Embed Size (px)
Citation preview

224
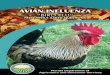
Journal of Avian Medicine and Surgery 17(4):224–234, 2003q 2003 by the Association of Avian Veterinarians
Xenogeneic Grafts Using Porcine Small IntestinalSubmucosa in the Repair of Skin Defects in 4 Birds
Stephen J. Hernandez-Divers, B Vet Med, Dipl Zoo Med, MRCVS, andSonia M. Hernandez-Divers, DVM, Dipl ACZM
Abstract: Trauma and skin defects are common presentations in companion and wild birds. Twobarn owls (Tyto alba), an umbrella cockatoo (Cacatua alba), and an American crow (Corvus bra-chyrhynchos) were presented for varied skin wounds. Porcine small intestinal submucosa was usedas a xenogeneic graft to repair wound defects in each bird. The wounds healed within 6 weeks inall 4 birds, with less intensive wound management than that required for healing by second intention.All birds returned to normal function.
Key words: porcine small intestinal submucosa, xenogeneic graft, wound management, skin, birds,barn owl, cockatoo, crow, Tyto alba, Cacatua alba, Corvus brachyrhynchos
Introduction
The structure of bird skin, characterized by epi-dermis, dermis, subcutis, and feathers, has been ex-tensively reviewed and documented,1 and severalsources exist on the topics of avian dermatology,dermatologic diseases, and treatment.2–6 Captivebirds are often presented for infectious and nonin-fectious dermatoses that require surgical treatment.Common avian traumatic skin conditions includemutilation, keel injuries, gunshot wounds, leg-holdtrap injuries, and entanglement. Skin trauma in thekeel region of psittacine birds is often associatedwith feather plucking, automutilation, and traumaticinjury after severe feather clips.2,3,5,7,8 Keel damageis one of the most commonly observed traumas incaptive bustards in the United Arab Emirates.7
Many keel wounds become chronic, necrotic, andgranulomatous lesions, and some can involve theunderlying keel bone. In raptors, the skin and un-derlying soft tissues of the tarsometatarsus can betraumatized from poorly fitted or damaged jesses.Similar wounds are seen in psittacine birds withtight leg bands.2 In free-ranging birds, trauma as-sociated with vehicular accidents, predation by do-mestic animals, and electrocution9 commonly re-sults in skin lacerations, soft-tissue damage, andbone fractures.
From the Exotic Animal, Wildlife, and Zoological Medicine,Department of Small Animal Medicine and Surgery, College ofVeterinary Medicine, University of Georgia, 501 D. W. BrooksDr, Athens, GA 30602-7390, USA.
Corresponding author: Stephen J. Hernandez-Divers.
Current techniques for the repair of keel injuriesinclude conservative care and surgery. One reportdescribing 15 cases of keel injuries caused by au-tomutilation in psittacine birds indicated that exten-sive surgery was more effective (100%) than wasprolonged conservative treatment (20%).8 Surgeryinvolved resecting the necrotic tissue, elevating andresuturing the superficial pectoral muscles and skin,bandaging the wing or wings, and placing a collarfor 6 weeks.
The progression of wound healing and the man-agement of soft-tissue wounds on the wings of birdshave been described.2 Wound-management tech-niques include preventing further contamination,cleaning the wound, surgically debriding necrotictissue, using topical and systemic antimicrobialtherapy, protecting new granulation tissue, andmanaging delayed wound closure. Additionally,wing injuries often require immobilizing the wingto facilitate bandaging and to prevent excessivemovement that might delay healing.2 Because of thelack of soft tissue on wings, the thin skin of birds,and the importance of tendons such as the tensorpropatagialis,10 wing injuries in free-ranging birdsintended for release must be managed with utmostcare.
