Embed Size (px)
Citation preview

1
WHO Drug Information Vol. 28 No. 1, 2014
Contents
Regulatory harmonizationThe International Generic Drug
Regulators Pilot 3WHO support for medicines regulatory
harmonization in Africa: focus on East African Community 11
Technologies, standards and normsStandards for biological products 16
Safety and efficacy issuesCombined hormonal contraceptives and
venous thromboembolism 21Clobazam: serious skin reactions 21Amiodarone: pulmonary toxicity 21Methylphenidate: rare risk of long-lasting
erections in males 22Glibenclamide: risk of hypoglycaemia in
elderly and renal-impaired patients 22Subcutaneous epoetin alfa:
contraindicated in Singapore in chronic kidney disease patients 22
Acipimox: only to be used as additional or alternative treatment 22
Estradiol-containing creams: new restrictions 23
Clopidogrel: rare reports of acquired haemophilia 23
Sodium phosphate products in high doses: severe dehydration 23
Emergency contraceptives – high bodyweight may reduce effectiveness 24
Testosterone: possible risk of stroke and heart attack 24
Lithium: hypercalcaemia and hyperparathyroidism 24
Saxagliptin: possible risk of heart failure 25
Strontium ranelate: further restrictions due to cardiovascular risks 25
Methysergide-containing medicines: new restrictions 25
Regulatory action and newsRegulatory options in the fight against
antimicrobial resistance 26EMA and FDA collaborate on
bioequivalence inspections 26Tafenoquine receives FDA Breakthrough
Therapy designation 27Regulatory action against Ranbaxy’s
Toansa facility 27WHO response to FDA findings at
Ranbaxy’s Toansa site 27New partnership to strengthen regulatory
systems 27Canada-US Common Electronic
Submissions Gateway 28Updated guidance for annual strain
change of seasonal influenza vaccines 28EMA and FDA strengthen collaboration on
pharmacovigilance 28European Medicines Agency publishes
first summary of a risk-management plan for a medicine 29
EMA and FDA extend parallel assessment pilot 29
Australia and New Zealand harmonization activities 29 ►Approvals
First adjuvanted vaccine for H5N1 avian influenza approved 29
Umeclidinium and vilanterol approved for chronic obstructive pulmonary disease 30
Dapaglifozin approved for type 2 diabetes 30
Continued
WHO Drug Information

WHO Drug Information Vol. 28 No. 1, 2014
2
Trametinib and dabrafenib approved in combination for advanced melanoma 30
Droxidopa approved for neurogenic orthostatic hypotension 31
Bedaquiline recommended for approval to treat multidrug-resistant tuberculosis 31
Metreleptin approved to treat rare metabolic disease 31
Recent publications, information and eventsWorld malaria report: financing needed to
sustain major progress 32WHO Prequalification: A quiet revolution
in global public health 32AIDS drugs for all: how global advocacy
transformed pharmaceutical markets 33Who are the originators of innovative
medicines in the EU? 33Medicines Patent Pool and Bristol-Myers
Squibb sign agreement 33Report calls for cooperation to strengthen
post-market surveillance systems 34 ►Events
Annual ATC/DDD Methodology course 34
Consultation documents ►The International Pharmacopoeia
Atazanavir sulfate 35
Atazanavir capsules 38Implementation of the revised general
monograph on parenteral preparations in The International Pharmacopoeia: Limits for the test for bacterial endotoxins (3.4) 41
Revision of general monograph: Suppositories 45
Revision of method of analysis: 5.3 Disintegration test for tablets and capsules 50
Revision of method of analysis: 5.4 Disintegration test for suppositories and rectal capsules 54
RADIOPHARMACEUTICALS: 56Sodium iodide (131I) solution 56Technetium (99mTc) exametazime complex
injection 59Thallous (201Tl) chloride injection 63
ATC/DDD ClassificationATC/DDD Classification (Temporary) 66ATC/DDD Classification (Final) 69
International Nonproprietary NamesRecommended List No. 71 71
Continued
WHO Drug Information is available electronically at http://www.who.int/medicines/publications/druginformation/en/
International Conference of Drug Regulatory Authorities (ICDRA)
The 16th ICDRA will be hosted by the Brazilian National Health surveillance Agency (ANVISA)
Rio de Janeiro, Brazil 24 - 29 August 2014
http://www.icdra.com.br/

3
WHO Drug Information Vol. 28 No. 1, 2014
3
Regulatory harmonization
The International Generic Drug Regulators Pilot
The pre-market review of generic medicines puts mounting pressures on health regulatory authorities around the world due to increasing workloads and risks associated with complex global supply chains. This has led a group of regulators to launch the International Generic Drug Regulators Pilot (IGDRP), aimed at regulatory convergence and cooperation. The three-year pilot entails a series of concrete measures to facilitate the timely authorization and availability of safe, effective and quality generic medicines.
Results of the pilot will inform decisions on establishing a more permanent information and work-sharing arrangement as part of broader international efforts related to regulation of medicines. The success of the initiative will require the support of industry as well as other stakeholders interested in promoting access to affordable, quality generic medicines.
IntroductionThe availability of quality generic drugs, also known as multi-source medicines or pharmaceuticals, plays an increasingly important role in helping to address rising health care costs and in promoting access to essential medicines worldwide. This, however, has led to significant pressures on medicines regulatory authorities (RAs) charged with the review and approval of these products. In addition to an increased workload associated with the growing number of generic drug applications, RAs must now also contend with more sophisticated generic drug products and complex global production and distribution chains.
Given these challenges, the need for regulatory cooperation and convergence has long been recognized. “Regulatory convergence” represents a process whereby the regulatory requirements and approaches across countries and
Article by Mike Ward, Manager, International Programs, Therapeutic Products Directorate, Health Products and Food Branch, Health Canada.
regions become aligned over time as the same harmonized technical guidance documents, standards and scientific principles are adopted and similar regulatory practices and procedures are introduced. Regulatory convergence in turn makes possible additional, enhanced forms of cooperation and collaboration between regulatory authorities.
Exploratory meetingIn an effort to address the challenges associated with the increasingly demanding review of generic drug applications, regulatory authorities from Australia, Brazil, Canada, the European Union, the Republic of Korea, Singapore, Switzerland and the United States as well as the World Health Organization (WHO) met in Ottawa in October 2011 to explore opportunities for collaboration. A number of positive developments and precedents were identified that favour a collaborative drug review model, including:• a common set of quality requirements
and application format provided by ICH

WHO Drug Information Vol. 28 No. 1, 2014
4
Regulatory harmonization
Quality guidelines (1) and the Common Technical Document (CTD);
• the increasing number of multi-national generic companies, including the generic arm of innovator companies, with a potential for common products, ingredients and manufacturing sites across markets;
• the success of existing collaborative models, including the WHO’s Prequalification Programme as well as the EU’s Centralised and Decentralised Procedures (and the EU’s Mutual Recognition Procedure, wherein a marketing authorization has already been granted by an EU Member State); and
• the restricted set of scientific disciplines involved in generic drug reviews, compared with reviews of first market entry drugs (“new drugs”).
Preliminary surveys The meeting in Ottawa was preceded by surveys, commissioned by Health Canada, with a number of multi-national generic drug manufacturers and with the participating RAs. Regulatory frameworks, data exclusivity, patent rules, submission management and other pertinent issues were also compared to help inform discussions.
RAs were asked about the potential advantages and disadvantages of a collaborative review process, when and what form of collaboration might be most beneficial and achievable, and desirable short, medium and longer term outcomes.
The survey of generic drug manufacturers was designed to establish current business practices and to solicit views on whether a business case existed for establishing a collaborative review programme if certain enablers were in place.
Findings from the surveys and views expressed in the exploratory meeting confirmed strong support in principle for regulatory collaboration in the pre-market review of generic drugs, although the degree of support was conditional for some RAs on the scope and form of collaborative model chosen. In general, there was also agreement on the main advantages, challenges and enablers to international collaboration (Table 1). Although important challenges were identified, they were not felt to be insurmountable.
The path forwardRecommendations from the exploratory meeting helped to shape the path forward. Key among these was the need to be pragmatic and to adopt a step-wise approach, starting with selected areas of collaboration, a mapping of regulatory programmes and information-sharing between authorities.
It was also recognized that many of the prerequisites for collaborative generic drug review – such as secure electronic platforms for sharing of documents, and mechanisms to treat and exchange confidential business information – also apply to other areas of potential cooperation. Finding solutions to these issues, together with the building of greater knowledge and trust between regulatory authorities, will facilitate additional areas of inter-agency cooperation in the future.
Participants further recognized the importance of industry support in realizing the full benefits of regulatory collaboration. Any work-sharing arrangement would clearly require the filing of common marketing applications to a consortium of RAs.
At the exploratory meeting, participants agreed on high level goals and objectives, on the general parameters of an operating model and on areas of initial focus based

5
WHO Drug Information Vol. 28 No. 1, 2014 Regulatory harmonization
Table 1. Benefits, challenges and enablers to a collaborative generic review process
Benefits:Improved operational efficienciesPotentially faster and more consistent review and approval processGreater availability of generics that may otherwise not be registered in certain marketsRegulatory convergence, promotion of regulatory science and the strengthening of RAsGreater regulatory oversight and peer reviewReduction in overall regulatory burden and less duplication of effortLower regulatory and product development costs/timesGreater alignment of industry submission practicesFewer parallel registrationsMore affordable generic medicinesMutual learning and consistency in applying international guidelines such as ICH Q8(R2)
Challenges:Unfamiliarity with regulatory systems of other RAsDifferences in:• Legal frameworks: definitions of terms (“generic”, “reference product”, “data exclusivity”,
“pharmacopoeia”, “variations”, etc.)• Treatment guidelines/therapeutic traditions between countries, both in terms of the
medicines acceptable for market authorizations by RAs and acceptable indications• Technical requirements, e.g. bioequivalence (BE) requirements for complex products• Product and active pharmaceutical ingredients (API) differences – source, method of
manufacture, packaging, etc.• Assessment timelines, which may be anchored in regulations• Timing of applications due to differences in data exclusivity/patent rulesDivergence following joint approval due to separate handling of post-approval changesCulture changePotential reduction in number of manufacturing sites, impacting on supplyComplexity of setting up and maintaining a collaborative review system
Enablers:Regulatory gap analysisSecure electronic platform for sharing of reports/commentsConfidentiality arrangements between RAs and/or consent of applicants Common technical requirements and definitionsPractices to enable filing of common dossiers: • Identify sections of CTD where content is identical or consolidated (e.g. multiple
pharmacopoeial references)• Allow different BE studies within a single application where use of different reference
products is unavoidableStaff exchange, workshops and trainingPilot programme, guided by policies, procedures to manage the pilotLeveraging the experience of jurisdictions and models such as EU and WHO
on both perceived value and the likelihood of success. Most importantly, participants undertook a commitment to pursue discussions towards the achievement of concrete deliverables.
Meeting participants further learned of the formation of the Heads of Agency Consortium involving the RAs of Australia, Canada, Singapore and Switzerland, as well as the advanced degree of

WHO Drug Information Vol. 28 No. 1, 2014
6
Regulatory harmonization
collaboration and work-sharing efforts that are already taking place in generic drug review. These experiences could help facilitate discussions with the larger grouping of RAs.
Launch of the International Generic Drug Regulators PilotA second meeting of regulators, co-chaired by the US Food and Drug Administration (FDA) and Health Canada, took place in Washington in April 2012, marking the official launch of the International Generic Drug Regulators Pilot (IGDRP), with the addition of regulators from China, Chinese Taipei, Japan and Mexico.
Participants reached consensus on a three-year duration and on interim operating procedures for the pilot. A formal governance structure and terms of reference would be adopted on the basis of experience gained during the pilot and broader regulatory cooperation discussions concurrently taking place at the international level.
Operating proceduresInterim operating procedures defining the mission, goal, objectives and operating arrangements are outlined in Table 2. Agreement was also reached on the following working definition of a generic drug, recognizing that precise regulatory definitions across the IGDRP jurisdictions may differ:
“A generic drug is generally defined as a drug product that is equivalent to a reference product in active pharmaceutical ingredient, dosage form, strength, route of administration, quality and performance characteristics and intended use.”
At the same time, IGDRP participants confirmed that biosimilars – also known as subsequent entry biologics – would not be included within the scope of the pilot. They
acknowledged the need to make progress in the area of generic drugs before considering an expansion of activities.
Participants recognized the diversity of requirements and capacity of IGDRP regulators, as well as the importance of selecting activities that would complement and not duplicate work undertaken elsewhere. The diversity issue was addressed by acknowledging the right of participants to “opt-out” from work plan activities. “Opting-out” could occur due to constraints presented by existing regulatory systems, or decisions to delay involvement until the conclusion of the pilot.
Together with the participants’ commitment to promote regulatory convergence, these realistic key operating principles position the new consortium to make tangible short and medium term progress with a long term vision in mind: to facilitate the timely authorization and availability of safe, effective and quality generic drugs. Participants felt that IGDRP has the potential to achieve this goal by changing the international business and regulatory model for generic drugs.
Progress to dateTo date, five meetings have taken place hosted respectively by the RAs of Canada (Ottawa, October 2011), United States (Washington, April 2012), China (Nanchang, December 2012), Australia (Canberra, May 2013) and Switzerland in conjunction with WHO (Geneva, October 2013). The next meeting is scheduled for May 2014 in Chinese Taipei.
Considerable progress has been made in identifying priorities and mechanisms for promoting convergence of regulatory approaches:• Working groups and proposals have
been established related to active substance master files (ASMF)/drug

7
WHO Drug Information Vol. 28 No. 1, 2014 Regulatory harmonization
Table 2. Interim IGDRP operating procedures
Mission: To promote collaboration and convergence in the area of generic drug regulation in order to strengthen the ability of health authorities to meet their respective mandates
Goal: To facilitate the timely authorization and availability of safe, effective and quality generic drugs
Objectives:• Faster review and greater availability of generics • More efficient use of resources through mutual reliance and work-sharing • Strengthen review process and international regulatory oversight while
reducing regulatory burden• Promote adoption of modern, science and risk-based approaches• Rapid exchange of safety and quality information on marketed products• Enhance development of human resources
Scope: Activities that best meet needs of participants with a focus on the premarket review of generic drugs. Does not include biosimilars
Key Operating Principles:• Decision-making: by consensus on matters related to the operation of the pilot.
Participating regulators may however “opt-out” from any work plan activities. • Activities will complement and not duplicate work undertaken elsewhere.
Governance, Structure and Meetings:• IGDRP is composed of a Steering Committee (SC), Working Groups (WG) and
Secretariat.• SC is composed of one representative from each participating RA and an
Observer from WHO.• Observers from RAs or international organizations may be designated by SC
on perceived value to IGDRP.• External experts may be consulted or invited to participate on WGs depending
on perceived value and SC endorsement.• Chair and host rotate with each meeting, with two in-person meetings per year.• Chair becomes co-chair of the next meeting.• Location of meetings will rotate among RAs/regions and WHO (Geneva).
Transparency: Information on IGDRP will be provided using WHO information-sharing tools.
master files (DMF), biowaivers and work-sharing models (see Table 3).
• ANVISA (Brazil) has conducted a survey to identify similarities and differences in regulatory requirements and approaches. The results, together with findings from the preliminary 2011 comparative study and a comprehensive analysis of international BE guidelines authored by current and former scientists from the US
FDA (2), should provide a solid baseline for regulatory convergence activities. It is anticipated that the most recent survey results will be published as one or more articles in WHO Drug Information.
• Health Canada has launched an initial survey on laws, policies and procedures related to the management and sharing of non-public regulatory information,

WHO Drug Information Vol. 28 No. 1, 2014
8
Regulatory harmonization
including confidential business and trade secret information.
• Swissmedic has created an electronic platform for the sharing of non-confidential information and documents between IGDRP members.
• The IGDRP operating procedures have been refined to clarify interim governance and work arrangements, with measures to improve transparency and outreach (as an example, information on IGDRP will be provided using WHO information-sharing tools).
• Participants are committed to assist WHO in implementing proposed changes to the WHO Prequalification of Medicines Programme as it moves to a new operating model, and to encourage generic drug applicants in respective IGDRP jurisdictions to apply for prequalification of medicines of interest.
• WHO will serve as secretariat for the IGDRP for the remainder of the pilot (until end of 2014).
• IGDRP has been granted observer status to the ASMF Work-Sharing Working Group of the Coordination Group for Mutual Recognition and Decentralised Procedures-Human (CMDh), and conversely the latter’s Chair will participate in the IGDRP ASMF/DMF working group, thereby
allowing for the sharing of best practices and possible opportunities to leverage ASMF/DMF reviews.
• New members from New Zealand, Russia and South Africa have joined the IGDRP, with the European Directorate for the Quality of Medicines and Healthcare (EDQM) joining as an observer organization. While the IGDRP steering committee recently agreed that membership should not be greatly expanded during the pilot in order to ensure efficiency of operations, members also agreed that increased communication and transparency of operations were important. Towards this goal, read-only access to the secure electronic platform could be granted on request to other RAs not actively participating in the IGDRP.
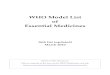
Decentralised Procedure as a model for cooperationOne of the most significant work-sharing developments relates to the possible use of the EU’s Decentralised Procedure (DCP) as a policy model for information-sharing with third-party RAs external to the EU /European Economic Area (EEA) during the scientific assessment phases of the DCP (Figure 1).
Table 3. IGDRP working groupsWorking Group Objective ScopeActive substance master files/ drug master files
Establish a framework for information- sharing and potential mutual reliance in the assessment of ASMFs/DMFs
APIs for human use that are the subject of Master File assessments
Biowaivers Establish a common set of conditions for granting biowaivers as well as the possible expanded application of waivers
Biopharmaceutical Classification System (BCS)-based waiversNon-biostudy strengths of solid dosage form product line
Work-sharing model
Explore various work-sharing models with a view to piloting (an) appropriate model(s) for the premarket review of generic drugs
To include the model of the European Decentralised Procedure and possibly other models

9
WHO Drug Information Vol. 28 No. 1, 2014 Regulatory harmonization
The model would be operationalized based on the following conditions:• The process is restricted to the DCP.• Integrity of the DCP is respected (e.g.
structure, technical standards, timelines, etc.), with minimal impact on resources.
• The process is initiated at request of the generic drug applicant.
• The applicant gives consent to share confidential business information.
• No legal impediments exist on the part of the respective third party RA to participate in such an arrangement.
At the 5th IGDRP meeting in Geneva, members agreed that a logical first step would be to test the model through a limited pilot involving one or two non-EU RAs. This requires the willingness of a few generic drug manufacturers to participate in the pilot.
Interested regulatory authorities are currently consulting with the generic industry to identify suitable candidates with a view to launching the pilot in 2014. Further discussions are planned to elucidate the details of how the pilot would operate.
IGDRP members agreed that other models should also be considered, taking into account the availability and use of existing review reports as well as WHO’s experience with various regulatory work-sharing initiatives.
Some observationsAs the IGDR initiative enters its third and final year as a pilot, some observations may be made regarding the necessary prerequisites to successful outcomes.
The first and foremost prerequisite is the strong and continued commitment of participants to IGDRP goals and objectives.
Secondly, regulatory authorities must get to know one another, for example through rotating meetings which expose staff from host agencies to different points of view, serving in turn to promote change and convergence.
Thirdly, key enablers such as secure IT platforms, mechanisms for the exchange of confidential information and common technical requirements play a crucial role.
Fourth, relationships should be established with other international
Figure 1. Decentralised Procedures as a model for regulatory cooperation
Source: (3)

WHO Drug Information Vol. 28 No. 1, 2014
10
Regulatory harmonization
initiatives to leverage resources and avoid duplication of work.
Finally, the critical need for industry support for regulatory work-sharing efforts must be emphasized. Success of the IGDRP will require productive engagement with generic drug applicants as well as other stakeholders interested in promoting timely access to affordable, quality generic drugs.
Conclusion Considerable progress has been made since the start of the IGDRP in establishing the necessary conditions for enhanced regulatory cooperation. It is expected that work underway should lead to advancing regulatory convergence and the piloting of new models of cooperation prior to the end of 2014. Results of the pilot phase will inform decisions on whether and how the initiative should transition to a more permanent information- and work-sharing arrangement as part of broader international efforts
aimed at the effective and timely regulation of medicines within an increasingly challenging global environment.
References1 International Conference on the
Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use (ICH). Quality Guidelines [website], at www.ich.org/products/guidelines/quality/article/quality-guidelines.html.
2 Davit B, Braddy A, Conner D, Yu L. International Guidelines for Bioequivalence of Systemically Available Orally Administered Generic Drug Products: A Survey of Similarities and Differences. The AAPS Journal 2013; 15(4): 974-90.
3 Bachmann P. Global Generic Dossier and Evaluation: an EU Regulators‘ Perspective. Presentation made to the 16th Annual International Generic Pharmaceutical Alliance (IGPA) Conference, Brussels, Belgium; 9-11 December 2013.

11
WHO Drug Information Vol. 28 No. 1, 2014 Regulatory harmonization
WHO support for medicines regulatory harmonization in Africa: focus on East African Community
The African Medicines Regulatory Harmonization (AMRH) initiative works with Regional Economic Communities (RECs) to increase access to good quality, safe and effective medicines through harmonizing medicines regulations, and expediting registration of essential medicines.
Encouraging progress has been achieved in the East African Community (EAC), where a harmonized medicines registration system is being set up. Continued advocacy and political support by the New Partnership for Africa’s Development (NEPAD) and technical support by WHO are critical for its continued success.
Medicines regulatory authorities in many countries struggle with administrative and technical bottlenecks in controlling medicines quality in their territories effectively. And as pharmaceutical production and distribution have become globalized, no regulatory authority can work in isolation any longer.
The World Health Organization (WHO) has a long history in providing medicines regulatory support to governments of its Member States. In 2008 at the 13th International Conference of the Drug Regulatory Authorities (ICDRA) – a forum bringing together regulators from around 100 WHO Member States – WHO was requested to support harmonization approaches enabling national medicines regulatory authorities (NMRAs) to use their limited resources more effectively.
The African Medicines Registration Harmonization initiative In response to the request by its Member States, WHO initiated discussions with global partners. This led to the formation of a consortium consisting of the New Partnership for Africa’s Development (NEPAD), the Pan African Parliament (PAP), the Bill & Melinda Gates Foundation, the UK Department for International Development (DFID), the Clinton Health Access Initiative (CHAI),
the Joint United Nations Programme on HIV/AIDS (UNAIDS) and the World Health Organization (WHO). In 2009 NEPAD and PAP organized a conference attended by a wide range of stakeholders, marking the emergence of the African Medicines Registration Harmonization (AMRH) initiative.
The AMRH initiative aims to promote harmonization of medicines regulation in Africa. It is a close partnership among the World Bank, NEPAD and WHO, and most of the activities involve at least two partners. WHO is the lead partner on the development of common technical standards, documents, tools and processes in line with international standards such as those of the International Conference on the Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use (ICH). WHO also provides technical assistance for capacity-building and organizes joint assessment and inspection activities.
In 2010 the donor consortium decided to establish a trust fund for the AMRH finances, and an administration agreement was signed in 2011 between the World Bank and the Bill & Melinda Gates Foundation. WHO became a sub-grantee to support the implementation of the AMRH initiative.

WHO Drug Information Vol. 28 No. 1, 2014
12
Regulatory harmonization
The role of Regional Economic CommunitiesAfrican countries are grouped into Regional Economic Communities (RECs), which play a crucial role in a wide range of integration activities in Africa. Accordingly they were chosen as platforms for AMRH projects, seeing that they already had commitments for medicines regulatory harmonization, and their Secretariats have the necessary infrastructure to coordinate the work. The donor consortium therefore invited the African RECs to submit project proposals for regional medicines registration harmonization.
In this preparatory phase, WHO helped to develop and review proposals, assessed regulatory systems, provided training on the Common Technical Document format for medicines registration in Francophone and Anglophone countries throughout Africa, and approached other organizations to provide technical and financial support.
The EAC Medicines Registration Harmonization projectThe first REC to secure funding from the trust fund was the East African Community (EAC). WHO became a sub-grantee to support the implementation of the AMRH initiative and signed a memorandum of understanding with the EAC to support the Medicines Registration Harmonization (MRH) project.
The EAC MRH project was formally launched in March 2012 in Arusha, Tanzania, marking the beginning of the implementation phase of the AMRH initiative across Africa. The project aims to achieve a harmonized medicines registration process in its member countries – Uganda, Kenya, the United Republic of Tanzania, Rwanda and Burundi – based on common documents, processes and shared information
systems. More specifically, its objectives are to:• develop and maintain a “common
documentation package” defining common technical requirements as a basis for other harmonization activities;
• build evaluator capacity to ensure adherence to agreed standards;
• streamline management systems and processes, with risk-based approaches to use available resources where it matters most;
• develop systems and processes to share regulatory information within and outside EAC countries; and
• conduct joint dossier assessments and manufacturing site inspections as a basis for national registration decisions.
NMRA assessmentsAssessments of NMRAs are important to identify gaps and take corrective measures. For NMRAs entering into a harmonization process, they also provide an objective mechanism to evaluate progress. WHO has developed a data collection tool to assess regulatory systems. This tool was used in all five EAC countries by WHO and by the NMRAs as self-assessments or mutual assessments, providing valuable inputs to the methodology and outcomes of a comprehensive situation analysis for the EAC (1).
The assessment tool was subsequently improved and consolidated to cover all relevant product areas including medicines, vaccines and medical devices. It was also adapted to match the structure of the future harmonized EAC documents, and to support implementation of the harmonized processes with built-in quality management systems. WHO will continue to refine the tool. It is planned to develop an electronic version to facilitate data capture and analysis.

13
WHO Drug Information Vol. 28 No. 1, 2014 Regulatory harmonization
Table 1. EAC / WHO prequalification joint dossier assessments
Product Review period Date prequalified Date registeredAbacavir sulfate tablets
12 March 2010 – 17 July 2010(3 joint sessions)
20 August 2010 TanzaniaUgandaKenya
4 October 201014 October 201031 March 2011
Amikacin sulfate for injection
12 March 2010 – 20 November 2010 (4 joint sessions)
14 January 2011 UgandaTanzaniaKenya
7 June 2011*9 June 2011***
* The products were registered after completion of legally required testing of registration samples.** Significant delays occurred in submission of registration samples for testing; the applicant did
subsequently not pursue national registration.
Joint dossier assessments Another activity initiated by WHO before the formal launch of the EAC MRH project was the joint assessment of product dossiers that had been submitted to the NMRAs of EAC countries for national registration and to WHO for prequalification. The aim was twofold: to accelerate registration of needed products and to build knowledge and experience in assessing dossiers according to unified, stringent standards.
The first joint assessment exercise, organized in 2010, resulted in prompt registration of products (Table 1). The registration times were considerably shorter than the average 18 month timeline for registration of generic products in EAC countries (1).
A second joint assessment exercise started in July 2013 with five products: misoprostol tablets, levonorgestrel tablets and three strengths of artesunate/amodiaquine fixed-dose combination tablets. Four assessment rounds have been completed at the time of writing. A fifth is planned for March 2014, with only a few issues remaining to be addressed by the applicants before the products can be jointly deemed acceptable.
In this second joint exercise, a total of 12 assessors from all six participating NMRAs - the five EAC countries and Zanzibar – actively contributed to the
assessment work. The contributions from all of the regulators merged in a very natural way and made for a very motivating experience. Importantly, some time was spent in the third and fourth round to clarify what steps the products – once jointly accepted – would have to complete for formal registration in each country, with a view to minimizing the time taken for these steps and working towards common, streamlined processes in the longer term.
Progress towards harmonized registrationWith joint assessments and other preparatory activities already under way, the EAC MRH project got off to a good start. Four technical working groups were officially constituted in 2012, and each NMRA took technical lead in the development of regional guidelines, with the support of another NMRA (2). The working groups deal respectively with medicines evaluation and registration based on the Common Technical Document (CTD); good manufacturing practices (GMP); information management systems (IMS); and quality management system (QMS). WHO provides technical support in line with internationally recognized standards and best practice.
Significant progress has been achieved as at the end of 2013:

WHO Drug Information Vol. 28 No. 1, 2014
14
Regulatory harmonization
• Draft regulatory tools and guidelines produced by the working groups have been shared as “living documents” through the EAC’s website.
• EAC inspectors are participating in joint inspections organized by the WHO Prequalification of Medicines Programme.
• WHO and EAC NMRAs share their inspection schedules through a WHO-administered password-protected website.
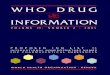
• Based on a WHO assessment of existing regulatory information systems in EAC countries and best practice recommendations, business process analysis is under way to design a harmonized information management system for regulatory functions (Figure 1).
WHO as the technical lead partner has provided input into all the above-mentioned activities. It has also proposed guidelines for developing and validating the EAC regulatory documentation, has set up a regulatory knowledge base containing
current, detailed bibliographies that are relevant to the EAC project, and has been issuing a quarterly newsletter for assessors and inspectors since 2011 with information on current regulatory concepts, guidance and standards.
Collaboration with other initiativesWHO’s long-standing collaboration with global regulatory initiatives such as ICH, the Asia-Pacific Economic Cooperation (APEC) Regulatory Harmonization initiative and the International Regulatory Cooperation for Herbal Medicines (IRCH) has been useful to establish linkages between the AMRH initiative and other regulatory initiatives in different regions.
This networking has facilitated the acceptance of the EAC as a member of the ICH Global Cooperation Group, which is a great achievement in its own right. WHO also supported EAC regulators to participate in ICH meetings, in the 2012 ICDRA conference and in annual WHO technical briefing seminars.
Figure 1. Towards a harmonized EAC medicines registration system: proposed high-level information system design
Source: (3)

15
WHO Drug Information Vol. 28 No. 1, 2014 Regulatory harmonization
ConclusionThe EAC Medicines Registration Harmonization project has achieved encouraging progress; and assessors and inspectors are working together with outstanding professionalism.
The main challenges, as identified by the project working groups, are twofold. Firstly, each partner state has its own laws and regulations, and the absence of a mutually recognized legal framework slows down many harmonization activities. Secondly, there is a marked difference in capacity among the NMRAs within the EAC region. Although a twinning system has been adopted – pairing each well-developed NMRA with a less advanced one – the harmonization moves at different speeds in the different countries.
Despite these challenges, the project has shown that regulators in EAC countries can implement effective, harmonized processes for review of registration submissions.
The AMRH initiative is soon to be expanded to other regional economic communities in Africa. Continued
support by concerned governments and international partners are crucial for its success. Provided that such support will be forthcoming on a sustained basis, the positive experiences made in the EAC region suggest that the AMRH initiative presents good opportunities for reshaping the regulatory landscape in Africa.
References1 Situation analysis study on medicines
registration harmonisation in Africa. Final report for the East African Community (EAC). November 2010.
2 Highlights from the Second Meeting of the Project Steering Committee for the EAC MRH Project, November 1-2 2012, Arusha. Meeting report.
3 EAC MRH Technical Working Group on Information Management System (IMS). Progress report to the national stakeholders meeting of the EAC regional steering committee [presentation]. September 2013. Posted on the EAC MRH Project working web site at http://health.eac.int/draftgmpdocuments.

16
WHO Drug Information Vol. 28 No. 1, 2014
16
Technologies, standards and norms
Standards for biological products
The 64th meeting of the WHO Expert Committee on Biological Standardization was held in Geneva from 21-25 October 2013. The large number of participants in attendance reflected the strong need expressed by Member States to WHO for support to appropriately regulate biological products.
The international standards established by the Committee are designed to be common global standards that promote regulatory convergence between countries. This is accomplished when the WHO standards are adapted into many national regulations, and when they are used by the WHO Prequalification Programme as the compliance standard for UN procurement. During the meeting, three new written standards were adopted that define regulatory expectations for biotherapeutic products, for adjuvanted vaccines, and for typhoid conjugate vaccines.
Biotherapeutic productsDevelopments in molecular genetics and nucleic acid chemistry have opened up new avenues for the production of medicines. Genes encoding natural biologically active proteins can be identified, modified and transferred from one organism to another in order to obtain highly efficient synthesis of their products. New recombinant DNA (rDNA)-derived biological medicines are now produced using a range of different expression systems such as bacteria, yeast, transformed cell lines of mammalian origin (including human origin), insect and plant cells, as well as transgenic animals and plants. rDNA technology is also used to produce biologically active proteins that do not exist in nature, such as chimeric, humanized or fully human monoclonal antibodies, or antibody-related proteins or other engineered biological medicines such as fusion proteins.
Together these technologies have enabled the production of large quantities of medicinal products that are difficult
to prepare from natural sources or were previously unavailable. Nevertheless, it is still not possible to fully predict the biological properties and clinical performance of these macromolecules on the basis of their physicochemical characteristics alone. In addition, they are produced in biological systems which are known to be inherently variable – with important consequences for the safety and efficacy of the resulting product. Therefore, before such biologicals are introduced into routine clinical use it must be ensured that their quality is consistent from lot to lot. This is achieved by developing robust manufacturing processes on the basis of process understanding and characterization, with appropriate in-process controls. Process understanding and consistency are critical since slight changes can occasionally have a major unwanted impact, for example on immunogenicity, with potentially serious safety implications.
The new guidelines on biotherapeutic products (1) are intended to provide

17
WHO Drug Information Vol. 28 No. 1, 2014 Technologies, standards and norms
national regulatory authorities (NRAs) and manufacturers with guidance on the quality, safety and efficacy of rDNA-derived biotherapeutics) and intended for use in humans. The guidelines are based on experience gained over three decades in this technically demanding field. Part A sets out updated guidelines for the manufacture and quality control of rDNA-derived biotherapeutics, including consideration of the effects of manufacturing changes and of devices used in the delivery of the product and on its stability. Part B provides guidelines on nonclinical evaluation, while Part C provides guidance on clinical evaluation. Product-specific vaccine-related recommendations and guidelines are available elsewhere1, as are additional considerations for similar biotherapeutic products (2).
Adjuvanted vaccinesThe second global standard adopted by the Expert Committee provides guidance to NRAs and manufacturers on the nonclinical and initial clinical evaluation of vaccine adjuvants and adjuvanted vaccines (3) by outlining the international regulatory expectations in this area.
Over the past decades, new approaches have been devised to develop and deliver vaccine antigens. Some of these antigens are weakly immunogenic and require the presence of adjuvants to induce or enhance an adequate immune response. Vaccines with aluminium-based adjuvants have been used extensively in immunization programmes worldwide, and a significant body of safety information has accumulated for them. As science and technology have advanced, vaccines containing adjuvants other than aluminium-containing compounds (e.g. human papillomavirus and hepatitis B vaccines)
1 For product-specific vaccine-related WHO recommendations and guidelines see: http://www.who.int/biologicals/vaccines/en/
have been authorized for use in many countries, and a number of vaccines with novel adjuvants are currently under development, such as vaccines against human immunodeficiency virus (HIV), malaria and tuberculosis, as well as new-generation vaccines against influenza and other diseases.
However, the development and evaluation of adjuvanted vaccines present regulatory challenges. Vaccine manufacturers and regulators have questions about the type of information and extent of data that would be required before adjuvanted vaccines can proceed to clinical trials and eventually be authorized for use. Existing WHO guidelines on nonclinical evaluation of vaccines (4) give valuable general guidance but provide limited information specifically related to new adjuvants and adjuvanted vaccines.
The new guideline provides updated and more extensive guidance on the nonclinical and preclinical testing of adjuvants and adjuvanted vaccines. It should allow manufacturers and regulators to proceed on the critical path towards licensure of adjuvanted vaccines that will help to control some diseases with important global public health impact.
Typhoid conjugate vaccinesThe third set of guidelines adopted by the Committee are intended to assist NRAs in evaluating the scientific issues connected with the quality, safety and efficacy of typhoid conjugate vaccines that use Vi polysaccharide covalently linked to a carrier protein (5). The available guidelines for Vi polysaccharide typhoid vaccine (6) and for live, attenuated Ty21a vaccines (7) are not applicable to this type of typhoid vaccines, which have carrier proteins such as diphtheria toxoid (DT), tetanus toxoid (TT), recombinant Pseudomonas aeruginosa exoprotein A (rEPA), the

WHO Drug Information Vol. 28 No. 1, 2014
18
Technologies, standards and norms
nontoxic mutated form of diphtheria toxin – for example, cross-reactive material 197 (CRM197) – or another suitable protein.
The evidence gathered thus far indicates that typhoid conjugate vaccines may have several advantages over unconjugated Vi polysaccharide vaccines, including: (i) greater efficacy and effectiveness; (ii) longer persistence of immunity; (iii) immunogenicity across all age groups, including infants and toddlers aged younger than 2 years; (iv) perhaps some degree of herd immunity; and (v) induction of immune memory with initial dosing, leading to anamnestic responses to a subsequent dose or doses.
The guidelines are based on experience gained during the development of experimental typhoid conjugate vaccines as well as relevant information obtained from the evidence for other types of bacterial polysaccharide–protein conjugate vaccines, such as Haemophilus influenzae type b (Hib), and meningococcal and pneumococcal conjugate vaccines. Part A of the guidelines sets out guidance on manufacturing and quality control, while Part B addresses the nonclinical evaluation of these vaccines and Part C addresses their clinical evaluation. Part D provides guidance for NRAs.
Reference preparationsThe provision of internationally accepted biological reference preparations is an important normative activity of WHO. These global measurement standards enable the efficacy, quality, purity and safety of very many biological products to be stated in a common language worldwide. Thus, biological reference preparations support:• Biological and immunological assays
for the quality control of a wide range of biologicals – therapeutics, blood-derived
products, vaccines and immunological products of traditional types – as well as those derived from modern biotechnological approaches.
• Standardization of materials and approaches used in medical diagnostics such as diagnosing disease, monitoring therapy, blood safety, and public health applications (such as monitoring immune status, screening for disease or susceptibility) or otherwise characterizing biological material from individuals.
• Development, evaluation, standardization and control of products by industry, by regulatory authorities, and also in biological research in academia and scientific organizations. They play a vital role in facilitating the transfer of laboratory science into worldwide clinical practice and the development of safe and effective biologicals.
These reference preparations are provided to Member States to calibrate national, or regional, quality control materials for biological medicines and regulated diagnostic tests. The latter, for example, enable quantitative limits to be expressed in regulations in standardized units of measurement. New reference preparationsTwelve new international biological reference preparations were adopted by the Expert Committee (see Table 1) and have been added to the catalogue of WHO biological reference preparations for blood products and related substances2. Discontinued reference preparationsThe Committee agreed to discontinue the following reference preparations which were considered no longer fit for purpose: • anti-echinococcus serum (code number
ECHS 75.1106);• anti-C complete blood typing serum
(code number W1004 84.1424);
2 http://www.who.int/bloodproducts/catalogue/Bloo2014.pdf

19
WHO Drug Information Vol. 28 No. 1, 2014 Technologies, standards and norms
• anti-E complete blood-typing serum, human (code number W1005 83.1424).
New projectsThe Committee endorsed a number of new projects. The timely development of new reference materials and standards is critically important to harness scientific developments for new biologicals. At the same time, the active management of the
existing inventory of reference preparations requires a carefully planned programme of work to replace established materials before the stock of containers, which comprises the standard, is exhausted. The Committee agreed to the initiation of the following new projects on reference preparations for vaccines and related materials:
Table 1. Additions to the list of WHO International Biological Reference Preparations and Reference Panels
Preparation Activity StatusCytokines, cell factors and biotherapeutics other than blood products:Pegylated Granulocyte Colony
Stimulating Factor 10 000 IU per ampoule First WHO Inter-
national Standard (IS)Tumor Necrosis Factor alpha,
recombinant, for bioassay43 000 IU per ampoule Third WHO IS
In vitro diagnostic device reagents:Antibodies to Hepatitis B virus “e”
antigen (anti-HBe) **120 IU/mL First IIS
Hepatitis A virus RNA for NAT-based assays *
54 000 IU/mL Second IS
Hepatitis B virus “e” antigen (HBeAg) **
100 IU/mL First IS
Hepatitis D virus RNA for NAT-based assays **
575 000 IU/mL First IS
HIV-1 Circulating Recombinant Forms RNA for NAT-based assays *
Ten panel members consisting of CRFs and other variants. No unitage assigned
First International Reference Panel
Human Serum IgE * 13 500 IU/mL Third ISMycoplasma DNA for NAT-based
assays designed for generic mycoplasma detection **
200 000 IU/mL First IS
Parvovirus B19 DNA for NAT-based assays *
1 410 000 IU/mL Third IS
Vaccines:Trivalent inactivated polio vaccine, for D antigen assay
277 DU/ml for poliovirus type 1 65 DU/ml for poliovirus type 2 248 DU/ml for poliovirus type 3
Third IS
Notes:Vaccines and related substances, cytokines, growth factors and biotherapeutics other than blood products, and in vitro diagnostic device reagents identified by * are held and distributed by the National Institute for Biological Standards and Control, Potters Bar, Herts, EN6 3QG, England. In vitro diagnostic device reagents identified by ** are held and distributed by the Paul-Ehrlich-Institut, 63225 Langen, Germany.

WHO Drug Information Vol. 28 No. 1, 2014
20
Technologies, standards and norms
• diphtheria toxoid for flocculation test (3rd IS);
• meningococcal Serogroup A polysaccharide (1st IS);
• typhoid Vi polysaccharide (1st IS);• high and low mutant virus reference
preparations for MAPREC assay of poliovirus type 2 (2nd IS);
• antiserum to Respiratory Syncytial Virus (1st IS).
Regarding the proposal for generic approval of standards and reference panels for cancer diagnostics, the Committee felt that this represents a large commitment that needs clarification from WHO in regard to the Committee’s focus and resources.
No requests were received to initiate new projects for cytokines, growth factors and endocrinological substances or for antibiotics.
The Committee agreed to the initiation of the following new projects on reference preparations on blood products and in vitro diagnostic devices: • replacement of Hepatitis C Virus RNA for
NAT assays (5th IS);• Anti-Cytomegalovirus IgG;• Malaria (P. falciparum) antibody
reference panel;• high and low titre anti-A and anti-B in
serum/plasma;• anti-Rubella Immunoglobulin;• replacement of Anti-Tetanus
Immunoglobulin (2nd IS);• assignment of FIX antigen value to
4th IS/5thFIX plasma/concentrate;• replacement of Ancrod (2nd IS);• replacement of Streptokinase (4th IS).
References
1 Guidelines on the quality, safety, and efficacy of biotherapeutic protein products prepared by recombinant DNA technology. Replacement of Annex 3 of WHO Technical Report Series (TRS), No. 814. Geneva: World Health Organization; 2013.
2 Guidelines on evaluation of similar biotherapeutic products (SBPs). In: WHO Expert Committee on Biological Standardization. Sixtieth report. Geneva: World Health Organization; 2013: Annex 2 (WHO TRS, No. 977).
3 Guidelines on the nonclinical evaluation of vaccine adjuvants and adjuvanted vaccines. Geneva: World Health Organization; 2013.
4 WHO guidelines on nonclinical evaluation of vaccines. In: WHO Expert Committee on Biological Standardization. Fifty-fourth report. Geneva: World Health Organization; 2005: Annex 1 (WHO TRS, No. 927).
5 Guidelines on the quality, safety and efficacy of typhoid conjugate vaccines. Geneva: World Health Organization; 2013.
6 Requirements for Vi polysaccharide typhoid vaccine (Requirements for Biological Substances No. 48). In: WHO Expert Committee on Biological Standardization. Forty-third report. Geneva: World Health Organization; 1994: Annex 1 (WHO TRS, No. 840).
7 Requirements for typhoid vaccine (live attenuated, Ty21a, oral) (Requirements for Biological Substances No. 34). In: WHO Expert Committee on Biological Standardization. Thirty-fourth report. Geneva: World Health Organization; 1983: Annex 3 (WHO Technical Report Series, No.700).

