Embed Size (px)
Citation preview
359
WHO Drug Information Vol. 30, No. 3, 2016
Contents
Regulatory collaboration361 IGDRP generic drug product regulatory gap
analysis
Generic medicines370 InterchangeabilityofWHO-prequalified
generics
Adopted guidance376WHOCertificationSchemeonthequality
ofpharmaceuticalproductsmovingininternationalcommerce: Questions and Answers (Q & A)
Safety news389 Safety warnings
Warfarin : calciphylaxis ;Eltrombopag:potentiallyfatalliverinjury;Etonogestrel implants:migrationfrominsertionsite;Ombitasvir/paritaprevir/ritonavir:
acute renal failure ;Carmustineintracerebralimplant:riskofairaccumulation
;Blinatumomab: pancreatitis; Idelalisib :updatedmeasurestomanageriskofinfections;Opioids and benzodiazepines :potentiallyfatalsideeffects; Levetiracetam: acute renal failure ;Citalopram: suspected drug interaction with cocaine;
392 RestrictionsRiociguat :notforpatientswithpulmonaryhypertensioncausedbyidiopathicinterstitialpneumonia; Fluoroquinolones : use only in certain serious infections;
392 Known risksCanagliflozin,dapagliflozin:kidneyinjury;Apixaban :Liverfunctiondisorder;
393 ClarificationofindicationsFingolimod:notproveninprogressivemultiplesclerosis;
393 Medical device-relatedBloodclottingtimemeasuringdevices: inaccurate
readings;N-acetylcysteineandbiochemistryassays394 Medicines safety reviews started
Dapagliflozin,empagliflozin; Factor VIII-containingmedicines;Modified-andprolongedreleaseparacetamol;Retinoid medicines
395 Non-compliance with good practicesAlkemLaboratoriesLtd,India: data integrity issues;Quest Life SciencesPvtLtd,India: data integrity issues;SemlerResearchCentrePvtLtd,India:EMAreviewconcluded; ZhejiangMedicineCoLtd,China:unreportedimpuritytestingresults;PharmaceuticsInternationalInc.,U.S.:non-compliancewithGMP;ShanghaiDesanoCoLtd,China:non-compliancewith
GMP; LaxachemOrganicsPvtLtd,India:importbanforrefusalofinspection;
398 FalsifiedmedicinesFalsifiedquininesulphatecirculatinginWestand Central Africa
Regulatory news399 Pre-market assessment
EMAreportonadaptivepathwayspilot;Experiencesinpublishingassessmentreports
399 CollaborationEMA and FDA collaborate on patient engagement
400 Post-market surveillanceNewEMAguidanceonmonitoringofbiologicalmedicines;ReportonpharmacovigilanceactivitiesinEurope
401 Good manufacturing practiceEMA adopts data integrity guidelines
401 LabellingImprovedproductlabelsinCanada
401 AntibioticsEMArecommendsreducingveterinaryuseof colistin;Globalimplicationsofantibioticscontrol in India; Tripartitemeetingonevaluationofnewantibacterialagents
402 Controlled substancesTighter control of W-18 in Canada;Canada proposes scheduling of fentanyl precursors
403 Blood safetyShorterdeferralperiodforMSMinCanada;AllU.S.blooddonationstobescreenedforZikavirus
404 Under discussion
405 ApprovedLixisenatide : for type 2 diabetes; Choleravaccine; Lifitegrast:
for dry eye disease; Cell-basedtherapytosupportstemcelltransplant in blood cancer patients
405 BiosimilarEtanercept-szzs
406 Extensions of indicationsEmtricitabine&tenofovirdisoproxil: for HIV pre-exposure prophylaxis;
Cabozantib,lenvatinib:approvedintheEUforkidneycancer;
406 Interim import approvalNaloxone nasal spray :topreventdeathsfromopioidoverdose;
406 DiagnosticsAssaytodetectmarkersforantibioticresistance
Continued
WHO Drug Information
WHODrugInformationVol.30,No.3,2016
360
Publications and events407 Access to medicines
UNHRCresolutiononaccesstomedicines;WHOtoconvenestakeholdersonfairmedicinespricing;New book on intellectual property rules and access tomedicines;Medicines Patent Pool signs new licences;Hepatitis C patent landscape; Insulin patent landscape
408 PharmacovigilanceTwonewCIOMSpublications
409 Disease updatesPoliovirus:publichealthemergencyofinternationalconcern; Zika :publichealthemergencycontinues;Sexuallytransmittedinfections :newWHOtreatmentguidelines;Non-communicablediseases:uneven
progress;Hepatitis B and C :needformoreaccesstotestingandtreatment;HIV411 Vaccines
Yellowfeveremergencyvaccinationcampaigns;Globalvaccinequalitycontrollaboratoriesnetworkingmeeting
412 WHO mattersNewWHOguidelinewelcomed;WHO PrequalificationTeamoffersGMPpre-inspections ;MQASFinishedpharmaceuticalproduct questionnaire posted
Consultation documents414 The International Pharmacopoeia414 Chlorhexidine digluconate solution421 Chlorhexidine digluconate topical solution424 Medroxyprogesterone acetate 429 Medroxyprogesteroneinjection432 Clindamycinpalmitatehydrochloride435 Clindamycinpalmitatefororalsuspension438 Clindamycinphosphate445 Clindamycinphosphateinjection448 Ceftriaxonesodium452 Ceftriaxoneforinjection455 Mebendazole459 Mebendazole chewable tablets 463 Methylthioniniumchloride468 Methylthioniniuminjection471 Proposedrevisionofthegeneralchapter
1.11 Colour of liquids
International Nonproprietary Names (INN)477 RecommendedINN:List76
Continued
Abbreviations and web sites
CHMP CommitteeforMedicinalProductsforHumanUse(EMA)EMA European Medicines Agency (www.ema.europa.eu)EU EuropeanUnionFDA U.S.FoodandDrugAdministration(www.fda.gov)HealthCanadaFederaldepartmentresponsibleforhealthproductregulationinCanada(www.hc-sc.gc.ca)MHLW MinistryofHealth,LabourandWelfare,JapanMHRA MedicinesandHealthcareProductsRegulatoryAgency,UnitedKingdom
(www.mhra.gov.uk)Medsafe NewZealandMedicinesandMedicalDevicesSafetyAuthority(www.medsafe.govt.nz)PRAC PharmacovigilanceRiskAssessmentCommittee(EMA)PMDA PharmaceuticalsandMedicalDevicesAgency,Japan(www.pmda.go.jp/english/index.htm)Swissmedic SwissAgencyforTherapeuticProducts(www.swissmedic.ch)TGA TherapeuticGoodsAdministration,Australia(www.tga.gov.au)U.S. UnitedStatesofAmerica
Note:Theonlineversionofthisissue(freelyavailableatwww.who.int/medicines/publications/druginformation) hasdirectclickablehyperlinkstothedocumentsandwebpagesreferenced.
361
WHO Drug Information Vol. 30, No. 3, 2016
Regulatory collaborationIGDRP generic drug product regulatory gap analysis
The International Generic Drug Regulators Pilot (IGDRP) was launched in 2012 as an international collaborative initiative for information- and work-sharing activities for the regulation and registration of generic drug products. Initially operating as a three-year pilot (2011–2014) the IGDRP was renamed a Programme in 2014, recognizing the progress achieved during the pilot phase, the strong commitment from regulators and their continued interest and need to cooperate to facilitate the timely authorization and availabilityofsafe,effectiveandhighqualitygenericdrugproducts.
A regulatory gap analysis survey was conducted to identify regulatory similarities amongst the IGDRP members as well as gaps that might create challengesforwork-sharingandcollaboration.TheWHOPrequalificationTeam, the European Union (EU) and eleven regulatory authorities participatedinthesurvey.Themaingapsobservedwere:thedefinitionofa generic drug product and what is considered to be the same active (or drug) substance; whether and when international reference products can beusedinbioequivalencestudies;thecriteriaforgrantingbiowaivers;requirementstousenationalorregionalpharmacopoeias;andtheminimum stability data to be included in a generic drug product application at the time of submission.
IntroductionThe International Generic Drug Regulator Programme(IGDRP),portrayedinanearlierissueofthisjournal(1),hasthemissiontopromotecollaborationandregulatoryconvergenceintheareaof generic drug products in order to strengthen the ability of health authorities tomeettheirrespectivemandates.Itsgoalistofacilitatethetimelyauthorizationandavailabilityofsafe,efficaciousandqualitygeneric drug products.Oneoftheenablersagreedamong
IGDRP participants to facilitate work-sharing was the conduct of a regulatory
gapanalysissurveytoidentifythesimilaritiesanddifferencesinregulatoryrequirementsandpracticesofparticipatingIGDRPmembersregardinggenericapplications.
The gap analysis surveyThesurveywasledbytheBrazilianHealthRegulatoryAgency(ANVISA).Itwasdividedintofourparts:1. Generalissues/referenceproducts;2. Bioequivalence/biowaivers;3.Qualityandgoodmanufacturingpractices(GMP);and
4. Other issues.
ThegapanalysissurveydescribedinthisarticlewasledbythemedicinesregulatoryauthorityofBrazil,ANVISA.WethankAnaCarolinaMoreiraMarinoAraujoandherteamatANVISAforcontributingthisarticle.on behalf of IGDRP.
Regulatory collaboration WHODrugInformationVol.30,No.3,2016
362
Participating organizationsThesurveywasansweredbyrepresenta-tivesoftheWHOPrequalificationTeam(WHO-PQT)1,theEuropeanUnionregulatorysystem(referredtoas“EU”inthis article) and 11 regulatory authorities including:Australia’sTherapeuticGoodsAdministration(TGA),theBrazilianHealthRegulatoryAgency(ANVISA),HealthCanada(HC),Japan’sPharmaceuticalsandMedicalDevicesAgency(PMDA),SouthKorea’sMinistryofFoodandDrugSafety(MFDS),Mexico’sFederalCommissionforProtectionagainstSanitaryRisks(COFEPRIS),Singapore’sHealthSciencesAuthority(HSA),SouthAfrica´s Medicines Control Council (MCC),theSwissAgencyforTherapeuticProducts(Swissmedic),theTaiwanFoodandDrugAdministration(TFDA)andtheUnitedStatesFoodandDrugAdministration(U.S.FDA).
TimelinesTheinitialgapanalysissurveytoolwaspresentedduringthefirstIGDRPmeetingheldinWashington,DC,USAinApril2012.Itwasagreedthatparticipantsshouldreviewthetoolandprovideadditionalcomments.
All organizations had the opportunity tocommentonthequestionsandtoupdate their answers. The data were furtherevaluatedandvalidatedduringsubsequentmeetingsandinteractions.TheresultspresentedinthisarticlereflectupdatedresponsesasofApril2016.
1 WHOPrequalificationTeam-Medicines; http://apps.who.int/prequal
Findings
1. General issues/reference products
▪ Definitionof“genericdrugproduct”All organizations answered that a genericproductmustfulfilthefollowingcriteria:samequantitativeandqualitativecompositionintermsofactive(ordrug)substance,same(orcomparable)dosageform,samerouteofadministration,andbioequivalencewiththereferenceproduct.However,thereweredifferencesindefiningwhatisconsideredthesameactive(ordrug)substance:TheTGA,HC,HSA,MCC,U.S.FDA,EU,SwissmedicandWHO-PQTacceptdifferentsaltsasthesameactive(ordrug)substance,provideditisthesameactivemoietyas the reference product and there are nosafetyandefficacyissueswiththedifferentformoftheactive(ordrug)substance.ANVISA,COFEPRIS,MFDS,PMDA and TFDA do not consider a differentsalttobethesameactive(ordrug) substance.
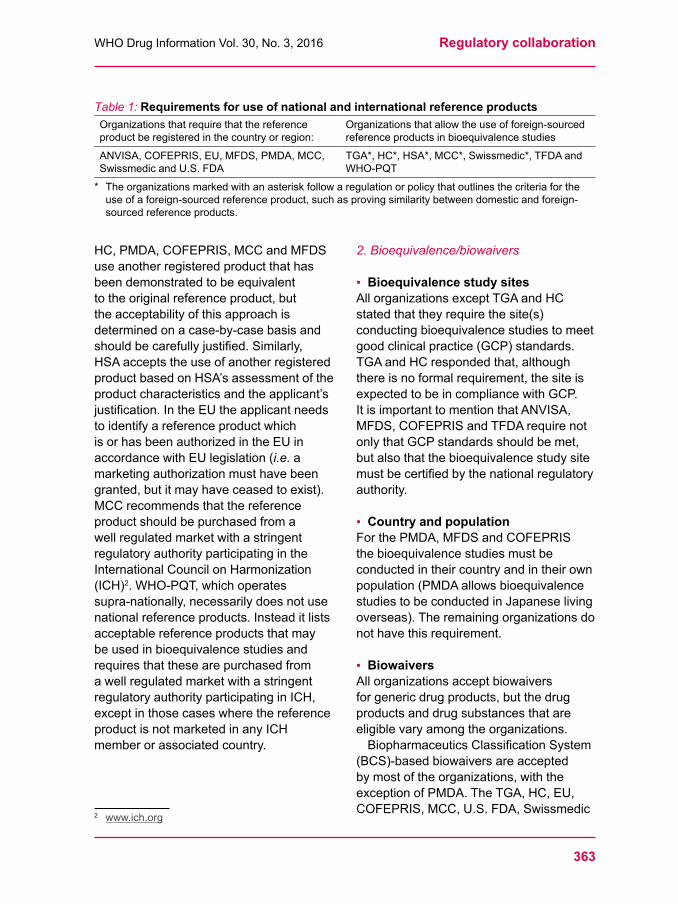
▪ RequirementsforreferenceproductThedefinitionofa“reference product” wassimilarforallorganizations:itistheinnovatorproduct thathasproveditssafety,efficacyandquality.However,notall organizations require that the reference productbemarketedorregisteredintheircountryorregion;somepermittheuseof foreign-sourced reference products (Table 1).
When the reference product is required to be sourced locally but the original referenceproduct–usuallytheinnovatorproduct–isnotavailableonthemarketinacountryorregion,itisnecessarytoidentify a new reference product. The variousorganizationshavedifferentapproachesfordoingso:TGA,ANVISA,
363
WHODrugInformationVol.30,No.3,2016 Regulatory collaboration
HC,PMDA,COFEPRIS,MCCandMFDSuse another registered product that has beendemonstratedtobeequivalenttotheoriginalreferenceproduct,butthe acceptability of this approach is determinedonacase-by-casebasisandshouldbecarefullyjustified.Similarly,HSAacceptstheuseofanotherregisteredproductbasedonHSA’sassessmentoftheproductcharacteristicsandtheapplicant’sjustification.IntheEUtheapplicantneedsto identify a reference product which isorhasbeenauthorizedintheEUinaccordancewithEUlegislation(i.e. a marketingauthorizationmusthavebeengranted,butitmayhaveceasedtoexist).MCCrecommendsthatthereferenceproductshouldbepurchasedfromawellregulatedmarketwithastringentregulatory authority participating in the InternationalCouncilonHarmonization(ICH)2.WHO-PQT,whichoperatessupra-nationally,necessarilydoesnotusenational reference products. Instead it lists acceptablereferenceproductsthatmaybeusedinbioequivalencestudiesandrequiresthatthesearepurchasedfromawellregulatedmarketwithastringentregulatoryauthorityparticipatinginICH,except in those cases where the reference productisnotmarketedinanyICHmemberorassociatedcountry.
2 www.ich.org
2. Bioequivalence/biowaivers
▪ BioequivalencestudysitesAll organizations except TGA and HC stated that they require the site(s) conductingbioequivalencestudiestomeetgood clinical practice (GCP) standards. TGAandHCrespondedthat,althoughthereisnoformalrequirement,thesiteisexpectedtobeincompliancewithGCP.ItisimportanttomentionthatANVISA,MFDS,COFEPRISandTFDArequirenotonlythatGCPstandardsshouldbemet,butalsothatthebioequivalencestudysitemustbecertifiedbythenationalregulatoryauthority.
▪ Country and populationForthePMDA,MFDSandCOFEPRISthebioequivalencestudiesmustbeconducted in their country and in their own population(PMDAallowsbioequivalencestudiestobeconductedinJapaneselivingoverseas).Theremainingorganizationsdonothavethisrequirement.
▪ BiowaiversAllorganizationsacceptbiowaiversforgenericdrugproducts,butthedrugproducts and drug substances that are eligiblevaryamongtheorganizations.BiopharmaceuticsClassificationSystem
(BCS)-basedbiowaiversareacceptedbymostoftheorganizations,withtheexceptionofPMDA.TheTGA,HC,EU,COFEPRIS,MCC,U.S.FDA,Swissmedic
Table 1:RequirementsforuseofnationalandinternationalreferenceproductsOrganizations that require that the reference productberegisteredinthecountryorregion:
Organizations that allow the use of foreign-sourced referenceproductsinbioequivalencestudies
ANVISA,COFEPRIS,EU,MFDS,PMDA,MCC,SwissmedicandU.S.FDA
TGA*,HC*,HSA*,MCC*,Swissmedic*,TFDAandWHO-PQT
* Theorganizationsmarkedwithanasteriskfollowaregulationorpolicythatoutlinesthecriteriafortheuseofaforeign-sourcedreferenceproduct,suchasprovingsimilaritybetweendomesticandforeign-sourced reference products.
Regulatory collaboration WHODrugInformationVol.30,No.3,2016
364
andWHO-PQTacceptBCS-basedbiowaiversforClassIandClassIIIdrugs,whereastheMFDS,HSA,ANVISAandTFDAacceptBCS-basedbiowaiversClassIdrugsonly.ANVISAandTFDAhavepositivelistsofthemedicinesthatareeligibleforbiowaivers.Allorganizationsacceptbiowaivers
for additional proportional strengths ofimmediate-releasesolidoraldrugproducts that are not included in the in vivo bioequivalencestudies,withtheappropriatescientificjustification.TheIGDRP’sBiowaiversWorking
Grouphasconductedaspecificandmoredetailedgapanalysisonthistopicasamechanismtoestablishacommonsetofconditionsforgrantingbiowaiversas well as expanding the application of
BCS-basedwaivers,additionalstrengthbiowaiversandbiowaiversforcertaindosageforms(e.g.oralandinjectablesolutions).
3. Quality and GMP
▪ Active pharmaceutical ingredients (API)
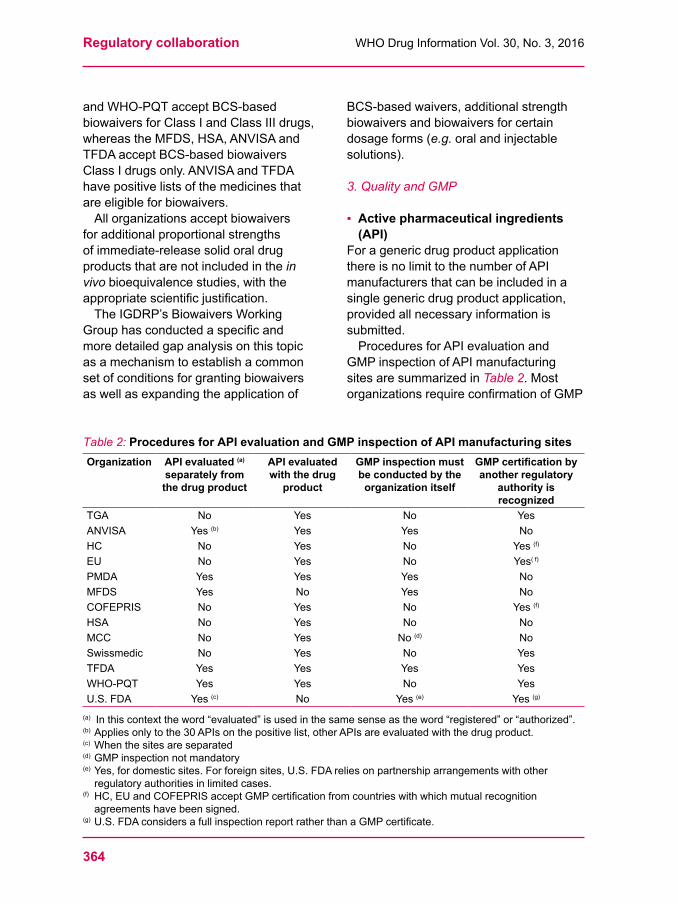
For a generic drug product application thereisnolimittothenumberofAPI manufacturersthatcanbeincludedinasinglegenericdrugproductapplication,providedallnecessaryinformationissubmitted.ProceduresforAPIevaluationand
GMPinspectionofAPImanufacturingsitesaresummarizedinTable 2. Most organizationsrequireconfirmationofGMP
Table 2: Procedures for API evaluation and GMP inspection of API manufacturing sitesOrganization API evaluated (a)
separately from the drug product
API evaluated with the drug
product
GMP inspection must be conducted by the
organization itself
GMPcertificationbyanother regulatory
authority is recognized
TGA No Yes No YesANVISA Yes (b) Yes Yes NoHC No Yes No Yes (f)
EU No Yes No Yes( f)
PMDA Yes Yes Yes NoMFDS Yes No Yes NoCOFEPRIS No Yes No Yes (f)
HSA No Yes No NoMCC No Yes No (d) NoSwissmedic No Yes No YesTFDA Yes Yes Yes YesWHO-PQT Yes Yes No YesU.S.FDA Yes (c) No Yes (e) Yes (g)
(a) Inthiscontexttheword“evaluated”isusedinthesamesenseastheword“registered”or“authorized”.(b) Appliesonlytothe30APIsonthepositivelist,otherAPIsareevaluatedwiththedrugproduct.(c) When the sites are separated(d) GMPinspectionnotmandatory(e) Yes,fordomesticsites.Forforeignsites,U.S.FDAreliesonpartnershiparrangementswithotherregulatoryauthoritiesinlimitedcases.
(f) HC,EUandCOFEPRISacceptGMPcertificationfromcountrieswithwhichmutualrecognitionagreementshavebeensigned.
(g) U.S.FDAconsidersafullinspectionreportratherthanaGMPcertificate.
365
WHODrugInformationVol.30,No.3,2016 Regulatory collaboration
complianceforAPImanufacturingsites,andmanyrequirethattheinspectionmustbe conducted by their own inspectorate. SomeIGDRPmembersrecognizeGMPcertificationbyotherauthorities,suchasstringentregulatoryauthorities(SRA)orregulatory authorities of countries with whichmutualrecognitionagreementshavebeensigned.Theorganizationsusedifferent
procedurestoevaluatethequalityinformationrelatedtothemanufactureandcontrolofAPIs.SomeauthorizeAPIsseparatelyfromthedrugproduct,others do so in connection with the marketingauthorizationapplicationforthedrugproduct,andinsomecasesbothprocedures are possible.TheTGA,HC,EU,HSA,MCC,
Swissmedic,TFDAandWHO-PQTrecognize the European Directorate for the QualityofMedicines–EDQM’scertificateof suitability (CEP) and do not duplicate theassessmentoftheAPIinformationcoveredbytheCEP.
▪ Stability studiesIngeneral,stabilitystudiesareconductedaspertherequirementsforthespecificclimaticzones(ZonesI,II,III,IVaandIVb)thatreflectacountry’sclimate(2). MostIGDRPmembersfollowtherecommendationsoftheICHQ1Aguideline (3). Three exceptions are HSA,ANVISAandWHO-PQT.TheseorganizationsrequirefinishedproductstabilitystudiesconductedinZoneIVb;HSAfollowstheASEANGuidelineonDrugProductStabilityData(4),ANVISAfollows its national guidelines for stability
studies (5),andWHO-PQTfollowsWHOstability guidelines (6).
All organizations require the stability study to be conducted with the drug substance or the drug product in its primarypackage.Ifthesecondarypackagehasaprotectiveorfunctionaleffect,thestudymaybeconductedinthispackage.ANVISAandTGArequireadditional
stability studies for the API in their own climaticzoneifitisimportedfromacountryinamilderclimaticzone.HSAevaluatesthestabilityimpactoftheAPIinthe drug product stability studies and does not require additional stability studies for the API.IftherearemultipleAPIorfinished
pharmaceuticalproduct(FPP)manufacturingsitesproposedforregistration,TGA,WHO-PQT,ANVISA,COFEPRIS,HSA,TFDAandMCCrequirestabilitydatafromallAPI–FPPsitecombinationsbutTGA,WHO-PQT,HSA,MCCandTFDAacceptscience-basedjustificationfornotrequiringallcombinationsofstabilitydata.HC,EU,PMDA,MFDSandSwissmedicdo not require the stability studies to be conducted with all API–FPP site combinations.ForPMDA,stabilitydatafortheAPI-FPPcombinationpreparedusingthemainmanufacturingroutemustbepresented,andthestabilitydataforothermanufacturingroutesmustbeconfirmedattheapplicant’sownresponsibility.Informationonthenumberofbatches
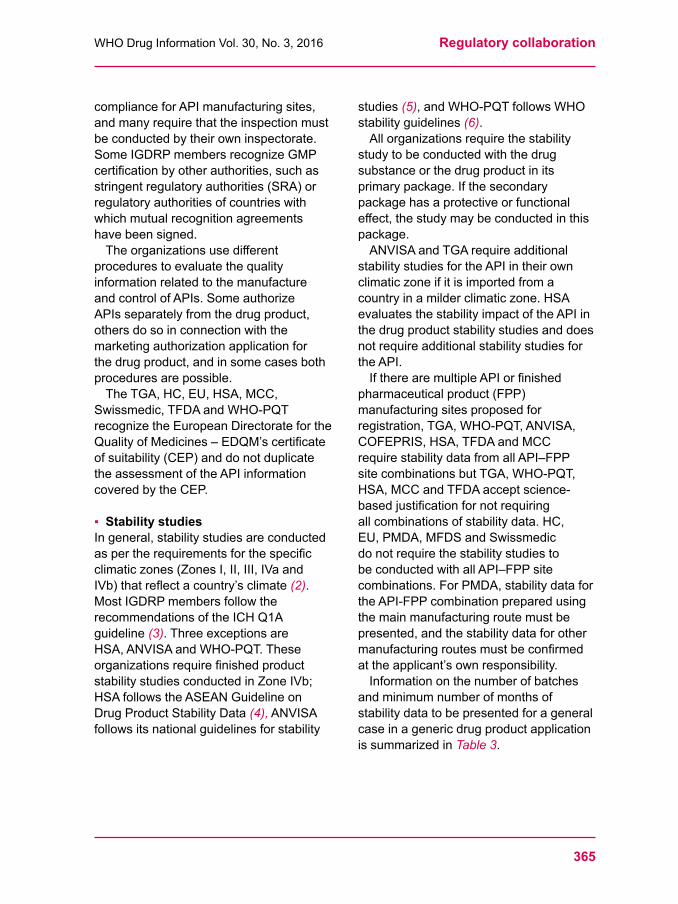
andminimumnumberofmonthsofstability data to be presented for a general case in a generic drug product application issummarizedinTable 3.
Regulatory collaboration WHODrugInformationVol.30,No.3,2016
366
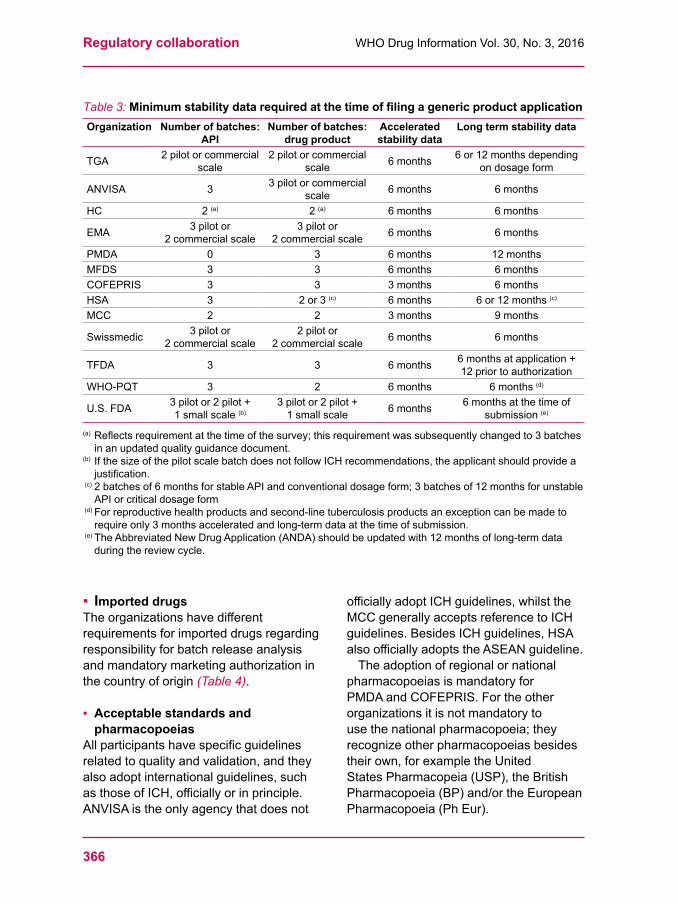
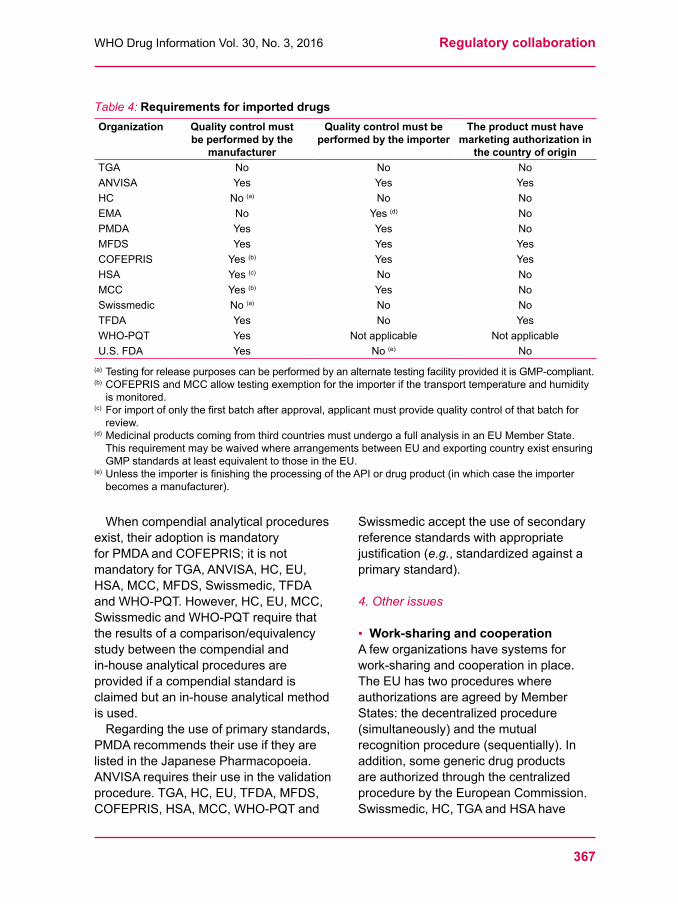
▪ Imported drugsTheorganizationshavedifferentrequirementsforimporteddrugsregardingresponsibility for batch release analysis andmandatorymarketingauthorizationinthe country of origin (Table 4).
▪ Acceptable standards and pharmacopoeias
Allparticipantshavespecificguidelinesrelatedtoqualityandvalidation,andtheyalsoadoptinternationalguidelines,suchasthoseofICH,officiallyorinprinciple.ANVISAistheonlyagencythatdoesnot
officiallyadoptICHguidelines,whilsttheMCC generally accepts reference to ICH guidelines.BesidesICHguidelines,HSAalsoofficiallyadoptstheASEANguideline.
The adoption of regional or national pharmacopoeiasismandatoryforPMDAandCOFEPRIS.Fortheotherorganizationsitisnotmandatorytousethenationalpharmacopoeia;theyrecognizeotherpharmacopoeiasbesidestheirown,forexampletheUnitedStatesPharmacopeia(USP),theBritishPharmacopoeia(BP)and/ortheEuropeanPharmacopoeia(PhEur).
Table 3:MinimumstabilitydatarequiredatthetimeoffilingagenericproductapplicationOrganization Number of batches:
APINumber of batches:
drug productAccelerated stability data
Long term stability data
TGA 2pilotorcommercialscale
2pilotorcommercialscale 6months 6or12monthsdepending
ondosageform
ANVISA 3 3pilotorcommercialscale 6months 6months
HC 2 (a) 2 (a) 6months 6months
EMA 3pilotor 2commercialscale
3pilotor 2commercialscale 6months 6months
PMDA 0 3 6months 12monthsMFDS 3 3 6months 6monthsCOFEPRIS 3 3 3months 6monthsHSA 3 2or3(c) 6months 6or12months(c)
MCC 2 2 3months 9months
Swissmedic 3pilotor 2commercialscale
2 pilot or 2commercialscale 6months 6months
TFDA 3 3 6months 6monthsatapplication+ 12 prior to authorization
WHO-PQT 3 2 6months 6months(d)
U.S.FDA 3pilotor2pilot+ 1smallscale(b)
3pilotor2pilot+ 1smallscale 6months 6monthsatthetimeof
submission(e)
(a) Reflectsrequirementatthetimeofthesurvey;thisrequirementwassubsequentlychangedto3batchesinanupdatedqualityguidancedocument.
(b) IfthesizeofthepilotscalebatchdoesnotfollowICHrecommendations,theapplicantshouldprovideajustification.
(c) 2batchesof6monthsforstableAPIandconventionaldosageform;3batchesof12monthsforunstableAPIorcriticaldosageform
(d) Forreproductivehealthproductsandsecond-linetuberculosisproductsanexceptioncanbemadetorequireonly3monthsacceleratedandlong-termdataatthetimeofsubmission.
(e) TheAbbreviatedNew Drug Application (ANDA) shouldbeupdatedwith12monthsoflong-termdataduringthereviewcycle.
367
WHODrugInformationVol.30,No.3,2016 Regulatory collaboration
Table 4:RequirementsforimporteddrugsOrganization Quality control must
be performed by the manufacturer
Quality control must be performed by the importer
The product must have marketing authorization in
the country of originTGA No No NoANVISA Yes Yes YesHC No (a) No NoEMA No Yes (d) NoPMDA Yes Yes NoMFDS Yes Yes YesCOFEPRIS Yes (b) Yes YesHSA Yes (c) No NoMCC Yes (b) Yes NoSwissmedic No (a) No NoTFDA Yes No YesWHO-PQT Yes Not applicable Not applicableU.S.FDA Yes No (e) No
(a) TestingforreleasepurposescanbeperformedbyanalternatetestingfacilityprovideditisGMP-compliant.(b) COFEPRISandMCCallowtestingexemptionfortheimporterifthetransporttemperatureandhumidityismonitored.
(c) Forimportofonlythefirstbatchafterapproval,applicantmustprovidequalitycontrolofthatbatchforreview.
(d) MedicinalproductscomingfromthirdcountriesmustundergoafullanalysisinanEUMemberState.ThisrequirementmaybewaivedwherearrangementsbetweenEUandexportingcountryexistensuringGMPstandardsatleastequivalenttothoseintheEU.
(e) UnlesstheimporterisfinishingtheprocessingoftheAPIordrugproduct(inwhichcasetheimporterbecomesamanufacturer).
Whencompendialanalyticalproceduresexist,theiradoptionismandatoryforPMDAandCOFEPRIS;itisnotmandatoryforTGA,ANVISA,HC,EU,HSA,MCC,MFDS,Swissmedic,TFDAandWHO-PQT.However,HC,EU,MCC,SwissmedicandWHO-PQTrequirethattheresultsofacomparison/equivalencystudybetweenthecompendialandin-house analytical procedures are providedifacompendialstandardisclaimedbutanin-houseanalyticalmethodis used.Regardingtheuseofprimarystandards,
PMDArecommendstheiruseiftheyarelistedintheJapanesePharmacopoeia.ANVISArequirestheiruseinthevalidationprocedure.TGA,HC,EU,TFDA,MFDS,COFEPRIS,HSA,MCC,WHO-PQTand
Swissmedicaccepttheuseofsecondaryreference standards with appropriate justification(e.g.,standardizedagainstaprimarystandard).
4. Other issues
▪ Work-sharing and cooperationAfeworganizationshavesystemsforwork-sharing and cooperation in place. TheEUhastwoprocedureswhereauthorizationsareagreedbyMemberStates:thedecentralizedprocedure(simultaneously)andthemutualrecognition procedure (sequentially). In addition,somegenericdrugproductsare authorized through the centralized procedurebytheEuropeanCommission.Swissmedic,HC,TGAandHSAhave

Regulatory collaboration WHODrugInformationVol.30,No.3,2016
368
a cooperation procedure under the Australia-Canada-Singapore-SwitzerlandConsortiumGenericsInitiative(theACSSConsortium),andHSAalsohasbilateralagreementsforwork-sharingongenericdrug products with Malaysia. HC is engagedinanumberofmulti-lateralandbilateralinternationalcooperationactivitiesregarding generic products but does not haveanymutualrecognitionagreementswith any other regulatory authority for the assessmentofgenerics.
▪ Performance targetsAllorganizationshavesetperformancetargetsortimelimitsfortheassessmentof generic drug product applications. It is importanttoidentifytheseperformancetargets for the work-sharing process. One of the enablers of the IGDRP is the constructionofatimelinewithtimelimitsanddetailedmilestones.
▪ Common Technical Document (CTD) TheTGA,HC,EU,HSA,MCC,MFDS,Swissmedic,U.S.FDA,TFDAandWHO-PQThaveofficiallyadoptedICH’sCommonTechnicalDocument(CTD)formatforgenericdrugproductapplications (7).PMDA,COFEPRISandANVISAhavespecificformatsthataresimilartotheCTD.
▪ Prioritization mechanismsANVISA,HC,PMDA,MFDS,COFEPRIS,HSA,MCC,U.S.FDAandWHO-PQThavemechanismstoprioritizegenericdrug product applications based on public healthinterests,consideringfactorssuchasdrugshortagesandgovernmentalpolicies.
▪ Intellectual property provisionsAllIGDRPmembershavedataprotectionand/orexclusivityperiodsbeforeageneric
drugproductcanbemarketed.Theseperiodsvaryfrom5–20years.
DiscussionWhiletheparticipatingorganizations’definitionsofa“genericdrugproduct”allappearsimilar,theirdefinitionsof“thesameactive(ordrug)substance”differ.Someorganizationsacceptdifferentsalts,estersandethersasthesameAPIaslongastheyhavethesameactivemoiety,whileothers do not. A product could therefore be considered a generic drug product in one country or region but not in another. This issuewasidentifiedasagap.Solvingitwouldenablegreaterinformation-sharingintheassessmentofgenericdrugproductapplications.
The use of a foreign-sourced reference productisallowedbysomeorganizationsbutnotbyothers.DifferencesamongIGDRPmembersinrequirementsforthereferenceproductanddocumentationsupportingthebioequivalenceofagenericdrugproductwerealsoidentifiedasagap.Inthisregard,theIGDRPconcludedthat it would be easier to start work-sharingactivitieswithdrugproductsthatareeligibleforabiowaiver,e.g.,oralandinjectablesolutions.Allorganizationsacceptbiowaivers
forgenerics,butthecriteriaforadrugproducttobeeligibleforabiowaivervaryamongthem.ThisgapisbeingdiscussedinmoredetailintheIGDRPBiowaiversWorkingGroup.Ascientificallybaseddiscussiontoworktowardsconvergenceandharmonizationisinprogress.Afurthergapwasidentifiedregarding
theminimumstabilitydata–i.e.,numbersof API and drug product batches to be tested,andtheminimumnumberofmonthsofacceleratedandlong-termstability data – that are required at the timeofsubmittingtheapplication.These
369
WHODrugInformationVol.30,No.3,2016 Regulatory collaboration
differencesmaydelaythefilingincertaincountries,thuscomplicatingthework-sharingamongorganizations.TheIGDRPmembersthatparticipated
inthesurveyarerepresentativeoftheworld’sregionsandtheirdifferentclimaticzones.Theconductofstabilitytestingaccordingtotherelevantclimaticzoneisindispensable,andthedifferentrequirementsarescientificallybasedandjustified.Forapplicationsfiledglobally,additionalorcomplementarydatamustbeprovidedbytheapplicantasappropriate.Differentproceduresareusedbythe
IGDRPmembersfortheassessmentofAPIs.SomeorganizationsauthorizeAPIsseparatelyfromthedrugproduct,othersauthorizetheminconjunctionwiththedrugproduct,andinsomecasesbothpathwaysarepossible.However,thedifferencesobservedinthesurveyweremostlyrelatedtoorganizationalworkingproceduresanddonothamperthework-sharingactivities.Therequirementtousethenationalor
regionalpharmacopoeiaofthecountryofapplication is a challenge for a globalized industry,sincetheuseofdifferentanalytical procedures and acceptance criteriaindifferentcountriesorregionswillcauseduplicationofefforts.Differencesinpharmacopoeialrequirementscomplicatecooperation and collaboration.
ConclusionThegapsobservedinthesurveywarrantreflectiononthereasonsforthedifferentrequirements.Iftheyarenotscientificallyjustified,discussionsoncommonpracticesshouldbestimulatedwithinandamongorganizations.
References1 The International Generic Drug Regulators
Pilot. WHODrugInformation2014;28(1);3-10.
2 WHO. Annex 2 to WHO Technical Report Series,No.953:Stabilitytestingofactivepharmaceuticalingredientsandfinishedpharmaceuticalproducts.Table2-updated1December2010.
3 ICHHarmonisedtripartiteguideline:StabilityTestingofNewDrugSubstanceand Products – Q1A(R2).ICH,2003.
4 ASEANguidelineonstabilitystudyofdrugproduct.Version6.0.Updaterevision:May2013.
5 ANVISA.Resolução - RE nº 1 de 29/07/2005.
6 WHO. Stabilitytestingofactivepharmaceuticalingredientsandfinishedpharmaceuticalproducts.Annex2.In:WHOExpertCommitteeonSpecificationsforPharmaceuticalPreparations.Forty-thirdreport.(WHOTechnicalReportSeries,No.953).Geneva,WorldHealthOrganization,2009.
7 ICHharmonisedtripartiteguideline:the commontechnicaldocumentfortheregistration of pharmaceuticalsforhumanuse:quality–M4Q(R1).ICH,2002. å
370
WHO Drug Information Vol. 30, No. 3, 2016
Generic medicinesInterchangeabilityofWHO-prequalifiedgenerics
Generic medicines can enable huge cost-savings as they create competition, driving down prices. In medicines regulation and in WHOprequalification,theefficacyofgenericsisdemonstratedbybioequivalencestudies.WHOmedicinesprequalificationhasfacilitatedacademicresearch,
and has itself been a subject of academic research. Adjusted indirect comparisons were conducted, using the results of separate bioequivalencestudiesforWHO-prequalifiedgenericsagainstthesamecomparator product. The comparisons found that the generics can be consideredasclinicallyequivalentamongeachother.Recommendationsare provided for regulatory assessment of generics in WHO Member Statesandforpossibleapproachestoharmonizationofbioequivalencerequirementstofacilitateaccesstoneededproducts.
Impact of generics in public healthUseofgenericmedicinessignificantlyreducesthecostofmedicinestobothgovernmentsandpatients.Genericmedicinesarethoseproducedwithoutalicencefromtheinnovatorcompanywhenthepatentorothermarketexclusivityrightsontheinnovatorproducthasexpired.Astrikingexampleoftheimpactof
genericsistheevolutionofpricesontheantiretroviral(ARV)market.Themedianpriceperpatientperyearoffirst-lineARVtherapydroppedfromaboutUS$10000tolessthanUS$100withtheintroductionofgenericFDCs,enablingthescaling-upofaccesstoantiretroviraltherapyfrom
0.5millionpeopleonARVsin2003to15.8milliongloballyin2015(1).
BioequivalenceassessmentApprovalofagenericmedicineisbasedonthedemonstrationofinterchangeabilityortherapeuticequivalencetotheinnovatorthroughbioequivalencestudies.Bioequivalenceistheabsenceofasignificantdifferenceintherateandextenttowhichtheactiveingredientoractivemoietyinpharmaceuticalequivalentsorpharmaceuticalalternativesbecomesavailableatthesiteofdrugactionwhenadministeredatthesamedose.Therequirementofbioequivalence
studies for generics in lieu of clinical efficacyandsafetystudieswasintroduced
ThisreviewarticleisbasedonaPhDthesisbyLutherGwazatitled“Adjustedindirectcomparisonsofbioequivalencestudies”,whichwasdefendedatUtrechtUniversityon8July2016.TheresearchpresentedinthePhDthesiswasconductedundertheumbrellaoftheUtrechtWHOCollaboratingCentre for Pharmaceutical Policy and Regulation (www.pharmaceuticalpolicy.nl), which is based at theDivisionofPharmacoepidemiologyandClinicalPharmacologyofUtrechtUniversityintheNetherlands.TheCollaboratingCentreaimstodevelopnewmethodsforindependentpharmaceuticalpolicyresearch,evidence-basedpolicyanalysisandconceptualinnovationintheareasofpolicy-makingandevaluationingeneral.
371
WHODrugInformationVol.30,No.3,2016 Generic medicines
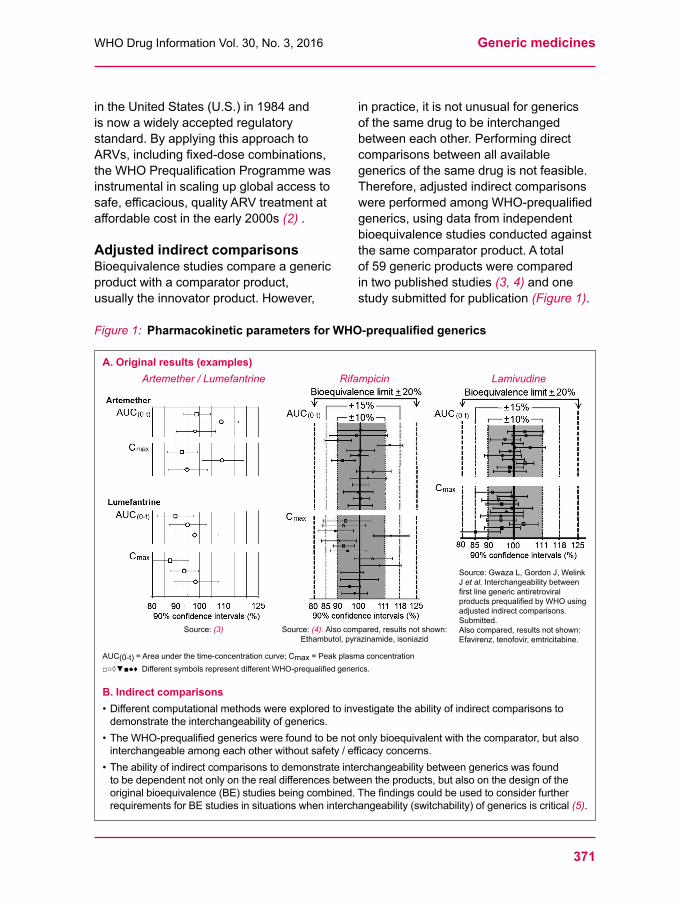
Figure 1: PharmacokineticparametersforWHO-prequalifiedgenerics
A. Original results (examples) Artemether / Lumefantrine Rifampicin Lamivudine
Source: (3) Source:(4). Alsocompared,resultsnotshown: Ethambutol,pyrazinamide,isoniazid
AUC(0-t) =Areaunderthetime-concentrationcurve;Cmax=Peakplasmaconcentration□○◊▼■●♦DifferentsymbolsrepresentdifferentWHO-prequalifiedgenerics.
