Embed Size (px)
Citation preview

Document of The World Bank
Report No: ICR2236
IMPLEMENTATION COMPLETION AND RESULTS REPORT (IBRD-73950)
ON A
LOAN
IN THE AMOUNT OF US$ 110 MILLION
TO THE
REPUBLIC OF THE PHILIPPINES
FOR A
NATIONAL SECTOR SUPPORT FOR HEALTH REFORM PROJECT
January 21, 2013
Human Development Sector Unit East Asia & Pacific Region
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
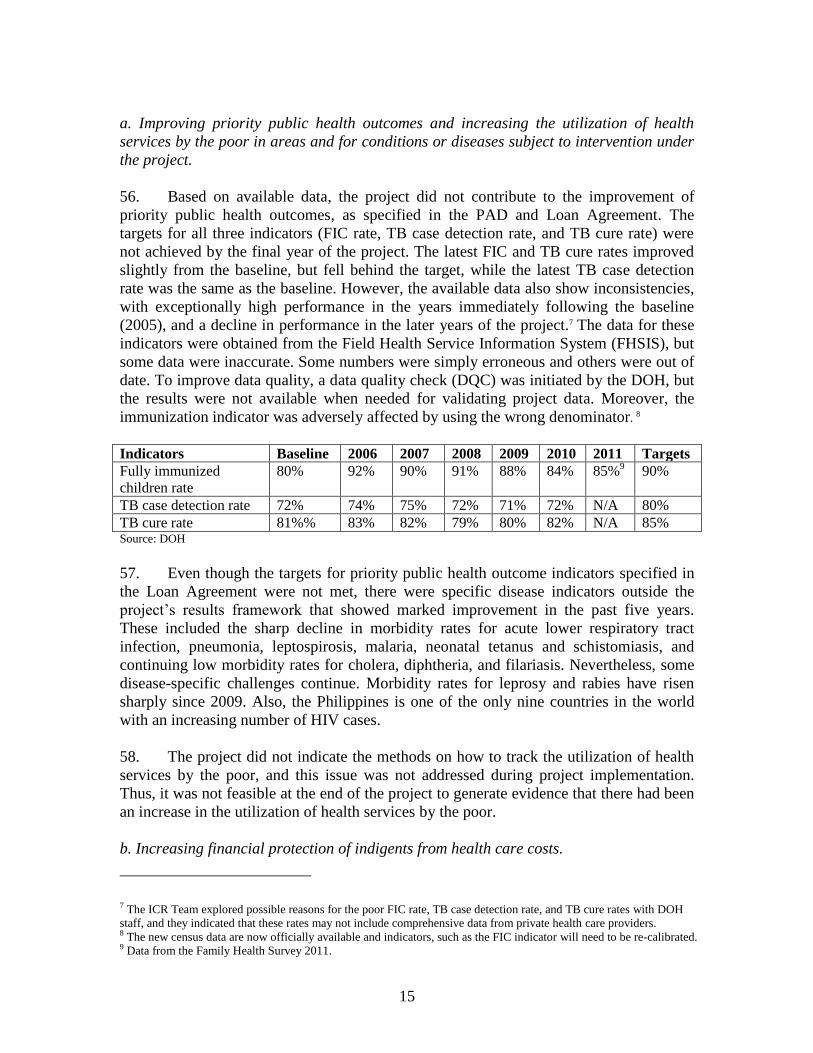
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized

CURRENCY EQUIVALENTS
(Exchange Rate Effective January 15, 2013)
Currency Unit = Philippine Peso (PhP)
PhP40.56 = US$1
FISCAL YEAR
January 1 – December 31
ABBREVIATIONS AND ACRONYMS
BFAD Bureau of Food and Drugs
CAS Country Assistance Strategy
CBMS Community-Based Monitoring System
CDR Case Detection Rate
CHD Center for Health Development
COA Commission on Audit
DBM Department of Budget and Management
DOF Department of Finance
DOH Department of Health
DPL Development Policy Lending
DQC Data Quality Check
DSWD Department of Social Welfare and Development
EC European Commission
eNGAS Electronic National Government Accounting System
EPI Expanded Program of Immunization
ETS Expenditure Tracking System
F1 FOURmula ONE for Health
FDA Food and Drug Administration
FHSIS Field Health Service Information System
FIC Fully Immunized Children
GAA General Appropriations Act
GOP Government of the Philippines
HiB Hemophilus Influenza B
HRH Human Resources in Health
HSEF Health Sector Expenditure Framework
HSRA Health Sector Reform Agenda
IA Internal Audit
IP Indigent Program
IPPF Indigenous People Planning Framework
ISR Implementation Status and Results Report
JAPI Joint Assessment and Planning Initiative
LGUs Local Government Units
M&E Monitoring and Evaluation

MDGs Millennium Development Goals
MoU Memorandum of Understanding
MMR Measles, Mumps and Rubella
MNCHN Maternal, Newborn, Child Health, and Nutrition
MOA Memorandum of Agreement
MTR Mid-Term Review
NCB National Competitive Bidding
NEDA National Economic Development Authority
NG National Government
NHIA National Health Insurance Act
NHIP National Health Insurance Program
NHTS National Household Targeting System
NHTS-PR National Household Targeting System – Poverty Reduction
NPS National Program Support
NSS National Sector Support
NSSHRP National Sector Support for Health Sector Reform
OOP Out-of-Pocket
P4R Program-for-results
PAD Project Appraisal Document
PDO Project Development Objective
PHIC Philippines Health Insurance Corporation
PHOs Provincial Health Offices
PhP Philippine Peso
PMT Proxy Means Test
PPA Plans, Projects and Activities
QAG Quality Assurance Group
QER Quality Enhancement Review
QMS Quality Management System
SDAH Sector Development Approach for Health
SEMP Social Expenditure Management Project
SEMP 2 Second Social Expenditure Management Project
SLA Service Level Agreements
TB Tuberculosis
TBC Tuberculosis Control
THE Total Health Expenditures
TTL Task Team Leader
UHC Universal Health Care
UN United Nations
WHO World Health Organization
Vice President: Ulrich Zachau (EAPVP)
Country Director: Motoo Konishi (EACPF)
Sector Manager: Toomas Palu (EASHH)
Project Team Leader: Roberto Rosadia (EASHH)
ICR Team Leader: Sutayut Osornprasop (EASHH)

PHILIPPINES
NATIONAL SECTOR SUPPORT FOR HEALTH REFORM PROJECT
CONTENTS
Data Sheet
A. Basic Information
B. Key Dates
C. Ratings Summary
D. Sector and Theme Codes
E. Bank Staff
F. Results Framework Analysis
G. Ratings of Project Performance in ISRs
H. Restructuring
I. Disbursement Graph
1. Project Context, Development Objectives and Design ............................................... 1
2. Key Factors Affecting Implementation and Outcomes .............................................. 6
3. Assessment of Outcomes .......................................................................................... 12
4. Assessment of Risk to Development Outcome ......................................................... 22
5. Assessment of Bank and Borrower Performance ..................................................... 23
6. Lessons Learned ....................................................................................................... 27
7. Comments on Issues Raised by Borrower/Implementing Agencies/Partners .......... 28
Annex 1. Project Costs and Financing .......................................................................... 29
Annex 2. Outputs by Component ................................................................................. 30
Annex 3. Economic and Financial Analysis ................................................................. 31
Annex 4. Bank Lending and Implementation Support/Supervision Processes ............ 32
Annex 5. Beneficiary Survey Results ........................................................................... 34
Annex 6. Stakeholder Workshop Report and Results ................................................... 35
Annex 7. Summary of Borrower's ICR and/or Comments on Draft ICR ..................... 36
Annex 8. Comments of Cofinanciers and Other Partners/Stakeholders ....................... 37
Annex 9. List of Supporting Documents ...................................................................... 38
MAP


A. Basic Information
Country: Philippines Project Name:
National Sector
Support for Health
Reform
Project ID: P075464 L/C/TF Number(s): IBRD-73950
ICR Date: 01/19/2012 ICR Type: Core ICR
Lending Instrument: SIM Borrower: REPUBLIC OF THE
PHILIPPINES
Original Total
Commitment: US$ 110.00M Disbursed Amount: US$ 104.72M
Revised Amount:
Environmental Category: C
Implementing Agencies: Department of Health
Cofinanciers and Other External Partners:
B. Key Dates
Process Date Process Original Date Revised / Actual
Date(s)
Concept Review: 07/25/2002 Effectiveness: 03/27/2007 03/27/2007
Appraisal: 03/06/2006 Restructuring(s): 08/16/2010
05/26/2011
Approval: 06/29/2006 Mid-term Review: 08/30/2008 02/08/2010
Closing: 06/30/2011 03/31/2012
C. Ratings Summary
C.1 Performance Rating by ICR
Outcomes: Moderately Unsatisfactory
Risk to Development Outcome: Moderate
Bank Performance: Moderately Unsatisfactory
Borrower Performance: Moderately Unsatisfactory
C.2 Detailed Ratings of Bank and Borrower Performance (by ICR)
Bank Ratings Borrower Ratings
Quality at Entry: Moderately
Unsatisfactory Government: Moderately Satisfactory
Quality of Supervision: Moderately
Unsatisfactory
Implementing
Agency/Agencies:
Moderately
Unsatisfactory
Overall Bank
Performance:
Moderately
Unsatisfactory Overall Borrower
Performance:
Moderately
Unsatisfactory

C.3 Quality at Entry and Implementation Performance Indicators
Implementation
Performance Indicators
QAG Assessments
(if any) Rating
Potential Problem Project
at any time (Yes/No): No
Quality at Entry
(QEA): No rating was provided
Problem Project at any
time (Yes/No): No
Quality of
Supervision (QSA): None
DO rating before
Closing/Inactive status: Satisfactory
D. Sector and Theme Codes
Original Actual
Sector Code (as % of total Bank financing)
Central government administration 10 10
Compulsory health finance 40 45
Health 40 45
Non-compulsory health finance 10 0
Theme Code (as % of total Bank financing)
Administrative and civil service reform 17 17
HIV/AIDS 16 0
Health system performance 33 40
Social risk mitigation 17 38
Tuberculosis 17 5
E. Bank Staff
Positions At ICR At Approval
Vice President: Ulrich Zachau Jeffrey S. Gutman
Country Director: Motoo Konishi Joachim von Amsberg
Sector Manager: Toomas Palu Fadia M. Saadah
Project Team Leader: Roberto Antonio F. Rosadia Loraine Hawkins
ICR Team Leader: Sutayut Osornprasop
ICR Primary Author: Sutayut Osornprasop
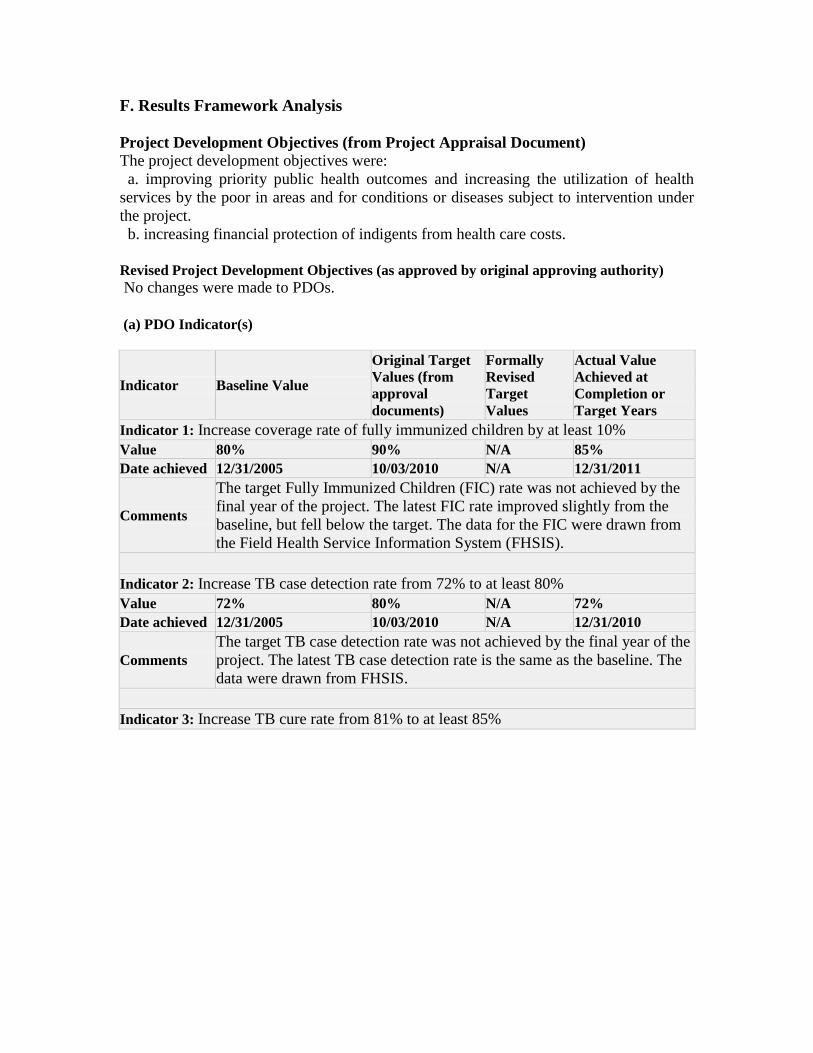
F. Results Framework Analysis
Project Development Objectives (from Project Appraisal Document) The project development objectives were:
a. improving priority public health outcomes and increasing the utilization of health
services by the poor in areas and for conditions or diseases subject to intervention under
the project.
b. increasing financial protection of indigents from health care costs.
Revised Project Development Objectives (as approved by original approving authority)
No changes were made to PDOs.
(a) PDO Indicator(s)
Indicator Baseline Value
Original Target
Values (from
approval
documents)
Formally
Revised
Target
Values
Actual Value
Achieved at
Completion or
Target Years
Indicator 1: Increase coverage rate of fully immunized children by at least 10%
Value 80% 90% N/A 85%
Date achieved 12/31/2005 10/03/2010 N/A 12/31/2011
Comments
The target Fully Immunized Children (FIC) rate was not achieved by the
final year of the project. The latest FIC rate improved slightly from the
baseline, but fell below the target. The data for the FIC were drawn from
the Field Health Service Information System (FHSIS).
Indicator 2: Increase TB case detection rate from 72% to at least 80%
Value 72% 80% N/A 72%
Date achieved 12/31/2005 10/03/2010 N/A 12/31/2010
Comments
The target TB case detection rate was not achieved by the final year of the
project. The latest TB case detection rate is the same as the baseline. The
data were drawn from FHSIS.
Indicator 3: Increase TB cure rate from 81% to at least 85%

Value 81% 85% N/A 82%
Date achieved 12/31/2005 10/03/2010 N/A 12/31/2010
Comments
The target TB cure rate was not achieved by the final year of the project.
The latest TB cure rate improved very slightly from the baseline, but fell
behind the target. The data were drawn from the FHSIS.
Indicator 4: Evidence of a statistically significant improvement (wherever feasible) or
validation by an alternative method of improvement, in prevention, diagnosis or
treatment rates in participating LGUs for diseases or conditions subject to performance
agreements and grants
Value 0 LGU 15 LGUs N/A 0 LGU
Date achieved 10/03/2006 10/03/2010 N/A 03/31/2012
Comments
No method has been finalized. Department of Health (DOH) sees that it is
very difficult to come up with an evidence of a statistically significant
improvement. DOH has not been able to get a third party to validate an
alternative method, as planned. Nevertheless, DOH conducted a small
scale self-assessment by using LGU scorecards.
(b) Intermediate Outcome Indicator(s)
Indicator Baseline Value
Original Target
Values (from
approval
documents)
Formally
Revised
Target
Values
Actual Value
Achieved at
Completion of
Target Years
Indicator 1: Increase in proportion of DOH budget allocated on the basis of criteria of
need and performance (from 0 to at least 5% of existing maintenance and other operating
expenses and at least 5% of any increment in DOH MOOE budget)
Value 0% 5% N/A 24%
Date
achieved 10/03/2006 10/03/2010 N/A 12/31/2010
Comments
DOH budget was allocated on the basis of need and performance. It rose
gradually to 5.4% in 2007, fell to 1.8%(during the world-wide economic
crisis), and reached 24% in 2010.
Indicator 2: Increase in number of development projects or programs using HSEF to
plan and program their health sector support (from 0 foreign assisted project to 100% of
FOURmula ONE PPAs)
Value 1 project 100% of projects N/A 100%
Date
achieved 10/03/2006 10/03/2010 N/A 12/31/2009
Comments
From 2009 onward, 100% of FOURmula ONE PPAs used HSEF to plan
and program their health sector support. This target was reached well
ahead of the project’s closing date.
Indicator 3: Increase in number of LGUs identifying the poor using acceptable, defined

methods of means testing and enrolling them in NHIP Indigent Program (from 0 to 993
LGUs)
Value 0 993 N/A 0
Date
achieved 10/03/2006 10/03/2010 N/A 03/31/2012
Comments
No LGU identified the poor using an acceptable, defined method of means
testing and enrolling them in the NHIP Indigent Program. With no
progress on the LGU front, the project shifted to support a nationally
developed means test, and was able to identify the poor using the NHTS-
PR, which is an acceptable, defined method of means testing. Although
this enabled enrollment of 5.2 million poor households in the NHIP
Indigent Program, unfortunately this change in approach was not formally
specified during the project restructuring. It should also be noted that the
number of “poor” households on the list adopted by LGUs was around 6-7
million. Out of these, only about 900,000 households were the same as
those identified by the NHTS-PR, raising the concern that many of the
households on the LGU list are not poor.
Indicator 4: Significant quantified reductions in date-expiry, stock-outs and losses of
public health commodity stocks at defined levels in supply chain
Value
Quarterly reporting on
inventory & method of
forecasting quantities
required of public
health commodities
satisfactory to the Bank
in place
Target agreed in
year 4 met N/A
No data are
available
Date
achieved 10/03/2006 10/03/2010 N/A 03/31/2012
Comments Information on stock-outs was not collected by the DOH beyond the level
of the Center for Health Development (CHD).
Indicator 5: LGU scorecard implemented and scores improve in convergence sites

