Pay-for-Performance Programs: the U.S. Experience
Eric Schneider, M.D., M.Sc.Harvard School of Public HealthBrigham and Women’s Hospital
Boston, MA


“Market-oriented” strategies for health care: a 20-year journey
Performance Visibility
Performance Rewards
Peers PatientsPublic Purchasers
PerformanceFeedback
Market Share Payments &Penalties
“Report Cards” “P4P”


Public Reporting:Limited Evidence of Impact
• Cardiac surgery patients did not use risk-adjusted mortality results on hospitals, surgeons
• Consumers are often befuddled by report cards
• Scant evidence that consumers use health plan report cards to select plans

PATHWAY 1
Results(Performance)
Knowledge aboutPerformance
Knowledge aboutProcess and Results
Care Delivery Teams and
Practitioners
ChangeSelection
Measurement for Improvement
OrganizationsConsumersPurchasersRegulators
PatientsHealth Plans
CliniciansAccreditors
Selection & Accountability
Purpose of Measurement
Goals PATHWAY 2
Two Pathways to Quality Improvement
Motivation
$$$

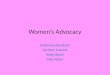
The PAY in Pay-for-Performance
Medicare
$242 billion
Private Health
Insurance
$496 billion
Out-of-pocket
$206 billion
Medicaid
$224 billion
Other public
$180 billion
Other private
$76 billion
Total U.S. Health Expenditures (2001) = $1.4 trillion
Source: Katharine Levit, et al., “Trends in U.S. Health Care Spending, 2001,”Health Affairs (January/February 2003)
5%17%
16%
13%35%
14%

Private Payers: 242 U.S. Health Plans on P4P
• 71% had programs to pay for performance
• 68% had P4P for physicians
• 42% had P4P for hospitals
Survey Data, 2005

Private Health Plans: Expanding Scope of P4P
• Broad range of total dollars and ambition – Thinking about it
– Modest payments, a few specific measures
– Large payments, many measures, grants for IT
– Tiered networks

Public Payers: Many New Demonstration Projects Under Way• Centers for Medicare and Medicaid Services
– Premier Hospital Demonstration– Physician Voluntary Reporting Initiative
• Medicaid state agencies– Eleven state agencies using some form of P4P with
health plans– Center for Health Care Strategies (CHCS) recently
initiated P4P Purchasing Institute for Medicaid agencies

Premier Hospital Demo• 2003-2006• 278 hospitals participate voluntarily• 34 process and outcome measures
– Heart failure, heart attack, pneumonia, coronary artery bypass graft and knee replacements
• Hospitals can receive bonus based on performance– Top decile: 2% bonus on DRG payment for the condition– Second decile: 1% bonus
• Year 1 bonus incentive payments: – $900 to $847,000

P4P: Does it Work?Early Results Paint a Nuanced Picture
• Quality improved– Pre-post evaluations without control groups
• Quality improved slightly or not at all– Quasi-experiments with contemporaneous
comparison groups
• Success and failure appear related to many complex factors– Program design– Implementation

Factors Related to P4P Success and Failure
• Sponsor leverage in fragmented payment environments
• Amount of incremental revenue• Selection, scope, and perceived validity of
quality measures• Design of payout (low-performing
practices?)• Readiness of physician practices for QI• Effectiveness of QI innovations

Concerns about P4P in the U.S.
• Business model for development and maintenance of standardized quality and efficiency measure sets?
• Is the data infrastructure adequate for valid measures?
• How will “gaming” be addressed?• Is “new money” needed to retool MD practices?• Will P4P undermine professionalism?• Will P4P impede access and increase
socioeconomic disparities in quality?

Conclusions
• Pay-for-performance has captured attention
• First formal evaluations show mixed results
• Many questions remain unanswered, but funding for rigorous evaluation may be limited
Recommended