Embed Size (px)
Citation preview

Joint Royal College of Anaesthetists and Royal College of Surgeons of England WTD 2009 Project
The Royal College of
Anaesthetists
The Royal College of
Surgeons of England
WTD - Implications and Practical Suggestions to Achieve
Compliance
WTD - Implications and Practical Suggestions to Achieve Compliance
Contents1. Foreword .......................................................................................................................... 12. Statement of endorsement .................................................................................... 23. Preface ............................................................................................................................. 34. Executive summary ................................................................................................... 4
4.1. Key findings and recommendations ....................................................................45. Introduction .................................................................................................................... 76. Findings and suggestions ....................................................................................... 8
6.1. Patient safety ...................................................................................................................96.2. Training .............................................................................................................................106.3. Delivery of service ....................................................................................................... 126.4. Engagement with management ......................................................................... 17
AppendicesAppendix A: Project method...................................................................................... 19Appendix B: Joint RCoA/RCSE WTD 2009 Project questionnaire .......... 21Appendix C: Panel membership and acknowledgements ........................24Appendix D: Assessment criteria for case studies ......................................... 26Appendix E: Educational approval of posts ....................................................... 30Appendix F: References and useful links ............................................................. 31
1
WTD - Implications and Practical Suggestions to Achieve Compliance
Foreword1. The patient liaison groups of the Royal College of Anaesthetists and the Royal College of Surgeons of England welcome this report, which proposes some possible solutions for planning 2009 Working Time Directive (WTD) compliance.
Achieving the highest standards of patient safety and quality of care must be at the heart of planning to achieve compliance with WTD. These principles must underpin all proposed solutions to the 48-hour restrictions.
While patients will appreciate the need to be treated by doctors who are not exhausted from working long hours, they will also want to be assured that the doctor treating them is appropriately trained and supervised. Patients would not wish to see the training of junior doctors compromised by the need for compliance with the WTD; this would not be in their best interests in the longer term.
It is recognised that achieving compliance could create the need for long-term structural changes in service delivery. Patients will want to know that delivering the highest standards of patient safety and care will continue to provide the rationale for decisions to reconfigure the way care is delivered rather than expediency on the part of the NHS in achieving compliance.
Patients will need to be reassured that the different solutions chosen by their local hospital will uphold levels of quality and safety and that the solutions taken on will be subject to rigorous audit, ensuring that only the best solutions are adopted in the longer term.
The WTD is enshrined in health and safety law. It would be a mockery if its implementation merely succeeded in giving rise to a whole new set of risks to patient and doctor safety and the quality of care. This report suggests solutions that are both realistic and have the patient’s wellbeing at their core. We hope it will be of use to you in achieving compliance.
Anne Murray Lay Chair Patient Liaison Group, RCoA
Lesley Bentley Lay Chair
Patient Liaison Group, RCSE

WTD - Implications and Practical Suggestions to Achieve Compliance
2
Statement of endorsement2. Anaesthetists and Surgeons are unique in the service they bring to the medical profession; both are craft specialties with training pathways based primarily on apprenticeship of trainees. Achieving compliance with the Working Time Directive (WTD) raises serious concerns over how training can be achieved in order to deliver the highest standards expected by patients.
We have seen that creating compliant rotas can be fairly straightforward, but ensuring rotas also maintain patient safety and continuity of care, provide the opportunity for appropriate training, ensure a suitable work/life balance for doctors and maintain required levels of service delivery is much more difficult.
We recognise that any currently proposed solution is likely to be partial and that the WTD is still likely to impact on patients and practitioners.
We present this report which provides key recommendations and practical solutions that have been successfully tried and tested in some Trusts in England and Wales. These are endorsed by the Royal College of Anaesthetists and the Royal College of Surgeons of England.
The timescale for WTD implementation is very short. We hope that this report will provide help in planning for August 2009 compliance and that it will contribute towards the successful implementation of such plans.
Dr Judith A Hulf President, RCoA
Mr John Black President, RCSE
3
WTD - Implications and Practical Suggestions to Achieve Compliance
Preface3. The Royal College of Anaesthetists and the Royal College of Surgeons of England have long been concerned about the impact of shortened working hours under the WTD on patient safety, training and service delivery. While the colleges support the patient and doctor safety aspect of the legislation, which is in itself enshrined in health and safety law, evidence suggests that the method of implementation thus far has, in some cases, been of detriment to the craft specialties of anaesthesia and surgery.
In January 2008 the two colleges embarked upon a joint project, funded by Skills for Health - Workforce Projects Team, to identify practical solutions to the WTD that would take into consideration the need to protect patient safety, maximise training opportunities and preserve levels of service delivery.
This report presents our findings and provides key recommendations and examples of strategies that have been successfully implemented by hospitals around the country. We acknowledge that there will be different aspects to take into consideration and recognise that many solutions will have an impact on other services.
We would emphasise the very short lead time that NHS trusts now have to become compliant. We hope that this report will assist in this regard and ensure that patient and doctor safety is maintained while securing the highest standard of training for future generations of surgeons and anaesthetists.
Professor Michael Horrocks WTD Council Lead, RCSE
Dr E Anne Thornberry WTD Council Lead, RCoA

WTD - Implications and Practical Suggestions to Achieve Compliance
4
Executive summary4. The project aimed to identify the solutions implemented by those trusts that reported compliance and to allow a selection of trusts that were not yet compliant to consider the practicality of the identified solutions for their own circumstances. The ultimate aim was to try and provide a broad and flexible set of solutions that enjoyed support from both colleges and key stakeholders to help with the implementation of the WTD. There are difficulties in achieving this aim as there is no single easy answer to becoming compliant; however, these solutions are suggested as the most practical and useful.
This project was overseen by a governance board, which directed the project through its various phases and was co-chaired by Council representatives from both colleges. Its objectives were achieved by using questionnaires, structured interviews, working groups and expert panels to obtain and validate information upon which to base advice and support for craft specialty compliance.
Further details of the methodology can be found in Appendix A.
Key findings and recommendations4.1. Both colleges believe that the implementation of the WTD is in serious danger of having a deleterious effect on medical training, patient safety and service delivery. We would like to have seen a more flexible approach to the implementation of this working time legislation in order to protect training programmes, ensure patient safety and achieve a sensible work-life balance. In particular the rigidity of SiMAP1 and Jaeger2 rulings, whilst offering some protection, have significantly hindered planning and successful implementation for compliance.
SafetyPatient safety is paramount. It must be recognised that ensuring patient •safety while becoming WTD 2009 compliant will require significant planning and incur considerable cost. Hospitals must accept these costs to ensure patient safety.

5
WTD - Implications and Practical Suggestions to Achieve Compliance
TrainingThe impact of the WTD on training is considerable. Ensuring continued •excellence in medical training is likely to require reorganisation of the whole programme of training. This could lead to a separation of training and service commitment and the impact of this will require significant planning and funding.
The separation of elective and emergency surgical care was reported •to maintain the quality of patient care and also facilitate training in some specialties, provided it was properly resourced and managed.
There was evidence that a properly resourced Hospital at Night team with •appropriate levels of cover contributed to an increased rate of compliance for surgery.
Full shifts and overnight duties for trainees result in a significant reduction •in daytime training opportunities. Where possible, higher surgical trainees should not be required to work at the hospital overnight unless there are specific training opportunities.
A large number of young doctors have been employed in new posts, without •training approval, in order to achieve compliant rotas. Although advertised as training positions, many of these posts are short term, with no career prospects for the doctors. The employment of young doctors, using short-term contracts outside training programmes, was universally condemned.
Delivery of serviceMany respondents reported that they had increased trainee numbers in order •to become compliant. This is not a long-term solution to the problem and is extremely unlikely to be successful due to the shortage of available junior doctors. In addition, there is strong evidence of a mismatch between supply and demand for trained doctors and so increasing trainee numbers is likely to make this problem worse.
Shortened hours have reduced the availability of trainees to support service •delivery. This will have an inevitable consequence on the workload of consultant staff. Job plans will need to be adjusted to reflect this increased workload and the required compensatory rest periods. It is inevitable that consultant expansion will be required to achieve compliance and to deliver the service volume required. Equity and agreement across the consultant workforce within a unit is desirable to successfully introduce new consultant patterns of work.
An increase in the consultant workforce is the only solution that will provide •long-term stability in hours compliance, patient safety and provision of good quality training.
Nurse practitioners (in surgery) and physicians’ assistants (anaesthesia) •are useful roles and can be used to reduce the workload and free up junior doctors for training opportunities during the day. However, these posts are not a solution to WTD compliance as they require close supervision by a competent doctor.
The implementation of WTD 2009 may contribute to the need for •reconfiguration of services. Not all hospitals will be able to continue to provide a full range of elective and emergency services. Careful strategic planning will be needed in the reorganisation of such services.

