
8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 1/69
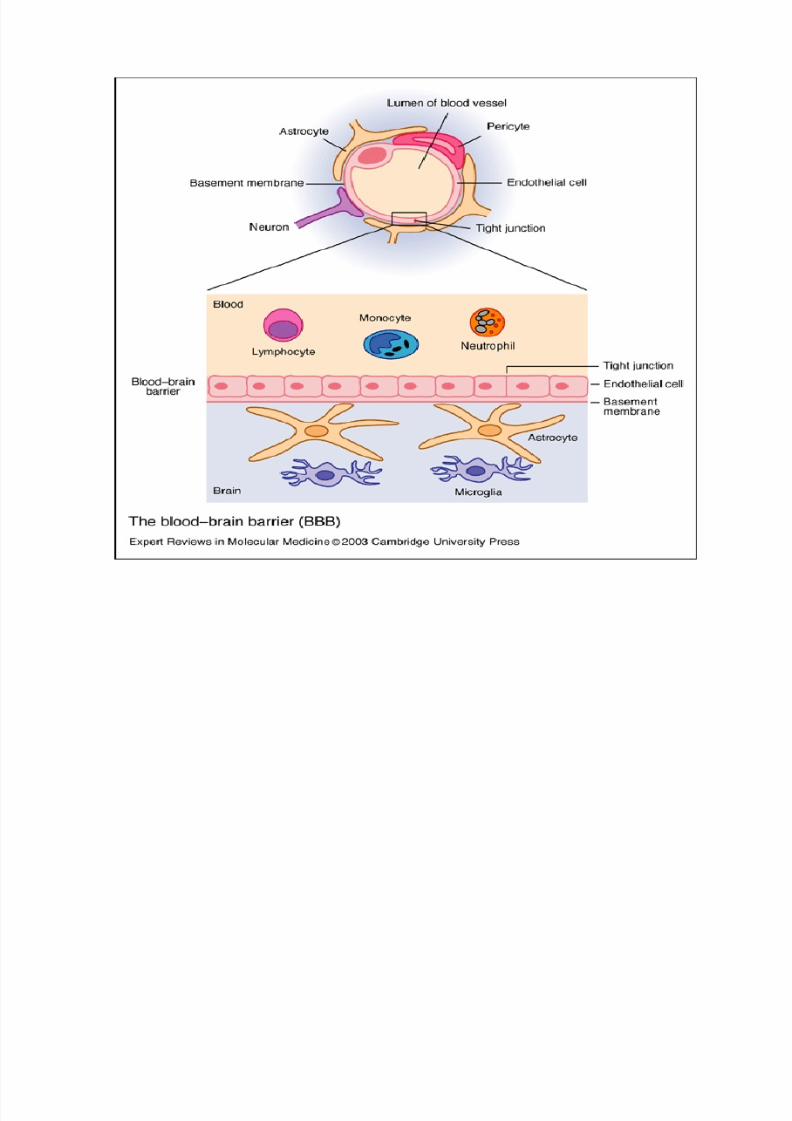
Blood brain barrier
� The CNS blood brain barrier is created by tight
junctions between endothelial cells and a
basement membrane supported by astrocytic
foot processes; this presents a formidable
barrier to drug penetration. Lipid soluble
agents or drugs with specific transport
mechanisms can penetrate rapidly.
8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 2/69

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 3/69

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 4/69
Approaches to BBB
� Use of permeation enhancers such as
dimethyl sulphoxide (DMSO)
� Osmotic disruption of the BBB by infusinginternal carotid artery with mannitol.
� Use of dihydropyridine redox system as drug
carriers to the brain.(Prodrug for polar drugs)
8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 5/69
Brain Cerebrospinal fluid barrier
� CSF is formed mainly by the choroid plexus of
the lateral, third and fourth ventricles
� It is similar in composition to the ECF of the
brain.
� Characteristics' similar to that of BBB

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 6/69
� The capillary endothelium that lines the
choroid plexus have open junctions or gapsand drugs can flow freely into the extracellular
space between the capillary walls and the
choroidal cells.
� Choroidal cells are joined to each other bytight junctions forming blood-CSF barrier
which has permeability similar to BBB

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 7/69

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 8/69
� For Any given drug conc. In brain higher than
in CSF, because bulk flow of CSF continuously
removes drug.

