Volume 40 Number 4 October – December 2014 Thai Journal of Anesthesiology 237
Gabapentin as an Adjuvant Analgesic with Opioids
for the Management of Metastatic Bone Pain:
Randomized, Double - Blind, Placebo - Controlled
Crossover Trial
* กลุ่มงานวิสัญญีวิทยา, *กลุ่มงานอายุรกรรม โรงพยาบาลมหาราชนครราชสีมา จ.นครราชสีมา,
** ภาควิชาวิสัญญีวิทยา คณะแพทยศาสตร์โรงพยาบาลรามาธิบดี มหาวิทยาลัยมหิดล กรุงเทพ
จตุพร ถ่อนสันเทียะ, พ.บ.*, วราภรณ์ ไวคกุล, พ.บ.**,
วันทกานต์ วงศ์วิกรม, พ.บ. *, ครองกมล สีหบัณฑ์, พ.บ. ***
Abstract: Gabapentin as an Adjuvant Analgesic with Opioids for the Management of
Metastatic Bone Pain: Randomized, Double - Blind, Placebo - Controlled Crossover
Trial
Jatuporn Thonsontia, M.D.*, Waraporn Waikakul, M.D.**,
Wantakan Wongwikrom, M.D.* Khrongkamol Sihaban, M.D.* **
Department of Anesthesiology*, Department of Internal Medicine***, Maharat Nakhon
Ratchasima Hospital, Nakhon Ratchasima 30000
Department of Anesthesiology**, Faculty of Medicine, Ramathibodi Hospital, Mahidol
University, Bangkok 10400, Thailand.
Background: Bone metastasis usually
causes severe pain in cancer patients. The solely
use of opioid may be inadequate or exert intolerable
side effects. Experts suggested the use of analgesic
adjuvants. However, gabapentinoids; anticonvulsants
used to treat neuropathic pain, are frequently added
_15-0191(237-252)P3.indd 237 2/25/15 2:24:55 PM

238 วิสัญญีสาร ปีที่ 40 ฉบับที่ 4 ตุลาคม – ธันวาคม 2557
to the pain control regimen. There is no evidence
that gabapentin is useful in controlling pain due
to bone metastasis. Objectives: To assess the
analgesic efficacy and side effects of gabapentin
900 mg/day compared with placebo as add-on
therapy to opioids in patients with metastatic bone
pain. Methods: The study is a randomized, double-
blinded, fix - dose, placebo-controlled crossover
trial. Thirty - two patients, who were on stable dose
of opioids for the treatment of metastatic bone
pain, were randomly allocated into 2 treatment
groups, 16 each. Patients in each group received 2
treatment periods with 4 - day washout in between;
10 days for gabapentin or matching placebo and
reciprocal. The subjects took either gabapentin 900
mg/day or placebo in identical pattern. Overall
time was 24 days during the double-blind treatment
period. The subjects were contacted by phone
on day 2, 4, 8, 16, 18 and 22 following a dose
adjustment to assess compliance and tolerability.
The subjects were followed up at clinic on day 1,
15 and 25. Outcome comparisons were; average
pain score reduction on day 1 and day 8 of each
period, percentage of patients who have average
pain score reduction ≥ 3, amount of rescue
analgesic and side effects. Results: Of the 32
patients enrolled, 30 patients received gabapentin
and 26 patients received placebo. Analysis of
covariance (ANCOVA) on the intention-to-treat
basis showed no significant difference in average
pain score reduction between gabapentin and
placebo group; 2.77 ± 2.10 vs 2.46 ± 1.25, (p =
0.533). Percentage of patients who had average
pain score reduction ≥ 3 during follow-up days
were not different (53.23 ± 2.81 vs 47.44 ± 3.53),
p = 0.586. Rescue medication for breakthrough
pain was not different (p = 0.607). Finally,
incidence of side effects; sedation, dizziness,
nausea, vomiting and constipation, were not
different. Conclusions: Adding gabapentin to
opioid analgesic did not accentuate efficacy of
opioids in relieving pain in metastatic bone pain
patient.
Key words: Gabapentin, metastatic bone pain,
opioids
Introduction Bone is one of the most common metastatic
site of common tumors such as breast, lung and
prostate cancers.1,2 In addition to severe pain, bone
metastasis is associated with pathologic fractures,
spinal cord compression, hypercalcemia, reduced
quality of life, decreased physical-social function
and increased depression and anxiety.3,4
The first line treatment for metastatic bone
pain is analgesics. The World Health Organization
recommended 3-step ladders starting with non-
opioids to relieve mild to moderate pain. If pain
still persists or increases, step 2 weak opioids such
as codeine or tramadol is added. For persistent or
moderate to severe pain, strong opioids such as
_15-0191(237-252)P3.indd 238 2/25/15 2:24:55 PM