Value
Scorecard methodology
and guidelines
completed and
disseminated by end of
year
End of term
evaluation finds
further progress
in scores
N/A
There is progress
on scores in 16 F1
provinces
Date
achieved 10/03/2006 10/03/2010 N/A 03/31/2012
Comments
LGU scorecards were generated in all 16 F1 provinces by 2008, and later
expanded to all LGUs. There was moderate progress on scores in 16 F1
provinces.
Indicator 6: Full compliance with the Borrower’s procurement law and standards,
monitored using agency procurement benchmark indicators
Value DOH procurement
Manual completed
Agency
indicators
maintained or
improved
N/A Agency indicators
slightly improved
Date
achieved 10/03/2006 10/03/2010 N/A 05/31/2011
Comments
There was continued full compliance with the Bank’s procurement
procedures and standards, monitored using agency procurement
benchmark indicators.
Indicator 7: eNGAS roll out; quarterly reports to managers on performance against plan
and budget under General Appropriations Act (GAA) program structure
Value
eNGAS training in 16
regions; installation of
eNGAS in 8 regions;
reporting formats
agreed
Quarterly
Report generated
from eNGAS
N/A
eNGAS has been
fully used in 5
regions
Date
achieved 10/03/2006 10/03/2010 N/A 03/31/2012
Comments
By the end of the project, the eNGAS was used fully in 5 CHDs, while 7
CHDs were in a transition phase, and the eNGAS still needed to be rolled
out in another 4 CHDs. In all CHDs, under the GAA program structure,
quarterly reports were submitted to managers on performance against plan
and budget. DOH should be congratulated for its persistence in expanding
the eNGAS, despite COA’s decision to suspend the national roll-out of the
eNGAS in 2008.
Indicator 8: Internal Audit (IA) staff trained; annual IA plan of scheduled audits
implemented; updating and improvement in agency IA benchmark indicators
Value
IA conducted
for 2006; IA plan
developed for 2007
At least 80% IA
staff trained;
2010 IA plan
N/A
Over 80% IA staff
trained and annual
IA plan of audits

implemented implemented
Date
achieved 10/03/2006 10/03/2010 N/A 03/31/2012
Comments
G. Ratings of Project Performance in ISRs
No. Date ISR
Archived DO IP
Actual
Disbursements
(US$ millions)
1 11/28/2006 Satisfactory Satisfactory 0.00
2 10/23/2007 Satisfactory Satisfactory 6.68
3 04/18/2008 Satisfactory Moderately Satisfactory 6.68
4 09/29/2008 Satisfactory Moderately Satisfactory 18.32
5 07/08/2009 Satisfactory Moderately Satisfactory 20.41
6 06/09/2010 Satisfactory Moderately Satisfactory 37.97
7 04/23/2011 Satisfactory Moderately Satisfactory 60.32
H. Restructuring (if any)
Two level-II restructurings took place in August 2010 and May 2011.
I. Disbursement Profile


1
1. Project Context, Development Objectives and Design
1.1 Context at Appraisal
1. At the time of the project appraisal, the Philippines had been making progress on
health reforms at the aggregate level, but the major disparities in health outcomes (across
provinces, and across income quintiles) had not been addressed. Overall health
expenditures as well as public expenditures on health were lower than the average for
other middle-income countries. Out-of-pocket (OOP) payments as a percentage of total
health expenditures (THE), was large (54 %) which threatened the financial security of
the poorest households. The country was still grappling with the impacts of two major
reforms – the 1991 decentralization of health services to Local Government Units
(LGUs) and the 1995 reform of the National Health Insurance Program (NHIP) that had
expanded health insurance coverage for the population and established the Philippines
Health Insurance Corporation (PHIC) or PhilHealth. The decentralization reforms led to
extreme fragmentation in health financing and the delivery system. While the 1995
national health insurance reforms addressed some of this fragmentation, as well as
providing funds through PhilHealth, progress in providing healthcare for the poor was
still limited.
2. The Health Sector Reform Agenda (HSRA), effective from 1998 to 2004, had
begun to address the problems described above; however, progress was slower than
expected. The HSRA aimed to achieve: increased financial protection for the poor and
sick; supply-side measures to upgrade public health facilities in all communities to meet
PhilHealth’s accreditation standards; more effective regulation of the private health sector
and of drugs and commodities; a stronger results-orientation and coordination between
the Department of Health (DOH) and LGUs in delivering public health programs; and
development of structures and processes to increase coordination among neighboring
LGUs, the DOH and the private sector in planning local health systems. As
implementation of HSRA’s recommendations was too slow, in 2002, the DOH adopted a
phased implementation strategy, beginning with select “convergence” provinces, and
sought development partner assistance to support HSRA in these sites.1
3. It has been recognized that the HSRA had limited success due to: (1) limitations
in prioritizing a complex reform agenda and translating it into achievable, fiscally
realistic action plans, (2) limited coordination between the DOH and PhilHealth over the
reform strategy, (3) limited capacity in results-based management, (4) excessively
cautious behavior by PhilHealth in scaling up the NHIP, (5) fragmented donor support,
(6) constrained fiscal space, and (7) challenges with fragmented, autonomous LGUs.
4. By 2005, a new Secretary of Health had taken stock of progress, and in
collaboration with development partners, defined “FOURmula ONE for Health” (F1).
1 Convergence provinces are pilot provinces that have committed to implement reform components in their locality.
2
Building on HSRA reform, F1 was set up to tackle major health sector problems, e.g.
disparities in health outcomes and financial protection for the population. F1 was to
organize the critical reform initiatives into four implementation components: health
financing, health regulation, health service delivery, and good governance in health. F1
was particularly aimed at ensuring access to and availability of essential health packages;
assuring the quality and affordability of health goods and services; securing better and
sustained financing for health; and, improving health system performance in the medium
term.
5. An important strength of F1 was a more comprehensive approach to health
reforms and aligning them with public expenditure management and governance reform.
Using the medium-term Health Sector Expenditure Framework (HSEF) and the annual
budgeting process, a performance-monitoring framework for DOH, PhilHealth and
convergence provinces linked budgeting and resource allocation to outputs and
intermediate results. These links were intended to reduce obstacles to reform. With regard
to fragmentation in financing, the Sector Development Approach for Health (SDAH) was
adopted under F1 to align development partner-supported reform activities across the
entire health sector under a single national implementation plan and under harmonized
local health investment plans in each convergence province.
6. The Country Assistance Strategy (CAS) 2006-2008 focused on supporting public
expenditure management reform, improved governance, and better targeting of public
expenditure at a time when the country’s fiscal situation was fragile. The approach of the
new CAS was well suited to supporting the F1 strategy by linking the health budget with
reforms to health expenditure management.
7. The above-mentioned circumstances led to the design of this project, which was
intended to support the overall F1 reforms, which included both PhilHealth and LGU
reforms, based on the national sector support approach. Hence, the project was to finance
a slice of the overall health sector reform program as part of the appropriated budget, i.e.
similar to sector budget support but with no financial increments to the sector. It was also
agreed that the project’s outcome measures were to be based on the overall sector
outcomes, rather than outcomes from specific Bank financing.
Major Milestones in Philippine Health Reform
1991 Local Government Code Devolution of administrative and other functions
(including health services) from the national
government to local government units (LGUs)
1995 National Health Insurance Act Compulsory coverage under the National Health
Insurance Program (NHIP)
1998 Health Sector Reform Agenda
(HSRA)
Adjustment for impacts of devolution and
implementation of the NHIP
2005 FOURmula ONE for Health (F1) Accelerating gains under the HSRA
2005 Sector Development Approach for
Health (SDAH)
Rationalizing and harmonizing donor support
3
1.2 Original Project Development Objectives (PDOs) and Key Indicators
i. Improving priority public health outcomes and increasing the utilization of health
services by the poor in areas and for conditions or diseases subject to intervention under
the project.
ii. Increasing financial protection of indigents from health care costs.
8. The Loan Agreement included the following outcome indicators:
Increase coverage rate of fully immunized children by at least 10% (from 80% to
90%)
Increase TB case detection rate from 72% to at least 80%
Increase TB cure rate from 81% to at least 85%
Evidence of a statistically significant improvement (wherever feasible) or
validation by an alternative method of improvement, in prevention, diagnosis or
treatment rates in participating LGUs for diseases or conditions subject to
performance agreements and grants (from 0 LGU to 15 LGUs)
9. Two additional outcome indicators were included in the project appraisal
document (PAD), but were not included in the Loan Agreement:
Increased number of indigent families enrolled in NHIP using acceptable, defined
means test (up to at least 1.51 million indigent families)
Insured indigent households have lower OOP spending on health, compared to
uninsured households, and compared to prior periods
1.3 Revised PDOs (as approved by the original approving authority) and Key Indicators,
and Reasons/Justification
10. No changes were made to the PDO and key indicators.
1.4 Main Beneficiaries,
11. The primary beneficiaries of the project were poor households identified by the
means test and enrolled in PhilHealth’s Indigent Program. Other beneficiaries across the
Philippines included users of Government of the Philippines (GOP)-financed primary
healthcare services, especially for vaccinations.
1.5 Original Components
12. Project activities were grouped into four main components: health financing,
health service delivery, regulation of pharmaceuticals, and health system governance.

4
Component A: Health Financing (US$50 million at appraisal; US$40 million
approved)
13. The component was intended to provide health insurance for indigents through
financing GOP’s payments to PhilHealth under the national contribution subsidy. To
identify beneficiaries, LGUs were to use acceptable, defined methods of means testing,
that were acceptable to PhilHealth and the Bank. Bank financing of premiums for
indigent households was expected to increase over the life of the project as more LGUs
implemented community-based poverty mapping (or other acceptable means tests) and
used this as a basis for identifying indigent beneficiaries.
14. In support of project objectives and the health reform strategy, PhilHealth was to
pursue the following reforms: (1) sustainable expansion of the regular Indigent Program;
(2) better targeting of the poor through (i) collaboration to encourage LGUs to scale up
community-based poverty mapping to identify poor households, and (ii) development of
a policy on acceptable alternative means tests; (3) development of a partially subsidized
health insurance scheme for the near-poor; (4) increased financial protection for NHIP
members through (i) improved membership services, (ii) preferred provider agreements
that limited extra billing, and (iii) incremental enhancement of the benefits package
targeted at cost-effective services, especially services benefiting the poor and helping to
achieve the Millennium Development Goals (MDGs); and (5) fostering synergies and a
convergent approach through coordination with other agencies concerned with the health
sector reform program.
Component B: Health Service Delivery: Public Health (US$48.5 million at
appraisal; US$38.5 approved)
B.1 Disease Prevention, Control and Elimination Programs (US$48 million at appraisal;
US$38 million approved)
15. The component was intended to support disease prevention and control measures
to eliminate, or reduce and control infectious diseases and micronutrient deficiencies.
This would be through provision of: Expanded Program of Immunization (EPI) vaccines
(including hepatitis B vaccines); tuberculosis control (TBC) drugs; laboratory supplies;
HIV/AIDS drugs; micronutrients; other drugs and related commodities; as well as
information and education materials to help eradicate malaria, rabies, leprosy,
schistosomiasis and filiarisis. Some of the commodities provided under this component (a
minimum of around US$5 million) were to be allocated on the basis of LGU performance,
as indicated under sub-component B.2.
B.2 Performance-based Resource Allocation for Public Health (US$0.5 million at
appraisal and as approved)
16. The project was intended to support the development of: (1) pilot service
performance agreements between the DOH and participating LGUs for carrying out Part
B.l of the Project; and (2) pilot performance-based public health award schemes for those

5
LGUs that met or exceeded their performance targets for measurable improvement in
disease prevention and control in carrying out Part B.l and Part B.2 of the project.
Component C: Regulation of Pharmaceuticals (US$0.5 million at appraisal and as
approved)
17. The component was intended to support implementation of a master plan to
upgrade the services of the Bureau of Food and Drugs (BFAD) in regulating the
manufacture, importing and distribution of pharmaceuticals. This was to be achieved
through support for the operating costs associated with new business processes, including
greater fiscal autonomy for the BFAD; improved services at its drug quality control
laboratories; and implementing a new program of providing “quality seals” to certify
pharmacies that offer quality drugs at competitive prices. Subject to resolution of a legal
question regarding use of the BFAD’s fee income, at the GOP’s request, the project
provided an option for the unallocated portion of the loan to finance US$5 million worth
of equipment upgrades in BFAD laboratories.
Component D: Health System Governance (US$10.725 million at appraisal and as
approved)
D.1 Health Human Resources (US$0.5 million at appraisal and as approved)
18. The sub-component was intended to support the development of strategic national
initiatives in the DOH’s human resources in health (HRH) master plan, especially the
deployment of health professionals to rural areas to reduce the shortage of doctors and
other health professionals, and provision of training, career path development, and job
information services for health professionals in rural areas.
D.2 Sector Management and Coordination of Local Health Systems Reform (US$10.225
million at appraisal and as approved)
19. The sub-component was intended to support the DOH’s contribution to an EC-
financed program of performance-linked local health systems reform grants for 16 F1
“convergence provinces”. 2 This was to assist LGUs in implementing the HSRA
implementation plan. DOH was to finance local capacity building, systems development,
and monitoring and evaluation (M&E). In coordination with support from other
development partners, this sub-component was designed also to finance DOH’s
contribution to a sector-wide program of M&E for the implementation of the health
sector reform program.
2 The EC-financed program provided performance-linked local health systems reform grants to LGUs in 16 F1
“convergence” provinces. The program, which was worth a total of US$15 million over three years, also provided US$ 1.2 million to the GOP to help strengthen the DOH’s internal management systems.

