Embed Size (px)
Citation preview
1
WHO Drug Information Vol. 31, No. 1, 2017
Contents
Collaboration3 Global network of national vaccine control
laboratories
11 The Self-medication Collaborative Asian Regulator Expert Roundtable (Self-CARER)
Norms and standards15 70 years of WHO standards on medicines
quality
Vaccine control27 Feasibility of a serological potency assay for
rabies vaccines for human use
Safety news30 Safety warnings
Belladonna-containing teething products:
risk to children; Hyoscine butylbromide injection: serious adverse events in patients with underlying heart
disease; Lenalidomide: reactivation of hepatitis B virus ; Canagliflozin and other SLGT2 inhibitors: risk of amputations; Gadolinium-based contrast agents: accumulation in the brain;
31 RestrictionsDienogest and ethinylestradiol: can be used for acne as a last resort;
32 Known risksChlorhexidine gluconate: serious allergic reactions; Fluoroquinolones:
severe, disabling side effects; Interferon beta-1b: thrombotic damage in small blood vessels; Menthol-containing topical analgesics: serious skin burns ; Tramadol: risk of serious breathing problems; Varenicline and bupropion: risks said to be lower than expected;
34 Herbal productsToxic alkaloids in plant-based products ;
34 Reviews startedCertain anaesthetics and sedatives; Selexipag; Systemic and inhaled quinolones and fluoroquinolones
35 Non-compliance with good practices Micro Therapeutic Research Labs Pvt Ltd, India; Chongqing Pharma Research Institute, China (and 11 others)
Regulatory news36 Vision statement
Japan announces Rational Medicine initiative
36 Pre-market assessmentTen years of EMA conditional marketing authorizations
37 Post-market monitoringAustralia to publish laboratory testing results; India releases medicines quality survey results
38 Antimicrobial resistanceTwo reports on antimicrobial resistance in Europe; Regulatory statement and new guidelines on antibiotic use in India
39 BiosimilarsEMA advice on development of biosimilars; FDA guidance on naming of biologicals
40 Substance useOpioid control in Canada
40 CollaborationLandmark EU– U.S. agreement on inspections; IGDRP roadmap to 2020; IGDRP biowaiver template; ASEAN joint assessment pilot
41 Under discussion
43 Approved
Plecanatide: for chronic idiopathic constipation; Telotristat ethyl: for carcinoid syndrome diarrhoea; Crisaborole: for atopic dermatitis;
Parathyroid hormone replacement therapy;
Rucaparib: for certain ovarian cancers; Nusinersen: for spinal muscular atrophy; Sublingual dust mite allergen extract; Sodium zirconium cyclosilicate: for hyperkalaemia; Two adalimumab biosimilars;
Three clinically important generics approved in China; Two tests for guiding antibiotic use
45 Extension of indicationsElvitegravir & cobicistat & emtricitabine & tenofovir: for children over 12 years of age
Publications and events46 Research and development
WHO publishes priority list of antibiotic-resistant pathogens
46 Access to medicinesIntellectual property rules amended to ease global access to medicines; OECD reports on health spending and new technologies; Calls for changes to European Commission’s R&D programme; Using human rights law to support access to medicines; First MPP licence for anti-tuberculosis medicine
Continued
WHO Drug Information

2
WHO Drug Information Vol. 31, No. 1, 2017
48 Medicines controlPapillomavirus vaccine review documents published ; New CIOMS guide on active vaccine surveillance ; Measuring pharmaceutical systems strengthening; Spotlight on flawed bioequivalence trials in India
49 Medicines useOver- and underuse of health care interventions
50 Disease updatesMalaria: global targets jeopardized; Ebola: vaccine shown to be effective; Polio: public health emergency continues; Cancer: WHO calls for early diagnosis;
51 WHO mattersWHO data portal on health coverage; WHO Director-General supports new prequalification funding model; New medicines invited for prequalification; New WHO prequalification website
52 Upcoming events2017 joint UNICEF–UNFPA–WHO manufacturers meeting
Consultation documents53 The International Pharmacopoeia 53 Ganciclovir58 Ganciclovir for injection
International Nonproprietary Names (INN)61 Recommended INN: List 77
Continued
Abbreviations and web sites
CHMP Committee for Medicinal Products for Human Use (EMA)EMA European Medicines Agency (www.ema.europa.eu)EU European UnionFDA U.S. Food and Drug Administration (www.fda.gov)Health Canada Federal department responsible for health product regulation in Canada (www.hc-sc.gc.ca)IGDRP International Generic Drug Regulators Programme (https://www.igdrp.com)MHLW Ministry of Health, Labour and Welfare, JapanMHRA Medicines and Healthcare Products Regulatory Agency, United Kingdom
(www.mhra.gov.uk)Medsafe New Zealand Medicines and Medical Devices Safety Authority (www.medsafe.govt.nz)PRAC Pharmacovigilance Risk Assessment Committee (EMA)PMDA Pharmaceuticals and Medical Devices Agency, Japan (www.pmda.go.jp/english/index.htm)Swissmedic Swiss Agency for Therapeutic Products (www.swissmedic.ch)TGA Therapeutic Goods Administration, Australia (www.tga.gov.au)U.S. United States of America WHO World Health Organization (www.who.int)WHO EMP WHO Essential medicines and health products (www.who.int/medicines/en/)WHO PQT WHO Prequalification team (https://extranet.who.int/prequal/)
Note:The online version of this issue (freely available at www.who.int/medicines/publications/druginformation) has direct clickable hyperlinks to the documents and web pages referenced.

3
WHO Drug Information Vol. 31, No. 1, 2017
CollaborationGlobal network of national vaccine control laboratories
Immunization is one of the most cost-effective public health interventions. However, vaccines are complex biological products that need comprehensive regulatory oversight, including control of each lot released onto the market. For WHO-prequalified vaccines, lot release is under the responsibility of the authority with the regulatory oversight of the respective vaccine, which is usually the national regulatory authority (NRA) of the producing country.
Lot release testing of vaccines is becoming more demanding and resource-intensive as globalization and scientific advances progress, making it necessary for national control laboratories (NCLs) to collaborate in order to ensure the timely supply of quality-assured vaccines to countries. With this in mind, WHO has brought together representatives of NCLs involved in testing of WHO-prequalified vaccines, industry and other stakeholders to explore the potential for more extensive sharing of work and information. A network of NCLs responsible for release of WHO-prequalified vaccines was established.
Background
Assuring the quality of vaccinesEnsuring the consistent safety and efficacy of vaccines is critical for the success of immunization programmes. It is also essential for continued public confidence in these programmes, enabling adequate immunization coverage to be achieved and maintained.
To facilitate access to needed vaccines of assured quality the WHO Prequalification Team (PQT) prequalifies vaccines for procurement by UN agencies according to a defined procedure (1). The outcomes are also used by governments and international organizations.
Vaccines are complex biological products with inherent variability between produced batches. A prerequisite for acceptance of applications for WHO prequalification is,
This article is based on the report of a meeting convened by the WHO Group for Technical Assistance and Laboratory Services (TAL) and coordinated by Dr Ute Rosskopf, WHO Department of Essential Medicines and Health Products (EMP), with input from Mrs Monika Zweygarth (consultant, WHO-EMP). The meeting was held in Lage Vuursche (Bilthoven), the Netherlands, on 30 August–2 September 2016 and was organized jointly with the Dutch National Institute for Public Health and the Environment (RIVM) through Dr Martijn Bruysters. The organizers thank the Government of the Netherlands and the United States Agency for International Development (USAID) for their financial contributions towards this event. We thank Dr Alireza Khadem Broojerdi from WHO Regulatory Systems Strengthening for helpful comments on the manuscript.Questions and comments on this article are welcome and can be addressed to Dr Ute Rosskopf ([email protected]).
Collaboration WHO Drug Information Vol. 31, No. 1, 2017
4
therefore, that the regulatory authority of the producing country is proven functional with regard to regulatory oversight of vaccines. Two of the nine common functions assessed by WHO1 are the access to a functional vaccine control laboratory and the ability to perform lot release, including risk-based laboratory testing, to confirm that each batch meets the specifications of its marketing authorization before it is released onto the market. This regulatory function, NRA lot release, is unique to vaccines and a few other biological products.
For WHO-prequalified vaccines intended for use in UN-funded programmes, lot release is conducted in accordance with WHO guidelines (2) by the NRA of the producing country as the responsible authority. In addition, the WHO Technical Assistance and Laboratory Services (TAL) Group coordinates the testing of vaccines submitted for prequalification (verification of quality in support of prequalification decision) and the targeted testing, by WHO-contracted NCLs2, of vaccine lots supplied to countries by UN agencies.
WHO collaborative activitiesWith increasing globalization and continuous scientific advances, quality
1 The nine common functions are defined in the WHO Global Benchmarking Tool, which is being phased in. They are:1. National regulatory system;2. Registration and marketing authorization;3. Vigilance;4. Market surveillance and control;5. Licensing premises;6. Regulatory inspection;7. Laboratory access and testing;8. Clinical trials oversight; and9. NRA lot release.
2 A list of contracted laboratories is available on the WHO website at www.who.int/immunization_standards/vaccine_quality/contracted_labs_vaccines/en/
assurance of vaccines is becoming more demanding. Challenges with regard to lot release of vaccines were discussed at a 2007 WHO/Health Canada consultation (3), where it was noted that the increased volume of vaccines being licensed and in use, the increasing complexity of new vaccines requiring more sophisticated tests and the increasing globalization of vaccine production created an increasing burden for NRAs and industry.
In response to these challenges WHO-PQT has initiated a range of activities to promote collaboration and work-sharing. A streamlined vaccine prequalification procedure (1) was introduced with effect from February 2012, allowing for case-by-case reliance on assessment reports, testing results and/or inspection reports shared by NRAs under specific collaboration agreements. To increase the efficiency of testing WHO-TAL has increased the number of its contracted laboratories, optimized the testing logistics, and invested in harmonization of test methodologies with hands-on training courses and information exchange (4). Since 2014, 16 agreements have been signed with manufacturers of prequalified vaccines, allowing the releasing NCLs to share the data gathered during their independent national lot release as part of their annual reporting to WHO.
First global network meetingBuilding on these collaborative activities, WHO-TAL initiated and coordinated a first kick-off networking meeting to create a strategic platform for NCLs to collaborate and share information. The meeting was jointly organized with the Dutch National Institute for Public Health and the Environment (RIVM). Representatives from national laboratories involved in testing WHO-prequalified
Global network of national vaccine control laboratories
5
WHO Drug Information Vol. 31, No. 1, 2017 Collaboration
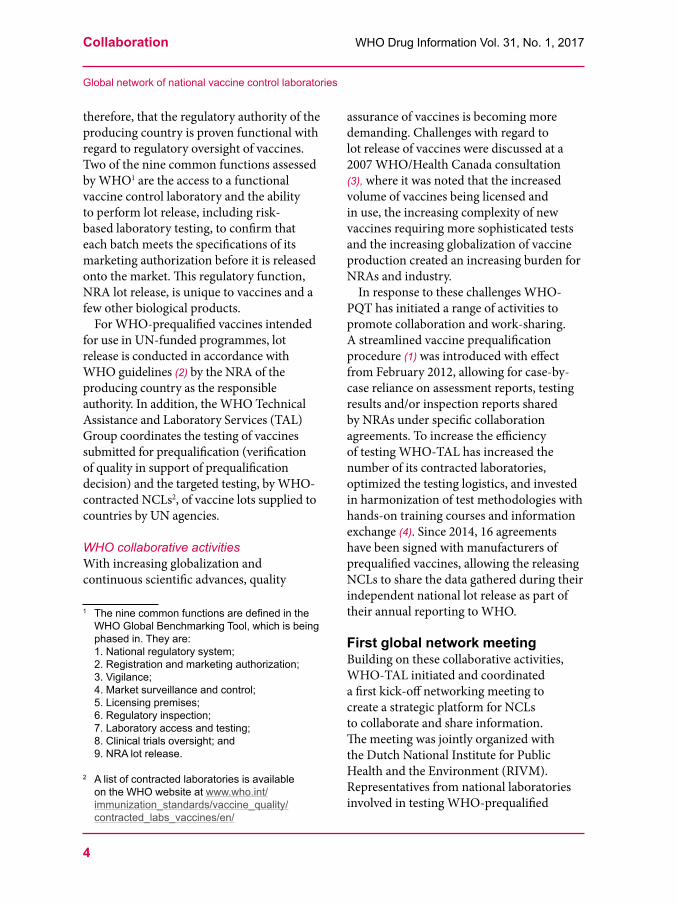
vaccines, industry associations and other stakeholders met on 30 August–2 September 2016 in Lage Vuursche, the Netherlands, to exchange information on their vaccine control strategies and explore opportunities to promote convergence. This was the first meeting of national vaccine control laboratories that had a global reach, with participation from NCLs in five of the six WHO regions (Table 1).
Lot release activities The laboratory representatives described the lot release activities performed at their institutions. The number of batches released per year at each NCL ranged from just over 100 to several thousand; an increasing trend was reported from several countries. All laboratories reported that they work according to ISO 17025 standards. Most were accredited, one had an audit-based system and one was working towards
accreditation. All laboratories reported being engaged in international and regional collaboration initiatives; collaborative studies and joint audits were highlighted as being particularly useful exercises.
Lot release proceduresReview of the lot summary protocol was part of the lot release procedure in all countries. For imported vaccines there was some reliance on the lot release by the responsible regulatory authorities in producing countries, particularly those affiliated to the International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH).
Some laboratories reported using different release certificates for the domestic market and for export, while others stated that they use the same testing schedules for all samples, as they do not know which samples are intended for export.
Table 1: Participating national vaccine control laboratoriesRegion Country (a) (b) (c) Region Country (a) (b) (c)
Europe Belgium Yes Yes Yes Africa Senegal YesBulgaria Yes Yes South Africa No YesDenmark Yes Yes Americas Brazil YesFrance Yes Yes Yes Canada Yes Yes PartiallyGermany Yes Yes Yes Cuba YesHungary No Yes(d) Yes United States(f) YesItaly Yes Yes Yes South East Asia India YesNetherlands Yes Yes Yes Indonesia YesSerbia No Thailand Yes YesSwitzerland No Yes Partially Western Pacific China YesUnited Kingdom Yes Yes(e) Yes Japan YesRussian Federation (f)
Yes Yes Republic of Korea
Yes Yes
Sweden(f) Yes Australia(f) YesLegend: (a) Country currently producing WHO-prequalified vaccine(s) (total: 22 countries)
(b) Laboratory is contracted by WHO for testing of vaccines (total: 12 contracted laboratories)(c) Laboratory uses the Official Control Authority Batch Release (OCABR) guidelines
(https://www.edqm.eu/en/human-ocabr-guidelines)(d) Laboratory formerly WHO-contracted(e) Two laboratories from the United Kingdom are WHO-contracted (f) Laboratory not represented at the meeting
“Global network of national vaccine control laboratories”

Collaboration WHO Drug Information Vol. 31, No. 1, 2017
6
Although all laboratories released batches of UN-procured vaccines according to WHO lot testing guidelines (2), it turned out that the actual lot release practices differed:• The decision to test was risk-based in
most countries, even where regulations require testing of all batches, as is the case in the EU and South Africa. In the Republic of Korea a risk-based system was introduced in April 2016. On the other hand, all batches of finished product and of drug substance are tested in the United Kingdom. Likewise, all batches are tested in Japan in line with public expectations; efforts are under way towards introducing a risk-based approach.
• The selection of lots for testing was based on the nature of the product and other factors such as consistency of production, product history – including inspection findings, complaints, adverse events following immunization (AEFI) – and change control. Some laboratories reported that they do not perform any testing at all for specific products which have been categorized as being of low risk.
• Where testing was performed, the percentage of lots tested ranged from 10% (or at least three lots per year) to 100% of batches released.
• The parameters tested were found to differ between countries. While some laboratories perform the full range of release tests in accordance with the manufacturer’s marketing authorization, the relevant WHO guideline or the pharmacopoeial monograph, others select critical parameters for testing based on the nature of the product and the laboratory’s technical capabilities. It was noted that certain tests, such as that for potency at the final bulk stage, can be performed in parallel with manufacturers’ tests to save time.
Manufacturers’ perspectiveRepresentatives of the International Federation of Pharmaceutical Manufacturers & Associations (IFPMA) and the Developing Countries Vaccine Manufacturers Network (DCVM) shared the manufacturers’ perspective. Manufacturers recognize the public health benefits of the independent lot release process and share the common goal to ensure timely availability of safe, efficacious and high quality vaccines.
Some prequalified vaccines are supplied to over 100 countries. Target countries have diverse national regulatory requirements, and many have requirements for full release testing of vaccine lots. Re-testing of the same batch in four or more recipient countries was said to be not uncommon. Often the testing provides no added value and can pose a risk of out-of-specification results that are not linked to actual product deficiencies. This creates significant barriers for manufacturers in supplying vaccines to end users.
In light of current regulatory developments, notably the move towards risk management and quality by design concepts, manufacturers are calling for risk-based testing as recommended in WHO guidelines (2) and for more reliance on the testing results of the competent authority in charge of the regulatory oversight of the product. The need for convergence of lot release requirements as a basis for information- and work-sharing was emphasized.
Discussions and outcomes
Best practice for lot releaseThe meeting participants noted that lot release is only one element of a more comprehensive oversight that includes a range of regulatory mechanisms such as licensing activities, market surveillance and
“Global network of national vaccine control laboratories”
7
WHO Drug Information Vol. 31, No. 1, 2017 Collaboration
inspection of production sites. They voiced their support for a move towards risk-based selection of lots and parameters for testing. It was further emphasized that unexpected findings in lot release testing should be investigated in close consultation with manufacturers.
There was general agreement that the same requirements should apply for vaccines released onto the local market and those for export, and that reliance on the batch release by the responsible NRA/NCL (usually that of the producing country) should be promoted.
Participants felt that a gradual convergence of lot release practices in line with WHO guidance (2) can be achieved by incorporating best practices into national guidelines. As a first step, the participating NCLs agreed to conduct a mapping exercise of the processes used in lot release of WHO-prequalified and other vaccines to complement the information that was shared during the meeting.
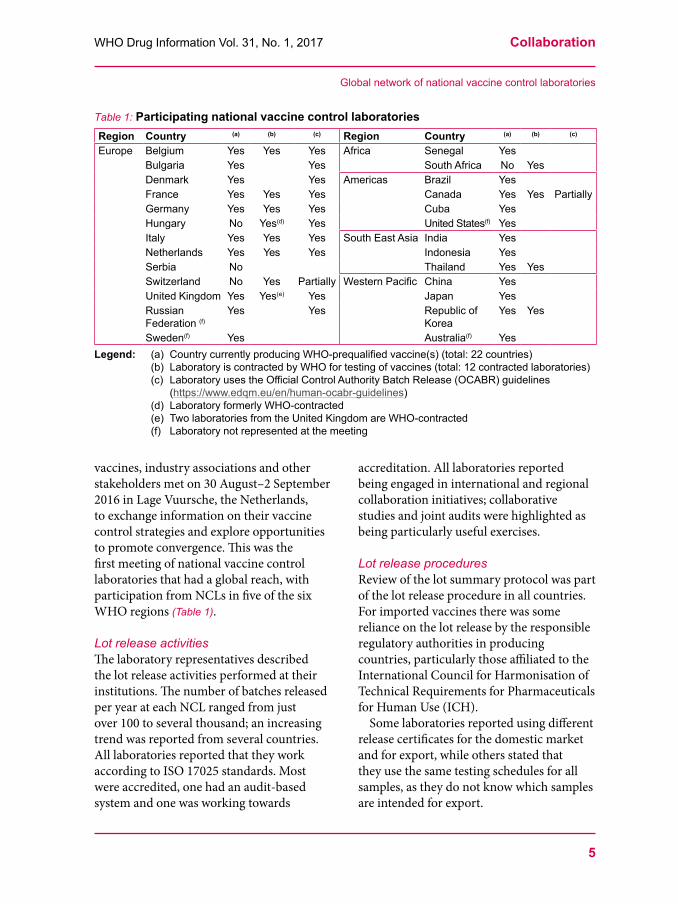
Lot release certificateRegulatory authorities/NCLs are required to issue a certificate of release for all lots of vaccines, including the prequalified vaccines that are distributed through United Nations agencies. An example (5) was reviewed at the meeting. A revised model template was proposed that can be used for all types of WHO-prequalified vaccines (Appendix 1). The proposed template includes a reference to Paragraph 7.3 of the WHO lot release guideline, which describes the role of lot release in the context of comprehensive regulatory oversight (Box 1), and mentions ISO 17025 as the common standard followed by the participating laboratories.
Information-sharingThe meeting participants considered various mechanisms to increase information-sharing among laboratories involved in testing of WHO-prequalified vaccines. It was proposed to adopt a structured, step-wise approach to information-sharing on an “as-needed” basis in consultation with manufacturers and with due arrangements to ensure confidentiality.
Box 1: Vaccine lot release in the context of comprehensive regulatory oversightFrom: WHO lot release guidelines (2), Paragraph 7.3: “The responsible national regulatory agencies (NRAs)/ national control laboratories (NCLs) are required to issue a certificate of release for vaccines that are distributed through United Nations agencies. Vaccines distributed through United Nations agencies are prequalified by WHO, to ensure that the products comply with the quality and safety standards established by the Organization. This release certificate is issued on the basis of, as a minimum, a review of the lot summary protocol for the relevant lot. The responsible NRA/NCL plays a key role in ensuring that products meet the specifications outlined in the marketing authorization and WHO recommendations. This is achieved by maintaining regulatory oversight, assessing and approving changes to manufacturing processes – including testing and specifications, compliance with good manufacturing practices (GMP) – and post-marketing surveillance of adverse events following immunization (AEFI). The release certificate issued by the responsible NRA/NCL should be forwarded by the United Nations agencies to the NRA/NCL of the receiving country, and the summary protocol will be provided upon request.”
“Global network of national vaccine control laboratories”

Collaboration WHO Drug Information Vol. 31, No. 1, 2017
8
The meeting itself was recognized as a starting point for this information-sharing as it established a common platform and provided a first overview of the participating NCLs’ strategies for vaccine control. By the end of 2017, shareable information could include the numbers of vaccine lots released as well as information relating to the laboratory testing, such as the risk-based considerations underlying the testing schedules. In the medium and long term, laboratories may go on to share lot release results and comparisons with manufacturer’s results, lot release certificates, and information on testing methodologies. The establishment of a secure and user-friendly electronic platform with access rights management for different user types will be considered.
Network of vaccine control laboratoriesThe meeting participants agreed to form a network of NCLs responsible for testing of WHO-prequalified vaccines, with the main objectives to promote information-sharing and convergence of lot release practices. The network may also serve to promote the “3R” principles – reducing, refining and replacing animal testing – as a means to make testing less variable and thus more efficient without compromising vaccine quality.
Draft terms of reference and management principles were agreed as follows at the meeting: Membership in the network is voluntary but strongly encouraged, and will be confirmed by the participating NCLs after the meeting. NCLs in countries that are recipients of UN-procured vaccines can join as associate members, while industry and other stakeholders can participate as observers.
An interim steering committee was appointed at the meeting. The first regular steering committee will be elected at the next
network meeting, which is planned to take place in India in the second half of 2017.
Conclusions With 194 Member States worldwide, WHO has a mandate to coordinate a strategic vaccine control laboratory network at the global level. The network established at the meeting has the potential to promote collaboration and reliance around the globe, considering that WHO-prequalified vaccines are used to immunize approximately two thirds of infants worldwide (6). The newly formed network will communicate its experience “upward”, providing input to WHO and national guidance to promote convergence of lot release practices, and “outward” to countries receiving WHO-prequalified vaccines in order to raise awareness and foster reliance on the release testing conducted by the network members. The potential benefits are significant. Convergence of lot release requirements and test protocols and minimization of redundant testing will help to increase access to quality-assured vaccines in WHO Member States, thus supporting the achievement of universal health coverage which is one of the targets in the United Nations’ health-related sustainable development goals.
References1 WHO. Procedure for assessing the
acceptability, in principle, of vaccines for purchase by United Nations Agencies. WHO Technical Report Series 978, Annex 6. Geneva: World Health Organization, 2010.
2 WHO. Guidelines for independent lot release of vaccines by regulatory authorities. Technical Report Series, 978, Annex 2. Geneva: World Health Organization, 2010.
3 WHO/Health Canada Consultation on Vaccine Lot Release. Meeting report. Ottawa, Canada, 28 February to 1 March 2007.
“Global network of national vaccine control laboratories”

9
WHO Drug Information Vol. 31, No. 1, 2017 Collaboration
4 Quality testing of vaccines. Hands-on training on a standardized protocol to test saccharide content of priority vaccines. WHO Drug Information 2016; 30(2): 176-9..
5 WHO Model certificate for the release of DT-based combined vaccines by NRAs. Appendix 2. In: Recommendations to assure the quality, safety and efficacy of DT-based combined vaccines. Technical Report Series 980, Annex 6. Geneva: World Health Organization; 2012.
6 Wood D, Dellepiane N. Twenty-five years of the WHO vaccines prequalification programme (1987–2012): Lessons learned and future perspectives. Vaccine, Volume 33, Issue 1, 1 January 2015, Pages 52–61. doi:10.1016/j.vaccine.2013.11.066.
“Global network of national vaccine control laboratories”
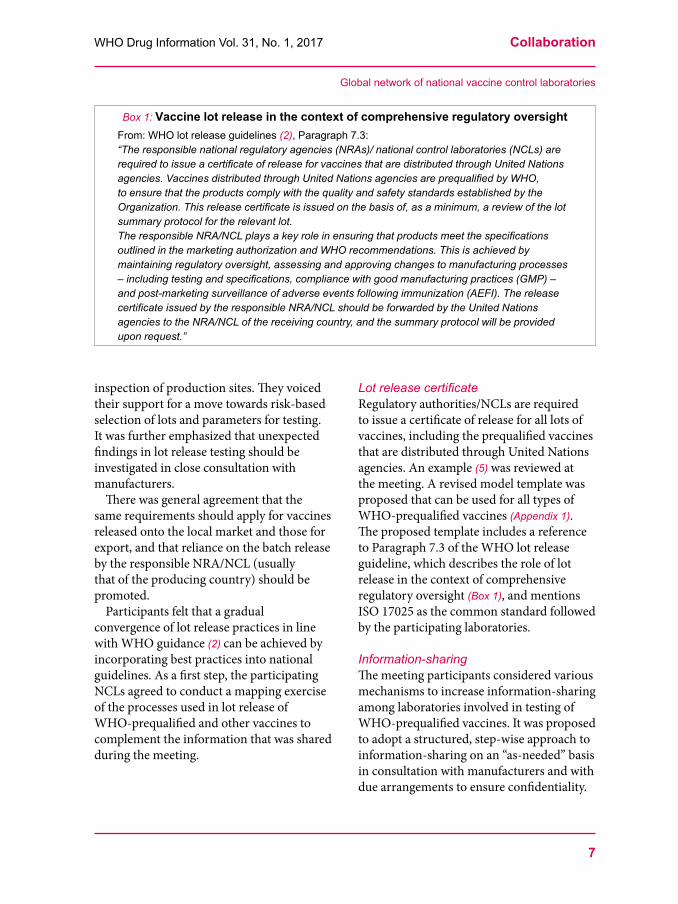
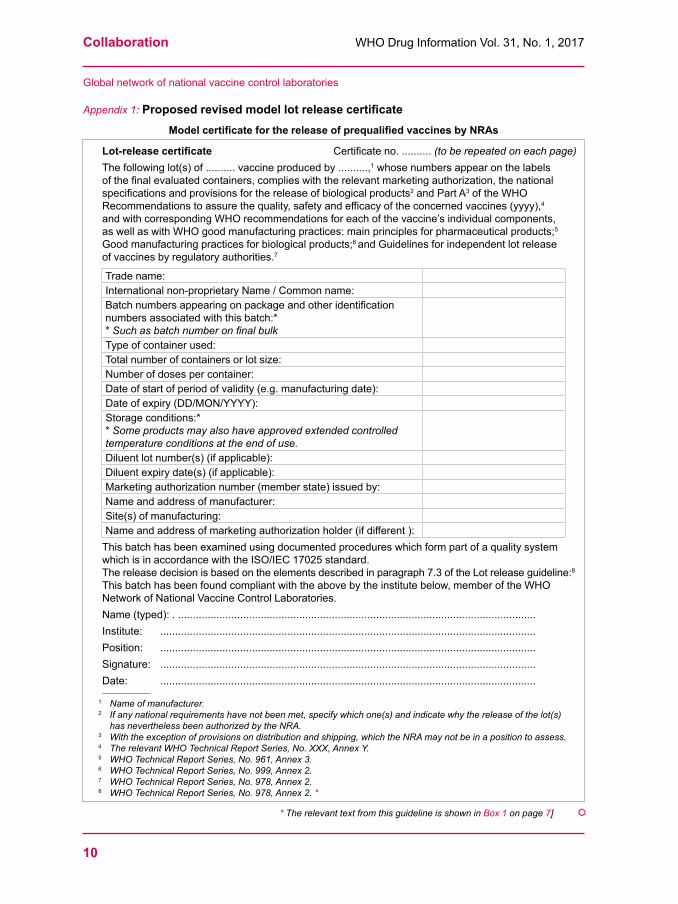
Appendix 1: Proposed revised model lot release certificate →
Collaboration WHO Drug Information Vol. 31, No. 1, 2017
10
Lot-release certificate Certificate no. .......... (to be repeated on each page)The following lot(s) of .......... vaccine produced by ..........,1 whose numbers appear on the labels of the final evaluated containers, complies with the relevant marketing authorization, the national specifications and provisions for the release of biological products2 and Part A3 of the WHO Recommendations to assure the quality, safety and efficacy of the concerned vaccines (yyyy),4 and with corresponding WHO recommendations for each of the vaccine’s individual components, as well as with WHO good manufacturing practices: main principles for pharmaceutical products;5 Good manufacturing practices for biological products;6 and Guidelines for independent lot release of vaccines by regulatory authorities.7
Trade name:International non-proprietary Name / Common name:Batch numbers appearing on package and other identification numbers associated with this batch:** Such as batch number on final bulkType of container used:Total number of containers or lot size:Number of doses per container:Date of start of period of validity (e.g. manufacturing date):Date of expiry (DD/MON/YYYY):Storage conditions:** Some products may also have approved extended controlled temperature conditions at the end of use.Diluent lot number(s) (if applicable):Diluent expiry date(s) (if applicable):Marketing authorization number (member state) issued by:Name and address of manufacturer:Site(s) of manufacturing:Name and address of marketing authorization holder (if different ):
This batch has been examined using documented procedures which form part of a quality system which is in accordance with the ISO/IEC 17025 standard.The release decision is based on the elements described in paragraph 7.3 of the Lot release guideline:8
This batch has been found compliant with the above by the institute below, member of the WHO Network of National Vaccine Control Laboratories.Name (typed): . ......................................................................................................................... Institute: ...............................................................................................................................Position: ...............................................................................................................................Signature: ...............................................................................................................................Date: ...............................................................................................................................________________
1 Name of manufacturer.2 If any national requirements have not been met, specify which one(s) and indicate why the release of the lot(s)
has nevertheless been authorized by the NRA.3 With the exception of provisions on distribution and shipping, which the NRA may not be in a position to assess.4 The relevant WHO Technical Report Series, No. XXX, Annex Y.5 WHO Technical Report Series, No. 961, Annex 3.6 WHO Technical Report Series, No. 999, Annex 2.7 WHO Technical Report Series, No. 978, Annex 2.8 WHO Technical Report Series, No. 978, Annex 2. *
“Global network of national vaccine control laboratories”
Appendix 1: Proposed revised model lot release certificateModel certificate for the release of prequalified vaccines by NRAs
* The relevant text from this guideline is shown in Box 1 on page 7] å