Various wound management techniques have beenused in birds with large skin defects. Cutaneous au-tografts have been used successfully in ostriches(Struthio camelus)11 and great horned owls (Bubovirginianus),12 whereas skin flaps have been used inring-necked pheasants (Phasianus colchicus), a rockdove (Columba livia), a red-tailed hawk (Buteo ja-

225HERNANDEZ-DIVERS AND HERNANDEZ-DIVERS—XENOGENEIC GRAFTS IN BIRDS
Figure 1. Initial presentation of wounds on the tarso-metatarsus of a barn owl (case 1). The left jess has beenremoved to reveal a necrotic and ulcerated wound.
maicensis),13 and other raptors.6 Allografts have beenused frequently in chickens (to determine inbreedingcoefficients), with graft survival positively correlatedwith genetic homogeneity.14 A recent publication de-tails the use of skin flaps and grafts in raptors.15
Vet Biosist (Global Veterinary Products Inc, NewBuffalo, MI, USA) is derived from porcine smallintestinal submucosa (SIS) that has been dehydratedand sterilized. This collagen-rich biological meshcontains fibronectin, decorin, hyaluronic acid,chrondriotin sulphate A, and various growth factors.Although only a single case report on the use ofporcine SIS in a raptor exists,15 it has been suc-cessfully used in dogs, cats, rats (Rattus norvegi-cus), and rabbits (Oryctolagus cuniculus) for appli-cations including bladder, muscle, tendon, bloodvessel, cornea, and skin repair.16–23
In this case series, we describe the successful useof porcine SIS as a xenogeneic graft in repairingsevere skin defects in 2 barn owls (Tyto alba), anumbrella cockatoo (Cacatua alba), and an Ameri-can crow (Corvus brachyrhynchos).
Case Reports
Cases 1 and 2
Two captive adult barn owls, both 3-year-oldmales that weighed 495 g and 512 g, were presentedfor examination because of severe left pelvic limblameness. General husbandry and feeding practiceswere considered appropriate for this species. How-ever, in both owls, physical examination revealedlocalized swelling of the tarsometatarsal region witha serosanguineous discharge. These injuries wereassociated with very tight jesses on the left pelviclimbs of both owls (Fig 1). The owner reportedlyhad placed new jesses on both owls 2 weeks earlier,but the poor-quality leather had shrunk to cause thecurrent condition. The owls were otherwise clini-cally normal.
Both owls were managed similarly. Each waspremedicated with butorphanol (1 mg/kg IM; Tor-bugesic, Fort Dodge Animal Health, Fort Dodge,IA, USA) 15 minutes before induction with 4% iso-flurane administered by face mask. A 3-mm inside-diameter endotracheal tube was placed, and anes-thesia was maintained at 1–3% isoflurane with in-termittent positive pressure ventilation every 4 sec-onds (Small Animal Ventilator, Vetronics BAS,West Lafayette, IN, USA). Anesthetic monitoringincluded assessment of reflexes, esophageal pulseoximetry, and ultrasonic doppler over the superficialulnar artery. Lactacted Ringer’s solution (10 ml/kgper hour) was given intravenously during surgeryfor each owl.
The feathers around the jess and in the immediatetarsometatarsal region were plucked, and the jesseswere carefully cut away from both limbs. In bothowls, the left tarsometatarsal region was necroticwith complete circumferential involvement under-neath the jess. The affected limb was prepared foraseptic surgery and draped in a standard manner.All devitalized and necrotic tissue was carefully andsharply dissected. Hemostasis was maintained bybipolar radiosurgery (Ellman EMC Surgitron 3.8MHz, Ellman International, Hewlett, NY, USA).The only noteworthy difference between the 2 owlswas that, because of the soft-tissue damage, theflexor tendon sheath of digits 2 and 3 was visiblein case 1. However, the tendon itself was not dis-rupted. Once the surgical site was ready for graft-ing, a single sheet of porcine SIS was placed insterile saline for 2 minutes to rehydrate the graft.The material was then cut in half to form a doublelayer and laid over the debrided area. The porcineSIS was cut to an approximate size that would per-mit complete circumferential enclosure of the skindefect. The graft was applied with the rough side

226 JOURNAL OF AVIAN MEDICINE AND SURGERY
Figure 2. Suturing the porcine small intestinal submucosa graft to a barn owl (case 2) with a wound similar to thatdescribed in Figure 1. The graft has been secured below the epidermal margin of the distal skin border with absorbablesuture in a simple interrupted pattern.