21
WHO Drug Information Vol. 28 No. 1, 2014
21
Safety and efficacy issues
Combined hormonal contraceptives and venous thromboembolismEuropean Un ion – The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has completed its review of risks associated with combined hormonal contraceptives (CHCs), and has concluded that the benefits of CHCs in preventing unwanted pregnancies continue to outweigh their risks.
The product information of CHCs will be updated to help women make informed decisions about their choice of contraception. When prescribing a CHC healthcare professionals should consider the individual woman’s current risk factors. CHCs are contraindicated if a woman has one serious risk factor or multiple risk factors for blood clots. Reference: EMA Press release,
22 November 2013.
Clobazam: serious skin reactionsUni ted S ta tes o f Amer ica – The Food and Drug Administration (FDA) is warning the public that clobazam (Onfi®), a benzodiazepine medication used with other medicines to treat seizures in a severe form of epilepsy, can cause rare but serious skin reactions that can result in permanent harm and death.
FDA identified clobazam as the likely cause in a number of reports of Stevens-Johnson syndrome and toxic epidermal necrolysis. The risk appeared to be greatest during the first 8 weeks after starting or re-starting clobazam treatment.
Patients taking clobazam should seek immediate medical attention if they develop
a rash, blistering or peeling of the skin, sores in the mouth, or hives. Health care professionals should discontinue clobazam and consider an alternate therapy at the first sign of rash, unless it is clearly not drug-related. Patients should not stop taking clobazam without consulting their health care professionals, as sudden withdrawal can cause serious problems such as seizures, hallucinations, shaking, nervousness, and stomach or muscle cramps. Reference: FDA Drug Safety
Communication, 3 December 2013
Amiodarone: pulmonary toxicityNew Zea land – MedSafe has informed health care professionals of pulmonary toxicity associated with amiodarone, used to treat tachyarrhythmias. Pulmonary toxicity is estimated to occur in approximately 5% of patients taking amiodarone. It can rarely present as acute respiratory distress – for example after recent surgery – with a mortality of up to 50%. Chronic symptoms are more frequent and have been associated with a mortality of up to 10% in some studies.
Early recognition is vital. All patients receiving amiodarone should be monitored for the development of pulmonary toxicity and other adverse effects; MedSafe has recommended a range of screening measures.
Pulmonary toxicity should be suspected in all patients with new or worsening symptoms whilst taking amiodarone. Amiodarone should be stopped in all suspected cases. Corticosteroids may be considered as a treatment option. Due to

WHO Drug Information Vol. 28 No. 1, 2014
22
Safety and efficacy issues
amiodarone’s long half-life symptoms may initially worsen or be slow to resolve. Slow withdrawal of the corticosteroids over at least two to six months is recommended to prevent rebound pulmonary toxicity. Reference: MedSafe, Publications,
Prescriber Update 34(4): 38-39. December 2013.
Methylphenidate: rare risk of long-lasting erections in malesUni ted S ta tes o f Amer ica – The Food and Drug Administration (FDA) is warning that methylphenidate products, a medicine used to treat attention deficit hyperactivity disorder (ADHD), may in rare instances cause prolonged and sometimes painful erections known as priapism. If not treated immediately, priapism can lead to permanent damage to the penis.
Priapism may be more likely to occur with the use of immediate-release methylphenidate, which has a shorter half-life. The risk with alternative treatments such as atomoxetine and amphetamine is unclear.
Male patients and their caregivers should be taught the signs and symptoms of priapism and the importance of seeking immediate medical treatment if erections lasting longer than four hours occur.Reference: FDA Drug Safety
Communication, 17 December 2013.
Glibenclamide: risk of hypoglycaemia in elderly and renal-impaired patientsSingapore – The Health Science Authority (HSA) had conducted a benefit-risk assessment of glibenclamide and advises against its use in patients over 60 years of age and those with impaired renal function, as these patients are at risk of developing severe, long-lasting hypoglycaemia.
In 2012, the World Health Organisation (WHO) had recommended to avoid using glibenclamide in patients older than 60 years of age. Similar recommendations were made by the US Kidney Disease Outcomes Quality Initiative (KDOQI) in 2012 and the Canadian Diabetes Association in 2013.Reference: HSA Product Safety Alert,
31 December 2013.
Subcutaneous epoetin alfa: contraindicated in Singapore in chronic kidney disease patientsSingapore – Further to local reports of antibody-mediated cases of pure red cell aplasia – a decline of red blood cells produced by the bone marrow – in patients with chronic kidney disease, the Health Sciences Authority (HSA) advises that subcutaneous (SC) epoetin alfa (Eprex®) is contraindicated in Singapore in these patients. Although a comprehensive review could not determine the root causes (such as storage/handling issues and quality/manufacturing issues), HSA considers that the totality of information on these serious and potentially life-threatening adverse events warrants a contraindication.Reference: HSA Product Safety Alert,
31 December 2013.
Acipimox: only to be used as additional or alternative treatment European Un ion – The Co-ordination Group for Mutual Recognition and Decentralised Procedures - Human (CMDh) – a body representing EU Member States – has confirmed that acipimox, a medicine to treat high triglyceride levels, should be used across the European Union only when diet, exercise, and treatment with other medicines are not adequate.

23
WHO Drug Information Vol. 28 No. 1, 2014 Safetyandefficacyissues
The benefit-risk balance of acipimox was reviewed as a result of outcomes of a study on nicotinic acid, a related medicine, in combination with laropiprant. Findings from that study were used to expand the warnings in the acipimox product information on a possible increased risk of painful muscle damage when acipimox is used together with a statin.Reference: EMA Press release,
20 December 2013.
Estradiol-containing creams: new restrictionsEuropean Un ion – The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) advises that Linoladiol N and Linoladiol HN, two high-strength estradiol-containing creams used in post-menopausal women, may continue to be used with certain restrictions. The estradiol being absorbed from the creams into the body can cause risks similar to those in systemic hormone replacement therapy, including venous thromboembolism, stroke and endometrial cancer.
Linoladiol N may continue to be used to treat vaginal atrophy when at least one topical, lower-dose oestrogen treatment has failed. The use of Linoladiol HN, which also contains a weak corticosteroid, should be limited to treatment of mild, inflammatory skin diseases of the external genital area. Both creams should be used for no longer than four weeks at a time. Reference: EMA Press release,
20 December 2013.
Clopidogrel: rare reports of acquired haemophiliaUni ted K ingdom – The Medicines and Healthcare Products Regulatory Agency MHRA draws attention to reports
of acquired haemophilia received in association with clopidogrel. This very rare but serious condition may be missed due to the established risk of bleeding associated with clopidogrel treatment.
Although these events are very rare (12 cases reported worldwide to the marketing authorization holder whereas more than 153 million patients use the medicine), healthcare professionals should be aware of this serious and possibly life-threatening risk. Prompt diagnosis is required to minimise the risks of bleeding. A possible sign of acquired haemophilia is an isolated prolonged activated partial thromboplastin time (aPTT). Patients with confirmed acquired haemophilia should be managed by specialists, and clopidogrel should be discontinued. Invasive procedures should be avoided.Reference: MHRA. Drug Safety Update 7
(5), December 2013: A2.
Sodium phosphate products in high doses: severe dehydrationUni ted S ta tes o f Amer ica – The Food and Drug Administration (FDA) is warning that using more than one dose in 24 hours of oral or rectal sodium phosphate products can cause severe dehydration and electrolyte abnormalities associated with serious complications such as acute kidney injury and arrhythmias. Sodium phosphate over-the-counter (OTC) products are used to treat constipation.
Nearly half of the adult cases and 3% of the pediatric cases reviewed by FDA had a fatal outcome. Life-threatening effects occurred in more than two-thirds of affected adults and in all of the affected children, with acute deterioration in respiratory status, mental status and heart function. Most cases involved older adults and children younger than 5 years.

WHO Drug Information Vol. 28 No. 1, 2014
24
Safety and efficacy issues
FDA reminds consumers and health care professionals to always use these products as recommended on the label, and not to exceed the labeled dose. The oral products should not be given to children 5 years and younger without discussing with a health care professional. The rectal form should never be given to children under 2 years. Reference: FDA Drug Safety
Communication, 8 January 2014.
Emergency contraceptives – high bodyweight may reduce effectivenessEuropean Un ion – New data suggest that a high bodyweight could impair the effectiveness of emergency contraceptives in preventing an unintended pregnancy following unprotected sexual intercourse or contraceptive failure. The European Medicines Agency (EMA) has initiated a review by its Committee for Medicinal Products for Human Use (CHMP) to assess whether any changes should be made to the product information for emergency contraceptive medicines containing levonorgestrel or ulipristal acetate.
Emergency contraceptives containing levonorgestrel can be used up to 72 hours after unprotected sexual intercourse or contraceptive failure while ulipristal acetate can be used up to 120 hours. Levonorgestrel-containing emergency contraceptives are available without a prescription in certain European countries. Ulipristal acetate can only be obtained with a prescription.Reference: EMA Press release, 24 January
2014.
Testosterone: possible risk of stroke and heart attackUni ted S ta tes o f Amer ica – Outcomes of two recent studies prompted the Food and Drug Administration (FDA) to reassess the risk of stroke, heart attack and death associated with testosterone products. These products are FDA-approved only for use in men who lack or have low testosterone levels due to a medical reason such as genetic problems or chemotherapy. Approved formulations include the topical gel, transdermal patch, buccal system (applied to upper gum or inner cheek), and injection.
Awaiting the outcomes of the FDA review, health care professionals should consider the risks and benefits of FDA-approved testosterone treatment, and should report side effects to the FDA MedWatch program.Reference: FDA Safety Announcement, 31
January 2014.
Lithium: hypercalcaemia and hyperparathyroidismCanada – Health Canada has reviewed available evidence and has determined that lithium therapy can cause hypercalcaemia, which may or may not be accompanied with hyperparathyroidism. However, the benefits of lithium in the treatment of manic episodes of manic-depressive illness continue to outweigh the known risks. The authority advises health professionals to consider calcium and parathormone blood levels before and during treatment, and to report any cases of serious hypercalcaemia and hyperparathyroidism or other serious or unexpected adverse events to Health Canada.Reference: Health Canada advisory safety
information, 5 February 2014.

25
WHO Drug Information Vol. 28 No. 1, 2014 Safetyandefficacyissues
Saxagliptin: possible risk of heart failureUni ted S ta tes o f Amer ica – The Food and Drug Administration (FDA) has requested clinical trial data from the manufacturer of saxagliptin (Onglyza®, Kombiglyze XR®) to investigate a possible association between use of the type 2 diabetes medicine and heart failure. A preliminary study did not find increased rates of death or other major cardiovascular risks. FDA urges health care professionals and patients to report side effects involving saxagliptin products to the FDA MedWatch programme.Reference: FDA Drug Safety
Communication, 11 February 2014.
Strontium ranelate: further restrictions due to cardiovascular risksEuropean Un ion – The Committee for Medicinal Products for Human Use (CHMP) of the European Medicines Agency has concluded its review of strontium ranelate (Proteos®/Osseor®) and has recommended further restricting its use to patients with severe osteoporosis who have a high risk of fracture and cannot be treated with other approved medicines. Treatment should be stopped if patients develop heart or circulatory problems such as uncontrolled high blood pressure or angina. As recommended in a previous review, patients who have a history of certain heart or circulatory problems must not use the medicine.
The Pharmacovigilance Risk Assessment Committee (PRAC) had recommended to suspend the medicine. The CHMP determined that for patients who have no alternative treatment it has
benefits in preventing fractures, and that regular screening and monitoring every 6 to 12 months to exclude cardiovascular disease will sufficiently reduce the risk. Educational material will be provided to prescribers to ensure that only the appropriate patients are treated with the medicine. The marketing authorization holder is required to conduct further research to demonstrate the effectiveness of the new measures. Reference: EMA Press release, 21 February
2014.
Methysergide-containing medicines: new restrictions European Un ion – The European Medicines Agency (EMA) has recommended restricting the use of methysergide, an ergot alkaloid medicine, due to concerns over its association with fibrosis raised by the French medicines agency ANSM in May 2012. Fibrosis is a condition in which scar tissue accumulates in the body’s organs.
Methysergide-containing medicines are now only to be used for preventing severe intractable migraines and cluster headaches when alternative treatment has failed. It is no longer recommended to treat diarrhoea caused by carcinoid disease.Treatment should be started and supervised by an experienced specialist. Patients should be screened for fibrosis at the start of treatment and every 6 months thereafter to prevent severe and potentially life-threatening damage to organs. Reference: EMA Press release, 21 February
2014.

26
WHO Drug Information Vol. 28 No. 1, 2014
26
Regulatory action and news
Regulatory options in the fight against antimicrobial resistanceEuropean Un ion – The European Medicines Agency (EMA) has published a report highlighting the outcomes of its workshop titled “Best use of medicines legislation to bring new antibiotics to patients and combat the resistance problem”. The event, held in November 2013, brought together key EU and international stakeholders. Recommendations were made in three areas:• the effective use of the current EU
regulatory framework for approval of new antibacterials, including a new evaluation guideline with a recently adopted addendum, as well as the EMA’s fee waiver system for small and medium enterprises;
• the appropriate use of antibacterials for human and veterinary use; and
• research and development, with an efficient and early dialogue between industry and EMA.
Reference: EMA News, 12. December 2013.
EMA and FDA collaborate on bioequivalence inspectionsEuropean Un ion / Un i ted S ta tes o f Amer ica – The European Medicines Agency (EMA) and the United States Food and Drug Administration (FDA) have launched a joint initiative to share information on inspections of bioequivalence studies submitted to participating authorities. These initially include the FDA and the regulatory authorities of France, Germany, Italy, the
Netherlands and the United Kingdom. Additional EU member states are expected to join the initiative in the future.
Bioequivalence studies submitted in support of generic medicines applications must demonstrate scientifically that the generic product performs in the same manner as the innovator medicine.
The initiative, which includes an 18-month pilot phase, will be carried out in the framework of the confidentiality arrangements established between the European Commission, the EMA, interested EU Members States and the FDA. Its key objectives are to:• streamline information-sharing on
inspections of bioequivalence studies conducted and planned for generic medicines marketing authorization applications (information will be shared for clinical facilities, analytical facilities or both);
• share information on negative inspection outcomes, which reveal system problems of these facilities;
• conduct joint inspections of clinical trial sites all over the world; and
• provide training opportunities to improve bioequivalence inspections.
The initiative builds on the successful 2009 EMA-FDA Good Clinical Practice (GCP) Initiative, designed to ensure that clinical trials submitted in marketing applications for medicines in the United States and Europe are conducted ethically and that the data generated by these trials are reliable.References:
EMA Press release, 18 December 2013. FDA News release, 18 December 2013.

27
WHO Drug Information Vol. 28 No. 1, 2014 Regulatory action and news
Tafenoquine receives FDA Breakthrough Therapy designation Uni ted S ta tes o f Amer ica – The US Food and Drug Administration has granted Breakthrough Therapy designation for tafenoquine, an investigational medicine for the treatment and relapse prevention of Plasmodium vivax malaria. The designation will expedite the regulatory review process of the potential new medicine, which recently completed Phase II clinical trials successfully.Reference: Medicines Venture for Malaria
(MMV). Press release, 20 December 2013.
Regulatory action against Ranbaxy’s Toansa facility Uni ted S ta tes o f Amer ica – The Food and Drug Administration (FDA) has prohibited the manufacturing site in Toansa, India of Ranbaxy Laboratories, Ltd from producing and distributing active pharmaceutical ingredients (APIs) for FDA-regulated drug products. The Toansa facility is now subject to certain terms of a consent decree of permanent injunction entered against Ranbaxy in January 2012.
The decree contains, among other things, provisions to ensure compliance with current good manufacturing practice (cGMP) requirements at Ranbaxy facilities in Paonta Sahib and Dewas, India, as well as provisions to address data integrity issues at those facilities. In September 2013, the FDA added Ranbaxy’s Mohali facility to the cGMP provisions of the decree.
The FDA’s inspection of the Toansa facility, which concluded in January 2014, identified significant cGMP violations. These included Toansa staff retesting raw materials, intermediate drug products and finished API after those items failed analytical testing and specifications in order to produce acceptable findings, and
subsequently not reporting or investigating these failures.Reference: FDA News Release, 23 January
2014.
WHO response to FDA findings at Ranbaxy’s Toansa siteWor ld Hea l th Organ iza t ion – In response to the US Food and Drug Administration (FDA)’s findings at Ranbaxy’s Toansa facility during an unannounced inspection in January 2014, the WHO Prequalification Programme has suspended its authorization to use active pharmaceutical ingredients (APIs) from that facility in WHO-prequalified finished products. It has also suspended all assessment of Ranbaxy’s applications to prequalify APIs from the Toansa site in their own right.
WHO had requested Ranbaxy to address major deficiencies observed at the Toansa site in June 2013. As WHO has verified, since 2010 Ranbaxy has used only approved APIs from sites other than Toansa in the manufacture of the four prequalified products concerned. With international regulatory partners WHO will now ascertain supply options to avoid shortages of needed formulations.
The WHO Prequalification Programme condemns GMP practices that lead to provision of misleading information and advises buyers of medicines to consider the manufacturer’s track record and API sources before undertaking any procurement.Reference: WHO Press note. 24 January
2014
New partnership to strengthen regulatory systemsSwi tzer land – The Bill & Melinda Gates Foundation, the Swiss Federal Department of Home Affairs and the

WHO Drug Information Vol. 28 No. 1, 2014
28
Regulatory action and news
Federal Department of Foreign Affairs have signed a Memorandum of Understanding (MOU) to improve and accelerate access to medicines in resource-constrained countries. This should be achieved through cooperation to strengthen regulatory systems in these countries. The cooperation aims to increase the efficiency of the regulatory review and registration process and will initially focus on sub-Saharan countries.Reference: Swissmedic Announcement, 23
January 2014.
Canada-US Common Electronic Submissions GatewayCanada - Health Canada has launched the Common Electronic Submissions Gateway (CESG), making it possible for companies to submit medicines authorization data online using a special dedicated channel of the United States Food and Drug Administration’s (US FDA) existing system. This ongoing shared mechanism was created part of ongoing work by the Canada-US Regulatory Cooperation Council to better align regulatory systems between Canada and the United States.Reference: Health Canada News release, 31
January 2014.
Updated guidance for annual strain change of seasonal influenza vaccinesEuropean Un ion – The European Medicines Agency (EMA) has updated its guidance for the annual strain change of influenza vaccines to reflect current knowledge and align it with the approaches of other regulatory authorities globally.
The update introduces a system for strengthened and sustainable monitoring of an influenza vaccine’s performance over the years in a real-life setting. From
the influenza season 2014-2015 onwards, vaccine manufacturers will be required to submit for each vaccine appropriate measures for proactive surveillance of the safety and effectiveness to regulatory authorities for review. From the influenza season 2015-2016, with the new system in place, EMA will longer requires routine submission of clinical trials for annual strain-change updates. EMA will publish interim guidance by March 2014 on the principles of safety monitoring commitments that should form part of the proactive surveillance.Reference: EMA News. 7 February 2014.
EMA and FDA strengthen collaboration on pharmacovigilance European Un ion / Un i ted S ta tes o f Amer ica – The European Medicines Agency (EMA) and the United States Food and Drug Administration (FDA) have set up a new forum for monthly teleconference meetings on pharmacovigilance (medicine safety) topics. Canadian and Japanese regulatory authorities will participate as observers. This increased degree of interaction will allow the authorities to work swiftly in the area of the safety of medicines and to coordinate communication activities.
The EMA and the FDA have already set up collaborative clusters to discuss issues related to biosimilars, medicines to treat cancer, orphan medicines, medicines for children and blood-based products, among other topics. The creation of the pharmacovigilance cluster is the latest step in the EMA’s and FDA’s wider approach to expand and reinforce international collaboration.References:
EMA News, 19 February 2014. FDA News release, 19 February 2014.

29
WHO Drug Information Vol. 28 No. 1, 2014 Regulatory action and news
European Medicines Agency publishes first summary of a risk-management plan for a medicineEuropean Un ion – The European Medicines Agency (EMA) has published the first summary for the public of the risk management plan (RMP) of a newly authorised medicine, namely florbetaben (18F) (Neuraceq®). The summary describes what is known and not known about the medicine’s safety and states what measures will be taken to prevent or minimize its risks. EMA will pilot the publishing of RMP summaries for all newly centrally authorized medicines during 2014.
This new type of publication is a further step towards increased transparency and is one of the requirements of the new European pharmacovigilance legislation. The RMP summary complements the European public assessment report (EPAR) summary. EMA had revised the EPAR format in 2013 to provide more information on the benefit-risk balance of medicines. Reference: EMA News, 11 March 2014.
EMA and FDA extend parallel assessment pilot European Un ion / Un i ted S ta tes o f Amer ica – The European Medicines Agency and the United States Food and
Drug Administration have extended their joint pilot programme for the parallel evaluation of quality-by-design (QbD) applications until 2015. The programme promotes the consistent implementation of the concepts of ICH quality guidelines Q8, Q9, Q10 and Q11. Applicants that volunteer to make use of the programme benefit from a harmonized evaluation of the relevant parts of their submission.Reference: EMA News, 6 March 2014.
Australia and New Zealand harmonization activitiesAust ra l ia / New Zea land – In working towards an Australia New Zealand Therapeutic Products Agency (ANZTPA) the TGA and Medsafe embarked on a regulatory alignment programme in November 2013. Of 14 activities in the areas of medicines, active pharmaceutical ingredients, safety, medical devices and biological and blood products, two have been completed in the first quarter of 2014: New Zealand changed paediatric dosage instructions for paracetamol and ibuprofen to align with Australia, and the two authorities have published a common list of colouring substances allowed for use in medicines for oral and topical use.Reference: ANZTPA News and updates as
at 17 March 2014.
Approvals
First adjuvanted vaccine for H5N1 avian influenza approved Uni ted S ta tes o f Amer ica – The Food and Drug Administration (FDA) has approved the first adjuvanted vaccine for the prevention of H5N1 influenza, commonly known as avian or bird flu, for use in people 18 years of age and older who are
at increased risk of exposure to the H5N1 influenza virus. The vaccine is not intended for commercial availability. The U.S. Department of Health and Human Services has purchased it from the manufacturer for the National Stockpile for distribution by public health officials if needed.

WHO Drug Information Vol. 28 No. 1, 2014
30
Regulatory action and news
The H5N1 component and the AS03 adjuvant component are supplied in two separate vials, which must be combined prior to use. The vaccine is administered via intramuscular injection in two doses, 21 days apart. Efficacy studies showed that 91% of individuals between the ages of 18 and 64 years and 74% of individuals 65 years and older who received the two-dose regimen developed antibodies at a level that is expected to reduce the risk of getting influenza.Reference: FDA news release, 22 November
2013.
Umeclidinium and vilanterol approved for chronic obstructive pulmonary diseaseUni ted S ta tes o f Amer ica – The Food and Drug Administration (FDA) has approved umeclidinium and vilanterol inhalation powder (Anoro Ellipta®) for the once-daily, long-term maintenance treatment of patients with chronic obstructive pulmonary disease (COPD).
Umeclidinium is an anticholinergic that relaxes the muscles around the large airways, and vilanterol is a long-acting beta2-adrenergic agonist (LABA) that relaxes the muscles of the airways. LABAs increase the risk of asthma-related death. Umeclidinium and vilanterol inhalation powder is not approved for the treatment of asthma, nor should it be used to treat acute bronchospasm. Side effects can be serious and include narrowing and obstruction of the respiratory airway (paradoxical bronchospasm), cardiovascular effects, increased pressure in the eyes (acute narrow-angle glaucoma), and worsening of urinary retention.Reference: FDA News Release,
18 December 2013.
Dapaglifozin approved for type 2 diabetesUni ted S ta tes o f Amer ica – The Food and Drug Administration (FDA) has approved dapaglifozin (Farxiga®) tablets to improve glycaemic control, along with diet and exercise, in adults with type 2 diabetes.
Dapaglifozin is a sodium-glucose co-transporter 2 (SGLT2) inhibitor that blocks the reabsorption of glucose by the kidney, increases glucose excretion and lowers blood glucose levels. It has been studied as a stand-alone therapy and in combination with other type 2 diabetes therapies.
Dapaglifozin should not be used to treat patients with type 1 diabetes,with increased ketones in their blood or urine (diabetic ketoacidosis), or with renal impairment. It is not recommended for patients with active bladder cancer and should be used with caution in patients with a history of bladder cancer. Dapaglifozin can cause dehydration, especially in patients with age-related or otherwise impaired renal function and those taking diuretics.Reference: FDA News Release, 8 January
2014.
Trametinib and dabrafenib approved in combination for advanced melanomaUni ted S ta tes o f Amer ica – The Food and Drug Administration (FDA) has approved trametinib (Mekinist®) in combination with dabrafenib (Tafinlar®) to treat patients with unresectable or metastatic melanoma. This follows the approval of the two medicines as single agents in May 2013. The combination was approved under the FDA’s Accelerated Approval Program. Reference: FDA News Release, 10 January
2014.

31
WHO Drug Information Vol. 28 No. 1, 2014 Regulatory action and news
Droxidopa approved for neurogenic orthostatic hypotension Uni ted S ta tes o f Amer ica – The Food and Drug Administration (FDA) has approved droxidopa (Northera®) capsules for the treatment of neurogenic orthostatic hypotension, a rare, chronic and often debilitating drop in blood pressure upon standing that is associated with Parkinson’s disease, multiple-system atrophy, and pure autonomic failure. Droxidopa was approved under the FDA’s accelerated approval programme and received orphan-product designation.
The product carries a warning about the risk of increased blood pressure while lying down (supine hypertension), a common problem that affects people with primary autonomic failure and can cause stroke. Patients must sleep with their upper body elevated. Supine blood pressure should be monitored before and during treatment. Reference: FDA News Release, 18 February
2014.
Bedaquiline recommended for approval to treat multidrug-resistant tuberculosisEuropean Un ion – The European Medicines Agency (EMA)’s Committee for Medicinal Products for Human Use (CHMP) has recommended granting a conditional marketing authorization for bedaquiline (Sirturo®) for use in combination therapy for pulmonary multidrug-resistant tuberculosis in adults when an effective treatment regimen cannot otherwise be composed for reasons of resistance or tolerability.
In recent years, the burden of tuberculosis resistant to first-line therapy has increased rapidly in the absence of new treatment options. Bedaquiline is
the first representative of a new class of medicines against mycobacteria. It has received the third positive opinion recently granted by the CHMP for a medicine to treat of multidrug-resistant tuberculosis, after the November 2013 recommendations for delamanid (also for a conditional approval) and para-aminosalicylic acid. Reference: EMA Press Release,
20 December 2013.
Metreleptin approved to treat rare metabolic diseaseUni ted S ta tes o f Amer ica – The Food and Drug Administration (FDA) has approved metreleptin for injection (Myalept®) as replacement therapy to treat the complications of leptin deficiency in patients with generalized lipodystrophy of both the congenital and the acquired type. These complications include severe insulin resistance at a young age, diabetes mellitus that is difficult to control, and hypertriglyceridaemia.
Because of the risk of development of anti-drug antibodies, as well as the risk of T-cell lymphoma in patients with acquired generalized lipodystrophy, metreleptin is available only through a designated treatment programme.
Metreleptin is contraindicated in patients with general obesity. It is not approved for use in patients with HIV-related lipodystrophy or those with metabolic disease, including diabetes mellitus and hypertriglyceridemia, without concurrent evidence of generalized lipodystrophy.Reference: FDA News release, 25 February
2014.

32
WHO Drug Information Vol. 28 No. 1, 2014
32
Recent publications, information and events
World malaria report: financing needed to sustain major progressThe World Health Organization (WHO) has released its World malaria report 2013. The report shows major progress in the fight against malaria and calls for sustained financing to preserve past gains.
Global efforts to control and eliminate malaria have saved an estimated 3.3 million lives between 2000 and 2012. Despite an increase in the global population at risk, new malaria cases have decreased by 29% and malaria deaths by 45% globally in that period. Access to WHO-recommended artemisinin-based combination therapies (ACTs) has risen more than fourfold from 2006 to 2012. Access to diagnostic testing has also increased in recent years.
However, an estimated 3.4 billion people remain at risk of malaria, with around 80% of malaria cases occurring in Africa. Less than half of the population at risk had access to an insecticide-treated bed net in 2013, and millions of people stilllack access to diagnosis and quality-assured treatment. The roll-out of preventive therapies – recommended for infants, children under 5 and pregnant women – has also been slow in recent years.
Malaria prevention and treatment requires continued financing. While the total international and domestic funding for malaria control has increased tremendously since 2000 to reach US$ 2.5 billion in 2012, it still falls short of the US$ 5.1 billion needed each year to achieve universal access to prevention and treatment interventions.
Adequate and predictable funding is also needed to combat emerging parasite resistance to artemisinin, the core component of ACTs, and mosquito resistance to insecticides. WHO is currently developing a global technical strategy for malaria control and elimination for the 2016-2025 period.Reference: World Health Organization.
World malaria report 2013. Geneva, Switzerland: WHO, 2013.
WHO Prequalification: A quiet revolution in global public healthA recently published article looks at the history of the WHO Prequalification of Medicines Programme, created in 2001. The Programme has improved the quality of life-saving medicines used today by millions of people in low- and middle-income countries. Although verifying medicines quality may appear a non-controversial activity, the Programme was initially criticized harshly for helping commercial generic producers gain access to markets until then dominated by originator companies.
Today the Programme is respected globally for its solid and transparent standards that come out of an international consensus process with WHO Member States, and for its close collaboration with national drug regulatory agencies in both developing and wealthy countries. The article terms it “the strongest mechanism currently in place to create sustainable medicines regulatory systems in low- and middle-income countries”, and concludes

33
WHO Drug Information Vol. 28 No. 1, 2014
33
Recent publications, information and events
that global health donors would be well advised to create a sustainable funding base for the continuation of its work, which is crucial to assure the quality of key medicines purchased with their finance.Reference: ‘t Hoen EFM, Hogerzeil HV,
Quick JD, Sillo HB. A quiet revolution in global public health: The World Health Organization’s Prequalification of Medicines Programme. Journal of Public Health Policy 2014; doi: 10.1057/jphp.2013.53.
AIDS drugs for all: how global advocacy transformed pharmaceutical marketsA recently published book looks back on how the global AIDS treatment advocacy campaign transformed pharmaceutical markets the history towards universal access to ARV treatment for all people living with AIDS. It describes how a product market was developed and altered to provide access to quality-assured, affordable medicines to treat HIV for all who need them.
The book acknowledges the important role of the WHO Prequalification of Medicines Programme in assuring the quality of affordable generic products. WHO prequalification has proved to be one of the crucial enablers in an unparalleled social and political movement to fulfil the entitlement of every person to access to treatment as a human right. Reference: Kapstein EB, Busby JW. AIDS
Drugs for All. Social Movements and Market Transformations. New York, USA: Cambridge University Press; 2013.
Who are the originators of innovative medicines in the EU?Over 40% of innovative medicines and over 70% of new medicines for the
treatment of rare diseases recommended for marketing authorisation in the European Union (EU) between 2010 and 2012 originated from small or medium-sized enterprises (SMEs), academia, public bodies and public-private partnerships, according to an article authored by staff members of the European Medicines Agency (EMA). On the other hand, SMEs are underrepresented as marketing-authorization holders while the other types of organizations mentioned above are not involved at the stage of marketing applications at all.
Acknowledging the role of SMEs as a motor of innovation for medicines, the EMA has a programme in place to support SMEs through all stages of medicine development. New platforms are also being set up that will facilitate the engagement with the academic world, further supporting the translation of innovation into successful developments in the interest of patients.Reference: Lincker H, Ziogas C, Carr M,
Porta N, Eichler HG. Regulatory watch: Where do new medicines originate from in the EU? Nature Reviews Drug Discovery 13, 92–93 (2014) doi:10.1038/nrd4232.
Medicines Patent Pool and Bristol-Myers Squibb sign agreementThe Medicines Patent Pool (MPP) and biopharmaceutical company Bristol-Myers Squibb have signed a licensing agreement to increase access to a key HIV medicine, atazanavir, in 110 developing countries. This is the MPP’s first agreement covering a World Health Organization (WHO)-preferred second-line therapy. WHO estimates there will be over 1 million people on second-line treatment by 2016, and many more will need access to these therapies.

WHO Drug Information Vol. 28 No. 1, 2014
34
Recent publications, information and events
34
Previous agreements with Gilead Sciences and ViiV Healthcare have expanded access to WHO-preferred first-line treatments for adults and children.
The Medicines Patent Pool works by creating a pool of relevant patents for licensing to generic manufacturers and other producers, facilitating the generic competition that brings down prices and can help to stimulate innovation. Medicines Patent Pool licensees are required to submit their products to either the WHO Prequalification Programme or to a stringent regulatory authority for evaluation. References:
MPP and Bristol-Myers Squibb Sign Agreement to Further Expand Access to a Key HIV Medicine. 12 December 2013. Licences in the MPP, at http://www.medicinespatentpool.org/licensing/current-licences/
Report calls for cooperation to strengthen post-market surveillance systemsThe Safety Surveillance Working Group, a collaborative effort initiated by the Bill &
Melinda Gates Foundation, has published a report that assesses the medicines and vaccines product pipeline and resulting demands on the regulatory systems in low- and middle-income countries. Based on that data analysis, the report outlines a strategy and implementation plan to strengthen post-market safety in these countries. The authors call for a coordinated international effort of policy makers, regulators, industry and health professionals to build sustainable safety surveillance systems. They point to the importance of cooperation and of leveraging existing infrastructure such as that offered by the WHO Programme for International Drug Monitoring, the WHO Global Vaccine Safety Initiative, the Brighton Collaboration and the CIOMS/WHO Working Group on Vaccine Pharmacovigilance.Reference: Bollyky TJ, Stergachis A. A
Report of the Safety and Surveillance Working Group. Seattle, USA: Bill & Melinda Gates Foundation; 2014.
Events
Annual ATC/DDD Methodology courseThe WHO Collaborating Centre for Drug Statistics Methodology announces its next annual course in ATC/DDD, to be held in Oslo, Norway, on 5-6 June 2014. The course is open to all interested parties. Basic knowledge in common medical terminology is recommended.
The Anatomical Therapeutic Chemical (ATC) classification system, together with the Defined Daily Dose (DDD) as a technical unit of measurement, provides an effective tool to present and compare drug consumption statistics at international and other levels in drug utilization research. Reference: WHO Collaborating Centre for
Drug Statistics Methodology [website] at www.whocc.no/courses/

35
WHO Drug Information Vol. 28 No. 1, 2014
35
Consultation documents
The International Pharmacopoeia
Atazanaviri sulfas Atazanavir sulfate
This is a draft proposal for The International Pharmacopoeia (Working document QAS/13.566, December 2013).
The working document with line numbers is available for comment at www.who.int/medicines/areas/quality_safety/quality_assurance/projects/en/. Please address any comments to: World Health Organization, Quality Assurance and Safety: Medicines, Dr Herbert Schmidt, 1211 Geneva 27, Switzerland; fax: +41 22 791 4730; email: [email protected].
Molecular formula. C38H52N6O7•H2SO4
Relative molecular mass. 802.9
Chemical name. (3S,8S,9S,12S)-3,12-Bis(1,1-dimethylethyl)-8-hydroxy-4,11-dioxo-9-(phenylmethyl)-6-[[4-(2-pyridinyl) phenyl]methyl]-2,5,6,10,13-pentaazatetradecanedioic acid dimethyl ester, sulfate (1:1).
Description. A white or almost white powder.
Solubility. Freely soluble in methanol, practically insoluble in water.
Category. Antiretroviral (protease inhibitor).
Storage. Atazanavir sulfate should be kept in a tightly closed container at a temperature not exceeding 30°C.
Additional information. Atazanavir sulfate is slightly hygroscopic.
Requirements. Atazanavir sulfate contains not less than 98.0% and not more than 102.0% of C38H52N6O7•H2SO4 calculated on the dried basis.
Identity tests
Either test A and D, or test B, C and D should be performed.
A. Carry out the examination as described under 1.7 Spectrophotometry in the infrared region. The infrared absorption spectrum is concordant with the spectrum obtained from atazanavir sulfate RS or with the reference spectrum of atazanavir sulfate.

36
WHO Drug Information Vol. 28 No. 1, 2014
36
B. Carry out test B.1, or where UV detection is not available, test B.2.
B.1 Carry out the test as described under 1.14.1 Thin-layer chromatography, using silica gel R6 as the coating substance and a mixture of 9.5 volumes of dichloromethane R and 0.5 volumes of 2-propanol R as the mobile phase. Apply separately to the plate 10 μl of each of 2 solutions in methanol R containing (A) 1 mg of the test substance per ml and (B) 1.0 mg of atazanavir sulfate RS per ml. After removing the plate from the chromatographic chamber allow it to dry exhaustively in air or in a current of air.
Examine the chromatogram in ultraviolet light (254 nm). The principal spot obtained with solution (A) corresponds in position, appearance and intensity to that obtained with solution (B).
B.2 Carry out the test as described under 1.14.1 Thin-layer chromatography, using the conditions described under test B.1, but using a plate containing silica gel R5 as the coating substance.
Spray the plate with potassium permanganate, basic (~5 g/l) TS. Examine the chromatogram in daylight. The principal spot obtained with solution (A) corresponds in position, appearance and intensity to that obtained with solution (B).
C. The absorption spectrum of a 10 µg/ml solution in methanol R, when observed between 230 nm and 340 nm, exhibits two maxima at about 250 nm and 280 nm, respectively.
A 20 mg/ml solution yields Reaction A described under 2.1 General identification tests as characteristic of sulfates.
Heavy metals. Use 1.0 g for the preparation of the test solution as described under 2.2.3 Limit test for heavy metals, Procedure 3; determine the heavy metals content according to method A; not more than 20 µg/g.
Sulfated ash (2.3). Not more than 1.0 mg/g.
Loss on drying. Dry for 3 hours at 105 °C; it loses not more than 10.0 mg/g.
pH value. Apparent pH of a 10 mg/ml solution in carbon-dioxide-free water R and acetonitrile R (50:50, v/v), 2.0–2.5.1
Related substances. Carry out the test as described under 1.14.4 High–performance liquid chromatography, using a column (150 mm x 4.6 mm) packed with end-capped base deactivated particles of silica gel the surface of which has been modified with chemically bonded octylsilyl groups (5 μm).2 Use the following conditions for gradient elution:
Mobile phase A: 0.02 M phosphate buffer pH 3.5.
Mobile phase B: Acetonitrile R.
Prepare the phosphate buffer pH 3.5 by dissolving 2.72 g of anhydrous potassium dihydrogen phosphate R in 800 ml of water R, adjust the pH to 3.5 by adding phosphoric acid (~105 g/l) TS and dilute to 1000 ml with water R.
1 Value subject to confirmation.2 An Inertsil C8 column has been found suitable.