6
D.3 Strengthening the DOH’s Internal Management Systems (funded by the EC Trust
Fund)
20. Building on earlier financial management reforms under the Second Social
Expenditure Management Project (SEMP 2), the project was to: strengthen DOH’s public
financial management systems; integrate DOH management information systems;
upgrade DOH materials management systems through provision of hardware, software
and technical assistance; and train DOH staff in financial management, inventory and
materials management, procurement, and internal audit. This part of the project was
financed from a US$1.2 million grant to the GOP from the EC, and administered by the
World Bank as a Trust Fund.
21. The Loan Agreement also earmarked an unallocated expenditure category of
US$20 million to be allocated at a later date to project components with the fastest pace
of reform.
1.6 Revised Components
22. The components were not revised.
1.7 Other significant changes
23. The project underwent level-II restructuring twice. In August 2010, the
restructuring was for the reallocation of funds from the unallocated expenditure category
(US$20 million) and a reallocation from slower-performing components to faster-
performing components. The restructuring document stated that there would be no
extension of the project’s closing date (June 30, 2011). The table below summarizes the
allocations before and after restructuring, as well as after the project’s end-of-
disbursement date (August 2012).
Project
Component
At Approval
(US$)
After
Restructuring
(US$)
Actual
disbursement
(US$)
% of
utilization
Component A 40,000,000 40,000,000 44,024,443.48 110.06
Component B 38,500,000 59,225,000 49,643,892.77 84.00
Sub-component
B1
38,000,000 58,225,000 48,664,257.03 83.58
Sub-component
B2
500,000 1,000,000 979,635.74 97.96
Component C 500,000 150,000 0 0
Component D 10,725,000 10,350,000 10,774,644.42 107.75
Sub-component
D1
500,000 350,000 0 0.00
Sub-component
D2
10,225,000 10,000,000 10,774,644.42 107.75
Unallocated 20,000,000 0 0 0
Front-end Fee 275,000 275,000 275,000.00 100.00
Total 110,000,000 110,000,000 104,717,980.67 95.20

7
24. The second restructuring took place in May 2011 to extend the project’s closing
date from June 30, 2011 to March 31, 2012. This extension was necessary to complete
implementation and reimbursement of project components, particularly the health
financing component. With PhilHealth then enrolling all the NHTS-identified poor
households, the DOH needed time to complete documentation of enrollments and to
calculate the National Government’s subsidies that the project was to finance. At the time
of the restructuring, DOH expected that nine months would be sufficient to complete all
activities, process reimbursements, and liquidate all advances, especially those for
vaccine purchases. DOH also expected to use the full amount that had been allocated.
2. Key Factors Affecting Implementation and Outcomes
2.1 Project Preparation, Design and Quality at Entry
25. The project design was finalized under a changing policy context that had to
balance the latest developments in both the Borrower’s and the Bank’s thinking about
how a health sector reform project should be designed for a middle-income country. The
Bank team sought to address the changing context and at the same time ensure that the
Borrower’s “ownership” of the project was fully secured. The project was originally
conceived of as a traditional investment loan that would support health system reform in
four provinces and would develop national-level policy and capacity in both the DOH
and PhilHealth. This was much more modest than the final design of the project. Taking
into account the lessons learned from the two Social Expenditure Management Projects
(SEMP),3 the Bank proposed implementing sector budget support through a National
Sector Support (NSS) approach. This was applied to the health and the education sectors.
As in the case of the SEMP projects, financing was underpinned by requirements to
improve the management of specific line items. The Country Assistance Strategy for
2006-2008 had proposed that future lending for national government agencies should be
programmatic and support reform through regular government programs and budgets. At
the same time, lending to LGUs should be offered separately and principally through a
multi-sector local lending platform.
26. On the Borrower’s side, the DOH had adopted the concept of the SDAH to
harmonize donor financing for the health sector. Thus, at the macro-level, the design of
the NSS approach for health was fully consistent with the Borrower’s thinking and there
was high ownership of the approach.
27. The DOH was also no longer interested in a narrow focus – as was the case under
the SEMP, which had mainly focused on procurement of public health goods and
commodities. In line with F1, it expected the NSS approach to be aligned with the broad
3 In the aftermath of the Asian financial crisis of 1997, the World Bank supported the GOP in protecting basic social
services (health education and social welfare) while at the same time leveraging overall improvements in levels of, and
allocation of public spending in these sectors, through two social expenditure management projects (SEMP 1 and 2).
These projects which operated under the broad stewardship of the DBM provided budget support for specific line items
of the sector budget.

8
health sector reform agenda of the GOP. The design team tried to marry the expectations
of both the Borrower and the Bank, and reflect these in the final project design, but the
team perhaps deeply under-estimated the capacity of the DOH to implement a budget
support approach on its own, with the Department of Budget and Management (DBM)
providing arm’s length oversight. The design team also perhaps over-estimated the speed
at which F1 reforms would be implemented.
28. In its identification of components, the project design was fully consistent with
the F1 reforms and included both PhilHealth reforms as well as LGU reforms. For
PhilHealth, a key issue was how poor households were to be identified. At the time of the
project, the LGUs had no consistent criteria for identifying poor households and thus the
project proposed that the LGUs use the Community-Based Monitoring System (CBMS).
The adoption and application of the CBMS was expected to align with the expansion of
providing PhilHealth health insurance for poor households.
29. The LGU component was absolutely essential to increase DOH stewardship of the
LGUs, and to ensure that the LGUs regularly provided health data to the DOH. A key
reform element was creating peer pressure among LGUs to perform better by
disseminating their annual scores on the LGU scorecard. In both health financing and
LGU components, the willingness and commitment of the LGUs to reform was perhaps
over-estimated. As implementation would show later, uptake of national reforms by the
LGUs was slow. This demonstrates that at the project design stage, more careful thinking
should have been given to the incentives provided for LGU engagement.
30. The procurement of key public health goods was a continuation of the SEMP 2,
and to enhance DOH stewardship of the LGUs, two small components on strengthening
regulatory capacity and governance of the DOH were added to support the F1 approach.
This was consistent with the intention that the project would support all four pillars of the
F1 reforms, while financing only a small part of the cost.
31. The project underwent a Quality Enhancement Review (QER) process in
February 2006. The QER panel was concerned with the capacity of the DOH to operate
under the new NSS approach, and recommended that more high-level stakeholders, such
as the DBM, Department of Finance (DOF), and National Economic Development
Authority (NEDA) be directly involved in the reform process. In line with the
recommendations of the QER panel, PDOs were revised to be more modest and specific,
most disbursement conditions were eliminated, the financial management risk rating of
the project was clarified, the active role of the DBM in the project was clearly identified
in the PAD, and financial management and actuarial assessments of PhilHealth were
initiated.
32. The negotiations took place in May 2006, and the World Bank Board approved
the project on June 29, 2006. Although the Loan Agreement was signed on October 3,
2006, it was not until March 27, 2007 that the project was declared effective. This
perhaps indicates that some issues about readiness for implementation were not
adequately addressed during the design stage. Visions differed between the DOH and the

9
DBM about whether to establish a “special account” and this delayed completion of the
project’s operational manual. This was finally resolved through the DOH and the DBM
agreeing to utilize the DBM’s reimbursement mechanisms if the DBM committed to
providing the DOH with adequate up-front releases of funds so that the DOH could
implement project reforms.
33. Even though the project was designed to operate within the framework of the
DOH, which used a programmatic and an SDAH approach (and within these financed
selected priority national elements that were ready for implementation), it should be
noted that the project’s design lacked flexibility. This resulted in relatively inflexible
sector budget support. The project was not sufficiently “sector wide” to allow for
financing to move frequently and flexibly from one budget line to another, without major
restructuring. Additionally, the design of M&E indicators and the institutional
arrangements for M&E were weak. These M&E design issues, which are described in
greater details below under the M&E section, plagued the project throughout
implementation.
2.2 Implementation
34. With the exception of Component B1, implementation of most project
components encountered substantial delays. Factors that likely led to slow disbursement
are described below. Component B1 disbursed funds the fastest throughout the whole
project. Perhaps this was because procuring vaccines through negotiated contracts with
UNICEF was relatively straightforward. Also the DOH had gained commodity
procurement experience under SEMP 2, so this was an area where DOH capacity in
implementation was already high.
35. Component A was the slowest to disburse. At the time of project negotiations, it
was agreed that the CBMS would be the primary means of identifying indigent
households. However, soon after the project became effective, the National Government
(NG) adopted the National Household Targeting System - Poverty Reduction (NHTS-PR)
under the Department of Social Welfare and Development (DSWD). The World Bank
had provided support for this major policy development through technical assistance.
This was the first time in the Philippines that a refined targeting mechanism, based on a
well-accepted proxy means test (PMT) methodology was available. Once this tool was
available, the GOP wanted to apply it to all NG-financed social assistance programs,
which included NG’s financing for poor households. The Bank supported the GOP’s
approach, although disbursements under the project were substantially delayed.
PhilHealth had to cross-match the list generated through the NHTS-PR with the existing
list of sponsored members. Other issues had to be resolved such as the NG-LGU cost
sharing arrangement under the NHIP. However, this was a significant policy success as it
led to enrollment of around 4.3 million households (approximately 20% of the
population) who had never had health insurance before. Use of the NHTS-PR also paved
the way for the GOP to scale up universal health care (UHC) which the Bank is expecting
to support through a new lending operation. Thus, while disbursements were significantly
delayed, the policy outcome was substantial.
10
36. Components B2 and D2 were initially delayed due to the delays in the completion
of operational manuals required for their disbursement. This indicates issues in readiness
to implement that should have been addressed at the preparation stage. After these issues
were addressed, Component D2 progressed positively. Component B2 progressed more
slowly, and only in the final months of the project was an agreement reached that the loan
money could be used to reimburse funds for the Maternal, Newborn, Child Health and
Nutrition (MNCHN) grants that the DOH had awarded to the LGUs in 2009 and 2010.
37. Components C and D1 were initially delayed due to prolonged discussions about
which specific BFAD- and HRH-related budget line items the NSSHRP was to finance.
The implementation of Component C was also affected by the 2008/2009 legislation that
ensured full income retention for the BFAD, strengthened its regulatory powers, and
renamed the BFAD as the Food and Drug Administration (FDA). The specific FDA
activity to be financed by the NSSHRP was finally proposed by the DOH in 2010. The
FDA implemented Quality Management System (QMS) accreditation, but due to the
delay, the activity could not be financed from the NSSHRP. The activities under
component D1 were identified by the DOH in 2009, and procurement started in that year.
However, due to lengthy procurement problems, these activities could also not be
financed from the NSSHRP.
38. Component D3, funded by the European Commission Trust Fund, was also
initially delayed, largely due to lack of familiarity with the new tools and lengthy reviews
of investment plans, annual plans, training plans, and project procurement and
management plans. Nevertheless, there was progress made in the development of the
Expenditure Tracking System (ETS) though this is still in its development stage. DOH
staff were trained in internal audit and finance. The Electronic National Government
Accounting System was rolled out to the regions by providing hardware, software, and
technical assistance.
39. It should be noted that though the project was designed to operate within the
framework of the DOH, which used a programmatic and SDAH approach, and within
these to finance selected priority national elements that were ready for implementation,
the project was not “programmatic” enough to allow for financing to move frequently
and flexibly from one budget line to another. With the exception of the US$20 million
unallocated portion, the specific amount of financing was allocated for each project
component, and restructuring was needed to reallocate the resources. Hence, the way that
the project was implemented appeared to more “traditional” in operation than
“programmatic”.
2.3 Monitoring and Evaluation (M&E) Design, Implementation and Utilization
40. The project suffered from weaknesses in M&E at all stages – design,
implementation, and utilization. Regarding M&E design, the results framework in the
project’s Loan Agreement included a mix of outcome and intermediate indicators, though
these were not adequate. Generally, the indicators were appropriate at the time of project
design, as these were based on broader national program indicators and were the same
indicators and targets as those used by the GOP. However, there were no indicators and

11
target values to track the progress of project components C and D1. Furthermore, six
indicators in the PAD did not have baseline data. These gaps were never addressed
during implementation.
41. Consistent with the SDAH, all development partners were expected to participate
in the Joint Assessment and Planning Initiative (JAPI) that was organized by the DOH
once or twice a year. The JAPI included field visits and a concluding workshop led by
DOH staff in which development partners provided their feedback, and follow-up action
was identified. While the JAPI helped harmonize development partners’ initiatives and
reduced transaction costs for the Borrower, under JAPI it was impossible for the Bank to
undertake as rigorous due diligence that is the norm in regular Bank supervision missions.
Moreover, since the JAPI did not use a formal M&E framework aligned to the project, it
was difficult to track and report on project indicators. This is perhaps one reason why the
tracking of project’s results framework indicators was not consistent over the whole
project.
42. Perhaps for the same reasons for aligning with the JAPI, no proper Mid-Term
Review (MTR) mission took place. The lack of a full MTR was a missed opportunity for
the GOP and Bank teams to re-align project indicators and targets, clean up the results
framework, and align to the situation on the ground. As mentioned before, there was a
significant shift in the policy environment that impacted implementation of Component A.
Despite these shifts, the lack of formal acknowledgement during the MTR and the lack of
restructuring the PDOs and associated indicators that normally follows an MTR meant
that at completion the performance of the project is judged as per the situation at
appraisal. At the same time, there were policy shifts as well as implementation
experience which could have been used to restructure the project.
43. Thus, no indicators were adjusted during project implementation, despite the fact
that some indicators were no longer applicable and should have been removed or adjusted
before or during project restructuring. For example, the indicator and target values for the
component “Increase in number of LGUs identifying the poor using acceptable means
test and enrolling them in NHIP indigent program” were no longer relevant by the time of
project restructuring in 2010 and 2011 since the Bank, DOH, and PhilHealth agreed to
use the NHTS-PR and enrolled the poor who were identified by the NHTS-PR in the
NHIP Indigent Program, instead of relying on LGUs to identify the poor using an
acceptable means test.
44. Based on available information, the ICR team concluded that during
implementation, the results framework for the project was not properly tracked by either
the Borrower or the Bank. In addition, the government did not submit annual project
Progress Reports to the Bank.4 Although according to the Loan Agreement, starting in
2007, the DOH was to submit an annual report to the Bank no later than March 31 of
4 The DOH produced annual reports on broader health collaboration, but there were no NSSHRP-specific indicators in
the report.

12
each year, this did not occur.5 Furthermore, efforts to identify the methods for tracking the
progress of certain objectives and targets were inadequate. For example, despite being
required in the PDO, at the time of project design no method was identified for tracking
the utilization of health services by the poor, and this problem was not addressed during
project implementation.
45. Despite the weaknesses in project M&E, specific M&E activities for Component
D2 “Sector Management and Coordination of Local Health Systems Reform” progressed
well. Although in the beginning, the DOH M&E framework initially proposed a long list
of indicators, without a clear strategy for data collection, the issues were later addressed.
The LGU scorecard later became one of the GOP’s flagship products, and was rolled out
from 16 convergence provinces to the rest of the country. While the DOH was unable to
obtain health data from the LGUs on a regular basis prior to implementation of the LGU
scorecard, the introduction of the scorecard, which was broadly supported under the
rubric of the project, has been successful in changing this pattern and provides a
framework for DOH-LGU relations that can be pursued through future reforms.
46. With regard to M&E utilization at the project level, M&E data were not used
sufficiently to inform decision-making and resource allocation. Decisions about where to
allocate and re-allocate project resources appear to have been based on where
disbursement was quickest, which was to support the purchase of public health
commodities (Component B). However, this did not take into consideration the
performance-based aspect of resource allocation, which was stated in the PAD.
Nevertheless, M&E data were appropriately utilized in Component D2. The DOH used
the Service Level Agreements (SLA) and the LGU scorecards to monitor performance in
all provinces, and scores based on the achievement of SLA performance targets were
released together with the corresponding variable tranches that the DOH provided to the
LGUs.
2.4 Safeguard and Fiduciary Compliance
47. Environment: The project did not trigger the environmental safeguard policy; it
was rated as environmental category “C”, which meant that no specific environmental
safeguards were required. The project did not invest in civil works or other activities in
health facilities that could have any significant impact on the environment.
48. Indigenous People: The project did not have any potential adverse impacts on
indigenous people. On the contrary, the project contributed positively to indigenous
people who benefited from the intensified public health efforts and expanded coverage
under the Indigent Program of PhilHealth. The Indigenous People Safeguard Policy
(OP/BP 4.10) was triggered by this positive impact. Related to this, the DOH
implemented an Indigenous People Planning Framework (IPPF), which outlined the
5 The annual report was expected to include (i) results of the monitoring and evaluation activities on the progress
achieved in carrying out the project during the 12-month period preceding the date of the report; (ii) setting out the
measures recommended to address problems and improve project efficiency.

13
measures that the DOH and PhilHealth had adopted to ensure that the health sector
reform program supported by the project adequately addressed the needs and cultural
preferences of indigenous people, and that the indigenous people participated in the
benefits of the reform program. The results of implementing the IPPF were mixed, with
some measures initiated but not completed. Some provinces also moved ahead on IP
issues faster than others (e.g. Oriental Mindoro, Ifugao, and Mountain Province).
49. Procurement: During the early years of project procurement, performance was
rated by the Bank team as moderately unsatisfactory. Progress occurred only in
Component 2, while the other components moved very slowly, because the project
encountered a number of systemic procurement challenges. First, procurement planning
was not systematic, leading to stock-outs in a number of cases. Second, there were delays
in the procurement of drugs and vaccines due to: (i) finalization of the Bank-required
memorandum of understanding (MoU) between the DOH and United Nations (UN)
agencies with regard to the procurement of drugs and vaccines from project resources;
and (ii) difficulties that the DOH had in complying with the rules of the Central Bank of
the Philippines regarding the purchase of dollars that were needed for advance payment
to UN agencies. The DOH also planned to procure TBC drugs through the World Health
Organization (WHO) using project resources, but the DOH and the WHO were not able
to reach agreement on certain issues and failed to sign the MoU, leading to a shortage of
TBC drugs in 2009.6 To address this shortage, the DOH shifted its procurement approach
to national competitive bidding (NCB), and was able to procure TBC drugs and other
drugs locally. The issue with the Central Bank was later resolved through the World
Bank making advance payments directly to UNICEF.
50. It should also be noted that the Bank’s position on procurement through
negotiated contracts with UN agencies changed over time. Prior to, and in the early years
of the NSSHRP, the Bank supported the procurement of vaccines and drugs through
negotiated contracts with UN agencies. However, the Bank advised the DOH in 2010 that
following that year, vaccines and drugs would have to be procured on a competitive basis.
Nevertheless, as explained later in this document, the DOH saw the benefits of procuring
vaccines through negotiated contracts with UNICEF and continued the practice with
DOH’s resources.
51. Financial Management: In the early years of the project, there were a number of
financial management challenges, primarily due to inadequate staffing at both the agency
and project level, leading to delayed recording and financial reporting and weaknesses in
internal control. The DOH committed to address the weaknesses, and the situation
improved gradually as more staff were hired to address financial management issues.
However, despite the improvement, delays in the submission of complete quarterly
financial reports, audit reports, and information from warehouses on the issuance of drugs
continued to some extent.
6 The main concern was about a clause related to governance and anti-corruption.