B. Indirect comparisons • Differentcomputationalmethodswereexploredtoinvestigatetheabilityofindirectcomparisonstodemonstratetheinterchangeabilityofgenerics.
• TheWHO-prequalifiedgenericswerefoundtobenotonlybioequivalentwiththecomparator,butalsointerchangeableamongeachotherwithoutsafety/efficacyconcerns.
• Theabilityofindirectcomparisonstodemonstrateinterchangeabilitybetweengenericswasfoundtobedependentnotonlyontherealdifferencesbetweentheproducts,butalsoonthedesignoftheoriginalbioequivalence(BE)studiesbeingcombined.ThefindingscouldbeusedtoconsiderfurtherrequirementsforBEstudiesinsituationswheninterchangeability(switchability)ofgenericsiscritical(5).
intheUnitedStates(U.S.)in1984andis now a widely accepted regulatory standard. By applying this approach to ARVs,includingfixed-dosecombinations,theWHOPrequalificationProgrammewasinstrumentalinscalingupglobalaccesstosafe,efficacious,qualityARVtreatmentataffordablecostintheearly2000s(2) .
Adjusted indirect comparisonsBioequivalencestudiescompareagenericproductwithacomparatorproduct,usuallytheinnovatorproduct.However,
inpractice,itisnotunusualforgenericsofthesamedrugtobeinterchangedbetweeneachother.Performingdirectcomparisonsbetweenallavailablegenericsofthesamedrugisnotfeasible.Therefore,adjustedindirectcomparisonswereperformedamongWHO-prequalifiedgenerics,usingdatafromindependentbioequivalencestudiesconductedagainstthesamecomparatorproduct.Atotalof59genericproductswerecomparedin two published studies (3, 4) and one studysubmittedforpublication(Figure 1).
Source:GwazaL,GordonJ,WelinkJet al. Interchangeability between firstlinegenericantiretroviralproductsprequalifiedbyWHOusingadjustedindirectcomparisons.Submitted. Alsocompared,resultsnotshown:Efavirenz,tenofovir,emtricitabine.

Generic medicines WHODrugInformationVol.30,No.3,2016
372
TheresultsshowthatthedifferentWHO-prequalifiedgenericsincludedineachstudy can indeed be considered as clinicallyequivalent.
Regulatory assessment of generics: the example of Zimbabwe
Uptake of genericsThe use of generic products is a national responsibility. Registration of generic products and generic substitution policiesarewelladvancedinhigh-incomecountries,butarestillunderdevelopmentinlow-andmiddle-incomecountries.WHOisprovidingnormsandstandardsformedicinesqualityassuranceinMemberStates,includingresource-constrainedones.Nonetheless,inmanycountriesthedemonstrationofinterchangeabilityremainsnon-existentorisnotfullyenforced.Likewise,somepharmaceuticalmanufacturersinthesecountriesareinexperiencedinperformingbioequivalencestudiestotherequiredregulatory standard.Evenwhereregulatoryreviewis
doneaccordingtoWHO-recommendedstandards,includingthoseonofdemonstrationofinterchangeabilityfor generics (6),regulatoryresourceconstraintsmayhindertheuptakeof generic products. An analysis of theregulatorysysteminZimbabwe1 showedthatthenumberofmarketingauthorizationapplicationsreceivedexceedstheavailableregulatorycapacity,resultinginlongtimelinestoapproval.Intheperiodfrom2003–2015atotalof2083applicationswerereceived,and1002productswereapproved,while
1 GwazaL,WekweteW,DubeA,García-ArietaA,LeufkensH.AssessmentoftheperformanceoftheMedicinesControlAuthorityofZimbabwefrom2003to2005.Draftmanuscript.
the rest were either pending or refused registration.Theoverallmediantimefromapplication to registration of a product was710days(inclusiveofmanufacturers’timetorespondtoqueries),withaninterquartilerangeof422-1065days.
Collaborative approaches Collaborationandinformation-sharingbetween regulatory authorities are the mostresource-efficientstrategiestoensureaccesstomedicines,particularlyin resource-constrained settings. Harmonizationandwork-sharingapproachesarebeingimplementedinallregionsoftheworld,includingtheregionaleconomiccommunitiesinAfrica.Since2012,Zimbabweparticipates
intheWHOcollaborativeprocedureforregistrationofWHO-prequalifiedproducts,whichhasbeentakenupby27countriesincluding21Africancountriesatthetimeof writing2. This procedure entails granting ofnationalmarketingauthorizationsbasedonaverificationthattheproductistechnicallythesameasprequalifiedbyWHO. Since2013,aregionalcollaborative
medicineregistrationprocessnamedZazibona3ispractisedamongBotswana,Namibia,ZambiaandZimbabwe.Applicantssubmitdossierstoatleasttwo of the four participating authorities. Assessmentisdonejointlywithoneauthorityasrapporteur,leadingtosimultaneousregistrationinallrelevantcountries.WHOprovidesanelectronicplatformforinformationexchangeandfacilitation support.Zazibonahasenabledproductapproval
withreducedtimelines.Areviewof
2 http://apps.who.int/prequal/info_applicants/collaborative_registration_main.htm
3 www.mcaz.co.zw/index.php/downloads/category/21-zazibona

373
WHODrugInformationVol.30,No.3,2016 Generic medicines
documentsfor85applicationsconsideredfromOctober2013toDecember20154 showedthat32hadreceivedapositiveopinion,15hadreceivedanegativeopinion,10werewithdrawnbytherespectiveapplicant,25wereawaitingresponsesfromapplicantsand3wereunderreview.Thetotalreviewtime,includingthetimeforapplicantstorespondtoquestions,amountedtoamedianof10.3monthsforapositiverecommendation–withanadditional1.5monthsuntilfinalapproval–and12.4monthsforanegativeopinion.Themainreasonsfornegativeopinionswere failure to respond to requests for additionalinformationorincompletesubmissions(50%),andbioequivalence-relateddeficiencies(40%).KeysuccessfactorsintheZazibona
initiativehavebeenidentified,includingownership,effectiveleadership,partnerresourcesincludingco-financing,acost-efficientmodel,socialcapital,clearrolesandstructure,effectivecommunicationanddemonstrableresults.Ontheotherhand,amonitoringandevaluationframework,committedfundingandinstitutionalization are still required toensuresustainability.Overall,theZazibonainitiativecanbeconsideredasaneffectivecollaborativemechanismto facilitate rapid access to needed medicines,andcouldserveasamodeltobefollowedbyotherdevelopingcountries.
Selection of comparator product Collaboration critically depends on harmonizedregulatorysystems.Amajorbarrierforglobalharmonizationwithrespecttogenericmedicines–and4 GwazaL,MahlanguGN,GaesebJ,SeleloS,MwapeE,García-ArietaAetal.CollaborativeProcessinMedicinesRegistrationtoImproveAccesstoMedicinesinSouthernAfricanCountries.Draftmanuscript.
fortheadjustedindirectcomparisonsdescribedearlier–isthedifficultytouseacommoncomparatorproductglobally. Despite considerable progress inharmonizingregulatoryrequirementsforbioequivalencestudies,disparitiesremainwithrespecttotherequirementsforcomparatorproducts.WHOrecommendsthatthecomparator
productshouldbe,inorderofpriority:1)aninnovatorproductavailableonthelocalmarket,2)thenationalmarketleader,3)aWHOcomparator,4)aninnovatorproductimportedfromanICHcountry,and5)agenericproductapprovedinanICHcountry (7).WHOrecommendsagainstusingagenericproductasacomparatoraslongasaninnovatorpharmaceuticalproductisavailable,becausethiscouldleadprogressivelytolesssimilaritybetweenproducts,aphenomenoncalled“biocreep”.
Most countries follow these general principlesandrequirethecomparatorproducttobeobtainedfromtheirnationalmarketstoensurethatthegenericswillbeinterchangeablewiththecomparatoraswellasamongeachother.Somecountriesacceptacomparatorfromaforeignmarket,providedthereisinvitrodemonstrationofsimilaritywiththelocalcomparator.Forpharmaceuticalcompanieshowever,
conductingspecificbioequivalencestudiesforeachcountrymakeseconomicsenseonlyifthemarketsizeislarge.Thus,therecommendationtousealocalcomparatorisimpracticalinmanysettings,particularlyinLMICswhichoftenhaveverysmallmarketsizes.Inthecontextofregionalharmonization
itmaybefoundadvantageoustoestablisharegionalcomparatorproductforwhichquality,safetyandefficacyhasbeenestablished.ForexampleintheEuropean

Generic medicines WHODrugInformationVol.30,No.3,2016
374
UniontheinnovatorproductasmarketedindifferentEUcountriesisconsideredtobethesamebecauseitsapprovalisbasedonthesamedocumentationprovingefficacyandsafety;itwouldthereforebe acceptable in all countries. In recent years,thecooperationapproachhasbeenextendingbeyondtheEUsystemwith the International Generic Drug RegulatorsProgramme(IGDRP)pilotforgenericmedicines(seealsothearticleon page 361),withaworkinggrouponbioequivalencelookingatsomeofthespecificissuesmentionedinthispaper.Itisacknowledgedthatdifferencesmay
existbetweentheinnovatorproductinonemarketandthesameinnovatorproductinothermarkets5.Toensurethesimilarityofcomparatorproducts,NMRAscouldcomparetheirqualitativeandquantitativecomposition,specifications,manufacturingsite and process to see whether the productsaresufficientlysimilar,andcouldmakethatinformationpublic.
Acceptance of foreign or international comparatorswouldreducethenumberofinvivobioequivalencestudiesneeded,savingresourcesthatcouldbespentonmorein-depthstudiesforexampleunder
5 Forexample,carbamazepine(Tegretol®)intheU.S.isdifferentfromcarbamazepine(Tegretol®)approvedinEurope.Thisisbecausetheproducthasevolvedseparatelyinthetwojurisdictionsaftertheclinicaltrials,atatimewhendemonstrationofbioequivalencewasnotyetrequiredfortheapprovalofchanges.Carbamazepineisanantiepilepticwithnarrowtherapeuticindex,anddifferencesbetweenthereferenceproductscouldmeanthatgenericsapprovedasbioequivalenttooneortheother reference product are not necessarily interchangeable. The European reference productisthereforenotacceptableintheU.S.andviceversa.InthespecificcaseofTegretol®themanufacturerhasdevelopedaninvitro-invivocorrelation,sothatasimpledissolutiontestcanprovideinformationaboutthesimilaritybetween these products.
fastingandfedconditions,ondifferentstrengthsofaproduct,orinpatientsunderreal conditions of use.WHOprequalifiesgenericsforsupply
tomultiplecountries,especiallyLMICs,where they are often accepted by NMRAs without requiring any further studies with alocalcomparatorproduct.Therefore,theexperienceofWHOPQTprovidesinsights on how to identify and obtain an acceptablecomparatorproductinaglobalcontext.
Conclusions and recommendationsTheindirectcomparisonsdescribedearlierinthispaperhaveshownthatWHO-prequalifiedgenericsmaybeinterchangedamongeachotherwithoutanysafetyandefficacyconcerns.Thisispivotalin supporting generic prescribing and substitutionpolicies,whichareimportanttoincreasingaccesstomedicines.However,thesefindingscannot
necessarily be extrapolated to other nationallyapprovedproducts,especiallyin resource-constrained settings. Although NMRAs should ensure that generic products are interchangeable before grantingapproval,theymayhavedifferentrequirementsandreviewpractices,andmanyhavesignificantlimitationsofcapacity and resources. Harmonizedrequirementsfor
bioequivalenceandcomparatorproductsarecriticalforcollaboration.Itmustbenoted that this approach works only amongcountriesapplyingsimilarandconsistent standards in line with WHO guidelines,whichmaynotbethecaseinmostSub-SaharanAfricancountries.Nevertheless,theWHOprequalification
approachfordemonstrationofbioequivalencecouldbefollowedasa global approach. This is done in the collaborativeregistrationprocedure,where

375
WHODrugInformationVol.30,No.3,2016 Generic medicines
theoutcomesofbioequivalencestudiessubmittedtoWHOareacceptedwithoutfurthercomparisonsoftheircomparatorproductagainstthenationalone.Similarly,intheZazibonacollaborativeinitiative,theWHOprequalificationapproachforselectingcomparatorproductsisapplied,andonebioequivalencestudyissufficientfor all four countries. Toverifygenericinterchangeability,the
adjustedindirectcomparisonapproachdescribed earlier in this paper could be usedtosupportevidence-basedclinicaldecisions by healthcare professionals. Toenablesuchcomparisons,theregulatorsshouldconsidermakingdatafromapprovedbioequivalencestudiespubliclyavailable.Forsituationswhenhigh assurance of interchangeability amonggenericsiscritical,forexampleformedicineswithanarrowtherapeuticindex,regulatorsmaywishtoapplystricternationalrequirementsforbioequivalence.
References
1 WaningB,DiedrichsenE,MoonS.Alifelinetotreatment:TheroleofIndiangenericmanufacturersinsupplyingantiretroviralmedicinestodevelopingcountries.JIntAIDSSoc.2010;13(1):1–9.
2 ’tHoenEFM,HogerzeilHV,QuickJD,SilloHB.Aquietrevolutioninglobalpublichealth:TheWorldHealthOrganization’sPrequalificationofMedicinesProgramme.JPublicHealthPolicy.2014:35(2):137–61.
3 GwazaL,GordonJ,WelinkJ,PotthastH,HanssonH,StahlMetal.Statisticalapproachestoindirectlycomparebioequivalencebetweengenerics:acomparisonofmethodologiesemployingartemether/lumefantrine20/120mgtabletsasprequalifiedbyWHO.EurJClinPharmacol.2012;68:1611-8.
4 GwazaL,GordonJ,WelinkJ,PotthastH,LeufkensH,StahlM,García-ArietaA.AdjustedindirecttreatmentcomparisonofthebioavailabilityofWHO-prequalifiedfirst-linegenericantituberculosismedicines.ClinPharmacolTher.2014;96:580–8.doi:10.1038/clpt.2014.144.
5 GwazaL,GordonJ,PotthastH,etal(2015)Influenceofpointestimatesandstudypowerofbioequivalencestudiesonestablishingbioequivalencebetweengenericsbyadjustedindirectcomparisons.EurJClinPharmacol.2015;71(9):1083-9.doi:10.1007/s00228-015-1889-9.
6 WHO. Multisource(generic)pharmaceuticalproducts:guidelinesonregistrationrequirementstoestablishinterchangeability.Annex7.In:WHOTechnicalReportSeriesNo.992,Geneva:WorldHealthOrganization;2015.
7 WHO. Guidance on the selection of comparatorpharmaceuticalproductsforequivalenceassessmentofinterchangeablemultisource(generic)products. Annex 8. WHO Technical Report SeriesNo.992,Geneva:WorldHealthOrganization;2015. å
376
WHO Drug Information Vol. 30, No. 3, 2016
Adopted guidance
WHOCertificationSchemeonthequalityofpharmaceuticalproductsmovingininternationalcommerce:
Questions and Answers (Q & A)
This is a revision of a WHO guidance document as adopted by the Expert Committee forSpecificationsonPharmaceuticalPreparationsatits50th Meeting held in October 2015. The meeting report is available at www.who.int/entity/medicines/publications/pharmprep/trs_996/en/index.html. Prior to its adoption the text was posted for public comment on the WHO web site as Working Document QAS/15.623, June 2016. WHO guidancerelatedtotheCertificationSchemeisavailableatwww.who.int/medicines/areas/quality_safety/regulation_legislation/certification.
Background
TheWHOCertificationSchemeforfinishedpharmaceuticalproductsisaninternationalvoluntaryagreementtoprovideassurancetocountriesparticipatingintheScheme,aboutthequalityofpharmaceuticalproductsmovingininternationalcommerce(WorldHealthAssemblyresolutionWHA22.50(1969),WorldHealthAssemblyresolutionWHA28.65(1975),WorldHealthAssemblyresolutionWHA41.18(1988),WorldHealthAssemblyresolutionWHA45.29(1992),WorldHealthAssemblyresolutionWHA50.3(1997).TheprimarydocumentoftheSchemewastheCertificateofPharmaceuticalProduct(CPP).TheWHOExpertCommitteeonSpecificationsforPharmaceuticalPreparations,duringitsforty-thirdmeeting,recommendedthattheWHOCertificationSchemeonthequalityofpharmaceuticalproductsmovingininternationalcommerceshouldbereviewedinlightofthechangingenvironment,includingtherapidglobalizationofthepharmaceuticalmanufacturingsectorcoupledwithchangesinthemake-upofboththeregulatorsandthegroupsinvolvedinprocurement.AnychangeoftheSchemewillnecessitateadiscussionbyMemberStates.
Inaddition,asaninterimmeasure,theExpertCommitteealsorequestedthataquestionsandanswers(Q&A)documentonthefunctionoftheSchemeshouldbeprepared(seeWHOTechnicalReportSeries,No.953,pp.47–48(2009)).ThepreviousversionoftheQ&Adocument(workingdocumentQAS/10.374)waspreparedandisavailableonthewebasfollows:http://www.who.int/medicines/areas/quality_safety/regulation_legislation/certification/qas_certif_scheme_2012.pdf?ua=1.
WethanktheCPPNetworkTeamoftheInternationalFederationofPharmaceuticalManufacturers&Associations(IFPMA)forpreparingtheworkingdocumentthatformedthebasisofthereviewthroughtheExpertCommittee’sconsultativeprocess.
377
WHODrugInformationVol.30,No.3,2016 WHOCertificationScheme:Q&A
ThefollowingisacollectionofquestionsandanswersrelatingtotheWHOCertificationSchemeonthequalityofpharmaceuticalproductsmovingininternationalcommerce1 and specificallytotheCPP.
The“WHOCertificationScheme”• representsWHOactivityonthequality,andpotentiallythesafetyandefficacyofpharmaceuticalproductsmovingintointernationalcommerce
• isanadministrativeinstrumentwhichenablesWHOCertificationSchemeMemberStatestorequestcertaininformationfromanotherWHOCertificationSchemeMemberStatebymeansofdefineddocuments,i.e.aCPP.
TheCPPgivesasnapshotoftheregulatorystatusofapharmaceuticalproductandoftheCPPapplicantinthecertifyingcountry.Itisforasingleproductonly,sincemanufacturingarrangementsandapprovedinformationfordifferentdosageformsanddifferentstrengthscanvary.Foreasierreference,questionshavebeengroupedintothefollowingcategoriestosupportthereviewprocess.
[Click on red links to navigate]←“1. AbouttheWHOCertificationScheme”
“2. Related to issuing country ”
“3. Related to recipient country ”
“4. GMP status”
“5. AlternativestoaCPP”
Contents Page
1. AbouttheWHOCertificationScheme 379“1.Q1 WhatistheWHOCertificationSchemeonthequalityofpharmaceuticalproductsmovingin
internationalcommerce?”
“1.Q2 WhyisitcalledtheWHOCertificationScheme?”
“1.Q3 WhenwastheSchemedeveloped?”
“1.Q4 HowcanaWHOMemberStateorregionalorganizationbeeligibleforparticipationintheScheme?”
“1.Q5 WherecanonefindthelistoforganizationsandcountriespartytotheScheme?”
“1.Q6 DoesthelistofMemberStatesandorganizationspartytotheSchemeprovidethenamesandaddressesofthosegovernmentorganizationsauthorizedtosignandissueaCertificateforaPharmaceuticalProduct(CPP)?”
“1.Q7 HowcantheSchemefacilitatetradeinpharmaceuticalproducts?”
“1.Q8 HowdoestheSchemeoperate?”
“1.Q9 IstheSchememandatory?”
“1.Q10 IsthereanywrittendocumentthatprovidesdetailedinformationontheWHOCertificationScheme?”
“1.Q11 WhatproductsarecoveredundertheWHOCertificationScheme?”
“1.Q12 WhatarethedifferenttypesofcertificatesthatcanberequestedwithinthescopeoftheScheme?”
“1.Q13 IsthereastandardformatforCPPs?”
“1.Q14 WhatshouldrecipientcountriesdoincaseofanydoubtaboutaCPP?”
“1.Q15 ArecertifyingauthoritiespenalizediftheyissueCPPs,butdonotmeetWHOrequirementsforself-certificationandsubsequentissueofCPPs?”
“1.Q16 WhatarethemainproblemsencounteredintheapplicationoftheScheme?”
“←”
1 Lateralsoreferredtoasthe“WHOCertificationScheme”.
WHOCertificationScheme:Q&A WHODrugInformationVol.30,No.3,2016
378
2. Related to issuing country 382“2.Q1 DoesWHOissueCPP?”
“2.Q2 CananyoneissueaCPP?”
“2.Q3 WhatshouldMemberStatesandregionalorganizationspossessinordertoissueaCPPtosupporttheexportpharmaceuticalproducts?”
“2.Q4 ShouldaCPPissuedbyMemberStatesbeartheWHOemblemortheacronym“W H O ”?”
“2.Q5 BywhomisaCPPissuedandforwhatrequirementintherecipientauthority?”
“2.Q6 IstheCPPevidenceofquality,safety,efficacyreviewandapproval?”
“2.Q7 Whatisthesignificanceofthedeclarationofmarketingstatus,i.e.whethertheproductisactuallyonthemarketintheexportingcountry?”
“2.Q8 Imagineasituationinwhichaproductisauthorizedformarketinginthecountryofmanufacture,butisnotactuallyavailableonthemarket.CanthecompetentauthorityoftheexportingcountryissueaCPPtosupportexport?”
“2.Q9 Sometimesacountrymaywishtoimportaspecialdosageform,strengthorformulationofacertainknownproduct,andthisparticularproductmaynotberegisteredinthemanufacturingcountry.Undersuchcircumstances,cantheauthorityoftheexportingcountryissueaCPP?”
“←”
3. Related to recipient country 384“3.Q1 WhenwouldaCPPberequired?”
“3.Q2 Isitamustthatapharmaceuticalproducthastobeexportedfromthesamecountryasthecertifyingauthority?”
“3.Q3 IsitpossibletoobtainaCPPfromacertifyingauthoritythatisnotthecountrywherethemanufactureofthefinishedproducttakesplace?”
“3.Q4 IsitnecessaryfortheCPPtocomefromthecountrywherefinishedproductmanufacturetakesplace?”
“3.Q5 ShouldrecipientauthoritiesrequireaCPPfrommorethanonecertifyingauthority?”
“3.Q6 BusinessProcessScenarioQuestionsforwhenaproductiscontractmanufactured?”
“3.Q6.1 Iscontractmanufacturingaccepted?”
“3.Q6.2 Incaseofacontract-manufacturedproduct:fromwhichcountryshouldtheauthorityintheimportingcountry(recipientauthority)accepttheCertificateforaPharmaceuticalProduct(CPP)?”
“3.Q7 CanaCPPalsobeusedtoprovideevidenceofanadministrativereviewandapproval(e.g.ascertificationofacceptabilityofacompanynamechange)?”
“3.Q8 IsitnecessarytolegalizetheCPP?”
“←”
4. GMP status 387“4.Q1 IsitnecessaryforrecipientauthoritiestorequireGMPcertificatesinadditiontoaCPP?”
“4.Q2 DoestheCPPprovideevidenceofGMP?”
“4.Q3 WhatisthedifferencebetweenapprovalofthequalitydatainthesubmissionandevidenceofGMP?”
“4.Q4 WhenaCPPformspartofaregulatoryreview,isitnecessarytoconductasiteinspectionaswell?”
“←”
5. Alternatives to a CPP 387“5.Q1 ArethereanyalternativestoaCPPasevidenceofapprovalbyanationalmedicineregulatory
authority(NMRA)?”
“5.Q2 Whenandbywhomisastatementoflicensingstatusofpharmaceuticalproduct(s)(SLSPP)issued?”
“5.Q3 Whatisabatchcertificate?”
“←”
6. Glossary 388
379
WHODrugInformationVol.30,No.3,2016 WHOCertificationScheme:Q&A
1.AbouttheWHOCertificationScheme
1.Q1 WhatistheWHOCertificationSchemeonthequalityofpharmaceuticalproductsmoving in international commerce?
1.A1 ItisaSchemedevelopedbytheWorldHealthOrganization(WHO)inresponsetotherequestofWHOMemberStatestofacilitateinternationaltradeinpharmaceuticalproductsbetweenMemberStatesanditgivesguidancetotheissuingaswellasrequesting health authorities.
“←”
1.Q2 WhyisitcalledtheWHOCertificationScheme?1.A2 ItiscalledtheWHOCertificationSchemebecauseitwasdevelopedbyWHOin
responsetotherequestofMemberStates.“←”
1.Q3 When was the Scheme developed? 1.A3 Itwasfirstdevelopedin1975.Sincethenithasbeenrevisedin1988,in1992andin
1997. “←”
1.Q4 How can a WHO Member State or regional organization be eligible for participation in the Scheme?
1.A4 AnyWHOMemberStateorregionalorganizationintendingtoparticipateintheSchememaydosobynotifyingtheDirector-GeneralofWHOinwriting,ofitswillingnesstoparticipateintheScheme;anysignificantreservationsitintendstoobserverelatingtothisparticipation;andbyprovidingthenamesandaddressofitsnationalmedicinesregulatoryauthority(NMRA)orothercompetentauthority.
“←””
1.Q5 WherecanonefindthelistoforganizationsandcountriespartytotheScheme?1.A5 WHOpublishesthenamesandaddressesofMemberStatespartytotheScheme.The
listisavailableontheWHOwebsite:http://www.who.int/entity/medicines/areas/quality_safety/regulation_legislation/certification/contacts/en/index.html. AhardcopyofthelistisalsopublishedanddistributedtoMemberStates.Thelistisupdatedfromtimetotime.
“←””
1.Q6 Does the list of Member States and organizations party to the Scheme provide the names and addresses of those government organizations authorized to sign and issueaCertificateforaPharmaceuticalProduct(CPP)?
1.A6 Yes,thelistprovidesthenamesandfulladdressesofthosegovernmentorganizationsauthorizedtosignandissueacertificateforapharmaceuticalproduct(CPP).NMRAsreceivingaCPPcanusethislisttocheckandverifyifthecertificatetheyarereceivinghas been issued by the authorized organization.
“←””
1.Q7 How can the Scheme facilitate trade in pharmaceutical products? 1.A7 TheSchemeisanadministrativeinstrumentthatrequiresacompetentauthorityofa
participatingMemberState(thecertifyingcountry),uponapplicationbyacommercially-interestedparty(theapplicantcompany),tocertify/attesttothecompetentauthorityofanotherparticipatingMemberState(therecipientcountry)that:• aspecificpharmaceuticalproductisauthorizedformarketinginthecertifyingcountry,orifnot,thereasonwhyauthorizationhasnotbeenaccorded;
WHOCertificationScheme:Q&A WHODrugInformationVol.30,No.3,2016
380
• confirmationofmarketingstatusinissuingcountry;• themanufacturingfacilitiesandoperationsconformtogoodmanufacturingpractices(GMP)asrecommendedbyWHO.
“←””
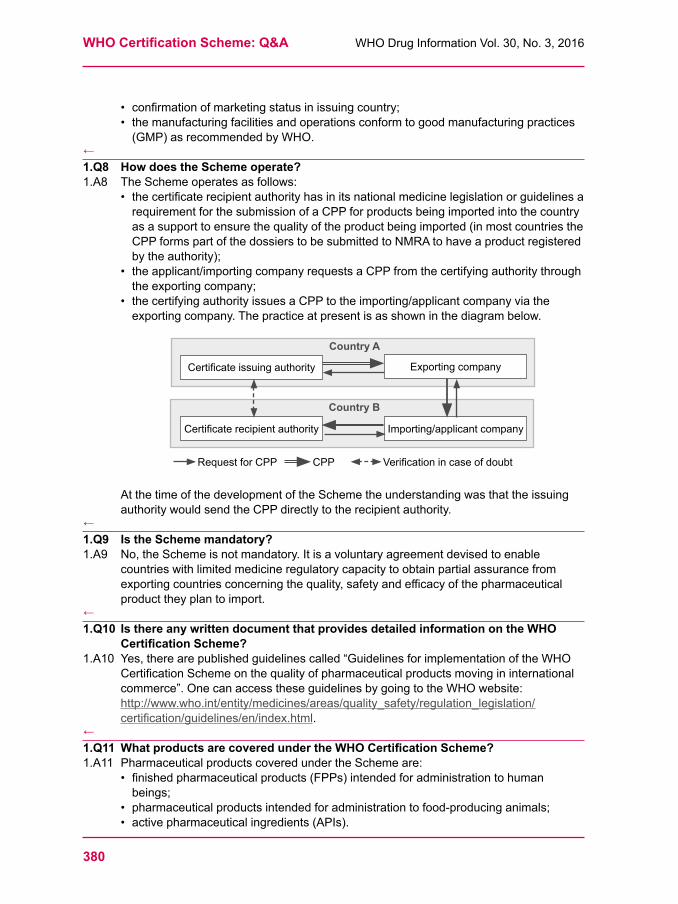
1.Q8 How does the Scheme operate?1.A8 TheSchemeoperatesasfollows:
• thecertificaterecipientauthorityhasinitsnationalmedicinelegislationorguidelinesarequirementforthesubmissionofaCPPforproductsbeingimportedintothecountryasasupporttoensurethequalityoftheproductbeingimported(inmostcountriestheCPPformspartofthedossierstobesubmittedtoNMRAtohaveaproductregisteredbytheauthority);
• theapplicant/importingcompanyrequestsaCPPfromthecertifyingauthoritythroughtheexportingcompany;
• thecertifyingauthorityissuesaCPPtotheimporting/applicantcompanyviatheexportingcompany.Thepracticeatpresentisasshowninthediagrambelow.
Certificateissuingauthority
Certificaterecipientauthority
Country A
Request for CPP CPP Verificationincaseofdoubt
Country B
Importing/applicantcompany
Exportingcompany
AtthetimeofthedevelopmentoftheSchemetheunderstandingwasthattheissuingauthority would send the CPP directly to the recipient authority.
“←””
1.Q9 Is the Scheme mandatory? 1.A9 No,theSchemeisnotmandatory.Itisavoluntaryagreementdevisedtoenable
countrieswithlimitedmedicineregulatorycapacitytoobtainpartialassurancefromexportingcountriesconcerningthequality,safetyandefficacyofthepharmaceuticalproducttheyplantoimport.
“←””
1.Q10 Is there any written document that provides detailed information on the WHO CertificationScheme?
1.A10 Yes,therearepublishedguidelinescalled“GuidelinesforimplementationoftheWHOCertificationSchemeonthequalityofpharmaceuticalproductsmovingininternationalcommerce”.OnecanaccesstheseguidelinesbygoingtotheWHOwebsite:http://www.who.int/entity/medicines/areas/quality_safety/regulation_legislation/certification/guidelines/en/index.html.
“←””
1.Q11WhatproductsarecoveredundertheWHOCertificationScheme?1.A11 PharmaceuticalproductscoveredundertheSchemeare:
• finishedpharmaceuticalproducts(FPPs)intendedforadministrationtohumanbeings;
• pharmaceuticalproductsintendedforadministrationtofood-producinganimals;• activepharmaceuticalingredients(APIs).
381
WHODrugInformationVol.30,No.3,2016 WHOCertificationScheme:Q&A
• ThereisnowaseparateschemecalledtheWHOpharmaceuticalstartingmaterialscertificationscheme(SMACS)whichhasguidelinesonimportationofAPIs (http://www.who.int/medicines/areas/quality_safety/regulation_legislation/certification/qas_certif_scheme_2012.pdf?ua=1).
“←””
1.Q12Whatarethedifferenttypesofcertificatesthatcanberequestedwithinthescopeof the Scheme?
1.A12 ThreetypesofcertificatecanberequestedforpharmaceuticalproductswithinthescopeoftheScheme:• aCPPorproductcertificate;• astatementoflicensingstatusofpharmaceuticalproduct(s);• abatchcertificateofpharmaceuticalproduct.FurtherinformationisgiveninSection“5 ”,alternativestotheCPP.
“←””
1.Q13 Is there a standard format for CPPs? 1.A13 Yes,thereisastandardformat.TheWHOstandardformatwaslastagreedbyWHO
MemberStatesin1997(reference:WHOguidelines,Section3.2).Thetemplategivesanumberingwhichisfollowedbyalmostallcertifyingcountries.TheystatethisonthetopoftheCPP.AlsotheexplanatorynotesattachedtotheCPParealmostthesameineverycertifyingcountry:• thestandardWHOformatforCPPsfacilitatesunderstandingandreviewbytherecipientauthority.Itobligescertifyingauthoritiestodiscloseimportantinformationtotheimportingcountry;
• bykeepingthenumberingoftheWHOtemplaterecipientauthoritiescaneasilyretrievetheinformationintheCPP;
• sinceCPPsareoftenissuedbilingually,thetextstylemaylookdifferentlybyhavingthenationallanguageandthetranslationorganizedincolumns,orthetranslationwritteninitaliclettersfollowseverysentenceofnationallanguage;
• theremaybedifferentmandatory/optionalattachmentsuponrequestinadditiontotheCPP,suchasquantitativecomposition,thesummaryofproductcharacteristics,thepackageinsertlabel,etc.,dependingontheperspectiveandthelegislationofeitherthecertifyingortherecipientcountry;
• recipientauthoritiesshouldrefrainfromobtainingdataotherthanintheWHOstandardformatorinadditiontothestandardCPPformat;
• certifyingauthoritiesshouldnotissuetheoutdated“freesalescertificates”.ThesehavebeenreplacedbytheWHOformatCPP.
“←””
1.Q14 What should recipient countries do in case of any doubt about a CPP?1.A14 Incaseofanydoubtthecompetentauthoritiesofrecipientcountriesshould
communicatedirectlywiththeauthorizedbodythathasissuedthecertificateorcontactWHOregionalbranchtoclarifythematter.
“←””
1.Q15 Are certifying authorities penalized if they issue CPPs, but do not meet WHO requirementsforself-certificationandsubsequentissueofCPPs?
1.A15 No,thereisnosystemtopenalizethem.WHOdoesnothavethepowertocertify,inspectorpenalizecertifyingauthorities.SincetheSchemeisvoluntary,MemberStatespartytotheSchemeself-certifytheircompliance.
“←””
WHOCertificationScheme:Q&A WHODrugInformationVol.30,No.3,2016
382
1.Q16 What are the main problems encountered in the application of the Scheme?1.A16 AnumberofproblemshavebeenencounteredintheuseoftheScheme,whichinclude:
• countriesnotpartytotheSchemeissuecertificates;• authoritiesthatdonotmeettherequirementsorformatstatedintheguidelinesfortheSchemewhentheyissueCPPs;
• someissuingauthoritiesputtheWHOemblem,logooracronymonthecertificate,therebycreatingtheimpressionthatthecertificateisauthenticatedbyWHO;
• certifyingauthoritieslimittheCPPtoproductsmanufacturedandexportedfromthecertifyingcountry;
• theCPPisnolongerrecognizedtosubstitutethefulldossierandQSE;• GMPstatusgivenintheCPPisnolongerenoughfortherecipientcountriesandadditionalGMPcertificatesarerequested;
• thereisalackofunderstandingthattheCPPreflectstheapprovalstatusofthecertifyingcountryonly;
• CPPscanbeaprerequisiteforaregulatorysubmissionratherthanbeingprovidedjustpriortoapproval;
• theleadtimesofthecertifyingauthoritiescanbeverylong,sometimesseveralmonths;
• thewaytoapplyforaCPPisnotharmonizedaseverycertifyingauthorityhasitsownsystem;
• thereisalackofelectronicrequestsystemsinthecertifyingauthoritiesandalsonopossibilityoftrackingthesubmittedrequests;
• someauthoritiesdonotallowopendiscussionsabouttheCPPrequests,e.g.priortoarejectionoftheCPPapplication,becauseofminormistakes/clarifications;
• chargingprocessesvaryacrosscertifyingauthoritieswhichcanleadtounnecessarydelaysinCPPissuance;
• thereareinconsistenciesinlistingthetrademarkoftherecipientcountryontheCPPifdifferentfromthecertifyingcountry;
• requiredlegalizationsleadtodelaysinCPPavailability(seeSection“3.Q8”).
“←””
2. Related to issuing country
2.Q1 Does WHO issue CPP?2.A1 No,WHOdoesnotissueCPPsoranyofthecertificatesdescribedundertheScheme.“←””
2.Q2 Can any one issue a CPP?2.A2 No,onlycountriesandregionalorganizations,suchastheEuropeanMedicinesAgency
(EMA),thatarepartytotheScheme,canissueCPPs.“←””
2.Q3 What should Member States and regional organizations possess in order to issue a CPP to support the export pharmaceutical products?
2.A3 MemberStatesandregionalorganizationsshouldhavethefollowingtoissueaCPP:• aneffectivenationallicensingsystemforpharmaceuticalproducts,manufacturersanddistributors;
• GMPrequirementsconsonantwiththoserecommendedbyWHOtowhichallmanufacturersofFPPsarerequiredtoconform;
383
WHODrugInformationVol.30,No.3,2016 WHOCertificationScheme:Q&A
• effectivecontrolstomonitorthequalityofpharmaceuticalproductsregisteredormanufacturedwithinthecountry,includingaccesstoanindependentqualitycontrollaboratory;
• anationalpharmaceuticalinspectoratehavingthetechnicalcompetenceexperienceandresourcestoassesswhetherGMPandothercontrolsareeffectivelyimplementedandlegalpowertoconductappropriateinvestigations;
• theadministrativecapacitytoissuetherequiredcertificates,toinstituteinquiriesinthecaseofcomplaintassociatedwithapotentiallyseriousqualitydefectsorotherhazard and to notify WHO and other concerned parties.
“←””
2.Q4 Should a CPP issued by Member States bear the WHO emblem or the acronym “WHO”?
2.A4 No,certificatesshouldnotbeartheWHOemblemortheacronym“WHO”.TheuseoftheemblemoracronymcreatestheimpressionthatthecertificateisissuedorendorsedbyWHO.ItisanillegalactandcountriesreceivingsuchCPPsshouldrejectthemandreporttoWHO.TheCPPshouldalwaysappearonthecertifyingauthority’sheadedpaperoremblem.
“←”
2.Q5 BywhomisaCPPissuedandforwhatrequirementintherecipientauthority?2.A5 ACPPisissuedbytheauthorizedbodyoftheexportingcountryandisintendedforuse
bythecompetentauthoritywithinanimportingcountry:• whenapharmaceuticalproductisunderconsiderationforaproductlicense/marketingauthorizationthatwillauthorizeitsimportationandsaleintheimportingcountry;
• whenadministrativeactionisrequiredtorenew,extendvaryorreviewsuchlicense;• itshouldbeprovidedattheendofthereviewprocessformarketsthatalsorequire
the detailed dossier. “←””
2.Q6 IstheCPPevidenceofquality,safety,efficacyreviewandapproval?2.A6 Yes,theCPPisbasedontheassumptionthattheauthoritiesissuingaCPPhavethe
capacitytoassessthequality,safetyandefficacy(QSE)oftheproducttheyapproveformarketing.BasedontheintentionoftheScheme,arecipientauthoritycouldrequireaCPPwhenitdoesnotundertakeafullreviewofQSEdatasubmittedforregistrationandevidenceofapprovalinanothercountryisrequired.
“←””
2.Q7 Whatisthesignificanceofthedeclarationofmarketingstatus,i.e.whethertheproduct is actually on the market in the exporting country?
2.A7 DeclarationofmarketingauthorizationapprovalistheaimoftheCPP.ItistruethattheWHOformatCPPincludesinformationonmarketingstatus(iftheproductisactuallyonthemarketofthecertifyingcountry)buttheSchemealsohasaprovisionwherethecertifyingauthoritycanindicatewhytheproductmaynotbemarketed.Incircumstanceswheretheproductisnotactuallyonthemarkettheissuingauthoritycanindicatethatinthecertificate.Theactualpresenceonthemarketoftheproductdependsonmanyotherfactors.Therecipientauthorityshouldnotrequirethataproductbemarketedinthecertifyingcountry.ThefocusoftheCPPistoensurethatafullreviewhasbeenundertakenbytheauthoritytoensureQSE.
“←”
WHOCertificationScheme:Q&A WHODrugInformationVol.30,No.3,2016
384
2.Q8 Imagine a situation in which a product is authorized for marketing in the country of manufacture, but is not actually available on the market. Can the competent authority of the exporting country issue a CPP to support export?
2.A8 Yes,itcanissueaCPP.Whatitshoulddoisexplainwhyitisnotonthemarket.Onereasonfornotbeingonthemarketcouldbethatthedisease/healthproblemforwhichtheproductisindicatedmaynotbeprevalentinthecountry.ForproductsapprovedaccordingtoArticle58(Regulation(EC)No.726–2004)fordiseases/healthproblemsincertainregions,theEMAonlycanissuetheCPPswithintheWHOformat.
“←””
2.Q9 Sometimes a country may wish to import a special dosage form, strength or formulation of a certain known product, and this particular product may not be registered in the manufacturing country. Under such circumstances, can the authority of the exporting country issue a CPP?
2.A9 Yes,itcanissueaCPP,butitshouldexplainonthecertificate:• thattheparticularproductisnotauthorizedformarketingintheexportingcountry;• thatithasbeenproducedbasedontherequestoftheimportingcountry:and• thatthemanufacturingisincompliancewithGMP.Theexportcertificatemaylookdifferentandhavedifferencesinformat.However,theremayberestrictionsonthisdependentonindividuallegislationintheexportingcountry.
“←””
3. Related to recipient country
3.Q1 WhenwouldaCPPberequired?3.A1 WhentheCPPreplaceseitherafullorpartialQSEreview,theCPPwouldbea
conditionofapprovalanditwouldnotberequiredatthetimeofsubmission.IflocallegislationstipulatesprovisionofaCPPatthetimeofsubmission,theauthorityreviewshouldbea“verification”procedurewithpublished,communicatedtimelinesthatshouldbeshortandthusnotdelayingpatientaccess(seeSection“1.Q16 ”).
““←””””
3.Q2 Is it a must that a pharmaceutical product has to be exported from the same country as the certifying authority?
3.A2 No,itisnotnecessaryfortheproducttobeexportedfromthecertifyingcountryaslongas a declaration of GMP assurance appears on the CPP.TheSchemewasestablishedonthebasisthatthecertifyingcountrywasalsothecountrywherefinishedproductmanufacturetookplaceandwasthereforetheexportingcountry.SubsequentrevisionstotheSchemehaveintroducedscopeforCPPstobeissuedbyotherreferenceauthorities.MostcertifyingauthoritiescurrentlyprovideCPPswhenthefinishedproductisnotmanufacturedinthecertifyingcountryonthebasisthatGMP is assured.MoreovermanyauthoritiesassumethatcertifyingauthoritiesissueCPPsevenwhenfinishedproductmanufacturedoesnotoccurinthecertifyingcountry.Strictadherencetotheaboveassumptionpotentiallylimitslicensingandregistrationoptionsandcandelaytheintroduction,oraffectthecontinuedsupply,ofimportantmedicines.
“←”””
385
WHODrugInformationVol.30,No.3,2016 WHOCertificationScheme:Q&A
3.Q3 Is it possible to obtain a CPP from a certifying authority that is not the country wherethemanufactureofthefinishedproducttakesplace?
3.A3 Yes,theSchemehasaprovisionthatwhenmanufacturetakesplaceinacountryotherthanthatwheretheproductcertificateisissued,anattestationthatsuchmanufacturecomplieswithGMPmaystillbeprovidedasanattachmenttotheproductcertificate,onthe basis of inspections undertaken for registration purposes.The GMP declaration in the CPP will refer to assurance of GMP for the product approvedinthecertifyingcountryatthestatedsite,evenifthemanufacturingsiteisinadifferentcountrythantheissuingauthority.
“←”
3.Q4 IsitnecessaryfortheCPPtocomefromthecountrywherefinishedproductmanufacture takes place?
3.A4 No,althoughtheSchemewassetupassumingthatthecertifyingcountrywasalsothecountrywherefinishedproductmanufacturetakesplace,thereisscopewithintheSchemeforCPPstobeissuedbyotherauthoritiesthatcanprovideindependentassuranceoftheGMPcompliancestatus.Thereneedstobeanappreciationofthecomplexityofmanufacturingandsourcingroutescurrentlyemployedbycompaniesoperatinginternationally.WHOMemberStatesdefinethe“source”differently:• countryoffinishedproductmanufacture;• countryoffinalpacking;• countryoffinalrelease;• countryofmainheadquartersofthepharmaceuticalcompany,etc.Thecriticalelementistheconfirmationthatallproduction/manufacturing/qualityoperations are carried out according to GMP.Duetocomplexmodern,sourcingroutes,togetherwithvaryinglocalregulatoryprocesses,theapprovalinthecountrywherefinishedproductmanufacturetakesplacemaybelaterthaninothercountries.InthiscaseitisamatterofjudgmentastowhetheritisnecessaryfortheCPPtobeissuedfromthecountrywherefinishedproductmanufacturetakesplace.Thepreference,inordertospeeduppatientaccess,wouldbetoaccepttheCPPfromtheearlierapprovingcountry–inordertoapprovetheproductthecertifyingauthoritymustalsobeassuredofGMP.ImplementationandcompliancewithGMPensuresqualityofproductirrespectiveofsource.RequirementofanadditionalCPPforthereleasesiteifitisdifferentfromtheproductmanufacturesite,delayspatientaccesssincemultipleCPPsprovidenoadditionalvalue.