Volume 40 Number 4 October – December 2014 Thai Journal of Anesthesiology 239
morphine, fentanyl or methadone are used.
Background pain is usually controlled by slow-
released opioids; such as morphine sulfate
sustained release tablet (MST continus® and
kapanol®) or fentanyl transdermal patch, which
should be given around the clock. Breakthrough
pain may be treated with an immediate release
opioid.5, 6
In many patients, if the bone pain is
localized, radiotherapy is the treatment of choice.5
But for some patients who have widespread lesions,
bisphosphonates is an alternative. Bisphosphonates
inhibit osteoclast activity. They decrease hyper -
calcemia and the subsequent risk of fractures
in addition to reducing bone pain.7 Usually,
moderate-to-high doses of opioids may be required
to achieve pain control in these patients. Opioids
have significant dose-dependent side effects such
as nausea, vomiting, sedation and constipation.
Therefore, adjuvant drugs; mainly antidepressants
or anticonvulsants, are used to improve analgesic
effectiveness with less opioids doses.
Even though tumor is confined in the bone,
metastatic bone pain is caused by tumor - derived
inflammation. In addition, the products released by
the tumor which injure the primary afferent nerve
fibers that innervate the bone are also the causes of
pain. These signify neuropathic mechanisms.8,9
The metastatic bone pain were both ongoing and
movement-evoked pain. Opioids are mainly
effective in background pain, which may explain
why high doses of opioids do not provide sufficient
pain relief.
Since the pain is not only nociceptive but
also neuropathic, mechanism-based therapy which
is the addition of anticonvulsant/antidepressant
into opioids regimen is reasonable. Data from
randomized study of pregabalin in patients with
cancer-induced bone pain indicates that pregabalin
may reduce metastatic bone pain (interim analysis).10
Gabapentin also has analgesic effect in several
nonmalignant chronic neuropathic pain and cancer
pain that has neuropathic component when
combined with opioid analgesics.11 Additionally,
previous study found that gabapentin attenuated
both ongoing and movement-evoked bone cancer-
related pain behaviors in animals. However, it did
not influence tumor growth or tumor-induced bone
destruction.12 Currently, no clinical data suggests
that gabapentin can enhance opioids analgesia but
the analgesic benefit of this popular practice is the
off-label use. Therefore, the aim of this study is to
assess the efficacy and safety of adding gabapentin
to opioid analgesia in relieving metastatic bone
pain.
Methods The study was a randomized, double-
blinded, fix - dose, placebo - controlled crossover
trial. It was approved by the Institutional Review
Board of Maharat Nakhon Ratchasima Hospital.
Informed consent was obtained from all the
patients. The enrolled patients were patients with
metastatic bone pain, both in the inpatient and
outpatient departments, at Maharat Nakhon
Ratchasima Hospital from September 2013 to
_15-0191(237-252)P3.indd 239 2/25/15 2:24:56 PM

