![Page 1: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/1.jpg)
A History of [Un]Vaccinated Diseases
Brian Altonen MS MPH
1/27/2015
![Page 2: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/2.jpg)
A Reminder to Us about the History of Diseases, before
there was Immunization
diseases covered . . .
Poliomyelitis, Measles, Chicken Pox, Small Pox, Mumps, Scarlet Fever, Diphtheria
![Page 3: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/3.jpg)
Sources and References•Many of the black and white images in this presentation come from my Second edition copy of Franklin H. Top’s Communicable Diseases, 1947.
• Images and materials obtained from other resources are so noted on the page and/or beneath the picture.
![Page 4: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/4.jpg)
Franklin Henry Top (1903 - )Portrait source: ihm.nlm.nih.gov
For Biog: http://medicine.yale.edu/publications/Images/[email protected]
![Page 5: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/5.jpg)
Polio is by far the most devastating infectious disease to have and then survive. Unlike Small Pox, which kills or leaves a scarred survivor capable of performing daily functions . . .
Polio may leave it survivors debilitated or disabled.
Major limbs experience loss of motor function and often a paralytic like state occurs from mid-body down.
<< Polio victim in Bangladesh www.demotix.com
![Page 6: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/6.jpg)
More examples
of polio’s impact,
from recent Web News pages
![Page 7: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/7.jpg)
One of the major deterrents to allowing a child to have a disease during the 1960s was the fear of what other illnesses or debilitating conditions could be suffered by that child due to this experience.
With polio, for example, we sat and watched as kids went through this and demonstrated its impact on their activities. The same could be true for the whooping cough, mumps, measles, rabies, tetanus, flu and pneumonia, depending on how bad the case was.
All of us knew a family that had a bad outcome from their child becoming ill—such as deafness, the inability to attend a parochial school, the need for a wheel chair, regular PT, a reduced physical education class performance.
![Page 8: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/8.jpg)
PoliomyelitisThe experience of Polio during the early 1950s
From the AMA Popular medical magazine: Hygieae
![Page 9: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/9.jpg)
Poliomyelitis can result in muscular atrophy in a small percentage of its victims. As many as 75% may recover from whatever paralysis it produces.
A common treatment for these patients was to improve quality of life through “muscle re-education”, in which a physical therapist or nurse encourages and assists the patient in making the appendages move.
Hygieia (AMA)
The “hamstring” muscle is being re-educated in this patient
![Page 10: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/10.jpg)
Muscle re-education was performed over much of the body, but we tended to focus on postural muscles and muscles used to move about with an ambulatory device. The nurse or PT in this case is stretching the back muscles of a patient, tightened due to lack of use.
Hygieia (AMA)
![Page 11: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/11.jpg)
Exercise had to be a part of the daily plan
for recovery as part of every
muscle re-education
process.Hygieia (AMA)
![Page 12: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/12.jpg)
Sternocleido-mastoid muscle
re-education.
Tendon stimulation by
the use of hands and pressure points over
tendons was thought to assist in this process. Hygieia (AMA)
![Page 13: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/13.jpg)
Stretching and movement
therapymay be
performed to prevent the
tightening and reduced mobility
of joints, ligaments and
tendons. Hygieia (AMA)
![Page 14: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/14.jpg)
“Full Packs” were used to treat Poliomyelitis bed-ridden patients.
http://www.minnpost.com/mnopedia/2012/11/sister-kenny-institute-revolutionized-treatment-polio-patients
Sister Kenny Institute revolutionized treatment of polio patientsBy R.L. Cartwright | 11/27/12
Sister Elizabeth Kenny, ca. 1911, Australia
The Sister Kenny Institute revolutionized the
treatment of paralyzed children with polio by
adding hot packs to their regimens, with the goal of
calm and soothing paralyzed muscles.
Hygieia (AMA)
(An offshoot of an early 1800s water cure practice)
Australiandoctor.com.au
![Page 15: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/15.jpg)
Intercostal Paralysis due to
Poliomyelitis is the reason many polio
victims required respiratory assistance.