14
2.5 Post-completion Operation/Next Phase
52. The health financing reform, which includes the aim of increasing financial
protection for indigent households, started during the implementation of the NSSHRP, is
expected to be continued and enhanced by the proposed National Sector Support for
Kalusugan Pangkalahatan (Universal Health Care) project, which is expected to receive
support from the World Bank. The proposed UHC project will tackle issues that were not
fully addressed under the NSSHRP. This may comprise enrolling more NHTS-PR
households (the near-poor) into the NHIP, implementing the enhanced NHIP benefits
package, and supporting NHIP reform through improving health services delivery. The
proposed UHC project is expected to build upon the lessons learned from the NSSHRP
by strongly emphasizing monitoring and evaluation. In addition, the current CAS
(FY2010-2013) has adopted the National Program Support (NPS) model as a key
instrument for support to social sectors.
3. Assessment of Outcomes
3.1 Relevance of Objectives, Design and Implementation
Rating: Substantial
53. Overall, relevance was rated as substantial. The PDOs remain highly relevant for
the Philippines as it strives to achieve UHC by 2016. The health financing component of
the project (Component A) has been instrumental in pushing ahead the agenda of
enrollment of the poorest households in the Philippines into PhilHealth’s Indigent
Program, using a transparent targeting mechanism. Prior to this project, there was no one
defined, uniform instrument that could be used to target the poor. This resulted in
politicization of enrollment of the poor at the LGU level. Although the project took a
long time to disburse Component A due to this LGU constraint, through introduction of
the NHTS-PR, the project eventually delivered a better method of identifying the poor so
that they could be enrolled into the Indigent Program. The Indigent Program is now being
scaled up by the NG to also include the near-poor in the program.
54. The project design features that focused on financial protection for the poor,
public health service delivery, and performance-linked Local Health Systems Reform
were highly relevant, and fully aligned with both the World Bank’s current CAS
(FY2010-13) and the government’s current national development strategy (Philippines
Development Plan 2011-2016), which supports UHC in order to achieve better health
outcomes, fair health financing and responsive health systems that provide all Filipinos,
especially the disadvantaged groups, with equitable access to quality health care and
improved financial risk protection.
3.2 Achievement of Project Development Objectives
Rating: Moderately Unsatisfactory
55. The Bank’s final evaluation was based on the project’s results framework and
established targets, as well as available evidence and data. Outcomes by PDO are briefly
summarized below.
15
a. Improving priority public health outcomes and increasing the utilization of health
services by the poor in areas and for conditions or diseases subject to intervention under
the project.
56. Based on available data, the project did not contribute to the improvement of
priority public health outcomes, as specified in the PAD and Loan Agreement. The
targets for all three indicators (FIC rate, TB case detection rate, and TB cure rate) were
not achieved by the final year of the project. The latest FIC and TB cure rates improved
slightly from the baseline, but fell behind the target, while the latest TB case detection
rate was the same as the baseline. However, the available data also show inconsistencies,
with exceptionally high performance in the years immediately following the baseline
(2005), and a decline in performance in the later years of the project.7 The data for these
indicators were obtained from the Field Health Service Information System (FHSIS), but
some data were inaccurate. Some numbers were simply erroneous and others were out of
date. To improve data quality, a data quality check (DQC) was initiated by the DOH, but
the results were not available when needed for validating project data. Moreover, the
immunization indicator was adversely affected by using the wrong denominator. 8
Indicators Baseline 2006 2007 2008 2009 2010 2011 Targets
Fully immunized
children rate
80% 92% 90% 91% 88% 84% 85%9 90%
TB case detection rate 72% 74% 75% 72% 71% 72% N/A 80%
TB cure rate 81%% 83% 82% 79% 80% 82% N/A 85% Source: DOH
57. Even though the targets for priority public health outcome indicators specified in
the Loan Agreement were not met, there were specific disease indicators outside the
project’s results framework that showed marked improvement in the past five years.
These included the sharp decline in morbidity rates for acute lower respiratory tract
infection, pneumonia, leptospirosis, malaria, neonatal tetanus and schistomiasis, and
continuing low morbidity rates for cholera, diphtheria, and filariasis. Nevertheless, some
disease-specific challenges continue. Morbidity rates for leprosy and rabies have risen
sharply since 2009. Also, the Philippines is one of the only nine countries in the world
with an increasing number of HIV cases.
58. The project did not indicate the methods on how to track the utilization of health
services by the poor, and this issue was not addressed during project implementation.
Thus, it was not feasible at the end of the project to generate evidence that there had been
an increase in the utilization of health services by the poor.
b. Increasing financial protection of indigents from health care costs.
7 The ICR Team explored possible reasons for the poor FIC rate, TB case detection rate, and TB cure rates with DOH
staff, and they indicated that these rates may not include comprehensive data from private health care providers. 8 The new census data are now officially available and indicators, such as the FIC indicator will need to be re-calibrated. 9 Data from the Family Health Survey 2011.

16
59. There were two indicators defined for measuring financial protection: (i) an
increased number of indigent families enrolled into the NHIP, and (ii) insured indigent
households have lower OOP spending on health, compared to uninsured households and
compared to prior periods.
60. The first indicator has been achieved, and the outcome has exceeded the target by
far. The project led to the enrollment of an additional 4.3 million indigent households into
PhilHealth’s Indigent Program.10 These are the poorest households in the Philippines and
were never enrolled into the NHIP through the LGU targeted program. This has increased
health coverage for the total population from 55% to 75%. Nevertheless, one constraint is
that these enrollment data have not been verified yet (by checking whether new enrollees
know that they had been enrolled into the NHIP).
61. The second indicator has not been achieved. This was expected since this group
was only enrolled under the NHIP in April 2011. Also, the PhilHealth benefits package
did not expand significantly during the period covered by the project. Increased financial
protection, as measured by reduced out-of-pocket spending on health, can only be
expected if the benefits package addresses gaps in coverage. These reforms are only just
beginning in PhilHealth.
62. Based on the lack of verifiable data for the PDO indicators and the project’s
inability to meet the targets set for priority health outcomes, but taking into account the
large increase in the number of indigent families enrolled into the NHIP, and marked
improvement in several disease-specific indicators outside of the project’s results
framework, development outcomes for the project have been rated as moderately
unsatisfactory. A summary of intermediate outcome results’ indicators by project
components is described below, while a more detailed discussion is provided in Annex 2.
Component A: Health Financing (US$44.024 million actual; US$40 million in the
Loan Agreement)
63. Overall, the rating for this component was judged to be satisfactory. The initial
efforts to encourage the LGUs to identify the poor using acceptable, defined methods of
means testing, e.g. CBMS, were plagued by deep-seated local political and governance
issues. When the DSWD successfully identified the poor by using the NHTS-PR,
PhilHealth exerted its efforts to convince LGU officials to enroll into the Indigent
Program all NHTS-identified households. However, no LGUs accepted this method.
Given the constraints on the LGU part, the project turned to the NG to support the
enrollment of the poor into the NHIP Indigent Program, using NHTS-PR. This is clearly
a significant policy progress that goes far beyond the project’s own objectives. With the
support of the NG, the project is able to identify the poor using NHTS-PR, which is an
acceptable, defined method of means testing and enrolled about 5.2 million poor
10 NHTS identified 5.2 million indigent households. Out of these, around 900,000 households were already on
PhilHealth’s Indigent Program list (identified by LGUs).

17
households into the NHIP Indigent Program in the final year of the project. In addition,
the original method of having the LGUs identifying the poor using CBMS was expected
to bring only 1.51 million poor households into NHIP Indigent Program by the end of the
project.11 Thus, the project has actually brought more than three times poor households
into the Indigent Program. Moreover, when PhilHealth cross-matched the NHTS-PR’s
list of poor households with the list of poor households identified by the LGUs, this
showed evidence of political influence and governance problems. Out of the 5.2 million
households that have been identified as poor using the NHTS-PR, only 912,696
households on the NHTS-PR list matched the list of over 6 million households originally
identified by LGUs as poor. This raises the suspicion that many of the households on the
LGU list were not actually poor.12
64. Some shortcomings remain. There was limited progress in the development of a
partially subsidized scheme for the near-poor. In addition, PhilHealth made slow progress
in increasing financial protection for existing members through preferred provider
agreements to limit extra billing and incremental enhancement of benefits package.
Furthermore, as explained above, many LGUs had disagreed with the NHTS-PR, and
refused to pay the premiums of the poor households that were identified by using NHTS-
PR. As a remedy measure, the premiums of the poor identified by using NHTS-PR are
paid by the NG, backed by the Joint Implementation Guideline adopted by DBM, DOH
and PhilHealth, while the premiums of the “poor” identified by LGU undefined methods
were paid by the LGUs.13 Challenges to be resolved in future are how to get the LGUs to
agree to co-pay the premiums for poor households identified under the NHTS-PR to
make the funding arrangement more sustainable, and how to address the problem of the
LGUs enrolling “poor” households that are not actually poor into the Indigent Program
and paying for their insurance premiums.
Component B1 and B2: Health Service Delivery: Public Health (US$49.643 million
actual; US$38.5 million in the Loan Agreement)
65. Overall performance for this component B1/B2 was judged to be moderately
unsatisfactory. Operationally, component B (driven by sub-component B1) was the
quickest-moving project component, with a high disbursement rate. Nearly half of the
loan was used for the purchase of vaccines and other public health commodities, largely
through UNICEF. However, the outcomes of the component appeared to be poor. Targets
for the five indicators in the Loan Agreement, used for tracking the progress of this
component, were not met. The first three indicators were similar to those used to track the
PDO – FIC rate, TB case detection rate, and TB cure rate. The latest FIC and TB cure
11 This target is stated in the PAD, but was later dropped by the government and does not appear in the Loan
Agreement. The national government dropped this indicator because it is beyond NG control. 12 The number of “poor” households identified by LGUs is around 6-7 million households. 13 As a remedy measure, the LGUs continue to pay the premiums for the LGU-identified poor, despite the fact that
these poor households were not identified by an acceptable, defined means test. Out of 5.2 million households that were
identified as poor using the NHTS-PR, only 912,696 families were identified by LGUs as poor. This indicates a serious
shortcoming in the method that the LGUs used for identifying the poor, and raises concerns that many of the
households identified by LGUs as ‘poor’ were not actually poor.
18
rates improved slightly from the baseline, but fell behind the target, while the latest TB
case detection rate was the same as the baseline. The target for the fourth indicator was
not met, as no method for validation was finalized nor did monitoring take place. 14
According to the DOH, the reason for not achieving this target was difficulty in coming
up with evidence of a statistically significant improvement. Also the DOH was not able
to identify a third party to validate an alternative method, as planned. The target for the
fifth indicator was also not met (quarterly reporting on inventory and method of
forecasting quantities required of public health commodities satisfactory to the Bank as
well as baseline data on stock levels/losses/targets agreed for each year).15 The teams of
the DOH and the Bank have explained that no data were available. The DOH could have
tracked data down to DOH’s Center for Health Development (CHD) at the regional level;
however, it was difficult to get data from the LGUs, as this was not part of the LGU
reporting mechanism. This highlights that, despite the availability of SLA, governance
issues occurred in central-local relations in the health system.
66. Another important reform that the project component failed to implement was
allocating commodities to different LGUs on the basis of appropriate and transparent
criteria combining considerations of both performance and need, despite the fact that the
project should have allocated at least US$5 million on the basis of performance. DOH
staff have explained that implementing the reform would have negatively affected the
residents of poor-performing LGUs, rather than the LGU administrators themselves.
However, the DOH did not raise this concern, as it should have, during project design and
appraisal.
67. Despite the failure to meet all results targets, the project significantly helped the
country’s immunization program and it financed the procurement of all necessary
Hepatitis B vaccines, and the first ever procurement of Hemophilus influenza B (HiB)
and Measles, Mumps and Rubella (MMR) vaccines. In addition, the project partially
contributed to increasing the share of the public health program out of total government
health spending. Prior to the project, the public health program’s share of total
government health spending (excluding staff salaries) was 25%, while 65% went into
hospital operations. By 2012, the public health program, which is considered pro-poor,
received 50-55% of total government health spending. Moreover, procurement of
essential vaccines and other commodities through UNICEF offered significant benefits to
the Philippines. Not only did it ensure the quality of vaccines,16 UNICEF also provided
technical advice to the government on improving its capacity to forecast and budget for
public health commodities, as well as to improve cold chain management. In addition, the
2008 logistics review showed important improvements in the country's cold chain
facilities, which were intact at the very least up to the level of municipalities.
14 The fourth indicator was “evidence of a statistically significant improvement or validation by an alternative method
of improvement, in prevention, diagnosis or treatment rates in participating LGUs for diseases or conditions subject to
performance agreements and grants (from 0 LGU to 15 LGUs)”. 15 The fifth indicator was “significant quantified reductions in date-expiry, stock-outs and losses of public health
commodity stocks at defined levels in supply chain”. 16 Previously the government experienced quality problems when procuring vaccines through nationally competitive
bidding.

19
Component C: Regulation of Pharmaceuticals (US$0 actual; US$0.5 million in the
Loan Agreement)
68. Overall performance for this component was judged to be unsatisfactory,
reflecting chronic and systemic lack of progress. This component encountered severe
shortcomings. First, there was no indicator for this component in the Loan Agreement,
which made M&E difficult. Second, the BFAD/FDA did not appear to be enthusiastic
about implementing activities using the loan. This is partly due to the fact that the loan
was for budget support and did not provide a new source of money for the BFAD/FDA.
On the other hand, the use of the Bank’s loan can be viewed as adding burdens to
BFAD/FDA staff, as the staff needed to learn and follow new procedures. Third, the
BFAD/FDA suffered from chronic shortage of competent managers, which severely
delayed BFAD/FDA’s key reform agendas. Finally, there appeared to be a lack of
coordination between the FDA and the BIHC regarding the project’s closing date, so the
FDA was unable to use the loan money to finance quality assurance activities.
Component D1: Health Human Resources (US$0 actual; US$0.5 million in the Loan
Agreement)
69. Overall performance for this component was judged to be unsatisfactory,
reflecting systemic lack of progress. Operationally, this component encountered severe
shortcomings. First, there was no indicator for this component in the Loan Agreement,
which made it difficult to carry out M&E. Second, those managing the DOH HRH unit
did not appear enthusiastic about implementing activities using the loan. This is partly
due to the fact that the loan was for budget support and did not provide a new source of
money for the HRH unit. On the other hand, the use of the Bank’s loan can be viewed as
adding burdens to HRH unit staff, as they had to learn and follow new procedures in
using the loan. Also, there was a lack of coordination between the BIHC and the HRH
unit in facilitating the HRH unit to use the loan money. Although the project’s HRH
component did not progress, it should be noted that there were positive development on
HRH activities financed by DOH own resources. This included the implementation of
programs to deploy health professionals to rural and under-served areas, particularly
Doctors to the Barrios (medical doctors), RNHeals (nurses) and midwives deployment
programs.
Component D2: Sector Management and Coordination of Local Health Systems
Reform (US$10.774 million actual; US$10.225 million in the Loan Agreement)
70. Overall performance for this component was judged to be satisfactory, reflecting
the rapid progress in implementing SLA and LGU scorecards, as well as the use of M&E
data from LGU scorecards that is linked with variable tranches from the DOH to the
LGUs. This achievement has gone beyond the target of LGU scorecards being
implemented in 16 F1 provinces, as the implementation of LGU scorecard has been
rolled out nationwide. Since the SLA for all 16 F1 provinces was finalized by July 2007,
it has been used, revised, and improved over the years. The implementation was

