CHRONIC OBSTRUCTIVE
PULMONARY DISEASE
Created by:
Muhammad Maulana, S. Ked.
M. Adin Archietobias, S. Ked.
Preceptor:
dr. Dedy Zairus, Sp. P.
SMF PENYAKIT DALAM BAGIAN PULMONOLOGI
RUMAH SAKIT UMUM DAERAH ABDUL MOELOEK
BANDAR LAMPUNG
2014

I. PATIENT STATUS
PATIENT IDENTITY
Initial Name : Mr. T
Sex : Male
Age : 68 years old
Nationally : Indonesia (Javanese)
Marital Status : Married
Religion : Islam
Occupation : Farmer
Educational Background : Elementary School
Address : Giri Mulyo, East Lampung
ANAMNESIS
Taken from : Autoanamnesis & Alloanamnesis
Date : March 18th, 2014
Time : 14.20
Chief Complain : Dyspneu
Additional Complaint : Productive cough, Cough up blood, Bloating, Stomachache,
Arm swollen
History of The Present Illness :
Patient came to hospital and told that he has gotten a dyspneu since six months ago, and
it was getting worse a month ago. Patient also complained about his cough with mucus
when he was coughing up and it was contain blood sometimes and he also complained
about his bloating and stomachache.
Patient felt dyspneu and productive cough since six month ago. History of bleeded
cough was approved. And he has history of taking 6 months drug package and it run the
2

fourth month. He had been a smoker since 50 years ago (1 packs/day). The patient
works as a farmer and often affected by dust.
The History of Illness :
(+) Small pox (+) Malaria (-) Kidney stone(-) Chicken pox (-) Disentri (-) Hernia(-) Difthery (-) Hepatitis (-) Prostat(-) Pertusis (-) TifusAbdominalis (-) Melena(-) Measles (-) Skirofula (-) Diabetic(+) Influenza (-) Siphilis (+) Alergy(-) Tonsilitis (-) Gonore (-) T u m o r
(-) Kholera (-) Hipertension. (-) Vaskular Disease(-) Acute Rheumatoid Fever (-) Ventrikuli Ulcer (-) Operation
(-) Pneumonia (-) Duodeni Ulcer (-) Pleuritic (+) Gastritis
Family’s diseases History :
Patient didn’t know about his Family’s Disease History
Is there any family who suffer :
Patient didn’t know
SYSTEM ANAMNESE
Note of Positive Complaints beside the title
Skin
(-) Boil (-) Hair (+) Night sweat(-) Nail (-) Yellow /Werus (-) Cyanotic
(-) Others
Head
Head
(-) Trauma (-) Headache
(-) Syncope (-) Pain of the sinus
3

Ear
(-) Pain (-) Tinitus(-) Secret (-) Ear disorders
(-) Deafness
Nose
(-) Trauma (-) Clogging(-) Pain (-) Nose disorders(-) Sekret (-) common cold(-) Epistaksis
Mouth
Mouth
(-) Lip (-) Tongue(-) Gums (-) Mouth disorders(-) Membrane (-) Stomatitis
Throat
(-) Throat Pain (-) Voice Change
Neck
(-) Protruding (-) Neck Pain
Cor/ Lung
(-) Chest pain (+) Dyspneu(-) Pulse (+) Hemoptoe(-) Ortopneu (+) Cough
Abdomen (Gaster/ Intestine)
(+) Puffing (-) Acites(-) Nausea (-) Hemoroid(-) Emesis (-) Diarrhea(-) Hematemesis (-) Melena(-) Disfagi (-) Pale colour of feses(+) Colic (-) Black colour of feses
(-) Nodul
4

Urogenital
(-) Dysuria (-) Pyuria(-) Stranguria (-) Kolik(-) Polyuria (-) Oliguria(-) Polakysuria (-) Anuria(-) Hematuria (-) Urine retention(-) Kidney stone (-) Drip urine(-) Wet the bed (-) Prostat
Katamenis
(-) Leukorhoe (-) Bleeding(-) Other
Muscle and Neuron
(-) Anestesi (-) Hard to bite
(-) Parestesi (-) Ataksia(-) Weak muscle (-) Hipo/hiper-estesi(-) Afasia (-) Tick(-) Amnesis (-) Vertigo(-) Others (-) Disartri
(-) Convultion (-) Syncope
Extremities
(+) Edema (-) Deformitas(-) Hinge pain (-) Cyanotic
Weight
Average weight (kg) : 45kg
Height (cm) : 165cm
Present Weight : 45kg
(if the patient doesn’t know certainly)
(+) steady
(-) down
(-) up
THE HISTORY OF LIFE
5

Birth place
(+) in home (-) matrinity (-) matrinity hospital
Helped by:
(+) Traditional matrinity (-) Doctor (-) Nurse (-) Others
Imunitation History (Unknown)
(-) Hepatitis (-) BCG (-) Campak (-) DPT (-) Polio Tetanus
Food History
Frequency/day : 3x/day
Amount/day : 3 times a day (health)
Variation/day : Rice, vegetables, fish
Appetite : Normal
Educational
(+) SD (-) SMP (-) SMA (-)SMK (-) Course Academy
Problem
Financial : -
Works : -
Family : -
Others : -
Body Check Up
General Check Up
Height : 165 cm
Weight : 45 kg
Blood Pressure : 100/80 mmHg
Pulse : 100x/minute
Temperature : 35,80C
Breath (Frequence&type) : 28x/minute
6

Nutrition Condition : Normal, IMT 19
Consciousness : Compos Mentis
Cyanotic : (-)
General Edema : pitting oedem
The way of walk : Normal
Mobility : Active
\ The age predicyion based on check up : 70 years old
Mentality Aspects
Behavior : Normal
Nature of Feeling : Normal
The thinking of process : Normal
Skin
Color : Brown
Keloid : (-)
Pigmentasi : (-)
Hair Growth : Normal
Arteries : Touchable
Touch temperature : Afrebris
Humid/dry : Dry
Sweat : Normal
Turgor : Normal
Icterus : Anicteric
Fat Layers : Enough
Efloresensi : (-)
Edema : (+)
Others : Superior Vena Cava Syndrome appearance in the chest &
abdomen
Lymphatic Gland
7

Submandibula : no enlargement
Neck : no enlargement
Supraclavicula : no enlargement
Armpit : no enlargement
Head
Face Expression : Mild Sickness appearance
Face Symmetric : Symmetric
Hair : Gray and Black
Temporal artery : Normal
Eye
Exopthalmus : (-)
Enopthalmus : (-)
Palpebra : edema (-)/(-)
Lens : Clear/Clear
Conjunctiva : Anemis -/-
Visus : Normal
Sklera : Anicteric
Ear
Deafnes : (-)
Foramen : (-)
Membrane tymphani : intak
Obstruction : (-)
Serumen : (-)
Bleeding : (-)
Liquid : (-)
Mouth
8

