-
7/30/2019 Zygoma Implants
1/5
The use of zygomatic implants for the rehabilitation of
atrophic
maxillas with 2 different techniques: Stella and Extrasinus
Ernesto Barquero Cordero, MSD,a Cesar A. Magalhes Benfatti,
PhD,b
Marco A. Bianchini, PhD,c
Leonardo Vieira Bez, MSD,d
Kyle Stanley, DDS,e
andRicardo de Souza Magini, PhD,f Santa Catarina,
BrazilUNIVERSITY FEDERAL OF SANTA CATARINA
The zygomatic implant anchorage is a surgical technique that
provides a new perspective for patients withsevere maxillary
atrophy, increasing predictability and reduced cost of treatment,
besides being a tool for the hardshipsof the rehabilitation of such
a challenging region. This article describes 2 clinical cases with
zygomatic implants withdifferent techniques (Stella and Extrasinus)
and both with immediate loading and accompanying clinical
radiographicfollow-up procedures of 12 and 24 months, respectively.
(Oral Surg Oral Med Oral Pathol Oral Radiol Endod
2011;112:e49-e53)
The rehabilitation of patients with severely atrophiedmaxillas
presents a major challenge owing to the com-
plexity of its implementation. The problem presents itself
because of the lack of height and width of the alveolar
ridge, this being a result of insufficient bone,
extractions,
trauma, infection, or maxillary sinus pneumatization.1-3
Several surgical techniques have been developed to
successfully increase the volume of bone: iliac crest
graft, Le Fort I, guided bone regeneration, sinus lifting,
and combinations of these procedures.4-9 These treat-
ments also reduce patient comfort, increase morbidity,
require several surgeries, and require the use of remov-
able prostheses for a long period of time.10,11
Implants placed in grafted areas have various success
rates, with the literature suggesting a rate of 82% to 84%
with a clinical follow-up of 12 to 60 months.12
Aiming to simplify the treatment of these patients,
increasing the predictability of outcomes and decreasing
morbidity, treatment time, and avoiding bone grafts,
Brnemark and his team13 in 1988 implemented the an-choring
technique known as zygomatic implants (ZI) in
some research centers.Initially this technique was designed to
treat victims of
trauma, tumor resection, or congenital defects. These pa-tients
present with a considerable loss of bone structure14
and few regions offering anchorage for the implants.These
regions consisted of the body of the zygoma or the
frontal portion of the zygomatic bone15 presenting a
greatalternative. With time, the technique has been refined,
allowing patients with severe bone resorption to be re-stored
predictably to proper function and esthetics and
with a success rate similar to implants placed using
theconventional technique.16
There are different techniques for fixation of
zygomaticimplants. The technique developed by Brnemark17 calls
for a Le Fort I incision, allowing the displacement of alarge
flap to facilitate exposure of the zygomatic bone, and
the realization of a window for the displacement of thesinus
membrane. The technique of Stella and Warner18
differs from the original technique, as there is no need fora
window opening on the wall of the maxillary sinus, only
1 channel orientation, and there is no concern for theintegrity
of the sinus membrane. The third technique19 has
no need for a window opening or a channel in the wall ofthe
maxillary sinus because of the externalization of the
zygomatic implants in relation to sinus. This article re-ports 2
clinical cases that were rehabilitated with different
fixation techniques, with a radiographic follow-up of 24and 48
months, respectively.
CASE DESCRIPTION
Case 1A 65-year-old female patient at the Center for
Teaching
and Research in Dental Implants (CEPID) at the Federal
University of Santa Catarina (UFSC) presented to perform an
aPhD program in Implantology, University Federal of Santa
Catarina,
Santa Catarina, Brazil.bAssociate Professor of Implantology,
University Federal of Santa
Catarina, Santa Catarina, Brazil.cProfessor of the Phd and
Masters Degree Program of Implantology,University Federal of Santa
Catarina, Santa Catarina, Brazil.dResident of Implantology Program,
University Federal of Santa
Catarina, Santa Catarina, Brazil.eResident of Implantology
Program, University Federal of Santa
Catarina, Santa Catarina, Brazil.fChairman and Professor of PhD
and Masters Degree Program of
Implantology, University Federal of Santa Catarina, Santa
Catarina,
Brazil.