This use of an artificial respirator
to assist in breathing was
mostly employed in the 1940s and
1950s.
Relate this to the following two Public Health questions . . .
What would the cost for such a device be
today?
Could we afford it for dozens or hundreds
of new cases? Hygieia (AMA), c. 1952
![Page 16: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/16.jpg)
Its common name:
“IRON LUNG”
Negative pressure regulator.
A Barometric Chamber used
to assist in respiration.
Hygieia (AMA), 1948
The Iron Lung was first called “Drinker Respirator”, invented 1928, by Philip A Drinker
Portrait is from: http://www.polioplace.org/people/philip-drinker-phd
![Page 17: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/17.jpg)
June 1948Hygieia
Magazine(AMA)
Treatingthe
patient as a person
in a typical 1948
“Polio Center”
![Page 18: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/18.jpg)
![Page 19: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/19.jpg)
![Page 20: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/20.jpg)
![Page 21: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/21.jpg)
![Page 22: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/22.jpg)
![Page 23: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/23.jpg)
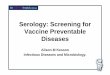
This distribution map for vaccine refusals based upon V-codes depicts a high
likelihood for the consequences
of these vaccine refusal behaviors now developing, with a clear peak
noted in the Pacific
Northwest.
![Page 24: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/24.jpg)
http://www.measlesrubellainitiative.org/tag/japan/
Measles
![Page 25: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/25.jpg)
Upon first glance, a disease like the measles appears mildly obtrusive, and not overly aggressive. So you decide to just lock the kid away in his or her room, in order to prevent others from making contact.
This is exactly what my parents did when I caught the measles in the early 1960s. (FYI: that is not me in this picture)
Then, my physician “Dr. D” came to our house, making “quarantine” less a problem back then than the same practice can be today.
Today, with both parents working and the need for a patient to be seen by his/her physician in the office setting, we set the stage for clusters of more cases to develop.
![Page 26: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/26.jpg)
Which leads me to ask . . . if you were a parent sitting in the waiting room, and saw the child in this photo sitting across the room, what medical condition would you suspect he has?
How might we distinguish Measles from Hives? Or even Poison Ivy? Or an allergic reaction to soap or detergent? Or a photosensitivity to the last medication he was prescribed, or some over the counter product?
Would you consider this a risk to your own health? The health of your child (children?
![Page 27: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/27.jpg)
Based on simple clinical observations, Measles, Chicken Pox or bothcould be infecting this patient. In fact, according to the source of this photograph (Top, 1947), both were infecting this child.
![Page 28: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/28.jpg)
Chicken Pox
http://www.today.com/health/angelina-jolie-has-chickenpox-its-no-joke-1D80370180http://www.dailymail.co.uk/tvshowbiz/article-2872257/Angelina-Jolie-reveals-s-got-chicken-pox-won-t-able-attend-Unbroken-premiere.html?ito=social-facebook
https://www.facebook.com/DailyMail/posts/836142159778867
Thirty-nine year old Angelina Jolie came down with Chicken Pox in early December, 2014.
![Page 29: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/29.jpg)
Chicken Pox cases are found across
the U.S. It is generally
perceived as a safe and natural
alternative to the recommended immunization
process.
![Page 30: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/30.jpg)
The early sign of Chicken Pox is very “plain”,
and non-extraordinary.
“Tear Drop” vesicles form.
![Page 31: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/31.jpg)
Chicken Pox, Day 2,
around a Small Pox
Vaccination Scar
On the second day we see more
vesicles and more of a reaction ensuing,
as well as new signs and
symptoms.
![Page 32: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/32.jpg)
And like any “Natural Disease Process”, Chicken Pox does have its
complications . . .
![Page 33: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/33.jpg)
A “normal”, but several looking Generalized, Polymorphic Eruption
![Page 34: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/34.jpg)
Chicken Pox with bullous impetigo
Chicken pox with facial cellulitis, and a secondary lesions formed in
front of the ear.