37
WHO Drug Information Vol. 28 No. 1, 2014 Consultation documents
37
Time (min)
Mobile phase A (% v/v)
Mobile phase B (% v/v)
Comments
0–2 70 30 Isocratic2–10 70–60 30–40 Linear gradient10–30 60–50 40–50 Linear gradient30–45 50–30 50–70 Linear gradient45–50 30 70 Isocratic50–52 30–70 70–30 Linear gradient52–60 70 30 Isocratic
Prepare the following solutions using as diluent a mixture of equal volumes of water R and acetonitrile R. For solution (1) use 1 mg of the test substance per ml. For solution (2) dilute a suitable volume of solution (1) to obtain a concentration equivalent to 5 μg of Atazanavir sulfate per ml. For solution (3) mix 1 ml of solution (1) with 4.5 ml of water R and 0.5 ml of sodium hydroxide (10 g/l) TS and heat the mixture in a water-bath at 85°C for 15 min.
Operate with a flow rate of 1.0 ml per minute. As a detector use an ultraviolet spectrophotometer set at a wavelength of 250 nm. Maintain the column at a temperature of 30°C.
Inject 20 µl of solution (3). The test is not valid unless the resolution between the peak due to atazanavir (retention time about 22 minutes) and the peak with a relative retention of about 1.2 is at least 4.
Inject alternatively 20 µl each of solutions (1) and (2).
In the chromatograms obtained with test solution (1), the area of any peak, other than the principal peak, is not greater than the area of the principal peak in the chromatogram obtained with solution (2) (0.5%). The sum of the areas of all peaks, other than the principal peak, is not greater than twice the area of the principal peak in the chromatogram obtained with solution (2) (1.0%). Disregard any peak with an area less than 0.1 times the area of the principal peak in the chromatogram obtained with solution (2) (0.05%).
Assay
Dissolve 0.150 g, accurately weighed, in 30 ml of methanol R and sonicate for 10 minutes. Then add 30 ml of water and titrate with sodium hydroxide (0.1 mol/l), carbonate-free, VS. Determine the end-point potentiometrically as described under 2.6 Non-aqueous titration Method A. Each ml of sodium hydroxide (0.1 mol/l) VS is equivalent to 40.145 mg of C38H52N6O7•H2SO4.
***

WHO Drug Information Vol. 28 No. 1, 2014
38
Consultation documents
38
Atazanaviri capsulae Atazanavir capsules
This is a draft proposal for The International Pharmacopoeia (Working document QAS/13.567, December 2013).
The working document with line numbers is available for comment at www.who.int/medicines/areas/quality_safety/quality_assurance/projects/en/. Please address any comments to: World Health Organization, Quality Assurance and Safety: Medicines, Dr Herbert Schmidt, 1211 Geneva 27, Switzerland; fax: +41 22 791 4730; email: [email protected].
Category. Antiretroviral (Protease Inhibitor).
Storage. Atazanavir sulfate capsules should be kept in a tightly closed container at a temperature not exceeding 30°C.
Additional information. Strength in the current WHO Model list of essential medicines: 100 mg, 150 mg, 300 mg of atazanavir (as sulfate). Strength in the current WHO Model List of essential medicines for children: 100 mg, 150 mg, 300 mg of atazanavir (as sulfate).
Each mg of atazanavir (C38H52N6O7) is equivalent to 1.139 mg of atazanavir sulfate (C38H52N6O7•H2SO4).
Requirements. Comply with the monograph for Capsules.
Definition. Atazanavir capsules contain atazanavir sulfate. They contain not less than 90.0% and not more than 110.0% of the amount of atazanavir, C38H52N6O7, stated on the label.
Identity tests
A. Carry out test A.1, or where UV detection is not available, test A.2.
A.1 Carry out the test as described under 1.14.1 Thin-layer chromatography, using silica gel R6 as the coating substance and a mixture of 9.5 volumes of dichloromethane R and 0.5 volumes of 2-propanol R as the mobile phase. Apply separately to the plate 10 µl of each of the following 2 solutions in methanol R. For solution (A) disperse a quantity of the contents of the capsules containing about 20 mg of atazanavir in 10 ml of methanol R, sonicate for 10 minutes, allow to cool to room temperature, dilute to 20 ml, filter and use the filtrate. For solution (B) use 1.1 mg of atazanavir sulfate RS per ml.
After removing the plate from the chromatographic chamber, allow it to dry exhaustively in a current of air. Examine the chromatogram in ultraviolet light (254 nm).
The principal spot obtained with solution (A) corresponds in position, appearance, and intensity to that obtained with solution (B).
A.2 Carry out the test as described under 1.14.1 Thin-layer chromatography, using the conditions described above under test A.1 but using a plate containing silica gel R5 as the coating substance. Spray with potassium permanganate, basic (~5 g/l) TS. Examine the chromatogram in daylight.
The principal spot obtained with solution (A) corresponds in position, appearance and intensity with that obtained with solution (B).
B. Disperse a quantity of the contents of the capsules containing about 20 mg of atazanavir in 10 ml of methanol R, sonicate for 10 min, allow to cool to room temperature, dilute to 20 ml and filter. Dilute 1 ml of the filtrate to 100 ml with methanol R. The absorption

39
WHO Drug Information Vol. 28 No. 1, 2014 Consultation documents
39
spectrum (1.6) of the resulting solution, when observed between 230 and 340 nm, exhibits two maxima at about 250 nm and 280 nm, respectively.
C. To a quantity of the contents of the capsules equivalent to 0.2 g of atazanavir add 10 ml of a mixture of 1 volume of water R and 1 volume of acetonitrile R, shake and filter. The filtrate yields Reaction A described under 2.1 General identification tests as characteristic of sulfates.
Dissolution. Carry out the test as described under 5.5 Dissolution test for solid oral dosage forms, using as the dissolution medium, 900 ml of dissolution buffer pH 2.5 TS, and rotating the paddle at 50 revolutions per minute. At 45 minutes withdraw a sample of 10 ml of the medium through an in-line filter. Allow the filtered sample to cool to room temperature. Measure the absorbance (1.6) of a 1 cm layer of the resulting solution, suitably diluted if necessary, at the maximum at about 250 nm. Determine the content of atazanavir (C38H52N6O7) in the medium from the absorbance obtained from a solution of known concentration of atazanavir sulfate RS. The amount in solution for each capsule is not less than 75% (Q) of the amount stated on the label.
Related substances. Carry out the test as described under 1.14.4 High–performance liquid chromatography, using a stainless steel column (150 mm x 4.6 mm) packed with end-capped base deactivated particles of silica gel the surface of which has been modified with chemically bonded octylsilyl groups (5 μm).1 Use the following conditions for gradient elution:
Mobile phase A: 0.02 M phosphate buffer pH 3.5.
Mobile phase B: Acetonitrile R.
Prepare the phosphate buffer pH 3.5 by dissolving 2.72 g of anhydrous potassium dihydrogen phosphate R in 800 ml of water R, adjust the pH to 3.5 by adding phosphoric acid (~105 g/l) and dilute to 1000 ml with water R.
Time (min)
Mobile phase A (% v/v)
Mobile phase B (% v/v)
Comments
0–2 70 30 Isocratic2 –10 70–60 30–40 Linear gradient10–30 60–50 40–50 Linear gradient30–45 50–30 50–70 Linear gradient45–50 30 70 Isocratic50–52 30–70 70–30 Linear gradient52–60 70 30 Isocratic
Prepare the following solutions using as diluent a mixture of equal volumes of acetonitrile R and water R. For solution (1) weigh and mix the contents of 20 capsules. Transfer a quantity of the mixed contents equivalent to 20 mg of atazanavir into a 20 ml volumetric flask. Add about 10 ml of the diluent, sonicate for 10 minutes, allow to cool to room temperature, make up to volume and filter. For solution (2) dilute a suitable volume of solution (1) with the diluent to obtain a concentration of 10 μg of atazanavir per ml. For solution (3) mix 1 ml of solution (1) with 4.5 ml of water R and 0.5 ml of sodium hydroxide (10 g/l) TS and heat the mixture in a water bath at 85°C for 15 min.
Operate with a flow rate of 1.0 ml per minute. As a detector use an ultraviolet spectrophotometer set at a wavelength of 250 nm. Maintain the column at a temperature of 30°C.
1 An Inertsil C8 column has been found suitable.

WHO Drug Information Vol. 28 No. 1, 2014
40
Consultation documents
40
Inject 20 µl of solution (3). The test is not valid unless the resolution between the peak due to atazanavir (retention time about 22 minutes) and the peak with a relative retention of about 1.2 is at least 4.
Inject alternatively 20 µl each of solutions (1) and (2).
In the chromatograms obtained with test solution (1), the area of any peak, other than the principal peak, is not greater than the area of the principal peak in the chromatogram obtained with solution (2) (1.0%). The sum of the areas of all peaks, other than the principal peak, is not greater than twice the area of the principal peak in the chromatogram obtained with reference solution (2) (2.0%). Disregard any peak with an area less than 0.05 times the area of the principal peak in the chromatogram obtained with solution (2) (0.05%).
Assay
Either test A or test B may be applied.
Carry out the test as described under 1.14.4 High–performance liquid chromatography, using a stainless steel column (150 mm x 4.6 mm) packed with end-capped base deactivated particles of silica gel the surface of which has been modified with chemically bonded octylsilyl groups (5 μm).2
As the mobile phase, use a solution prepared as follows: 60 volumes of acetonitrile R and 40 volumes of 0.02 M phosphate buffer pH 3.5. Prepare the phosphate buffer pH 3.5 by dissolving 2.72 g of anhydrous potassium dihydrogen phosphate R in 800 ml of water R, adjust the pH to 3.5 by adding phosphoric acid (~105 g/l) TS and dilute to 1000 ml with water R.
Prepare the following solutions using as diluent a mixture of equal volumes of acetonitrile R and water R. For solution (1) weigh and mix the contents of 20 capsules. Transfer a quantity equivalent to 20.0 mg of atazanavir, accurately weighed, into a 20 ml volumetric flask. Add about 10 ml of the diluent, sonicate for about 10 minutes, allow to cool to room temperature and make up to volume. Filter a portion of this solution, discarding the first few ml. Dilute 1.0 ml of the filtrate to 10.0 ml with the diluent. For solution (2) use 0.11 mg of atazanavir sulfate RS per ml.
Operate with a flow rate of 1.0 ml per minute. As a detector use a ultraviolet spectrophotometer set at a wavelength of 250 nm. Maintain the column at a temperature of 30°C.
Inject alternatively 20 µl each of solutions (1) and (2) and record the chromatograms for 1.5 times the retention time of atazanavir.
Measure the areas of the peak responses obtained in the chromatograms from solutions (1) and (2) and calculate the percentage content of atazanavir, (C38H52N6O7), using the declared content of C38H52N6O7 in atazanavir sulfate RS.
Weigh and mix the contents of 20 capsules. Transfer a quantity equivalent to 20 mg of atazanavir, accurately weighed, to a 20 ml volumetric flask. Add about 10 ml of methanol R, sonicate for about 10 minutes, allow to cool to room temperature and make up to volume. Filter a portion of this solution through a 0.45 µm filter, discarding the first few ml of the filtrate. Dilute 1.0 ml of the filtrate to 10.0 ml with methanol R. Measure the absorbance of this solution in a 1 cm layer at the maximum at about 250 nm against a solvent cell containing methanol R. Calculate the content of C38H52N6O7, using an absorptivity value of 15.9 (A 1 cm 1% = 159).3
***
2 An Inertsil C8 column has been found suitable.3 Value subject to confirmation.

41
WHO Drug Information Vol. 28 No. 1, 2014 Consultation documents
41
Implementation of the revised general monograph on parenteral preparations in The International Pharmacopoeia:
Limits for the test for bacterial endotoxins (3.4)This is a revised draft proposal for The International Pharmacopoeia (Working document QAS/13.539/Rev.1, January 2014). The working document with line numbers is available for comment at www.who.int/medicines/areas/quality_safety/quality_assurance/projects/en/. Please address any comments to: World Health Organization, Quality Assurance and Safety: Medicines, Dr Herbert Schmidt, 1211 Geneva 27, Switzerland; fax: +41 22 791 4730; email: [email protected].
Limits for bacterial endotoxins in monographs on parenteral preparations During the forty-seventh meeting of the Expert Committee on Specifications for Pharmaceutical Preparations in October 2012 a revision of the general monograph on parenteral preparations was adopted.
One of the major changes to the monograph on parenteral preparations was the required compliance of all parenteral preparations with the test for bacterial endotoxins (or, where justified, pyrogens). As a consequence individual monographs on injectable dosage forms in The International Pharmacopoeia (Ph.Int.) were investigated with a view to add a limit for bacterial endotoxins to each monograph that currently does not include such a requirement. The endotoxin limits shown in Table 1 are proposed for inclusion in The International Pharmacopoeia. The limits are determined following the approaches listed in Annex 1.
Table 1. Proposed limits for bacterial endotoxins in Ph.Int. monographs on parenteral preparations lacking such specification
Ph.Int. monographs on parenteral preparations currently lacking limits for the bacterial endotoxins test
Proposed limits for the bacterial endotoxins test 1
Artemether injection Less than 1.56 IU of endotoxin per mg Artemether
Artemotil injection Less than 1.04 IU of endotoxin per mg Artemotil
Ephedrine sulfate injection Less than 1.7 IU of endotoxin per mg Ephedrine sulfate
Ergometrine hydrogen maleate injection Less than 700 IU of endotoxin per mg of ergometrine hydrogen maleate
Melarsoprol injection Less than 1.39 IU of endotoxin per mg Melarsoprol
Magnesium sulfate injection Less than 0.18 IU of endotoxin per mg magnesium sulfate heptahydrate
Oxytocin injection Less than 0.5 IU of endotoxin per IU of Oxytocin
Pentamidine isetionate powder for injections2
Less than 1.25 IU of endotoxin per mg Pentamidine isetionate
Prednisolone sodium phosphate injection3
Less than 4.09 IU of endotoxin per mg Prednisolone
Quinine dihydrochloride injection Less than 1.0 IU of endotoxin per mg Quinine dihydrochlorideZidovudine intravenous infusion Less than 1.0 IU of endotoxin per mg Zidovudine 1 The complete phrase to be used in The International Pharmacopoeia should be: “Bacterial
Endotoxins. Carry out the test as described under 3.4 Test for bacterial endotoxins; contains … (phrase of the table to be added).”
2 Title of the monograph to be changed to: Pentamidine isetionate for injection. 3 Title of the monograph to be changed to: Prednisolone phosphate injection.

WHO Drug Information Vol. 28 No. 1, 2014
42
Consultation documents
42
Further changes to The International Pharmacopoeia following the implementation of the revised general monograph on parenteral preparations
The following additional changes to The International Pharmacopoeia are proposed:
In the new general monograph on Parenteral preparations the statement is made that:“For powders and concentrates for injections and intravenous infusions, the amount of the preparation to be tested and the nature and volume of the liquid in which it is to be dissolved, suspended or diluted is specified in the individual monograph.”
It is proposed to delete this sentence since the preparation of the sample solution is described in Chapter 3.4 Test for bacterial endotoxins. The text requires that samples should be dissolved or diluted in aqueous solutions so that the final solutions do not exceed the maximum valid dilution (MVD).
In the monograph on Metronidazole injection the following provision for the test for bacterial endotoxins is made:
“Carry out the test as described under 3.4 Test for bacterial endotoxins. Dilute the injection, if necessary, with water LAL to give a solution containing 5 mg per ml (solution A). Solution A contains not more than 3.5 IU of endotoxin per ml. Carry out the test using the maximum valid dilution of solution A calculated from the declared sensitivity of the lysate used in the test.”
Again, details of the sample solution preparation should be deleted and the sentence should be changed to read:
“Carry out the test as described under 3.4 Test for bacterial endotoxins; contains not more than 3.5 IU of endotoxin per ml.”
In general, two phrases are used to specify endotoxin limits in The International Pharmacopoeia:
“… not more that x IU of endotoxin per mg/ml …” ; and “… not more that x IU of endotoxin RS per mg/ml …”.
All expressions using “IU of endotoxin RS” should be changed to “IU of endotoxin”. Chapter 3.4 Test for bacterial endotoxins already requires the use of the WHO International Standard for endotoxin when performing the test (or an endotoxin reference standard that has been calibrated against this standard; see section Preparation of standard endotoxin stock solution).
Annex 1
Calculation of bacterial endotoxin limits
The endotoxin limits proposed in Table 1 are calculated using the following approaches:
For the monograph on Ergometrine hydrogen maleate injection, the limit given in The International Pharmacopoeia for the active pharmaceutical ingredient (for parenteral use) was applied.
For the monographs on Ephedrine sulfate injection, Magnesium sulfate injection, Oxytocin injection, Prednisolone sodium phosphate injection and Zidovudine intravenous infusion, limits given in monographs of other pharmacopoeias were taken over.
For the monographs on Artemether injection, Artemotil injection, Melarsoprol injection, Pentamidine isetionate powder for injections and Quinine dihydrochloride injection, the endotoxin limits were calculated using recommendations given in Chapter 3.4 Test for bacterial endotoxins.

43
WHO Drug Information Vol. 28 No. 1, 2014 Consultation documents
43
The endotoxin limit for parenteral preparations, defined on the basis of dose, is equal to:
K = threshold pyrogenic dose of endotoxin per kilogram of body mass (i.e. 5.0 IU per kg body weight for any route of administration other than intrathecal; 2.5 IU per kg body weight for intravenous route of radiopharmaceuticals; 0.2 IU per kg body weight for intrathecal route).M = maximum recommended bolus dose of product per kilogram of body mass. (When the product is to be injected at frequent intervals or infused continuously, M is the maximum total dose administered in a single hour period.)
Table 2 lists data used in the calculation of the proposed bacterial endotoxin limits.
Table 2. Data used in the calculation of bacterial endotoxin limitsPh.Int. monographs lacking endotoxin limit
Endotoxin limits in pharmacopoeias
Information on dosage and route of application
K M
Artemether injection
“Intramuscular injection for adults, artesunate 2.4 mg/kg BW IV or IM given on admission (time = 0), then at 12 h and 24 h, then once a day is the recommended treatment. Artemether, or quinine, is an acceptable alternative if parenteral artesunate is not available: artemether 3.2 mg/kg BW IM given on admission then 1.6 mg/kg BW per day. ” 1
5 IU/kg
3.2 mg/kg
Artemotil injection
“Artecef® 150 must only be applied via the intramuscular route. Medical treatment consists of a 3-day course. The initial dose consists of an injection of 4.8 mg artemotil per kg body weight evenly divided over both anterior thighs. The follow-up doses consist of 1.6 mg per kg body weight after 6, 24, 48 and 72 hours in alternating thighs.” 2
5 IU/kg
4.8 mg/kg
Ephedrine sulfate injection
Ephedrine sulfate injection (USP 36): NMT 1.7 USP Endotoxin Unit per mg of ephedrine sulfate
Ergometrine hydogen maleate injection
Ergometrine hydrogen maleate (Ph.Int. 4.3): NMT 700.0 IU of endotoxin RS per mg substance for parenteral use
Melarsoprol injection
“Treatment of T. brucei rhodesiense and T. brucei gambiense with meningoencephalitic involvement [ ], by slow intravenous injection, ADULT and CHILD, dose gradually increased from 1.2 mg/kg to maximum of 3.6 mg/kg daily in courses of 3–4 days with intervals of 7–10 days between courses; [ ].” 3 (page 209)
5 IU/kg
3.6 mg/kg
Continued/

WHO Drug Information Vol. 28 No. 1, 2014
44
Consultation documents
44
Ph.Int. monographs lacking endotoxin limit
Endotoxin limits in pharmacopoeias
Information on dosage and route of application
K M
Magnesium sulfate injection
Magnesium sulfate injection (USP 36): NMT 0.09 USP Endotoxin Unit per mg of magnesium sulfate
Oxytocin injection
Oxytocin Injection (USP 36): NMT 35.7 Endotoxin Units per USP Oxytocin UnitOxytocin (EP 7.8): less than 300 IU per mg Oxytocin, corresponding to less than 0.5 IU per IU of Oxytocin
Pentamidine isetionate powder for injections
“Visceral leishmaniasis (unresponsive to, or intolerant of, antimonial compounds), by deep intramuscular injection or by intravenous infusion, ADULT and CHILD, 4 mg/kg 3 times a week for 5–25 weeks or longer, until 2 consecutive splenic aspirates taken 14 days apart are negative.”3 (page 186)
5 IU/kg
4 mg/kg
Prednisolone sodium phosphate injection
Prednisolone sodium phosphate injection (USP 36): NMT 5.0 USP Endotoxin Units per mg of prednisolone phosphate
Quinine dihydro-chloride injection
“Treatment of multidrug-resistant P. falciparum malaria (in patients unable to take quinine by mouth), by slow intravenous infusion (over 4 hours), ADULT, initially 20 mg/kg (quinine dihydrochloride), followed by 10 mg/kg (quinine dihydrochloride) every 8 hours; CHILD, initially 20 mg/kg (quinine dihydrochloride), followed by 10 mg/kg (quinine dihydrochloride) every 12 hours; initial dose should be halved in patients who have received quinine, quinidine or mefloquine during the previous 12–24 hours.” 3 (page 198)
5 IU/kg
5 mg/kg
Zidovudine intravenous infusion
Zidovudine injection (USP 36): NMT 1.0 USP Endotoxin Unit per mg of zidovudine
1 Guidelines for the treatment of malaria. 2nd Edition. Geneva: World Health Organization; 2010: p. 41.2 Product Information Leaflet, Artecef BV 150 mg/ml injection. See WHO Prequalification website at
www.who.int/prequal – Dossier assessment – WHO Public Inspection Reports (WHOPARs) for MA027 and MA028.
3 Information taken from the WHO Model Formulary 2008. Geneva: World Health Organization; 2009.
***

45
WHO Drug Information Vol. 28 No. 1, 2014 Consultation documents
45
Revision of general monograph: SuppositoriesThis is a draft proposal for The International Pharmacopoeia (Working document QAS/14.571, February 2014).
The working document with line numbers is available for comment at www.who.int/medicines/areas/quality_safety/quality_assurance/projects/en/. Please address any comments to: World Health Organization, Quality Assurance and Safety: Medicines, Dr Herbert Schmidt, 1211 Geneva 27, Switzerland; fax: +41 22 791 4730; email: [email protected].
[Note from the Secretariat. The proposed general monograph is part of the review of general monographs endorsed by the Expert Committee at its 42nd meeting. It is proposed to replace the current general monograph on suppositories with a general monograph including solid, liquid and semi-solid dosage forms intended for rectal application.]
RECTAL PREPARATIONS
Definition
Rectal preparations are liquid, semi-solid or solid preparations that may contain one or more active ingredients. They are intended for rectal application in order to obtain a systemic or local effect.
Rectal preparations may require the use of excipients of various types. Any excipient must be proven through product development studies not to adversely affect the stability of the final product, nor the availability of the active ingredient(s) at the site of action; incompatibility between any of the components of the dosage form should be avoided.
The different categories of rectal preparations include:
• suppositories;• rectal capsules;• rectal solutions, emulsions and suspensions;• powders and tablets for rectal solutions and suspensions;• semi-solid rectal preparations.
Manufacture
The following information is intended to provide broad guidelines concerning main steps to be followed during production.
Manufacturing and filling processes for rectal preparations should meet the requirements of good manufacturing practices (GMP).
During development, the effectiveness of any antimicrobial preservative present in the preparation shall be demonstrated to the satisfaction of the relevant regulatory authority.
During development it must be demonstrated that the nominal contents can be withdrawn from the container of liquid and semi-solid rectal preparations presented in single-dose containers.
In the manufacture, packaging, storage and distribution of rectal preparations, suitable measures are taken to ensure their microbial quality; recommendations on this aspect are

WHO Drug Information Vol. 28 No. 1, 2014
46
Consultation documents
46
provided in the chapter Microbial examination of non-sterile products: acceptance criteria for pharmaceutical preparations, published in the Supplementary information section.
In the manufacture of rectal preparations containing dispersed particles, measures are taken to ensure a suitable and controlled particle size.
Throughout manufacturing, certain procedures should be validated and monitored by carrying out appropriate in-process controls. These should be designed to guarantee the effectiveness of each stage of production.
Labelling
Every rectal preparation must comply with the labelling requirements established under GMP.
The label should include:
1. name of the pharmaceutical product;2. name(s) of the active ingredient(s); International Nonproprietary Names (INN) should be
used whenever possible;3. amount of active ingredient(s) in a dose unit and the number of dose units in the container
or the amount of active ingredient(s) in suitable dose volume and the volume of the container;
4. where applicable, the name of any added antimicrobial agent;5. batch (lot) number assigned by the manufacturer;6. expiry date and, when required, the date of manufacture;7. any special storage conditions or handling precautions that may be necessary;8. directions for use, warnings and precautions that may be necessary; 9. name and address of the manufacturer or the person responsible for placing the product on
the market.
REQUIREMENTS FOR SPECIFIC TYPES OF RECTAL PREPARATIONS
Suppositories
Definition
Suppositories are solid single-dose preparations intended for rectal application. They are prepared by moulding or compression. The shape, volume and consistency of suppositories are suitable for rectal application.
Suppositories contain one or more active ingredients dispersed or dissolved in a suitable basis that may be soluble or dispersible in water or may melt at body temperature. When prepared by moulding, suppository bases such as magrogols, gelatinous mixtures consisting of, for example, gelatin, water and glycerol, hydrogenated vegetable oils, hard fat or cocoa butter are usually employed.
Excipients such as diluents, adsorbents, surface-active agents preferably of nonionic type, lubricants, antimicrobial preservatives and colouring matter authorized by the appropriate national or regional authority, may be added when necessary.

47
WHO Drug Information Vol. 28 No. 1, 2014 Consultation documents
47
Manufacture
It is common to use a suppository base in which the active ingredient(s) does not dissolve in order to avoid problems associated with partition between the molten or softened base and the rectal liquid. The release of the active ingredient(s) may in case of a suspension be dependent on sedimentation of the solid particles in the molten or softened base to the interface of the rectal liquid. The particle size of the active ingredient(s) should therefore be optimized to take both sedimentation and dissolution in the rectal liquid into account.
In the manufacture of suppositories containing dispersed active ingredient(s), measures are taken to ensure a suitable and controlled particle size.
When prepared by moulding, the medicated mass, sufficiently liquefied by heating, is poured into suitable moulds. The suppositories solidify on cooling. In certain cases, it is also possible to cold-mould by compression in a suitable press.
The softening time is determined according to the text Softening time determination of lipophilic suppositories, published in the Supplementary information section.
A suitable test is carried out to demonstrate the appropriate release of the active ingredient(s) from suppositories.
Packaging must be adequate to protect suppositories from light, excessive heat, moisture, and damage due to handling and transportation. It is necessary to ensure that the suppositories can be released from the packaging easily and without damage.
Visual inspection
Suppositories are elongated, smooth and have a uniform texture and appearance.
Evidence of physical and/or chemical instability is demonstrated by noticeable changes in:
• surface texture or form, and• colour and odour.
Disintegration
Suppositories comply with 5.4 Disintegration test for suppositories and rectal capsules unless intended for sustained release. For suppositories with a lipophilic base, examine after 30 minutes, and for suppositories with a water-soluble base, examine after 60 minutes.
Uniformity of mass
Suppositories comply with 5.2 Uniformity of mass of single-dose preparations.
Uniformity of content
Suppositories comply with 5.1 Uniformity of content of single-dose preparations when the content of active ingredient is 5 mg or less per suppository or 5% or less of the total mass. If the suppository has more than one active ingredient, the requirement applies only to those active ingredients that fall into the above category. If the test for uniformity of content is prescribed, the test for uniformity of mass is not required.
Containers
Suppositories should be supplied in a well-closed container. The container material should not adversely affect the quality of the preparation, nor should it allow diffusion into or across the container material or yield foreign substances into the preparation.

WHO Drug Information Vol. 28 No. 1, 2014
48
Consultation documents
48
Rectal capsules
Definition
Rectal capsules are solid, single-dose preparations generally similar to soft capsules as defined in the monograph on Capsules, except that they may have a lubricating coating. The contents of rectal capsules are usually solutions or suspensions of the active ingredient(s) in non-aqueous liquids, e.g. vegetable oil, or in semi-solid mixtures of suitable excipients.
Manufacture
See the manufacturing instructions for soft capsules. Other considerations for soft capsule suppositories include the study of and suitable controls for pH, leakage and pellicle formation.
A suitable test is carried out to demonstrate the appropriate release of the active ingredient(s) from rectal capsules.
Visual inspection
Rectal capsules are of elongated shape, smooth and have a uniform external appearance.
Unpack and inspect at least 20 rectal capsules. They should be smooth and undamaged. Evidence of physical instability is demonstrated by gross changes in physical appearance, including hardening or softening, cracking, swelling, mottling or discoloration of the shell.
Disintegration
Rectal capsules comply with 5.4 Disintegration test for suppositories and rectal capsules unless intended for sustained release. Examine the state of the rectal capsules after 30 minutes unless otherwise prescribed in the individual monograph.
Uniformity of mass
Rectal capsules comply with the requirements to capsules in 5.2 Uniformity of mass of single-dose preparations.
Uniformity of content
Rectal capsules comply with 5.1 Uniformity of content of single-dose preparations when the content of active ingredient is 5 mg or less per suppository or 5% or less of the total mass. If the rectal capsule has more than one active ingredient, the requirement applies only to those active ingredients that fall into the above category. If the test for uniformity of content is prescribed, the test for uniformity of mass is not required.
Rectal solutions, emulsions and suspensions
Definition
Rectal solutions, emulsions and suspensions (also called enemas) are liquid preparations intended for rectal application to obtain a local or systemic effect, or they may be intended for diagnostic purposes. They contain one or more active ingredients dissolved or dispersed in water, glycerol, macrogols, vegetable oil or mixtures thereof.
Rectal emulsions may show evidence of phase separation but are readily redispersed on shaking. Rectal suspensions may show a sediment that is readily dispersible on shaking to give a suspension that remains sufficiently stable to enable the correct dose to be delivered.

49
WHO Drug Information Vol. 28 No. 1, 2014 Consultation documents
49
They may contain excipients, for example to adjust the viscosity of the preparation, to adjust or stabilize pH, to increase the solubility of the active ingredient(s) and to stabilize the preparation. The excipients do not, at the concentrations used, cause undue local irritation.
Rectal solutions, emulsions and suspensions are supplied in single-dose containers containing a volume in the range of 2.5 ml to 2000 ml. The container is adapted to deliver the preparation to the rectum or is accompanied by a suitable applicator.
Powders and tablets for rectal solutions and suspensions
Definition
Powders and tablets intended for the preparation of rectal solutions or suspensions are single-dose preparations that are dissolved or dispersed in water or other suitable solvents at the time of administration. They may contain excipients to facilitate dissolution or dispersion or to prevent aggregation of the particles.
After dissolution or suspension, the preparation complies with the requirements for rectal solutions or rectal suspensions as appropriate.
Disintegration
Tablets for rectal solutions or suspensions comply with the following test: Place one tablet in a 250 ml beaker containing 200 ml of water R at 15–25 °C. Repeat the operation on five additional tablets. The tablets comply with the test if each of the six tablets used in the test dissolves or disintegrates within 3 minutes, unless otherwise specified in the individual monograph.
Labelling
The label states:
• the method of preparing the rectal solution or suspension;• when necessary, conditions and duration of storage of the final preparation.
Semi-solid rectal preparations
Definition
Semi-solid rectal preparations are ointments, creams or gels intended for local treatment in the rectum.
They are usually supplied as single-dose preparations in containers adapted to deliver the preparation to the rectum or are accompanied by a suitable applicator.
Semi-solid rectal preparations comply with the requirements for Topical semi-solid dosage forms.
Manufacture
When supplied in multidose containers, the expected reproducibility of the delivery of the intended volume must be ensured.
***

WHO Drug Information Vol. 28 No. 1, 2014
50
Consultation documents
50
Revision of method of analysis: 5.3 Disintegration test for tablets and capsules
This is a draft proposal for The International Pharmacopoeia (Working document QAS/14.572, February 2014).
The working document with line numbers and tracked changes is available for comment at www.who.int/medicines/areas/quality_safety/quality_assurance/projects/en/. Please address any comments to: World Health Organization, Quality Assurance and Safety: Medicines, Dr Herbert Schmidt, 1211 Geneva 27, Switzerland; fax: +41 22 791 4730; email: [email protected].
[Note from the Secretariat. It is proposed to include a disintegration test for large tablets in the test for disintegration of tablets and capsules. The proposed method is reproduced with permission from The European Pharmacopoeia.
This test is provided to determine whether tablets or capsules disintegrate within the prescribed time when placed in a liquid medium under the experimental conditions presented below.
For the purposes of this test disintegration does not imply complete dissolution of the unit or even of its active constituent. Complete disintegration is defined as that state in which any residue of the unit, except fragments of insoluble coating or capsule shell, remaining on the screen of the test apparatus or adhering to the lower surface of the discs, if used, is a soft mass having no palpably firm core.
Use apparatus A for tablets and capsules that are not greater than 18 mm. For larger tablets and capsules use apparatus B.
Test A. Tablets and capsules of normal size
This text is based on the internationally-harmonized texts developed by the Pharmacopoeial Discussion Group (PDG). Some editorial modifications have been made in order to be in line with the style used in The International Pharmacopoeia.
Apparatus. The apparatus (Figure 1) consists of a basket-rack assembly, a 1000 ml, low-form beaker, 138–160 mm in height and having an inside diameter of 97–115 mm for the immersion fluid, a thermostatic arrangement for heating the fluid between 35 °C and 39 °C, and a device for raising and lowering the basket in the immersion fluid at a constant frequency rate between 29 and 32 cycles per minute, through a distance of not less than 53 mm and not more than 57 mm. The volume of the fluid in the vessel is such that at the highest point of the upward stroke the wire mesh remains at least 15 mm below the surface of the fluid and descends to not less than 25 mm from the bottom of the vessel on the downward stroke. At no time should the top of the basket-rack assembly become submerged. The time required for the upward stroke is equal to the time required for the downward stroke and the change in stroke direction is a smooth transition, rather than an abrupt reversal of motion. The basket-rack assembly moves vertically along its axis. There is no appreciable horizontal motion or movement of the axis from the vertical.

51
WHO Drug Information Vol. 28 No. 1, 2014 Consultation documents
51
Figure 1. Diagram for disintegration apparatus A (dimensions are expressed in millimeters)
Basket-rack assembly. The basket-rack assembly consists of six open-ended transparent tubes, each 75.0–80.0 mm long and having an internal diameter of 20.70–23.00 mm and a wall 1.0–2.8 mm thick; the tubes are held in a vertical position by two plates, each 88–92 mm in diameter and 5.00–8.50 mm in thickness, with six holes, each 22–26 mm in diameter, equidistant from the centre of the plate and equally spaced from one another. Attached to the lower surface of the lower plate is a woven stainless steel wire mesh, which has a plain square weave with 1.8–2.2 mm apertures and with a wire diameter of 0.570–0.660 mm. The parts of the apparatus are assembled and rigidly held by means of three bolts passing through the two plates. A suitable means is provided to suspend the basket-rack assembly from the raising and lowering device using a point on its axis.
The design of the basket-rack assembly may be varied somewhat provided the specifications for the glass tubes and the screen mesh size are maintained. The basket-rack assembly conforms to the dimensions shown in Figure 1.
Discs. The use of discs is permitted only where specified or allowed. Each tube is provided with a cylindrical disc 9.35–9.65 mm thick and 20.55–20.85 mm in diameter. The disc is made of a suitable, transparent plastic material having a specific gravity of 1.18–1.20. Five parallel 1.9–2.1 mm holes extend between the ends of the cylinder. One of the holes is centered on the cylindrical axis. The other holes are centered 5.8–6.2 mm from the axis on imaginary lines perpendicular to the axis and parallel to each other. Four identical trapezoidal-shaped planes are cut into the wall of the cylinder, nearly perpendicular to the ends of the cylinder. The trapezoidal shape is symmetrical; its parallel sides coincide with the ends of the cylinder and are parallel to an imaginary line connecting the centres of two adjacent holes 6 mm from the cylindrical axis. The parallel side of the trapezoid on the bottom of the cylinder has a length of 1.5–1.7 mm and its bottom edges lie at a depth of 1.50–1.80 mm from the cylinder’s circumference. The parallel side of the trapezoid on the top of the cylinder has a length of 9.2–9.6 mm and its centre lies at a depth of 2.5–2.7 mm from the cylinder’s circumference. All surfaces of the disc are smooth. If the use of discs is specified, add a disc to each tube and operate the apparatus as directed under procedure. The discs conform to the dimensions found in Figure 1.

WHO Drug Information Vol. 28 No. 1, 2014
52
Consultation documents
52
The use of automatic detection employing modified discs is permitted where the use of discs is specified or allowed. Such discs must comply with the requirements of density and dimension given in this chapter.
Procedure. Place one dosage unit in each of the six tubes of the basket and if specified add a disc. Operate the apparatus using water as the immersion fluid unless another liquid is specified and maintain its temperature at 35–39 °C. At the end of the specified time, lift the basket from the fluid and observe the dosage units: all of the dosage units have disintegrated completely. If one or two dosage units fail to disintegrate, repeat the test on 12 additional dosage units. The requirements of the test are met if not less than 16 of the 18 dosage units tested are disintegrated.
Test B. Large tablets and large capsules
This test is reproduced with permission from The European Pharmacopoeia.
Apparatus. The main part of the apparatus (Figure 2) is a rigid basket-rack assembly supporting 3 cylindrical transparent tubes 77.5 ± 2.5 mm long, 33.0 mm ± 0.5 mm in internal diameter, and with a wall thickness of 2.5 ± 0.5 mm. Each tube is provided with a cylindrical disc 31.4 ± 0.13 mm in diameter and 15.3 ± 0.15 mm thick, made of transparent plastic with a relative density of 1.18–1.20. Each disc is pierced by 7 holes, each 3.15 ± 0.1 mm in diameter, 1 in the centre and the other 6 spaced equally on a circle of radius 4.2 mm from the centre of the disc. The tubes are held vertically by 2 separate and superimposed rigid plastic plates 97 mm in diameter and 9 mm thick, with 3 holes. The holes are equidistant from the centre of the plate and equally spaced. Attached to the under side of the lower plate is a piece of woven gauze made from stainless steel wire 0.63 ± 0.03 mm in diameter and having mesh apertures of 2.0 ± 0.2 mm. The plates are held rigidly in position and 77.5 mm apart by vertical metal rods at the periphery. A metal rod is also fixed to the centre of the upper plate to enable the assembly to be attached to a mechanical device capable of raising and lowering it smoothly at a constant frequency of between 29 and 32 cycles per minute, through a distance of 55 ± 2 mm.
The assembly is suspended in the specified liquid medium in a suitable vessel, preferably a 1 litre beaker. The volume of the liquid is such that when the assembly is in the highest position the wire mesh is at least 15 mm below the surface of the liquid, and when the assembly is in the lowest position the wire mesh is at least 25 mm above the bottom of the beaker and the upper open ends of the tubes remain above the surface of the liquid. A suitable device maintains the temperature of the liquid at 35–39 °C.
The design of the basket-rack assembly may be varied provided the specifications for the tubes and wire mesh are maintained.
Method. Test 6 tablets or capsules either by using 2 basket-rack assemblies in parallel or by repeating the procedure. In each of the 3 tubes, place 1 tablet or capsule and, if prescribed, add a disc; suspend the assembly in the beaker containing the specified liquid. Operate the apparatus using water as the immersion fluid unless another liquid is specified for the prescribed period, withdraw the assembly and examine the state of the tablets or capsules. To pass the test, all 6 of the tablets or capsules must have disintegrated.

53
WHO Drug Information Vol. 28 No. 1, 2014 Consultation documents
53
Figure 2. Diagram for disintegration apparatus B (dimensions are expressed in millimeters)
***

WHO Drug Information Vol. 28 No. 1, 2014
54
Consultation documents
54
Revision of method of analysis: 5.4 Disintegration test for suppositories and rectal capsules
This is a draft proposal for The International Pharmacopoeia (Working document QAS/14.573, February 2014).
The working document with tracked changes and line numbers is available for comment at www.who.int/medicines/areas/quality_safety/quality_assurance/projects/en/. Please address any comments to: World Health Organization, Quality Assurance and Safety: Medicines, Dr Herbert Schmidt, 1211 Geneva 27, Switzerland; fax: +41 22 791 4730; email: [email protected].
[Note from the Secretariat: At its meeting in October 2012 the Expert Committee on Specifications adopted a general method for determination of the softening time of lipophilic suppositories to be placed in the Supplementary information section of The International Pharmacopoeia. Consequently, it is proposed to revise chapter 5.4 Disintegration test for suppositories and to replace the current Method 2 by the method for determination of the softening time of lipophilic suppositories.
This test measures the time elapsed for a suppository placed in water to disintegrate.
The disintegration test determines whether suppositories soften or disintegrate within a prescribed time when placed in an immersion fluid using the experimental conditions described below.
Disintegration is considered to be achieved when:
• dissolution is complete;• the components of the suppositories have separated, e.g. melted fatty substances have
collected on the surface of the liquid, insoluble powders have fallen to the bottom and soluble components have dissolved or are distributed in one or more of the ways described in Methods 1 and 2;
• there is softening of the test sample, usually accompanied by an appreciable change of shape without complete separation of the components. The softening process is such that a solid core no longer exists when pressure is applied with a glass rod; or
• rupture of the gelatin shell or rectal capsule occurs resulting in release of the contents.
Method 1 (for water-soluble, hydrodispersible and fat-based suppositories and rectal capsules):
This test measures the time elapsed for a suppository placed in water to disintegrate.
Apparatus
The apparatus (Figure 1) consists of a 60 mm long cylinder of glass or transparent plastic and a metal device consisting of two perforated stainless steel discs, held about 30 mm apart. These discs each have 39 holes, 4mm in diameter, which are evenly spaced in a concentric pattern. The diameter of the discs is marginally inferior to that of the interior of the cylinder. Once inserted into the cylinder, the metal device is attached to the rim of the cylinder by means of three spring clips. The test is carried out using three such apparatuses, each containing a single test sample. Each apparatus is placed in a beaker with a minimum capacity of 4 litres filled with water unless otherwise prescribed. The beaker is fitted with a slow stirrer and a support that holds the apparatus vertically 90 mm below the surface of the water so that it can be inverted without emerging from the water.

55
WHO Drug Information Vol. 28 No. 1, 2014 Consultation documents
55
Figure 1. Apparatus for water-soluble, hydrodispersible, and fat-based suppositories
A. Horizontal view. B. Vertical view. Measurements in mm.Procedure
Unless otherwise described in the individual monograph, use water maintained at a temperature of 36–37 °C as the immersion fluid. The test requires three suppositories and the procedure is applied to each of the suppositories.
Place the sample on the lower disc of the metal device and then insert it into the cylinder. Place the apparatus into the beaker and invert it every 10 minutes without removing it from the liquid. Repeat the operation with the remaining two suppositories. Record the time required for the disintegration of the suppositories.
Unless otherwise stated in the individual monograph, for each of the three suppositories or rectal capsules, examine the state of the sample after 30 minutes for fat-based suppositories and rectal capsules, and after 60 minutes for water-soluble suppositories.
Method 2 (alternative for fat-based suppositories):
This test measures the time elapsed for a suppository placed in water to soften to the extent that it no longer offers resistance when a defined weight is applied.
The method is described in the chapter Softening time determination of lipophilic suppositories, published in the Supplementary information section.
The test requires three suppositories and the procedure is applied to each of the suppositories. Unless otherwise stated in the individual monograph, for each of the three suppositories, examine the state of the sample after 30 minutes.
***

WHO Drug Information Vol. 28 No. 1, 2014
56
Consultation documents
56
RADIOPHARMACEUTICALS: Sodium iodide (131I) solution
This is a revised draft proposal for The International Pharmacopoeia (Working document QAS/13.547/Rev.2, March 2014).
The working document with line numbers is available for comment at www.who.int/ medicines/areas/quality_safety/quality_assurance/projects/en/. Please address any comments to: World Health Organization, Quality Assurance and Safety: Medicines, Dr Herbert Schmidt, 1211 Geneva 27, Switzerland; fax: +41 22 791 4730; email: [email protected].
Monographs: Radiopharmaceuticals: Specific monographs: Natrii iodidi (131I) solutio - Sodium iodide (131I) solution
Latin. Natrii iodide (131I) solutio.
English. Sodium iodide (131I) solution.
Structural formula. Na+………..131I–
Relative molecular mass. 153.895.
Empirical formula. Na131I
Chemical name. Sodium [131I] iodide
Other names. Natrii radioiodidum, Iodotope Sodium iodide-I 131
Description. Sodium iodide (131I) solution is a clear colourless solution. Iodine-131 has a half-life of 8.02 days.
Category. Diagnostic or therapeutic.
Storage. Stored at room temperature in a single-dose or multiple-dose containers.
Labelling. The label complies with the General monograph, the monograph of Radiopharmaceuticals.
Manufacture. No carrier added iodine-131 may be obtained by neutron bombardment of tellurium or by extraction from uranium fission products. Sodium iodide (131I) solution may contain sodium thiosulfate, sodium hydrogen carbonate or other suitable reducing agents and may contain a suitable buffer.
Additional information. Wherever V is used within the tests of this monograph, V is the maximum recommended dose, in millilitres.RequirementsComplies with the monographs for Liquid preparations for oral use, Parenteral Preparations and with that for Radiopharmaceuticals as and where appropriate.
Definition. Sodium iodide solution is an aqueous solution containing radioactive (131I) in the form of sodium iodide (131I), suitable for either oral or intravenous administration. The solution contains not less than 90% and not more than 110% of the declared radioactivity due to iodine-131 stated on the label at the reference date and time. Not less than 99.9% of the total radioactivity is due to iodine-131. Not less than 95% of the total iodine-131 radioactivity is present as iodide. It contains minute amounts of naturally occurring iodine 127. The specific activity is not less than 185 MBq per microgram of iodine at the reference date and time stated on the label. The iodide content of maximum recommended dose should not be more than 20 µg.

