Embed Size (px)
Citation preview
MSHP Annual Meeting 2017
Yellow Card: FDA Warnings on
Antibiotics
Monica V. Mahoney, PharmD, BCPS AQ-ID
Disclosures
In this presentation I will be:
Discussing off-label indications and uses
Challenging FDA warnings and alerts
All doses and most studies refer to adult
patients
MSHP Annual Meeting 2017
Objectives
Identify the role the FDA plays in updating
drug warnings and communication
Evaluate the literature behind the recent FDA
antimicrobial drug interactions and adverse
drug events
Given a patient scenario, recommend a
treatment plan to manage and mitigate the
FDA warnings
FDA Background
Food and Drug Administration (1906)
Responsibilities Include:
Ensuring safety, efficacy, and security of
drugs, biologics, and medical devices
Regulates the manufacturing, marketing, and
distribution of tobacco
Involved in counterterrorism (food/drug
response to public health threats)
http://www.fda.gov/AboutFDA/default.htm
MSHP Annual Meeting 2017
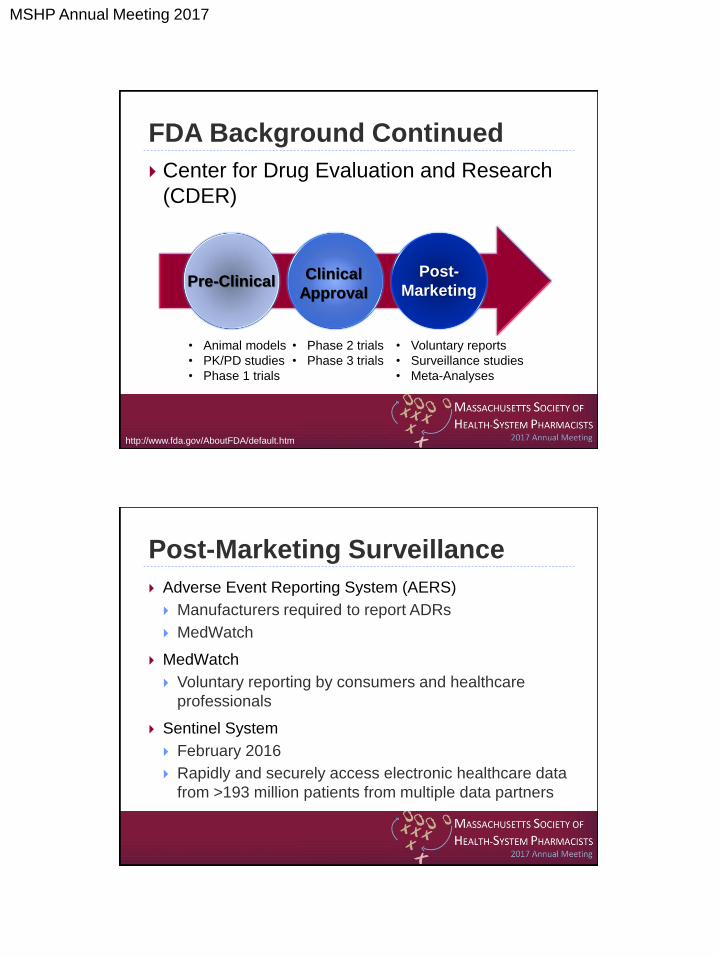
FDA Background Continued
Center for Drug Evaluation and Research
(CDER)
Pre-Clinical Clinical
Approval
Post-
Marketing
• Animal models
• PK/PD studies
• Phase 1 trials
• Phase 2 trials
• Phase 3 trials
• Voluntary reports
• Surveillance studies
• Meta-Analyses
http://www.fda.gov/AboutFDA/default.htm
Post-Marketing Surveillance
Adverse Event Reporting System (AERS)
Manufacturers required to report ADRs
MedWatch
MedWatch
Voluntary reporting by consumers and healthcare
professionals
Sentinel System
February 2016
Rapidly and securely access electronic healthcare data
from >193 million patients from multiple data partners
MSHP Annual Meeting 2017
FDA Drug Safety Communications
Information for consumers and health
professionals on new drug warnings and
other safety information, drug label
changes, and shortages of medically
necessary drug products
http://www.fda.gov/Drugs/DrugSafety
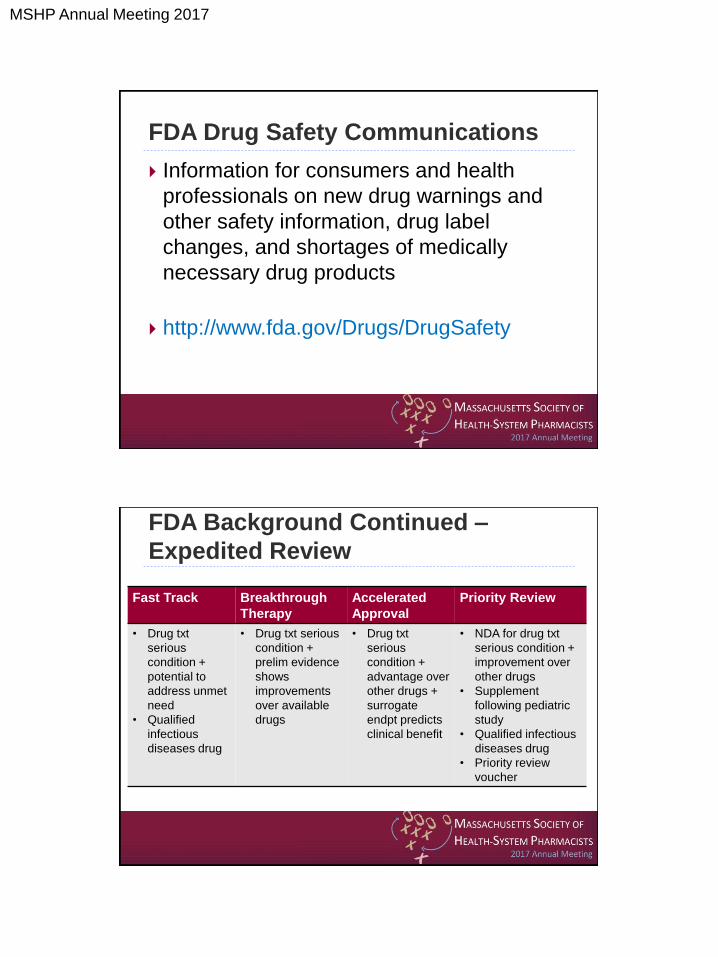
FDA Background Continued –
Expedited Review
Fast Track Breakthrough
Therapy
Accelerated
Approval
Priority Review
• Drug txt
serious
condition +
potential to
address unmet
need
• Qualified
infectious
diseases drug
• Drug txt serious
condition +
prelim evidence
shows
improvements
over available
drugs
• Drug txt
serious
condition +
advantage over
other drugs +
surrogate
endpt predicts
clinical benefit
• NDA for drug txt
serious condition +
improvement over
other drugs
• Supplement
following pediatric
study
• Qualified infectious
diseases drug
• Priority review
voucher
MSHP Annual Meeting 2017
A Cautionary Tale
http://www.fda.gov/Drugs/DrugSafety
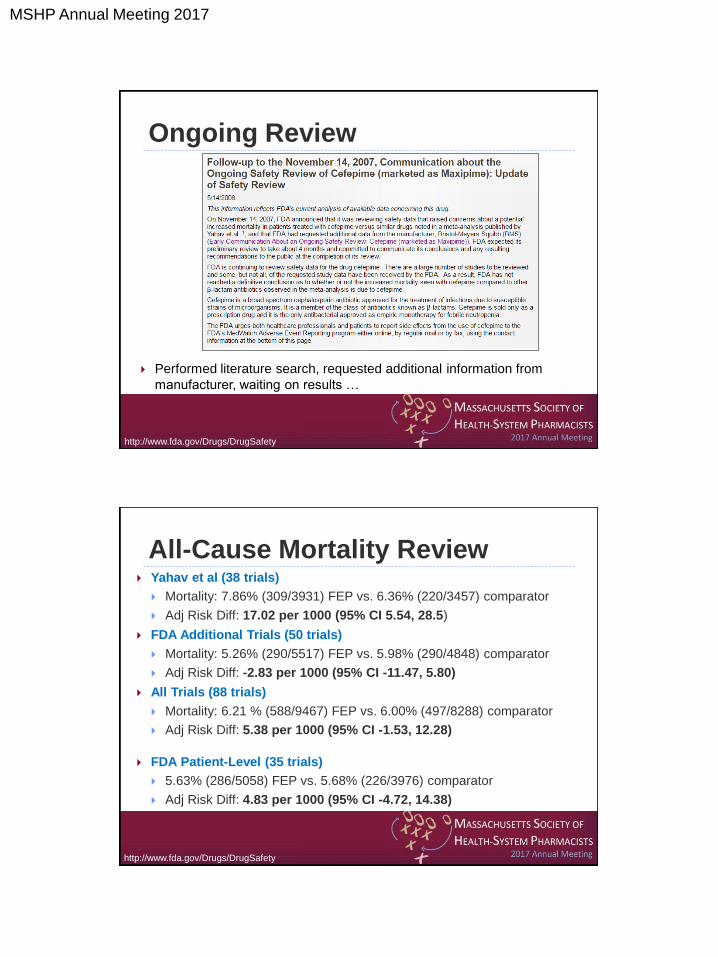
Yahav et al. Design • Systemic review of RCT comparing cefepime (FEP) vs. other β-lactams
Patients • n=11,723 patients (7,388 all-cause mortality data)
• n=57 RCTs (41 provided all-cause mortality data)
Primary
Outcome
• 30 day, all-cause mortality
Results
Conclusions • Mortality significantly higher for FEP than comparators
• No explanations could be determined
Yahav et al. Lancet Infect Dis.2007;7:338-48
MSHP Annual Meeting 2017
Ongoing Review
Performed literature search, requested additional information from
manufacturer, waiting on results …
http://www.fda.gov/Drugs/DrugSafety
All-Cause Mortality Review Yahav et al (38 trials)
Mortality: 7.86% (309/3931) FEP vs. 6.36% (220/3457) comparator
Adj Risk Diff: 17.02 per 1000 (95% CI 5.54, 28.5)
FDA Additional Trials (50 trials)
Mortality: 5.26% (290/5517) FEP vs. 5.98% (290/4848) comparator
Adj Risk Diff: -2.83 per 1000 (95% CI -11.47, 5.80)
All Trials (88 trials)
Mortality: 6.21 % (588/9467) FEP vs. 6.00% (497/8288) comparator
Adj Risk Diff: 5.38 per 1000 (95% CI -1.53, 12.28)
FDA Patient-Level (35 trials)
5.63% (286/5058) FEP vs. 5.68% (226/3976) comparator
Adj Risk Diff: 4.83 per 1000 (95% CI -4.72, 14.38)
http://www.fda.gov/Drugs/DrugSafety
MSHP Annual Meeting 2017
Febrile Neutropenia Review Yahav et al (19 trials)
Mortality: 6.36% (130/2043) FEP vs. 4.51% (87/1928) comparator
Adj Risk Diff: 18.99 per 1000 (95% CI 4.96, 33.02)
All Trials (24 trials)
Adj Risk Diff: 9.67 per 1000 (95% CI -2.87, 22.21)
FDA Patient-Level (7 trials)
7.86% (61/776) FEP vs. 6.55% (41/626) comparator
Adj Risk Diff: 18.1 per 1000 (95% CI -9.22, 45.42)
Most patients died from their underlying malignancies and/or
comorbid conditions
http://www.fda.gov/Drugs/DrugSafety
FDA Review Conclusion
FDA has finished its analysis of a possible risk of higher death with cefepime, an antibiotic,
following publication of a study that suggested a higher rate of death in patients treated with this
drug, as compared to patients treated with similar drugs. FDA has determined that the data do not
indicate a higher rate of death in cefepime-treated patients. Cefepime remains an appropriate
therapy for its approved indications.