Lip : (-)
Tonsil : (-)
Palatal : Normal
Halibsts : No
Teeth : (-)
Trismus : (-)
Farings : Unhiperemis
Liquid Layers : (-)
Tongue : Clean
Neck
JVP : Normal
Tiroid Gland : no enlargement
Limfe Gland : no enlargement
Chest
Shape : Simetric
Artery : Normal
Breast : Normal
Lung
Inspection : Left : simetric
Right : simetric
Palpation : Left : pain (-)
Right : vokal fremitus decreased, pain (-)
Percussion : Left : sonor
Right : dim
Auscultation : Left : vesiculer
Right : decreased vesicular
Cor
9

Inspection : Ictus cordis seen in ICS V left midclavicula
Palpation : Ictus Cordis feel in ICS V left midclavicula
Percussion : difficult to assess
Auscultation : Heart Sound 1 & 2 Regular
Artery
Temporalic artery : No aberration
Caritic artery : No aberration
Brachial artery : No aberration
Radial artery : No aberration
Femoral artery : No aberration
Poplitea artery : No aberration
Posterior tibialis artery : No aberration
Stomach
Inspection : Flat , Symetrics
Palpation : Stomach Wall : undulation (-), pain (-)
Heart : Hepatomegali (-)
Limfe : Splenomegali (-)
Kidney : Ballotement (-)
Percussion : Shifting Dullness (-)
Auscultation : Intestine Sounds (+)
Genital (no indication)
Movement Joint
Arm Right Left
Muscle Normal Normal
Tones Normal Normal
Mass Normal Normal
Joint Normal Normal
Movement Normal Normal
10

Strength Normal Normal
Heel and Leg
Wound/injury : not found
Varices : (-)
Muscle (tones&mass) : Normal
Joint : Normal
Movement : Normal
Strength/Power : Normal
Edema : (+)
Others : (-)
Reflexs
Right Left
Tendon Reflex Normal Normal
Bisep Normal Normal
Trisep Normal Normal
Pattela Normal Normal
Achiles Normal Normal
Cremaster Normal Normal
Skin Reflex Normal Normal
Patologic Reflex Not Found Not Found
Laboratory
Routine Blood
- Hb : 11,2 gr/dl
- Leukosit : 6500 /ul
- LED : 78 mm/jam
- Trombosit : 270.000
- Diff. Count
o Basofil : 0%
o Eosinofil : 0%
11

o Stem : 0%
o Segment : 80%
o Limfosit : 9 %
o Monosit : 11%
Chest X-Ray
Pulmo : radioopaque in pulmo dextra, intercostal space increase
Resume
Patient came to hospital and told that he has gotten a dyspneu since six months ago, and
it was getting worse a month ago. Patient also complained about his cough with mucus
when he was coughing up and it was contain blood sometimes and he also complained
about his bloating and stomachache.
Patient felt dyspneu and productive cough since six month ago. History of bleeded
cough was approved. And he has history of taking 6 months drug package and it run the
fourth month. History of diabetic mellitus and hypertenton were denied. He had been a
smoker since 50 years ago (1 packs/day). The patient works as a farmer and often
affected by dust.
Working Diagnose
- Dextra Pleural Effusion due to Suspect Tubercullosis
Basic Diagnose
Anamnesis
- Recurrent cough with or without sputum
- History of hemaptoe
- Dyspneu
- History of taking Anti Tubecullosa Drugs
Physics Examination
12

- Inspection : Simetric, Appearance of Superior Vein Cava Syndrome
- Palpation : Decreased fremitus tactil in the dextra side
- Percution : Dim sound in the dextra side
- Auscultation : Decreased of vesicular sound in the dextra side
Support Examination
LABORATORY
(RSAM March 15th 2014)
Routine blood
- Hb : 11,2 gr % (N : 13,5 – 18 gr% )
- LED : 78 mm/hour (N : 0-10 mm/hour)
- WBC : 6.500 mm³ (N : 4500 – 10.700/ul )
- Diff. Count :
Basofil : 0 % ( 0 - 1 % )Eusinofil : 0% ( 1 - 3 % )Stem : 0 % (2 — 6 %)Begment : 80% (50 — 70 %)Limfosit : 9% (20 — 40 %)Monosit : 11% (2 — 8 %)
Chemical Blood
- SGOT : 16 (6-25 u/l)
- SGPT : 10 (6-35 u/l)
- Total protein : 5,9 (6-8,5 g/dl)
- Albumin : 3 (3,5-5,0 g/dl)
- Globulin : 2,9 (2,3-3,5 g/dl)
- At the time blood glucose : 166 mg/dl (70-200 mg/dl)
- Ureum : 14 mg/dl (10-40 mg/dl)
- Creatinin : 0,6 mg/dl (0,7-1,3 mg/dl)
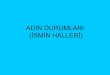
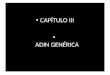
Roentgen Thorax AP :
13

- Pulmo dextra shows radiopaque, trachea deviation and cor to the left side
Dextra Pleural Effusion.
Pre-WSD Rontgen
Post-WSD Rontgen
Differential Diagnose
14

- Dextra Pleural Effusion due to malignancy
Basic Differential Diagnose
Anamnesis
- Chronic Productive Cough
- Recurrent Dyspneu
- Nocturnal sweating
- Hemaptoe
Physics Examination
- Inspection : Simetric, Appearance of Superior Vein Cava Syndrome
- Palpation : Decreased fremitus tactil in the dextra side
- Percution : Dim sound in the dextra side
- Auscultation : Decreased of vesicular sound in the dextra side
Support Check Up
- Sputum and pleura fluid culture and resistance test
- Acid-fast Bacillus (AFB) Sputum at the time - at the morning – at the time
- EKG
Treatment Plan
(1) General Treatment
- Bed Rest
- Nutrition (high calory, high protein)
(2) Special Treatment
- Medicamentosa
o O2 2-3 L/minute
o Bed rest
o High calory and protein diet
o IVFD RL 20 gtt/mnt
o Salbutamol 0,5 mg/Metyl Prednisolon 1 mg/Cetirizine ½ tab/GG 1 tab 3 x 1
cap
o Ceftriaxone 1 gr vial/ 12 h
o Ranitidin amp/12 h
o WSD
15

o primary category TB therapy planning
- Non Medicamentosa
o Stop Tobacco
o Avoid Tobacco Smoke
o Activity adjustment
o Go to doctor immedietly if appear any symptoms
Prognose
Quo ad Vitam : Dubia ad bonam
Quo ad Functonam : Dubia ad malam
Quo ad Sanationam : Dubia ad malam
16