57
WHO Drug Information Vol. 28 No. 1, 2014 Consultation documents
57
Identity tests• Either tests A and C or tests B and C may be applied.
A. Record the gamma-ray and X-ray spectrum using a suitable instrument with a sample of iodine-131, suitably diluted if needed. The spectrum is concordant with the reference spectrum of a specimen of iodine-131 in that it exhibits a major peak of 365 keV. Standardized iodine-131 solutions are available from laboratories recognized by the relevant national or regional authority.
B. The half-life determined using a suitable detector system is between 7.61 and 8.42 days.
C. Examine the radiochromatogram obtained in the test for radiochemical purity. The principal peak in the chromatogram obtained with the test solution (a) is similar in retention time to the principal peak in the chromatogram obtained with the reference solution (c).
pH value. Carry out the test as described under 1.13 Determination of pH or R1.5 under the monograph for Radiopharmaceuticals. pH is between 7.0 and 10.0 with 3.2.1 Test for sterility of non-injectable preparations, modified as described in the monograph for Radiopharmaceuticals. If intended for intravenous administration, it complies with 3.2 Test for sterility for injectable preparations, modified as described in the monograph for Radiopharmaceuticals. The solution may be released for use before completion of the test.
Bacterial endotoxinsCarry out the test as described under 3.4 Test for bacterial endotoxins, for solution intended for intravenous use modified as described in the monograph for Radiopharmaceuticals. The injection contains not more than 175/V (I.U of endotoxins per millilitre).
Radionuclidic purity. Record the gamma-ray and X-ray spectrum using a suitable instrument and measure the half-life using a suitable method. Determine the relative amounts of iodine-131, iodine-133, iodine-135 and other radionuclidic impurities that may be present. Iodine-133 has a half-life of 20.8 hours and exhibits major peaks of 530 keV and 875 keV. Iodine-135 has a half-life of 6.57 hours and exhibits major peaks of 527 keV, 1132 keV and 1260 keV. Not less than 99.9% of the total radioactivity is due to iodine-131.
Chemical purityIodide. Carry out the test as described under 1.14.4 High-performance liquid chromatography, using a stainless steel column (0.25 m x 4.0 mm) packed with particles of silica gel, the surface of which has been modified with chemically-bonded octadecylsilyl groups (5 µm), maintain the temperature constant between 20 °C and 30 °C. Dissolve 5.844 g of sodium chloride R in 1000 mL of water R, add 650 µL of octylamine R and adjust to pH 7.0 with phosphoric acid R, add 50 mL of acetonitrile R and mix. Use the mixture as the mobile phase. Use flow rate of 1.5 mL/min, and spectrophotometer detector at 220 nm and radioactivity detector (connected in series) for detection. Prepare the test solution (a) which is the preparation to be examined. Prepare the test solution (b) by diluting test solution (a) using 0.05 M sodium hydroxide until the radioactivity is equivalent to about 74 MBq/mL and add an equal volume of a solution containing 1 g/L of potassium iodide R, 2 g/L of potassium iodate R and 10 g/L of sodium hydrogen carbonate R and mix. The reference solution (c) is prepared by diluting 1 mL of a 26.2 mg/L solution of potassium iodide R to V with water R, (V being the maximum recommended dose in millilitres). Prepare the reference solution (d) by dilution 1 mL of a 24.5 mg/L solution of potassium iodate R to V with water R, (V being the maximum recommended dose in millilitres). Mix equal volumes of this solution and of reference solution (c). Prepare a solution containing 2 mg/mL of each of the components stated on the label, apart from iodide, used as blank solution. Inject 25 µL of test solution (a), the blank solution

WHO Drug Information Vol. 28 No. 1, 2014
58
Consultation documents
58
and reference solutions (c) and (d). The run time is 12 minutes. The relative retention of iodate with reference to iodide (retention time of iodide is about 5 minutes): iodate is from 0.2 to 0.3.
System suitability. Regarding the chromatogram due to the blank solution, none of the obtained peaks shows a retention time similar to that of the peak due to iodide. The resolution is a minimum of 2 between the peaks due to iodide and iodate in the chromatogram obtained with reference solution (d) recorded with the spectrophotometer.
The limit of iodide is detected by studying the chromatogram obtained with the spectrophotometer and comparing the peak due to iodide with the chromatogram due to reference solution (c). The area of the peak due to iodide is not more than the area of the corresponding peak in the chromatogram obtained with reference solution (c).
Radiochemical purity• Either test A, B, or C may be applied
A. Carry out the test as described under 1.14.2 Paper chromatography and ascending conditions, using paper for chromatography R (25 × 300 mm). Place a measured volume of a solution containing 100 mg of potassium iodide, 200 mg of potassium iodate and 1 g of sodium bicarbonate, and 25 mm from one end of the chromatographic paper. Allow the paper to dry. To the same area of the paper add an equal volume of appropriately diluted solution such that it provides a count rate of about 20 000 counts per minute and allow the paper to dry. Develop the chromatogram over a period of about 4 hours by ascending chromatography, using dilute methanol (7:10, v/v). Allow the paper to dry in air and determine the radioactivity distribution by scanning with a suitable radiation detector: the radioactivity of the [131I]iodide band is not less than 95% of the total radioactivity and its RF value falls within ±5% of the value found for sodium iodide when determined under parallel conditions. Confirmation of the identity of the iodide band is made by the addition to the suspected iodide band of 6 drops of acidified hydrogen peroxide solution (prepared by adding 6 drops of 1 N hydrochloric acid to 10 mL of hydrogen peroxide solution), followed by the dropwise addition of starch TS; the development of a blue color indicates presence of iodide.
B. Carry out the test 1.14.4 High-performance liquid chromatography as described in the test for iodide with the following modification: • inject test solution (b), • using the chromatogram obtained with the radioactivity detector, determine the radioactivity of the peak for iodide as a percentage of the total radioactivity. Not less than 95% of the total radioactivity is due to [131I] iodide.
C. Carry out the test as described under 1.15 Electrophoresis, Paper-electrophoresis Prepare paper strips, type Whatman No. 3 MM for electrophoresis with dimensions of 65 cm × 3 cm. Apply 10–20 μL samples at a distance of 10–13 cm from the end of the stripes. Use borate buffer with a concentration of 9.0 g/L and pH 9.0 ± 0.1. Carry out the electrophoresis at a potential of 900 V for 50 minutes. The Rf values for iodide are between 0.7 and 0.9, Rf for iodate is 0.4, periodate from 0.0 to 0.1. The product can be accepted if the 131I anion content is higher than 95% even on the expiry date.
Radioactivity. Measure the radioactivity using a suitable instrument as described under R.1.1 Detection and measurement of radioactivity.
Impurities[131I] iodate ion.
***

59
WHO Drug Information Vol. 28 No. 1, 2014 Consultation documents
59
Technetium (99mTc) exametazime complex injectionThis is a revised draft proposal for The International Pharmacopoeia (Working document QAS/13.548/Rev.2, March 2014).
The working document with line numbers is available for comment at www.who.int/ medicines/areas/quality_safety/quality_assurance/projects/en/. Please address any comments to: World Health Organization, Quality Assurance and Safety: Medicines, Dr Herbert Schmidt, 1211 Geneva 27, Switzerland; fax: +41 22 791 4730; email: [email protected].
Monographs: Radiopharmaceuticals: Specific monographs: Technetii (99mTc) exametazimi multiplex injectio -
Technetium (99mTc) exametazime complex injection
Latin. Technetii (99mTc) exametazimi multiplex injection.
English. Technetium (99mTc) exametazime complex injection.
Structural formula
and enantiomer
C13H25N4O3 . 99mTc
Relative molecular mass. 384.269
Chemical name. Racemic mixture of (3RS,9RS)-4,8-diaza-3,6,6,9-tetramethylundecane-2,10-dione bisoxime complex with (99mTc) technetium.
Other names. (99mTc)-D,L-Hexamethylpropyleneamine oxime complex injection; (99mTc)-D,L-HMPAO injection.
Description. Technetium (99mTc) exametazime complex injection is a clear, colourless aqueous solution. Technetium-99m has a half-life of 6.01 hours.
Category. Diagnostic.
Storage. Technetium (99mTc) exametazime complex injection should be kept at a temperature between 2°C to 8°C.
Technetium (99mTc) exametazime complex injection should be used within 30 minutes of reconstitution of the unlabelled kit with Technetium-99m, unless the preparation has been stabilized with cobalt chloride solution or methylene blue solution or any other stabilizer.
Labelling. The label complies with the General monograph, the monograph of Radiopharmaceuticals. The label includes the name stabilizer if added.

WHO Drug Information Vol. 28 No. 1, 2014
60
Consultation documents
60
Manufacture. Technetium (99mTc) exametazime injection is prepared aseptically from sterile starting materials such as a sterile kit containing a mixture of (3RS, 9RS)-4, 8-diaza-3,6,6,9-tetramethylundecane-2,10-dione bisoxime and stannous salt with Sodium pertechnetate (99mTc) injection (Fission) or Sodium Pertechnetate (99mTc) injection (Non-fission). The injection may have the pH adjusted and may contain stabilizing agents. The injection may also be prepared under aseptic processing combined with sterilization by Filtration (see 5.8 Methods of sterilization).
Additional information. Wherever V is used within the tests of this monograph, V is the maximum recommended dose in millilitre.
Requirements
Complies with the monograph for Parenteral Preparations and with that for Radiopharmaceuticals.
Definition. Technetium (99mTc) exametazime injection is a sterile lipophilic solution of racemic mixture of (3RS, 9RS)-4, 8-diaza-3,6,6,9-tetramethylundecane-2,10-dione bisoxime (exametazime) complexes with sodium pertechnetate (99mTc) injection (fission or non-fission) in presence of stannous salt. The injection is suitable for intravenous administration and contains sufficient sodium chloride to make the solution isotonic with blood. The content of technetium-99m is not less than 90% and not more than 110% of the content of technetium-99m. Not less than 80% of the total technetium-99m radioactivity is present as lipophilic (99mTc) exametazime complex and its meso isomer.
Identity tests
• Either tests A and C or tests B and C may be applied.A. Record the gamma-ray spectrum using a suitable instrument with a sample of technetium-99m, suitably diluted if needed. The spectrum is concordant with the reference spectrum of a specimen of technetium-99m in that it exhibits a major peak of 142 keV.
Standardized technetium-99m solutions are available from competent laboratories recognized by the relevant national or regional authority.
B. The half-life determined using a suitable detector system is between 5.72 and 6.32 hours.
C. Examine the chromatograms obtained in the test of Impurity A under Radiochemical purity. The principal peak in the chromatogram obtained with the test solution is similar in retention time to the peak due to lipophilic technetium-99m exametazime in the chromatogram obtained with the reference solution.
pH value. Carry out the test as described under 1.13 Determination of pH or R1.5 under the monograph for Radiopharmaceuticals. The pH of the injection is between 5.0 and 10.0.
Sterility. The injection complies with 3.2 Test for sterility, modified as described in the monograph for Radiopharmaceuticals. Test for sterility will be initiated on the day of manufacture. The injection may be released for use before completion of the test.
Bacterial endotoxins. Carry out the test as described under 3.4 Test for bacterial endotoxins, modified as described in the monograph for Radiopharmaceuticals. The injection contains not more than 175/V I.U of endotoxins per millilitre.
Radionuclidic purity. Complies with the tests of radionuclidic purity under the monographs of Sodium pertechnetate (99mTc) injection (Fission) or Sodium Pertechnetate (99mTc) injection

61
WHO Drug Information Vol. 28 No. 1, 2014 Consultation documents
61
(Non-fission) used for the preparation of Technetium (99mTc) exametazime injection. Not less than 99.9% of the total radioactivity is due to technetium-99m.
Radiochemical purity
Impurity C. Carry out the test described under 1.14.1 Thin-layer chromatography for impurity C use TLC silica gel plate R, a glass fiber plate and 9 g/L solution of sodium chloride as a mobile phase. Apply to the plate about 5 μl of the injection to be examined and develop immediately for a distance over 2/3 of the plate. Allow the plate to dry in air and determine the radioactivity distribution using a suitable detector. Impurity C has Rf value of 0.8 to 1.0; lipophilic technetium-99m exametazime and impurities A, B, D and E do not migrate. The maximum limit of impurity C is 10% of the total radioactivity.
Total of lipophilic technetium-99m exametazime and impurity A. Carry out the test under 1.14.1 Thin-layer chromatography. Use TLC silica gel plate R, a glass fibre plate and methyl ethyl ketone as a mobile phase. Apply to the plate about 5 μl of the injection to be examined and develop immediately for a distance over 2/3 of the plate. Allow the plate to dry in air and determine the radioactivity distribution using a suitable detector. The lipophilic technetium-99m exametazime, impurities A and C have Rf value of 0.8 to 1.0; for impurities B, D and E do not migrate.
Calculate the percentage of radioactivity due to impurities B, D and E from test C and the percentage of the radioactivity due to impurity C from test B. Calculate the total percentage of lipophilic technetium-99m exametazime and impurity A from the expression: 100- A- B.
Not less than 80% of the total technetium-99m radioactivity is present as lipophilic technetium-99m exametazime and impurity A.
Impurity A. Carry out the test as descried under 1.14.4 High-performance liquid chromatography, using a stainless steel column (0.25 m x 4.6 mm) packed with particles of silica gel, the surface of which has been modified with chemically-bonded octadecylsilyl groups (5 µm). As a mobile phase use a mixture of 33 volumes of acetonitrile R and 67 volumes of 0.1 M phosphate buffer solution R pH 3.0 to use as mobile phase. The flow rate is 1.5 mL/min, the detector is radioactivity detector with loop injector and the run time is 20 min. Prepare the reference solution by dissolving the contents of a vial of meso-rich exametazime CRS in 0.5 ml of a 9 g/L solution of sodium chloride and transfer to a lead-shielded, nitrogen-filled vial. Add 6 µL of a freshly prepared 1 g/L solution of stannous chloride R in 0.05 M hydrochloric acid and 2.5 mL of sodium pertechnetate (99mTc) injection (fission or non-fission) containing 370–740 MBq. Mix carefully and use within 30 min of preparation. The relative retention with reference to lipophilic technetium-99m exametazime to impurity A is about 1.2.
The produced chromatogram is similar to the chromatogram provided with meso-rich exametazime CRS. The resolution is minimum of 2 between the peaks due to lipophilic technetium-99m exametazime and to impurity A. Impurity A should not more than 5% of the radioactivity due to lipophilic technetium-99m exametazime and impurity A.
Tin estimation. Carry out the test as described under R2.1.4 Tin estimation by UV absorption, using 1.0 ml of a test solution prepared by diluting 1.5 ml of the injection to be examined to 25.0 ml with hydrochloric acid (103 g/L) VS and mixing thoroughly. Prepare the reference solution by dissolving 0.115 g of stannous chloride R using a solution in hydrochloric acid R (103 g/L HCl) and dilute to 1000.0 mL using the same acid. To the test solution and to 1 mL of each of the reference solutions add 0.05 mL of thioglycollic acid R, 0.1 mL of dithiol reagent R, 0.4 mL of a 20 g/L solution of sodium laurilsulfate R, 3 mL of 21g/L solution of hydrochloric acid R. Mix and measure the absorbance of each solution at 540 nm using 21g/L solution of

WHO Drug Information Vol. 28 No. 1, 2014
62
Consultation documents
62
hydrochloric acid as a compensation liquid. The absorbance of the test solution is not greater than that of the reference solution; not more than 0.6 µg of Sn per ml.
Radioactivity. Measure the radioactivity using a suitable instrument as described under R.1.1 Detection and measurement of radioactivity.
Impurities
A. Meso isomer of lipophilic technetium-99m exametazime,
B. Technetium-99m in colloidal form,
C. [99mTc]pertechnetate ion,
D. Non lipophilic technetium-99m exametazime complex,
E. Meso isomer of non-lipophilic technetium-99m exametazime complex.
***

63
WHO Drug Information Vol. 28 No. 1, 2014 Consultation documents
63
Thallous (201Tl) chloride injectionThis is a revised draft proposal for The International Pharmacopoeia (Working document QAS/13.549/Rev.2, March 2014).
The working document with line numbers is available for comment at www.who.int/ medicines/areas/quality_safety/quality_assurance/projects/en/. Please address any comments to: World Health Organization, Quality Assurance and Safety: Medicines, Dr Herbert Schmidt, 1211 Geneva 27, Switzerland; fax: +41 22 791 4730; email: [email protected].
Monographs: Radiopharmaceuticals: Specific monographs: Thallosi (201Tl) chloridi injectio - Thallous (201Tl) chloride injection
Latin. Thallosi (201Tl) chloridi injectio
English. Thallous (201Tl) chloride injection
Structural formula. 201Tl+…….Cl–
Empirical formula. 201TlCl
Relative molecular mass. 236.423
Chemical name. [201Tl]Thallium chloride
Other names. Thallous (201Tl) chloride
Description. Thallous (201Tl) chloride injection is a clear colourless, aqueous solution. Thallium-201 has a half-life of 72.96 hours.
Category. Diagnostic.
Storage. After aseptic withdrawal of the first dose from a multidose container, the container should be stored at a temperature between 2°C to 8°C.
Labelling. The label complies with the General monograph, the monograph of Radiopharmaceuticals.
Manufacture
No-carrier-added thallium-201 radioisotope is produced by proton bombardment of enriched thallium-203 target followed by chemical separation of radioactive lead-201 isotope. The lead-201 isotope has a half-life of 9.4 hours and decays to thallium-201. Separation of thallium-201 may be done using anion-exchange resin chromatography or solvent extraction. Thallous (201Tl) chloride injection may be sterilized by “Heating in an autoclave” (see 5.8 Methods of Sterilization).
Additional information
Wherever V is used within the tests of this monograph, V is the maximum recommended dose in millilitres.
Requirements
Complies with the monograph for Parenteral Preparations and with that for Radiopharmaceuticals.

WHO Drug Information Vol. 28 No. 1, 2014
64
Consultation documents
64
Definition. Thallous (201Tl) chloride injection is a sterile, isotonic, aqueous solution of thallium-201 as thallous chloride, suitable for intravenous administration. It contains sufficient sodium chloride to make the solution isotonic with blood and may contain suitable antimicrobial preservatives such as benzyl alcohol or stabilizing agents. The injection contains not less than 90% and not more than 110% of the content of thallium-201 at the reference date and time stated on the label. Not less than 97% of the total radioactivity is due to thallium-201. Not more than 2% of the total radioactivity is due to thallium-202. The specific activity is not less than 3.7 GBq of thallium-201 per milligram of thallium at the reference date and time stated on the label.
Identity tests
• Either tests A and C or tests B and C may be applied.A. Record the gamma-ray using a suitable instrument with a sample of thallium-201, suitably diluted if needed. The spectrum is concordant with the reference spectrum of a specimen of thallium-201 in that it exhibits major peaks of 135, 166 and 167 keV and X-rays of 69 and 83 keV.
B. The half-life determined using a suitable detector system is between 69.31 and 76.6 hours.
C. Examine the radiochromatogram obtained in the test for radiochemical purity. Not less than 95% of the radioactivity present as [201Tl]Thallium chloride and migrates on the strip towards the cathode as a single peak.
pH value. Carry out the test as described under 1.13 Determination of pH or R1.5 under the monograph for Radiopharmaceuticals. The pH of the injection is between 4.0 and 7.0.
Sterility. The injection complies with 3.2 Test for sterility, modified as described in the monograph for Radiopharmaceuticals. Test for sterility will be initiated on the day of manufacture. The injection may be released for use before completion of the test.
Bacterial endotoxins. Carry out the test as described under 3.4 Test for bacterial endotoxins, modified as described in the monograph for Radiopharmaceuticals. The injection contains not more than 175/V (I.U. of endotoxins per millilitre). The injection may be released for use before completion of the test.
Radionuclidic purity. Record the gamma-ray and X-ray spectrum using a suitable instrument and measure the half-life using a suitable method. Determine the relative amounts of thallium-200, thallium-201, thallium-202, lead-201, lead-203 and other radionuclidic impurities that may be present. Thallium-202 has a half-life of 12.2 days and exhibits a main peak of 440 keV. Thallium-200 has a half-life of 1.09 days and exhibits main peaks of 368, 579, 828 and 1206 keV. Lead-201 has a half-life of 9.4 hours and exhibits a main peak of 331 keV. Lead-203 has a half-life of 2.17 days and exhibits a main peak of 270 keV. Not less than 97% of the total radioactivity is due to thallium-201. Not more than 2% of the total radioactivity is due to thallium-202.
Standardized solutions of thallium-201 and thallium-202 are available from laboratories recognized by the relevant national or regional authority.
Radiochemical purity. Carry out the test as described under 1.15 Electrophoresis, zone-electrophoresis. Prepare a suitable cellulose polyacetate strip as the supporting medium and soak the strip in a solution of disodium edetate R (18.6 g/l) as the electrolyte solution. Soak the strip in the electrolyte solution for 45–60 min. Remove the strip with forceps, taking care to handle the outer edges only. Place the strip between 2 absorbent pads and blot to remove excess solution. Apply not less than 5 µl of a mixture of equal volumes of the preparation to

65
WHO Drug Information Vol. 28 No. 1, 2014 Consultation documents
65
be examined and the electrolyte solution to the centre of the blotted strip and mark the point of application. Attach the strip to the support bridge of an electrophoresis chamber containing equal volumes of disodium edetate R in each side of the chamber. Ensure that each end of the strip is in contact with the disodium edetate R. Apply an electric field of 250 volts per metre for 30 minutes. Allow the strip to dry in air. Determine the distribution of radioactivity using suitable detector.
Not less than 95% of the radioactivity on the strip migrates towards the cathode as a single peak.
Chemical purity
Thallium. Transfer 1.0 ml of the injection and 1.0 ml of thallium standard (2 µg/ml Tl) TS to separate screw-cap test tubes. To each tube add the following five solutions (A, B, C, D and E) and mix after each addition: 2 drops of a solution prepared by carefully mixing 18 ml of nitric acid (~1000 g/l) TS and 82 ml of hydrochloric acid (~250 g/l) TS (solution A); 1.0 ml of sulfosalicylic acid (0.1 mol/l) VS (solution B); 2 drops of hydrochloric acid (~250 g/l) TS (solution C); 4 drops of a solution prepared by dissolving 50 mg of rhodamine B R in hydrochloric acid (~250 g/l) TS and diluting to 100.0 ml (solution D); 1.0 ml of diisopropyl ether R (solution E). Screw the caps on tightly, shake the tubes by hand for exactly 1 minute, releasing any pressure build-up by loosening the caps slightly. Recap the tubes and allow the phases to separate. Transfer 0.5 ml of the ether layer from each tube to clean tubes. The colour of the ether layer obtained from the injection is not darker than that from the thallium standard (2 µg/ml Tl) TS.
Iron. Into separate cavities of a spot plate place 0.1 ml of the injection and 0.1 ml of iron standard TS diluted with water R to a concentration of 5 µg/ml. Add to each cavity 0.1 ml of a solution of hydroxylamine hydrochloride R (1 in 10), 1 ml of a solution of sodium acetate R (1 in 4) and 0.1 ml of a 0.5% dipyridyl solution prepared by dissolving 0.5 g of 2,2’-dipyridyl R in 100 ml of water R containing 0.15 ml of hydrochloric acid (~250 g/l) TS and mix. After 5 minutes the colour obtained from the injection is not darker than that of the iron standard solution.
Copper. Into separate cavities of a spot plate place 0.2 ml of the injection and 0.2 ml of copper standard (5 µg/ml Cu) TS. Add to each cavity the following 3 solutions (A, B and C) and mix after each addition: 0.2 ml of water R (solution A) and 0.1 ml of a solution of iron thiocyanate prepared by dissolving 1.5 g of ferric chloride R and 2 g of potassium thiocyanate R in water R and diluting to 100.0 ml with the same solvent (solution B); 0.1 ml of a solution of sodium thiosulphate R (1 in 100) (solution C). The time required for the injection to decolorize is equal to or longer than that observed for the copper standard solution.
Radioactivity. Measure the radioactivity using a suitable instrument as described under R.1.1 Detection and measurement of radioactivity.
Impurities
A. Lead-201,
B. Lead-203,
C. Thallium-200,
D. Thallium-202,
E. [201Tl] Thallic (III) ion.
***

66
WHO Drug Information Vol. 28 No. 1, 2014
66
ATC/DDD Classification
ATC/DDD Classification (Temporary)
The following ATC codes, DDDs and alterations were agreed at the meeting of the WHO International Working Group for Drug Statistics Methodology in October 2013. Comments or objections to the decisions should be forwarded to the WHO Collaborating Centre for Drug Statistics Methodology at [email protected]. The new ATC codes, DDDs and alterations will then be considered final and be included in the January 2015 version of the ATC/DDD index. The inclusion of a substance in the lists does not imply any recommendation for use in medicine or pharmacy.
New ATC 5th level codes:ATC level INN/Common name ATC code
albiglutide A10BX13amithiozone J04AK07atorvastatin and acetylsalicylic acid C10BX08atorvastatin, acetylsalicylic acid and ramipril
C10BX06
avanafil G04BE10azilsartan medoxomil and diuretics C09DA09azithromycin, fluconazole and secnidazole
J01RA07
balugrastim L03AA15brinzolamide, combinations S01EC54bromelains M09AB03cabozantinib L01XE26cangrelor B01AC25cariprazine N05AX15cefepime and amikacin J01RA06cefotaxime, combinations J01DD51cepeginterferon alfa-2b L03AB14ciprofloxacin and metronidazole J01RA10ciprofloxacin and ornidazole J01RA12ciprofloxacin and tinidazole J01RA11coagulation factor X B02BD13combinations N06DX30cyclopentolate, combinations S01FA54darunavir and cobicistat J05AR14dexketoprofen M02AA27dexrabeprazole A02BC07diltiazem C05AE03dinutuximab L01XC16donepezil, memantine and Ginkgo folium
N06DA53
Continued/

67
WHO Drug Information Vol. 28 No. 1, 2014 ATC/DDDClassification(Temporary)
New ACT 5th level codes, continued:ATC level INN/Common name ATC code
elosulfase alfa A16AB12enzalutamide L02BB04faldaprevir J05AE13florbetaben (18F) V09AX06fluocortolone D07XC05formoterol and aclidinium bromide R03AL05furazidin J01XE03hexetidine G01AX16ibrutinib L01XE27idelalisib L01XX47indanazoline R01AA15indometacin and antiinfectives S01CC02itropride A03FA07lamivudine and tenofovir disoproxil J05AR12lamivudine, abacavir and dolutegravir
J05AR13
lansoprazole, amoxicillin and levofloxacin
A02BD10
lansoprazole, clarithromycin and tinidazole
A02BD09
lansoprazole, combinations A02BC53metformin and acarbose A10BD17metformin and canagliflozin A10BD16metronidazole, combinations P01AB51montelukast, combinations R03DC53nadifloxacin D10AF05nebivolol and other hypertensives C07FB12nitrofurantoin, combinations J01XE51norfloxacin and tinidazole J01RA13ofloxacin and ornidazole J01RA09olaparib L01XX46palonosetron, combinations A04AA55peginterferon beta-1a L03AB13perflubutane polymer microspheres V08DA06pheniramine D04AA16pipenzolate and psycholeptics A03CA09rabeprazole, combinations A02BC54raxibacumab J06BB18riociguat C02KX05risedronic acid and colecalciferol M05BB07rosuvastatin and amlodipine C10BX09rosuvastatin, amlodipine and lisinopril
C10BX07
sertaconazole G01AF19simeprevir J05AE14
Continued/

WHO Drug Information Vol. 28 No. 1, 2014
68
ATC/DDD Classification (Temporary)
New ACT 5th level codes, continued:ATC level INN/Common name ATC code
sulfacetamide D10AF06tetracycline and oleandomycin J01RA08thiocolchicoside, combinations M03BX55tiotropium bromide, combinations R03BB54trimethobenzamide R06AA10trolamine D03AX12udenafil G04BE11umeclidinium bromide R03BB07umifenovir J05AX13valethamate A03AX14vedolizumab L04AA33
Change of ATC codes:INN/Common name Previous ATC New ATCalemtuzumab L01XC04 L04AA34
Change of ATC level names:Previous New ATC codeacetylsalicylic acid and esomeprazole
acetylsalicylic acid, combinations with proton pump inhibitors
B01AC56
Other antihypertensives Antihypertensives for pulmonary arterial hypertension
C02KX
cefuroxime, combinations with other antibacterials
cefuroxime and metronidazole J01RA03
spiramycin, combinations with other antibacterials
spiramycin and metronidazole J01RA04
New DDDs: INN/Common name DDD unit Adm. R.a ATC codeavanafil 0.1 g O G04BE10bilastine 20 mg O R06AX29catridecacog 2.5 TU P B02BD11cepeginterferon alfa-2b 17 mcg P L03AB14dimethyl fumarate 0.48 g O N07XX09dolutegravir 50 mg O J05AX12enzalutamide 0.16 g O L02BB04linaclotide 0.29 mg O A06AX04lipegfilgrastim 0.3 mg P L03AA14lixisenatide 20 mcg P A10BX10lurasidone 60 mg O N05AE05nafcillin 3 g P J01CF06 nalmefene 18 mg O N07BB05palonosetron 0.5 mg O A04AA05pegloticase 0.57 mg P M04AX02pomalidomide 3 mg O L04AX06regadenoson 0.4 mg P C01EB21umifenovir 0.8 g O J05AX13
a Administration Route: O=oral; P=parenteral

69
WHO Drug Information Vol. 28 No. 1, 2014 ATC/DDDClassification(Final)
ATC/DDD Classification (Final)
The following ATC codes, DDDs and alterations were agreed at the meeting of the WHO International Working Group for Drug Statistics Methodology in March 2013. These are considered as final and will be included in the January 2014 version of the ATC/DDD index. The WHO Collaborating Centre for Drug Statistics Methodology can be contacted at [email protected]. The inclusion of a substance in the lists does not imply any recommendation for use in medicine or pharmacy.
New ATC 5th level codes:ATC level INN/Common name ATC code
afamelanotide D02BB02apremilast L04AA32brimonidine D11AX21calcium citrate A12AA13carfilzomib L01XX45colestilan V03AE06delamanid J04AK06dienogest and ethinylestradiol G03AA16eliglustat A16AX10empagliflozin A10BX12encephalitis, Japanese, live
attenuatedJ07BA03
formoterol and fluticasone R03AK11insulin degludec A10AE06insulin degludec and insulin aspart A10AD06levofloxacin and ornidazole J01RA05lamivudine, tenofovir disoproxil and
efavirenzJ05AR11
macitentan C02KX04metformin and dapagliflozin A10BD15nalmefene N07BB05naloxegol A06AH03nomegestrol and estrogen G03FB12obinutuzumab L01XC15ocriplasmin S01XA22ospemifene G03XC05pomalidomide L04AX06serelaxin C01DX21strontium ranelate and colecalciferol M05BX53sucroferric oxyhydroxide V03AE05technetium (99mTc) tilmanocept V09IA09 tolperisone M02AX06vortioxetine N06AX26
Change of ATC codes:INN/common name Previous ATC New ATCbromelains B06AA11 D03BA03

WHO Drug Information Vol. 28 No. 1, 2014
70
ATC/DDD Classification (Final)
Change of ATC level names:Previous New ATC codenabiximols cannabinoids N02BG10Insulins and analogues for injection, intermediate-acting combined with fast-acting
Insulins and analogues for injection, intermediate- or long-acting combined with fast-acting
A10AD
Oxytocics Uterotonics G02AOther oxytocics Other uterotonics G02AXAntiprogestogens Progesterone receptor modulators G03XB
New DDDs:
ACT/Common name DDD unit Adm.R.a ATC codeaclidinium bromide* 0.644 mg Inhal powder R03BB05bedaquiline 86 mg O J04AK05ceftaroline fosamil 1.2 g P J01DI02dapagliflozin 10 mg O A10BX09glycopyrronium bromide** 44 mcg Inhal powder R03BB06mannitol 0.8 g Inhal powder R05CB16mirabegron 50 mg O G04BD12perampanel 8 mg O N03AX22tafamidis 20 mg O N07XX08teriflunomide 14 mg O L04AA31ulipristal 5 mg O G03XB02
a Administration Route: O=oral; P=parenteral* refers to aclidinium, delivered dose ** refers to glycopyrronium, delivered dose

WHO Drug Information, Vol. 28, No. 1, 2014 Recommended INN: List 71
71
International Nonproprietary Names for Pharmaceutical Substances (INN)
RECOMMENDED International Nonproprietary Names: List 71 Notice is hereby given that, in accordance with paragraph 7 of the Procedure for the Selection of Recommended International Nonproprietary Names for Pharmaceutical Substances [Off. Rec. Wld Health Org., 1955, 60, 3 (Resolution EB15.R7); 1969, 173, 10 (Resolution EB43.R9); Resolution EB115.R4 (EB115/2005/REC/1)], the following names are selected as Recommended International Nonproprietary Names. The inclusion of a name in the lists of Recommended International Nonproprietary Names does not imply any recommendation of the use of the substance in medicine or pharmacy. Lists of Proposed (1–109) and Recommended (1–70) International Nonproprietary Names can be found in Cumulative List No. 15, 2013 (available in CD-ROM only).
Dénominations communes internationales des Substances pharmaceutiques (DCI)
Dénominations communes internationales RECOMMANDÉES: Liste 71 Il est notifié que, conformément aux dispositions du paragraphe 7 de la Procédure à suivre en vue du choix de Dénominations communes internationales recommandées pour les Substances pharmaceutiques [Actes off. Org. mond. Santé, 1955, 60, 3 (résolution EB15.R7); 1969, 173, 10 (résolution EB43.R9); résolution EB115.R4 (EB115/2005/REC/1)] les dénominations ci-dessous sont choisies par l’Organisation mondiale de la Santé en tant que dénominations communes internationales recommandées. L’inclusion d’une dénomination dans les listes de DCI recommandées n’implique aucune recommandation en vue de l’utilisation de la substance correspondante en médecine ou en pharmacie. On trouvera d’autres listes de Dénominations communes internationales proposées (1–109) et recommandées (1–70) dans la Liste récapitulative No. 15, 2013 (disponible sur CD-ROM seulement).
Denominaciones Comunes Internacionales para las Sustancias Farmacéuticas (DCI) Denominaciones Comunes Internacionales RECOMENDADAS: Lista 71 De conformidad con lo que dispone el párrafo 7 del Procedimiento de Selección de Denominaciones Comunes Internacionales Recomendadas para las Sustancias Farmacéuticas [Act. Of. Mund. Salud, 1955, 60, 3 (Resolución EB15.R7); 1969, 173, 10 (Resolución EB43.R9); Résolution EB115.R4 (EB115/2005/REC/1) EB115.R4 (EB115/2005/REC/1)], se comunica por el presente anuncio que las denominaciones que a continuación se expresan han sido seleccionadas como Denominaciones Comunes Internacionales Recomendadas. La inclusión de una denominación en las listas de las Denominaciones Comunes Recomendadas no supone recomendación alguna en favor del empleo de la sustancia respectiva en medicina o en farmacia. Las listas de Denominaciones Comunes Internacionales Propuestas (1–109) y Recomendadas (1–70) se encuentran reunidas en Cumulative List No. 15, 2013 (disponible sólo en CD-ROM).

Recommended INN: List 71 WHO Drug Information, Vol. 28, No. 1, 2014
72
Latin, English, French, Spanish: Recommended INN DCI Recommandée DCI Recomendada
Chemical name or description; Molecular formula; Graphic formula Nom chimique ou description; Formule brute; Formule développée Nombre químico o descripción; Fórmula molecular; Fórmula desarrollada
abaloparatidum abaloparatide synthetic human parathyroid hormone (37-70) analogue:
C2.29-methyl[22-L-glutamic acid(F>E),23-L-leucine(F>L),25-L-glutamic acid(H>E),26-L-lysine(H>K),28-L-leucine(I>L),30-L-lysine(E>K), 31-L-leucine(I>L)]human parathyroid hormone-related protein-(1-34)-proteinamide
abaloparatide analogue de l'hormone parathyroïdienne humaine (37-70) synthétique: C2.29-méthyl[22-L-acide glutamique(F>E),23-L-leucine(F>L), 25-L-acide glutamique(H>E),26-L-lysine(H>K),28-L-leucine(I>L), 30-L-lysine(E>K),31-L-leucine(I>L)]protéine apparentée à l'hormone parathyroïdienne humaine-(1-34)-protéinamide
abaloparatida análogo sintético de la hormona paratiroidea humana (37-70): C2.29-metil[22-L-ácido glutámico(F>E),23-L-leucina(F>L),25-L-ácido glutámico(H>E),26-L-lisina(H>K),28-L-leucina(I>L), 30-L-lisina(E>K),31-L-leucina(I>L)]proteína relacionada con la hormona paratiroidea humana-(1-34)-proteinamida
C174H300N56O49
H2N
CH3HNH2
OH2N CO2H
CH3H3C
Sequence / Séquence / SecuenciaAVSEHQLLHDKGKSIQDLRRRELLEKLLXKLHTA 34
Modified residues / Résidus modifiés / Restos modificados
X29
2-methylAla
A34
Ala-NH2
abecomotidum abecomotide human insulin-like growth factor 2 mRNA-binding protein 3 (IMP-3,
hKOC)-(508-513)-peptide (part of the KH4 domain): L-lysyl-L-threonyl-L-valyl-L-asparaginyl-L-α-glutamyl-L-leucyl- L-glutaminyl-L-asparaginyl-L-leucine
abécomotide protéine 3, se liant à l'ARN messager, du facteur 2 de croissance humain analogue de l'insuline (IMP-3, hKOC)-(508-513)-peptide (partie du domaine KH4): L-lysyl-L-thréonyl-L-valyl-L-asparaginyl-L-α-glutamyl-L-leucyl- L-glutaminyl-L-asparaginyl-L-leucine
abecomotida proteína 3, que se une al ARN mensajero del factor 2 de crecimiento humano análogo de la insulina (IMP-3, hKOC)-(508-513)-péptido (parte del dominio KH4) : L-lisil-L-treonil-L-valil-L-asparaginil-L-α-glutamil-L-leucil-L-glutaminil- L-asparaginil-L-leucina
C45H79N13O16
Sequence / Séquence / SecuenciaKTVNELQNL 9

WHO Drug Information, Vol. 28, No. 1, 2014 Recommended INN: List 71
73
abituzumabum # abituzumab immunoglobulin G2-kappa, anti-[Homo sapiens ITGAV (integrin
alphaV, CD51)], humanized monoclonal antibody; gamma2 heavy chain (1-447) with IGHG1 hinge region [humanized VH (Homo sapiens IGHV1-46*01 (77.30%) -(IGHD)-IGHJ6*01) [8.8.11] (1-118) -Homo sapiens IGHG (IGHG2*03 CH1 (119-216), IGHG1 hinge C5>S (221) (217-231), IGHG2*03 CH2 F84.3>A (296), N84.4>Q (297) (232-340), CH3 (341-445), CHS (446-447)) (119-447)], (132-214')-disulfide with kappa light chain (1'-214') [humanized V-KAPPA (Homo sapiens IGKV1-33*01 (86.30%) -IGKJ2*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01 (108'-214')]; dimer (227-227":230-230")-bisdisulfide
abituzumab immunoglobuline G2-kappa, anti-[Homo sapiens ITGAV (intégrine alphaV, CD51)], anticorps monoclonal humanisé; chaîne lourde gamma2 (1-447) avec une région charnière IGHG1 [VH humanisé (Homo sapiens IGHV1-46*01 (77.30%) -(IGHD)-IGHJ6*01) [8.8.11] (1-118) -Homo sapiens IGHG (IGHG2*03 CH1 (119-216), IGHG1 charnière C5>S (221) (217-231), IGHG2*03 CH2 F84.3>A (296), N84.4>Q (297) (232-340), CH3 (341-445), CHS (446-447)) (119-447)], (132-214')-disulfure avec la chaîne légère kappa (1'-214') [V-KAPPA humanisé (Homo sapiens IGKV1-33*01 (86.30%) -IGKJ2*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01 (108'-214')]; dimère (227-227":230-230")-bisdisulfure
abituzumab inmunoglobulina G2-kappa, anti-[ ITGAV (integrina alfaV, CD51) de Homo sapiens], anticuerpo monoclonal humanizado; cadena pesada gamma2 (1-447) con una región bisagra GHG1 [VH humanizada (Homo sapiens IGHV1-46*01 (77.30%) -(IGHD)-IGHJ6*01) [8.8.11] (1-118) -Homo sapiens IGHG (IGHG2*03 CH1 (119-216), IGHG1 bisagra C5>S (221) (217-231), IGHG2*03 CH2 F84.3>A (296), N84.4>Q (297) (232-340), CH3 (341-445), CHS (446-447)) (119-447)], (132-214')-disulfuro con la cadena ligera kappa (1'-214') [V-KAPPA humanizada (Homo sapiens IGKV1-33*01 (86.30%) -IGKJ2*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01 (108'-214')]; dímero (227-227":230-230")-bisdisulfuro
Heavy chain / Chaîne lourde / Cadena pesada
QVQLQQSGGE LAKPGASVKV SCKASGYTFS SFWMHWVRQA PGQGLEWIGY 50INPRSGYTEY NEIFRDKATM TTDTSTSTAY MELSSLRSED TAVYYCASFL 100GRGAMDYWGQ GTTVTVSSAS TKGPSVFPLA PCSRSTSEST AALGCLVKDY 150FPEPVTVSWN SGALTSGVHT FPAVLQSSGL YSLSSVVTVP SSNFGTQTYT 200CNVDHKPSNT KVDKTVEPKS SDKTHTCPPC PAPPVAGPSV FLFPPKPKDT 250LMISRTPEVT CVVVDVSHED PEVQFNWYVD GVEVHNAKTK PREEQAQSTF 300RVVSVLTVVH QDWLNGKEYK CKVSNKGLPA PIEKTISKTK GQPREPQVYT 350LPPSREEMTK NQVSLTCLVK GFYPSDIAVE WESNGQPENN YKTTPPMLDS 400DGSFFLYSKL TVDKSRWQQG NVFSCSVMHE ALHNHYTQKS LSLSPGK 447
Light chain / Chaîne légère / Cadena ligeraDIQMTQSPSS LSASVGDRVT ITCRASQDIS NYLAWYQQKP GKAPKLLIYY 50TSKIHSGVPS RFSGSGSGTD YTFTISSLQP EDIATYYCQQ GNTFPYTFGQ 100GTKVEIKRTV AAPSVFIFPP SDEQLKSGTA SVVCLLNNFY PREAKVQWKV 150DNALQSGNSQ ESVTEQDSKD STYSLSSTLT LSKADYEKHK VYACEVTHQG 200LSSPVTKSFN RGEC 214
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H (C23-C104)22-96 145-201 261-321 367-425 22''-96''145''-201''261''-321''367''-425''Intra-L (C23-C104)23'-88' 134'-194' 23'''-88'''134'''-194'''Inter-H-L (CH1 10-CL 126)132-214'132''-214'''Inter-H-H (h 11, h 14)227-227''230-230''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónNone (owing to amino acid change: H CH2 N84.4>Q (297)), aucun (dû au changement d'acide aminé), ninguno (a causa del cambio de ácido amino)