![Page 35: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/35.jpg)
and worse . . . .
![Page 36: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/36.jpg)
Small Pox
![Page 37: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/37.jpg)
A few days into a Small Pox infection, pustules begin merging together on adjacent parts of the body, forming a large crusty material that with time sloughs off. Pustules tend to aggregate the most on the face, head and appendages.
![Page 38: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/38.jpg)
https://dittrickmuseumblog.files.wordpress.com/2014/06/image_3.jpg
Small Pox, at its worst
![Page 39: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/39.jpg)
“Polysquamous secondary lesions” . . .
![Page 40: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/40.jpg)
Treating Small Pox
FromInoculations to Vaccines
![Page 41: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/41.jpg)
timelines.tv
From Benjamin Jesty, of Yetminster in Dorset, England, who inoculated his family with cowpox in 1774
Inoculation . . .
![Page 42: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/42.jpg)
Before vaccinations, there were inoculations.
For inoculations, you took some material from the diseased part and exposed a previously uninfected person to it. The disease would then erupt. Sometimes a full fledged disease. Sometimes a simpler version of it. The goal of course was the latter.
Inoculations were part of the Revolutionary War soldier’s experience, and were required of nearly all troops starting in 1777 (in 1776, they were still uncertain).
As a result of infection, an inoculation forms and then naturally reduces, leaving the patient with a scar as evidence of the experience. In the Hudson valley of New York, inoculation was practiced up until about April 1803.
Source: Poughkeepsie Journal, Microfilm at Adriance Library, Poughkeepsie, NYThe replacement of inoculation with vaccines.
![Page 43: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/43.jpg)
www.historyofvaccines.org
“Courtesy Wellcome Library, London.Francisco Javier de Balmis shows smallpox vaccination scars.”
. . . versus Vaccination
Map of de Balmis’s trips
![Page 44: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/44.jpg)
The cowpox or kine pox was brought to the U.S. by Benjamin Waterhouse, of Harvard University, 1802.
Due to proximity, its first promoters in 1802/3, included a Quaker doctor and close friend of the Shakers residing in the Hudson Valley, and some New York and Philadelphia Medical School physicians.
See The Vaccination Inquirer and Health Review, Vol. 3 at https://books.google.com/books?id=xgUDAAAAYAAJ
Benjamin Waterhouse
![Page 45: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/45.jpg)
Small Pox reaction,
reduced by Vaccinationrather than Inoculation.
[F.H. Top, 1947]
![Page 46: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/46.jpg)
Vaccine Scar Fresh Vaccine
Telltale Signs
of your
history
![Page 47: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/47.jpg)
MUMPS
Pittsburgh Penguins Captain Sidney CrosbyDecember 12, 2014
Kevin Allen and Nancy Armour, USA TODAY Sports. “ NHL mumps outbreak rare, but 'could happen anywhere‘ ”
Dec. 17, 2014.
Accessed at http://www.usatoday.com/story/sports/nhl/2014/12/17/nhl-mumps-outbreak-could-happen-anywhere/20562733/
![Page 48: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/48.jpg)
The Mumps is produced by a viral infection of the parotid (salivary) gland.
http://www.immunize.org/photos/mumps-photos.asp FH Top, 1947
![Page 49: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/49.jpg)
Those who had the mumps in the 1960s may remember this question from your family doctor:
‘Do you remember what side it was on?’*
It can spread from one side to the next, making it last for several weeks.
The mumps virus can enter the body and then impact kidneys, sexual organs, thyroid gland and pancreas. Cases infecting the nervous system can led to meningitis.
*I am not sure if the answer here really made much of a difference, like could it return if it infected just one side?