II. DISCUSSION
1. Is the patient diagnosis has been correct ?
In this case, the patient had been diagnosed as a pleural effusion ec suspect TB based on
history taking, physical examination, and support examination.
a. The anamnesis :
- Breathlessness and productive cough since 6 months ago. He also said that
he had ever been productive cough, sweaty night, fever, bloating.
b. Physical examination
Conjungtiva : anemic (-/-)
Neck : Trachea deviation to the left
Chest : Shape Hemithorax dextra looks convex
Lung
Inspection : Left : hemithorax movement normal, retraction (-)
Right : hemithorax movement normal, retraction (-)
Palpation : tactil fremitus asimetris, dextra weaker than sinistra
Percussion : Dim/Sonor
Auscultation : Vesiculer decreased in dextra , Ronchi (-/-), Wheezing (-/-)
Suspect dextra pleura effusion.
17

c. Supporting examination
Routine blood
- LED and segment neutrofil increased commonly on TB.
Roentgen Thorax AP :
- Pulmo dextra shows radioopaque, not look dextra contophrenicus angle, trachea
deviation and cor to the left side Dextra Pleural Effusion.
Thoracosentesis
Serohemoragic DD : TB, Malignancy, Trauma.
Cytology: no malignancy.
2. How the pathogenesis pleura effusion from this patient ?
18

19

3. Is the patient treatment has been correct ?
- O2 2-3 L/minute suplly oxygen based on tidal volume.
- Bed rest preventing worse breathlessness.
- High calory and protein diet
- IVFD RL 20 gtt/mnt preventing dehidration.
- Salbutamol 0,5 mg/Metyl Prednisolon 1 mg/Cetirizine ½ tab/GG 1 tab 3 x 1 cap
for reducing breathlessness.and cough.
- Ceftriaxone 1 gr vial/ 12 h for temporary treatment for 1 week for evaluation
whether because of TB or the others bacterial. Beside that, because of thoracosentesis
for preventing infection from it.
- Ranitidin amp/12 h preventing gaster acid due to his complained about bloating
- Continue Primary category TB therapy because relapse TB is the basic of
pleura effusion from this patient.
4. How the prognosis from this patient ?
Quo ad vitam : dubia ad bonam because vital signs are still good.
Quo ad functionam : dubia ad bonam because it would indicate repeated pleura
effusion again because of TB. Of course the function of pulmo is still bad. Pleurodesis
is the definitif treatment of malignant pleural effusion.
Quo ad sanationam : dubia ad malam it can always interfere with daily activities
of the patient.
III. PLEURAL EFFUSION
20

A. Overview
A pleural effusion is an abnormal collection of fluid in the pleural space
resulting from excess fluid production or decreased absorption. It is the most
common manifestation of pleural disease, with etiologies ranging from
cardiopulmonary disorders to symptomatic inflammatory or malignant diseases
requiring urgent evaluation and treatment.
A.1. Anatomy
The pleural space is bordered by the parietal and visceral pleurae. The parietal
pleura covers the inner surface of the thoracic cavity, including the mediastinum,
diaphragm, and ribs. The visceral pleura envelops all lung surfaces, including
the interlobar fissures. The right and left pleural spaces are separated by the
mediastinum.
The pleural space plays an important role in respiration by coupling the
movement of the chest wall with that of the lungs in 2 ways. First, a relative
vacuum in the space keeps the visceral and parietal pleurae in close proximity.
Second, the small volume of pleural fluid, which has been calculated at 0.13
mL/kg of body weight under normal circumstances, serves as a lubricant to
facilitate movement of the pleural surfaces against each other in the course of
respirations. This small volume of fluid is maintained through the balance of
hydrostatic and oncotic pressure and lymphatic drainage, a disturbance of which
may lead to pathology.
A.2. Etiology
21

The normal pleural space contains approximately 1 mL of fluid, representing the
balance between (1) hydrostatic and oncotic forces in the visceral and parietal
pleural vessels and (2) extensive lymphatic drainage. Pleural effusions result
from disruption of this balance.
Pleural effusion is an indicator of an underlying disease process that may be
pulmonary or nonpulmonary in origin and may be acute or chronic. Although
the etiologic spectrum of pleural effusion is extensive, most pleural effusions are
caused by congestive heart failure, pneumonia, malignancy, or pulmonary
embolism. The following mechanisms play a role in the formation of pleural
effusion:
Altered permeability of the pleural membranes (eg, inflammation,
malignancy,pulmonary embolus)
Reduction in intravascular oncotic pressure (eg, hypoalbuminemia, cirrhosis)
Increased capillary permeability or vascular disruption (eg, trauma,
malignancy, inflammation, infection, pulmonary infarction, drug
hypersensitivity, uremia, pancreatitis)
Increased capillary hydrostatic pressure in the systemic and/or pulmonary
circulation (eg, congestive heart failure, superior vena cava syndrome)
Reduction of pressure in the pleural space, preventing full lung expansion (eg,
extensive atelectasis, mesothelioma)
Decreased lymphatic drainage or complete blockage, including thoracic duct
obstruction or rupture (eg, malignancy, trauma)
Increased peritoneal fluid, with migration across the diaphragm via the
lymphatics or structural defect (eg, cirrhosis, peritoneal dialysis)
Movement of fluid from pulmonary edema across the visceral pleura
Persistent increase in pleural fluid oncotic pressure from an existing pleural
effusion, causing further fluid accumulation
22

The net result of effusion formation is a flattening or inversion of the diaphragm,
mechanical dissociation of the visceral and parietal pleura, and a restrictive
ventilatory defect.
Pleural effusions are generally classified as transudates or exudates, based on the
mechanism of fluid formation and pleural fluid chemistry. Transudates result
from an imbalance in oncotic and hydrostatic pressures, whereas exudates are
the result of inflammation of the pleura or decreased lymphatic drainage. In
some cases, the pleural fluid may have a combination of transudative and
exudative characteristics.
A.3 Prognosis
The prognosis in pleural effusion varies in accordance with the condition’s
underlying etiology. However, patients who seek medical care earlier in the
course of their disease and those who obtain prompt diagnosis and treatment
have a substantially lower rate of complications than do patients who do not.
Morbidity and mortality
Morbidity and mortality of pleural effusions are directly related to cause, stage
of disease at the time of presentation, and biochemical findings in the pleural
fluid.
23