Recommended INN: List 71 WHO Drug Information, Vol. 28, No. 1, 2014
74
acalisibum acalisib 6-fluoro-3-phenyl-2-[(1S)-1-(7H-purin-6-ylamino)ethyl]quinazolin-
4(3H)-one
acalisib 6-fluoro-3-phényl-2-[(1S)-1-(7H-purin-6-ylamino)éthyl]quinazolin-4(3H)-one
acalisib 6-fluoro-3-fenil-2-[(1S)-1-(7H-purin-6-ilamino)etil]quinazolin- 4(3H)-ona
C21H16FN7O
N
N
O
NH
F
N
N
NHNCH3H
aftobetinum aftobetin 2-[2-(2-methoxyethoxy)ethoxy]ethyl (2E)-2-cyano-3-[6-(piperidin-
1-yl)naphthalen-2-yl]prop-2-enoate
aftobétine (2E)-2-cyano-3-[6-(pipéridin-1-yl)naphtalén-2-yl]prop-2-énoate de 2-[2-(2-méthoxyéthoxy)éthoxy]éthyle
aftobetina (2E)-2-ciano-3-[6-(piperidin-1-il)naftalen-2-il]prop-2-enoato de 2-[2-(2-metoxietoxi)etoxi]etilo
C26H32N2O5
1208971-05-4
N
OO
O
CN
O
OCH3
alicdamotidum alicdamotide human kinetochore protein Nuf2 (cell division cycle-associated
protein 1)-(55-64)-peptide
alicdamotide protéine cinétochore Nuf2 humaine (protéine 1 associée au cycle de la division cellulaire)-(55-64)-peptide
alicdamotida proteína humana de cinetocoro Nuf2 (proteína 1 asociada al ciclo de división celular)-(55-64)-péptido
C54H80N14O13
Sequence / Séquence / SecuenciaVYGIRLEHF 9

WHO Drug Information, Vol. 28, No. 1, 2014 Recommended INN: List 71
75
anetumabum ravtansinum # anetumab ravtansine immunoglobulin G1-lambda2, anti-[Homo sapiens MSLN
(mesothelin, pre-pro-megakaryocyte-potentiating factor, megakaryocyte potentiating factor, MPF, CAK1)], Homo sapiens monoclonal antibody conjugated to maytansinoid DM4; gamma1 heavy chain (1-450) [Homo sapiens VH (IGHV5-51*01 (94.90%) -(IGHD)-IGHJ4*01) [8.8.13] (1-120) -IGHG1*01 (CH1 (121-218), hinge (219-233), CH2 (234-343), CH3 (344-448), CHS (449-450)) (121-450)], (223-216')-disulfide with lambda light chain (1'-217') [Homo sapiens V-LAMBDA (IGLV2-14*01 (95.60%) -IGLJ2*01) [9.3.11] (1'-111') -IGLC2*01 A43>G (155) (112'-217')]; dimer (229-229'':232-232'')-bisdisulfide; conjugated, on an average of 3 lysyl, to maytansinoid DM4 [N2'-deacetyl-N2'-(4-mercapto-4-methyl- 1-oxopentyl)-maytansine] via the reducible SPDB linker [N-succinimidyl 4-(2-pyridyldithio)butanoate] For the ravtansine part, please refer to the document "INN for pharmaceutical substances: Names for radicals, groups and others"*
anétumab ravtansine immunoglobuline G1-lambda2, anti-[Homo sapiens MSLN (mésothéline, facteur de potentialisation du pré-pro-mégacaryocyte, facteur de potentialisation des mégacaryocytes, MPF, CAK1)], Homo sapiens anticorps monoclonal conjugué au maytansinoïde DM4; chaîne lourde gamma1 (1-450) [Homo sapiens VH (IGHV5-51*01 (94.90%) -(IGHD)-IGHJ4*01) [8.8.13] (1-120) -IGHG1*01 (CH1 (121-218), charnière (219-233), CH2 (234-343), CH3 (344-448), CHS (449-450)) (121-450)], (223-216')-disulfure avec la chaîne légère lambda (1'-217') [Homo sapiens V-LAMBDA (IGLV2-14*01 (95.60%) -IGLJ2*01) [9.3.11] (1'-111') -IGLC2*01 A43>G (155) (112'-217')]; dimère 229-229'':232-232'')-bisdisulfure; conjugué, sur 3 lysyl en moyenne, au maytansinoïde DM4 [N2'-déacétyl-N2'-(4-mercapto- 4-méthyl-1-oxopentyl)-maytansine] via le linker SPDB réductible [4-(2-pyridyldithio)butanoate de N-succinimidyle] Pour la partie ravtansine, veuillez-vous référer au document "INN for pharmaceutical substances: Names for radicals, groups and others"*.
anetumab ravtansina inmunoglobulina G1-lambda2, anti-[MSLN de Homo sapiens (mesotelina, factor de potenciación del pre-pro-megacariocito, factor de potenciación de megacariocitos, MPF, CAK1)], anticuerpo monoclonal de Homo sapiens conjugado con el maitansinoide DM4; cadena pesada gamma1 (1-450) [Homo sapiens VH (IGHV5-51*01 (94.90%) -(IGHD)-IGHJ4*01) [8.8.13] (1-120) -IGHG1*01 (CH1 (121-218), bisagra (219-233), CH2 (234-343), CH3 (344-448), CHS (449-450)) (121-450)], (223-216')-disulfuro con la cadena ligera lambda (1'-217') [Homo sapiens V-LAMBDA (IGLV2-14*01 (95.60%) -IGLJ2*01) [9.3.11] (1'-111') -IGLC2*01 A43>G (155) (112'-217')]; dimère 229-229'':232-232'')-bisdisulfuro; conjugado, en tres restos lisil por término medio, con el maitansinoide DM4 [N2'-desacetil- N2'-(4-mercapto-4-metil-1-oxopentil)-maitansina] mediante el conector SPDB reducible [4-(2-piridilditio)butanoato de N-succinimidilo] La información sobre la ravtansina, la encontrarán en el documento "INN for pharmaceutical substances: Names for radicals, groups and others"*.

Recommended INN: List 71 WHO Drug Information, Vol. 28, No. 1, 2014
76
Heavy chain / Chaîne lourde / Cadena pesada
QVELVQSGAE VKKPGESLKI SCKGSGYSFT SYWIGWVRQA PGKGLEWMGI 50IDPGDSRTRY SPSFQGQVTI SADKSISTAY LQWSSLKASD TAMYYCARGQ 100LYGGTYMDGW GQGTLVTVSS ASTKGPSVFP LAPSSKSTSG GTAALGCLVK 150DYFPEPVTVS WNSGALTSGV HTFPAVLQSS GLYSLSSVVT VPSSSLGTQT 200YICNVNHKPS NTKVDKKVEP KSCDKTHTCP PCPAPELLGG PSVFLFPPKP 250KDTLMISRTP EVTCVVVDVS HEDPEVKFNW YVDGVEVHNA KTKPREEQYN 300STYRVVSVLT VLHQDWLNGK EYKCKVSNKA LPAPIEKTIS KAKGQPREPQ 350VYTLPPSRDE LTKNQVSLTC LVKGFYPSDI AVEWESNGQP ENNYKTTPPV 400LDSDGSFFLY SKLTVDKSRW QQGNVFSCSV MHEALHNHYT QKSLSLSPGK 450
Light chain / Chaîne légère / Cadena ligeraDIALTQPASV SGSPGQSITI SCTGTSSDIG GYNSVSWYQQ HPGKAPKLMI 50YGVNNRPSGV SNRFSGSKSG NTASLTISGL QAEDEADYYC SSYDIESATP 100VFGGGTKLTV LGQPKAAPSV TLFPPSSEEL QANKATLVCL ISDFYPGAVT 150VAWKGDSSPV KAGVETTTPS KQSNNKYAAS SYLSLTPEQW KSHRSYSCQV 200THEGSTVEKT VAPTECS 217
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H (C23-C104)22-96 147-203 264-324 370-428 22''-96''147''-203''264''-324''370''-428''Intra-L (C23-C104)22'-90' 139'-198' 22'''-90'''139'''-198'''Inter-H-L (h 5-CL 126)223-216' 223''-216'''Inter-H-H (h 11, h 14) 229-229''232-232''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:300, 300''
For the ravtansine part, please refer to the document "INN for pharmaceutical substances: Names for radicals,groups and others"* Pour la partie ravtansine, veuillez vous référer au document "INN for pharmaceutical substances: Names forradicals, groups and others"*.Para la fracción ravtansina, se pueden dirigir al documento "INN for pharmaceutical substances: Names for radicals, groups and others"*.
anifrolumabum # anifrolumab immunoglobulin G1-kappa, anti-[Homo sapiens IFNAR1 (interferon
alpha, beta and omega receptor 1, interferon alpha/beta receptor 1)], Homo sapiens monoclonal antibody; gamma1 heavy chain (1-447) [Homo sapiens VH (IGHV5-51*01 (93.90%) -(IGHD)-IGHJ2*01) [8.8.10] (1-117) -IGHG1*01 (CH1 (118-215), hinge (216-230), CH2 L1.3>F (234), L1.2>E (235), P116>S (331) (231-340), CH3 (341-445), CHS (446-447)) (118-447)], (220-215')-disulfide with kappa light chain (1'-215') [Homo sapiens V-KAPPA (IGKV3-20*01 (94.70%) -IGKJ5*01) [7.3.9] (1'-108') -IGKC*01 (109'-215')]; dimer (226-226'':229-229'')-bisdisulfide
anifrolumab immunoglobuline G1-kappa, anti-[Homo sapiens IFNAR1 (récepteur 1 de l'interféron alpha, bêta and oméga, récepteur de l'interféron alpha/bêta)], Homo sapiens anticorps monoclonal; chaîne lourde gamma1 (1-447) [Homo sapiens VH (IGHV5-51*01 (93.90%) -(IGHD)-IGHJ2*01) [8.8.10] (1-117) -IGHG1*01 (CH1 (118-215), charnière (216-230), CH2 L1.3>F (234), L1.2>E (235), P116>S (331) (231-340), CH3 (341-445), CHS (446-447)) (118-447)], (220-215')-disulfure avec la chaîne légère kappa (1'-215') [Homo sapiens V- KAPPA (IGKV3-20*01 (94.70%) -IGKJ5*01) [7.3.9] (1'-108') -IGKC*01 (109'-215')]; dimère (226-226'':229-229'')-bisdisulfure
anifrolumab inmunoglobulina G1-kappa, anti-[IFNAR1 de Homo sapiens (receptor 1 de interferón alfa, beta and omega, receptor de interferón alfa/beta)], anticuerpo monoclonal de Homo sapiens ; cadena pesada gamma1 (1-447) [Homo sapiens VH (IGHV5-51*01 (93.90%) -(IGHD)-IGHJ2*01) [8.8.10] (1-117) -IGHG1*01 (CH1 (118-215), bisagra (216-230), CH2 L1.3>F (234), L1.2>E (235), P116>S (331) (231-340), CH3 (341-445), CHS (446-447)) (118-447)], (220-215')-disulfuro con la cadena ligera kappa (1'-215') [Homo sapiens V- KAPPA (IGKV3-20*01 (94.70%) -IGKJ5*01) [7.3.9] (1'-108') -IGKC*01 (109'-215')]; dímero (226-226'':229-229'')-bisdisulfuro

WHO Drug Information, Vol. 28, No. 1, 2014 Recommended INN: List 71
77
Heavy chain / Chaîne lourde / Cadena pesada
EVQLVQSGAE VKKPGESLKI SCKGSGYIFT NYWIAWVRQM PGKGLESMGI 50IYPGDSDIRY SPSFQGQVTI SADKSITTAY LQWSSLKASD TAMYYCARHD 100IEGFDYWGRG TLVTVSSAST KGPSVFPLAP SSKSTSGGTA ALGCLVKDYF 150PEPVTVSWNS GALTSGVHTF PAVLQSSGLY SLSSVVTVPS SSLGTQTYIC 200NVNHKPSNTK VDKRVEPKSC DKTHTCPPCP APEFEGGPSV FLFPPKPKDT 250LMISRTPEVT CVVVDVSHED PEVKFNWYVD GVEVHNAKTK PREEQYNSTY 300RVVSVLTVLH QDWLNGKEYK CKVSNKALPA SIEKTISKAK GQPREPQVYT 350LPPSREEMTK NQVSLTCLVK GFYPSDIAVE WESNGQPENN YKTTPPVLDS 400DGSFFLYSKL TVDKSRWQQG NVFSCSVMHE ALHNHYTQKS LSLSPGK 447
Light chain / Chaîne légère / Cadena ligeraEIVLTQSPGT LSLSPGERAT LSCRASQSVS SSFFAWYQQK PGQAPRLLIY 50GASSRATGIP DRLSGSGSGT DFTLTITRLE PEDFAVYYCQ QYDSSAITFG 100QGTRLEIKRT VAAPSVFIFP PSDEQLKSGT ASVVCLLNNF YPREAKVQWK 150VDNALQSGNS QESVTEQDSK DSTYSLSSTL TLSKADYEKH KVYACEVTHQ 200GLSSPVTKSF NRGEC 215
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H (C23-C104)22-96 144-200 261-321 367-425 22''-96''144''-200''261''-321''367''-425''Intra-L (C23-C104)23'-89' 135'-195' 23'''-89'''135'''-195'''Inter-H-L (h 5-CL 126)220-215' 220''-215'''Inter-H-H (h 11, h 14) 226-226''229-229''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:297, 297''
artefenomelum artefenomel 4-{2-{4-(cis-dispiro[adamantane-2,3'-[1,2,4]trioxolane-
5',1''-cyclohexane]-4''-yl)phenoxy]ethyl}morpholine
artéfénomel 4-{2-{4-(cis-dispiro[adamantane-2,3'-[1,2,4]trioxolane- 5',1''-cyclohexane]-4''-yl)phénoxy]éthyl}morpholine
artefenomel 4-{2-{4-(cis-diespiro[adamantano-2,3'-[1,2,4]trioxolano- 5',1''-ciclohexano]-4''-il)fenoxi]etil}morfolina
C28H39NO5
HOO
O
ON
O
asapiprantum asapiprant 2-[2-(oxazol-2-yl)-5-(4-{4-[(propan-
2-yl)oxy]benzenesulfonyl}piperazin-1-yl)phenoxy]acetic acid
asapiprant acide 2-[2-(oxazol-2-yl)-5-(4-{4-[(propan- 2-yl)oxy]benzènesulfonyl}pipérazin-1-yl)phénoxy]acétique
asapiprant ácido 2-[2-(oxazol-2-il)-5-(4-{4-[(propan- 2-il)oxi]bencenosulfonil}piperazin-1-il)fenoxi]acético
C24H27N3O7S
O CO2HN
O
N
NS
OH3C
CH3
OO

Recommended INN: List 71 WHO Drug Information, Vol. 28, No. 1, 2014
78
axelopranum axelopran 3-{(1R,3r,5S)-8-(2-{cyclohexylmethyl[(2S)-2,3-
dihydroxypropanoyl]amino}ethyl)-8-azabicyclo[3.2.1]octan- 3-yl}benzamide
axélopran 3-[(1R,3r,5S)-8-(2-{(cyclohexylméthyl)[(2S)-2,3-dihydroxypropanoyl]amino}éthyl)-8-azabicyclo[3.2.1]octan- 3-yl]benzamide
axeloprán 3-{(1R,3r,5S)-8-(2-{ciclohexilmetil[(2S)-2,3-dihidroxipropanoil]amino}etil)-8-azabiciclo[3.2.1]octan-3-il}benzamida
C26H39N3O4
H2N
O NN OH
O
OHH
H
H
H
basimglurantum basimglurant 2-chloro-4-{2-[1-(4-fluorophenyl)-2,5-dimethyl-1H-imidazol-
4-yl]ethynyl}pyridine
basimglurant 2-chloro-4-{2-[1-(4-fluorophényl)-2,5-diméthyl-1H-imidazol- 4-yl]éthynyl}pyridine
basimglurant 2-cloro-4-{2-[1-(4-fluorofenil)-2,5-dimetil-1H-imidazol-4-il]etin- 1-il}piridina
C18H13ClFN3
N
NN
Cl
F
CH3
CH3
binimetinibum binimetinib 5-[(4-bromo-2-fluorophenyl)amino]-4-fluoro-N-(2-hydroxyethoxy)-
1-methyl-1H-benzimidazole-6-carboxamide
binimétinib 5-[(4-bromo-2-fluorophényl)amino]-4-fluoro-N-(2-hydroxyéthoxy)- 1-méthyl-1H-benzimidazole-6-carboxamide
binimetinib 5-[(4-bromo-2-fluorofenil)amino]-4-fluoro-N-(2-hidroxietoxi)-1-metil-1H-benzoimidazol-6-carboxamida

WHO Drug Information, Vol. 28, No. 1, 2014 Recommended INN: List 71
79
C17H15BrF2N4O3
NN CH3F
HN
F
Br
OHN
OOH
ceralifimodum ceralifimod 1-({6-[(2-methoxy-4-propylphenyl)methoxy]-1-methyl-
3,4-dihydronaphthalen-2-yl}methyl)azetidine-3-carboxylic acid
céralifimod acide 1-({6-[(2-méthoxy-4-propylphényl)méthoxy]-1-méthyl- 3,4-dihydronaphtalén-2-yl}méthyl)azétidine-3-carboxylique
ceralifimod ácido 1-({1-metil-6-[(2-metoxi-4-propilfenil)metoxi]- 3,4-dihidronaftalen-2-il}metil)azetidina-3-carboxílico
C27H33NO4
N
O CO2H
H3C OCH3
CH3
ceritinibum ceritinib 5-chloro-N2-{5-methyl-4-(piperidin-4-yl)-2-[(propan-2-yl)oxy]phenyl}-
N4-[2-(propane-2-sulfonyl)phenyl]pyrimidine-2,4-diamine
céritinib 5-chloro-N2-{5-méthyl-4-(pipéridin-4-yl)-2-[(propan-2-yl)oxy]phényl}-N4-[2-(propane-2-sulfonyl)phényl]pyrimidine-2,4-diamine
ceritinib 5-cloro-N2-{5-metil-4-(piperidin-4-il)-2-[(propan-2-il)oxi]fenil}- N4-[2-(propano-2-sulfonil)fenil]pirimidina-2,4-diamina
C28H36ClN5O3S
N
N
Cl
HN
HN
O
H3C CH3
H3C
S CH3
CH3O
O
HN
codrituzumabum # codrituzumab immunoglobulin G1-kappa, anti-[Homo sapiens GPC3 (glypican 3)],
humanized monoclonal antibody; gamma1 heavy chain (1-445) [humanized VH (Homo sapiens IGHV1-46*01 (82.70%) -(IGHD)-IGHJ5*02) [8.8.8] (1-115) -Homo sapiens IGHG1*01 (CH1 (116-213, hinge (214-228), CH2 (229-338), CH3 (339-443), CHS (444-445)) (116-445)], (218-219')-disulfide with kappa light chain (1'-219') [humanized V-KAPPA (Homo sapiens IGKV2-28*01 (86.00%) -IGKJ2*01) [11.3.9] (1'-112') -Homo sapiens IGKC*01 (113'-219')]; dimer (224-224":227-227")-bisdisulfide

Recommended INN: List 71 WHO Drug Information, Vol. 28, No. 1, 2014
80
codrituzumab immunoglobuline G1-kappa, anti-[Homo sapiens GPC3 (glypicane
3)], anticorps monoclonal humanisé; chaîne lourde gamma1 (1-445) [VH humanisé (Homo sapiens (Homo sapiens IGHV1-46*01 (82.70%) -(IGHD)-IGHJ5*02) [8.8.8] (1-115) -Homo sapiens IGHG1*01 (CH1 (116-213, charnière (214-228), CH2 (229-338), CH3 (339-443), CHS (444-445)) (116-445)], (218-219')-disulfure avec la chaîne légère kappa (1'-219') [V-KAPPA humanisé (Homo sapiens IGKV2-28*01 (86.00%) -IGKJ2*01) [11.3.9] (1'-112') -Homo sapiens IGKC*01 (113'-219')]; dimère (224-224":227-227")-bisdisulfure
codrituzumab inmunoglobulina G1-kappa, anti-[GPC3 (glipicano 3) de Homo sapiens], anticuerpo monoclonal humanizado; cadena pesada gamma1 (1-445) [VH humanizado (Homo sapiens (Homo sapiens IGHV1-46*01 (82.70%) -(IGHD)-IGHJ5*02) [8.8.8] (1-115) -Homo sapiens IGHG1*01 (CH1 (116-213, bisagra (214-228), CH2 (229-338), CH3 (339-443), CHS (444-445)) (116-445)], (218-219')-disulfuro con la cadena ligera kappa (1'-219') [V-KAPPA humanizado (Homo sapiens IGKV2-28*01 (86.00%) -IGKJ2*01) [11.3.9] (1'-112') -Homo sapiens IGKC*01 (113'-219')];dímero (224-224":227-227")-bisdisulfuro
Heavy chain / Chaîne lourde / Cadena pesada
QVQLVQSGAE VKKPGASVKV SCKASGYTFT DYEMHWVRQA PGQGLEWMGA 50LDPKTGDTAY SQKFKGRVTL TADKSTSTAY MELSSLTSED TAVYYCTRFY 100SYTYWGQGTL VTVSSASTKG PSVFPLAPSS KSTSGGTAAL GCLVKDYFPE 150PVTVSWNSGA LTSGVHTFPA VLQSSGLYSL SSVVTVPSSS LGTQTYICNV 200NHKPSNTKVD KKVEPKSCDK THTCPPCPAP ELLGGPSVFL FPPKPKDTLM 250ISRTPEVTCV VVDVSHEDPE VKFNWYVDGV EVHNAKTKPR EEQYNSTYRV 300VSVLTVLHQD WLNGKEYKCK VSNKALPAPI EKTISKAKGQ PREPQVYTLP 350PSRDELTKNQ VSLTCLVKGF YPSDIAVEWE SNGQPENNYK TTPPVLDSDG 400SFFLYSKLTV DKSRWQQGNV FSCSVMHEAL HNHYTQKSLS LSPGK 445
Light chain / Chaîne légère / Cadena ligeraDVVMTQSPLS LPVTPGEPAS ISCRSSQSLV HSNRNTYLHW YLQKPGQSPQ 50LLIYKVSNRF SGVPDRFSGS GSGTDFTLKI SRVEAEDVGV YYCSQNTHVP 100PTFGQGTKLE IKRTVAAPSV FIFPPSDEQL KSGTASVVCL LNNFYPREAK 150VQWKVDNALQ SGNSQESVTE QDSKDSTYSL SSTLTLSKAD YEKHKVYACE 200VTHQGLSSPV TKSFNRGEC 219
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H (C23-C104)22-96 142-198 259-319 365-423 22''-96''142''-198''259''-319''365''-423''Intra-L (C23-C104)23'-93' 139'-199' 23'''-93'''139'''-199'''Inter-H-L (h 5-CL 126)218-219' 218''-219'''Inter-H-H (h 11, h 14) 224-224''227-227''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:295, 295''
coltuximabum ravtansinum # coltuximab ravtansine immunoglobulin G1-kappa, anti-[Homo sapiens CD19 (B lymphocyte
surface antigen B4, Leu-12)], chimeric monoclonal antibody conjugated to maytansinoid DM4; gamma1 heavy chain (1-450) [Mus musculus VH (IGHV1-69*02 -(IGHD)-IGHJ4*01) [8.8.13] (1-120) -Homo sapiens IGHG1*01 (CH1 (121-218), hinge (219-233), CH2 (234-343), CH3 (344-448), CHS (449-450)) (121-450)], (223-211')-disulfide with kappa light chain (1'-211') [Mus musculus V-KAPPA (IGKV4-70*01 -IGKJ1*01) [5.3.7] (1'-104') -Homo sapiens IGKC*01 (105'-211')]; dimer (229-229'':232-232'')-bisdisulfide; conjugated, on an average of 3 to 4 lysyl, to maytansinoid DM4 [N2'-deacetyl-N2'-(4-mercapto-4-methyl- 1-oxopentyl)-maytansine] via the reducible SPDB linker [N-succinimidyl 4-(2-pyridyldithio)butanoate] For the ravtansine part, please refer to the document "INN for pharmaceutical substances: Names for radicals, groups and others"*

WHO Drug Information, Vol. 28, No. 1, 2014 Recommended INN: List 71
81
coltuximab ravtansine immunoglobuline G1-kappa, anti-[Homo sapiens CD19 (antigène de surface B4 des lymphocytes B, Leu-12)], anticorps monoclonal chimérique conjugué au maytansinoïde DM4; chaîne lourde gamma1 (1-450) [Mus musculus VH (IGHV1-69*02 -(IGHD)-IGHJ4*01) [8.8.13] (1-120) -Homo sapiens IGHG1*01 (CH1 (121-218), charnière (219-233), CH2 (234-343), CH3 (344-448), CHS (449-450)) (121-450)], (223-211')-disulfure avec la chaîne légère kappa (1'-211') [Mus musculus V-KAPPA (IGKV4-70*01 -IGKJ1*01) [5.3.7] (1'-104') -Homo sapiens IGKC*01 (105'-211')]; dimère (229-229'':232-232'')-bisdisulfure; conjugué, sur 3 à 4 lysyl en moyenne, au maytansinoïde DM4 [N2'-déacétyl-N2'-(4-mercapto- 4-méthyl-1-oxopentyl)-maytansine] via le linker SPDB réductible [4-(2-pyridyldithio)butanoate de N-succinimidyle] Pour la partie ravtansine, veuillez-vous référer au document "INN for pharmaceutical substances: Names for radicals, groups and others"*.
coltuximab ravtansina inmunoglobulina G1-kappa, anti-[CD19 de Homo sapiens (antígeno de superficie B4 de los linfocitos B, Leu-12)], anticuerpo monoclonal quimérico conjugado con el maitansinoide DM4; cadena pesada gamma1 (1-450) [Mus musculus VH (IGHV1-69*02 -(IGHD)-IGHJ4*01) [8.8.13] (1-120) -Homo sapiens IGHG1*01 (CH1 (121-218), bisagra (219-233), CH2 (234-343), CH3 (344-448), CHS (449-450)) (121-450)], (223-211')-disulfuro con la cadena ligera kappa (1'-211') [Mus musculus V-KAPPA (IGKV4-70*01 -IGKJ1*01) [5.3.7] (1'-104') -Homo sapiens IGKC*01 (105'-211')]; dímero (229-229'':232-232'')-bisdisulfuro;conjugado en 3 -4 restos lisil por término medio, con el maitansinoide DM4 [N2'-desacetil-N2'-(4-mercapto- 4-metil-1-oxopentil)-maitansina] mediante un conector SPDB reducible [4-(2-piridilditio)butanoato de N-succinimidilo] La información sobre la ravtansina, la encontrarán en el documento "INN for pharmaceutical substances: Names for radicals, groups and others"*.
Heavy chain / Chaîne lourde / Cadena pesada
QVQLVQPGAE VVKPGASVKL SCKTSGYTFT SNWMHWVKQA PGQGLEWIGE 50IDPSDSYTNY NQNFQGKAKL TVDKSTSTAY MEVSSLRSDD TAVYYCARGS 100NPYYYAMDYW GQGTSVTVSS ASTKGPSVFP LAPSSKSTSG GTAALGCLVK 150DYFPEPVTVS WNSGALTSGV HTFPAVLQSS GLYSLSSVVT VPSSSLGTQT 200YICNVNHKPS NTKVDKKVEP KSCDKTHTCP PCPAPELLGG PSVFLFPPKP 250KDTLMISRTP EVTCVVVDVS HEDPEVKFNW YVDGVEVHNA KTKPREEQYN 300STYRVVSVLT VLHQDWLNGK EYKCKVSNKA LPAPIEKTIS KAKGQPREPQ 350VYTLPPSRDE LTKNQVSLTC LVKGFYPSDI AVEWESNGQP ENNYKTTPPV 400LDSDGSFFLY SKLTVDKSRW QQGNVFSCSV MHEALHNHYT QKSLSLSPGK 450
Light chain / Chaîne légère / Cadena ligeraEIVLTQSPAI MSASPGERVT MTCSASSGVN YMHWYQQKPG TSPRRWIYDT 50SKLASGVPAR FSGSGSGTDY SLTISSMEPE DAATYYCHQR GSYTFGGGTK 100LEIKRTVAAP SVFIFPPSDE QLKSGTASVV CLLNNFYPRE AKVQWKVDNA 150LQSGNSQESV TEQDSKDSTY SLSSTLTLSK ADYEKHKVYA CEVTHQGLSS 200PVTKSFNRGE C 211
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H (C23-C104)22-96 147-203 264-324 370-428 22''-96''147''-203''264''-324''370''-428''Intra-L (C23-C104)23'-87' 131'-191' 23'''-87'''131'''-191'''Inter-H-L (h 5-CL 126)223-211' 223''-211'''Inter-H-H (h 11, h 14) 229-229''232-232''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:300, 300''For the ravtansine part, please refer to the document "INN for pharmaceutical substances: Names for radicals, groups and others"* Pour la partie ravtansine, veuillez vous référer au document "INN for pharmaceuticalsubstances: Names for radicals, groups and others"*.Para la fracción ravtansina, se pueden dirigir al documento "INN for pharmaceutical substances: Names for radicals, groups and others"*.

Recommended INN: List 71 WHO Drug Information, Vol. 28, No. 1, 2014
82
damoctocogum alfa pegolum # damoctocog alfa pegol recombinant DNA derived pegylated B domain deleted human blood
coagulation factor VIII (single protein chain) analogue, produced in BHK21 cells (glycoform alfa): des-(743-1636)-[1804-[S-(1-{3-[(3-{2,3-bis[ω-methoxypoly(oxyethylene)]propoxy}propyl)amino]-3-oxopropyl}- 2,5-dioxopyrrolidin-3-yl)-L-cysteine](K>C)]human coagulation factor VIII
damoctocog alfa pégol analogue du facteur de coagulation sanguine VIII humain amputé du domaine B (une seule chaîne protéique), produit par des cellules BHK21 à partir d'ADN recombinant (glycoforme alfa) : dès-(743-1636)-[1804-[S-(1-{3-[(3-{2,3-bis[ω-méthoxypoly(oxyéthylène)]propoxy}propyl)amino]-3-oxopropyl}- 2,5-dioxopyrrolidin-3-yl)-L-cystéine](K>C)]facteur VIII de coagulation humain
damoctocog alfa pegol análogo del factor VIII de coagulación humano privado del domanio B (una sola cadena proteica), producido por células BHK21 a partir de ADN recombinante (glicoforma alfa) : des-(743-1636)-[1804-[S-(1-{3-[(3-{2,3-bis[ω-metoxipoli(oxietileno)]propoxi}propil)amino]-3-oxopropil}- 2,5-dioxopirrolidin-3-il)-L-cisteina](K>C)]factor VIII de coagulación humano
N S
H2N CO2H
O
OH
HHN
O
n
O
O
O
H3CO
H3COn
CO2H
NH2HO
SHO
O O
Y346 , 718 , 719 , 723 , 1664 , 1680
O-sulfoTyr
C1804
S-(pegol)Cys
Glycosylation sites / Sites de glycosylation / Posiciones de glicosilaciónAsn-41Asn-239Asn-1810Asn-2118
Single chain protein / Protéine monocaténaire / Proteína monocatenaria (1438 AA)ATRRYYLGAVELSWDYMQSDLGELPVDARFPPRVPKSFPFNTSVVYKKTL50FVEFTDHLFNIAKPRPPWMGLLGPTIQAEVYDTVVITLKNMASHPVSLHA100VGVSYWKASEGAEYDDQTSQREKEDDKVFPGGSHTYVWQVLKENGPMASD150PLCLTYSYLSHVDLVKDLNSGLIGALLVCREGSLAKEKTQTLHKFILLFA200VFDEGKSWHSETKNSLMQDRDAASARAWPKMHTVNGYVNRSLPGLIGCHR250KSVYWHVIGMGTTPEVHSIFLEGHTFLVRNHRQASLEISPITFLTAQTLL300MDLGQFLLFCHISSHQHDGMEAYVKVDSCPEEPQLRMKNNEEAEDYDDDL350TDSEMDVVRFDDDNSPSFIQIRSVAKKHPKTWVHYIAAEEEDWDYAPLVL400APDDRSYKSQYLNNGPQRIGRKYKKVRFMAYTDETFKTREAIQHESGILG450PLLYGEVGDTLLIIFKNQASRPYNIYPHGITDVRPLYSRRLPKGVKHLKD500FPILPGEIFKYKWTVTVEDGPTKSDPRCLTRYYSSFVNMERDLASGLIGP550LLICYKESVDQRGNQIMSDKRNVILFSVFDENRSWYLTENIQRFLPNPAG600VQLEDPEFQASNIMHSINGYVFDSLQLSVCLHEVAYWYILSIGAQTDFLS650VFFSGYTFKHKMVYEDTLTLFPFSGETVFMSMENPGLWIL GCHNSDFRNR700GMTALLKVSSCDKNTGDYYEDSYEDISAYLLSKNNAIEPRSF 742 SQNPPVLKRHQREI1650TRTTLQSDQEEIDYDDTISVEMKKEDFDIYDEDENQSPRSFQKKTRHYFI1700AAVERLWDYGMSSSPHVLRNRAQSGSVPQFKKVVFQEFTDGSFTQPLYRG1750ELNEHLGLLGPYIRAEVEDNIMVTFRNQASRPYSFYSSLISYEEDQRQGA1800EPRCNFVKPNETKTYFWKVQHHMAPTKDEFDCKAWAYFSDVDLEKDVHSG1850LIGPLLVCHTNTLNPAHGRQVTVQEFALFFTIFDETKSWYFTENMERNCR1900APCNIQMEDPTFKENYRFHAINGYIMDTLPGLVMAQDQRIRWYLLSMGSN1950ENIHSIHFSGHVFTVRKKEEYKMALYNLYPGVFETVEMLPSKAGIWRVEC2000LIGEHLHAGMSTLFLVYSNKCQTPLGMASGHIRDFQITASGQYGQWAPKL2050ARLHYSGSINAWSTKEPFSWIKVDLLAPMIIHGIKTQGARQKFSSLYISQ2100FIIMYSLDGKKWQTYRGNSTGTLMVFFGNVDSSGIKHNIFNPPIIA RYIR2150LHPTHYSIRSTLRMELMGCDLNSCSMPLGMESKAISDAQITASSYFTNMF2200ATWSPSKARLHLQGRSNAWRPQVNNPKEWLQVDFQKTMKVTGVTTQGVKS2250LLTSMYVKEFLISSSQDGHQWTLFFQNGKVKVFQGNQDSFTPVVNSLDPP2300LLTRYLRIHPQSWVHQIALRMEVLGCEAQDLY 2332
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuro153-179248-329528-554630-7111832-18581899-19032021-21692174-2326
Modified residues / Résidus modifiés / Restos modificados

WHO Drug Information, Vol. 28, No. 1, 2014 Recommended INN: List 71
83
dasabuvirum dasabuvir N-(6-{3-tert-butyl-5-[2,4-dioxo-3,4-dihydropyrimidin-1(2H)-yl]-
2-methoxyphenyl}naphthalen-2-yl)methanesulfonamide
dasabuvir N-(6-{3-tert-butyl-5-[2,4-dioxo-3,4-dihydropyrimidin-1(2H)-yl]- 2-méthoxyphényl}naphtalén-2-yl)méthanesulfonamide
dasabuvir N-(6-{3-terc-butil-5-[2,4-dioxo-3,4-dihidropirimidin-1(2H)-il]- 2-metoxifenil}naftalen-2-il)metanosulfonamida
C26H27N3O5S
HN
SCH3
OCH3
H3C
NHN O O
CH3
CH3
O
O
decoglurantum decoglurant 5-[2-[7-(trifluoromethyl)-5-[4-(trifluoromethyl)phenyl]pyrazolo[1,5-
a]pyrimidin-3-yl]ethynyl]pyridin-2-amine
décoglurant 5-(2-{7-(trifluorométhyl)-5-[4-(trifluorométhyl)phényl]pyrazolo[1,5-a]pyrimidin-3-yl}ethynyl)pyridin-2-amine
decoglurant 5-(2-{7-(trifluorometil)-5-[4-(trifluorometil)fenil]pirazolo[1,5-a]pirimidin-3-il}etinil)piridin-2-amina
C21H11F6N5
N
H2N
NN
N
CF3
CF3
dianexinum # dianexin recombinant DNA derived annexin A5 dimer covalently linked by a
14 residues peptide linker, produced in Escherichia coli (nonglycosylated): L-methionyl-human annexin A5 fusion protein with glycyl-L-seryl- L-leucyl-L-α-glutamyl-L-valyl-L-leucyl-L-phenylalanyl- L-glutaminylglycyl-L-prolyl-L-serylglycyl-L-lysyl-L-leucyl-human annexin A5
dianexine dimère de l'annexine A5 liées de façon covalente par une chaîne peptidique de 14 acides aminés, produit par Escherichia coli à partir d'ADN recombinant (non glycosylé) : L-méthionyl-annexine A5 humaine protéine de fusion avec la glycyl-L-séryl-L-leucyl-L-α-glutamyl-L-valyl-L-leucyl-L-phénylalanyl- L-glutaminylglycyl-L-prolyl-L-sérylglycyl-L-lysyl-L-leucyl-annexine A5 humaine

Recommended INN: List 71 WHO Drug Information, Vol. 28, No. 1, 2014
84
dianexina dímero de la anexina A5 covalentemente unido por una cadena peptídica de 14 aminoácidos, producido por Escherichia coli a partir de ADN recombinante (no glicosilado) : L-metionil-anexina A5 humana proteína de fusión con la glicil-L-seril-L-leucil-L-α-glutamil-L-valil-L-leucil-L-fenilalanil-L-glutaminilglicil- L-prolil-L-serilglicil-L-lisil-L-leucil-anexina A5 humana
H2N CO2H
HOPO
OHOHH2N CO2H
HNHH3C
O
K = N6-acetylLys70-76-79-97-101-403-409-412-430-434
Y = phosphoTyr94-427
Sequence / Séquence / SecuenciaMAQVLRGTVTDFPGFDERADAETLRKAMKGLGTDEESILTLLTSRSNAQR50QEISAAFKTLFGRDLLDDLKSELTGKFEKLIVALMKPSRLYDAYELKHAL100KGAGTNEKVLTEIIASRTPEELRAIKQVYEEEYGSSLEDDVVGDTSGYYQ150RMLVVLLQANRDPDAGIDEAQVEQDAQALFQAGELKWGTDEEKFITIFGT200RSVSHLRKVFDKYMTISGFQIEETIDRETSGNLEQLLLAVVKSIRSIPAY250LAETLYYAMKGAGTDDHTLIRVMVSRSEIDLFNIRKEFRKNFATSLYSMI300KGDTSGDYKKALLLLCGEDDGSLEVLFQGPSGKLAQVLRGTVTDFPGFDE350RADAETLRKAMKGLGTDEESILTLLTSRSNAQRQEISAAFKTLFGRDLLD400DLKSELTGKFEKLIVALMKPSRLYDAYELKHALKGAGTNEKVLTEIIASR450TPEELRAIKQVYEEEYGSSLEDDVVGDTSGYYQRMLVVLLQANRDPDAGI500DEAQVEQDAQALFQAGELKWGTDEEKFITIFGTRSVSHLRKVFDKYMTIS550GFQIEETIDRETSGNLEQLLLAVVKSIRSIPAYLAETLYYAMKGAGTDDH600TLIRVMVSRSEIDLFNIRKEFRKNFATSLYSMIKGDTSGDYKKALLLLCG650EDD 653
Modified residues / Résidus modifiés / Restos modificados
dinutuximabum # dinutuximab immunoglobulin G1-kappa, anti-ganglioside GD2, chimeric
monoclonal antibody; gamma1 heavy chain (1-443) [Mus musculus VH (IGHV1S135*01 -(IGHD)-IGHJ4*01) [8.8.6] (1-113) -Homo sapiens IGHG1*03 (CH1 (114-211), hinge (212-226), CH2 (227-336), CH3 (337-441), CHS (442-443)) (114-443)], (216-220')-disulfide with kappa light chain (1'-220') [Mus musculus V-KAPPA (IGKV1-110*01 -IGKJ5*01) 11.3.10] (1'-113') -Homo sapiens IGKC*01 (114'-220')]; dimer (222-222'':225-225'')-bisdisulfide
dinutuximab immunoglobuline G1-kappa, anti-ganglioside GD2, anticorps monoclonal chimérique; chaîne lourde gamma1 (1-443) [Mus musculus VH (IGHV1S135*01 -(IGHD)-IGHJ4*01) [8.8.6] (1-113) -Homo sapiens IGHG1*03 (CH1 (114-222), charnière (223-237), CH2 (238-347), CH3 (348-452), CHS (453-454)) (125-454)], (216-220')-disulfure avec la chaîne légère kappa (1'-220') [Mus musculus V-KAPPA (IGKV1-110*01 -IGKJ5*01) 11.3.10] (1'-113') -Homo sapiens IGKC*01 (114'-220')]; dimère (222-222'':225-225'')-bisdisulfure
dinutuximab inmunoglobulina G1-kappa, anti-gangliósido GD2, anticuerpo monoclonal quimérico; cadena pesada gamma1 (1-443) [Mus musculus VH (IGHV1S135*01 -(IGHD)-IGHJ4*01) [8.8.6] (1-113) -Homo sapiens IGHG1*03 (CH1 (114-222), bisagra (223-237), CH2 (238-347), CH3 (348-452), CHS (453-454)) (125-454)], (216-220')-disulfuro con la cadena ligera kappa (1'-220') [Mus musculus V-KAPPA (IGKV1-110*01 -IGKJ5*01) 11.3.10] (1'-113') -Homo sapiens IGKC*01 (114'-220')]; dímero(222-222'':225-225'')-bisdisulfuro