240 วิสัญญีสาร ปีที่ 40 ฉบับที่ 4 ตุลาคม – ธันวาคม 2557
October 2014.
Inclusion criteria were: (1) age ≥ 18 years,
(2) cancer with at least one metastatic bone lesion
and bone pain was the major pain. Bone metastasis
was established by radiographic confirmation such
as CT scan, MRI and bone scan. (3) Average pain
score in the last 24 hours was ≥ 4 (assessed on a 0
to 10 numerical rating scale (NRS) at the screening
visit. (4) Life expectancy was ≥ 30 days and
Palliative Performance Scale (PPS) was ≥ 3013. (5)
On regular and stable dose of basal opioids. Stable
opioid use was defined as constant for at least 24
hours with rescue morphine sulfate solution (MSS)
≤ 3 doses/day. And finally, (6) opioid related side
effects was ≤ Grade 2 of Common Terminology
Criteria for Adverse Events (CTCAE) Version
4.0.14
Exclusion criteria were hypersensitivity to
gabapentin, unable take oral medication, creatinine
clearance < 60 mL/min (calculated by the Cockcroft-
Gault equation), gabapentin ≥ 900 mg/day
or pregabalin ≥ 150 mg/day consumption at
screening, pathologic fracture, spinal cord com -
pression or cauda equina syndrome, chemotherapy
within 2 weeks before screening15 and radiotherapy
to the pain-producing lesion within 1 month before
screening.15
Figure 1 and 2 show scheme of the study.
Patients were randomly allocated into 2 treatment
groups by computer in a non - stratified block - of -
four. Each group of patients received 2 treatment
periods with 4 - day washout in between; gabapentin
or matching placebo. Study medications were in
identical appearance capsules containing either 300
mg of gabapentin (Neurontin®, Pfizer) or placebo.
They were prepared in sealed envelopes by the
hospital pharmacist who was not involved in the
study. All participants and researchers were
blinded to the group allocation. The treatment
phase started on the day of the screening visit (day
1). In addition to the aforementioned inclusion and
exclusion, the patients were screened for ongoing
non-opioid or gabapentinoid use and washout for 4
days was done before recruitment. At first visit, the
patients were taught about how to complete daily
pain diary and the use of rescue analgesics by p.r.n.
doses of MSS if NRS was ≥ 4. The pain diaries
were filled daily by the patient or their caregiver.
During the study, the patients took either
gabapentin (300 mg) or placebo in identical
pattern; at bed time on day 1, bid on day 2. If the
patients tolerated, the doses were increased to
3 times a day on day 3 through day 8. Day 9 and 10
were the tapering off days; bid and OD respectively.
Day 11 through day 14 were the washout period.
Then the study was repeated with the comparing
drug in the same manner on day 15 through day 24.
Overall study period was 24 days.
The patients were assessed at pain clinic on
day 1 (screening and randomization visit), days 15
and 25. They were contacted by phone by one of
the researchers following a dose adjustment to
assess compliance, tolerability and pain diary
completion. Telephone contact was done on the
day 2, 4, 8, 16, 18 and 22. Previous adjuvant
analgesics were unchanged throughout the study
_15-0191(237-252)P3.indd 240 2/25/15 2:24:56 PM

Volume 40 Number 4 October – December 2014 Thai Journal of Anesthesiology 241
period. Demographic data, primary tumor site,
Palliative Performance Scale, oral morphine daily
equivalent dose and side effects, concomitant pain
medication, pain on average in the last 24 hours at
the screening visit, right now pain, and best and
worst pain scores in the last 24 hours were
recorded.
Patients could be withdrawn from the trial at
any time of the study. Any other analgesics apart
from MSS were not allowed during the study
period. The patient was withdrawn if there were ≥
grade 3 adverse events on CTCAE version 4.0,
patients needed more than three daily p.r.n. MSS
doses, extreme unexpected events such as gut
obstruction, brain metastasis, unable to take
oral medication, bone fractures, chemotherapy,
radiotherapy, bisphosphonate therapy or surgery
during the treatment phase for disease control, and
finally, noncompliance: missing ≥ 2 consecutive
days of study medication or less than 80% study
medication.
Primary outcome of the study was to
determine the analgesic efficacy. The primary
efficacy was defined as the average pain score
reduction between day 1 and day 8 of each study
period. Secondary outcome comparisons were
percentage of patients who had pain intensity at
least 3 points average pain score reduction for
follow-up days, amount of rescue MSS for
breakthrough pain, and incidence of side effects
such as sedation, dizziness, nausea, vomiting and
constipation.
Statistical Methods A sample size was determined from a
minimum difference of mean pain score reduction
between the two groups equaled to two16, assumed
that standard deviation (SD) was 2.5. The power
was 80% and two - tailed α was 0.05. Calculation
resulted in 26 patients per group. To compensate
for 20% attrition rate, we included 32 patients.
Analysis of the analgesic efficacy was performed
by an analysis of covariance (ANCOVA). Intention -
to - treat (ITT) basis was used for the main
analysis. The percentage of patients achieving
average pain score reduction at least 3 was plotted
by day.
Chi - square test was used to analyze safety
data using ITT basis. Statistically significance was
when p < 0.05.
_15-0191(237-252)P3.indd 241 2/25/15 2:24:56 PM

242 วิสัญญีสาร ปีที่ 40 ฉบับที่ 4 ตุลาคม – ธันวาคม 2557
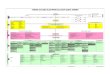
Figure 1 Study protocol flow chart
_15-0191(237-252)P3.indd 242 2/25/15 2:24:57 PM

Volume 40 Number 4 October – December 2014 Thai Journal of Anesthesiology 243
Figure 2 Protocol flowchart and follow up
_15-0191(237-252)P3.indd 243 2/25/15 2:24:58 PM