![Page 50: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/50.jpg)
Long Term Side Effects of the Mumps
•Deafness
•Meningoencephalitis and complications•Seizures•Paralysis•Hydrocephaly . . .
http://www.cdc.gov/mumps/clinical/qa-disease.htmlhttp://www.livestrong.com/article/40876-longterm-side-effects-mumps/
![Page 51: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/51.jpg)
SCARLET FEVER
wiki wiki
Streptococcus pyogenes
![Page 52: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/52.jpg)
www.healthofchildren.com
http://www.tamworthinformed.co.uk/scarlet-fever-on-the-rise-in-midlands/
A Scarlet Fever patient’s presentation –Chief Signs and Symptoms
![Page 53: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/53.jpg)
Stages for the “Strawberry Tongue” of Scarlet Fever
(Strep A)
![Page 54: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/54.jpg)
The Ophthalmic Emergency: Orbital Abscess in Scarlet Fever
For more: http://www.patient.co.uk/doctor/orbital-and-preseptal-cellulitis
• Can lead to severe long term complications.
• Offers the streptococcus pathogen a more direct connection to the nervous system.
![Page 55: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/55.jpg)
Complication 2
Nephritis (Kidney inflammation) with subsequent edema (kidney failure)
(also note swelling around the neck due to adenitis)
![Page 56: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/56.jpg)
NonsuppurativeArthritis,
with a swollen left hand and
wrist(right side is not
impacted, and appears
normal)
Complication 3
![Page 57: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/57.jpg)
The Consequences
of Acute
Mastoiditis and Nephritis,
associated with Scarlet Fever
Complication 4
![Page 58: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/58.jpg)
Ethmoiditis
This child experienced infection of the
ethmoid sinus cavity by the streptococcus also responsible for
the scarlet fever.
Complication 5
![Page 59: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/59.jpg)
Toxins produced by the organism can lead to renal failure and other organ system damage.
The continued growth of the organism throughout the body leads to the development of pustulence (pus), especially in the neck and tonsils area. This can be followed by abscessing.
Nearby tissues may then die and slough off, including blood vessels. This subsequent break down of blood vessels can result in severe hemorrhaging and untimely death.
![Page 60: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/60.jpg)
This case demonstrates the results of the Schultz-Charlton Phenomenon or Blanching Test for diagnosis and treatment (note arrows on the belly). This result is produced by the application of an antitoxin for the Streptococcal pathogen on the skin.
See https://books.google.com/books?id=CQIWAQAAIAAJ&pg=RA1-PA15https://books.google.com/books?id=b7rtAAAAMAAJ&pg=PA62
Pityriasis rosea of the skin
![Page 61: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/61.jpg)
Septic Scarlet Fever, with severe thrombosis and gangrenous nose
The streptococci responsible for Scarlet Fever may develop into a hemolytic form, which is assessed clinically by placing a tight (but not perfect) tourniquet on an appendage if it displays a significant scarlatina rash. This results in the formation of petechiae in just 10-20 minutes.
![Page 62: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/62.jpg)
Also linked to the onset of a gangrenous state in Scarlet Fever patients:
Swelling of the Eyelids
Discharge of the Nose
Forchheimer Spots (red dots) on the soft palate
and tongue (the “strawberry tongue”)
See:http://www.cdc.gov/features/scarletfever/
![Page 63: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/63.jpg)
DIPHTHERIA
1930s, Ohio http://flickrhivemind.net/Tags/diphtheria/Interesting
Pierre Bretonneau (1778-1862), coined the name diphtérite for this disease
![Page 64: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/64.jpg)
In 1735, a major Diphtheria Epidemic spread across the Colonies in North America. This was one of the first epidemics to have corroborative evidence for the same event shared by several colonies.
![Page 65: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/65.jpg)
http://dittrickmuseumblog.com/category/online-exhibits/
Examples of the Presentation of “Distemper”/Diphtheria to a Physician
![Page 66: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/66.jpg)
More Modern Illustrations
![Page 67: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/67.jpg)
This is the Pseudomembrane
or “False Membrane”, that is visible in the Throat of a
diphtheria patient. This sample is a near perfect
casting of the inner surface of the respiratory passages. It consists of waste material,
dead cells and debris left over by organisms growing within
the air passage.