Morbidity and mortality rates in patients with pneumonia and pleural effusions
are higher than those in patients with pneumonia alone. Parapneumonic
effusions, when recognized and treated promptly, typically resolve without
significant sequelae. However, untreated or inappropriately treated
parapneumonic effusions may lead to empyema, constrictive fibrosis, and sepsis.
Development of a malignant pleural effusion is associated with a very poor
prognosis, with median survival of 4 months and mean survival of less than 1
year. The most common associated malignancy in men is lung cancer, and the
most common associated malignancy in women is breast cancer. Median
survival ranges from 3-12 months, depending on the malignancy. Effusions from
cancers that are more responsive to chemotherapy, such as lymphoma or breast
cancer, are more likely to be associated with prolonged survival, compared with
those from lung cancer or mesothelioma.
Cellular and biochemical findings in the fluid may also be indicators of
prognosis. For example, a lower pleural fluid pH is often associated with a
higher tumor burden and a worse prognosis.
B. Clinical Presentation
A detailed medical history should be obtained from all patients presenting with a
pleural effusion, as this may help to establish the etiology. For example, a
history of chronic hepatitis or alcoholism with cirrhosis suggests hepatic
hydrothorax or alcohol-induced pancreatitis with effusion. Recent trauma or
surgery to the thoracic spine raises the possibility of a CSF leak. The patient
should be asked about a history of cancer, even remote, as malignant pleural
effusions can develop many years after initial diagnosis.
An occupational history should also be obtained, including potential asbestos
exposure, which could predispose the patient to mesothelioma or asbestos
24

pleural effusion. The patient should also be asked about medications they are
taking.
B.1 Clinical Manifestations
The clinical manifestations of pleural effusion are variable and often are related
to the underlying disease process. The most commonly associated symptoms are
progressive dyspnea, cough, and pleuritic chest pain.
Dyspnea
Dyspnea is the most common symptom associated with pleural effusion and is
related more to distortion of the diaphragm and chest wall during respiration
than to hypoxemia. In many patients, drainage of pleural fluid alleviates
symptoms despite limited improvement in gas exchange. Drainage of pleural
fluid may also allow the underlying disease to be recognized on repeat chest
radiographs. Note that dyspnea may be caused by the condition producing the
pleural effusion, such as underlying intrinsic lung or heart disease, obstructing
endobronchial lesions, or diaphragmatic paralysis, rather than by the effusion
itself.
Cough
Cough in patients with pleural effusion is often mild and nonproductive. More
severe cough or the production of purulent or bloody sputum suggests an
underlying pneumonia or endobronchial lesion.
25

Chest pain
The presence of chest pain, which results from pleural irritation, raises the
likelihood of an exudative etiology, such as pleural infection, mesothelioma, or
pulmonary infarction.
Pain may be mild or severe. It is typically described as sharp or stabbing and is
exacerbated with deep inspiration. Pain may be localized to the chest wall or
referred to the ipsilateral shoulder or upper abdomen, usually because of
diaphragmatic involvement. Pain often diminishes in intensity as the pleural
effusion increases in size.
Additional symptoms
Other symptoms in association with pleural effusions may suggest the
underlying disease process. Increasing lower extremity edema, orthopnea, and
paroxysmal nocturnal dyspnea may all occur with congestive heart failure.
Night sweats, fever, hemoptysis, and weight loss should suggest TB.
Hemoptysis also raises the possibility of malignancy, other endotracheal or
endobronchial pathology, or pulmonary infarction. An acute febrile episode,
purulent sputum production, and pleuritic chest pain may occur in patients with
an effusion associated with pneumonia.
B.2 Physical Examinations
Physical findings in pleural effusion are variable and depend on the volume of
the effusion. Generally, there are no physical findings for effusions smaller than
300 mL. With effusions larger than 300 mL, findings may include the following:
Dullness to percussion, decreased tactile fremitus, and asymmetrical chest
expansion, with diminished or delayed expansion on the side of the effusion,
are the most reliable physical findings of pleural effusion.
Mediastinal shift away from the effusion - This is observed with effusions of
greater than 1000 mL; displacement of the trachea and mediastinum toward
26

the side of the effusion is an important clue to obstruction of a lobar bronchus
by an endobronchial lesion, which can be due to malignancy or, less
commonly, to a nonmalignant cause, such as a foreign body.
Diminished or inaudible breath sounds
Egophony ("e" to "a" changes) at the most superior aspect of the pleural
effusion
Pleural friction rub
Other physical findings, as follows, may suggest the underlying cause of the
pleural effusion:
Peripheral edema, distended neck veins, and S3 gallop suggest congestive
heart failure. Edema may also be a manifestation of nephrotic syndrome;
pericardial disease; or, combined with yellow nails, the yellow nail syndrome.
Cutaneous changes with ascites suggest liver disease
Lymphadenopathy or a palpable mass suggests malignancy.
C. Workup
C.1 Approach Consideration
Thoracentesis should be performed for new and unexplained pleural effusions
when sufficient fluid is present to allow a safe procedure. Observation of pleural
effusion is reasonable when benign etiologies are likely, as in the setting of overt
congestive heart failure, viral pleurisy, or recent thoracic or abdominal surgery.
Laboratory testing helps to distinguish pleural fluid transudates from exudates;
however, certain types of exudative pleural effusions might be suspected simply
by observing the gross characteristics of the fluid obtained during thoracentesis.
Note the following:
Frankly purulent fluid indicates an empyema
A putrid odor suggests an anaerobic empyema
27

A milky, opalescent fluid suggests a chylothorax, resulting most often from
lymphatic obstruction by malignancy or thoracic duct injury by trauma or
surgical procedure
Grossly bloody fluid may result from trauma, malignancy,
postpericardiotomy syndrome, or asbestos-related effusion and indicates the
need for a spun hematocrit test of the sample; a pleural fluid hematocrit level
of more than 50% of the peripheral hematocrit level defines a hemothorax,
which often requires tube thoracostomy.
C.2 Distinguishing Transduates from Exudates
Transudates are usually ultrafiltrates of plasma in the pleura due to imbalance in
hydrostatic and oncotic forces in the chest. However, they can also be caused by
the movement of fluid from peritoneal spaces or by iatrogenic infusion into the
pleural space from misplaced or migrated central venous catheters or nasogastric
feeding tubes.
Exudates are produced by a variety of inflammatory conditions and often require
more extensive evaluation and treatment than transudates. Exudates arise from
pleural or lung inflammation, impaired lymphatic drainage of the pleural space,
transdiaphragmatic movement of inflammatory fluid from the peritoneal space,
altered permeability of pleural membranes, and increased capillary wall
permeability or vascular disruption. Pleural membranes are involved in the
pathogenesis of the fluid formation. Permeability of pleural capillaries to
proteins is high, resulting in an elevated protein content.
The initial diagnostic consideration is distinguishing transudates from exudates.
Although a number of chemical tests have been proposed to differentiate pleural
fluid transudates from exudates, the tests first proposed by Light et al have
become the criterion standards.
28