244 วิสัญญีสาร ปีที่ 40 ฉบับที่ 4 ตุลาคม – ธันวาคม 2557
Figure 3 Enrollment of study participants.
Results Patient enrollment
In Figure 3, thirty - two patients were eligible
and randomly assigned; 30 in gabapentin and 26 in
placebo group. Two patients in gabapentin group
were excluded because one had chemotherapy
during period B and another one had radiation
in period A. Six patients in placebo group were
excluded; period B chemotherapy 1, period B
pamidronate 1, period A radiation 1, period B
radiation 1, period B loss to follow up 2. Finally,
30 patients in gabapentin group and 26 in the
placebo group completed the 24 - day study protocol.
Patient Demographic and Baseline Clinical
Characteristics
Demographic and baseline pain characteristics
of the patients are shown in Table 1. Both groups
were comparable in age, sex, primary tumor site,
metastatic bone lesion as the major pain, Palliative
Performance Scale, stabilized oral morphine daily
equivalent in mg and side effects, concomitant pain
medication, average pain score in the last 24 hours,
right now pain, best pain scores in the last 24 hours
and worst pain scores in the last 24 hours. The
majority of patients had anticonvulsant analgesic
_15-0191(237-252)P3.indd 244 2/25/15 2:24:58 PM

Volume 40 Number 4 October – December 2014 Thai Journal of Anesthesiology 245
include gabapentin <900 mg/day and pregabalin
<150 mg/day before recruitment. The demographic
characteristics of patients were comparable.
Table 1 Demographic characteristics of the patients
Gabapentin (n = 30) Placebo (n = 26) p - value
Age, year (mean±SD)
Sex, n (%)
Male
Female
Primary tumor site, n (%)
Lung
Breast
Hepatobiliary
Colon-rectum
Head & neck
Gynecological
Urological
Unknown
Others
Metastatic bone lesion as the major pain, n (%)
Spine
Long bone/extremities
Pelvis
Rib, clavicle
Chest wall
Palliative Performance Scale, n (%)
20
30
40
50
60
70
80
55.07±12.60
9(30.0)
21(70.0)
5(16.7)
8(26.7)
2(6.7)
2(6.7)
2(6.7)
6(20.0)
2(6.7)
3(10.0)
13(43.3)
4(13.3)
7(23.3)
1(3.3)
5(16.7)
0
1(3.3)
3(10.0)
7(23.3)
7(23.3)
10(3.3)
2(6.7)
55.54±12.80
6(23.1)
20(76.9)
5(19.2)
8(30.8)
1(3.8)
2(7.7)
2(7.7)
5(19.2)
1(3.8)
2(7.7)
11(42.3)
4(15.4)
7(26.9)
0
4(15.4)
0
1(3.8)
3(11.5)
5(19.2)
6(23.1)
9(34.6)
2(7.7)
0.890
0.560
>0.999
0.910
>0.999
_15-0191(237-252)P3.indd 245 2/25/15 2:24:58 PM

246 วิสัญญีสาร ปีที่ 40 ฉบับที่ 4 ตุลาคม – ธันวาคม 2557
Gabapentin (n = 30) Placebo (n = 26) p - value
Palliative Performance Scale, median(range)
Oral morphine daily equivalent, mg
median (range)
Concomitant pain medication, n (%)
NSAIDs
Antidepressant
Anticonvulsant
Bisphosphonates
Pain characteristics at recruitment, (mean±SD)
Average pain score in the last 24 hours
Right now pain
Best pain scores in the last 24 hours
Worst pain scores in the last 24 hours
Untoward symptoms at beginning of the study,
n (%)
Somnolence
Dizziness
Nausea
Vomiting
Constipation
60(80-30)
60(120-20)
0
2(6.7)
4(13.3)
0
5(10-4)
5(10-3)
3(7-0)
9(10-3)
1(3.3)
3(10.0)
1(3.3)
0
15(51.7)
60(80-30)
60(120-20)
0
1(3.8)
4(15.4)
0
5(4-9)
6(4-10)
3(7-2)
8.5(10-5)
5(19.2)
4(15.4)
0
0
11(42.3)
0.899
0.719
-
>0.999
>0.999
-
0.946
0.086
0.638
0.928
0.055
0.543
0.348
-
0.485
*p-value <0.05
Primary Efficacy Outcome
The average pain score reduction between
day 1 and day 8 of each period of the study for
gabapentin and placebo groups were similar, 2.77 ±
2.10 and 2.46 ± 1.25, p = 0.533. Mean average pain
in the last 24 hours, right now pain, best and worst
pain scores in the last 24 hours for two treatment
groups were also comparable (Table 2). Repeated
measures ANOVA indicated that there was no
significant time effect between the groups.
_15-0191(237-252)P3.indd 246 2/25/15 2:24:59 PM