WTD - Implications and Practical Suggestions to Achieve Compliance
6
Engagement with managementHospital compliance with WTD 2009 in both anaesthesia and surgery was •found to be very poor. Many of the non-compliant hospitals did not appear to have an agreed and costed plan in place to achieve compliance by August 2009.
Where compliance had been achieved this was principally as a result of •increasing medical staff and/or rota redesign.
Barriers to achieving compliance were mainly a combination of financial •restrictions and staff reservations. These reservations were largely due to concerns about patient safety and medical training.
Where hospitals were compliant there was evidence of active engagement •with senior management within a WTD planning group. This group appeared to work best when it included a senior medical person (eg medical director), a senior manager from HR, a member of the finance team and a range of clinicians involved in delivering health care including trainees.
Where hospitals reported non-compliance it was clear that in many cases •senior management staff were not engaged in the process.

7
WTD - Implications and Practical Suggestions to Achieve Compliance
Introduction5. The European WTD was originally introduced in October 19983 and is now enshrined in UK health and safety legislation. The directive imposed a limit on the average weekly working time and a limit on night workers’ average working time as well as a requirement to offer health assessments to night workers, prescribe minimal daily and weekly rest periods and to ensure rest breaks at work. The WTD has applied to all consultant and career grade staff since October 1998. Individual doctors can opt out of the working hours restriction placed by the WTD but they cannot opt out of the rest requirements.
As doctors in training provided a large service commitment to the NHS it was recognised that a phased approach would be required to bring them in line with other professions. By August 2004 doctors in training were restricted to an average of 58 hours per week and this was subsequently reduced to 56 hours per week in August 2007. In August 2009 there will be a further reduction to a maximum of 48 hours per week, averaged over a 26-week reference period. Trainees also have to comply with New Deal regulations.4 This poses a huge challenge in both anaesthesia and surgery.
Compliance with the WTD is a legal requirement and health and safety laws can be enforced by the Health and Safety Executive (HSE). The difficulty in achieving compliance has been compounded by two rulings made by the European Court of Justice:
The SiMAP rulingi. 1 means that doctors who are on call at the hospital are deemed to be working even if they are asleep; and
The Jaeger judgementii. 2 on compensatory rest means that a rest period must be taken as soon as possible after the period of work from which it is generated.
In the UK, employers who breach WTD requirements can be penalised by the HSE under health and safety legislation or via an employment tribunal where an employee brings a complaint about their working hours. If successful, the complainant could be awarded compensation. As employers, hospitals must take reasonable steps to obey the law. On inspection of premises, HSE inspectors can issue improvement notices and failure to comply with these can lead to a conviction. This could mean a summary conviction in a magistrate’s court with a maximum fine of £5,000 per breach or, if convicted on indictment in a Crown Court, could lead to an unlimited fine for the trust. The EU may take steps to prosecute member states if they are found to be in breach of the directive.
Anaesthesia and surgery are unique high-risk craft specialties and training for these specialties involves the development of advanced technical skills. These are taught using an apprenticeship model. It takes time for such competencies to be acquired and the level of consultant supervision in the early years of training is consequently very high. Sub-specialty interests require further specialised training. Although the individual problems related to each specialty are different, many of the principles are the same.
WTD - Implications and Practical Suggestions to Achieve Compliance
8
Findings and suggestions6. From the questionnaires and interviews it was identified that levels of compliance with August 2009 requirements were low and, worryingly, most trusts that were not compliant reported having no costed and agreed plan in place to become so. It was also found that this lack of planning was pronounced in small to medium-sized trusts.
It had taken an average of 6-12 months for trusts to become 48-hour compliant. This included planning and implementing new or adapted rotas and troubleshooting any problems that arose. Most hospitals that claimed to be 48-hour compliant had become so in the last 18 months, which was too short a period to have carried out evaluation or audit of implications and effects on performance and patient safety. However, no respondent was able to cite any adverse patient safety incident directly related to the reduction in hours.
From the structured interviews it was apparent that those hospitals that had achieved compliance enjoyed the support of senior management.
As a general rule, compliant hospitals had a recognised clinical and/or administrative lead for WTD compliance. Many had a dedicated committee established to achieve trust-wide compliance. The opposite appeared to be true for hospitals that were not yet compliant and it was apparent that in most cases senior management did not seem to be engaging with the process. When the project team chased non-respondents to the questionnaire it was common to find that there was no identified contact for WTD.
Surgical specialties that had achieved compliance had generally done so independently of other surgical departments. There seemed to be little communication across surgery.
From the given list (Appendix B) the most popular solutions implemented were increasing medical staff and rota redesign. The most commonly cited barriers were financial restrictions, staff resistance to change in working patterns and the perceived deterioration of training. The solutions and barriers identified were common across anaesthesia and surgery.
Consultants and registrars in both specialties commonly reported that they were required to take on additional service level work as junior trainees were now less experienced or absent. Although service commitment is necessary it should not detract from training.
Trainees agreed that work-life balance in most cases had improved albeit at the expense of their training. Many still came in to the hospital outside of their rostered hours to gain extra experience. In addition, they reported that working conditions had generally improved with trainees saying they were less fatigued and HR recording that in some cases sickness levels had reduced.
All trainees and consultants interviewed had concerns that trainees were gaining less exposure to training opportunities than an equivalent trainee before the reduction in hours.

9
WTD - Implications and Practical Suggestions to Achieve Compliance
Patient safety6.1. The surveys and interviews found no evidence of increased patient safety incidents but respondents were clearly concerned about the negative effects on patient safety of reduced doctors’ hours. Patient safety must be at the centre of changes made to achieve compliance.
Continuity of care6.1.1. There was widespread concern throughout the project at the lack of continuity of care as a result of decreased hours and the increased number of handovers. This was felt to have a negative impact on training. Trainees were less likely to see patients through their care pathway and therefore could not learn how the impact of their management may have affected patient outcome.
Handover6.1.2. A direct result of reduced working hours is an increase in the number of handovers required and the increased opportunity for error that this presents. It should be noted that throughout the project no respondent could cite any specific example of negative repercussions caused by handover errors. There was, however, widespread concern about this issue.
When correctly structured and organised, handovers can be an invaluable training resource and need not impact negatively on continuity of care.5 A project sponsored by Skills for Health - Workforce Projects Team at Salisbury NHS Foundation Trust has developed software that can be used in planning handovers that is strongly recommended.6
Cross-cover6.1.3. Cross-cover has been defined in this project as a doctor or team of doctors from one specialty providing cover across one or more specialties as well as their own, typically during the out-of-hours period (eg Hospital at Night).
The specialist advisory committees in surgery have stated that there is to be no cross-cover between surgical specialties within ST3-8.7 Senior trainees in one specialty may not have sufficient competence in clinical decision making or operative skill in another specialty. Cross-cover within a specialty is acceptable.
Cross-cover at junior trainee level can be useful although it would depend on the intensity of work and appropriate supervision. If cover across specialties by junior trainees is planned, then well written protocols are needed and good induction and training on the use of these protocols is required.
It was agreed that cross-cover was not appropriate for anaesthesia and critical care services.
Named consultant6.1.4. Both colleges feel strongly that patients should be under the care of a named consultant and, if going to theatre, a named consultant anaesthetist. Whenever possible the patient should remain under the care of the same consultant for each admission.

