CONCEPT OF STIMULATION &RECENT FINDINGS FROM A
LONGITUDINAL STUDY
Dr. Shahnaz Vazir
National Conference on
“Early Learning: Status and The Way Forward”
September 25th to 27th, 2013
IHC New Delhi

CONCEPT OF STIMULATION
‘Responsive and increasingly complex developmentally appropriate interactions between caregivers and children that promote their emerging abilities, improve learning and enhance children’s development’ -Young, 2002, Landry et al, 2006).
Help infants and young children lagging behind in cognitive, language, socio-emotional development to catch up.
Advances in brain development indicate that provision of meaningful sustained challenging stimuli from birth can increase neural interconnectivity
Stimulated children can improve their abilities by strategies
that offer age appropriate new learning opportunities

Why focus on infancy/early childhood?
• Brain development rapid and vulnerable from
conception to 3 years
• Insults and interventions can have lasting effects
• Interventions are more cost effective than at other ages
• Cognitive ability & behavior on school entry predict
academic success

Fetus Late Infancy/Toddler Pubertal
Vulnerable period birth – age 3
Developmental Perspective
Thompson & Nelson, 2000

Brain requires stimulation for synaptic growth

2007 Lancet Series on Child Development
• >200 million <5 y children in LAMI countries do not reach their developmental potential.
• Most live in South Asia and Sub-Saharan Africa.• Prevalence data on early stunting & number of people
living in absolute poverty can used as indicators of poor development as few national statistics on child development
• Poor school performance/ drop out, subsequent low incomes, high fertility, poor care for their children contribute to the intergenerational transmission of poverty & illiteracy.

2011 Lancet Series on Child Development
• Inequality & early childhood risk factors for CD:
• Stunting, inadequate cognitive stimulation, iodine
deficiency, and iron deficiency anaemia.
• Toxicity in the environment: intrauterine growth
restriction, maternal depression, exposure to
violence, malaria, diarrhoea, exposure to heavy
metals.
• Risks often occur together and cumulatively increase
adverse effects on the development

2011 Lancet Series on Child Development
Strategies & effective interventions to promote CD:
• Programs that provide direct learning experiences to children and families, • Targeted toward younger and disadvantaged children, • Of longer duration, high quality, and high intensity, • Integrated with family support, health, nutrition, or educational systems
and services.
• Despite convincing evidence, program coverage is low.
MDGs of reducing poverty and ensuring primary school completion can be achieved by expansion of high quality, cost-effective early child development programs.

The Efficacy of an Integrated Feeding & Care Intervention Among 3 to 15 Months Old Children in Andhra Pradesh, India
INDO-US Program On MCHDR 3-R01-HD042219-02-04Funding: ICMR, NIH, UNICEF
Indian Investigators US InvestigatorsDr. Shahnaz Vazir (PI) Dr. Margaret Bentley (PI)Dr. N. Balakrishna Dr. Patrice EngleMs. Sylvia Fernandez Dr. Paula GriffithsDr. Usha Naik Dr. Susan Johnson
Dr. Hilary Creed-KanashiroDr. Monal Shroff
National Institute of Nutrition (ICMR) Hyderabad, India
Carolina Population CenterThe University of North Carolina at Chapel Hill

• To implement a randomized controlled behavioural intervention trial to assess effects of breastfeeding, complementary and responsive feeding education to caregivers, and promotion of developmental skills to improve infant growth & development.
• 3 Arm Study: – 200 in each group, 60 villages, 600 mother-infant pairs
– Group 1 Control : no intervention, assessment only– Group 2 Intervention for complementary feeding education– Group 3 Intervention for complementary feeding plus
responsive feeding and infant development
OBJECTIVES
Vazir S., P. Engle, N. Balakrishna, P.L. Griffiths, S.L. Johnson, H. Creed-Kanashiro, S. et al. 2013. Cluster-randomized trial on complementary and responsive feeding education to caregivers found improved dietary intake, growth and development among rural Indian toddlers. MCN 9: 99-117.

Care for Development Module Provides age-based recommendations for parents on
• how to play (cognitive development) & communicate (language and social development) with their children from birth through 2 years of age,
• possible solutions to problems that caregivers may have.
The Mother- Child Protection Card has C for D recommendations along with those for infant and young child feeding.
The C & D module should improve parents’ ability to support their children’s development, and
Link development with effective feeding practices, including responsive feeding.

Goals of child development intervention
• Language development Increase total language Encourage conversation
• Help caregiver expand child’s play Expand use of toys Explore objects

Child development messages
• Smile & look in your child’s eyes• Respond to child’s sounds, gestures and interests• Play simple games e.g. peek a boo• Talk to child and give names for things and people• Ask your child simple questions• Give time to explore objects / persons / things• Help your child find new things to do with toys• Explain and show children how to do things


Intervention through
• Home visits by VLW• Flipcharts included culturally appropriate photographs &
messages– Promote conversations and discussion– Tailored opportunities - motivation
• ‘Tell me what you see’ in this picture• Checking questions: ‘Last time we talked about allowing
your child to explore the food and self-feed…play…did you try this?’