Figure 3. Surgical site of the barn owl (case 2) in Figure 2 immediately after applying the graft. The small intestinalsubmucosa graft has been sutured around the circumferential skin defect in the tarsometatarsal region.
against the wound, as recommended by the manu-facturer. Starting distally, the graft was tucked underand sutured to the skin with polyglactin 910 (4-0Coated Vicryl, Ethicon, Somerville, NJ, USA) in asimple interrupted pattern. The porcine SIS was
then cut precisely to reach the proximal skin marginand similarly sutured to the skin below the epider-mis (Fig 2). Once suturing was complete, the graftand wound were inspected for integrity (Fig 3) be-fore the graft was covered with silver sulfadiazine

227HERNANDEZ-DIVERS AND HERNANDEZ-DIVERS—XENOGENEIC GRAFTS IN BIRDS
Figure 4. Surgical site of the barn owl (case 2) 1 weekafter surgery. The dark coloration is caused by coagulatedblood and serum within the graft matrix.
Figure 5. Surgical site of the barn owl (case 2) 2 weeksafter surgery. The sutures have started to be absorbed.
cream (Silvadene Cream 1%, Hoechst MarionRoussel, Kansas City, MO, USA), a hydrocolloiddressing (ULTEC Pro Alginate Hydrocolloid Dress-ing, Kendall, Mansfield, MA, USA), and self-ad-hering elastic bandaging tape. Both owls recoveredfrom anesthesia uneventfully and were fed thatnight. A second dose of butorphanol (2 mg/kg IM)was administered 8 hours after the initial dose. Theowls were discharged the next day, and the ownerwas asked to maintain them in a small aviary (2 m3 2 m 3 2 m).
For 3 days after surgery, the wounds were ex-amined and the dressings were changed daily. Ateach bandage change, silver sulfadiazene cream wasreapplied to maintain the porcine SIS in a moistenvironment as directed by the manufacturer. Noevidence of lameness was observed, and both owlscould flex and extend all digits normally. For thenext 8 weeks, the owls were re-evaluated onceweekly. At 1 week after surgery, the grafts wereintact and uninfected (Fig 4). Coagulated blood hadaccumulated to form a dark scab involving the graft.The bandages were permanently removed at this
time. After 2 weeks, the grafts were still intact, andscab involved most of the graft matrix. The arearemained uninfected and the sutures started to beshed (Fig 5). By 3 weeks, all suture material waslost and feather regrowth had begun (Fig 6). At 6weeks, the scabs had been shed to reveal intact skinwith minimal scar tissue and progressive feather re-growth (Fig 7). The wounds were considered healedat this time. At 10 weeks, the owner reported con-tinued feather regrowth and said that little evidenceof the previous injuries was visible.
Case 3
A 6-year-old male umbrella cockatoo, weighing782 g, was presented with a keel injury of 4-monthsduration. The initial injury had been caused by atraumatic landing onto a concrete floor after thebird’s wings were clipped. Previous conservativetreatment including collars and topical medicationshad failed. The cockatoo was frequently observedself-mutilating the area and had caused a secondlesion distal to the original wound. Husbandry andfeeding practices were considered appropriate forthis species.

228 JOURNAL OF AVIAN MEDICINE AND SURGERY
Figure 6. Surgical site of the barn owl (case 1) 4 weeksafter surgery. All the sutures have been lost, and featherregrowth distal to the graft site is evident.
Figure 7. Surgical site of the barn owl (case 2) 6 weeksafter surgery. The scab has been lost, and regeneratedskin with minimal scarring, along with prominent featherregrowth on the graft site, is present.
On physical examination, a 3-cm 3 2-cm gran-ulomatous lesion was visible on the ventral midline,approximately 2 cm caudal to the thoracic inlet. Thesecond lesion, 2 cm 3 1 cm, was located on themidventral border of the right pectoral region (Fig8). Both lesions were well circumscribed and ul-cerated, with dry exudate. The surrounding area wasdevoid of feathers because of self-plucking. Thecockatoo was otherwise clinically normal. Resultsof routine hematologic and plasma biochemical test-ing, as well as dorsoventral and lateral radiographs,did not indicate any other abnormalities.