11
WHO Drug Information Vol. 31, No. 1, 2017 Collaboration
The Self-medication Collaborative Asian Regulator Expert Roundtable (Self-CARER)
The Self-medication Collaborative Asian Regulator Expert Roundtable (Self-CARER) is an international coalition of medicines regulatory authorities in the Asia Pacific region. It is a unique regulatory network in the sense that it deals with non-prescription medicines.
The Self-CARER members meet annually to devise coordinated and strategic plans to improve the effectiveness and efficiency of regulatory activities concerning self-care medicines in the region. Self-CARER is a non-binding forum devoted to fostering mutual public health and economic benefits in its member nations and regions through enhanced self-care medicine product regulation.
BackgroundThe regulations applicable to pharmaceutical products in the Asia Pacific region, including over-the-counter (OTC) and traditional medicines, vary significantly between regulatory authorities. Currently, the majority of health and medical product regulators in this region focus their attention and resources primarily on issues related to prescription products rather than non-prescription medicines. In connection with the activities described in this article, the term “self-care medicines” is used instead of more specific terms such as “OTC” (Box 1).
Unlike prescription drugs, self-care medicines do not necessarily need to be used under the supervision and guidance of a medical professional. As such, considering the reasons for which a given medicine is designated as a self-care medicinal product,
its review, registration, and post-approval regulation should be conducted within a framework that is optimized for this product category.(1) Success in this regard would increase the efficiency of self-care medicine product reviews and thus bring about needed improvements in public access to safe and efficacious non-prescription medicines throughout the Asia Pacific region.
To accomplish this goal, leaders of regulatory authorities in the region, with support from the corresponding industry association,(2) determined that greater international cooperation was necessary to identify mutually beneficial regulatory reforms, and that harmonization would then be integral to fully realizing the benefits of such reforms.
Authors: Ariel D Weber, JD, MS (1); Jun Kitahara, PhD (corresponding author) (1); Yoshihiro Katsura, PhD (1); Naoyuki Yasuda, MS (1)
(1) Pharmaceuticals and Medical Devices Agency (PMDA), Chiyoda-ku, Tokyo, JapanContact information for the corresponding author: Jun Kitahara, PhD, Office of International Programs,
Pharmaceuticals and Medical Devices Agency, Shin-Kasumigaseki Bldg., 3-3-2 Kasumigaseki, Chiyoda-ku, Tokyo 100-0013, Japan. Email: [email protected]
Collaboration WHO Drug Information Vol. 31, No. 1, 2017
12
The Self-CARER networkTo promote regulatory cooperation and harmonization in the area of self-care medicines, the Self-medication Collaborative Asian Regulator Expert Roundtable (Self-CARER) was formed in 2014. Chaired by the Thai Food and Drug Administration, it is the first platform to materialize cooperative efforts and opinion exchange between Asia Pacific regulators focused on self-care medicine products. The members of Self-CARER meet annually to discuss initiatives and concerns related to improving self-care medicine regulation in the Asia Pacific region in a non-binding, mutually respectful environment.
Past effortsTo date, Self-CARER has focused its activities on three major areas with the goal of realizing overall improvements in self-care medicine product regulation: (1) streamlining product review and registration, (2) establishing a shared directory of active pharmaceutical ingredients (APIs) found in self-care medicines, and (3) simplifying the criteria governing the reclassification of
prescription products to self-care medicine status.
Simplified registrationThe safety and efficacy profiles of most APIs used in self-care medicines have been established through evidence generated over many years of appropriate use. In some regulatory environments the physicochemical, quality, purity, and potency attributes of self-care medicine APIs are standardized in the form of pharmacopoeias or drug monographs. This practice allows for more rapid and consistent review and classification of self-care medicine products in comparison to prescription products, which require full-scale reviews.
Despite the differences between prescription-only and self-care medicines, various regulatory authorities in the Asia Pacific region use the same procedure to review applications for new self-care medicine products and those for switching from prescription-only status. This suggests that there is room for improvement in the efficiency of product reviews by such regulators.
Box 1: What are “self-care medicines”?In order to avoid misunderstanding over the meaning of over-the-counter (OTC) products, which can vary between regulatory authorities, the members of Self-CARER newly defined and adopted the term “self-care medicine” at the Self-CARER’s inaugural meeting. The new term refers to all OTC and off-the-shelf medicines usable by consumers to treat self-recognized minor injuries or illnesses. The members agreed to use this term in connection with all future Self-CARER activities and discussions. In relation to this definition, WHO defines “self-medication” as “the selection and use of medicines by individuals to treat self-recognised illnesses or symptoms.”(3)
Self-medication Collaborative Asian Regulator Expert Roundtable (Self-CARER)

13
WHO Drug Information Vol. 31, No. 1, 2017 Collaboration
At previous Self-CARER meetings, the members discussed options for simplified product registration following two potential models: abbreviated registration or a monograph system. The Self-CARER members are currently in ongoing discussions with the goal of producing various ideas for ways to simplify or streamline product reviews and registration systems. These ideas will take the form of model operating procedures that will serve to aid regulators in converging on mutually agreed-upon best practices. Ideas proposed thus far have included reforms such as exempting certain types of data from application requirements for self-care medicines, allocating dedicated review staff to self-care products to simultaneously build expertise and increase efficiency, adopting a monograph system, or establishing a framework for receiving and utilizing reference data from pre-defined reference regulatory authorities.
Ingredient directoryIn a departure from the status quo in which the different regulators each maintain their own databases, it has been proposed to establish a single database of APIs contained in self-care medicines. The primary advantages of such a shared repository include greater regulatory efficiency as well as mitigation of linguistic and cultural obstacles encountered through the use of the existing multiple parallel databases. However, although the members recognize the utility of a shared ingredient directory, various concerns remain such as how this initiative will be funded, what form of entity will be tasked with maintaining the database, and what types of content are most critical. Discussions between the members concerning potential solutions are currently ongoing.
Reclassification criteriaAnother common issue recognized by the members of Self-CARER is that the criteria used to reclassify or “switch” prescription-only medications to self-care medicine or off-the-shelf status are an important area for discussion.
The most common factors considered by Asia Pacific regulators in such applications for reclassification include the safety profile of a medicine under its approved use, the severity and frequency of adverse drug reactions, the pharmacokinetic and pharmacodynamic properties of the APIs, product indication(s), route(s) of administration, extent of use, time on the market, and risks when the product is misused. Sharing of information regarding these criteria among the members of Self-CARER would both increase the speed of application reviews by each regulator as well as improve the consistency of the review results.
ObstaclesSelf-CARER functions as a level field for discussions between the regulators of both developed and developing countries and regions on how to achieve greater effectiveness and efficiency in the regulation of self-care medicines. However, Self-CARER faces various challenges, such as:• Lack of specific review/registration
schemes for self-care medications, or of assigned dedicated review staff;
• Difficulty to achieve necessary legislation changes without disrupting routine operations;
• Scarce resources for necessary training of reviewers regarding evaluation processes and best practices for decision-making;
• Shortages of qualified review staff; and • Lack of a shared model for how to simplify
product review/registration procedures.
“Self-medication Collaborative Asian Regulator Expert Roundtable (Self-CARER)”

Collaboration WHO Drug Information Vol. 31, No. 1, 2017
14
To overcome these obstacles, Self-CARER is currently considering working with each of its members as needed to develop basic model regulatory frameworks that are still similar enough to those of other Asia Pacific regulators to promote streamlining and harmonization across the region.
Future goalsIn the years to come, Self-CARER plans to focus its efforts on overcoming its various challenges and bringing about both public health and economic benefits for its members. The network intends to prioritize policy adjustments that can increase regulatory efficiency by several means: creating a review scheme for self-care medicines that is separate from that used for
prescription-only products, devising ways to further streamline review processes, and developing concrete plans to expand the safe and effective use of self-care medicines.
References1 WHO. Guidelines for Regulatory Assessment
of Medicinal Products for use in Self-Medication. Geneva, Switzerland: World Health Organization; 2008.
2 Asia-Pacific Self-Medication Industry (APSMI). APSMI Activities [webpage]. Available at: www.apsmi.net/activities, accessed 21 February 2017.
3 WHO. The Role of the Pharmacist in Self-Care and Self-Medication. Report of the 4th WHO Consultative Group on the Role of the Pharmacist. The Hague, The Netherlands 26-28 August 1998. å
“Self-medication Collaborative Asian Regulator Expert Roundtable (Self-CARER)”
15
WHO Drug Information Vol. 31, No. 1, 2017
Norms and standards70 years of WHO standards on medicines quality
Expert Committee on Specifications for Pharmaceutical Preparations, 1947-2017: Addressing changing public health challenges
The Expert Committee on Specifications for Pharmaceutical Preparations advises the WHO Director-General and Member States on matters of medicines quality assurance. When it started its work in 1947 it focused on maintaining The International Pharmacopoeia. Its scope of work broadened and deepened over the years, reflecting the emergence of new approaches to quality management in pharmaceutical production and regulation. This article highlights the Committee’s main areas of work. A list of current guidelines and work in progress is provided in the Appendix.
BackgroundExpert Committees advise the WHO Director-General and Member States in technical areas related to public health. Their members are recruited from WHO’s Expert Advisory Panels. Stringent procedures are in place for their selection and for the management of conflicts of interest. The technical guidance adopted by the Committees is developed through a public consultation process. Once adopted, the guidelines are published as annexes to the Committees’ meeting reports in the WHO Technical Report Series (TRS).
The Expert Committee on Specifications for Pharmaceutical Preparations (ECSPP) is one of the WHO Expert Committees that meet regularly1. It advises the WHO 1 See www.who.int/about/collaborations/expert_
panels/en/. Others are the WHO Expert Committee on Biological Standardization (ECBS), the Joint FAO/WHO Expert Committee on Food Additives (JECFA), the WHO Expert Committee on Selection and Use of Essential Medicines and the WHO Expert Committee on Drug Dependence.
Director-General and Member States on quality assurance during the life cycle of medicines and in their regulation. In 2017 it looks back on seventy years of standard-setting work.
HistoryThe ECSPP was established as “Expert Committee on the Unification of Pharmacopoeias”. It met for the first time in 1947 (1), and the report of its fourth session was published in 1950 in the very first WHO Technical Report Series (2). At that time many of today’s WHO Member States were not yet part of WHO. Modern concepts of medicines quality assurance were only starting to emerge, often in response to unfortunate incidents with medicines that caused serious harm (Box 1).
The decades that followed saw the development of scientific approaches to ensure the quality, safety and efficacy of pharmaceutical products. However, many developing countries did not have the

Norms and standards WHO Drug Information Vol. 31, No. 1, 2017
16
resources to establish medicines regulatory authorities that could effectively protect the health of their populations.
The operations of the pharmaceutical industry are guided by the legal requirements in force in the target markets. In a globalized marketplace this often
means that high quality medicines are being produced for use in stringently regulated environments, while fewer requirements and lower standards are applied for medicines used elsewhere. Moreover, as starting materials and services are sourced from across the globe, local weaknesses in
Box 1: Medicines quality assurance: a timeline1937 Over 100 people in the U.S. die following
the use of an elixir which used diethylene glycol as a solvent without any safety testing
1937 League of Nations sets up a Technical Commission of Pharmacopoeial Experts
1938 U.S. Federal Food, Drug and Cosmetic Act introduced, with a premarket notification requirement for new drugs
1947 WHO Interim Commission takes over the work on pharmacopoeias from the League of Nations and reports on its first session
1948 First World Health Assembly establishes the “Expert Committee on the Unification of Pharmacopoeias” (renamed twice thereafter)
1956–60 Thalidomide marketed in 46 countries worldwide, leading to an estimated 10 000 babies being born with deformities
1962 New U.S. legislation requires proof of safety and efficacy before approval of new drug applications for the first time. FDA authorized to require compliance with current Good Manufacturing Practices (GMP)
1963 World Health Assembly adopts Resolution WHA16.36 on Clinical and pharmacological Evaluation of Drugs. U.K. Committee of Drug Safety established
1969 First WHO guidance on Good practices in the manufacture and quality control of drugs published with World Health Assembly Resolution WHA22.50, (following up on Resolutions WHA20.34 of 1967 and WHA21.37 of 1968)
1970 Pharmaceutical Inspection Convention (now: Pharmaceutical Inspection Cooperation Scheme, PIC/S) established, with GMP guidelines based on those of WHO
1975 Multistate procedure for medicines registration introduced in Europe, starting harmonization of medicines regulation
1984 U.S. legislation introduces bioequivalence studies for generic medicines in lieu of clinical efficacy and safety studies
1985 First international conference on essential medicines policies held in Nairobi, leading to the adoption of the WHO revised drug strategy
1989 At the Fifth International Conference of Drug Regulatory Authorities (ICDRA) Europe, Japan and U.S agree on action plans for harmonization. Pharmacopoeial Discussion Group formed
1990 International Conference for Harmonisation of Technical Requirements for Pharmaceuti-cals for Human Use (ICH) established
1990 First WHO Guiding principles for small national drug regulatory authorities published
2001 UN Secretary General Kofi Annan calls for a Global Fund to fight HIV, tuberculosis and other infectious diseases
2001 WHO prequalification of medicines launched to assess key medicines against WHO norms and standards
2005 WHO guideline on assessing bioequivalence of fixed-dose combinations published, supporting a global scale-up of antiretrovirals
2006 WHO Model Quality Assurance System for procurement agencies published, required for all Global Fund-financed health products
2008 WHO biowaiver procedure proposed2010 WHO introduces joint assessments with East
African Community and joint inspections2014 World Health Assembly Resolution
WHA67.20 makes the first-ever global-level call for Regulatory capacity-building
2015 EMA suspends over 700 products over concerns with their bioequivalence data
2016 WHO guideline on Good data and record management practices published
70 years of WHO standards on medicines quality

17
WHO Drug Information Vol. 31, No. 1, 2017 Norms and standards
regulatory control can have global impact. Today all the world’s regulatory authorities – including the well-established ones – are calling for cooperation and convergence of standards to close the regulatory gaps.
These developments have been shaping the need for comprehensive WHO guidance on medicines quality assurance that can be implemented in all Member States.
WHO technical guidanceIn the 70 years of its history the ECSPP has broadened its scope of work to cater for the changing needs. It has come to provide unified international norms and standards for all aspects of quality assurance in a medicine’s life cycle, supporting the global move towards convergence, collaboration and reliance among regulatory authorities. The current guidelines are listed in Appendix 1. An overview of the ECSPP’s work in the different areas is provided below.
Pharmacopoeial standardsMaintaining pharmacopoeial standards was the initial mandate of ECSPP. The first volume of The International Pharmacopoeia was published in 1951. The current Sixth Edition includes monographs for 439
pharmaceutical substances, 142 dosage forms and 27 radiopharmaceuticals, 174 infrared reference spectra, as well as monographs on general dosage forms, analytical methods and other supplementary texts. By providing publicly available standards for testing of commonly used medicines, many which are not included in any other pharmacopoeia, The International Pharmacopoeia fulfils a unique public health role.
Although “unification of pharmacopoeias” has been a goal since the Committee took up its work, the world’s pharmacopoeias have evolved separately. The WHO Index of World Pharmacopoeias2 lists pharmacopoeial authorities of 53 countries and two regions.
In 2012, WHO convened representatives of pharmacopoeias from 23 countries for the first time to discuss options for convergence of standards. The WHO international meetings of world pharmacopoeias became a regular event and have served as a forum to develop a guideline on Good Pharmacopoeial Practices (GPhP), published in 2016. By promoting collaboration among pharmacopoeias this 2 Available on the WHO webpage on Medicines
quality assurance, www.who.int/medicines/areas/quality_safety/quality_assurance/en/
Figure 1: The titles of fhe first (1) and fourth (2) reports of the WHO Expert Committee tasked with providing standards and specifications for medicines. The Committee was renamed “Expert Committee on International Pharmacopoeia” in 1951 and received its current name, “Expert Committee on Specifications of Pharmaceutical Preparations”, in 1959.
“70 years of WHO standards on medicines quality”

Norms and standards WHO Drug Information Vol. 31, No. 1, 2017
18
guidance is expected to lead to a prospective harmonization of standards, with significant potential benefits for manufacturers and regulatory authorities.
Quality controlIn the early days of the ECSPP’s history quality control testing was the mainstay of medicines control. While the emphasis has shifted away from pre-market testing towards an ongoing control whether batches supplied meet the agreed specifications, quality control testing remains an important regulatory function. At a time when shortages of various types of medicines are a persistent concern, efficient quality monitoring is critical for continued supply of products.
WHO provides detailed guidance on all aspects of laboratory testing. In 1984 the Committee recommended that countries should set up national pharmaceutical quality control laboratories, and provided guidance on organization and staffing. The first text on good laboratory practice (GLP) followed in 1987 – last revised in 2010 – and a specific text for pharmaceutical microbiology laboratories was added in 2011. WHO prequalification of quality control laboratories was introduced in 2006 and is based on the standards adopted by the ECSPP.
Production and inspectionsWhen modern medicines regulation started to develop in the 1960s it was recognized that quality cannot be “tested into a product”. Instead it must be built into a product at every step of development and production. The regulatory paradigm has shifted from quality control of the finished product to control of the manufacturing processes, as verified in inspections.
Accordingly, the ECSPP took on the development of norms and standards for the manufacture of finished pharmaceutical
products and their active pharmaceutical ingredients (APIs). The first WHO guideline on good manufacturing practice (GMP) was published in 1969 (3) and formed the basis for the GMP text of the Pharmaceutical Inspection Convention (PIC) upon its establishment in 1970.
The WHO GMP guidance has been continuously updated and supplemented by guidance on specific aspects and for specific product types. The current texts reflect today’s focus on quality management systems with effective mechanisms to identify, quantify and manage risks throughout the entire life cycle of a medicine.
Guidance on GMP inspections and classification of deficiencies has also been updated to support collaboration and reliance, reducing the burden of inspections on both manufacturers and regulators. A text on desk reviews of inspection information is in preparation.
DistributionAs pharmaceutical operations have become globalized, active ingredients and finished products cross many borders before they reach the end users. Joint global efforts are needed to safeguard the quality of pharmaceuticals in the supply chains. WHO has provided guidelines on good practices for trade and distribution both for medicines and starting materials as well as good storage practices including for time-and temperature-sensitive products.
Procurement agencies play a crucial role in assuring the quality of medicines that they delivered. The WHO Model Quality Assurance System for procurement agencies (MQAS) was first adopted in 2006. It provides a comprehensive toolkit for procurement organizations to safeguard the quality of medicines at all stages, from the qualification of suppliers throughout purchasing, storage
“70 years of WHO standards on medicines quality”

19
WHO Drug Information Vol. 31, No. 1, 2017 Norms and standards
and distribution of the products. The MQAS was updated in 2014 with input from the major international organizations that procure and/or fund medicines.
Quality surveys through testing of samples provide information about the quality of medicines circulating on the market at a given time. They are useful to verify the effectiveness of other regulatory measures such as marketing authorization, inspections and post-marketing surveillance activities. The 2016 Guidelines on the conduct of surveys of the quality of medicines outline the steps to consider when preparing and conducting a sample testing survey.
Special methods are required to detect and test products that have been introduced into the supply chains with fraudulent intent. Responding to a need expressed by quality control laboratories in a survey, WHO proposes a new guidance on testing of suspected spurious, falsely-labelled, falsified and counterfeit medicines. This technical guidance complements the work of the Member State Mechanism on substandard/spurious/falsely-labelled/falsified/counterfeit (SSFFC) medical products, which was established in 20123 .
Good pharmacy practicePharmacists play an important role in delivering medicines to patients. WHO and the International Pharmaceutical Federation (FIP) have a long history of collaboration in providing guidelines on good pharmacy practice. The most recent addition is a “points to consider” document on preparing children-specific medicines that are not available as authorized products.
3 WHO Essential medicines and health products. WHO Member State Mechanism. www.who.int/medicines/regulation/ssffc/mechanism/en/
Regulation and prequalificationWork on the first WHO Guidelines for small drug regulatory authorities started in 1985 as a component of the Organization’s Revised Drug Strategy (4). The regulatory guidance adopted by the ECSPP has been completed and updated in line with evolving regulatory concepts. Unlike national and regional regulations, the WHO guidelines reflect global perspectives on issues such as stability of medicines across climatic zones, or the selection of comparator products when demonstrating bioequivalence of generics.
Comprehensive guidance has been generated by the Committee to underpin WHO prequalification of medicines.Established in 2001, when HIV treatment was unaffordable in the public sector of most WHO Member States, this programme has increased global access to affordable key medicines of assured quality. The WHO guidance on assessing bioequivalence of fixed-dose combinations, which was published in 2005, contributed significantly to scaling up global access to ARV therapy (5). Prequalification was subsequently extended to additional medicines categories. A procedure to prequalify APIs in their own right was introduced in 2009. Since 2013 WHO offers a collaborative registration procedure for WHO-prequalified medicines in participating countries, which accelerates the review process while ensuring that the stringent quality standards used in prequalification are maintained.
The WHO prequalification team provides important input to the ECSPP’s work from its experience with implementing stringent standards in a wide variety of settings. Several prequalification guidelines have been subsequently adapted for use by regulatory authorities.
With increasing globalization, digitalization and outsourcing of services,
“70 years of WHO standards on medicines quality”
Norms and standards WHO Drug Information Vol. 31, No. 1, 2017
20
new issues are emerging. An example are the recurring concerns about data integrity at contract research organizations that perform bioequivalence studies. The 2016 WHO Guideline on good data and record management practices is the first text of its kind globally to bring together the relevant information in one place, completing the existing good practice guidelines in the various areas (GXP).
Today, no regulatory authority can achieve its mandate without using smart ways of reviewing data and making decisions. 2015 saw the publication of the WHO guidelines on Good review practices intended to support Member States, including those with less mature regulatory systems. A more comprehensive, high level framework document on all aspects of Good regulatory practices is under development.
Reliance on the decisions of stringent regulatory authorities (SRA), defined as members or associates of ICH, is provided for in several WHO guidelines. As ICH is evolving to become a global organization, this definition need revisiting. At its 51st Meeting the ECSPP adopted an interim revised definition and noted the work being done towards new assessment approaches that will enable collaboration and reliance on regulatory authorities with proven efficiency in specific fields.
Regulatory capacity needs to be strengthened in additional areas, notably for medical devices, including diagnostics. This complex and growing product group is increasingly important for public health, yet few Member States regulate it fully. The 2016 WHO global model regulatory framework for medical devices comes at a time when there is significant scope for the introduction of unified standards in this area.
ConclusionWHO is the only organization with a mandate to protect global health. The development, establishment and promotion of international standards for pharmaceuticals are among the functions laid down in its constitution. Its technical guidance on medicines quality is designed to serve regulatory authorities of all Member States, as well United Nations agencies and other major international bodies. It provides a technical platform for convergence as recommended by the 17th International Conference of Drug Regulatory Authorities (ICDRA) (6). At a time when access to essential medicines is a pressing issue on the sustainable development agenda, the ECSPP’s standard-setting work makes a unique and critical contribution towards more equitable access to needed medicines of assured quality.
References1 WHO. Expert Committee on the Unification of
Pharmacopoeias: Report on the first session, held 13-17 October 1947, Palais des Nations, Geneva. WHO; 1947.
2 WHO. Technical Report Series No. 1. Expert Commmittee on the Unification of Pharmacopoeias. Report on the Fourth Session. Geneva, 20-30 April 1949. WHO; 1950.
3 Annex 12. In: Official Records of the World Health Organization. No. 176. Twenty-second World Health Assembly. Boston, Massachusetts, 8-25 July 1969. WHO; 1969.
4 Thirty-ninth World Health Assembly. WHO’s revised drug strategy: report by the Director-General. Geneva: WHO; 1986.
5 ‘t Hoen EF, Hogerzeil HV, Quick JD, Sillo HB. A quiet revolution in global public health: The World Health Organization’s Prequalification of Medicines Programme. J Public Health Policy. 2014 May;35(2):137-61.
6 17th International Conference of Drug Regulatory Authorities. WHO Drug Information. 2016; 30(4): 547-57.
“70 years of WHO standards on medicines quality”
21
WHO Drug Information Vol. 31, No. 1, 2017 Norms and standards
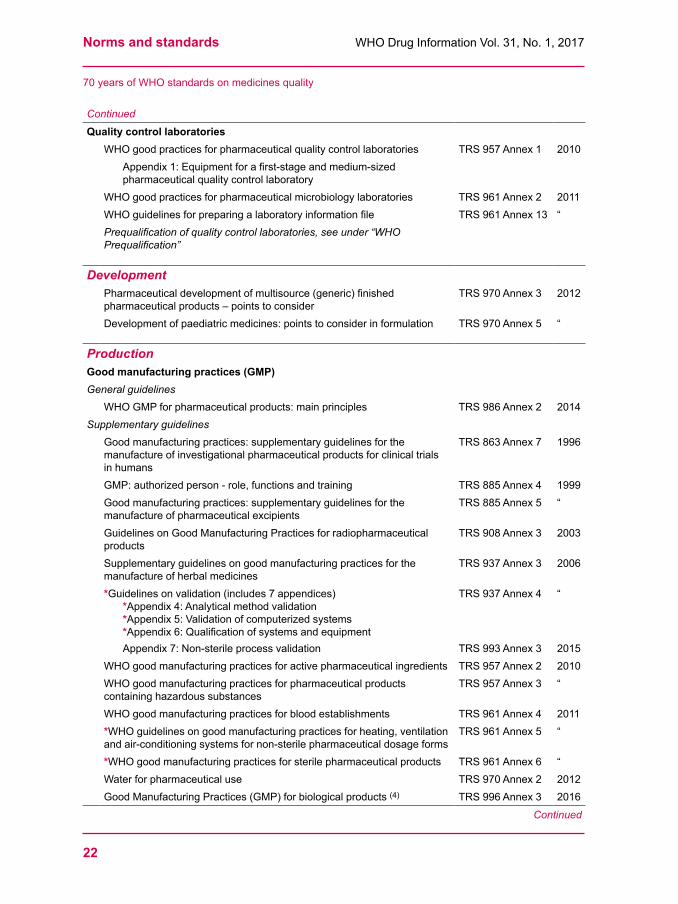
Appendix 1: WHO guidelines on medicines quality assuranceOnly the latest revised versions of the guidelines are listed. The guidelines shown under each heading are listed in chronological order of their adoption. The texts are available in the different sections of the WHO medicines “Guidelines” website (www.who.int/medicines/areas/quality_safety/quality_assurance/guidelines/en/), Texts marked with an asterisk (*) are under revision or under development. The draft texts or revisions are available in the public consultation section of the above website, titled “Current Projects”, at www.who.int/entity/medicines/areas/quality_safety/quality_assurance/projects/.
Quality controlPharmacopoeial standards and practicesThe International Pharmacopoeia, Sixth Edition (1) 2016
Recommendations on Risk of Transmitting Animal Spongiform Encephalopathy Agents via Medicinal Products
TRS 908 Annex 1 2003
The International Pharmacopoeia – related substances tests: dosage form monographs guidance notes
TRS 943 Annex 1 2007
General guidelines for the establishment, maintenance and distribution of chemical reference substances
TRS 943 Annex 3 “
List of available International Chemical Reference Substances and International Infrared Reference Spectra
TRS 953 Annex 1 2009
List of reference substances of other pharmacopoeias found to be suitable for use according to The International Pharmacopoeia
Living document (2)
Release procedure of International Chemical Reference Substances TRS 981 Annex 1 2013Procedure of the development of monographs and other texts for The International Pharmacopoeia
TRS 992 Annex 1 2015
Trade names of stationary phases found suitable in performing chromatographic tests described in The International Pharmacopoeia
Living document (3)
Updating mechanism for the section on radiopharmaceuticals in The International Pharmacopoeia
TRS 992 Annex 2 2015
Good pharmacopoeial practices*Glossary
TRS 996 Annex 1 2016
*The International Pharmacopoeia: revised concepts and future perspectives (Update of TRS 908, Annex 2)
To be published 2017
Quality control testing*Considerations for requesting analyses of drug samples TRS 902 Annex 4 2002*Model certificate of analysis TRS 902 Annex 10 “
Continued
(1) Available on CD ROM and on the WHO website at http://apps.who.int/phint/en/p/about/(2) Since 2010 the European Directorate for the Quality of Medicines & HealthCare (EDQM) is responsible
for the distribution of WHO’s International Chemical Reference Substances (ICRS). See www.who.int/medicines/areas/quality_safety/quality_assurance/qas_icrs/en/ for information on ICRS
(3) Available at www.who.int/medicines/publications/pharmacopoeia/en/
“70 years of WHO standards on medicines quality”
Norms and standards WHO Drug Information Vol. 31, No. 1, 2017
22
Continued
Quality control laboratoriesWHO good practices for pharmaceutical quality control laboratories TRS 957 Annex 1 2010
Appendix 1: Equipment for a first-stage and medium-sized pharmaceutical quality control laboratory
WHO good practices for pharmaceutical microbiology laboratories TRS 961 Annex 2 2011WHO guidelines for preparing a laboratory information file TRS 961 Annex 13 “Prequalification of quality control laboratories, see under “WHO Prequalification”
DevelopmentPharmaceutical development of multisource (generic) finished pharmaceutical products – points to consider
TRS 970 Annex 3 2012
Development of paediatric medicines: points to consider in formulation TRS 970 Annex 5 “
ProductionGood manufacturing practices (GMP) General guidelines
WHO GMP for pharmaceutical products: main principles TRS 986 Annex 2 2014Supplementary guidelines
Good manufacturing practices: supplementary guidelines for the manufacture of investigational pharmaceutical products for clinical trials in humans
TRS 863 Annex 7 1996
GMP: authorized person - role, functions and training TRS 885 Annex 4 1999Good manufacturing practices: supplementary guidelines for the manufacture of pharmaceutical excipients
TRS 885 Annex 5 “
Guidelines on Good Manufacturing Practices for radiopharmaceutical products
TRS 908 Annex 3 2003
Supplementary guidelines on good manufacturing practices for the manufacture of herbal medicines
TRS 937 Annex 3 2006
*Guidelines on validation (includes 7 appendices) *Appendix 4: Analytical method validation *Appendix 5: Validation of computerized systems *Appendix 6: Qualification of systems and equipment
Appendix 7: Non-sterile process validation
TRS 937 Annex 4
TRS 993 Annex 3
“
2015WHO good manufacturing practices for active pharmaceutical ingredients TRS 957 Annex 2 2010WHO good manufacturing practices for pharmaceutical products containing hazardous substances
TRS 957 Annex 3 “
WHO good manufacturing practices for blood establishments TRS 961 Annex 4 2011*WHO guidelines on good manufacturing practices for heating, ventilation and air-conditioning systems for non-sterile pharmaceutical dosage forms
TRS 961 Annex 5 “
*WHO good manufacturing practices for sterile pharmaceutical products TRS 961 Annex 6 “Water for pharmaceutical use TRS 970 Annex 2 2012Good Manufacturing Practices (GMP) for biological products (4) TRS 996 Annex 3 2016
Continued
“70 years of WHO standards on medicines quality”
23
WHO Drug Information Vol. 31, No. 1, 2017 Norms and standards
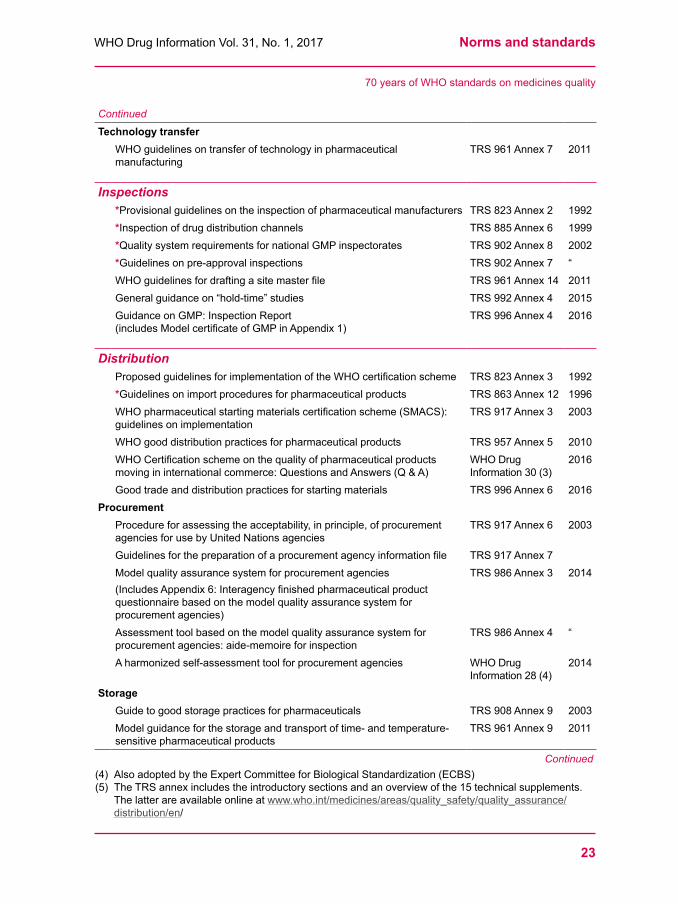
Continued
Technology transferWHO guidelines on transfer of technology in pharmaceutical manufacturing
TRS 961 Annex 7 2011
Inspections*Provisional guidelines on the inspection of pharmaceutical manufacturers TRS 823 Annex 2 1992*Inspection of drug distribution channels TRS 885 Annex 6 1999*Quality system requirements for national GMP inspectorates TRS 902 Annex 8 2002*Guidelines on pre-approval inspections TRS 902 Annex 7 “WHO guidelines for drafting a site master file TRS 961 Annex 14 2011General guidance on “hold-time” studies TRS 992 Annex 4 2015Guidance on GMP: Inspection Report(includes Model certificate of GMP in Appendix 1)
TRS 996 Annex 4 2016
DistributionProposed guidelines for implementation of the WHO certification scheme TRS 823 Annex 3 1992*Guidelines on import procedures for pharmaceutical products TRS 863 Annex 12 1996WHO pharmaceutical starting materials certification scheme (SMACS): guidelines on implementation
TRS 917 Annex 3 2003
WHO good distribution practices for pharmaceutical products TRS 957 Annex 5 2010WHO Certification scheme on the quality of pharmaceutical products moving in international commerce: Questions and Answers (Q & A)
WHO Drug Information 30 (3)
2016
Good trade and distribution practices for starting materials TRS 996 Annex 6 2016Procurement
Procedure for assessing the acceptability, in principle, of procurement agencies for use by United Nations agencies
TRS 917 Annex 6 2003
Guidelines for the preparation of a procurement agency information file TRS 917 Annex 7Model quality assurance system for procurement agencies (Includes Appendix 6: Interagency finished pharmaceutical product questionnaire based on the model quality assurance system for procurement agencies)
TRS 986 Annex 3 2014
Assessment tool based on the model quality assurance system for procurement agencies: aide-memoire for inspection
TRS 986 Annex 4 “
A harmonized self-assessment tool for procurement agencies WHO Drug Information 28 (4)
2014
StorageGuide to good storage practices for pharmaceuticals TRS 908 Annex 9 2003Model guidance for the storage and transport of time- and temperature-sensitive pharmaceutical products
TRS 961 Annex 9 2011
Continued(4) Also adopted by the Expert Committee for Biological Standardization (ECBS)(5) The TRS annex includes the introductory sections and an overview of the 15 technical supplements.
The latter are available online at www.who.int/medicines/areas/quality_safety/quality_assurance/distribution/en/
“70 years of WHO standards on medicines quality”