![Page 68: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/68.jpg)
An Important Diphtheria Lesson: Animals were/are very important to the development of vaccines.
Edward Jennings documented the value of kine poxvaccine as a preventive agent, due to the exposure ladies had while they were milking cows.
Whereas cows were the primary source for producing large amounts of vaccine for the pox, horses were preferred for diphtheria.
In 1811, Isaac I. Van Voorhis of Fishkill, NY, studied the use of horses to develop a better understanding of vaccines. He used much the same technique as Edward Jennings. After receiving his MD in 1812, he removed to Fort Dearborn, Chicago, where he served as a Surgeon. (He died in the Chicago Massacre one year later; and so, this story got lost.)http://history.amedd.army.mil/booksdocs/rev/gillett1/ch8.htmlhttp://wp.me/Puh6r-6u0
A f
org
ott
en p
iece
of
Am
eric
an M
ed
ical
his
tory
!!!
![Page 69: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/69.jpg)
Horses were the primary means for producing Diphtheria vaccines throughout the late 1800s.
Aside from Horses, Sheep were tried for the same purpose, and a few small businesses even tried producing vaccines using this method.
When vaccines were required of kids by law by the mid-19th century, this technique of manufacturing was essential for pharmaceutical industries to meet the growing demand.
In 1876, New York City became the first public health agency to establish a “Vaccine Farm” using cattle raised in Lakeview, New Jersey.
These vaccines required the lymph of a living animal and an antitoxin to lessen the reaction patients had to the vaccine itself. A specific ratio of the two was required for all products, and became the standard for defining potency and efficacy of a vaccine.
Whereas Cattle were the staple for producing pox vaccines, horses were
required to produce diphtheria vaccines.
![Page 70: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/70.jpg)
Diphtheria, Croup, and PertussisIn contrast with Diphtheria, kids can also catch the Croup and Whooping Cough.
Bacterial croup in its worst form mimicked the diphtheria. Caused by Staphylococcus aureus, Streptococcus pneumoniae, Hemophilus influenzae, and Moraxella catarrhalis, it could produce symptoms ranging from laryngeal diphtheria, to bacterial tracheitis, to laryngotracheobronchitis, and to laryngotracheobronchopneumonitis.
Depicted here is a very early example of a vaporizer used to treat these cases (later made famous by Vick’s). Many early attempts to use this method for treating diphtheria were to no avail.
![Page 71: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/71.jpg)
Whereas Croup and Whooping Cough did not completely close off air passages, diphtheria did. The laryngotomy process was used to treat countless diphtheria victims up until about 1885, when an intubation process was developed.
For the 1874 argument on this, in the Richmond and Lousiville Medical Jl, , go to: https://books.google.com/books?id=bXYCAAAAYAAJ&pg=PA354 From: medical-dictionary.thefreedictionary.com
Emergency Laryngotomy
![Page 72: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/72.jpg)
In 1885, Joseph P. O'Dwyerinvented an intubation process that could be used to treat the obstruction of the larynx for a diphtheria patient.
By the early 1900s, this process, demonstrated in this photo, became an essential part of treating diphtheria patients to increase their survival rates.
A “Life-saver”: From Tracheotomy to Intubation
![Page 73: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/73.jpg)
Other Lessons from the Past
Rotary International. . . on Pinterest
Brian Altonen . . . on Pinterest
National Institutes of Health
![Page 74: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/74.jpg)
Lesson 1
Why immunize?
![Page 75: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/75.jpg)
Lesson 2: What about Quarantine?• A public health, professional, and personal responsibility• Can people abide by this Public Health concept today? [recall recent Ebola incidents]
![Page 76: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/76.jpg)
Cattle for Pox, 1880s-early 1900s (no longer practiced)
The entire body was shaved and sterilized. The skin was infected.
The pustules that formed had their lymph collected.
Animal aights activists currently are against the use of animals for
producing or testing medications and cosmetics. Ca. 1900
Pharmacognosy course text, Columbia University
Lesson 3: Respect our past . . . be grateful for new technology.
