Conflicto de intereses:
AstraZeneca

¿Qué es la doble terapia antiagregante, y cuánto
debe durar?

3.6
2.7
0.5
Aspirin
Aspirin & warfarin
Aspirin & ticlopidine
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 0
1.0
2.0
3.0
Days after Stenting
Cu
mu
lati
ve I
ncid
en
ce
Of
Pri
mary
En
dp
oin
t (%
)
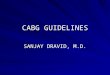
Primary Endpoint: Death, MI, TLR or thrombosis at 30 days
Leon MB et al. N Engl J Med 1998;339:1665-71
p<0.01
STARS: DAPT with Aspirin and a Thienopyridine Reduces Thrombotic Events after PCI

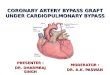
Registros a favor del tratamiento prolongado con
DAPT en pacientes con DES de 1ra generación
% D
/MI
P=0.02
50% RRR
637 579
N=1,216
Eisenstein EL et al, JAMA 2007
P=0.50
417 1,976 %
D/M
I
18 Month Events After Clopidogrel
Discontinuation at 6 Months Stratif ied
by Stent Type*
73% RRR
499 244
*N=3 *N=24
Pfisterer M et al, J Am Coll Cardiol 2006
24 Month Events in Patients who
Discontinued or did not Discontinue Clopidogrel
at 6 Months Stratif ied by Stent

M. Valgimigli, MD, PhD
University of Ferrara, ITALY
On behalf of the PRODIGY Investigators
PROlonging Dual antiplatelet treatment after
Grading stent-induced Intimal hyperplasia studY
ESC, Hotline III, Paris, August, 30, 2011

Aspirin
PRODIGY Study Flow Chart Intent-to-stent
1:1
1:1:1:1
30-Days
Balancing Randomization
1° Endpoint Randomization
6 mos
12 mos
18 mos
24 mos
6 mos
12 mos
18 mos
Aspirin
6 mos
12 mos
18 mos
24 mos
Short
DAPT
Clopidogrel
6 Mos*
24 Mos
Prologned
DAPT
Xience V® Taxus® Endeavor® BMS
*: <6 months clopidogrel was allowed in BMS pts with stable CAD at the time of PCI
Clopidogrel

Primary Endpoint
No. at Risk
24-Month Clopidogrel 987 925 884
6-Month Clopidogrel 983 919 881
Overall Death, MI or CVA
24 mo DAPT 6 mo DAPT %
10.0
Hazard Ratio: 0.98 (0.74-1.29)
10.1
0 180 360 540 720
12
8
4
0
P=0.91
CEC adjudicated

Key Safety Endpoint
No. at Risk
24-Month Clopidogrel 987 925 884
6-Month Clopidogrel 983 919 881
Type II, III or V BARC bleeding
24 mo DAPT 6 mo DAPT %
3.5
Hazard Ratio: 0.46 (0.1-0.69)
7.4
P=0.00018
CEC adjudicated
0 180 360 540 720
12
8
4
0

OPTIMIZE: Diseño
N= 3120 patients
1:1 randomization
33 sites in Brazil
Broad patient population
undergoing PCI with Endeavor ZES
RVD 2.5 mm–4.0 mm
Primary Endpoint: NACCE (Death/MI/Stroke/Major Bleeding) at 12 months Secondary Endpoints: ARC-defined ST, TVR, TLR, MACE, DAPT compliance, and major bleeding
(REPLACE-2 & GUSTO definitions)
6 mo 18 mo 12 mo
Clinical endpoints
30 d 36 mo 3 mo
3 months DAPT
N=1560
12 months DAPT
N=1560
NACCE=Net Adverse Clinical and Cerebral Events.
MACE (major adverse cardiac events) is composed of death, MI, emergent CABG, TLR.
Feres F et al. JAMA. 2013;310:2510-2522
24 mo

Landmark at 3M: NACCE (All-Cause Death, MI, Stroke, Major Bleeding)
Month 0 1 3 6 12
No. at risk 1563 1520 1504 1468 1384
No. events 18 25 11 18 21
No. at risk 1556 1514 1497 1466 1381
No. events 16 25 11 16 22
HR 1.03
(0.66–1.60)
P=0.91
Inc
ide
nc
e o
f N
AC
CE
(%
)
Time After Initial Procedure (months)
0 12
0
10
15
5
3 6 9
3M DAPT
2.6
2.6
HR 1.03
(0.71–1.51)
P=0.86
12M DAPT
3.3 3.5
Feres F et al. JAMA. 2013;310:2510-2522.

Stent Thrombosis vs Bleeding
Month 0 1 3 6 12
No. at risk 1563 1555 1540 1506 1505
No. events 0 6 3 4 0
No. at risk 1556 1541 1525 1501 1500
No. events 5 3 3 1 0
Month 0 1 3 6 12
No. at risk 1563 1538 1516 1482 1439
No. events 4 15 10 4 2
No. at risk 1556 1528 1501 1472 1387
No. events 11 8 12 6 8
Any Bleeding*
Time After Initial Procedure (months)
0.4
1.0
HR 0.43 (0.16-1.11)
P=0.07
0 12
0
10
5
3 6 9
HR 0.93
(0.56-1.54)
P=0.78
3M DAPT
12M DAPT
1.9
2.0
ARC Def/Prob Stent Thrombosis
3M DAPT
12M DAPT
Time After Initial Procedure (months)
0.3
0.1
HR 3.97 (0.44-35.49)
P=0.18
0 12
0
10
5
3 6 9
HR 0.81
(0.34-1.96)
P=0.64
Incid
en
ce (
%)
0.7
0.6
*Any bleeding according to the combined REPLACE-2 and GUSTO criteria. Feres F et al. JAMA. 2013;310:2510-2522.