The fluid is considered an exudate if any of the following applies:
Ratio of pleural fluid to serum protein greater than 0.5
Ratio of pleural fluid to serum LDH greater than 0.6
Pleural fluid LDH greater than two thirds of the upper limits of normal serum
value
These criteria require simultaneous measurement of pleural fluid and serum
protein and LDH. However, a meta-analysis of 1448 patients suggested that the
following combined pleural fluid measurements might have sensitivity and
specificity comparable to the criteria from Light et al for distinguishing
transudates from exudates :
Pleural fluid LDH value greater than 0.45 of the upper limit of normal serum
values
Pleural fluid cholesterol level greater than 45 mg/dL
Pleural fluid protein level greater than 2.9 g/dL
Clinical judgment is required when pleural fluid test results fall near the cutoff
points. The criteria from Light et al and these alternative criteria identify nearly
all exudates correctly, but they misclassify approximately 20-25% of transudates
as exudates, usually in patients on long-term diuretic therapy for congestive
heart failure (because of the concentration of protein and LDH within the pleural
space due to diuresis).
Using the criterion of serum minus pleural protein concentration level of less
than 3.1 g/dL, rather than a serum/pleural fluid ratio of greater than 0.5, more
correctly identifies exudates in these patients.
Although pleural fluid albumin is not typically measured, a gradient of serum
albumin to pleural fluid albumin of less than 1.2 g/dL also identifies an exudate
in such patients.
29

In addition, studies suggest that pleural fluid levels of N-terminal pro-brain
natriuretic peptide (NT-proBNP) are elevated in effusions due to congestive
heart failure. Moreover, elevated pleural NT-proBNP was shown to out-perform
pleural fluid BNP as a marker of heart failure–related effusion. Thus, at
institutions where this test is available, high pleural levels of NT-proBNP
(defined in different studies as >1300-4000 ng/L) may help to confirm heart
failure as the cause of an otherwise idiopathic chronic effusion.
Transudates are caused by a small, defined group of etiologies, including the
following:
Congestive heart failure
Cirrhosis (hepatic hydrothorax)
Atelectasis - Which may be due to malignancy or pulmonary embolism
Hypoalbuminemia
Nephrotic syndrome
Peritoneal dialysis
Myxedema
Constrictive pericarditis
Urinothorax - Usually due to obstructive uropathy
Cerebrospinal fluid (CSF) leaks to the pleura - Generally in the setting of
ventriculopleural shunting or of trauma or surgery to the thoracic spine
Duropleural fistula - Rare, but may be a complication of spinal cord surgery
Extravascular migration of central venous catheter
Glycinothorax - A rare complication of bladder irrigation with 1.5% glycine
solution following urologic surgery
The more common causes of exudates include the following:
Parapneumonic causes
Malignancy (most commonly, lung or breast cancer, lymphoma, leukemia;
less commonly, ovarian carcinoma, stomach cancer, sarcomas, melanoma)[9]
30

Pulmonary embolism
Collagen-vascular conditions (rheumatoid arthritis, systemic lupus
erythematosus )
Tuberculosis (TB)
Pancreatitis
Trauma
Postcardiac injury syndrome
Esophageal perforation
Radiation pleuritis
Sarcoidosis
Fungal infection
Pancreatic pseudocyst
Intra-abdominal abscess
Status-post coronary artery bypass graft surgery
Pericardial disease
Meigs syndrome (benign pelvic neoplasm with associated ascites and pleural
effusion)
Ovarian hyperstimulation syndrome
Drug-induced pleural disease (see Pneumotox On Line for an extensive list of
drugs that can cause pleural effusion)
Asbestos-related pleural disease
Yellow nail syndrome (yellow nails, lymphedema, pleural effusions)
Uremia
Trapped lung (localized pleural scarring with the formation of a fibrin peel
prevents incomplete lung expansion, at times leading to pleural effusion)
Chylothorax (acute illness with elevated triglycerides in pleural fluid)
Pseudochylothorax (chronic condition with elevated cholesterol in pleural
fluid)
Fistula (ventriculopleural, biliopleural, gastropleural)
C.3 Radiography
31

Effusions of more than 175 mL are usually apparent as blunting of the
costophrenic angle on upright posteroanterior chest radiographs. On supine chest
radiographs, which are commonly used in the intensive care setting, moderate to
large pleural effusions may appear as a homogenous increase in density spread
over the lower lung fields. Apparent elevation of the hemidiaphragm, lateral
displacement of the dome of the diaphragm, or increased distance between the
apparent left hemidiaphragm and the gastric air bubble suggests subpulmonic
effusions. (See the images below.)
Left lateral decubitus film showing freely layering pleural effusion.
C.4. CT Scanning and Ultrasonography
A study by Gurung et al involving 41 consecutive patients with hepatic
hydrothorax indicated that hepatic hydrothorax virtually always presents with
ascites that can be revealed by ultrasonography or computed tomography (CT)
scanning.
Chest CT scanning with contrast should be performed in all patients with an
undiagnosed pleural effusion, if it has not previously been performed, to detect
thickened pleura or signs of invasion of underlying or adjacent structures. The 2
32

diagnostic imperatives in this situation are pulmonary embolism and
tuberculouspleuritis. In both cases, the pleural effusion is a harbinger of
potential future morbidity. In contrast, a short delay in diagnosing metastatic
malignancy to the pleural space has less impact on future clinical outcomes. CT
angiography should be ordered if pulmonary embolism is strongly suggested.
C.5. Diagnostic Thoracentesis
Perform diagnostic thoracentesis if the etiology of the effusion is unclear or if
the presumed cause of the effusion does not respond to therapy as expected.
Pleural effusions do not require thoracentesis if they are too small to safely
aspirate or, in clinically stable patients, if their presence can be explained by
underlying congestive heart failure (especially bilateral effusions) or by recent
thoracic or abdominal surgery.
Depending on the clinician’s experience, a pulmonologist can be consulted for
assistance with high-risk diagnostic thoracentesis.
Contraindications
Relative contraindications to diagnostic thoracentesis include a small volume of
fluid (< 1 cm thickness on a lateral decubitus film), bleeding diathesis or
systemic anticoagulation, mechanical ventilation, and cutaneous disease over the
proposed puncture site. Mechanical ventilation with positive end-expiratory
pressure does not increase the risk of pneumothorax after thoracentesis, but it
increases the likelihood of severe complications (tension pneumothorax or
persistent bronchopleural fistula) if the lung is punctured.
C.6. Pleural Fluid examinations
Normal pleural fluid
Normal pleural fluid has the following characteristics:
Clear ultrafiltrate of plasma that originates from the parietal pleura
A pH of 7.60-7.64
Protein content of less than 2% (1-2 g/dL)
33