Received for publication Apr 28, 2011; accepted for publication
May
15, 2011.
1079-2104/$ - see front matter
2011 Mosby, Inc. All rights reserved.
doi:10.1016/j.tripleo.2011.05.008
e49
-
7/30/2019 Zygoma Implants
2/5
implant reconstruction. Examining the panoramic radiograph
revealed bone loss around the upper and lower teeth,
observed
clinically. With the impossibility of keeping these teeth,
treat-ment options were introduced in the upper arch that would
use 4 implants, 2 anchored in the zygomatic bone and 2 in
the
anterior region. The lower jaw had a treatment plan to place
4 implants. Both treatments had the possibility of immediate
loading.
The procedure was performed under general anesthesia
and was initiated by tooth extractions and smoothing maxil-
lary and mandibular alveolar ridges. Once the tissue was
reflected and the body of the zygoma was located, drilling
was initiated. With a round bur, a channel or slot was com-
pleted to define the orientation of the trajectory of the
drills.
Then, the following sequence was used: 2.9-mm drill bit,
2.9-mm twist drill, 3.5-mm pilot drill, and 3.5-mm twist
drill,always aiming the position of the platform of the implant
to
lie as close as possible to the crest of the ridge. The next
step
was the installation of the zygomatic implants, 4.1 diameter
52.0 mm in the posterior left ridge and 4.1 diameter 45.0 mm
in the right posterior border. Two implants measuring 4.1
13.0 mm were placed in the anterior. We used the posterior
multiunit abutments on 17 (right side) and 30 (left side),
both with a height of 4 mm, in order to have the emergence
profile located in the molar region. Because the torque was
greater than 40 Ncm for the implants in both arches, an
imme-
diate loading protocol was initiated, tissue was sutured,
and
acrylic resin (Duralay, Reliance) was used to secure the
abut-
ment transfers in both arches and an impression for
manufactur-
ing the prostheses was completed. After 48 hours, the
prostheses
were installed, restoring function and esthetics for the
patient.Panoramic radiographs were performed at 12 and 24 months
for
the control treatment (Fig. 1, A-G).
Clinical case 2A 68-year-old male patient presented to the CEPID
at
UFSC for rehabilitation of the upper jaw. On clinical exam-
ination there was a fixed prosthesis supported by implants
in
the lower jaw and upper jaw with a thin ridge. It was sug-
gested that the patient have implants anchored in the zygo-
matic bone owing to the desire not to undergo a complex
reconstruction with extraoral donor sites. The procedure
started in the hospital with a LeFort type I incision, using
the
ZI externalized technique. After the flap was reflected,
thesequence of drilling included 2.9-mm pilot drill, 2.9-mm
twist
drill, 3.5-mm pilot drill, and 3.5-mm twist drill. After the
placement of the implant platform directly over the ridge,
the
installation of four zygomatic implants was completed, two
on the left side: 4.1 diameter 48 mm and 4.1 diameter 45
mm; on the right side 4.1 diameter 45 mm, 4.1 diameter
48 mm. We used a microunit-type abutment 17 with a height
of 4 mm, so as to have the emergence profile located in the
molar region. Because the torque was greater than 40 Ncm for
the implants in both arches, an immediate loading protocol
was initiated, tissue was sutured, and acrylic resin
(Duralay,
Reliance) was used to secure the abutment transfers in both
Fig. 1. Patient 1. A, Intraoral photograph. B, Initial
radiograph. C, A channel or slot was completed to define the
orientation of
the trajectory of the drills. D, Zygomatic and conventional
implants installed. E, Postoperative radiograph. F, Clinical
photograph
showing the final prosthetic result. G, Radiographic follow-up
at 24 months.