13
DAPT Study: Diseño
50% of patients continue on
dual antiplatelet therapy
18 mos. 12 mos.
50% of patients receive
aspirin + placebo
Total 33-month patient evaluation including additional 3-month follow-up
All patients on
aspirin + open-label
thienopyridine
therapy for
12 months
DES n=
23,210
BMS n=
2985
Completed
enrollment
2011
1:1 randomization
at month 12
www.daptstudy.org
www.clinicaltrials.gov – NCT00977938
Mauri L et al. Am Heart J. 2010;160:1035-1041.

European Heart Journal online, oct 2013 - DOI:10.1093/eurheartj/eht438
Registro SWEDEHEART

European Heart Journal online, oct 2013 - DOI:10.1093/eurheartj/eht438
Estudio observacional de cohorte prospectivo del
registro sueco SWEDEHEART.
56000 pacientes con SCA seguidos entre 2006 y 2010.
Relación entre duración de DAPT y eventos en el
“mundo real”, en una población contemporánea no
seleccionada de gran tamaño.

European Heart Journal online, oct 2013 - DOI:10.1093/eurheartj/eht438

¿Cuánto tiempo debe mantenerse la doble
antiagregación en SCA según las guías?
PCI ACC/AHA/SCAI
2009 Update
I BMS or DES – at least 12 months
IIb ADP blockade beyond 15 months may be
considered in patients with DES
NSTE-
ACS
ACC/AHA
2007 Update
I Conservative – at least 1 month and up to 12
[see 2009 PCI Update]
ESC 2007 Ia Clopidogrel should be maintained for 12 mos
unless there is an excessive risk of bleeding
STEMI ACC/AHA
2007 Update
I Clopidogrel for at least 14 days (Class I)
IIa Maintenance with clopidogrel ( eg, 1 year) is
reasonable
ESC 2008 IIa Clopidogrel for 12 months in all patients
irrespective of acute treatment
Desde 2007 en adelante, todas las guías y consensos recomiendan 12
meses de doble terapia antiagregante en SCA.

Trombosis del stent
Airoldi F, Colombo A et al. Circulation 2007; 116: 745-754.

Trombosis del stent:
un evento poco frecuente, pero catastrófico
Airoldi F, Colombo A et al. Circulation 2007; 116: 745-754.
3021 pac. con 5389 lesiones coronarias tratadas con
DES.
Trombosis del stent (TS): 58 pacientes (1,9%) a 18
meses de seguimiento, 42 (1,4%) dentro de los 6
meses de la ATC. De los casos con TS, presentaron:
IAM: 46 pacientes (79%)
Muerte: 23 pacientes (39%).

Trombosis del stent
Airoldi F, Colombo A et al. Circulation 2007; 116: 745-754.

Cirugía no cardíaca post ATC con stent
La cirugía promueve una respuesta inflamatoria y un estado
protrombótico. Existe liberación de mediadores de inflamación, activación plaquetaria
y disminución de la fibrinolisis.
Esto predispone a eventos coronarios, tanto en el sitio del
stent como así también a nivel de otras lesiones
ateroescleróticas.
Se estima que 5-10% de pac. con stents coronarios serán
sometidos a una cirugía no cardíaca dentro del año de la ATC.
La decisión acerca del momento óptimo de la cirugía y el
manejo de la antiagregación es crucial.

Hawn M et al. JAMA 2013;310:1462-1472.

Hawn M et al. JAMA 2013;310:1462-1472.

Hawn M et al. JAMA 2013;310:1462-1472.

Hawn M et al. JAMA 2013;310:1462-1472.

Hawn M et al. JAMA 2013;310:1462-1472.

Wijeysundera D et al. Circulation 2012;126:1355-1362

Wijeysundera D et al. Circulation 2012;126:1355-1362

European Heart Journal online, sept 2014 - doi:10.1093/eurheartj/ehu278

European Heart Journal online, sept 2014 - doi:10.1093/eurheartj/ehu278

European Heart Journal 2014; 35:2383-2431.

European Heart Journal 2014; 35:2383-2431.

European Heart Journal 2014; 35:2383-2431.

Análisis de la evidencia - Recomendaciones
No existen ensayos controlados y randomizados que
aborden el problema; la evidencia es nivel C.
La discontinuación de DAPT antes de los plazos
recomendados se asocia a un incremento en el riesgo de
eventos mayores (M-IAM-TS).
Por otra parte, ciertas cirugías tienen un riesgo
inaceptablemente elevado de complicaciones en caso de
sangrado (intracraneales, canal espinal, cámara posterior del
ojo), lo cual obliga a suspender todo antitrombótico.

Se sugiere diferir las cirugías electivas por al menos 6
meses luego de la angioplastia siempre que sea posible,
independientemente del tipo de stent.
En pacientes que no pueden esperar el plazo ideal de al
menos 6 meses, se sugiere posponer la cirugía al menos por
6 semanas post ATC.
Para la mayoría de los pacientes que no han alcanzado el
plazo óptimo de duración de DAPT post ATC, se sugiere
operar sin suspender DAPT. En cirugías de alto riesgo de sangrado, tratar de suspender los inhib.
P2Y12 y continuar con aspirina sola.
En cirugías donde el sangrado sería catastrófico (intracraneales,
canal espinal, cámara posterior del ojo) suspender todo antiagregante.
Idealmente en estos casos, diferir 6 semanas (BMS) o 6 meses (DES).
Recommended