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 9/69
Blood placental barrier
� Number of tissue layers
� Mean thickness of the barrier 25 microns in
early pregnancy, 2 microns in full term� < 1000 Daltons MW & moderately high lipid
soluble drugs cross the barrier by simple
diffusion quite rapidly.
� Not as effective a barrier as BBB
� Nutrients carrier mediated process

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 10/69
Drugs in the mother's blood can cross the placental
membrane into blood vessels in the villi and pass
through the umbilical cord to the fetus

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 11/69
PERFUSION OR PERMEATION RATE
LIMITED

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 12/69
� Perfusion rate: defined as the vol. of
blood that flows per unit time per unitvol. of tissue, ml/min/ml
� Highly perfused :lungs,kidneys,liver,heart
,brain
� Moderately perfused: muscles, skin
� Poorly perfused: bones,fat(adipose
tissue)

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 13/69
� Kt=perfusion rate/Kt/b
� Kt/b=tissue/blood partition coefficent of drug
� Kt=Distribution rate constant� Tissue Distribution half life=0.693/Kt=
0.693/Kt/b
� Eg thiopental: lipophilic, high Kt/b towards brain still higher for
adipose tissue. Brain highly perfused organ, iv inj. Rapid onset of
action, adipose tissue poorly perfused, vol 5 times that of brain.
Rapid termination of action due to tissue redistribution.

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 14/69
8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 15/69

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 16/69

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 17/69
ORGAN TISSUE AND PERFUSION
RA
TE

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 18/69

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 19/69
Miscellaneous factors
� Age
� Total body water: much greater in infants
� Fat contents: higher in infants& elderly� Skeletal muscles: lesser in infants & elderly
� Organ composition: BBB poorly developed in
infants , mylein content high,>penetration of drugs in brain
� Plasma protein content : low albumin in
infants and elderly

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 20/69
� Pregnancy : Vol. available fordistribution of drugs is high.
� Plasma and ECF vol. also increase but
there is fall in albumin content.

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 21/69
Miscellaneous factors
� Obesity: high adipose tissue
� Diet� Disease States: altered albumin and other
drug-binding protein conc.
� Altered organ/tissue perfusion.� Altered pH

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 22/69
Drugs appear to distribute in the body as if it werea single compartment. The magnitude of the drug¶s
distribution is given by the apparent volume of distribution (Vd). Vd bears no direct relation shipwith real vol of distribution.
Amount of drug in bodyConcentration in Plasma
Vd =
VOLUME OF DISTRIBUTIONVOLUME OF DISTRIBUTION

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 23/69
Volume of Distribution
Volume into which a drug appears todistribute with a concentration equal to its
plasma concentration