http://www.fda.gov/Drugs/DrugSafety
MSHP Annual Meeting 2017
FDA Review Conclusion
FDA has finished its analysis of a possible risk of higher death with cefepime, an antibiotic,
following publication of a study that suggested a higher rate of death in patients treated with this
drug, as compared to patients treated with similar drugs. FDA has determined that
the data do not indicate a higher rate of death in cefepime-
treated patients. Cefepime remains an appropriate therapy
for its approved indications.
http://www.fda.gov/Drugs/DrugSafety
Newsstand
Azithromycin
Monitor
Cefepime
Post
Quinolone
Chronicle
Linezolid
Ledger
Subscription Expired
MSHP Annual Meeting 2017
Azithromycin TM is a 48 y/o male h/o HTN [controlled on diltiazem] and COPD, who
presents to the pharmacy with a prescription for a 3 day course of
azithromycin (500mg qDay) for a COPD exacerbation. He’s had several
days of increased dyspnea and increased sputum production. He read on
the internet that azithromycin can “kill him” and his barber recommended he
ask his doctor to switch to that “leave-a-floxa-something” drug instead.
Upon further questioning you learn that he doesn’t currently smoke, doesn’t
have diabetes, and cholesterol is normal. What antibiotic would you
recommend?
A. Azithromycin 500 mg PO qDay x 3 days
B. Levofloxacin 500 mg PO qDay x 5 days
C. Linezolid 600 mg PO q12h x 7 days
D. Amoxicillin 500 mg PO q6h x 7 days
Azithromycin: Initial FDA Alert
http://www.fda.gov/Drugs/DrugSafety
MSHP Annual Meeting 2017
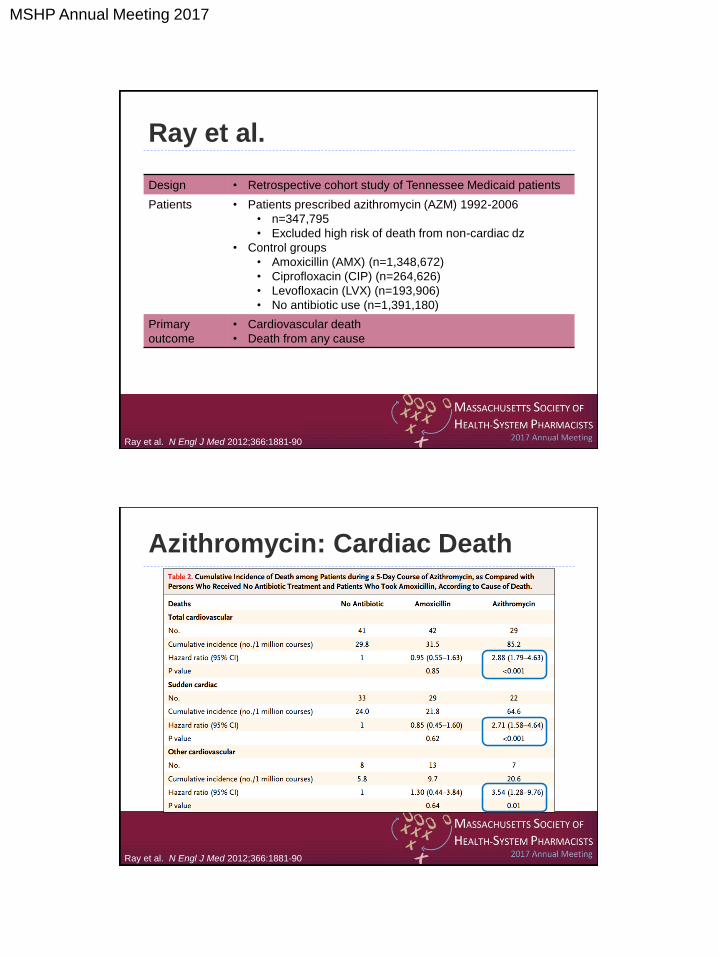
Ray et al.
Design • Retrospective cohort study of Tennessee Medicaid patients
Patients • Patients prescribed azithromycin (AZM) 1992-2006
• n=347,795
• Excluded high risk of death from non-cardiac dz
• Control groups
• Amoxicillin (AMX) (n=1,348,672)
• Ciprofloxacin (CIP) (n=264,626)
• Levofloxacin (LVX) (n=193,906)
• No antibiotic use (n=1,391,180)
Primary
outcome
• Cardiovascular death
• Death from any cause
Ray et al. N Engl J Med 2012;366:1881-90
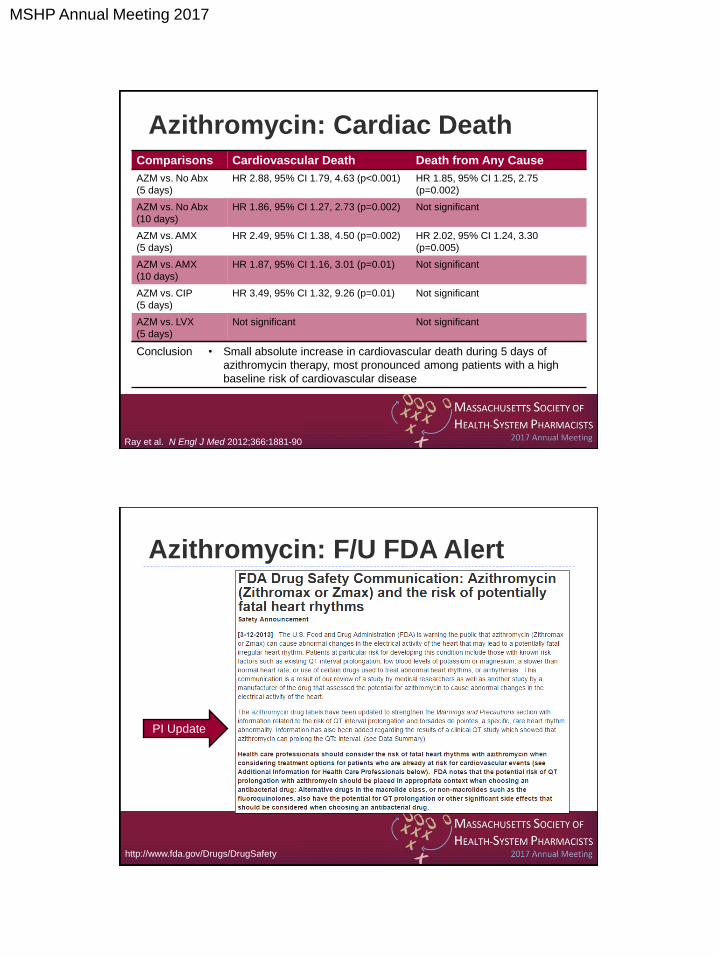
Azithromycin: Cardiac Death
Ray et al. N Engl J Med 2012;366:1881-90
MSHP Annual Meeting 2017
Comparisons Cardiovascular Death Death from Any Cause
AZM vs. No Abx
(5 days)
HR 2.88, 95% CI 1.79, 4.63 (p<0.001) HR 1.85, 95% CI 1.25, 2.75
(p=0.002)
AZM vs. No Abx
(10 days)
HR 1.86, 95% CI 1.27, 2.73 (p=0.002) Not significant
AZM vs. AMX
(5 days)
HR 2.49, 95% CI 1.38, 4.50 (p=0.002) HR 2.02, 95% CI 1.24, 3.30
(p=0.005)
AZM vs. AMX
(10 days)
HR 1.87, 95% CI 1.16, 3.01 (p=0.01) Not significant
AZM vs. CIP
(5 days)
HR 3.49, 95% CI 1.32, 9.26 (p=0.01) Not significant
AZM vs. LVX
(5 days)
Not significant Not significant
Azithromycin: Cardiac Death
Conclusion • Small absolute increase in cardiovascular death during 5 days of
azithromycin therapy, most pronounced among patients with a high
baseline risk of cardiovascular disease
Ray et al. N Engl J Med 2012;366:1881-90
Azithromycin: F/U FDA Alert
http://www.fda.gov/Drugs/DrugSafety
PI Update
MSHP Annual Meeting 2017
Additional Studies
Propensity-matched Danish study comparing AZM to no antibiotics or penicillin V
in all-comers (n=~10 million)
Increased risk of CV death compared to no abx (HR 2.85, 95% CI 1.13, 7.24)
No increased risk compared to penicillin V (HR 0.93, 95% CI 0.56, 1.55)
Retrospective review of VA records comparing outpatient AZM, AMX, and LVX
(n=~1.75 million)
Compared to AMX, both AZM and LVX were associated with higher rates of all-
cause mortality (HR 1.48, 95% CI 1.05, 2.09 and HR 2.49, 95% CI 1.70, 3.64,
respectively)
Svanström et al. N Engl J Med 2013;368:1704-12
Rao et al. Ann Fam Med 2014;12:121-7