Assessment Schedule Month of Child’s Life 3-4 6 9 12 15
INFANT OUTCOME:
Anthropometry (length, wt)
Hb levels
CHILD DEVELOPMENT:
Child development: play videos
Bayley Scales of Infant Development II
Denver Developmental Screening
DIETARY INTAKE:
Food freq : 1 wk; 24 h recall;
Breast milk frequency & duration
MATERNAL FACTORS:
Age, Education
BMI, Hb levels,
PROCESS VARIABLES:
Maternal knowledge, beliefs: ch hlth, dev HOME scale (age appropriate)
Feeding behaviors (videos)

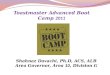
At 15 months mothers in group 3 report more stimulation than
others
0
20
40
60
80
100
120
Books*
Toys
Smile
/look*
Ask q
uest*
Play-
smar
t*
Way
s of p
lay*
Per
cen
t
Group 1 Group 2 Group 3
* P < .05
No significant difference between Groups at 3 months (Baseline)

Change in total HOME by age of child
78
79
80
81
82
83
84
85
86
87
88
89
90
3m 6m 9m 12m 15m
1
2
3
1<2 and 3

Change in caregiver responsivity by age of child
18
19
20
21
22
3m 6m 9m 12m 15m
1
2
3
1<2 and 3

Change in learning opportunities by age of child
13
14
15
16
17
3m 6m 9m 12m 15m
1
2
3
1<2 and 3
1<2 and 3 1<2<3

DQs vary by group
98100102104106108110112114116118
Mental Motor
group 1
group 2
group 3
1 <3;2<3*
Mental p=.018, 2<3 p=.07; motor not different
NS


Results on Growth
Group 2 compared to Group 1 had:• better improvement in haemoglobin from 3-15 months• less morbidity • higher HAZ at 15 m
Group 3 compared to Group 1 had:• no sig differences on growth outcomes• better improvement in haemoglobin from 3-15 months• less morbidity

Results on Food Intake
• Increases in maternal knowledge on infant feeding • Changes in behavior
– Rice given more times per day (increase in energy as per RD)
– Earlier introduction of animal products• Meat, liver, eggs (though in small amounts)
– Earlier introduction of green leafy vegetables and fruits
– Increases in amount of food consumed & nutrients but not equal to RDA

RESPONSE TO CHILD REFUSAL
“One more bite
verbal/ non-verbal distractions

Study recommendations for effective parenting interventions
1. Need for practice with children, for feedback, and rationale – not just information
2. Requires reinforcement on several channels
3. Strengthen, motivate and support caregiver to be positive about self and about child; build peer support
4. Toys, books, or household objects (to play) do help
5. Recommendations:• culturally appropriate stimulation• specific enough to understand and to do (formative
research)• simple and not too many messages


STRATEGIES TO PROMOTE COGNITION AMONG LOW-INCOME RURAL INFANTS & PRESCHOOLERS IN INDIA: Micronutrient Supplementation & Early Learning Opportunities
Research Team:
PIs: Drs. Sesikeran & Maureen Black
NIN: Drs. Shahnaz Vazir, K. Madhavan Nair, Radha Krishna, N. Balakrishna, Sylvia Fernandez Rao
UMB: Drs. Kristen Hurley, Yan Wang, Larry Magder
MI: Drs. Kim Harding, Lynnette Neufeld
The Mathile Institute: Dr. Greg Reinhart

OBJECTIVE
• To examine how innovative multiple micronutrient (MN) fortification strategies for infants and preschoolers combined with early learning opportunities impact children’s micronutrient status, growth and development through a randomized double-blind controlled trial in Nalgonda district of Andhra Pradesh, India.

MMN Fortification
MMN* 6-12 months 12-24 months Preschool
Iron 8 mg 10 mg 13 mg
Zinc 5 mg 5 mg 5 mg
Folic acid 20 mg 20 mg 20 mg
Vitamin A 200 ug 200 ug 150 ug
Vitamin C 20 mg 20 mg 20 mg
Vitamin B12 0.5 ug 0.5 ug 0.5 ug
Vitamin B2 0.5 ug 0.5 ug 0.5 ug
*MN products was determined by considering the level of MN deficiency among young children in India, the Indian RDA for each MN by age, and data from efficacy trials on the dose of MN required for changes in cognition.

Play and Communication Intervention
• Infant Phase (Educational Flip Charts)– Trial informed by:
• Care for Development (WHO, 2001)• Pakistan Early Development Study (Yousafzai, 2010)
• Preschool Phase– No educational intervention– Rating of AWCs using Early Childhood Environmental
Rating Scale, Modified (ECERS)
Data collection completed and data analyses ongoing

CARE - A HAPPY LEARNING OPPORTUNITY
THANK YOU

Recommended