WTD - Implications and Practical Suggestions to Achieve Compliance
10
Training6.2. There was universal concern about the tension between providing adequate training and the necessities of service provision. Trainees on an approved training programme should not be used to ‘prop up’ the service requirements of the NHS. It is acknowledged, however, that a sensible measure of service provision is of educational value.
It was agreed that there needed to be a change in attitude and culture towards training so that a viable and supported training pathway can be provided for all trainees. It was recognised that there needed to be better utilisation of all training opportunities.
See Appendix E for information on educational approval of posts.
Increasing training opportunities6.2.1. Twilight and weekend sessions
Consultants working twilight sessions have been shown to reduce night-time emergency surgery so that only absolutely essential operating is done after 10pm when staffing can be reduced to a minimum. These twilight sessions can increase training opportunities by allowing trainees to be on call from home or, in some circumstances, by taking trainees off the rota altogether after 10pm, leaving a consultant-only service overnight. This only works satisfactorily when consultants in both anaesthesia and surgery participate equally in this initiative. Scheduled trauma and emergency lists over the weekend and consultant-led fracture clinics have a similar effect. For these to contribute to WTD compliance there needs to be a multidisciplinary commitment, with appropriate theatre staffing support.
Gaining experience in emergency cover6.2.2. Hospital at Night
It was felt that a well managed and resourced Hospital at Night (H@N) system could have a favourable impact on helping to achieve compliance for surgery. It was acknowledged that H@N was primarily service orientated. Although trainees gain some experience at night as part of the H@N team, the majority of valuable training opportunities occurred during the day.
NCEPOD lists
The principles of the National Confidential Enquiry into Patient Outcome and Death (NCEPOD) are immutable. Full-shift working is not a reason for operating unnecessarily at night.
Emergency experience in the first year of anaesthetic training can be obtained by working with consultants during the day on NCEPOD and trauma lists or, in some cases, by working a twilight shift.
11
WTD - Implications and Practical Suggestions to Achieve Compliance
Blocks of emergency and elective experience
Separating emergency and elective care can greatly assist with WTD compliance where trainees undertake modular blocks of training in both elective and emergency care.8 This may entail trainees working in excess of the 48 hours per week for their emergency blocks but reducing their hours of work during elective modules, thus averaging 48 hours per week over the reference period.
It is strongly recommended that separate teams are designated to handle elective and emergency cases. The emergency team should be led by a consultant with appropriate support. If surgical trainees are able to follow a consultant through their on-call rota, and rotate through emergency and elective cases with the same consultant, this creates a surgical team. Good practice would be for the entire team to rotate between electives and emergency services.
This solution is attractive for trainees as their on-call commitment is concentrated into a short timeframe. However, it does mean that trainees can only take annual leave or study leave during the elective period, which consumes valuable daytime training opportunities.
Supervised training and protected teaching6.2.3. Both colleges have provided guidance on standards and numbers of supervised training sessions (Appendix F). These are agreed principles and competency should be based on quality and be appropriate to the curriculum.
The Royal College of Anaesthetists sets a standard of an average of three sessions of supervised training per week, plus some structured teaching.9 The surgical royal colleges’ Joint Committee on Surgical Training is in the process of publishing a document outlining recommended standards for training.10
Adequate structured teaching is possible within the recommended minimum of 1:8 on a full-shift rota. However, a proactive approach is required to ensure trainees can attend.
Trainees often commented that they were unable to attend structured teaching sessions as compensatory rest requirements meant they were unavailable. In order to enable trainees to participate in protected teaching time, different solutions can be considered. Those that had been successfully modelled included:
duplicating structured training twice in a week to ensure all trainees •can attend;
arranging whole days of teaching on a less frequent basis; and•
rotating the day of teaching to maximise possible attendance.•
It is essential that the requirements for medical training are fully recognised by trust management and that these are taken into account when planning rotas. There was evidence that arrangements for on-call rotas had resulted in reduced opportunities for training. Both colleges feel strongly that proper training must be maintained to ensure high standards in the future.
WTD - Implications and Practical Suggestions to Achieve Compliance
12
Delivery of service6.3.
Increasing the workforce6.3.1. Many respondents reported an increase in medical staffing in order to achieve compliance. It was not always clear from the data gathered at which grade additional staff had been employed, nor whether additional posts had received educational approval or were purely service posts. (See Appendix E on educational approval of posts.) There are limited numbered national training posts available and limited capacity to train. In addition, the pool of staff from which service grades have been employed is now significantly diminished. Increasing these medical staff is not a viable and sustainable solution.
Trainees in educationally approved training posts
It is not feasible to plan to increase national training numbers (NTNs) to provide WTD solutions. In anaesthesia there is a limit to the training capacity of schools of anaesthesia and in some deaneries there are insufficient applicants to fill all the NTNs currently available.
The number of NTNs available in surgery was increased in 2008 to accommodate the senior house officer bulge but the NHS Workforce Review Team has recommended a reduction in training numbers not only in general surgery and trauma and orthopaedics but also in urology and otorhinolaryngology. Doctors in posts who do not have an NTN are not eligible for a Certificate of Completion of Training.
Non-consultant service posts
Many compliant hospitals have increased the number of staff and associate specialist (SAS) doctors, trust doctors and clinical fellow posts. Most of these posts are not recognised for training but do require some element of training, supervision and provision of continuing professional development. The level of service these doctors can provide depends on the individual’s level of competence.
Over half of non-compliant hospitals reported that they were planning to increase SAS/service-grade appointments to solve the WTD challenge. This is no longer a viable option in anaesthesia as there are insufficient doctors available for recruitment.
In surgery it has been suggested that the new specialty doctor contract may have the effect of expanding the pool of doctors wanting these types of post but doubt was cast on this as a solution.
Use of research fellows
Research fellows in post can be asked to contribute to out-of-hours service work to a limited extent, eg covering a fixed night or day on the rota. An example in anaesthesia includes providing long day cover at weekends. This may provide good opportunities to increase their clinical exposure and maintain their skills and can also supplement the salaries of those doing research without compromising research time.

13
WTD - Implications and Practical Suggestions to Achieve Compliance
Medical training initiative
Non-EU doctors can apply for fixed-term training opportunities for up to two years.11 These posts are not numbered but may provide a level of training that these doctors could not otherwise access. Funding is at trust level. It is acknowledged that the initial application is highly bureaucratic, however, once in place, the process should get smoother and it may be possible to develop ongoing rotations. This does depend on a hospital’s training capacity.
Consultants
Appointing additional consultants is the principal solution for maintaining service provision and training. While this is an expensive option that requires careful negotiation and job planning, it has the advantage of providing a long-term solution and safeguarding patient safety.
Resident consultant cover overnight is not normally appropriate for the surgical specialties although it is a reality for some consultant anaesthetists, especially in intensive care medicine. While consultants can opt out of the working hours limits of the WTD by signing a waiver with their employer, they must still adhere to the rest requirements laid down in the legislation. Therefore, consultant cover will require a well negotiated job plan. For this to be successful equity and agreement is required across all consultants within a department with some provision for recognising that as consultants age they become less able to fulfil out-of-hours commitments.
Locums
Any solution that depends on locums is very stressful and expensive and should not be relied upon. Both colleges strongly discourage the use of locums to support WTD compliance.

WTD - Implications and Practical Suggestions to Achieve Compliance
14
Reducing tiers of cover6.3.2. A common solution advocated by compliant hospitals is reducing the number of tiers of cover out of hours. Several hospitals have audited the workload out of hours and by expanding the daytime emergency and trauma cover have reduced the requirement for overnight surgery and where emergency surgery does take place it is done by consultant anaesthetists and surgeons. This is a particularly useful model in smaller hospitals. It has the added advantage that very sick patients who cannot wait for surgery are anaesthetised and operated on by consultants, as recommended by NCEPOD.12 In the examples reviewed, the time when the consultant cover began varied between 8pm and midnight.
In anaesthesia, ST1 trainees have been removed from the on-call rota and ST2 trainees have contributed to the obstetric and intensive care rotas with more senior trainees. Careful audit of trainee logbooks is required to ensure they achieve a balanced case mix to support their training needs. Similarly, some hospitals have included surgical ST2s on middle-grade rotas. Although useful, this needs to be competency based. There are real concerns that reducing tiers of cover increases the burden on the intensive care team, which is increasingly being asked for support despite already being heavily committed.
With the reduction of tiers of cover, one possible solution is to increase the number of consultants on call at any one time in order to reduce the workload of each individual consultant. It is unlikely this is an appropriate solution for surgery but may be a possible solution for anaesthesia in large hospitals.
Role substitution6.3.3. Role substitution in this project has been defined as extending the roles of nurses and other non-medical health care professionals to free up doctor time.
It was agreed that use of nurses and other non-medical health care professionals was not appropriate for anaesthesia and intensive care medicine and would not assist with WTD compliance. Physicians’ assistants (anaesthesia) may be present on call but cannot practise independently. They are, however, valuable members of the workforce and can help by undertaking routine lists under supervision, thus freeing trainees to be allocated to the most appropriate lists for their training needs.
Advanced critical care practitioners, a new role, are few in number at present in the UK. The potential advantages include a stable, highly trained workforce able to support the medical team in a new way of working in critical care. However, as they will take at least two years to train, this is not currently a realistic solution but one worth considering for the future.
Use of nurse practitioners in some surgical specialties, particularly trauma and orthopaedics, has proved beneficial. However, it should be noted that although nurse practitioners can be used to reduce the intensity of a surgeon’s workload, they cannot replace the need for a surgeon to be present. Use of nurse practitioners is not appropriate for every specialty.