Volume 40 Number 4 October – December 2014 Thai Journal of Anesthesiology 247
Table 2 Pain Scores during treatment period (Day 3 - 8)
Pain characteristics, (mean ± SD) Gabapentin (n = 30) Placebo (n = 26) p - value
Average pain score in the last 24 hours
Right now pain
Best pain scores in the last 24 hours
Worst pain scores in the last 24 hours
3.34±1.22
3.62±1.04
2.61±0.88
5.56±1.71
3.40±1.07
3.78±1.27
2.51±0.92
5.54±1.86
0.865
0.615
0.699
0.971
Secondary Efficacy Outcomes
Percentage of patients who had average pain
score reduction at least 3 points for follow - up
days per patient was not different between the
groups (Figure 4). The average percentage of
follow - up days per patient (day 3 - 8) with
average pain score reduction ≥ 3 are 53.23 ± 2.81
in the gabapentin group and vs 47.44 ± 3.53 in
the placebo group, p = 0.586. The use of rescue
analgesic was not different. Average doses of MSS
in gabapentin and placebo group were similar; 9.25
± 7.77 mg/patient vs 11.73 ± 11.62 mg/patient,
respectively, p = 0.607. No patients in both groups
discontinued the treatment due to adverse events.
Figure 4 Percentage of patients with average pain score reduction ≥ 3 from baseline at each study day
No statistically significant difference between the two groups
_15-0191(237-252)P3.indd 247 2/25/15 2:24:59 PM

248 วิสัญญีสาร ปีที่ 40 ฉบับที่ 4 ตุลาคม – ธันวาคม 2557
Table 3 Incidence of adverse events during treatment period (day 3 - 8)
Side effect Gabapentin (n = 30) Placebo (n = 26) p - value
Somnolence, n (%)
Grade 1
Grade 2
Grade 3
Dizziness, n (%)
Grade 1
Grade 2
Grade 3
Nausea, n (%)
Grade 1
Grade 2
Grade 3
Vomiting, n (%)
Grade 1
Grade 2
Grade 3
Constipation, n (%)
Grade 1
Grade 2
Grade 3
24(82.76)
8(27.59)
1(3.45)
27 (90.00)
4(13.33)
0
30(100)
2(6.67)
0
30(100)
1(3.30)
1(3.30)
19(63.30)
11(36.67)
0
20(76.92)
11(42.31)
2(7.69)
21(80.77)
7(23.33)
2(7.69)
26(100)
6(23.08)
0
26(100)
2(7.69)
1(3.85)
16(61.54)
11(42.31)
2(7.69)
0.780
0.218
0.470
0.325
0.202
0.122
-
0.080
-
-
0.470
0.918
0.890
0.666
0.122
Grading of severity of every adverse event are classified as followed
Grade 1 - Mild; asymptomatic or mild symptoms; clinical or diagnostic observations only; intervention not
indicate
Grade 2 - Moderate; minimal, local or noninvasive intervention indicated; limiting age-appropriate
instrumental ADL
Grade 3 - Severe or medically significant but not immediately life-threatening; hospitalization or
prolongation of hospitalization indicated; disabling; limiting self-care ADL
_15-0191(237-252)P3.indd 248 2/25/15 2:25:00 PM