Patients at Highest Risk
Pre-existing QTc prolongation
Uncorrected hypomagnesemia
Uncorrected hypokalemia
Bradycardia
On concomitant Class IA or Class III
antiarrythmic agents
http://www.fda.gov/Drugs/DrugSafety
MSHP Annual Meeting 2017
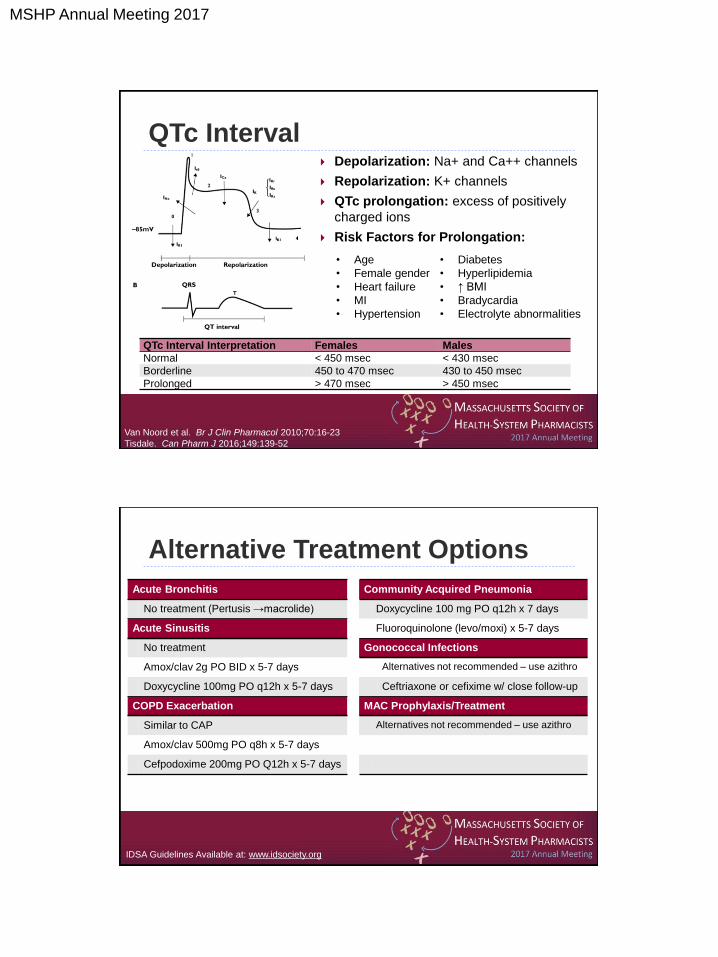
QTc Interval Depolarization: Na+ and Ca++ channels
Repolarization: K+ channels
QTc prolongation: excess of positively
charged ions
Risk Factors for Prolongation:
• Age
• Female gender
• Heart failure
• MI
• Hypertension
• Diabetes
• Hyperlipidemia
• ↑ BMI
• Bradycardia
• Electrolyte abnormalities
Van Noord et al. Br J Clin Pharmacol 2010;70:16-23
Tisdale. Can Pharm J 2016;149:139-52
QTc Interval Interpretation Females Males
Normal < 450 msec < 430 msec
Borderline 450 to 470 msec 430 to 450 msec
Prolonged > 470 msec > 450 msec
Alternative Treatment Options
IDSA Guidelines Available at: www.idsociety.org
Acute Bronchitis Community Acquired Pneumonia
No treatment (Pertusis →macrolide) Doxycycline 100 mg PO q12h x 7 days
Acute Sinusitis Fluoroquinolone (levo/moxi) x 5-7 days
No treatment Gonococcal Infections
Amox/clav 2g PO BID x 5-7 days Alternatives not recommended – use azithro
Doxycycline 100mg PO q12h x 5-7 days Ceftriaxone or cefixime w/ close follow-up
COPD Exacerbation MAC Prophylaxis/Treatment
Similar to CAP Alternatives not recommended – use azithro
Amox/clav 500mg PO q8h x 5-7 days
Cefpodoxime 200mg PO Q12h x 5-7 days
MSHP Annual Meeting 2017
Role of the Pharmacist
Evaluate need for azithromycin
Recommend alternative antibiotics
Evaluate risk factors for QTc
prolongation/Torsades
Evaluate drug-drug interactions
Replete magnesium, potassium
Monitor EKG
Azithromycin TM is a 48 y/o male h/o HTN [controlled on diltiazem] and COPD, who
presents to the pharmacy with a prescription for a 3 day course of
azithromycin (500mg qDay) for a COPD exacerbation. He’s had several
days of increased dyspnea and increased sputum production. He read on
the internet that azithromycin can “kill him” and his barber recommended he
ask his doctor to switch to that “leave-a-floxa-something” drug instead.
Upon further questioning you learn that he doesn’t currently smoke, doesn’t
have diabetes, and cholesterol is normal. What antibiotic would you
recommend?
A. Azithromycin 500 mg PO qDay x 3 days
B. Levofloxacin 500 mg PO qDay x 5 days
C. Linezolid 600 mg PO q12h x 7 days
D. Amoxicillin 500 mg PO q6h x 7 days
MSHP Annual Meeting 2017
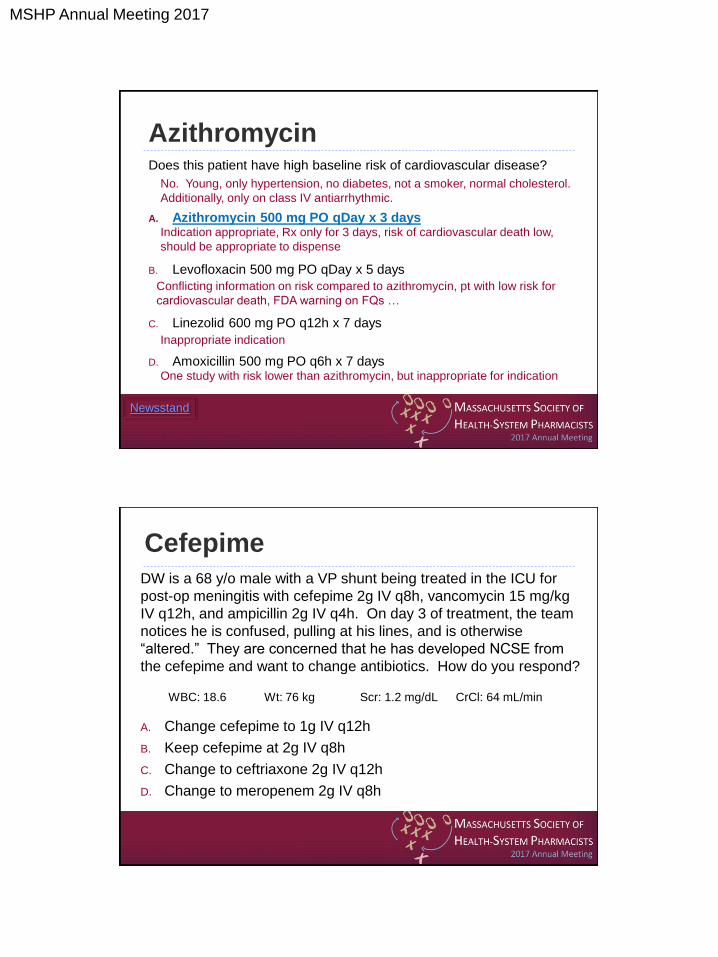
Azithromycin Does this patient have high baseline risk of cardiovascular disease?
A. Azithromycin 500 mg PO qDay x 3 days
B. Levofloxacin 500 mg PO qDay x 5 days
C. Linezolid 600 mg PO q12h x 7 days
D. Amoxicillin 500 mg PO q6h x 7 days
Newsstand
No. Young, only hypertension, no diabetes, not a smoker, normal cholesterol.
Additionally, only on class IV antiarrhythmic.
Indication appropriate, Rx only for 3 days, risk of cardiovascular death low,
should be appropriate to dispense
Conflicting information on risk compared to azithromycin, pt with low risk for
cardiovascular death, FDA warning on FQs …
Inappropriate indication
One study with risk lower than azithromycin, but inappropriate for indication
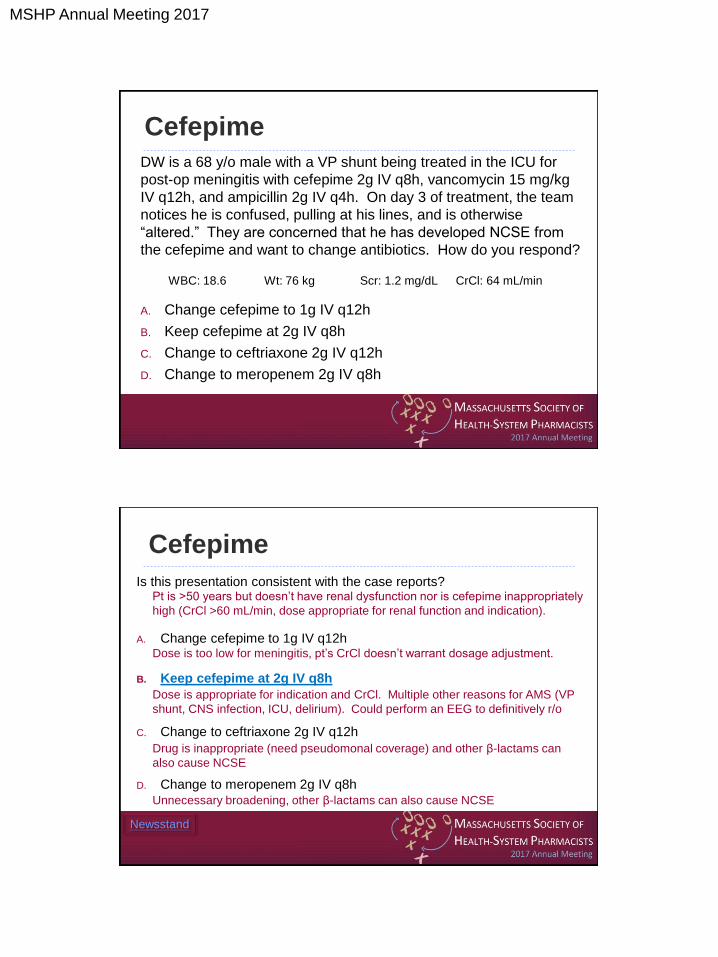
DW is a 68 y/o male with a VP shunt being treated in the ICU for
post-op meningitis with cefepime 2g IV q8h, vancomycin 15 mg/kg
IV q12h, and ampicillin 2g IV q4h. On day 3 of treatment, the team
notices he is confused, pulling at his lines, and is otherwise
“altered.” They are concerned that he has developed NCSE from
the cefepime and want to change antibiotics. How do you respond?