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 24/69

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 25/69

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 26/69
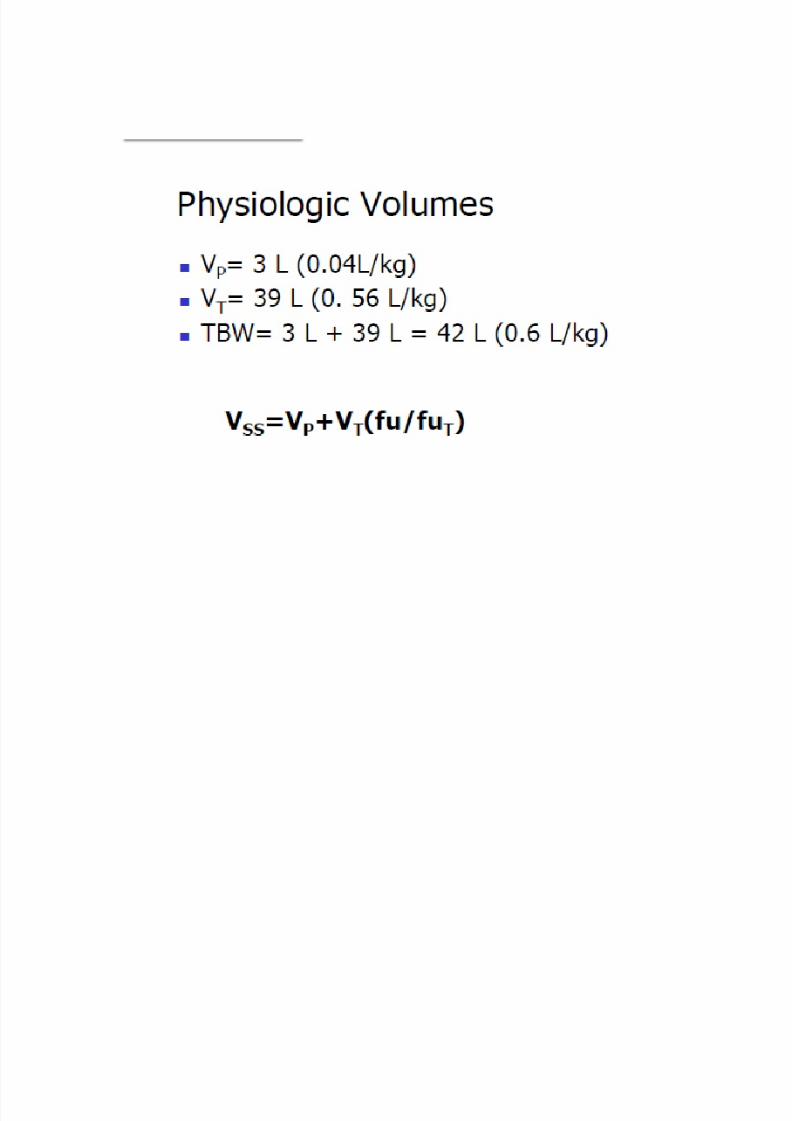
Determination of Physio. Vol.
� Plasma vol:Tracers or markers ; subs of high mol
wt totally bound to plasma ALBUMIN Evans
blue, Indocyanine green, I-131
� ECF: easily penetrate capillary membrane &
rapidly distribute through ECF but donot cross
cell memb.:mannitol,inulin,ions(Na+,Cl-
,sulphate)
� TBW: subs that distribute equally in all water
compts. Heavy water, tritiated water,antipyrine

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 27/69

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 28/69

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 29/69
Vd is useful in determining an appropriate dose toobtain a particular plasma level, therapeuticlevels are measured and referenced to plasmalevels.
A large Vd has an important influence on the half-life of a drug because elimination usuallydepends on the amount of free drug deliveredto the liver or kidney, with a large volume of distribution much/most of a drug will beextravascular or protein bound and not readilyavailable to excretory organs.

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 30/69
CONCLUSION:
FACTORS THAT PRODUCE ALTERATION IN
BINDING OF DRUG TO BLOOD COMPONENTS:
INCREASES Vd
FACTORS THAT INFLUENCE DRUG BINDING TO
EXTRAVASCULAR COMPONENTS: DECREASES
Vd
OTHER FACTORS:TISSUEPERFUSION,PERMEATION,IONISATION,
DISEASE STATE ETC.