WHO Drug Information, Vol. 28, No. 1, 2014 Recommended INN: List 71
85
Heavy chain / Chaîne lourde / Cadena pesada
EVQLLQSGPE LEKPGASVMI SCKASGSSFT GYNMNWVRQN IGKSLEWIGA 50IDPYYGGTSY NQKFKGRATL TVDKSSSTAY MHLKSLTSED SAVYYCVSGM 100EYWGQGTSVT VSSASTKGPS VFPLAPSSKS TSGGTAALGC LVKDYFPEPV 150TVSWNSGALT SGVHTFPAVL QSSGLYSLSS VVTVPSSSLG TQTYICNVNH 200KPSNTKVDKR VEPKSCDKTH TCPPCPAPEL LGGPSVFLFP PKPKDTLMIS 250RTPEVTCVVV DVSHEDPEVK FNWYVDGVEV HNAKTKPREE QYNSTYRVVS 300VLTVLHQDWL NGKEYKCKVS NKALPAPIEK TISKAKGQPR EPQVYTLPPS 350REEMTKNQVS LTCLVKGFYP SDIAVEWESN GQPENNYKTT PPVLDSDGSF 400FLYSKLTVDK SRWQQGNVFS CSVMHEALHN HYTQKSLSLS PGK 443
Light chain / Chaîne légère / Cadena ligeraEIVMTQSPAT LSVSPGERAT LSCRSSQSLV HRNGNTYLHW YLQKPGQSPK 50LLIHKVSNRF SGVPDRFSGS GSGTDFTLKI SRVEAEDLGV YFCSQSTHVP 100PLTFGAGTKL ELKRTVAAPS VFIFPPSDEQ LKSGTASVVC LLNNFYPREA 150KVQWKVDNAL QSGNSQESVT EQDSKDSTYS LSSTLTLSKA DYEKHKVYAC 200EVTHQGLSSP VTKSFNRGEC 220
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H (C23-C104)22-96 140-196 257-317 363-421 22''-96''140''-196''257''-317''363''-421''Intra-L (C23-C104)23'-93' 140'-200' 23'''-93'''140'''-200'''Inter-H-L (h 5-CL 126) 216-220' 216''-220'''Inter-H-H (h 11-h 14) 222-222''225-225''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:293, 293''
doravirinum doravirine 3-chloro-5-({1-[(4-methyl-5-oxo-4,5-dihydro-1H-1,2,4-triazol-
3-yl)methyl]-2-oxo-4-(trifluoromethyl)-1,2-dihydropyridin- 3-yl}oxy)benzonitrile
doravirine 3-chloro-5-({1-[(4-méthyl-5-oxo-4,5-dihydro-1H-1,2,4-triazol- 3-yl)méthyl]-2-oxo-4-(trifluorométhyl)-1,2-dihydropyridin- 3-yl}oxy)benzonitrile
doravirina 3-cloro-5-({1-[(4-metil-5-oxo-4,5-dihidro-1H-1,2,4-triazol-3-il)metil]- 2-oxo-4-(trifluorometil)-1,2-dihidropiridin-3-il}oxi)benzonitrilo
C17H11ClF3N5O3
N
O
O
CF3
NHN
N
OCH3
CN
Cl
eldelumabum # eldelumab immunoglobulin G1-kappa, anti-[Homo sapiens CXCL10 (chemokine
C-X-C motif ligand 10, 10 kDa interferon gamma-induced protein gamma-IP10, IP-10, INP10, small inducible cytokine B10, SCYB10)], Homo sapiens monoclonal antibody;gamma1 heavy chain (1-454) [Homo sapiens VH (IGHV3-33*01 (89.80%) -(IGHD)-IGHJ6*01) [8.8.17] (1-124) -IGHG1*01 (CH1 (125-222), hinge (223-237), CH2 (238-347), CH3 (348-452), CHS (453-454)) (125-454)], (227-216')-disulfide with kappa light chain (1'-216') [Homo sapiens V-KAPPA (IGKV3-20*01 (100.00%) -IGKJ3*01) [7.3.10] (1'-109') -IGKC*01 (110'-216')]; dimer (233-233'':236-236'')-bisdisulfide

Recommended INN: List 71 WHO Drug Information, Vol. 28, No. 1, 2014
86
eldélumab immunoglobuline G1-kappa, anti-[Homo sapiens CXCL10 (chémokine C-X-C motif ligand 10, protéine gamma-IP10 de 10 kDa induite par l'interféron gamma, IP-10, INP10, petite cytokine inductible B10, SCYB10)], Homo sapiens anticorps monoclonal; chaîne lourde gamma1 (1-454) [Homo sapiens VH (IGHV3-33*01 (89.80%) -(IGHD)-IGHJ6*01) [8.8.17] (1-124) -IGHG1*01 (CH1 (125-222), charnière (223-237), CH2 (238-347), CH3 (348-452), CHS (453-454)) (125-454)], (227-216')-disulfure avec la chaîne légère kappa (1'-216') [Homo sapiens V- KAPPA (IGKV3-20*01 (100.00%) -IGKJ3*01) [7.3.10] (1'-109') -IGKC*01 (110'-216')]; dimère (233-233'':236-236'')-bisdisulfure
eldelumab inmunoglobulina G1-kappa, anti-[CXCL10 de Homo sapiens (quimioquina C-X-C motivo ligando 10, proteína gamma-IP10 de 10 kDa inducida por el interferón gamma, IP-10, INP10, pequeña citoquina inducible B10, SCYB10)], anticuerpo monoclonal de Homo sapiens; cadena pesada gamma1 (1-454) [Homo sapiens VH (IGHV3-33*01 (89.80%) -(IGHD)-IGHJ6*01) [8.8.17] (1-124) -IGHG1*01 (CH1 (125-222), bisagra (223-237), CH2 (238-347), CH3 (348-452), CHS (453-454)) (125-454)], (227-216')-disulfuro con la cadena ligera kappa (1'-216') [Homo sapiens V-KAPPA (IGKV3-20*01 (100.00%) -IGKJ3*01) [7.3.10] (1'-109') -IGKC*01 (110'-216')]; dimero (233-233'':236-236'')-bisdisulfuro
Heavy chain / Chaîne lourde / Cadena pesada
QMQLVESGGG VVQPGRSLRL SCTASGFTFS NNGMHWVRQA PGKGLEWVAV 50IWFDGMNKFY VDSVKGRFTI SRDNSKNTLY LEMNSLRAED TAIYYCAREG 100DGSGIYYYYG MDVWGQGTTV TVSSASTKGP SVFPLAPSSK STSGGTAALG 150CLVKDYFPEP VTVSWNSGAL TSGVHTFPAV LQSSGLYSLS SVVTVPSSSL 200GTQTYICNVN HKPSNTKVDK RVEPKSCDKT HTCPPCPAPE LLGGPSVFLF 250PPKPKDTLMI SRTPEVTCVV VDVSHEDPEV KFNWYVDGVE VHNAKTKPRE 300EQYNSTYRVV SVLTVLHQDW LNGKEYKCKV SNKALPAPIE KTISKAKGQP 350REPQVYTLPP SREEMTKNQV SLTCLVKGFY PSDIAVEWES NGQPENNYKT 400TPPVLDSDGS FFLYSKLTVD KSRWQQGNVF SCSVMHEALH NHYTQKSLSL 450SPGK 454
Light chain / Chaîne légère / Cadena ligeraEIVLTQSPGT LSLSPGERAT LSCRASQSVS SSYLAWYQQK PGQAPRLLIY 50GASSRATGIP DRFSGSGSGT DFTLTISRLE PEDFAVYYCQ QYGSSPIFTF 100GPGTKVDIKR TVAAPSVFIF PPSDEQLKSG TASVVCLLNN FYPREAKVQW 150KVDNALQSGN SQESVTEQDS KDSTYSLSST LTLSKADYEK HKVYACEVTH 200QGLSSPVTKS FNRGEC 216
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H (C23-C104)22-96 151-207 268-328 374-432 22''-96''151''-207''268''-328''374''-432''Intra-L (C23-C104)23'-89' 136'-196' 23'''-89'''136'''-196'''Inter-H-L (h 5-CL 126)227-216' 227''-216'''Inter-H-H (h 11, h 14) 233-233''236-236''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:304, 304''
eluxadolinum eluxadoline 5-({[(2S)-2-amino-3-(4-carbamoyl-
2,6-dimethylphenyl)propanoyl][(1S)-1-(4-phenyl-1H-imidazol- 2-yl)ethyl]amino}methyl)-2-methoxybenzoic acid
éluxadoline acide 5-({[(2S)-2-amino-3-(4-carbamoyl- 2,6-diméthylphényl)propanoyl][(1S)-1-(4-phényl-1H-imidazol- 2-yl)éthyl]amino}méthyl)-2-méthoxybenzoïque
eluxadolina ácido 5-({[(2S)-2-amino-3-(4-carbamoil- 2,6-dimetilfenil)propanoil][(1S)-1-(4-fenil-1H-imidazol- 2-il)etil]amino}metil)-2-metoxibenzoico

WHO Drug Information, Vol. 28, No. 1, 2014 Recommended INN: List 71
87
C32H35N5O5
NH NH2
O
CH3
CH3
H2N
O
CO2H
OCH3
NHN
HCH3
encorafenibum encorafenib methyl N-{(2S)-1-[(4-{3-[5-chloro-2-fluoro-
3-(methanesulfonamido)phenyl]}-1-(propan-2-yl)-1H-pyrazol- 4-yl}pyrimidin-2-yl)amino]propan-2-yl}carbamate
encorafénib N-{(2S)-1-[(4-{3-[5-chloro-2-fluoro-3-(méthanesulfonamido)phényl]}-1-(propan-2-yl)-1H-pyrazol-4-yl}pyrimidin-2-yl)amino]propan- 2-yl}carbamate de méthyle
encorafenib N-{(2S)-1-[(4-{3-[5-cloro-2-fluoro-3-(metanosulfonamido)fenil]}- 1-(propan-2-il)-1H-pirazol-4-il}pirimidin-2-il)amino]propan- 2-il}carbamato de metilo
C22H27ClFN7O4S
NH
SH3C
N N
Cl
F
H3C
CH3
OON
NHN
NH
OCH3
OCH3H
enfortumabum vedotinum # enfortumab vedotin immunoglobulin G1-kappa, anti-[Homo sapiens PVRL4 (poliovirus
receptor-related 4, nectin-4, nectin 4, PPR4, LNIR], Homo sapiens monoclonal antibody conjugated to auristatin E; gamma1 heavy chain (1-447) [Homo sapiens VH (IGHV3-48*02 (98.00%) -(IGHD)-IGHJ6*01) [8.8.10] (1-117) -IGHG1*03 (CH1 (118-215), hinge (216-230), CH2 (231-340), CH3 (341-445), CHS (446-447)) (118-447)], (220-214')-disulfide with kappa light chain (1'-214') [Homo sapiens V-KAPPA (IGKV1-12*01 (96.80%) -IGKJ4*01) [6.3.9] (1'-107') -IGKC*01 (108'-214')]; dimer (226-226'':229-229'')-bisdisulfide; conjugated, on an average of 3 to 4 cysteinyl, to monomethylauristatin E (MMAE), via a cleavable maleimidecaproyl-valyl-citrullinyl-p-aminobenzylcarbamate (mc-val-cit-PABC) linker For the vedotin part, please refer to the document "INN for pharmaceutical substances: Names for radicals, groups and others"*.

Recommended INN: List 71 WHO Drug Information, Vol. 28, No. 1, 2014
88
enfortumab védotine immunoglobuline G1-kappa, anti-[Homo sapiens PVRL4 (membre 4 de la famille du récepteur du poliovirus, nectine-4, nectine 4, PPR4, LNIR], Homo sapiens anticorps monoclonal conjugué à l'auristatine E; chaîne lourde gamma1 (1-447) [Homo sapiens VH (IGHV3-48*02 (98.00%) -(IGHD)-IGHJ6*01) [8.8.10] (1-117) -IGHG1*03 (CH1 (118-215), charnière (216-230), CH2 (231-340), CH3 (341-445), CHS (446-447)) (118-447)], (220-214')-disulfure avec la chaîne légère kappa (1'-214') [Homo sapiens V- KAPPA (IGKV1-12*01 (96.80%) -IGKJ4*01) [6.3.9] (1'-107') -IGKC*01 (108'-214')]; dimère (226-226'':229-229'')-bisdisulfure; conjugué, sur 3 à 4 cystéinyl en moyenne, au monométhylauristatine E (MMAE), via un linker clivable maléimidecaproyl-valyl-citrullinyl-p-aminobenzylcarbamate (mc-val-cit-PABC) Pour la partie védotine, veuillez-vous référer au document "INN for pharmaceutical substances: Names for radicals, groups and others"*.
enfortumab vedotina inmunoglobulina G1-kappa, anti-[PVRL4 de Homo sapiens (miembro 4 de la familia del receptor de poliovirus, nectina-4, nectina 4, PPR4, LNIR], anticuerpo monoclonal de Homo sapiens conjugado con auristatina E; cadena pesada gamma1 (1-447) [Homo sapiens VH (IGHV3-48*02 (98.00%) -(IGHD)-IGHJ6*01) [8.8.10] (1-117) -IGHG1*03 (CH1 (118-215), bisagra(216-230), CH2 (231-340), CH3 (341-445), CHS (446-447)) (118-447)], (220-214')-disulfuro con la cadena ligera kappa (1'-214') [Homo sapiens V-KAPPA (IGKV1-12*01 (96.80%) -IGKJ4*01) [6.3.9] (1'-107') -IGKC*01 (108'-214')]; dímero (226-226'':229-229'')-bisdisulfuro; conjugado, en 3- 4 restos cisteinil por término medio, con monometilauristatinea E (MMAE), mediante un conector escindible maleimidocaproil-valil-citrulinil-p-aminobencilcarbamato (mc-val-cit-PABC) La información sobre la vedotina, la encontrarán en el documento "INN for pharmaceutical substances: Names for radicals, groups and others"*.
Heavy chain / Chaîne lourde / Cadena pesadaEVQLVESGGG LVQPGGSLRL SCAASGFTFS SYNMNWVRQA PGKGLEWVSY 50ISSSSSTIYY ADSVKGRFTI SRDNAKNSLS LQMNSLRDED TAVYYCARAY 100YYGMDVWGQG TTVTVSSAST KGPSVFPLAP SSKSTSGGTA ALGCLVKDYF 150PEPVTVSWNS GALTSGVHTF PAVLQSSGLY SLSSVVTVPS SSLGTQTYIC 200NVNHKPSNTK VDKRVEPKSC DKTHTCPPCP APELLGGPSV FLFPPKPKDT 250LMISRTPEVT CVVVDVSHED PEVKFNWYVD GVEVHNAKTK PREEQYNSTY 300RVVSVLTVLH QDWLNGKEYK CKVSNKALPA PIEKTISKAK GQPREPQVYT 350LPPSREEMTK NQVSLTCLVK GFYPSDIAVE WESNGQPENN YKTTPPVLDS 400DGSFFLYSKL TVDKSRWQQG NVFSCSVMHE ALHNHYTQKS LSLSPGK 447
Light chain / Chaîne légère / Cadena ligeraDIQMTQSPSS VSASVGDRVT ITCRASQGIS GWLAWYQQKP GKAPKFLIYA 50ASTLQSGVPS RFSGSGSGTD FTLTISSLQP EDFATYYCQQ ANSFPPTFGG 100GTKVEIKRTV AAPSVFIFPP SDEQLKSGTA SVVCLLNNFY PREAKVQWKV 150DNALQSGNSQ ESVTEQDSKD STYSLSSTLT LSKADYEKHK VYACEVTHQG 200LSSPVTKSFN RGEC 214
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H (C23-C104)22-96 144-200 261-321 367-425 22''-96''144''-200''261''-321''367''-425''Intra-L (C23-C104)23'-88' 134'-194' 23'''-88'''134'''-194'''Inter-H-L (h 5-CL 126) *220-214'220''-214'''Inter-H-H (h 11, h 14) *226-226''229-229''*Two or three of the inter-chain disulfide bridges are not present, an average of 3 to 4 cysteinyl being conjugated each to a drug linker.*Deux ou trois des ponts disulfures inter-chaînes ne sont pas présents, 3 à 4 cystéinyl en moyenne étant chacun conjugué à un linker-principe actif. *Faltan dos o tres puentes disulfuro inter-catenarios, una media de 3 a 4 cisteinil está conjugada a conectores de principio activo.
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:297, 297''
For the vedotin part, please refer to the document "INN for pharmaceutical substances:
Names for radicals, groups and others"*
Pour la partie védotine, veuillez vous référer au document "INN for pharmaceutical
substances: Names for radicals, groups and others"*.
Para la fracción vedotina, se pueden dirigir al documento "INN for pharmaceutical
substances: Names for radicals, groups and others"*.

WHO Drug Information, Vol. 28, No. 1, 2014 Recommended INN: List 71
89
fevipiprantum fevipiprant 2-(1-{[4-methanesulfonyl-2-(trifluoromethyl)phenyl]methyl}-2-methyl-
1H-pyrrolo[2,3-b]pyridin-3-yl)acetic acid
févipiprant acide 2-(1-{[4-méthanesulfonyl-2-(trifluorométhyl)phényl]méthyl}- 2-méthyl-1H-pyrrolo[2,3-b]pyridin-3-yl)acétique
fevipiprant ácido 2-(1-{[4-metanosulfonil-2-(trifluorometil)fenil]metil}-2-metil- 1H-pirrolo[2,3-b]piridin-3-il)acético
C19H17F3N2O4S
N NCH3
CO2H
SCH3
F3C O O
filanesibum filanesib (2S)-2-(3-aminopropyl)-5-(2,5-difluorophenyl)-N-methoxy-N-methyl-
2-phenyl-1,3,4-thiadiazole-3(2H)-carboxamide
filanésib (2S)-2-(3-aminopropyl)-5-(2,5-difluorophényl)-N-méthoxy-N-méthyl-2-phényl-1,3,4-thiadiazole-3(2H)-carboxamide
filanesib (2S)-2-(3-aminopropil)-5-(2,5-difluorofenil)-2-fenil-N-metil-N-metoxi- 1,3,4-tiadiazol-3(2H)-carboxamida
C20H22F2N4O2S
SN
NO
NH2
NH3C O
CH3
F
F
galunisertibum galunisertib 4-[2-(6-methylpyridin-2-yl)-5,6-dihydro-4H-pyrrolo[1,2-b]pyrazol-
3-yl]quinoline-6-carboxamide
galunisertib 4-[2-(6-méthylpyridin-2-yl)-5,6-dihydro-4H-pyrrolo[1,2-b]pyrazol- 3-yl]quinoléine-6-carboxamide
galunisertib 4-[2-(6-metilpiridin-2-il)-5,6-dihidro-4H-pirrolo[1,2-b]pirazol- 3-il]quinolina-6-carboxamida
C22H19N5O
N
H2N
O
N NN CH3

Recommended INN: List 71 WHO Drug Information, Vol. 28, No. 1, 2014
90
guselkumabum # guselkumab immunoglobulin G1-lambda2, anti-[Homo sapiens IL23 (interleukin
23, IL-23)], Homo sapiens monoclonal antibody; gamma1 heavy chain (1-446) [Homo sapiens VH (IGHV5-51*01 (93.90%) -(IGHD)-IGHJ3*01 M123>L (112)) [8.8.10] (1-117) -IGHG1*01 (CH1 (118-215), hinge (216-230), CH2 (231-340), CH3 (341-444), CHS (445-446)) (118-446)], (220-216')-disulfide with lambda light chain (1'-217') [Homo sapiens V-LAMBDA (IGLV1-40*01 (91.80%) -IGLJ2*01) [9.3.11] (1'-111') -IGLC2*01 (112'-217')]; dimer (226-226'':229-229'')-bisdisulfide
guselkumab immunoglobuline G1-lambda2, anti-[Homo sapiens IL23 (interleukine 23, IL-23)], Homo sapiens anticorps monoclonal; chaîne lourde gamma1 (1-446) [Homo sapiens VH (IGHV5-51*01 (93.90%) -(IGHD)-IGHJ3*01 M123>L (112)) [8.8.10] (1-117) -IGHG1*01 (CH1 (118-215), charnière (216-230), CH2 (231-340), CH3 (341-444), CHS (445-446)) (118-446)], (220-216')-disulfure avec la chaîne légère lambda (1'-217') [Homo sapiens V-LAMBDA (IGLV1-40*01 (91.80%) -IGLJ2*01) [9.3.11] (1'-111') -IGLC2*01 (112'-217')]; dimère (226-226'':229-229'')-bisdisulfure
guselkumab inmunoglobulina G1-lambda2, anti-[IL23 (interleukina 23, IL-23) de Homo sapiens], anticuerpo monoclonal de Homo sapiens; cadena pesada gamma1 (1-446) [Homo sapiens VH (IGHV5-51*01 (93.90%) -(IGHD)-IGHJ3*01 M123>L (112)) [8.8.10] (1-117) -IGHG1*01 (CH1 (118-215), bisagra (216-230), CH2 (231-340), CH3 (341-444), CHS (445-446)) (118-446)], (220-216')-disulfuro con la cadena ligera lambda (1'-217') [Homo sapiens V-LAMBDA (IGLV1-40*01 (91.80%) -IGLJ2*01) [9.3.11] (1'-111') -IGLC2*01 (112'-217')]; dímero (226-226'':229-229'')-bisdisulfuro
Heavy chain / Chaîne lourde / Cadena pesada
EVQLVQSGAE VKKPGESLKI SCKGSGYSFS NYWIGWVRQM PGKGLEWMGI 50IDPSNSYTRY SPSFQGQVTI SADKSISTAY LQWSSLKASD TAMYYCARWY 100YKPFDVWGQG TLVTVSSAST KGPSVFPLAP SSKSTSGGTA ALGCLVKDYF 150PEPVTVSWNS GALTSGVHTF PAVLQSSGLY SLSSVVTVPS SSLGTQTYIC 200NVNHKPSNTK VDKKVEPKSC DKTHTCPPCP APELLGGPSV FLFPPKPKDT 250LMISRTPEVT CVVVDVSHED PEVKFNWYVD GVEVHNAKTK PREEQYNSTY 300RVVSVLTVLH QDWLNGKEYK CKVSNKALPA PIEKTISKAK GQPREPQVYT 350LPPSRDELTK NQVSLTCLVK GFYPSDIAVE WESNGQPENN YKTTPPVLDS 400DGSFFLYSKL TVDKSRWQQG NVFSCSVMHE ALHNHYTQKS LSLSPG 446
Light chain / Chaîne légère / Cadena ligeraQSVLTQPPSV SGAPGQRVTI SCTGSSSNIG SGYDVHWYQQ LPGTAPKLLI 50YGNSKRPSGV PDRFSGSKSG TSASLAITGL QSEDEADYYC ASWTDGLSLV 100VFGGGTKLTV LGQPKAAPSV TLFPPSSEEL QANKATLVCL ISDFYPGAVT 150VAWKADSSPV KAGVETTTPS KQSNNKYAAS SYLSLTPEQW KSHRSYSCQV 200THEGSTVEKT VAPTECS 217
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H (C23-C104)22-96 144-200 261-321 367-425 22''-96''144''-200''261''-321''367''-425''Intra-L (C23-C104)22'-90' 139'-198' 22'''-90'''139'''-198'''Inter-H-L (h 5-CL 126)220-216' 220''-216'''Inter-H-H (h 11, h 14) 226-226''229-229''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:297, 297''
idarucizumabum # idarucizumab immunoglobulin Fab G1-kappa, anti-[dagibatran], humanized
monoclonal antibody; VH-(CH1-hinge) gamma1 heavy chain (1-225) [humanized VH (Homo sapiens IGHV4-59*01 (82.30%) -(IGHD)-IGHJ4*01) [8.7.16] (1-122) -Homo sapiens IGHG1*01 (CH1 (123-220), hinge 1-5 (221-225)) (123-225)], (225-219')-disulfide with kappa light chain (1'-219') [humanized V-KAPPA (Homo sapiens IGKV2-30*01 (88.00%) -IGKJ4*01) [11.3.9] (1'-112') -Homo sapiens IGKC*01 (113'-219')]

WHO Drug Information, Vol. 28, No. 1, 2014 Recommended INN: List 71
91
idarucizumab immunoglobuline Fab G1-kappa, anti-[dagibatran], anticorps monoclonal humanisé; chaîne lourde VH-(CH1-charnière) gamma1 (1-225) [VH humanisé (Homo sapiens IGHV4-59*01 (82.30%) -(IGHD)-IGHJ4*01) [8.7.16] (1-122) -Homo sapiens IGHG1*01 (CH1 (123-220), charnière 1-5 (221-225)) (123-225)], (225-219')-disulfure avec la chaîne légère kappa (1'-219') [V-KAPPA humanisé (Homo sapiens IGKV2-30*01 (88.00%) -IGKJ4*01) [11.3.9] (1'-112') -Homo sapiens IGKC*01 (113'-219')]
idarucizumab inmunoglobulina Fab G1-kappa, anti-[dagibatrán], anticuerpo monoclonal humanizado; cadena pesada VH-(CH1-bisagra) gamma1 (1-225) [VH humanizado (Homo sapiens IGHV4-59*01 (82.30%) -(IGHD)-IGHJ4*01) [8.7.16] (1-122) -Homo sapiens IGHG1*01 (CH1 (123-220), bisagra 1-5 (221-225)) (123-225)], (225-219')-disulfuro con la cadena ligera kappa (1'-219') [V-KAPPA humanizado (Homo sapiens IGKV2-30*01 (88.00%) -IGKJ4*01) [11.3.9] (1'-112') -Homo sapiens IGKC*01 (113'-219')]
Heavy chain / Chaîne lourde / Cadena pesada
QVQLQESGPG LVKPSETLSL TCTVSGFSLT SYIVDWIRQP PGKGLEWIGV 50IWAGGSTGYN SALRSRVSIT KDTSKNQFSL KLSSVTAADT AVYYCASAAY 100YSYYNYDGFA YWGQGTLVTV SSASTKGPSV FPLAPSSKST SGGTAALGCL 150VKDYFPEPVT VSWNSGALTS GVHTFPAVLQ SSGLYSLSSV VTVPSSSLGT 200QTYICNVNHK PSNTKVDKKV EPKSC 225
Light chain / Chaîne légère / Cadena ligeraDVVMTQSPLS LPVTLGQPAS ISCKSSQSLL YTDGKTYLYW FLQRPGQSPR 50RLIYLVSKLD SGVPDRFSGS GSGTDFTLKI SRVEAEDVGV YYCLQSTHFP 100HTFGGGTKVE IKRTVAAPSV FIFPPSDEQL KSGTASVVCL LNNFYPREAK 150VQWKVDNALQ SGNSQESVTE QDSKDSTYSL SSTLTLSKAD YEKHKVYACE 200VTHQGLSSPV TKSFNRGEC 219
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H (C23-C104)22-95 149-205Intra-L (C23-C104)23'-93'139'-199'Inter-H-L (h 5-CL 126)225-219'
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónNone - Aucun - Ninguno
ipafriceptum # ipafricept fusion protein for immune applications (FPIA) comprising Homo
sapiens FZD8 (frizzled family receptor 8, Frizzled-8) extracellular domain, fused with Homo sapiens immunoglobulin G1 Fc fragment; Homo sapiens FZD8 precursor fragment 28-158 (1-131) -Homo sapiens IGHG1*01 H-CH2-CH3 fragment (hinge 1-15 C5>S (136) (132-146), CH2 (147-256), CH3 (257-361), CHS (362-363)) (132-363); dimer (142-142':145-145')-bisdisulfide
ipafricept protéine de fusion pour applications immunitaires (FPIA) comprenant le domaine extracellulaire d'Homo sapiens FZD8 (membre 8 de la famille de récepteurs frizzled, Frizzled-8), fusionné au fragment Fc de l'Homo sapiens immunoglobuline G1; Homo sapiens FZD8 fragment 28-158 du précurseur (1-131) -Homo sapiens IGHG1*01 fragment H-CH2-CH3 (charnière 1-15 C5>S (136) (132-146), CH2 (147-256), CH3 (257-361), CHS (362-363)) (132-363); dimère (142-142':145-145')-bisdisulfure

Recommended INN: List 71 WHO Drug Information, Vol. 28, No. 1, 2014
92
ipafricept proteína de fusión para aplicaciones inmunitarias (que comprende el dominio extracelular de FZD8 de Homo sapiens (miembro 8 de la familia de receptores frizzled, Frizzled-8), fusionado con el fragmento Fc de inmunoglobulina G1 de Homo sapiens; fragmento precursor 28-158 (1-131) de FZD8 de Homo sapiens -Homo sapiens IGHG1*01 fragmento H-CH2-CH3 (bisagra 1-15 C5>S (136) (132-146), CH2 (147-256), CH3 (257-361), CHS (362-363)) (132-363); dímero(142-142':145-145')-bisdisulfuro
Fused chain / chaine fusionnée / cadena fusionada
ASAKELACQE ITVPLCKGIG YNYTYMPNQF NHDTQDEAGL EVHQFWPLVE 50IQCSPDLKFF LCSMYTPICL EDYKKPLPPC RSVCERAKAG CAPLMRQYGF 100AWPDRMRCDR LPEQGNPDTL CMDYNRTDLT TEPKSSDKTH TCPPCPAPEL 150LGGPSVFLFP PKPKDTLMIS RTPEVTCVVV DVSHEDPEVK FNWYVDGVEV 200HNAKTKPREE QYNSTYRVVS VLTVLHQDWL NGKEYKCKVS NKALPAPIEK 250TISKAKGQPR EPQVYTLPPS RDELTKNQVS LTCLVKGFYP SDIAVEWESN 300GQPENNYKTT PPVLDSDGSF FLYSKLTVDK SRWQQGNVFS CSVMHEALHN 350HYTQKSLSLS PGK 363 Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntrachainFZD8 8-6916-6253-9180-12184-108 8'-69'16'-62'53'-91'80'-121'84'-108' C23-C104177-237283-341 177'-237'283'-341'Interchainh 11, h 14142-142'145-145'
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilación22, 125, 22', 125': bi-, tri- and tetra-antennary oligosaccharides containing up to 4 sialic acids213, 213' (CH2 N84.4): complex biantennary oligosaccharide
Post-translational modifications/ modifications post-traductionnelles / modificaciones post-traduccionales 363, 363': C-terminal K processed by carboxypeptidase-like activity
ledipasvirum ledipasvir methyl [(1S)-1-{(1R,3S,4S)-3-[5-(9,9-difluoro-7-{2-[(6S)-5-{(2S)-2-
[(methoxycarbonyl)amino]-3-methylbutanoyl}-5-azaspiro[2.4]hept- 6-yl]-1H-imidazol-4-yl}-9H-fluoren-2-yl)-1H-benzimidazol-2-yl]- 2-azabicyclo[2.2.1]heptane-2-carbonyl}-2-methylpropyl]carbamate
lédipasvir [(1S)-1-{(1R,3S,4S)-3-[5-(9,9-difluoro-7-{2-[(6S)-5-{(2S)-2-[(méthoxycarbonyl)amino]-3-méthylbutanoyl}-5-azaspiro[2.4]hept- 6-yl]-1H-imidazol-4-yl}-9H-fluorén-2-yl)-1H-benzimidazol-2-yl]- 2-azabicyclo[2.2.1]heptane-2-carbonyl}-2-méthylpropyl]carbamate de méthyle
ledipasvir [(1S)-1-{(1R,3S,4S)-3-[5-(9,9-difluoro-7-{2-[(6S)-5-{(2S)-2-[(metoxicarbonil)amino]-3-metilbutanoil}-5-azaespiro[2.4]hept-6-il]-1H-imidazol-4-yl}-9H-fluoren-2-il)-1H-benzimidazol-2-il]- 2-azabiciclo[2.2.1]heptano-2-carbonil}-2-metilpropil]carbamato de metilo
C49H54F2N8O6
FFN
HN
NH
O
H
H
N
HN
OO
HN
N
OCH3H3C
CH3
H
NHOH
H
CH3
CH3
OCH3

WHO Drug Information, Vol. 28, No. 1, 2014 Recommended INN: List 71
93
lexanopadolum lexanopadol trans-6'-fluoro-N-methyl-4-phenyl-4',9'-dihydro-
3'H-spiro[cyclohexane-1,1'-pyrano[3,4-b]indol]-4-amine
lexanopadol trans-6'-fluoro-N-méthyl-4-phényl-4',9'-dihydro- 3'H-spiro[cyclohexane-1,1'-pyrano[3,4-b]indol]-4-amine
lexanopadol trans-6'-fluoro-N-metil-4-fenil-4',9'-dihidro-3'H-espiro[ciclohexano-1,1'-pirano[3,4-b]indol]-4-amina
C23H25FN2O
HN
H3C
OHN
F
liafensinum liafensine 6-[(4S)-2-methyl-4-(naphthalen-2-yl)-1,2,3,4-tetrahydroisoquinolin-
7-yl]pyridazin-3-amine
liafensine 6-[(4S)-2-méthyl-4-(naphtalén-2-yl)-1,2,3,4-tétrahydroisoquinolin- 7-yl]pyridazin-3-amine
liafensina 6-[(4S)-2-metil-4-(naftalen-2-il)-1,2,3,4-tetrahidroisoquinolin- 7-il]piridazin-3-amina
C24H22N4
NCH3
H
NN
H2N
margetuximabum # margetuximab immunoglobulin G1-kappa, anti-[Homo sapiens ERBB2 (epidermal
growth factor receptor 2, HER-2, p185c-erbB2, NEU, EGFR2)], chimeric monoclonal antibody; gamma1 heavy chain (1-450) [Mus musculus VH (IGHV14-3*02 -(IGHD)-IGHJ4*01) [8.8.13] (1-120) - Homo sapiens IGHG1*01 (CH1 K120>R (217) (121-218), hinge (219-233), CH2 L1.2>V (238), F7>L (246), R83>P (295), Y85.2>L (303) (234-343), CH3 P83>L (399) (344-448), CHS (449-450)) (121-450)], (223-214')-disulfide with kappa light chain (1'-214') [Mus musculus V-KAPPA (IGKV6-17*01 -IGKJ1*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01 (108'-214')]; dimer (229-229'':232-232'')-bisdisulfide

Recommended INN: List 71 WHO Drug Information, Vol. 28, No. 1, 2014
94
margétuximab immunoglobuline G1-kappa, anti-[Homo sapiens ERBB2 (récepteur 2 du facteur de croissance épidermique, HER-2, p185c-erbB2, NEU, EGFR2)], anticorps monoclonal chimérique; chaîne lourde gamma1 (1-450) [Mus musculus VH (IGHV14-3*02 -(IGHD)-IGHJ4*01) [8.8.13] (1-120) - Homo sapiens IGHG1*01 (CH1 K120>R (217) (121-218), charnière (219-233), CH2 L1.2>V (238), F7>L (246), R83>P (295), Y85.2>L (303) (234-343), CH3 P83>L (399) (344-448), CHS (449-450)) (121-450)], (223-214')-disulfure avec la chaîne légère kappa (1'-214') [Mus musculus V-KAPPA (IGKV6-17*01 -IGKJ1*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01 (108'-214')]; dimère (229-229'':232-232'')-bisdisulfure
margetuximab inmunoglobulina G1-kappa, anti-[ERBB2 de Homo sapiens (receptor 2 del factor de crecimiento epidérmico, HER-2, p185c-erbB2, NEU, EGFR2)], anticuerpo monoclonal quimérico; cadena pesada gamma1 (1-450) [Mus musculus VH (IGHV14-3*02 -(IGHD)-IGHJ4*01) [8.8.13] (1-120) - Homo sapiens IGHG1*01 (CH1 K120>R (217) (121-218),bisagra (219-233), CH2 L1.2>V (238), F7>L (246), R83>P (295), Y85.2>L (303) (234-343), CH3 P83>L (399) (344-448), CHS (449-450)) (121-450)], (223-214')-disulfuro con la cadena ligera kappa (1'-214') [Mus musculus V-KAPPA (IGKV6-17*01 -IGKJ1*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01 (108'-214')]; dímero (229-229'':232-232'')-bisdisulfuro
Heavy chain / Chaîne lourde / Cadena pesada
QVQLQQSGPE LVKPGASLKL SCTASGFNIK DTYIHWVKQR PEQGLEWIGR 50IYPTNGYTRY DPKFQDKATI TADTSSNTAY LQVSRLTSED TAVYYCSRWG 100GDGFYAMDYW GQGASVTVSS ASTKGPSVFP LAPSSKSTSG GTAALGCLVK 150DYFPEPVTVS WNSGALTSGV HTFPAVLQSS GLYSLSSVVT VPSSSLGTQT 200YICNVNHKPS NTKVDKRVEP KSCDKTHTCP PCPAPELVGG PSVFLLPPKP 250KDTLMISRTP EVTCVVVDVS HEDPEVKFNW YVDGVEVHNA KTKPPEEQYN 300STLRVVSVLT VLHQDWLNGK EYKCKVSNKA LPAPIEKTIS KAKGQPREPQ 350VYTLPPSRDE LTKNQVSLTC LVKGFYPSDI AVEWESNGQP ENNYKTTPLV 400LDSDGSFFLY SKLTVDKSRW QQGNVFSCSV MHEALHNHYT QKSLSLSPGK 450
Light chain / Chaîne légère / Cadena ligeraDIVMTQSHKF MSTSVGDRVS ITCKASQDVN TAVAWYQQKP GHSPKLLIYS 50ASFRYTGVPD RFTGSRSGTD FTFTISSVQA EDLAVYYCQQ HYTTPPTFGG 100GTKVEIKRTV AAPSVFIFPP SDEQLKSGTA SVVCLLNNFY PREAKVQWKV 150DNALQSGNSQ ESVTEQDSKD STYSLSSTLT LSKADYEKHK VYACEVTHQG 200LSSPVTKSFN RGEC 214
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H (C23-C104)22-96 147-203 264-324 370-428 22''-96''147''-203''264''-324''370''-428''Intra-L (C23-C104)23'-88' 134'-194' 23'''-88'''134'''-194'''Inter-H-L (h 5-CL 126)223-214' 223''-214'''Inter-H-H (h 11, h 14) 229-229''232-232''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:300, 300''
mavatrepum mavatrep 2-[2-(2-{(1E)-2-(trifluoromethyl)phenyl]ethenyl}-1H-benzimidazol-
5-yl)phenyl]propan-2-ol
mavatrep 2-[2-(2-{(1E)-2-(trifluorométhyl)phényl]éthényl}-1H-benzimidazol- 5-yl)phényl]propan-2-ol
mavatrep 2-[2-(2-{(1E)-2-(trifluorometil)fenil]etenil}-1H-benzoimidazol- 5-il)fenil]propan-2-ol

WHO Drug Information, Vol. 28, No. 1, 2014 Recommended INN: List 71
95
C25H21F3N2O
N
HNOHH3C
H3C
CF3
methylsamidorphani chloridum methylsamidorphan chloride (17R)-3-carbamoyl-17-(cyclopropylmethyl)-4,14-dihydroxy-
17-methyl-6-oxomorphinan-17-ium chloride
chlorure de méthylsamidorphan chlorure de (17R)-3-carbamoyl-17-(cyclopropylméthyl)- 4,14-dihydroxy-17-méthyl-6-oxomorphinanium
cloruro de metilsamidorfano cloruro de (17R)-3-carbamoil-17-(ciclopropilmetil)-4,14-dihidroxi- 17-metil-6-oxomorfinanio
C22H29ClN2O4
N
HO
H
OOHH2NO
H3C
Cl
mirogabalinum mirogabalin [(1R,5S,6S)-6-(aminomethyl)-3-ethylbicyclo[3.2.0]hept-3-en-
6-yl]acetic acid
mirogabaline acide [(1R,5S,6S)-6-(aminométhyl)-3-éthylbicyclo[3.2.0]hept-3-én- 6-yl]acétique
mirogabalina ácido 2-[(1R,5S,6S)-6-(aminometil)-3-etilbiciclo[3.2.0]hept-3-en- 6-il]acético
C12H19NO2
H3C
H
H
NH2
CO2H
neboterminum # nebotermin recombinant DNA derived L-methionyl-human bone morphogenetic
protein 2 (BMP-2 or BMP-2A), produced in Escherichia coli (nonglycosylated)
nébotermine L-méthionyl-protéine 2 morphogénétique de l'os humaine (BMP-2 ou BMP-2A), produite par Escherichia coli (non glycosylée) à partir d'ADN recombinant
nebotermina L-metionil-proteína 2 morfogenética humana de hueso (BMP-2 o BMP-2A), producida por Escherichia coli (no glicosilada) a partir de ADN recombinante

Recommended INN: List 71 WHO Drug Information, Vol. 28, No. 1, 2014
96
C1152H1776N322O330S20
Monomer / Monomère / Monómero MQAKHKQRKRLKSSCKRHPLYVDFSDVGWNDWIVAPPGYHAFYCHGECPFP50LADHLNSTNHAIVQTLVNSVNSKIPKACCVPTELSAISMLYLDENEKVVL100KNYQDMVVEGCGCR 114
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuro14-7914'-79'43-11143'-111'47-11347'-113'78-78'
nobiprostolanum nobiprostolan propan-2-yl (5E)-7-{(1R,2R,3R,5S)-2-[2-(2-heptyl-1,3-dioxolan-
2-yl)ethyl]-3,5-dihydroxycyclopentyl}hept-5-enoate
nobiprostolan (5E)-7-{(1R,2R,3R,5S)-2-[2-(2-heptyl-1,3-dioxolan-2-yl)éthyl]- 3,5-dihydroxycyclopentyl}hept-5-énoate de propan-2-yle
nobiprostolán (5E)-7-{(1R,2R,3R,5S)-2-[2-(2-heptil-1,3-dioxolan-2-il)etil]- 3,5-dihidroxiciclopentil}hept-5-enoato de propan-2-ilo
C27H48O6
OHH
HOH
O CH3
CH3O
CH3O OH
H
ombitasvirum ombitasvir dimethyl N,N'-{[(2S,5S)-1-(4-tert-butylphenyl)pyrrolidene-2,5-diyl]-
bis-{[(4,1-phenyleneazanediyl)carbonyl][(2S)-pyrrolidine- 2,1-diyl]}[(2S)-3-methyl-1-oxobutane-1,2-diyl])}biscarbamate
ombitasvir N,N'-{[(2S,5S)-1-(4-tert-butylphényl)pyrrolidine-2,5-diyl]-bis-{[(4,1-phénylèneazanediyl)carbonyl][(2S)-pyrrolidine-2,1-diyl]}[(2S)-3-méthyl-1-oxobutane-1,2-diyl])}biscarbamate de diméthyle
ombitasvir N,N'-{[(2S,5S)-1-(4-terc-butilfenil)pirrolideno-2,5-diil]-bis-{[(4,1-fenilenoazanodiil)carbonil][(2S)-pirrolidina-2,1-diil]}[(2S)-3-metil- 1-oxobutano-1,2-diil])}biscarbamato de dimetilo
C50H67N7O8
O N
HNH
OO
H3C
CH3
HNH
O
ON
HHN
O O
CH3
CH3
HNH
ON
H3C CH3
CH3
HH H3CCH3

