Hirsutism & Virilization
Assoc. Prof. Gazi YILDIRIM, M.D.
Yeditepe University, Medical Faculty Dept of Ob&Gyn

• To define– Hirsutism
• To learn– Androgen biosynthesis
• To treat– Hirsutism
Objectives


HIRSUTISM APPEARANCE OF EXCESSIVE COARSE
(TERMINAL)HAIR IN A PATTERN NOT NORMAL IN THE FEMALE
• Definition highlights the abnormal distribution of excess hair growth ,such as facial ,chest,or upper abdominal hair

HYPERTRICHOSIS GROWTH OF HAIR IN EXCESS OF THE NORMAL
WHILE LIMITED TO A NORMAL PATTERN OF DISTRIBUTION
• It is frequently associated with the use of medication such as antiepileptics
VIRILIZATION REFERS TO CONCURRENT PRESENTATION OF HIRSUTISM WITH A BROAD RANGE OF SIGNS SUGGESTIVE OF ANDROGEN EXCESS,SUCH AS
• ACNE,• FRONTOTEMPORAL BALDING,• DEPPENING OF THE VOICE ,• A DECREASE IN BREAT SIZE• CLITORAL HYPERTROPHY
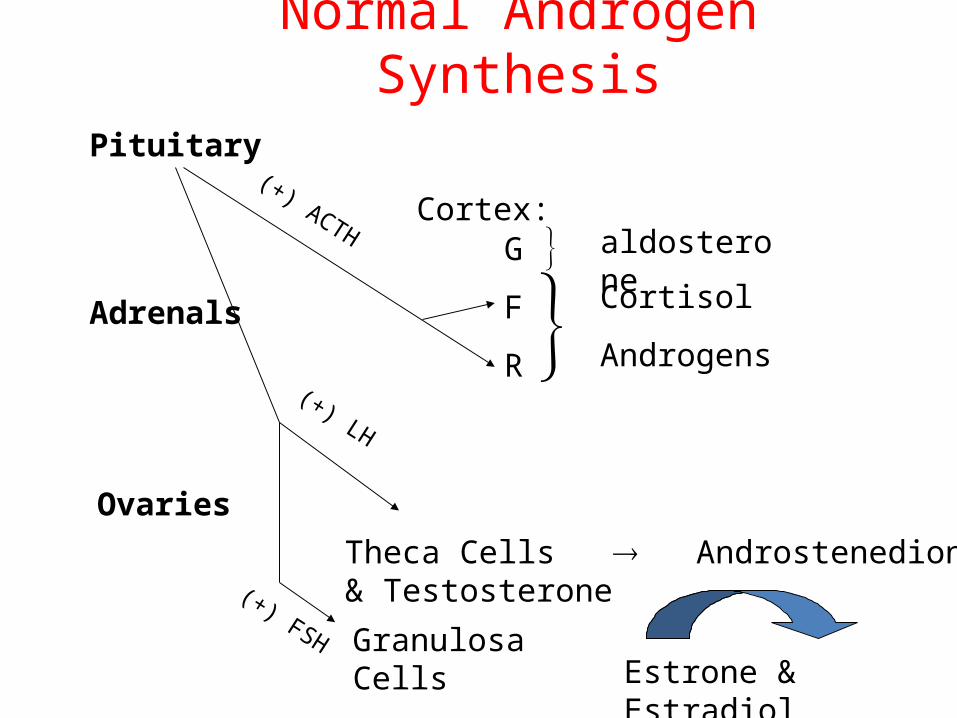
Normal Androgen Synthesis
Pituitary
Ovaries
Adrenals
G
F
R
Cortex:
aldosterone Cortisol
Androgens
(+) ACTH
Theca Cells Androstenedione & Testosterone
Granulosa CellsEstrone & Estradiol
(+) FSH
(+) LH

Sitokrom P450 scc
17 α OH ase 17 α OH ase
17-20 Desmolase
17 β OH SDH 17 β OH SDH
17-20 Desmolase ?
5 α redüktase
Asetat
Kolesterol
Pregnanolon Progesteron
17 OH Pregnanolon 17 OH Progesteron
DHEA Androstenedion
Androstenediol Testosteron
DHT
E2
E1
E3
3 β
OH
SD
H
17 β OH SDH
AROMATAZ
AROMATAZ

T Androstenedion DHEA
Adrenal Korteks
Over
%25
%25
%50
%50
%50
%50
%20
%100
%30 DHEAS

In women Major circulating androgens (in descending order of serum concentration)
• DHEA-S (100-350 micg/dl)
• DHEA (1-10 ng/ml)
• Androstenedion (0.5-2.0 ng/ml)
• Testosterone (20-80 ng/dl)
• DHT