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 31/69
PROTEIN BINDING
8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 32/69
� Intracellular binding: when drug is bound to a
cell protein which may be the drug receptor, if
so, binding elicits a pharmacological
response.receptors:primary receptors
� Extracellular binding: when drug is bound to a
extracellular protein but the binding doesnot
elicits a pharmacologicalresponse.receptors:secondary,silent receptors
� Binding reversible, suggests weak
bonds(hydrogen, vanderwalls)

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 33/69
PROTEIN ± DRUG BINDING
8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 34/69
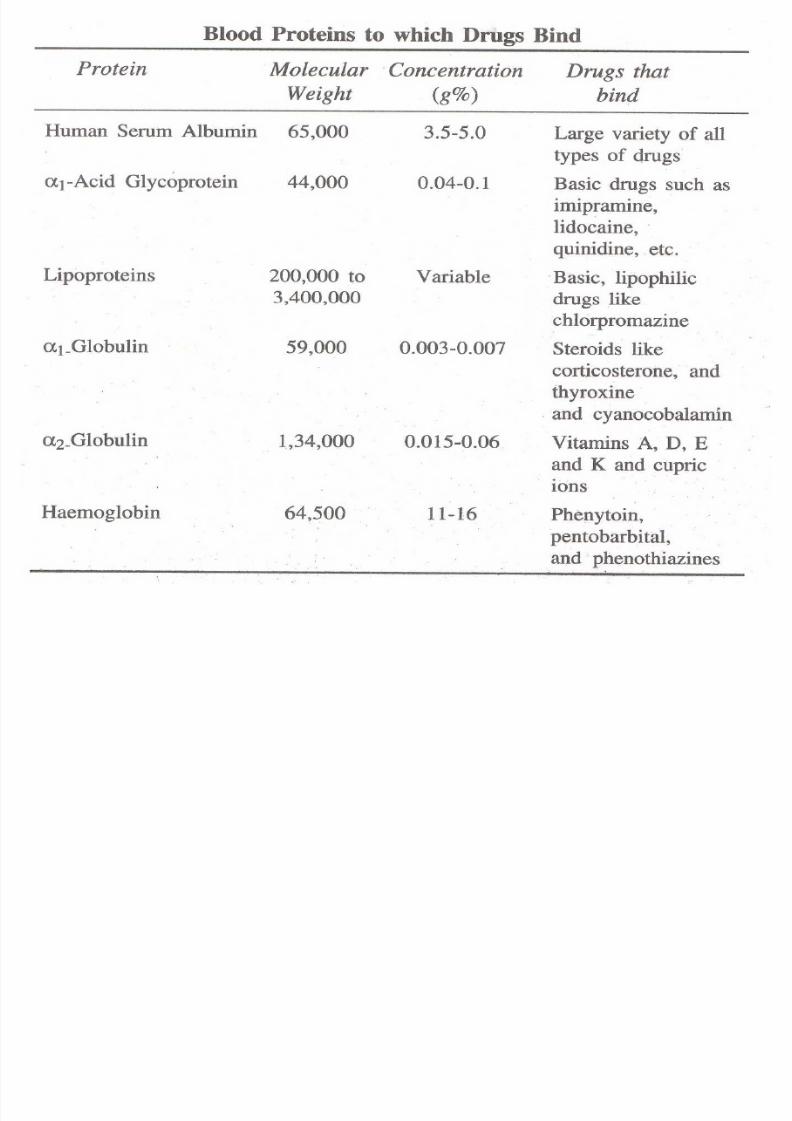
Plasma protein binding
� Entry into systemic circulation, first thing
which can interact with drug: blood
components, like plasma proteins, blood cells,
Hb
� Binding to plasma protein reversible
� Mostly bound to albumin
� HAS: MW 65000, abundant(59% of total
plasma)
8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 35/69

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 36/69
Binding of drugs to HSA
� Warfarin site: NSAIDs,bilirubin,phenytoin,
sodium valproate
� Diazepam binding site: benzodiazepines,ketoprofen, ibuprofen, trytophan
� Site III and IV : very few drugs bind.