“←””
3.Q5 ShouldrecipientauthoritiesrequireaCPPfrommorethanonecertifyingauthority?
3.A5 No,undermostcircumstancestheyshouldnotrequireaCPPfrommorethanonecertifyingauthority.AWHO-formatCPPfromasinglecertifyingauthorityshouldprovideappropriateevidenceofapprovalandGMPstatus.However,certainregulationsmayrequireprovisionofmorethanoneCPP.
“←””
3.Q6 Business Process Scenario Questions for when a product is contract manufactured?
3.A6 ImagineasituationinwhichacompanywithinEuropeproducesapharmaceuticalproduct,andtheproductisauthorizedformarketinginthatEuropeancountry.However,
WHOCertificationScheme:Q&A WHODrugInformationVol.30,No.3,2016
386
thecompanyalsoproducestheproductundercontractmanufacturinginasecondcountry,e.g.inAsia,andwantstoexportfromtheretoAfrica.TheauthorityoftheimportingcountryshouldreceivetheCPPfromtheEuropeancountrytoprovequalityefficacyandsafetyoftheapprovedproduct.
Supportingquestions:3.Q6.1 Is contract manufacturing accepted?3.A6.1 Yes,contractmanufacturingisacceptedunderGMP.3.Q6.2 In case of a contract-manufactured product: from which country should
the authority in the importing country (recipient authority) accept the CertificateforaPharmaceuticalProduct(CPP)?
3.A6.2 ThecountrywherethecontractmanufactureistakingplacecanissueaCPPif the product is registered by the authority of that country. If the product is not registeredwherethecontractmanufactureistakingplacethentheauthoritycannotissuetheCPP,butanexportcertificate(seeSection2,Q/A9).• Ifthecontract-manufacturedproductisalsoauthorizedformarketingintheEuropeancountry,thentheEuropeancountrycanissuecertificate.
• Ifthecontract-manufacturedproductisalsoauthorizedbyanadditionalstringenthealthauthority,thenthisauthoritycanissueaCPP.
“←””
3.Q7 Can a CPP also be used to provide evidence of an administrative review and approval(e.g.ascertificationofacceptabilityofacompanynamechange)?
3.A7 Yes,theCPPcanalsoprovideevidenceofanadministrativereviewandapproval(e.g.ascertificationofacceptabilityofacompanynamechange:• foranamechangeoftheownerofamanufacturingorproductionsite),whichoftenhappensinthecontextofcompanymergersandacquisitions;
• foradministrativeapprovalsthatnowinvolveaQSEreview,recipientauthoritiesshouldusealternativestoaCPPasapreferredandquickeroption;
• issuesrelatedtomanufacturingcompanynamechange(“administrativereview”)mayindeedcreatevariouspracticaldifficultiesforexporters–importers,butarenotassociateddirectlywithsafety/qualityconcernsandshouldbegivenlessprominence).
“←”
3.Q8 Is it necessary to legalize the CPP? 3.A8 No,legalizationisnotpartoftheWHOSchemeandthisisnotconsideredtoprovide
additionalassuranceofauthenticity.Approvalstatusesinkeyreferencecountriesarecurrentlyavailableaspublicinformation.Legalizationshouldnotbenecessarysinceanofficialgovernmentalauthorityofthecertifying country signs the CPP. LegalizationdoesnotaddvaluetotheCPP,asitconfirmsonlythesignaturesontheCPPbutdoesnotconfirmanydetailsoftheCPPcontent.LegalizationdelaysavailabilityoftheCPPandthereforedelaysaccesstomedicinesforpatients.IfarecipientauthorityhasanydoubtsaboutthevalidityofaCPPitshouldcontactthecertifyingauthoritydirectly.Inaddition,cashpaymentrequiredbycertainembassiescouldcauseunnecessarydelaystotheCPPavailability.AnumberofrecipientcountriesarenolongeraskingforlegalizationaslongastheCPPstrictlyfollowstheWHOformat.
“←”
387
WHODrugInformationVol.30,No.3,2016 WHOCertificationScheme:Q&A
4. GMP status
4.Q1 IsitnecessaryforrecipientauthoritiestorequireGMPcertificatesinadditiontoaCPP?
4.A1 No,theCPPincludesaGMPdeclaration,soadditionalGMPcertificateisnotnecessary.• FollowingtheintroductionoftheWHOCPPsomeauthoritiesnolongerissueGMPcertificates(e.g.US-FDA).
• IntheCPPcontextseparateGMPcertificatesareredundantandarethereforediscouraged.CPPsshouldbeaccepted(inparticularfromthePharmaceuticalInspectionCo-operationScheme(PIC/S)andInternationalConferenceonHarmonisation(ICH)regions)asevidenceofGMPstatus.
• OutsideoftheScheme,thereareoccasionswhenitisappropriatetorequireaGMPcertificate.
“←”
4.Q2 Does the CPP provide evidence of GMP?4.A2 Yes,theGMPdeclarationintheCPPreferstoassuranceofGMPfortheproduct
approvedinthecertifyingcountryatthestatedmanufacturingsite(s).Inaddition,CPPsissuedbyNMRAspartytothePIC/SandICHregions(EuropeanUnion,JapanandUnitedStatesofAmerica)provideevidenceofGMPstatus.WhenaCPPisprovideditisnotnecessarytoprovideadditionalGMPsforfinishedproducts.
“←”
4.Q3 Whatisthedifferencebetweenapprovalofthequalitydatainthesubmissionandevidence of GMP?
4.A3 Theapprovalofthequalityinformationinasubmissionisanapprovalofhowtheapplicantcompanyproposestomanufactureandcontrolthequalityoftheproductatthetimeofmanufactureandthroughouttheproduct’slife.TheevidenceofGMPcomplianceshows,thattheapplicantcompanyhasbeenabletodemonstratethatthemanufacturingsitefulfilstheunderlyingGMPprinciples.
“←””
4.Q4 When a CPP forms part of a regulatory review, is it necessary to conduct a site inspection as well?
4.A4 AninspectionshouldnotbenecessarywhentheGMPdeclarationontheCPPcoverstheproducttobeapprovedintherecipientcountry.• Inspectionsoutsideofthisconditionareamatterofjudgmentanddecisionbytherecipientcountry.MembershipofPIC/S,ICHorothermeansofrecognizinginspections by other authorities is encouraged.
• The acceptance of the GMP status in the CPP helps to reduce unnecessary inspections.
• CPPsshouldbeaccepted(inparticularfromPIC/SandICHregions)asevidenceofMPstatus.Thedecisiontoinspectshouldbemadeafterarisk-basedassessmentofthefacility,takingintoaccountGMPandinspectionstatusfromotherauthorities.
“←”
5. Alternatives to a CPP
5.Q1 Are there any alternatives to a CPP as evidence of approval by a national medicine regulatory authority (NMRA)?
5.A1 OutsidetheWHOCertificationSchemeotherformsofevidenceinclude:
WHOCertificationScheme:Q&A WHODrugInformationVol.30,No.3,2016
388
• productapprovalletters(orcopiesoflicenses)fromwell-establishedNMRAs,e.g.Australia,Canada,People’sRepublicofChina,Denmark,Finland,Germany,India,Japan,Norway,RepublicofKorea,Spain,UnitedKingdom,UnitedStatesofAmerica;
• positivescientificopinionfromEMA;• decisionsoftheEuropeanCommission;• Europeanpublicassessmentreport;• licensing/approvalinformationonregulatoryauthoritywebsitesandevidenceofapprovalontheUnitedStatesFoodandDrugAdministrationwebsite.
5.Q2 When and by whom is a statement of licensing status of pharmaceutical product(s) (SLSPP) issued?
5.A2 AnSLSPPisissuedbythecompetentauthorityoftheexportingcountryandisintendedforusebyimportingagentswhenconsideringbidsinaninternationaltender.Itisrequestedbytheimportingagentasaconditionforbidding.TheSLSPPisnotintendedforuseforregulatorysubmissions.
“←””
5.Q3 Whatisabatchcertificate?5.A3 Abatchcertificateisacertificatethataccompaniesandatteststothequalityandexpiry
dateofaspecificbatchorconsignmentthathasalreadybeenlicensed/approvedformarketingintheimportingcountry.• Abatchcertificateisusuallyissuedbythemanufacturer.• Incaseofbiologicalproducts,alotcertificateisissuedbythecompetentauthorityof
the exporting country.“←”
6. GlossaryTerms
Competent authorityAmedicinesregulatoryauthoritywhichhasthelegallydelegatedorinvestedauthority,capacity,orpowertoperformadesignatedfunction
Stringent authority Thesameascompetentauthority,butrelatedtoacertainreputationandgenerallyanauthorityofadevelopedmarket,suchastheFoodandDrugAdministration,EuropeanMedicinesAgency,TherapeuticGoodsAdministration,etc.
The following terms are used with the same meaning:
Certifying/issuing countryCertifying/issuing (health) authorityExporting country
Thesetermsalwaysrefertothecompetentauthority–inmostcasesofadevelopedmarketwhichissuestheCPP
RequestingcountryRecipient countryImporting country
ThesetermsalwaysrefertotheemergingmarketwhichneedstheCPPfromadevelopedmarket,asstipulatedintheregulatoryrequirements
***

WHO Drug Information Vol. 30, No. 3, 2016
389
Safety news
Safety warnings
Warfarin: calciphylaxis U n i t e d K i n g d o m – The MHRA has informedhealthcareprofessionalsabouttheconclusionsofanEU-widereviewwhich found that on rare occasions warfarinusemightleadtocalciphylaxis,includinginpatientswithnormalrenalfunction.Ifcalciphylaxisisdiagnosed,appropriatetreatmentshouldbestartedandconsiderationshouldbegiventostoppingwarfarintreatment.Calciphylaxis,alsoknownascalcific
uraemicarteriolopathy,isaveryrarebutseriousconditionthatcausesvascularcalcificationandcutaneousnecrosis.Themortalityrateishigh.Theconditionismostcommonlyobservedinpatientswith known risk factors such as end-stage renal disease.►DrugSafetyUpdateVolume9Issue12July
2016:1.PRACrecommendationsonsignals.EMA/PRAC/313187/2016.26May2016.
Eltrombopag: potentially fatal liver injury C a n a d a – Health Canada has published awarningabouttheriskofseverelivertoxicityassociatedwiththesystemichaemostaticmedicineeltrombopag(Revolade®).Thisfollowstheidentificationoffivecasesfulfillingthecriteriaforseveredrug-inducedliverinjuryinarecentreviewofallclinicaltrialandpost-marketingcases. Tomitigatetheriskofsevere
hepatotoxicityandpotentiallyfatalliver
injury,healthcareprofessionalsshould:measureserumalanineaminotransferase(ALT),aspartateaminotransferase(AST)andbilirubinbeforeinitiatingeltrombopag,everytwoweeksduringthedoseadjustmentphase,andthenmonthlyfollowingestablishmentofastabledose.Inpatientswithnormalliverfunction,eltrombopagshouldbediscontinuedifALTlevelsincreaseto≥3×upperlimitofnormal(ULN).Inpatientswithelevationsintransaminasesbeforetreatment,eltrombopagshouldbestoppedifALTlevelsincreaseto≥3×baselineor>5×ULN,whicheveristhelower.TheCanadianproductmonographhasbeenupdatedtoreflectthisnewsafetyinformation.(1)
The risk of hepatotoxicity and precautionsforusehavealsobeenincludedintheproductinformationforeltrombopagapprovedintheEU.(2)►(1) HealthCanadaAdvisory,25August
2016.(2) EMAProductinformation.Revolade-EMEA/H/C/001110-IAIN/0034/G.
Etonogestrel implants: migration from insertion siteU n i t e d K i n g d o m – The MHRA has issued a warning about rare reports ofcomplicationswithetonogestrel(Nexplanon®)contraceptiveimplants.Inrarecases,suchimplantshavemovedfromtheinsertionsiteandreachedthelungviathepulmonaryartery.Animplantthat cannot be palpated at its insertion siteinthearmshouldbelocatedassoonaspossibleandremovedatthe

Safety news WHODrugInformationVol.30,No.3,2016
390
earliestopportunity.Ifanimplantcannotbelocatedwithinthearm,chestimagingshouldbeperformed.Correctsubdermalinsertionreducestheriskoftheseevents.►MHRADrugsafetyupdate,15June2016.
Ombitasvir/paritaprevir/ritonavir: acute renal failure J a p a n – Following reported cases of acute renal failure in patients treated withthehepatitisCmedicineombitasvir/paritaprevir/ritonavir(Viekirax®)inJapan,theMinistryofHealth,LabourandWelfare(MHLW)hasrecommendedupdatestotheproductinformationtoincludethefollowingadvice:Beforestartingthisdrugandperiodicallyduringtreatment,renalfunctiontestsshouldbeperformed.Asrenalfunctionmaysuddenlydeteriorateinparticular in patients with decreased renal functionandinpatientsconcomitantlyreceivingcalciumchannelblockers,thesepatientsshouldbecarefullymonitored.Ifanyabnormalitiesareobserved,thedrugshould be discontinued and appropriate measuresshouldbeadopted.►MHLWPharmaceuticalsandMedical
DevicesSafetyInformationNo.335,June2016[English translation issued on 2 August 2016].Pages10-13.
Carmustine intracerebral implant: risk of air accumulation J a p a n –ThePMDAhasinformedhealthprofessionalsthatinpatientsreceivingacarmustine(Gliadel®)intracerebralimplant,airaccumulationmayoccurattheimplantsite,andtherehavebeenreportsofneurologicalsymptoms.Accordingly,theMinistryofHealth,LabourandWelfare(MHLW)hasrecommendedupdatestotheproductinformationforcarmustine.Aftertheimplantationpatientsshouldbe
monitoredforneurologicalsymptoms,suchashemiplegia,aphasia,anddisturbedconsciousness,andappropriatemeasuresadoptedifanyabnormalitiesareobserved.►PMDASummaryofinvestigationresults and
MHLWRevisionsofprecautions,5July2016.
Blinatumomab: pancreatitisC a n a d a –HealthCanadahasinformedhealth professionals about reported casesoflife-threatening,sometimesfatalpancreatitis associated with the use of blinatumomab(Blincyto®)inclinicaltrialandpost-marketsettings,andaboutnewrecommendedprecautions.Thediagnosisof pancreatitis should be considered in patientstreatedwithblinatumomabwhoexperiencesevereupperabdominalpainaccompaniedwithnausea,vomitingorabdominaltenderness.Ifpancreatitisissuspected,blinatumomabshouldbeeithertemporarilyinterruptedordiscontinued.Blinotumumabisamonoclonalantibody
approvedinCanadaforthetreatmentofadultpatientswithcertainformsofrelapsedorrefractoryacutelymphoblasticleukaemia.TheCanadianproductinformationhasbeenupdatedtoreflectthisnewsafetyinformation.►HealthCanadaAdvisory,13July2016.
Idelalisib: updated measures to manage risk of infectionsE u r o p e a n U n i o n – The EMA has completeditsreviewofidelalisib(Zydelig®),confirmingthatitsbenefitsoutweighitsrisksinthetreatmentoftwotypesofbloodcancers,chroniclymphocyticleukaemia(CLL)andfollicularlymphoma.Updatedrecommendationshavebeenprovidedtomanagetheriskof serious infections which was also
391
WHODrugInformationVol.30,No.3,2016 Safety news
confirmedbythereview.AllpatientstreatedwithidelalisibshouldbegivenantibioticstopreventPneumocystis jirovecii pneumoniaduringtreatmentandforupto2to6monthsthereafter.Patientsshouldbemonitoredforinfectionand white blood cell counts should be performedregularly.Idelalisibshouldnotbe started in patients with a generalized infection.Aprecautionaryrecommendationhad
initiallybeenissued,advisingagainststartingidelalisibtreatmentinpatientswithpreviouslyuntreatedCLLwhosecancercellshavecertaingeneticmutations.Theupdatedadvicenowallowsinitiationofidelalisibinthesepatients,providedthattherearenoalternativetreatmentoptionsandthattherecommendedmeasurestopreventinfectionarefollowed.►EMAPressrelease,22July2016.
Opioids and benzodiazepines: potentiallyfatalsideeffectsU n i t e d S t a t e s o f A m e r i c a – An extensiveFDAreviewhasfoundthatthegrowingcombineduseofopioidmedicineswith benzodiazepines or other central nervoussystem(CNS)depressantshasresultedinserioussideeffects,includingslowedordifficultbreathinganddeaths.Aboxedwarningandrevisionsto the Warnings and Precautions,Drug Interactions,andPatient Counseling Informationsectionshavebeenincludedintheproductinformationforopioidandbenzodiazepinemedicinesclass-wide.Opioidpainmedicinesshouldonlybe
prescribed together with benzodiazepines orotherCNSdepressantsifalternativetreatmentoptionsareinadequate.Insuchcases,thelowestpossibledosageandduration of each drug should be used to achievethedesiredclinicaleffect.Health
professionals should warn patients and caregiversabouttherisksofslowedordifficultbreathingand/orsedationandtheassociatedsignsandsymptoms.Theuseofopioidcoughmedicines
shouldbeavoidedinpatientstakingbenzodiazepinesorotherCNSdepressants,includingalcohol.►FDADrugsafetycommunication,31August
2016.FDANewsrelease,31August2016.
Levetiracetam: acute renal failure J a p a n –Revisionstotheapprovedproductinformationhavebeenrecommendedfortheanti-epilepticmedicinelevetiracetam(Keppra®)inJapantowarnabouttheriskofacuterenal failure. This follows reported cases of acute kidney failure in patients treated withlevetiracetaminJapan.Revisedproductinformationrecommendsthatpatientsshouldbecarefullymonitoredandthatifanyabnormalitiesareobserved,administrationofthisdrugshouldbediscontinued,andappropriatemeasuresshould be adopted.►MHLWPharmaceuticalsandMedical
DevicesSafetyInformationNo.334,May2016[Englishtranslationissuedon28June2016].Pages23-24.
Citalopram: suspected drug interaction with cocaine;
U n i t e d K i n g d o m – The MHRA has advisedhealthprofessionalstoenquireaboutpossiblenonmedicaldrugusebeforeprescribingmedicinesthathavethepotentialtointeractadverselywithillicit drugs. This follows the death of a manfromsubarachnoidhaemorrhagethatraised concerns about a suspected drug interaction between the antidepressant
Safety news WHODrugInformationVol.30,No.3,2016
392
citalopramandcocaine.Anexpertgroupadvisedthathypertensionrelatedtococaineandanadditiveincreasedbleedingriskincombinationwithcitalopramcouldbeplausiblemechanismsfor such an interaction.
Health professionals were also remindedofpotentialinteractionsbetweencocaineandselectiveserotoninreuptakeinhibitors(SSRIs),andoftheneedtoavoidconcurrentuseofmultipleserotonergic drugs.►DrugSafetyUpdateVolume9Issue12,July
2016:2.
Restrictions
Riociguat: not for patients with pulmonary hypertension caused by idiopathic interstitial pneumoniaE u r o p e a n U n i o n , C a n a d a – The EMA andHealthCanadahaveremindedhealthprofessionalsthattheantihypertensivemedicineriociguat(Adempas®)shouldnotbeusedinpatientswithsymptomaticpulmonaryhypertensionassociatedwithidiopathicinterstitialpneumonia.A contraindication will be added to the productinformationtohelpensurethatthemedicineisnotusedinthispatientpopulation.Therecommendationfollowstheearly
terminationofaphaseIIclinicaltrialcalledRISE-IIPwhichwasinvestigatingtheeffectsofthemedicineinthesepatients.Preliminaryresultsshowedanincreasednumberofdeathsandseriousadverseevents,withnoclinicallysignificantbenefit.►EMAPressrelease,24June2016.
MHRADrugSafetyUpdatevolume10issue1,August2016:1.HealthCanadaAdvisory,15August2016.
Fluoroquinolones:useonlyincertain serious infections;
U n i t e d S t a t e s o f A m e r i c a – The FDA hasapprovedlabellingchangestolimittheuseoffluoroquinolonesinacutebacterialsinusitis,acutebacterialexacerbationofchronicbronchitisanduncomplicatedurinary tract infections to patients that havenoothertreatmentoptions.ThisfollowsawarningcommunicatedinMay2016abouttheriskofdisablingandpotentiallypermanentserioussideeffectsthatcanoccur,includingtendoninflammationandrupture,peripheralneuropathy,psychiatricreactions,photosensitivity,andprolongationofQTcinterval..Thebenefitsoffluoroquinolonescontinue to outweigh their risks in certain serious bacterial infections such as anthrax,plagueandbacterialpneumonia.►FDANewsrelease,26July2016.
FDADrugsafetycommunication,26July2016.
Known risks
Canagliflozin,dapagliflozin:kidneyinjuryU n i t e d S t a t e s o f A m e r i c a – The FDA has strengthened its warnings about the riskofacutekidneyinjuryassociatedwiththetype2diabetesmedicinescanagliflozin(Invokana®,Invokamet®)anddapagliflozin(Farxiga®,XigduoXR®).Health professionals should consider individualriskfactorsforkidneyinjuryand should assess kidney function before startingcanagliflozinordapagliflozintherapy.Kidneyfunctionshouldbemonitoredperiodicallythereafter.Ifacutekidneyinjuryoccurs,themedicineshould
393
WHODrugInformationVol.30,No.3,2016 Safety news
bediscontinuedpromptlyandthekidneyimpairmenttreated.►FDADrugsafetycommunication,15June
2016.
Apixaban: Liver function disorder;
J a p a n –ThePharmaceuticalsandMedicalDevicesAgency(PMDA)hasinformedhealthprofessionalsthatcasesofliverfunctiondisorderhavebeenreportedinJapaninpatientstreatedwiththeanti-thromboticagentapixaban(Eliquis®).Basedonthesefindings,theMinistryofHealth,LabourandWelfare(MHLW)hasrecommendedchangestotheproductinformationstatingthathepatic function disorder associated with increasedlevelsofAST(GOT),ALT(GPT)andotherfindingsinliverfunctiontestsmayoccur,andthatpatientsshouldbecarefullymonitored.Ifanyabnormalitiesareobserved,administrationofapixabanshould be discontinued and appropriate measuresshouldbetaken.(1)Elevationoflivertransaminasesarealso
listedasadversereactionsintheproductinformationforapixabanapprovedintheEuropeanUnion.(2)►(1) PMDASummaryofinvestigationresults
and MHLWRevisionsofprecautions,5July2016.(2) EMA. Eliquis:EPAR-ProductInformation.Lastupdated15April2016.
Clarificationofindications
Fingolimod: not proven in progressive multiple sclerosis ;
J a p a n –ThePMDAhasrecommendedupdatestotheproductinformationforfingolimod(Gilenya®)toclarifytheprecautions concerning its indications. TheproductisapprovedinJapanto
preventrelapseandtodelayaccumulationofphysicaldisabilityinmultiplesclerosis.
Wording has been added to the product informationstatingthatfingolimoddidnotslow progression of physical disability in anoverseasplacebo-controlledstudyinpatientswithprimaryprogressivemultiplesclerosis,andprovidinganoverviewofthefindingsandareferencetothepublishedstudy. ►PMDAReportontheinvestigationresults.
23June2016.
Medical device-related
Blood clotting time measuring devices: inaccurate readingsC a n a d a – Alere Inc. has withdrawn theAlereINRatio®andINRatio®2ProthrombinTimeMonitoringSystems(professionalandself-test)devicesfromtheCanadianmarket.Thesedevicesmeasurebloodclottingtimeinpatientsrequiring warfarin and other oral blood-thinningmedicines.Thereisariskthatthedevicesprovide
an inaccurate low reading. This could resultinanimproperdosageofwarfarinorotherblood-thinningmedicationsbeingadministered,leadingtoexcessivebleedingwithpotentiallyseriousadverseoutcomes.►HealthCanadaAdvisory,16July2016and
22July2016.TGAAlert,21July2016.
N-acetylcysteine and biochemistry assaysU n i t e d K i n g d o m – The MHRA has advisedhealthprofessionalswhoaretreating patients with N-acetylcysteine forparacetamoloverdosetoestablishwhetherSiemensADVIAChemistryand
Safety news WHODrugInformationVol.30,No.3,2016
394
Medicines safety reviews started
Product Use Concerns Reviewing authority reference
Dapagliflozin,empagliflozin(extension of the ongoingreviewofcanagliflozin)
Treatmentoftype2diabetes
Increaseinamputationsmostlyaffectingtoesreported in the ongoing CANVAStrial.
►EMANews,8July2016.
Factor VIII-containing medicines
TreatmentofhaemophiliaA
Increased risk of developinginhibitorproteins. A recent study has suggested that this risk is higher with factor VIII medicinesmadebyDNArecombinanttechnologythanthosederivedfromblood.
Asabove
Modified-andprolonged release paracetamol
Analgesic Possibleneedtodevelopdosageform-specificstandard procedures for assessingandmanagingoverdose
Asabove
Retinoid medicines(acitretin,adapalene,alitretinoin,bexarotene,isotretinoin,tazaroteneand tretinoin)
Treatmentofskinconditions,including acne and psoriasis.Someretinoids are used to treat certain formsofcancer.
Needtoevaluatecurrentmeasuresforpregnancypreventionandforminimizingthepossiblerisk of neuropsychiatric disorders.
AsaboveSeealso:
►Health Canada Advisory,7September2016.
Dimension/DimensionVistainstrumentsare used for laboratory testing of biochemistry.Ifso,theyshoulddovenipunctureandbloodsamplingbeforeN-acetylcysteineadministration,asthereisariskoffalselowbiochemistrytestresultsifbloodissampledduringorimmediatelyafteradministration.Whenrequestingbiochemistrytests
(suchascholesterol,uricacid,lactate)thatincludeanyaffectedassaysfromtheseinstruments,healthprofessionalsshouldstatethatapatientisreceivingN-acetylcysteine.►DrugSafetyUpdatevolume9issue12,July
2016:3.MHRAMedicalsafetyalert,22June2016 (includesafulllistofaffectedassays).
395
WHODrugInformationVol.30,No.3,2016 Safety news
Non-compliance with good practices
Thissectionprovidesanoverviewofrecentwarnings and alerts issued as a result of inspectionfindings.Increasingly,suchfindingshaveledtoconcernsaboutdataintegrity.Thereasonsarediverseandincludetheincreaseduseofcomputerizedsystemsinpharmaceuticaldevelopmentandmanufacturing,improvedcapacitiesofinspectors,andalackofawarenessamongmanufacturersofthesignificanceofdataintegrityandregulatoryexpectations (1). Thishaspromptedthedevelopmentofnew
regulatoryguidanceondataintegrity,includingfinalizedEMAguidance(seepage401),draftFDA guidance (2) and draft MHRA guidance (see page 404).In2015,WHOissuedanewguidancetext–thefirstinternationaltext–ongooddataandrecordmanagementpractices(3). Itconsolidatesthenormativeprinciplesintoonecomprehensivedocumentandgivesdetailedexamplesofhowtheycanbeimplemented.Indeliveringthe2016MHRAannuallecture,theWHO Director-General thanked international expertswhocontributedtothisguidance,sayingthatitwill“helpreduceincidentsofincompletepresentationofdatabymanufacturersordeliberatedatafalsification”(4).
►(1) WHOEssentialmedicinesandhealthproductsnews,3June2016. (2)FDA.DataIntegrityandComplianceWith Current Good Manufacturing Practice Guidance for Industry. Draft Guidance. Issued 14April2016.(3) WHO. Guidance on good data and record managementpractices.Annex5.In:WHOExpertCommitteeonSpecificationsforPharmaceuticalPreparations.Fiftiethreport.WHOTechnicalReportSeries996.Geneva:WorldHealthOrganization,2016.(4) Annual lecture of the Medicines and Healthcare Products Regulatory Agency. Fromhealthcareproductstotrustandreliance:theexpanded role of regulatory authorities in an era of global health perils.London,UnitedKingdom.1March2016.
Alkem Laboratories Ltd, India: data integrity issuesE u r o p e a n U n i o n – The EMA concluded itsreviewofmedicinesforwhichstudieshavebeenconductedbyAlkemLaboratoriesLtd,andhasannouncedthatbioequivalencestudiesconductedattheAlkemsiteinTaloja,India,cannotbeusedtosupportmarketingauthorizationintheEU.Ariluzole-containingproducthasbeensuspended,andanibuprofen-containingproduct will be refused authorization untilalternativedataarepresentedfromother sources. For three other antibiotic products – two authorized products andoneunderevaluation–alternativebioequivalencedatahavebeenprovided.Therecommendationsfollowajoint
routineinspectionbyGermanandDutchauthoritiesinMarch2015,whichrevealedmisrepresentationofdataintwodifferenttrialsperformedin2013and2014attheTalojasite.Thefindingscastdoubtsonthequalitymanagementsysteminplaceatthesite,andthusonthereliabilityofthedataofbioequivalencestudiesconductedbetweenMarch2013andMarch2015.►EMAPressrelease,24June2016.
Quest Life Sciences Pvt Ltd, India: data integrity issuesU n i t e d K i n g d o m – The MHRA has suspendedthemarketingauthorizationofagenericerythromycinproductthathadbeenapprovedbasedonclinicaltrialsconductedbyIndia’sQuestLifeSciences.This follows an MHRA inspection of the QuestLifeSciencessiteinFebruary2016,whichrevealedseveraldataintegrityissues. Four other pending applications formarketingauthorizationthatrelyonstudiesconductedbyQuestLifeSciencesmayberejected.Thisaffectsproducts
Safety news WHODrugInformationVol.30,No.3,2016
396
containingdoxycycline,cephalexinandmetformin.(1)TheWHOPrequalificationTeam(PQT)
had issued a notice of concern to Quest LifeSciencesinJuly2015.(2)►(1) UKdrugsregulatorhaltsapprovalsfor
Indianclinicaltrialsfirm.Reuters,1July2016. (2) WHOPrequalificationupdate,3July2015.
Semler Research Centre Pvt Ltd, India: EMA review concludedE u r o p e a n U n i o n – The EMA has concludeditsreviewofSemlerResearchCentrePrivateLtd,Bangalore,India,andhasrecommendedsuspendinganumberofnationallyapprovedmedicinesforwhichbioequivalencestudieswereconductedatSemler.Nationalauthoritiescanpostponethesuspensionformedicinesofcriticalimportance.Furthermore,medicinesstillunderevaluationcannotbegrantedauthorizationintheEUonthebasisofstudiesconductedatSemler.(1)ThereviewfollowedanFDAinspection
thatidentifiedseveralissuesatSemler’sbioanalyticalsite,includingthesubstitutionandmanipulationofsubjects’clinicalsamples.TheFDAhadnotifiedpharmaceuticalcompaniesthatstudiesconductedatSemlerareunacceptabletosupportapprovalofmedicines(2).TheWHOPrequalificationTeamhad
also raised serious concerns regarding dataintegrityandmanipulationofstudysamplesfollowingitsowninspectionsofSemler’sbioanalyticalandclinicalsites.A WHO Notice of Concern was issued to SemlerinApril2016(3).►(1) EMAPressrelease,22July2016.
(2) FDANotificationtopharmaceuticalcompanies,20April2016.(3) WHONoticeofConcern,12April2016.
Zhejiang Medicine Co Ltd, China: unreported impurity testing resultsU n i t e d S t a t e s o f A m e r i c a – The FDA hasissuedawarninglettertoZhejiangMedicine Co. Ltd as a follow-up to observationsmadeaninspectionofitsXinchangPharmaceuticalFactoryinJune2015.Theinvestigatorshadfoundchromatogramsfromunofficialtesting,showinglargeunknownpeaksofuncharacterizedimpurities,includingpotentialcontaminants,intheactivepharmaceuticalingredients(APIs)tested.These results were not reported in the officialrecordsfortheAPIsamples.Inaddition,worksheetswerefoundtohavebeenbackdated,andactionswerenottraceabletospecificindividualsduetofailuresinthecompany’sdataintegritysystems.Thecompanywasrequestedtoconductacomprehensiveinvestigationinto the extent of the failures and a risk assessmentoftheirpotentialeffects.InAugust2016,theFDACenterforDrug
EvaluationandResearchalsoissuedwarningletterstotheAPImanufacturerUnimarkRemediesLtd,Indiaoversimilardeficiencies(2),thefinishedproductmanufacturerHuzhouAupowerSanitaryCommodityCo.,Ltd, Zhejiang,China(3),theAPImanufacturerXinxiangTuoxinBiochemicalCo.Ltd,Henan,China(4),andthefinishedproductmanufacturersPan Drugs Ltd,Vadodara,India(5),andLima&PergherIndustriaeComercioS/A,MinasGerais,Brazil(6). All FDA warning lettersareavailableontheAgency’swebsite (7).►(1) FDAWarningletter,4August2016.
(2) FDAWarningletter,12August2016.(3) FDAWarningletter,10August2016.(4) FDAWarningLetter,19August2016.(5) FDAWarningletter,25August2016.(6) FDAWarningletter,25August2016.(7) www.fda.gov/ICECI/EnforcementActions/WarningLetters/
397
WHODrugInformationVol.30,No.3,2016 Safety news
Pharmaceutics International Inc., U.S.: non-compliance with GMPE u r o p e a n U n i o n – The EMA has started areviewofmedicinesmanufacturedbyPharmaceuticsInternationalInc.,USA,followingseveralshortcomingsobservedingoodmanufacturingpractice(GMP) inspections conducted by the MHRAinJune2015andFebruary2016.Theshortcomingsincludedinsufficientmeasurestoreducetheriskofcross-contamination,aswellasdeficienciesindatamanagementandqualityassurancesystems.PharmaceuticsInternationalInc.
manufacturessodiumphenylbutyrate(Ammonaps®),whichiscentrallyauthorizedintheEU,andanumberofnationallyauthorizedmedicines.►EMAPressrelease,24June2016.
Shanghai Desano Co Ltd, China: non-compliance with GMPU n i t e d S t a t e s o f A m e r i c a – The FDA has issued a warning letter to theactivepharmaceuticalingredients(API)manufacturerShanghaiDesanoChemicalPharmaceuticalCoLtdfollowingfindingsonnon-compliancewithgoodmanufacturingpractices(GMP)duringan inspection conducted at the site in LaogangTown,PudongDistrict,inMay2015.Noimportalerthasbeenissuedbythe FDA. (1)
In response to the issuance of the FDA warningletter,theWHOPrequalification
TeamhasrequestedmanufacturersofprequalifiedproductsthatuseAPImanufacturedbyShanghaiDesanototakeadditionalmeasuressuchascomprehensivetestinguponreceipt,tohelp ensure that the quality of all API batches is assured. (2)►(1) FDAWarningletter,16June2016.
(2) WHOPQTInformationnote,5July2016.
Laxachem Organics Pvt Ltd, India: import ban for refusal of inspection;
U n i t e d S t a t e s o f A m e r i c a – The FDA hasissuedanimportalertforproductsfromLaxachemOrganicsPvt.Ltd.,Ahmednagar,Maharashtra,India,becausethecompanyhasrefusedtoallowFDAinvestigatorstoinspectitsfacility.Laxachemmanufacturesactivepharmaceuticalingredient(API)forrepackagers,labelersandwholesaledrugdistributors Accordingtothecompany’swebsite,
oneoftheAPIssuppliedbyLaxachemisdocusatesodium.AvoluntarynationwiderecalloforalliquiddocusatesodiumfromadomesticmanufacturerhadbeenorganizedintheUnitedStatesinJulyduetocontaminationwithBurkholderia cepacia,abacterialinkedtoanoutbreakinfiveU.S.states.Thiswasfollowedbyavoluntaryrecallofallliquidproductsbythatmanufacturer.►FDAUpdate,15August2016.
Safety news WHODrugInformationVol.30,No.3,2016
398
Falsifiedmedicines
FalsifiedquininesulphatecirculatinginWestandCentralAfrica
G e n e v a – WHO has issued a Medical Product Alert relating to the recent circulation oftwoconfirmedfalsifiedversionsofquininesulphatecirculatinginCameroonandtheDemocraticRepublicoftheCongo,containingzeroactivepharmaceuticalingredient.
QuininesulphateisusedforthetreatmentofP. falciparummalariaintheregion.
Theproductswerefirstdiscoveredbyalocalnon-governmentalorganization.TheyfailedfieldscreeningandweresubmittedtoaWHO-prequalifiedqualitycontrollaboratory.Subsequentanalysisshowedthatneitherproductcontainedanyofthestatedactivepharmaceuticalingredient.
Details of the products are shown below.ProductdiscoveredinCameroon:
ProductdiscoveredinBunia,Dem. Rep. of the Congo:
Productname: QuinineSulfate300mg QuinineSulphate300mgNumberoftabletspercontainer: 1000tablets 100tablets
Batchnumber: 10H05 F4387ExpiryDate: 09/2018 11/18
Dateofmanufacture: 09/2014 12/14
Statedmanufacturer:NovadinaPharmaceuticalLtd,London,UnitedKingdom
CADPharm,India
WHOrequestsincreasedvigilancewithinthesupplychainsofcountrieslikelytobeaffectedbythesefalsifiedproducts.Increasedvigilanceshouldincludehospitals,clinics,healthcentres,pharmaciesandanyothersuppliersofmedicalproducts.HealthauthoritiesareaskedtoimmediatelynotifyWHOifthesefalsifiedproductsarediscoveredintheircountry.Anyinformationontheirsupplyand/[email protected].
►WHOMedicalProductAlertNo.4/2016 (includes photographs). å

WHO Drug Information Vol. 30, No. 3, 2016
399
Regulatory news
Pre-market assessment
EMA report on adaptive pathways pilot E u r o p e a n U n i o n – The EMA has publishedafinalreportontheexperiencegainedduringitspilotprojectonadaptivepathways. The pilot was launched in March2014andhasnowended.Theadaptivepathwaysapproachmakesuseof existing regulatory tools to address unmetmedicalneeds.Amedicinewillfirstbeauthorizedinasmallpatientpopulationthatislikelytobenefitmostfromit.Additionalevidenceisthengatheredovertimeresultinginprogressivelicensingadaptations to extend or restrict the previouslyauthorizedindications.Of62applicationsreceivedduringthe
pilot,18ledtomeetingswithstakeholders,andsevenoftheseprogressedtoreceivefurtheradvicethroughtheadaptivelicensing route. The pilot has shown that adaptivepathwayscanbringmultiplestakeholders together to agree on a plan togeneratedataonamedicineacrossitslifespan,particularlyinareaswhereevidencegenerationischallenging.Aspectsforfurtherreflectionhavebeenidentified.Astakeholderworkshopontheadaptivepathwaysapproachwillbeheldon8December2016.Medicinesdevelopersareinvitedto
submitproposalsforadaptivelicensingtotheEMA.AnupdatedguidancedocumenthasbeenpublishedontheAgency’swebsite,outliningthestepstofollow.►EMAPressrelease,3August2016.
Experiences in publishing assessment reportsAjointarticlepublishedinDrug Discovery Today describesthepositiveexperiencesof the EMA and the TGA with the publicationofassessmentreportsformedicines.Accordingtotheauthors,increasingwebtraffichighlightstheregulators’successinfacilitatingaccesstoinformationonmedicinesandhowtheyareevaluated.ThearticleconcludesthatEuropeanpublicassessmentreports (EPARs) and Australian Public AssessmentReports(AusPARs)ensurehigh transparency about the reasons for marketingauthorizationofmedicines,andthatregulatoryauthoritiescanlearnfromeachotherwhenmakinginformationonmedicinespubliclyavailable.►EMANews,5August2016.
PapathanasiouP,BrassartL,BlakePetal.Transparencyindrugregulation:publicassessmentreportsinEuropeandAustralia.DrugDiscoveryToday.InPress.Correctedproofavailableonline,29June2016.doi:10.1016/j.drudis.2016.06.025.
Collaboration
EMA and FDA collaborate on patient engagementE u r o p e a n U n i o n , U n i t e d S t a t e s o f A m e r i c a – The EMA and the FDA havesetupanewworkinggrouptoexchangebestpracticesonhowtoinvolvepatientsindevelopment,evaluationandpost-authorizationactivitiesrelatedtomedicines.
Patients bring real-life experience as wellasspecificknowledgeandexpertise
Regulatory news WHODrugInformationVol.30,No.3,2016
400
toregulatorydiscussionsonmedicines.Theirinvolvementisapriorityforbothagencies. The new cluster is expected tomeetthreetofourtimesperyearviateleconference. Areas for discussion will include the processes for selecting and preparing patients to take part in the agencies’activities,ensuringthatpatientsareindependentandrepresentative,andreportingontheimpactofpatientinvolvement.►EMANews,22June2016.
Post-market surveillance
New EMA guidance on monitoring of biological medicinesE u r o p e a n U n i o n – The EMA has publishedanumberoffinalizedguidancetextsonitsEUGoodPharmacovigilancePractices(EU-GVP)website,includinganew chapter titled Product- or population-specific considerations II: Biological medicinal products.Thechapterprovidesguidanceonhowtobettermonitorandmanagethesafetyofbiologicalmedicinestooptimizethesafeandeffectiveuseofthese products in Europe.Biologicalmedicinescontainoneor
moreactivesubstancesmadebyorderivedfromabiologicalsource,suchasbloodorplasma.Theactivesubstancesofbiologicalmedicinesarelargerandmorecomplexthanthoseofnon-biologicalmedicines.Thenewguidancetakesintoaccountthecomplexityofbiologicalmedicinesandtheirinherentvariabilityinmoleculesofthesameactivesubstance,particularlyindifferentbatchesofamedicine.Ithighlightsspecificissuesandchallengesforthepharmacovigilanceofbiologicalmedicines,e.g. in relation tovariabilityoftheactivesubstanceortraceabilityofproducts,provides
recommendationsonhowtoaddressthesespecificitiesandchallenges,andoutlines the roles and responsibilities of thevariousactors.Thenewchaptercomesintoforceon
16August2016.Itappliestobiologicalmedicines,biosimilarsandmedicineswhichcontainthesameoracloselyrelatedactivesubstancebutarenotauthorizedasbiosimilars.Itdoesnotapplytovaccinesoradvancedtherapymedicinalproducts,asseparateguidancealready exists for these.TheEU-GVPisakeydeliverableof
the2010pharmacovigilancelegislation.It applies to centrally authorized and nationallyauthorizedmedicines.Anupdatedmoduleonpost-authorizationsafetystudieshasalsobeenreleased,givingclearerguidanceforthesestudies and distinguishing between legalobligationsandrecommendations.Inaddition,EU-GVPdrafttextsonmanagementandreportingofadversereactions,signalmanagementandsignaldetectionhavebeenpublishedforcomment.►EMANews,15August2016.
EMA.Goodpharmacovigilancepractices[web site].Updated15August2016.
Report on pharmacovigilance activities in EuropeE u r o p e a n U n i o n –The European CommissionhaspublishedareportonthepharmacovigilanceactivitiesoftheEuropeanmedicinesregulatorynetworkinthe three years following the introduction ofthenewpharmacovigilancelegislationinJuly2012.ThecreationofthePharmacovigilance
RiskAssessmentCommittee(PRAC)andtheregulatorytoolsmadeavailableundertherevisedlegislationhaveenabled
401
WHODrugInformationVol.30,No.3,2016 Regulatory news
fasterdetectionofsafetyissues.Someoftheconcreteachievementsduringthe past three years include the use of riskmanagementplansasanintegralpartofproactivesafetymanagement,improvedreportingofside-effectswithanincreaseby50%indirectreportsfrompatients,investigationofsafetysignalsbythePRACandpromptregulatoryactionswhereneeded,submissionofperiodicsafetyupdatereports(PSURs)bypharmaceuticalcompaniesforassessmentofthebenefit-riskbalanceofmarketedmedicinesbyregulators,andsafety-related referrals leading to PRAC recommendationsforaharmonizedpositionacrosstheEU.►EMANews,8August2016.
Good manufacturing practice
EMA adopts data integrity guidelinesE u r o p e a n U n i o n – The EMA has releasednewgoodmanufacturingpractice(GMP) guidance to ensure the integrity of datageneratedintheprocessoftesting,manufacturing,packaging,distributionandmonitoringofmedicines.Regulatorsrelyonthesedatatoevaluatethequality,safetyandefficacyofmedicinesandtomonitortheirbenefit-riskprofilethroughouttheir life span.
Data integrity is key to public health protection. Controlling of data records helps ensure that the data generated are accurate and consistent to support good decision-makingbybothpharmaceuticalmanufacturersandregulatoryauthorities.Theadvice,whichappliestobothpaper-basedandelectronicsystems,isalignedwith existing GMP guidance published by someregulatoryauthoritiesparticipatinginthePharmaceuticalInspection
Co-operationScheme(PIC/S).Itshouldbereadinconjunctionwithnationalguidance,medicineslegislationandtheGMP standards published in Eudralex volume4.►EMANews,11August2016.
Labelling
Improved product labels in CanadaC a n a d a – Health Canada has released newguidanceforindustryonimprovedlabelsandpackagesthatwillminimizetheriskofconfusion.Two“GoodLabelandPackagePractices”guideshavebeenprovided,oneforover-the-countermedicinesandanotherforprescriptiondrugs. The guidance includes instructions for a new standardized Facts Table that will be required on the outer labels of over-the-counterdrugs,witheasy-to-readproductinformationsuchasingredients,directionsandwarnings.TherequirementwillbephasedinfromJune2017.►GovernmentofCanadaNewsrelease,
30June2016.
Antibiotics
EMA recommends reducing veterinary use of colistinE u r o p e a n U n i o n – The EMA has recommendedthatcountriesshouldreduce the use of the last-resort antibiotic colistininanimalstodecreasetheriskofantimicrobialresistance.Thegoalistocutcolistinsalesby65%.Colistin-containingmedicinesshouldonlybeusedasasecondlinetreatmentinanimals.Inaddition,colistinshouldbereclassifiedintothecategoryofantimicrobialslistedbyWHOascriticallyimportanttohumanhealth.
Regulatory news WHODrugInformationVol.30,No.3,2016
402
TheadviceupdatesEMAguidancefrom2013andtakesintoaccountcommentsmadebystakeholdersduringapublicconsultationthatendedon26June2016.TheEuropeanCommissionrequestedthisupdateinresponsetothediscoveryofanewmechanismofcolistinresistancecausedbythemcr-1gene,whichcanbetransferredbetweendifferenttypesofbacteria.ThegenewasfirstidentifiedinEnterobacteriaceaeinSouthChina,andhasalsobeenfoundintheEUandotherregions.►EMAPressrelease,27July2016.