Fewer than 1000 white blood cells (WBCs) per cubic millimeter
Glucose content similar to that of plasma
Lactate dehydrogenase (LDH) less than 50% of plasma
Pleural fluid LDH
Pleural fluid LDH levels greater than 1000 IU/L suggest empyema, malignant
effusion, rheumatoid effusion, or pleural paragonimiasis. Pleural fluid LDH
levels are also increased in effusions from Pneumocystis jiroveci (formerly, P
carinii) pneumonia; the diagnosis is suggested by a pleural fluid/serum LDH
ratio of greater than 1, with a pleural fluid/serum protein ratio of less than 0.5.
Pleural fluid glucose and pH
In addition to the previously discussed tests, glucose and pleural fluid pH should
be measured during the initial thoracentesis in most situations.
A low pleural glucose concentration (30-50 mg/dL) suggests malignant effusion,
tuberculouspleuritis, esophageal rupture, or lupus pleuritis. A very low pleural
glucose concentration (ie, < 30 mg/dL) further restricts diagnostic possibilities,
to rheumatoid pleurisy or empyema.
Pleural fluid pH is highly correlated with pleural fluid glucose levels. A pleural
fluid pH of less than 7.30 with a normal arterial blood pH level is caused by the
same diagnoses as listed above for low pleural fluid glucose. However, for
parapneumonic effusions, a low pleural fluid pH level is more predictive of
complicated effusions (that require drainage) than is a low pleural fluid glucose
level. In such cases, a pleural fluid pH of less than 7.1-7.2 indicates the need for
urgent drainage of the effusion, while a pleural fluid pH of more than 7.3
suggests that the effusion may be managed with systemic antibiotics alone.
34

In malignant effusions, a pleural fluid pH of less than 7.3 has been associated in
some reports with more extensive pleural involvement, higher yield on cytology,
decreased success of pleurodesis, and shorter survival times.
Handle pleural fluid samples as carefully as arterial samples for pH
measurements, with fluid collected in heparinized syringes and ideally
transported on ice for measurement within 6 hours. However, studies have
shown that when collected in heparinized syringes, pleural fluid pH does not
change significantly even over several hours at room temperature. Consequently,
if appropriately collected samples can be processed quickly, pH measurements
should not be canceled simply because the sample was not transported on ice.
Pleural Fluid Culture and Cytology
Culture of infected pleural fluid yields positive results in approximately 60% of
cases; this occurs even less often for anaerobic organisms. Diagnostic yields,
particularly for anaerobic pathogens, may be increased by directly culturing
pleural fluid into blood culture bottles.
Malignancy is suspected in patients with known cancer or with lymphocytic,
exudative effusions, especially when bloody. Direct tumor involvement of the
pleura is diagnosed most easily by performing pleural fluid cytology.
Heparinize samples (1 mL of 1:1000 heparin per 50 mL of pleural fluid) if
bloody, and refrigerate if samples will not be processed within 1 hour.
The reported diagnostic yields in cytology vary from 60-90%, depending on the
extent of pleural involvement and the type of primary malignancy. Cytology
findings are positive in 58% of effusions related to mesothelioma.
The sensitivity of cytology is not highly related to the volume of pleural fluid
tested; sending more than 50-60 mL of pleural fluid for cytology does not
increase the yield of direct cytospin analysis, and volumes of approximately 150
mL are sufficient when both cytospin and cell block preparations are analyzed.
35

Tumor markers, such as carcinoembryonic antigen, Leu-1, and mucin, are
suggestive of malignant effusions (especially adenocarcinoma) when pleural
fluid values are very high. However, because of low sensitivity, they are not
helpful if the values are normal or only modestly increased.
Tuberculous pleuritis
Suspect tuberculouspleuritis in patients with a history of exposure or a positive
PPD finding and in patients with lymphocytic exudative effusions, especially if
less than 5% mesothelial cells are detected on differential blood cell counts.
Because most tuberculous pleural effusions probably result from a
hypersensitivity reaction to the Mycobacterium rather than from microbial
invasion of the pleura, acid-fast bacillus stains of pleural fluid are rarely
diagnostic (< 10% of cases), and pleural fluid cultures grow M tuberculosis in
less than 65% of cases.
In contrast, the combination of histology and culture of pleural tissue obtained
by pleural biopsy increases the diagnostic yield to 90%.
ADA activity of greater than 43 U/mL in pleural fluid supports the diagnosis of
tuberculouspleuritis. However, the test has a sensitivity of only 78%; therefore,
pleural ADA values of less than 43-50 U/mL do not exclude the diagnosis of TB
pleuritis. Interferon-gamma concentrations of greater than 140 pg/mL in pleural
fluid also support the diagnosis of tuberculouspleuritis, but this test is not
routinely available.
C.7. Additional Laboratory Test
Additional specialized tests are warranted when specific etiologies are
suspected. Measure pleural fluid amylase levels if a pancreatic origin or ruptured
esophagus is suspected or if a unilateral, left-sided pleural effusion remains
undiagnosed after initial testing. Of note, increased pleural fluid amylase can
also be seen with malignancy. An additional assay of amylase isoenzymes can
36

help distinguish a pancreatic source (diagnosed by elevated pleural fluid
pancreatic isoenzymes) from other etiologies.
Measure triglyceride and cholesterol levels in milky pleural fluids when
chylothorax or pseudochylothorax is suspected.
Consider immunologic studies, including pleural fluid antinuclear antibody and
rheumatoid factor, when collagen-vascular diseases are suspected.
D. Differential Diagnoses
Sjögren syndrome, liver or lung transplantation, upper genitourinary trauma, and
abdominal trauma are among the conditions to consider in the differential
diagnosis of pleural effusion, but note they are rare.
Transudative pleural effusion
Considerations in the differential diagnosis of transudative pleural effusion
include the following:
Congestive heart failure (most common)
Cirrhosis with hepatic hydrothorax
Nephrotic syndrome
Peritoneal dialysis/continuous ambulatory peritoneal dialysis
Hypoproteinemia
Glomerulonephritis
Superior vena cava obstruction
Fontan procedure
Urinothorax
CSF leak to the pleural space
Exudative pleural effusion
37