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 37/69

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 38/69
� Primary site
� Secondary site:
� eg. Dicoumarol primary site1, secondary site 2� Drugs compete for site
8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 39/69
Tissue binding of drugs
� 40% of body wt is tissue. 100 times that of HSA.
� it increases Vd
� Results in localisation of drug at specific site in
body, some drugs bind irreversibly to tissues
eg. oxidation pdts of PCM,
phenacetin,chloroform etc. bind covalently to
hepatic tissues.
� Extensive tissue binding suggest tissue can act
as a storage site for drugs.
� liver>kidney>lung>muscles

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 40/69

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 41/69
DETERMINATION OF PROTEIN BINDING
� Indirect techniques: based on separation of
bound form from the free micromolecule.
:equilibrium dialysis, dynamic dialysis, ultra
filtration, gel filtration, ultracentrifugation
� Direct techniques: Do not require separationof bound form of drug from the free
micromolecule: spectroscopy, fluorimetry, ion
selective electrodes

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 42/69
FACTORS AFFECTING PROTEIN BINDING
� Drug related factors
� Protein-tissue related factors
� Drug interactions
� Patient related factors

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 43/69
Drug related factors
� Conc. of drug in the body: HSA
no saturation, lidocaine can saturate AAG
� Drug-protein tissue affinity� Lidocaine greater affinity for AAG than has ,
digoxin greater affinity for protein of cardiacmuscles than skeletal muscles

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 44/69
Physicochemical characteristics of the drug
� Lipophilicity and larger binding, eg.slowabsorption of cloxacillin in comparison to
ampicillin after im inj.
� Anionic or acidic drugs bind more to HAS
� Cationic or basic drugs bind more to AAG
� Neutral unionized drugs bind more tolipoproteins
� Stereo selective binding eg.
Chloroquin,propranolol,ibuprofen

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 45/69
Protein-tissue related factors
� Physicochemical properties of
protein/Binding component
� Lipoproteins & adipose tissue bind lipophilic drugs
by dissolving them in the lipid core.
� Conc. of protein/Binding component
� Number of binding sites on proteins� AAG limited binding sites, albumin large no.

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 46/69
DRUG INTERACTIONS
� Competition between Drugs for binding sites� Drug -drug interaction for the common
binding site is called displacement reaction.
� Displaced drug---displacer� Eg. Warfarin displace by phenylbutazone
phenylbutazone---HAS
� Free warfain may cause hemorrhagicreactionwhich may be lethal.
� Unexpected rise in free drug conc. ---toxicity
or enhanced clinical response

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 47/69
� Clinically significant interaction occurs when:
� Displaced drug:
� is more than 95% bound� Has a small Vd (less than 0.15L/kg)
� Shows rapid onset of therapeutic or adverse
effects� Has a narrow therapeutic index

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 48/69
� Displacer drug:
� has higher degree of affinity for protein
competes for same binding site
� Drug/ protein conc. ratio is high(above 0.10)
� Showa a rapid and large increase in plasma
drug conc.

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 49/69
� 95% bound drug, displacement of 5% bound
drug results in 100% increse in free drug conc.
� Small Vd: remains in blood ---toxicity
� Large Vd; redistributes into large vol of body
fluids----insignificant clinical effects
� increase in free drug conc.---more available for
elimination
� If drug easily metabolisable or excretable
displacement results in in elimination half
life

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 50/69

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 51/69
� Competition between drugs and normal body
constituents
� Free fatty acids are known to interact with a no. of
drugs that bind primarily to HSA.
� Free fatty acid in fasting, pathological conditions,
pcologically induced conditions(after caffeine,heparin admin.)
� Influence binding of several benzodiazepines,
prpranolol, warfarin� Bilirubin binding to HSA-acidic drugs--free bilirubin
not conjugatedneonates---kernicterus.

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 52/69
Patient related factors
� Age
� Inter subject variation� Disease state

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 53/69

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 54/69
Conclusion
� All factors that affect protein bindinginfluence:
� 1. Pharmacokinetics---in plasma-protein
drug binding--- in unbound drug---tissue
redistribution/clearanceenhnace
biotransformation, excretion
� 2. Pharmacodynamics---- in conc. of free or
unbound drug results in intensity of action
(therapeutic/toxic)

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 55/69
Significance of protein tissue binding of drugs
�A
bsorption� Displacement interactions & toxicity
� Systemic solubility of drug
� Distribution
� Tissue binding
� Elimination
� Diagnosis(thyroid gland iodine compds)
� Therapy and drug targeting