OOOOE
e50 Baquero et al. December 2011
-
7/30/2019 Zygoma Implants
3/5
arches and an impression for manufacturing the prosthesis
was completed. After 48 hours, the prosthesis was installed,
reestablishing the function and esthetics for the patient.
Pan-
oramic radiographs were performed at 24 and 48 months for
the control treatment (Fig. 2, A-H).
DISCUSSIONAfter extractions, the process of bone remodeling
in
the jaw suffers, causing inadequate dimensions for im-
plant placement. This atrophy is physiological and oc-curs in a
chronic and irreversible fashion.6 The lack of
internal pressure along with posterior tooth extractionleads to
bone resorption of the edentulous alveolar
ridge, making the retention of functional prosthesesdifficult
and can lead patients to a disabled state in their
mouth with a decreased quality of life.20,21
Patients with major destruction of the premaxilla,maxillary
sinus pneumatization, or defects owing totumor resection have
limitations on treatment with oral
implants. Maxillary bone atrophy is classified by sev-eral
authors19,20,21 as a major challenge, with a high
difficulty of rehabilitating a severely resorbed
maxilla,indicating a major reconstruction with autogenous bone
grafts using extraoral donor sites,22 subsequent to theplacement
of implants or anchoring techniques, without
bone reconstruction.The reconstruction techniques involve an
increase in
the jawbone structure, aiming at the application of
conventional fixation in places where there is sufficient
alveolar height and thickness, providing the use of
implants in a much better position and, consequently,
better biomechanic distribution. The reconstructionscan be made
on the alveolar ridge (onlay) or within
cavities, particularly the sinus (inlay).22 The grafts have
inevitably some element of risk, because they demand
good surgical technique, good quality of recipient bone,
soft tissue overlying the graft, great cooperation from
the patient, and general health of the patient that en-
courages healing.23 The literature shows a variability in
the survival percentage of the different techniques of
bone grafting being 80% to 95%,24-26 with a follow-up
time of 12 to 124 months. It also reports that the
success rate of implants in bone grafts is 74% to
87%.27-29
Initially, the ZI was designed to treat patients suffer-
ing from trauma or surgically resected tumors, where
there is great loss of jaw structures.11,23,30 Subse-
quently, the technique was applied to patients with
severe maxillary atrophy to simplify the treatment and
avoid a reconstruction.31 There are different techniques
for fixation of zygomatic implants, including the orig-
inal technique by Brnemark, which recommends
opening a window on the wall of the maxillary sinus as
well as maintaining the integrity of the sinus mem-
brane. The first case used a protocol originally pro-
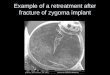
Fig. 2. Patient 2. A, Intraoral photograph. B, Initial
radiograph. C, Extrasinus zygomatic implant. D, Four zygomatic
implants.
E, Clinical photograph. F, Postoperative radiograph. G, Final
result (a, intraoral; b, extraoral). H, Radiographic follow-up at
48
months.
OOOOE
Volume 112, Number 6 Baquero et al. e51
-
7/30/2019 Zygoma Implants
4/5
posed by the Stella technique with the use of a channel
or slot through which the implant installation is guidedinto the
sinus, eliminating the bony window and the
sinus lifting, having a larger implantbone interfacewith a
vertical orientation and better emergence place-
ment of the implant closest to the crest of the alveolar
ridge. In the second case study, the extrasinus zygo-matic
implant technique traces an imaginary line fromthe insertion point
on the ridge to the point of attach-
ment to the body of the zygoma and the implant can becompletely
or partially outside the sinus cavity. The
choice of technique is determined by the patients boneanatomy as
well as technical skill of the clinician.