WHO Drug Information, Vol. 28, No. 1, 2014 Recommended INN: List 71
97
ontuxizumabum # ontuxizumab immunoglobulin G1-kappa, anti-[Homo sapiens CD248 (endosialin,
tumor endothelial marker 1, TEM1), humanized/chimeric monoclonal antibody; gamma1 heavy chain (1-454) [chimeric VH (Homo sapiens IGHV4-59*04 (68.00%) -(IGHD)-IGHJ4*01) [8.8.17] (1-124) -Homo sapiens IGHG1*01 (CH1 (125-222), hinge (223-237), CH2 (238-347), CH3 S85.3>F (410) (348-452), CHS (453-454)) (125-454)], (227-215')-disulfide with kappa light chain (1'-215') [humanized V-KAPPA (Homo sapiens IGKV1-33*01 (83.20%) -IGKJ1*01) [6.3.10] (1'-108') -Homo sapiens IGKC*01 (109'-215')]; dimer (233-233'':236-236'')-bisdisulfide
ontuxizumab immunoglobuline G1-kappa, anti-[Homo sapiens CD248 (endosialine, marqueur endothélial tumoral 1, TEM1)], anticorps monoclonal humanisé/chimérique; chaîne lourde gamma1 (1-454) [VH chimérique (Homo sapiens IGHV4-59*04 (68.00%) -(IGHD)-IGHJ4*01) [8.8.17] (1-124) -Homo sapiens IGHG1*01 (CH1 (125-222), charnière (223-237), CH2 (238-347), CH3 S85.3>F (410) (348-452), CHS (453-454)) (125-454)], (227-215')-disulfure avec la chaîne légère kappa (1'-215') [V-KAPPA humanisé (Homo sapiens IGKV1-33*01 (83.20%) -IGKJ1*01) [6.3.10] (1'-108') -Homo sapiens IGKC*01 (109'-215')]; dimère (233-233'':236-236'')-bisdisulfure
ontuxizumab inmunoglobulina G1-kappa, anti-[CD248 de Homo sapiens (endosialina, marcador endotelial tumoral 1, TEM1)], anticuerpo monoclonal humanizado/quimérico; cadena pesada gamma1 (1-454) [VH quimérico (Homo sapiens IGHV4-59*04 (68.00%) -(IGHD)-IGHJ4*01) [8.8.17] (1-124) -Homo sapiens IGHG1*01 (CH1 (125-222), bisagra (223-237), CH2 (238-347), CH3 S85.3>F (410) (348-452), CHS (453-454)) (125-454)], (227-215')-disulfuro con la cadena ligera kappa (1'-215') [V-KAPPA humanizada (Homo sapiens IGKV1-33*01 (83.20%) -IGKJ1*01) [6.3.10] (1'-108') -Homo sapiens IGKC*01 (109'-215')]; dímero (233-233'':236-236'')-bisdisulfuro
Heavy chain / Chaîne lourde / Cadena pesada
QVQLQESGPG LVRPSQTLSL TCTASGYTFT DYVIHWVKQP PGRGLEWIGY 50INPYDDDTTY NQKFKGRVTM LVDTSSNTAY LRLSSVTAED TAVYYCARRG 100NSYDGYFDYS MDYWGSGTPV TVSSASTKGP SVFPLAPSSK STSGGTAALG 150CLVKDYFPEP VTVSWNSGAL TSGVHTFPAV LQSSGLYSLS SVVTVPSSSL 200GTQTYICNVN HKPSNTKVDK KVEPKSCDKT HTCPPCPAPE LLGGPSVFLF 250PPKPKDTLMI SRTPEVTCVV VDVSHEDPEV KFNWYVDGVE VHNAKTKPRE 300EQYNSTYRVV SVLTVLHQDW LNGKEYKCKV SNKALPAPIE KTISKAKGQP 350REPQVYTLPP SRDELTKNQV SLTCLVKGFY PSDIAVEWES NGQPENNYKT 400TPPVLDSDGF FFLYSKLTVD KSRWQQGNVF SCSVMHEALH NHYTQKSLSL 450SPGK 454
Light chain / Chaîne légère / Cadena ligeraDIQMTQSPSS LSASVGDRVT ITCRASQNVG TAVAWLQQTP GKAPKLLIYS 50ASNRYTGVPS RFSGSGSGTD YTFTISSLQP EDIATYYCQQ YTNYPMYTFG 100QGTKVQIKRT VAAPSVFIFP PSDEQLKSGT ASVVCLLNNF YPREAKVQWK 150VDNALQSGNS QESVTEQDSK DSTYSLSSTL TLSKADYEKH KVYACEVTHQ 200GLSSPVTKSF NRGEC 215
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H (C23-C104)22-96 151-207 268-328 374-432 22''-96''151''-207''268''-328''374''-432''Intra-L (C23-C104)23'-88' 135'-195' 23'''-88'''135'''-195'''Inter-H-L (h 5-CL 126)227-215' 227''-215'''Inter-H-H (h 11, h 14) 233-233''236-236''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:304, 304''

Recommended INN: List 71 WHO Drug Information, Vol. 28, No. 1, 2014
98
oreptacogum alfa (activatum) # oreptacog alfa (activated) recombinant DNA derived human blood coagulation factor VIIa (two
protein chains) analogue, produced in CHO cells (glycoform alfa): [10-L-glutamine(P>Q),32-L-glutamic acid(K>E),34-L-glutamic acid(A>E),36-L-glutamic acid(R>E),106-L-asparagine(T>N), 253-L-asparagine(V>N)]activated human coagulation factor VII (proconvertine, SPCA)
oreptacog alfa (activé) analogue du facteur de coagulation sanguine VIIa (deux chaînes protéiques) humain, produit par des cellules ovariennes de hamster chinois (CHO) à partir d'ADN recombinant (glycoforme alfa) : [10-L-glutamine(P>Q),32-L-acide glutamique(K>E),34-L-acide glutamique(A>E),36-L-acide glutamique(R>E), 106-L-asparagine(T>N),253-L-asparagine(V>N)]facteur de coagulation VII humain activé (proconvertine, SPCA)
oreptacog alfa (activado) análogo del factor VIIa de coagulación (dos cadenas proteicas ) humano, producido por células ováricas de hamster chino (CHO) a partir de ADN recombinante (glicoforma alfa) : [10-L-glutamina(P>Q),32-L-ácido glutámico(K>E),34-L-ácido glutámico (A>E),36-L-ácido glutámico(R>E), 106-L-asparagina(T>N),253-L-asparagina(V>N)]factor de coagulación VII humano activado (proconvertina, SPCA)
HO2C CO2H
NH2HHO2C
Light chain / Chaîne légère / Cadedena ligeraANAFLEELRQGSLERECKEEQCSFEEAREIFEDEEETKLFWISYSDGDQC50ASSPCQNGGSCKDQLQSYICFCLPAFEGRNCETHKDDQLICVNENGGCEQ100YCSDHNGTKRSCRCHEGYSLLADGVSCTPTVEYPCGKIPILEKRNASKPQ150GR 152
Heavy chain / Chaîne lourde / Cadena pesada IVGGKVCPKGECPWQVLLLVNGAQLCGGTLINTIWVVSAAHCFDKIKN200WRNLIAVLGEHDLSEHDGDEQSRRVAQVIIPSTYVPGTTNHDIALLRLHQ250PVNLTDHVVPLCLPERTFSERTLAFVRFSLVSGWGQLLDRGATALELMVL300NVPRLMTQDCLQQSRKVGDSPNITEYMFCAGYSDGSKDSCKGDSGGPHAT350HYRGTWYLTGIVSWGQGCATVGHFGVYTRVSQYIEWLQKLMRSEPRPGVL400LRAPFP 406
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuro17-22 50-61 55-70 72-81 91-102 98-112114-127135-262159-164178-194310-329340-368
Modified residues / Résidus modifiés / Restos modificadosE
6-7-14-16-19-20-25-26-29-32-34-35-364-carboxyGlu
Glycosylation sites (S or N) / Sites de glycosylation (S ou N) / Posiciones de glicosilación (S o N)Ser-52Ser-60Asn-106Asn-145Asn-253Asn-322
paclitaxelum trevatidum paclitaxel trevatide short modified fragment of human amyloid beta A4 protein covalently
linked to three molecules of paclitaxel through succinyl linkers: N2.1,N6.10, N6.15-tris{4-[(1S,2R)-1-benzamido-3-{[(2S,5R,7S,10R,13S)-10,12-bis(acetyloxy)-2-benzoyl-1,7-dihydroxy-9-oxo-5,20-epoxytax-11-en-13-yl]oxy}-3-oxo-1-phenylpropan-2-yl)oxy]-4-oxobutanoyl} ([318-L-threonine(P>T1),324-L-serine(C>S7),325-L-arginine(G>R8),327-L-lysine(N>K10),332-L-lysine(N>K15)] human amyloid beta A4 protein precursor-(318-336)-peptide)
paclitaxel trévatide fragment court et modifié de la protéine bêta A4 amyloïde humaine lié de façon covalente à trois molécules de paclitaxel par autant de succinyles : N2.1,N6.10, N6.15-tris{4-[(1S,2R)-1-benzamido-3-{[(2S,5R,7S,10R,13S)-10,12-bis(acétyloxy)-2-benzoyl-1,7-dihydroxy-9-oxo-5,20-époxytax-11-en-13-yl]oxy}-3-oxo-1-phénylpropan-2-yl)oxy]-4-oxobutanoyl} ([318-L-thréonine(P>T1),324-L-sérine(C>S7),325-L-arginine(G>R8),327-L-lysine(N>K10),332-L-lysine(N>K15)] précurseur de la protéine amyloïde bêta A4 humaine-(318-336)-peptide)

WHO Drug Information, Vol. 28, No. 1, 2014 Recommended INN: List 71
99
paclitaxel trevatida fragmento corto y modificado de la proteína beta A4 amiloide humana unido covalentemente a tres moléculas de paclitaxel mediante succinilos : N2.1,N6.10, N6.15-tris{4-[(1S,2R)-1-benzamido-3-{[(2S,5R,7S,10R,13S)-10,12-bis(acetiloxi)-2-benzoil-1,7-dihidroxi-9-oxo-5,20-epoxitax-11-en-13-il]oxi}-3-oxo-1-fenilpropan-2-il)oxi]-4-oxobutanoil} ([318-L-treonina(P>T1),324-L-serina(C>S7),325-L-arginina(G>R8),327-L-lisina(N>K10),332-L-lisina(N>K15)] precursor de la proteína amiloide beta A4 humana-(318-336)-péptido
C257H308N32O79
HO
OH
O
HOH
O
OH
CH3
O
HH
O CH3
H3C
CH3
CH3
O
O CH3
O
HHN H
HOO
OO
C= OR
H3CCO2H
HNH
H OH
R
H2N CO2H
HHNR
Peptide / Peptide / PéptidoTFFYGGSRGKRNNFKTEEY 19
Modified residues / Résidus modifiés / Restos modificados
K 10, 15
T 1
palbociclibum palbociclib 6-acetyl-8-cyclopentyl-5-methyl-2-{[5-(piperazin-1-yl)pyridin-
2-yl]amino}pyrido[2,3-d]pyrimidin-7(8H)-one
palbociclib 6-acétyl-8-cyclopentyl-5-méthyl-2-{[5-(pipérazin-1-yl)pyridin- 2-yl]amino}pyrido[2,3-d]pyrimidin-7(8H)-one
palbociclib 6-acetil-8-ciclopentil-5-metil-2-{[5-(piperazin-1-il)piridin- 2-il]amino}pirido[2,3-d]pirimidin-7(8H)-ona
C24H29N7O2
N
NHNN
N
HN N CH3
O
CH3
O
panulisibum panulisib 2-(5-{(2EZ)-8-[6-amino-5-(trifluoromethyl)pyridin-3-yl]-
2-(cyanoimino)-3-methyl-2,3-dihydro-1H-imidazo[4,5-c]quinolin- 1-yl}pyridin-2-yl)-2-methylpropanenitrile
panulisib 2-(5-{(2EZ)-8-[6-amino-5-(trifluorométhyl)pyridin-3-yl]- 2-(cyanoimino)-3-méthyl-2,3-dihydro-1H-imidazo[4,5-c]quinoléin- 1-yl}pyridin-2-yl)-2-methylpropanenitrile
panulisib 2-(5-{(2EZ)-8-[6-amino-5-(trifluorometil)pyridin-3-il]-2-(cianoimino)- 3-metil-2,3-dihidro-1H-imidazo[4,5-c]quinolin-1-il}piridin-2-il)- 2-metilpropanonitrilo

Recommended INN: List 71 WHO Drug Information, Vol. 28, No. 1, 2014
100
C27H20F3N9
N
N
NN
N
CH3
N
CNH3C
H3C
H2N
F3C
CN
patisiranum patisiran small interfering RNA (siRNA);
RNA duplex of guanylyl-(3'→5')-2'-O-methyluridylyl-(3'→5')-adenylyl-(3'→5')-adenylyl-(3'→5')-2'-O-methylcytidylyl-(3'→5')-2'-O-methylcytidylyl-(3'→5')-adenylyl-(3'→5')-adenylyl-(3'→5')-guanylyl-(3'→5')-adenylyl-(3'→5')-guanylyl-(3'→5')-2'-O-methyluridylyl-(3'→5')-adenylyl-(3'→5')-2'-O-methyluridylyl-(3'→5')-2'-O-methyluridylyl-(3'→5')-2'-O-methylcytidylyl-(3'→5')-2'-O-methylcytidylyl-(3'→5')-adenylyl-(3'→5')-2'-O-methyluridylyl-(3'→5')-thymidylyl-(3'→5')-thymidine with thymidylyl-(5'→3')-thymidylyl-(5'→3')-cytidylyl-(5'→3')-adenylyl-(5'→3')-2'-O-methyluridylyl-(5'→3')-uridylyl-(5'→3')-guanylyl-(5'→3')-guanylyl-(5'→3')-uridylyl-(5'→3')-uridylyl-(5'→3')-cytidylyl-(5'→3')-uridylyl-(5'→3')-cytidylyl-(5'→3')-adenylyl-(5'→3')-2'-O-methyluridylyl-(5'→3')-adenylyl-(5'→3')-adenylyl-(5'→3')-guanylyl-(5'→3')-guanylyl-(5'→3')-uridylyl-(5'→3')-adenosine
patisiran petit ARN interférant (siRNA); duplex ARN du brin guanylyl-(3'→5')-2'-O-méthyluridylyl-(3'→5')-adénylyl-(3'→5')-adénylyl-(3'→5')-2'-O-méthylcytidylyl-(3'→5')-2'-O-méthylcytidylyl-(3'→5')-adénylyl-(3'→5')-adénylyl-(3'→5')-guanylyl-(3'→5')-adénylyl-(3'→5')-guanylyl-(3'→5')-2'-O-méthyluridylyl-(3'→5')-adénylyl-(3'→5')-2'-O-méthyluridylyl-(3'→5')-2'-O-méthyluridylyl-(3'→5')-2'-O-méthylcytidylyl-(3'→5')-2'-O-méthylcytidylyl-(3'→5')-adénylyl-(3'→5')-2'-O-méthyluridylyl-(3'→5')-thymidylyl-(3'→5')-thymidine avec le brin anti-sens thymidylyl-(5'→3')-thymidylyl-(5'→3')-cytidylyl-(5'→3')-adénylyl-(5'→3')-2'-O-méthyluridylyl-(5'→3')-uridylyl-(5'→3')-guanylyl-(5'→3')-guanylyl-(5'→3')-uridylyl-(5'→3')-uridylyl-(5'→3')-cytidylyl-(5'→3')-uridylyl-(5'→3')-cytidylyl-(5'→3')-adénylyl-(5'→3')-2'-O-méthyluridylyl-(5'→3')-adénylyl-(5'→3')-adénylyl-(5'→3')-guanylyl-(5'→3')-guanylyl-(5'→3')-uridylyl-(5'→3')-adénosine
patisirán ARN interferente pequeño (siRNA); ARN dúplex de la cadena guanilil-(3'→5')-2'-O-metiluridilil-(3'→5')-adenilil-(3'→5')-adenilil-(3'→5')-2'-O-metilcitidilil-(3'→5')-2'-O-metilcitidilil-(3'→5')-adenilil-(3'→5')-adenilil-(3'→5')-guanilil-(3'→5')-adenilil-(3'→5')-guanilil-(3'→5')-2'-O-metiluridilil-(3'→5')-adenilil-(3'→5')-2'-O-metiluridilil-(3'→5')-2'-O-metiluridilil-(3'→5')-2'-O-metilcitidilil-(3'→5')-2'-O-metilcitidilil-(3'→5')-adenilil-(3'→5')-2'-O-metiluridilil-(3'→5')-timidilil-(3'→5')-timidina con la cadena antisentido timidilil-(5'→3')-timidilil-(5'→3')-citidilil-(5'→3')-adenilil-(5'→3')-2'-O-metiluridilil-(5'→3')-uridilil-(5'→3')-guanilil-(5'→3')-guanilil-(5'→3')-uridilil-(5'→3')-uridilil-(5'→3')-citidilil-(5'→3')-uridilil-(5'→3')-citidilil-(5'→3')-adenilil-(5'→3')-2'-O-metiluridilil-(5'→3')-adenilil-(5'→3')-adenilil-(5'→3')-guanilil-(5'→3')-guanilil-(5'→3')-uridilil-(5'→3')-adenosina

WHO Drug Information, Vol. 28, No. 1, 2014 Recommended INN: List 71
101
C412H480N148O290P40
N
HNO O
O
HO OCH3
N
NO NH2
O
HO OCH3
C = mC U = mU
HOHO
(3'-5')G-U-A-A-C-C-A-A-G-A-G-U-A-U-U-C-C-A-U-dT-dT(5'-3')dT-dT-C-A-U-U-G-G-U-U-C-U-C-A-U-A-A-G-G-U-A
Modified nucleosides (C and U) / Nucléosides modifiés (C et U) / Nucleósidos modificados (C y U)
pegbovigrastimum # pegbovigrastim recombinant DNA derived bovine granulocyte colony-stimulating
factor (G-CSF) analogue, produced in Escherichia coli (nonglycosylated), covalently bonded to methoxy polyethylene glycol: L-methionyl-[133-{4-(1-{[2-({[ω-methoxypoly(oxyethylene)]carbonyl}amino)ethoxy]imino}ethyl)- L-phenylalanine(T>F)}]bovine granulocyte colony-stimulating factor (G-CSF)
pegbovigrastim analogue du facteur de stimulation de colonies de granulocytes bovin, produit par Escherichia coli à partir d'ADN recombinant (non glycosylé), auquel est liée de façon covalente une chaîne méthoxypolyéthylèneglycol : L-méthionyl-[133-{4-(1-{[2-({[ω-méthoxypoly(oxyéthylène)]carbonyl}amino)éthoxy]imino}éthyl)- L-phénylalanine(T>F)}]facteur de stimulation des colonies de granulocytes (G-CSF) bovin
pegbovigrastim análogo del factor bovino estimulante de colonias de granulocitos, producido por Escherichia coli a partir de ADN recombinante (no glicosilado), al cual se une covalentemente una cadena metoxipolietilenglicol : L-metionil-[133-{4-(1-{[2-({[ω-metoxipoli(oxietileno)]carbonil}amino)etoxi]imino}etil)- L-fenilalanina(T>F)}]factor estimulante de colonias de granulocitos (G-CSF) bovino
C859H1370N236O248S9 . [C2H4O]n
n
CO2H
NH2HN
CH3
ONH
O
O
H3CO
Sequence / Séquence / Secuencia MTPLGPARSLPQSFLLKCLEQVRKIQADGAELQERLCAAHKLCHPEELMLL50RHSLGIPQAPLSSCSSQSLQLTSCLNQLHGGLFLYQGLLQALAGISPELA100PTLDTLQLDVTDFATNIWLQMEDLGAAPAVQPFQGAMPTFTSAFQRRAGG150VLVASQLHRFLELAYRGLRYLAEP 174
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuro36-4264-74
Modified residue / Résidu modifié / Resto modificado
F 1334-(methoxyPEGcarbonylaminoethoxyiminoethyl)Phe

Recommended INN: List 71 WHO Drug Information, Vol. 28, No. 1, 2014
102
pegteograstimum # pegteograstim recombinant DNA derived human granulocyte colony-stimulating
factor (G-CSF) analogue, produced in Escherichia coli (nonglycosylated), covalently bonded to methoxy polyethylene glycol: endo-139a-S-{(3RS)-1-[3-({3-[ω-methoxypoly(oxyethylene)]propyl}amino)-3-oxopropyl]- 2,5-dioxopyrrolidin-3-yl}-L-cysteine (->C137)-des-(37-39)- [1-L-methionine(A>M),18-L-serine(C>S)]human granulocyte colony stimulating factor (G-CSF, pluripoietin)
pegtéograstim analogue du facteur humain de stimulation de colonies de granulocytes, produit par Escherichia coli à partir d'ADN recombinant (non glycosylé), auquel est lié de façon covalente une chaîne méthoxypolyéthylèneglycol : endo-139a-S-{(3RS)-1-[3-({3-[ω-méthoxypoly(oxyéthylène)]propyl}amino)-3-oxopropyl]- 2,5-dioxopyrrolidin-3-yl}-L-cystéine(->C137)-dès-(37-39)- [1-L-méthionine(A>M),18-L-sérine(C>S)]facteur humain de stimulation de colonies de granulocytes (G-CSF, pluripoïétine)
pegteograstim análogo del factor humano estimulante de colonias de granulocitos, producido por Escherichia coli a partir de ADN recombinante (no glicosilado), al que se une covalentemente una cadena metoxipolietilenglicol: endo-139a-S-{(3RS)-1-[3-({3-[ω-metoxipoli(oxietileno)]propil}amino)-3-oxopropil]-2,5-dioxopirrolidin-3-il}-L-cisteina(->C137)-des-(37-39)- [1-L-metionina(A>M),18-L-serina(C>S)]factor humano estimulante de colonias de granulocitos (G-CSF, pluripoyetina)
C859H1360N226O249S9 . [C2H4O]n
N S
H2N CO2H
O
OH
HHN
O
OO
H3Cn
Sequence / Séquence / SecuenciaMTPLGPASSLPQSFLLKSLEQVRKIQGDGAALQEKLCATYKLCHPEELVL50LGHSLGIPWAPLSSCPSQALQLAGCLSQLHSGLFLYQGLLQALEGISPEL100GPTLDTLQLDVADFATTIWQQMEELGMAPALQPTQGCAMPAFASAFQRRA150GGVLVASHLQSFLEVSYRVLRHLAQP 176
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuro37-4365-75
Modified residue / Résidu modifié / Resto modificado
C137(139a)
PEG-linker-Cys
pevonedistatum pevonedistat [(1S,2S,4R)-4-(4-{[(1S)-2,3-dihydro-1H-inden-1-yl]amino}-
7H-pyrrolo[2,3-d]pyrimidin-7-yl)-2-hydroxycyclopentyl]methyl sulfamate
pévonédistat sulfamate de [(1S,2S,4R)-4-(4-{[(1S)-2,3-dihydro-1H-indén- 1-yl]amino}-7H-pyrrolo[2,3-d]pyrimidin-7-yl)- 2-hydroxycyclopentyl]méthyle
pevonedistat sulfamato de (1S,2S,4R)-4-(4-{[(1S)-2,3-dihidro-1H-inden- 1-il]amino}-7H-pirrolo[2,3-d]pirimidin-7-il)-2-hidroxiciclopentil]metilo

WHO Drug Information, Vol. 28, No. 1, 2014 Recommended INN: List 71
103
C21H25N5O4S
N N
NHN
H H
H OH
H
OS
NH2
OO
ralimetinibum ralimetinib 5-[2-tert-butyl-5-(4-fluorophenyl)-1H-imidazol-4-yl]-
3-(2,2-dimethylpropyl)-3H-imidazo[4,5-b]pyridin-2-amine
ralimétinib 5-[2-tert-butyl-5-(4-fluorophényl)-1H-imidazol-4-yl]- 3-(2,2-diméthylpropyl)-3H-imidazo[4,5-b]pyridin-2-amine
ralimetinib 5-[2-terc-butil-5-(4-fluorofenil)-1H-imidazol-4-il]-3-(2,2-dimetilpropil)-3H-imidazo[4,5-b]piridin-2-amina
C24H29FN6
N
NH
H3C N N
N
H3CCH3
NH2
F
CH3
H3C CH3
remeglurantum remeglurant (6-bromopyrazolo[1,5-a]pyrimidin-2-yl)[(1R)-1-methyl-
3,4-dihydroisoquinolin-2(1H)-yl]methanone
réméglurant (6-bromopyrazolo[1,5-a]pyrimidin-2-yl)[(1R)-1-méthyl- 3,4-dihydroisoquinoléin-2(1H)-yl]méthanone
remeglurant (6-bromopirazolo[1,5-a]pirimidin-2-il)[(1R)-1-metil- 3,4-dihidroisoquinolin-2(1H)-il]metanona
C17H15BrN4O
N
CH3H O
N NN
Br
ricolinostatum ricolinostat 2-(diphenylamino)-N-[7-(hydroxyamino)-7-oxoheptyl]pyrimidine-
5-carboxamide
ricolinostat 2-(diphénylamino)-N-[7-(hydroxyamino)-7-oxoheptyl]pyrimidine- 5-carboxamide
ricolinostat 2-(difenilamino)-N-[7-(hidroxiamino)-7-oxoheptil]pirimidina- 5-carboxamida

Recommended INN: List 71 WHO Drug Information, Vol. 28, No. 1, 2014
104
C24H27N5O3
N
N
HN
HN
OH
O
N
O
rimegepantum rimegepant (5S,6S,9R)-5-amino-6-(2,3-difluorophenyl)-6,7,8,9-tetrahydro-
5H-cyclohepta[b]pyridin-9-yl 4-(2-oxo-2,3-dihydro-1H-imidazo[4,5-b]pyridin-1-yl)piperidine-1-carboxylate
rimégépant 4-(2-oxo-2,3-dihydro-1H-imidazo[4,5-b]pyridin-1-yl)pipéridine- 1-carboxylate de (5S,6S,9R)-5-amino-6-(2,3-difluorophényl)- 6,7,8,9-tétrahydro-5H-cyclohepta[b]pyridin-9-yle
rimegepant 4-(2-oxo-2,3-dihidro-1H-imidazo[4,5-b]piridin-1-il)piperidina- 1-carboxilato de (5S,6S,9R)-5-amino-6-(2,3-difluorofenil)- 6,7,8,9-tetrahidro-5H-ciclohepta[b]piridin-9-ilo
C28H28F2N6O3
H
O
O
N
N
NH
N
O
HH
H2N
N
F
F
ripasudilum ripasudil 4-fluoro-5-{[(2S)-2-methyl-1,4-diazepan-1-yl]sulfonyl}isoquinoline
ripasudil 4-fluoro-5-{[(2S)-2-méthyl-1,4-diazépan-1-yl]sulfonyl}isoquinoléine
ripasudil 4-fluoro-5-{[(2S)-2-metil-1,4-diazepan-1-il]sulfonil}isoquinolina
C15H18FN3O2S
NF
SN
NH
OO CH3H
riviciclibum riviciclib 2-(2-chlorophenyl)-5,7-dihydroxy-8-[(2R,3S)-2-(hydroxymethyl)-
1-methylpyrrolidin-3-yl]-4H-1-benzopyran-4-one
riviciclib 2-(2-chlorophényl)-5,7-dihydroxy-8-[(2R,3S)-2-(hydroxyméthyl)- 1-méthylpyrrolidin-3-yl]-4H-1-benzopyran-4-one
riviciclib 2-(2-clorofenil)-5,7-dihidroxi-8-[(2R,3S)-2-(hidroximetil)- 1-metilpirrolidin-3-il]-4H-1-benzopiran-4-ona

WHO Drug Information, Vol. 28, No. 1, 2014 Recommended INN: List 71
105
C21H20ClNO5
O
O
HO
OH
N
HH
CH3
OHCl
rivipanselum rivipansel (2S)-3-cyclohexyl-2-([(1R,2R,3S,5R)-2-[(6-deoxy-
α-L-galactopyranosyl)oxy]-3-(2,6-dioxo-1,2,3,6-tetrahydropyrimidin- 4-carboxamido)-5-{13-[(3,6,8-trisulfonatonaphthalene-1-yl)amino]-6,13-dioxo-2,5-diaza-8,11-dioxatridecanoyl}cyclohexyl] {2-O-benzoyl-β-D-galactopyranosid-3-O-yl})propanoic acid
rivipansel acide (2S)-3-cyclohexyl-2-([(1R,2R,3S,5R)-2-[(6-déoxy- α-L-galactopyranosyl)oxy]-3-(2,6-dioxo-1,2,3,6-tétrahydropyrimidin- 4-carboxamido)-5-{13-[(3,6,8-trisulfonatonaphtalèn-1-yl)amino]- 6,13-dioxo-2,5-diaza-8,11-dioxatridécanoyl}cyclohexyl] {2-O-benzoyl-β-D-galactopyranosid-3-O-yl})propanoïque
rivipansel ácido (2S)-3-ciclohexil-2-([(1R,2R,3S,5R)-2-[(6-desoxi- α-L-galactopiranosil)oxi]-3-(2,6-dioxo-1,2,3,6-tetrahidropirimidin- 4-carboxamido)-5-{13-[(3,6,8-trisulfonatonaftalen-1-il)amino]- 6,13-dioxo-2,5-diaza-8,11-dioxatridecanoil}ciclohexil] {2-O-benzoil- β-D-galactopiranosid-3-O-il})propanoico
C58H74N6O31S3
HN
OO
NHHN
O
O
O
OHHO
HO
H3C
O
HOHO
O
O
O
HCO2H
NH
HNHO3S
HO3S SO3H
HN
O
O
O
O
O
O

Recommended INN: List 71 WHO Drug Information, Vol. 28, No. 1, 2014
106
roniciclibum roniciclib cyclopropyl(4-{[4-{[(2R,3R)-3-hydroxybutan-2-yl]oxy}-
5-(trifluoromethyl)pyrimidin-2-yl]amino}phenyl)imino-λ5-sulfanone
roniciclib cyclopropyl(4-{[4-{[(2R,3R)-3-hydroxybutan-2-yl]oxy}- 5-(trifluorométhyl)pyrimidin-2-yl]amino}phényl)imino-λ5-sulfanone
roniciclib ciclopropil(4-{[4-{[(2R,3R)-3-hidroxibutan-2-il]oxi}- 5-(trifluorometil)pirimidin-2-il]amino}fenil)imino-λ5-sulfanona
C18H21F3N4O3S
N
N
NH
SNHO
OH3C
F3CHH3C
H OH
ropeginterferonum alfa-2b # ropeginterferon alfa-2b recombinant DNA derived human interferon alfa-2b with an added
pegylated proline at its N-terminal, produced in Escherichia coli (nonglycosylated): {1-[(3RS)-3,7-bis{[(ω-methoxypoly(oxyethylene)carbonyl]amino}heptyl]-L-prolyl}human interferon alpha-2B
ropéginterféron alfa-2b interféron alfa-2b humain auquel une proline pégylée a été rajoutée du coté N-terminal, produit par Escherichia coli (non glycosylé) à partir d'ADN recombinant : {1-[(3RS)-3,7-bis{[(ω-méthoxypoly(oxyéthylène)carbonyl]amino}heptyl]-L-prolyl}interféron alpha-2B humain
ropeginterferon alfa-2b interferón alfa-2b humano con una prolina pegilada unida al extremo N-terminal, producido por Escherichia coli (no glicosilado) a partir de ADN recombinante : {1-[(3RS)-3,7-bis{[(ω-metoxipoli(oxietilen)carbonil]amino}heptil]- L-prolil}interferón alfa-2B humano
C876H1376N232O260S9[C2H4O]2n
N
CHNH
O
OO
H3C
HN
OOO
n
H3Cn
OP
1-[(mPEG)2link]Prolyl
Sequence / Séquence / Secuencia P0CDLPQTHSLGSRRTLMLLAQMRRISLFSCLKDRHDFGFPQEEFGNQFQKA50ETIPVLHEMIQQIFNLFSTKDSSAAWDETLLDKFYTELYQQLNDLEACVI100QGVGVTETPLMKEDSILAVRKYFQRITLYLKEKKYSPCAWEVVRAEIMRS150FSLSTNLQESLRSKE 165
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuro1-9829-138
Modified residue / Résidu modifié / Resto modificado

WHO Drug Information, Vol. 28, No. 1, 2014 Recommended INN: List 71
107
sacubitrilum sacubitril 4-{[(2S,4R)-1-([1,1'-biphenyl]-4-yl)-5-ethoxy-4-methyl-5-oxopentan-
2-yl]amino}-4-oxobutanoic acid
sacubitril acide 4-{[(2S,4R)-1-([1,1'-biphényl]-4-yl)-5-éthoxy-4-méthyl- 5-oxopentan-2-yl]amino}-4-oxobutanoïque
sacubitrilo ácido 4-{[(2S,4R)-1-([1,1'-bifenil]-4-il)-5-etoxi-4-metil-5-oxopentan- 2-il]amino}-4-oxobutanoico
C24H29NO5
O
HN
OCO2H
HH3C HH3C
O
sarecyclinum sarecycline (4S,4aS,5aR,12aS)-4-(dimethylamino)-3,10,12,12a-tetrahydroxy-
7-{[methoxy(methyl)amino]methyl}-1,11-dioxo-1,4,4a,5,5a,6,11,12a-octahydrotetracene-2-carboxamide
sarécycline (4S,4aS,5aR,12aS)-4-(diméthylamino)-3,10,12,12a-tétrahydroxy- 7-{[méthoxy(méthyl)amino]méthyl}-1,11-dioxo-1,4,4a,5,5a,6,11,12a-octahydrotétracène-2-carboxamide
sareciclina (4S,4aS,5aR,12aS)-4-(dimetilamino)-3,10,12,12a-tetrahidroxi- 7-{[metoxi(metil)amino]metil}-1,11-dioxo-1,4,4a,5,5a,6,11,12a-octahidrotetraceno-2-carboxamida
C24H29N3O8
OOH OH
NH2
H NH3C
CH3
OOH
HH
O
OH
N
CH3
OH3C
sarsageninum sarsagenin (25S)-5β-spirostan-3β-ol
sarsagénine (25S)-5β-spirostan-3β-ol
sarsagenina (25S)-5β-espirostan-3β-ol

Recommended INN: List 71 WHO Drug Information, Vol. 28, No. 1, 2014
108
C27H44O3
O
HH3C
CH3
H
HOH
OCH3
H
H
CH3H
H
H H
sisapronilum sisapronil 5-amino-1-[2,6-dichloro-4-(trifluoromethyl)phenyl]-4-[(1RS)-2,2-
difluoro-1-(trifluoromethyl)cyclopropyl]-1H-pyrazole-3-carbonitrile
sisapronil 5-amino-1-[2,6-dichloro-4-(trifluorométhyl)phényl]-4-[(1RS)-2,2-difluoro-1-(trifluorométhyl)cyclopropyl]-1H-pyrazole-3-carbonitrile
sisapronilo 5-amino-1-[2,6-dicloro-4-(trifluorometil)fenil]-4-[(1RS)-2,2-difluoro- 1-(trifluorometil)ciclopropil]-1H-pirazol-3-carbonitrilo
C15H6Cl2F8N4
N
N
CN
NH2Cl
Cl
F3C
CF3
F
F and enantiomeret énantiomèrey enantiómero
smilageninum smilagenin (25R)-5β-spirostan-3β-ol
smilagénine (25R)-5β-spirostan-3β-ol
esmilagenina (25R)-5β-espirostan-3β-ol
C27H44O3
O
HH3C
CH3
H
HOH
OH
CH3
H
CH3H
H
H H
tanurmotidum tanurmotide human lymphocyte antigen 6K-(101-111)-peptide
tanurmotide antigène 6K lymphocytaire humain-(101-111)-peptide
tanurmotida antígeno 6K linfocitario humano-(101-111)-péptido
C51H80N14O15S
Sequence / Séquence / SecuenciaRYCNLEGPPI10

WHO Drug Information, Vol. 28, No. 1, 2014 Recommended INN: List 71
109
tarextumabum # tarextumab immunoglobulin G2-kappa, anti-[Homo sapiens NOTCH2 and
NOTCH3], Homo sapiens monoclonal antibody; gamma2 heavy chain (1-441) [Homo sapiens VH (IGHV3-66*01 (93.90%) -(IGHD)-IGHJ6*01 T123>L (110)) [8.8.8] (1-115) -IGHG2*01 (CH1 (116-213), hinge (214-225), CH2 (226-334), CH3 (335-439), CHS (440-441)) (116-441)], (129-215')-disulfide with kappa light chain (1'-215') [Homo sapiens V-KAPPA (IGKV3-20*02 (94.40%) -IGKJ1*01) [7.3.9] (1'-108') -IGKC*01 (109'-215')]; dimer (217-217'':218-218'':221-221'':224-224'')-tetrakisdisulfide
tarextumab immunoglobuline G2-kappa, anti-[Homo sapiens NOTCH2 et NOTCH3], Homo sapiens anticorps monoclonal; chaîne lourde gamma2 (1-441) [Homo sapiens (IGHV3-66*01 (93.90%) -(IGHD)-IGHJ6*01 T123>L (110)) [8.8.8] (1-115) -IGHG2*01 (CH1 (116-213), charnière (214-225), CH2 (226-334), CH3 (335-439), CHS (440-441)) (116-441)], (129-215')-disulfure avec la chaîne légère kappa (1'-215') [Homo sapiens V-KAPPA (IGKV3-20*02 (94.40%) -IGKJ1*01) [7.3.9] (1'-108') -IGKC*01 (109'-215')]; dimère (217-217'':218-218'':221-221'':224-224'')-tétrakisdisulfure
tarextumab inmunoglobulina G2-kappa, anti-[NOTCH2 y NOTCH3 de Homo sapiens], anticuerpo monoclonal de Homo sapiens; cadena pesada gamma2 (1-441) [Homo sapiens (IGHV3-66*01 (93.90%) -(IGHD)-IGHJ6*01 T123>L (110)) [8.8.8] (1-115) -IGHG2*01 (CH1 (116-213), bisagra (214-225), CH2 (226-334), CH3 (335-439), CHS (440-441)) (116-441)], (129-215')-disulfuro con la cadena ligera kappa (1'-215') [Homo sapiens V-KAPPA (IGKV3-20*02 (94.40%) -IGKJ1*01) [7.3.9] (1'-108') -IGKC*01 (109'-215')]; dímero (217-217'':218-218'':221-221'':224-224'')-tetrakisdisulfuro
Heavy chain / Chaîne lourde / Cadena pesada
EVQLVESGGG LVQPGGSLRL SCAASGFTFS SSGMSWVRQA PGKGLEWVSV 50IASSGSNTYY ADSVKGRFTI SRDNSKNTLY LQMNSLRAED TAVYYCARSI 100FYTTWGQGTL VTVSSASTKG PSVFPLAPCS RSTSESTAAL GCLVKDYFPE 150PVTVSWNSGA LTSGVHTFPA VLQSSGLYSL SSVVTVPSSN FGTQTYTCNV 200DHKPSNTKVD KTVERKCCVE CPPCPAPPVA GPSVFLFPPK PKDTLMISRT 250PEVTCVVVDV SHEDPEVQFN WYVDGVEVHN AKTKPREEQF NSTFRVVSVL 300TVVHQDWLNG KEYKCKVSNK GLPAPIEKTI SKTKGQPREP QVYTLPPSRE 350EMTKNQVSLT CLVKGFYPSD IAVEWESNGQ PENNYKTTPP MLDSDGSFFL 400YSKLTVDKSR WQQGNVFSCS VMHEALHNHY TQKSLSLSPG K 441
Light chain / Chaîne légère / Cadena ligeraDIVLTQSPAT LSLSPGERAT LSCRASQSVR SNYLAWYQQK PGQAPRLLIY 50GASSRATGVP ARFSGSGSGT DFTLTISSLE PEDFAVYYCQ QYSNFPITFG 100QGTKVEIKRT VAAPSVFIFP PSDEQLKSGT ASVVCLLNNF YPREAKVQWK 150VDNALQSGNS QESVTEQDSK DSTYSLSSTL TLSKADYEKH KVYACEVTHQ 200GLSSPVTKSF NRGEC 215
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H (C23-C104)22-96 142-198 255-315 361-419 22''-96''142''-198''255''-315''361''-419''Intra-L (C23-C104)23'-89' 135'-195' 23'''-89'''135'''-195'''Inter-H-L (CH1 10-CL 126) 129-215' 129''-215'''Inter-H-H (h 4, h 5, h 8, h 11)217-217''218-218''221-221''224-224''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:291, 291''