Global implications of antibiotics control in IndiaI n d i a – Following the recent ban of around330fixed-dosecombinations(FDCs)bytheGovernmentofIndia,including63productscontainingantibiotics,theauthorsofanarticleinThe Lancet Global Healthhaveurgedtheinternationalcommunitytosupportthefullimplementationoftheban,emphasizingthat controlling antibiotic resistance in India is key for controlling antibiotic resistance worldwide. Growingworldwidetradeandtravel
hasallowedresistantmicroorganismstospreadrapidly.NewDelhimetallo-β-lactamase,anenzymethatcausesbacteriatoberesistanttoantibiotics,wasfirstreportedinIndiain2008andisnowfoundworldwide.SomeofthebannedFDCshavereportedlybeenexportedtoAfrican and Asian countries.►AhmadA,KhanMU,BalkrishnanR.Fixed-
dosecombinationantibioticsinIndia:globalperspectives.TheLancetGlobalHealth.Volume4,No.8,e521,August2016.DOI:http://dx.doi.org/10.1016/S2214-109X(16)30093-6.
Tripartite meeting on evaluation of new antibacterial agentsL o n d o n –AtameetingheldbetweentheregulatoryauthoritiesofEurope,JapanandtheUnitedStateson1-2September2016,thethreeagenciesdiscussedregulatoryapproachesthatcouldstimulatethedevelopmentofnewantibioticstofightantimicrobialresistanceandprotectglobal public health. They agreed that alignmentofdatarequirementsfortheevaluationofnewantibacterialagentscansupportthisaim,butthatsomeflexibilityisneededwheretreatmentoptionsarelimitedduetoantimicrobialresistance,andthatabbreviatedclinicaldevelopmentprogrammesfornewantibioticsmaybeappropriatetoaddressunmetneedsrelatedtoantimicrobialresistance.Theyalsoidentifiedareasofclosercollaborationandcoordinationofeffortstoencouragethedevelopmentofsafeandeffectiveantibacterialtreatments.Thenexttripartitemeetingisscheduled
totakeplaceinspring2017.►EMANews,7September2016.
PMDANews,7September2016.
Controlled substances
Tighter control of W-18 in CanadaC a n a d a –TheGovernmentofCanadahaspublishedfinalamendmentstoaddthesynthetic,potentiallyharmfulsubstanceW-18toScheduleIoftheControlledDrugsandSubstancesAct(CDSA)andtotheRestrictedDrugssectionoftheFoodandDrugRegulations,makingunauthorizedactivitiessuchasproduction,possession,importationorexportationandtraffickingillegal.ThereisevidencethatW-18hasbeenusedrecreationally in Europe and Canada. W-18hasbeenfoundinsamplesfalsely
403
WHODrugInformationVol.30,No.3,2016 Regulatory news
labelledaslegitimatemedicinessuchasoxycodone that were seized by Canadian lawenforcementauthoritiesin2015.(1)HealthCanadahasclarifiedthatthe
tightenedcontrolswereadoptedinviewofdata published in the patent application for W-18showingitsveryhighactivityagainstpainonmice,suggestingapotentiallysevereriskforharm.IntheabsenceofdataontheuseofW-18inhumansthereisnospecificknowledgeonitsmechanismsofaction,itspharmacology,orwhethernaloxonewouldbeeffectivetoreverseitseffects.(2)►(1) GovernmentofCanadaNewsrelease,1
June2016. (2) HealthCanadaadvisory,13June2016.
Canada proposes scheduling of fentanyl precursorsC a n a d a – Health Canada has proposed tomoveforwardwithplanstorestrictsixchemicalsusedintheproductionoffentanyl,tomaketheirunauthorizedimportationandexportationillegal.Thisfollowsanincreaseindomesticproductionof illicit fentanyl reported by the Canadian police.
The proposed regulatory change is part ofHealthCanada’sopioidactionplan,which was announced by the Health MinisterinJune2016.►GovernmentofCanadaNewsrelease,
31August2016.
Blood safety
Shorter deferral period for MSM in CanadaC a n a d a – Health Canada has authorized two Canadian blood operators to reduce the deferral period for blood donation for menwhohavesexwithmen(MSM)fromfiveyearstooneyear.ThetwooperatorshadsubmittedscientificdatawhichwerereviewedbyHealthCanadaandfoundtosupport the conclusion that the change would not reduce the safety to recipients of donated blood.
This change brings Canada into line withseveralothercountrieswhichhaveimplementedaone-yeardeferralperiodformenwhohavesexwithmen,includingtheUnitedStates,Australia,NewZealand,England,ScotlandandFrance.►GovernmentofCanadaNewsrelease,
20June2016.
All U.S. blood donations to be screened for Zika virusU n i t e d S t a t e s o f A m e r i c a – As a further safetymeasureagainsttheemergingZikavirusoutbreak,theFDAhasissuedarevisedguidancerecommendinguniversaltesting of donated whole blood and blood componentsforZikavirusintheU.S.anditsterritories.Inearlierguidance,screeninghadbeenrecommendedonlyinareaswithactiveZikavirustransmission.The expanded testing will reduce the risk ofZikavirustransmission.►FDANewsrelease,26August2016.
Regulatory news WHODrugInformationVol.30,No.3,2016
404
Under discussion
U n i t e d K i n g d o m – The MHRA has published draft data integrity guidance for industry.Theguidancecoversdatagovernancesystemsacrossgoodpracticesrelatedtothelaboratory,clinical,manufacturing,distributionandpharmacovigilanceareas.Itaddressesfundamentalfailuresidentifiedinregulatoryinspections.Thedeadlineforcommentsis31October2016.►MHRAAnnouncement,21July2016.
E u r o p e a n U n i o n – The EMA has published adraftguidelineontheuseofinnovativemodellingandsimulationinmedicinesdevelopment.Thedraftguidelinegivesdetailedadviceonthedatathatshouldbeincludedinamodellingreportofanapplicationdossier,andthesupportivedataneededtoassessamodellingplatform.Commentsareinviteduntil31January2017.►EMANews,29July2016.
E u r o p e a n U n i o n – The EMA has launched apublicconsultationonrevisedguidanceregarding the developmentofmedicinesto treat tuberculosis. The guidance is anaddendumtoEMA’sguidelineontheevaluationofmedicinestotreatbacterialinfections.CommentscanbesenttotheAgencyuntil31January2017.►EMANews,1August2016.
E u r o p e a n U n i o n –Updatedguidancetexts on themanagementandreportingofadversereactions,signalmanagementand signal detection havebeenpublishedforcommentontheEMAgood pharmacovigilancepractices(GVP) website. Thedeadlineforcommentis18October2016.►EMA.Goodpharmacovigilancepractices
[web site].Updated15August2016.
U n i t e d S t a t e s o f A m e r i c a – The FDA has published two draft guidance texts on next generationsequencing(NGS)diagnostics,anewtechnologytoscanhumanDNAtodetectgenomicvariationsthatmaypointtoindividualhealthrisksorhelptoinformtreatmentdecisions.Publiccommentsareinvitedduringa90-daycommentperiod.►FDANewsrelease,6July2016.
U n i t e d S t a t e s o f A m e r i c a – The FDA has established a public docket and requested commentsregardingoptionsforblood donor deferral policies to reduce the risk of HIV transmission.Specifically,commentsareinvitedonthefeasibilityofmovingfromtheexistingtime-baseddeferralstoalternateoptionssuchastheuseofindivid ualriskassessment.Thecommentperiodis120days.FDA.Bulletin,26July2016.
405
WHODrugInformationVol.30,No.3,2016 Regulatory news
Approved
Lixisenatide: for type 2 diabetesProduct name:Adlyxin®Dosage form:Once-dailyinjectionClass:Glucagon-likepeptide-1(GLP-1)receptoragonist;ATC code:A10BX10
Approval:FDAUse:Treatmentofadultswithtype2diabetes.Benefits:ImprovementofhaemoglobinA1clevels.
Safety information:• Severehypersensitivityreactions,includinganaphylaxis,werereportedinclinicaltrials.
• TheFDAhasrequiredpost-marketstudiesonimmunogenicityandonsafetyandefficacyinchildren.
• Lixisenatide should not be used to treat people with type 1 diabetes or patients with diabetic ketoacidosis.
►FDANewsrelease,28July2016.
Cholera vaccineProduct name:Vaxchora®Dosage form:OralliquidClass:Live,attenuatedcholeravaccine;
ATC code:J07AE02Approval:FDA(fast-trackdesignation,priorityreview)
Use:Preventionofcholeraintravellers.Benefits:Additionalcholera-preventionmeasurefortravellers.
►FDANewsrelease,10June2016.
Lifitegrast: for dry eye diseaseProduct name:Xiidra®Dosage form:OphthalmicsolutionClass:Lymphocytefunction-associated
antigen 1 (LFA-1) antagonistApproval:FDAUse:Treatmentofdryeyedisease.Benefits:Improvementinsignsandsymptomsofeyedryness.
Safety information:Thesafetyandefficacyoflifitegrastinpatientsbelowtheageof17years has not been studied.
►FDANewsrelease,12July2016.
Cell-based therapy to support stem cell transplant in blood cancer patientsProduct name:Zalmoxis®Dosage form:DispersionforinfusionClass:GeneticallymodifiedallogeneicTcellsApproval:EMA(conditionalapproval;orphan
designation)Use:Add-ontreatmentinhaploidenticalhaematopoieticstemcelltransplantationof adult patients with high-risk haematologicalmalignancies.
Benefits:Abilitytoincreaseoverallsurvivalrates.
Safety information:Thisproductcancausegraft-versus-hostdisease.AsuicidegeneinthemodifiedTcellsmakesthemsusceptibletoganciclovirorvalganciclovir.Oneofthesemedicinescanthereforebegiventopreventfurtherdevelopmentofthe disease.
►EMAPressrelease,24June2016.
Biosimilar
Etanercept-szzsProduct name:Erelzi®Dosage form:InjectionBiosimilar to:Enbrel®(etanercept)Approval:FDA(approvedasabiosimilar,not
as an interchangeable product)Use:Treatmentofmultipleinflammatory
diseases.Safety information:Etanercept-szzsshouldnotbegiventopatientswithsepsis.
►FDANewsrelease,30August2016.
Regulatory news WHODrugInformationVol.30,No.3,2016
406
Approved
Extensions of indications
Emtricitabine&tenofovirdisoproxil: for HIV pre-exposure prophylaxisProduct name:Truvada®Approval:EMArecommendationNewly approved use:Incombinationwithsafersexpractices,toreducetheriskofsexually-acquiredhumanimmunodeficiencyvirustype1(HIV-1)infection in adults at high risk.
Note:ThisindicationwasapprovedtoenableintensificationofpreventivemeasuresagainstHIV,giventhehighnumberofnewinfections worldwide.
►EMAPressrelease,22July2016.
Cabozantib, lenvatinib: approved in the EU for kidney cancer ;
Product name:Cabometyx®(cabozantib),Kisplyx®(lenvatinib)
Approval:EMArecommendation(acceleratedassessment)
Newly approved use:Treatmentofadvancedrenalcellcancer(inthecaseoflenvatinib:incombinationwitheverolimus)
Note:ThetwomedicineswerepreviouslyapprovedforthyroidcancerbothintheEUandintheU.S.underthenamesofCometriq®(cabozantib)andLenvima®(lenvatinib).IntheU.S.,theirindicationswereextendedinAprilandMay2016respectivelytoincludeadvancedrenalcancer.
►EMAPressrelease,22July2016.
Interim import approval
Naloxone nasal spray: to prevent deaths from opioid overdose ;
C a n a d a – The Canadian Minister of Health hassignedanInterimOrdertotemporarilyallownaloxoneinnasalsprayformtobeimportedfromtheU.S.andsoldinCanada.Untilnow,onlytheinjectableformatofnaloxonewasavailableinCanada.
Naloxone nasal spray is under expedited reviewforauthorizationinCanada.Theimportorderwasgrantedtoenableimmediateaccesstoeasy-to-useformatsofnaloxonebypoliceandfamilymembers,tohelppreventdeathsfromopioidoverdoses.An English and French instruction sheet will beprovidedtogetherwiththeproduct.►GovernmentofCanadaNewsrelease,
6July2016.
Diagnostics
Assay to detect markers for antibiotic resistanceProduct name:XpertCarba-R®AssayApproval:FDAUse:Detectionofspecificgeneticmarkersassociatedwithcarbapenemase,theenzymeproducedbyCarbapenem-resistant Enterobacteriaceae,inpatientspecimens.Thetestisintendedtobeusedinconjunctionwithotherclinicalandlaboratoryfindings.
Benefits:Testingofspecimensfrompatientsenables faster detection of resistance markersthantestingofsamplesderivedfrombacterialcultures.
Note:TheXpertCarba-R®Assaytestsonlyforgeneticmaterial.Itdoesnotdetectbacteria,carbapenemaseactivityorotherpossiblenon-enzymaticcausesofcarbapenemresistance.Neitherdoesitdetectalltypesofcarbapenemasegenes.Itisimportanttorecoverbacteriafor accurate tracking of the spread of carbapenemresistance.LaboratoriesshouldcontinuetoperformstandardbacterialcultureinconjunctionwiththeuseoftheXpertCarba-R®Assay.Inaddition,concomitantculturesarenecessarytorecoverorganismsforepidemiologicaltyping,antimicrobialsusceptibilitytestingandconfirmatorybacterialidentification.
►FDANewsrelease,29June2016. å

407
WHO Drug Information Vol. 30, No. 3, 2016
Publications and events
Access to medicines
UNHRC resolution on access to medicinesG e n e v a –TheUNHumanRightsCouncil(UNHRC)hasadoptedbyconsensusaresolutiononaccesstomedicinesthatreaffirmstherightofeveryonetotheenjoymentofthehighestattainablestandardofphysicalandmentalhealth.TheresolutionurgesallStates,
theWHOandrelevantorganizationstopromoteinnovativeresearchanddevelopmenttoaddresshealthneedsindevelopingcountries,includingaccesstoquality,safe,efficaciousandaffordablemedicines,takingintoaccounttheWHOGlobalStrategyandPlanofActiononPublicHealth,InnovationandIntellectual Property. It further calls on memberstatestomakefulluseoftheflexibilitiesprovidedbytheagreementon Trade-Related Aspects of Intellectual PropertyRights(TRIPS)andtocontinuecollaborating,“asappropriate,onmodelsandapproachesthatsupportthedelinkage of the cost of new research and developmentfromthepricesofmedicines,vaccinesanddiagnosticsfordiseasesthatpredominantlyaffectdevelopingcountries”.ApaneldiscussionwillbeheldinMarch2017onbestpracticesandchallengesinaccesstomedicines.►IntellectualPropertyWatchnews,1July
2016. UNHumanRightsCouncil.A/HRC/32/L.23/Rev.1.Accesstomedicinesinthecontextoftherightofeveryonetotheenjoymentofthe highest attainable standard of physical andmentalhealth.Draftresolution.30June2016.
WHO to convene stakeholders on fair medicines pricingG e n e v a –InanonlinecommentarytheWHO Assistant Director-General for HealthSystemsandInnovation,DrMarie-PauleKieny,hasannouncedthatWHOisplanningtoconvenegovernments,patient groups and industry stakeholders todevelopafairpricingmodelthatcanaffordablydeliverthemedicinesneededby patients. Assomenewmedicinesare
unaffordableevenforwealthycountries,andsomeoldermedicinesareingreatshortage,newapproachesareneededtoreachuniversalhealthcoverage,whichisatthecentreofglobalhealtheffortsundertheSustainableDevelopmentGoals.DrKienyproposedthat,forthisobjectivetobereachedby2030,thepublicandprivatespheresshouldenterintoasocialcontract,enablinginnovationandgenericproductiontorespondeffectivelytoglobalpublichealthneedsbyproviding,quality,safe,effectivetreatmentswhicharebothavailableandaffordable.►WHOMediaCentre.CommentarybyMarie-
PauleKieny,AssistantDirector-General,HealthSystemsandInnovation.5July2016.
New book on intellectual property rules and access to medicinesA m s t e r d a m – A book and web site launched by Health Action International (HAI)describetheimpactofthepatentsystemonaccesstomedicinesandencouragegovernmentstouseavailablelegalflexibilitiestosafeguardaccessto
Publications and events WHODrugInformationVol.30,No.3,2016
408
neededtreatment.Thewebsiteprovidesinformationabouttherelationshipbetween intellectual property and access tomedicinesaswellasmorein-depthanalysesintokeyissues,alongwithresources and infographics.►HAIPressrelease,13July2016.
Medicines Patent Pool signs new licencesG e n e v a – The Medicines Patent Pool (MPP) has announced new genericmanufacturinglicencesforfourantiretrovirals–lopinavir/ritonavir,atazanavirandraltegravir–aswellasthedirect-actingantiviraldaclatasvirtotreathepatitis C. The MPP has signed licences withAurobindo,Desano,Emcure,HeteroLabs,LaurusLabs,LupinandnewpartnerZydus Cadila for a total of nine new agreementstoproducegenericversionsofkeyWHO-prioritytreatmentsforHIVand hepatitis C. ►MPPPressrelease,16July2016.
Hepatitis C patent landscapeG e n e v a – WHO has published updated patentinformationforsevennewhepatitisCmedicineswhichareincludedintheWHOListofEssentialMedicines:sofosbuvir,ledipasvir,daclatasvir,simeprevir,paritaprevir,ombitasviranddasabuvir.Thereportscovermorethan40countries,territoriesandregionsandprovideclarityonwhetherornotthemedicinesarepatent-protectedinindividualcountries.Thisknowledgeisimportantforgovernmentsinmakingtreatmentavailabletotheirpopulations.►WHOPublichealth,innovation,intellectual
property and trade. WHO updates patent informationontreatmentsforHepatitisC[web page].
Insulin patent landscapeA new publication in the Journal of Pharmaceutical Policy and Practice providesanoverviewofthepatentlandscape for insulin. The authors concludethattheglobalmarketdominanceofexpensiveanalogoverhumaninsulins,offeredbyafewmanufacturers,willlikelycontinueeventhoughmanypatentsforinsulinanalogswill expire soon. A way forward would be tofindgenericmanufacturersthatwillofferacceptableoff-patenthumaninsulinproducts for export. (1)
The paper is one in a series produced undertheACCISSProject,amulti-yearefforttounderstandwhatiscausingthebarriers to insulin access and to address theinequitiesintheglobalmarket.(2)►(1)KaplanWA,BeallRF.Theglobal
intellectualpropertyecosystemforinsulinanditspublichealthimplications:anobservationalstudy.JournalofPharmaceuticalPolicyandPractice.2016;10:3. DOI:10.1186/s40545-016-0072-8. (2)HealthActionInternational.ACCISSstudy[website].http://haiweb.org/what-we-do/acciss/
Pharmacovigilance
Two new CIOMS publicationsG e n e v a – The Council for International OrganizationsofMedicalSciences(CIOMS)hasreleasedtwonewpublications for health professionals involvedinsafetysurveillanceofmedicines.
The publication Evidence Synthesis and Meta-Analysis for Drug Safety, Report of CIOMS Working Group X is for readers who are interested in analysis of drugsafetydataormeta-analysismoregenerally.Itprovidestherationalefor
409
WHODrugInformationVol.30,No.3,2016 Publications and events
whyandwhenameta-analysisshouldbeconsidered in the context of regulatory decision-making,anddescribesthetasks,datacollection,andanalysesthatneedtobecarriedouttoinformthosedecisions.Whilemostguidanceandreviewsinthisareagivemoreattentiontoassessmentofpre-definedbenefits,thisreportfocusesoncombiningevidenceonharmsthatemergeinthepost-marketsetting.
The book titled Development and Rational Use of Standardised MedDRA Queries (SMQs): Retrieving Adverse Drug Reactions with MedDRA – Second Edition is useful for those wishing to searchdatabasesonIndividualCaseSafetyReports(ICSRs)codedaccordingtotheMedDRA®system.Itprovidesexamplesofstandardizedqueriesthatarerelevantindifferentcontextssuchassystematicanalyses,interventionalclinicaltrials,signaldetectionorsafetysignalassessment.CIOMSisaninternational,non-
governmental,non-profitorganizationestablishedjointlybyWHOandUNESCOin1949.ItspublicationsareavailabledirectlyfromCIOMS(www.cioms.ch) or fromtheWHObookshop(http://apps.who.int/bookorders/). ►CIOMSNews,30August2016.
Disease updates
Polio virus: public health emergency of international concernG e n e v a –AttheadviceoftheEmergencyCommitteeundertheInternationalHealthRegulations(2005)(IHR),theWHO Director-General has declared the continuation of the public health emergencyofinternationalconcernwithregardtothespreadofbothwildpoliovirusandcirculatingvaccine-derivedpoliovirus.
Temporaryrecommendationswillremaininplaceforcountriesthatareinfectedby,vulnerableto,and/orexportingthetwotypesofvirus.TheCommitteewasgravelyconcerned
aboutinformationindicatingthatwildpoliovirushadbeencirculatingundetectedinNigeriaforseveralyearsandwouldlikelyspreadtoCameroon,ChadandNiger,aswellasthedeterioratingsecurityinpartsofAfghanistanwhichmaydelayeffortsforpolioeradication.►WHOStatement,22August2016.
Zika: public health emergency continuesG e n e v a –BasedontheadviceprovidedbytheEmergencyCommitteeundertheInternationalHealthRegulations(2005)atitsthirdandfourthmeetings(1, 2),the WHO Director-General has declared the continuation of the Public Health EmergencyofInternationalConcernposedbyZikavirusinfectionandhasreaffirmedtheexistingrecommendationsforpublichealthmeasures.AtthetimeofthefourthCommitteemeeting,therewerenoreportsofconfirmedcasesofZikavirusamongpeoplewhoattendedtheGames.TheCommitteereaffirmeditspreviousadvicethatthereshouldbenogeneralrestrictionsontravelandtradewithareaswithZikavirustransmission,includingthe cities in Brazil that will be hosting the ParalympicGames.AcknowledgingthattheimpactofZikavirusisalongtermconcern,theCommitteerecommendedfocusonseveralnewresearchissues.ItfurtherrecommendedthattheDirector-Generalshouldconsiderdevelopinganappropriate infrastructure and response plan within WHO.WHO,thePanAmericanHealth
Organization(PAHO)andpartnershave
Publications and events WHODrugInformationVol.30,No.3,2016
410
set out their strategic response to Zika. A greaterfocuswillbeplacedonpreventingandmanagingmedicalcomplications,informationandcounsellingservices,andintegratedvectorcontrolmeasures.ImplementationofthestrategicresponseplanfromJuly2016toDecember2017willcostUS$122million.(3)►(1) WHOStatement,14June2016.
(2) WHOStatement,3September2016.(3) WHONoteforthemedia,17June2016.
Sexually transmitted infections: new WHO treatment guidelines G e n e v a – WHO has issued new guidelinesforthetreatmentofchlamydia,gonorrhoea and syphilis in response to the growing threat of antibiotic resistance. Someantibioticsarefailinginthe
treatmentoftheseSTIsasaresultofmisuseandoveruse.Withouteffectivetreatment,complicationscanresultthatcancauseseriousillnessandsometimesdeath.Thenewrecommendationsarebasedonthelatestavailableevidence.Forgonorrhoea,thenewWHOguidelinesrecommendagainsttheuseofquinolonesduetowidespreadhighlevelsofresistance.Forsyphilis,thenewWHOguidelinestronglyrecommendsasingledoseofbenzathinepenicillingivenbyinjection,insteadoforalantibiotics.WHOis working with partners to help address prevailingshortagesofbenzathinepenicillin.
WHO is calling on countries to update theirnationaltreatmentguidelinesandtostartusingtheupdatedrecommendationsimmediately.WHONewsrelease,30August2016.
Non-communicable diseases: uneven progressG e n e v a – A new WHO report highlights the need to intensify national action to meettheglobaltargetstoprotectpeoplefromheartdisease,cancers,diabetes,andlungdiseases.Globally,thesefournoncommunicablediseases(NCDs)remaintheleadingcausesofmortality.Thesustainabledevelopmentgoalsincludeagoaltoreduce,byonethird,theprematuremortalityfromNCDsinpeopleagedunder70years.Thefindingsofaglobal2015survey
showthatanumberofcountrieshaveadoptedmeasurestopreventtobaccouse,harmfuluseofalcohol,unhealthydiet,andphysicalinactivity.However,progressisinsufficientanduneven.►WHONoteforthemedia,18July2016.
WHO. Assessing national capacity for the preventionandcontrolofnoncommunicablediseases.Geneva:WHO,2016.
Hepatitis B and C: need for more access to testing and treatmentG e n e v a – WHO has urged countries to increase access to hepatitis testing andtreatmentandtostepuppreventivestrategies.Thisfollowstheadoption,atthe2016WorldHealthAssembly,ofthefirsteverGlobalHealthSectorStrategyandglobaltargetstofightviralhepatitis.TheSecondWorldHepatitisSummitwilltakeplaceinBrazilinMarch2017.Globally,400millionpeopleareinfected
withhepatitisBandC,morethan10timesthenumberofpeoplelivingwithHIV.Onlyonein20peoplewithviralhepatitisisdiagnosedwiththedisease,andonlyonein100isbeingtreated.Direct-actingantiviralscancuremore
than90%ofpatientswithin2-3months.While their high costs continue to put
411
WHODrugInformationVol.30,No.3,2016 Publications and events
treatmentoutofmostpeople’sreach,prices are declining especially in countries thathaveaccesstogenerics.Forexample,inEgyptthecostofahepatitisCtreatmentcoursedroppedfromUS$900in2014tolessthanUS$200in2016.►WHONewsrelease,20July2016.
HIV
Key challengesD u r b a n –AttheInternationalAIDSConferenceinDurban,SouthAfrica,WHOhasflaggedfourkeychallengestotheglobalHIVresponse.Firstly,thenumberofnewinfectionshasremainedhigh,andrenewedattentionmustbepaidtoprevention,forexamplebyexploitingnewinterventionssuchaspre-exposureprophylaxis(PrEP).Secondly,whileWHOhasrecommendedthatallpeoplediagnosedwithHIVstartantiretroviraltherapy(ART)assoonaspossible,thereisaneedformorereadyaccesstosimpleandaffordabletestingservicesandfortailoredtreatmentprogrammestoreachallthoseinneed.Thirdly,vigilanceandquickactionarerequiredtominimizetheemergenceofdrugresistance,andlastly,thereisaneedforsustainablefinancingofthe global response. (1)
HIV and injectable contraceptivesG e n e v a –WHOwillconveneanexpertreviewgrouplaterin2016toexaminethelinksbetweentheuseofvarioushormonalcontraceptivemethodsandwomen’sriskofHIVacquisition.Theexpertreviewgroup will assess whether current WHO guidance needs to change in light of thefindingsofaWHO-commissionedsystematicreview,publishedinAIDS on 9 August2016(2).
While the data continue to indicate no association with risk of HIV acquisitionfororalcontraceptivepills,injectablenorethisteroneenanthateandlevonorgestrelimplants,theystrengthenexisting concerns about a possible increase in risk of HIV acquisition inwomenusinginjectabledepotmedroxyprogesteroneacetate.(3)►(1) WHONoteforthemedia,15July2016.
(2) PolisCB,CurtisKM,HannafordPCetal.UpdateonhormonalcontraceptivemethodsandriskofHIVacquisitioninwomen:asystematicreviewofepidemiologicalevidence,2016.[Pre-publicationabstract].AIDS.PostAcceptance:August5,2016.doi:10.1097/QAD.0000000000001228.(3) WHOSexualandreproductivehealth.News.9August2016.
Vaccines
Yellow fever emergency vaccination campaigns G e n e v a –TheEmergencyCommitteeunder the International Health Regulations (2005)determinedthatthecurrentstatusoftheyellowfeveroutbreaksinAngolaandtheDemocraticRepublicofthe Congo (DRC) does not constitute a PublicHealthEmergencyofInternationalConcern(PHEIC)atthistime,butrequiressustainedscaledupresponseactivitiesandclosemonitoring.(1)
In the last two weeks of August 2016,morethan7.7millionpeopleinKinshasaandafurther1.5millionpeopleinDRC’sborderregionswithAngolawerevaccinatedinanemergencycampaignaccomplishedthroughanextraordinary network of partnerships andcollaborations.Thecampaignbuiltonpreviousemergencycampaignsledbynationalgovernments,whichhadreachedmorethan13millionpeopleinAngola
Publications and events WHODrugInformationVol.30,No.3,2016
412
andmorethan3millioninDRCsincethebeginningoftheoutbreakinDecember2015(2). Toachievemaximumpopulation
coveragetherecentcampaignusedthe‘fractionaldosing’approachrecommendedbytheWHOStrategicAdvisoryGroupofExperts(SAGE)onImmunization,wherebyonefifthoftheregulardoseofyellowfevervaccinecanconferimmunityforatleast12months(3). Full doses were giventopregnantwomenandinfants,whomayhaveaweakerimmuneresponse.AUSAID-fundedstudywillevaluatetheimmuneresponseachievedduringthecampaign.
The International Health Regulations still requireafulldosefortravellers.A2014amendmententeredintoforceinJuly2016underwhichallcountriesrecognizethat a single full dose confers life-long immunity.WHOhasprequalifiedyellowfever
vaccinesfromfourdifferentvaccinemanufacturerswhichtogetherproduceanannualvolumeofaround80-90milliondoses.Aglobalstockpileof6milliondosesisfundedbyGavi,theVaccineAlliance,The stockpile was depleted twice between FebruaryandJune2016duetotheneedto control outbreaks. (3)►(1) WHOStatement,31August2016.
(2) WHONewsrelease,2September2016.(3) WHOStatement,17June2016.
Globalvaccinequalitycontrollaboratories networking meetingL a g e Vu u r s c h e , N e t h e r l a n d s – At ameetinghostedjointlybyWHOandthe Dutch National Institute for Public HealthandtheEnvironment(RIVM)from30Augustto2September2016,participantsfrom22countriesagreedto establish a global network of control
laboratoriesperforminglotreleaseofWHO-prequalifiedvaccines.
Lot release by regulatory authorities isanimportantelementintheregulationofvaccines.Itservestoconfirmthateachbatchofavaccinemeetsthespecificationsoftheproductaslaiddownintheapprovedmarketingauthorization.WHO-prequalifiedvaccinesareused
toimmunize65%ofinfantsworldwide.Theproposednetwork–thefirstatthegloballevel–isintendedasaplatformfor participating laboratories to share informationinordertostrengthenmechanismsforrelianceandwork-sharingandpromoteharmonizationoftesting.Thisisexpectedtoresultinmoreeffectiveandstreamlinedprocessesbothforregulatorsandformanufacturers,thus increasing global access to WHO-prequalifiedvaccinesataffordablecosts.►WHOImmunizationstandards.WHO-RIVM
Global Vaccine Quality Control Laboratories NetworkingMeeting[web page].
WHO matters
New WHO guideline welcomedT h e H a g u e , N e t h e r l a n d s – New guidelineshavebeenreleasedjointlybyWHOandtheInternationalPharmaceuticalFederation(FIP)onprovidingmedicinesforchildrenwhennoauthorized product exists. Healthprofessionalsallovertheworld
havelongstruggledwiththelackofauthorizedandcommerciallyavailablechild-specificmedicines.Theyareoftenforcedtouseadultmedicineswhentreatingchildrenforexamplebycrushingtablets,ortomakeproductsfromscratch.These approaches pose a certain risk ofinaccuratedosingandcanimpactonthequality,safetyandefficacyofthe
413
WHODrugInformationVol.30,No.3,2016 Publications and events
medicine.Thenewguidanceprovidesadvicebasedonavailableevidence,bestpracticesandsoundscientificandtherapeuticprinciples,andprovidespracticalexamples.►FIPNews,13June2016.
FIP-WHOtechnicalguidelines:Pointstoconsiderintheprovisionbyhealthcareprofessionalsofchildren-specificpreparationsthatarenotavailableasauthorized products.
WHOPrequalificationTeamoffersGMP pre-inspections G e n e v a –Toassistmanufacturersinresource-limitedcountrieswhoarekeentoattainproductprequalification,theWHOPrequalificationTeam(PQT)isinitiatingapilotcollaborationenablingmanufacturerstorequestverificationoftheircompliancewiththeprinciplesofgoodmanufacturingpractice(GMP)evenbeforetheyhavesubmittedanapplicationforWHOprequalification.
The concept of this approach has been tested successfully in cooperation with theNigeria’sNationalAgencyforFoodandDrugAdministration(NAFDAC)andthePharmaceuticalManufacturersAssociation of Nigeria (PMG-MAN). ►PQUpdate,17June2016.
MQAS Finished pharmaceutical productquestionnairepostedG e n e v a – WHO has posted a Word versionoftheInteragencyFinishedProduct Questionnaire (1)onitswebsite,foreaseofusebymanufacturersandother parties.
The Interagency FPP questionnaire is an appendix to the WHO Model QualityAssuranceSystem(MQAS)forprocurementagencies(2). It is thecommonformattobeusedbymanufacturerstosubmitproductdatatointernationalorganizations.SuchdataarereviewedforthoseneededmedicinesofwhichnoWHO-prequalifiedorstringentlyauthorizedproductsareavailable.TheWHOMQASwasupdatedin2014
in collaboration with the Interagency pharmaceuticalworkinggroup,whichbringstogetherthemajororganizationsinvolvedininternationalprocurementofmedicines.►(1) WHOMQASAppendix6-Interagency
finishedpharmaceuticalproductquestionnairebasedonthemodelqualityassurancesystemforprocurementagencies.Availableat:
WHO.Essentialmedicinesandhealthproducts. Guidelines. – Distribution
(2) WHO.Modelqualityassurancesystemforprocurementagencies.Annex3.In:WHOTechnicalReportSeries,No.986.Geneva,Switzerland:2014.
See also: Medicines quality assurance. Aharmonizedself-assessmenttoolforprocurementagencies. WHO Drug Information.2014;28(4):434-447. å
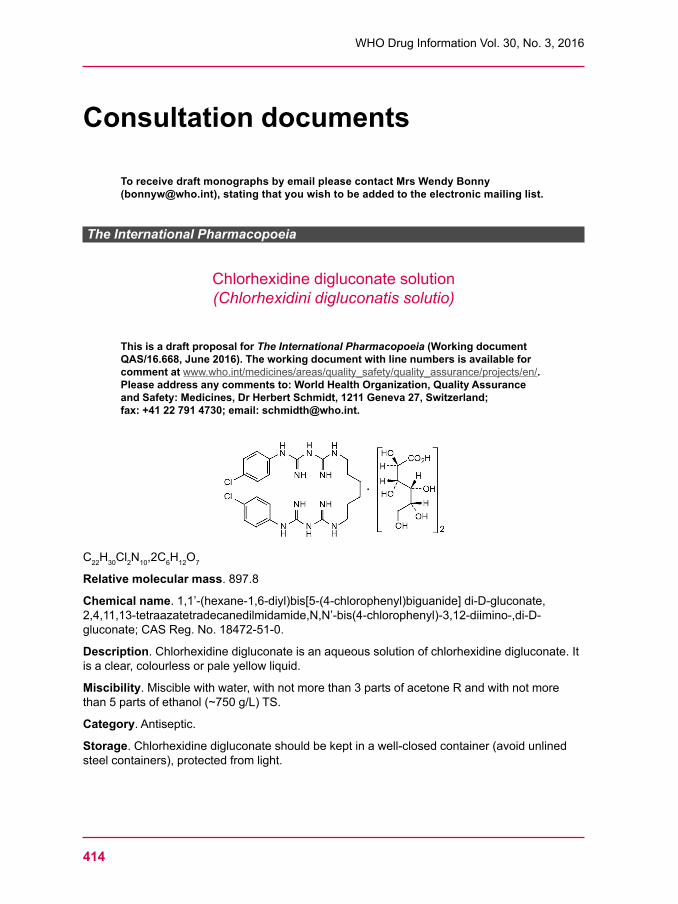
414
WHO Drug Information Vol. 30, No. 3, 2016
Consultation documents
To receive draft monographs by email please contact Mrs Wendy Bonny ([email protected]), stating that you wish to be added to the electronic mailing list.
The International Pharmacopoeia
Chlorhexidine digluconate solution(Chlorhexidini digluconatis solutio)
This is a draft proposal for The International Pharmacopoeia (Working document QAS/16.668, June 2016). The working document with line numbers is available for comment at www.who.int/medicines/areas/quality_safety/quality_assurance/projects/en/. Please address any comments to: World Health Organization, Quality Assurance and Safety: Medicines, Dr Herbert Schmidt, 1211 Geneva 27, Switzerland; fax: +41 22 791 4730; email: [email protected].
C22H30Cl2N10,2C6H12O7
Relative molecular mass.897.8
Chemical name.1,1’-(hexane-1,6-diyl)bis[5-(4-chlorophenyl)biguanide]di-D-gluconate,2,4,11,13-tetraazatetradecanedilmidamide,N,N’-bis(4-chlorophenyl)-3,12-diimino-,di-D-gluconate;CASReg.No.18472-51-0.
Description. Chlorhexidine digluconate is an aqueous solution of chlorhexidine digluconate. It isaclear,colourlessorpaleyellowliquid.
Miscibility.Misciblewithwater,withnotmorethan3partsofacetoneRandwithnotmorethan5partsofethanol(~750g/L)TS.
Category. Antiseptic.
Storage.Chlorhexidinedigluconateshouldbekeptinawell-closedcontainer(avoidunlinedsteelcontainers),protectedfromlight.
415
WHODrugInformationVol.30,No.3,2016 Consultation documents
RequirementsChlorhexidinedigluconatesolutioncontainsnotlessthan190gperLandnotmorethan210gper L of C22H30Cl2N10,2C6H12O7.
Identity tests• EithertestsAandB,ortestsB,CandDmaybeapplied.
A.To1mLofthesolutionadd40mLofwaterR,coolinicedwater,makealkalinetotitanyellowpaperRbyaddingdropwise,andwithstirring,sodiumhydroxide(~420g/L)TSandadd1mLinexcess.Filter,washtheprecipitatewithwaterRuntilthewashingsarefreefromalkali.RecrystallizefrommethanolR.Drythecrystalsat100–105ºC.Carryouttheexaminationasdescribedunder1.7Spectrophotometryintheinfraredregion. The infraredabsorptionspectrumisconcordantwiththespectrumobtainedfromchlorhexidineRSorwiththereference spectrum of chlorhexidine. If the spectra thus obtained are not concordant,repeatthetestusingtheresiduesobtainedbyseparatelydissolvingthetestsubstanceandchlorhexidineRSinasmallamountofmethanolRandevaporatingtodryness.TheinfraredabsorptionspectrumisconcordantwiththespectrumobtainedfromchlorhexidineRS.
B. Carry out the test as described under 1.14.1Thin-layerchromatography usingsilicaR5asthecoatingsubstanceandamixtureof10volumesofammonia(~260g/L)TS,10volumesofethylacetateR,30volumesofwaterRand50volumesofethanol(~750g/L)TSasthemobilephase.Applyseparatelytotheplate5μLofeachofthefollowing2solutionsinwaterR.Forsolution(A)dilute10mLofthepreparationtobeexaminedtoafinalvolumeof50mL.Forsolution(B)use25mgofcalciumgluconateRpermL.Afterremovingtheplatefromthechromatographicchamberdrytheplateat100ºCfor20minutesandallowtocool.Spraytheplatewithasolutioncontaining25g/LammoniummolybdateRand10g/LcericsulfateRinsulfuricacid(~98g/L)TS.Heattheplateforabout10minutesat110°C.Examinethechromatogramindaylight.Theprincipalspotobtainedwithsolution(A)correspondsinposition,appearanceandintensity to that obtained with solution (B).
C.Dissolve1mLofthesolutionin10mLofwaterandadd,withshaking,0.15mLofcopper(II)chloride/ammoniaTS;apurpleprecipitateisproducedimmediately.Continuetoadd0.5mLofcopper(II)chloride/ammoniaTS;thecolouroftheprecipitatechangestoblue.
D. Carry out the test as described under 1.14.4High-performanceliquidchromatographyusingtheconditionsgivenunder“Relatedsubstances”.Theretentiontimeoftheprincipalpeakinthechromatogramobtainedwithsolution(1)issimilartothatoftheprincipalpeakinthechromatogramobtainedwithsolution(3).
pH value (1.13).Dilute1mLto20mLincarbon-dioxide-freewaterR,5.5–7.0.
Relative density (1.3). =1.06–1.07.
Impurity P (p-Chloroaniline)
Preparesamplesolution(A)bydiluting0.20gofthetestsolutionto30mLwithwaterR.Addrapidlyandwiththoroughmixingaftereachaddition:5mLofhydrochloricacid(~103g/L)TS,0.35mLofsodiumnitrite(100g/L)TS,2mLofammoniumsulfamate(50g/L)TS,5mLofN-(1-naphthyl)ethylenediaminehydrochloride(1g/L)TSand1mLofethanol(~750g/L)TS.Transferthissolutionquantitativelytoa50.0mLvolumetricflask,dilutetovolumewithwaterRandallowtostandfor30minutes.
Consultation documents WHODrugInformationVol.30,No.3,2016
416
Preparereferencesolutions(B)–(F)representingrespectively0.005%(m/v),0.01%(m/v),0.02%(m/v)and0.06%(m/v)ofchloroanilineinthetestsampleasfollows:Dilute1.0mL,2.0mL,4.0mL,10.0mLand12.0mLofasolutioncontaining10μgpermLofchloroanilineRinhydrochloricacid(200g/L)TSto20mLwithwaterR.Thenadd10.0mLofwaterR.Addrapidlyandwiththoroughmixingaftereachaddition:5mLofhydrochloricacid(~103g/L)TS,0.35mLofsodiumnitrite(100g/L)TS,2mLofammoniumsulfamate(50g/L)TS,5mLof N-(1-naphthyl)ethylenediaminehydrochloride(1g/L)TSand1mLofethanol(~750g/L)TS.Transfereachsolutionquantitativelytoa50.0mLvolumetricflask,dilutetovolumewithwaterRandallowtostandfor30minutes.
Measure the absorbance (1.6)ofsolutions(A)–(F)ina1cmlayeratthemaximumatabout556nm.Plotacalibrationcurveforsolutions(B)–(F).Determinetheconcentrationofchloroanilinefromthecalibrationcurve.
Thecontentofp-chloroanilineisnotmorethan0.05%(m/v),calculatedwithreferencetochlorhexidine gluconate solution.
Related substancesPreparefreshsolutionsandperformthetestswithoutdelay.
Carry out the test as described under 1.14.4High-performanceliquidchromatographyusing astainlesssteelcolumn(25cm×4.6mm)packedwithparticlesofsilicagel,thesurfaceofwhichhasbeenmodifiedwithchemically-bondedoctadecylsilylgroups(5µm).Maintainthecolumnat30°C.
Usethefollowingconditionsforgradientsolution:
MobilephaseA: Mix20volumesofa0.1%(v/v)solutionoftrifluoroaceticacidRinacetonitrileRand80volumesofa0.1%(v/v)solutionoftrifluroaceticacidRinwaterR;
MobilephaseB: Mix10volumesofa0.1%(v/v)solutionoftrifluoroaceticacidRinwaterRand90volumesofa0.1%(v/v)solutionoftrifluoroaceticacidRinacetonitrile R.
Usethefollowinggradientelution:
Time (min)
Mobile phase A (%v/v)
Mobile phase B (%v/v)
Comments
0–2 100 0 Isocratic2–32 100to80 0to20 Linear gradient32–37 80 20 Isocratic37–47 80to70 20to30 Linear gradient47–54 70 30 Isocratic54–56 70to100 30to0 Returntoinitialcomposition56–66 100 0 Re-equilibration
PreparethefollowingsolutionsinmobilephaseA:Forsolution(1)transfer1.0mLofthepreparationtobeexaminedtoa100mLvolumetricflaskanddilutetovolume.Forsolution(2)transfer1.0mLofsolution(1)toa100mLvolumetricflaskanddilutetovolume.For
417
WHODrugInformationVol.30,No.3,2016 Consultation documents
solution(3)dissolvethecontentsofavialofchlorhexidineforsystemsuitabilityRS(containingimpuritiesA,B,F,G,H,I,J,K,L,NandO)in1.0mL.
Operatewithaflowrateof1.0mLperminute.Asadetectoruseanultravioletspectrophotometersetatawavelengthof254nm.
Injectalternately10µLeachofsolutions(1),(2)and(3).
UsethechromatogramsuppliedwithchlorhexidineforsystemsuitabilityRSandthechromatogramobtainedwithsolution(3)toidentifythepeaksduetoimpuritiesA,B,F,G,H,I,J,K,L,NandO.
RelativeretentionWithreferencetochlorhexidine(retentiontime=about35min): impurityL=about0.23;impurityQ=about0.24;impurityG=about0.25; impurityN=about0.35;impurityB=about0.36;impurityF=about0.5; impurityA=about0.6;impurityH=about0.85;impurityO=about0.90; impurityI=about0.91;impurityJ=about0.96;andimpurityK=about1.4.
Thetestisnotvalidunlessinthechromatogramobtainedwithsolution(3):• theresolutionbetweenthepeaksduetoimpuritiesLandGisatleast3.0;• thepeak-to-valleyratio(Hp/Hv)isatleast2.0,whereHp=heightabovethebaselineofthepeakduetoimpurityBandHv=theheightabovethebaselineofthelowestpointofthecurveseparatingthispeakfromthatduetoimpurityN.
Inthechromatogramobtainedwithsolution(1):• theareaofanypeakcorrespondingtoimpurityNisnotgreaterthantheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(2)(1.0%);
• theareaofanypeakcorrespondingtoimpurityHisnotgreaterthan0.5timestheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(2)(0.5%);
• theareasofanypeakcorrespondingtoeitherimpuritiesA,JorKisnotgreaterthan0.4timestheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(2)(0.4%);
• thesumoftheareasofanypeakscorrespondingtoimpuritiesIandOisnotgreaterthan0.4timestheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(2)(0.4%);
• theareaofanypeakcorrespondingtoimpurityGisnotgreaterthan0.3timestheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(2)(0.3%);
• theareasofanypeakcorrespondingtoeitherimpuritiesB,F,LorQisnotgreaterthan0.2timestheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(2)(0.2%);
• theareasofanypeakcorrespondingtoeitherimpuritiesA,JorKisnotgreaterthan0.4timestheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(2)(0.4%);
• theareaofanyotherimpuritypeakisnotgreaterthan0.1timestheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(2)(0.10%);
• thesumoftheareasofallimpuritypeaksisnotgreaterthan3timestheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(2)(3.0%).Disregardanypeakwithanarealessthan0.05timestheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(2)(0.05%).