Norms and standards WHO Drug Information Vol. 31, No. 1, 2017
24
Continued
Technical supplement materials to the WHO guidance for storage and transport of time- and temperature-sensitive pharmaceutical products
TRS 992 Annex 5 (5)
2015
Monitoring medicines qualityGuidelines on the conduct of surveys of the quality of medicines TRS 996 Annex 7 2016*WHO guidance on testing of “suspect” substandard/spurious/falsely-labelled/falsified/counterfeit medicines
In preparation
Good pharmacy practice (6)
Joint FIP/WHO guidelines on good pharmacy practice: standards for quality of pharmacy services
TRS 961 Annex 8 2011
FIP-WHO technical guidelines: Points to consider in the provision by health-care professionals of children-specific preparations that are not available as authorized products
TRS 996 Annex 2 2016
WHO prequalification (6)
Medicines(7)
Guidelines on the requalification of prequalified dossiers TRS 957 Annex 6 2010Procedure for prequalification of pharmaceutical products TRS 961 Annex 10 2011Guidelines on submission of documentation for a multisource (generic) finished product: general format: preparation of product dossiers in common technical document format
TRS 961 Annex 15
Guidelines on submission of documentation for a multisource (generic) finished pharmaceutical product for the WHO Prequalification of Medicines Programme: quality part
TRS 970 Annex 4 2012
Guidance on variations to a prequalified product TRS 981 Annex 3 2013Guidelines on submission of documentation for prequalification of finished pharmaceutical products approved by stringent regulatory authorities
TRS 986 Annex 5 2014
Collaborative procedure between the World Health Organization (WHO) prequalification team medicines and national medicines regulatory authorities in the assessment and accelerated national registration of WHO- prequalified pharmaceutical products and vaccines
TRS 996 Annex 8 2016
Active pharmaceutical ingredientsGuidelines on active pharmaceutical ingredient master file procedure TRS 948 Annex 4 2008Procedure for assessing the acceptability, in principle, of active pharmaceutical ingredients for use in pharmaceutical products
TRS 953 Annex 4 2009
Other related productsProcedure for Assessing the acceptability, in principle of male latex condoms for purchase by United Nations agencies
TRS 948 Annex 2 2008
Procedure for Assessing the acceptability, in principle of TCU 380A intrauterine devices for purchase by United Nations agencies
TRS 948 Annex 3 “
Continued
(6) The guidelines are available in the “Related regulatory standards” section of the WHO guidelines website, www.who.int/medicines/areas/quality_safety/quality_assurance/regulatory_standards/en/
(7) Prequalification of vaccines is conducted in line with standards provided by the WHO Expert Committee for Biological Standardization; prequalification of diagnostics is largely based on standards proposed by the International Medical Device Regulators Forum (IMDRF).
“70 years of WHO standards on medicines quality”
25
WHO Drug Information Vol. 31, No. 1, 2017 Norms and standards
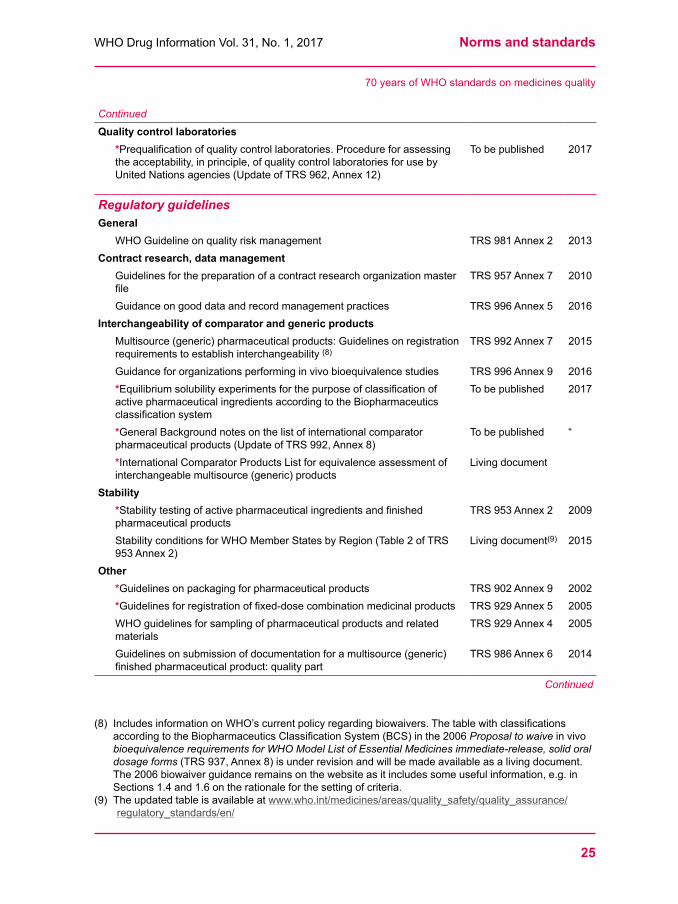
Continued
Quality control laboratories *Prequalification of quality control laboratories. Procedure for assessing the acceptability, in principle, of quality control laboratories for use by United Nations agencies (Update of TRS 962, Annex 12)
To be published 2017
Regulatory guidelinesGeneral
WHO Guideline on quality risk management TRS 981 Annex 2 2013Contract research, data management
Guidelines for the preparation of a contract research organization master file
TRS 957 Annex 7 2010
Guidance on good data and record management practices TRS 996 Annex 5 2016Interchangeability of comparator and generic products
Multisource (generic) pharmaceutical products: Guidelines on registration requirements to establish interchangeability (8)
TRS 992 Annex 7 2015
Guidance for organizations performing in vivo bioequivalence studies TRS 996 Annex 9 2016*Equilibrium solubility experiments for the purpose of classification of active pharmaceutical ingredients according to the Biopharmaceutics classification system
To be published 2017
*General Background notes on the list of international comparator pharmaceutical products (Update of TRS 992, Annex 8)
To be published “
*International Comparator Products List for equivalence assessment of interchangeable multisource (generic) products
Living document
Stability*Stability testing of active pharmaceutical ingredients and finished pharmaceutical products
TRS 953 Annex 2 2009
Stability conditions for WHO Member States by Region (Table 2 of TRS 953 Annex 2)
Living document(9) 2015
Other*Guidelines on packaging for pharmaceutical products TRS 902 Annex 9 2002*Guidelines for registration of fixed-dose combination medicinal products TRS 929 Annex 5 2005WHO guidelines for sampling of pharmaceutical products and related materials
TRS 929 Annex 4 2005
Guidelines on submission of documentation for a multisource (generic) finished pharmaceutical product: quality part
TRS 986 Annex 6 2014
Continued
(8) Includes information on WHO’s current policy regarding biowaivers. The table with classifications according to the Biopharmaceutics Classification System (BCS) in the 2006 Proposal to waive in vivo bioequivalence requirements for WHO Model List of Essential Medicines immediate-release, solid oral dosage forms (TRS 937, Annex 8) is under revision and will be made available as a living document. The 2006 biowaiver guidance remains on the website as it includes some useful information, e.g. in Sections 1.4 and 1.6 on the rationale for the setting of criteria.
(9) The updated table is available at www.who.int/medicines/areas/quality_safety/quality_assurance/regulatory_standards/en/
“70 years of WHO standards on medicines quality”
Norms and standards WHO Drug Information Vol. 31, No. 1, 2017
26
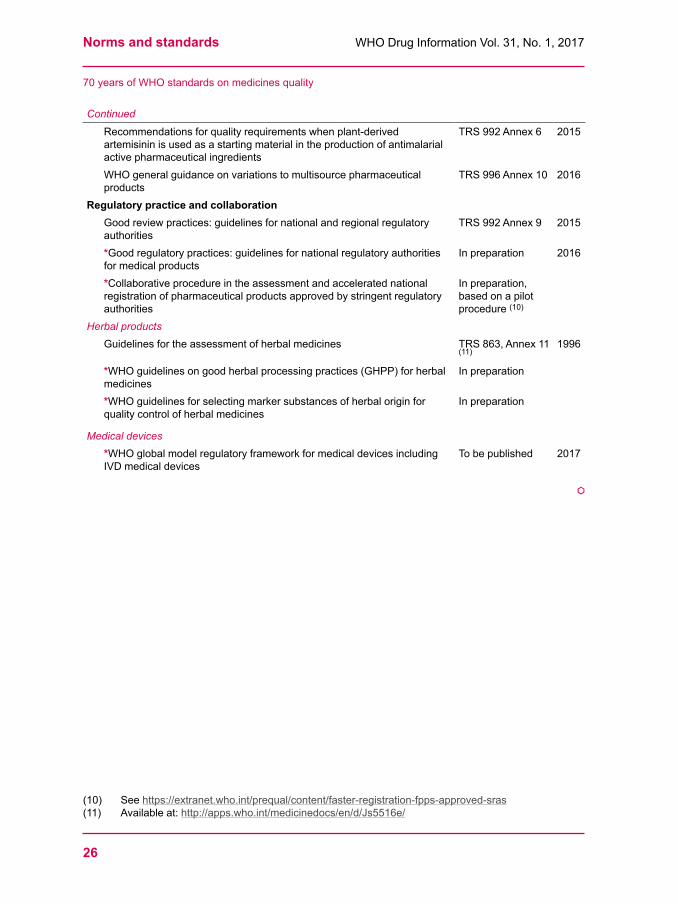
Continued
Recommendations for quality requirements when plant-derived artemisinin is used as a starting material in the production of antimalarial active pharmaceutical ingredients
TRS 992 Annex 6 2015
WHO general guidance on variations to multisource pharmaceutical products
TRS 996 Annex 10 2016
Regulatory practice and collaborationGood review practices: guidelines for national and regional regulatory authorities
TRS 992 Annex 9 2015
*Good regulatory practices: guidelines for national regulatory authorities for medical products
In preparation 2016
*Collaborative procedure in the assessment and accelerated national registration of pharmaceutical products approved by stringent regulatory authorities
In preparation, based on a pilot procedure (10)
Herbal productsGuidelines for the assessment of herbal medicines TRS 863, Annex 11
(11)1996
*WHO guidelines on good herbal processing practices (GHPP) for herbal medicines
In preparation
*WHO guidelines for selecting marker substances of herbal origin for quality control of herbal medicines
In preparation
Medical devices*WHO global model regulatory framework for medical devices including IVD medical devices
To be published 2017
å
“70 years of WHO standards on medicines quality”
(10) See https://extranet.who.int/prequal/content/faster-registration-fpps-approved-sras(11) Available at: http://apps.who.int/medicinedocs/en/d/Js5516e/
27
WHO Drug Information Vol. 31, No. 1, 2017
Vaccine controlFeasibility of a serological potency assay for
rabies vaccines for human use
The method currently recommended to determine the potency of rabies vaccines, the NIH mouse protection test, is demanding to perform and causes significant suffering to experimental animals. WHO initiated a feasibility study in order to determine whether a simpler serological assay developed at the Paul-Ehrlich-Institut (PEI) may be a suitable alternative for use by vaccine control laboratories globally. The findings suggest that the serological assay is promising but needs further verification.
IntroductionThe National Institute of Health (NIH) potency test, which is based on a mouse protection assay, is used to determine the potency of rabies vaccines.(1) However, only a limited number of national control laboratories are performing this assay due to its high requirements in terms of safety and technical capability. Moreover, this assay requires high animal numbers and causes severe suffering to the test animals. It is also known to have high variability and can be problematic in terms of meeting all of the validity criteria.(2)
In the interest of refining, reducing and replacing animal testing (3R principle) the Paul-Ehrlich-Institut (PEI) has developed
an alternative method (3, 4) that could potentially replace the rabies mouse challenge test. The proposed method is a multi-dose serological assay, based on vaccination of mice and subsequent determination of neutralizing antibodies in vitro.
The WHO Technical Assistance and Laboratory Services (TAL) Group initiated and coordinated a small scale feasibility study to evaluate whether this alternative assay can be successfully used for the potency determination of rabies vaccines for human use, and whether the test protocol can be transferred and applied at other laboratories.
This short communication was contributed by Dr Ute Rosskopf of the WHO Regulatory Systems Strengthening Team with input from Mrs Monika Zweygarth. It reflects the outcomes of a WHO-PEI Feasibility study to determine the potency of rabies vaccines by serology. The testing was conducted at the Institute of Biological Products (IBP), Department of Medical Sciences, Ministry of Public Health, Nonthaburi, Thailand, and at the Paul-Ehrlich-Institut (PEI), Laboratory for Product Testing of Immunological Medicinal Products for Veterinary Use, Langen, Germany.Study directors:Dr Ute Rosskopf, WHO Technical Assistance and Laboratory Services (TAL) Group ([email protected]):
Study initiation and coordination.Dr Beate Krämer, Paul-Ehrlich-Institut (Federal Institute for Vaccines and Biomedicines): Development of
study protocol and training of technical staff.

Vaccine control WHO Drug Information Vol. 31, No. 1, 2017
28
MethodThe study was performed at PEI and at the Institute of Biological Products (IBP) in Thailand. Training was provided to ensure the appropriate and timely performance of the testing.
Each of the two participating laboratories was asked to test a panel of three prequalified rabies vaccine samples against a standard vaccine (the WHO 6th International Standard for rabies vaccine), using the serological assay. One of the three test vaccines was heat-treated in order to induce a sub-potent quality. This sub-potent vaccine was tested using both serology and the NIH mouse protection test.
Each test vaccine was investigated in two independent test runs at four dilutions, against four equivalent dilutions of the standard vaccine. A fifth dilution of the standard vaccine equivalent to the minimum required potency (2.5 IU/ml) was added to investigate the suitability of a single-dose approach (cut-off test).
Groups of mice were immunized twice with either the test vaccine or the standard vaccine. Each dilution of each vaccine was administered into 10 mice.
Seven days after the second immunization blood samples were taken and the sera were tested for rabies antibodies using the proposed virus neutralization assay, a modified rapid fluorescent focus inhibition test (RFFIT).
The statistical analysis was performed at PEI and by Dr Stanley Norris Deming, Statistical Designs, Houston. Individual titers as well as pool sera were evaluated with a parallel line model to obtain a potency value for each sample relative to the WHO standard vaccine (with an assigned potency of 8 IU/ml).
Findings – in briefWhile differences with regard to estimated potencies were observed between the participating laboratories, a vaccine dose-dependent immune response of rabies antibody titres could be shown in almost all of the tests. The results of the NIH tests (manufacturer’s results at time point of release) could only partly be confirmed by the serological assay. This comes as little surprise since the comparison is based on the measurement of two different parameters: survival rates are enumerated with the NIH test, whereas antibody responses are determined in the serological assay.
Development of a single dilution assay (cut-off test) did not seem feasible as the serum activities obtained with the standard, adjusted to the minimum potency, were higher than those obtained with the test vaccines in all tests.
When potencies were calculated for individual sera, 3 out of 12 tests gave estimated curves that fulfilled the validity criteria for both linearity and parallelism. When potencies were calculated for serum pools, parallelism was observed in all cases, provided that deviations from linearity were accepted.
The sub-potent vaccine was correctly classified by means of the NIH test at both laboratories. In the serological assay, when analyzing serum pools, the sub-potent quality of the vaccines was correctly assigned in 3 out of 4 cases.
ConclusionsRoutine testing of individual sera using the serological assay does not seem appropriate due to the high number of plates to be handled and the difficulty to meet the current validity criteria. Testing of serum pools seems preferable. This
Feasibility of a serological potency assay for rabies vaccines for human use

29
WHO Drug Information Vol. 31, No. 1, 2017 Vaccine control
was a first feasibility study. The suitability of the serological assay for the potency quantification of rabies vaccines for human use would need to be further proven.
A further, exhaustive publication on the study is in preparation.
References1 Wilbur LA, Aubert MFA. The NIH test
for potency. Chapter 37. In: Laboratory techniques in rabies. Meslin F-X, Kaplan MM, Koprowski H (editors). Geneva: WHO; 1996.
2 Ferguson M, Heath A. Report of the WHO collaborative study to calibrate a candidate replacement for the 5th international standard of rabies vaccine. Expert committee on biological standardization. Geneva: WHO; 2008.
3 Krämer B, Kamphuis E, Hanschmann KM, Milne C, Daas A, Duchow K. A multi-dose serological assay suitable to quantify the potency of inactivated rabies vaccines for veterinary use. Biologicals. 2013; 41:400-406.
4 Krämer B, Schildger H, Behrensdorf-Nicol H, Hanschmann KM, Duchow K. The rapid fluorescent focus inhibition test is a suitable method for batch potency testing of inactivated rabies vaccines. Biologicals. 2009; 37:119-126. å
Feasibility of a serological potency assay for rabies vaccines for human use
30
WHO Drug Information Vol. 31, No. 1, 2017
Safety news
Safety warnings
Belladonna-containing teething products: risk to childrenU n i t e d S t a t e s o f A m e r i c a – An FDA laboratory analysis has found inconsistent amounts of belladonna in certain homoeopathic teething tablets, sometimes far exceeding the amount claimed on the label. The agency is warning that homoeopathic teething tablets containing the toxic substance belladonna pose a risk to infants and children, who may experience seizures, difficulty breathing, lethargy, excessive sleepiness, muscle weakness, skin flushing, constipation, difficulty urinating and agitation. The FDA urges consumers not to use these products. Homoeopathic teething products have not been evaluated or approved by the FDA for safety or effectiveness. In 2016 the FDA had warned consumers against the use of such products after receiving adverse event reports. (1)
A u s t r a l i a – Urgent testing conducted by the TGA in response to the safety concerns described above did not identify any quality issues. (2)
► (1) FDA News release, 27 January 2017.(2) TGA Update, 1 February 2017.
Hyoscine butylbromide injection: serious adverse events in patients with underlying heart diseaseU n i t e d K i n g d o m – The MHRA has warned health professionals that hyoscine butylbromide (also known as butylscopolamine) injection (Buscopan®)
can cause serious adverse effects, including tachycardia, hypotension and anaphylaxis. These effects can result in fatal outcomes, especially in patients with underlying cardiac conditions such as such as heart failure, coronary heart disease, cardiac arrhythmia or hypertension.
Injectable hyoscine butylbromide is used to treat acute muscular spasm and to reduce spasm in certain diagnostic procedures. The MHRA recommends to use this medicine with caution in patients that have any of the above-mentioned conditions. These patients should be monitored, and it should be ensured that resuscitation equipment as well as personnel who are trained in its use are readily available. The MHRA has reminded health professionals that hyoscine butylbromide injection remains contraindicated in patients with tachycardia.
The warning was published following nine reported deaths of patients in the United Kingdom after administration of hyoscine butylbromide injection. The product information has been updated to include the new recommendations.
► Drug Safety Update volume 10 issue 7, February 2017: 1.
Lenalidomide: reactivation of hepatitis B virus J a p a n – The PMDA has informed health professionals that cases of reactivation of hepatitis B virus (HBV) have been reported in patients treated with lenalidomide (Revlimide®) in Japan. HBV reactivation may occur in HBV carriers or in patients with a history of HBV infection.

31
WHO Drug Information Vol. 31, No. 1, 2017 Safety news
Recommendations have been added to the product information to test patients for HBV before starting treatment, and to monitor them during treatment with lenalidomide by appropriate measures such as periodic hepatic function tests and monitoring of HBV markers.
► PMDA Summary of investigation results and MHLW Revisions of precautions, 10 January 2017.
Canagliflozin and other SLGT2 inhibitors: risk of amputationsE u r o p e a n U n i o n – The EMA has informed the public about a potential increased risk of lower limb amputations (mostly affecting the toes) in patients taking the sodium-glucose co-transporter 2 (SGLT2) inhibitors canagliflozin, dapagliflozin and empagliflozin. A review of these medicines was carried out by EMA’s Pharmacovigilance Risk Assessment Committee (PRAC) in response to an increase in lower limb amputations observed in two ongoing clinical trials in patients treated with the canagliflozin. The mechanism by which canagliflozin may increase the risk of amputation is still unclear. An increased risk may also be associated with dapagliflozin and empagliflozin. Further data are expected from ongoing studies with these three SLGT2 inhibitors.
The product information for canagliflozin, dapagliflozin and empagliflozin will be updated based on available data; a warning of the potential increased risk of toe amputation highlighting the importance of routine preventative foot care will be included. For canagliflozin the risk of lower limb amputation will be listed as an uncommon side effect. If patients on canagliflozin develop significant foot complications such as infection or skin
ulcers, treatment discontinuation should be considered.
► EMA Press release, 24 February 2017.
Gadolinium-based contrast agents: accumulation in the brain;
C a n a d a – Health Canada has conducted a safety review of gadolinium-based contrast agents (GBCAs) due to growing scientific evidence that gadolinium may accumulate in the brain following multiple contrast-enhanced magnetic resonance imaging (MRI) scans. The evidence suggests that gadolinium accumulation in the brain is higher with the use of linear agents than with the use of macrocyclic agents.
Although no health consequences have been identified with gadolinium accumulation in the brain, Health Canada is requiring updates to the product information for GBCAs, advising health professionals to limit the use of these contrast agents to situations where they are considered necessary, to use the lowest effective dose, and to assess the benefits and potential risks to individual patients before administering repeated doses. (1)Reviews are also ongoing in the United States (2) and the European Union (3).
► (1) Health Canada Advisory, 5 January 2017.(2) FDA Drug safety announcement, 27 July 2015.(3) EMA. Article 31 Review started, 18 March 2016.
Restrictions
Dienogest and ethinylestradiol: can be used for acne as a last resort ; E u r o p e a n U n i o n – The EMA has recommended that combination products containing dienogest and ethinylestradiol
Safety news WHO Drug Information Vol. 31, No. 1, 2017
32
can be used for the treatment of moderate acne, but only if suitable local therapies or oral antibiotic treatment have failed, and only in women who also choose to use oral contraception.
Like all combined hormonal contraceptives dienogest and ethinyl-estradiol is associated with a risk of venous thromboembolism. While the risk is generally considered as low, available data are insufficient to quantify it for this specific combination. EMA recommends to consider each individual woman’s risk factors for venous thromboembolism before prescribing dienogest and ethinylestradiol for acne, and to reassess the need for continued treatment 3–6 months after starting treatment and periodically thereafter.
► EMA Press release, 27 January 2017.
Known risks
Chlorhexidine gluconate: serious allergic reactionsU n i t e d S t a t e s o f A m e r i c a – The FDA has warned health professional that rare but serious allergic reactions, including anaphylaxis, have been reported with the widely used topical antiseptic products containing chlorhexidine gluconate. The number of reports has increased in past years.
Prescription-only mouthwashes and oral chips containing chlorhexidine gluconate approved in the U.S. include a warning about the risk of serious allergic reactions in the product information. Such a warning is now also required for over-the-counter (OTC) products containing chlorhexidine gluconate.
► FDA Drug safety announcement, 2 February 2017.
Fluoroquinolones: severe, disabling side effectsC a n a d a – Healthcare professionals have been reminded about the potential for disabling and persistent serious adverse events with oral and injectable fluoroquinolone antibiotics. Health Canada is working with manufacturers to strengthen the prescribing information for these medicines.
The reminder follows rare reports of adverse events, including tendinopathy, peripheral neuropathy and central nervous system disorders, following systemic use of fluoroquinolones in Canada. In 2016, the U.S. FDA had restricted the use of fluoroquinolones to certain serious infections because of this risk. The EMA has started a review of this known risk associated with quinolones and fluoroquinolones (see under “Reviews started”).
► Health Canada Advisory, 23 January 2017.
Interferon beta-1b: thrombotic damage in small blood vesselsJ a p a n – The PMDA has informed health professionals about reports of thrombotic thrombocytopenic purpura (TTP) and haemolytic uraemic syndrome (HUS) in patients treated with interferon beta-1b in Japan and in other countries. Patients should be monitored through periodic blood tests such as platelet tests or red blood cell counts, and/or renal function tests as appropriate. The product information has been updated accordingly. (1)
A warning about thrombotic microangiopathy (TMA), manifesting as TPP or HUS, was added to the EMA-approved product information for interferon beta-1b products in July 2014, together with recommendations for monitoring of
33
WHO Drug Information Vol. 31, No. 1, 2017 Safety news
early symptoms, prompt treatment and discontinuation of interferon beta as soon as the reaction is diagnosed.(2) The FDA-approved product information for interferon beta-1B was updated in December 2015 to include a warning about TMA.(3)
► (1) PMDA Summary of investigation results and MHLW Revisions of precautions, 10 January 2017.(2) EMA. Summary of product characteristics. Betaferon.(3) FDA. Prescribing information for Extavia. May 2016.
Menthol-containing topical analgesics: serious skin burns C a n a d a – A Health Canada review has found a risk of serious skin burns with the use of certain OTC topical pain relievers containing menthol. Available data were not sufficient to determine whether the risk is linked to any specific brand, formulation or menthol concentration, or any ingredient other than menthol. The review also looked at the ingredients methyl salicylate and capsaicin, and did not find sufficient evidence to confirm the same risk with either of these ingredients alone.
A warning about the risk of burns is already included in the product information for certain products. Health Canada will publish an updated labelling standard for all menthol-containing topical analgesics.
► Health Canada Advisory, 13 February 2017.
Tramadol: risk of serious breathing problemsC a n a d a – Based on the findings of a Health Canada safety review, the product information for tramadol-containing
products has been updated to further highlight the risk of serious breathing problems. A warning has also been added that this risk is increased in patients who are “ultra-rapid metabolizers” of tramadol. The opioid medicine tramadol is approved in Canada to treat moderate to moderately severe pain in adults. Health professionals have been reminded that tramadol is not approved in Canada for use in patients under 18 years of age.(1)
A similar review was initiated in the United States in 2015.(2)
► (1) Health Canada. Summary safety review, 17 February 2017.(2) FDA Drug safety communication, 21 September 2015.
Varenicline and bupropion: risks said to be lower than expected;
U n i t e d S t a t e s o f A m e r i c a – Based on the findings of a large clinical trial the FDA has determined that the benefits of varenicline and bupropion in helping people to stop smoking outweigh their risks of serious adverse effects on mood, behaviour or thinking. The results showed that these risks were present, especially in people having being treated for mental illnesses, but that in most patients they did not have serious consequences such as hospitalization. The warning sections of the medicines are being updated accordingly. Products containing bupropion, which is an antidepressant, will continue to carry a “Boxed Warning” about suicidality in patients treated with antidepressant medicines.
► FDA Drug safety communication, 16 December 2016.

Safety news WHO Drug Information Vol. 31, No. 1, 2017
34
Herbal products
Toxic alkaloids in plant-based products;
S w i t z e r l a n d – Swissmedic has required marketing authorization holders to conduct risk evaluation and assays in order to mitigate the risk of toxic pyrrolizidine alkaloids contained in plant-based foods, teas and medicinal products. The toxic substances enter the products through weeds that are harvested with the plants.
Hundreds of structurally different pyrrolizidine alkaloids occurring in several thousand different plant species have been identified, and their toxic effect has been known for a long time. Many plant-based foods and medicinal plants are affected by the weed problem. It has been shown that measures going beyond the existing Good Agricultural and Collection Practice (GACP) are needed to ensure the quality and safety of these products. In May 2016 the EMA had published a statement with
Reviews started
Medicine Use Concerns Reviewing authority reference
Certain anaesthetics and sedativeswhen used in children under the age of three or in pregnant women during their third trimester
General anaesthesia and sedation
Lengthy use in young children or pregnant women may have potential negative effects on the development of children’s brains
► Health Canada Advisory, 22 December 2016.See also: FDA Drug safety communication, 14 December 2016
Selexipag(Uptravi®)
Treatment of pulmonary arterial hypertension
Deaths of 5 patients taking the medicine in France. Based on a preliminary review of available data, EMA advised that the product may continue to be used both in existing and new patients, provided that the recommendations and precautions in the current prescribing information are followed carefully.
► EMA Press release, 10 February 2017. (As updated on 14 February 2017).
Systemic and inhaled quinolones and fluoroquinolones
Treatment of infections
Persistent serious side effects mainly affecting muscles, joints and the nervous system.
► EMA. Article 31 Referral. Quinolone- and fluoroquinolone-containing medicinal products. 10 February 2017.