20
successful, and DOH in 2010 decided to roll out the use of LGU scorecard in monitoring
the performance of all provinces, in addition to 16 F1 provinces. There is, of course,
room for improvement in future, as the data is self-reported by the LGUs, and the DOH
should put in place a system for the validation of these reports.
Component D3: Strengthening DOH internal management systems (financed by the
EC Trust Fund for the amount of US$1.2 million)
71. This component supported the strengthening of DOH public financial
management systems, integrated its management information systems, and trained DOH
staff in financial management, procurement, and internal audit. Overall implementation
for this component was judged to be satisfactory. This reflects: continued full compliance
with the Bank’s procurement procedures and standards; monitoring using agency
procurement benchmark indicators; training of and over 80% of internal audit (IA) staff
to meet international IA standards; and implementing the annual IA plan for scheduled
audits. The DOH was also able to roll out the Electronic National Government
Accounting System (eNGAS). By the end of the project, the eNGAS was in full use in 5
CHDs, 7 CHDs were in a transition phase, and the eNGAS was being rolled out in
another 4 CHDs. In all the CHDs, quarterly reports were submitted to managers on
performance against plan and budget under the GAA program structure. Even though
roll-out of the eNGAS was slower than the project targets, the DOH should be given
credit for its persistence in expanding use of the eNGAS. The DOH persevered in using
the eNGAS, despite the fact that in 2008 the Commission on Audit (COA) decided to
suspend the national roll-out of the eNGAS and stop supporting the DOH in
implementing the eNGAS, while waiting for a new comprehensive system (which was
still not available at the time of ICR). After COA’s decision to suspend the roll-out of the
eNGAS, this project indicator and its target values should have been adjusted, but since
no MTR was conducted, this did not occur.
3.3 Efficiency
Rating: Modest
72. Net present value, economic and financial rate of return, and cost-effectiveness
were not calculated a priori for the project.17 Overall national health spending shows
mixed results. Out-of-pocket spending continued to be the largest source of health
spending (54%). Nevertheless, ever since the current government came on board in May
2010, there was a strong commitment to health spending, and the DOH budget has
increased significantly – from PhP31 billion in 2011, to PhP42 billion in 2012, and
PhP53.8 billion in 2013. An increasingly larger share of the DOH budget now goes to
financing premiums for indigents – from PhP3 billion in 2011 to PhP12.6 billion in 2012.
As indicated above, there was also an increase in the public health program’s share of
17 The efficiency section of the PAD does not provide economic and financial analysis, but more of a national budget
execution review.
21
total government health spending, rising from 25% prior to the project to 50-55% by
2012.18
73. The efficiency of project execution, as measured by the speed of disbursement,
was very poor. Actual disbursement significantly lagged behind the plan, and over half of
the project’s resources were disbursed only in the last year before the project closed.
There were also inactive component and sub-component, which were never disbursed.
There were inadequate efforts by the government and the Bank team to re-allocate
resources from these inactive sub-components to active ones. Essentially, slow
disbursement imposes opportunity costs by tying up resources that could have been made
available to other projects or activities.
74. Despite the inefficiency of project execution, the project achieved a limited level
of efficiency through expenditures on vaccinations, which are considered a cost-effective
intervention. Moreover, the project also contributed to better targeting of resources at the
poor, which is theoretically an efficient way to improve health outcomes since scarce
resources are concentrated on those who are likely to have greater health deficits.
However, the enrollment of the poor into PhilHealth’s Indigent Program, using an
acceptable means test, only took place in late 2011 and 2012, and no data are available to
show that the poor made greater use of health services or had improved health outcomes.
Based on the above-mentioned assessment, the project’s overall efficiency was rated as
modest.
3.4 Justification of Overall Outcome Rating
Rating: Moderately Unsatisfactory
75. The overall outcome rating was moderately unsatisfactory based on substantial
relevance, modest efficacy, and modest efficiency. While the project has contributed to
an increase in the number of indigents covered by national health insurance, and
supported the implementation of LGU performance grants and the LGU scorecards, no
data were available to show higher utilization of health services by the poor. Nor were
data available which show that OOP payments had reduced. This was understandable,
however, since the poor households were only enrolled in April 2011, and PhilHealth
only recently enhanced its benefits packages which would ensure better financial
protection. In addition, though the project made public health products, and especially
vaccines, more available in rural areas, none of the three priority public health targets
were met.
18 Prior to the project, the share of public health program out of the government health spending (excluding staff
salaries) was 25%, while 65% went into hospital operations.

22
3.5 Overarching Themes, Other Outcomes and Impacts
(a) Poverty Impacts, Gender Aspects, and Social Development
76. No data were available that show direct impact on poverty. Nevertheless, there
were indirect impacts on poverty. Through the enrollment of 5.2 million indigent
households into PhilHealth’s Indigent Program, the project increased financial protection
of the poor from catastrophic health care costs. The project also increased the availability
of public health products, particularly vaccines, in rural areas, and these vaccines were
disproportionally provided to the poor.
(b) Institutional Change/Strengthening
77. The project made significant contributions through promoting key policy reforms,
including the identification of the poor using an acceptable, defined method of means
testing, and enrolling them en masse into PhilHealth’s Indigent Program. The project also
successfully supported the reform of providing performance-based grants to local health
systems, including the creation and use of the SLA and of the LGU scorecards. This has
strengthened coordination between the DOH and the LGUs.
(c) Other Unintended Outcomes and Impacts (positive or negative)
78. The main unintended outcome is the introduction of a new method to identify the
poor and enrolling them into PhilHealth’s Indigent Program. The new method of
identification is based on a nationally standardized proxy means test under the NHTS-PR,
conducted by DSWD. The number of beneficiaries would have been significantly fewer
if the project had followed the original plan of having the LGUs identified the poor using
acceptable, defined methods.
3.6 Summary of Findings of Beneficiary Survey and/or Stakeholder Workshops
N/A
4. Assessment of Risk to Development Outcomes Rating: Moderate
79. The risk to development outcomes has been rated as moderate. A risk to
development outcomes is sustaining the reform to increase financial protection of
indigent households so that they do not suffer from catastrophic health care costs.
According to the law, half of the financing of the government’s payments to PhilHealth
for health insurance premiums of each indigent family under the Indigent Program is
contributed by the NG, while the other half is contributed by respective LGU. However,
LGUs do not agree to pay their share of premiums for the indigents identified by PMT
method of NHTS-PR. An interim arrangement has been agreed that the NG would be
responsible for paying premiums of the indigents identified under NHTS-PR, reducing
the LGU contribution to zero. On the other hand, the LGUs would be responsible for
paying premiums of the LGU-identified “indigents” that are not included in the NHTS-
PR list, and the contribution from the NG for this group would be reduced to zero. Even

23
though this change has not been incorporated into the law, the NG is committed in the
long term to identifying more sustainable ways to finance the premiums for NHTS-
identified poor households, e.g. through the DOH’s increased budget and the introduction
of “sin” taxes.19 For example, the DOH budget rose by 44% from 2011 to 2012 to cover
the enhanced premium of PhP2400 (US$54) for all poor households identified by NHTS-
PR. The 2013 budget includes PhP13.8 billion (approximately US$305 million) to cover
the remaining 5.6 million households identified under the NHTS-PR, many of which are
in quintile 2 (the near-poor).
5. Assessment of Bank and Borrower Performance
5.1 Bank Performance
(a) Bank Performance in Ensuring Quality at Entry
Rating: Moderately Unsatisfactory
80. Although the project took four years to prepare, the project design was adapted by
the team to align with the thinking of the GOP and the Bank about sector direction and
instruments. The previous design – which was developed from 2002 to 2004 – was no
longer relevant for the project. In this regard, the Bank’s team showed prudence in
revising the design to align with emerging country and Bank priorities. The Bank’s team
should also be given credit for designing a highly relevant project to leverage a number
of important health sector reforms, including increased financial protection for the poor
from catastrophic health care costs, performance-based resource allocation for public
health commodities and grants as well as local health system reform through the
provision of grants based on service level agreements and LGU scorecards. The project
helped push the frontier in terms of Bank projects and is a precursor to the program-for-
results (P4R) operation.
81. However, there were gaps in project preparation and design, namely in fully
underpinning the operation on a realistic assessment of DOH’s and PhilHealth’s capacity
to implement the new budget support approach as well as associated reforms. Although
the project was designed to operate within the framework of the DOH, which used a
programmatic approach, and within this to finance selected priority national elements that
were ready for implementation, the project design lacked flexibility. This made the
project a relatively inflexible sector budget support operation, as it did not allow for
financing to move frequently and flexibly, without restructuring. Hence, the project
design appears to have been more traditional than “programmatic”.
82. Furthermore, the results and M&E framework was weak and not comprehensive,
leaving some components without indicators. Unfortunately, all the components without
indicators underperformed. A number of indicators in the PAD also had no target values,
and this was not corrected or revised at a later stage, rendering these indicators useless.
19 “Sin tax” is a state-sponsored tax that is added to products or services that are seen as vices, such as alcohol, tobacco
and gambling. This type of taxes is levied by governments to discourage individuals from partaking in such activities
without making the use of the products illegal. These taxes also provide a source of government revenue.
24
In addition, a key element of the design was not conducive to success, e.g. the project
design provided no incentives for the LGUs to identify the poor using the acceptable
method.
83. Additionally, the Bank team may not have had sufficient information to carefully
assess local politics and governance, which led the project to put too much emphasis on
CBMS, conducted at the LGU level. The project attempted this method in the first few
years. However, due to local political and governance issues and vested interests, very
few of the LGUs adopted this method to identify the poor and enroll them in the Indigent
Program. Had the project not switched to the NHTS-PR in the later years of the project,
the number of indigents enrolled in PhilHealth’s Indigent Program by the end of the
project would have been much smaller.
84. The Bank team also underestimated implementation capacity, and pushed forward
the reform to introduce performance-based allocation of public health commodities.
While the concept was good in theory, linking performance with the allocation of public
health commodities was quite unrealistic in the context of the Philippines. When the
DOH officials met the ICR team, the DOH staff objected to this approach, as they said it
would punish the poor, not poorly-performing LGUs. Furthermore, the Bank’s design
team underestimated the supervision capacity of the Bank team, particularly that the
Bank needs a multi-sectoral team to supervise this large and complicated project
effectively. Based on the above-mentioned analysis, Bank performance during project
preparation was judged as moderately unsatisfactory.
(b) Quality of Supervision
Rating: Moderately Unsatisfactory
85. The Bank’s team should be credited with closely following-up on the
implementation of the SLAs and the LGU scorecards, and for making sure that they were
on track. The team was also prudent in adjusting the health financing component of the
project design, in accordance with changing conditions, i.e. moving away from using
CBMS that relied on the LGUs to instead promoting use of the NHTS-PR, with the
national government fully financing the premiums of indigent households identified by
the NHTS-PR. This occurred after it became clear that few of the LGUs were interested
in adopting the CBMS to identify the poor in their localities, and that the LGUs would
not adopt the NHTS-PR either. Use of the NHTS-PR has contributed to the enrollment of
over five million indigent households into PhilHealth’s Indigent Program, which is three
times more than the project’s original target. The Bank’s fiduciary team also provided
timely advice and other forms of support to enhance the project’s procurement and
financial management activities.
86. Nevertheless, there were shortcomings in the quality of supervision by the Bank’s
team. The team was under constant pressure to achieve quicker disbursement, which
distracted the team’s focus from results and making sure that proper M&E was carried
out. There were inadequate efforts as well to identify methods for measuring the progress
of certain objectives and targets, and certain project indicators were not properly tracked.
Moreover, in accordance with the SDAH, the DOH’s JAPI process made it difficult for
25
the Bank to organize its own twice-yearly supervision missions, as is standard in most
countries. The SDAH process was still evolving and the DOH was also just beginning to
use the JAPI. When the Bank saw that JAPI did not work well for tracking project’s
progress, the Bank could have undertaken its own follow-up missions; however, this did
not occur. As a result, supervision of the project was judged sub-par. Moreover, given
that the policy environment was quite dynamic and there were lessons learned early in
project implementation, the supervision team should have conducted a mid-term review.
An MTR would have provided an opportunity to revise the results framework and
indicators as well as better align to existing conditions on the ground. At project closure,
this would have given a more balanced view of the project, including better development
outcomes. For example, although the indicator on the LGUs adopting the CBMS for
targeting the poorest households was not relevant by the middle period of the project, this
was never formally acknowledged in a restructured project document. Eventually there
was no proper MTR, and a number of important mid-term evaluation of indicators
specified in the PAD did not take place.
87. Furthermore, the team did not appropriately follow up on issues required by the
Loan Agreement. For example, the DOH, per the Loan Agreement, was required to
submit an annual report with analysis on project progress and how to address
shortcomings. But the DOH did not submit such reports to the Bank, and the Bank team
did not follow up to get them. This, in turn, partly contributed to DOH’s weakness on
M&E of the project. It also appeared that the team did not follow up sufficiently with the
DOH for other key activities specified in the PAD, e.g. performance-based resource
allocation for public health, or conducting baseline surveys, and follow-up surveys to
monitor progress during implementation.
88. In February 2006, the QER process highlighted that the DOH appeared to have
little capacity to implement reforms, and that it was critical that more high-level
stakeholders, such as the DBM, DOF and NEDA be explicitly involved in the reform
process. Moreover, the DBM’s active role in the project was clearly identified in the PAD.
However, it appeared that the team did not make sufficient effort to engage these more
high-level stakeholders in unsuccessful project reform activities, e.g. performance-based
allocation of public health commodities and the BFAD/FDA reforms. Based on this
analysis, Bank performance during project supervision was moderately unsatisfactory.
(c) Justification of Rating for Overall Bank Performance
Rating: Moderately Unsatisfactory
89. On the basis of moderately unsatisfactory performance during preparation and
supervision, overall Bank performance was rated as moderately unsatisfactory.
5.2 Borrower Performance
(a) Government Performance Rating: Moderately Satisfactory
90. The NG should be credited with having a strong commitment to achieving, by the
end of the project, the PDO of increasing financial protection for over five million