Volume 40 Number 4 October – December 2014 Thai Journal of Anesthesiology 249
Discussion Mechanisms of metastatic bone pain include
both neuropathic and nociceptive. Previous study
showed that 17% of patients (95% CI, 10% to
24%) had positive Self-Reported Leeds Assessment
of Neuropathic Symptoms and Signs scores,
indicating that metastatic bone pain might be
neuropathic. Moreover, these patients had higher
brief pain inventory worst pain score than patients
without neuropathic characters (8.3 vs 7.0,
respectively; P = 0.016).17 This findings explain
refractory outcome of opioid treatment of bone
pain. Moderate-to-high doses of opioids may be
required to achieve pain control in metastatic bone
pain. Opioids have significant dose-limiting side
effects. Hoping that gabapentin in adequate dose
for the relief of neuropathic pain may accentuate
opioid analgesic effects thereby reduces the
untoward incidence; gabapentin is usually added
into treatment regimen.
There is also a randomized controlled study
of pregabalin; a gabapentinoid, in patients with
metastatic bone pain indicated that pregabalin use
may reduce metastatic bone pain10. Unfortunately,
the study was terminated early because of difficulty
in patient recruitment and big sample size required
causing delayed in the study timing. However, the
preliminary results showed that mean change ± SD
of NRS worst pain in pregabalin vs placebo groups
were 1.53 ± 1.81 vs 1.23 ± 1.74. The NRS average
pain in pregabalin vs placebo group were 1.24 ±
1.65 vs 0.85 ± 1.59. But more patients in pregabalin
group reported reductions in pain compared with
placebo group both for 30% and 50%.
Gabapentin, another α2 δ1 N-type calcium
channel may exert either the same or different
effect. It has analgesic effect in several clinical
trials of nonmalignant chronic neuropathic pain
and adjuvant treatment for cancer pain with
a neuropathic component in combination with
opioid analgesics. But there is still no conformed
evidence.
This study required patients with a stable
disease period and no plan for chemotherapy or
radiotherapy. The results of this study showed no
difference in average pain score reduction ≥ 3 from
baseline between the groups. The reason could be
due to: (1) Most of the participants had moderate
pain score before entering the study, not severe
pain. (2) We used cut-off value the absolute pain
score reduction follow-up period ≥ 3 to determine
significant difference. If we had used cut-off value
the pain score reduction follow-up period at least
216, the outcome might have been more approach
to significant difference. In Figure 4, average
percentage of patients with average pain score
reduction ≥ 3 at each study day tends to be higher
in the gabapentin group (53.23 ± 2.81 %) than in
the placebo group (47.44 ± 3.53), p = 0.586, even
though it is not significant. In addition, peak of
percentage of patients with average pain score
reduction ≥ 3 was at the study day 7 - 9. Therefore,
if gabapentin was used further, it might be possible
to find discrepancy of the result. Side effects of
gabapentin treatment group were mild in most
cases and not different from placebo.
Gabapentin is usually added into pain
_15-0191(237-252)P3.indd 249 2/25/15 2:25:00 PM

250 วิสัญญีสาร ปีที่ 40 ฉบับที่ 4 ตุลาคม – ธันวาคม 2557
management regimen. It is difficult to find any
patient who did not have it before recruitment. So
we excluded ones who got gabapentin ≥ 900 mg/
day or pregabalin ≥ 150 mg/day but for ones who
had less than aforementioned doses could be
included. Nevertheless, these doses were decreased
20-30% daily until completely stop in 4 days. By
that time opioid doses were adjusted to control
pain. Four days is the effective period of wash out
the drug because it is 5 times the half-life of
gabapentinoids. In our plan, patient who consumed
more than three daily p.r.n. MSS doses would be
withdrawn because it might indicate progression of
the disease and basal opioid dose should be
escalated. Fortunately, there was no such patient in
the study.
This study is the first well controlled study
to prove benefit of adding gabapentin to opioid
analgesia in metastatic bone pain patients. We
conducted crossover design in order to remove
patient variability and increasing precision of
estimation. However, there are some limitations.
Recruitment of cancer patients in clinical trials is
difficult. It is unethical to withhold all other
concomitant treatments such as radiotherapy,
chemotherapy, analgesic adjuvants and surgery
because they are usually needed for controlling of
the disease. The second limitation is that our
patients are only the ones with moderate pain.
Participants who had severe pain might want
radiation or chemotherapy for the disease and pain
control. Furthermore, we had to wait for at least
one month after radiation and two weeks after
chemotherapy before recruitment, otherwise there
might have carry over effect which would confound
the drug effects. Finally, after randomization,
changing in cancer treatment plan such as
chemotherapy, radiation, bisphosphonate therapy
led to dropping out.
The result is that gabapentin did not
accentuate analgesic efficacy of opioid in metastatic
bone pain. There may be a significant change in the
study result if (1) the study duration is extended;
(2) using a cut-off value of pain score reduction in
follow-up period at least 2 or pain intensity
difference was 33%. Suggestion for further study is
to use varied gabapentin dosage in order to achieve
an optimal dose. Nevertheless, as gabapentin is
usually safe and has wide therapeutic index, adding
gabapentin to opioid analgesic dose not add risk,
especially when there is an indication of adjuvant
treatment for cancer pain such as neuropathic pain
component.
Conclusion Adding gabapentin to opioid analgesic dose
not accentuate efficacy of pain relief by opioids in
metastatic bone pain patients.
Acknowledgement The authors are grateful for the “Prasert
Prasarttong - Osoth fund” via Thai Medical
Association. Thanks to Research Support Group,
Department of Anesthesiology, Faculty of Medicine
Ramathibodi Hospital.
None of the authors has conflict of interes
_15-0191(237-252)P3.indd 250 2/25/15 2:25:00 PM