The cockatoo was premedicated with butorphanol(1 mg/kg IM) and anesthetized in a similar manneras previously described. The entire keel region wasprepared and draped for surgery. The primary le-sion, including a small area of damaged keel bone,was excised with a #15 scalpel blade. A 2-mm mar-gin of normal tissue was removed to ensure com-plete excision. Hemorrhage was controlled by bi-polar radiosurgery. The excision created a large tis-sue defect that could not be closed by conventionalmeans. A single layer of porcine SIS was cut to the
shape and size of the defect and rehydrated in sterilesaline. The graft was then positioned over the de-fect, rough side toward the wound, and sutured tothe skin below the epidermal border with 4-0 poly-glactin 910 absorbable suture (Vicryl, Ethicon) in asimple continuous pattern. The graft was coveredwith silver sulfadiazine cream, and a moisture-per-meable adhesive film dressing (OpSite, Smith andNephew, Largo, FL, USA) was applied to the area.The second lesion, which involved only the skinand subcutis, was surgically resected and the skinwas closed routinely (Fig 9). The cockatoo recov-ered uneventfully from anesthesia and began eatingwithin 1 hour. A collar was placed around its neckto prevent self-trauma of the surgical sites. A sec-ond dose of butorphanol (2 mg/kg IM) was admin-istered 8 hours after the initial dose. The cockatoowas discharged the day after surgery.
The cockatoo was examined 2 and 4 days aftersurgery to inspect the wound and to change thedressing. On each occasion, the dressing and anti-biotic cream were carefully removed and replaced.This procedure was completed without sedation or

229HERNANDEZ-DIVERS AND HERNANDEZ-DIVERS—XENOGENEIC GRAFTS IN BIRDS
Figure 8. Umbrella cockatoo (case 3) with a primarykeel injury and a smaller self-inflicted wound.
Figure 9. Surgical site of the umbrella cockatoo (case3) described in Figure 8 immediately after applying thegraft. The graft was secured, and the surgical wound cre-ated by excising the second smaller lesion was closedwith absorbable suture in a continuous pattern.anesthesia. The graft became progressively darker
over the first week after surgery because of accu-mulated coagulated serum and blood within and un-der the graft matrix (Fig 10). The bandage was per-manently removed at day 6, but the owner was in-structed to apply the silver sulfadiazine cream onthe wound twice daily for another week. By 2weeks after surgery, the graft was intact and unin-fected and all wound treatment ceased. At 6 weeks,the scab was shed to reveal healed integument withno visible scarring, and the collar was removed. Thecockatoo resisted feather picking and self-mutilationof the site and was considered clinically normal at10 weeks after surgery.
Case 4
An American crow in good body condition (500g) was presented for evaluation of a traumatic winginjury presumably sustained during a collision witha vehicle. On examination, the crow was recumbentand depressed and had poor peripheral pulses andpale mucous membranes. A 5-cm long, 2-cm wideskin defect was present on the ventral aspect of theleft wing, and the metacarpal bones were exposed(Fig 11). Small particles of soil and a hemorrhagicdischarge covered the wound. Several other super-ficial abrasions and contusions were present on thehead, pectoral region, and opposite wing. No bonefractures or joint abnormalities were found. Thecrow was treated symptomatically with warmed lac-tated Ringer’s solution (90 ml/kg IV administeredover 20 minutes), dexamethasone (2 mg/kg IM), tri-methoprim-sulfa (60 mg/kg IM), and butorphanol(1 mg/kg IM). The wound was gently flushed witha dilute chlorhexidine solution and rinsed withphysiologic saline. A light wet-to-dry dressing wasapplied and overlaid by a figure-of-eight bandage.
Lactated Ringer’s solution was administered sub-cutaneously 6 hours after admission (60 ml/kg). By8 hours after admission, the crow was standing andwas gavage fed with a nutritional supplement. Thenext morning, the crow was bright, alert, perching,and eating. Treatment with trimethoprim-sulfa andbutorphanol was continued.