Assay. DeterminetheweightpermL(1.3.1)ofthepreparationtobeexamined.Transferabout1g,accuratelyweighed,toa250mLbeakerandadd50mLofanhydrousaceticacidR.Titratewith0.1Mperchloricacid(0.1mol/L)VSasdescribedunder2.6Non-aqueoustitration,methodA,determiningtheend-pointpotentiometrically.
EachmLofperchloricacid(0.1mol/L)VSisequivalentto22.44mgofC34H54Cl2N10O14.
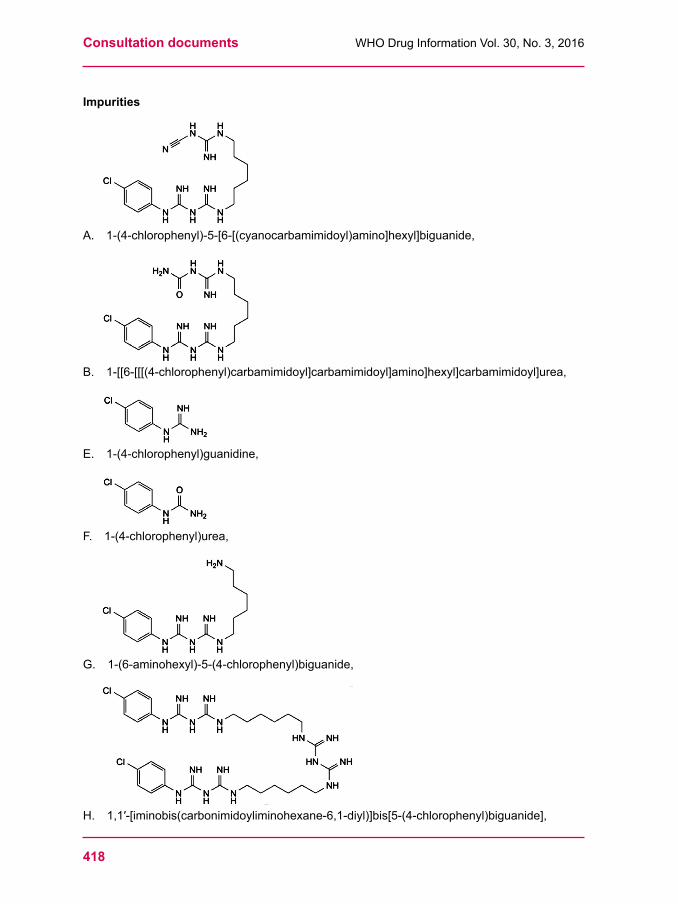
Consultation documents WHODrugInformationVol.30,No.3,2016
418
Impurities
A. 1-(4-chlorophenyl)-5-[6-[(cyanocarbamimidoyl)amino]hexyl]biguanide,
B. 1-[[6-[[[(4-chlorophenyl)carbamimidoyl]carbamimidoyl]amino]hexyl]carbamimidoyl]urea,
E. 1-(4-chlorophenyl)guanidine,
F. 1-(4-chlorophenyl)urea,
G. 1-(6-aminohexyl)-5-(4-chlorophenyl)biguanide,
H. 1,1′-[iminobis(carbonimidoyliminohexane-6,1-diyl)]bis[5-(4-chlorophenyl)biguanide],
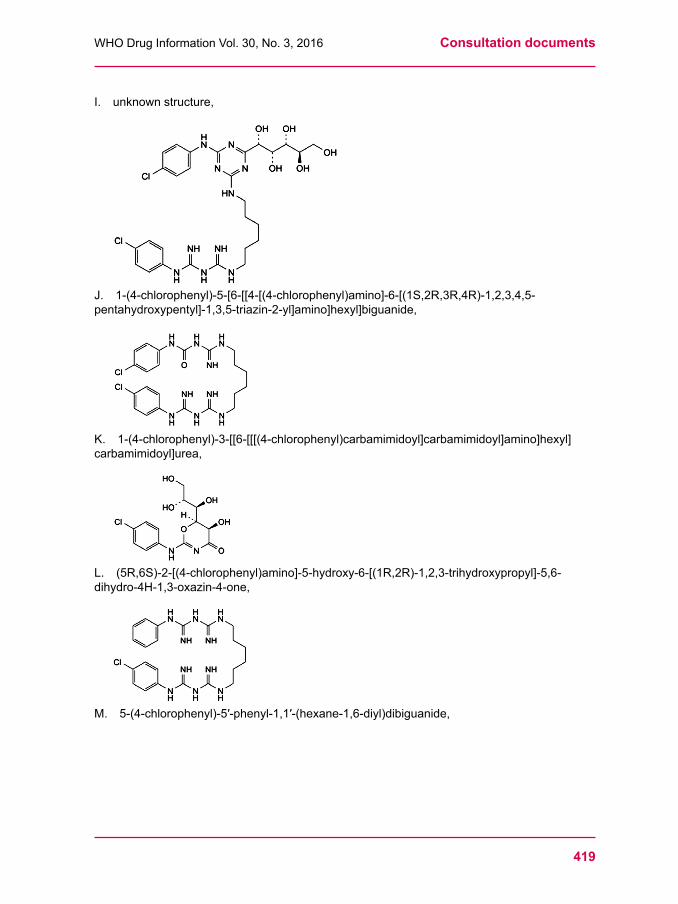
419
WHODrugInformationVol.30,No.3,2016 Consultation documents
I. unknownstructure,
J. 1-(4-chlorophenyl)-5-[6-[[4-[(4-chlorophenyl)amino]-6-[(1S,2R,3R,4R)-1,2,3,4,5-pentahydroxypentyl]-1,3,5-triazin-2-yl]amino]hexyl]biguanide,
K. 1-(4-chlorophenyl)-3-[[6-[[[(4-chlorophenyl)carbamimidoyl]carbamimidoyl]amino]hexyl]carbamimidoyl]urea,
L. (5R,6S)-2-[(4-chlorophenyl)amino]-5-hydroxy-6-[(1R,2R)-1,2,3-trihydroxypropyl]-5,6-dihydro-4H-1,3-oxazin-4-one,
M. 5-(4-chlorophenyl)-5′-phenyl-1,1′-(hexane-1,6-diyl)dibiguanide,
Consultation documents WHODrugInformationVol.30,No.3,2016
420
N. 1-[6-(carbamimidoylamino)hexyl]-5-(4-chlorophenyl)biguanide,
O. 5-(2-chlorophenyl)-5′-(4-chlorophenyl)-1,1′-(hexane-1,6-diyl)dibiguanide,
P. 4-chloroaniline,
Q. unknown structure.
Reference substances to be establishedchlorhexidineforsystemsuitabilityRS
Reagents to be added to Reagents, test solutions and volumetric solutionsSodium hydroxide (~420 g/L) TS. AsolutionofsodiumhydroxideRcontainingabout420g/LofNaOH.
Titan yellow paper RImpregnatefilterpaperwithtitanyellowTS.Allowtodryatroomtemperature.
Sulfuric acid (~98 gLl) TS. Procedure.Add55mLofsulfuricacid(~1760g/L)TStosufficientwatertoproduce1000mL;d~1.063.
Hydrochloric acid (~103 g/L) TSHydrochloricacid(~420g/L)TS,dilutewithwatertocontain103gofHClin1000mL.
Hydrochloric acid (~200 g/L) TSHydrochloricacid(~420g/L)TS,dilutewithwatertocontain200gofHClin1000mL.
***
421
WHODrugInformationVol.30,No.3,2016 Consultation documents
Chlorhexidine digluconate topical solution(Chlorhexidini digluconatis solutio topicalis)
This is a draft proposal for The International Pharmacopoeia (Working document QAS/16.669, June 2016). The working document with line numbers is available for comment at www.who.int/medicines/areas/quality_safety/quality_assurance/projects/en/. Please address any comments to: World Health Organization, Quality Assurance and Safety: Medicines, Dr Herbert Schmidt, 1211 Geneva 27, Switzerland; fax: +41 22 791 4730; email: [email protected].
Category. Antiseptic.
Storage.Chlorhexidinedigluconatetopicalsolutionshouldbekeptinawell-closedcontainer,protectedfromlight.
Additional information. StrengthinthecurrentWHOModelListofEssentialMedicines(EML):5%(digluconate)and7.1%(digluconate),delivering4%chlorhexidine(forumbilicalcordcare);strengthsinthecurrentEMLforchildren:5%(digluconate)and7.1%(digluconate),delivering4%chlorhexidine(forumbilicalcordcare).
Definition. Chlorhexidine digluconate topical solution is a solution of Chlorhexidine digluconate solutioninasuitablevehicle.Itcontainsnotlessthan90.0%andnotmorethan110.0%oftheamountofchlorhexidinedigluconate(C22H30Cl2N10▪2C6H12O7) stated on the label.
Identity testsA. Carry out the test as described under 1.14.1Thin-layerchromatography using silica
gelR5asthecoatingsubstanceandamixtureof50volumesofdehydratedethanolR,10volumesofethylacetateR,10volumesofammonia(~260g/L)TSRand30volumesofwaterRasthemobilephase.Applyseparatelytotheplate2μLofeachofthefollowing2 solutions in water R. For solution (A) dilute a quantity of the topical solution to obtain asolutioncontaining20mgofchlorhexidinedigluconatepermL.Forsolution(B)useasolutioncontaining10mgofpotassiumgluconateRpermL.Afterremovingtheplatefromthechromatographicchamberheattheplatefor20minutesat110°Candallowtheplatetocool.Spraywithammoniummolybdate/cericsulfate/sulfuricacidTS.Heattheplatefor10minutesat110°C.Examinethechromatogramindaylight.
Theprincipalspotobtainedwithsolution(A)correspondsinposition,appearanceandintensity to that obtained with solution (B).
B.Transferaquantityofthetopicalsolutioncontaining5mgofchlorhexidinedigluconateintoa500mLvolumetricflaskanddilutetovolumewithwaterR.Theabsorptionspectrum(1.6) oftheresultingsolution,whenobservedbetween200nmand320nm,exhibitstwomaximaatabout231nmand255nm,andtwominimaatabout218nmand242nm.
C. Carry out the test as described under 1.14.4High-performanceliquidchromatography usingtheconditionsgivenunder“Assay”.Theretentiontimeoftheprincipalpeakinthechromatogramobtainedwithsolution(1)correspondstotheretentiontimeofthepeakduetochlorhexidineinthechromatogramobtainedwithsolution(2).
pH value (1.13).5.0–7.0.
Consultation documents WHODrugInformationVol.30,No.3,2016
422
Impurity P (4-Chloroaniline)Preparefreshsolutionsandperformthetestswithoutdelay.Carryoutthetestasdescribedunder 1.14.4High-performanceliquidchromatographyusingthesamechromatographicconditionsasdescribedunder“Assay”.
PreparethefollowingsolutionsinmobilephaseA:
Forsolution(1)transferanamountofthetopicalsolution,equivalentto40.0mgchlorhexidinedigluconatetoa100mLvolumetricflask,anddilutetovolume.
Forsolution(2)use1.0μgof4-chloroaniline RpermL.
Forsolution(3)prepareasolutionthatcontains50μgpermLofchlorhexidinediacetateRSand1μgpermL4-chloroaniline R.
Inject50µLofsolution(3)Inthechromatogramobtainedwithsolution(3)thepeakdueto4-chloroanilineiselutedatarelativeretentionofabout1.3withreferencetochlorhexidine(retentiontimeabout6minutes).Thetestisnotvalidunlesstheresolutionbetweenthepeaksdueto4-chloroanilineandchlorhexidineisatleast3.0.
Injectalternately50μLofeachofsolutions(1)and(2).
Measure the areas of the peaks corresponding to 4-chloroaniline obtained in the chromatogramsofsolutions(1)and(2).
Inthechromatogramobtainedwithsolution(1):• the area of any peak corresponding to 4-chloroaniline is not greater than the area of the principalpeakinthechromatogramobtainedwithsolution(2)(0.05%(m/v)withreferencetothe concentration of chlorhexidine digluconate in the topical solution).
Assay Preparefreshsolutionsandperformthetestswithoutdelay.
Carry out the test as described under 1.14.4High-performanceliquidchromatography using a stainlesssteelcolumn(25cmx4.6mm)packedwithparticlesofsilicagel,thesurfaceofwhichhasbeenmodifiedwithchemically-bondedoctadecylsilanegroups(5μm).1
Usethefollowingconditionsforgradientelution:
mobilephaseA: Dissolve27.6gofsodiumdihydrogenphosphateRand10mLoftriethylamineRin1.5Lwater.AdjustthepHto3.0usingphosphoricacid(~1440g/L)TS.DilutewithwaterRtoafinalvolumeof2L.Preparea70:30mixtureoftheresultingsolutionandacetonitrileR;
mobilephaseB: AcetonitrileR.Time (min)
Mobile phase A (%v/v)
Mobile phase B (%v/v)
Comments
0–9 100 0 Isocratic9–10 100to45 0to55 Linear gradient10–15 45 55 Isocratic15–16 45to100 55to0 Linear gradient16–21 100 0 Isocratic
1 SymmetryC18,250mmx4.6mm–5μmwasfoundsuitable.
423
WHODrugInformationVol.30,No.3,2016 Consultation documents
Operatewithaflowrateof1.5mLperminute.Asadetectoruseanultravioletspectrophotometersetatawavelengthof239nm.
Maintainthecolumntemperatureat40°C.
Preparethefollowingsolutions:
Forsolution(1)transferanamountofthetopicalsolution,equivalenttoabout40mgchlorhexidinedigluconate,accuratelyweighed,toa100mLvolumetricflask,anddilutetovolumewithmethanolR.Furtherdilutea10mLportionofthissolutionwithmobilephaseAto50mL.
Forsolution(2)use50μgofchlorhexidinediacetateRSpermLinmobilephaseA.
Forsolution(3)prepareasolutionthatcontains50μgpermLofchlorhexidinediacetateRSand1μgpermL4-chloroanilineRinmobilephaseA.
Inject50µLofsolution(3).
Inthechromatogramobtainedwithsolution(3)thepeakdueto4-chloroanilineiselutedatarelativeretentionofabout1.3withreferencetochlorhexidine(retentiontimeabout6minutes).Theassayisnotvalidunlesstheresolutionbetweenthepeaksdueto4-chloroanilineandchlorhexidineisatleast3.0.
Injectalternately50μLofeachofsolutions(1)and(2).
Measuretheareasofthepeakscorrespondingtochlorhexidineobtainedinthechromatogramsofsolutions(1)and(2).DeterminetheweightpermL(1.3.1) and calculate the percentage contentofchlorhexidinedigluconate,weightinvolume,inthetopicalsolutionusingthedeclaredcontentofchlorhexidineinchlorhexidinediacetateRS(C22H30Cl2N10· 2C2H4O2). Each mgofchlorhexidine(C22H30Cl2N10)isequivalentto1.776mgofchlorhexidinedigluconate(C22H30Cl2N10· 2C6H12O7).
Impurities.TheimpuritylimitedbytherequirementsofthismonographisimpurityPlistedinthemonographforChlorhexidinedigluconatesolution.
Reagents to be added to Reagents, test solutions and volumetric solutionsPotassium gluconate R C6H11KO7
Reference substances to be establishedChlorhexidine diacetate RS 4-chloroaniline RS
***
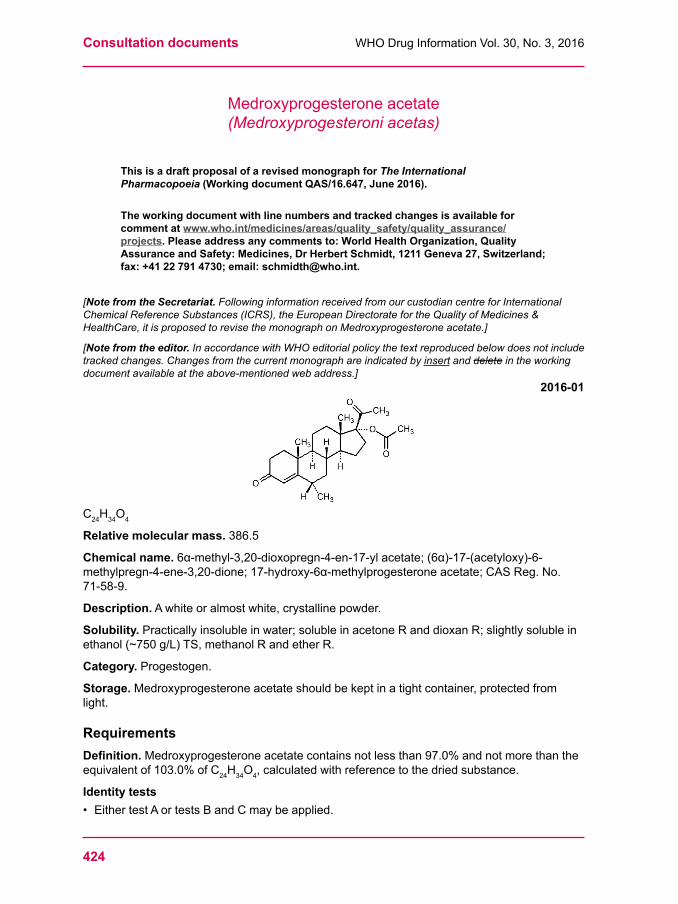
Consultation documents WHODrugInformationVol.30,No.3,2016
424
Medroxyprogesterone acetate (Medroxyprogesteroni acetas)
This is a draft proposal of a revised monograph for The International Pharmacopoeia (Working document QAS/16.647, June 2016).
The working document with line numbers and tracked changes is available for comment at www.who.int/medicines/areas/quality_safety/quality_assurance/projects. Please address any comments to: World Health Organization, Quality Assurance and Safety: Medicines, Dr Herbert Schmidt, 1211 Geneva 27, Switzerland; fax: +41 22 791 4730; email: [email protected].
[Note from the Secretariat. Following information received from our custodian centre for International Chemical Reference Substances (ICRS), the European Directorate for the Quality of Medicines & HealthCare, it is proposed to revise the monograph on Medroxyprogesterone acetate.]
[Note from the editor. In accordance with WHO editorial policy the text reproduced below does not include tracked changes. Changes from the current monograph are indicated by insert and delete in the working document available at the above-mentioned web address.]
2016-01
C24H34O4
Relative molecular mass.386.5
Chemical name.6α-methyl-3,20-dioxopregn-4-en-17-ylacetate;(6α)-17-(acetyloxy)-6-methylpregn-4-ene-3,20-dione;17-hydroxy-6α-methylprogesteroneacetate;CASReg.No.71-58-9.
Description.Awhiteoralmostwhite,crystallinepowder.
Solubility.Practicallyinsolubleinwater;solubleinacetoneRanddioxanR;slightlysolubleinethanol(~750g/L)TS,methanolRandetherR.
Category. Progestogen.
Storage.Medroxyprogesteroneacetateshouldbekeptinatightcontainer,protectedfromlight.
RequirementsDefinition.Medroxyprogesteroneacetatecontainsnotlessthan97.0%andnotmorethantheequivalentof103.0%ofC24H34O4,calculatedwithreferencetothedriedsubstance.
Identity tests• EithertestAortestsBandCmaybeapplied.
425
WHODrugInformationVol.30,No.3,2016 Consultation documents
A.Carryouttheexaminationasdescribedunder1.7Spectrophotometryintheinfraredregion.TheinfraredabsorptionspectrumisconcordantwiththespectrumobtainedfrommedroxyprogesteroneacetateRSorwiththereferencespectrumofmedroxyprogesteroneacetate.
B.CarryouttestB.1or,whereUVdetectionisnotavailable,testB.2.
B.1 Carry out the test as described under 1.14.1.Thin-layerchromatography using silicaR5asthecoatingsubstanceandamixtureof10volumesofdichloromethaneRand1volumeofethylacetateRasthemobilephase.Applyseparatelytotheplate10μLofeachofthefollowingthreesolutionsindichloromethaneR.Forsolution(A)use 2.5mgofMedroxyprogesteroneacetatepermL.Forsolution(B)use2.5mgofmedroxyprogesteroneacetateRSpermL.Afterremovingtheplatefromthechromatographicchamberheatitat120°Cfor30minutes,spraywith4-toluenesulfonicacid/ethanolTSandheatfurtherat120°Cfor10minutes.Allowtheplatetocoolandexaminethechromatograminultravioletlight(365nm).
Theprincipalspotobtainedwithsolution(A)correspondsinposition,appearanceandintensity to that obtained with solution (B).
B.2 Carry out the test as described under 1.14.1Thin-layerchromatography using the conditionsdescribedundertestB.1,butspraytheplatewithamixtureofequalvolumesofsulfuricacidRandethanol(~750g/L)TSandheatfurtherat120°Cfor10minutes.Allowtheplatetocoolandexaminethechromatogramindaylight.Theprincipalspotobtainedwithsolution(A)correspondsinposition,appearanceandintensity to that obtained with solution (B).
C.Use20mg;ityieldsthereactiondescribedunder2.1Generalidentificationtests as characteristic of acetylated substances.
Specificopticalrotation.Usea10mg/mLsolutioninacetoneR;[a]20°C=+47°to+53°.
Sulfated ash.Notmorethan1.0mg/g.
Loss on drying.Dryat105°Cfor3hours;itlosesnotmorethan10mg/g.
Impurity FA. Carry out the test as described under 1.14.4High-performanceliquidchromatography
usingastainlesssteelcolumn(10cm×4.6mm)packedwithparticlesofsilicagel,thesurfaceofwhichhasbeenmodifiedwithchemically-bondedoctadecylsilylgroups(3µm).
Asthemobilephaseuseasolutionpreparedasfollows:mix44volumesofwaterRand56volumesofacetonitrileR.
Forsolution(1)dissolve20mgofMedroxyprogesteroneacetatein5.0mLofacetonitrileRanddiluteto10.0mLwithwaterR.Forsolution(2)dilute0.5volumeofsolution(1)to100volumeswiththemobilephase.Forsolution(3)use0.2mgofmedroxyprogesteroneacetateRSand0.01mgofmedroxyprogesteroneacetateimpurityFRSpermLmobilephase.
Operatewithaflowrateof1.0mLperminute.Asadetectoruseanultravioletspectrophotometersetatawavelengthof200nm.
Inject25µLofsolution(1),(2)and(3).Inthechromatogramobtainedwithsolution(3)impurityFiselutedatarelativeretentionofabout1.8withreferencetomedroxyprogesteroneacetate(retentiontimeabout8minutes).
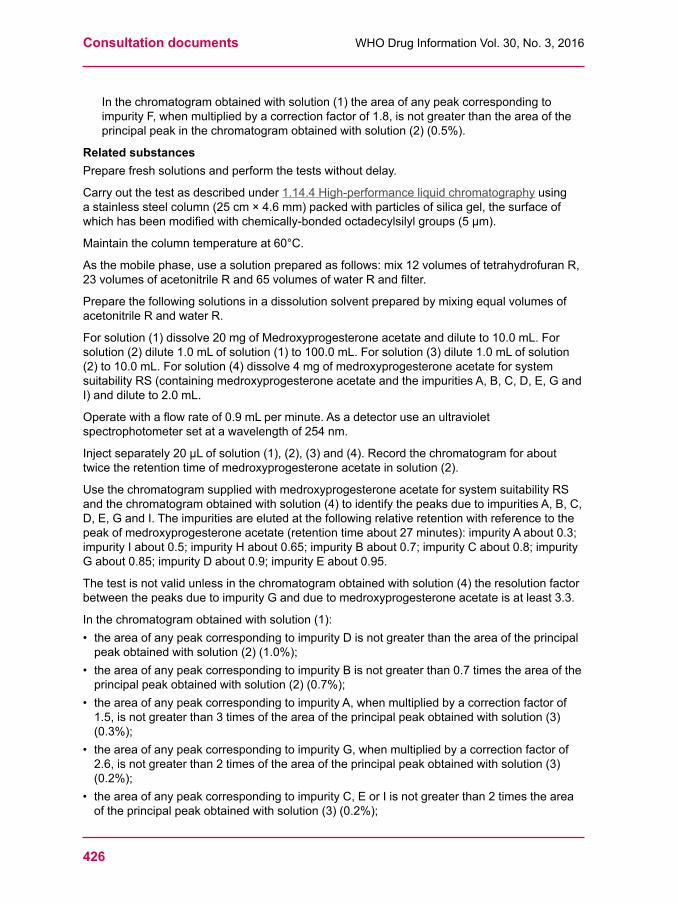
Consultation documents WHODrugInformationVol.30,No.3,2016
426
Inthechromatogramobtainedwithsolution(1)theareaofanypeakcorrespondingtoimpurityF,whenmultipliedbyacorrectionfactorof1.8,isnotgreaterthantheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(2)(0.5%).
Related substancesPreparefreshsolutionsandperformthetestswithoutdelay.
Carry out the test as described under 1.14.4High-performanceliquidchromatography using astainlesssteelcolumn(25cm×4.6mm)packedwithparticlesofsilicagel,thesurfaceofwhichhasbeenmodifiedwithchemically-bondedoctadecylsilylgroups(5µm).
Maintainthecolumntemperatureat60°C.
Asthemobilephase,useasolutionpreparedasfollows:mix12volumesoftetrahydrofuranR,23volumesofacetonitrileRand65volumesofwaterRandfilter.
Preparethefollowingsolutionsinadissolutionsolventpreparedbymixingequalvolumesofacetonitrile R and water R.
Forsolution(1)dissolve20mgofMedroxyprogesteroneacetateanddiluteto10.0mL.Forsolution(2)dilute1.0mLofsolution(1)to100.0mL.Forsolution(3)dilute1.0mLofsolution(2)to10.0mL.Forsolution(4)dissolve4mgofmedroxyprogesteroneacetateforsystemsuitabilityRS(containingmedroxyprogesteroneacetateandtheimpuritiesA,B,C,D,E,GandI)anddiluteto2.0mL.
Operatewithaflowrateof0.9mLperminute.Asadetectoruseanultravioletspectrophotometersetatawavelengthof254nm.
Injectseparately20µLofsolution(1),(2),(3)and(4).Recordthechromatogramforabouttwicetheretentiontimeofmedroxyprogesteroneacetateinsolution(2).
UsethechromatogramsuppliedwithmedroxyprogesteroneacetateforsystemsuitabilityRSandthechromatogramobtainedwithsolution(4)toidentifythepeaksduetoimpuritiesA,B,C,D,E,GandI.Theimpuritiesareelutedatthefollowingrelativeretentionwithreferencetothepeakofmedroxyprogesteroneacetate(retentiontimeabout27minutes):impurityAabout0.3;impurityIabout0.5;impurityHabout0.65;impurityBabout0.7;impurityCabout0.8;impurityGabout0.85;impurityDabout0.9;impurityEabout0.95.
Thetestisnotvalidunlessinthechromatogramobtainedwithsolution(4)theresolutionfactorbetweenthepeaksduetoimpurityGandduetomedroxyprogesteroneacetateisatleast3.3.
Inthechromatogramobtainedwithsolution(1):• theareaofanypeakcorrespondingtoimpurityDisnotgreaterthantheareaoftheprincipalpeakobtainedwithsolution(2)(1.0%);
• theareaofanypeakcorrespondingtoimpurityBisnotgreaterthan0.7timestheareaoftheprincipalpeakobtainedwithsolution(2)(0.7%);
• theareaofanypeakcorrespondingtoimpurityA,whenmultipliedbyacorrectionfactorof1.5,isnotgreaterthan3timesoftheareaoftheprincipalpeakobtainedwithsolution(3)(0.3%);
• theareaofanypeakcorrespondingtoimpurityG,whenmultipliedbyacorrectionfactorof2.6,isnotgreaterthan2timesoftheareaoftheprincipalpeakobtainedwithsolution(3)(0.2%);
• theareaofanypeakcorrespondingtoimpurityC,EorIisnotgreaterthan2timestheareaoftheprincipalpeakobtainedwithsolution(3)(0.2%);
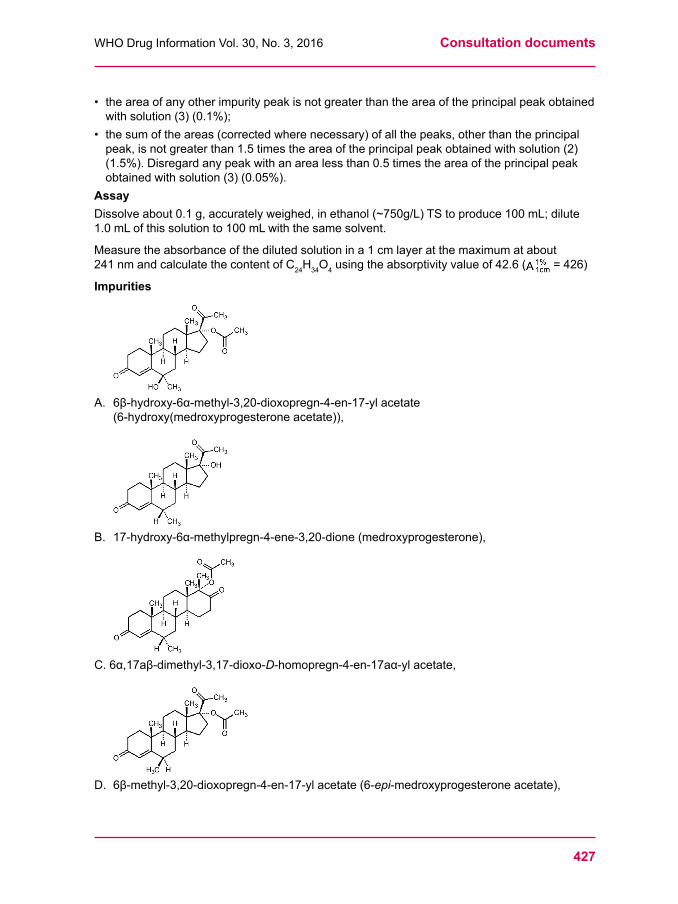
427
WHODrugInformationVol.30,No.3,2016 Consultation documents
• theareaofanyotherimpuritypeakisnotgreaterthantheareaoftheprincipalpeakobtainedwithsolution(3)(0.1%);
• thesumoftheareas(correctedwherenecessary)ofallthepeaks,otherthantheprincipalpeak,isnotgreaterthan1.5timestheareaoftheprincipalpeakobtainedwithsolution(2)(1.5%).Disregardanypeakwithanarealessthan0.5timestheareaoftheprincipalpeakobtainedwithsolution(3)(0.05%).
AssayDissolveabout0.1g,accuratelyweighed,inethanol(~750g/L)TStoproduce100mL;dilute1.0mLofthissolutionto100mLwiththesamesolvent.
Measuretheabsorbanceofthedilutedsolutionina1cmlayeratthemaximumatabout241nmandcalculatethecontentofC24H34O4usingtheabsorptivityvalueof42.6( =426)
Impurities
A.6β-hydroxy-6α-methyl-3,20-dioxopregn-4-en-17-ylacetate(6-hydroxy(medroxyprogesteroneacetate)),
B. 17-hydroxy-6α-methylpregn-4-ene-3,20-dione(medroxyprogesterone),
C.6α,17aβ-dimethyl-3,17-dioxo-D-homopregn-4-en-17aα-ylacetate,
D.6β-methyl-3,20-dioxopregn-4-en-17-ylacetate(6-epi-medroxyprogesteroneacetate),
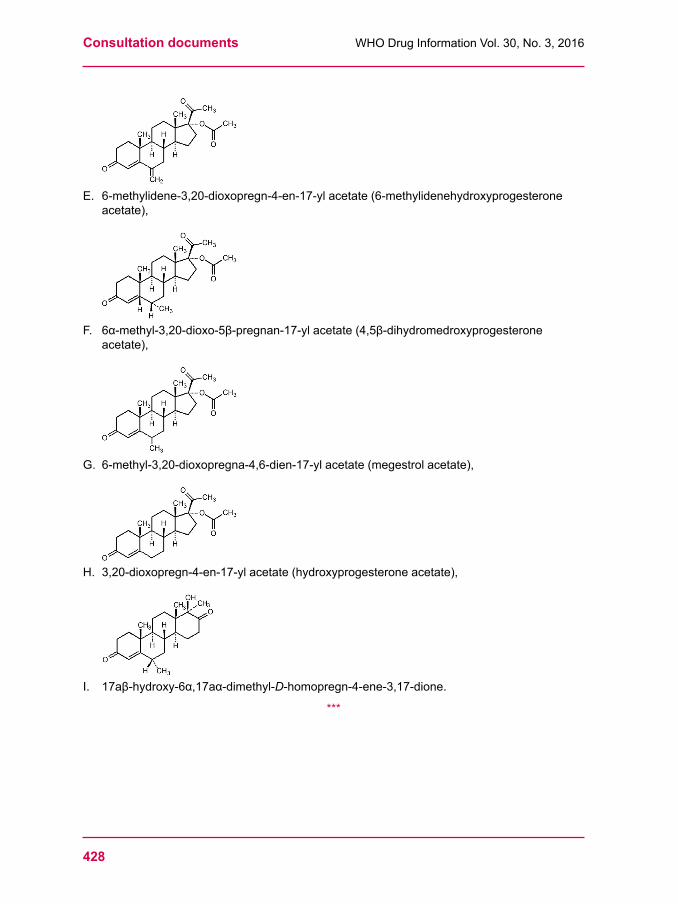
Consultation documents WHODrugInformationVol.30,No.3,2016
428
E.6-methylidene-3,20-dioxopregn-4-en-17-ylacetate(6-methylidenehydroxyprogesteroneacetate),
F. 6α-methyl-3,20-dioxo-5β-pregnan-17-ylacetate(4,5β-dihydromedroxyprogesteroneacetate),
G.6-methyl-3,20-dioxopregna-4,6-dien-17-ylacetate(megestrolacetate),
H.3,20-dioxopregn-4-en-17-ylacetate(hydroxyprogesteroneacetate),
I. 17aβ-hydroxy-6α,17aα-dimethyl-D-homopregn-4-ene-3,17-dione.
***
429
WHODrugInformationVol.30,No.3,2016 Consultation documents
Medroxyprogesteroneinjection(Medroxyprogesteroni injectio)
This is a draft proposal of a revised monograph for The International Pharmacopoeia (Working document QAS/16.670, June 2016). The working document with line numbers and tracked changes is available for comment at www.who.int/medicines/areas/quality_safety/quality_assurance/projects. Please address any comments to: World Health Organization, Quality Assurance and Safety: Medicines, Dr Herbert Schmidt, 1211 Geneva 27, Switzerland; fax: +41 22 791 4730; email: [email protected].
[Note from the Secretariat. Following information received from our custodian centre for International Chemical Reference Substances (ICRS), the European Directorate for the Quality of Medicines & HealthCare, it is proposed to revise the monograph on Medroxyprogesterone injection.]
[Note from the editor. In accordance with WHO editorial policy the text reproduced below does not include tracked changes. Changes from the current monograph are indicated by insert and delete in the working document available at the above-mentioned web address.]
2016-01Category.Contraceptive.
Storage.Medroxyprogesteroneinjectionshouldbeprotectedfromlight.Onstandingsolidmattermayseparate;itshouldberesuspendedbeforeuse.
Additional information.StrengthinthecurrentWHOModelListofEssentialMedicines:150mg/mLin1mLvial.
RequirementsComplieswiththemonographforParenteral preparations.
Definition.MedroxyprogesteroneinjectionisasterileaqueoussuspensionofMedroxyprogesteroneacetate.Itcontainsnotlessthan90.0%andnotmorethan110.0%oftheamountofMedroxyprogesteroneacetate(C24H34O4) stated on the label.
Identity tests• EithertestAaloneortestsBandCortestsCandDmaybeapplied.A. Centrifugeavolumeoftheinjectiontobeexaminedcontaining50mgofMedroxyprogesterone acetate. Decant the supernatant liquid and discard. Dry the residue at 105°Cfor3hoursandcarryouttheexaminationasdescribedunder1.7Spectrophotometryin the infrared region.TheinfraredabsorptionspectrumisconcordantwiththespectrumobtainedfrommedroxyprogesteroneacetateRSorwiththereference spectrum of medroxyprogesteroneacetate.
B.CarryouttestB.1or,whereUVdetectionisnotavailable,testB.2.
B.1 Carry out the test as described under 1.14.1Thin-layerchromatography using silica R5asthecoatingsubstanceandamixtureof10volumesofdichloromethaneRand1volumeofethylacetateRasthemobilephase.Applyseparatelytotheplate10μLofeachofthefollowingthreesolutionsindichloromethaneR.Forsolution(A)measureavolumeofinjectiontobeexaminedcontainingabout40mgofMedroxyprogesteroneacetate,add15mLofdichloromethaneR,shakevigorouslyfor
Consultation documents WHODrugInformationVol.30,No.3,2016
430
20minutes,allowtostandfor30minutes,add2.5gsodiumsulphateanhydrousR,shakefor5minutesandallowtostandforanother10minutes.Forsolution(B)use2.5mgofmedroxyprogesteroneacetateRSpermL.Afterremovingtheplatefromthechromatographicchamberheatitat120°Cfor30minutes,spraywith4-toluenesulfonicacid/ethanolTSandheatfurtherat120°Cfor10minutes.Allowtheplatetocoolandexaminethechromatograminultravioletlight(365nm).
Theprincipalspotobtainedwithsolution(A)correspondsinposition,appearanceandintensity to that obtained with solution (B).
B.2 Carry out the test as described under 1.14.1Thin-layerchromatography using the conditionsdescribedundertestB.1,butspraytheplatewithamixtureofequalvolumesofsulfuricacidRandethanol(~750g/L)TSandheatfurtherat120°Cfor10minutes.Allowtheplatetocoolandexaminethechromatogramindaylight.Theprincipalspotobtainedwithsolution(A)correspondsinposition,appearanceandintensity to that obtained with solution (B).
C.Centrifugeavolumeofinjectiontobeexaminedcontaining30mgofMedroxyprogesteroneacetate.Decantthesupernatantliquid,dissolvetheresiduein5mLofsulfuricacidRandintroduce5mLofethanol(~750g/L)TStoformanupperlayer;abluishvioletringisformedattheinterfaceofthetwolayers.
D.Seethetestdescribedbelowunder“Assay”.Theretentiontimeoftheprincipalpeakinthechromatogramobtainedwithsolution(1)issimilartothatinthechromatogramobtainedwith solution (2).
pH.pHoftheinjection,3.0–7.0.
Impurity F (4,5-Dihydromedroxyprogesterone acetate). Carry out the test as described under 1.14.1Thin-layerchromatographyusingsilicagelR5asthecoatingsubstanceandamixtureof10volumesoftetrahydrofuranR,45volumesof tert-butylmethyletherRand45volumesofhexaneRasthemobilephase.
Applyseparatelytotheplate10µLofeachofthefollowingthreesolutionsindichloromethaneR.Forsolution(A)accuratelymeasureavolumeofinjectiontobeexaminedcontaining300mgofMedroxyprogesteroneacetate,add15mLofdichloromethaneR,shakevigorouslyfor20minutes,allowtostandfor30minutes,add10gsodiumsulphateanhydrousR,shakefor5minutesandallowtostandforanother10minutes.Forsolution(B)dilute0.5volumeofsolution(1)to100volumes.Forsolution(C)use20mgofmedroxyprogesteroneacetateRSand0.1mgofmedroxyprogesteroneacetateimpurityFRSpermL.
Developtheplateforadistanceofabout10cm.Allowittodryinairandcarryoutaseconddevelopmentinthesamedirectionusingafreshlypreparedmobilephase.Afterremovingtheplatefromthechromatographicchamberheatitat100°Cto105°Cfor30minutesandspraywith4-toluenesulfonicacid/ethanolTS.Heatagainat120°Cfor10minutes,allowtocoolandexaminethechromatograminultravioletlight(365nm).
Inthechromatogramobtainedwithsolution(C)impurityFhasaRfvalueofabout0.66andmedroxyprogesteroneacetateanRfvalueofabout0.56.Thetestisnotvalidunlessthechromatogramobtainedwithsolution(C)showstwoclearlyseparatedspots.Inthechromatogramobtainedwithsolution(A)anyspotduetoimpurityFisnotmoreintensethanthecorrespondingspotinthechromatogramobtainedwithsolution(B)(0.5%).
Related substancesPreparefreshsolutionsandperformthetestswithoutdelay.
431
WHODrugInformationVol.30,No.3,2016 Consultation documents
Carry out the test as described under 1.14.4High-performanceliquidchromatography using theconditionsgivenunder“Assay”.
Preparethefollowingsolutionswiththemobilephase.Forsolution(1)diluteasuitablevolumeoftheinjectiontobeexaminedtoobtainaconcentrationof0.4mgofMedroxyprogesteroneacetatepermL.Forsolution(2)dilute1.0mLofsolution(1)to100.0mL.Forsolution(3)dissolve4mgofmedroxyprogesteroneacetateforsystemsuitabilityRS(containingmedroxyprogesteroneacetateandtheimpuritiesA,B,C,D,E,GandI)anddiluteto2.0mL.Forsolution(4)use3.65μgofmethylhydroxybenzoateRand0.4μgofpropylhydroxybenzoateRpermL.Injectseparately20µLofsolution(1),(2),(3)and(4).Recordthechromatogramforabouttwicetheretentiontimeofmedroxyprogesteroneacetateinsolution(2).UsethechromatogramsuppliedwithmedroxyprogesteroneacetateforsystemsuitabilityRSandthechromatogramobtainedwithsolution(4)toidentifythepeaksduetoimpuritiesA,B,C,D,E,GandI.Theimpuritiesareelutedatthefollowingrelativeretentionwithreferencetothepeakofmedroxyprogesteroneacetate(retentiontimeabout27minutes):impurityAabout0.3;impurityIabout0.5;impurityHabout0.65;impurityBabout0.7;impurityCabout0.8;impurityGabout0.85;impurityDabout0.9;impurityEabout0.95.ThetestisnotvalidunlesstheresolutionfactorbetweenthepeaksduetomedroxyprogesteroneacetateandduetoimpurityGisatleast3.3.Inthechromatogramobtainedwithsolution(1):• theareaofanypeak,otherthantheprincipalpeak,isnotgreaterthantheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(2)(1.0%);
• thesumoftheareasofallpeaks,otherthantheprincipalpeak,isnotgreaterthan1.5timestheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(2)(1.5%).Disregardanypeakduetohydroxybenzoatederivativesinthechromatogramobtainedwithsolution(4).Disregardanypeakwithanarealessthan0.05timestheareaoftheprincipalpeakobtainedwithsolution(2)(0.05%).
AssayCarry out the test as described under 1.14.4High-performanceliquidchromatography using astainlesssteelcolumn(25cm×4.6mm)packedwithparticlesofsilicagel,thesurfaceofwhichhasbeenmodifiedwithchemically-bondedoctadecylsilylgroups(5µm).
Asthemobilephaseuseasolutionpreparedasfollows:mix100volumesoftetrahydrofuranR,350volumesofacetonitrileRand500volumesofwaterR.
Preparethefollowingsolutionsinthemobilephase.Forsolution(1)diluteasuitablevolumeoftheinjectiontobeexaminedtoobtainaconcentrationof40μgofMedroxyprogesteroneacetatepermL.Forsolution(2)dissolve10mgofmedroxyprogesteroneacetateRSin50mL.Dilute5mLofthissolutionto25mL.
Operatewithaflowrateof0.9mLperminute.Asadetectoruseanultravioletspectrophotometersetatawavelengthof241nm.
Injectseparately20µLofsolution(1)and(2).
Measuretheareasofthepeakresponsesobtainedinthechromatogramsfromsolutions(1)and(2)andcalculatethepercentagecontentofmedroxyprogesteroneacetate(C24H34O4),using the declared content of C24H34O4inmedroxyprogesteroneacetateRS.
***
Consultation documents WHODrugInformationVol.30,No.3,2016
432
Clindamycinpalmitatehydrochloride(Clindamycini palmitas hydrochloridum)
This is a draft proposal of a monograph for The International Pharmacopoeia (Working document QAS/16.654, July 2016). The working document with line numbers is available for comment at www.who.int/medicines/areas/quality_safety/quality_assurance/projects. Please address any comments to: World Health Organization, Quality Assurance and Safety: Medicines, Dr Herbert Schmidt, 1211 Geneva 27, Switzerland; fax: +41 22 791 4730; email: [email protected].
Molecular formula. C34H63ClN2O6S·HCl
Relative molecular mass. 699.85
Graphic formula
Chemical name. L-threo-α-D-galacto-Octopyranoside,methyl7-chloro-6,7,8-trideoxy-6-[[(1-methyl-4-propyl-2-pyrrolidinyl)-carbonyl]amino]-1-thio-2-hexadecanoate,monohydrochloride,(2S-trans)-;Methyl7-chloro-6,7,8-trideoxy-6-(1-methyl-trans-4-propyl-L-2-pyrrolidinecarboxamido)-1-thio-L- threo-α-D-galacto-octopyranoside2-palmitatemonohydrochloride;CASReg.No.25507-04-4.
Description. Awhiteoralmostwhitepowder.
Solubility. Freelysolubleinethanolandindichloromethane;solubleinwater.
Category. Antibacterial.
Storage.Clindamycinpalmitatehydrochlorideshouldbepreservedinatightlyclosedcontainer.
Additional information.Clindamycinpalmitatehydrochlorideisasemi-syntheticproductderivedfromafermentationproduct.
RequirementsDefinition.Clindamycinpalmitatehydrochloridecontainsnotlessthan91.0%andnotmorethan102.0%ofC34H63ClN2O6S.HCl,calculatedwithreferencetotheanhydroussubstance.Identity tests• EithertestsAandDortestsB,CandDmaybeappliedA.Carryouttheexaminationasdescribedunder1.7Spectrophotometryintheinfrared
region.TheinfraredabsorptionspectrumisconcordantwiththespectrumobtainedfromclindamycinpalmitatehydrochlorideRSorwiththereferencespectrumofclindamycinpalmitatehydrochloride.