Volume 40 Number 4 October – December 2014 Thai Journal of Anesthesiology 251
Reference 1. Coleman RE, Rubens RD. The clinical course
of bone metastases from breast cancer. Br J
Cancer. 1987;55:61-6.
2. Buga S, Sarria JE. The management of pain in
metastatic bone disease. Cancer Control.
2012;19:154-66.
3. Smith HS. Painful boney metastases. Ann
Palliat Med. 2012;1(1):14-31.
4. Rustøen T, Moum T, Padilla G, Paul S,
Miaskowski C. Predictors of quality of life in
oncology outpatients with pain from bone
metastasis. J Pain Symptom Manage. 2005;
30:234-42.
5. Bruera E, Kim HN. Cancer pain. JAMA.
2003;290:2476-9.
6. Hanks GW. The pharmacological treatment of
bone pain. Cancer Surv. 1988;7:87-101.
7. Coleman RE. Management of bone metastases.
Oncologist. 2000;5:463-70.
8. Peters CM, Ghilardi JR, Keyser CP, Kubota K,
Lindsay TH, Luger NM, et al. Tumor-induced
injury of primary afferent sensory nerve fibers
in bone cancer pain. Exp Neurol. 2005;193:
85-100.
9. Ballantyne JC, Cousins MJ, Giamberardino
MA, McGrath PA, Rajagopal MR, Smith MT,
et al. Pain clinical update; bone cancer pain.
Pain Clinical Update. 2009;17:1-6.
10. Sjo¨lund KF, Yang R, Lee KH, Resnick M.
Randomized study of pregabalin in patients
with cancer-induced bone pain. Pain Ther.
2013; 2: 37-48.
11. Caraceni A, Zecca E, Bonezzi C, Arcuri E,
Tur RY, Maltoni M, et al. Gabapentin for
neuropathic cancer pain: A randomized
controlled trial from the gabapentin cancer pain
study group. J Clin Oncol. 2004;22:2909-17.
12. Donovan-Rodriguez T, Dickenson AH, Urch
CE. Gabapentin normalizes spinal neuronal
responses that correlate with behavior in a rat
model of cancer-induced bone pain. Anesthesiology.
2005;102:132-40.
13. Chewaskulyong B, Sapinun L, Downing GM,
Intaratat P, Lesperance M, Leautrakul S, et al.
Reliability and validity of the Thai translation
(Thai PPS adult Suandok) of the palliative
performance scale (PPSv2). Palliat Med.
2012;26(8):1034-41.
14. National Institutes of Health National Cancer
Institute, Department of Health and Human
Services. Common terminology criteria for
adverse events (CTCAE) version 4.0, 2009-
2010. United States:2009.
15. Serafini AN. Therapy of metastatic bone pain.
The J Nucl Med. 2001;72(6):895-906.
16. Farrara JT, Portenoy RK, Berlina JA, Kinmana
JL, Stroma BL. Defining the clinically important
difference in pain outcome measures. Pain.
2000;88:287-94.
17. Kerba M, Wu J, Duan Q, Hagen NA, Bennett
MI. Neuropathic pain features in patients with
bone metastases referred for palliative radio-
therapy. J Clin Oncol. 2010;28:4892-97.
_15-0191(237-252)P3.indd 251 2/25/15 2:25:01 PM