Anesthesia was induced with 3% isoflurane ad-ministered by face mask. The crow was then intu-bated with a 3-mm endotracheal tube and ventilatedmanually every 5 seconds during surgery. The ban-dage was removed and the wound was asepticallyprepared. Feathers were plucked from surroundingtissues while avoiding primary feathers, which wereheld away from the surgical site with self-adhesivebandaging tape. Any foreign material was removedfrom the wound. The skin edges of the defect wereidentified, and edges that did not appear viable weretrimmed until hemorrhage occurred. A single layerof porcine SIS was cut to approximate the size ofthe wound and rehydrated in saline. Beginning withthe dorsal edge of the wound, the porcine SIS wastucked under the epidermal edges of the entirewound and sutured in place, rough side toward thewound, with 4-0 absorbable monofilament poly-dioxanone suture (Ethicon) in a simple interruptedpattern. The porcine SIS was trimmed as needed tooverlap approximately 1 mm under the epidermaledges (Fig 12). The graft was covered with tripleantibiotic ointment and a nonadherent dressing. Afigure-of-eight bandage was applied to immobilizethe wing and maintain the dressing in place. Flu-nixin meglumine (1 mg/kg IM; Banamine, ScheringPlough Animal Health) was administered before re-covery. The crow recovered from anesthesia un-

230 JOURNAL OF AVIAN MEDICINE AND SURGERY
Figure 10. Surgical site of the umbrella cockatoo (case 3) 1 week after surgery. The dark discoloration at the graftsite is caused by coagulated serum and blood within the graft matrix.
Figure 11. Ventral aspect of the traumatized left wing of a crow (case 4) after debriding and cleaning the wound.Note the exposed metacarpal bones.
eventfully. After surgery, treatment with trimetho-prim-sulfa (60 mg/kg PO q12h for 10 days) andflunixin meglumine (1 mg/kg IM q48h for 6 days)was continued.
The crow was re-evaluated daily for the first
week and every 2 days thereafter. The bandage wasremoved every other day to inspect the graft andreapply triple antibiotic ointment. The graft ap-peared intact and uninfected throughout the firstweek. At the end of the first week, triple antibiotic

231HERNANDEZ-DIVERS AND HERNANDEZ-DIVERS—XENOGENEIC GRAFTS IN BIRDS
Figure 12. Ventral aspect of the distal left wing of the crow (case 4) described in Figure 11 after applying the graft.
was discontinued and a sterile surgical lubricant wasapplied to prevent graft desiccation. At the end ofthe third week, the graft appeared dark and adheredto underlying granulation tissue. Some sutures onthe ventral aspect had been shed. At this time, thedressing and figure-of-eight bandage were discon-tinued. The crow was discharged to a licensed wild-life rehabilitator with instructions to inspect thegraft 3 times weekly and to maintain the crow in asmall enclosure, which would restrict wing move-ment. By week 7, the rehabilitator reported that thescab had shed and the new epithelium overlying theprevious defect appeared normal. The crow wasplaced in a large aviary intended for flight recon-ditioning. Three weeks later, the crow was flyingnormally and was released into a similar environ-ment from which it came.
Discussion
In this case report series, we present the detailsof the successful use of a xenogeneic graft materialin 4 birds. Skin grafting is often difficult in birdsbecause of the lack of easily harvested skin. PorcineSIS offers a valuable alternative that has beenshown to be both practical and effective. Skin re-construction techniques currently used in veterinarymedicine include long-term wound care and sur-gery.24,25 In avian medicine, wound managementand healing by second intention is more commonlyused than surgical repair.2 The medical management
of avian wounds is similar in many ways to that ofother animals and centers on accurate assessment,wound preparation, and the appropriate use of top-ical medications and dressings.
