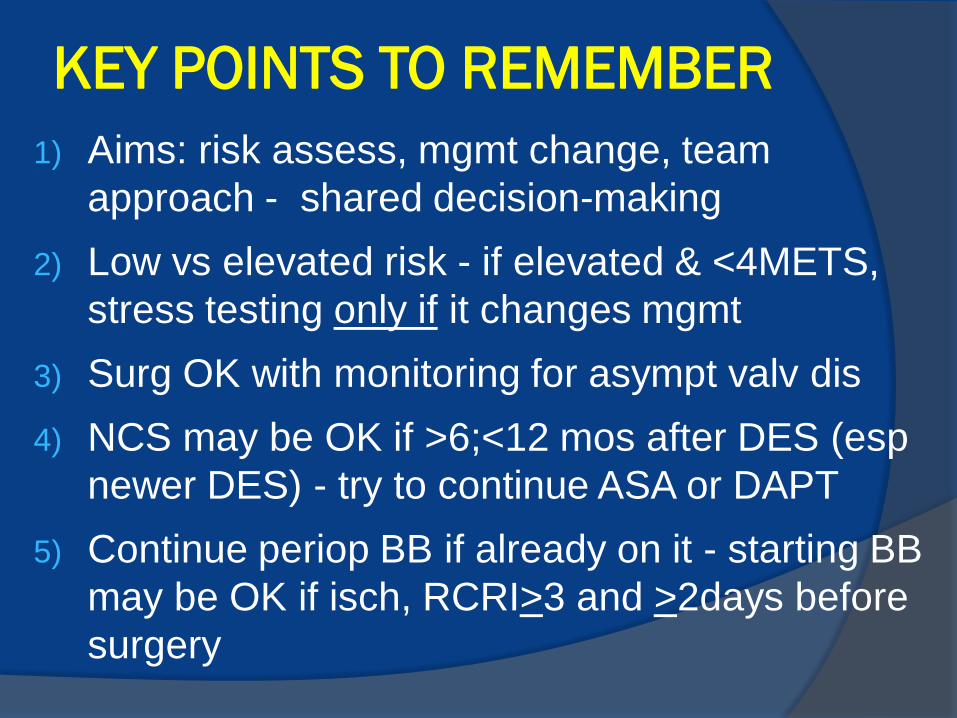
KEY POINTS TO REMEMBER
1) Aims: risk assess, mgmt change, team
approach - shared decision-making
2) Low vs elevated risk - if elevated & <4METS,
stress testing only if it changes mgmt
3) Surg OK with monitoring for asympt valv dis
4) NCS may be OK if >6;<12 mos after DES (esp
newer DES) - try to continue ASA or DAPT
5) Continue periop BB if already on it - starting BB
may be OK if isch, RCRI>3 and >2days before
surgery





