Conditions to consider in the differential diagnosis of exudative pleural effusion
include the following:
Malignancy
Pneumonia
Tuberculosis
Pulmonary embolism
Fungal infection
Pancreatic pseudocyst
Intra-abdominal abscess
After coronary artery bypass graft surgery
Postcardiac injury syndrome
Pericardial disease
Meigs syndrome
Ovarian hyperstimulation syndrome
Rheumatoid pleuritis
Lupus erythematosus
Drug-induced pleural disease
Asbestos pleural effusion
Yellow nail syndrome
Uremia
Trapped lung
Chylothorax
Pseudochylothorax
Acute respiratory distress syndrome
Chronic pleural thickening
Malignant mesothelioma
E. Treatment and Management
Transudative effusions are usually managed by treating the underlying medical
disorder. However, whether transudates or exudates, large, refractory pleural
38

effusions causing severe respiratory symptoms, even if the cause is understood
and disease-specific treatment is available, can be drained to provide relief.
The management of exudative effusions depends on the underlying etiology of
the effusion. Pneumonia, malignancy, or TB causes most diagnosed exudative
pleural effusions, with the remainder typically deemed idiopathic. Complicated
parapneumonic effusions and empyemas should be drained to prevent
development of fibrosingpleuritis. Malignant effusions are usually drained to
palliate symptoms and may require pleurodesis to prevent recurrence.
Medications cause only a small proportion of all pleural effusions and are
associated with exudative pleural effusions. However, early recognition of these
iatrogenic causes of pleural effusion avoids unnecessary additional diagnostic
procedures and leads to definitive therapy, which is discontinuation of the
medication. Implicated drugs include medications that cause drug-induced lupus
syndrome (eg, procainamide, hydralazine, quinidine), nitrofurantoin, dantrolene,
methysergide, procarbazine, and methotrexate.
Tuberculouspleuritis
Tuberculouspleuritis typically is self-limited. However, because 65% of patients
with primary tuberculouspleuritis reactivate their disease within 5 years, empiric
anti-TB treatment is usually begun pending culture results when sufficient
clinical suspicion is present, such as an unexplained exudative or lymphocytic
effusion in a patient with a positive PPD finding.
Chylous effusions
Chylous effusions are usually managed by dietary and surgical modalities.
However, studies suggest that somatostatin analogues also may help in reducing
the efflux of chyle into the pleural space.
Surgical treatment
39

Surgical intervention is most often required for parapneumonic effusions that
cannot be drained adequately by needle or small-bore catheters. Surgery may
also be required for the diagnosis and sclerosis of exudative effusions.
Video-assisted thoracoscopy with the patient under local or general anesthesia
allows direct visualization and biopsy of the pleura for diagnosis of exudative
effusions.
Pleurodesis by insufflating talc directly onto the pleural surface using video-
assisted thoracoscopy is an alternative to using talc slurries.
Decortication is usually needed for trapped lungs to remove a thick, inelastic
pleural peel that restricts ventilation and produces progressive or refractory
dyspnea. In patients with chronic, organizing parapneumonic pleural effusions,
technically demanding operations may be required to drain loculated pleural
fluid and to obliterate the pleural space.
Surgically implanted pleuroperitoneal shunts are another treatment option for
recurrent, symptomatic effusions, most often in the setting of malignancy, but
they are also used for management of chylous effusions. However, the shunts are
prone to malfunction over time, are poorly tolerated by patients, and can require
surgical revision.
In unusual cases, surgery might be required to close diaphragmatic defects
(thereby preventing recurrent accumulation of pleural effusions in patients with
ascites) and to ligate the thoracic duct to prevent reaccumulation of chylous
effusions.
E.1. TherapeuaticThoracentesis
Therapeutic thoracentesis to remove larger amounts of pleural fluid is used to
alleviate dyspnea and to prevent ongoing inflammation and fibrosis in
parapneumonic effusions. In addition to the precautions listed previously for
40

diagnostic thoracentesis, note 3 additional considerations when performing
therapeutic thoracentesis.
First, to avoid producing a pneumothorax during the removal of large quantities
of fluid, remove fluid during therapeutic thoracentesis with a catheter, rather
than with a sharp needle, introduced into the pleural space. Various specially
designed thoracentesis trays are available for introducing small catheters into the
pleural space. Alternatively, newer systems using spring-loaded, blunt-tip
needles that avoid lung puncture are also available.
Second, monitor oxygenation closely during and after thoracentesis because
arterial oxygen tension paradoxically might worsen after pleural fluid drainage
due to shifts in perfusion and ventilation in the reexpanding lung. Consider use
of empiric supplemental oxygen during the procedure.
Third, remove only moderate amounts of pleural fluid to avoid reexpansion
pulmonary edema and to avoid causing a pneumothorax. Removal of 400-500
mL of pleural fluid is often sufficient to alleviate shortness of breath. The
recommended limit is 1000-1500 mL in a single thoracentesis procedure.
Larger amounts of pleural fluid can be removed if pleural pressure is monitored
by pleural manometry and is maintained above -20 cm water. However, this
monitoring is rarely used by most proceduralists.
The onset of chest pressure or pain during the removal of fluid indicates a lung
that is not freely expanding, and the procedure should be stopped immediately to
avoid reexpansion pulmonary edema. In contrast, cough frequently occurs
during removal of fluid, and this is not an indication to stop the procedure,
unless the cough is causing the patient discomfort.
Mediastinal position and lung entrapment
The position of the mediastinum on the chest radiograph may predict whether a
patient is likely to benefit from the procedure. A mediastinal shift away from the
41

pleural effusion indicates a positive pleural pressure and compression of the
underlying lung that can be relieved by thoracentesis. (See the images below.)
Massive right pleural effusion with shift of mediastinum towards left
In contrast, a mediastinal shift towards the side of the effusion indicates lung
entrapment by extensive pleural involvement or endobronchial obstruction that
prevents reexpansion of the lung when the pleural fluid is removed, or it
indicates a lung trapped by encasement by chronic pleural thickening. Lung
entrapment with malignant effusions is most common with mesothelioma or
primary lung cancer.
Attempts at therapeutic thoracentesis usually do not improve dyspnea in patients
with lung entrapment, due to the inability of the lung to reexpand. In fact,
attempts at drainage of fluid in these patients usually results in a
hydropneumothorax being visualized on postprocedure imaging studies. (See the
image below.)
42