35
WHO Drug Information Vol. 31, No. 1, 2017 Safety news
recommendations for risk management and quality control.
► Swissmedic announcement, 6 February 2017.EMA. Public statement on contamination of herbal medicinal products/traditional herbal medicinal products with pyrrolizidine alkaloids; Transitional recommendations for risk management and quality control. 31 May 2016.
Non-compliance with good practices
Micro Therapeutic Research Labs Pvt Ltd, IndiaE u r o p e a n U n i o n – The EMA has started a review of medicines for which studies have been conducted by Micro Therapeutic Research Labs at its Chennai site or its Coimbatore site in India. This follows a good clinical practice (GCP) inspection in February 2016, which raised concerns about the study data used to support a number of marketing authorization applications in the EU. Several national medicines regulatory agencies have requested EMA to assess the impact of the findings on medicines currently authorized or under evaluation in the EU on the basis of studies performed at the two sites.
► EMA. Article 31 Review started, 16 December 2017.
Chongqing Pharma Research Institute, China (and 11 others)U n i t e d S t a t e s o f A m e r i c a – Following an inspection conducted in May 2016, the FDA has warned the active pharmaceutical ingredient manufacturer Chongqing Pharma Research Institute Co. Ltd over data integrity issues. Audit trails from laboratory equipment used to perform high performance liquid chromatography and gas
chromatography analyses showed that entire chromatographic sequences and individual injections had been deleted. The FDA investigator was told that it is laboratory practice to perform more injections than required by procedure, and then to delete any undesirable result. Analyses were repeated – without any scientific justification, investigation or documentation of original out-of-specification or otherwise undesirable test results – until acceptable results were obtained. These manipulated test results and incomplete records were used to support batch release decisions.
The FDA has requested the company to respond within 15 days providing details of remedial action.
► FDA Warning letter No. 320-17-24, 14 February 2017.
Since the beginning of 2017 the FDA’s Center for Drug Evaluation and Research has issued a total of 12 warning letters to foreign companies, as published on the FDA website as of 8 March. The warnings were issued to five companies based in China, three in India, and two each in Japan and Europe. FDA warning letters are publicly available at https://www.fda.gov/ICECI/EnforcementActions/WarningLetters/. å

36
WHO Drug Information Vol. 31, No. 1, 2017
Regulatory news
Vision statement
Japan announces Rational Medicine initiativeJ a p a n – The Pharmaceuticals and Medical Devices Agency (PMDA) has announced its “Rational Medicine” initiative, which aims to serve the best overall interests of the patient through an all-inclusive approach to medicine that is thoroughly based on the latest science and most advanced technology in all relevant areas.
This holistic, patient-centred approach to medicine is intended to advance regulatory science and to create an environment where medical care is strictly evidence-based. To this end, the PMDA plans to continue its initiatives in four areas: (1) innovation through product approval reviews of enhanced rigour and rationality; (2) further promotion of regulatory science; (3) increased sophistication of safety measures through the use of real-world data; and (4) enhanced international partnerships.
Through this approach the PMDA will ensure that patients receive optimal medical treatment, including treatment based on innovative new technologies.
► PMDA Announcement, 9 February 2017.
Scientific integrity was also named by the WHO Director-General as one of four priorities that should guide health policies in the next decade. In delivering the keynote address at the 10th anniversary of the University of Washington’s Department of Global Health, she said: “Regulatory agencies everywhere must resist the push to replace randomized clinical trials,
long the gold standard for approving new drugs, with research summaries provided by pharmaceutical companies. As some argue, making this change would speed up regulatory approval, lower the costs to industry, and get more products on the market sooner. This kind of thinking is extremely dangerous. We must not let anything, including economic arguments or industry pressure, lower our scientific standards or compromise our integrity. ”
► WHO Director-General. Keynote address. Seattle, Washington, USA. 8 February 2017.
Pre-market assessment
Ten years of EMA conditional marketing authorizations E u r o p e a n U n i o n – The EMA has published a report on its ten years of experience with conditional marketing authorizations since their introduction in 2006 until June 2016. Thirty products were granted a conditional marketing authorization during that period, and none of them were subsequently revoked or suspended. On average, it took four years to convert the conditional approval into a full marketing authorization based on additional data. The report concludes that conditional marketing authorization enables patients with life-threatening or seriously debilitating conditions to access promising medicines earlier.
The report characterizes the data on which conditional approvals have been granted and the additional data generated through specific obligations. Some areas for improvement are identified, notably with
37
WHO Drug Information Vol. 31, No. 1, 2017 Regulatory news
regard to prospective planning and early dialogue between stakeholders, including health technology assessment bodies that make decisions on reimbursement.
► EMA Press release, 23 January 2017.
Post-market monitoring
Australia to publish laboratory testing resultsA u s t r a l i a – The TGA has announced that it will begin publishing the outcomes of its laboratory testing on its website from mid-2017.(1) Where products fail any aspect of testing, details of the test(s) that failed and outcomes of any follow-up action will also be provided. Results will be published in May and November of each year, allowing six months after the end of each reporting period for follow-up on any non-compliant findings.
The TGA tests approximately 2000 samples of therapeutic goods annually. The planned publication of the results is part of the TGA’s response to a 2015 expert review of medicines and medical devices regulation, which had recommended to establish a more comprehensive post-market monitoring scheme for medical products in Australia. Similar information is also published by the U.S. FDA (2) and the EMA (3).
► (1) TGA Statement, 7 February 2017.(2) FDA. Drugs > Science & Research (Drugs) > Drug Quality Sampling and Testing Programs.(3) EMA website. Human regulatory > Overview > Compliance > Sampling and testing.
India releases medicines quality survey results I n d i a – The Central Drug Standards Control Organization (CDSCO) and the Ministry of Health and Family Welfare have released
the report of a nationwide medicines quality survey.
The survey was conducted by the National Institute of Biologicals and covered the period 2014-2016. With almost 48000 samples from all major therapeutic categories collected across the country, it was the largest-ever such survey to be conducted in India. A specially designed in-house software was used for collection, transmission and analysis of data. Testing was done at India’s seven Central and three State Government drug testing laboratories.
Overall the survey found that 3.16% of samples were not of standard quality, and 0.0245% were spurious drugs.
Of 33656 samples from Indian retail outlets tested in the survey, 1011 (3%) failed one or more tests. Dissolution accounted for a third of the failures, followed by assay. The list of molecules with the most non-compliant samples was led by four antibacterials: erythromycin (28.7%), gentamicin (21.1%), ceftriaxone (19.8%) and amikacin (19.5%).
Samples taken at government facilities had above-average failure rates. Of 8369 samples analyzed, 839 (10%) failed one or more tests. The most frequently failed tests were assay and dissolution, followed by related substances. Non-compliance in the latter test accounted for about every seventh failure, occurring almost twice as frequently as in samples collected at retail outlets. The highest percentages of non-compliant samples were seen for bisacodyl (66.7%), zinc sulfate (51.3%), amikacin (43.3%), oxytocin (41.3%) and gentamicin (40.2%); ceftriaxone ranked 9th with 24.6%.
A breakdown by manufacturing units from which at least 25 samples were tested showed some particularly high failure rates in the retail outlet part of the survey: four sites, including an Indian manufacturing site
Regulatory news WHO Drug Information Vol. 31, No. 1, 2017
38
of a well-known multinational company, had failure rates >50%.
Of 4987 samples taken at ports none failed any tests.
Thirteen samples tested in the survey were found to be spurious as defined in Indian legislation. These samples failed to meet the identification test of the labelled drug or had zero active ingredient. The molecules concerned were amoxicillin with or without clavulanic acid (7 samples), prednisolone or methylprednisolone (3 samples), sulfamethoxazole/trimethoprim fixed-dose combination (2 samples) and cefixime (1 sample).
► CDSCO website. What’s new. Drugs Survey Report. 17 February 2017.Available at http://www.cdsco.nic.in/forms/list.aspx?lid=2254&Id=23, accessed 22 February 2017. Includes links to the full report. Ministry of Health and Welfare, Announcement. February 2017.
WHO has published guidelines which outline the steps to consider when preparing and conducting a survey of medicines quality. The guidelines provide recommendations and examples of methodological approaches with a discussion of their advantages and disadvantages, and suggestions on how to prepare reports on the results obtained from such surveys. An overview of WHO guidelines on medicines quality is provided in the Norms and standards section (pp. 15-26) ► WHO. Guidelines on the conduct of surveys of the quality of medicines. Annex 7. In: WHO Technical Report Series 996, 2016.
Antimicrobial resistance
(See also page 46: WHO has published its first-ever list of antibiotic-resistant priority pathogens)
Two reports on antimicrobial resistance in EuropeE u r o p e a n U n i o n – Experts from the European Food Safety Authority (EFSA) and the European Medicines Agency (EMA) have reviewed the measures taken in the European Union (EU) to reduce antimicrobials use in food-producing animals. In their report they emphasize that there is no one-size-fits-all solution. The experts conclude that reducing and replacing antimicrobials can reasonably be assumed to decrease antimicrobial resistance; however, due to lack of data they were unable to quantify the impact of single measures. In addition to reduction measures the experts recommend to rethink the livestock production system and to introduce innovative solutions to prevent and control infectious diseases in animals.
► EMA Press release, 24 January 2017.
In February 2017 EFSA and the European Centre for Disease Prevention and Control (ECDC) published their annual report on the levels of antimicrobial resistance in food, animals and humans across the EU. The findings underline that antimicrobial resistance remains high and poses a serious threat to public and animal health. Infections caused by bacteria that are resistant to antimicrobials lead to about 25000 deaths in the EU every year. Countries where actions have been taken to reduce, replace and re-think the use of antimicrobials in animals, show lower levels of antimicrobial resistance and decreasing trends.
► EFSA News, 22 February 2017.

39
WHO Drug Information Vol. 31, No. 1, 2017 Regulatory news
Regulatory statement and new guidelines on antibiotic use in IndiaI n d i a – The Central Drugs Standard Control Organisation (CDSCO) of India has released an advisory statement with recommendations about the rational use of antibiotics to limit antimicrobial resistance. The statement outlines the measures implemented by CDSCO and lists the steps to be taken by other stakeholders. It calls on the regulators of each of India’s States to enforce compliance with laws and regulations and to raise public awareness about the consequences of misuse of antibiotics. The statement further asks the All India Organization of Chemists and Druggists to educate its members on the licensing conditions for medicines sales and cooperate with regulatory authorities, and calls on the pharmaceutical industry to use its network to discourage the sale of antibiotics without a prescription.(1)
In February 2017 the Indian Council of Medical Research (ICMR) released its guidelines on antimicrobial use. As stated in the foreword to the guidelines, an estimated 50% or more of hospital antimicrobial use is inappropriate. The document is intended to guide treatment in order to bring down the burden of antimicrobial resistance in India.(2)
► (1) CDSCO Advisory, 1 February 2017.(2) ICMR. Treatment Guidelines for Antimicrobial Use in Common Syndromes. New Delhi, India: Indian Council of Medical Research: 2017.
Biosimilars
EMA advice on development of biosimilarsE u r o p e a n U n i o n – The EMA will launch a pilot project in February 2017 to test the added value and feasibility of tailored scientific advice for the development of
biosimilar medicines. The advice will support the stepwise approach recommended in EU guidelines, where the level and robustness of previously accumulated quality, analytical and functional data should determine the extent and nature of the required studies and tests.
The advice is intended to inform the development strategy for biosimilars. It will not constitute a formal pre-assessment of the data submitted as part of the marketing authorization application.
► EMA News, 16 December 2016.
FDA guidance on naming of biologicalsU n i t e d S t a t e s o f A m e r i c a – The FDA has released its guidance for industry titled Nonproprietary Naming of Biological Products. The guidance provides for nonproprietary names to include a core name and a distinguishing FDA-designated suffix that is devoid of meaning and composed of four lowercase letters. The guidance applies to previously licenced and newly licenced originator biological products, related biological products and biosimilar products. FDA is still considering the appropriate suffix format for interchangeable biological products.
In commenting on the guidance at the draft stage, many responders suggested that a meaningful, distinguishable suffix may help to improve pharmacovigilance, enhance safety and facilitate identification between biological products. Some supported the use of a random suffix to avoid creating an unfair advantage for specific manufacturers. Several comments stated that the current practices of FDA and non-FDA entities for identifying products is sufficient for the purpose of pharmacovigilance, and designation of a suffix is not needed.
► U.S. Federal Register. Notice, 13 January 2017.
Regulatory news WHO Drug Information Vol. 31, No. 1, 2017
40
Substance use
Opioid control in CanadaC a n a d a – Following the launch of the Canadian Drugs and Substances Strategy in December 2016, which reinstates harm reduction as a core pillar of Canada’s drug policy, the Government of Canada has announced new funding of 65 million Canadian dollars (approximately US$ 50 million) over five years to be used to support the federal government’s ongoing implementation of the Opioid Action Plan.(1)
To raise awareness on the safe use of opioids Health Canada will put forward a regulatory proposal to make warning stickers and patient information handouts mandatory with all opioids dispensed in Canada. The sticker on the medicine container would warn patients about the risks of addiction and overdose with opioid use. The handout would contain broader information on the safe use of opioids and important risks.(2)
► (1) Health Canada News release, 17 February 2017.(2) Health Canada Statement, 17 February 2017.
Collaboration
Landmark EU– U.S. agreement on inspectionsE u r o p e a n U n i o n , U n i t e d S t a t e s o f A m e r i c a – EMA and FDA have agreed to mutually recognize inspections of manufacturing sites for human medicines conducted in their respective territories. This will enable better use of inspection resources with greater focus other parts of the world where there may be greater risk. Around 40% of finished medicines marketed in the EU come from overseas and 80% of the manufacturers of active pharmaceutical ingredients for
medicines available in the EU are located outside the Union.
The agreement is an annex to the EU-U.S. mutual recognition agreement which was signed in 1998. Many provisions of the agreement are already effective, and others will enter into force on 1 November 2017. To reach the agreement on inspections the two regulatory authorities have worked together closely since May 2014 and have been auditing and assessing the respective supervisory systems.
► EMA Press release, 2 March 2017.FDA News release, 2 March 2017.
IGDRP roadmap to 2020The Steering Committee of the International Generic Drug Regulators Programme (IGDRP) has released the Programme’s Roadmap to 2020. The document describes the five overarching strategic priorities for the initiative as well the key objectives for each of these priorities.
The IGDRP was launched in 2012 as a pilot to increase the efficiency of review procedures for generic medicines and reduce regulatory burden without comprising the safety, efficacy, and quality of products. Availability of quality generic medicines plays an increasingly important role in helping to address rising health care costs.
► IGDRP News, 21 December 2016.
IGDRP biowaiver templateThe IGDRP Bioequivalence Working Group has developed a template for biowaiver assessment reports to ensure that the relevant information for a biowaiver is consistently taken into account during assessment, despite the IGDRP members’ differing requirements for biowaivers based on the Biopharmaceutics Classification
41
WHO Drug Information Vol. 31, No. 1, 2017 Regulatory news
Under discussion
E u r o p e a n U n i o n – The European Commission has invited comments on its revised guidelines on excipients in the labelling and package leaflet of medicinal products for human use. The purpose of the guideline is to define requirements on how excipients must feature on the labelling of medicinal products. The original guidance was adopted in 2003.
► European Commission. Public consultation, 27 February 2017.Closing date: 22 May 2017.
E u r o p e a n U n i o n – The EMA has launched a public consultation on the proposed revision to its 2010 policy on access to documents. The new version extends the scope of the policy to include explicitly corporate documents and takes into account the move towards more transparency that has led to the publication of additional documents on the EMA website since 2010.
► EMA news, 17 February 2017.Closing date: 18 May 2017.
E u r o p e a n U n i o n – The EMA has released a concept paper on developing a guideline on
quality requirements of medicinal products containing a device component for delivery or use of the medicinal product. Such requirements are intended for situations where a medicinal product is used along with a specified medical device, and there is no intention to duplicate the CE marking process for medical devices.
► EMA Consultation, 16 February 2017.Closing date: 16 May 2017.
U n i t e d S t a t e s o f A m e r i c a – The FDA has released three texts regarding different types of manufacturers’ communications about medical products, including: communications with funders and similar entities, communications conveying content that is not included in the product information; and communications on unapproved uses of approved products.
► FDA Statement, 18 January 2017.Closing date: 19 April 2017.
N e w Z e a l a n d – Medsafe has launched a public consultation on labelling requirements for over-the-counter miconazole products to include a compulsory warning about
System (BCS). As this template can also benefit applicants and the broader regulatory community it has been made available on the IGDRP website.
► IGDRP News, 28 February 2017.
ASEAN joint assessment pilotThe medicines regulatory authorities of the Association of Southeast Asian Nations (ASEAN) have developed a new procedure for joint assessment of marketing
authorization applications. The procedure will be implemented, with support and technical advice from WHO, for a pilot period of up to two years starting in January 2017. Participation by applicants and regulators is voluntary for each product to be assessed. The procedure is intended lead to faster review of priority medicines throughout ASEAN while respecting existing national decision-making processes.
► National Pharmaceutical Regulatory Agency (NPRA) of Malaysia. Announcement, 9 December 2016.

Regulatory news WHO Drug Information Vol. 31, No. 1, 2017
42
Under discussion
a known interaction with warfarin. The revision is proposed because potentially life-threatening events continue to be reported in New Zealand in patients taking the two medicines concomitantly.
► Medsafe Advice, 15 February 2017.Closing date: 13 April 2017.
U n i t e d K i n g d o m – The MHRA is developing a strategy for the creation of pharmacopoeial public quality standards for biological medicines and has launched a consultation to seek input on the strategy, and on how the standards are used and can be improved.
► MHRA Open consultation, 9 January 2017.Closing date: 10 April 2017.
A u s t r a l i a – The 2015 Review of Medicines and Medical Devices Regulation in Australia included three recommendations to improve access to unapproved therapeutic goods through changes to existing schemes. The recommendations made are to decrease duplication of work and to streamline access to unapproved therapeutic goods considered to have an established history of use.
► TGA Consultation, 15 February 2017.Consultation closed 29 March 2017.
A u s t r a l i a – The TGA has released a consultation paper on reforms to its complementary medicines regulation. The document proposes a three-tiered risk-based framework, introducing a new assessment pathway sitting between the existing pathways for listed medicines (low risk) and registered medicines (high risk).
► TGA News, 14 February 2017.Consultation closed 28 March 2017.
U n i t e d S t a t e s o f A m e r i c a – The FDA has published its draft guidance on the data and information expected for a biological product
to meet the standard for interchangeability. The availability of biosimilar and interchangeable products will provide more treatment options, potentially driving down costs to give more patients access to needed medicines.
► U.S. Federal Register. Notice. 18 January 2017.Consultation closed 20 March 2017.
The International Council for Harmonisation of Technical Requirements for Pharma-ceuticals for Human Use (ICH) has released its reflection paper on Good Clinical Practice (GCP) Renovation. The paper proposes a revision of the ICH E8 General Considerations for Clinical Trials, as well as further revisions to the E6 Guideline for GCP.
► ICH News, 12 January 2017.Consultation closed 11 March 2017.
E u r o p e a n U n i o n – The EMA has published a summary of ideas on advanced therapy medicinal products (ATMP) put forward at a May 2016 workshop. While revisions to the legislation on ATMPs in Europe are currently not foreseen, the workshop outcomes will be considered for a wider EU plan to be developed.
► EMA News, 3 February 2017.
E u r o p e a n U n i o n – In response to a European Commission consultation on the development of good manufacturing practice (GMP) guidelines for ATMPs,(1) the Pharmaceutical Inspection Cooperation Scheme (PIC/S) has expressed its concern about proposed lowered GMP standards for ATMPs, leading to an internationally non-harmonized approach in this area.(2)
► (1) EC. Summary of the responses to the targeted stakeholder consultation.(2) PIC/S News, March 2017.
43
WHO Drug Information Vol. 31, No. 1, 2017 Regulatory news
Approved
Plecanatide : for chronic idiopathic constipationProduct name: Trulance®Dosage form: TabletsClass: Guanylate cyclase-C agonist, human
uroguanylin analogApproval: FDAUse: Treatment of chronic idiopathic
constipation (CIC) in adults.Benefits: Additional treatment option for
adult patients with CIC.Safety information: Plecanatide should not
be used in children under six years due to the risk of serious dehydration. Its use should be avoided in patients aged 6-18 years, as its safety and effectiveness have not been established in these patients. The product should not be used in patients with known or suspected mechanical gastrointestinal obstruction. The most common and serious side effect was diarrhoea. If severe diarrhoea occurs, patients should stop taking the medicine and contact their health care provider. ► FDA News release, 19 January 2017.
Telotristat ethyl : for carcinoid syndrome diarrhoeaProduct name: Xermelo®Dosage form: TabletsClass: Serotonin synthesis inhibitor Approval: FDA (fast-track designation,
priority review; orphan drug designation) Use: Adjunctive treatment of carcinoid
syndrome diarrhoea in adults when the condition is inadequately controlled with somatostatin analog therapy alone.
Benefits: Inhibits the production of serotonin by carcinoid tumours and reduces the frequency of carcinoid syndrome diarrhoea.
Safety information: Patients should be monitored for severe constipation. If a patient experiences severe constipation or severe, persistent or worsening abdominal pain, they should discontinue telotristat ethyl and contact their healthcare provider. ► FDA News release, 28 February 2017.
Crisaborole : for atopic dermatitisProduct name: Eucrisa®Dosage form: OintmentClass: Phosphodiesterase 4 (PDE-4)
inhibitorApproval: FDAUse: Treatment of adults and children over
two years of age with mild to moderate chronic atopic dermatitis.
Benefits: Additional treatment option for with mild to moderate atopic dermatitis.
Safety information: Serious side effects include hypersensitivity reactions to crisaborole. ► FDA News release, 14 December 2016.
Parathyroid hormone replacement therapyProduct name: Natpar®Dosage form: InjectionClass: Hormone; ATC code: H05AA03Approval: EMA (conditional marketing
authorization; orphan designation)Use: Adjunctive treatment of patients with
chronic hypoparathyroidism who cannot be adequately controlled with calcium and vitamin D
Benefits: Ability to reduce the need for calcium and vitamin D supplements while maintaining adequate serum calcium levels.

Regulatory news WHO Drug Information Vol. 31, No. 1, 2017
44
Approved
Note: This is the first EMA-approved hormone replacement therapy for parathyroid disorder. ► EMA Press release, 24 February 2017.
Rucaparib : for certain ovarian cancersProduct name: Rubraca®Dosage form: TabletsClass: Poly ADP-ribose polymerase (PARP)
inhibitor; ATC code: L01XX55 (temporary)Approval: FDA (accelerated approval,
breakthrough therapy, priority review; orphan drug designation)
Use: Treatment of advanced ovarian cancer in women who have been treated with two or more chemotherapies and whose tumours have a specific gene mutation (deleterious BRCA) as identified by an FDA-approved companion diagnostic test.
Benefits: Additional treatment option for women with BRCA-mutated ovarian cancer.
Safety information: Serious risks associated with rucaparib include myelodysplastic syndrome, acute myeloid leukaemia and foetal harm. ► FDA News release, 19 January 2017.
Nusinersen : for spinal muscular atrophyProduct name: Spinraza®Dosage form: InjectionClass: Survival motor neuron-2 (SMN2)-
directed antisense oligonucleotideApproval: FDA (fast-track designation,
priority review; orphan drug designation)Use: Treatment of adults and children with
spinal muscular atrophy (SMA)Benefits: Improvement in motor functions
such as head control, sitting, ability to kick in supine position, rolling, crawling, standing and walking.
Safety information: Risk of thrombocytopenia and coagulation abnormalities as well as renal toxicity.
Notes: This is the first medicine approved in the U.S. for the treatment of SMA, a rare and often fatal hereditary condition affecting muscle strength and movement.
According to an article in the New York Times, treatment could cost US$ 625,000-$750,000 in the first year, and about $375,000 annually after that. ► FDA News release, 23 December 2016.Costly Drug for Fatal Muscular Disease Wins F.D.A. Approval. New York Times, 30 December 2017.
Sublingual dust mite allergen extractProduct name: Odactra®Dosage form: Sublingual tabletClass: AllergenApproval: FDAUse: Treatment of house dust mite-induced
allergic rhinitis.Benefits: Reduction in allergy symptomsSafety information: Boxed warning about the
risk of severe allergic reactions, some of which can be life-threatening. As with all sublingual allergen extracts, patients should be prescribed auto-injectable epinephrine (adrenaline). ► FDA News release, 1 March 2017.
Sodium zirconium cyclosilicate : for hyperkalaemiaProduct name: Lokelma®Dosage form: Powder for oral suspension;
ATC code: V03AE10 Approval: EMA/CHMP recommendationUse: Treatment of hyperkalaemia in adult
patients.Benefits: Ability to lower serum potassium
levels. ► EMA/CHMP Summary of opinion, 23 February 2017.
45
WHO Drug Information Vol. 31, No. 1, 2017 Regulatory news
Approved
Two adalimumab biosimilars
Product name: Amgevita®Reference product: Humira®Approval: EMA recommendationUse: Treatment of rheumatoid arthritis,
juvenile idiopathic arthritis, axial spondylo-arthritis, psoriatic arthritis, psoriasis, paediatric plaque psoriasis, hidradenitis suppurativa, Crohn’s disease, paediatric Crohn’s disease, ulcerative colitis and uveitis. ► EMA/CHMP Opinion, 26 January 2017.
Product name: Solymbic®Reference product: Humira®Approval: EMA recommendationUse: Treatment of rheumatoid arthritis,
enthesitis-related arthritis, axial spondyloarthritis, psoriatic arthritis, psoriasis, hidradenitis suppurativa, Crohn’s disease, ulcerative colitis and uveitis. ► EMA/CHMP Opinion, 26 January 2017.
Three clinically important generics approved in ChinaThe China Food and Drug Administration (CFDA) has announced the approval of three clinically important generics manufactured by Chinese companies, as well as the active pharmaceutical ingredients contained in the products. The medicines concerned are the anti-cancer medicine gefitinib and the antiretrovirals efavirenz and tenofovir disoproxil fumarate (TDF). TDF can also be used to treat hepatitis B.(1)
This follows a drive by the CFDA to raise the standards of generic drugs developed, produced and sold in China. In late 2015 the authority had released draft guidance calling for manufacturers of approved generics to perform conformity assessments of their products.(2) Draft guidelines on inspections
for generic medicines were released in January 2017.(3)
► (1) Third World Network. Info Service on Intellectual Property Issues. 18 January 2017.(2) Regulatory Affairs Professionals Society (RAPS). Asia Regulatory Roundup. 8 March 2016.(3) RAPS. Asia Regulatory Roundup. 3 January 2017.
Two tests for guiding antibiotic use The FDA has cleared two tests that can help to guide the use of antibiotics. The Vidas Brahms PCT Assay was cleared for expanded use in guiding treatment in lower respiratory tract infections, in addition to its use in sepsis. The test measures procalcitonin (PCT), a protein associated with the body’s response to a bacterial infection. It is intended to be used in the hospital or emergency room setting. The FDA also cleared the PhenoTest BC Kit, which can identify various infective agents causing bloodstream infections and provide sensitivity results for selected antibiotics.
► (1) FDA News release, 23 February 2017.(2) FDA News release, 23 February 2017.
Extension of indications
Elvitegravir & cobicistat & emtricitabine & tenofovir: for children over 12 years of ageProduct name: Stribild®Approval: FDANewly approved use: Treatment of HIV in
children over 12 years of age weighing at least 35 kg. ► FDA. What’s new in HIV and AIDS. 31 January 2017. å
46
WHO Drug Information Vol. 31, No. 1, 2017
Publications and events
Research and development
WHO publishes priority list of antibiotic-resistant pathogensG e n e v a – WHO has published its first-ever list of antibiotic-resistant “priority pathogens” that pose the greatest threat to human health. The list was drawn up in a bid to guide and promote research and development (R&D) of new antibiotics, as part of WHO’s efforts to address growing global resistance to antimicrobial medicines. The issue of antimicrobial resistance is to be brought to the attention of the G20 health experts at their meeting in Berlin in early March 2017.
The list is reproduced below. It highlights in particular the threat of gram-negative bacteria that are resistant to multiple antibiotics.
WHO priority pathogens list for R&D of new antibiotics
Priority 1: CRITICAL• Acinetobacter baumannii, carbapenem-resistant• Pseudomonas aeruginosa, carbapenem-
resistant• Enterobacteriaceae, carbapenem-resistant,
ESBL-producing
Priority 2: HIGH• Enterococcus faecium, vancomycin-resistant• Staphylococcus aureus, methicillin-resistant,
vancomycin-intermediate and resistant• Helicobacter pylori, clarithromycin-resistant• Campylobacter spp., fluoroquinolone-resistant• Salmonellae, fluoroquinolone-resistant• Neisseria gonorrhoeae, cephalosporin-resistant,
fluoroquinolone-resistant
Priority 3: MEDIUM• Streptococcus pneumoniae, penicillin-non-
susceptible• Haemophilus influenzae, ampicillin-resistant• Shigella spp., fluoroquinolone-resistant
Tuberculosis – whose resistance to traditional treatment has been growing in recent years – was not included because it is targeted by other, dedicated programmes.(1) WHO has stressed the urgent need for R&D for drug-resistant tuberculosis in a separate statement.(2)
► (1) WHO News release, 27 February 2017.WHO. Global priority list of antibiotic-resistant bacteria to guide research, discovery, and development of new antibiotics. Publication date: 27 February 2017.(2) WHO News release, 28 February 2017.
Access to medicines
Intellectual property rules amended to ease global access to medicinesG e n e v a – An amendment to the WTO Trade Related Aspects of Intellectual Property Rights (TRIPS) Agreement entered into force on 23 January 2017, securing for developing countries a legal pathway to access affordable medicines under WTO rules. As two-thirds of the WTO members have ratified the amendment, the threshold has been reached which was needed to formally amend the TRIPS Agreement. The amendment empowers importing developing and least-developed countries facing public health problems and lacking the capacity to generic medicines to seek such medicines from third country producers under compulsory licensing arrangements.
► World Trade Organization News, 23 January 2017.
47
WHO Drug Information Vol. 31, No. 1, 2017 Publications and events
OECD reports on health spending and new technologiesL o n d o n – The Organisation for Economic Co-operation and Development (OECD) has launched two reports that show how pharmaceutical spending is increasingly skewed towards high-cost products and technologies, with little or no benefits for people’s health. In some cases there is even a risk of worse health outcomes.
The first report recommends strategies for countries to spend significantly less on health care while maintaining health system performance and health outcomes.(1) The second report provides analyses on the adoption and impact of medical technology and identifies opportunities to optimize their use in health systems. It discusses the need for an integrated and cyclical approach to managing health technology in order to mitigate clinical and financial risks and ensure acceptable value for money. A new governance framework is proposed to address current challenges faced by policy-makers.(2)
► OECD Press release, 16 January 2017. (1) Tackling wasteful spending on health. Paris: OECD Publishing; 2017 (12 pages).(2) New Health Technologies: Managing Access, Value and Sustainability. Paris: OECD Publishing; 2017 (228 pages). DOI: http://dx.doi.org/10.1787/9789264266438-en.
Calls for changes to European Commission’s R&D programmeA m s t e r d a m – Health Action International has released a joint position paper calling upon the European Commission to make substantial changes to how it funds research and development (R&D) projects for new medicines to allow for greater public access. The paper highlights the EU’s responsibility to ensure public returns on its R&D investments, reducing the major inequalities
that persist in the quality of healthcare available in EU Member States
The call comes after the Commission’s public consultation for the mid-term review of the European Union’s (EU) Research and Innovation programme, Horizon 2020, which administers a funding pool of nearly €80 billion. At a time when there is general concern over high prices for new medicines such as cancer and hepatitis C products, the joint paper has been endorsed by many humanitarian groups.
► Health Action International (HAI). Press release, 2 February 2017.
Using human rights law to support access to medicinesTwo recent articles highlight the human rights approach to reimbursing expensive medicines. In the first article, the authors argue that while all patients have an equal right to access essential medicines, the order and timing of its fulfilment is gradual. This justifies ranking treatments for reimbursement, with more cost-effective treatments being included first.(1) The second article looks at thirteen national constitutions that include a state duty to provide access to essential medicines as part of the right to health. Nine of these constitutions were amended or adopted after 2008.(2) The research was conducted under a collaboration between the Medical Centre and the Faculty of Law at the University of Groningen in the Netherlands.
► (1) Perehudoff K, Toebes B, Hogerzeil H. A human rights-based approach to the reimbursement of expensive medicines. Bull World Health Organ 2016;94:935–6. doi: http://dx.doi.org/10.2471/BLT.15.166371.(2) Perehudoff K, Toebes B, Hogerzeil H. Essential Medicines in National Constitutions: Progress Since 2008. Health & Human Rights Journal 2016;18(1): 141-56.
Publications and events WHO Drug Information Vol. 31, No. 1, 2017
48
First MPP licence for anti-tuberculosis medicineG e n e v a – The Medicines Patent Pool (MPP) has signed a licence with Johns Hopkins University to facilitate the clinical development of sutezolid, an investigational antibiotic that has shown promise in the treatment of both drug-sensitive and drug-resistant tuberculosis. The exclusive, royalty-free licence covers all countries that have patents issued or pending for a combination therapy comprising sutezolid and two additional anti-tuberculosis medicines. The patent for sutezolid expired in 2014, but the patent for the use of sutezolid in combination therapy for tuberculosis – held jointly by Pfizer Inc and Johns Hopkins University – is valid until August 2029 in the countries in which it was filed.(1)
Public health groups have welcomed the move but warn that the deal lacks safeguards that would ensure worldwide affordability. They have also called on Pfizer and Sequella, who hold secondary patents and clinical data on sutezolid, to provide open access to all existing data.(2)
► (1) MPP Press release, 25 January 2017.
(2) MSF Access Campaign. Press release, 24 January 2017.
Medicines control
Papillomavirus vaccine review documents published A paper published in the Indian Journal of Medical Ethics makes available the procedural documents that were used in the EMA’s review of human papillomavirus (HPV) vaccine. The review, which was completed in November 2015, found that there was no evidence of an association between the HPV vaccines and two
dysautonomic syndromes (complex regional pain syndrome and postural orthostatic tachycardia syndrome), despite the existence of independently clustered reports (signals). The paper reveals the process that led to the conclusions of the EMA review.
► Jefferson T, Jørgensen L. Human papillomavirus vaccines, complex regional pain syndrome, postural orthostatic tachycardia syndrome, and autonomic dysfunction – a review of the regulatory evidence from the European Medicines Agency [Published online]. IJME. 2016; 2 (1 (NS)), 30.
New CIOMS guide on active vaccine surveillance G e n e v a – The Council for International Organizations of Medical Sciences (CIOMS) has announced the publication of its Guide to Active Vaccine Safety Surveillance. The Guide addresses the situation facing national immunization programmes and regulatory authorities when a new vaccine is being introduced and vaccine safety needs to be assured. It offers a structured process for evaluating whether significant knowledge gaps exist, whether passive safety surveillance is adequate, and if not, how active vaccine safety surveillance studies can be designed and implemented.
With novel vaccines on the horizon, many of which are likely to be introduced early and/or exclusively into countries with limited pharmacovigilance experience and infrastructure, there is an urgent need for guidance on generating reliable post-licensure safety assessment data.
► CIOMS. Guide to Active Vaccine Safety Surveillance. Report of CIOMS Working Group on Vaccine Safety. Geneva: Council for International Organizations of Medical Sciences (CIOMS); 2017. Available at: www.cioms.ch/