![Page 77: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/77.jpg)
Lesson 4: Horses for Diphtheria
1898
![Page 78: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/78.jpg)
Lesson 5: Once upon a time . . . Lymph + Antitoxin = Vaccine
This original Antitoxin-Lymph approach is of course no longer used
![Page 79: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/79.jpg)
Lesson 6: The “Old” and “New” in vaccines, 19th to early 20th century
![Page 80: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/80.jpg)
19th C20th C
21st C
Signs of change!
![Page 81: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/81.jpg)
Recent History - Present Status
![Page 82: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/82.jpg)
(On this poster are the years we initiated vaccines for . . . . )
Here is What we’ve Accomplished . . .
“the Vaccine Years”
The 1960s was a transitional period in the U.S. immunization program.
Much momentum was developed following the successful development of an oral polio vaccine, and according to this poster, the rapidly decreasing measles epidemic problem for the 1960s and early 1970s.
![Page 83: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/83.jpg)
During the 1960s:Sabin’s Oral Poliovaccine was developedWe saw reductions in the number of Polio children Rubella pathogen was isolatedDTaP and MMR combos were being developedMeasles was the focus
Here is what has
happened:
![Page 84: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/84.jpg)
Will we go back to: • the 90s • the 80s • the 70s • the 60s • Or earlier?
![Page 85: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/85.jpg)
These recent
outbreaks,from
2012-15, are like
going back in time . . .
![Page 86: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/86.jpg)
May 31, 1803 Poughkeepsie JournalSmall Pox Eradication
began about 1800(some argue
earlier)
It finally became
a Success in1980
Vaccine manufacturing ceased 1990
![Page 87: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/87.jpg)
1984 & 2012 Hudson Valley, NY 2014
In recent years we’ve regressed, back to the 80’s perhaps.
Example
![Page 88: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/88.jpg)
www.cdc.gov
http://www.cdc.gov/measles/cases-outbreaks.html
Most of the 2014 cases are
linked to the
Disneyland outbreak in California
The most recent
Measles outbreak confirms
this.
![Page 89: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/89.jpg)
Signs of reverting back to . . .
• The 80s – Measles outbreaks, Mumps and Whooping Cough; numbers and events increase. [Current status? as of 1/2015]
• The 70s -- 2 or 3 of Measles, Whooping Cough, Mumps, with trace numbers of Rubella/Scarlet Fever, a Diphtheria “spike”.• Partial decreases (10%-25%) in DTaP and MMR combinations
• The 60s – 3 of 4 of Measles, Whooping Cough, Mumps, Tetanus, Hib, with spikes for Scarlet Fever/Diphtheria• Major decreases, esp. for DTaP and MMR combinations
• The 50s -- Measles, Whooping Cough, Mumps, and Tetanus; Scarlet Fever, Diphtheria, Hib; Polio especially a concern.
• The 40s – Scarlet Fever and Diphtheria are the indicators of severity; Polio is a major concern, if not already present.
theatlantic.com
www.huffingtonpost.com
healthymamas.com
National Institutes for Health
![Page 90: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/90.jpg)
Vaccinate? The Sooner, the Better (but remain on schedule)
• The “Too Many Vaccines for my child” argument can be
eliminated through the use of new technology.
• But “Too many vaccines” is not the only excuse mothers use for not vaccinating their children.
• Today’s parents have no memories of experiencing measles or having a neighbor who child was disabled or deceased due to experiencing a disease “the way nature planned it.”
• This argument for avoiding vaccinations is based mostly on personal philosophy. Who wouldn’t regret learning he/she did not grow up to their fullest life potential due to vaccine their parents “missed” or ignored?
• Vaccines improve quality of life, and in the long run greatly reduce the cost for care we will need as we grow older.
![Page 91: A History of [Un]Immunized Diseases](https://reader039.dokumen.tips/reader039/viewer/2022032421/55a75a391a28ab71458b4756/html5/page/91.jpg)
The End
Recommended