15
WTD - Implications and Practical Suggestions to Achieve Compliance
Examples where nurse practitioners had been successfully used included:
ward cover to help the F1 tier;•
a morning paediatric trauma clinic to reduce workload and increase •efficiency;
supporting the general surgery and trauma and orthopaedics •generic rota and helping to support the four-hour A&E wait; and
peri-operative care.•
Nurse practitioners work well from protocols and provide a more stable workforce. They can provide good triage, particularly when ‘patient-at-risk scoring’ is used.
It is important to note that use of nurse practitioners should not weaken the traditional nursing model. Care needs to be taken to ensure that nursing duties are not compromised if nurses are being taken out of their rotas to help doctors.
H@N and Taking Care 24:76.3.4. There was general support for well established and managed H@N programmes.
‘Taking Care 24:7’ is a model that is currently being piloted by Skills for Health - Workforce Projects Team.13 This group of pilots is looking at new ways of working for health care services over the full 24-hour day by taking the principles of H@N and using them during the day. The aim is to support health care organisations across the NHS to refocus ways of working and use different staffing models to reduce the dependence on junior medical staff.
Rota design6.3.5. Good rota design is essential to achieving compliance. There are many useful resources on designing rotas from both colleges and software packages have been developed. For a list of resources see Appendix F.
There is good evidence that the incidence of clinical errors increases exponentially with the number of days on call.14,15 Ideally, no more than four consecutive days or nights continuous on call should be rostered. Neither college condones working seven consecutive days or nights. Small units/specialties may benefit from working single nights.
Full-shift rotas for senior trainees are not recommended, except where training opportunities are available at all hours.
A 1:8 rota is the minimum to be able to include prospective cover and adequate training. A 1:10 rota allows for more flexibility and training opportunities but it is acknowledged that many of the smaller specialties will be unable to achieve this.
It is important to build annual leave and study leave into rota plans. Running the minimum number required will create difficulties as leave, novices, recruitment problems, etc will immediately cause a breach.

WTD - Implications and Practical Suggestions to Achieve Compliance
16
If there are fewer people on site at night, additional cover can be provided with an individual working non-resident on call from home. This can be useful in specialised units that occasionally need an extra pair of hands. Non-resident on-call rotas should ensure that rest requirements can be met on 75% of occasions.4 Having an on-call rota and no resident may be a good solution for a small hospital but the on-call doctor needs to be able to get to the hospital within a reasonable time.
Depending on the level of emergency admissions to the specialty, it may be appropriate to have the consultant on call from home, with senior specialist trainees either resident or non-resident first on call and foundation year and/or CT1-2 trainees on site to provide cover overnight. Specialties/units with a high emergency admission rate might benefit from having the consultant on site during the out-of-hours period. Hospitals will need to profile their activity to decide whether this is a feasible option.
Reconfiguration of services6.3.6. Reconfiguration is the re-organisation of services within a given region or trust. This may involve separating emergency and elective care into ‘hot’ and ‘cold’ sites, moving services from one location to another, opening or closing services, or changing referral patterns.
Certain trusts will wish to critically examine the services they provide to make the best use of resources and this may involve major reconfiguration. This will be difficult to achieve by August 2009 because of political sensitivities, lengthy consultation processes and the knock-on effects of change on other services. However, incremental reconfiguration of services may be achieved in the meantime.
Patients should be reassured that the delivery of the highest standards of patient safety and care is the guiding principle in any decision on reconfiguration.
Examples of reconfiguration from the project included:
Separating emergency and elective care
A well managed separation of elective and emergency care can reduce cancellations, achieve a more predictable workflow, provide excellent training opportunities, increase senior supervision of complex or emergency cases and therefore improve the quality of care delivered to patients.
Acute assessment units
Assessment units can provide a dedicated, centralised area where acutely ill patients can be assessed and monitored prior to being admitted to the hospital or receiving appropriate treatment. They can provide speedy access to assessment, diagnosis and treatment, and avoid unnecessary admissions. Assessment units also provide a supportive teamworking environment for trainees and the opportunity for them to gain experience of the entire pathway of care.

17
WTD - Implications and Practical Suggestions to Achieve Compliance
Networking services
Trusts could investigate the possibility of networking both within and outside their organisational boundaries in order to provide patient care in a safe and WTD-compliant manner. For example, a trust may transfer its inpatients to a neighbouring hospital over the weekend to ensure continuity of care and maximise the competencies and availability of staff. Trusts could also rotate acute on-call duties among several hospitals but this requires good planning and transfer protocols. There are examples of service reconfiguration into confederated units, especially in the smaller surgical specialties. These include managed clinical networks where inpatients are admitted to a single ‘hub’ hospital (unless their condition precludes transfer) with day care surgery and outpatient clinics undertaken at a number of ‘spoke’ units. Innovative arrangements are required to ensure maximum utilisation of staff and resources while ensuring safe and timely treatment for patients and an appropriate work-life balance for staff.
NCEPOD lists
NCEPOD recommends that only operations for life- and limb-threatening conditions be conducted after midnight, thus minimising the requirement to operate at night. Many hospitals provide an NCEPOD theatre during normal working hours but there is good evidence that extending the availability of these during twilight hours and, where necessary, increasing their number is an efficient way of dealing with the majority of urgent and emergency work.
Engagement with management6.4. There were concerns that very few non-compliant hospitals had costed and agreed plans to achieve compliance. This section highlights some of the systems that compliant hospitals had in place to assist in implementing the WTD.
Leadership6.4.1. Safe patient care and employee safety is paramount. Support for achieving WTD 2009 compliance needs to come at trust level and from senior management. It may be particularly helpful to have a champion on the hospital board. Trust quality boards should also take a keen interest in the implementation of WTD compliance and its effect on patient safety.
Hospitals that had achieved 2009 compliance had enjoyed support and input from senior management and had an identified clinical and/or administrative lead in place. Several trusts had appointed an administrative WTD coordinator or project manager to coordinate the process across the trust and support clinicians.
The colleges and expert panels (Appendix A) strongly endorsed the formation of a committee dedicated to WTD planning and implementation at trust level. Engagement between consultants, trainees, senior staff, HR/medical staffing and finance departments is essential. It might also be useful to have a lay member/patient representative on this committee. It is important that trainees are engaged throughout the process.

WTD - Implications and Practical Suggestions to Achieve Compliance
18
It is not the college tutor’s responsibility to achieve compliance. The responsibility begins with the chief executive of the trust and through the management line to the medical director and clinical director.
Finance6.4.2. WTD 2009 compliance cannot be achieved without cost. Trusts must accept the costs as failure to comply could result in even larger financial penalties. Re-banding of junior medical staff has provided a financial surplus in many compliant trusts; it is vital that such surpluses are reinvested in patient care and ensuring WTD compliance.
If posts are to be re-banded, it is recommended that planning takes place as early as possible so money can be saved against pay protection. Changes to rotas need to be agreed and signed off as soon as possible in order to save on pay protection. The proposed new pay band should appear in advertisements for trainee posts.
In order to support any service reconfiguration, trusts and directorates may require financial support. The Department of Health will make approximately £300m available in 2009 to primary care trusts to support WTD compliance. Trust boards will need to engage with strategic health authorities and primary care trusts to secure funding where appropriate.
Recognition of the impact on consultant workload6.4.3. There needs to be a realistic appraisal of consultant responsibilities and job plans. Throughout the project the most common issue raised was the increased workload of consultants and senior trainees. Both groups consistently commented that those in senior positions were required to perform procedures traditionally allocated to more junior doctors because these doctors were relatively inexperienced or simply not available during normal working hours. This model of substitution of consultants for trainees is not sustainable unless consultant expansion is planned. This will inevitably require additional investment.