433
WHODrugInformationVol.30,No.3,2016 Consultation documents
B. Carry out the test as described under 1.14.4High-performanceliquidchromatography usingtheconditionsgivenunder“Assay”.Theretentiontimeoftheprincipalpeakinthechromatogramobtainedwithsolution(1)correspondstothatoftheprincipalpeakinthechromatogramobtainedwithsolution(2).
C.Dissolveabout10mgin2mLofhydrochloricacid(~200g/L)TSandheatonawater-bathfor3minutes.Add3mLofsodiumcarbonate(106g/L)TSand1mLofsodiumnitroprusside(20g/L)TS.Aviolet-redcolourdevelops[test to be verified].
D.A10mg/mLsolutionyieldsreactionBdescribedunder2.1Generalidentificationtests as characteristic of chlorides.
Water.Determineasdescribedunder2.8DeterminationofwaterbytheKarlFischermethod,MethodA,using0.1gofthesubstance;thewatercontentisnotmorethan30mg/g.
pH value. pHofa10mg/mLsolutionincarbon-dioxide-freewaterR,2.8–3.8.Sulfated ash.Notmorethan5mg/g.
Related substances Carry out the test as described under 1.14.4High-performanceliquidchromatography using acolumn(25cm×4.6mm)packedwithparticlesofsilicagel,thesurfaceofwhichhasbeenmodifiedwithchemically-bondedoctylsilylgroups(5μm).1
Usethefollowingconditionsforgradientelution:mobilephaseA:Ammoniumacetate(~0,40g/L)TS-acetonitrileR(50:50);mobilephaseB:AcetonitrileR.
Time(min) MobilephaseA(%v/v) MobilephaseB(%v/v) Comment0–30 100to0 0to100 Linear gradient30–80 0 100 Isocratic80–81 0to100 100to0 Returntoinitialcomposition81–90 100 0 Re-equilibration
PreparethefollowingsolutionsinmethanolR.Forsolution(1)dissolve100mgofclindamycinpalmitatehydrochlorideanddiluteto10.0mL.Forsolution(2)dilute2.0mLofsolution(1)to100mL.Forsolution(3)dissolveabout74mgclindamycinpalmitatehydrochlorideRS(containingclindamycinpalmitatehydrochlorideandimpurityA)anddiluteto10.0mL.Operatewithaflowrateof1.0mLperminute.Asadetectoruseanultravioletspectrophotometersetatawavelengthof230nm.Injectalternately20μLeachofsolution(1),(2)and(3).Inthechromatogramobtainedwithsolution(3)theretentiontimeofclindamycinpalmitateisabout37minutes.ThetestisnotvalidunlesstheresolutionbetweenthepeaksduetoclindamycinpalmitateandimpurityA(relativeretentionabout0.9)isatleast3.0.
Inthechromatogramobtainedwithsolution(1):• theareaofanyimpuritypeakisnotmorethantheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(2)(2.0%);
• thesumoftheareasofallimpuritypeaksisnotmorethan3.5timestheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(2)(7.0%).Disregardanypeakwithanarealessthan0.025timestheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(2)(0.05%).
1 AgilentZorbaxElipseXDB-C8hasbeenfoundsuitable.
Consultation documents WHODrugInformationVol.30,No.3,2016
434
Assay [The method is currently under validation. Some parameters need to be amended.]
Carry out the test as described under 1.14.4High-performanceliquidchromatography using astainlesssteelcolumn(25cm×4.6mm)packedwithparticlesofsilicagel,thesurfaceofwhichhasbeenmodifiedwithchemically-bondedoctylsilylgroups(5μm).2 Asthemobilephaseuseamixtureof10volumesofammoniumacetate(~0,40g/L)TSand90volumesofacetonitrileR.Preparethefollowingsolutionsinmobilephase.Forsolution(1)transfer50.0mgofclindamycinpalmitatehydrochlorideintoa50mLvolumetricflaskanddilutetovolume.Forsolution(2)dissolve50mgofclindamycinpalmitatehydrochlorideRS(containingclindamycinpalmitatehydrochlorideandimpurityA)intoa50mLvolumetricflaskanddiluteto50.0mL.Operatewithaflowrateof1.0mLperminute.Asadetectoruseanultravioletspectrophotometersetatawavelengthof230nm.Injectalternately20μLeachofsolutions(1)and(2).Theretentiontimeofclindamycinpalmitateisaboutxminutes.Theassayisnotvalidunlessinthechromatogramobtainedwithsolution(2)theresolutionbetweenthepeaksduetoclindamycinpalmitateandtoimpurityA(relativeretentiontimeisaboutx)isatleastx.Measuretheareasofthepeakscorrespondingtoclindamycinpalmitateobtainedinthechromatogramsfromsolutions(1)and(2)andcalculatethepercentagecontentofclindamycinpalmitatehydrochloride(C34H63ClN2O6S.HCl),usingthedeclaredcontentofclindamycinpalmitatehydrochloride(C34H63ClN2O6S.HCl)inclindamycinpalmitatehydrochlorideRS
Impurities
A. L-threo-α-D-galacto-Octopyranoside,methyl7-chloro-6,7,8-trideoxy-6-[[(1-methyl-4-ethyl-2-pyrrolidinyl)-carbonyl]amino]-1-thio-2-hexadecanoate,(2S-trans)-;Methyl7-chloro-6,7,8-trideoxy-6-(1-methyl-trans-4-ethyl-L-2-pyrrolidinecarboxamido)-1-thio-L-threo-α-D-galacto-octopyranoside2-palmitate(clindamycinBpalmitate)(synthesis-relatedimpurity)
Reagents to be establishedAmmonium acetate (~0,40 g/L) TSAsolutionofammoniumacetateRcontainingabout0.385gofC2H7NO2 per litre (approximately0.005mol/L).
Docusate sodium RC20H37NaO7SAcommerciallyavailablereagentofsuitablegrade.
***
2 AgilentZorbaxElipseXDB-C8hasbeenfoundsuitable.

435
WHODrugInformationVol.30,No.3,2016 Consultation documents
Clindamycinpalmitatefororalsuspension(Clindamycini palmitas ad suspensionem peroralem)
This is a draft proposal of a monograph for The International Pharmacopoeia (Working document QAS/16.655, July 2016). The working document with line numbers is available for comment at www.who.int/medicines/areas/quality_safety/quality_assurance/projects. Please address any comments to: World Health Organization, Quality Assurance and Safety: Medicines, Dr Herbert Schmidt, 1211 Geneva 27, Switzerland; fax: +41 22 791 4730; email: [email protected].
Category. Antibacterial.
Storage.Clindamycinpalmitatehydrochloridefororalsuspensionshouldbekeptinatightlyclosed container.
Additional information. StrengthinthecurrentWHOModelListofEssentialMedicines(EML):75mg/5mL(aspalmitate).StrengthsinthecurrentWHOEMLforChildren:75mg/5mL(aspalmitate).
Labelling.Thedesignationonthecontainerofclindamycinpalmitatefororalsuspensionshouldstatethattheactiveingredientisclindamycinpalmitatehydrochlorideandthequantityshouldbeindicatedintermsofequivalentamountofclindamycin.
RequirementsComplieswiththemonographforLiquid preparations for oral use;thepowdercomplieswiththesectionofthemonographentitled“Powders for oral solutions, oral suspensions and oral drops”.
Definition.ClindamycinpalmitatefororalsuspensionisasuspensionofClindamycinpalmitatehydrochlorideinasuitablevehicle,whichmaybeflavoured.Itispreparedfromthepowderasstatedonthelabeljustbeforeissueforuse.Whenfreshlyconstitutedtheoralsuspensioncontainsnotlessthan90.0%andnotmorethan110.0%ofthelabelledamountofclindamycin(C18H33ClN2O5S).
Identity testsCarry out the test as described under 1.14.4High-performanceliquidchromatography usingtheconditionsgivenunder“Assay”.Theretentiontimeoftheprincipalpeakinthechromatogramobtainedwithsolution(1)correspondstothatoftheprincipalpeakinthechromatogramobtainedwithsolution(2).
pH value.pHofasolutionconstitutedasdirectedinthelabelling,2.5–5.0.Loss on drying. Drythepowderfororalsuspensiontoconstantmassat60°Cunderreducedpressure;itlosesnotmorethan20mg/g.
Related substances Usetheoralsuspensionimmediatelyafterpreparation.
Consultation documents WHODrugInformationVol.30,No.3,2016
436
Carry out the test as described under 1.14.4High-performanceliquidchromatography using acolumn(25cm×4.6mm)packedwithparticlesofsilicagel,thesurfaceofwhichhasbeenmodifiedwithchemically-bondedoctylsilylgroups(5μm).1
Usethefollowingconditionsforgradientelution:mobilephaseA:Ammoniumacetate(~0,40g/L)TS–acetonitrileR(50:50);mobilephaseB:AcetonitrileR.
Time(min) MobilephaseA(%v/v) MobilephaseB(%v/v) Comment0–30 100to0 0to100 Linear gradient30–80 0 100 Isocratic80–81 0to100 100to0 Returntoinitialcomposition81–90 100 0 Re-equilibrationPreparethefollowingsolutionsinmethanolR.Forsolution(1)transferaquantityoftheoralsuspension,equivalentofabout57mgofclindamycintoa10mLvolumetricflaskanddilutetovolume.Forsolution(2)dilute2.0mlofsolution(1)to100.0mL.Forsolution(3)dissolveabout74mgclindamycinpalmitatehydrochlorideRS(containingclindamycinpalmitatehydrochlorideandimpurityA)anddiluteto10.0mL.
Operatewithaflowrateof1.0mLperminute.Asadetectoruseanultravioletspectrophotometersetatawavelengthof230nm.
Injectalternately20μLeachofsolution(1),(2)and(3).
Inthechromatogramobtainedwithsolution(3)theretentiontimeofclindamycinpalmitateisabout37minutes.ThetestisnotvalidunlesstheresolutionbetweenthepeaksduetoclindamycinpalmitateandimpurityA(relativeretentiontimeabout0.9)isatleast3.0.
Inthechromatogramobtainedwithsolution(1):
• theareaofanyimpuritypeakisnotmorethantheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(2)(2.0%).
Assay [The method is currently under validation. Some parameters need to be amended.]
Usetheoralsuspensionimmediatelyafterpreparation.
Carry out the test as described under 1.14.4High-performanceliquidchromatography using astainlesssteelcolumn(25cm×4.6mm)packedwithparticlesofsilicagel,thesurfaceofwhichhasbeenmodifiedwithchemically-bondedoctylsilylgroups(5μm).2
Asthemobilephaseuseamixtureof10volumesofammoniumacetate(~0,40g/L)TSand90volumesofacetonitrileR.
Preparethefollowingsolutionsinthemobilephase.Forsolution(1)dissolveaquantityoftheoralsuspension,equivalenttoabout225mgofclindamycin,accuratelyweighed,anddiluteto50.0mL,filterandusethefiltrate.Forsolution(2)dissolveabout74mgclindamycinpalmitatehydrochlorideRS(containingclindamycinpalmitatehydrochlorideandimpurityA)anddiluteto10.0mL.
Operatewithaflowrateof1.0mLperminute.Asadetectoruseanultravioletspectrophotometersetatawavelengthof230nm.1 AgilentZorbaxElipseXDB-C8(4.6×250mm,5μm)hasbeenfoundsuitable.2 AgilentZorbaxElipseXDB-C8hasbeenfoundsuitable.

437
WHODrugInformationVol.30,No.3,2016 Consultation documents
Injectalternately20μLeachofsolutions(1)and(2).Theretentiontimeofclindamycinpalmitateisaboutxminutes.Theassayisnotvalidunlessinthechromatogramobtainedwithsolution(2)theresolutionbetweenthepeaksduetoclindamycinpalmitateandimpurityA(relativeretentiontimeisaboutx)isatleastx.
Measuretheareasofthepeakresponsesobtainedinthechromatogramsfromsolutions(1)and(2).DeterminetheweightpermL(1.3.1) of the oral suspension and calculate the percentagecontentofclindamycin(C18H33ClN2O5S)intheoralsuspension,usingthedeclaredcontentofclindamycinpalmitatehydrochloride(C34H63ClN2O6S.HCl)inclindamycinpalmitatehydrochlorideRS.Eachmgofclindamycinpalmitatehydrochloride(C34H63ClN2O6S.HCl)isequivalentto0.607mgclindamycin(C18H33ClN2O5S).
Impurities TheimpuritieslimitedbytherequirementsofthismonographincludeimpurityAlistedinthemonographforClindamycinpalmitatehydrochloride.
***
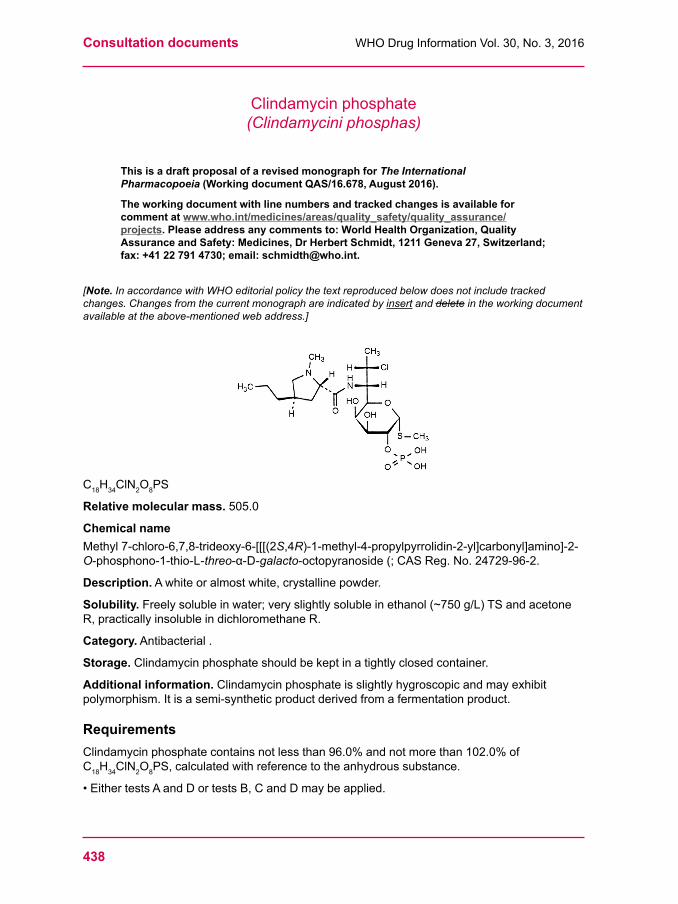
Consultation documents WHODrugInformationVol.30,No.3,2016
438
Clindamycinphosphate(Clindamycini phosphas)
This is a draft proposal of a revised monograph for The International Pharmacopoeia (Working document QAS/16.678, August 2016).
The working document with line numbers and tracked changes is available for comment at www.who.int/medicines/areas/quality_safety/quality_assurance/projects. Please address any comments to: World Health Organization, Quality Assurance and Safety: Medicines, Dr Herbert Schmidt, 1211 Geneva 27, Switzerland; fax: +41 22 791 4730; email: [email protected].
[Note. In accordance with WHO editorial policy the text reproduced below does not include tracked changes. Changes from the current monograph are indicated by insert and delete in the working document available at the above-mentioned web address.]
C18H34ClN2O8PS
Relative molecular mass.505.0
Chemical nameMethyl7-chloro-6,7,8-trideoxy-6-[[[(2S,4R)-1-methyl-4-propylpyrrolidin-2-yl]carbonyl]amino]-2-O-phosphono-1-thio-L-threo-α-D-galacto-octopyranoside(;CASReg.No.24729-96-2.
Description.Awhiteoralmostwhite,crystallinepowder.
Solubility.Freelysolubleinwater;veryslightlysolubleinethanol(~750g/L)TSandacetoneR,practicallyinsolubleindichloromethaneR.
Category. Antibacterial .
Storage.Clindamycinphosphateshouldbekeptinatightlyclosedcontainer.
Additional information.Clindamycinphosphateisslightlyhygroscopicandmayexhibitpolymorphism.Itisasemi-syntheticproductderivedfromafermentationproduct.
RequirementsClindamycinphosphatecontainsnotlessthan96.0%andnotmorethan102.0%ofC18H34ClN2O8PS,calculatedwithreferencetotheanhydroussubstance.
•EithertestsAandDortestsB,CandDmaybeapplied.
439
WHODrugInformationVol.30,No.3,2016 Consultation documents
A.Carryouttheexaminationasdescribedunder1.7Spectrophotometryintheinfraredregion.TheinfraredabsorptionspectrumisconcordantwiththespectrumobtainedfromclindamycinphosphateRSorwiththereference spectrumofclindamycinphosphate.Ifthe spectra thus obtained are not concordant repeat the test using the residues obtained. SeparatelydissolvethetestsubstanceandclindamycinphosphateRSinasmallamountofwaterRandheatuntilthesubstancesarecompletelydissolved.Evaporatetodrynessunderreducedpressureanddrytheresiduesat100–105°Cfor2hours.TheinfraredabsorptionspectrumisconcordantwiththespectrumobtainedfromclindamycinphosphateRS.
B. Carry out the test as described under 1.14.1Thin-layerchromatographyusingsilicagelR3asthecoatingsubstanceandamixtureof6volumesof1-butanolR,2volumesofwaterand2volumesofglacialaceticacidRasthemobilephase.Applyseparatelytotheplate5μLofeachof3solutionsinmethanolRcontaining(A)2.0mgofClindamycinphosphatepermL,(B)2.0mgofclindamycinphosphateRSandforsolution(C)dissolve10mgoflincomycinhydrochlorideRSin5mLofsolutionB.Afterremovingtheplatefromthechromatographicchamberallowittodryat105°Cfor30minutesandspraywithpotassiumpermanganate(1g/L)TS.Examinethechromatogramindaylight.TheprincipalspotobtainedwithsolutionAcorrespondsinposition,appearanceandintensitytothatobtainedwithsolutionB.Thetestisnotvalidunlessthechromatogramobtained with solution C shows two clearly separated spots.
C.Dissolve10mgin2mLofhydrochloricacid(~70g/L)TSandheatdirectlyinaflamefor1minute;adisagreeablesulfurousodourisperceptible.Cool,add4mLofsodiumcarbonate(75g/L)TSand0.5mLofsodiumnitroprusside(45g/L)TS;aviolet-redringisformedthatfades quickly.
D.Boil0.1gunderarefluxcondenserwithamixtureof5mLofsodiumhydroxide(~400g/L)TSand5mLofwaterfor90minutes.Coolandadd5mLofnitricacid(~1000g/L)TS.Extractwiththree15mLquantitiesofdichloromethaneRanddiscardtheextracts.Filtertheaqueouslayerthroughapaperfilter;thefiltrateyieldsreactionBdescribedunder2.1 Generalidentificationtests as characteristic of orthophosphates.
Specificopticalrotation.Usea10mg/mLsolutionandcalculatewithreferencetotheanhydroussubstance; =+115°to+130°.
Clarity and colour of solution.Dissolve1.00gincarbondioxide-freewaterR.Heatgentlyifnecessary.Coolanddiluteto25.0mLwithcarbondioxide-freewaterR.Thissolutionisclearandcolourless,whenanalysedasdescribedunder1.11.2 Degree of coloration of liquids,Method II.[Note from the Secretariat. The chapter 1.11 Colour of liquids is currently under revision. Reference is already made to the new test procedure to be added under the section 1.11.2 Degree of coloration of liquids.]
Water.Determineasdescribedunder2.8DeterminationofwaterbytheKarlFischermethod,methodA,using0.2gofthesubstance;thewatercontentisnotmorethan0.050g/g.
pH value.pHofa10mg/mLsolutionincarbon-dioxide-freewaterR,3.5–4.5.
Related substances. Carry out the test as described under 1.14.4High-performanceliquidchromatographyusingastainlesssteelcolumn(15cm×4.6mm)packedwithend-cappedparticlesofsilicagel,thesurfaceofwhichhasbeenmodifiedwithchemically-bondedoctadecylsilylgroups(5µm).1
1 ASymmetryC18columnwasfoundsuitable.
Consultation documents WHODrugInformationVol.30,No.3,2016
440
Usethefollowingconditionsforgradientelution:mobilephaseA:21volumesofacetonitrileforchromatographyRand79volumesofphosphatebufferpH6.0;mobilephaseB:60volumesofacetonitrileforchromatographyRand40volumesofphosphatebufferpH6.0.
PreparethephosphatebufferpH6.0bydissolving13.6gofpotassiumdihydrogenphosphateRin750mLofwaterR,adjustthepHto6.0withpotassiumhydroxide(~450g/L)TSanddiluteto1000mLwithwaterR.Time(min)
Mobile phase A(%v/v)
Mobile phase B(%v/v) Comments
0–13 100 0 Isocratic13–18 100to50 0to50 Linear gradient18–39 50 50 Isocratic39–40 50to100 50to0 Returntoinitialcomposition40–55 100 0 Re-equilibration
Operatewithaflowrateof1.1mLperminute.Asadetectoruseanultravioletspectrophotometersetatawavelengthof210nm.Maintainthecolumntemperatureat30°C.PreparethefollowingsolutionsinmobilephaseA.Forsolution(1)dissolveabout30mgofthetestsubstanceanddiluteto10mL.Forsolution(2)dilute1.0mLofsolution(1)to200.0mL.Forsolution(3)dilute2.0mLofsolution(2)to10.0mL.Forsolution(4)dissolve3.0mgofclindamycinphosphateforsystemsuitabilityRS(containingclindamycinphosphateandtheimpuritiesB,E,F,G,I,J,KandL)anddiluteto1.0mL.Inject20μLofsolution(4).Usethechromatogramobtainedwithsolution(4)andthechromatogramsuppliedwithclindamycinphosphateforsystemsuitabilityRStoidentifythepeaksduetotheimpuritiesB,E,F,G,I,J,KandL.Theimpuritiesareelutedatthefollowingrelativeretentionwithreferencetoclindamycinphosphate(retentiontimeabout12minutes):impurityFabout0.15;impurityGabout0.19;impurityIabout0.34;impurityBabout0.45;impurityLabout0.64;impurityJabout1.20;impurityEabout1.73;andimpurityKabout1.90.ThetestisnotvalidunlesstheresolutionbetweenthepeaksduetoimpurityFandthepeakduetoimpurityGisatleast2.0.Injectalternately20μLeachofsolution(1),(2)and(3).Inthechromatogramobtainedwithsolution(1):• theareaofanypeakcorrespondingtoeitherimpurityBorLisnotgreaterthan2timestheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(2)(1.0%);
• theareaofanypeakcorrespondingtoeitherimpurityEorFisnotgreaterthantheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(2)(0.5%);
• theareaofanypeakcorrespondingtoeitherimpurityG,I,JorKisnotgreaterthan5timestheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(3)(0.5%);
• theareaofanyotherimpuritypeakisnotgreaterthantheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(3)(0.10%);
• thesumoftheareasofallimpuritiesisnotgreaterthan4timestheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(2)(2.0%).Disregardanypeakwithanarealess
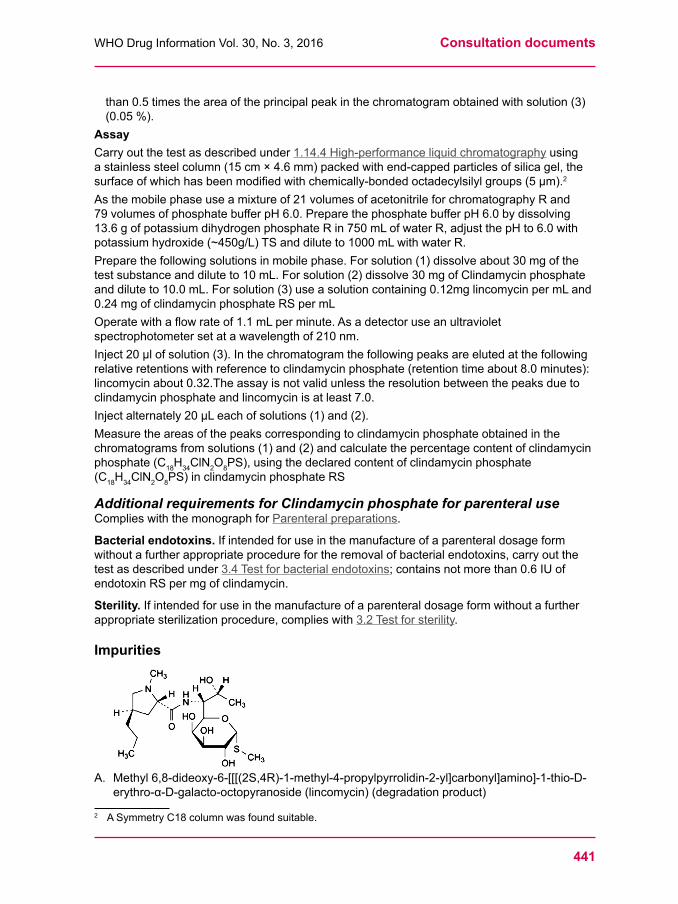
441
WHODrugInformationVol.30,No.3,2016 Consultation documents
than0.5timestheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(3)(0.05%).
AssayCarry out the test as described under 1.14.4High-performanceliquidchromatography using astainlesssteelcolumn(15cm×4.6mm)packedwithend-cappedparticlesofsilicagel,thesurfaceofwhichhasbeenmodifiedwithchemically-bondedoctadecylsilylgroups(5µm).2
Asthemobilephaseuseamixtureof21volumesofacetonitrileforchromatographyRand79volumesofphosphatebufferpH6.0.PreparethephosphatebufferpH6.0bydissolving13.6gofpotassiumdihydrogenphosphateRin750mLofwaterR,adjustthepHto6.0withpotassiumhydroxide(~450g/L)TSanddiluteto1000mLwithwaterR.Preparethefollowingsolutionsinmobilephase.Forsolution(1)dissolveabout30mgofthetestsubstanceanddiluteto10mL.Forsolution(2)dissolve30mgofClindamycinphosphateanddiluteto10.0mL.Forsolution(3)useasolutioncontaining0.12mglincomycinpermLand0.24mgofclindamycinphosphateRSpermLOperatewithaflowrateof1.1mLperminute.Asadetectoruseanultravioletspectrophotometersetatawavelengthof210nm.Inject20μlofsolution(3).Inthechromatogramthefollowingpeaksareelutedatthefollowingrelativeretentionswithreferencetoclindamycinphosphate(retentiontimeabout8.0minutes):lincomycinabout0.32.Theassayisnotvalidunlesstheresolutionbetweenthepeaksduetoclindamycinphosphateandlincomycinisatleast7.0.Injectalternately20μLeachofsolutions(1)and(2).Measuretheareasofthepeakscorrespondingtoclindamycinphosphateobtainedinthechromatogramsfromsolutions(1)and(2)andcalculatethepercentagecontentofclindamycinphosphate (C18H34ClN2O8PS),usingthedeclaredcontentofclindamycinphosphate(C18H34ClN2O8PS)inclindamycinphosphateRS
Additional requirements for Clindamycin phosphate for parenteral useComplieswiththemonographforParenteral preparations.
Bacterial endotoxins.Ifintendedforuseinthemanufactureofaparenteraldosageformwithoutafurtherappropriateprocedurefortheremovalofbacterialendotoxins,carryoutthetest as described under 3.4Testforbacterialendotoxins;containsnotmorethan0.6IUofendotoxinRSpermgofclindamycin.
Sterility.Ifintendedforuseinthemanufactureofaparenteraldosageformwithoutafurtherappropriatesterilizationprocedure,complieswith3.2Testforsterility.
Impurities
A.Methyl6,8-dideoxy-6-[[[(2S,4R)-1-methyl-4-propylpyrrolidin-2-yl]carbonyl]amino]-1-thio-D-erythro-α-D-galacto-octopyranoside(lincomycin)(degradationproduct)
2 ASymmetryC18columnwasfoundsuitable.
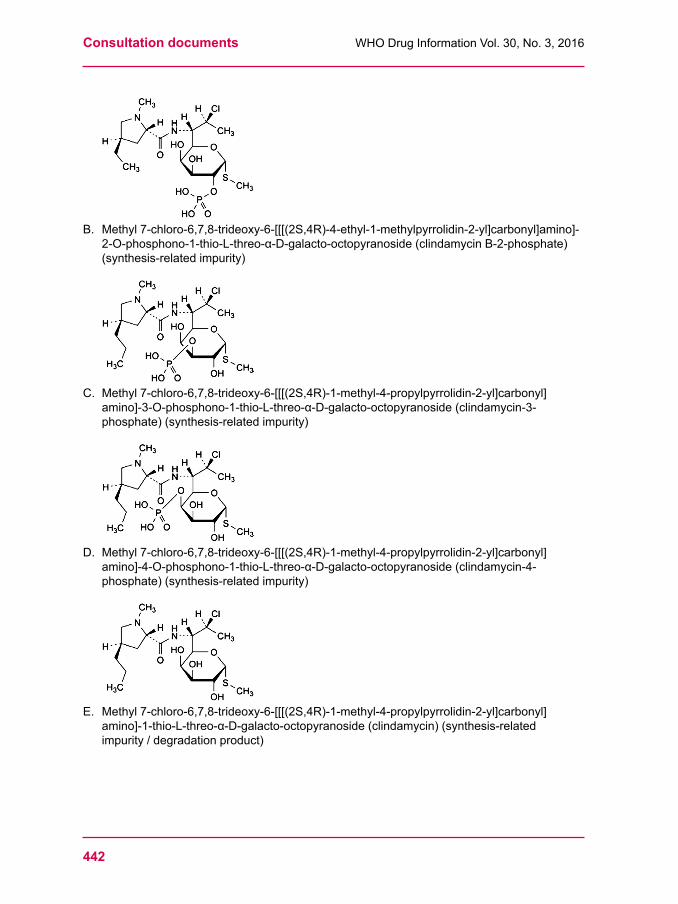
Consultation documents WHODrugInformationVol.30,No.3,2016
442
B.Methyl7-chloro-6,7,8-trideoxy-6-[[[(2S,4R)-4-ethyl-1-methylpyrrolidin-2-yl]carbonyl]amino]-2-O-phosphono-1-thio-L-threo-α-D-galacto-octopyranoside(clindamycinB-2-phosphate)(synthesis-relatedimpurity)
C.Methyl7-chloro-6,7,8-trideoxy-6-[[[(2S,4R)-1-methyl-4-propylpyrrolidin-2-yl]carbonyl]amino]-3-O-phosphono-1-thio-L-threo-α-D-galacto-octopyranoside(clindamycin-3-phosphate)(synthesis-relatedimpurity)
D.Methyl7-chloro-6,7,8-trideoxy-6-[[[(2S,4R)-1-methyl-4-propylpyrrolidin-2-yl]carbonyl]amino]-4-O-phosphono-1-thio-L-threo-α-D-galacto-octopyranoside(clindamycin-4-phosphate)(synthesis-relatedimpurity)
E.Methyl7-chloro-6,7,8-trideoxy-6-[[[(2S,4R)-1-methyl-4-propylpyrrolidin-2-yl]carbonyl]amino]-1-thio-L-threo-α-D-galacto-octopyranoside(clindamycin)(synthesis-relatedimpurity/degradationproduct)
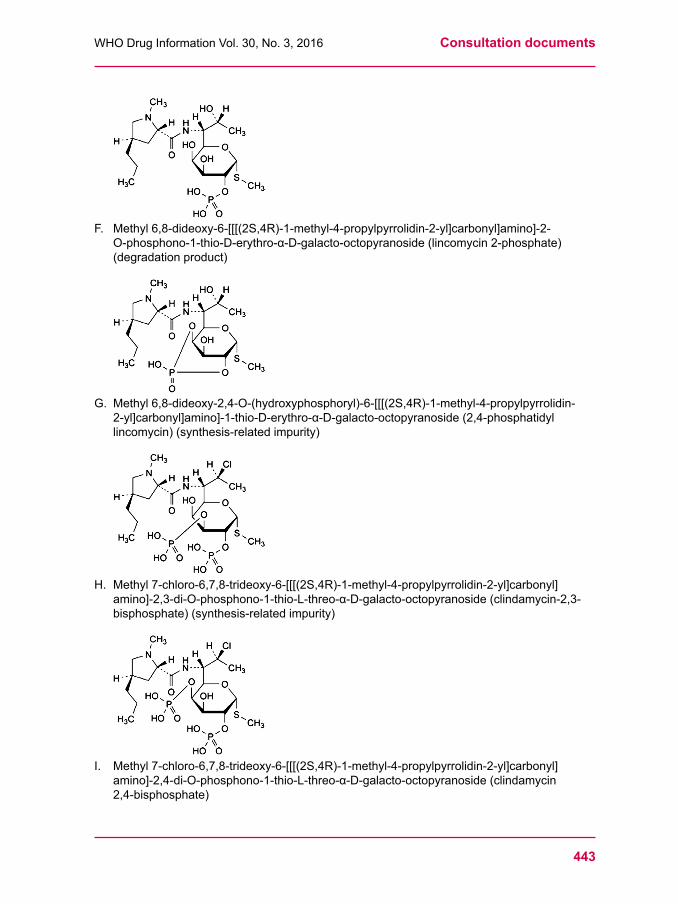
443
WHODrugInformationVol.30,No.3,2016 Consultation documents
F. Methyl6,8-dideoxy-6-[[[(2S,4R)-1-methyl-4-propylpyrrolidin-2-yl]carbonyl]amino]-2-O-phosphono-1-thio-D-erythro-α-D-galacto-octopyranoside(lincomycin2-phosphate)(degradation product)
G.Methyl6,8-dideoxy-2,4-O-(hydroxyphosphoryl)-6-[[[(2S,4R)-1-methyl-4-propylpyrrolidin-2-yl]carbonyl]amino]-1-thio-D-erythro-α-D-galacto-octopyranoside(2,4-phosphatidyllincomycin)(synthesis-relatedimpurity)
H.Methyl7-chloro-6,7,8-trideoxy-6-[[[(2S,4R)-1-methyl-4-propylpyrrolidin-2-yl]carbonyl]amino]-2,3-di-O-phosphono-1-thio-L-threo-α-D-galacto-octopyranoside(clindamycin-2,3-bisphosphate)(synthesis-relatedimpurity)
I. Methyl7-chloro-6,7,8-trideoxy-6-[[[(2S,4R)-1-methyl-4-propylpyrrolidin-2-yl]carbonyl]amino]-2,4-di-O-phosphono-1-thio-L-threo-α-D-galacto-octopyranoside(clindamycin2,4-bisphosphate)
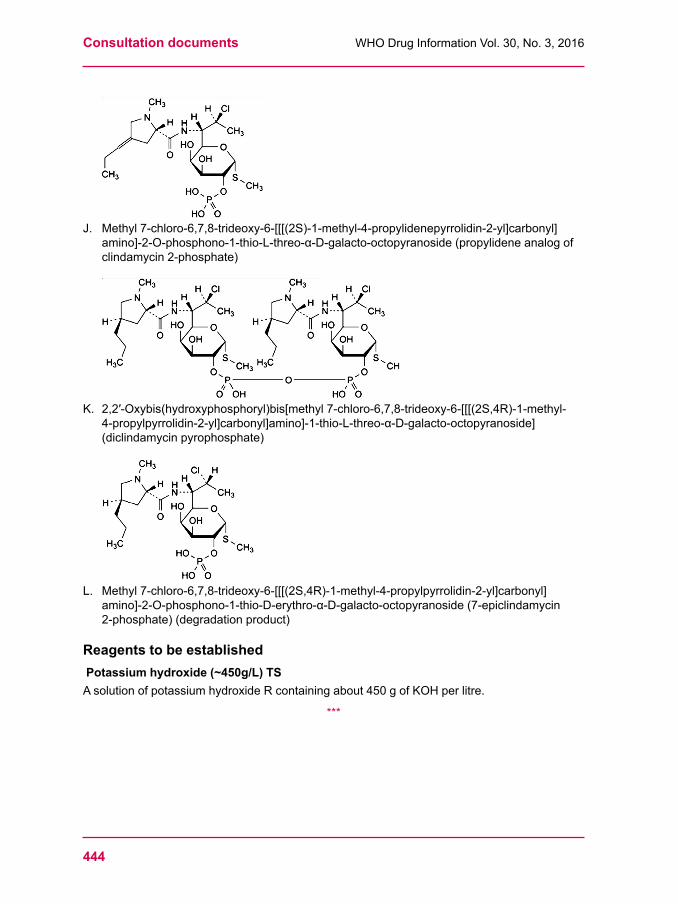
Consultation documents WHODrugInformationVol.30,No.3,2016
444
J. Methyl7-chloro-6,7,8-trideoxy-6-[[[(2S)-1-methyl-4-propylidenepyrrolidin-2-yl]carbonyl]amino]-2-O-phosphono-1-thio-L-threo-α-D-galacto-octopyranoside(propylideneanalogofclindamycin2-phosphate)
K.2,2′-Oxybis(hydroxyphosphoryl)bis[methyl7-chloro-6,7,8-trideoxy-6-[[[(2S,4R)-1-methyl-4-propylpyrrolidin-2-yl]carbonyl]amino]-1-thio-L-threo-α-D-galacto-octopyranoside](diclindamycinpyrophosphate)
L. Methyl7-chloro-6,7,8-trideoxy-6-[[[(2S,4R)-1-methyl-4-propylpyrrolidin-2-yl]carbonyl]amino]-2-O-phosphono-1-thio-D-erythro-α-D-galacto-octopyranoside(7-epiclindamycin2-phosphate) (degradation product)
Reagents to be established Potassium hydroxide (~450g/L) TSAsolutionofpotassiumhydroxideRcontainingabout450gofKOHperlitre.
***
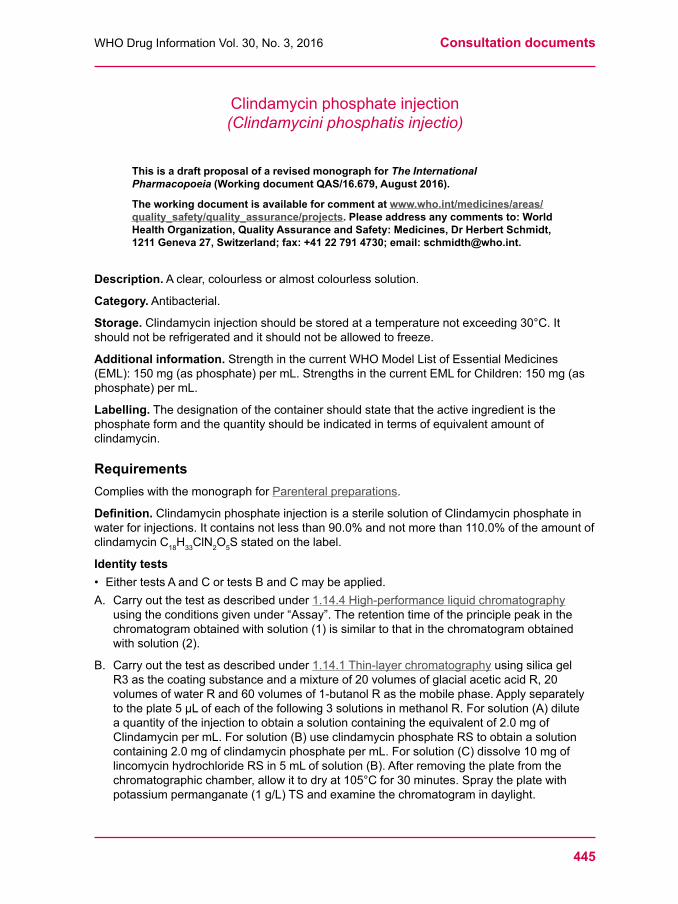
445
WHODrugInformationVol.30,No.3,2016 Consultation documents
Clindamycinphosphateinjection(Clindamycini phosphatis injectio)
This is a draft proposal of a revised monograph for The International Pharmacopoeia (Working document QAS/16.679, August 2016).
The working document is available for comment at www.who.int/medicines/areas/quality_safety/quality_assurance/projects. Please address any comments to: World Health Organization, Quality Assurance and Safety: Medicines, Dr Herbert Schmidt, 1211 Geneva 27, Switzerland; fax: +41 22 791 4730; email: [email protected].
Description.Aclear,colourlessoralmostcolourlesssolution.
Category. Antibacterial.
Storage.Clindamycininjectionshouldbestoredatatemperaturenotexceeding30°C.Itshould not be refrigerated and it should not be allowed to freeze.
Additional information.StrengthinthecurrentWHOModelListofEssentialMedicines(EML):150mg(asphosphate)permL.StrengthsinthecurrentEMLforChildren:150mg(asphosphate)permL.
Labelling.Thedesignationofthecontainershouldstatethattheactiveingredientisthephosphateformandthequantityshouldbeindicatedintermsofequivalentamountofclindamycin.
RequirementsComplieswiththemonographforParenteral preparations.
Definition.ClindamycinphosphateinjectionisasterilesolutionofClindamycinphosphateinwaterforinjections.Itcontainsnotlessthan90.0%andnotmorethan110.0%oftheamountofclindamycinC18H33ClN2O5Sstatedonthelabel.
Identity tests• EithertestsAandCortestsBandCmaybeapplied.A. Carry out the test as described under 1.14.4High-performanceliquidchromatography
usingtheconditionsgivenunder“Assay”.Theretentiontimeoftheprinciplepeakinthechromatogramobtainedwithsolution(1)issimilartothatinthechromatogramobtainedwith solution (2).
B. Carry out the test as described under 1.14.1Thin-layerchromatography using silica gel R3asthecoatingsubstanceandamixtureof20volumesofglacialaceticacidR,20volumesofwaterRand60volumesof1-butanolRasthemobilephase.Applyseparatelytotheplate5μLofeachofthefollowing3solutionsinmethanolR.Forsolution(A)diluteaquantityoftheinjectiontoobtainasolutioncontainingtheequivalentof2.0mgofClindamycinpermL.Forsolution(B)useclindamycinphosphateRStoobtainasolutioncontaining2.0mgofclindamycinphosphatepermL.Forsolution(C)dissolve10mgoflincomycinhydrochlorideRSin5mLofsolution(B).Afterremovingtheplatefromthechromatographicchamber,allowittodryat105°Cfor30minutes.Spraytheplatewithpotassiumpermanganate(1g/L)TSandexaminethechromatogramindaylight.
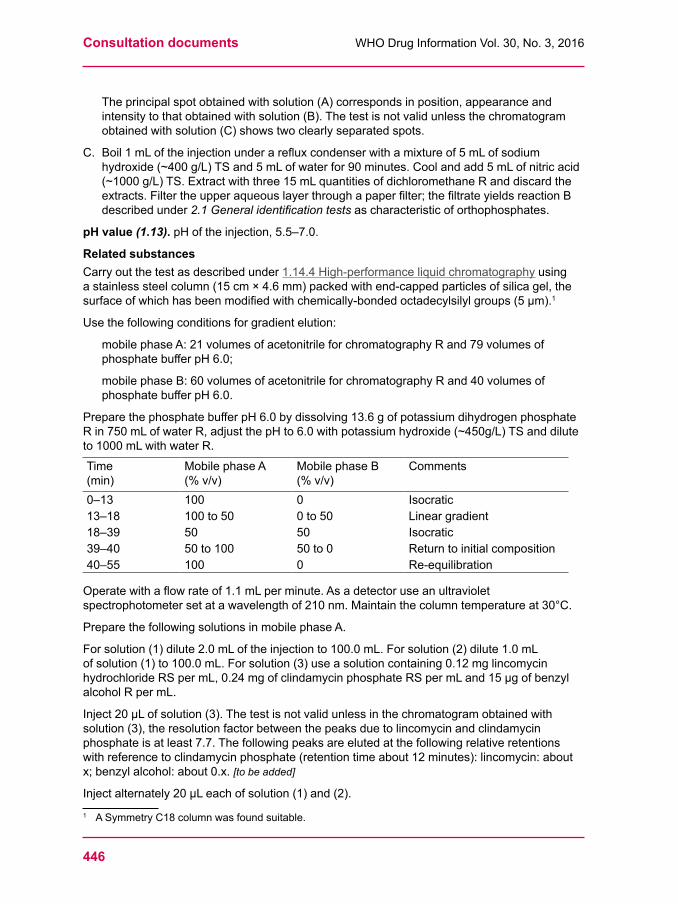
Consultation documents WHODrugInformationVol.30,No.3,2016
446
Theprincipalspotobtainedwithsolution(A)correspondsinposition,appearanceandintensitytothatobtainedwithsolution(B).Thetestisnotvalidunlessthechromatogramobtained with solution (C) shows two clearly separated spots.
C.Boil1mLoftheinjectionunderarefluxcondenserwithamixtureof5mLofsodiumhydroxide(~400g/L)TSand5mLofwaterfor90minutes.Coolandadd5mLofnitricacid(~1000g/L)TS.Extractwiththree15mLquantitiesofdichloromethaneRanddiscardtheextracts.Filtertheupperaqueouslayerthroughapaperfilter;thefiltrateyieldsreactionBdescribed under 2.1 General identification tests as characteristic of orthophosphates.
pH value (1.13).pHoftheinjection,5.5–7.0.
Related substancesCarry out the test as described under 1.14.4High-performanceliquidchromatography using astainlesssteelcolumn(15cm×4.6mm)packedwithend-cappedparticlesofsilicagel,thesurfaceofwhichhasbeenmodifiedwithchemically-bondedoctadecylsilylgroups(5µm).1
Usethefollowingconditionsforgradientelution:
mobilephaseA:21volumesofacetonitrileforchromatographyRand79volumesofphosphatebufferpH6.0;
mobilephaseB:60volumesofacetonitrileforchromatographyRand40volumesofphosphatebufferpH6.0.
PreparethephosphatebufferpH6.0bydissolving13.6gofpotassiumdihydrogenphosphateRin750mLofwaterR,adjustthepHto6.0withpotassiumhydroxide(~450g/L)TSanddiluteto1000mLwithwaterR.Time(min)
Mobile phase A(%v/v)
Mobile phase B(%v/v)
Comments
0–13 100 0 Isocratic13–18 100to50 0to50 Linear gradient18–39 50 50 Isocratic39–40 50to100 50to0 Returntoinitialcomposition40–55 100 0 Re-equilibration
Operatewithaflowrateof1.1mLperminute.Asadetectoruseanultravioletspectrophotometersetatawavelengthof210nm.Maintainthecolumntemperatureat30°C.
PreparethefollowingsolutionsinmobilephaseA.