Common surgical practice for wound repair inbirds has largely been restricted to debridement andprimary closure by standard suturing techniques.2
However, some reports have offered more advancedapproaches to repairing skin defects that involve thecranium, tarsus, and keel regions.8,11,13 Keel injurieshave been repaired by surgically excising diseasedskin, pectoral muscle, and keel bone, then closingthe wound to allow healing by primary intention.8
Postoperative management consists of collars, wingbandages, and examinations every 5–6 days for 6weeks. Dorsal cervical pedicle advancement flapshave been successfully used in a ring-necked pheas-ant, a rock dove, a red-tailed hawk, and other rap-tors.6,11 Postoperative care was minimal and healingwas complete within 2 weeks. Free skin grafts havebeen used in poultry for genetic research and in 2clinical cases involving an ostrich with a tarsalwound and 2 great horned owls.11,12 The ostrich re-ceived a full-thickness meshed skin autograft (takenfrom under the left wing) to cover a skin defect leftby the excision of a large tarsal granuloma. In theostrich, postsurgical wound management was inten-sive, with dressings changed daily for 3 weeks. Thegraft procedure was successful and, despite a local-ized area of rejection caused by focal tenosynovitis

232 JOURNAL OF AVIAN MEDICINE AND SURGERY
of the long digital extensor, complete healing wasreported by 90 days after surgery.11 In the report ofthe 2 great horned owls, the skin graft was har-vested from the inguinal area and the midpropata-gium. In both owls, several sites were needed toharvest sufficient skin, and in 1 owl, an externalfixator was needed to immobilize the graft site onthe foot.12
Skin defects in all species can be repaired withadvancement flaps or free grafts (auto-, allo-, or xe-nografts). Advancement flaps are typically consid-ered the most successful of the 3 procedures be-cause they are easier to apply and an intact vascularsupply to the graft is maintained.24,26 However, be-cause avian skin is thin, skin flaps can be problem-atic in birds; skin is tight over most areas of thebody and thus cannot be easily manipulated forflaps without disrupting vascularity.
Grafts of any kind may fail because of infection,movement between the graft and the tissue bed, flu-id accumulation under the graft, or poor vasculari-zation, usually associated with immunogenic rejec-tion.14,24,25 The use of autografts minimizes this risk.In birds, the main disadvantage of autografts is thepoor availability of excess skin required for har-vesting. In large species, such as the ostrich, full-thickness grafts of sufficient size can be harvestedfrom several areas. However, in smaller birds, thesurgeon may be restricted to areas of freely movableskin such as the neck or the inguinal areas.
The use of grafts from other animals may alle-viate the problem of graft availability, but the ne-cessity of a surgical procedure on a second animalmay be impractical, unethical, or illegal dependingon circumstances and jurisdiction. In addition, hostrejection of the graft is an overriding concern. Al-lografts (grafts from genetically distinct individualsof the same species) have been used in poultry re-search to assess inbreeding, as increasing geneticdiversity increases the likelihood and speed of graftrejection.14 For this reason, xenografts (from ani-mals of a different species) have not been tried clin-ically for fear of immediate rejection.
Porcine SIS has been studied, both in vitro andin vivo, as a multipurpose tissue graft in severalspecies.27–30 Results have indicated that 80% of por-cine SIS venous grafts remain successful and patentafter 6 months, compared with 88% success for au-tografts.27 The success of porcine SIS xenograftscan be related to several characteristics of this bio-scaffold material. The low immunogenicity of por-cine SIS is attributed to glutaraldehyde sterilizationand stabilization which removes surface antigensduring the manufacturing process.28 The typical dis-advantage of such treatment is calcification leading
to poor host-tissue incorporation and mechanicalfailure of the graft. However, studies using a ratsubcutaneous model have shown porcine SIS tocause no implant mineralization and little peri-im-plant fibrosis.28 Porcine SIS also contains variousextracellular and basement membrane factors thatare considered key for successful implantation. Gly-cosaminoglycans (hyaluronic acid, heparin, heparansulfate, chondroitin sulfate A, and dermatan sulfate)are important components of the extracellular ma-trix that have been isolated from porcine SIS. Thesefactors, along with fibronectin, have been linked toantithrombosis and anticoagulation, angiogenesis,rapid neovascularization, cell differentiation andproliferation, organized deposition of collagen, andtissue regeneration.29,30 Although the process is onlypoorly understood, in mammals the graft can be re-modeled and replaced by the host tissue within 90days.27–30 This phenomenon, which depends onmaintaining a moist graft environment for the first7–10 days, would explain the new avian integu-ment, including feathers, observed at the graft sitesin the cases we describe.