19
WTD - Implications and Practical Suggestions to Achieve Compliance
Appendix AProject methodGovernance of projectA governance board comprising anaesthetic and surgical clinicians was established with a mandate of overseeing the project and directing it through its various stages. The board was jointly chaired by Professor Michael Horrocks, WTD Council lead for the Royal College of Surgeons of England, and Dr Anne Thornberry, WTD Council lead for the Royal College of Anaesthetists. For a list of members see Appendix C.
ObjectivesThe specific objectives of the project were to:
obtain information about arrangements for staffing and service provision in relation to WTD •2009 compliance in both anaesthesia and surgery across a range of hospitals;
identify a cross-section of units/specialties that reported 2009 compliance for further study;•
identify solutions employed, areas of good practice, common obstacles encountered and •methods for overcoming these;
use specialty working groups (comprising representatives from hospitals that were not yet •compliant) to evaluate the safety, effectiveness and transferability of identified solutions;
engage national organisations in the form of specialty expert panels to consider solutions •presented and make recommendations for implementation in the workplace; and
formulate advice and guidance to anaesthetists, surgeons, hospital management, service •planners, commissioners, deans, etc and present a single guidance document endorsed by both colleges.
QuestionnaireAn online questionnaire was sent to the clinical directors in anaesthesia and surgery in 74 trusts in February 2008. For details of the results see Appendix B.
It was difficult to build an overall picture of compliance in the surgical specialties because there were often several clinical directors for surgery and its sub-specialties within a hospital or trust. Anaesthesia, however, usually had one identified clinical director. No data was obtained from an independent directorate of intensive care medicine.
Structured interviewsA number of hospitals reporting compliance were selected to take part in structured telephone interviews across both anaesthesia and surgery. These hospitals were selected to represent a cross-section of sizes and geographical location.
Telephone interviews were undertaken with clinical directors or surgical/clinical tutors, representatives from hospital HR departments, trainees and, where they existed, the administrative WTD lead.
Appendices
WTD - Implications and Practical Suggestions to Achieve Compliance
20
Criteria developmentThe governance board agreed a set of criteria against which reported solutions were measured (Appendix D). These criteria were developed from the requirements of the WTD legislation, national guidelines on training and service delivery, and policy and guidance documents from both colleges.
After interviews were complete, the governance board selected a number of hospitals to use as case studies. These were chosen to represent the variety of solutions reported and were mapped against the agreed criteria.
Working groupsThe case studies were presented to working groups made up of clinical directors, HR representatives and trainees from hospitals that had indicated non-compliance. There were separate working groups for anaesthesia and surgery. Representatives were asked to comment on:
whether aspects of the solutions could be used in their trust;•
whether and how solutions could be adapted; and•
whether some of the solutions were unsuitable for particular specialties or hospitals.•
Expert panelsExpert panels were established for both anaesthesia and surgery. These comprised the major stakeholders of the project and representatives from national organisations. For a list of panel members see Appendix C. The expert panels examined the case studies and feedback from the working groups and identified those solutions that they would be prepared to endorse. The panels also provided additional information and suggestions on implementation.
Final reportThis report brings together all the stages of the project and contains the findings, solutions and recommendations agreed by both colleges.
21
WTD - Implications and Practical Suggestions to Achieve Compliance
Appendix B
Joint RCoA/RCSE WTD 2009 Project questionnaire
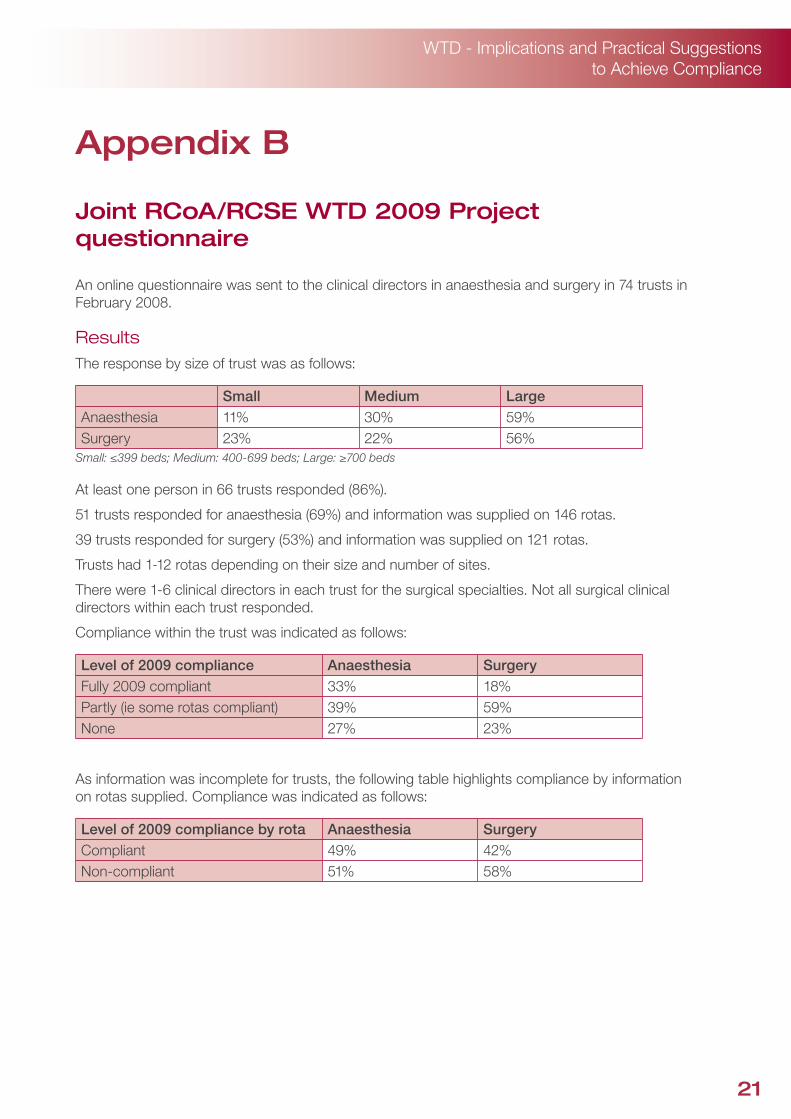
An online questionnaire was sent to the clinical directors in anaesthesia and surgery in 74 trusts in February 2008.
ResultsThe response by size of trust was as follows:
Small Medium LargeAnaesthesia 11% 30% 59%Surgery 23% 22% 56%
Small: ≤399 beds; Medium: 400-699 beds; Large: ≥700 beds
At least one person in 66 trusts responded (86%).
51 trusts responded for anaesthesia (69%) and information was supplied on 146 rotas.
39 trusts responded for surgery (53%) and information was supplied on 121 rotas.
Trusts had 1-12 rotas depending on their size and number of sites.
There were 1-6 clinical directors in each trust for the surgical specialties. Not all surgical clinical directors within each trust responded.
Compliance within the trust was indicated as follows:
Level of 2009 compliance Anaesthesia SurgeryFully 2009 compliant 33% 18%Partly (ie some rotas compliant) 39% 59%None 27% 23%
As information was incomplete for trusts, the following table highlights compliance by information on rotas supplied. Compliance was indicated as follows:
Level of 2009 compliance by rota Anaesthesia SurgeryCompliant 49% 42%Non-compliant 51% 58%

WTD - Implications and Practical Suggestions to Achieve Compliance
22
How was compliance achieved? (Respondents were able to choose more than one option)
Method Anaesthesia SurgeryRota redesign 46% 71%
Increased medical staff 36% 25%
Reconfiguration 13% 17%
Consultant evening sessions 17% 0%
Role substitution 13% 15%
Reduced tiers of cover 13% 12%
Cross-cover 6% 15%
Consultant resident out of hours 4% 0%
Additional consultants on call 1% 2%
None 26% 15%
The most popular solutions in both anaesthesia and surgery were rota redesign and increasing medical staff. These were followed by increased consultant evening sessions in anaesthesia and reconfiguration in surgery.
What were the barriers to achieving compliance? (Respondents were able to choose more than one option)
Barrier Anaesthesia SurgeryFinancial restrictions 41% 40%Staff resistance to changed working patterns 37% 48%Staff resistance to perceived deterioration in training 43% 35%Organisational capacity 21% 15%Staff resistance due to concerns about quality of patient care and safety
9% 27%
Lack of support from senior management 3% 8%None 24% 23%
Financial restrictions, staff resistance to changed working patterns and perceived deterioration in training were stated as the main barriers faced in becoming compliant. A significant proportion of respondents claimed not to have had to overcome any of the given barriers.
The other common barrier cited was recruitment difficulties due to the implementation of Modernising Medical Careers and the Medical Training Application Service in 2007.