26
indigent households from catastrophic health care costs, by paying for their health
insurance premiums. The NG also contributed to the achievement of performance-linked
local health system reform grants, with the development and use of the SLAs and LGU
scorecards in 16 convergence provinces and later successfully rolling these out nationally.
91. The adoption of the NHTS-PR as a mechanism to identify the poor was a
remarkable government policy achievement. This not only led to the enrollment, during
the project, of an additional 4.3 million poor households, that had never had access to
health insurance before, but it also paved the way for the identification of the near-poor
(quintile 2), and for their enrollment into PhilHealth’s Indigent Program in the near future.
The government should be commended as well for institutionalizing this mechanism of
proxy means test through the President of the Philippines signing Executive Order 867.
This order directed all NG agencies to adopt the NHTS-PR as a mechanism to identify
poor households. It would be beneficial for the Philippines if the NG is able to continue
promoting this method of identification of the poor among LGUs.
92. While taking note of these achievements, the NG could have done more to
address the shortcomings in data tracking and M&E process, which affected the
availability and accuracy of data. These data were needed for the project, particularly in
the context of a decentralized health system. This system-wide weakness goes beyond the
DOH, and hence it is appropriate for the NG to take the lead in strengthening the
country’s data tracking and M&E mechanisms. As a notable example, the NG could have
done more to address the results of the logistics reviews of 2005 and 2008 that
highlighted the grave situation with regard to date-expiry, stock-outs and losses of public
health commodity commodities. Very importantly, a significant volume of drugs and
vaccines were expiring without being used. These losses were common at the level below
the CHDs and local governments. With appropriate NG intervention, “significant,
quantified reductions in date-expiry, stock-outs and losses of public health commodity
stocks at defined levels in [the] supply chain” could be achieved in future. In addition, it
would be very beneficial for the NG to build and strengthen the DOH’s stewardship of
the Philippines’ health sector to improve links between the central and local governments
and between the public and private sectors.
93. Despite shortcomings on M&E and data tracking, the NG should be credited with
a number of achievements. As a result, the government’s performance was rated as
moderately satisfactory.
(b) Implementing Agency or Agencies Performance Rating: Moderately Unsatisfactory
94. The main implementing agency was the Department of Health. The DOH should
be credited with spearheading a number of successful reforms, including the
strengthening of performance-linked local health systems reform grants. This was made
possible through the development and use of the flagship products – the SLAs and the
LGU scorecards – that were first used in the 16 convergence provinces. Thanks to the
27
DOH’s initiative, the SLAs and the LGU scorecards have been rolled out and used
nationwide, and now form the backbone of central-local relations of the health system.
95. Despite facing initial resistance from local politicians, the DOH’s decision to use
negotiated procurement with UNICEF for the purchase of vaccines has generated a
number of benefits for the health system. The quality of vaccines and the timeliness of
deliveries have been ensured. Moreover, through technical assistance from UNICEF,
DOH had the opportunity to strengthen its capacity in forecasting and budgeting for
vaccines as well as improving cold chain management.
96. In addition, since the early years of the project, the DOH successfully met the
targets for two performance indicators: (1) increasing the proportion of the DOH budget
allocated on the basis of need and performance; and (2) increasing the number of
development projects using the HSEF to plan and program their health sector support,
and thus ensuring a sector development approach for health.
97. Nevertheless, there were significant shortcomings during project implementation,
which have affected project outcomes. First and foremost, monitoring and evaluation
activities by the DOH were consistently weak. Per the Loan Agreement, annual reports
should have been prepared and submitted to the Bank by March 31 in each calendar year,
beginning March 31, 2007. 20 The report was supposed to provide the results of
monitoring and evaluation activities for the previous 12-month period and set out
measures to address shortcomings and ensure efficient implementation of the project.
However, no such reports were provided to the Bank. It would be valuable for the
implementing agency and the Bank’s team to discuss how to develop an innovative
means of tracking and reporting progress and achievements of project indicators for the
lowest transaction cost on the government’s side.
98. The DOH could have paid more attention to the results framework in the PAD
and the Loan Agreement, and exerted more efforts to fulfill the key reforms in the
project: (1) to generate evidence of a statistically significant improvement or validate by
an alternative method of improvement, in prevention, diagnosis or treatment rates in
participating LGUs for diseases or conditions subject to performance agreements and
grants, and (2) to ensure that there is significant quantified reductions in date-expiry,
stock-outs and losses of public health commodity stocks at defined levels in supply chain.
99. It also appeared that the DOH overestimated the implementing capacity of
agencies that were in charge of certain project components, including performance-based
allocation for public health commodities, regulation of pharmaceuticals and developing
human resources in health. Judging from the results of these components, the DOH
should have provided more intensive supervision and coordination to ensure effective
implementation of these components.
20 In addition, according to the Loan Agreement, the DOH needed to submit by June 30, 2008, a mid-term report with
the results of monitoring and evaluation activities, the progress achieved, as well as measures to ensure the efficient
implementation of the project and the achievement of the objectives. No such report was submitted.
28
100. Although the DOH should be credited with a number of achievements, there were
significant shortcomings. On this basis, DOH’s performance was rated as moderately
unsatisfactory.
(c) Justification of Rating for Overall Borrower Performance Rating: Moderately Unsatisfactory
101. On the basis of an overall moderately satisfactory rating for the performance of
the government and a moderately unsatisfactory rating for the performance of
implementing agencies, overall borrower performance was rated as moderately
unsatisfactory.
6. Lessons Learned
102. Implications for “National Program Support” and the need to move closer to
country systems: the NSSHRP utilized the “budget support” model to finance priority line
items/programs in the DOH budget. This yielded both advantages and constraints.
Regarding the advantages, budget support assured the availability of cash for priority
expenditures as well as providing the DBM with more authority and an entry point for
improving national fiduciary systems. Moreover, it provided an opportunity for the DOH,
in partnership with the Bank, for strong implementation of the identified programs. If
initiatives were carefully selected, as was the case in this project, benefits for the
country’s health system would be considerable. However, in the absence of complete
alignment with country systems, including fiduciary and M&E systems, such budget
support operations could be burdensome for the client. This was one of the major reasons
why Component C never disbursed. In addition, there was no operational M&E
framework for F1 when the project was designed. Perhaps this was the reason why there
was no link between the project’s indicators and the DOH’s own M&E framework and
also perhaps why the DOH did not take ownership of the M&E framework and track it. A
Bank project’s M&E framework, unless aligned to the country’s own, can increase
transaction costs for the client and is somewhat against the principles of the NSS and
SDAH.
103. Design of “programmatic” operations should be flexible: Even though the project
was designed to operate within the framework of the DOH, which used a programmatic
approach and SDAH, and within these financed a selection of priority national elements
which were ready for implementation, it should be noted that the project design lacked
flexibility, which made it a relatively inflexible sector budget support operation. The
project design was not flexible enough to allow for financing to move frequently and
flexibly. With the exception of an unallocated US$20 million, specific amounts of
financing were allocated for each project component, and restructuring of the project was
necessary when resources needed to be reallocated. Hence, the way that the project was
implemented appeared to lean more toward a traditional operation than a “programmatic”
sector-support operation. The design of the project should have been adjusted to make it
easier to reallocate resources across any component that supported F1. For instance, a
29
single disbursement category, without dividing it by components, could have been used.
This would have helped move funds more easily from an inactive component to a faster-
moving one.
104. Strengthening results and policy focus of National Sector Support: Budget
support operations provide a unique opportunity to link policy dialogue with enhanced
lending. However, in the case of Development Policy Lending (DPL) and results-based
operations, disbursements are linked to the achievement of specific targets. This approach
is not entirely problem-free but provides a framework for the NG and Bank teams to stay
focused on results. In this project, there were some strong policy components such as
Component A where disbursement was linked to a policy result. While this component
took a long time to disburse, it was also one of the most successful components of the
projects. In the other components, policy changes were implicit and required tracking the
indicators, but disbursements were not linked to results. This demonstrates the benefits of
a results-based approach. However, it would have been advisable to link to a range of
policy and program results rather than to a single indicator, thereby managing risks better
throughout the project cycle.
105. Strengthening the focus on M&E: The project suffered from weaknesses in M&E
at all stages – design, implementation, and utilization. Efforts to identify methods for how
to track the progress of certain objectives and targets were inadequate. For example,
during project design, methods for tracking the utilization of health services by the poor
were not identified. Unfortunately during implementation, tracking this important project
development objective was not addressed. The project’s results framework was not
properly tracked either during implementation. In addition, no indicators were adjusted
during project restructuring, despite the fact that some indicators were no longer
applicable. This also highlights an important lesson as both the Borrower and the Bank
could have used M&E data to identify needs to address in restructuring and, in turn, used
the restructuring to bring to date the project, through changes in directions, increased
flexibility, and improved measures of implementation, including adjustment of the results
framework.
106. The need for strong and dynamic approach to implementation support. While
Bank projects are implemented solely by the Borrower, the Bank team can leverage good
results through high-quality, strong, and dynamic technical support provided to the
Borrower. This Bank support during implementation provides an opportunity for a joint,
frank assessment of the policy context and how the project can contribute to the stated
development outcomes. An MTR, which provides a chance for the Bank’s core
implementation team to bring in outside expertise for a full review, also provides a
chance for adapting the project to maximize development outcomes. While the Bank
teams focused on policy dialogue during implementation and many issues were identified,
these were never formalized through regular missions, an MTR, or restructuring of the
project. As a result, at project closure, the project had to be evaluated based on original
project design, although major changes had occurred, such as the adoption of a national
targeting mechanism.

30
107. Strengthening central-local relations, particularly through promoting among
LGUs the introduction of defined method of identification of the poor: While the NG
adopted the NHTS-PR as the method to identify the poor and enrolled poor households
into PhilHealth’s Indigent Program, the LGUs still retain undefined methods of
identifying the poor, and pay for their insurance premiums out of public funds. This was
an unsatisfactory compromise between the LGUs and the NG, as two parallel systems
exist to cover two sets of populations. The premium of the poor identified by the NHTS-
PR is paid for by the national government, while the premium of the “poor” identified by
LGUs’ undefined method is paid for by the LGUs. Building on the achievements of the
SLAs and LGU scorecards, the NG should continue to work together with the LGUs to
promote the NHTS-PR. Public resources would be used even more efficiently if the
LGUs would adopt the NHTS-PR as the method of identifying the poor, and co-pay their
insurance premiums with the national government. Alternatively, a new arrangement
could make the LGUs no longer responsible for paying insurance premiums at all, and
instead assign the NG to be solely responsible for paying the insurance premiums of poor
households.
108. Effectively utilize the Bank’s international experience and “good practices”
within the sector or cross-sectorally in project implementation: The Bank has
demonstrated the value of international “good practices” by bringing a successful
experience from the social protection sector in Latin America to apply to the Philippines’
health sector. In the Philippines, implementation of the project’s health financing
component had clearly reached an impasse by the project’s mid-term – no LGUs had
identified the poor using acceptable methods of means testing and enrolled them into
PhilHealth’s Indigent Program. The breakthrough came with the Bank’s introducing the
PMT approach from Latin America, and the DSWD adopting it under the National
Household Targeting System (NHTS). This PMT method under NHTS was later
successfully used by PhilHealth to identify poor households and enroll them into its
Indigent Program.
7. Comments on Issues Raised by Borrower/Implementing Agencies/Partners
(a) Borrower/implementing agencies
(b) Cofinanciers
(c) Other partners and stakeholders
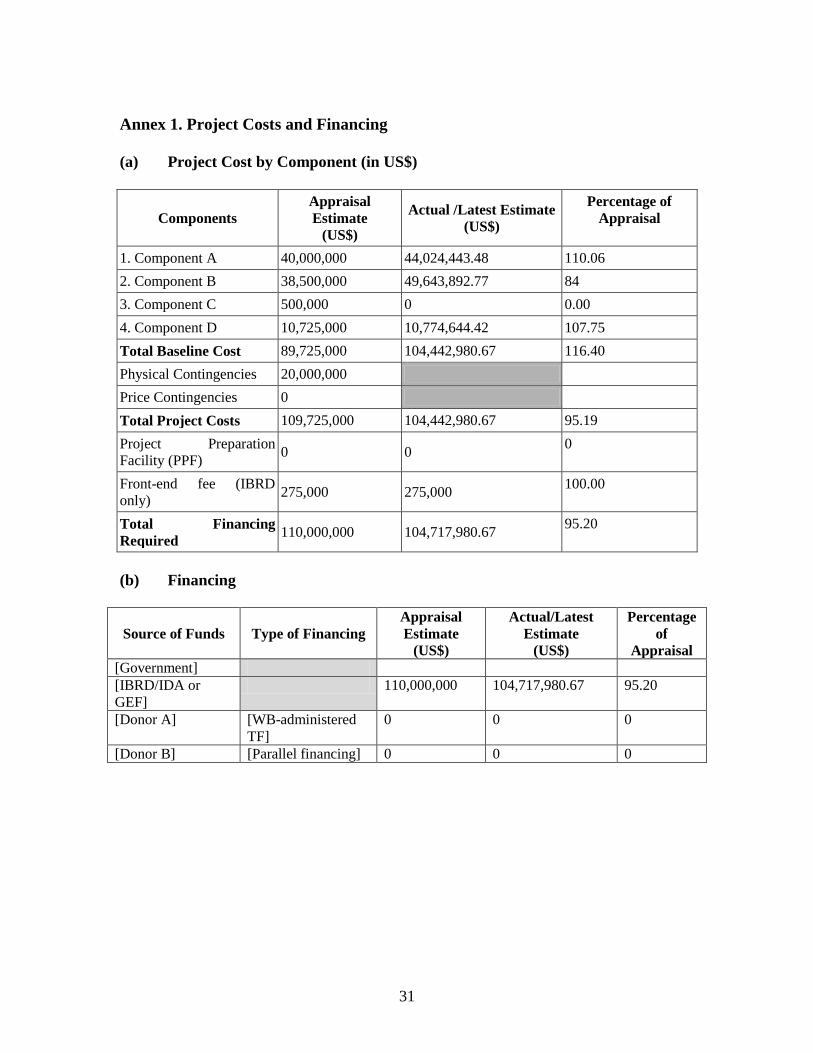
31
Annex 1. Project Costs and Financing
(a) Project Cost by Component (in US$)
Components
Appraisal
Estimate
(US$)
Actual /Latest Estimate
(US$)
Percentage of
Appraisal
1. Component A 40,000,000 44,024,443.48 110.06
2. Component B 38,500,000 49,643,892.77 84
3. Component C 500,000 0 0.00
4. Component D 10,725,000 10,774,644.42 107.75
Total Baseline Cost 89,725,000 104,442,980.67 116.40
Physical Contingencies 20,000,000
Price Contingencies 0
Total Project Costs 109,725,000 104,442,980.67 95.19
Project Preparation
Facility (PPF) 0 0
0
Front-end fee (IBRD
only) 275,000 275,000
100.00
Total Financing
Required 110,000,000 104,717,980.67
95.20
(b) Financing
Source of Funds Type of Financing
Appraisal
Estimate
(US$)
Actual/Latest
Estimate
(US$)
Percentage
of
Appraisal
[Government]
[IBRD/IDA or
GEF]
110,000,000 104,717,980.67 95.20
[Donor A] [WB-administered
TF]
0 0 0
[Donor B] [Parallel financing] 0 0 0

32
Annex 2. Outputs and Outcomes by Component
A detailed analysis of output and outcome indicators by project component is
summarized below.
Component A: Health Financing (US$44.024 million actual; US$40 million in the
Loan Agreement)
The overall rating for this component was judged as satisfactory. Initial efforts to
encourage the LGUs to identify the poor using acceptable, defined methods of means
testing, e.g. the CBMS, were plagued by deep-seated local political and governance
issues. There were only a handful of LGUs which fully implemented the CBMS as the
primary source of poverty data (e.g. Capiz, Biliran, Eastern Samar, and Agusan del Sur).
Yet, PhilHealth’s assessment of these LGUs that implemented the CBMS revealed that
none of them, except Capiz, used the CBMS as the source data for identifying indigents.
When the DSWD successfully identified the poor with the NHTS-PR, PhilHealth exerted
its efforts to convince LGU officials to enroll all PMT-identified households into the
Indigent Program. However, none of the LGUs agreed to this.
Given the constraints on the LGU part, the project turned to the NG to support the
enrollment of the poor into the NHIP Indigent Program, based on NHTS-PR. This is
clearly significant progress in policy that goes far beyond the project’s own objectives.
With the support of the NG, the project was able to identify the poor using the NHTS-PR,
which is an acceptable, defined method of means testing. Through this, in the final year
of the project, the NG quickly enrolled about 5.2 million poor households into the NHIP
Indigent Program. This was faster than using the CBMS method. Furthermore, the
original method of having the LGUs identify the poor using the CBMS was expected to
bring only 1.51 million poor households into the NHIP Indigent Program by the end of
the project. Thus, the project enrolled more than three times the target for poor
households that have their premiums paid by the Indigent Program.
Despite subsequent technical difficulties in the application of the NHTS-PR, in the long
term its adoption aligned the project with the national strategy. In 2011, the General
Appropriations Act (GAA) formally adopted the NHTS-PR as the basis for determining
who would be eligible for government subsidized enrollment into PhilHealth. Moreover,
through the adoption of the NHTS-PR, PhilHealth cross-matched the NHTS-PR’s list of
the poor with the list of enrollees identified by the LGUs, and this showed that the LGU
list of poor households was questionable. Out of 5.2 million households that were
identified as poor using the NHTS-PR, only 912,696 households were on the list of over
6 million households that the LGUs had identified as “poor”.
Some shortcomings remain. There was limited progress in the development of a partially
subsidized scheme for the near-poor. In addition, there was slow progress in PhilHealth
increasing financial protection for existing members through preferred provider
agreements that limited extra billing, and through incremental enhancement of the
benefits package. Furthermore, LGUs did not agree with NHTS-PR, and would not pay
33
the premiums for poor households identified by the NHTS-PR. As a remedial measure,
the premiums of the poor identified by the NHTS-PR were paid by the NG, backed by the
Joint Implementation Guideline adopted by the DBM, DOH and PhilHealth. A challenge
in the longer term is how to get the LGUs to support use of the NHTS-PR, who to make
the existing funding arrangements sustainable, and how to address the issue of
households enrolled into the Indigent Program by the LGUs that are not actually “poor”.
In summary, while taking note of the long delay in the implementation of this component
and the fact that the project did not achieve its original intention to get the LGUs to use
acceptable means test to identify indigents, the outcome of this component exceeded the
original targets in terms of increasing financial protection for the poor from catastrophic
health care costs.
Component B1 and B2: Health Service Delivery: Public Health (US$49.643 million
actual; US$38.5 million in the Loan Agreement)
Overall performance for B1/B2 was judged to be moderately unsatisfactory. The sub-
component B1 was intended to leverage health service delivery reforms that would help:
(i) improve accuracy in projecting the quantities of public health commodities required;
(ii) revise the criteria for allocating commodities to different LGUs and service providers
on the basis of appropriate and transparent criteria combining considerations of need,
performance, and public-private utilization patterns; (iii) implement measures to improve
warehousing, inventory management, inventory reports, and the distribution of public
health commodities to end users.
Operationally, component B (driven by sub-component B1) was the quickest-moving
project component, with a high disbursement rate. Nearly half of the loan was used for
the purchase of vaccines and other public health commodities, largely through UNICEF.
However, the outcomes of the component appear to be poor. Targets for five Loan
Agreement indicators used for tracking the progress of this component were not met. The
first three indicators were similar to the indicators used to track the PDO – FIC rate, TB
case detection rate, and TB cure rate. The latest FIC and TB cure rates improved slightly
from the baseline, but fell short of the target, while the latest TB case detection rate was
the same as the baseline. (Please refer to the relevant table in the section on the
achievement of PDOs on page 15).
The fourth indicator was “evidence of a statistically significant improvement, or
validation by an alternative method of improvement, in prevention, diagnosis or
treatment rates in participating LGUs for diseases or conditions subject to performance
agreements and grants (from 0 LGU to 15 LGUs)”. The target for this indicator was not
met, as no method was finalized and no validation took place. According to DOH
management, it was difficult to come up with an evidence of a statistically significant
improvement, and that it was not been able to find a third party, as planned, who could
provide an alternative method of validation. Nevertheless, the DOH has been able to
conduct a small-scale self-assessment by using data from the LGU scorecards.