Forsolution(1)dilute2.0mLoftheinjectionto100.0mL.Forsolution(2)dilute1.0mLofsolution(1)to100.0mL.Forsolution(3)useasolutioncontaining0.12mglincomycinhydrochlorideRSpermL,0.24mgofclindamycinphosphateRSpermLand15µgofbenzylalcoholRpermL.
Inject20μLofsolution(3).Thetestisnotvalidunlessinthechromatogramobtainedwithsolution(3),theresolutionfactorbetweenthepeaksduetolincomycinandclindamycinphosphateisatleast7.7.Thefollowingpeaksareelutedatthefollowingrelativeretentionswithreferencetoclindamycinphosphate(retentiontimeabout12minutes):lincomycin:aboutx;benzylalcohol:about0.x.[to be added]
Injectalternately20μLeachofsolution(1)and(2).1 ASymmetryC18columnwasfoundsuitable.
447
WHODrugInformationVol.30,No.3,2016 Consultation documents
Inthechromatogramobtainedwithsolution(1):
• theareaofanyimpuritypeakisnotgreaterthan3timestheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(3)(3.0%);
• thesumoftheareasofallimpuritiesisnotgreaterthan8timestheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(2)(8.0%).Disregardanypeakduetobenzylalcohol,ifpresent,andanypeakwithanarealessthan0.1timestheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(2)(0.1%).
AssayCarry out the test as described under 1.14.4High-performanceliquidchromatography using astainlesssteelcolumn(15cm×4.6mm)packedwithend-cappedparticlesofsilicagel,thesurfaceofwhichhasbeenmodifiedwithchemically-bondedoctadecylsilylgroups(5µm).2
Asthemobilephaseuseamixtureof21volumesofacetonitrileforchromatographyRand79volumesofphosphatebufferpH6.0.PreparethephosphatebufferpH6.0bydissolving13.6gofpotassiumdihydrogenphosphateRin750mLofwaterR,adjustthepHto6.0withpotassiumhydroxide(~450g/L)TSanddiluteto1000mLwithwaterR.
Preparethefollowingsolutionsinmobilephase.Forsolution(1)dilute1.0mLoftheinjectionto100.0mL.Forsolution(2)dissolve36mgofclindamycinphosphateRSanddiluteto20.0mL.Forsolution(3)useasolutioncontaining0.12mglincomycinpermL,0.24mgofclindamycinphosphateRSpermLand15µgofbenzylalcoholRpermL.
Operatewithaflowrateof1.1mLperminute.Asadetectoruseanultravioletspectrophotometersetatawavelengthof210nm.
Inject20μlofsolution(3).Inthechromatogramthefollowingpeaksareelutedatthefollowingrelativeretentionswithreferencetoclindamycinphosphate(retentiontimeabout8.0minutes):benzylalcoholabout0.6.Theassayisnotvalidunlesstheresolutionbetweenthepeaksduetoclindamycinphosphateandbenzylalcoholisatleast3.0andtheresolutionbetweenthepeaksduetoclindamycinphosphateandlincomycinisatleast7.0.
Injectalternately20μLeachofsolutions(1)and(2).Measuretheareasofthepeakscorrespondingtoclindamycinphosphateobtainedinthechromatogramsfromsolutions(1)and(2)andcalculatethepercentagecontentofclindamycin(C18H33ClN2O5S)intheinjectionusingthe declared content of C18H34ClN2O8PSinclindamycinphosphateRS.Eachmgofclindamycinphosphate (C18H34ClN2O8PS)isequivalentto0.8416mgofclindamycin(C18H33ClN2O5S).
Bacterial endotoxins. Carry out the test as described under 3.4Testforbacterialendotoxins;containsnotmorethan0.10IUofendotoxinRSpermgofclindamycin.
ImpuritiesTheimpuritieslimitedbytherequirementsofthismonographincludethoselistedinthemonographonClindamycinphosphate.
***
2 ASymmetryC18columnwasfoundsuitable.
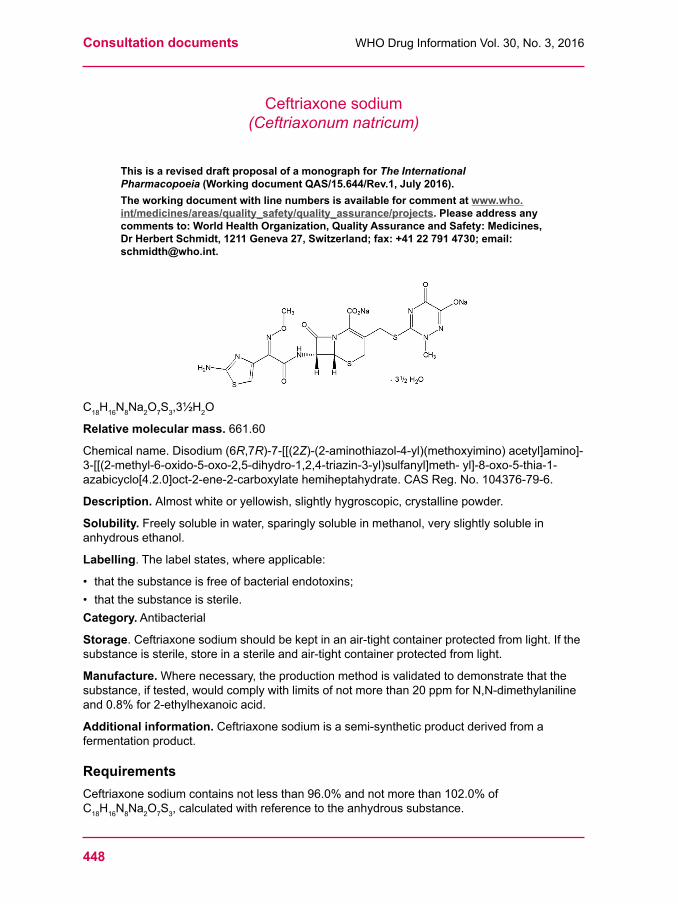
Consultation documents WHODrugInformationVol.30,No.3,2016
448
Ceftriaxonesodium(Ceftriaxonum natricum)
This is a revised draft proposal of a monograph for The International Pharmacopoeia (Working document QAS/15.644/Rev.1, July 2016). The working document with line numbers is available for comment at www.who.int/medicines/areas/quality_safety/quality_assurance/projects. Please address any comments to: World Health Organization, Quality Assurance and Safety: Medicines, Dr Herbert Schmidt, 1211 Geneva 27, Switzerland; fax: +41 22 791 4730; email: [email protected].
C18H16N8Na2O7S3,3½H2O
Relative molecular mass. 661.60
Chemicalname.Disodium(6R,7R)-7-[[(2Z)-(2-aminothiazol-4-yl)(methoxyimino)acetyl]amino]-3-[[(2-methyl-6-oxido-5-oxo-2,5-dihydro-1,2,4-triazin-3-yl)sulfanyl]meth-yl]-8-oxo-5-thia-1-azabicyclo[4.2.0]oct-2-ene-2-carboxylatehemiheptahydrate.CASReg.No.104376-79-6.
Description. Almostwhiteoryellowish,slightlyhygroscopic,crystallinepowder.
Solubility.Freelysolubleinwater,sparinglysolubleinmethanol,veryslightlysolubleinanhydrous ethanol.
Labelling.Thelabelstates,whereapplicable:
• thatthesubstanceisfreeofbacterialendotoxins;• that the substance is sterile.Category. Antibacterial
Storage.Ceftriaxonesodiumshouldbekeptinanair-tightcontainerprotectedfromlight.Ifthesubstanceissterile,storeinasterileandair-tightcontainerprotectedfromlight.
Manufacture. Wherenecessary,theproductionmethodisvalidatedtodemonstratethatthesubstance,iftested,wouldcomplywithlimitsofnotmorethan20ppmforN,N-dimethylanilineand0.8%for2-ethylhexanoicacid.
Additional information.Ceftriaxonesodiumisasemi-syntheticproductderivedfromafermentationproduct.
RequirementsCeftriaxonesodiumcontainsnotlessthan96.0%andnotmorethan102.0%ofC18H16N8Na2O7S3,calculatedwithreferencetotheanhydroussubstance.
449
WHODrugInformationVol.30,No.3,2016 Consultation documents
Identity tests• EithertestsAandCortestsBandCmaybeapplied.A.Carryouttheexaminationasdescribedunder1.7Spectrophotometryintheinfrared
region.TheinfraredabsorptionspectrumisconcordantwiththespectrumobtainedfromceftriaxonesodiumRSorwiththereferencespectrumofceftriaxonesodium.
B. Carry out the test as described under 1.14.4High-performanceliquidchromatography usingtheconditionsgivenundertheAssay.Theretentiontimeoftheprincipalpeakinthechromatogramobtainedwithsolution(1)correspondstotheretentiontimeofthepeakcorrespondingtoceftriaxoneinthechromatogramobtainedwithsolution(2).
C. Whentestedforsodiumasdescribedunder2.1Generalidentificationtests,yieldsthecharacteristic reaction.
Specificopticalrotation(1.4).Dissolve0.250ginwaterRanddiluteto25.0mLwiththesamesolvent.Calculatewithreferencetotheanhydroussubstance; =–155⁰to–170⁰.
Clarity and colour of solution.Dissolve2.40gincarbon-dioxide-freewaterRanddiluteto20.0mLwiththesamesolvent(SolutionA).Dilute2mLofSolutionAto20mLcarbon-dioxide-freewaterR.ThesolutionisclearandnotmoreintenselycolouredthanreferencesolutionY5 or BY5whencomparedasdescribedunder1.11.2 Degree of coloration of liquids.(Keeptheremainingsolution(SolutionA)forthe“pHvalue”.)[Note from the Secretariat. The chapter 1.11 Colour of liquids is currently under revision. Reference is already made to a new test procedure to be added under the section 1.11.2 Degree of colouration of liquids.]
pH value (1.13). pHofthesolutionpreparedforthe“Clarityandcolourofsolution”(SolutionA),6.0to8.0.
Water. Determineasdescribedunder2.8DeterminationofwaterbytheKarlFischermethod,methodA,using0.100gofthetestsubstance.Thewatercontentisnotlessthan80mgpergandnotmorethan110mgperg.
Bacterial endotoxins. Ifintendedforuseinthemanufactureofaparenteraldosageformwithoutafurtherappropriateprocedurefortheremovalofbacterialendotoxins,carryoutthetest as described under 3.4Testforbacterialendotoxins;containsnotmorethan0.20IUofendotoxinpermgofceftriaxonesodium.
Related substancesCarry out the test as described under 1.14.4High-performanceliquidchromatography using theconditionsgivenbelowunderassaymethod.
Preparethefollowingsolutionsinmobilephase:forsolution(1)dissolveabout30mgofthetestsubstanceanddiluteto100.0mL.Forsolution(2)dilute1volumeofsolution(1)to100volumes.Forsolution(3)dissolveabout5mgceftriaxonesodiumRSand5mgofceftriaxoneimpurityAto100.0mL.
Inject20µLofsolution(3).ThetestisnotvalidunlesstheresolutionfactorbetweenthepeaksduetoceftriaxoneandceftriaxoneimpurityAisatleast3.0.CeftriaxoneimpurityAiselutedatarelativeretentionofabout1.4withreferencetoceftriaxone(retentiontimeabout9min).
Injectalternately20µLeachofsolution(1)and(2).Recordthechromatogramsforabout2timestheretentiontimeofceftriaxone.
Consultation documents WHODrugInformationVol.30,No.3,2016
450
Inthechromatogramobtainedwithsolution(1):
• theareaofanypeak,otherthantheprincipalpeak,isnotgreaterthantheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(2)(1.0%);
• thesumoftheareasofallpeaks,otherthantheprincipalpeak,isnotgreaterthan2.5timestheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(2)(2.5%).Disregardanypeakwithanarealessthan0.1timestheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(2)(0.1%).
AssayCarry out the test as described under 1.14.4High-performanceliquidchromatography using a stainlesssteelcolumn(25cmx4.6mm)packedwithparticlesofbase-deactivatedsilicagel,thesurfaceofwhichhasbeenmodifiedwithchemically-bondedoctadecylsilylgroups(5µm)1.
Asthemobilephaseuseasolutionpreparedasfollows:dissolve2.0goftetradecylammoniumbromideRand2.0goftetraheptylammoniumbromideRinamixtureof440mLofwaterR,55mLofphosphatebufferpH7.0(0.067mol/L)TS,5.0mLofcitratebufferpH5.0TSand500mLofacetonitrileRandfilter.
Preparethefollowingsolutionsinmobilephase.Forsolution(1)dissolve30mgofthetestsubstance,accuratelyweighedanddiluteto100.0mL.Forsolution(2)dissolveabout30mgofceftriaxonesodiumRS,accuratelyweighedanddiluteto100.0mL.Forsolution(3)dissolveabout5mgceftriaxonesodiumRSandabout5mgofceftriaxoneimpurityAanddiluteto100.0mL.
Operatewithaflowrateof1.5mLperminute.Asadetectoruseanultravioletspectrophotometersetatawavelengthof254nm.
Inject20µLofsolution(3).ThetestisnotvalidunlesstheresolutionfactorbetweenthepeaksduetoceftriaxoneandceftriaxoneimpurityAisatleast3.0.
Injectalternately20µLeachofsolution(1)and(2).Measuretheareasofthepeakscorresponding to ceftriaxone and calculate the percentage content of C18H16N8Na2O7S3,usingthe declared content of C18H16N8Na2O7S3inceftriaxonesodiumRS.
Sterility.Ifintendedforuseinthemanufactureofaparenteraldosageformwithoutafurtherappropriatesterilizationprocedure,complieswith3.2Testforsterility.
Impurities[Note from the Secretariat. The structures of the impurities will be added at a later stage.]
A. (6R,7R)-7-[(E)-2-(2-Aminothiazol-4-yl)-2-(methoxyimino)acetamido]-3-{[(6-hydroxy-2-methyl-5-oxo-2,5-dihydro-1,2,4-triazin-3-yl)thio]methyl}-8-oxo-5-thia-1-azabicyclo[4.2.0]oct-2-ene-2-carboxylicacid(CeftriaxoneE-isomer)
B. (Z)-2-(2-Aminothiazol-4-yl)-N-{(5aR,6R)-1,7-dioxo-1,3,4,5a,6,7-hexahydroazeto[2,1-b]furo[3,4-d][1,3]thiazin-6-yl}-2-(methoxyimino)acetamide.(Deacetylcefotaximelactone)
C. (6R,7R)-7-Amino-3-{[(6-hydroxy-2-methyl-5-oxo-2,5-dihydro-1,2,4-triazin-3-yl)thio]methyl}-8-oxo-5-thia-1-azabicyclo[4.2.0]oct-2-ene-2-carboxylicacid(Deacylceftriaxone)
D. (Z)-S-Benzothiazol-2-yl2-(2-aminothiazol-4-yl)-2-(methoxyimino)thioacetate(Ceftriaxonebenzothiazolyloxime)
1 HypersilBDSC18hasbeenfoundsuitable.
451
WHODrugInformationVol.30,No.3,2016 Consultation documents
E.(6R,7R)-3-(Acetoxymethyl)-7-amino-8-oxo-5-thia-1-azabicyclo[4.2.0]oct-2-ene-2-carboxylicacid.(7-Aminocephalosporanicacid)
F.3-Mercapto-2-methyl-1,2-dihydro-1,2,4-triazine-5,6-dione.(Ceftriaxonetriazineanalog)
G.(6R,7R)-7-[(Z)-2-(2-Aminothiazol-4-yl)-2-(methoxyimino)acetamido]-3-{[(6-hydroxy-2-methyl-5-oxo-2,5-dihydro-1,2,4-triazin-3-yl)thio]methyl}-8-oxo-5-thia-1-azabicyclo[4.2.0]oct-3-ene-2-carboxylicacid(Ceftriaxone3-eneisomer).
Reagents to be included Citratebuffer,pH5TSProcedure.Dissolve20.17gofcitricacidRin800mlofwaterR,adjusttopH5.0withsodiumhydroxide(~400g/L)TSanddiluteto1000mLwithwaterR.
Tetradecylammonium bromide R C40H84BrN.Chromatographicreagentgradeofcommerce.
Description.Whitetoalmostwhitecrystals,oracrystallinepowder.
Melting point.88-89°C.
Tetraheptylammonium bromide R C28H60BrN.Chromatographicreagentgradeofcommerce.
Description.White,flakypowder.
Melting range.Between89-91°C.
***
Consultation documents WHODrugInformationVol.30,No.3,2016
452
Ceftriaxoneforinjection(Ceftriaxoni ad injectionem)
This is a revised draft proposal of a monograph for The International Pharmacopoeia (Working document QAS/15.645/Rev.1, July 2016). The working document with line numbers is available for comment at www.who.int/medicines/areas/quality_safety/quality_assurance/projects. Please address any comments to: World Health Organization, Quality Assurance and Safety: Medicines, Dr Herbert Schmidt, 1211 Geneva 27, Switzerland; fax: +41 22 791 4730; email: [email protected].
Description. Awhitetoalmostwhitepowder.
Category. Antibacterial.
Storage.Ceftriaxoneforinjectionshouldbestoredinatightlyclosedcontainer.Thereconstitutedsolutionshouldbeusedimmediatelyafterpreparation.
Labelling.Thedesignationonthecontainerofceftriaxoneforinjectionshouldstatethattheactiveingredientisceftriaxonesodiumandthequantityshouldbeindicatedintermsofequivalentamountofceftriaxone.
Additional information. StrengthsinthecurrentWHOModelListofEssentialMedicines(EML):250mg,1g(assodiumsalt)invial.StrengthinthecurrentWHOEMLforchildren:250mg,1g(assodiumsalt)invial.
TheinjectionisreconstitutedbydilutionofCeftriaxoneforinjectioninWaterforinjections.
RequirementsThepowderforinjectionandthereconstitutedsolutionforinjectioncomplywiththemonographon Parenteral preparations.
Definition.CeftriaxoneforinjectionisasterilepowdercontainingCeftriaxonesodiumwithorwithout excipients.
CeftriaxoneforInjectioncontainsnotlessthan90.0%andnotmorethan110.0%ofthelabelledamountofceftriaxone(C18H18N8O7S3).
Identity tests• EithertestsAandCortestsBandCmaybeapplied.A.Carryouttheexaminationasdescribedunder1.7Spectrophotometryintheinfrared
region.TheinfraredabsorptionspectrumisconcordantwiththespectrumobtainedfromceftriaxonesodiumRSorwiththereferencespectrumofceftriaxonesodium.
B. Carry out the test as described under 1.14.4High-performanceliquidchromatography usingtheconditionsgivenunder“Assay”.Theretentiontimeoftheprincipalpeakinthechromatogramobtainedwithsolution(1)correspondstotheretentiontimeoftheceftriaxonepeakinthechromatogramobtainedwithsolution(2).
C. Whentestedforsodiumasdescribedunder2.1Generalidentificationtests,yieldsthecharacteristic reaction.
453
WHODrugInformationVol.30,No.3,2016 Consultation documents
Water. Determineasdescribedunder2.8DeterminationofwaterbytheKarlFischermethod,methodA,usingabout0.100gofthepowder.Thewatercontentisnotmorethan110mgper g.
Clarity and colour of solution. Dissolve2.40gincarbon-dioxide-freewaterRanddiluteto20.0mLwiththesamesolvent(SolutionA).Dilute2mLofSolutionAto20mLcarbon-dioxide-freewaterR.ThesolutionisclearandnotmoreintenselycolouredthanreferencesolutionYW2whencomparedasdescribedunder1.11 Colour of liquids.(Keeptheremainingsolution(SolutionA)forthe“pHvalue”.)
pH value (1.13). pHofthesolutionpreparedforthe“Clarityandcolourofsolution”(SolutionA),6.0to8.0.
Bacterial endotoxins. Carry out the test described under 3.4Testforbacterialendotoxins,containsnotmorethan0.20IUofendotoxinpermgofceftriaxone.
Related substancesCarry out the test as described under 1.14.4High-performanceliquidchromatography using theconditionsgivenbelowunderassaymethod.
Preparethefollowingsolutionsinmobilephase:forsolution(1)dissolveabout30mgofthepowderanddiluteto100.0mL.Forsolution(2)dilute1volumeofsolution(1)to100volumes.Forsolution(3)dissolveabout5mgceftriaxonesodiumRSand5mgofceftriaxoneimpurityAto100.0mL.
Inject20µLofsolution(3).ThetestisnotvalidunlesstheresolutionfactorbetweenthepeaksduetoceftriaxoneandceftriaxoneimpurityAisatleast3.0.CeftriaxoneimpurityAiselutedatarelativeretentionofabout1.4withreferencetoceftriaxone(retentiontimeabout9min).
Injectalternately20μLeachofsolutions(1)and(2).Recordthechromatogramsforabout2timestheretentiontimeofceftriaxone.
Inthechromatogramobtainedwithsolution(1):
• theareaofanypeak,otherthantheprincipalpeak,isnotgreaterthantheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(2)(1.0%);
• thesumoftheareasofallpeaks,otherthantheprincipalpeak,isnotgreaterthan2.5timestheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(2)(2.5%).Disregardanypeakwithanarealessthan0.1timestheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(2)(0.1%).
AssayCarry out the test as described under 1.14.4High-performanceliquidchromatography using a stainlesssteelcolumn(25cmx4.6mm)packedwithparticlesofbase-deactivatedsilicagel,thesurfaceofwhichhasbeenmodifiedwithchemically-bondedoctadecylsilylgroups(5µm).1
Asthemobilephaseuseasolutionpreparedasfollows:dissolve2.0goftetradecylammoniumbromideRand2.0goftetraheptylammoniumbromideRinamixtureof440mLofwaterR,55mlofphosphatebuffer,pH7.0(0.067mol/L)TS,5.0mLofacitratebufferpH5.0TSand500mLofacetonitrileRandfilter.
Preparethefollowingsolutionsinmobilephase:forsolution(1)determinetheweightofthecontentsof10containers.Transferaquantityofthemixedcontentscontainingabout30mgofceftriaxone,accuratelyweighed,toa100mLvolumetricflask,dissolveanddilutetovolume.
1 HypersilBDSC18hasbeenfoundsuitable.
Consultation documents WHODrugInformationVol.30,No.3,2016
454
Forsolution(2)dissolveabout35mgofceftriaxonesodiumRS,accuratelyweighedanddiluteto100.0mL.Forsolution(3)dissolveabout5mgceftriaxonesodiumRSand5mgofceftriaxoneimpurityAto100.0mL.
Operatewithaflowrateof1.5mLperminute.Asadetectoruseanultravioletspectrophotometersetatawavelengthof254nm.
Inject20µLofsolution(3).ThetestisnotvalidunlesstheresolutionfactorbetweenthepeaksduetoceftriaxoneandceftriaxoneimpurityAisatleast3.0.
Inject20µLofsolution(1)and(2)Measuretheareasofthepeakscorrespondingtoceftriaxone and calculate the content of ceftriaxone (C18H16N8O7S3)percontainer,usingthedeclared content of C18H16N8Na2O7S3inceftriaxonesodiumRS.EachmgofC18H16N8Na2O7S3 is equivalentto0.9274mgofC18H16N8O7S3.
ImpuritiesTheimpuritieslimitedbytherequirementsofthismonographincludethoselistedinthemonographforCeftriaxonesodium.
***
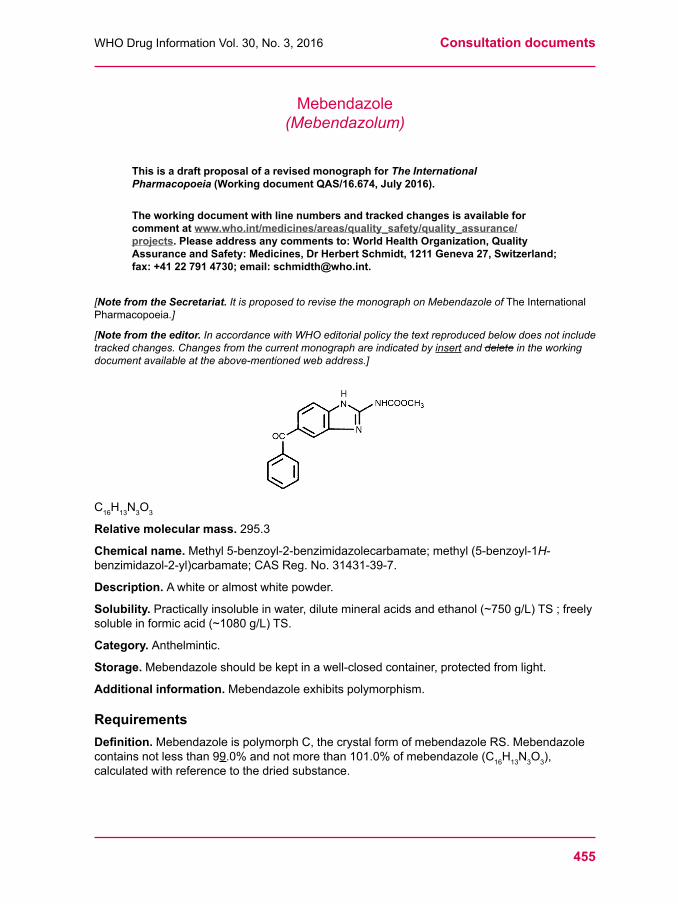
455
WHODrugInformationVol.30,No.3,2016 Consultation documents
Mebendazole(Mebendazolum)
This is a draft proposal of a revised monograph for The International Pharmacopoeia (Working document QAS/16.674, July 2016).
The working document with line numbers and tracked changes is available for comment at www.who.int/medicines/areas/quality_safety/quality_assurance/projects. Please address any comments to: World Health Organization, Quality Assurance and Safety: Medicines, Dr Herbert Schmidt, 1211 Geneva 27, Switzerland; fax: +41 22 791 4730; email: [email protected].
[Note from the Secretariat. It is proposed to revise the monograph on Mebendazole of The International Pharmacopoeia.]
[Note from the editor. In accordance with WHO editorial policy the text reproduced below does not include tracked changes. Changes from the current monograph are indicated by insert and delete in the working document available at the above-mentioned web address.]
C16H13N3O3
Relative molecular mass. 295.3
Chemical name. Methyl5-benzoyl-2-benzimidazolecarbamate;methyl(5-benzoyl-1H-benzimidazol-2-yl)carbamate;CASReg.No.31431-39-7.
Description. Awhiteoralmostwhitepowder.
Solubility. Practicallyinsolubleinwater,dilutemineralacidsandethanol(~750g/L)TS;freelysolubleinformicacid(~1080g/L)TS.
Category. Anthelmintic.
Storage.Mebendazoleshouldbekeptinawell-closedcontainer,protectedfromlight.
Additional information.Mebendazoleexhibitspolymorphism.
RequirementsDefinition.MebendazoleispolymorphC,thecrystalformofmebendazoleRS.Mebendazolecontains not less than 99.0%andnotmorethan101.0%ofmebendazole(C16H13N3O3),calculated with reference to the dried substance.
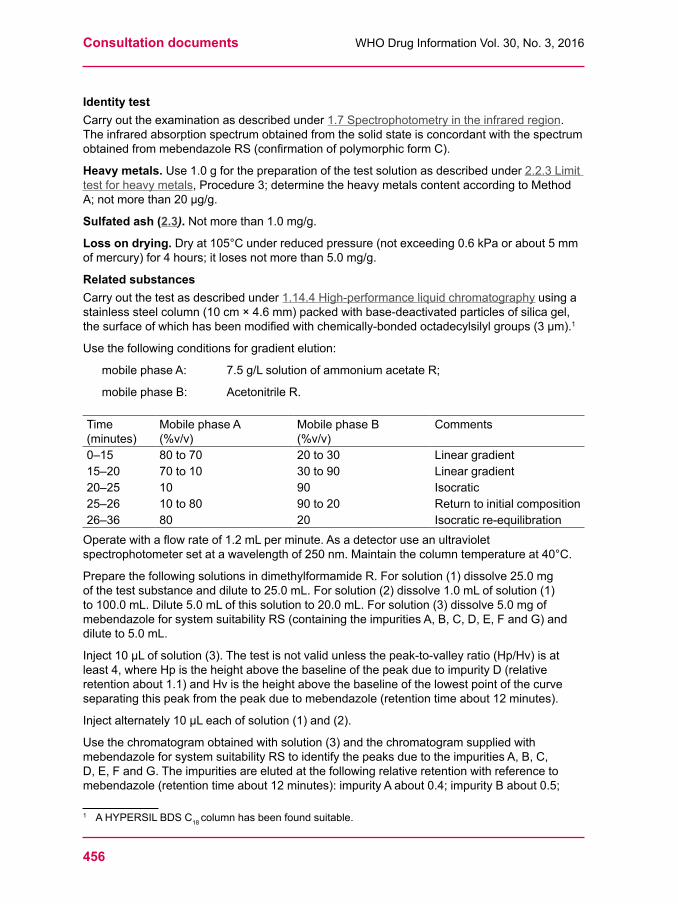
Consultation documents WHODrugInformationVol.30,No.3,2016
456
Identity test Carryouttheexaminationasdescribedunder1.7Spectrophotometryintheinfraredregion. TheinfraredabsorptionspectrumobtainedfromthesolidstateisconcordantwiththespectrumobtainedfrommebendazoleRS(confirmationofpolymorphicformC).
Heavy metals. Use1.0gforthepreparationofthetestsolutionasdescribedunder2.2.3Limittestforheavymetals,Procedure3;determinetheheavymetalscontentaccordingtoMethodA;notmorethan20μg/g.
Sulfated ash (2.3).Notmorethan1.0mg/g.
Loss on drying. Dryat105°Cunderreducedpressure(notexceeding0.6kPaorabout5mmofmercury)for4hours;itlosesnotmorethan5.0mg/g.
Related substancesCarry out the test as described under 1.14.4High-performanceliquidchromatography using a stainlesssteelcolumn(10cm×4.6mm)packedwithbase-deactivatedparticlesofsilicagel,thesurfaceofwhichhasbeenmodifiedwithchemically-bondedoctadecylsilylgroups(3μm).1
Usethefollowingconditionsforgradientelution:
mobilephaseA: 7.5g/LsolutionofammoniumacetateR;
mobilephaseB: AcetonitrileR.
Time (minutes)
Mobile phase A (%v/v)
Mobile phase B (%v/v)
Comments
0–15 80to70 20to30 Linear gradient15–20 70to10 30to90 Linear gradient20–25 10 90 Isocratic25–26 10to80 90to20 Returntoinitialcomposition26–36 80 20 Isocratic re-equilibrationOperatewithaflowrateof1.2mLperminute.Asadetectoruseanultravioletspectrophotometersetatawavelengthof250nm.Maintainthecolumntemperatureat40°C.
PreparethefollowingsolutionsindimethylformamideR.Forsolution(1)dissolve25.0mgofthetestsubstanceanddiluteto25.0mL.Forsolution(2)dissolve1.0mLofsolution(1)to100.0mL.Dilute5.0mLofthissolutionto20.0mL.Forsolution(3)dissolve5.0mgofmebendazoleforsystemsuitabilityRS(containingtheimpuritiesA,B,C,D,E,FandG)anddiluteto5.0mL.
Inject10μLofsolution(3).Thetestisnotvalidunlessthepeak-to-valleyratio(Hp/Hv)isatleast4,whereHpistheheightabovethebaselineofthepeakduetoimpurityD(relativeretentionabout1.1)andHvistheheightabovethebaselineofthelowestpointofthecurveseparatingthispeakfromthepeakduetomebendazole(retentiontimeabout12minutes).
Injectalternately10μLeachofsolution(1)and(2).
Usethechromatogramobtainedwithsolution(3)andthechromatogramsuppliedwithmebendazoleforsystemsuitabilityRStoidentifythepeaksduetotheimpuritiesA,B,C,D,E,FandG.Theimpuritiesareelutedatthefollowingrelativeretentionwithreferencetomebendazole(retentiontimeabout12minutes):impurityAabout0.4;impurityBabout0.5;
1 AHYPERSILBDSC18 columnhasbeenfoundsuitable.
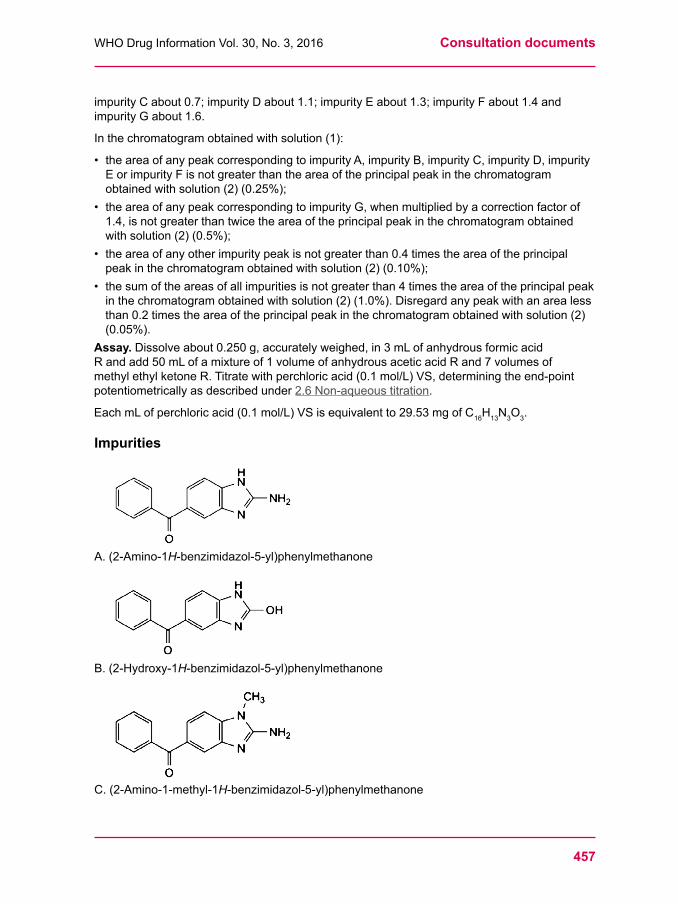
457
WHODrugInformationVol.30,No.3,2016 Consultation documents
impurityCabout0.7;impurityDabout1.1;impurityEabout1.3;impurityFabout1.4andimpurityGabout1.6.
Inthechromatogramobtainedwithsolution(1):
• theareaofanypeakcorrespondingtoimpurityA,impurityB,impurityC,impurityD,impurityEorimpurityFisnotgreaterthantheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(2)(0.25%);
• theareaofanypeakcorrespondingtoimpurityG,whenmultipliedbyacorrectionfactorof1.4,isnotgreaterthantwicetheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(2)(0.5%);
• theareaofanyotherimpuritypeakisnotgreaterthan0.4timestheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(2)(0.10%);
• thesumoftheareasofallimpuritiesisnotgreaterthan4timestheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(2)(1.0%).Disregardanypeakwithanarealessthan0.2timestheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(2)(0.05%).
Assay. Dissolveabout0.250g,accuratelyweighed,in3mLofanhydrousformicacidRandadd50mLofamixtureof1volumeofanhydrousaceticacidRand7volumesofmethylethylketoneR.Titratewithperchloricacid(0.1mol/L)VS,determiningtheend-pointpotentiometricallyasdescribedunder2.6Non-aqueoustitration.
EachmLofperchloricacid(0.1mol/L)VSisequivalentto29.53mgofC16H13N3O3.
Impurities
A.(2-Amino-1H-benzimidazol-5-yl)phenylmethanone
B. (2-Hydroxy-1H-benzimidazol-5-yl)phenylmethanone
C.(2-Amino-1-methyl-1H-benzimidazol-5-yl)phenylmethanone
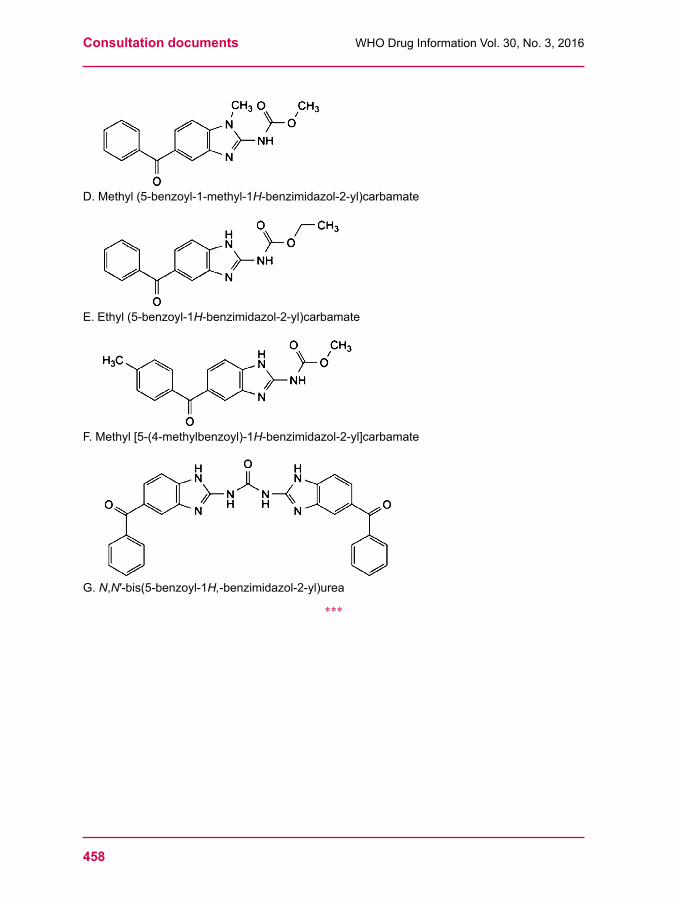
Consultation documents WHODrugInformationVol.30,No.3,2016
458
D.Methyl(5-benzoyl-1-methyl-1H-benzimidazol-2-yl)carbamate
E.Ethyl(5-benzoyl-1H-benzimidazol-2-yl)carbamate
F.Methyl[5-(4-methylbenzoyl)-1H-benzimidazol-2-yl]carbamate
G. N,N′-bis(5-benzoyl-1H,-benzimidazol-2-yl)urea
***
459
WHODrugInformationVol.30,No.3,2016 Consultation documents
Mebendazole chewable tablets (Mebendazoli compressi manducabili)
This is a draft proposal of a revised monograph for The International Pharmacopoeia (Working document QAS/16.661, July 2016). The working document with line numbers is available for comment at www.who.int/medicines/areas/quality_safety/quality_assurance/projects. Please address any comments to: World Health Organization, Quality Assurance and Safety: Medicines, Dr Herbert Schmidt, 1211 Geneva 27, Switzerland; fax: +41 22 791 4730; email: [email protected].
[Note from the Secretariat. The draft revision of the monograph is based on samples received in response to a letter sent out to pharmaceutical manufacturers in November 2014, inviting their collaborating in the development of this document. Manufacturers that have not yet donated samples and/or specifications are again kindly invited to do so. For more information, kindly contact Dr Herbert Schmidt at [email protected].]
Category.Anthelmintic.
Storage. Mebendazole chewable tablets should be kept in a tightly closed container.
Labelling.Thedesignationonthecontainershouldstatethatthetabletsmaybechewed,swallowedwhole,crushedandmixedwithfoodorliquidordispersedinwater.
Additional information. StrengthsinthecurrentWHOModelListofEssentialMedicines(EML):100mg,500mg.StrengthsinthecurrentWHOEMLforchildren:100mg,500mg.
RequirementsComplywiththemonographforTablets.
Definition.MebendazolechewabletabletscontainMebendazoleinasuitablebasisthatmaycontainsuitableflavouringagents.Mebendazolechewabletabletscontainnotlessthan90.0%andnotmorethan110.0%oftheamountofmebendazole(C16H13N3O3) stated on the label.
Manufacture.Theformulation,manufacturingprocessandproductpackagingofMebendazolechewabletabletsaredesignedandcontrolledsoastominimizetheconversionofthepolymorphicformofmebendazolefromCtoA.Theyensurethat,atanystageofthelife-cycleoftheproduct,whentestedbyasuitablemethodsuchasinfraredspectrometry(seeIdentitytestA)orX-raypowderdiffractometry,themebendazoleinthetabletsispredominantlyintheformofpolymorphC.
Identity tests • EithertestsA,BandCortestsA,BandDmaybeapplied.A.Toaquantityofthepowderedtabletscontaining0.05gofMebendazoleadd20mLofwater
R,shake,filterandwashtheresiduewiththreequantities,eachof10mLofwaterR.Drytheresidueovernightundervacuumatroomtemperatureandcarryouttheexaminationwith the residue as described under 1.7Spectrophotometryintheinfraredregion. The two infraredabsorptionbandsatabout3405cm-1and1720cm-1 are concordant with those in thespectrumobtainedfrommebendazoleRS(containingmebendazolepolymorphC).
Consultation documents WHODrugInformationVol.30,No.3,2016
460
B.Shakeaquantityofthepowderedtabletscontaining0.04gofMebendazolewith2mLofsodiumhydroxide(~80g/L)TSandheattheyellowishcolouredsuspension;thesolutionisyellow.Addafewdropsofcopper(II)sulfate(160g/L)TS;agreenishprecipitateisproduced.Addafewdropsofammonia(~100g/L)TS;thecolouroftheprecipitateturnstogreenish blue.
C. Carry out the test as described under 1.14.1Thin-layerchromatographyusingsilicagelR6asthecoatingsubstanceandamixtureof85volumesofdichloromethaneR,5volumesofmethanolR,5volumesofacetoneRand5volumesofanhydrousformicacidRasthemobilephase.Applyseparatelytotheplate5μLofeachofthefollowingsolutions.Forsolution(A)add2mLofformicacidtoaquantityofthepowderedtabletscontaining20mgofMebendazoleandsonicateforabout5minutes.Add18mLofacetoneR,mix,filterandusethefiltrate.Forsolution(B)dissolve10mgofmebendazoleRSin1mLofformicacidandshake.Add9mLofacetoneRandmix.Afterremovingtheplatefromthechromatographicchamberallowittodryinairandexaminethechromatograminultravioletlight(254nm).
Theprincipalspotobtainedwithsolution(A)correspondsinposition,appearanceandintensity with that obtained with solution (B).
D. Carry out the test as described under 1.14.4High-performanceliquidchromatography usingtheconditionsunder“Assay”,Theretentiontimeoftheprincipalpeakinthechromatogramobtainedwithsolution(1)correspondstotheretentiontimeofthepeakduetomebendazoleobtainedwithsolution(2).
Related substancesCarry out the test as described under 1.14.4High-performanceliquidchromatography using a stainlesssteelcolumn(10cm×4.6mm)packedwithbase-deactivatedparticlesofsilicagel,thesurfaceofwhichhasbeenmodifiedwithchemically-bondedoctadecylsilylgroups(3μm).1
Usethefollowingconditionsforgradientelution:
mobilephaseA: 7.5g/LsolutionofammoniumacetateR;
mobilephaseB: AcetonitrileR.
Time (min)
Mobile phase A (%v/v)
Mobile phase B (%v/v)
Comments
0–15 80to70 20to30 Linear gradient15–20 70to10 30to90 Linear gradient20–25 10 90 Isocratic25–26 10to80 90to20 Returntoinitialcomposition26–36 80 20 Isocratic re-equilibrationOperatewithaflowrateof1.2mLperminute.Asadetectoruseanultravioletspectrophotometersetatawavelengthof250nm.Maintainthecolumntemperatureat40°C.Prepareasasolventamixtureof60volumesofmethanolRand40volumesofwaterR.
Forsolution(1)transferaquantityofthepowderedtablets,containingabout100mgofmebendazole,accuratelyweighed,toa100mLvolumetricflask.Add30mLofanhydrousformicacidRandsonicateforabout20minutes.Dilutetovolumewiththesolventmixture,mixandfilter.Forsolution(2)dilute1.0mLofsolution(1)to100.0mLwiththesolventmixture.
1 AHYPERSILBDSC18 columnhasbeenfoundsuitable.
461
WHODrugInformationVol.30,No.3,2016 Consultation documents
Dilute5.0mLofthissolutionto20.0mLwiththesolventmixture.Forsolution(3)transfer10mgmebendazoleRtoa10mLvolumetricflask,add5mLofmethanolRand1mLofsodiumhydroxide(~40g/L)TSsolution,heatinawaterbathat60°Cfor1hour,cooltoroomtemperatureandadjustthesolutiontopH7withhydrochloricacid(~36.5g/L)TS.DilutewithmethanolRtovolumeandmix.
Inject10µlofsolution(3).UsethechromatogramtoidentifythepeakduetoimpurityA.Theimpurityiselutedattherelativeretentionof0.4withreferencetomebendazole(retentiontimeabout12minutes).
Thetestisnotvalidunlessinthechromatogramobtainedwithsolution(3)theresolutionbetweenmebendazoleandimpurityAisatleast10.
Injectalternately10µleachofsolution(1)and(2).
Inthechromatogramobtainedwithsolution(1):
• theareaofanypeakcorrespondingtoimpurityAisnotgreaterthantheareaoftheprincipalpeakinthechromatogramobtainedwithsolution(2)(0.25%).
Dissolution
For 100 mg tablets. Carry out the test as described under 5.5Dissolutiontestforsolidoraldosageformsusing900mLofhydrochloricacid(~3.65g/L)TSasthedissolutionmediumandrotatingthepaddleat75revolutionsperminute.At120minuteswithdrawasampleof10mLofthedissolutionmediumthroughanin-linefilter.Allowthefilteredsampletocooltoroomtemperature.Dilute5.0mLofthefiltrateto50.0mLwiththedissolutionmedium.
Determinethecontentofmebendazole(C16H13N3O3)inthemediumby1.14.4 High-performanceliquidchromatographyusingtheconditionsdescribedunder“Assay”andasuitablesolutionofmebendazoleRSasareferencesolution.
Foreachofthesixtabletstestedcalculatethetotalamountofmebendazole(C16H13N3O3) in themediumusingthedeclaredcontentof(C16H13N3O3)inmebendazoleRS.Theamountinsolutionforeachtabletisnotlessthan60%(Q)oftheamountdeclaredonthelabel.
For 500 mg tablets. Carry out the test as described under 5.5Dissolutiontestforsolidoraldosageformsusing900mLofa1.0%solutionofsodiumdodecylsulfateRinhydrochloricacid(~0.365g/L)TSasthedissolutionmediumandrotatingthepaddleat75revolutionsperminute.At60minuteswithdrawasampleof10mLofthedissolutionmediumthroughanin-linefilter.Allowthefilteredsampletocooltoroomtemperature.Dilute1.0mLofthefiltrateto50.0mLwiththedissolutionmedium.