23
WTD - Implications and Practical Suggestions to Achieve Compliance
Safety and training
A series of questions on safety and training were included for trusts that were 2009 compliant. All respondents indicated they were operating within recommended parameters of training and safety.
Rotas that were not yet 2009 compliant
Of trusts that reported non-compliance, the following indicated they had a costed and agreed plan to become 2009 compliant (by size of trust):
Small Medium LargeAnaesthesia 8% 12% 15%Surgery 0% 9% 14%
Small: ≤399 beds; Medium: 400-699 beds, Large: ≥700 beds
Trusts that were not yet 2009 compliant were asked which solutions they planned to use and what the anticipated barriers were. The results were similar to those reported by compliant trusts.

WTD - Implications and Practical Suggestions to Achieve Compliance
24
Appendix C
Panel membership and acknowledgements
Project governance board
Professor Michael Horrocks (Chair) RCSE Council Representative, Consultant Surgeon
Dr E Anne Thornberry (Chair) RCoA Council Representative, Consultant Anaesthetist
Dr Yasmin Ahmed-Little Project Director, EWTD Workforce Medical Team, NHS North West
Dr Anna Batchelor Consultant Anaesthetist, Intensive Care Medicine
Dr Adrian England Consultant Anaesthetist
Dr Neil Flint Trainee Anaesthetist Representative
Mr Conor Marron Trainee Surgeon Representative
Miss Wendy Reid Postgraduate Dean
Mr Paul Rowe Consultant Surgeon
Mr Nigel Burgess Skills for Health - Workforce Projects Team
Mr Rayaz Patel Skills for Health - Workforce Projects Team
Mrs Jo Cripps Project Manager, Delivery of Surgical Services (RCSE)
Mrs Kirsten English Joint RCoA/RCSE WTD 2009 Project Manager
Expert panel - anaesthesia
Dr E Anne Thornberry (Chair) RCoA Council Representative, Project Governance Board Chair
Professor Chris Dodd Vice-president RCoA and Faculty of Chronic Pain Representative
Dr Hazel Adams Schools of Anaesthesia Representative
Dr Adrian England Project Governance Board Member
Dr Neil Flint Project Governance Board Member
Dr Les Gemmell Association of Anaesthetists of Great Britain and Ireland
Mrs Rosemary Harris RCoA Patient Liaison Group Representative
Dr Roop Kishen Intensive Care Medicine Representative
Dr Andy Lim RCoA Staff and Associate Specialist representative
Dr Alan McGlennan Trainee Anaesthetist Representative
Ms Fiona Moss Postgraduate Dean
Mr Rayaz Patel Skills for Health - Workforce Projects Team Representative and Governance Board Member
Mrs Kirsten English Joint RCoA/RCSE WTD 2009 Project Manager

25
WTD - Implications and Practical Suggestions to Achieve Compliance
Expert panel - surgery
Professor Michael Horrocks (Chair) RCSE Council Representative, Project Governance Board Chair
Mrs Linda De Cossart Vice-president RCSE, Schools of Surgery Representative
Dr Yasmin Ahmed-Little Project Governance Board Member
Mrs Lesley Bentley RCSE Patient Liaison Group Chair
Mr Ben Cresswell Association of Surgeons in Training Representative
Mr Peter Lamont SAC Representative, SAC General Surgery Chair
Mr Paul Rowe Project Governance Board Member
Mr Thangasamy Sankar RCSE Staff and Associate Specialist representative
Mr Nigel Standfield Postgraduate Dean
Mr James Steers President of Federation of Surgical Specialty Associations
Ms Sian Thomas Joint Acting Director, NHS Employers
Mr Rayaz Patel Skills for Health - Workforce Projects Team Representative and Project Governance Board Member
Mrs Jo Cripps Project Governance Board Member
Mrs Kirsten English Joint RCoA/RCSE WTD 2009 Project Manager
Project team
Mrs Kirsten English Joint RCoA/RCSE WTD 2009 Project Manager
Mrs Jo Cripps Project Manager, Delivery of Surgical Services (RCSE)
Miss Farhiya Hassan Administrative Assistant
AcknowledgementsWe would like to thank everyone who participated in this project at the different stages and gave up their time to fill in questionnaires, take part in interviews and attend panel meetings. We would particularly like to thank those who participated in telephone interviews and attended the working group sessions to present case studies.
Without your help this project would not have been possible. Thank you.

WTD - Implications and Practical Suggestions to Achieve Compliance
26
Appendix D
Assessment criteria for case studies
The governance board agreed a set of criteria against which case studies were measured.
Criteria related to compliance
Criteria Source Recommended standard1 Average weekly
working timeWTD legislation Maximum of 48 hours (measured over a
reference period, nominally 26 weeks)2 Maximum period of
continuous dutyWTD legislation 13 hours
NB: Rota duty lengths should have a reasonable margin to the maximum (13 hours) and should include time for handover, otherwise doctors will be likely to breach
3 Minimum break between duties
WTD legislation 11 hours (ie 11 hours’ continuous rest in every 24-hour period)
4 Maximum days on duty
WTD legislation 12 days (with minimum 24 hour rest in every 7 days or minimum 48 hours’ rest in every 14 days unless compensatory rest is taken)