Conservative wound management is often pro-longed and is prone to failure or scarring of thearea.2,8 In addition, management is often long termand intensive, requiring frequent handling of pa-tients. Although habituated pet birds typically tol-erate intensive wound management, owners andkeepers may be frustrated by frequent visits to theclinic. The barn owls we describe were habituatedto perching on a gloved hand; however, they werenot accustomed to additional restraint. The crowwas unaccustomed to any form of human contact.The stress associated with frequent handling maynot be tolerated by some species of free-rangingbirds, or it may lead to negative sequelae such asdelayed healing, secondary bacterial or fungal in-fection, or trauma from capture or restraint. Withthe crow, conservative management was not an ap-propriate option because the exposed metacarpalbones necessitated rapid closure of the wound toprevent the bones from desiccating or becoming in-fected. In this case, the porcine SIS graft not onlyprovided a suitable network for wound healing butalso protected viable underlying structures duringthe healing process.
By using porcine SIS, wound healing may be re-duced to 2–6 weeks, depending on the species ofbird, wound characteristics, and technique.8–10 In the2 barn owls and the crow, skin from surroundingareas was not available for primary closure or a skinflap. In the cockatoo, the pectoral musculature couldhave been undermined and closed after surgical re-pair of keel wounds.8 However, that technique re-

233HERNANDEZ-DIVERS AND HERNANDEZ-DIVERS—XENOGENEIC GRAFTS IN BIRDS
quires wing bandaging for 6 weeks, which wasdeemed unsuitable for this cockatoo. Healing oc-curred within 6 weeks in the birds we describe,without the need for wing immobilization which isin accordance with observations made in other spe-cies.16–23,27 All 4 birds returned to normal function.
When used correctly, porcine SIS grafts requirecareful management with topical antibacterial med-ication and bandaging for the first 7–10 days to pre-vent graft desiccation. After that time, bandagingdoes not appear to be crucial. In contrast, healingby secondary intention in the cases described wouldhave required at least 6 weeks of bandaging andsustained wound management.8 No restraint deviceswere necessary for the owls or crow after surgery,but a collar was deemed essential for the cockatooto prevent self-trauma.
Porcine SIS is commercially available as a singlelyophilized sterile sheet, 70 mm 3 100 mm, with ashelf life of 12 months (Vet Biosist). It is convenientto use and, with little practice, is easy to fashion tosuit surgical requirements. The main disadvantageof this product is expense; however, when consid-ered against the alternative costs of long-term con-servative management, the expense of the graft isacceptable. Our success in using porcine SIS in the4 cases we describe indicates that this productshould be considered a potentially valuable xeno-graft material in avian wound management and re-constructive surgery.
References
1. Lucas AM, Stettenheim PR. Avian Anatomy Integu-ment, Parts 1 and 2. Washington, DC: United StatesDept of Agriculture; 1972.
2. Ritchie BW, Harrison GJ, Harrison LR, eds. AvianMedicine: Principles and Application. Lake Worth,FL: Wingers Publishing; 1994.
3. Burgmann PM. Common psittacine dermatologic dis-eases. Semin Avian Exotic Pet Med. 1995;4:169–183.
4. Gill JH. Avian skin diseases. Vet Clin North Am Ex-otic Anim Pract. 2001;4:463–492.
5. Malley AD. Feather and skin problems. In: BenyonPH, Forbes NA, Lawton MPC, eds. Manual of Psit-tacine Birds. Cheltenham, England: British SmallAnimal Veterinary Association; 1996:96–105.
6. Malley AD, Whitbread T. The integument. In: Ben-yon PH, Forbes NA, Harcourt-Brown NH, eds. Man-ual of Raptors, Pigeons and Waterfowl. Cheltenham,England: British Small Animal Veterinary Associa-tion; 1996:129–139.
7. Bailey TA, Samour JH, Naldo J, et al. Causes ofmorbidity in bustards in the United Arab Emirates.Avian Dis. 1996;40:121–129.
8. Hochleithner M, Hochleithner C. Surgical treatment
of ulcerative lesions caused by automutiliation of thesternum of birds. J Avian Med Surg. 1996;10:84–88.
9. Cooper JE. Physical injury. In: Fairbrother A, LockeLN, Hoff GL, eds. Noninfectious Diseases of Wild-life. Ames, IA: Iowa State University Press; 1996:157–173.