A. Change cefepime to 1g IV q12h
B. Keep cefepime at 2g IV q8h
C. Change to ceftriaxone 2g IV q12h
D. Change to meropenem 2g IV q8h
Cefepime
WBC: 18.6 Wt: 76 kg Scr: 1.2 mg/dL CrCl: 64 mL/min
MSHP Annual Meeting 2017
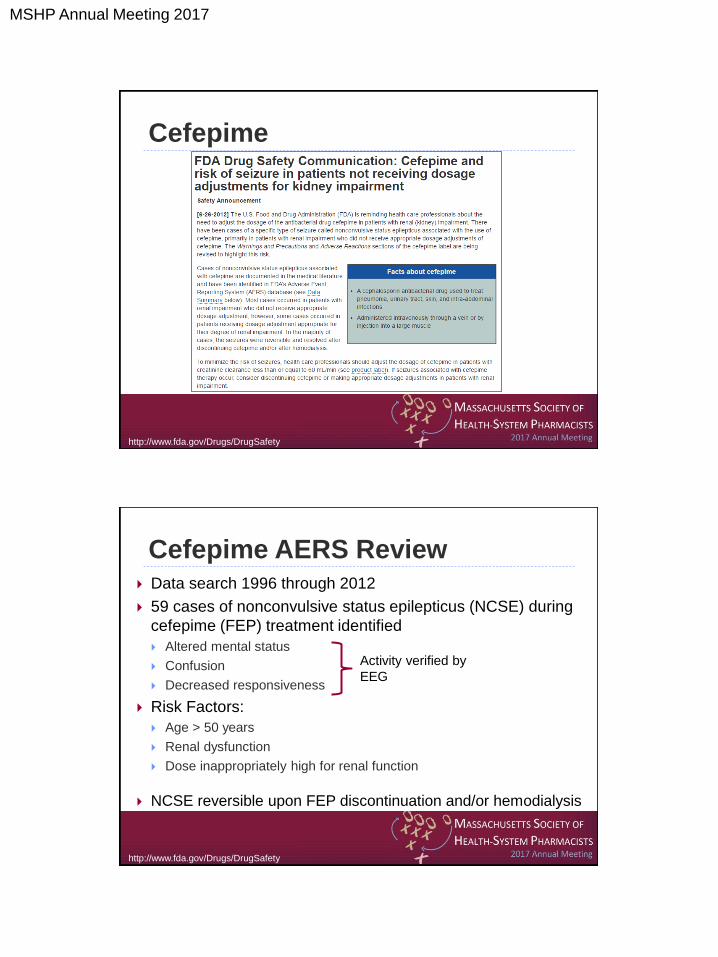
Cefepime
http://www.fda.gov/Drugs/DrugSafety
Cefepime AERS Review Data search 1996 through 2012
59 cases of nonconvulsive status epilepticus (NCSE) during
cefepime (FEP) treatment identified
Altered mental status
Confusion
Decreased responsiveness
Risk Factors:
Age > 50 years
Renal dysfunction
Dose inappropriately high for renal function
NCSE reversible upon FEP discontinuation and/or hemodialysis
Activity verified by
EEG
http://www.fda.gov/Drugs/DrugSafety

MSHP Annual Meeting 2017
Mayo Clinic Review Design • Retrospective review
Patients • ICU adults treated with FEP 2009-2011
• n=100 patients
Methods • Primary outcome = FEP neurotoxicity
• Encephalopathy, delirium, altered mental status, confusion, acute
confusional state
Results • 15 patients met criteria for neurotoxicity
• Impaired consciousness (n=13)
• Myoclonus (n=11)
• Disorientation (n=6)
• NCSE (n=1)
• Risk factors:
• Inappropriate high dose (62.4%. Vs 24.7%, p=0.001)
• History of chronic kidney disease (66.7% vs. 35.3%, p=0.04)
Conclusions • FEP-associated seizures may be rare, but other manifestations of CNS
toxicity may not be
Fugate et al. Crit Care 2013;17:R264
β-Lactams
Cross the BBB
Renally excreted
Dosage adjustment in renal impairment
Cockcroft-Gault:
Modification of Diet in Renal Disease (MDRD):
140 – (age) x (weight)
72 x (Scr) (x 0.85 if female)
186.3 x Scr -1.154 x age -0.203 x 0.742 (if female) x 1.212 (if black)
MSHP Annual Meeting 2017
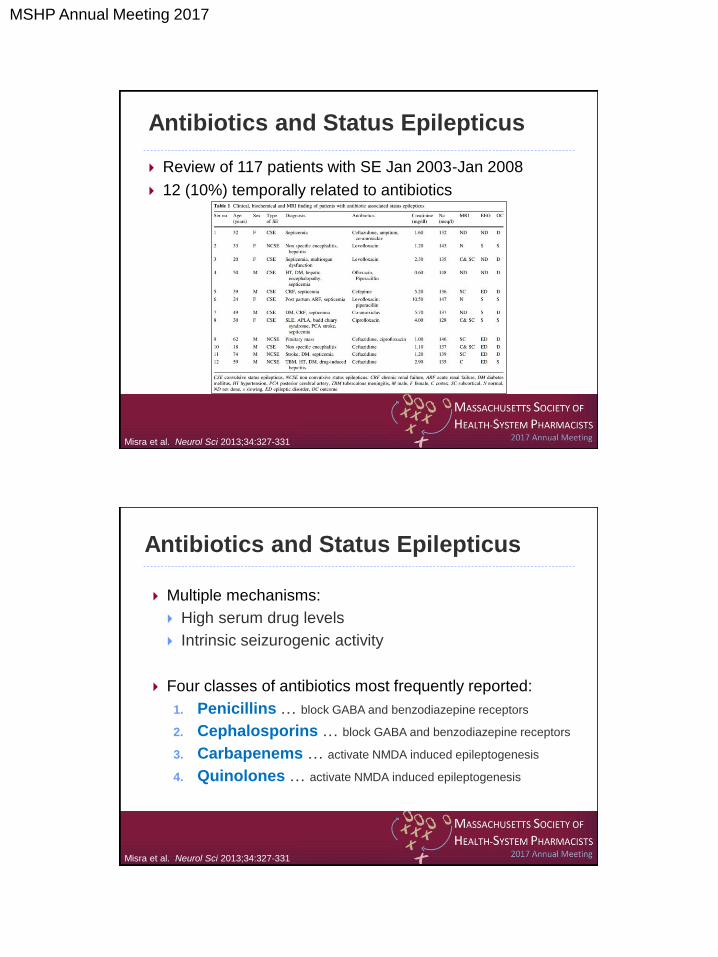
Antibiotics and Status Epilepticus
Review of 117 patients with SE Jan 2003-Jan 2008
12 (10%) temporally related to antibiotics
Misra et al. Neurol Sci 2013;34:327-331
Antibiotics and Status Epilepticus
Multiple mechanisms:
High serum drug levels
Intrinsic seizurogenic activity
Four classes of antibiotics most frequently reported:
1. Penicillins … block GABA and benzodiazepine receptors
2. Cephalosporins … block GABA and benzodiazepine receptors
3. Carbapenems … activate NMDA induced epileptogenesis
4. Quinolones … activate NMDA induced epileptogenesis
Misra et al. Neurol Sci 2013;34:327-331
MSHP Annual Meeting 2017
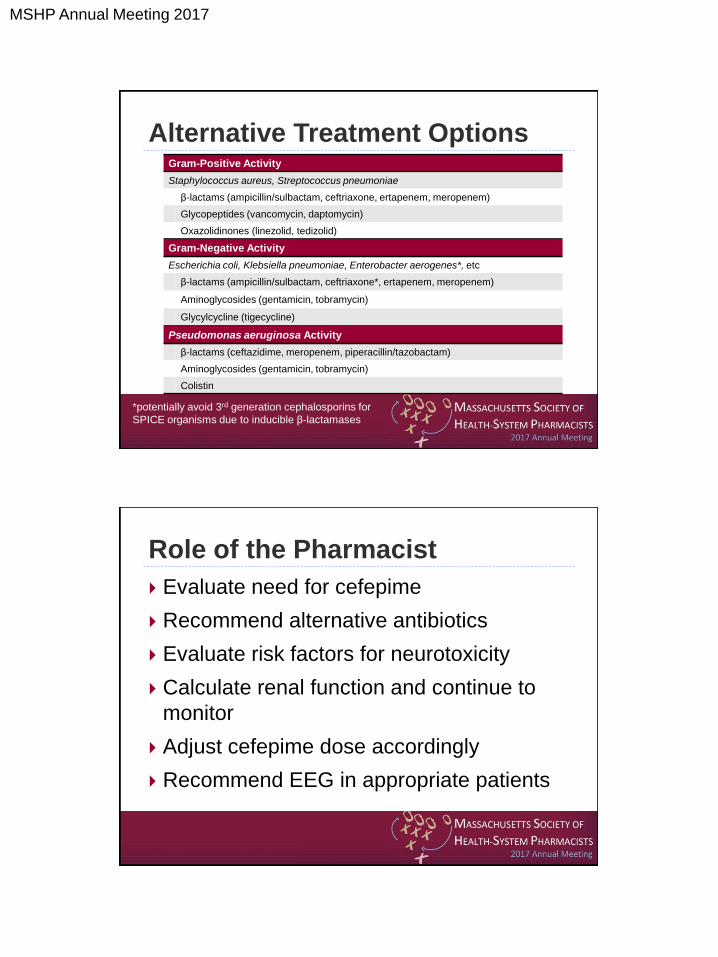
Alternative Treatment Options Gram-Positive Activity
Staphylococcus aureus, Streptococcus pneumoniae
β-lactams (ampicillin/sulbactam, ceftriaxone, ertapenem, meropenem)
Glycopeptides (vancomycin, daptomycin)
Oxazolidinones (linezolid, tedizolid)
Gram-Negative Activity
Escherichia coli, Klebsiella pneumoniae, Enterobacter aerogenes*, etc
β-lactams (ampicillin/sulbactam, ceftriaxone*, ertapenem, meropenem)
Aminoglycosides (gentamicin, tobramycin)
Glycylcycline (tigecycline)
Pseudomonas aeruginosa Activity
β-lactams (ceftazidime, meropenem, piperacillin/tazobactam)
Aminoglycosides (gentamicin, tobramycin)
Colistin
*potentially avoid 3rd generation cephalosporins for
SPICE organisms due to inducible β-lactamases
Role of the Pharmacist
Evaluate need for cefepime
Recommend alternative antibiotics
Evaluate risk factors for neurotoxicity
Calculate renal function and continue to
monitor
Adjust cefepime dose accordingly
Recommend EEG in appropriate patients
MSHP Annual Meeting 2017
DW is a 68 y/o male with a VP shunt being treated in the ICU for
post-op meningitis with cefepime 2g IV q8h, vancomycin 15 mg/kg
IV q12h, and ampicillin 2g IV q4h. On day 3 of treatment, the team
notices he is confused, pulling at his lines, and is otherwise
“altered.” They are concerned that he has developed NCSE from
the cefepime and want to change antibiotics. How do you respond?