Recommended INN: List 71 WHO Drug Information, Vol. 28, No. 1, 2014
110
taselisibum taselisib 2-methyl-2-(4-{2-[3-methyl-1-(propan-2-yl)-1H-1,2,4-triazol-5-yl]-
5,6-dihydroimidazo[1,2-d][1,4]benzoxazepin-9-yl}-1H-pyrazol- 1-yl)propanamide
tasélisib 2-méthyl-2-(4-{2-[3-méthyl-1-(propan-2-yl)-1H-1,2,4-triazol-5-yl]- 5,6-dihydroimidazo[1,2-d][1,4]benzoxazépin-9-yl}-1H-pyrazol- 1-yl)propanamide
taselisib 2-metil-2-(4-{2-[3-metil-1-(propan-2-il)-1H-1,2,4-triazol-5-yl]- 5,6-dihidroimidazo[1,2-d][1,4]benzoxazepin-9-il}-1H-pirazol- 1-il)propanamida
C24H28N8O2
ON
N
NN
N N
N
NH2
O
CH3CH3H3C
CH3
H3C
technetii (99mTc) trofolastati chloridum technetium (99mTc) trofolastat chloride (OC-6-33)-tricarbonyl{(2S)-2-[({(1S)-1-carboxy-4-{[(1S)-1-carboxy-
5-(bis{[1-(2-{[bis(carboxymethyl)]amino}-2-oxoethyl)-1H-imidazol- 2-yl-κN3]methyl}amino-κN)pentyl]amino}- 4-oxobutyl]carbamoyl}amino)pentanedioic acid}(99mTc)technetium chloride
chlorure de technétium (99mTc) trofolastat chlorure de (99mTc)technétium acide (OC-6-33)-tricarbonyl{(2S)-2-[({(1S)-1-carboxy-4-{[(1S)-1-carboxy-5-(bis{[1-(2-{[bis(carboxyméthyl)]amino}-2-oxoéthyl)-1H-imidazol- 2-yl-κN3]méthyl}amino-κN)pentyl]amino}- 4-oxobutyl]carbamoyl}amino)pentanedioïque}
cloruro de tecnecio (99mTc) trofolastat cloruro de ácido (OC-6-33)-tricarbonil{(2S)-2-[({(1S)-1-carboxi- 4-{[(1S)-1-carboxi-5-(bis{[1-(2-{[bis(carboximetil)]amino}-2-oxoetil)-1H-imidazol-2-il-κN3]metil}amino-κN)pentil]amino}- 4-oxobutil]carbamoil}amino)pentanedioico }(99mTc)tecnecio
C40H50ClN10O23Tc
NH
CO2HNH
HO2C
OH H
CO2HNH
OH
CO2HN
Tc
N
NN
N
OC
OC COO
N
CO2H
O
N CO2HHO2C
CO2H
Cl99m

WHO Drug Information, Vol. 28, No. 1, 2014 Recommended INN: List 71
111
topsalysinum # topsalysin recombinant DNA derived proaerolysin, pore-forming protein, from
Aeromonas hydrophila, with the furin site substituted with a prostate specific antigen (PSA), fusion protein with 6 histidines, produced in Escherichia coli (nonglycosylated): [427-L-histidine(K>H),428-L-serine(V>S),429-L-serine(R>S),430-L-lysine(R>K),431-L-leucine(A>L),432-L-glutamine(R>Q)]proaerolysin Aeromonas hydrophila fusion protein with hexa-L-histidine
topsalysine proaérolysine, protéine formant des pores, d'Aeromonas hydrophila dont le site furine est substitué par un antigène prostatique spécifique, protéine de fusion avec 6 histidines, produit par Escherichia coli à partir d'ADN recombinant (non glycosylé) : [427-L-histidine(K>H),428-L-sérine(V>S),429-L-sérine(R>S),430-L-lysine(R>K),431-L-leucine(A>L),432-L-glutamine(R>Q)]proaérolysine d'Aeromonas hydrophila protéine de fusion avec l'hexa-L-histidine
topsalisina proaerolisina, proteína formadora de poros, d'Aeromonas hydrophila cuyo sitio furina está substituido por un antígeno prostático específico, proteína de fusión con 6 histidinas, producida por Escherichia coli a partir de ADN recombinante (no glicosilado) : [427-L-histidina(K>H),428-L-serina(V>S),429-L-serina (R>S),430-L-lisina(R>K),431-L-leucina(A>L),432-L-glutamina(R>Q)]proaerolisina d'Aeromonas hydrophila proteina de fusión con hexa-L-histidina
Sequence / Séquence / Secuencia
AEPVYPDQLRLFSLGQGVCGDKYRPVNREEAQSVKSNIVGMMGQWQISGL50ANGWVIMGPGYNGEIKPGTASNTWCYPTNPVTGEIPTLSALDIPDGDEVD100VQWRLVHDSANFIKPTSYLAHYLGYAWVGGNHSQYVGEDMDVTRDGDGWV150IRGNNDGGCDGYRCGDKTAIKVSNFAYNLDPDSFKHGDVTQSDRQLVKTV200VGWAVNDSDTPQSGYDVTLRYDTATNWSKTNTYGLSEKVTTKNKFKWPLV250GETELSIEIAANQSWASQNGGSTTTSLSQSVRPTVPARSKIPVKIELYKA300DISYPYEFKADVSYDLTLSGFLRWGGNAWYTHPDNRPNWNHTFVIGPYKD350KASSIRYQWDKRYIPGEVKWWDWNWTIQQNGLSTMQNNLARVLRPVRAGI400TGDFSAESQFAGNIEIGAPVPLAADSHSSKLQSVDGAGQGLRLEIPLDAQ450ELSGLGFNNVSLSVTPAANQHHHHHH 476
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuro19-75159-164
tosatoxumabum # tosatoxumab immunoglobulin G1-lambda2, anti-[Staphylococcus aureus alpha-
toxin (alpha-hemolysin, alpha-HL, hly, hla)], Homo sapiens monoclonal antibody;gamma1 heavy chain (1-451) [Homo sapiens VH (IGHV5-51*01 (81.60%) -(IGHD)-IGHJ1*01 L123>M (116)) [8.8.14] (1-121) -IGHG1*01 (CH1 (122-219), hinge (220-234), CH2 (235-344), CH3 (345-449), CHS (450-451)) (122-451)], (224-216')-disulfide with lambda light chain (1'-217') [Homo sapiens V-LAMBDA (IGLV1-44*01 (93.90%) -IGLJ1*01) [8.3.12] (1'-111') -IGLC1*01 (112'-217')]; dimer (230-230'':233-233'')-bisdisulfide
tosatoxumab immunoglobuline G1-lambda2, anti-[Staphylococcus aureus toxine alpha (hémolysine alpha, HL-alpha, hly, hla)], Homo sapiens anticorps monoclonal; chaîne lourde gamma1 (1-451) [Homo sapiens VH (IGHV5-51*01 (81.60%) -(IGHD)-IGHJ1*01 L123>M (116)) [8.8.14] (1-121) -IGHG1*01 (CH1 (122-219), charnière (220-234), CH2 (235-344), CH3 (345-449), CHS (450-451)) (122-451)], (224-216')-disulfure avec la chaîne légère lambda (1'-217') [Homo sapiens V-LAMBDA (IGLV1-44*01 (93.90%) -IGLJ1*01) [8.3.12] (1'-111') -IGLC1*01 (112'-217')]; dimère (230-230'':233-233'')-bisdisulfure

Recommended INN: List 71 WHO Drug Information, Vol. 28, No. 1, 2014
112
tosatoxumab inmunoglobulina G1-lambda2, anti-[toxina alfa de Staphylococcus aureus (hemolisina alfa, HL-alfa, hly, hla)], anticuerpo monoclonal de Homo sapiens; gamma1 (1-451) [Homo sapiens VH (IGHV5-51*01 (81.60%) -(IGHD)-IGHJ1*01 L123>M (116)) [8.8.14] (1-121) -cadena pesada (224-216')-disulfuro con la cadena ligera lambda (1'-217') [Homo sapiens (IGLV1-44*01 (93.90%) -IGLJ1*01) [8.3.12] (1'-111') -IGLC1*01 (112'-217')]; dímero (230-230'':233-233'')-bisdisulfuro
Heavy chain / Chaîne lourde / Cadena pesada
EVQMVQSGAE VKKPGEPLKI SCKGSGYKFG THWIGWVRQR PGKGLEWMGI 50IHPADSETKY SPSFQGQVSF SADKSSNTAY LHWSTLRASD TAMYYCARRS 100GSSSWYALDF WGQGTMVTVS SASTKGPSVF PLAPSSKSTS GGTAALGCLV 150KDYFPEPVTV SWNSGALTSG VHTFPAVLQS SGLYSLSSVV TVPSSSLGTQ 200TYICNVNHKP SNTKVDKRVE PKSCDKTHTC PPCPAPELLG GPSVFLFPPK 250PKDTLMISRT PEVTCVVVDV SHEDPEVKFN WYVDGVEVHN AKTKPREEQY 300NSTYRVVSVL TVLHQDWLNG KEYKCKVSNK ALPAPIEKTI SKAKGQPREP 350QVYTLPPSRE EMTKNQVSLT CLVKGFYPSD IAVEWESNGQ PENNYKTTPP 400VLDSDGSFFL YSKLTVDKSR WQQGNVFSCS VMHEALHNHY TQKSLSLSPG 450K 451
Light chain / Chaîne légère / Cadena ligeraQSVLTQSPSA SGTPGQRVTI SCSGGSSNIG SNTVNWYQQF PGAAPKLLIY 50TNNQRPSGVP DRFSGSKSGT SASLAISGLQ SEDEADYYCA TWDDSLNGLY 100VFGTGTKVTV LGQPKANPTV TLFPPSSEEL QANKATLVCL ISDFYPGAVT 150VAWKADGSPV KAGVETTKPS KQSNNKYAAS SYLSLTPEQW KSHRSYSCQV 200THEGSTVEKT VAPTECS 217
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H (C23-C104)22-96 148-204 265-325 371-429 22''-96''148''-204''265''-325''371''-429''Intra-L (C23-C104)22'-89' 139'-198' 22'''-89'''139'''-198''' Inter-H-L (h 5-CL 126)224-216' 224''-216'''Inter-H-H (h 11, h 14) 230-230''233-233''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:301, 301''
tovetumabum # tovetumab immunoglobulin G2-kappa, anti-[Homo sapiens PDGFRA (platelet-
derived growth factor receptor alpha subunit, PDGFR2, CD140a)], Homo sapiens monoclonal antibody; gamma2 heavy chain (1-446) [Homo sapiens VH (IGHV3-11*01 (98.00%) -(IGHD)-IGHJ6*01) [8.8.13] (1-120) -IGHG2*01 (CH1 (121-218), hinge (219-230), CH2 (231-339), CH3 (340-444), CHS (445-446)) (121-446)], (134-215')-disulfide with kappa light chain (1'-215') [Homo sapiens V-KAPPA (IGKV1-39*01 (89.50%) -IGKJ5*01 I126>M (107)) [6.3.10] (1'-108') -IGKC*01 (109'-215')]; dimer (222-222'':223-223'':226-226'':229-229'')-tetrakisdisulfide
tovétumab immunoglobuline G2-kappa, anti-[Homo sapiens PDGFRA (sous-unité alpha du récepteur du facteur de croissance dérivé des plaquettes, PDGFR2, CD140a)], Homo sapiens anticorps monoclonal; chaîne lourde gamma2 (1-446) [Homo sapiens VH (IGHV3-11*01 (98.00%) -(IGHD)-IGHJ6*01) [8.8.13] (1-120) -IGHG2*01 (CH1 (121-218), charnière (219-230), CH2 (231-339), CH3 (340-444), CHS (445-446)) (121-446)], (134-215')-disulfure avec la chaîne légère kappa (1'-215') [Homo sapiens V-KAPPA (IGKV1-39*01 (89.50%) -IGKJ5*01 I126>M (107)) [6.3.10] (1'-108') -IGKC*01 (109'-215')]; dimère (222-222'':223-223'':226-226'':229-229'')-tétrakisdisulfure

WHO Drug Information, Vol. 28, No. 1, 2014 Recommended INN: List 71
113
tovetumab inmunoglobulina G2-kappa, anti-[PDGFRA de Homo sapiens (subunidad alfa del receptor del factor de crecimiento derivado de las plaquetas, PDGFR2, CD140a)], anticuerpo monoclonal de Homo sapiens; cadena pesada gamma2 (1-446) [Homo sapiens VH (IGHV3-11*01 (98.00%) -(IGHD)-IGHJ6*01) [8.8.13] (1-120) -IGHG2*01 (CH1 (121-218), bisagra (219-230), CH2 (231-339), CH3 (340-444), CHS (445-446)) (121-446)], (134-215')-disulfuro con la cadena ligera kappa (1'-215') [Homo sapiens V-KAPPA (IGKV1-39*01 (89.50%) -IGKJ5*01 I126>M (107)) [6.3.10] (1'-108') -IGKC*01 (109'-215')]; dímero (222-222'':223-223'':226-226'':229-229'')-tetrakisdisulfuro
Heavy chain / Chaîne lourde / Cadena pesada
QVQLVESGGG LVKPGGSLRL SCAASGFTFS DYYMNWIRQA PGKGLEWVSY 50ISSSGSIIYY ADSVKGRFTI SRDNAKNSLY LQMNSLRAED TAVYYCAREG 100RIAARGMDVW GQGTTVTVSS ASTKGPSVFP LAPCSRSTSE STAALGCLVK 150DYFPEPVTVS WNSGALTSGV HTFPAVLQSS GLYSLSSVVT VPSSNFGTQT 200YTCNVDHKPS NTKVDKTVER KCCVECPPCP APPVAGPSVF LFPPKPKDTL 250MISRTPEVTC VVVDVSHEDP EVQFNWYVDG VEVHNAKTKP REEQFNSTFR 300VVSVLTVVHQ DWLNGKEYKC KVSNKGLPAP IEKTISKTKG QPREPQVYTL 350PPSREEMTKN QVSLTCLVKG FYPSDIAVEW ESNGQPENNY KTTPPMLDSD 400GSFFLYSKLT VDKSRWQQGN VFSCSVMHEA LHNHYTQKSL SLSPGK 446
Light chain / Chaîne légère / Cadena ligeraDIQMTQSPSS LSASVGDRVS ITCRPSQSFS RYINWYQQKP GKAPKLLIHA 50ASSLVGGVPS RFSGSGSGTD FTLTISSLQP EDFATYYCQQ TYSNPPITFG 100QGTRLEMKRT VAAPSVFIFP PSDEQLKSGT ASVVCLLNNF YPREAKVQWK 150VDNALQSGNS QESVTEQDSK DSTYSLSSTL TLSKADYEKH KVYACEVTHQ 200GLSSPVTKSF NRGEC 215
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H (C23-C104)22-96 147-203 260-320 366-424 22''-96''147''-203''260''-320''366''-424''Intra-L (C23-C104) 23'-88' 135'-195' 23'''-88'''135'''-195'''Inter-H-L (CH1 10-CL 126) 134-215' 134''-215'''Inter-H-H (h 4, h 5, h 8, h 11)222-222''223-223''226-226''229-229''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:296, 296''
ubrogepantum ubrogepant (3'S)-N-[(3S,5S,6R)-6-methyl-2-oxo-5-phenyl-
1-(2,2,2-trifluoroethyl)piperidin-3-yl]-2'-oxo- 1',2',5,7-tetrahydrospiro[cyclopenta[b]pyridine-6,3'-pyrrolo[2,3-b]pyridine]-3-carboxamide
ubrogépant (3'S)-N-[(3S,5S,6R)-6-méthyl-2-oxo-5-phényl- 1-(2,2,2-trifluoroéthyl)pipéridin-3-yl]-2'-oxo- 1',2',5,7-tétrahydrospiro[cyclopenta[b]pyridine-6,3'-pyrrolo[2,3-b]pyridine]-3-carboxamide
ubrogepant (3'S)-N-[(3S,5S,6R)-6-metil-2-oxo-5-fenil- 1-(2,2,2-trifluoroetil)piperidin-3-il]-2'-oxo- 1',2',5,7-tetrahidrospiro[ciclopenta[b]piridina-6,3'-pirrolo[2,3-b]piridina]-3-carboxamida
C29H26F3N5O3
NNH
N
O
NH
ON O
CF3
H3C
H
H
H

Recommended INN: List 71 WHO Drug Information, Vol. 28, No. 1, 2014
114
valbenazinum valbenazine (2R,3R,11bR)-9,10-dimethoxy-3-(2-methylpropyl)-1,3,4,6,7,11b-
hexahydro-2H-pyrido[2,1-a]isoquinolin-2-yl L-valinate
valbénazine L-valinate de (2R,3R,11bR)-9,10-diméthoxy-3-(2-méthylpropyl)-1,3,4,6,7,11b-hexahydro-2H-pyrido[2,1-a]isoquinoléin-2-yle
valbenazina L-valinato de (2R,3R,11bR)-9,10-dimetoxi-3-(2-metilpropil)-1,3,4,6,7,11b-hexahidro-2H-pirido[2,1-a]isoquinolein-2-ylo
C24H38N2O4
NH3CO
H3CO
H
O
O
H3C
CH3
H2N H CH3
CH3
H
H
vantictumabum # vantictumab immunoglobulin G2-lambda, anti-[Homo sapiens frizzled family
receptor (FZD), including FZD1, FZD2, FZD5, FZD7 and FZD8)], Homo sapiens monoclonal antibody; gamma2 heavy chain (1-443) [Homo sapiens VH (IGHV3-23*04 (90.80%) -(IGHD)-IGHJ6*01 T123>L (113)) [8.8.11] (1-118) -IGHG2*01 (CH1 (119-216), hinge (217-228), CH2 (229-337), CH3 (338-441), CHS (442-443)) (119-443)], (132-212')-disulfide with lambda light chain (1'-213') [Homo sapiens V-LAMBDA (IGLV3-25*02 (81.60%) -IGLJ2*01) [6.3.10] (1'-107') -IGLC2*01 (108'-213')]; dimer (220-220'':221-221'':224-224'':227-227'')-tetrakisdisulfide
vantictumab immunoglobuline G2-lambda, anti-[Homo sapiens récepteur de la famille frizzled (FZD), incluant FZD1, FZD2, FZD5, FZD7 et FZD8)], Homo sapiens anticorps monoclonal; chaîne lourde gamma2 (1-443) [Homo sapiens VH (IGHV3-23*04 (90.80%) -(IGHD)-IGHJ6*01 T123>L (113)) [8.8.11] (1-118) -IGHG2*01 (CH1 (119-216), charnière (217-228), CH2 (229-337), CH3 (338-441), CHS (442-443)) (119-443)], (132-212')-disulfure avec la chaîne légère lambda (1'-213') [Homo sapiens V-LAMBDA (IGLV3-25*02 (81.60%) -IGLJ2*01) [6.3.10] (1'-107') -IGLC2*01 (108'-213')]; dimère (220-220'':221-221'':224-224'':227-227'')-tétrakisdisulfure
vantictumab inmunoglobulina G2-lambda, anti-[receptor de la familia frizzled (FZD) de Homo sapiens, incluyendo FZD1, FZD2, FZD5, FZD7 et FZD8)], anticuerpo monoclonal de Homo sapiens ; cadena pesada gamma2 (1-443) [Homo sapiens VH (IGHV3-23*04 (90.80%) -(IGHD)-IGHJ6*01 T123>L (113)) [8.8.11] (1-118) -IGHG2*01 (CH1 (119-216), bisagra (217-228), CH2 (229-337), CH3 (338-441), CHS (442-443)) (119-443)], (132-212')-disulfuro con la cadena ligera lambda (1'-213') [Homo sapiens V-LAMBDA (IGLV3-25*02 (81.60%) -IGLJ2*01) [6.3.10] (1'-107') -IGLC2*01 (108'-213')]; dímero (220-220'':221-221'':224-224'':227-227'')-tetrakisdisulfuro

WHO Drug Information, Vol. 28, No. 1, 2014 Recommended INN: List 71
115
Heavy chain / Chaîne lourde / Cadena pesada
EVQLVESGGG LVQPGGSLRL SCAASGFTFS HYTLSWVRQA PGKGLEWVSV 50ISGDGSYTYY ADSVKGRFTI SSDNSKNTLY LQMNSLRAED TAVYYCARNF 100IKYVFANWGQ GTLVTVSSAS TKGPSVFPLA PCSRSTSEST AALGCLVKDY 150FPEPVTVSWN SGALTSGVHT FPAVLQSSGL YSLSSVVTVP SSNFGTQTYT 200CNVDHKPSNT KVDKTVERKC CVECPPCPAP PVAGPSVFLF PPKPKDTLMI 250SRTPEVTCVV VDVSHEDPEV QFNWYVDGVE VHNAKTKPRE EQFNSTFRVV 300SVLTVVHQDW LNGKEYKCKV SNKGLPAPIE KTISKTKGQP REPQVYTLPP 350SREEMTKNQV SLTCLVKGFY PSDIAVEWES NGQPENNYKT TPPMLDSDGS 400FFLYSKLTVD KSRWQQGNVF SCSVMHEALH NHYTQKSLSL SPG 443
Light chain / Chaîne légère / Cadena ligeraDIELTQPPSV SVAPGQTARI SCSGDNIGSF YVHWYQQKPG QAPVLVIYDK 50SNRPSGIPER FSGSNSGNTA TLTISGTQAE DEADYYCQSY ANTLSLVFGG 100GTKLTVLGQP KAAPSVTLFP PSSEELQANK ATLVCLISDF YPGAVTVAWK 150ADSSPVKAGV ETTTPSKQSN NKYAASSYLS LTPEQWKSHR SYSCQVTHEG 200STVEKTVAPT ECS 213
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H (C23-C104)22-96 145-201 258-318 364-422 22''-96''145''-201''258''-318''364''-422''Intra-L (C23-C104)22'-87' 135'-194' 22'''-87'''135'''-194'''Inter-H-L (CH1 10-CL 126) 132-212'132''-212'''Inter-H-H (h 4, h 5, h 8, h 11) 220-220''221-221''224-224''227-227''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:294, 294''
vatiquinonum vatiquinone 2-[(3R,6E,10E)-3-hydroxy-3,7,11,15-tetramethylhexadeca-
6,10,14-trien-1-yl]-3,5,6-trimethylcyclohexa-2,5-diene-1,4-dione
vatiquinone 2-[(3R,6E,10E)-3-hydroxy-3,7,11,15-tétraméthylhexadéca- 6,10,14-trién-1-yl]-3,5,6-triméthylcyclohexa-2,5-diène-1,4-dione
vatiquinona 2-[(3R,6E,10E]-3-hidroxi-3,7,11,15-tetrametilhexadeca-6,10,14-trien-1-il]-3,5,6-trimetilciclohexa-2,5-dieno-1,4-diona
C29H44O3
CH3
CH3
CH3CH3CH3CH3HOH3C
H3C
O
O
vedroprevirum vedroprevir 1-{[(2S,4R)-1-{(2S)-2-[({[(1R,3r,5S)-bicyclo[3.1.0]hexan-
3-yl]oxy}carbonyl)amino]-3,3-dimethylbutanoyl}-4-((8-chloro- 7-[2-(morpholin-4-yl)ethoxy]-2-{2-[(propan-2-yl)amino]-1,3-thiazol- 4-yl}quinolin-4-yl)oxy]pyrrolidin-2-yl]carbonylamino}- 2-ethylcyclopropane-1-carboxylic acid
védroprévir acide 1-{[(2S,4R)-1-{(2S)-2-[({[(1R,3r,5S)-bicyclo[3.1.0]hexan- 3-yl]oxy}carbonyl)amino]-3,3-diméthylbutanoyl}-4-((8-chloro- 7-[2-(morpholin-4-yl)éthoxy]-2-{2-[(propan-2-yl)amino]-1,3-thiazol- 4-yl}quinoléin-4-yl)oxy]pyrrolidin-2-yl]carbonylamino}- 2-éthylcyclopropane-1-carboxylique
vedroprevir ácido 1-{[(2S,4R)-1-{(2S)-2-[({[(1R,3r,5S)-biciclo[3.1.0]hexan- 3-il]oxi}carbonil)amino]-3,3-dimetilbutanoil}-4-((8-cloro-7-[2-(morfolin-4-il)etoxi]-2-{2-[(propan-2-il)amino]-1,3-tiazol-4-il}quinolin- 4-il)oxi]pirrolidin-2-il]carbonilamino}-2-etilciclopropano-1-carboxílico

Recommended INN: List 71 WHO Drug Information, Vol. 28, No. 1, 2014
116
C45H60ClN7O9S
O NH
O
N
O
H3C CH3
CH3
H
HN
O
HCO2H
OH
N
H
CH3
O
Cl
N
SNH
CH3H3C
HH
H
N
O
vericiguatum vericiguat methyl [4,6-diamino-2-{5-fluoro-1-[(2-fluorophenyl)methyl]-
1H-pyrazolo[3,4-b]pyridin-3-yl}pyrimidin-5-yl]carbamate
vériciguat [4,6-diamino-2-{5-fluoro-1-[(2-fluorophényl)méthyl]-1H-pyrazolo[3,4-b]pyridin-3-yl}pyrimidin-5-yl]carbamate de méthyle
vericiguat N-{4,6-diamino-2-[5-fluoro-1-[(2-fluorofenil)metil]-1H-pirazolo[3,4-b]-piridin-3-il]pirimidin-5-il}carbamato de metilo
C19H16F2N8O2
N
N
NH2HN O
NN
N
F NH2O
CH3
F
vilaprisanum vilaprisan 20,20,21,21,21-pentafluoro-17-hydroxy-
11β-[4-(methanesulfonyl)phenyl]-19-nor-17α-pregna-4,9-dien-3-one
vilaprisan 20,20,21,21,21-pentafluoro-17-hydroxy- 11β-[4-(méthanesulfonyl)phényl]-19-nor-17α-prégna-4,9-dién-3-one
vilaprisán 20,20,21,21,21-pentafluoro-17-hidroxi-11β-[4-(metanosulfonil)fenil]-19-nor-17α-pregna-4,9-dien-3-ona
C27H29F5O4S
OH
O
SH3C
H
CH3
H
H CF3
FF
OO

WHO Drug Information, Vol. 28, No. 1, 2014 Recommended INN: List 71
117
voruciclibum voruciclib 2-[2-chloro-4-(trifluoromethyl)phenyl]-5,7-dihydroxy-
8-[(2R,3S)-2-(hydroxymethyl)-1-methylpyrrolidin-3-yl]- 4H-1-benzopyran-4-one
voruciclib 2-[2-chloro-4-(trifluoromethyl)phenyl]-5,7-dihydroxy- 8-[(2R,3S)-2-(hydroxymethyl)-1-methylpyrrolidin-3-yl]- 4H-1-benzopyran-4-one
voruciclib 2-[2-cloro-4-(trifluorometil)fenil]-5,7-dihidroxi- 8-[(2R,3S)-2-(hidroximetil)-1-metilpirrolidin-3-il]-4H-1-benzopiran- 4-ona
C22H19ClF3NO5
O
O
HO
OH
N
HH
CH3
OHCl CF3
# Electronic structure available on Mednet: http://mednet.who.int/ # Structure électronique disponible sur Mednet: http://mednet.who.int/ # Estructura electrónica disponible en Mednet: http://mednet.who.int/ * http://www.who.int/entity/medicines/services/inn/Radical_Book_2012.pdf

Recommended INN: List 71 WHO Drug Information, Vol. 28, No. 1, 2014
118
AMENDMENTS TO PREVIOUS LISTS
MODIFICATIONS APPORTÉES AUX LISTES ANTÉRIEURES MODIFICACIONES A LAS LISTAS ANTERIORES
Recommended International Nonproprietary Names (Rec. INN): List 1 (Chron. Wld Hlth Org., Vol. 9, No 6, 1955) p. 190 delete insert methacholinii chloridum methacholini chloridum
methacholinium chloride methacholine chloride
Dénominations communes internationales recommandées (DCI rec.): Liste 1 (Chron. Org. mond. Santé, Vol. 9, No 6, 1955) p. 206 supprimer insérer methacholinii chloridum methacholini chloridum chlorure de méthacholinium chlorure de méthacholine Denominaciones Comunes Internacionales Recomendadas (DCI Rec.): Lista 1 (Crón. Org. mund. Salud, Vol. 9, No 6, 1955) p. 209 suprimáse insertese methacholinii chloridum methacholini chloridum cloruro de metacolinio cloruro de metacolina Recommended International Nonproprietary Names (Rec. INN): List 3 (Chron. Wld Hlth Org., Vol. 13, No. 12, 1959) p. 463 delete insert acetylcholinii chloridum acetylcholini chloridum
p. 465 delete insert cholinii chloridum cholini chloridum
p. 470 delete insert nitricholinii perchloras nitricholini perchloras nitricholinium perchlorate nitricholine perchlorate
Dénominations communes internationales recommandées (DCI rec.): Liste 3 (Chron. Org. mond. Santé, Vol. 13, No. 12, 1959) p. 482 supprimer insérer acetylcholinii chloridum acetylcholini chloridum

WHO Drug Information, Vol. 28, No. 1, 2014 Recommended INN: List 71
119
p. 484 supprimer insérer cholinii chloridum cholini chloridum
p. 489 supprimer insérer nitricholinii perchloras nitricholini perchloras perchlorate de nitricholinium perchlorate de nitricholine Denominaciones Comunes Internacionales Recomendadas (DCI Rec.): Lista 3 (Crón. Org. mund. Salud, Vol. 13, No. 12, 1959) p. 496 suprimáse insertese acetylcholinii chloridum acetylcholini chloridum
p. 498 suprimáse insertese cholinii chloridum cholini chloridum
p. 503 suprimáse insertese nitricholinii perchloras nitricholini perchloras perclorato de nitricolinio perclorato de nitrocolina Recommended International Nonproprietary Names (Rec. INN): List 4 (Chron. Wld Hlth Org., Vol. 16, No. 3, 1962) p. 103 delete insert cholinii gluconas cholini gluconas cholinium gluconate choline gluconate Dénominations communes internationales recommandées (DCI rec.): Liste 4 (Chron. Org. mond. Santé, Vol. 16, No. 3, 1962) p. 114 supprimer insérer cholinii gluconas cholini gluconas gluconate de cholinium gluconate de choline Denominaciones Comunes Internacionales Recomendadas (DCI Rec.): Lista 4 (Crón. Org. mund. Salud, Vol. 16, No. 3, 1962) p. 154 suprimáse insertese cholinii gluconas cholini gluconas gluconato de colinio gluconato de colina

Recommended INN: List 71 WHO Drug Information, Vol. 28, No. 1, 2014
120
Recommended International Nonproprietary Names (Rec. INN): List 62 Dénominations communes internationales recommandées (DCI Rec.): Liste 62 Denominaciones Comunes Internacionales Recomendadas (DCI Rec.): Lista 62 (WHO Drug Information, Vol. 23, No. 3, 2009) p. 258 & ramucirumabum # 259 ramucirumab replace the description and the structure by the following ones ramucirumab remplacer la description et la structure par les suivantes ramucirumab sustitúyase la descripción y la estructura por los siguientes
immunoglobulin G1-kappa, anti-[Homo sapiens KDR (kinase insert domain receptor,
vascular endothelial growth factor receptor 2, VEGFR2, VEGF-R2, FLK1, CD309) extracellular domain], Homo sapiens monoclonal antibody; gamma1 heavy chain (1-446) [Homo sapiens VH (IGHV3-21*01(99.00%) -(IGHD)-IGHJ3*02) [8.8.9] (1-116) - IGHG1*03 (CH1 F5>L (125), hinge (215-229), CH2 (230-339), CH3 (340-444), CHS (445-446)) (117-446)], (219-214')-disulfide with kappa light chain (1'-214') [Homo sapiens V-KAPPA (IGKV1-12*01 (85.30%) -IGKJ4*01 E125>D (105)) [6.3.9] (1'-107') -IGKC*01 (108'-214')]; dimer (225-225'':228-228'')-bisdisulfide
immunoglobuline G1-kappa, anti-[Homo sapiens KDR (récepteur à domaine insert kinase, récepteur 2 du facteur de croissance endothélial vasculaire, VEGFR2, VEGF-R2, FLK1, CD309) domaine extracellulaire], Homo sapiens anticorps monoclonal; chaîne lourde gamma1 (1-446) [Homo sapiens VH (IGHV3-21*01 (99.00%) -(IGHD)-IGHJ3*02) [8.8.9] (1-116) -IGHG1*03 (CH1 F5>L (125), charnière (215-229), CH2 (230-339), CH3 (340-444), CHS (445-446)) (117-446)], (219-214')-disulfure avec la chaîne légère kappa (1'-214') [Homo sapiens V-KAPPA (IGKV1-12*01 (85.30%) -IGKJ4*01 E125>D (105)) [6.3.9] (1'-107') -IGKC*01 (108'-214')]; dimère (225-225'':228-228'')-bisdisulfure
inmunoglobulina G1-kappa, anti-[Homo sapiens KDR (receptor con dominio insert-kinasa, receptor 2 del factor de crecimiento endotelial vascular, VEGFR2, VEGF-R2, FLK1, CD309) dominio extracelular], Homo sapiens anticuerpo monoclonal; cadena pesada gamma1 (1-446) [Homo sapiens VH (IGHV3-21*01 (99.00%) -(IGHD)-IGHJ3*02) [8.8.9] (1-116) -IGHG1*03 (CH1 F5>L (125), bisagra (215-229), CH2 (230-339), CH3 (340-444), CHS (445-446)) (117-446)], (219-214')-disulfuro con la cadena ligera kappa (1'-214') [Homo sapiens V-KAPPA (IGKV1-12*01 (85.30%) -IGKJ4*01 E125>D (105)) [6.3.9] (1'-107') -IGKC*01 (108'-214')]; dímero (225-225'':228-228'')-bisdisulfuro
Heavy chain / Chaîne lourde / Cadena pesadaEVQLVQSGGG LVKPGGSLRL SCAASGFTFS SYSMNWVRQA PGKGLEWVSS 50ISSSSSYIYY ADSVKGRFTI SRDNAKNSLY LQMNSLRAED TAVYYCARVT 100DAFDIWGQGT MVTVSSASTK GPSVLPLAPS SKSTSGGTAA LGCLVKDYFP 150EPVTVSWNSG ALTSGVHTFP AVLQSSGLYS LSSVVTVPSS SLGTQTYICN 200VNHKPSNTKV DKRVEPKSCD KTHTCPPCPA PELLGGPSVF LFPPKPKDTL 250MISRTPEVTC VVVDVSHEDP EVKFNWYVDG VEVHNAKTKP REEQYNSTYR 300VVSVLTVLHQ DWLNGKEYKC KVSNKALPAP IEKTISKAKG QPREPQVYTL 350PPSREEMTKN QVSLTCLVKG FYPSDIAVEW ESNGQPENNY KTTPPVLDSD 400GSFFLYSKLT VDKSRWQQGN VFSCSVMHEA LHNHYTQKSL SLSPGK 446
Light chain / Chaîne légère / Cadena ligeraDIQMTQSPSS VSASIGDRVT ITCRASQGID NWLGWYQQKP GKAPKLLIYD 50ASNLDTGVPS RFSGSGSGTY FTLTISSLQA EDFAVYFCQQ AKAFPPTFGG 100GTKVDIKRTV AAPSVFIFPP SDEQLKSGTA SVVCLLNNFY PREAKVQWKV 150DNALQSGNSQ ESVTEQDSKD STYSLSSTLT LSKADYEKHK VYACEVTHQG 200LSSPVTKSFN RGEC 214
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H22-96 143-199 260-320 366-424 22''-96''143''-199''260''-320''366''-424''Intra-L23'-88' 134'-194' 23'''-88'''134'''-194'''Inter-H-L (h 5-CL 126)219-214'219''-214'''Inter-H-H (h 11, h 14)225-225''228-228''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:296, 296''

WHO Drug Information, Vol. 28, No. 1, 2014 Recommended INN: List 71
121
Recommended International Nonproprietary Names (Rec. INN): List 67 Dénominations communes internationales recommandées (DCI Rec.): Liste 67 Denominaciones Comunes Internacionales Recomendadas (DCI Rec.): Lista 67 (WHO Drug Information, Vol. 26, No. 1, 2012) p. 91 upamostatum upamostat replace the chemical name by the following one upamostat remplacer le nom chimique par le suivant upamostat sustitúyase el nombre químico por el siguiente ethyl 4-{(2S)-3-{3-[(E)-N'-hydroxycarbamimidoyl]phenyl}-
2-[2,4,6-tri(propan-2-yl)benzenesulfonamido]propanoyl}piperazine- 1-carboxylate}
4-{(2S)-3-{3-[(E)-N'-hydroxycarbamimidoyl]phényl}- 2-[2,4,6-tri(propan-2-yl)benzènesulfonamido]propanoyl}pipérazine- 1-carboxylate d'éthyle
4-{(2S)-3-{3-[(E)-N’-hidroxicarbamimidoil]fenil}-2-[2,4,6-tri(propan- 2-il)bencenosulfonamido]propanoil}piperazina-1-carboxilato de etilo
Recommended International Nonproprietary Names (Rec. INN): List 69 Dénominations communes internationales recommandées (DCI Rec.): Liste 69 Denominaciones Comunes Internacionales Recomendadas (DCI Rec.): Lista 69 (WHO Drug Information, Vol. 27, No. 1, 2013) p. 82 tenapanorum tenapanor replace the chemical name by the following one ténapanor remplacer le nom chimique par le suivant tenapanor sustitúyase el nombre químico por el siguiente N,N'-(10,17-dioxo-3,6,21,24-tetraoxa-9,11,16,18-tetraazahexacosane-
1,26-diyl)bis{3-[(4S)-6,8-dichloro-2-methyl-1,2,3,4-tetrahydroisoquinolin- 4-yl]benzenesulfonamide}
N,N'-(10,17-dioxo-3,6,21,24-tétraoxa-9,11,16,18-tétraazahexacosane- 1,26-diyl)bis{3-[(4S)-6,8-dichloro-2-méthyl-1,2,3,4-tétrahydroisoquinoléin- 4-yl]benzènesulfonamide}
N,N'-(10,17-dioxo-3,6,21,24-tetraoxa-9,11,16,18-tetraazahexacosano- 1,26-diyl)bis{3-[(4S)-6,8-dicloro-2-metil-1,2,3,4-tetrahidroisoquinolin- 4-il]bencenosulfonamida}
Recommended International Nonproprietary Names (Rec. INN): List 70 Dénominations communes internationales recommandées (DCI Rec.): Liste 70 Denominaciones Comunes Internacionales Recomendadas (DCI Rec.): Lista 70 (WHO Drug Information, Vol. 27, No. 3, 2013) p. 306 polatuzumabum vedotinum # & 307 polatuzumab vedotin replace the description by the following one polatuzumab védotine remplacer la description par la suivante polatuzumab vedotina sustitúyase la descripción por la siguiente immunoglobulin G1-kappa auristatin E conjugate, anti-[Homo sapiens CD79B
(immunoglobulin-associated CD79 beta)], humanized monoclonal antibody conjugated to auristatin E; gamma1 heavy chain (1-447) [humanized VH (Homo sapiens IGHV3-23*04 (76.50%) -(IGHD)-IGHJ4*01) [8.8.10] (1-117) -Homo sapiens IGHG1*03 (CH1 R120>K (214) (118-215), hinge (216-230), CH2 (231-340), CH3 (341-445), CHS (446-447)) (118-447)], (220-218')-disulfide with kappa light chain (1’-218’) [humanized V-KAPPA (Homo sapiens IGKV1-39*01 (85.90%) -IGKJ1*01) [10.3.9] (1'-111') -Homo sapiens IGKC*01 (112'-218')]; dimer (226-226":229-229")-bisdisulfide; conjugated, on an average of 3 to 4 cysteinyl, to monomethylauristatin E (MMAE), via a cleavable maleimidocaproyl-valyl-citrullinyl- p-aminobenzyloxycarbonyl (mc-val-cit-PABC) type linker For the vedotin part, please refer to the document “INN for pharmaceutical substances: Names for radicals, groups and others”*.

Recommended INN: List 71 WHO Drug Information, Vol. 28, No. 1, 2014
122
immunoglobuline G1-kappa conjuguée à l’auristatine E, anti-[Homo sapiens CD79B (CD79 bêta associé à l’immunoglobuline)], anticorps monoclonal humanisé conjugué à l’auristatine E; chaîne lourde gamma1 (1-447) [VH humanisé (Homo sapiens IGHV3-23*04 (76.50%) -(IGHD)-IGHJ4*01) [8.8.10] (1-117) -Homo sapiens IGHG1*03 (CH1 R120>K (214) (118-215), charnière (216-230), CH2 (231-340), CH3 (341-445), CHS (446-447)) (118-447)], (220-218')-disulfure avec la chaîne légère kappa (1’-218’) [V-KAPPA humanisé (Homo sapiens IGKV1-39*01 (85.90%) -IGKJ1*01) [10.3.9] (1'-111') -Homo sapiens IGKC*01 (112'-218')]; dimère (226-226":229-229")-bisdisulfure; conjugué, sur 3 à 4 cystéinyl en moyenne, au monométhylauristatine E (MMAE), via un linker clivable de type maléimidocaproyl-valyl-citrullinyl-p-aminobenzyloxycarbonyl (mc-val-cit-PABC) Pour la partie védotine, veuillez vous référer au document “INN for pharmaceutical substances: Names for radicals, groups and others”*.
inmunoglobulina G1-kappa conjugada con auristatina E, anti-[Homo sapiens CD79B (CD79 beta associado a la inmunoglobulina)], anticuerpo monoclonal humanizado conjugado con auristatina E; cadena pesada gamma1 (1-447) [VH humanizado (Homo sapiens IGHV3-23*04 (76.50%) -(IGHD)-IGHJ4*01) [8.8.10] (1-117) -Homo sapiens IGHG1*03 (CH1 R120>K (214) (118-215), bisagra (216-230), CH2 (231-340), CH3 (341-445), CHS (446-447)) (118-447)], (220-218')-disulfuro con la cadena ligera kappa (1’-218’) [V-KAPPA humanizado (Homo sapiens IGKV1-39*01 (85.90%) -IGKJ1*01) [10.3.9] (1'-111') -Homo sapiens IGKC*01 (112'-218')]; dímero (226-226":229-229")-bisdisulfuro; conjuguado, en 3 a 4 restos cisteinil por término medio, con monometilauristatina E (MMAE), mediante un vínculo escindible maleimidocaproil-valil-citrullinil- p-aminobenziloxicarbonil (mc-val-cit-PABC) Para la fracción vedotina se pueden referir al documento "INN for pharmaceutical substances: Names for radicals, groups and others"*.
p. 313 sofosbuvirum sofosbuvir replace the structure by the following one sofosbuvir remplacer la structure par la suivante sofosbuvir sustitúyase la estructura por la siguiente
O N
HN
OP
NH
OH3C
O OOO
HO FCH3
OCH3
HH3C
Procedure and Guiding Principles / Procédure et Directives / Procedimientos y principios generales The text of the Procedures for the Selection of Recommended International Nonproprietary Names for Pharmaceutical Substances and General Principles for Guidance in Devising International Nonproprietary Names for Pharmaceutical Substances will be reproduced in proposed INN lists only. Les textes de la Procédure à suivre en vue du choix de dénominations communes internationales recommandées pour les substances pharmaceutiques et des Directives générales pour la formation de dénominations communes internationales applicables aux substances pharmaceutiques seront publiés seulement dans les listes des DCI proposées. El texto de los Procedimientos de selección de denominaciones comunes internacionales recomendadas para las sustancias farmacéuticas y de los Principios generales de orientación para formar denominaciones comunes internacionales para sustancias farmacéuticas aparece solamente en las listas de DCI propuestas.

WHO Drug Information, Vol. 28, No. 1, 2014 Recommended INN: List 71
123