34
The fifth indicator was “significant quantified reductions in date-expiry, stock-outs and
losses of public health commodity stocks at defined levels in supply chain”. The target
for this indicator (i.e. quarterly reporting on inventory and method of forecasting
quantities required of public health commodities, satisfactory to the Bank, as well as data
on the stock levels/losses/targets agreed for each year) is also not met. The DOH and
Bank teams explained that no data were available. Potentially, the DOH could track data
down to the DOH’s Center for Health Development (CHD) at the regional level; however,
it was difficult to get data from the LGUs, as this was not part of the LGU reporting
mechanism. This highlights the governance challenge of the central-local relations in the
health system that occurred, despite the use of the SLAs.
Despite the government’s weakness in tracking date-expiry, stock-outs and losses of
public health commodity stocks, the Bank supported a logistics review in 2008, as a
follow-up to the 2005 logistics review. The first review revealed that among key players
there was not a functional coordination system for procurement and logistics. The 2005
review also showed non-compliance with the normal quarterly delivery cycle of vaccines,
and the breakdown in distribution, inventory, and reporting at the LGU level, and in some
CHDs.
Findings of the 2008 review revealed that there were still a number of weaknesses,
including the expiry of a significant volume of drugs and vaccines before they were used,
and a low level of immunization (65-70%), despite full funding for vaccines. The review
also found that the delivery of “near date-expiry” drugs and vaccines to health facilities
persisted. The DOH continued to only use the “push” allocation system, instead of
utilizing other triggers such as inventory and consumption reports on distributing
vaccines and public health drugs. It appeared that the DOH logistics system was unable
to report on stock levels of vaccines and drugs at the LGU level. With the exception of
Cebu province, there was no inventory management below the CHD level. In most cases,
there were no housekeeping rules for pest control or for the disposal of expired stocks. At
the LGU level, there was minimal use of inventory cards and if inventory and utilization
reports by the CHDs and the LGUs were available, the information was inconsistent or
lacking.
Although the logistics review provided useful information, it did not provide a roadmap
to address issues and track progress, and this weakened the effectiveness of the DOH
M&E system. No logistics review took place in the final year of the project to track
progress before project completion. Based on the 2008 findings, it appears that failure to
achieve the target of FIC rate, TB cure rate, and TB case detection rate, could be
attributed, in part, to drug/vaccine expiry, stock-outs and unnecessary losses of public
health commodities.
Another important activity that the project component failed to implement was the reform
to allocate commodities to different LGUs on the basis of appropriate and transparent
criteria that combined considerations of performance and need. This problem occurred,
despite the fact that the project should have allocated at least US$ 5 million on the basis
of performance. The DOH’s explanation for not pursuing this reform was that this

35
method was not appropriate, because it would have negatively affected the residents of
poor-performing LGUs, rather than the LGU administrations. Nevertheless, this response
raised a question about why the DOH did not raise this concern at the project design and
appraisal stage.
Despite the failure to meet all results targets, the project significantly helped the
country’s immunization program. It also financed the procurement of all necessary
Hepatitis B vaccines, and the first ever procurement of Hemophilus influenza B (HiB)
and Measles, Mumps and Rubella (MMR) vaccines. In addition, the project partially
contributed to the increase in public health program financing. Prior to the project, the
share of public health program financing out of the government health spending
(excluding staff salaries) was 25%, while 65% went into hospital operations. Currently,
the public health program’s share, which is considered pro-poor, stands at 50-55%.
Moreover, procurement through UNICEF for essential vaccination and commodities
offered significant benefits to the Philippines. Not only did UNICEF procurement ensure
the quality of vaccines, UNICEF also provided technical advice to the government on
improving the capacity to forecast and budget for public health commodities as well as
improving cold chain management. Prior to contracting with UNICEF, the government
found quality problems when procuring vaccines through nationally competitive bidding.
In addition, the 2008 logistics review showed that there was improvement in the country's
cold chain facilities, which are functioning properly, at the very least, down to the level
of municipalities.
The implementation of sub-component B2 was slow, and agreement was only reached in
the final year of the project that US$1 million would be disbursed to reimburse the
government for MNCHN grants allocated in 2009 and 2010. However, the Bank team did
not discuss the benefits and outcomes of these grants in the ISR reports.
This rating reflects the project’s inability to meet specified targets for all five indicators,
despite quick disbursement and the sheer resources that went into the purchase of
vaccines and other public health commodities. Nevertheless, the level of dissatisfaction
was judged to be moderate, taking into account the project’s positive contribution to the
expansion of the country’s immunization program, increases in public health program
resources, improvement in cold chain management and assurance of vaccine quality.
Component C: Regulation of Pharmaceuticals (US$0 actual; US$0.5 million in the
Loan Agreement)
Overall performance for this component was judged to be unsatisfactory, reflecting
chronic and systemic lack of progress. Despite being one of the key pillars of F1, the
implementation of this component experienced multiple delays. Given the 2009
legislation strengthening the BFAD, which ensured full income retention for the BFAD
and strengthened its regulatory powers, the DOH could not decide what the NSSHRP
should finance in improving the regulatory capacity of the BFAD (renamed the FDA by
RA 9711). There was a suggestion that the loan should be used to support the full

36
implementation of the delayed BFAD Integrated Information System by 2010, but the
“budget support” nature of the loan (that this is not new money for the FDA) did not
appeal to FDA, and led to further delays.
In 2010, the DOH formally requested a reduction in the allocation to only US$60,000 in
order to fund studies that would analyze the impact of BFAD reform. Later, the DOH
indicated that it planned to use project funds to reimburse the quality assurance
accreditation activities of the FDA, but the FDA was only able to start processing its
request for DOH reimbursement in June 2012, after the project’s closing date. By then
the money had been reallocated elsewhere, so financing this activity from project funds
was not possible.
This component encountered severe shortcomings. First, there was no indicator for this
component in the Loan Agreement, which made M&E difficult. Second, the BFAD/FDA
did not appear to be enthusiastic about implementing activities using the loan. This is
partly due to the fact that the loan was for budget support and did not provide a new
source of money for the BFAD/FDA. On the other hand, use of the Bank’s loan was
viewed as adding burdens to BFAD/FDA staff, as there are specified criteria and
procedures that BFAD/FDA staff needed to learn and follow. Third, the BFAD/FDA
suffered from chronic shortage of competent managers, which severely delayed the key
reform agenda of the BFAD/FDA. Finally, there was lack of coordination and
communication between the FDA and the BIHC regarding the project’s closing date, and
this made it impossible for the FDA to finance quality assurance activities with the loan
money.
Component D1: Health Human Resources (US$0 actual; US$0.5 million in the Loan
Agreement)
Overall performance for this component was judged to be unsatisfactory, reflecting
chronic lack of progress. This component was expected to support the development of
selected strategic national initiatives in the DOH’s HRH master plan to address health
sector personnel issues, especially the deployment of health professionals to rural areas. It
was agreed that the project would support HRH information system development, but the
project faced substantial delays in procurement for this. In 2010, while the HRH
information system product was being procured, there was discussion about using project
finance to deploy health personnel to poor and remote LGUs. However, in the end no
decision was made about this. In addition, procurement of the HRH information system
product took too long, and could not be financed by the loan.
Operationally, this component encountered severe shortcomings. First, there was no
indicator for this component in the Loan Agreement, which made M&E difficult. Second,
DOH’s HRH unit management did not appear enthusiastic to implement activities using
the loan. This is partly due to the fact that the loan was for budget support and did not
provide a new source of money for the HRH unit. On the other hand, the use of the
Bank’s loan was viewed as adding burdens to HRH unit staff, as there were specified
criteria and procedures that the HRH unit needed to learn and follow. Also, there was a

37
lack of coordination between the BIHC and the HRH unit in facilitating the HRH unit’s
use of the loan money.
Although the project’s HRH component did not progress, it should be noted that there
were positive developments in HRH activities financed through DOH’s own resources.
This included the implementation of programs to deploy health professionals to rural and
under-served areas, particularly Doctors to the Barrios (medical doctors), RNHeals
(nurses) and midwives deployment programs.
Component D2: Sector Management and Coordination of Local Health Systems
Reform (US$10.774 million actual; US$10.225 million in the Loan Agreement)
Overall performance for this component was judged to be satisfactory, reflecting rapid
progress in implementing the SLA and LGU scorecards, as well as the utilization of
M&E data from the LGU scorecards that was linked with variable tranches from the
DOH to the LGUs. Since the SLA for all 16 F1 provinces was finalized in July 2007,
over the years it has been used, revised, and improved. This achievement went beyond
the target of the LGU scorecards being implemented in 16 provinces, as the LGU
scorecards were rolled out nationwide.
It should be noted that most of the LGUs initially thought of the SLA as a document that
must be signed prior to the release of their fixed tranche funds. The intended purpose of
SLA became clearer when scores based on the achievement of SLA performance targets
were released together with their corresponding variable tranche funds. In 2008, the
DOH allowed the LGUs to select some of the SLA indicators. Several Provincial Health
Offices (PHOs) admitted that they selected indicators that they thought would be the
easiest to carry out in order to increase their chances of getting a bigger percentage of the
variable tranches. Starting 2009, indicators, now based on LGU scorecard, became
uniform in all provinces. There is, of course, room for improvement in future, as the data
is self-reported by the LGUs, and the DOH should put in place a system for the validation
of these reports.
Component D3: Strengthening DOH internal management systems (financed by EC
TF)
This component supported the strengthening of DOH’s public financial management
systems, integrated management information systems, and trained DOH staff in financial
management, procurement, and internal audit. Overall implementation for this component
was judged to be satisfactory. This reflected continued full compliance with the Bank’s
procurement procedures and standards, which were monitored using agency procurement
benchmark indicators. Also, over 80% of internal audit (IA) staff were trained to
international IA standards, and the annual IA plan of scheduled audits was implemented.
The DOH was also able to roll out the Electronic National Government Accounting
System (eNGAS). By the end of the project, the eNGAS was fully used in 5 CHDs, while
7 CHDs were in a transition phase, and the eNGAS was being rolled out in another 4
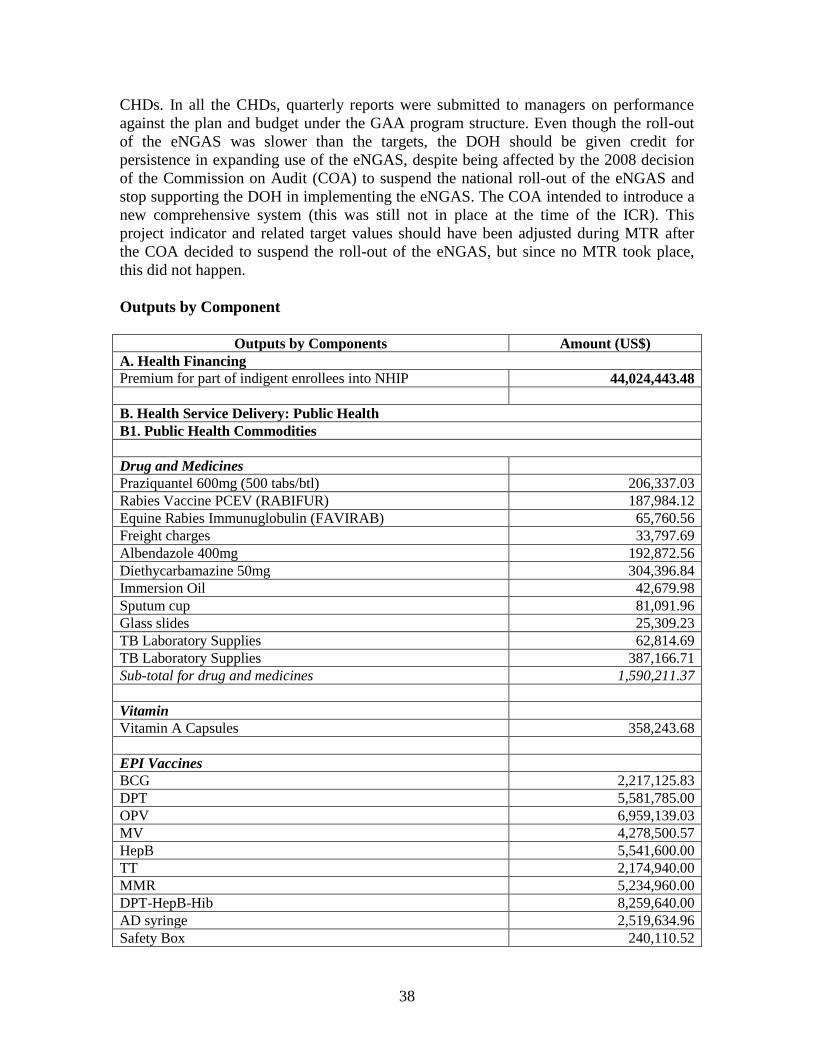
38
CHDs. In all the CHDs, quarterly reports were submitted to managers on performance
against the plan and budget under the GAA program structure. Even though the roll-out
of the eNGAS was slower than the targets, the DOH should be given credit for
persistence in expanding use of the eNGAS, despite being affected by the 2008 decision
of the Commission on Audit (COA) to suspend the national roll-out of the eNGAS and
stop supporting the DOH in implementing the eNGAS. The COA intended to introduce a
new comprehensive system (this was still not in place at the time of the ICR). This
project indicator and related target values should have been adjusted during MTR after
the COA decided to suspend the roll-out of the eNGAS, but since no MTR took place,
this did not happen.
Outputs by Component
Outputs by Components Amount (US$)
A. Health Financing
Premium for part of indigent enrollees into NHIP 44,024,443.48
B. Health Service Delivery: Public Health
B1. Public Health Commodities
Drug and Medicines
Praziquantel 600mg (500 tabs/btl) 206,337.03
Rabies Vaccine PCEV (RABIFUR) 187,984.12
Equine Rabies Immunuglobulin (FAVIRAB) 65,760.56
Freight charges 33,797.69
Albendazole 400mg 192,872.56
Diethycarbamazine 50mg 304,396.84
Immersion Oil 42,679.98
Sputum cup 81,091.96
Glass slides 25,309.23
TB Laboratory Supplies 62,814.69
TB Laboratory Supplies 387,166.71
Sub-total for drug and medicines 1,590,211.37
Vitamin
Vitamin A Capsules 358,243.68
EPI Vaccines
BCG 2,217,125.83
DPT 5,581,785.00
OPV 6,959,139.03
MV 4,278,500.57
HepB 5,541,600.00
TT 2,174,940.00
MMR 5,234,960.00
DPT-HepB-Hib 8,259,640.00
AD syringe 2,519,634.96
Safety Box 240,110.52