Lung entrapment with right hydropneumothorax and pleural drain in place
E.2. Tube Thoracostomy
Although small, freely flowing parapneumonic effusions can be drained by
therapeutic thoracentesis, most larger effusions and complicated parapneumonic
effusions or empyemas require drainage by tube thoracostomy.
Traditionally, large-bore chest tubes (20-36F) have been used to drain thick
pleural fluid and to break up loculations in empyemas. However, such tubes are
not always well tolerated by patients and are difficult to direct correctly into the
pleural space. However, small-bore tubes (7-14F) inserted at the bedside or
under radiographic guidance have been shown to provide adequate drainage,
even when empyema is present. These tubes cause less discomfort and are more
likely to be placed successfully within a pocket of pleural fluid. Using 20-cm
water suction and flushing the tube with normal saline every 6-8 hours may
prevent occlusion of small-bore catheters.
43

Insertion of additional pleural catheters, usually under radiographic guidance, or
instilling fibrinolytics (eg, streptokinase, urokinase, or alteplase) through the
pleural catheter can help to drain multiloculated pleural effusions.
A randomized trial of 210 participants with pleural infection showed that
instillation of alteplase and DNase produced significantly greater drainage of
pleural effusion, less need for surgical referral or surgical intervention, shorter
hospital stays, and a decrease in pleural fluid inflammatory markers compared
with placebo.
E.4. Pleurodesis
Pleurodesis (also known as pleural sclerosis) involves instilling an irritant into
the pleural space to cause inflammatory changes that result in bridging fibrosis
between the visceral and parietal pleural surfaces, effectively obliterating the
potential pleural space. Pleurodesis is most often used for recurrent malignant
effusions, such as in patients with lung cancer or metastatic breast or ovarian
cancer. Given the limited life expectancy of these patients, the goal of therapy is
to palliate symptoms while minimizing patient discomfort, hospital length of
stay, and overall costs.
Patients with poor performance status (Karnofsky score < 70) and a life
expectancy of less than 3 months can be treated with repeated outpatient
thoracentesis as needed to palliate symptoms. Unfortunately, pleural effusions
can reaccumulate rapidly, and the risk of complications increases with repeated
drainage.
In addition, patients with lung entrapment from malignant effusions are not
candidates for repeated thoracentesis, which does not relieve dyspnea in such
patients, nor for pleurodesis, as the visceral and parietal pleural surfaces cannot
44

stay apposed to allow the bridging fibrosis. The best treatment for effusions in
such patients is the insertion of an indwelling tunneled catheter, which allows
patients to remove pleural fluid as needed at home.
A 2006 systematic review found that in pleurodesis, rotating the patient through
different positions did not appear necessary to ensure distribution of soluble
sclerosing agents throughout the pleural space. In addition, neither protracted
drainage after instillation of sclerotics nor the use of larger-bore chest tubes
increased the effectiveness of pleurodesis.
Pleurodesis is likely to be successful only if the pleural space is drained
completely before pleurodesis and if the lung is fully reexpanded to appose the
visceral and parietal pleura after sclerosis. Animal studies suggest that systemic
corticosteroids can reduce inflammation during sclerosis and can cause
pleurodesis failures.
Sclerosing agents
Various agents, including talc, doxycycline, bleomycin sulfate (Blenoxane), zinc
sulfate, and quinacrine hydrochloride, can sclerose the pleural space and
effectively prevent recurrence of the malignant pleural effusion.
Talc is the most effective sclerosing agent and can be administered as slurry
through chest tubes or pleural catheters. Although a systematic review suggested
that direct insufflation of talc via thoracoscopy was more effective than talc
slurry, both were equally effective in a 2005 prospective trial of malignant
effusions. Importantly, talc particles tend to occlude the small drainage holes in
small pleural catheters. Therefore, pleural catheters should be at least 10-12F if
intended for talc pleurodesis.
45

Doxycycline and bleomycin are also effective in most patients and can be
administered more easily through small-bore catheters, although they are
somewhat less effective and substantially more expensive than talc.
All sclerosing agents can produce fever, chest pain, and nausea. Talc rarely
causes more serious adverse effects, such as empyema and acute lung injury.
The latter appears to be related to the particle size and the amount of talc
injected for pleurodesis.
Injection of 50 mL of 1% lidocaine hydrochloride prior to instillation of the
sclerosing agent may help to alleviate pain. Additional analgesia might be
required in some cases. Clamp chest tubes for approximately 2 hours after
instillation of the sclerosing agent.
E.2. Monitoring Pleuaral Drainage
Record the amount and quality of fluid drained and monitor for an air leak
(bubbling through the water seal) at each shift. Large air leaks (steady streams of
air throughout the respiratory cycle) may be indications of loose connectors or
of a drainage port on the catheter that has migrated out to the skin. Alternatively,
they may indicate large bronchopleural fistulae. Consequently, dressings should
be taken down and the position of the catheter inspected at the puncture site.
Briefly clamping the catheter at the skin helps to determine whether the air leak
is originating from within the pleural cavity (in which case, it stops when the
tube is clamped) or from outside the chest (in which case, the leak persists).
Repeat the chest radiographs when drainage decreases to less than 100 mL/day
to evaluate whether the effusion has been fully drained. If a large effusion
persists radiographically, reevaluate the position of the chest catheter using chest
CT scanning to ensure that the drainage ports are still positioned within the
pleural collection. If the catheter is positioned appropriately, consider injecting
46

lytics through the chest tube to break up clots that may be obstructing drainage.
Alternatively, chest CT scanning may reveal lung entrapment/trapped lung,
which is unlikely to respond to further drainage in the hospital.
IV. CONCLUSION
Treating the underlying disease is the definitif treatment of pleura effusion. So,
it must be found the etiology.
Massive pleura effusion can be removed through the thoracosentesis, WSD, or
pleurodesis.
REFERENCE
W, Aru. Sudoyo, et all. 2006. Ilmu Peyakit Dalam Ed IV Jilid I. Department of Internal
Medicine Medical Faculty of Indonesian University. Jakarta.
Arun Gopi, Sethu M. Madhavan, Surendra K. Sharma and Steven A.Sahn. 2007.
Diagnosis and Treatment of Tuberculous Pleural Effusion in 2006. American College of
Chest Physicians.
Halim, Hadi. 2007. Penyaki-Penyakit Pleura dalam Buku Ajar Ilmu Penyakit Dalam,
Jilid II, Edisi IV. Department of Internal Medicine Medical Faculty of Indonesian
University. Jakarta.
47
Recommended