Determinethecontentofmebendazole(C16H13N3O3)inthemediumby1.14.4 High-performanceliquidchromatographyusingtheconditionsdescribedunder“Assay”andasuitablesolutionofmebendazoleRSasareferencesolution.
Foreachofthesixtabletstestedcalculatethetotalamountofmebendazole(C16H13N3O3) in themediumusingthedeclaredcontentof(C16H13N3O3)inmebendazoleRS.Theamountinsolutionforeachtabletisnotlessthan75%(Q)oftheamountdeclaredonthelabel.
Consultation documents WHODrugInformationVol.30,No.3,2016
462
Assay Carry out the test as described under 1.14.4High-performanceliquidchromatography using a stainlesssteelcolumn(10cm×4.6mm)packedwithoctadecylsilylbase-deactivatedsilicagelforchromatographyR(3µm).2
Asthemobilephaseuseasolutionpreparedasfollows:dissolve7.5gofammoniumacetateRin1000mLofwaterR,mixandfilter.Mix750mLofthissolutionwith250mLofacetonitrileR.
Prepareasasolventamixtureof60volumesofmethanolRand40volumesofwaterR.
Preparethefollowingsolutions.Forsolution(1)weighandpowder20tablets.Transferaquantityofthepowderedtablets,containingabout100mgofmebendazole,accuratelyweighed,toa100mLvolumetricflask.Add30mLofanhydrousformicacidandsonicateforabout20minutes.Dilutetovolumewithsolventmixture,mixandfilter.Dilute5.0mLofthefiltrateto100.0mLwiththesolventmixture.Forsolution(2)transfer25.0mgofmebendazoleRStoa25mLvolumetricflask,add10mLoftheanhydrousformicacidRandsonicatetodissolve.Dilutetovolumewiththesolventmixture.Dilute5.0mLofthissolutionto100.0mLwiththesolventmixture.
Operatewithaflowrateof1.2mLperminute.Asadetectoruseanultravioletspectrophotometersetatawavelengthof250nm.
Injectalternately10µLeachofsolutions(1)and(2).
Measuretheareasofthepeakscorrespondingtomebendazoleobtainedinthechromatogramsfromsolution(1)and(2)andcalculatethepercentagecontentofmebendazole(C16H13N3O3) in the chewable tablets using the declared content of C16H13N3O3inmebendazoleRS.
ImpuritiesTheimpuritieslimitedbytherequirementsofthismonographincludesimpurityAlistedinthemonographforMebendazole.
Reagents to be establishedMebendazole RMebendazole of a suitable quality should be used.
Hydrochloric acid (~0.365 g/L) TS Hydrochloricacid(~250g/L)TS,dilutewithwatertocontain0.365gofHClin1000mL.
***
2 AHYPERSILBDSC18columnhasbeenfoundsuitable.
463
WHODrugInformationVol.30,No.3,2016 Consultation documents
Methylthioniniumchloride(Methylthioninii chloridum)
This is a draft proposal of a monograph for The International Pharmacopoeia (Working document QAS/16.675, July 2016). The working document with line numbers is available for comment at www.who.int/medicines/areas/quality_safety/quality_assurance/projects. Please address any comments to: World Health Organization, Quality Assurance and Safety: Medicines, Dr Herbert Schmidt, 1211 Geneva 27, Switzerland; fax: +41 22 791 4730; email: [email protected].
[Note from the Secretariat. It is proposed to revise the monograph on Methylthioninium chloride.]
[Note from the editor. In accordance with WHO editorial policy the text reproduced below does not include tracked changes. Changes from the current monograph are indicated by insert and delete in the working document available at the above-mentioned web address.]
Molecular formula. C16H18ClN3S(anhydrous);C16H18ClN3S∙H2O(monohydrate);C16H18ClN3S∙3H2O(trihydrate); C16H18ClN3S∙5H2O (pentahydrate).
Relative molecular mass.319.9(anhydrous);337.9(monohydrate);373.9(trihydrate);409.9(pentahydrate).
Graphic formula
n=0(anhydrous)n=1(monohydrate)n=3(trihydrate)n=5(pentahydrate)
Chemical name.C.I.BasicBlue9;3,7-bis(dimethylamino)phenothiazin-5-iumchloride;CASReg.No.61-73-4(anhydrous).
C.I.BasicBlue9monohydrate;3,7-bis(dimethylamino)phenothiazin-5-iumchloridemonohydrate;CASReg.No.122965-43-9(monohydrate).
C.I.BasicBlue9trihydrate;3,7-bis(dimethylamino)phenothiazin-5-iumchloridetrihydrate;CASReg.No.7220-79-3(trihydrate).
C.I.BasicBlue9pentahydrate;3,7-bis(dimethylamino)phenothiazin-5-iumchloridepentahydrate;CASReg.No.32680-41-4(pentahydrate).
Other name. Methylene blue
Description.Darkgreencrystalswithametalliclustreoradarkgreen,crystallinepowder.
Solubility.SparinglysolubleinwaterR;slightlysolubleinethanol(~750g/L)TS.
Consultation documents WHODrugInformationVol.30,No.3,2016
464
Category. Antidote.
Storage.Methylthioniniumchlorideshouldbekeptinatightlyclosedcontainer,protectedfromlight,atatemperaturenotexceeding30°C.
Additional information.Methylthioniniumchlorideishygroscopic.
RequirementsDefinition.Methylthioniniumchloridecontainsnotlessthan93.0%andnotmorethan102.0%(“Assay”,methodA)ornotlessthan98.0%andnotmorethan102.0%(“Assay”,methodB)ofC16H18ClN3S,calculatedwithreferencetothedriedsubstance.
Identity tests• EithertestsAandForanytwooftestsB,C,DorEtogetherwithtestFmaybeapplied.A. Carryouttheexaminationasdescribedunder1.7Spectrophotometryintheinfrared
region.TheinfraredabsorptionspectrumisconcordantwiththespectrumobtainedfrommethylthioniniumchlorideRSorwiththereference spectrumofmethylthioniniumchloride.
B. Carry out the test as described under 1.14.4High-performance-liquidchromatography usingtheconditionsgivenunder“Assay”,methodA.Theretentiontimeoftheprincipalpeakinthechromatogramobtainedwithsolution(1)correspondstotheretentiontimeofthepeakduetomethylthioniniuminthechromatogramobtainedwithsolution(2).
C. Theabsorptionspectrum(1.6)ofa5μg/mLsolutioninhydrochloricacid(~70g/L)TS,whenobservedbetween230nmand800nm,exhibits4maximaatabout258nm,288nm,680nm,and745nm.
D. Carry out the test as described under 1.14.1Thin-layerchromatography,usingsilicagelR6asthecoatingsubstanceandamixtureof3volumesofaceticacidR,3volumesofethanolRand4volumesofwaterRasthemobilephase.Applyseparatelytotheplate2µLofeachofthefollowing2solutionsinmethanolRcontaining(A)0.1mgofthetestsubstancepermLand(B)0.1mgofmethylthioniniumchlorideRSpermL.Afterremovingtheplatefromthechromatographicchamberallowittodryinairorinacurrentofcoolair.Examinethechromatogramindaylight.Theprincipalspotobtainedwithsolution(A)correspondsinposition,appearanceandintensity to that obtained with solution (B).
E. Dissolve1mgin10mLofwaterR;adeepbluecolorisproduced.Add2.0mLofhydrochloricacid(~70g/L)TSand0.25gofzincRpowder;thecolorofthesolutionisdischarged.Filterandexposethefiltratetotheair;thebluecolorofthesolutionreappears.
F. Mix0.05gofthesubstancetobeinvestigatedwith0.5gofanhydroussodiumcarbonateRinaporcelaincrucible.Carefullyheatthemixturetoaredglowfor10minutes.Cool,dissolvetheresiduein10mLofnitricacid(~130g/L)TSandfilter.Thefiltrateyieldsreaction A described under 2.1Generalidentificationtests as characteristic of chlorides.
Copper or zinc.Preparethefollowingsolutions.Forsolution(1)ignite1.0ginaporcelaincrucibleusingaslowatemperatureaspracticable,untilallofthecarbonisoxidized.Cooltheresidue,add15mLofnitricacid(~130g/L)TSandboilfor5minutes.Forsolution(2)boilaquantityofcopper(II)sulfateR,equivalentto200μgofCu,with15mLofnitricacid(~130g/L)TSfor5minutes.Filterseparatelythecooledsolutions(1)and(2)andwashanyresiduewith10mLofwater.Combinethefiltrateandwashingsofthesolution(1)andsimilarlycombinethefiltrateandwashingsofthesolution(2);addtoeachanexcessofammonia(~100g/L)TS
465
WHODrugInformationVol.30,No.3,2016 Consultation documents
andfilterthesolutionsinto50mLvolumetricflasks.Washtheprecipitateswithsmallportionsofwater,addingthewashingstothefiltrates;dilutethecontentsofeachflaskwithwatertovolume,mixingthoroughly.To25mLofeachofthesolutionsadd10mLofhydrogensulfideTS;noturbidityisproducedwithin5minutes(absenceofzinc)andanydarkcolourproducedinsolution(1)isnotmoreintensethanthatofsolution(2)(thecoppercontentisnotmorethan0.20mg/g).
Iron.Mix4gwith200mLofwaterRinalong-necked,round-bottomedflask,add15mLofnitricacid(~1000g/L)TS,heatcarefullytoboilingandcontinueboilinguntilthevolumeofliquidisreducedtoabout20mL.Allowtocool,add10mLofsulfuricacid(~1760g/L)TSandmix.Heattoboilingandaddsmallsuccessivequantitiesofnitricacid(~1000g/L)TS,coolingbeforeeachaddition,untilacolourlessliquidisobtained.Heatuntilwhitefumesareevolved;ifdarkeningoccursatthisstagecontinuethetreatmentwithnitricacid(~1000g/L)TS.Finallyheatuntilwhitefumesareagainevolved.Allowthecolourlessliquidtocool,add25mLofasaturatedsolutionofammoniumoxalateRinwater,andboiluntiltheslightfrothcompletelysubsides.Cool,diluteto50mLwithwater;5mLofthedilutedsolutioncomplieswiththe2.2.4 Limittestforiron;notmorethan0.10mg/g.
Sulfated ash.Notmorethan2.5mg/g.
Loss on drying.Dryat105°Cfor5hours;itlosesnotmorethan240mg/g.(Thedriedsubstancemaybeusedtoproducesolution(4)ofthetest“Relatedsubstances”).
Related substancesCarry out test as described under 1.14.4High-performanceliquidchromatography using the chromatographicconditionsasdescribedunder“Assay”,methodA.Preparethefollowingsolutionsusingasthediluentamixtureof70volumesofa0.1%(v/v)solutionoftrifluoroaceticacidR(mobilephaseA)and30volumesofacetonitrileR(mobilephase B).Forsolution(1)dissolveabout50mgofthesubstancetobeexaminedanddiluteto50.0mL.Sonicatefor5minutes.Forsolution(2)dilute1.0mLofsolution(1)to100.0mL.Forsolution(3)dilute5.0mLofsolution(2)to50.0mL.Forsolution(4)dissolve2.5mgmethylthioniniumchlorideimpurityARSanddiluteto10.0mL.Transfer1.0mLofthissolutiontoa10mLvolumetricflaskandmakeuptovolumewithsolution(1).Alternatively,drythesubstancetobeexaminedat105°Cfor5h(thedriedsubstanceofthetest“Lossondrying”maybeused),dissolve100mgofthedriedsubstanceanddiluteto100.0mL.Sonicatefor5minutes.Injectalternately5µLeachofsolutions(1),(2),(3),(4).Usethechromatogramsobtainedwithsolution(4)andsolution(1)toidentifythepeakduetoimpurityA.ImpurityAiselutedattherelativeretentionofabout0.8withreferencetomethylthioninium(retentiontimeabout11minutes).ThetestisnotvalidunlesstheresolutionbetweenthepeakscorrespondingtomethylthioniniumandimpurityAisatleast3.5.Inthechromatogramobtainedwithsolution(1):
• theareaofanypeakcorrespondingtoimpurityAisnotgreaterthan5timestheareaoftheprincipalpeakobtainedwithsolution(2)(5.0%);
• theareaofanyotherimpuritypeakisnotgreaterthantheareaoftheprincipalpeakobtainedwithsolution(3)(0.10%);
• thesumoftheareasofallimpuritypeaks,otherthanthepeakcorrespondingtoimpurityA,isnotgreaterthan5timestheareaoftheprincipalpeakobtainedwithsolution(3)(0.5%).Disregardanypeakwithanarealessthan0.5timestheareaoftheprincipalpeakobtainedwithsolution(3)(0.05%).
Consultation documents WHODrugInformationVol.30,No.3,2016
466
Assay• EithermethodAorBmaybeapplied.A. Carry out test as described under 1.14.4High-performanceliquidchromatography using a
stainlesssteelcolumn(10cmx4.6mm)packedwithparticlesofsilicagel,thesurfaceofwhichhasbeenmodifiedwithchemically-bondedphenylsilylgroups(3.5µm).1
Usethefollowingconditionsforgradientelution:mobilephaseA:0.1%(v/v)solutionoftrifluoroaceticacidR mobilephaseB:acetonitrileR.
Time(minutes)
Mobile phase A(%v/v)
Mobile phase B(%v/v)
Comments
0–5 80 20 Isocratic 5–25 80to30 20to70 Linear gradient25–32 30 70 Isocratic 32–35 30to80 70to20 Returntoinitialcomposition35–40 80 20 Re-equilibration
Operatewithaflowof1.0mL/min.Asadetectorusanultravioletspectrophotometersetatawavelengthof246nm.Maintainthecolumntemperatureat30°C.
Preparethefollowingsolutionsusingasdiluentamixtureof30volumesofacetonitrileRand70volumesofmobilephaseA.Forsolution(1)dissolveabout50mgofthesubstancetobeexamined,accuratelyweighed,anddiluteto50.0mL.Sonicatefor5minutes.Forsolution(2)dissolve50.0mgofmethylthioniniumchlorideRSanddiluteto50.0mL.Sonicatefor5min.
Injectalternately5µLeachofsolutions(1)and(2).Thetestisnotvalidunlessthesymmetryfactorofmethylthioniniumisnotmorethan3.0.
Measuretheareasofthepeakresponsesobtainedinthechromatogramsfromsolutions(1)and(2)andcalculatethepercentagecontentofmethylthioniniumchloride(C16H18ClN3S),using the declared content of C16H18ClN3SinmethylthioniniumchlorideRS.
B.Dissolveabout100mg,accuratelyweighed,insufficientethanol(~457g/L)TStoproduce250.0mL.Dilute5.0mLofthissolutionto100.0mLwithethanol(~457g/L)TS.Dilute5.0mLofthissolutionto50.0mLwithethanol(~457g/L)TS.Measuretheabsorbance(1.6)ofa1cmlayerofthedilutedsolutionatthemaximumatabout664nmandcalculatethepercentagecontentofmethylthioniniumchloride(C16H18ClN3S)usingtheabsorptivityvalueof2950methylthioniniumchloride.
[Note from the Secretariat. The absorptivity value is so far based on a single determination. It is intended to perform further independent determinations to confirm the value.]
AdditionalrequirementsforMethylthioniniumchlorideforparenteraluseComplieswiththemonographforParenteral preparations.
Bacterial endotoxins.Ifintendedforuseinthemanufactureofaparenteraldosageformswithoutafurtherappropriateprocedurefortheremovalofbacterialendotoxins,carryoutthetest as described under 3.4Testforbacterialendotoxins;containsnotmorethan2.5IUofendotoxinRSpermg.
1 AnX-BridgePhenylcolumnandaPhenomenexLuna3μmPhenyl-Hexylcolumnwerefoundsuitable.
467
WHODrugInformationVol.30,No.3,2016 Consultation documents
Impurities
A.3-(Dimethylamino)-7-(methylamino)phenothiazin-5-iumchloride(azureB).
B.3-Amino-7-(dimethylamino)phenothiazin-5-ium(azureA)
C.3-amino-7-(methylamino)phenothiazin-5-ium(azureC)
***
Consultation documents WHODrugInformationVol.30,No.3,2016
468
Methylthioniniuminjection(Methylthioninii injectio)
This is a draft proposal of a monograph for The International Pharmacopoeia (Working document QAS/16.676, July 2016). The working document with line numbers is available for comment at www.who.int/medicines/areas/quality_safety/quality_assurance/projects. Please address any comments to: World Health Organization, Quality Assurance and Safety: Medicines, Dr Herbert Schmidt, 1211 Geneva 27, Switzerland; fax: +41 22 791 4730; email: [email protected].
[Note from the Secretariat. The monograph is proposed for inclusion in The International Pharmacopoeia.]
Description.Aclear,darkbluesolution.
Category. Antidote
Storage.Storeatroomtemperature,protectedfromlight.
Additional information.StrengthinthecurrentWHOModelListofEssentialMedicines(EML):10mg/mLin10mLampoule;otheravailablestrength:5mg/mL.
RequirementsComplieswiththemonographforParenteral preparations.
Definition.MethylthioniniuminjectionisasterilesolutionofMethylthioniniumchlorideinwaterforinjection.Itcontainsnotlessthan90.0%andnotmorethan110.0%oftheamountofC16H18ClN3Sstatedonthelabel.
Identity tests• AnytwooftestsA,BandCmaybeapplied.A. Carry out the test as described under 1.14.4High-performance-liquidchromatography
usingtheconditionsgivenunder“Assay”,methodA.Theretentiontimeoftheprincipalpeakinthechromatogramobtainedwithsolution(1)correspondstotheretentiontimeofthepeakduetomethylthioniniuminthechromatogramobtainedwithsolution(2).
B. Carry out test as described under 1.14.1Thin-layerchromatographyusingsilicagelR6asthecoatingsubstanceandamixtureof3volumesofaceticacidR,3volumesofethanolRand4volumesofwaterRasthemobilephase.Applyseparatelytotheplate1µLofeachofthefollowing2solutions:Forsolution(A)dilute1.0mLoftheinjectionto20.0mLwithmethanolRtoobtainasolutionwithaconcentrationof0.5mgofthemethylthioniniumchloridepermL.Forsolution(B)dissolve10.0mgofmethylthioniniumchlorideRSanddiluteto20.0mLwithamixtureofwaterRandmethanolR(20:80v/v).Afterremovingtheplatefromthechromatographicchamberallowittodryinairorinacurrentofcoolair.Examinethechromatogramindaylight.
Theprincipalspotobtainedwithsolution(A)correspondsinposition,appearanceandintensity to that obtained with solution (B).
469
WHODrugInformationVol.30,No.3,2016 Consultation documents
C. Theabsorptionspectrum(1.6)ofa5μg/mLsolutioninhydrochloricacid(~70g/L)TS,whenobservedbetween230nmand800nm,exhibits4maximaatabout258nm,288nm,680nmand745nm.
pHvalue(1.13).pHoftheinjection,3.0–4.5
Related substancesCarry out test as described under 1.14.4High-performanceliquidchromatography using the chromatographicconditionsasdescribedunder“Assay”,methodA.
Preparethefollowingsolutionsusingasthediluentamixtureof70volumesofa0.1%(v/v)solutionoftrifluoroaceticacidR(mobilephaseA)and30volumesofacetonitrileR(mobilephase B).
Forsolution(1)dilute1.0mLoftheinjectionto20.0mLtoobtainasolutionwithaconcentrationof0.5mgofthemethylthioniniumchloridepermL.Forsolution(2)dilute1.0mLofsolution(1)to100.0mL.Forsolution(3)dilute5.0mLofsolution(2)to50.0mL.Forsolution(4)dissolve2.5mgmethylthioniniumchlorideimpurityARSanddiluteto10.0mL.Transfer1.0mLofthissolutiontoa10mLvolumetricflaskandmakeuptovolumewithsolution(1).Alternatively,dry100mgofmethylthioniniumchlorideRat105°Cfor5hours,dissolve50mgofthedriedsubstanceanddiluteto100.0mL.Sonicatefor5minutes.
Injectalternately5µLeachofsolutions(1),(2),(3)and(4).
Usethechromatogramsobtainedwithsolution(4)andsolution(1)toidentifythepeakduetoimpurityA.ImpurityAiselutedattherelativeretentionofabout0.8withreferencetomethylthioninium(retentiontimeabout11minutes).ThetestisnotvalidunlesstheresolutionbetweenthepeakscorrespondingtomethylthioniniumandimpurityAisatleast3.5.
Inthechromatogramobtainedwithsolution(1):
• theareaofanypeakcorrespondingtoimpurityAisnotgreaterthan5timestheareaoftheprincipalpeakobtainedwithsolution(2)(5.0%);
• theareaofanyotherimpuritypeakisnotgreaterthantwotimestheareaoftheprincipalpeakobtainedwithsolution(3)(0.20%);
• thesumoftheareasofallimpuritypeaks,otherthanthepeakcorrespondingtoimpurityA,isnotgreaterthantheareaoftheprincipalpeakobtainedwithsolution(2)(1.0%).Disregardanypeakwithanarealessthan0.5timestheareaoftheprincipalpeakobtainedwithsolution(3)(0.05%).
Assay• EithermethodAorBmaybeapplied.A. Carry out test as described under 1.14.4High-performanceliquidchromatography using a
stainlesssteelcolumn(10cmx4.6mm)packedwithparticlesofsilicagel,thesurfaceofwhichhasbeenmodifiedwithchemically-bondedphenylsilylgroups(3.5µm).1
Usethefollowingconditionsforgradientelution:mobilephaseA:0.1%(v/v)solutionoftrifluoroaceticacidR; mobilephaseB:acetonitrileR.
1 AnX-BridgePhenylcolumnandaPhenomenexLuna3μmPhenyl-Hexylcolumnwerefoundsuitable.
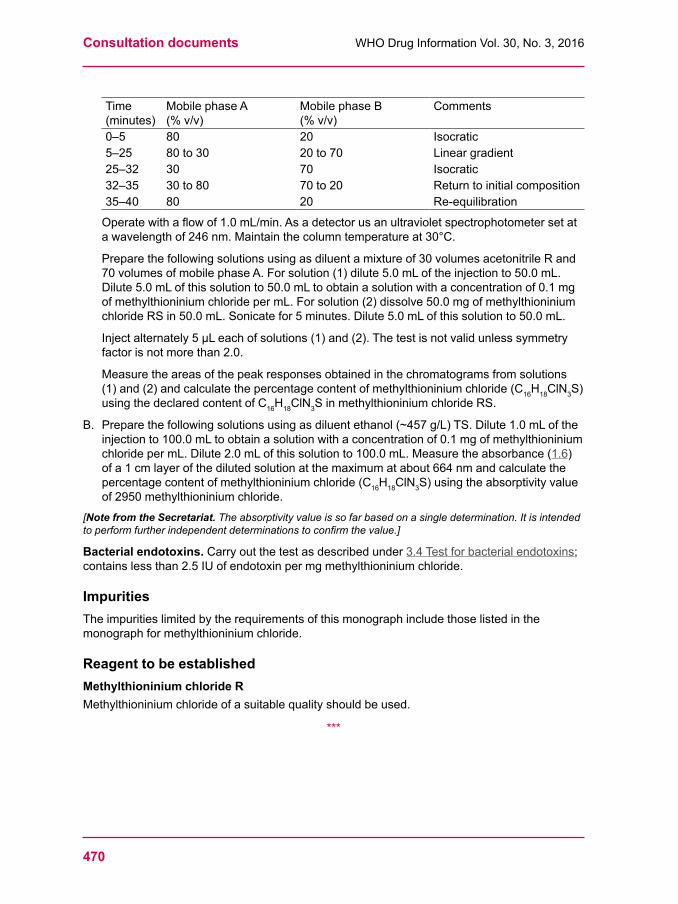
Consultation documents WHODrugInformationVol.30,No.3,2016
470
Time(minutes)
Mobile phase A(%v/v)
Mobile phase B(%v/v)
Comments
0–5 80 20 Isocratic 5–25 80to30 20to70 Linear gradient25–32 30 70 Isocratic 32–35 30to80 70to20 Returntoinitialcomposition35–40 80 20 Re-equilibration
Operatewithaflowof1.0mL/min.Asadetectorusanultravioletspectrophotometersetatawavelengthof246nm.Maintainthecolumntemperatureat30°C.
Preparethefollowingsolutionsusingasdiluentamixtureof30volumesacetonitrileRand70volumesofmobilephaseA.Forsolution(1)dilute5.0mLoftheinjectionto50.0mL.Dilute5.0mLofthissolutionto50.0mLtoobtainasolutionwithaconcentrationof0.1mgofmethylthioniniumchloridepermL.Forsolution(2)dissolve50.0mgofmethylthioniniumchlorideRSin50.0mL.Sonicatefor5minutes.Dilute5.0mLofthissolutionto50.0mL.
Injectalternately5µLeachofsolutions(1)and(2).Thetestisnotvalidunlesssymmetryfactorisnotmorethan2.0.
Measuretheareasofthepeakresponsesobtainedinthechromatogramsfromsolutions(1)and(2)andcalculatethepercentagecontentofmethylthioniniumchloride(C16H18ClN3S)using the declared content of C16H18ClN3SinmethylthioniniumchlorideRS.
B.Preparethefollowingsolutionsusingasdiluentethanol(~457g/L)TS.Dilute1.0mLoftheinjectionto100.0mLtoobtainasolutionwithaconcentrationof0.1mgofmethylthioniniumchloridepermL.Dilute2.0mLofthissolutionto100.0mL.Measuretheabsorbance(1.6) ofa1cmlayerofthedilutedsolutionatthemaximumatabout664nmandcalculatethepercentagecontentofmethylthioniniumchloride(C16H18ClN3S)usingtheabsorptivityvalueof2950methylthioniniumchloride.
[Note from the Secretariat. The absorptivity value is so far based on a single determination. It is intended to perform further independent determinations to confirm the value.]
Bacterial endotoxins. Carry out the test as described under 3.4Testforbacterialendotoxins;containslessthan2.5IUofendotoxinpermgmethylthioniniumchloride.
ImpuritiesTheimpuritieslimitedbytherequirementsofthismonographincludethoselistedinthemonographformethylthioniniumchloride.
Reagent to be establishedMethylthioninium chloride RMethylthioniniumchlorideofasuitablequalityshouldbeused.
***
471
WHODrugInformationVol.30,No.3,2016 Consultation documents
Proposedrevisionofthegeneralchapter 1.11 Colour of liquids
Thisisaproposedrevisionofthegeneralchapter1.11ColourofliquidsforThe International Pharmacopoeia (Working document QAS/16.659, July 2016). The working document with line numbers is available for comment at www.who.int/medicines/areas/quality_safety/quality_assurance/projects. Please address any comments to: World Health Organization, Quality Assurance and Safety: Medicines, Dr Herbert Schmidt, 1211 Geneva 27, Switzerland; fax: +41 22 791 4730; email: [email protected].
[Note from the Secretariat. Addition of the test Degreeofcolorationofliquids(1.11.2), reproduced from the European PharmacopoeiaIn the current procedure for the preparation of the four colour stock standard test solutions used in chapter 1.11 Colour of liquid (yellow stock standard TS, red stock standard TS, green stock standard TS and brown stock standard TS) dichromate colour TS is used. In order to replace chromium (VI) salts it is propose to gradually replace the existing procedure with the one used in the EuropeanPharmacopoeia. (The permission to reproduce the procedure will be requested when the proposed text is adopted by the WHO Expert Committee on Specifications for Pharmaceutical Preparations).For the period of transition, the original text shall be kept under the section 1.11.1; the new test procedure shall be added under the section 1.11.2. With the publication of the proposed revision of chapter 1.11 Colour of liquid, references to this chapter in existing monographs will be replaced with the reference to chapter 1.11.1. In new and revised monographs the new test procedure 1.11.2 will be applied. The definition of “colourless” under General NoticesIn the section General Notices a colourless solution is defined by referring to chapter 1.11 Colour of liquids as follows:
“A solution is considered colourless if it is not more intensely coloured than any of the standard colour solutions Bn0, Yw0, Gn0, or Rd0. The matching is made with the solution of most appropriate hue as described under 1.11 Colour of liquids.”
The specification colourless is mostly used in the sections “Clarity and colour of solution” of monographs, with and without explicit reference to chapter 1.11 Colour of liquids.For the sake of clarity, it is proposed to delete the definition of “colourless” under General Notes and to put the definition of “colourless” under 1.11.1. Those specifications under “clarity and colour of solution” that currently do not refer to chapter 1.11 Colour of liquids are to be supplemented by a respective reference.][Note from the editor. In accordance with WHO editorial policy the text reproduced below does not include tracked changes. Changes from the current monograph are indicated by insert and delete in the working document available at the above-mentioned web address.]
1.11ColourofliquidInordertoreplacechromium(VI)saltsinThe International Pharmacopoeia the procedure previouslyusedtodeterminethecolourofliquidswillbereplacedgraduallywiththecorrespondingproceduretakenoverfromtheEuropean Pharmacopoeia.
Fortheperiodoftransition,bothproceduresarekept:thepreviousprocedureundersection1.11.1 and the new procedure under section 1.11.2.
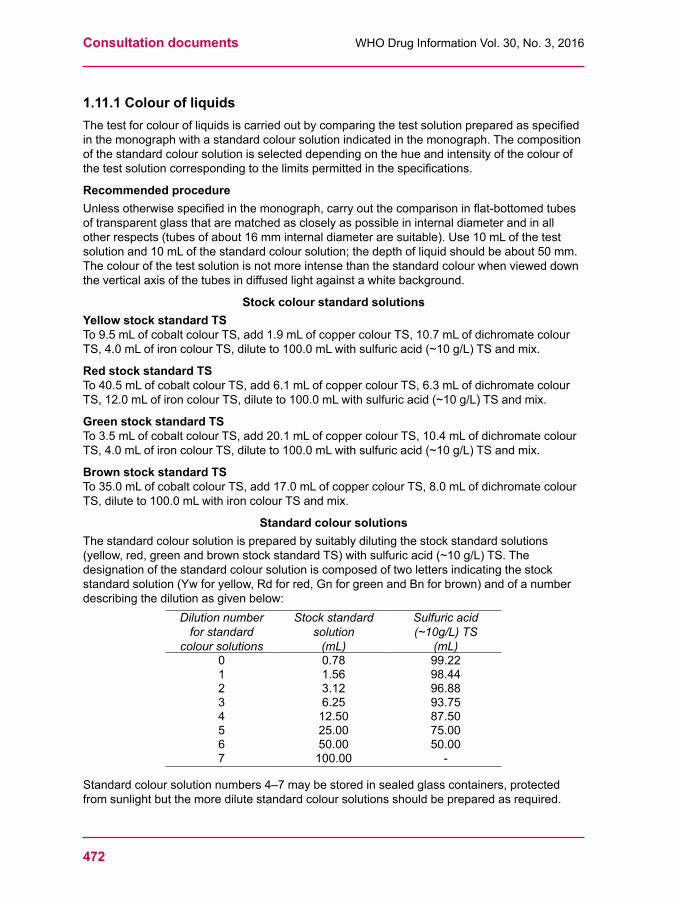
Consultation documents WHODrugInformationVol.30,No.3,2016
472
1.11.1ColourofliquidsThetestforcolourofliquidsiscarriedoutbycomparingthetestsolutionpreparedasspecifiedinthemonographwithastandardcoloursolutionindicatedinthemonograph.Thecompositionof the standard colour solution is selected depending on the hue and intensity of the colour of thetestsolutioncorrespondingtothelimitspermittedinthespecifications.
Recommended procedureUnlessotherwisespecifiedinthemonograph,carryoutthecomparisoninflat-bottomedtubesoftransparentglassthatarematchedascloselyaspossibleininternaldiameterandinallotherrespects(tubesofabout16mminternaldiameteraresuitable).Use10mLofthetestsolutionand10mLofthestandardcoloursolution;thedepthofliquidshouldbeabout50mm.Thecolourofthetestsolutionisnotmoreintensethanthestandardcolourwhenvieweddowntheverticalaxisofthetubesindiffusedlightagainstawhitebackground.
Stock colour standard solutionsYellow stock standard TSTo9.5mLofcobaltcolourTS,add1.9mLofcoppercolourTS,10.7mLofdichromatecolourTS,4.0mLofironcolourTS,diluteto100.0mLwithsulfuricacid(~10g/L)TSandmix.
Red stock standard TSTo40.5mLofcobaltcolourTS,add6.1mLofcoppercolourTS,6.3mLofdichromatecolourTS,12.0mLofironcolourTS,diluteto100.0mLwithsulfuricacid(~10g/L)TSandmix.
Green stock standard TSTo3.5mLofcobaltcolourTS,add20.1mLofcoppercolourTS,10.4mLofdichromatecolourTS,4.0mLofironcolourTS,diluteto100.0mLwithsulfuricacid(~10g/L)TSandmix.
Brown stock standard TSTo35.0mLofcobaltcolourTS,add17.0mLofcoppercolourTS,8.0mLofdichromatecolourTS,diluteto100.0mLwithironcolourTSandmix.
Standard colour solutionsThe standard colour solution is prepared by suitably diluting the stock standard solutions (yellow,red,greenandbrownstockstandardTS)withsulfuricacid(~10g/L)TS.Thedesignationofthestandardcoloursolutioniscomposedoftwolettersindicatingthestockstandardsolution(Ywforyellow,Rdforred,GnforgreenandBnforbrown)andofanumberdescribingthedilutionasgivenbelow:
Dilution number for standard
colour solutions
Stock standard solution
(mL)
Sulfuric acid (~10g/L) TS
(mL)0 0.78 99.221 1.56 98.442 3.12 96.883 6.25 93.754 12.50 87.505 25.00 75.006 50.00 50.007 100.00 -
Standardcoloursolutionnumbers4–7maybestoredinsealedglasscontainers,protectedfromsunlightbutthemoredilutestandardcoloursolutionsshouldbepreparedasrequired.

473
WHODrugInformationVol.30,No.3,2016 Consultation documents
Definitionof“colourless”AsolutionisconsideredcolourlessifitisnotmoreintenselycolouredthananyofthestandardcoloursolutionsBn0,Yw0,Gn0orRd0.
1.11.2DegreeofcolourationofliquidsThis text is reproduced from the EuropeanPharmacopoeia with permission and with appropriate editorial modifications.
[Note from the Secretariat. The permission will be requested when the text is adopted by the WHO Expert Committee on Specifications for Pharmaceutical Preparations.]
Theexaminationofthedegreeofcolorationofliquidsintherangebrown-yellow-rediscarriedoutbyoneofthe2methodsbelowasprescribedinthemonograph.
A solution is colourlessifithastheappearanceofwaterRorthesolventorisnotmoreintensely coloured than reference solution B9.
METHOD IUsingidenticaltubesofcolourless,transparent,neutralglassof12mmexternaldiameter,compare2.0mLoftheliquidtobeexaminedwith2.0mLofwaterRorofthesolventorofthereferencesolution(seetablesofreferencesolutions)prescribedinthemonograph.Comparethecoloursindiffuseddaylight,viewinghorizontallyagainstawhitebackground.
METHOD IIUsingidenticaltubesofcolourless,transparent,neutralglasswithaflatbaseandaninternaldiameterof15mmto25mm,comparetheliquidtobeexaminedwithwaterRorthesolventorthereferencesolution(seetablesofreferencesolutions)prescribedinthemonograph,thedepthofthelayerbeing40mm.Comparethecoloursindiffuseddaylight,viewingverticallyagainst a white background.
REAGENTS
Primary solutions
Yellow solution.Dissolve46gofferricchlorideRinabout900mLofamixtureof25mLofhydrochloricacid(~330g/L)TSand975mLofwaterRanddiluteto1000.0mLwiththesamemixture.Titrateandadjustthesolutiontocontain45.0mgofFeCl3,6H2OpermLbyaddingthesameacidicmixture.Protectthesolutionfromlight.Titration.Placeina250mLconicalflaskfittedwithaground-glassstopper,10.0mLofthesolution,15mLofwaterR,5mLofhydrochloricacid(~330g/L)TSand4gofpotassiumiodideR,closetheflask,allowtostandinthedarkfor15minutesandadd100mLofwaterR.Titratetheliberatediodinewithsodiumthiosulfate(0.1mol/L)VS,using0.5mLofstarchsolutionTS,addedtowardstheendofthetitration,asindicator.1mLofsodiumthiosulfate(0.1mol/L)VSisequivalentto27.03mgofFeCl3,6H2O.
Red solution.Dissolve60gofcobalt(II)chlorideRinabout900mLofamixtureof25mLofhydrochloricacid(~330g/L)TSand975mLofwaterRanddiluteto1000.0mLwiththesamemixture.Titrateandadjustthesolutiontocontain59.5mgofCoCl2,6H2OpermLbyaddingthesameacidicmixture.
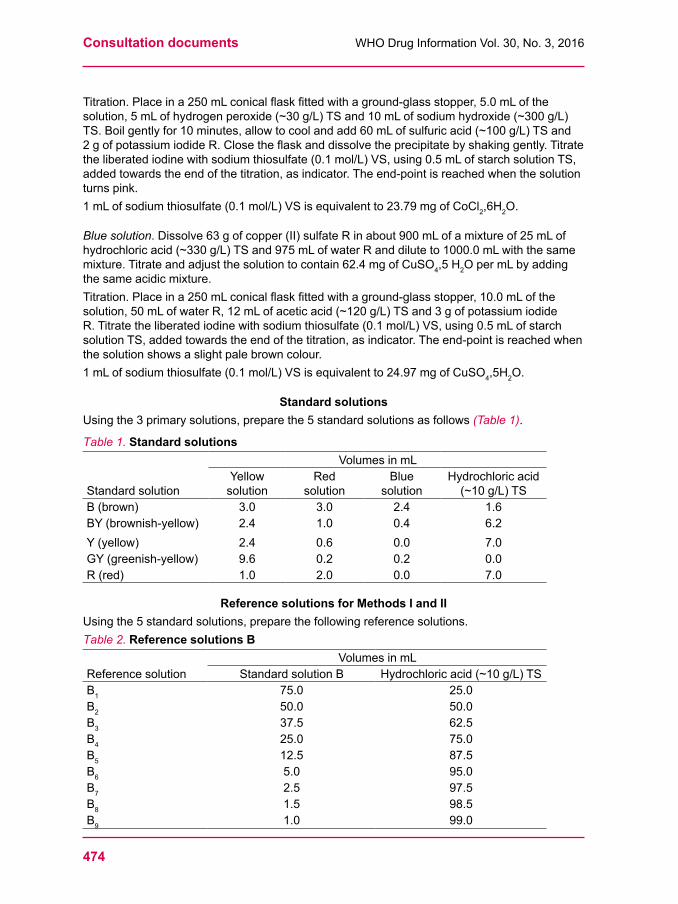
Consultation documents WHODrugInformationVol.30,No.3,2016
474
Titration.Placeina250mLconicalflaskfittedwithaground-glassstopper,5.0mLofthesolution,5mLofhydrogenperoxide(~30g/L)TSand10mLofsodiumhydroxide(~300g/L)TS.Boilgentlyfor10minutes,allowtocoolandadd60mLofsulfuricacid(~100g/L)TSand2gofpotassiumiodideR.Closetheflaskanddissolvetheprecipitatebyshakinggently.Titratetheliberatediodinewithsodiumthiosulfate(0.1mol/L)VS,using0.5mLofstarchsolutionTS,addedtowardstheendofthetitration,asindicator.Theend-pointisreachedwhenthesolutionturns pink.1mLofsodiumthiosulfate(0.1mol/L)VSisequivalentto23.79mgofCoCl2,6H2O.
Blue solution.Dissolve63gofcopper(II)sulfateRinabout900mLofamixtureof25mLofhydrochloricacid(~330g/L)TSand975mLofwaterRanddiluteto1000.0mLwiththesamemixture.Titrateandadjustthesolutiontocontain62.4mgofCuSO4,5H2OpermLbyaddingthesameacidicmixture.Titration.Placeina250mLconicalflaskfittedwithaground-glassstopper,10.0mLofthesolution,50mLofwaterR,12mLofaceticacid(~120g/L)TSand3gofpotassiumiodideR.Titratetheliberatediodinewithsodiumthiosulfate(0.1mol/L)VS,using0.5mLofstarchsolutionTS,addedtowardstheendofthetitration,asindicator.Theend-pointisreachedwhenthe solution shows a slight pale brown colour.1mLofsodiumthiosulfate(0.1mol/L)VSisequivalentto24.97mgofCuSO4,5H2O.
Standard solutionsUsingthe3primarysolutions,preparethe5standardsolutionsasfollows(Table 1).
Table 1. Standard solutions
Standardsolution
VolumesinmLYellow
solutionRed
solutionBlue
solutionHydrochloric acid (~10g/L)TS
B (brown) 3.0 3.0 2.4 1.6BY (brownish-yellow) 2.4 1.0 0.4 6.2Y (yellow) 2.4 0.6 0.0 7.0GY (greenish-yellow) 9.6 0.2 0.2 0.0R (red) 1.0 2.0 0.0 7.0
Reference solutions for Methods I and IIUsingthe5standardsolutions,preparethefollowingreferencesolutions.Table 2. Reference solutions B
Reference solutionVolumesinmL
StandardsolutionB Hydrochloricacid(~10g/L)TSB1 75.0 25.0B2 50.0 50.0B3 37.5 62.5B4 25.0 75.0B5 12.5 87.5B6 5.0 95.0B7 2.5 97.5B8 1.5 98.5B9 1.0 99.0
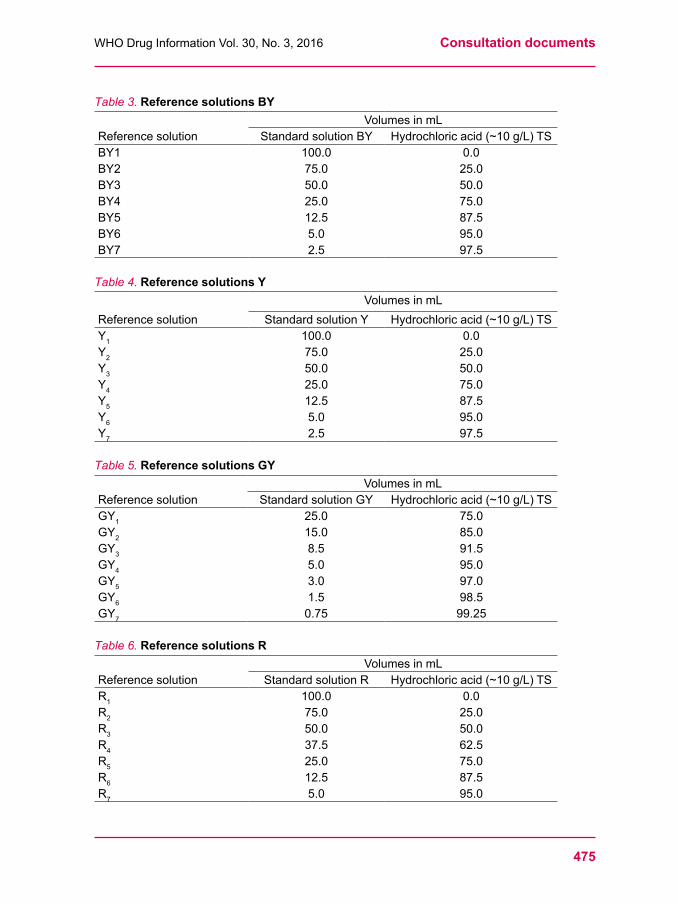
475
WHODrugInformationVol.30,No.3,2016 Consultation documents
Table 3. Reference solutions BY
Reference solutionVolumesinmL
StandardsolutionBY Hydrochloricacid(~10g/L)TSBY1 100.0 0.0BY2 75.0 25.0BY3 50.0 50.0BY4 25.0 75.0BY5 12.5 87.5BY6 5.0 95.0BY7 2.5 97.5
Table 4. Reference solutions Y
Reference solutionVolumesinmL
StandardsolutionY Hydrochloricacid(~10g/L)TSY1 100.0 0.0Y2 75.0 25.0Y3 50.0 50.0Y4 25.0 75.0Y5 12.5 87.5Y6 5.0 95.0Y7 2.5 97.5
Table 5. Reference solutions GY
Reference solutionVolumesinmL
StandardsolutionGY Hydrochloricacid(~10g/L)TSGY1 25.0 75.0GY2 15.0 85.0GY3 8.5 91.5GY4 5.0 95.0GY5 3.0 97.0GY6 1.5 98.5GY7 0.75 99.25
Table 6. Reference solutions R
Reference solutionVolumesinmL
StandardsolutionR Hydrochloricacid(~10g/L)TSR1 100.0 0.0R2 75.0 25.0R3 50.0 50.0R4 37.5 62.5R5 25.0 75.0R6 12.5 87.5R7 5.0 95.0
Consultation documents WHODrugInformationVol.30,No.3,2016
476
StorageForMethodIthereferencesolutionsmaybestoredinsealedtubesofcolourless,transparent,neutralglassof12mmexternaldiameter,protectedfromlight.
ForMethodIIpreparethereferencesolutionsimmediatelybeforeusefromthestandardsolutions.
Reagents to be establishedStarch solution TS Triturate1.0gofsolublestarchRwith5mLofwaterRandwhilststirringpourthemixtureinto100mLofboilingwaterRcontaining10mgofmercuriciodideR.
NOTE:commerciallyavailablereagentsmaybeused;includingmercury-freesolutionsorthosecontainingalternativepreservatives.
Carryoutthetestforsensitivityeachtimethereagentisused.
Testforsensitivity.Toamixtureof1mLofthestarchsolutionand20mLofwaterR,addabout50mgofpotassiumiodideRand0.05mLofiodinesolutionTS.Thesolutionisblue.gentstobe established
Hydrogen peroxide (~30 g/L) TSAsolutioninwatercontainingabout30gofH2O2perlitre.
Hydrochloric acid (~10 g/L) TSHydrochloricacid(~250g/L)TS,dilutewithwatertocontain10gofHClin1000mL.
Iodine solution TS To10.0mLofMiodine(0.05mol/L)VSadd0.6gofpotassiumiodideRanddiluteto100.0mLwithwaterR.Prepareimmediatelybeforeuse.
***





