39
Freight charges 3,708,420.07
Sub-total for EPI vaccines 46,715,855.98
Grand Total for B1 48,664,311.03
B2. Performance-based Public Health Award
Performance-based grants using the CY 2009 MNCHN grant
allocation released to Abra, Apayao, Benguet, Ifugao, Kalinga,
Mt. Province, Baguio city
979,635.74
C. Regulation of Pharmaceuticals 0
D. Health System Governance
D1. Human Resources in Health 0
D2. Sector Management and Coordination
Local Health System Grants to 16 F1 convergence provinces
from CY 2007 to CY 2010 as national government counterpart
funds from the EC grant managed by the World Bank
10,774,644.42
40
Annex 3. Economic and Financial Analysis (including assumptions in the analysis)
The PAD did not provide an economic and financial analysis of the project, but instead
undertook a budget execution review. No net present value, economic and financial rate
of return, or cost-effectiveness was calculated a priori for the project.
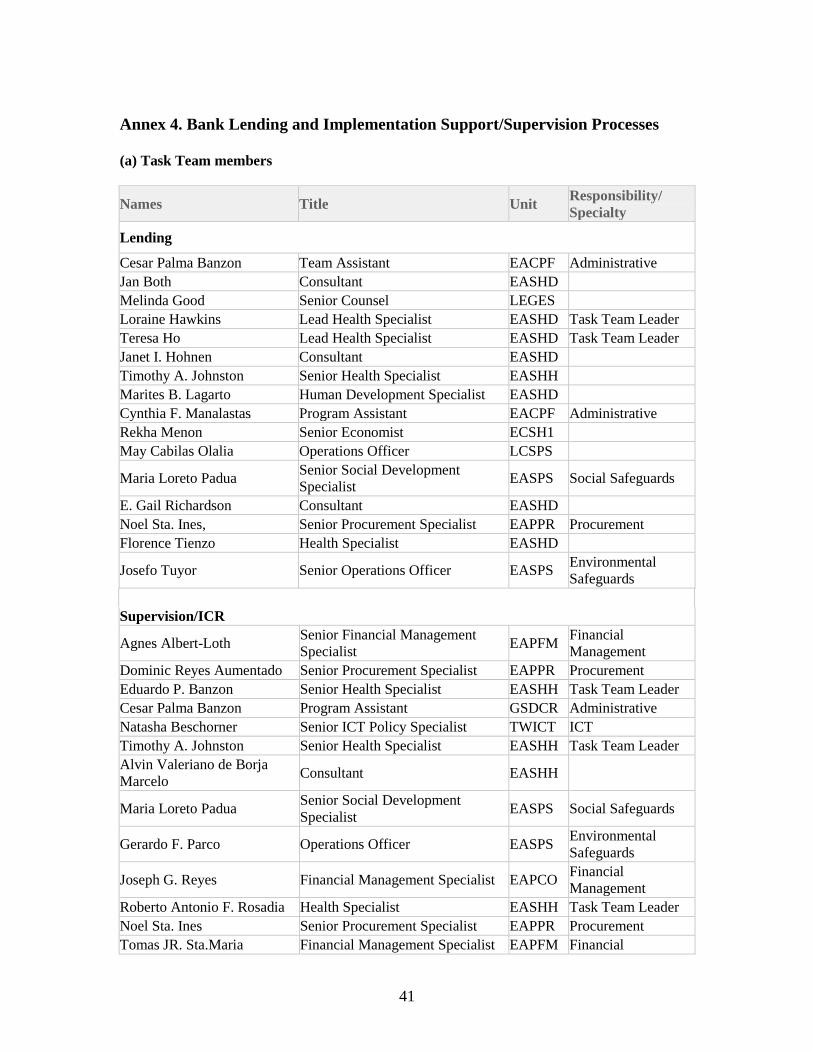
41
Annex 4. Bank Lending and Implementation Support/Supervision Processes
(a) Task Team members
Names Title Unit Responsibility/
Specialty
Lending
Cesar Palma Banzon Team Assistant EACPF Administrative
Jan Both Consultant EASHD
Melinda Good Senior Counsel LEGES
Loraine Hawkins Lead Health Specialist EASHD Task Team Leader
Teresa Ho Lead Health Specialist EASHD Task Team Leader
Janet I. Hohnen Consultant EASHD
Timothy A. Johnston Senior Health Specialist EASHH
Marites B. Lagarto Human Development Specialist EASHD
Cynthia F. Manalastas Program Assistant EACPF Administrative
Rekha Menon Senior Economist ECSH1
May Cabilas Olalia Operations Officer LCSPS
Maria Loreto Padua Senior Social Development
Specialist EASPS Social Safeguards
E. Gail Richardson Consultant EASHD
Noel Sta. Ines, Senior Procurement Specialist EAPPR Procurement
Florence Tienzo Health Specialist EASHD
Josefo Tuyor Senior Operations Officer EASPS Environmental
Safeguards
Supervision/ICR
Agnes Albert-Loth Senior Financial Management
Specialist EAPFM
Financial
Management
Dominic Reyes Aumentado Senior Procurement Specialist EAPPR Procurement
Eduardo P. Banzon Senior Health Specialist EASHH Task Team Leader
Cesar Palma Banzon Program Assistant GSDCR Administrative
Natasha Beschorner Senior ICT Policy Specialist TWICT ICT
Timothy A. Johnston Senior Health Specialist EASHH Task Team Leader
Alvin Valeriano de Borja
Marcelo Consultant EASHH
Maria Loreto Padua Senior Social Development
Specialist EASPS Social Safeguards
Gerardo F. Parco Operations Officer EASPS Environmental
Safeguards
Joseph G. Reyes Financial Management Specialist EAPCO Financial
Management
Roberto Antonio F. Rosadia Health Specialist EASHH Task Team Leader
Noel Sta. Ines Senior Procurement Specialist EAPPR Procurement
Tomas JR. Sta.Maria Financial Management Specialist EAPFM Financial

42
Management
Dennis Streveler Consultant LCSHH
Florence Tienzo Health Specialist EASHD
John Q. Wong Consultant EASHH
Kristine May San Juan Ante Program Assistant EACPF
Sutayut Osornprasop Human Development Specialist EASHH ICR TTL and
Primary Author
(b) Staff Time and Cost
Stage of Project Cycle
Staff Time and Cost (Bank Budget Only)
No. of staff weeks US$ Thousands (including
travel and consultant costs)
Lending
FY02 10.44 62.94
FY03 16.11 57.62
FY04 17.49 108.71
FY05 27.08 103.69
FY06 46.84 176.22
FY07 3.41 9.41
FY08 - 0.00
Total: 121.37 518.59
Supervision/ICR
FY02 - 0.00
FY03 - 0.00
FY04 - 0.00
FY05 - 0.00
FY06 - 0.00
FY07 23.90 75.86
FY08 30.68 85.02
FY09 27.39 86.79
FY10 7.7 63.95
FY11 14.73 51.22
FY12 27.81 57.29
FY13 1.32 1.27 1
Total: 133.53 421.4

43
Annex 5. Beneficiary Survey Results (if any)
N/A

44
Annex 6. Stakeholder Workshop Report and Results (if any)
There was no stakeholder workshop.

45
Annex 7. Summary of the Borrower's ICR and/or Comments on the Draft ICR
The DOH reviewed the Draft ICR and provided comments related to the trends on TB
during implementation of NSSHRP project. The DOH advised that the private sector
reporting was not included in the FHSIS report, which was the source of data that the
DOH shared with the Bank’s ICR team. The National TB Program has its own data that
captures the private sector, per the table below.
Trends of Case Detection Rate (CDR), Cure Rate and Treatment Success Rate from 2005 - 2010
Indicator 2005 2006 2007 2008 2009 2010
CDR (NSP)* 70 74 75 72 74 72
CDR (NSP)** 70 74 76 78 77 78
Cure Rate (NSP) 83 82 79 77 82 83
Tx Success Rate (NSP)*** 90 90 89 85 89 90
*Est. Incidence = constant at 131/100,000
**Est. Incidence = declining per year
***Success Rate = Cure Rate + Completion Rate
Nevertheless, DOH concluded that even though the private sector data was already
included in the data above, the outcomes still did not reach the 80% target of case
detection rate and 85% target of cure rate. The National TB program also mentioned that
they also use the treatment success rate as their parameter where they monitor the TB
cases which finished the 6 months treatment.
The DOH also shared a note prepared by the Health Human Resource Development
Bureau, dated January 18, 2013. The Bureau responded to Component D1: Health
Human Resources, on page 36 under Annex 2, and clarified on the non-utilization of
funds allocated to HRH.
The Bureau expressed regrets that it was unable to access the loan as budget support to
Human Resources for Health (HRH), and explained that this was not due to “lack of
enthusiasm”. The Bureau recognizes the value of the loan in implementing priority
human resources for health (HRH) programs/activities/projects (P/A/Ps) as outlined in
the HRH Master Plan 2005-2030. However accessing the fund is a tedious process that
the Bureau, even in coordination with the Bureau of International Cooperation (BIHC),
could not bring into fruition the potential of using the loan as budget support. The Bureau
was able to implement the planned P/A/Ps by tapping other sources of fund.

46
Annex 8. Comments of Co-financiers and Other Partners/Stakeholders
N/A
47
Annex 9. List of Supporting Documents
Project documentation:
NSSHRP Aide Memoires, Back-to-Office Reports, Quality Enhancement Review
Reports, Project Implementation, Status, and Results Reports, Project Monitoring Reports,
2002-2011
NSSHRP Loan Agreement, 2006
NSSHRP Project Appraisal Document, 35405-PH, 2006
PH-EC TF for Health Sector Reform Implementation, Status, and Results Report, 2012
SEMP 2 Implementation Completion and Results Report, 2008
Reports, studies, and references:
Department of Health (DOH), Field Health Services Information System (FHSIS) Annual
Reports, National Epidemiology Center, various years
DOH, LGU Scorecards data, 2006-2011
DOH, National Health Accounts, various years
DOH, National Tuberculosis Program Manual of Procedures, 2005
DOH, National Tuberculosis Program (NTP) Report, various years
DOH, Philippine Plan of Action to Control Tuberculosis (PhilPACT), Health Sector
Reform Agenda Monograph No. 11, 2010
DOH, Registered Nurses for Health Enhancement and Local Service Brief, not dated
European Union, Philippine Health Sector Support Programme, ASIE/2005/017-638,
July 2012
National Statistical Coordination Board, National Health Account data, various years
Utilization of the Community-based Monitoring System (CBMS) as a Tool for Localizing
the Millennium Development Goals (MDGs), on-line report, not dated
The World Bank and Government Procurement Policy Board, Agency Procurement
Compliance & Performance Indicator Assessment for Selected Government Agencies,
May 2010

IliganIligan
PasigPasigQuezon Quezon
GeneralGeneralSantosSantos
LucenaLucena
ViracViracBatangasBatangas
BoacBoacMamburaoMamburao
RomblonRomblon
Santa CruzSanta Cruz
AntipoloAntipolo
BalerBalerPalayan Palayan
TarlacTarlacIbaIba
MalolosMalolosBalangaBalanga
Trece MartiresTrece Martires
Laoag CityLaoag City
ViganViganBanguedBangued
TabukTabuk
IlaganIlagan
CabarroguisCabarroguis
BontocBontocLagaweLagawe
BayombongBayombongLa TrinidadLa Trinidad
LingayenLingayen
KabugaoKabugao
BascoBasco
Puerto PrincesaPuerto Princesa
PiliPili
SorsogonSorsogon
DaetDaet
MasbateMasbateCatarmanCatarman
BoronganBoronganCatbaloganCatbalogan
NavalNaval
MaasinMaasin
BacolodBacolod
DumagueteDumaguete SiquijorSiquijor
TagbilaranTagbilaran
MambajaoMambajao
SurigaoSurigao
San JoseSan Jose
TandagTandag
Tubod Tubod
ProsperidadProsperidad
TagumTagumNabunturanNabunturan
MatiMatiKidapawanKidapawan
DigosDigosIsulanIsulan
Marawi Marawi
MalaybalayMalaybalay
OroquietaOroquietaDipologDipolog
IpilIpil
IsabelaIsabelaCityCity
JoloJolo
KaliboKaliboRoxas CityRoxas City
San Jose deSan Jose deBuenavistaBuenavista
JordanJordan
AlabelAlabel
PanglimaPanglimaSugalaSugala
ZamboangaZamboanga Shariff AguakShariff Aguak(Maganoy)(Maganoy)
San FernandoSan Fernando
TuguegaraoTuguegarao
BaguioBaguioSan FernandoSan Fernando
LegaspiLegaspi
TaclobanTacloban
CebuCebu
ButuanButuan
DavaoDavaoCotabatoCotabato
CagayanCagayande Oro de Oro
IloiloIloilo
PagadianPagadian
KoronadalKoronadal
CalapanCalapan
CalambaCalamba
MANILAMANILA
MALAYSIAMALAYSIA
Iligan
PasigQuezon
GeneralSantos
Lucena
ViracBatangas
BoacMamburao
Romblon
Santa Cruz
Antipolo
BalerPalayan
TarlacIba
MalolosBalanga
Trece Martires
Laoag City
ViganBangued
Tabuk
Ilagan
Cabarroguis
BontocLagawe
BayombongLa Trinidad
Lingayen
Kabugao
Basco
Puerto Princesa
Pili
Sorsogon
Daet
MasbateCatarman
BoronganCatbalogan
Naval
Maasin
Bacolod
Dumaguete Siquijor
Tagbilaran
Mambajao
Surigao
San Jose
Tandag
Tubod
Prosperidad
TagumNabunturan
MatiKidapawan
DigosIsulan
Marawi
Malaybalay
OroquietaDipolog
Ipil
IsabelaCity
Jolo
KaliboRoxas City
San Jose deBuenavista
Jordan
Alabel
PanglimaSugala
Zamboanga Shariff Aguak(Maganoy)
San Fernando
Tuguegarao
BaguioSan Fernando
Legaspi
Tacloban
Cebu
Butuan
DavaoCotabato
Cagayande Oro
Iloilo
Pagadian
Koronadal
Calapan
Calamba
MANILA
1
2
4
6
7
11
14
17
18
19
20
2122
16
23
2425
27
31
39
42 46
47
49
54
75
59
62
65
66
71
73
74
76
80
79
77
78
63
3
5 9
10
8
12
13
15
28
29
30
26
32
33
34
35 36
37
38
40
41
43
44 45
48
50
51
52
53
55
56
58
61
64
68
69
70
60
67
72
57
ZAMBOANGA CITY
ICAR II
III
IV-A
V
IV-B VI VII
VIII
IX X
XIII
XI
XII
ARMM
NCR
MALAYSIA
Celebes Sea
Moro
Sulu Sea
Leyte Gulf
Visayan
Sea
Mindoro Strait
SibuyanSea
Phi l ippine
Sea
Babuyan Channel
Luzon Strai t
Gulf
DavaoGulf
MindanaoSea
BatanIslands
BabuyanIslands
PolilloIslands
LubangIslands
Catanduanes
TicaoSibuyanTablas
Busuanga
SemiraraIslands
CuyoIslands
Culion
Linapacah
Dumaran
Bugsuk
Balabac
Cagayan Sulu
Tawi-Tawi
Sulu
Basilan
Mindanao
CamiguinSiquijor
Negros
Panay
Bohol
Cebu Leyte
SamarMasbate
Marinduque
BuriasMindoro
Palawan
Luzon
Dinagat
Siargao
Sarangani
20ºN
10ºN
5ºN125ºE
120ºE
125ºE
IlocosIlocos NorteIlocos SurLa UnionPangasinan
Cordillera Admin. Reg.AbraApayaoBenguetIfugaoKalingaMountain Province
Cagayan ValleyBatanesCagayanIsabelaNueva VizcayaQuirino
Central LuzonAuroraBataanBulacanNueva EcijaPampangaTarlacZambales
National Capital Reg.
CALABARZONBatangasCaviteLagunaQuezonRizal
MIMAROPAMarinduqueMindoro OccidentalMindoro OrientalPalawan*Romblon
BicolAlbayCamarines NorteCamarines SurCatanduanesMasbateSorsogon
Western VisayasAklanAntiqueCapizGuimarasIloiloNegros Occidental
Central VisayasBoholCebuNegros OrientalSiquijor
Eastern VisayasBiliranEastern SamarLeyteNorthern SamarSamarSouthern Leyte
Zamboanga PeninsulaZamboanga del NorteZamboanga del SurZamboanga SibugayZamboanga City
I1234
CAR56789
10
II1112131415
III16171819202122
NCR
IV-A2324252627
IV-B2829303132
V333435363738
VI394041424344
VII45464748
VIII495051525354
IX555657---
Northern MindanaoBukidnonCamiguinLanao del NorteMisamis OccidentalMisamis Oriental
Davao Reg.Compostela ValleyDavao del NorteDavao del SurDavao Oriental
SOCCSKSARGENNorth CotabatoSaranganiSouth CotabatoSultan Kudarat
CaragaAgusan del NorteAgusan del SurDinagat IslandsSurigao del NorteSurigao del Sur
Autonomous Reg. inMuslim MindanaoBasilanLanao del SurMaguindanao**SuluTawi-Tawi
X5859606162
XI63646566
XII67686970
XIII7172737475
ARMM
7677787980
**Shariff Aguak (Maganoy) andSultan Kudarat serve as co-capitalsof the province.
*Executive Order 429, May 23, 2005,provides for the transfer of Palawanprovince (#31) from Region IV toRegion VI; Administrative Order 129holds EO429 in abeyance until animplementation plan is approvedby the President.
PHILIPPINES
0 50 100
0 50 100 Miles
150 Kilometers
IBRD 33466R4
NOVEMBER 2012
PHIL IPPINESSELECTED CITIES
PROVINCE CAPITALS
REGION CAPITALS
NATIONAL CAPITAL
RIVERS
MAIN ROADS
RAILROADS
PROVINCE BOUNDARIES
REGION BOUNDARIES
INTERNATIONAL BOUNDARIES
This map was produced by the Map Design Unit of The World Bank. The boundaries, colors, denominations and any other information shown on this map do not imply, on the part of The World Bank Group, any judgment on the legal status of any territory, o r any endo r s emen t o r a c c e p t a n c e o f s u c h boundaries.