27
WTD - Implications and Practical Suggestions to Achieve Compliance
Criteria related to patient safety
Criteria Source Recommended standard5 Handover PMETB,16
RCoA,9 RCSE,5 BMA17
Anaesthesia
Time must be available for safe handover of work between shifts in differing clinical areas. A minimum of 30 minutes is recommended and must be included in shift length.
Surgery
Compliant rotas should allow for a formal handover of least 30 minutes’ duration. Consultants must be involved and the handover must be used as a training opportunity.
Intensive Care Medicine
The RCoA Council agreed that the standard for ICM should be the same as for surgery.
6 Cell size RCoA,9 RCSE7
Anaesthesia
To ensure the minimum acceptable training and experience is maintained the RCoA position is that trainee full-shift night work is no more onerous than 1 night in 8.
Surgery
There should be a minimum of eight in a cell on a full-shift rota.
7 Rota night working pattern
NSG,18 RCoA,9 RCSE7
Ideally, no more than 2 or 3 nights should be worked consecutively and these should be followed by 2 nights’ uninterrupted sleep. 7 consecutive nights is not acceptable.
8 Supervision of trainees
RCoA,9 RCSE7
Anaesthesia
There should be sufficient access during the out-of-hours period to senior input for trainee doctors. It is recommended that those on call should be able to be on site within 30 minutes.
Surgery
Trainees must be appropriately supervised, particularly in the out-of-hours period.
WTD - Implications and Practical Suggestions to Achieve Compliance
28
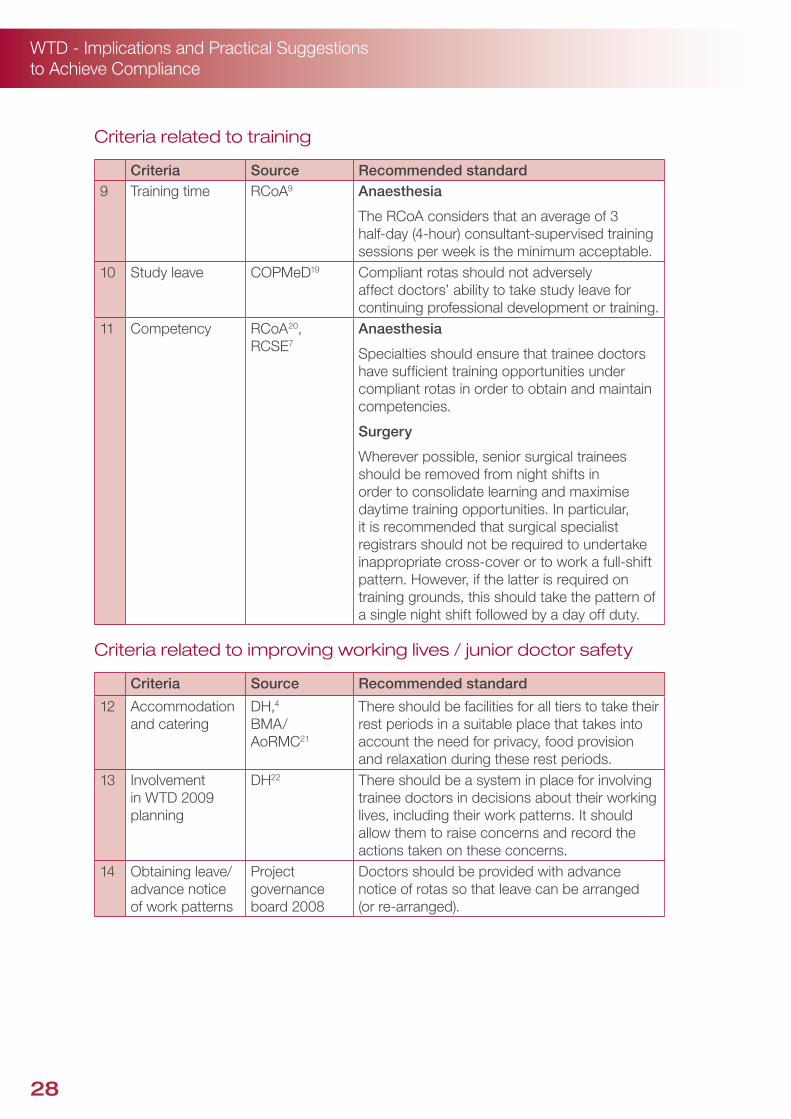
Criteria related to training
Criteria Source Recommended standard9 Training time RCoA9 Anaesthesia
The RCoA considers that an average of 3 half-day (4-hour) consultant-supervised training sessions per week is the minimum acceptable.
10 Study leave COPMeD19 Compliant rotas should not adversely affect doctors’ ability to take study leave for continuing professional development or training.
11 Competency RCoA20, RCSE7
Anaesthesia
Specialties should ensure that trainee doctors have sufficient training opportunities under compliant rotas in order to obtain and maintain competencies.
Surgery
Wherever possible, senior surgical trainees should be removed from night shifts in order to consolidate learning and maximise daytime training opportunities. In particular, it is recommended that surgical specialist registrars should not be required to undertake inappropriate cross-cover or to work a full-shift pattern. However, if the latter is required on training grounds, this should take the pattern of a single night shift followed by a day off duty.
Criteria related to improving working lives / junior doctor safety
Criteria Source Recommended standard
12 Accommodation and catering
DH,4 BMA/ AoRMC21
There should be facilities for all tiers to take their rest periods in a suitable place that takes into account the need for privacy, food provision and relaxation during these rest periods.
13 Involvement in WTD 2009 planning
DH22 There should be a system in place for involving trainee doctors in decisions about their working lives, including their work patterns. It should allow them to raise concerns and record the actions taken on these concerns.
14 Obtaining leave/advance notice of work patterns
Project governance board 2008
Doctors should be provided with advance notice of rotas so that leave can be arranged (or re-arranged).
29
WTD - Implications and Practical Suggestions to Achieve Compliance
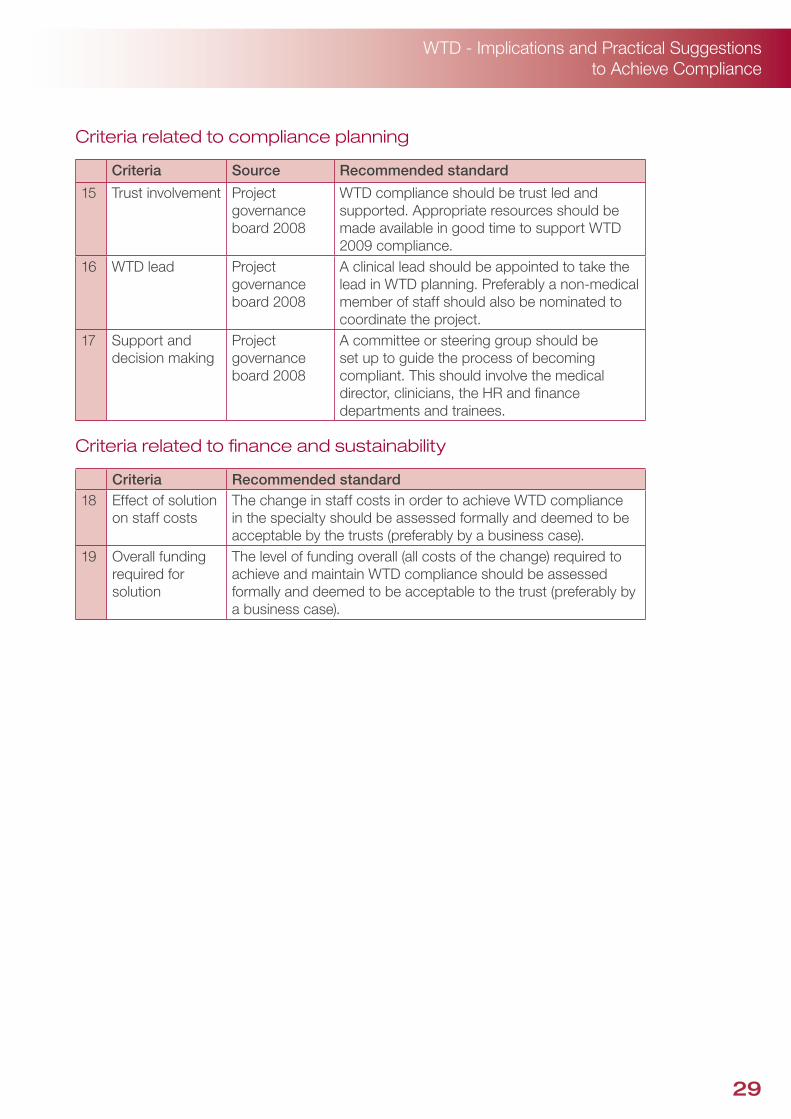
Criteria related to compliance planning
Criteria Source Recommended standard
15 Trust involvement Project governance board 2008
WTD compliance should be trust led and supported. Appropriate resources should be made available in good time to support WTD 2009 compliance.
16 WTD lead Project governance board 2008
A clinical lead should be appointed to take the lead in WTD planning. Preferably a non-medical member of staff should also be nominated to coordinate the project.
17 Support and decision making
Project governance board 2008
A committee or steering group should be set up to guide the process of becoming compliant. This should involve the medical director, clinicians, the HR and finance departments and trainees.
Criteria related to finance and sustainability
Criteria Recommended standard18 Effect of solution
on staff costsThe change in staff costs in order to achieve WTD compliance in the specialty should be assessed formally and deemed to be acceptable by the trusts (preferably by a business case).
19 Overall funding required for solution
The level of funding overall (all costs of the change) required to achieve and maintain WTD compliance should be assessed formally and deemed to be acceptable to the trust (preferably by a business case).
WTD - Implications and Practical Suggestions to Achieve Compliance
30
Appendix E
Educational approval of posts
The Postgraduate Medical Education and Training Board (PMETB) process of educational approval requires that a suitable post is identified for a training programme by the training programme director, who may consult with the college regional advisor and the specialist advisory committee liaison member for the deanery. The deanery must then guarantee to PMETB that the post will uphold training standards for the specialty and that it will take responsibility for ensuring those standards. If PMETB approves the post, it is incorporated into the programme.
PMETB is responsible for approving training programmes, not individual posts. There is no limit on the number of posts that may be given educational approval. However, the number of national training numbers (NTNs) available in each specialty and deanery/training programme is strictly controlled and limited.
Within anaesthesia there are core modules that every trainee must complete. These are only available within large teaching hospitals. There is a limit to the number of trainees who can undertake these modules at any one time, thus defining the training capacity of the school. Peripheral hospitals, with funding, cannot appoint additional trainees unless there is capacity within the school to provide a complete training programme.
In 2007 the Department of Health released a small number of fully funded NTNs to those deaneries that bid for additional posts. The Department of Health also temporarily increased the number of NTNs at ST3 level to deal with the senior house officer bulge for one year only. These posts were not re-appointed to in 2008.
It is probable that a number of these new posts have been created to enable WTD compliance. It will take five to six years for these additional NTN holders to work through their specialist training programme. When trainees achieve their Certificate of Completion of Training, it is unlikely that the NTN posts will be renewed. This may de-stabilise rotas that are currently compliant.
31
WTD - Implications and Practical Suggestions to Achieve Compliance
Appendix F
References and useful links
ReferencesCase C-303/98, Sindicato de Medicos de Asistencia Publica (SiMAP) v Conselleria de Sanidad 1. y Consumo de la Generalidad Valenciana. Judgement of 3 October 2000. European Court Reports 2000: I-7963.
Case C-151/02, Landeshauptstadt Kiel v Norbert Jaeger. Judgement of 9 October 2003. 2. European Court of Justice; 2003.
Council directive 93/104/EC of 23 November 1993 concerning certain aspects of the 3. organisation of working time. Council of the European Union; 1993.
Department of Health. HSC 1998/240: Reducing Junior Doctors’ Hours. NHS Executive 4. Annexes A, B and C. London: DH; 1998. www.dh.gov.uk/en/Publicationsandstatistics/Lettersandcirculars/Healthservicecirculars/DH_4003928
Royal College of Surgeons of England. Safe Handover: Guidance from the Working Time 5. Directive Working Party. London: RCSE; 2007. www.rcseng.ac.uk/publications/docs/publication.2007-05-14.3777986999
Skills for Health - Workforce Projects Team: Salisbury Foundation Trust. 6. www.healthcareworkforce.nhs.uk/salisbury/
Royal College of Surgeons of England. Safe Shift Working for Surgeons in Training: Revised 7. Policy Statement from the Working Time Directive Working Party. London: RCSE; 2007. www.rcseng.ac.uk/rcseng/content/publications/docs/safe_shift_revised.html
Royal College of Surgeons of England. Separating Emergency and Elective Surgical Care: 8. Recommendations for Practice. London: RCSE; 2007 www.rcseng.ac.uk/rcseng/content/publications/docs/separating_emergency_and_elective.html
Royal College of Anaesthetists. Working Time Directive 2009 and Shift Working. London: 9. RCoA; 2007. www.rcoa.ac.uk/docs/WTD2009_shift-working.pdf
Joint Committee on Surgical Training 10. www.jcst.org/
Home Office UK Border Agency: Training and Work Experience Scheme (TWES) Work Permit 11. Arrangements. www.ukba.homeoffice.gov.uk/workingintheuk/tier2/workpermits/workpermitarrangements/twesworkpermits/
National Confidential Enquiry into Perioperative Deaths. Who Operates When? II. London: 12. NCEPOD; 2003. www.ncepod.org.uk/2003wow.htm
Skills for Health - Workforce Projects Team: Taking Care 24:7. 13. www.healthcareworkforce.nhs.uk/takingcare247.html