49
WHO Drug Information Vol. 31, No. 1, 2017 Publications and events
Measuring pharmaceutical systems strengtheningA recently published review article highlights the importance of policy, laws and governance as the central hub for an efficient and equitable system, with medicines regulatory functions to ensure the safety, efficacy and quality of pharmaceutical products and related services. The article proposes definitions for a pharmaceutical system and proposes seven components to measure pharmaceutical systems strengthening: (1) pharmaceutical products and related services; (2) policy, laws and governance; (3) regulatory systems; (4) innovation, research and development, manufacturing, and trade; (5) financing; (6) human resources; and (7) information.
► Hafner T, Walkowiak H, Lee D, Aboagye-Nyame F. Defining Pharmaceutical Systems Strengthening: Concepts to Enable Measurement. Health Policy and Planning Journal 2016; Health Policy and Planning 2016; 1–13. doi: 10.1093/heapol/czw153.
Spotlight on flawed bioequivalence trials in IndiaH y d e r a b a d – An online Reuters article has highlighted the dangers of “India’s flawed generic drugs trials business”. More than a dozen volunteers interviewed by Reuters across four Indian cities said that they participated in as many studies as possible to earn money, waiting much less than the internationally recommended 90 days between trials. This waiting period is needed to protect the health of study participants and ensure the validity of the trial data.
In recent years, there has been increasing concern about the integrity of data generated at Indian contract research organizations. In 2015, the EMA suspended more than 700 generic products because of issues with the
bioequivalence data submitted in support of their marketing authorization applications.
► Reuters Health News, 27 December 2016.
Medicines use
Over- and underuse of health care interventionsA series of articles published in The Lancet shows that underuse of proven medical care and overuse of unproven services exist side by side in all economic settings, causing suffering to millions of people as well as wasteful misallocation of resources for society.
In the final paper of the series the authors argue that overuse and underuse are symptoms of a health-care system that does not reflect the ethics of medicine and that, with universal health coverage adopted as a target under the UN Sustainable Development Goals, focusing the world’s attention on achieving the right care is both an urgent task and an enormous opportunity.
The authors conclude that the deepest drivers of poor care arise out of fundamental inequalities of information, wealth and power. The path to the right care will therefore require more data on medicines use, a deeper understanding of care delivery as a science, political consensus for redirecting investments towards new, more balanced delivery models, and leadership from clinicians to create an activated, informed and mobilized citizenry.
A comment to the series points out that WHO and other bodies have courageously led moves to increase patient safety and to reduce inappropriate use of antimicrobial agents, and that they should also engage in promoting strategies to reduce the overuse of ineffective care.
► The Lancet Right Care series. http://www.thelancet.com/series/right-care
Publications and events WHO Drug Information Vol. 31, No. 1, 2017
50
Disease updates
Malaria: global targets jeopardizedG e n e v a – WHO has released its World Malaria Report 2016. According to the report, there were 212 million new cases of malaria and 429 000 deaths worldwide in 2015. Ten countries and territories reported fewer than 150 indigenous cases of malaria, and a further nine countries reported between 150 and 1000 cases. Kyrgyzstan and Sri Lanka were recently certified by WHO to have eliminated malaria, having achieved at least three consecutive years of zero indigenous cases.
Sub-Saharan Africa accounted for to 90% of malaria cases and 92% of malaria deaths in 2015. Children under five years accounted for an estimated 70% of all malaria deaths globally. The report shows that children and pregnant women in sub-Saharan Africa have greater access to effective malaria control, with a steep increase in diagnostic testing for children and preventive treatment for pregnant women reported over the last five years.
Funding shortfalls and fragile health systems are undermining overall progress, jeopardizing the attainment of the targets defined in the Global Technical Strategy for Malaria 2016-2030. Funding has flat-lined since 2010, totalling US$ 2.9 billion in 2015 or 45% of the 2020 funding milestone.
► WHO News release, 13 December 2016.WHO. World Malaria report 2016.
Ebola: vaccine shown to be effectiveG e n e v a – The results of a clinical trial conducted in Guinea on the rVSV-ZEBOV Ebola vaccine have been published in The Lancet. The trial was led by WHO, together with Guinea’s Ministry of Health, Médecins
sans Frontières and the Norwegian Institute of Public Health, in a unique collaboration with international partners. Its findings confirm that the vaccine is safe and provides high protection against the disease. Additional studies are ongoing to provide more data on the safety of the vaccine in children and other vulnerable populations such as people with HIV.
In January, GAVI, the Vaccine Alliance provided US$5 million to Merck towards the future procurement of the vaccine once it is approved, prequalified and recommended by WHO. As part of this agreement, Merck committed to ensure that 300 000 doses of the vaccine are available for emergency use in the interim, and to submit the vaccine for licensure by the end of 2017. Merck has also submitted the vaccine to WHO’s Emergency Use and Assessment Listing procedure (EUAL).
The rapid development of rVSV-ZEBOV contributed to the development of WHO’s R&D Blueprint, a global strategy to fast-track the development of effective tests, vaccines and medicines during epidemics.
► WHO News release, 23 December 2016.
Polio: public health emergency continuesG e n e v a – The Emergency Committee under the International Health Regulations (2005) (IHR) unanimously agreed that the international spread of poliovirus remains a Public Health Emergency of International Concern (PHEIC). At the recommendation of the Committee, the WHO Director-General extended the Temporary Recommendations for a further three months. The recommendations aim mainly at raising political awareness and official recognition of the emergency, ensuring strategic vaccination of people

51
WHO Drug Information Vol. 31, No. 1, 2017 Publications and events
at risk with documentation of people’s vaccination status, and maintaining surveillance and detection measures. The importance of regional cooperation and cross-border coordination was emphasized. The Committee urged all countries to avoid complacency which could easily lead to a polio resurgence.
► WHO Statement, 13 February 2017.
Cancer: WHO calls for early diagnosis;
G e n e v a – Ahead of World Cancer Day 2017, WHO has released new guidelines aiming to improve early diagnosis of cancer and ensure prompt treatment, especially for breast, cervical, and colorectal cancers. Treatment of cancer at an early stage is generally more effective, less complex and less expensive. Low- and middle-income countries tend to have the greatest challenges in providing effective diagnostic and treatment services. WHO encourages these countries to prioritize basic, high-impact and low-cost services and to reduce the need for out-of-pocket payment for these services to increase their uptake.(1)
According to new WHO figures cancer caused 8.8 million deaths in 2015, making it the second leading cause of death globally. Two thirds of cancer deaths occur in low- and middle-income countries. In 2010, the global economic cost of cancer through healthcare expenditure and loss of productivity was estimated at US$ 1.16 trillion. Approximately 14 million new cases occurred in 2012, and the incidence is expected to rise by about 70% over the next two decades.(2)
► (1) WHO News release, 3 February 2017.(2) WHO. Cancer. Fact sheet. Updated February 2017.
WHO matters
WHO data portal on health coverageG e n e v a – WHO has launched a new data portal to track progress towards universal health coverage. The portal features the latest data on access to health services globally and in each of WHO’s 194 Member States, along with information about equity of access. Next year WHO will add data on the impact that paying for health services has on household finances.
Universal health coverage is essential to achieving the targets of the Sustainable Development Goal (SDG) for good health and well-being, which will in turn support other SDGs. The portal highlights the areas where governments need to act to strengthen their health systems. For example it shows that less than half of children with suspected pneumonia in low income countries are taken to an appropriate health provider, that 44% of WHO Member States report having less than one physician per 1000 population, and that the African Region has only 3% of the world’s health workers although it bears almost 25% of the global burden of disease.
► WHO News release, 12 December 2016.
WHO Director-General supports new prequalification funding modelG e n e v a – The WHO Director-General expressed her support for the new financing arrangements, announced in September 2016, that are intended to make WHO Prequalification sustainable in the future. In her report to the WHO Executive Board she stated: “The programme is one of our most successful initiatives. It has transformed the market for public health vaccines and other medical products, making supplies more abundant and predictable and prices more
Publications and events WHO Drug Information Vol. 31, No. 1, 2017
52
affordable. In addition, the new financing model is designed to ensure equity among manufacturers, with provisions included to enable small manufacturers that meet quality standards to enter the market on an equal footing with large companies.”
► WHO. Report by the Director-General to the Executive Board at its 140th session. 23 January 2017.
New medicines invited for prequalificationG e n e v a – The WHO Prequalification Team–Medicines (PQT) has published new invitations for expression of interest (EOI) for product evaluation. In the area of reproductive health the newly eligible products include benzathine benzylpenicillin and procaine benzylpenicillin injectables. Products added for neglected tropical diseases include miltefosine capsules, injectable sodium stibogluconate, injectable paromomycin as well as azithromycin tablets. The respective active pharmaceutical ingredients (API) have been added to the EOI for APIs. Details are found in the EOIs listed below, available on the WHO prequalification website.
► WHO PQT. 8th EOI for Reproductive Health. 22 December 2016.WHO PQT. 5th EOI for Neglected Tropical Diseases. 9 February 2017.WHO PQT. 12th EOI for APIs. 27 December 2016.WHO PQT. 13th EOI for APIs. 15 February 2017.
New WHO prequalification websiteG e n e v a – The WHO Prequalification Team-Medicines has released its new website. The site has been reshaped to streamline the content, improve navigation and enhance
data retrieval and search features. Greater use is also made of visual elements.
The new website is the result of close collaboration with manufacturers, regulators, procurers, quality control laboratories and health workers and other stakeholders. Feedback was sought before the launch, and is still invited as a basis for further improvements if warranted. The websites of the prequalification workstreams for vaccines and diagnostics will also be reviewed and updated.
► WHO. Essential Medicines and Health Products: Prequalification of medicines [website]. https://extranet.who.int/prequal
Upcoming events
2017 joint UNICEF–UNFPA–WHO manufacturers meeting The 2017 joint UNICEF–UNFPA–WHO manufacturers meeting will take place in Copenhagen, Denmark, on 18–21 September 2017. Due to a clash of meeting events it was not possible to hold a joint UNICEF–UNFPA–WHO meeting in 2016.
The joint manufacturers meeting provides information for suppliers of medical products for use by UN agencies and other international organizations.
► WHO Prequalification website. Events. å

53
WHO Drug Information Vol. 31, No. 1, 2017
Consultation documents
To receive draft monographs by email please contact Mrs Wendy Bonny ([email protected]), stating that you wish to be added to the electronic mailing list.
The International Pharmacopoeia
Ganciclovir(Ganciclovirum)
This is a draft proposal of a monograph for The International Pharmacopoeia (Working document QAS/16.652, January 2017).
The working document with line numbers is available for comment at www.who.int/medicines/areas/quality_safety/quality_assurance/projects. Please address any comments to: World Health Organization, Quality Assurance and Safety: Medicines, Dr Herbert Schmidt, 1211 Geneva 27, Switzerland; fax: +41 22 791 4730; email: [email protected].
Molecular formula. C9H13N5O4
Relative molecular mass. 255.23
Graphic formula
Chemical name. 2-Amino-9-[[2-hydroxy-1-(hydroxymethyl)ethoxy]methyl]-1,9-dihydro-6H-purin-6-one. CAS Reg. No. 82410-32-0.
Description. White or almost white, crystalline powder.
Solubility. Slightly soluble in water or glacial acetic acid, practically insoluble in methanol and dichloromethane. It dissolves in dilute solutions of mineral acids and alkali hydroxides.
Category. Antiviral (Purine nucleoside analogue).
Storage. Preserve in well-closed containers. Protect from light and moisture.
Additional information. Ganciclovir is hygroscopic and may exhibit polymorphism.
Consultation documents WHO Drug Information Vol. 31, No. 1, 2017
54
Requirements
Definition. Ganciclovir contains not less than 99.0% and not more than 101.0% of C9H13N5O4, calculated with reference to the anhydrous substance.
Identity testsEither test A alone, or any two of tests B, C and D may be applied.
A. Carry out the test as described under 1.7 Spectrophotometry in the infrared region. The infrared absorption spectrum is concordant with the spectrum obtained from ganciclovir RS or with the reference spectrum of ganciclovir. If the spectra thus obtained are not concordant, repeat the test using the residues obtained by separately dissolving the test substance and ganciclovir RS in a small amount of hot water R (80°C), allowing to cool in an ice-bath, filtering and drying the precipitate at 105°C for 3 hours. The infrared absorption spectrum is concordant with the spectrum obtained from ganciclovir RS.
B. Carry out test B.1 or, where UV detection is not available, test B.2.B.1 Carry out the test as described under 1.14.1 Thin-layer chromatography using silica gel R6 as
the coating substance and a mixture of 4 volumes of ammonia (260 g/L) TS, 40 volumes of methanol R and 60 volumes of dichloromethane R as the mobile phase. Apply separately to the plate 5 μL of each of the following three solutions. For solution (A) dissolve 10 mg of the substance to be examined in 2 mL of sodium hydroxide (~0.8 g/L) TS and dilute to 10 mL with methanol R. For solution (B) dissolve 10 mg of ganciclovir RS in 2 mL of sodium hydroxide (~0.8 g/L) TS and dilute to 10 mL with methanol R. For solution (C) dissolve 10 mg of ganciclovir RS and 10 mg of aciclovir R in 2 mL of sodium hydroxide (~0.8 g/L) TS and dilute to 10 mL with methanol R. After removing the plate from the chromatographic chamber allow it to dry exhaustively in air and examine the chromatogram under ultraviolet light (254 nm). The test is not valid unless the chromatogram obtained with solution (C) shows two clearly separated spots. The principal spot in the chromatogram obtained with solution (A) corresponds in position, appearance and intensity with the spot due to ganciclovir in the chromatogram obtained with solution (B).
B.2 Carry out the test as described under 1.14.1 Thin-layer chromatography using the conditions described above under test B.1 but using silica gel R5 as the coating substance. After removing the plate from the chromatographic chamber allow it to dry exhaustively in air or heat the plate for five minutes at 120°C. Spray the plate with Dragendorff reagent TS and allow it to dry exhaustively in air.Then spray the plate with a mixture of sulfuric acid (~1760 g/L) TS and dehydrated ethanol R (1:1). Examine the chromatogram in daylight. The test is not valid unless the chromatogram obtained with solution (C) shows two clearly separated spots. The principal spot in the chromatogram obtained with solution (A) corresponds in position, appearance and intensity with the spot due to ganciclovir in the chromatogram obtained with solution (B).
C. Carry out the test as described under 1.14.4 High-performance liquid chromatography using the conditions given under “Related substances”. The retention time of the principal peak in the chromatogram obtained with solution (1) corresponds to the retention time of the ganciclovir peak in the chromatogram obtained with solution (3).
D. Dissolve about 5 mg of the sample in 500 mL of water R. The absorption spectrum (1.6) of this solution, when observed between 200 nm and 300 nm, exhibits a minimum at about 222 nm and maximum at about 252 nm with a shoulder at about 275 nm.

55
WHO Drug Information Vol. 31, No. 1, 2017 Consultation documents
Clarity and colour of solution. Dissolve 1.25 g in sodium hydroxide (~40 g/L) TS and dilute to 25 mL. This solution is clear and not more intensely coloured than reference solution Y5, when compared as described under 1.11.2 Degree of coloration of liquids, Method II. [Note from the Secretariat. The chapter 1.11 Colour of liquids is currently under revision. Reference is already made to a new test procedure to be added under the section 1.11.2 Degree of coloration of liquids.]
Heavy metals. Use 1.0 g for the preparation of the test solution as described under 2.2.3 Limit test for heavy metals, Procedure 3; determine the content of heavy metals according to Method A; not more than 10 μg/g.
Sulfated ash (2.3). Not more than 1.0 mg/g.
Water. Determine as described under 2.8 Determination of water by the Karl Fischer method, Method A, using 0.3 g of the substance and methanol as solvent. The substance to be examined has a limited solubility in methanol and will appear as a slurry. Replace the solvent after each titration. The water content is not more than 40 mg/g.
Related substances. Carry out the test as described under 1.14.4 High performance liquid chromatography using a stainless steel column (25 cm × 4.6 mm) packed with particles of silica gel, the surface of which has been modified with chemically-bonded strong acidic cation-exchange groups (3–10 μm).1
Use the following mobile phase: Dilute 0.5 mL of trifluoroacetic acid R to 1000 mL with water R. Mix 500 volumes of this solution with 500 volumes of acetonitrile R.
Operate with a flow rate of 1.5 mL per minute. As a detector use an ultraviolet spectrophotometer set at a wavelength of 254 nm. Maintain the column at 40°C.
Prepare the following solutions using mobile phase as a diluent. For solution (1) dissolve about 30 mg of the test substance using sonication and dilute to 50.0 mL. For solution (2) dilute 1.0 mL of solution (1) to 100.0 mL. Dilute 1.0 mL of this solution to 10.0 mL. For solution (3) dissolve 3.0 mg of ganciclovir RS using sonication and dilute to 5.0 mL. For solution (4) dissolve the content of a vial of ganciclovir for system suitability RS (containing the impurities A, B, C, D, E and F) in 1.0 mL of solution (3).
Inject alternately 20 μL each of solutions (1), (2), (3) and (4). Record the chromatograms for about 2.5 times the retention time of ganciclovir (retention time about 14 minutes).
Use the chromatogram supplied with ganciclovir for system suitability RS and the chromatograms obtained with reference solution (3) and (4) to identify the peaks due to ganciclovir and the impurities A, B, C, D, E and F. The following peaks are eluted at the following relative retention with reference to the peak of ganciclovir: impurity A about 0.6; impurity B about 0.67; impurity C about 0.71; impurity D about 0.8; impurity E about 0.9; impurity F about 2.0.
The test is not valid unless in the chromatogram obtained with solution (4) the peak-to-valley ratio (Hp/Hv) is at least 5, where Hp is the height above the baseline of the peak due to impurity E and Hv is the height above the baseline of the lowest point of the curve separating this peak from the peak due to ganciclovir.
1 A Thermo BioBasic SCX column (4.6 mm × 250 mm, 5 µm) has been found suitable.
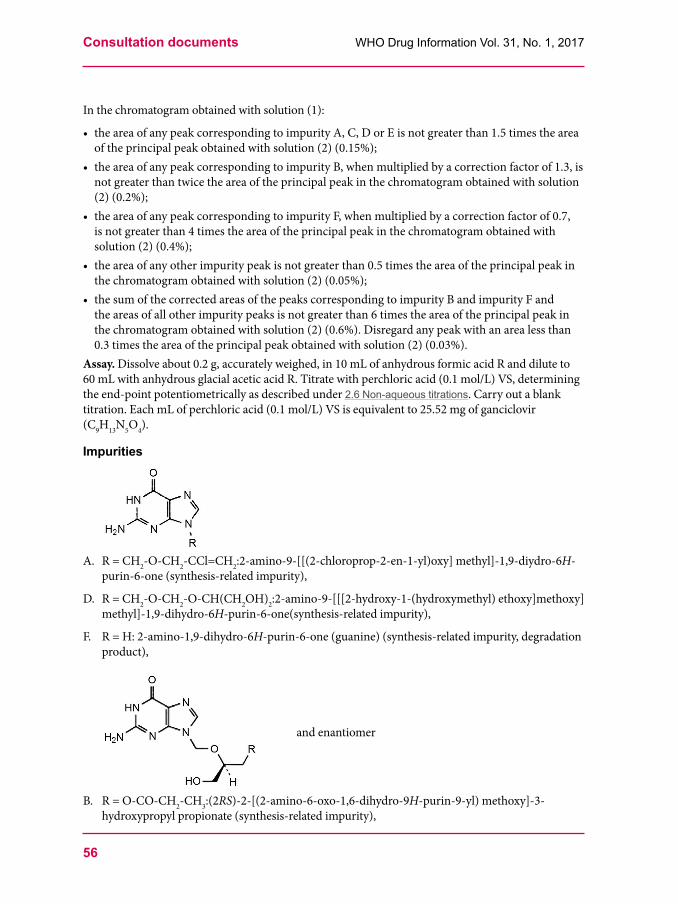
Consultation documents WHO Drug Information Vol. 31, No. 1, 2017
56
In the chromatogram obtained with solution (1):
• the area of any peak corresponding to impurity A, C, D or E is not greater than 1.5 times the area of the principal peak obtained with solution (2) (0.15%);
• the area of any peak corresponding to impurity B, when multiplied by a correction factor of 1.3, is not greater than twice the area of the principal peak in the chromatogram obtained with solution (2) (0.2%);
• the area of any peak corresponding to impurity F, when multiplied by a correction factor of 0.7, is not greater than 4 times the area of the principal peak in the chromatogram obtained with solution (2) (0.4%);
• the area of any other impurity peak is not greater than 0.5 times the area of the principal peak in the chromatogram obtained with solution (2) (0.05%);
• the sum of the corrected areas of the peaks corresponding to impurity B and impurity F and the areas of all other impurity peaks is not greater than 6 times the area of the principal peak in the chromatogram obtained with solution (2) (0.6%). Disregard any peak with an area less than 0.3 times the area of the principal peak obtained with solution (2) (0.03%).
Assay. Dissolve about 0.2 g, accurately weighed, in 10 mL of anhydrous formic acid R and dilute to 60 mL with anhydrous glacial acetic acid R. Titrate with perchloric acid (0.1 mol/L) VS, determining the end-point potentiometrically as described under 2.6 Non-aqueous titrations. Carry out a blank titration. Each mL of perchloric acid (0.1 mol/L) VS is equivalent to 25.52 mg of ganciclovir (C9H13N5O4).
Impurities
A. R = CH2-O-CH2-CCl=CH2:2-amino-9-[[(2-chloroprop-2-en-1-yl)oxy] methyl]-1,9-diydro-6H-purin-6-one (synthesis-related impurity),
D. R = CH2-O-CH2-O-CH(CH2OH)2:2-amino-9-[[[2-hydroxy-1-(hydroxymethyl) ethoxy]methoxy]methyl]-1,9-dihydro-6H-purin-6-one(synthesis-related impurity),
F. R = H: 2-amino-1,9-dihydro-6H-purin-6-one (guanine) (synthesis-related impurity, degradation product),
and enantiomer
B. R = O-CO-CH2-CH3:(2RS)-2-[(2-amino-6-oxo-1,6-dihydro-9H-purin-9-yl) methoxy]-3-hydroxypropyl propionate (synthesis-related impurity),
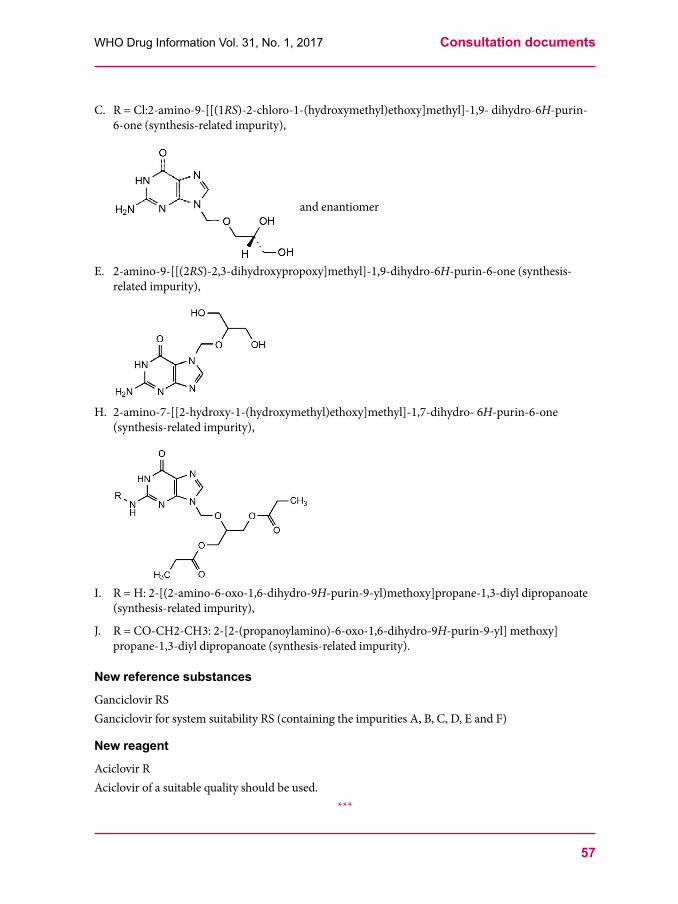
57
WHO Drug Information Vol. 31, No. 1, 2017 Consultation documents
C. R = Cl:2-amino-9-[[(1RS)-2-chloro-1-(hydroxymethyl)ethoxy]methyl]-1,9- dihydro-6H-purin-6-one (synthesis-related impurity),
and enantiomer
E. 2-amino-9-[[(2RS)-2,3-dihydroxypropoxy]methyl]-1,9-dihydro-6H-purin-6-one (synthesis-related impurity),
H. 2-amino-7-[[2-hydroxy-1-(hydroxymethyl)ethoxy]methyl]-1,7-dihydro- 6H-purin-6-one (synthesis-related impurity),
I. R = H: 2-[(2-amino-6-oxo-1,6-dihydro-9H-purin-9-yl)methoxy]propane-1,3-diyl dipropanoate (synthesis-related impurity),
J. R = CO-CH2-CH3: 2-[2-(propanoylamino)-6-oxo-1,6-dihydro-9H-purin-9-yl] methoxy]propane-1,3-diyl dipropanoate (synthesis-related impurity).
New reference substances
Ganciclovir RSGanciclovir for system suitability RS (containing the impurities A, B, C, D, E and F)
New reagent
Aciclovir RAciclovir of a suitable quality should be used.
***

Consultation documents WHO Drug Information Vol. 31, No. 1, 2017
58
Ganciclovir for injection(Gancicloviri ad injectionem)
This is a draft proposal of a monograph for The International Pharmacopoeia (Working document QAS/16.653, January 2017). The working document with line numbers is available for comment at www.who.int/medicines/areas/quality_safety/quality_assurance/projects. Please address any comments to: World Health Organization, Quality Assurance and Safety: Medicines, Dr Herbert Schmidt, 1211 Geneva 27, Switzerland; fax: +41 22 791 4730; email: [email protected].
Description. A white powder or loose lumps.Category. Antiviral (Purine nucleoside analogue).Storage. Ganciclovir for injection should be kept in a tightly closed container, protected from moisture and light.Additional information. Ganciclovir for injection 500 mg is listed on the 12th invitation to manufacturers of medicinal products for HIV infection and related diseases to submit an Expression of Interest (EOI) for product evaluation to the WHO Prequalification of Medicines Team. Handle Ganciclovir for injection with great care because it is a potent cytotoxic agent and suspected carcinogen.Ganciclovir for injection is hygroscopic.
Requirements
The powder for injection and the reconstituted solution for injection complies with the monograph for Parenteral preparations.Definition. Ganciclovir for injection is a freeze-dried powder prepared by the neutralization of Ganciclovir with the aid of sodium hydroxide. Ganciclovir for injection contains not less than 90.0% and not more than 110.0% of the labelled amount of ganciclovir (C9H13N5O4).
Identity tests Either test A alone or any two of tests B, C and D may be applied.A. Dilute a quantity of the test substance, containing the equivalent of about 0.2 g of Ganciclovir
with 10 mL water R. Adjust the suspension to pH 6–7 with hydrochloric acid (0.1 mol/L) TS and allow to stand for 30 minutes. Filter the suspension, wash the filtrate with 20 mL water R and dry it at 105°C for 3 hours. Carry out the test as described under 1.7 Spectrophotometry in the infrared region. The infrared absorption spectrum is concordant with the reference spectrum of ganciclovir or with the spectrum obtained from ganciclovir RS treated similarly. If the spectra thus obtained are not concordant repeat the test using the residues obtained by separately dissolving the dried filtrate and ganciclovir RS in a small amount of hot water R (80°C), allowing to cool in an ice-bath, filtering and drying the precipitate at 105°C for 3 hours. The infrared absorption spectrum is concordant with the spectrum obtained from ganciclovir RS.
B. Carry out test B.1 or, where UV detection is not available, test B.2.
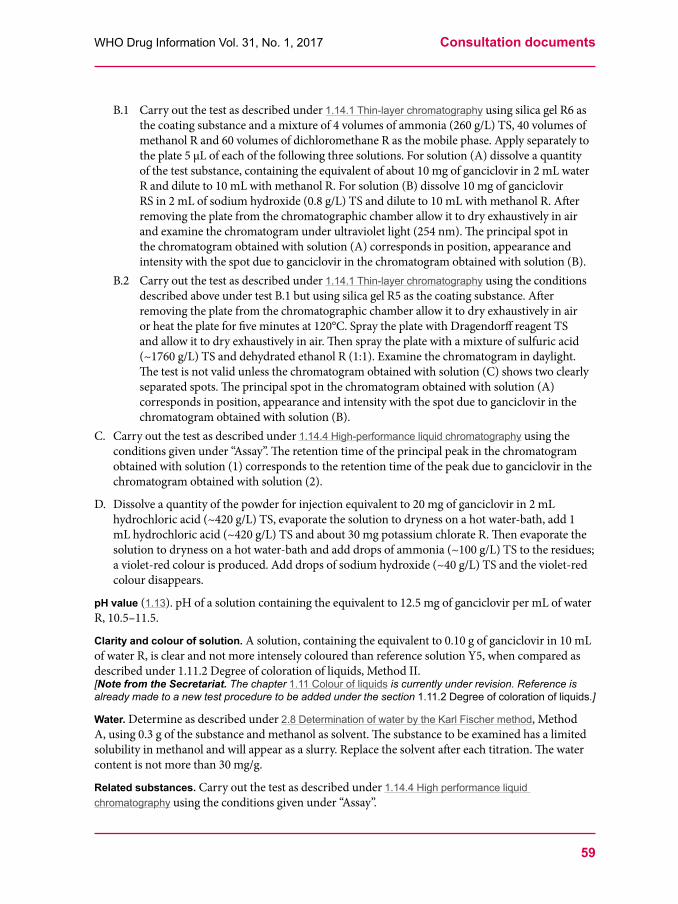
59
WHO Drug Information Vol. 31, No. 1, 2017 Consultation documents
B.1 Carry out the test as described under 1.14.1 Thin-layer chromatography using silica gel R6 as the coating substance and a mixture of 4 volumes of ammonia (260 g/L) TS, 40 volumes of methanol R and 60 volumes of dichloromethane R as the mobile phase. Apply separately to the plate 5 μL of each of the following three solutions. For solution (A) dissolve a quantity of the test substance, containing the equivalent of about 10 mg of ganciclovir in 2 mL water R and dilute to 10 mL with methanol R. For solution (B) dissolve 10 mg of ganciclovir RS in 2 mL of sodium hydroxide (0.8 g/L) TS and dilute to 10 mL with methanol R. After removing the plate from the chromatographic chamber allow it to dry exhaustively in air and examine the chromatogram under ultraviolet light (254 nm). The principal spot in the chromatogram obtained with solution (A) corresponds in position, appearance and intensity with the spot due to ganciclovir in the chromatogram obtained with solution (B).
B.2 Carry out the test as described under 1.14.1 Thin-layer chromatography using the conditions described above under test B.1 but using silica gel R5 as the coating substance. After removing the plate from the chromatographic chamber allow it to dry exhaustively in air or heat the plate for five minutes at 120°C. Spray the plate with Dragendorff reagent TS and allow it to dry exhaustively in air. Then spray the plate with a mixture of sulfuric acid (~1760 g/L) TS and dehydrated ethanol R (1:1). Examine the chromatogram in daylight. The test is not valid unless the chromatogram obtained with solution (C) shows two clearly separated spots. The principal spot in the chromatogram obtained with solution (A) corresponds in position, appearance and intensity with the spot due to ganciclovir in the chromatogram obtained with solution (B).
C. Carry out the test as described under 1.14.4 High-performance liquid chromatography using the conditions given under “Assay”. The retention time of the principal peak in the chromatogram obtained with solution (1) corresponds to the retention time of the peak due to ganciclovir in the chromatogram obtained with solution (2).
D. Dissolve a quantity of the powder for injection equivalent to 20 mg of ganciclovir in 2 mL hydrochloric acid (~420 g/L) TS, evaporate the solution to dryness on a hot water-bath, add 1 mL hydrochloric acid (~420 g/L) TS and about 30 mg potassium chlorate R. Then evaporate the solution to dryness on a hot water-bath and add drops of ammonia (~100 g/L) TS to the residues; a violet-red colour is produced. Add drops of sodium hydroxide (~40 g/L) TS and the violet-red colour disappears.
pH value (1.13). pH of a solution containing the equivalent to 12.5 mg of ganciclovir per mL of water R, 10.5–11.5.
Clarity and colour of solution. A solution, containing the equivalent to 0.10 g of ganciclovir in 10 mL of water R, is clear and not more intensely coloured than reference solution Y5, when compared as described under 1.11.2 Degree of coloration of liquids, Method II. [Note from the Secretariat. The chapter 1.11 Colour of liquids is currently under revision. Reference is already made to a new test procedure to be added under the section 1.11.2 Degree of coloration of liquids.]
Water. Determine as described under 2.8 Determination of water by the Karl Fischer method, Method A, using 0.3 g of the substance and methanol as solvent. The substance to be examined has a limited solubility in methanol and will appear as a slurry. Replace the solvent after each titration. The water content is not more than 30 mg/g.
Related substances. Carry out the test as described under 1.14.4 High performance liquid chromatography using the conditions given under “Assay”.