EXCESS REPONSIVITY TO ANDROGEN
TESTOSTERONE
5-ALPHA -REDUCTASE
DIHIDROTESTOSTERONE
DHT
• Major nuclear androgen• Produced only in the periphery• Circulating level is low and do not reflect the 5
alpha reductase activity
• 3alpa androstenediol glucuronide (3alpha-AG) is the peripheral metabolite of DHT and can be used as a marker of peripheral androgen metabolism.
• Low clinical utility…

%80 SHBG
%19 Albumin
%1 serbest
T
%69 SHBG
%30 Albumin
%1 serbest
E2
%8 SHBG
%85 Albumin
%7 serbest
Androstenedion
%18 CBG
%80 Albumin
%2 serbest
P4

%78 SHBG
%19 Albumin
%3 serbest
T (200-800 ng/dl)
Men
%80 SHBG
%19 Albumin%1 serbest
T (20-80 ng/dl)
Normal Women
%79 SHBG
%19 Albumin%2 serbest
T (20-80 ng/dl)
Hirsute Women

Causes of Hirsutism (1)AdrenalCongenital adrenal hyperplasia
21-hydroxylase deficiency11 -hydroxylase deficiency3 -hydroxysteroid dehydrogenase deficiency
Cushing’s syndromeAndrogen-secreting adrenal tumors

Causes of Hirsutism (2)Ovarian Androgen-secreting ovarian neoplasms
Sertoli-leydig cell tumorsGranulosa-theca cell tumorsHillus-cell tumors
Pregnancy-relatedLuteomaHyperreactive leuteinalis
Hyperthecosis Polycystic ovary syndrome

Causes of Hirsutism (3)Exogeneous medications Hormonal
Anabolic steroidsDanazolOral contraceptives containing androgenic progestinsGlucocorticoidsACTHMetyrapone

Causes of Hirsutism (4) Not-Hormonal
Diazoxide Phenytoin Psoralens Streptomycin Phenothiazine Minoxidil
Severe insulin resistance syndromes Hyperprolactinemia SHBG defect (primary or secondary) Menopause Idiopathic hirsutism Idiopathic hyperandrogenism

Physical Exam
• Hair pattern• Balding• Body habitus• Female contours• Atrophic breast changes• Clitoromegaly• Ovarian masses• Cushingoid features• Acanthosis nigricans (associated w/ PCOS)

Laboratory investigation
Indication
Ultrasonography Identification of the adrenal/ovarian tumorto demonstrate PCO
FSH-LH-Estradiol Evaluation of gonadal axis
Testosterone Demonstration of androgen excess (mostly indicate ovarian source)
DHEAS Demonstration of androgen excess (mostly indicate adrenal source)
17-OH P When NCAH considered
ACTH test Hormonal diagnosis of NCAH
Suggested laboratory investigations in hirsute women
Unluhizarci K, Yilmaz S, Kelestimur F. Women’s Health, 2005

Lab.Evaluation of Hirsutism
Three basic hormonal evaluation1. Total testosterone2. DHEAS3. AM 17-hydroxyprogesterone
Diagnosis & Evaluatoin
• T, androstenedione, DHEAS – adrenal source– Abdominal CT & medical tests r/o CAH or Cushings
• DEAHS normal or minimally elevated– Ovarian source– Pelvice U/S r/o tumor
• Elevated LH-FSH ratio– Ratio>3 suggests PCOS
• Rapid Onset Virilization w/ T>200ng/dL– May indicate ovarian neoplasm

Total TestosteroneNormal Value (0.2 –0.8 ng/ml) - (20 –80 ng/dl)
>150-200 ng/dl

DHEAS (100-350 micg/dl)
>700 micg/dl

17 –hydroxyprogesterone (<0.2) ng/ml ) - (<200) ng/dl )
<200 ng/dl 200-800 ng/dl >800 ng/dl
<1000 ng/dl >1000 ng/dl


TreatmentTreatment1-1-General principlesGeneral principles
--Detection and treatment of the underlying diseaseDetection and treatment of the underlying disease
--Multidisciplinary interventionsMultidisciplinary interventions
--Obesity treatmentObesity treatment
2-2-Drug therapyDrug therapy
--Adrenal suppressionAdrenal suppression
--Ovarian suppressionOvarian suppression
--Anti-androgen therapyAnti-androgen therapy
--ThTherapy for insulin resistanceerapy for insulin resistance
3-3-Cosmetic therapyCosmetic therapy
4-4-Education and psychotherapyEducation and psychotherapy
5-5-Combination therapy methodsCombination therapy methods