WTD - Implications and Practical Suggestions to Achieve Compliance
32
Royal College of Physicians. Designing Safer Rotas for Junior Doctors in the 48 Hour Week. 14. London: RCP; 2006 www.rcplondon.ac.uk/pubs/contents/779336a5-b884-4b5f-8c23-efd75d123868.pdf
Knauth P. Speed and direction of shift rotation. J Sleep Res 1995; 4(suppl 2): 41-46.15.
Postgraduate Medical Education and Training Board. Generic Standards for Training. London: 16. PMETB; 2008. www.pmetb.org.uk/index.php?id=gst
British Medical Association Junior Doctors Committee. Safe Handover: Safe Patients. London: 17. BMA; 2004. www.bma.org.uk/ap.nsf/AttachmentsByTitle/PDFsafehandover/$FILE/safehandover.pdf
National Stakeholder Group. Working Time Directive National Stakeholder Group discourages 18. the use of 7 x 13 hour shift patterns. National Stakeholder Group press release; January 2007. www.healthcareworkforce.nhs.uk/working_time_directive/wtd_resources/7_x_13_hour_shift_patterns.html
Conference of Postgraduate Medical Deans. A policy for a modern approach to study leave for 19. modernised medical careers for doctors and dentists in training. London: COPMeD; 2006. www.copmed.org.uk/document_store/1140427835Geae_study_leave_policy.doc
Royal College of Anaesthetists. The CCT in Anaesthetics and Guidance for Trainers and 20. Trainees. London: RCoA; 2007-2008. www.rcoa.ac.uk/index.asp?PageID=991
British Medical Association Junior Doctors Committee/Academy of Medical Royal Colleges. 21. Joint Position Statement on On-call Rooms. London: BMA; 2006. www.bma.org.uk/ap.nsf/Content/jntposstmtsleep
NHS Employers. The IWL Standard. London: DH; 2000. 22. www.nhsemployers.org/practice/excellence-342.cfm

33
WTD - Implications and Practical Suggestions to Achieve Compliance
Useful links and further readingAcademy of Medical Royal Colleges. Implementing the European Working Time Directive: A Position Paper from the Academy of Medical Royal Colleges. London: AoMRC; 2004. www.aomrc.org.uk/aomrc/admin/reports/docs/ewtd-acad-6.pdf
Department of Health. The New Deal on Junior Doctors’ Hours. London: DH; 2000. www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4008510
Skills for Health - Workforce Projects Team: New Deal and WTD booklets for junior doctors, consultants, managers and clinical directors www.healthcareworkforce.nhs.uk/working_time_directive/pilot_projects/new_deal_and_wtd_booklets.html
WTD 2009 Resources www.healthcareworkforce.nhs.uk/working_time_directive/wtd_resources/full_wtd_2009_resources.html
Intensive Care Society and the Intercollegiate Board for Training in Intensive Care Medicine. Standards for Consultant Staffing of Intensive Care Units. London: ICS and IBTICM; 2007. www.ics.ac.uk/icmprof/downloads/Standards%20Consult%20staff%2021_08_2008.pdf
Royal College of Physicians. Working the Night Shift: Preparation, Survival and Recovery. London: RCP; 2006. www.rcplondon.ac.uk/pubs/books/nightshift/
Royal College of Surgeons of England. Delivering Surgical Services: Options for Maximising Resources. London: RCSE; 2007. www.rcseng.ac.uk/publications/docs/maximising_resources.html
Royal College of Surgeons of England. Rota Planning: Guidance from the Working Time Directive Working Party. London: RCSE; 2007. www.rcseng.ac.uk/publications/docs/rotaplanning.html/?searchterm=rota%20planning
Royal College of Surgeons of England. Working Time Directive 2009: Meeting the Challenge in Surgery. London: RCSE; 2008. www.rcseng.ac.uk/rcseng/content/publications/docs/working-time-directive-2009-meeting-the-challenge-in-surgery-1

The Royal College of Surgeons of England 35-43 Lincoln’s Inn Fields London WC2A 3PE T: 020 7405 3474 W: www.rcseng.ac.uk
Registered charity number 212808
The Royal College of Anaesthetists Churchill House, 35 Red Lion Square London WC1R 4SG T: 020 7092 1500 W: www.rcoa.ac.uk
Skills for Health - Workforce Projects Team 1st Floor, 3000 Manchester Business Park Aviator Way Manchester M22 5TG
Tel: 0161 266 2300 Fax: 0161 266 1001 Email: [email protected] Website: www.healthcareworkforce.nhs.ukProduct code: WTD-0809-012
© Skills for Health - Workforce Projects Team, 2008. All rights reserved.





