A. Change cefepime to 1g IV q12h
B. Keep cefepime at 2g IV q8h
C. Change to ceftriaxone 2g IV q12h
D. Change to meropenem 2g IV q8h
Cefepime
WBC: 18.6 Wt: 76 kg Scr: 1.2 mg/dL CrCl: 64 mL/min
Is this presentation consistent with the case reports?
A. Change cefepime to 1g IV q12h
B. Keep cefepime at 2g IV q8h
C. Change to ceftriaxone 2g IV q12h
D. Change to meropenem 2g IV q8h
Cefepime
Newsstand
Pt is >50 years but doesn’t have renal dysfunction nor is cefepime inappropriately
high (CrCl >60 mL/min, dose appropriate for renal function and indication).
Dose is too low for meningitis, pt’s CrCl doesn’t warrant dosage adjustment.
Dose is appropriate for indication and CrCl. Multiple other reasons for AMS (VP
shunt, CNS infection, ICU, delirium). Could perform an EEG to definitively r/o
Drug is inappropriate (need pseudomonal coverage) and other β-lactams can
also cause NCSE
Unnecessary broadening, other β-lactams can also cause NCSE
MSHP Annual Meeting 2017
PG is a 38 y/o female diagnosed with her 2nd UTI in 2 years. She
has no urogenital abnormalities, is allergic to “sulfa”, and takes
migraine medicine as needed. She is finishing a prednisone taper
for an unknown indication. She complains of 2 days of urinary
frequency and “burning.” A dipstick urinalysis shows + leukocyte
esterase, 40 WBC, and + nitrites. Which of the following treatments
would you recommend?
A. Sulfamethoxazole/trimethoprim 1 DS PO BID x 3 days
B. Ciprofloxacin 250 mg PO BID x 5 days
C. Fosfomycin 3g PO x 1
D. Treat symptoms only: phenazopyridine + ibuprofen
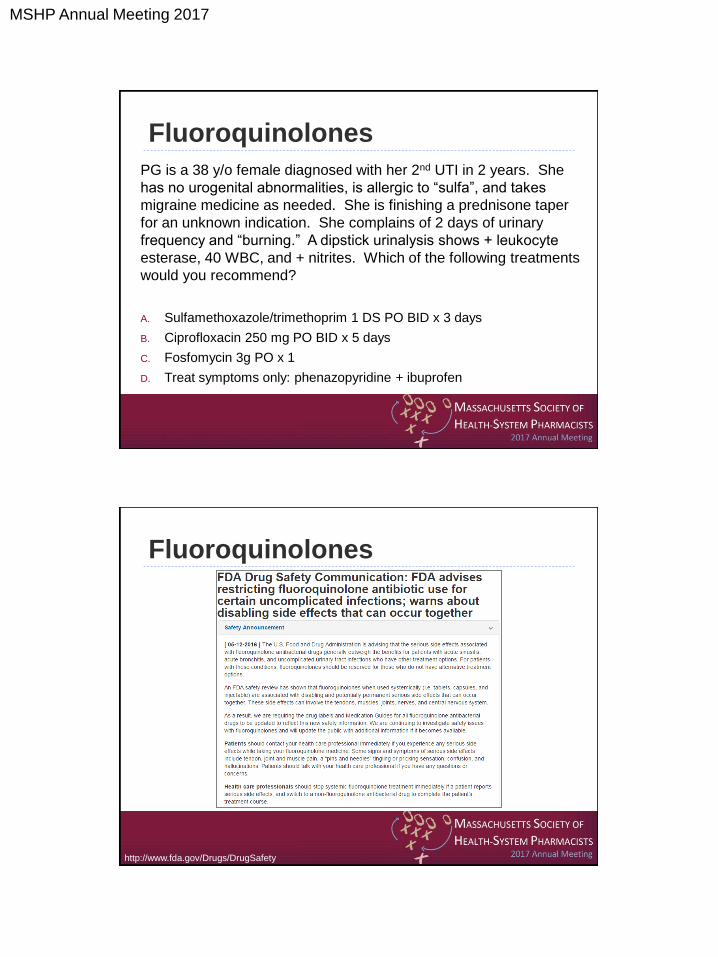
Fluoroquinolones
Fluoroquinolones
http://www.fda.gov/Drugs/DrugSafety

MSHP Annual Meeting 2017
Fluoroquinolone FDA Update
http://www.fda.gov/Drugs/DrugSafety
November 2015 Special Meeting
• Acute bacterial sinusitis
(ABS)
• Acute bacterial
exacerbation of chronic
bronchitis (ABECB)
• Uncomplicated urinary
tract infection (uUTI)
• Nov 1997 to May 2015
• 178 cases of healthy
pts who developed
irreversible ADRs
http://www.fda.gov/Drugs/DrugSafety
Placebo-
Controlled
Trials
AERS
Review
FDA Safety
Communication
MSHP Annual Meeting 2017
Placebo-Controlled Trials: ABS 20 placebo-controlled trials
6 showed statistically significant differences
Cochrane Review 2012 Acute rhinosinusitis (adults) concluded
there is “no place for antibiotics for the patient with clinically
diagnosed, uncomplicated acute rhinosinusitis”
Cochrane Review 2014 Acute maxillary sinusitis (adults)
concluded “there is moderate evidence that antibiotics provide a small
benefit … however about 80% improved within 2 weeks” with no
antibacterial therapy
IDSA Guidelines 2012 Acute bacterial rhinosinusitis (adults/kids)
comment that 90% ABS is caused by viruses and antibiotics should
be reserved for “patients with greater severity of symptoms”
http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesM
eetingMaterials/Drugs/Anti-
InfectiveDrugsAdvisoryCommittee/UCM472655.pdf
Placebo-Controlled Trials: ABECB
15 placebo-controlled trials
6 showed statistically significant differences
Cochrane Review 2009 Antibiotics for exacerbations of
COPD supports “antibiotics for patients who are moderately
or severely ill”
Multiple societal/organizational position papers echo finding
for moderately/severely ill patients
FDA definitions:
Mild: patients treated as outpatients
Moderate to severe: pts needing hospitalization for txt of ABECB
http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesM
eetingMaterials/Drugs/Anti-
InfectiveDrugsAdvisoryCommittee/UCM472655.pdf
MSHP Annual Meeting 2017
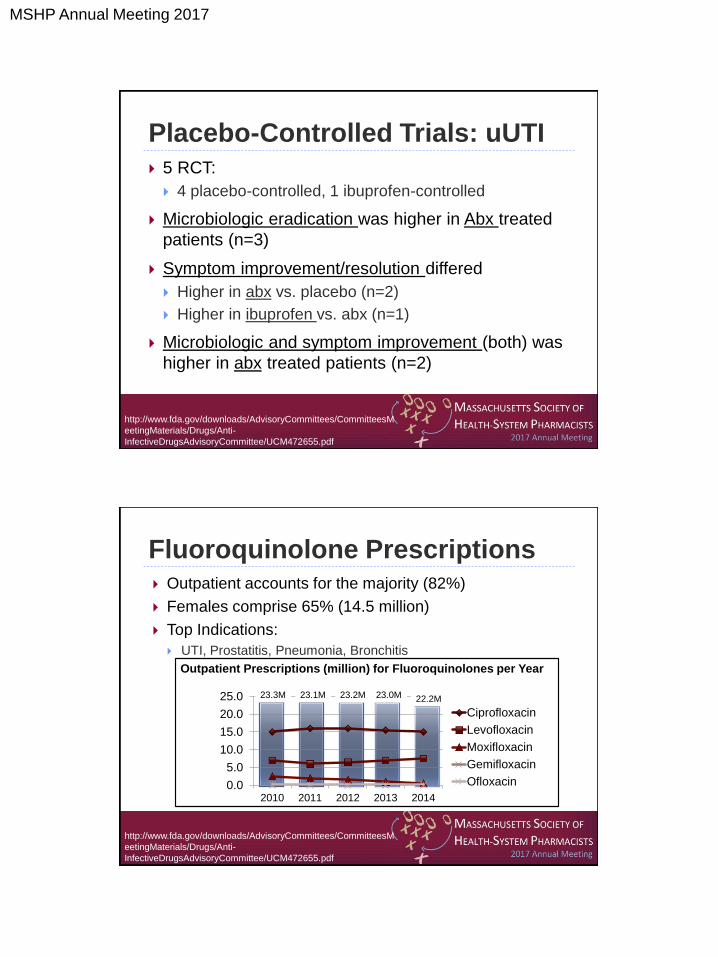
Placebo-Controlled Trials: uUTI
5 RCT:
4 placebo-controlled, 1 ibuprofen-controlled
Microbiologic eradication was higher in Abx treated
patients (n=3)
Symptom improvement/resolution differed
Higher in abx vs. placebo (n=2)
Higher in ibuprofen vs. abx (n=1)
Microbiologic and symptom improvement (both) was
higher in abx treated patients (n=2)
http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesM
eetingMaterials/Drugs/Anti-
InfectiveDrugsAdvisoryCommittee/UCM472655.pdf
Fluoroquinolone Prescriptions
0.0
5.0
10.0
15.0
20.0
25.0
2010 2011 2012 2013 2014
Ciprofloxacin
Levofloxacin
Moxifloxacin
Gemifloxacin
Ofloxacin
23.3M 23.1M 23.2M 23.0M 22.2M
Outpatient accounts for the majority (82%)
Females comprise 65% (14.5 million)
Top Indications:
UTI, Prostatitis, Pneumonia, Bronchitis
Outpatient Prescriptions (million) for Fluoroquinolones per Year
http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesM
eetingMaterials/Drugs/Anti-
InfectiveDrugsAdvisoryCommittee/UCM472655.pdf

MSHP Annual Meeting 2017
Fluoroquinolone ADRs
Existing Warnings:
Tendinitis and tendon rupture
Cardiac arrhythmia
Peripheral neuropathy
http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesM
eetingMaterials/Drugs/Anti-
InfectiveDrugsAdvisoryCommittee/UCM472655.pdf
Fluoroquinolone ADRs
Existing Warnings:
Tendinitis and tendon rupture
Age > 60 years
Concomitant corticosteroids
Kidney, heart, lung transplant?