252 วิสัญญีสาร ปีที่ 40 ฉบับที่ 4 ตุลาคม – ธันวาคม 2557
ผลของ Gabapentin เสริมกับ Opioids ในการระงับปวดจากมะเร็งแพร่กระจายมากระดูก การศึกษาแบบไขว้กัน
บทคัดย่อ
ที่มาและเหตุผล: มะเร็งแพร่กระจายมายังกระดูกมักทำให้ผู้ป่วยมีความปวดรุนแรง ซึ่งการระงับปวด
ด้วยยากลุ่มโอปิออยด์อาจไม่พียงพอ หรือมีฤทธิ์ข้างเคียงที่ทำให้ผู้ป่วยไม่สบายมากขึ้น ผู้เชี่ยวชาญจึงแนะนำ
ให้ใช้ยาเสริม อย่างไรก็ตามมักมีผู้นิยมใช้ยากาบาเพ็นตินอยด์ซึ่งเป็นยาระงับปวดประสาท แม้ว่าจะไม่เป็นที่
แน่ชัดว่ายากลุ่มนี้มีประโยชน์จริงสำหรับปวดจากมะเร็งแพร่กระจายมายังกระดูก วัตถุประสงค์: เพื่อศึกษา
ประสิทธิภาพการระงับปวดและผลข้างเคียงของยา gabapentin 900 mg/วัน ที่ให้ร่วมกับยา opioids ในการ
ระงับปวดจากภาวะมะเร็งแพร่กระจายมากระดูกที่มีความปวดระดับปานกลางถึงปวดมาก วิธีการศึกษา:
เป็นการศึกษาแบบไขว้โดยมีกลุ่มควบคุมและสุ่มผู้ป่วย โดยใช้ขนาดยาคงที่ ศึกษาในผู้ป่วยที่มีภาวะมะเร็งแพร่
กระจายมากระดูกจำนวน 32 คน ทุกรายได้รับยาโอปิออย์จนกระทั่งขนาดยาคงที่ แบ่งผู้ป่วยเป็น 2 กลุ่ม คือ
กลุ่ม gabapentin และ placebo โดยการสุ่ม, กลุ่มละ 16 คน แต่ละกลุ่มได้รับยา 2 ช่วง ช่วงละ 10 วัน ระยะพัก
4 วัน แล้วสลับยาที่ศึกษาในขนาดและวิธีเดียวกัน กลุ่มศึกษาได้รับกาบาเพ็นติน 900 มก/วัน กลุ่มควบคุมได้
รับยาหลอก รวมเวลาศึกษาทั้งสิ้น 24 วัน ประเมินว่าผู้ป่วยได้รับยาตามแผนการวิจัยและปัญหาที่เกิดจากยา
โดยทางโทรศัพท์ในวันที่ 2, 4, 8, 16, 18 และ 22 ประเมินที่ห้องตรวจในโรงพยาบาลวันที่ 1, 15, และ 25 สิ่งที่
ประเมินคือ ค่าเฉลี่ยคะแนนปวดที่ลดลงในวันที่ 1 เทียบกับ 8 ของแต่ละช่วงการศึกษา, ร้อยละของผู้ป่วยที่มี
คะแนนปวดเฉลี่ยที่ลดลง >3 จำนวนยาโอปิออย์ที่ผู้ป่วยต้องรับเสริม และภาวะแทรกซ้อน ผลการศึกษา:
ผู้ป่วย 30 รายได้รับกาบาเพ็นติน และ 26 รายได้รับยาหลอก ค่าเฉลี่ยคะแนนปวดที่ลดลงของทั้งสองกลุ่ม
ไม่ต่างกันอย่างมีนัยสำคัญทางสถิติ กลุ่มกาบาเพ็นติน 2.77 ± 2.10 และกลุ่มยาหลอก 2.46 ± 1.25, (p = 0.533)
ผู้ป่วยที่มีค่าเฉลี่ยคะแนนปวดที่ลดลง > 3 ร้อยละ 53.23 ± 2.81 และ 47.44 ± 3.53), p = 0.586 ปริมาณ
ยาแก้ปวดเสริมไม่ต่างกัน p = 0.607 ภาวะแทรกซ้อนต่างๆได้แก่ ง่วง มึนงง คลื่นไส้อาเจียน และท้องผูก
ไม่ต่างกัน
สรุป: การใช้กาบาเพ็นตินเสริมไม่ได้เพิ่มผลระงับปวดจากโอปิออยด์ในผู้ป่วยปวดจากภาวะมะเร็งแพร่กระจาย
มากระดูก
คำสำคัญ: กาบาเพ็นติน ภาวะมะเร็งแพร่กระจายมากระดูก ปวดกระดูก โอปิออยด์
_15-0191(237-252)P3.indd 252 2/25/15 2:25:01 PM
Recommended
![ISSN 2224-6509 [Online] Journal of Gastroenterology ...anesthai.org/public/rcat/Documents/library/1455471386Sedation for... · Seng-Kee Chuah Sen-Yung Hsieh Yong Shao Shih-Sung Chuang](https://img.dokumen.tips/doc/110x75/5b94bca409d3f219658d9829/issn-2224-6509-online-journal-of-gastroenterology-for-seng-kee-chuah.jpg)