The zygomatic implant requires care in relation tothe
biomechanical forces of curvature, whose forces
may impair the long-term stability of an implant-sup-ported
restoration and, because of this, there must be
stiff prosthetic work, because flexing of the materials
used can cause deformation and deviation resulting inloss of
fixation of the implants or loosening of the
junction between the prosthesis and fixation.32
The use of immediate loading with the 1 or 2 ZI on
each side is justified by some authors because theybelieve that
the quality of the zygomatic bone, the rigid
stabilization and polygons created in the technique,coupled with
the benefits provided to the patient (less
time, less cost, and possibility of social life) allows
thisprocedure to be used.33,34 The use of prototypes seems
to be an interesting tool in the planning of this tech-nique,
but high cost still hampers its use.35 An impor-
tant question is what could cause the presence of zy-gomatic
implants inside the maxillary sinus. A study by
Nakai et al.36 in 2003 reported using computed tomog-raphy
scans, performed 6 months after the installation
of 15 zygomatic implants, in 9 patients and showed nosigns of
sinusitis. Petruson, in 2004,37 evaluated the
zygomatic implants in the maxillary sinus through asinuscopy in
14 patients, finding no infection or inflam-
mation in the mucosa around the implants.The success rates of
implants in the zygomatic bone
vary from 95% to 97% with 12 to 124 months offollow-up
observation,16,19,23,36-42 and a patient satis-
faction rate of 80% after 1 year of installation of
theprosthesis.43
CONCLUSIONSClinically, the technique of zygomatic implants is
an
excellent therapeutic modality for patients with atro-phic
maxillas wishing to avoid a bone graft and there-
fore increasing predictability and reducing costs andmorbidity
of treatment. The most important point in
this procedure is the clinical mastery of the techniquesfor this
surgical approach, determining the success of
the treatment.
REFERENCES1. Adell R, Eriksson B, Lekholm U, Brnemark PI, Jemt
T. Long-
term follow-up study of osseointegrated implants in the
treatment
of totally edentulous jaws. Int J Oral Maxillofac Implants
1990;5:347-59.
2. Tolman DE, Laney WR. Tissue-integrated prosthesis
complica-
tions. Int J Oral Maxillofac Implants 1992;7:477-84.
3. Jemt T, Lekholm U. Implant treatment in edentulous maxillae:
a5-year follow-up report on patients with different degrees of
jaw
resorption. Int J Oral Maxillofac Implants 1995;10:303-11.
4. Esposito M, Hirsch JM, Lekholm U, Thomsen P. Biological
factors contributing to failures of osseointegrated oral
implants.
Series I. Success criteria and epidemiology. Eur J Oral Sci
1998;
106:527-51.
5. Breine U, Brnemark PI. Reconstruction of alveolar jaw
bone.
An experimental and clinical study of immediate and
preformed
autologous bone grafts in combination with osseointegrated
im-
plants. Scand J Plast Reconstr Surg 1980;14:23-48.
6. Isaksson S, Ekfeldt A, Alberius P, Blomqvist JE. Early
results
from reconstruction of severely atrophic (class VI) maxillas
by
immediate endosseous implants in conjunction with bone
graft-
ing and Le Fort I osteotomy. J Oral Maxillofac Surg 1993;
22:144-8.
7. Adell R, Lekholm U, Grndahl K, Brnemark PI, Lindstrom L,
Jacobsson M. Reconstruction of severely resorbed edentulous
maxillae using osseointegrated fixtures in immediate
autogenous
bone grafts. Int J Oral Maxillofac Implants 1990;5:233-46.
8. Isaksson S, Alberius P. Maxillary alveolar ridge
augmentation
with onlay bone-grafts and immediate endosseous implants. J
Craniomaxillofac Surg 1992;20:2-7.
9. Boyne PJ, James RA. Grafting of the maxillary sinus floor
with
autogenous marrow and bone. J Oral Surg 1980;38:613-6.
10. Wood RM, Moore DL. Grafting of the maxillary sinus with
intraorally harvested autogenous bone prior to implant
place-
ment. Int J Oral Maxillofac Implants 1988;3:209-14.
11. Bedrossian E, Stumpel L, Beckely ML, Indresano T. The
zygo-
matic implant: preliminary data on treatment of severely
re-sorbed maxillae. A clinical report. Int J Oral Maxillofac
Implants
2002;17:861-5.