http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesM
eetingMaterials/Drugs/Anti-
InfectiveDrugsAdvisoryCommittee/UCM472655.pdf
MSHP Annual Meeting 2017
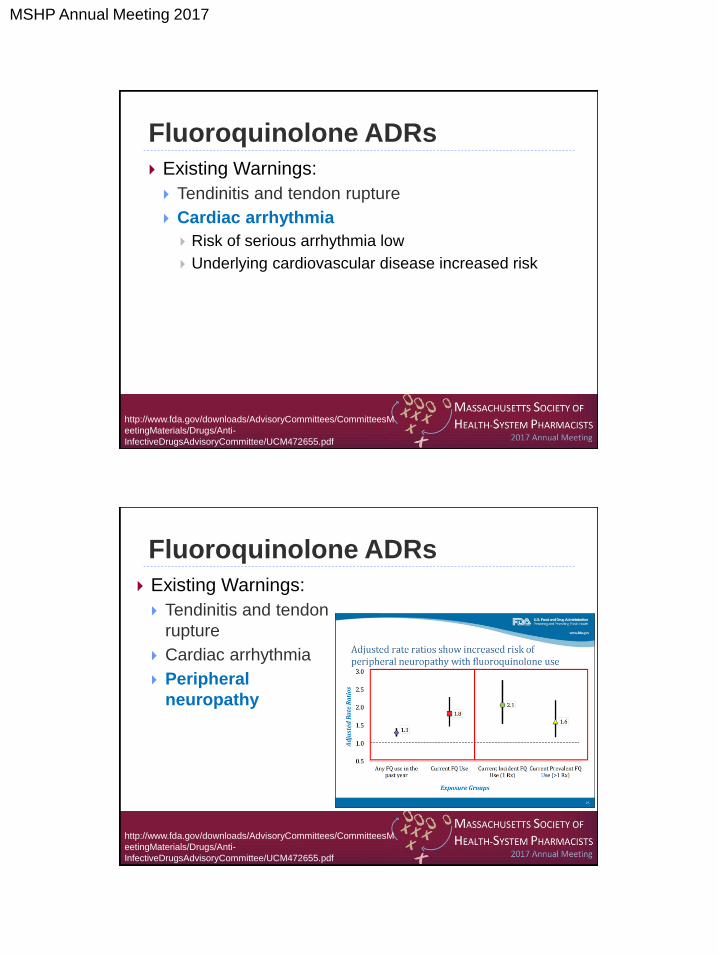
Fluoroquinolone ADRs
Existing Warnings:
Tendinitis and tendon rupture
Cardiac arrhythmia
Risk of serious arrhythmia low
Underlying cardiovascular disease increased risk
http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesM
eetingMaterials/Drugs/Anti-
InfectiveDrugsAdvisoryCommittee/UCM472655.pdf
Fluoroquinolone ADRs
Existing Warnings:
Tendinitis and tendon
rupture
Cardiac arrhythmia
Peripheral
neuropathy
http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesM
eetingMaterials/Drugs/Anti-
InfectiveDrugsAdvisoryCommittee/UCM472655.pdf
MSHP Annual Meeting 2017
Fluoroquinolone-Associated Disability (FQAD)
Reviewed AERS Nov 1997-May 2015
FQAD: ADRS from ≥ 2 body systems
ADRs persist for >30 days after d/c FQ
• Musculoskeletal
• Neuropsychiatric
• Cardiovascular
• Senses
• Skin
• Peripheral Nervous System
Organ System Cases Involved (n=178)
Musculoskeletal (tendon/joint/muscle) 173 (97%)
Neuropsychiatric 121 (68%)
Peripheral Nervous System 113 (63%)
Senses (vision, hearing, etc) 57 (32%)
Skin 27 (15%)
Cardiovascular 22 (12%)
http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesM
eetingMaterials/Drugs/Anti-
InfectiveDrugsAdvisoryCommittee/UCM472655.pdf
FDA Recommendations
“… serious side effects associated with
fluoroquinolone antibacterial drugs
generally outweigh the benefits for patients
with acute sinusitis, acute bronchitis, and
uncomplicated urinary tract infections who
have other treatment options”
http://www.fda.gov/Drugs/DrugSafety
MSHP Annual Meeting 2017
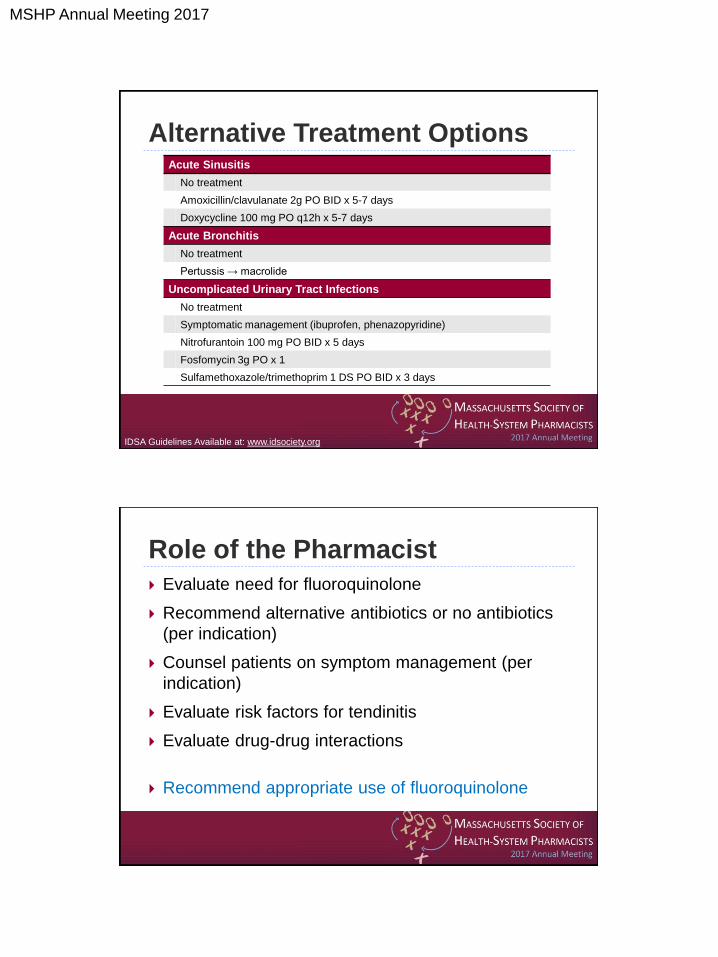
Alternative Treatment Options Acute Sinusitis
No treatment
Amoxicillin/clavulanate 2g PO BID x 5-7 days
Doxycycline 100 mg PO q12h x 5-7 days
Acute Bronchitis
No treatment
Pertussis → macrolide
Uncomplicated Urinary Tract Infections
No treatment
Symptomatic management (ibuprofen, phenazopyridine)
Nitrofurantoin 100 mg PO BID x 5 days
Fosfomycin 3g PO x 1
Sulfamethoxazole/trimethoprim 1 DS PO BID x 3 days
IDSA Guidelines Available at: www.idsociety.org
Role of the Pharmacist
Evaluate need for fluoroquinolone
Recommend alternative antibiotics or no antibiotics
(per indication)
Counsel patients on symptom management (per
indication)
Evaluate risk factors for tendinitis
Evaluate drug-drug interactions
Recommend appropriate use of fluoroquinolone

MSHP Annual Meeting 2017
PG is a 38 y/o female diagnosed with her 2nd UTI in 2 years. She
has no urogenital abnormalities, is allergic to “sulfa”, and takes
migraine medicine as needed. She is finishing a prednisone taper
for an unknown indication. She complains of 2 days of urinary
frequency and “burning.” A dipstick urinalysis shows + leukocyte
esterases, 40 WBC, and + nitrites. Which of the following
treatments would you recommend?
A. Sulfamethoxazole/trimethoprim 1 DS PO BID x 3 days
B. Ciprofloxacin 250 mg PO BID x 5 days
C. Fosfomycin 3g PO x 1
D. Treat symptoms only – phenazopyridine + ibuprofen
Fluoroquinolones
Fluoroquinolones Is this an uncomplicated UTI?
A. Sulfamethoxazole/trimethoprim 1 DS PO BID x 3 days
B. Ciprofloxacin 250 mg PO BID x 5 days
C. Fosfomycin 3g PO x 1
D. Treat symptoms only – phenazopyridine + ibuprofen
Newsstand
No structural abnormalities, young healthy female, last UTI 1-2 years ago.
Yes, this is uncomplicated.
Patient endorses allergy to “sulfa”. Since alternative options exist, would
not want to challenge patient.
As this is uUTI, FDA warns against using this agent if alternatives exist. If
we were to use, increased risk of tenditinis, given concomitant steroids.
Appropriate option with no contra-indications
Also appropriate option if patient willing to “watch and wait”
MSHP Annual Meeting 2017
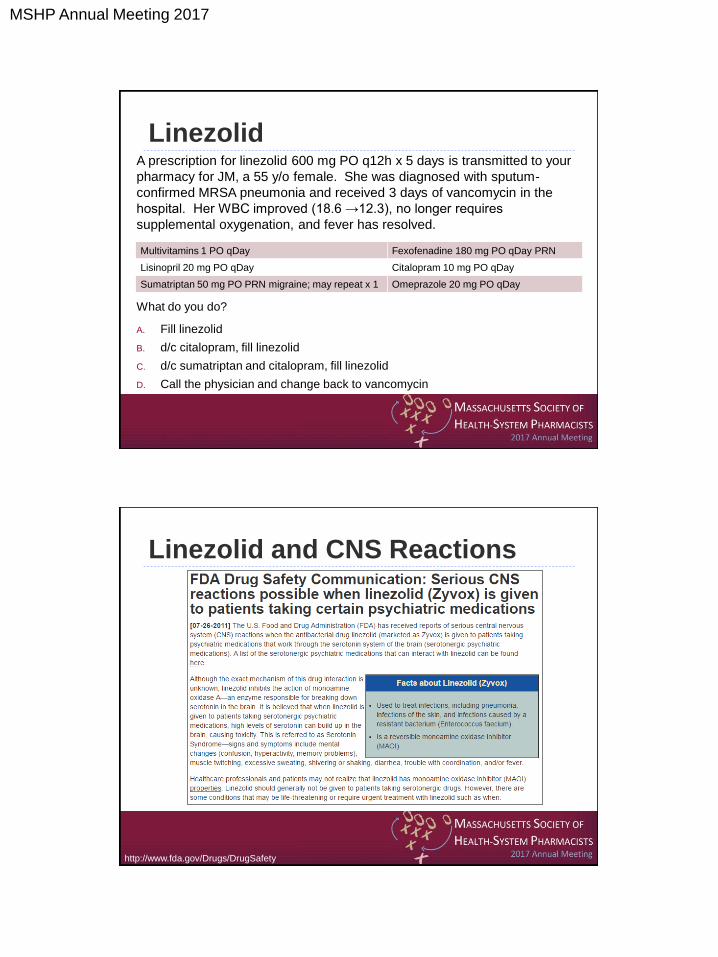
Linezolid A prescription for linezolid 600 mg PO q12h x 5 days is transmitted to your
pharmacy for JM, a 55 y/o female. She was diagnosed with sputum-
confirmed MRSA pneumonia and received 3 days of vancomycin in the
hospital. Her WBC improved (18.6 →12.3), no longer requires
supplemental oxygenation, and fever has resolved.