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 56/69

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 57/69

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 58/69
8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 59/69
8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 60/69

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 61/69

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 62/69

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 63/69
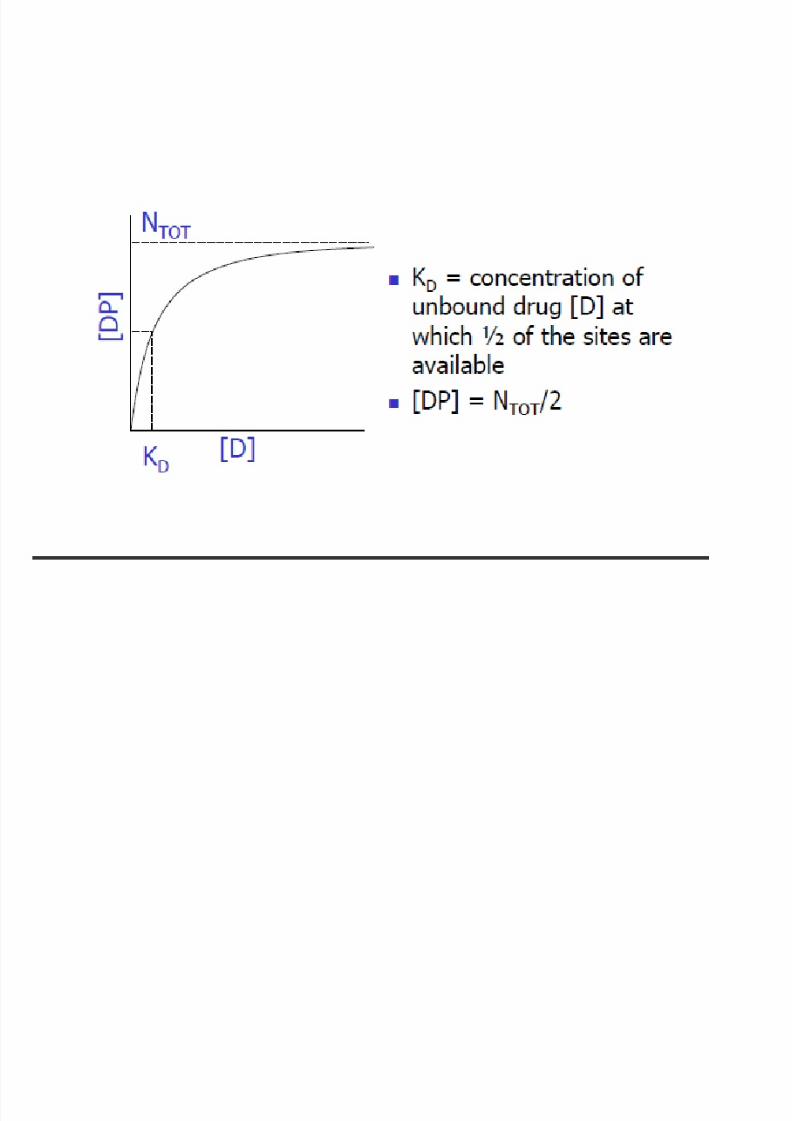
KINETICS OF PROTEIN BINDING

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 64/69

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 65/69

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 66/69

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 67/69
8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 68/69

8/6/2019 Distribution Scop
http://slidepdf.com/reader/full/distribution-scop 69/69
Recommended


![Sociétés coopératives - QUIZZ ANNONCES [Info]Scop · 2014-05-01 · La lettre de l’Union Régionale des Scop de l’Ouest [Info]Scop[Numéro 32] JUILLET 2009 ÉDITORIAL Traditionnellement,](https://img.dokumen.tips/doc/110x75/5f3ec9236e8d9c629d6b8e04/socits-coopratives-quizz-annonces-infoscop-2014-05-01-la-lettre-de-launion.jpg)