12. Sjrtrom M, Sennerby L, Nilson H, Lundgren S.
Reconstruction
of the atrophic edentulous maxilla with free iliac crest grafts
and
implants: a 3-year report of a prospective clinical study.
Clin
Implant Dent Relat Res 2007;9:46-59.
13. Brnemark PI. Surgery and fixture installation zygomaticus
fix-
ture clinical procedures. 1st ed. Gotemburgo, Sweden: Nobel
Biocare; 1998.
14. Darle C. Minimized treatment for maximal predictability:
a
new procedure for rehabilitating the severely resorbed max-
illa. Talk of the times 4. 1st ed. Gteborg, Sweden: Nobel
Biocare; 1999. p. 5.
15. Balshi TJ, Wolfinger GJ. Treatment of congenital
ectodermal
dysplasia with zygomatic implants: a case report. Int J
OralMaxillofac Implants 2002;17:277-81.
16. Aparicio C, Ouazzani W, Hatano N. The use of zygomatic
implants for prosthetic rehabilitation of the severely
resorbed
maxilla. Periodontol 2000 2008;47:162-71.
17. Parel SM, Brnemark PI, Ohrnell LO, Svensson B. Remote
implant anchorage for the rehabilitation of maxillary defects.
J
Prosthet Dent 2001;86:377-81.
18. Stella JP, Warner MR. Sinus slot technique for
simplification and
improved orientation of zygomaticus dental implants: a
technical
note. Int J Oral Maxillofac Implants 2000;15:889-93.
19. Migliorana RM, Ilg JP, Serrano AS, Souza RP, Zamperlini
MS.
Exteriorizao de fixao zigomticas em relao Ao seio maxi-
lar: Uma nova abordagem cirrgica. Implant. News 2006;3:30-4.
OOOOE
e52 Baquero et al. December 2011
-
7/30/2019 Zygoma Implants
5/5
20. Reinert S, Knig S, Bremerich A, Eufinger H, Krimmel M.
Stability of bone grafting and placement of implants in the
severely atrophic maxilla. Br J Oral Maxillofac Surg 2003;
41:249-55.
21. Jensen OT, Brownd C, Blacker J. Nasofacial prostheses
sup-
ported by osseointegrated implants. Int J Oral Maxillofac
Im-
plants 1992;7:203-11.
22. Weischer T, Schettler D, Mohr C. Titanium implants in
thezygoma as retaining elements after hemimaxillectomy. Int J
Oral
Maxillofac Implants 1997;12:211-4.
23. Nystrm E, Ahlqvist J, Kahnberg KE, Rosenquist JB.
Autoge-
nous onlay bone grafts fixed with screw implants for the
treat-
ment of severely resorbed maxillae. Radiographic evaluation
of
preoperative bone dimension, postoperative bone loss, and
changes in soft-tissue profile. Int J Oral Maxillofac Surg
1996;25:351-9.
24. Sutton DN. Changes in facial form relative to progressive
atrophy of
the edentulous jaws. Int J Oral Maxillofac Surg
2004;17:676-82.
25. Lundgren S, Sjstrm M, Nystrm E, Sennerby L. Strategies
in
reconstruction of the atrophic maxilla with autegenous bone
grafts
and endosseous implants. Periodontol 2000 2008;17:143-61.
26. Johansson B, Wannfors K, Ekenbck J, Smedberg JI, Hirsch
J.Implants and sinus-inlay bone grafts in a 1-stage procedure
on
severely atrophied maxillae: surgical aspects of a 3-year
fol-
low-up study. Int J Oral Maxillofac Implants 1999;14:811-8.
27. Keller EE, Tolman DE, Eckert SE. Maxillary antral-nasal
inlay
autogenous bone graft reconstruction of compromised maxilla:
a
12-year retrospective study. Int J Oral Maxillofac Implants
1999;14:707-21.
28. Nystrm E, Ahlqvist J, Gunne J, Kahnberg KE. 10-year fol-
low-up of onlay bone grafts and implants in severely
resorbed
maxillae. Int J Oral Maxillofac Surg 2004;33:258-62.