What do you do?
A. Fill linezolid
B. d/c citalopram, fill linezolid
C. d/c sumatriptan and citalopram, fill linezolid
D. Call the physician and change back to vancomycin
Multivitamins 1 PO qDay Fexofenadine 180 mg PO qDay PRN
Lisinopril 20 mg PO qDay Citalopram 10 mg PO qDay
Sumatriptan 50 mg PO PRN migraine; may repeat x 1 Omeprazole 20 mg PO qDay
Linezolid and CNS Reactions
http://www.fda.gov/Drugs/DrugSafety
MSHP Annual Meeting 2017
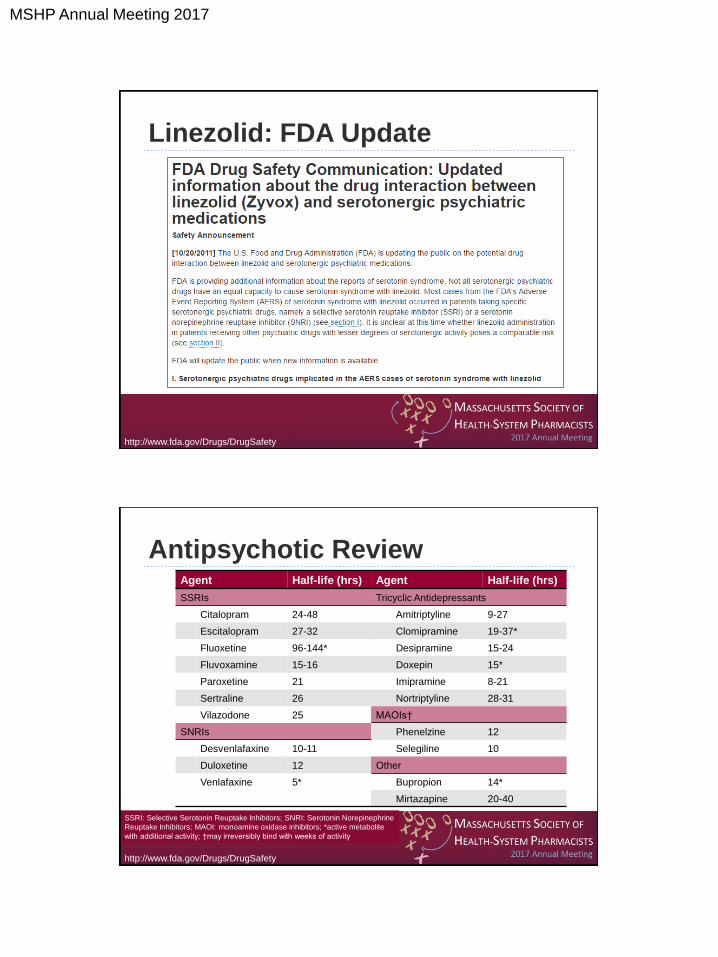
Linezolid: FDA Update
http://www.fda.gov/Drugs/DrugSafety
Antipsychotic Review Agent Half-life (hrs) Agent Half-life (hrs)
SSRIs Tricyclic Antidepressants
Citalopram 24-48 Amitriptyline 9-27
Escitalopram 27-32 Clomipramine 19-37*
Fluoxetine 96-144* Desipramine 15-24
Fluvoxamine 15-16 Doxepin 15*
Paroxetine 21 Imipramine 8-21
Sertraline 26 Nortriptyline 28-31
Vilazodone 25 MAOIs†
SNRIs Phenelzine 12
Desvenlafaxine 10-11 Selegiline 10
Duloxetine 12 Other
Venlafaxine 5* Bupropion 14*
Mirtazapine 20-40
SSRI: Selective Serotonin Reuptake Inhibitors; SNRI: Serotonin Norepinephrine
Reuptake Inhibitors; MAOI: monoamine oxidase inhibitors; *active metabolite
with additional activity; †may irreversibly bind with weeks of activity
http://www.fda.gov/Drugs/DrugSafety

MSHP Annual Meeting 2017
Excess serotonin
Mental status changes
Autonomic hyperactivity
Neuromuscular abnormalities
Symptoms:
Agitation, tachycardia, diaphoresis, tremor,
restlessness, muscular rigidity, hyperreflexia, clonus
Life threatening:
Metabolic acidosis, rhabdomyolysis, seizures, renal
failure, disseminated intravascular coagulation
Serotonin Syndrome
Woytowish et al. Ann Pharmacother 2013;47:388-97
Butterfield et al. Design • Review of Phase 3 and 4 comparator-controlled trials
Methods • Intensive word search algorithms for serotonin syndrome
• Sternbach Criteria
• Hunter Serotonin Toxicity Criteria
• Compared linezolid (n=5426) vs. comparator study drug (n=5058)
Sternbach Criteria
1. Recent addition of serotonergic
medication
2. At least 3 serotonergic
symptoms: MS changes, agitation, myoclonus,
hyperreflexia, diaphoresis,
shivering, tremor, diarrhea, fever,
and/or incoordination
3. All other causes ruled out
Hunter Criteria
1. Recent addition of serotonergic
medication
2. At least 1 of the following: Spontaneous clonus,
Inducible clonis + agitation/diaphoresis,
Ocular clonus + agitation/diaphoresis,
Tremor + hyperreflexia,
And/or hypertonia plus T>100.4⁰F +
ocular clonus/inducible clonus
Butterfield et al. J Antimicrob Chemother 2012;67:494-502
MSHP Annual Meeting 2017
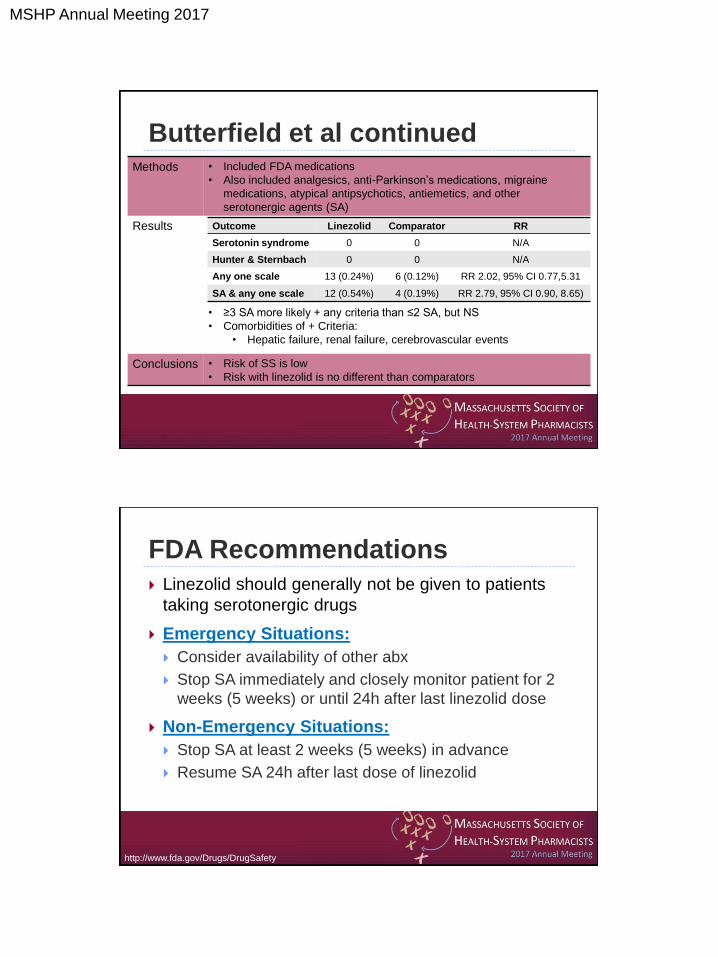
Butterfield et al continued Methods • Included FDA medications
• Also included analgesics, anti-Parkinson’s medications, migraine
medications, atypical antipsychotics, antiemetics, and other
serotonergic agents (SA)
Results
• ≥3 SA more likely + any criteria than ≤2 SA, but NS
• Comorbidities of + Criteria:
• Hepatic failure, renal failure, cerebrovascular events
Conclusions • Risk of SS is low
• Risk with linezolid is no different than comparators
Outcome Linezolid Comparator RR
Serotonin syndrome 0 0 N/A
Hunter & Sternbach 0 0 N/A
Any one scale 13 (0.24%) 6 (0.12%) RR 2.02, 95% CI 0.77,5.31
SA & any one scale 12 (0.54%) 4 (0.19%) RR 2.79, 95% CI 0.90, 8.65)
FDA Recommendations
Linezolid should generally not be given to patients
taking serotonergic drugs
Emergency Situations:
Consider availability of other abx
Stop SA immediately and closely monitor patient for 2
weeks (5 weeks) or until 24h after last linezolid dose
Non-Emergency Situations:
Stop SA at least 2 weeks (5 weeks) in advance
Resume SA 24h after last dose of linezolid
http://www.fda.gov/Drugs/DrugSafety
MSHP Annual Meeting 2017
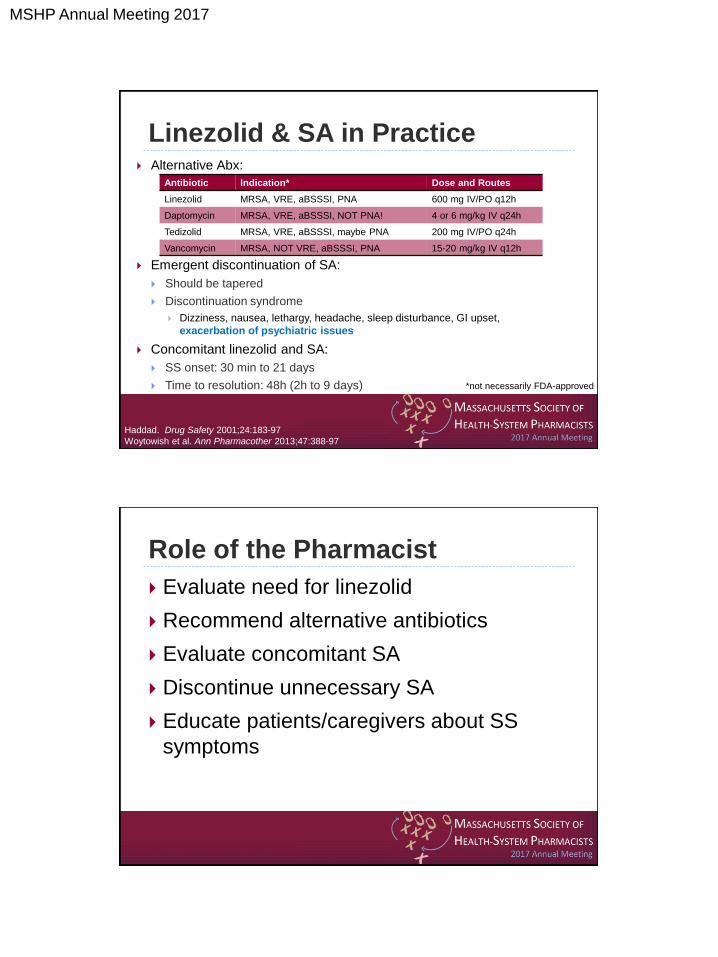
Linezolid & SA in Practice Alternative Abx:
Emergent discontinuation of SA:
Should be tapered
Discontinuation syndrome
Dizziness, nausea, lethargy, headache, sleep disturbance, GI upset,
exacerbation of psychiatric issues
Concomitant linezolid and SA:
SS onset: 30 min to 21 days
Time to resolution: 48h (2h to 9 days)
Antibiotic Indication* Dose and Routes
Linezolid MRSA, VRE, aBSSSI, PNA 600 mg IV/PO q12h
Daptomycin MRSA, VRE, aBSSSI, NOT PNA! 4 or 6 mg/kg IV q24h
Tedizolid MRSA, VRE, aBSSSI, maybe PNA 200 mg IV/PO q24h
Vancomycin MRSA, NOT VRE, aBSSSI, PNA 15-20 mg/kg IV q12h
Haddad. Drug Safety 2001;24:183-97
Woytowish et al. Ann Pharmacother 2013;47:388-97
*not necessarily FDA-approved
Role of the Pharmacist
Evaluate need for linezolid
Recommend alternative antibiotics
Evaluate concomitant SA
Discontinue unnecessary SA
Educate patients/caregivers about SS
symptoms
MSHP Annual Meeting 2017
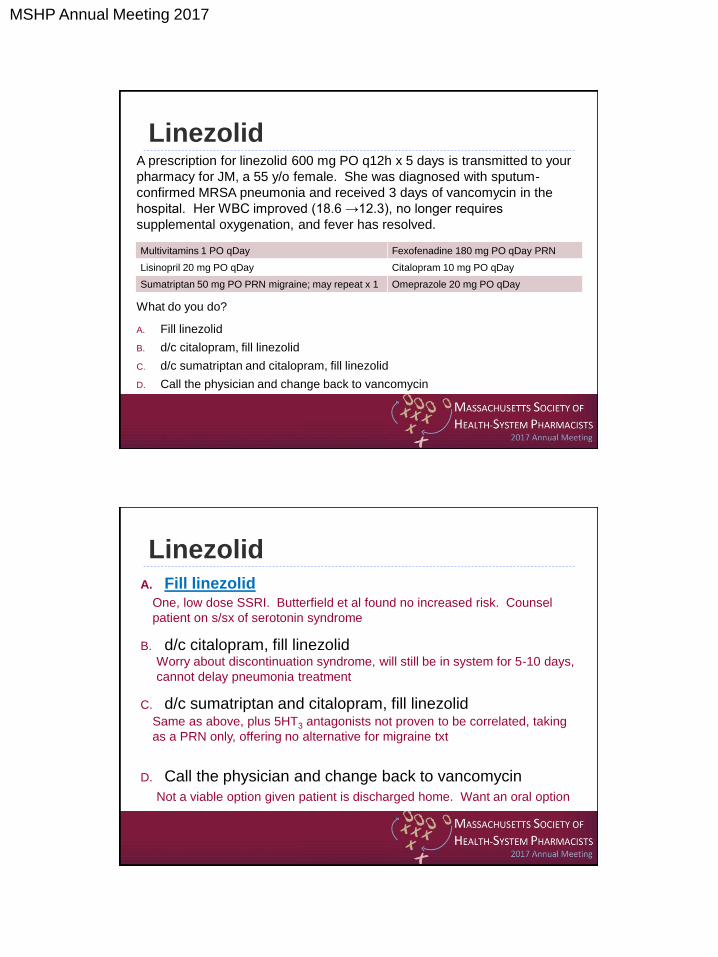
Linezolid A prescription for linezolid 600 mg PO q12h x 5 days is transmitted to your
pharmacy for JM, a 55 y/o female. She was diagnosed with sputum-
confirmed MRSA pneumonia and received 3 days of vancomycin in the
hospital. Her WBC improved (18.6 →12.3), no longer requires
supplemental oxygenation, and fever has resolved.
What do you do?
A. Fill linezolid
B. d/c citalopram, fill linezolid
C. d/c sumatriptan and citalopram, fill linezolid
D. Call the physician and change back to vancomycin
Multivitamins 1 PO qDay Fexofenadine 180 mg PO qDay PRN
Lisinopril 20 mg PO qDay Citalopram 10 mg PO qDay
Sumatriptan 50 mg PO PRN migraine; may repeat x 1 Omeprazole 20 mg PO qDay
Linezolid A. Fill linezolid
B. d/c citalopram, fill linezolid
C. d/c sumatriptan and citalopram, fill linezolid
D. Call the physician and change back to vancomycin
One, low dose SSRI. Butterfield et al found no increased risk. Counsel
patient on s/sx of serotonin syndrome
Worry about discontinuation syndrome, will still be in system for 5-10 days,
cannot delay pneumonia treatment
Same as above, plus 5HT3 antagonists not proven to be correlated, taking
as a PRN only, offering no alternative for migraine txt
Not a viable option given patient is discharged home. Want an oral option
MSHP Annual Meeting 2017
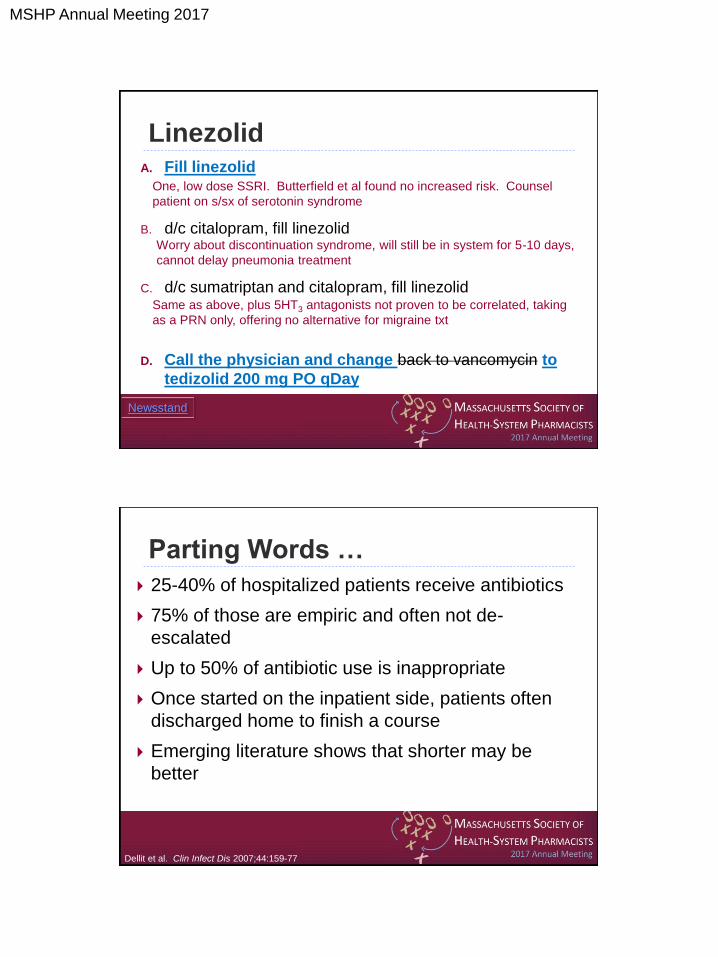
Linezolid A. Fill linezolid
B. d/c citalopram, fill linezolid
C. d/c sumatriptan and citalopram, fill linezolid
D. Call the physician and change back to vancomycin to
tedizolid 200 mg PO qDay
One, low dose SSRI. Butterfield et al found no increased risk. Counsel
patient on s/sx of serotonin syndrome
Worry about discontinuation syndrome, will still be in system for 5-10 days,
cannot delay pneumonia treatment
Same as above, plus 5HT3 antagonists not proven to be correlated, taking
as a PRN only, offering no alternative for migraine txt
Newsstand
Parting Words …
25-40% of hospitalized patients receive antibiotics
75% of those are empiric and often not de-
escalated
Up to 50% of antibiotic use is inappropriate
Once started on the inpatient side, patients often
discharged home to finish a course
Emerging literature shows that shorter may be
better
Dellit et al. Clin Infect Dis 2007;44:159-77
MSHP Annual Meeting 2017
More Parting Words …
Document, document, document
Pharmacist/technician malpractice insurance
available from multiple sources
Affordable
$100-150/year
Always a good idea
Compare to physician: $5,000-10,000/year
In Conclusion
FDA will release warnings and alerts
Contain broad statements and
recommendations
Important to understand the details
Treat each patient and situation as a unique
encounter
It is ok to deviate from FDA recommendations in
patient specific scenarios
MSHP Annual Meeting 2017
Yellow Card: FDA Warnings on
Antibiotics
Monica V. Mahoney, PharmD, BCPS AQ-ID





