The management of hirsutism depends on; 1-Underlying cause, 2-Contraceptive needs, 3-Patient’s preference
At least 6-9 months of treatment is necessary for clinical response

THERAPEUTIC OPTIONSGENERAL MEASURES :• Eliminating causative factors• Optimizing weight• Manage hairBleachingCutting or shavingElectrolysisLaser epilation

THERAPEUTIC OPTIONSManagement of excess ovarian androgen production :Standard therapy is :combined E+P,most commonly
OCs• It reduces ovarian androgen production• It increases SHBG• It induces competition at the cellular level for binding
to the androgen receptor

THERAPEUTIC OPTIONSChoice of OC• EE + Norgestimarte approved in USA• Cyproterone acetate used as progesterone
component in OcsOVARIAN SUPPRESSION BY LONG ACTING GnRH
ANALOGUE• Can be used for functional ovarian androgen
overproduction and even for malignant condition• But to be used for long with back-up

THERAPEUTIC OPTIONS• Long acting GnRH analogues used• But there is doubt that this therapy will be
beneficial over Ocs• INSULIN SENSITIZING AGENTS:
For PCO with acanthosis nigicansCommonly used agent is : Metformin andTroglitazone,Pioglitazone,Rosiglitazone

THERAPEUTIC OPTIONS• MANAGEMENT OF EXCESS ADRENAL
ANDROGEN PRODUCTION• Metabolic correction of the disorder,usually
with exogenous steroids• Dexamethasone,mostly used,But LIMITED
ROLE

THERAPEUTIC OPTIONSManagement directed to the target organ and
cells• Competition with Androgen receptors:
– Spironolactone,– Flutamide, – Ketoconazole,– Cyproterone acetate
• 5-alpha reductase Inhibitors :– Finasteride

Mechanisms of anti-androgen treatmentMechanisms of anti-androgen treatment
1)1) Gonadotropin suppression Gonadotropin suppression
2)2) Stimulation of SHBG synthesis Stimulation of SHBG synthesis
3)3) Inhibition of 5- Inhibition of 5- reductase enzyme reductase enzyme
4)4) Binding to androgen receptor Binding to androgen receptor
5)5) Effects to steroid biosynthesis Effects to steroid biosynthesis

Mechanisms of actions of the commonly used anti-androgens
Androgen receptor blockade
Clearence of
androgens
Effect on LH
secretion
Glucocorticoid activity
5-a reductase
activity
Progestogen
like activity
Cyproterone acetate + + + + - +
Spironolactone
+ + - - - +
Drospirenone
+ + + - - -
Flutamide + - - - - -
Finasteride - - - - + -

SpironolactoneSpironolactone
**Synthetic steroidSynthetic steroid
**Aldosterone and androgen antagonistAldosterone and androgen antagonist
**Competition with DHT for binding to receptorsCompetition with DHT for binding to receptors
**Inhibition of androgen synthesisInhibition of androgen synthesis

Cyproterone acetateCyproterone acetate
**A steroidic anti-androgen derivated from 17-A steroidic anti-androgen derivated from 17-
hydroxyprogesteronehydroxyprogesterone
**Inhibitory effect to testosterone and Inhibitory effect to testosterone and
dihydrotestosterone by binding to dihydrotestosterone by binding to
intracellular receptorsintracellular receptors
**Decreased ovarian testosterone production Decreased ovarian testosterone production
due to inhibition of LH secretiondue to inhibition of LH secretion
**There is a low glucocorticoid effectThere is a low glucocorticoid effect

Cyproterone AcetateCyproterone Acetate
Side effectsSide effects
Weight gainEdemaDecreased libidoHeadacheVomitingHepatotoxicityFatigueEnlarged mammary glandsMood changes

FinasterideFinasteride
**5 5 -reductase inhibitor-reductase inhibitor
**Inhibits conversion of testosterone to DHTInhibits conversion of testosterone to DHT
**It does not bind to androgen receptorsIt does not bind to androgen receptors
**There is no effect in testosterone secretionThere is no effect in testosterone secretion

FlutamideFlutamide
**Non-steroid, periferic androgen antagonistNon-steroid, periferic androgen antagonist
**Inhibitory effect in steroid biosynthesis (adrenal)Inhibitory effect in steroid biosynthesis (adrenal)

Eflornithine hydrochloride 13.9%
• Eflornithine 13.9% cream is a topical treatment that does not
remove the hairs, but acts to reduce the rate of growth and
appears to be effective for unwanted facial hair on the mustache
and chin area.
• It can be used in combination with other treatments to give
the patient the best chance for successful hair removal.
• Eflornithine acts as an inhibitor of L-ornithine
decarboxylase which may be important in controlling hair
growth and proliferation

Recommended