29. Nystrm E, Kahnberg KE, Gunne J. Bone grafts and Brnemark
implants in the treatment of the severely resorbed maxilla:
a
2-year longitudinal study. Int J Oral Maxillofac Implants
1993;8:45-53.30. Nystrm E, Lundgren S, Gunne J, Nilson H.
Interpositional bone
grafting and Le Fort I osteotomy for reconstruction of the
atro-
phic edentulous maxilla. A two stage technique. Int J Oral
Maxillofac Surg 1997;26:423-7.
31. Nystrm E, Ahlqvist J, Legrell PE, Kahnberg KE. Bone
graft
remodelling and implant success rate in the treatment of the
severely resorbed maxilla: a 5-year longitudinal study. Int J
Oral
Maxillofac Surg 2002;31:158-64.
32. Van Steenberghe D, Naert I, Bossuyt M, De Mars G, Calberson
L,
Ghyselen J, et al. The rehabilitation of the severely resorbed
maxilla
by simultaneous placement of autogenous bone grafts and
implants:
a 10-year evaluation. Clin Oral Investig 1997;1:102-8.
33. Muela R, Arvalo X, Caro L, Codesal M, Fortes V, Franch M,
et
al. Immediate and early load on zygoma implants. Initial
results
of a 3-year prospective study. J Clin Periodontol
2006;33:125.
34. Becktor JP, Isaksson S, Abrahamsson P, Sennerby L.
Evaluation
of 31 zygomatic implants and 74 regular dental implants used
in
16 patients for prosthetic reconstruction of the atrophic
maxillawith cross-arch fixed bridges. Clin Implant Dent Relat
Res
2005;7:159-65.
35. Stoker NG, Mankovich NJ, Valentino D. Stereolithographic
models for surgical planning: preliminary report. J Oral
Maxil-
lofac Surg 1992;50:466-71.
36. Nakai H, Okazaki Y, Ueda M. Clinical application of
zygomatic
implants for rehabilitation of the severely resorbed maxilla:
a
clinical report. Int J Oral Maxillofac Implants
2003;18:566-70.
37. Petruson B. Sinuscopy in patients with titanium implants in
the
nose and sinuses. Scand J Plast Reconstr Surg Hand Surg
2004;38:86-93.
38. Landes CA. Zygoma implant-supported midfacial prosthetic
re-
habilitation: a 4-year follow-up study including assessment
of
quality of life. Clin Oral Implants Res 2005;16:313-25.
39. Pearrocha M, Garca B, Mart E, Boronat A. Rehabilitation
ofseverely atrophic maxillae with fixed implant-supported
prosthe-
ses using zygomatic implants placed using the sinus slot
tech-
nique: clinical report on a series of 21 patients. Int J
Oral
Maxillofac Implants 2007;22:645-50.
40. Malevez C, Abarca M, Durdu F, Daelemans P. Clinical
outcome
of 103 consecutive zygomatic implants: a 6-48 months
follow-up
study. Clin Oral Implants Res 2004;15:18-22.
41. Pi Urgell J, Revilla Gutirrez V, Gay Escoda C.
Rehabilitation of
atrophic maxilla: a review of 101 zygomatic implants. Med
Oral
Patol Oral Cir Bucal 2008;13:E363-70.
42. Schmidt BL, Pogrel MA, Young CW, Sharma A.
Reconstruction
of extensive maxillary defects using zygomaticus implants.
J Oral Maxillofac Surg 2004;62:82-9.
43. Pearrocha M, Carrillo C, Boronat A, Mart E. Level of
satis-faction in patients with maxillary full-arch fixed
prostheses:
zygomatic versus conventional implants. Int J Oral
Maxillofac
Implants 2007;22:769-73.
Reprint requests:
Ernesto Barquero Cordero, PhD
Rua Duarte Schuttel 262, Ap 301
Centro, Florianpolis
Santa Catarina, Brasil 88015-640
[email protected]
OOOOE
Volume 112, Number 6 Baquero et al. e53
mailto:[email protected]:[email protected]