10. Orosz SE, Ensley PK, Haynes CJ. Avian SurgicalAnatomy—Thoracic and Pelvic Limbs. Philadelphia,PA: WB Saunders; 1992:111–129.
11. Johnson JH, Schumacher J, McClure SR, Jensen JM.Use of a full thickness autograft on the tarsus of anostrich. J Am Vet Med Assoc. 1994;205:1019–1020.
12. Hannon DE, Swaim SF, Milton JL, et al. Full-thick-ness mesh skin grafts in two great horned owls (Bubovirginianis). J Zoo Wildl Med. 1993;24:539–552.
13. Gentz EJ, Linn KA. Use of a dorsal cervical singlepedicle advancement flap in three birds with cranialskin defects. J Avian Med Surg. 2000;14:31–36.
14. Dietrich HM, Oliveira-Dos-Santos AJ, Hala K, WickG. Skin allograft survival in chicken strains withspontaneous autoimmune diseases. Poult Sci. 1996;75:285–293.
15. Stroud PK, Amalsadvala T, Swain SF. The use of skinflaps and grafts for wound management in raptors. JAvian Med Surg. 2003;17:78–85.
16. Cook JL, Tomlinson JL, Arnoczky SP, et al. Kineticstudy of the replacement of porcine small intestinalsubmucosa grafts and the regeneration of meniscal-like tissue in large avascular meniscal defects indogs. Tissue Eng. 2001;7:321–334.
17. Featherstone HJ, Sansom J, Heinrich CL. The use ofporcine small intestinal submucosa in ten cases offeline corneal disease. Vet Ophthalmol. 2001;4:147–153.
18. Prevel CD, Eppley BL, Summerlin DJ, et al. Smallintestinal submucosa: utilization for repair of rodentabdominal wall defects. Ann Plast Surg. 1995;35:374–380.
19. Prevel CD, Eppley BL, Summerlin DJ, et al. Smallintestinal submucosa: utilization as a wound dressingin full-thickness rodent wounds. Ann Plast Surg.1995;35:381–388.
20. Hodde JP, Badylak SF, Shelbourne KD. The effect ofrange of motion upon remodeling of small intestinalsubmucosa (SIS) when used as an achille’s tendonrepair material in the rabbit. Tissue Eng. 1997;3:27–37.
21. Matheny RG, Hutchinson ML, Dryden PE, et al. Por-cine small intestine submucosa as a pulmonary valveleaflet substitute. J Heart Valve Dis. 2000;9:769–774.
22. Kropp BP, Badylak S, Thor KB. Regenerative blad-der augmentation: a review of the initial preclinicalstudies with porcine small intestinal submucosa. AdvExp Med Biol. 1995;385:229–235.
23. Lantz GC, Badylak SF, Coffey AC, et al. Small in-testinal submucosa as a vascular graft: a review. JInvest Surg. 1993;6:297–310.
24. Pavletic M. Atlas of Small Animal Reconstructive

234 JOURNAL OF AVIAN MEDICINE AND SURGERY
Surgery. Philadelphia, PA: JB Lippincott; 1991:145–259.
25. Swaim SF. Skin grafts. In: Slater D, ed. Textbook ofSmall Animal Surgery. Vol 2. 2nd ed. Philadelphia,PA: WB Saunders; 1993:325–340.
26. Pavletic MM. Pedicle grafts. In: Slater D, ed. Text-book of Small Animal Surgery. Vol 2. 2nd ed. Phil-adelphia, PA: WB Saunders; 1993:295–325.
27. Bell E. Strategy of the selection of scaffolds for tis-sue engineering. Tissue Eng. 1995;1:163–179.
28. Owen TJ, Lantz GC, Hiles MC, et al. Calcificationpotential of small intestinal submucosa in a rat sub-cutaneous model. J Surg Res. 1997;71:179–186.
29. Hodde JP, Badylak SF, Brightman AO, Voytik-HarbinSL. Glycosaminoglycan content of small intestinalsubmucosa: a bioscaffold for tissue replacement. Tis-sue Eng. 1996;2:209–217.
30. McPherson TR, Badylak SF. Characterization of fi-bronectin derived from porcine small intestinal sub-mucosa. Tissue Eng. 1998;4:75–83.