Consultation documents WHO Drug Information Vol. 31, No. 1, 2017
60
Prepare the following solutions using mobile phase as a diluent. For test solution (1) dissolve using sonication a quantity of the powder for injection, containing the equivalent of about 30 mg ganciclovir, and dilute to 50.0 mL. For solution (2) dilute 1.0 mL of solution (1) to 100 mL. Dilute 1.0 mL of this solution to 10.0 mL. For solution (3) dissolve using sonication 3.0 mg of ganciclovir RS and dilute to 5.0 mL. For solution (4) dissolve the content of a vial of ganciclovir for system suitability RS (containing the impurities A, B, C, D, E and F) in 1.0 mL of solution (3).Inject alternately 20 μL each of solutions (1), (2), (3) and (4). Record the chromatograms for 2.5 times of the retention time of ganciclovir (retention time about 14 minutes).Use the chromatogram supplied with ganciclovir for system suitability RS and the chromatogram obtained with reference solution (4) to identify the peaks due to ganciclovir and the impurities A, B, C, D, E and F. The following peaks are eluted at the following relative retention with reference to the peak of ganciclovir: impurity A = about 0.6; impurity B = about 0.67; impurity C = about 0.71; impurity D = about 0.8; impurity E = about 0.9; impurity F = about 2.0.The test is not valid unless in the chromatogram obtained with solution (4) the peak-to-valley ratio (Hp/Hv) is at least 5, where Hp is the height above the baseline of the peak due to impurity E and Hv is the height above the baseline of the lowest point of the curve separating this peak from the peak due to ganciclovir.In the chromatogram obtained with solution (1): • the area of any peak corresponding to impurity F, when multiplied by a correction factor of 0.7, is
not greater than 4 times the area of the principal peak in the chromatogram obtained with solution (2) (0.4%);
Assay. Carry out the test as described under 1.14.4 High-performance liquid chromatography using a stainless steel column (25 cm × 4.6 mm) packed with particles of silica gel, the surface of which has been modified with chemically-bonded strong acidic cation-exchange groups (3–10 μm).1
Use the following mobile phase: Dilute 0.5 mL of trifluoroacetic acid R to 1000 mL with water R. Mix 500 volumes of this solution with 500 volumes of acetonitrile R.Operate with a flow rate of 1.5 mL per minute. As a detector use an ultraviolet spectrophotometer set at a wavelength of 254 nm. Maintain the column at 40°C.Weigh and mix the contents of 5 containers. Prepare the following solutions in mobile phase. For solution (1) dissolve a quantity of the powder of injection, equivalent to about 30 mg of ganciclovir, accurately weighed, and dilute to 50.0 mL. Dilute 10.0 mL of this solution to 100.0 mL. For solution (2) dissolve 15.0 mg of ganciclovir RS, and dilute to 25.0 mL. Dilute 10.0 mL of this solution to 100.0 mL.Inject alternately 20 µL each of solution (1) and (2). Measure the areas of the peaks corresponding to ganciclovir in the chromatograms of solution (1) and (2) and calculate the percentage content of ganciclovir (C9H13N5O4) per container, using the declared content of C9H13N5O4 in ganciclovir RS. Bacterial endotoxins. Carry out the test as described under 3.4 Test for bacterial endotoxins; contains not more than 0.50 IU of endotoxin per mg of ganciclovir.
Impurities• The impurities limited by the requirements of this monograph include impurity B listed in the
monograph on Ganciclovir.***
1 The Thermo BioBasic SCX column (4.6 mm × 250 mm, 5 µm) has been found suitable.
WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
61
International Nonproprietary Names for Pharmaceutical Substances (INN) RECOMMENDED International Nonproprietary Names: List 77
Notice is hereby given that, in accordance with paragraph 7 of the Procedure for the Selection of Recommended International Nonproprietary Names for Pharmaceutical Substances [Off. Rec. Wld Health Org., 1955, 60, 3 (Resolution EB15.R7); 1969, 173, 10 (Resolution EB43.R9); Resolution EB115.R4 (EB115/2005/REC/1)], the following names are selected as Recommended International Nonproprietary Names. The inclusion of a name in the lists of Recommended International Nonproprietary Names does not imply any recommendation of the use of the substance in medicine or pharmacy. Lists of Proposed (1–113) and Recommended (1–74) International Nonproprietary Names can be found in Cumulative List No. 16, 2015 (available in CD-ROM only).
Dénominations communes internationales des Substances pharmaceutiques (DCI)
Dénominations communes internationales RECOMMANDÉES: Liste 77
Il est notifié que, conformément aux dispositions du paragraphe 7 de la Procédure à suivre en vue du choix de Dénominations communes internationales recommandées pour les Substances pharmaceutiques [Actes off. Org. mond. Santé, 1955, 60, 3 (résolution EB15.R7); 1969, 173, 10 (résolution EB43.R9); résolution EB115.R4 (EB115/2005/REC/1)] les dénominations ci-dessous sont choisies par l’Organisation mondiale de la Santé en tant que dénominations communes internationales recommandées. L’inclusion d’une dénomination dans les listes de DCI recommandées n’implique aucune recommandation en vue de l’utilisation de la substance correspondante en médecine ou en pharmacie. On trouvera d’autres listes de Dénominations communes internationales proposées (1–113) et recommandées (1–74) dans la Liste récapitulative No. 16, 2015 (disponible sur CD-ROM seulement).
Denominaciones Comunes Internacionales para las Sustancias Farmacéuticas (DCI)
Denominaciones Comunes Internacionales RECOMENDADAS: Lista 77
De conformidad con lo que dispone el párrafo 7 del Procedimiento de Selección de Denominaciones Comunes Internacionales Recomendadas para las Sustancias Farmacéuticas [Act. Of. Mund. Salud, 1955, 60, 3 (Resolución EB15.R7); 1969, 173, 10 (Resolución EB43.R9); Résolution EB115.R4 (EB115/2005/REC/1) EB115.R4 (EB115/2005/REC/1)], se comunica por el presente anuncio que las denominaciones que a continuación se expresan han sido seleccionadas como Denominaciones Comunes Internacionales Recomendadas. La inclusión de una denominación en las listas de las Denominaciones Comunes Recomendadas no supone recomendación alguna en favor del empleo de la sustancia respectiva en medicina o en farmacia. Las listas de Denominaciones Comunes Internacionales Propuestas (1–113) y Recomendadas (1–74) se encuentran reunidas en Cumulative List No. 16, 2015 (disponible sólo en CD-ROM).
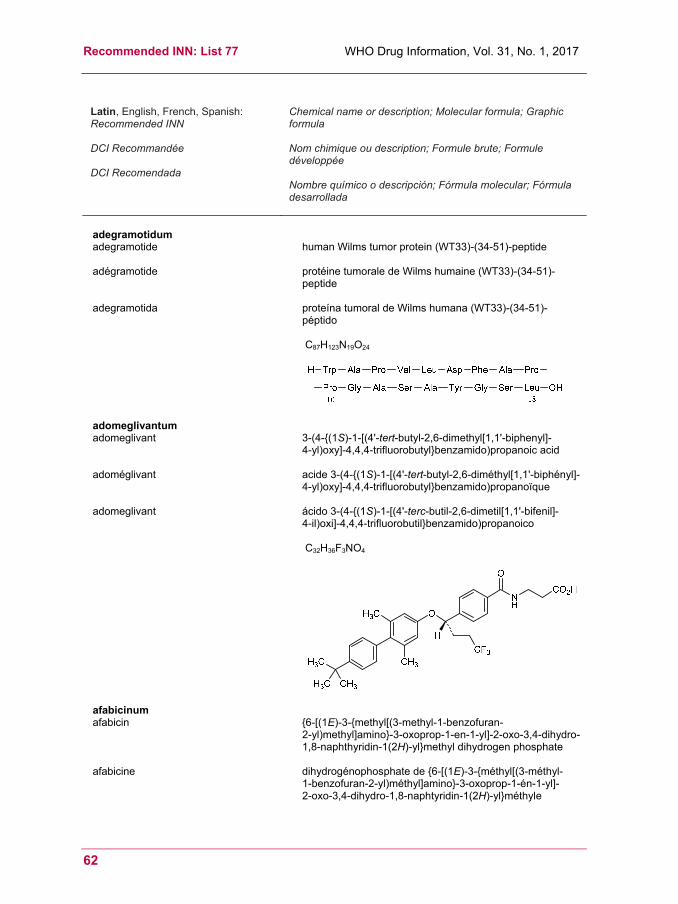
Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
62
Latin, English, French, Spanish: Recommended INN DCI Recommandée DCI Recomendada
Chemical name or description; Molecular formula; Graphic formula Nom chimique ou description; Formule brute; Formule développée Nombre químico o descripción; Fórmula molecular; Fórmula desarrollada
adegramotidum adegramotide human Wilms tumor protein (WT33)-(34-51)-peptide
adégramotide protéine tumorale de Wilms humaine (WT33)-(34-51)-
peptide
adegramotida proteína tumoral de Wilms humana (WT33)-(34-51)-péptido
C87H123N19O24
adomeglivantum adomeglivant 3-(4-{(1S)-1-[(4'-tert-butyl-2,6-dimethyl[1,1'-biphenyl]-
4-yl)oxy]-4,4,4-trifluorobutyl}benzamido)propanoic acid
adoméglivant acide 3-(4-{(1S)-1-[(4'-tert-butyl-2,6-diméthyl[1,1'-biphényl]-4-yl)oxy]-4,4,4-trifluorobutyl}benzamido)propanoïque
adomeglivant ácido 3-(4-{(1S)-1-[(4'-terc-butil-2,6-dimetil[1,1'-bifenil]- 4-il)oxi]-4,4,4-trifluorobutil}benzamido)propanoico
C32H36F3NO4
afabicinum afabicin {6-[(1E)-3-{methyl[(3-methyl-1-benzofuran-
2-yl)methyl]amino}-3-oxoprop-1-en-1-yl]-2-oxo-3,4-dihydro-1,8-naphthyridin-1(2H)-yl}methyl dihydrogen phosphate
afabicine dihydrogénophosphate de {6-[(1E)-3-{méthyl[(3-méthyl- 1-benzofuran-2-yl)méthyl]amino}-3-oxoprop-1-én-1-yl]- 2-oxo-3,4-dihydro-1,8-naphtyridin-1(2H)-yl}méthyle
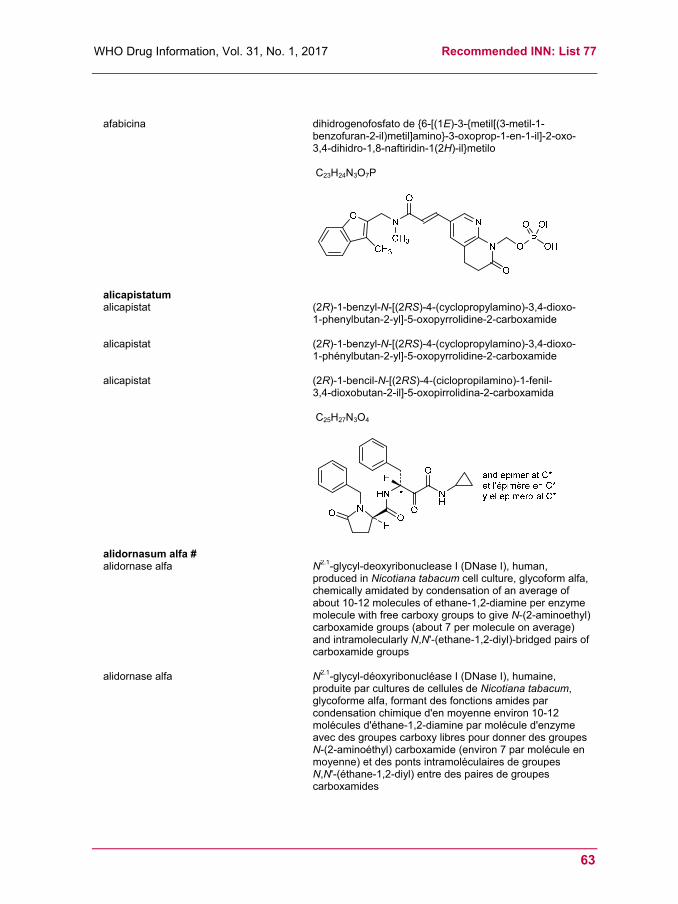
WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
63
afabicina
dihidrogenofosfato de {6-[(1E)-3-{metil[(3-metil-1-benzofuran-2-il)metil]amino}-3-oxoprop-1-en-1-il]-2-oxo-3,4-dihidro-1,8-naftiridin-1(2H)-il}metilo
C23H24N3O7P
alicapistatum alicapistat (2R)-1-benzyl-N-[(2RS)-4-(cyclopropylamino)-3,4-dioxo-
1-phenylbutan-2-yl]-5-oxopyrrolidine-2-carboxamide
alicapistat (2R)-1-benzyl-N-[(2RS)-4-(cyclopropylamino)-3,4-dioxo- 1-phénylbutan-2-yl]-5-oxopyrrolidine-2-carboxamide
alicapistat (2R)-1-bencil-N-[(2RS)-4-(ciclopropilamino)-1-fenil- 3,4-dioxobutan-2-il]-5-oxopirrolidina-2-carboxamida
C25H27N3O4
alidornasum alfa # alidornase alfa N2.1-glycyl-deoxyribonuclease I (DNase I), human,
produced in Nicotiana tabacum cell culture, glycoform alfa, chemically amidated by condensation of an average of about 10-12 molecules of ethane-1,2-diamine per enzyme molecule with free carboxy groups to give N-(2-aminoethyl) carboxamide groups (about 7 per molecule on average) and intramolecularly N,N'-(ethane-1,2-diyl)-bridged pairs of carboxamide groups
alidornase alfa N2.1-glycyl-déoxyribonucléase I (DNase I), humaine, produite par cultures de cellules de Nicotiana tabacum, glycoforme alfa, formant des fonctions amides par condensation chimique d'en moyenne environ 10-12 molécules d'éthane-1,2-diamine par molécule d'enzyme avec des groupes carboxy libres pour donner des groupes N-(2-aminoéthyl) carboxamide (environ 7 par molécule en moyenne) et des ponts intramoléculaires de groupes N,N'-(éthane-1,2-diyl) entre des paires de groupes carboxamides
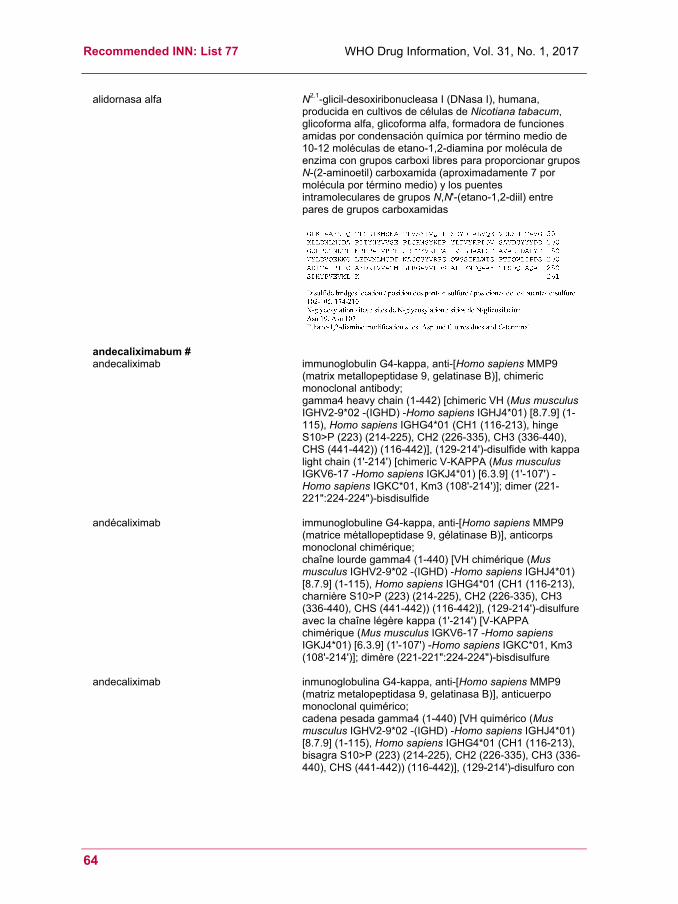
Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
64
alidornasa alfa N2.1-glicil-desoxiribonucleasa I (DNasa I), humana, producida en cultivos de células de Nicotiana tabacum, glicoforma alfa, glicoforma alfa, formadora de funciones amidas por condensación química por término medio de 10-12 moléculas de etano-1,2-diamina por molécula de enzima con grupos carboxi libres para proporcionar grupos N-(2-aminoetil) carboxamida (aproximadamente 7 por molécula por término medio) y los puentes intramoleculares de grupos N,N'-(etano-1,2-diil) entre pares de grupos carboxamidas
andecaliximabum # andecaliximab immunoglobulin G4-kappa, anti-[Homo sapiens MMP9
(matrix metallopeptidase 9, gelatinase B)], chimeric monoclonal antibody; gamma4 heavy chain (1-442) [chimeric VH (Mus musculus IGHV2-9*02 -(IGHD) -Homo sapiens IGHJ4*01) [8.7.9] (1-115), Homo sapiens IGHG4*01 (CH1 (116-213), hinge S10>P (223) (214-225), CH2 (226-335), CH3 (336-440), CHS (441-442)) (116-442)], (129-214')-disulfide with kappa light chain (1'-214') [chimeric V-KAPPA (Mus musculus IGKV6-17 -Homo sapiens IGKJ4*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 (108'-214')]; dimer (221-221":224-224")-bisdisulfide
andécaliximab immunoglobuline G4-kappa, anti-[Homo sapiens MMP9 (matrice métallopeptidase 9, gélatinase B)], anticorps monoclonal chimérique; chaîne lourde gamma4 (1-440) [VH chimérique (Mus musculus IGHV2-9*02 -(IGHD) -Homo sapiens IGHJ4*01) [8.7.9] (1-115), Homo sapiens IGHG4*01 (CH1 (116-213), charnière S10>P (223) (214-225), CH2 (226-335), CH3 (336-440), CHS (441-442)) (116-442)], (129-214')-disulfure avec la chaîne légère kappa (1'-214') [V-KAPPA chimérique (Mus musculus IGKV6-17 -Homo sapiens IGKJ4*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 (108'-214')]; dimère (221-221":224-224")-bisdisulfure
andecaliximab inmunoglobulina G4-kappa, anti-[Homo sapiens MMP9 (matriz metalopeptidasa 9, gelatinasa B)], anticuerpo monoclonal quimérico; cadena pesada gamma4 (1-440) [VH quimérico (Mus musculus IGHV2-9*02 -(IGHD) -Homo sapiens IGHJ4*01) [8.7.9] (1-115), Homo sapiens IGHG4*01 (CH1 (116-213), bisagra S10>P (223) (214-225), CH2 (226-335), CH3 (336-440), CHS (441-442)) (116-442)], (129-214')-disulfuro con

WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
65
la cadena ligera kappa (1'-214') [V-KAPPA quimérico (Mus musculus IGKV6-17 -Homo sapiens IGKJ4*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 (108'-214')]; dímero (221-221":224-224")-bisdisulfuro
apararenonum apararenone N-[4-(4-fluorophenyl)-2,2-dimethyl-3-oxo-3,4-dihydro-
2H-1,4-benzoxazin-7-yl]methanesulfonamide
apararénone N-[4-(4-fluorophényl)-2,2-diméthyl-3-oxo-3,4-dihydro- 2H-1,4-benzoxazin-7-yl]méthanesulfonamide
apararenona N-[4-(4-fluorofenil)-2,2-dimetil-3-oxo-3,4-dihidro- 2H-1,4-benzoxazin-7-il]metanosulfonamida
C17H17FN2O4S
apimostinelum apimostinel L-threonyl-L-prolyl-2-benzyl-L-prolyl-L-threoninamide
apimostinel L-thréonyl-L-prolyl-2-benzyl-L-prolyl-L-thréoninamide
apimostinel L-treonil-L-prolil-2-bencil-L-prolil-L-treoninamida
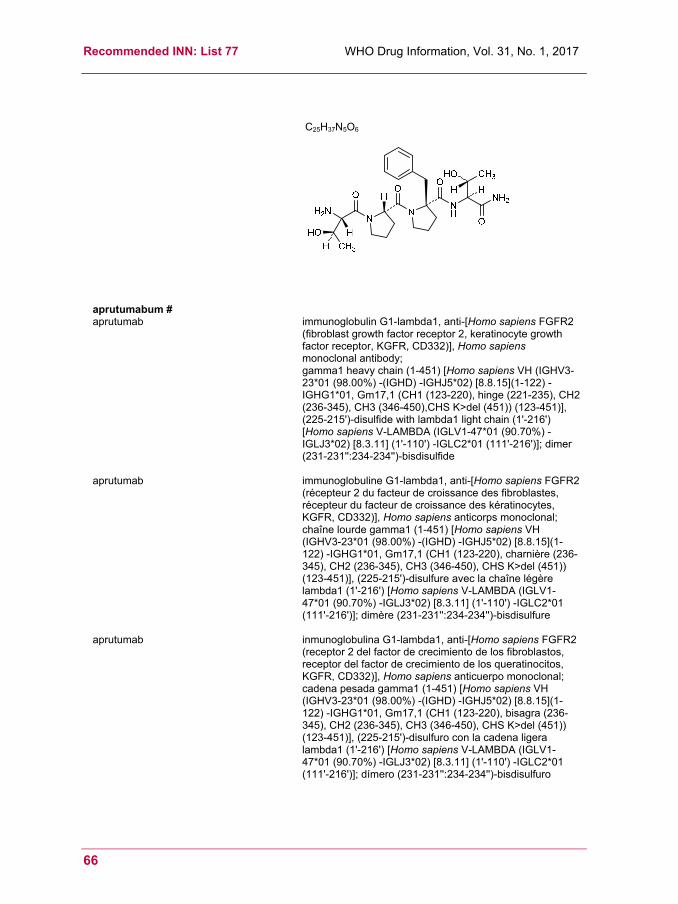
Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
66
C25H37N5O6
aprutumabum # aprutumab immunoglobulin G1-lambda1, anti-[Homo sapiens FGFR2
(fibroblast growth factor receptor 2, keratinocyte growth factor receptor, KGFR, CD332)], Homo sapiens monoclonal antibody; gamma1 heavy chain (1-451) [Homo sapiens VH (IGHV3-23*01 (98.00%) -(IGHD) -IGHJ5*02) [8.8.15](1-122) -IGHG1*01, Gm17,1 (CH1 (123-220), hinge (221-235), CH2 (236-345), CH3 (346-450),CHS K>del (451)) (123-451)], (225-215')-disulfide with lambda1 light chain (1'-216') [Homo sapiens V-LAMBDA (IGLV1-47*01 (90.70%) -IGLJ3*02) [8.3.11] (1'-110') -IGLC2*01 (111'-216')]; dimer (231-231'':234-234'')-bisdisulfide
aprutumab immunoglobuline G1-lambda1, anti-[Homo sapiens FGFR2 (récepteur 2 du facteur de croissance des fibroblastes, récepteur du facteur de croissance des kératinocytes, KGFR, CD332)], Homo sapiens anticorps monoclonal; chaîne lourde gamma1 (1-451) [Homo sapiens VH (IGHV3-23*01 (98.00%) -(IGHD) -IGHJ5*02) [8.8.15](1-122) -IGHG1*01, Gm17,1 (CH1 (123-220), charnière (236-345), CH2 (236-345), CH3 (346-450), CHS K>del (451)) (123-451)], (225-215')-disulfure avec la chaîne légère lambda1 (1'-216') [Homo sapiens V-LAMBDA (IGLV1-47*01 (90.70%) -IGLJ3*02) [8.3.11] (1'-110') -IGLC2*01 (111'-216')]; dimère (231-231'':234-234'')-bisdisulfure
aprutumab inmunoglobulina G1-lambda1, anti-[Homo sapiens FGFR2 (receptor 2 del factor de crecimiento de los fibroblastos, receptor del factor de crecimiento de los queratinocitos, KGFR, CD332)], Homo sapiens anticuerpo monoclonal; cadena pesada gamma1 (1-451) [Homo sapiens VH (IGHV3-23*01 (98.00%) -(IGHD) -IGHJ5*02) [8.8.15](1-122) -IGHG1*01, Gm17,1 (CH1 (123-220), bisagra (236-345), CH2 (236-345), CH3 (346-450), CHS K>del (451)) (123-451)], (225-215')-disulfuro con la cadena ligera lambda1 (1'-216') [Homo sapiens V-LAMBDA (IGLV1-47*01 (90.70%) -IGLJ3*02) [8.3.11] (1'-110') -IGLC2*01 (111'-216')]; dímero (231-231'':234-234'')-bisdisulfuro

WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
67
aprutumabum ixadotinum # aprutumab ixadotin immunoglobulin G1-lambda1, anti-[Homo sapiens FGFR2
(fibroblast growth factor receptor 2, keratinocyte growth factor receptor, KGFR, CD332)], Homo sapiens monoclonal antibody conjugated to an auristatin W derivative; gamma1 heavy chain (1-451) [Homo sapiens VH (IGHV3-23*01 (98.00%) -(IGHD) -IGHJ5*02) [8.8.15](1-122) -IGHG1*01, Gm17,1 (CH1 (123-220), hinge (221-235), CH2 (236-345), CH3 (346-450),CHS K>del (451)) (123-451)], (225-215')-disulfide with lambda1 light chain (1'-216') [Homo sapiens V-LAMBDA (IGLV1-47*01 (90.70%) -IGLJ3*02) [8.3.11] (1'-110') -IGLC2*01 (111'-216')]; dimer (231-231'':234-234'')-bisdisulfide; conjugated, on an average of 4 lysyl, to N-(5-carboxypentyl)-N-demethyl-auristatin W (AW) C1.5-(1,2-oxazinan-2-yl) derivative
aprutumab ixadotine immunoglobuline G1-lambda1, anti-[Homo sapiens FGFR2 (récepteur 2 du facteur de croissance des fibroblastes, récepteur du facteur de croissance des kératinocytes, KGFR, CD332)], Homo sapiens anticorps monoclonal conjugué à un dérivé de l'auristatine W; chaîne lourde gamma1 (1-451) [Homo sapiens VH (IGHV3-23*01 (98.00%) -(IGHD) -IGHJ5*02) [8.8.15](1-122) -IGHG1*01, Gm17,1 (CH1 (123-220), charnière (236-345), CH2 (236-345), CH3 (346-450), CHS K>del (451)) (123-451)], (225-215')-disulfure avec la chaîne légère lambda1 (1'-216') [Homo sapiens V-LAMBDA (IGLV1-47*01 (90.70%) -IGLJ3*02) [8.3.11] (1'-110') -IGLC2*01 (111'-216')]; dimère (231-231'':234-234'')-bisdisulfure; conjugué, sur 4 lysyl en moyenne, au dérivé C1.5-(1,2-oxazinan-2-yle) de N-(5-carboxypentyl)-N-desméthyl-auristatine W (AW)
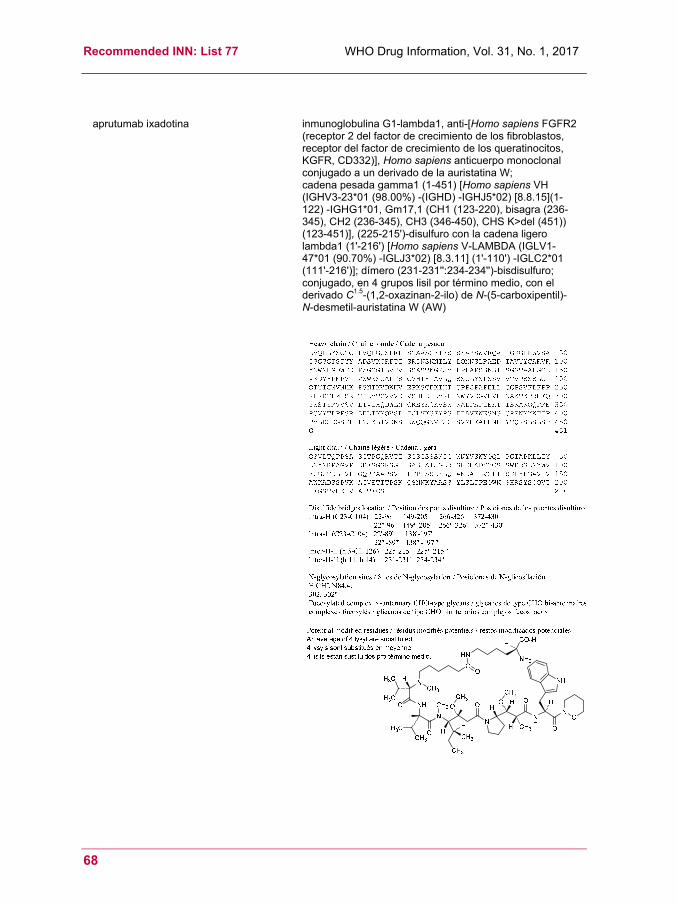
Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
68
aprutumab ixadotina
inmunoglobulina G1-lambda1, anti-[Homo sapiens FGFR2 (receptor 2 del factor de crecimiento de los fibroblastos, receptor del factor de crecimiento de los queratinocitos, KGFR, CD332)], Homo sapiens anticuerpo monoclonal conjugado a un derivado de la auristatina W; cadena pesada gamma1 (1-451) [Homo sapiens VH (IGHV3-23*01 (98.00%) -(IGHD) -IGHJ5*02) [8.8.15](1-122) -IGHG1*01, Gm17,1 (CH1 (123-220), bisagra (236-345), CH2 (236-345), CH3 (346-450), CHS K>del (451)) (123-451)], (225-215')-disulfuro con la cadena ligero lambda1 (1'-216') [Homo sapiens V-LAMBDA (IGLV1-47*01 (90.70%) -IGLJ3*02) [8.3.11] (1'-110') -IGLC2*01 (111'-216')]; dímero (231-231'':234-234'')-bisdisulfuro; conjugado, en 4 grupos lisil por término medio, con el derivado C1.5-(1,2-oxazinan-2-ilo) de N-(5-carboxipentil)- N-desmetil-auristatina W (AW)
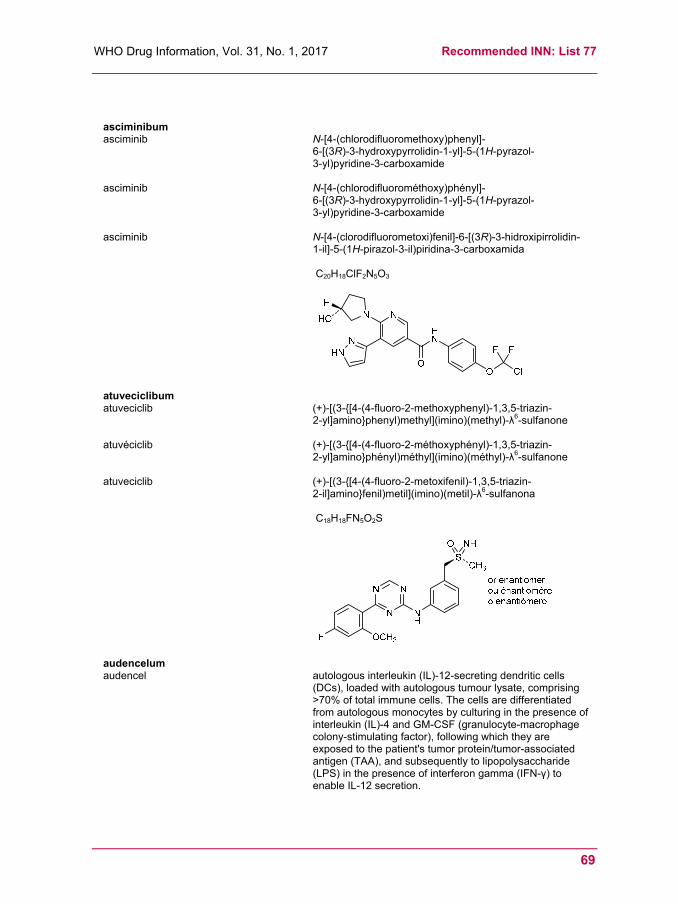
WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
69
asciminibum asciminib N-[4-(chlorodifluoromethoxy)phenyl]-
6-[(3R)-3-hydroxypyrrolidin-1-yl]-5-(1H-pyrazol- 3-yl)pyridine-3-carboxamide
asciminib N-[4-(chlorodifluorométhoxy)phényl]- 6-[(3R)-3-hydroxypyrrolidin-1-yl]-5-(1H-pyrazol- 3-yl)pyridine-3-carboxamide
asciminib N-[4-(clorodifluorometoxi)fenil]-6-[(3R)-3-hidroxipirrolidin- 1-il]-5-(1H-pirazol-3-il)piridina-3-carboxamida
C20H18ClF2N5O3
atuveciclibum atuveciclib (+)-[(3-{[4-(4-fluoro-2-methoxyphenyl)-1,3,5-triazin-
2-yl]amino}phenyl)methyl](imino)(methyl)-λ6-sulfanone
atuvéciclib (+)-[(3-{[4-(4-fluoro-2-méthoxyphényl)-1,3,5-triazin- 2-yl]amino}phényl)méthyl](imino)(méthyl)-λ6-sulfanone
atuveciclib (+)-[(3-{[4-(4-fluoro-2-metoxifenil)-1,3,5-triazin- 2-il]amino}fenil)metil](imino)(metil)-λ6-sulfanona
C18H18FN5O2S
audencelum audencel autologous interleukin (IL)-12-secreting dendritic cells
(DCs), loaded with autologous tumour lysate, comprising >70% of total immune cells. The cells are differentiated from autologous monocytes by culturing in the presence of interleukin (IL)-4 and GM-CSF (granulocyte-macrophage colony-stimulating factor), following which they are exposed to the patient's tumor protein/tumor-associated antigen (TAA), and subsequently to lipopolysaccharide (LPS) in the presence of interferon gamma (IFN-γ) to enable IL-12 secretion.

Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
70
audencel cellules dendritiques autologues secrétant de l'interleukine-12 (IL-12), chargées avec un lysat de tumeur autologue, comprenant plus de 70% du total des cellules immunitaires. Les cellules sont différenciées à partir de monocytes autologues par une culture en présence d'interleukine-4 (IL-4) et de facteur de stimulation des colonies de granulocytes et de macrophages (GM-CSF), ensuite elles sont exposées à la protéine tumorale/antigène associé à la tumeur du patient, puis au lipopolysaccharide (LPS) en présence d'interféron gamma (IFN- γ) afin de permettre la sécrétion d'IL-12.
audencel células dendríticas autólogas que secretan la interleukina-12 (IL-12), cargadas con un lisado de tumor autólogo, que comprende más del 70% del total de células inmunitarias. Las células se diferencian a partir de monocitos autólogos a través de un cultivo en presencia de interleukina-4 (IL-4) y del factor de estimulación de las colonias de granulocitos y de macrófagos (GM-CSF), a continuación ellas se exponen a la proteína tumoral/antigénica asociada al tumor del paciente (TAA), y después al lipopolisacárido (LPS) en presencia del interferón gamma (IFN-γ) para permitir la secreción de la IL-12.
birabresibum birabresib 2-[(6S)-4-(4-chlorophenyl)-2,3,9-trimethyl-
6H-thieno[3,2-f][1,2,4]triazolo[4,3-a][1,4]diazepin-6-yl]- N-(4-hydroxyphenyl)acetamide
birabrésib 2-[(6S)-4-(4-chlorophényl)-2,3,9-triméthyl- 6H-thiéno[3,2-f][1,2,4]triazolo[4,3-a][1,4]diazépin-6-yl]- N-(4-hydroxyphényl)acétamide
birabresib 2-[(6S)-4-(4-clorofenil)-2,3,9-trimetil- 6H-tieno[3,2-f][1,2,4]triazolo[4,3-a][1,4]diazepin-6-il]- N-(4-hidroxifenil)acetamida
C25H22ClN5O2S
N
N
S
NN
H3C
H3C
H3C
Cl
H
HN
OHO
branaplamum branaplam 5-(1H-pyrazol-4-yl)-2-{6-[(2,2,6,6-tetramethylpiperidin-
4-yl)oxy]pyridazin-3-yl}phenol
branaplam 5-(1H-pyrazol-4-yl)-2-{6-[(2,2,6,6-tétraméthylpipéridin- 4-yl)oxy]pyridazin-3-yl}phenol

WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
71
branaplam 5-(1H-pirazol-4-il)-2-{6-[(2,2,6,6-tetrametilpiperidin- 4-il)oxi]piridazin-3-il}fenol
C22H27N5O2
brazikumabum # brazikumab immunoglobulin G2-lambda, anti-[Homo sapiens IL23A
(interleukin 23 subunit alpha, IL-23A, IL-23 subunit p19, IL23p19)], Homo sapiens monoclonal antibody; gamma2 heavy chain (1-450) [Homo sapiens VH (IGHV3-33*01 (99.00%) -(IGHD)-IGHJ3*02) [8.8.17] (1-124) -IGHG2*01, G2m.. (CH1 (125-222), hinge (223-234), CH2 (235-343), CH3 (344-448), CHS (449-450)) (125-450)], (138-216')-disulfide with lambda light chain (1'-217') [Homo sapiens V-LAMBDA (IGLV1-40*01 (96.00%) -IGLJ3*02) [9.3.11] (1'-111') -IGLC2*01 (112'-217')]; dimer (226-226'':227-227'':230-230'':233-233'')-tetrakisdisulfide
brazikumab immunoglobuline G2-lambda, anti-[Homo sapiens IL23A (interleukine 23 sous-unité alpha, IL-23A, IL-23 sous-unité p19, IL23p19)], Homo sapiens anticorps monoclonal; chaîne lourde gamma2 (1-450) [Homo sapiens VH (IGHV3-33*01 (99.00%) -(IGHD)-IGHJ3*02) [8.8.17] (1-124) -IGHG2*01, G2m.. (CH1 (125-222), charnière (223-234), CH2 (235-343), CH3 (344-448), CHS (449-450)) (125-450)], (138-216')-disulfure avec la chaîne légère lambda (1'-217') [Homo sapiens V-LAMBDA (IGLV1-40*01 (96.00%) -IGLJ3*02) [9.3.11] (1'-111') -IGLC2*01 (112'-217')]; dimère (226-226'':227-227'':230-230'':233-233'')-tétrakisdisulfure
brazikumab inmunoglobulina G2-lambda, anti-[Homo sapiens IL23A (interleukina 23 subunidad alfa, IL-23A, IL-23 subunidad p19, IL23p19)], Homo sapiens anticuerpo monoclonal; cadena pesada gamma2 (1-450) [Homo sapiens VH (IGHV3-33*01 (99.00%) -(IGHD)-IGHJ3*02) [8.8.17] (1-124) -IGHG2*01, G2m.. (CH1 (125-222), bisagra (223-234), CH2 (235-343), CH3 (344-448), CHS (449-450)) (125-450)], (138-216')-disulfuro con la cadena ligera lambda (1'-217') [Homo sapiens V-LAMBDA (IGLV1-40*01 (96.00%) -IGLJ3*02) [9.3.11] (1'-111') -IGLC2*01 (112'-217')]; dímero (226-226'':227-227'':230-230'':233-233'')-tetrakisdisulfuro
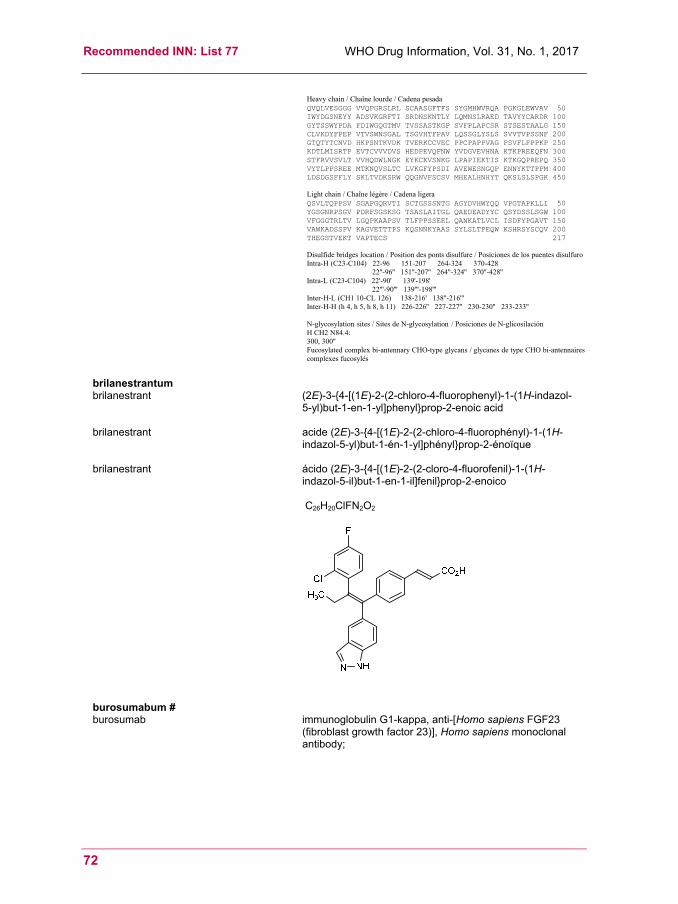
Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
72
Heavy chain / Chaîne lourde / Cadena pesadaQVQLVESGGG VVQPGRSLRL SCAASGFTFS SYGMHWVRQA PGKGLEWVAV 50IWYDGSNEYY ADSVKGRFTI SRDNSKNTLY LQMNSLRAED TAVYYCARDR 100GYTSSWYPDA FDIWGQGTMV TVSSASTKGP SVFPLAPCSR STSESTAALG 150CLVKDYFPEP VTVSWNSGAL TSGVHTFPAV LQSSGLYSLS SVVTVPSSNF 200GTQTYTCNVD HKPSNTKVDK TVERKCCVEC PPCPAPPVAG PSVFLFPPKP 250KDTLMISRTP EVTCVVVDVS HEDPEVQFNW YVDGVEVHNA KTKPREEQFN 300STFRVVSVLT VVHQDWLNGK EYKCKVSNKG LPAPIEKTIS KTKGQPREPQ 350VYTLPPSREE MTKNQVSLTC LVKGFYPSDI AVEWESNGQP ENNYKTTPPM 400LDSDGSFFLY SKLTVDKSRW QQGNVFSCSV MHEALHNHYT QKSLSLSPGK 450
Light chain / Chaîne légère / Cadena ligeraQSVLTQPPSV SGAPGQRVTI SCTGSSSNTG AGYDVHWYQQ VPGTAPKLLI 50YGSGNRPSGV PDRFSGSKSG TSASLAITGL QAEDEADYYC QSYDSSLSGW 100VFGGGTRLTV LGQPKAAPSV TLFPPSSEEL QANKATLVCL ISDFYPGAVT 150VAWKADSSPV KAGVETTTPS KQSNNKYAAS SYLSLTPEQW KSHRSYSCQV 200THEGSTVEKT VAPTECS 217
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H (C23-C104) 22-96 151-207 264-324 370-428
22''-96'' 151''-207'' 264''-324'' 370''-428''Intra-L (C23-C104) 22'-90' 139'-198'
22'''-90''' 139'''-198'''Inter-H-L (CH1 10-CL 126) 138-216' 138''-216'''Inter-H-H (h 4, h 5, h 8, h 11) 226-226'' 227-227'' 230-230'' 233-233''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:300, 300''Fucosylated complex bi-antennary CHO-type glycans / glycanes de type CHO bi-antennairescomplexes fucosylés
brilanestrantum brilanestrant (2E)-3-{4-[(1E)-2-(2-chloro-4-fluorophenyl)-1-(1H-indazol-
5-yl)but-1-en-1-yl]phenyl}prop-2-enoic acid
brilanestrant acide (2E)-3-{4-[(1E)-2-(2-chloro-4-fluorophényl)-1-(1H-indazol-5-yl)but-1-én-1-yl]phényl}prop-2-énoïque
brilanestrant ácido (2E)-3-{4-[(1E)-2-(2-cloro-4-fluorofenil)-1-(1H-indazol-5-il)but-1-en-1-il]fenil}prop-2-enoico
C26H20ClFN2O2
burosumabum # burosumab immunoglobulin G1-kappa, anti-[Homo sapiens FGF23
(fibroblast growth factor 23)], Homo sapiens monoclonal antibody;
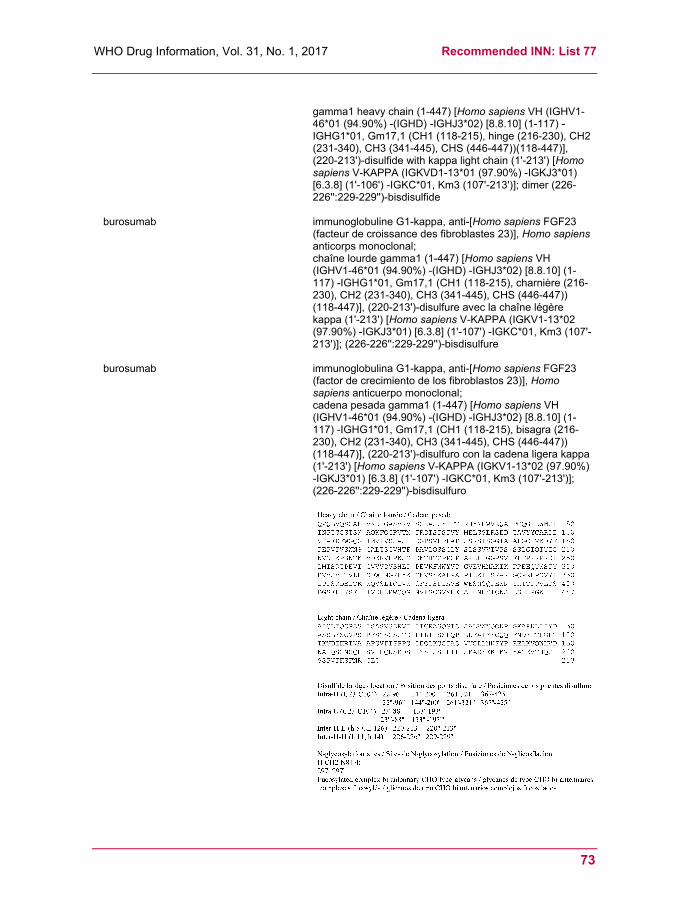
WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
73
gamma1 heavy chain (1-447) [Homo sapiens VH (IGHV1-46*01 (94.90%) -(IGHD) -IGHJ3*02) [8.8.10] (1-117) -IGHG1*01, Gm17,1 (CH1 (118-215), hinge (216-230), CH2 (231-340), CH3 (341-445), CHS (446-447))(118-447)], (220-213')-disulfide with kappa light chain (1'-213') [Homo sapiens V-KAPPA (IGKVD1-13*01 (97.90%) -IGKJ3*01) [6.3.8] (1'-106') -IGKC*01, Km3 (107'-213')]; dimer (226-226'':229-229'')-bisdisulfide
burosumab immunoglobuline G1-kappa, anti-[Homo sapiens FGF23 (facteur de croissance des fibroblastes 23)], Homo sapiens anticorps monoclonal; chaîne lourde gamma1 (1-447) [Homo sapiens VH (IGHV1-46*01 (94.90%) -(IGHD) -IGHJ3*02) [8.8.10] (1-117) -IGHG1*01, Gm17,1 (CH1 (118-215), charnière (216-230), CH2 (231-340), CH3 (341-445), CHS (446-447)) (118-447)], (220-213')-disulfure avec la chaîne légère kappa (1'-213') [Homo sapiens V-KAPPA (IGKV1-13*02 (97.90%) -IGKJ3*01) [6.3.8] (1'-107') -IGKC*01, Km3 (107'-213')]; (226-226'':229-229'')-bisdisulfure
burosumab immunoglobulina G1-kappa, anti-[Homo sapiens FGF23 (factor de crecimiento de los fibroblastos 23)], Homo sapiens anticuerpo monoclonal; cadena pesada gamma1 (1-447) [Homo sapiens VH (IGHV1-46*01 (94.90%) -(IGHD) -IGHJ3*02) [8.8.10] (1-117) -IGHG1*01, Gm17,1 (CH1 (118-215), bisagra (216-230), CH2 (231-340), CH3 (341-445), CHS (446-447)) (118-447)], (220-213')-disulfuro con la cadena ligera kappa (1'-213') [Homo sapiens V-KAPPA (IGKV1-13*02 (97.90%) -IGKJ3*01) [6.3.8] (1'-107') -IGKC*01, Km3 (107'-213')]; (226-226'':229-229'')-bisdisulfuro
Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
74
camrelizumabum # camrelizumab immunoglobulin G4-kappa, anti-[Homo sapiens PDCD1
(programmed cell death 1, PD-1, PD1, CD279)], humanized monoclonal antibody; gamma4 heavy chain (1-443) [humanized VH (Homo sapiens IGHV3-7*01 (90.80%) -(IGHD) -IGHJ4*01) [8.8.9] (1-116) -IGHG4*01 (CH1 (117-214), hinge S10>P (224) (215-226), CH2 (227-336), CH3 (337-441), CHS (442-443)) (117-443)], (130-214')-disulfide with kappa light chain (1'-214') [humanized V-KAPPA (Homo sapiens IGKV1-39*01 (87.40%) -IGKJ1*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 (108'-214')]; dimer (222-222":225-225")-bisdisulfide
camrélizumab immunoglobuline G4-kappa, anti-[Homo sapiens PDCD1 (protéine 1 de mort cellulaire programmée, PD-1, PD1, CD279)], anticorps monoclonal humanisé; chaîne lourde gamma4 (1-443) [VH humanisé (Homo sapiens IGHV3-7*01 (90.80%) -(IGHD) -IGHJ4*01) [8.8.9] (1-116) -IGHG4*01 (CH1 (117-214), charnière S10>P (224) (215-226), CH2 (227-336), CH3 (337-441), CHS (442-443)) (117-443)], (130-214')-disulfure avec la chaîne légère kappa (1'-214') [V-KAPPA humanisé (Homo sapiens IGKV1-39*01 (87.40%) -IGKJ1*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 (108'-214')]; dimère (222-222":225-225")-bisdisulfure
camrelizumab inmunoglobulina G4-kappa, anti-[Homo sapiens PDCD1 (proteína 1 de muerte celular programada, PD-1, PD1, CD279)], anticuerpo monoclonal humanizado; cadena pesada gamma4 (1-443) [VH humanizado (Homo sapiens IGHV3-7*01 (90.80%) -(IGHD) -IGHJ4*01) [8.8.9] (1-116) -IGHG4*01 (CH1 (117-214), bisagra S10>P (224) (215-226), CH2 (227-336), CH3 (337-441), CHS (442-443)) (117-443)], (130-214')-disulfuro con la cadena ligera kappa (1'-214') [V-KAPPA humanizado (Homo sapiens IGKV1-39*01 (87.40%) -IGKJ1*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 (108'-214')]; dímero (222-222":225-225")-bisdisulfuro

WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
75
cannabidiolum cannabidiol 2-[(1R,6R)-3-methyl-6-(prop-1-en-2-yl)cyclohex-2-en-1-yl]-
5-pentylbenzene-1,3-diol
cannabidiol 2-[(1R,6R)-3-méthyl-6-(prop-1-én-2-yl)cyclohex-2-én-1-yl]-5-pentylbenzène-1,3-diol
cannabidiol 2-[(1R,6R)-3-metil-6-(prop-1-en-2-il)ciclohex-2-en-1-il]- 5-pentilbenceno-1,3-diol
C21H30O2
casimersenum casimersen all-P-ambo-[2',3'-azanediyl-P-(dimethylamino)-
P,2',3'-trideoxy-2',3'-seco](2'-N→5')(C-A-A-T-G-C-C-A-T-C-C-T-G-G-A-G-T-T-C-C-T-G) 5'-{P-[4-({2-[2-(2-hydroxyethoxy)ethoxy]ethoxy}carbonyl)piperazin-1-yl]-N,N-dimethylphosphonamidate}
casimersen 5'-{P-[4-({2-[2-(2-hydroxyéthoxy)éthoxy]éthoxy}carbonyl)pipérazin-1-yl]- N,N-diméthylphosphonamidate} de tout-P-ambo-[2',3'-azanediyl-P-(diméthylamino)-P,2',3'-tridéoxy-2',3'-séco](2'-N→5')(C-A-A-T-G-C-C-A-T-C-C-T-G-G-A-G-T-T-C-C-T-G)

Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
76
casimersén 5'-{P-[4-({2-[2-(2-hidroxietoxi)etoxi]etoxi}carbonil)piperazin-
1-il]-N,N-dimetilfosfonamidato} de todo-P-ambo-[2',3'-azanediil-P-(dimetilamino)-P,2',3'-tridesoxi-2',3'-seco](2'-N→5')(C-A-A-T-G-C-C-A-T-C-C-T-G-G-A-G-T-T-C-C-T-G)
C268H424N124O95P22
cenegerminum # cenegermin human beta-nerve growth factor (beta-NGF)-(1-118)-
peptide (non-covalent dimer) produced in Escherichia coli
cénégermine facteur de croissance bêta des cellules nerveuses (beta-NGF)-(1-118)-peptide, humain, produit par Escherichia coli
cenegermina factor de crecimiento beta de las células nerviosas (beta-NGF)-(1-118)-péptido humano (dímero no covalente), producido por Escherichia coli
C583H902N166O173S8
cenplacelum cenplacel Human placenta-derived adherent (PDA) cells that are
culture-expanded, undifferentiated mesenchymal-like cells derived from full-term placental tissue of a human donor. Cellular identity: Mesenchymal-like stromal cell: CD34-, CD10+, CD105+, and CD200+. Cells lack the human leukocyte antigen (HLA) and costimulatory molecules on their membrane surface.
cenplacel Cellules humaines adhérentes dérivées du placenta, en culture d'expansion, cellules semblables aux cellules mésenchymateuses non-différenciées dérivées de tissu placentaire à terme de donneur humain. identité des cellules: cellules stromales semblables aux cellules mésenchymateuses: CD34-, CD10+, CD105+, and CD200+. Les cellules sont dépourvues de l'antigène leucocytaire humain (HLA) et des molécules co-stimulantes à la surface de la membrane.
WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
77
cenplacel Células humanas adherentes derivadas de la placenta
(PDA) expandidas por cultivo, células semejantes a las células mesenquimales no diferenciadas derivadas del tejido placentario a término. Identificación de las células: células estromales semejantes a las células mesenquimales: CD34-, CD10+, CD105+, et CD200+. Las células están desprovistas del antígeno leucocitario humano (HLA) y de las moléculas coestimulantes de la superficie de la membrana
cibinetidum cibinetide 5-oxo-L-prolyl-L-α-glutamyl-L-glutaminyl-L-leucyl-
L-α-glutamyl-L-arginyl-L-alanyl-L-leucyl-L-asparaginyl- L-seryl-L-serine
cibinétide 5-oxo-L-prolyl-L-α-glutamyl-L-glutaminyl-L-leucyl- L-α-glutamyl-L-arginyl-L-alanyl-L-leucyl-L-asparaginyl- L-séryl-L-sérine
cibinetida 5-oxo-L-prolil-L-α-glutamil-L-glutaminil-L-leucil-L-α-glutamil- L-arginyl-L-alanil-L-leucil-L-asparaginil-L-seril-L-serina
C51H84N16O21
crizanlizumabum # crizanlizumab immunoglobulin G2-kappa, anti-[Homo sapiens SELP
(selectin P, CD62)], humanized monoclonal antibody; gamma2 heavy chain (1-448) [humanized VH (Homo sapiens IGHV1-8*01 (81.60%) -(IGHD) -IGHJ4*01) [8.8.15] (1-122) -Homo sapiens IGHG2*02 (CH1 (123-220), hinge (221-232), CH2 K105>A (323) (233-341), CH3 (342-446), CHS (447-448)) (123-448)], (136-218')-disulfide with kappa light chain (1'-218') [humanized V-KAPPA (Homo sapiens IGKV1-39*01 (86.90%) -IGKJ4*01) [10.3.9] (1'-111') -Homo sapiens IGKC*01, Km3 (112'-218')]; dimer (224-224":225-225":228-228":231-231")-tetrakisdisulfide
crizanlizumab immunoglobuline G2-kappa, anti-[Homo sapiens SELP (sélectine P, CD62)], anticorps monoclonal humanisé; chaîne lourde gamma2 (1-448) [VH humanisé (Homo sapiens IGHV1-8*01 (81.60%) -(IGHD) -IGHJ4*01) [8.8.15] (1-122) -Homo sapiens IGHG2*02 (CH1 (123-220), charnière (221-232), CH2 K105>A (323) (233-341), CH3 (342-446), CHS (447-448)) (123-448)], (136-218')-disulfure avec la chaîne légère kappa (1'-218') [V-KAPPA humanisé (Homo sapiens IGKV1-39*01 (86.90%) -IGKJ4*01) [10.3.9] (1'-111') -Homo sapiens IGKC*01, Km3 (112'-218')]; dimère (224-224":225-225":228-228":231-231")-tétrakisdisulfure
Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
78
crizanlizumab inmunoglobulina G2-kappa, anti-[Homo sapiens SELP (selectina P, CD62)], anticuerpo monoclonal humanizado; cadena pesada gamma2 (1-448) [VH humanizado (Homo sapiens IGHV1-8*01 (81.60%) -(IGHD) -IGHJ4*01) [8.8.15] (1-122) -Homo sapiens IGHG2*02 (CH1 (123-220), bisagra (221-232), CH2 K105>A (323) (233-341), CH3 (342-446), CHS (447-448)) (123-448)], (136-218')-disulfuro con la cadena ligera kappa (1'-218') [V-KAPPA humanizado (Homo sapiens IGKV1-39*01 (86.90%) -IGKJ4*01) [10.3.9] (1'-111') -Homo sapiens IGKC*01, Km3 (112'-218')]; dímero (224-224":225-225":228-228":231-231")-tetrakisdisulfuro
cupabimodum cupabimod all-P-ambo-2'-deoxy-P-thiocytidylyl-(3'→5')-2'-deoxy-P-
thiocytidylyl-(3'→5')-P-thiothymidylyl-(3'→5')-P-thiothymidylyl-(3'→5')-2'-deoxy-P-thioguanylyl-(3'→5')-2'-deoxy-P-thioadenylyl-(3'→5')-2'-deoxy-P-thioadenylyl-(3'→5')-2'-deoxy-P-thioguanylyl-(3'→5')-2'-deoxy-P-thioguanylyl-(3'→5')-2'-deoxy-P-thioguanylyl-(3'→5')-2'-deoxy-P-thioadenylyl-(3'→5')-P-thiothymidylyl-(3'→5')-P-thiothymidylyl-(3'→5')-P-thiothymidylyl-(3'→5')-2'-deoxy-P-thiocytidylyl-(3'→5')-2'-deoxy-P-thiocytidylyl-(3'→5')-2'-deoxy-P-thiocytidylyl-(3'→5')-P-thiothymidylyl-(3'→5')-2'-deoxy-P-thiocytidylyl-(3'→5')-2'-deoxycytidine duplex with all-P-ambo-2'-deoxy-P-thioguanylyl-(3'→5')-2'-deoxy-P-thioguanylyl-(3'→5')-2'-deoxy-P-thioadenylyl-(3'→5')-2'-deoxy-P-thioadenylyl-(3'→5')-2'-deoxy-P-thiocytidylyl-(3'→5')-P-thiothymidylyl-(3'→5')-P-thiothymidylyl-(3'→5')-2'-deoxy-P-thiocytidylyl-(3'→5')-2'-deoxy-P-thiocytidylyl-(3'→5')-2'-deoxy-P-thiocytidylyl-(3'→5')-P-thiothymidylyl-(3'→5')-2'-deoxy-P-thioadenylyl-(3'→5')-2'-deoxy-P-thioadenylyl-(3'→5')-2'-deoxy-P-thioadenylyl-(3'→5')-2'-
WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
79
deoxy-P-thioguanylyl-(3'→5')-2'-deoxy-P-thioguanylyl-(3'→5')-2'-deoxy-P-thioguanylyl-(3'→5')-2'-deoxy-P-thioadenylyl-(3'→5')-2'-deoxy-P-thioguanylyl-(3'→5')-2'-deoxyguanosine
cupabimod duplex de tout-P-ambo-2'-déoxy-P-thiocytidylyl-(3'→5')-2'-déoxy-P-thiocytidylyl-(3'→5')-P-thiothymidylyl-(3'→5')-P-thiothymidylyl-(3'→5')-2'-déoxy-P-thioguanylyl-(3'→5')-2'-déoxy-P-thioadénylyl-(3'→5')-2'-déoxy-P-thioadénylyl-(3'→5')-2'-déoxy-P-thioguanylyl-(3'→5')-2'-déoxy-P-thioguanylyl-(3'→5')-2'-déoxy-P-thioguanylyl-(3'→5')-2'-déoxy-P-thioadénylyl-(3'→5')-P-thiothymidylyl-(3'→5')-P-thiothymidylyl-(3'→5')-P-thiothymidylyl-(3'→5')-2'-déoxy-P-thiocytidylyl-(3'→5')-2'-déoxy-P-thiocytidylyl-(3'→5')-2'-déoxy-P-thiocytidylyl-(3'→5')-P-thiothymidylyl-(3'→5')-2'-déoxy-P-thiocytidylyl-(3'→5')-2'-déoxycytidine avec tout-P-ambo-2'-déoxy-P-thioguanylyl-(3'→5')-2'-déoxy-P-thioguanylyl-(3'→5')-2'-déoxy-P-thioadénylyl-(3'→5')-2'-déoxy-P-thioadénylyl-(3'→5')-2'-déoxy-P-thiocytidylyl-(3'→5')-P-thiothymidylyl-(3'→5')-P-thiothymidylyl-(3'→5')-2'-déoxy-P-thiocytidylyl-(3'→5')-2'-déoxy-P-thiocytidylyl-(3'→5')-2'-déoxy-P-thiocytidylyl-(3'→5')-P-thiothymidylyl-(3'→5')-2'-déoxy-P-thioadénylyl-(3'→5')-2'-déoxy-P-thioadénylyl-(3'→5')-2'-déoxy-P-thioadénylyl-(3'→5')-2'-déoxy-P-thioguanylyl-(3'→5')-2'-déoxy-P-thioguanylyl-(3'→5')-2'-déoxy-P-thioguanylyl-(3'→5')-2'-déoxy-P-thioadénylyl-(3'→5')-2'-désoxy-P-thioguanylyl-(3'→5')-2'-déoxyguanosine
cupabimod duplex de todo-P-ambo-2'-desoxi-P-tiocitidilil-(3'→5')-2'-desoxi-P-tiocitidilil-(3'→5')-P-tiotimidilil-(3'→5')-P-tiotimidilil-(3'→5')-2'-desoxi-P-tioguanilil-(3'→5')-2'-desoxi-P-tioadenilil-(3'→5')-2'-desoxi-P-tioadenilil-(3'→5')-2'-desoxi-P-tioguanilil-(3'→5')-2'-desoxi-P-tioguanilil-(3'→5')-2'-desoxi-P-tioguanilil-(3'→5')-2'-desoxi-P-tioadenilil-(3'→5')-P-tiotimidilil-(3'→5')-P-tiotimidilil-(3'→5')-P-tiotimidilil-(3'→5')-2'-desoxi-P-tiocitidilil-(3'→5')-2'-desoxi-P-tiocitidilil-(3'→5')-2'-desoxi-P-tiocitidilil-(3'→5')-P-tiotimidilil-(3'→5')-2'-desoxi-P-tiocitidilil-(3'→5')-2'-desoxicitidina con todo-P-ambo-2'-desoxi-P-tioguanilil-(3'→5')-2'-desoxi-P-tioguanilil-(3'→5')-2'-desoxi-P-tioadenilil-(3'→5')-2'-desoxi-P-tioadenilil-(3'→5')-2'-desoxi-P-tiocitidilil-(3'→5')-P-tiotimidilil-(3'→5')-P-tiotimidilil-(3'→5')-2'-desoxi-P-tiocitidilil-(3'→5')-2'-desoxi-P-tiocitidilil-(3'→5')-2'-desoxi-P-tiocitidilil-(3'→5')-P-tiotimidilil-(3'→5')-2'-desoxi-P-tioadenilil-(3'→5')-2'-desoxi-P-tioadenilil-(3'→5')-2'-desoxi-P-tioadenilil-(3'→5')-2'-desoxi-P-tioguanilil-(3'→5')-2'-desoxi-P-tioguanilil-(3'→5')-2'-desoxi-P-tioguanilil-(3'→5')-2'-desoxi-P-tioadenilil-(3'→5')-2'-desoxi-P-tioguanilil-(3'→5')-2'-desoxiguanosina
C389H491N151O198P38S38
(3'-5')d(P-thio)(C-C-T-T-G-A-A-G-G-G-A-T-T-T-C-C-C-T-C-C)
(5'-3')d(P-thio)(G-G-A-A-C-T-T-C-C-C-T-A-A-A-G-G-G-A-G-G)
daclizumabum beta #
daclizumab beta immunoglobulin G1-kappa, anti-[Homo sapiens IL2RA (interleukin 2 receptor alpha subunit, IL-2RA, TAC, p55, CD25)], humanized monoclonal antibody;
Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
80
gamma1 heavy chain (1-446) [humanized VH (Homo sapiens IGHV1-46*01 (82.70%) -(IGHD)-IGHJ4*01) [8.8.9] (1-116) -Homo sapiens IGHG1*01, G1m17,1 (CH1 (117-214), hinge (215-229), CH2 (230-339), CH3 (340-444), CHS (445-446)) (117-446)], (219-213')-disulfide with kappa light chain (1’-213’) [humanized V-KAPPA (Homo sapiens IGKV1-5*01 (84.00%) -IGKJ1*01) [5.3.9] (1'-106') -Homo sapiens IGKC*01, Km3 (107'-213')]; dimer (225-225":228-228")-bisdisulfide
daclizumab bêta immunoglobuline G1-kappa, anti-[Homo sapiens IL2RA (sous-unité alpha du récepteur de l’interleukine 2, IL-2RA, TAC, p55, CD25)], anticorps monoclonal humanisé; chaîne lourde gamma1 (1-446) [VH humanisé (Homo sapiens IGHV1-46*01 (82.70%) -(IGHD)-IGHJ4*01) [8.8.9] (1-116) -Homo sapiens IGHG1*01, G1m17,1 (CH1 (117-214), charnière (215-229), CH2 (230-339), CH3 (340-444), CHS (445-446)) (117-446)], (219-213')-disulfure avec la chaîne légère kappa (1’-213’) [V-KAPPA humanisé (Homo sapiens IGKV1-5*01 (84.00%) -IGKJ1*01) [5.3.9] (1'-106') -Homo sapiens IGKC*01, Km3 (107'-213')]; dimère (225-225":228-228")-bisdisulfure
daclizumab beta inmunoglobulina G1-kappa, anti-[Homo sapiens IL2RA (subunidad alfa del receptor de la interleukina 2, IL-2RA, TAC, p55, CD25)], anticuerpo monoclonal humanizado; cadena pesada gamma1 (1-446) [VH humanizado (Homo sapiens IGHV1-46*01 (82.70%) -(IGHD)-IGHJ4*01) [8.8.9] (1-116) -Homo sapiens IGHG1*01, G1m17,1 (CH1 (117-214), bisagra (215-229), CH2 (230-339), CH3 (340-444), CHS (445-446)) (117-446)], (219-213')-disulfuro con la cadena ligera kappa (1’-213’) [V-KAPPA humanizado (Homo sapiens IGKV1-5*01 (84.00%) -IGKJ1*01) [5.3.9] (1'-106') -Homo sapiens IGKC*01, Km3 (107'-213')]; dímero (225-225":228-228")-bisdisulfuro

WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
81
darolutamidum darolutamide N-{(2S)-1-[3-(3-chloro-4-cyanophenyl)-1H-pyrazol-
1-yl]propan-2-yl}-5-[(1RS)-1-hydroxyethyl]-1H-pyrazole- 3-carboxamide
darolutamide N-{(2S)-1-[3-(3-chloro-4-cyanophényl)-1H-pyrazol- 1-yl]propan-2-yl}-5-[(1RS)-1-hydroxyéthyl]-1H-pyrazole- 3-carboxamide
darolutamida N-{(2S)-1-[3-(4-ciano-3-clorofenil)-1H-pirazol-1-il]propan- 2-il}-5-[(1RS)-1-hidroxietil]-1H-pirazol-3-carboxamida
C19H19ClN6O2
depatuxizumabum # depatuxizumab immunoglobulin G1-kappa, anti-[Homo sapiens EGFR
(epidermal growth factor receptor, receptor tyrosine-protein kinase erbB-1, ERBB1, HER1, HER-1, ERBB)], humanized and chimeric monoclonal antibody; gamma1 heavy chain humanized (1-446) [humanized VH (Homo sapiens IGHV4-30-4*01 (84.50%) -(IGHD)-IGHJ4*01) [9.7.9] (1-116) -Homo sapiens IGHG1*01, G1m17,1 (CH1 (117-214), hinge (215-229),CH2 (230-339), CH3 (340-444), CHS (445-446)) (117-446)], (219-214')-disulfide with kappa light chain chimeric (1'-214') [Mus musculus V-KAPPA (Mus musculus IGKV14-100*01 -IGKJ1*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 (108'-214')]; dimer (225-225":228-228")-bisdisulfide
dépatuxizumab immunoglobuline G1-kappa, anti-[Homo sapiens EGFR (Récepteur du facteur de croissance épidermique, récepteur tyrosine-protéine kinase erb-1, ERBB1, HER1, HER-1, ERBB)], anticorps monoclonal humanisé et chimérique; chaîne lourde gamma1 humanisée (1-446) [VH humanisé (Homo sapiens IGHV4-30-4*01 (84.50%) -(IGHD)-IGHJ4*01) [9.7.9] (1-116) -Homo sapiens IGHG1*01, G1m17,1 (CH1 (117-214), charnière (215-229),CH2 (230-339), CH3 (340-444), CHS (445-446)) (117-446)], (219-214')-disulfure avec la chaîne légère kappa chimérique (1'-214') [Mus musculus V-KAPPA (Mus musculus IGKV14-100*01 -IGKJ1*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 (108'-214')]; dimère (225-225":228-228")-bisdisulfure
depatuxizumab inmunoglobulina G1-kappa, anti-[Homo sapiens EGFR (Receptor del factor de crecimiento epidérmico, receptor tirosina-proteína kinasa erb-1, ERBB1, HER1, HER-1, ERBB)], anticuerpo monoclonal humanizado y quimérico;

Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
82
cadena pesada gamma1 humanizada (1-446) [VH humanizado (Homo sapiens IGHV4-30-4*01 (84.50%) -(IGHD)-IGHJ4*01) [9.7.9] (1-116) -Homo sapiens IGHG1*01, G1m17,1 (CH1 (117-214), bisagra (215-229),CH2 (230-339), CH3 (340-444), CHS (445-446)) (117-446)], (219-214')-disulfuro con la cadena ligera kappa quimérica (1'-214') [Mus musculus V-KAPPA (Mus musculus IGKV14-100*01 -IGKJ1*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 (108'-214')]; dímero (225-225":228-228")-bisdisulfuro
depatuxizumabum mafodotinum # depatuxizumab mafodotin immunoglobulin G1-kappa, anti-[Homo sapiens EGFR
(epidermal growth factor receptor, receptor tyrosine-protein kinase erbB-1, ERBB1, HER1, HER-1, ERBB)], humanized and chimeric monoclonal antibody conjugated to auristatin F; gamma1 heavy chain humanized (1-446) [humanized VH (Homo sapiens IGHV4-30-4*01 (84.50%) -(IGHD)-IGHJ4*01) [9.7.9] (1-116) -Homo sapiens IGHG1*01, G1m17,1 (CH1 (117-214), hinge (215-229), CH2 (230-339), CH3 (340-444), CHS (445-446)) (117-446)], (219-214')-disulfide with kappa light chain chimeric (1'-214') [Mus musculus V-KAPPA (Mus musculus IGKV14-100*01 -IGKJ1*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 (108'-214')]; dimer (225-225":228-228")-bisdisulfide; conjugated, on an average of 4 cysteinyl, to monomethylauristatin F (MMAF), via a noncleavable maleimidocaproyl (mc) linker For the mafodotin part, please refer to the document "INN for pharmaceutical substances: Names for radicals, groups and others"*.
dépatuxizumab mafodotine immunoglobuline G1-kappa, anti-[Homo sapiens EGFR (Récepteur du facteur de croissance épidermique, récepteur tyrosine-protéine kinase erb-1, ERBB1, HER1, HER-1, ERBB)], anticorps monoclonal humanisé et chimérique conjugué à l'auristatine F;

WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
83
chaîne lourde gamma1 humanisée (1-446) [VH humanisé (Homo sapiens IGHV4-30-4*01 (84.50%) -(IGHD)-IGHJ4*01) [9.7.9] (1-116) -Homo sapiens IGHG1*01, G1m17,1 (CH1 (117-214), charnière (215-229),CH2 (230-339), CH3 (340-444), CHS (445-446)) (117-446)], (219-214')-disulfure avec la chaîne légère kappa chimérique (1'-214') [Mus musculus V-KAPPA (Mus musculus IGKV14-100*01 -IGKJ1*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 (108'-214')]; dimère (225-225":228-228")-bisdisulfure; conjugué, sur 4 cystéinyl en moyenne, au monométhylauristatine F (MMAF), via un linker maléimidocaproyl (mc) non clivable Pour la partie mafodotine, veuillez-vous référer au document "INN for pharmaceutical substances: Names for radicals, groups and others"*.
depatuxizumab mafodotina inmunoglobulina G1-kappa, anti-[Homo sapiens EGFR (Receptor del factor de crecimiento epidérmico, receptor tirosina-proteína kinasa erb-1, ERBB1, HER1, HER-1, ERBB)], anticuerpo monoclonal humanizado y quimérico conjugado con la auristatina F; cadena pesada gamma1 humanizada (1-446) [VH humanizado (Homo sapiens IGHV4-30-4*01 (84.50%) -(IGHD)-IGHJ4*01) [9.7.9] (1-116) -Homo sapiens IGHG1*01, G1m17,1 (CH1 (117-214), bisagra (215-229),CH2 (230-339), CH3 (340-444), CHS (445-446)) (117-446)], (219-214')-disulfuro con la cadena ligera kappa quimérica (1'-214') [Mus musculus V-KAPPA (Mus musculus IGKV14-100*01 -IGKJ1*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 (108'-214')]; dímero (225-225":228-228")-bisdisulfuro; conjugado, en 4 grupos cisteinil por término medio, con monometilauristatina F (MMAF), mediante un conector no escindible de tipo maleimidocaproil (mc) Por la parte mafodotina, por favor vaya al documento "INN for pharmaceutical substances: Names for radicals, groups and others"*.

Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
84
dexisometheptenum dexisometheptene (2R)-N,6-dimethylhept-5-en-2-amine
dexisométhéptène (2R)-N,6-diméthylhept-5-én-2-amine
dexisometepteno (2R)-N,6-dimetilhept-5-en-2-amina
C9H19N
dezamizumabum # dezamizumab immunoglobulin G1-kappa, anti-[Homo sapiens APCS
(amyloid P component serum, serum amyloid P component, SAP, pentraxin-2, PTX2)], humanized monoclonal antibody; gamma1 heavy chain (1-452) [humanized VH (Homo sapiens IGHV1-69*02 (85.70%) -(IGHD)-IGHJ5*01) [8.8.15] (1-122) -Homo sapiens IGHG1*01, G1m17,1 (CH1 (123-220), hinge (221-235),CH2 (236-345), CH3 (346-450), CHS (451-452)) (123-452)], (225-214')-disulfide with kappa light chain (1'-214') [humanized V-KAPPA (Homo sapiens IGKV1-39*01 (85.30%) -IGKJ2*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 (108'-214')]; dimer (231-231":234-234")-bisdisulfide
dézamizumab immunoglobuline G1-kappa, anti-[Homo sapiens APCS (composant amyloïde P du sérum, composant amyloïde P sérique, APS, pentraxine-2, PTX2)], anticorps monoclonal humanisé; chaîne lourde gamma1 (1-452) [VH humanisé (Homo sapiens IGHV1-69*02 (85.70%) -(IGHD)-IGHJ5*01) [8.8.15] (1-122) -Homo sapiens IGHG1*01, G1m17,1 (CH1 (123-220), charnière (221-235),CH2 (236-345), CH3 (346-450), CHS (451-452)) (123-452)], (225-214')-disulfure avec la chaîne légère kappa (1'-214') [V-KAPPA humanisé (Homo sapiens IGKV1-39*01 (85.30%) -IGKJ2*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 (108'-214')]; dimère (231-231":234-234")-bisdisulfure
dezamizumab inmunoglobulina G1-kappa, anti-[Homo sapiens APCS (componente amiloide P del suero, componente amiloide P serico, APS, pentraxina-2, PTX2)], anticuerpo monoclonal humanizado; cadena pesada gamma1 (1-452) [VH humanizado (Homo sapiens IGHV1-69*02 (85.70%) -(IGHD)-IGHJ5*01) [8.8.15] (1-122) -Homo sapiens IGHG1*01, G1m17,1 (CH1 (123-220), bisagra (221-235),CH2 (236-345), CH3 (346-450), CHS (451-452)) (123-452)], (225-214')-disulfuro con la cadena lígera kappa (1'-214') [V-KAPPA humanizado (Homo sapiens IGKV1-39*01 (85.30%) -IGKJ2*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 (108'-214')]; dímero (231-231":234-234")-bisdisulfuro

WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
85
dinutuximabum beta # dinutuximab beta immunoglobulin G1-kappa, anti-[Homo sapiens ganglioside
GD2 (disialoganglioside GD2)], chimeric monoclonal antibody; gamma1 heavy chain (1-443) [Mus musculus VH (IGHV1S135*01 -(IGHD)-IGHJ4*01) [8.8.6] (1-113) -Homo sapiens IGHG1*03, G1m3 (CH1 (114-211), hinge (212-226), CH2 (227-336), CH3 (337-441), CHS (442-443)) (114-443)], (216-220')-disulfide with kappa light chain (1'-220') [Mus musculus V-KAPPA (IGKV1-110*01 -IGKJ5*01) [11.3.10] (1'-113') -Homo sapiens IGKC*01, Km3 (114'-220')]; dimer (222-222'':225-225'')-bisdisulfide
dinutuximab bêta immunoglobuline G1-kappa, anti-[Homo sapiens ganglioside GD2 (disialoganglioside GD2)], anticorps monoclonal chimérique; chaîne lourde gamma1 (1-443) [Mus musculus VH (IGHV1S135*01 -(IGHD)-IGHJ4*01) [8.8.6] (1-113) -Homo sapiens IGHG1*03, G1m3 (CH1 (114-211), charnière (212-226), CH2 (227-336), CH3 (337-441), CHS (442-443)) (114-443)], (216-220')-disulfure avec la chaîne légère kappa (1'-220') [Mus musculus V-KAPPA (IGKV1-110*01 -IGKJ5*01) [11.3.10] (1'-113') -Homo sapiens IGKC*01, Km3 (114'-220')]; dimère (222-222'':225-225'')-bisdisulfure
dinutuximab beta inmunoglobulina G1-kappa, anti-[Homo sapiens gangliósido GD2 (disialogangliósido GD2)], anticuerpo monoclonal quimérico;
Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
86
gamma1 heavy chain (1-443) [Mus musculus VH (IGHV1S135*01 -(IGHD)-IGHJ4*01) [8.8.6] (1-113) -Homo sapiens IGHG1*03, G1m3 (CH1 (114-211), hinge (212-226), CH2 (227-336), CH3 (337-441), CHS (442-443)) (114-443)], (216-220')-disulfide with kappa light chain (1'-220') [Mus musculus V-KAPPA (IGKV1-110*01 -IGKJ5*01) [11.3.10] (1'-113') -Homo sapiens IGKC*01, Km3 (114'-220')]; dimer (222-222'':225-225'')-bisdisulfide
dinutuximab bêta immunoglobuline G1-kappa, anti-[Homo sapiens ganglioside GD2 (disialoganglioside GD2)], anticorps monoclonal chimérique; chaîne lourde gamma1 (1-443) [Mus musculus VH (IGHV1S135*01 -(IGHD)-IGHJ4*01) [8.8.6] (1-113) -Homo sapiens IGHG1*03, G1m3 (CH1 (114-211), charnière (212-226), CH2 (227-336), CH3 (337-441), CHS (442-443)) (114-443)], (216-220')-disulfure avec la chaîne légère kappa (1'-220') [Mus musculus V-KAPPA (IGKV1-110*01 -IGKJ5*01) [11.3.10] (1'-113') -Homo sapiens IGKC*01, Km3 (114'-220')]; dimère (222-222'':225-225'')-bisdisulfure
dinutuximab beta inmunoglobulina G1-kappa, anti-[Homo sapiens gangliósido GD2 (disialogangliósido GD2)], anticuerpo monoclonal quimérico; cadena pesada gamma1 (1-443) [Mus musculus VH (IGHV1S135*01 -(IGHD)-IGHJ4*01) [8.8.6] (1-113) -Homo sapiens IGHG1*03, G1m3 (CH1 (114-211), bisagra (212-226), CH2 (227-336), CH3 (337-441), CHS (442-443)) (114-443)], (216-220')-disulfuro con la cadena ligera kappa (1'-220') [Mus musculus V-KAPPA (IGKV1-110*01 -IGKJ5*01) [11.3.10] (1'-113') -Homo sapiens IGKC*01, Km3 (114'-220')]; dímero (222-222'':225-225'')-bisdisulfuro
Heavy chain / Chaîne lourde / Cadena pesadaEVQLLQSGPE LEKPGASVMI SCKASGSSFT GYNMNWVRQN IGKSLEWIGA 50IDPYYGGTSY NQKFKGRATL TVDKSSSTAY MHLKSLTSED SAVYYCVSGM 100EYWGQGTSVT VSSASTKGPS VFPLAPSSKS TSGGTAALGC LVKDYFPEPV 150TVSWNSGALT SGVHTFPAVL QSSGLYSLSS VVTVPSSSLG TQTYICNVNH 200KPSNTKVDKR VEPKSCDKTH TCPPCPAPEL LGGPSVFLFP PKPKDTLMIS 250RTPEVTCVVV DVSHEDPEVK FNWYVDGVEV HNAKTKPREE QYNSTYRVVS 300VLTVLHQDWL NGKEYKCKVS NKALPAPIEK TISKAKGQPR EPQVYTLPPS 350REEMTKNQVS LTCLVKGFYP SDIAVEWESN GQPENNYKTT PPVLDSDGSF 400FLYSKLTVDK SRWQQGNVFS CSVMHEALHN HYTQKSLSLS PGK 443
Light chain / Chaîne légère / Cadena ligeraEIVMTQSPAT LSVSPGERAT LSCRSSQSLV HRNGNTYLHW YLQKPGQSPK 50LLIHKVSNRF SGVPDRFSGS GSGTDFTLKI SRVEAEDLGV YFCSQSTHVP 100PLTFGAGTKL ELKRTVAAPS VFIFPPSDEQ LKSGTASVVC LLNNFYPREA 150KVQWKVDNAL QSGNSQESVT EQDSKDSTYS LSSTLTLSKA DYEKHKVYAC 200EVTHQGLSSP VTKSFNRGEC 220
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H (C23-C104) 22-96 140-196 257-317 363-421 22''-96'' 140''-196'' 257''-317'' 363''-421''Intra-L (C23-C104) 23'-93' 140'-200' 23'''-93''' 140'''-200''' Inter-H-L (h 5-CL 126) 216-220' 216''-220''' Inter-H-H (h 11, h 14) 222-222'' 225-225''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:293, 293''Fucosylated complex bi-antennary CHO-type glycans / glycanes de type CHO bi-antennaires complexes fucosylés / glicanos de tipo CHO biantenarios complejos fucosilados
diroximeli fumaras diroximel fumarate 2-(2,5-dioxopyrrolidin-1-yl)ethyl methyl (2E)-but-
2-enedioate
WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
87
fumarate de diroximel (2E)-but-2-ènedioate de 2-(2,5-dioxopyrrolidin-1-yl)éthyle
et de méthyle
fumarato de diroximel (2E)-but-2-enodioato de 2-(2,5-dioxopirrolidin-1-il)etilo y de metilo
C11H13NO6
elacestrantum elacestrant (6R)-6-{2-[ethyl({4-[2-
(ethylamino)ethyl]phenyl}methyl)amino]-4-methoxyphenyl}-5,6,7,8-tetrahydronaphthalen-2-ol
élacestrant (6R)-6-{2-[éthyl({4-[2-(éthylamino)éthyl]phényl}méthyl)amino]-4-méthoxyphényl}-5,6,7,8-tétrahydronaphtalén-2-ol
elacestrant (6R)-6-{2-[etil({4-[2-(etilamino)etil]fenil}metil)amino]- 4-metoxifenil}-5,6,7,8-tetrahidronaftalen-2-ol
C30H38N2O2
elapegademasum # elapegademase [Cys74>Ser,Ala245>Thr]adenosine deaminase (Bos taurus,
bovine)-(1-356)-peptide, produced in Escherichia coli, substituted on N2 of the N-terminal alanyl residue (A1) and on N6 of lysyl residues (K) with an average of approximately 13 ω-methoxypoly(oxyethylene)-α-carbonyl groups (~5 kDa each)
élapégadémase [Cys74>Ser,Ala245>Thr]adénosine déaminase (Bos taurus, bovine)-(1-356)-peptide, produit par Escherichia coli, substitué sur les N2 du résidu alanyl N-terminal (A1) et sur les N6 des résidus lysyl (K) avec en en moyenne 13 groupes ω-métoxipoli(oxietileno)-α-carbonyle (~5 kDa chacun) approximativement
Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
88
elapegademasa [Cys74>Ser,Ala245>Thr]adenosina deaminasa (Bos taurus, bovino)-(1-356)-péptido, producido por Escherichia coli, sustituido en los N2 del resto alanilN-terminal (A1) y en los N6 de los restos lisil (K) con una media de 13 grupos ω-metoxipoli(oxietileno)-α-carbonilo (~5 kDa cada uno de ellos) de forma aproximada
Sequence / Séquence / Secuencia
AQTPAFNKPK VELHVHLDGA IKPETILYYG RKRGIALPAD TPEELQNIIG 50MDKPLSLPEF LAKFDYYMPA IAGSREAVKR IAYEFVEMKA KDGVVYVEVR 100YSPHLLANSK VEPIPWNQAE GDLTPDEVVS LVNQGLQEGE RDFGVKVRSI 150LCCMRHQPSW SSEVVELCKK YREQTVVAID LAGDETIEGS SLFPGHVKAY 200AEAVKSGVHR TVHAGEVGSA NVVKEAVDTL KTERLGHGYH TLEDTTLYNR 250LRQENMHFEV CPWSSYLTGA WKPDTEHPVV RFKNDQVNYS LNTDDPLIFK 300STLDTDYQMT KNEMGFTEEE FKRLNINAAK SSFLPEDEKK ELLDLLYKAY 350GMPSPA 356
Potential pegylated residues / Résidus pégylés potentiels / Restos pegilados potenciales
H2N CO2H
HNH
O
O
H3CO n
NH
CO2H
CH3H
O
O
H3CO
n
A (1) K
elezanumabum # elezanumab immunoglobulin G1-lambda1, anti-[Homo sapiens RGMA
(repulsive guidance molecule family member a, repulsive guidance molecule A, RGMa)], Homo sapiens monoclonal antibody; gamma1 heavy chain (1-450) [Homo sapiens VH (IGHV1-18*01 (92.90%) -(IGHD) -IGHJ6*03) [8.8.13](1-120) -IGHG1*01, Gm17,1 (CH1 (121-218), hinge (219-233), CH2 L1.2>A (238), L1.3>A (237), T14>Q (253) (234-343), CH3 M107>L (431) (344-448),CHS (449-450)) (121-450)], (223-214')-disulfide with lambda1 light chain (1'-215') [Homo sapiens V-LAMBDA (IGLV2-11*01 (89.90%) -IGLJ2*01) [9.3.9] (1'-109') -IGLC2*01 (110'-215')]; dimer (229-229'':232-232'')-bisdisulfide
élézanumab immunoglobuline G1-lambda1, anti-[Homo sapiens RGMA (membre a de la famille de molécules d'orientation répulsive, molécule d'orientation répulsive A, RGMa)], Homo sapiens anticorps monoclonal; chaîne lourde gamma1 (1-450) [Homo sapiens VH (IGHV1-18*01 (92.90%) -(IGHD) -IGHJ6*03) [8.8.13] (1-120) -IGHG1*01, Gm17,1 (CH1 (121-218), charnière (219-233),CH2 L1.2>A (238), L1.3>A (237), T14>Q (253) (234-343), CH3 M107>L (431) (344-448), CHS (449-450)) (121-450)], (223-214')-disulfure avec la chaîne légère lambda1 (1'-215') [Homo sapiens V-LAMBDA (IGLV2-11*01 (89.90%) -IGLJ2*01) [9.3.9] (1'-109') -IGLC2*01 (110'-215')]; dimère (229-229'':232-232'')-bisdisulfure
elezanumab inmunoglobulina G1-lambda1, anti-[Homo sapiens RGMA (miembro de la familia de moléculas de orientación repulsiva, molécula de orientación repulsiva A, RGMa)], Homo sapiens anticuerpo monoclonal;

WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
89
cadena pesada gamma1 (1-450) [Homo sapiens VH (IGHV1-18*01 (92.90%) -(IGHD) -IGHJ6*03) [8.8.13] (1-120) -IGHG1*01, Gm17,1 (CH1 (121-218), bisagra (219-233),CH2 L1.2>A (238), L1.3>A (237), T14>Q (253) (234-343), CH3 M107>L (431) (344-448), CHS (449-450)) (121-450)], (223-214')-disulfuro con la cadena ligera lambda1 (1'-215') [Homo sapiens V-LAMBDA (IGLV2-11*01 (89.90%) -IGLJ2*01) [9.3.9] (1'-109') -IGLC2*01 (110'-215')]; dímero (229-229'':232-232'')-bisdisulfuro
elivaldogenum tavalentivecum # elivaldogene tavalentivec A VSV-G*-pseudotyped self-inactivating HIV-1-derived
lentiviral vector (pLBP100 hALD) encoding human adrenoleukodystrophy (ALD) protein (ABCD1 gene) under the control of a modified myeloproliferative sarcoma virus promoter (MND**) * VSV-G = vesicular stomatitis virus G envelope protein ** MND = myeloproliferative sarcoma virus enhancer with negative control region deleted, dl587rev primer-binding site substituted
élivaldogène tavalentivec vecteur lentiviral dérivé du VIH-1 auto-inactivant (pLBP100 hALD) pseudotypé VSV-G*, codant pour la protéine humaine (gène ABCD1) de l'adrénoleucodystrophie (ALD), sous le contrôle d'un promoteur du virus du sarcome myéloprolifératif modifié (MND**) * VSV-G = glycoprotéine G de l'enveloppe du virus de la stomatite vésiculaire ** MND = promoteur du virus du sarcome myéloprolifératif dont la région de contrôle négatif a été supprimée, le site de liaison de l'amorce substitué par dl587rev
Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
90
elivaldogén tavalentivec vector lentiviral derivado del VIH-1 auto-inactivante
(pLBP100 hALD) pseudotipo VSV-G*, que codifica para la proteína humana (gen ABCD1) de la adrenoleucodistrofia (ALD), bajo el control de un promotor del virus del sarcoma mieloproliferativo modificado (MND**) * VSV-G = glicoproteína G del virus de la estomatitis vesicular ** MND = promotor del virus del sarcoma mieloproliferativo bajo la región de control negativo ha sido suprimido, el sitio de enlace del inicio substituido por dl587rev
eltrapuldencelum eltrapuldencel Autologous dendritic cells loaded with antigen from self-
renewing, proliferating autologous irradiated tumour cells, in a solution of granulocyte-macrophage colony stimulating factor (GM-CSF). Patient's monocytes are collected from peripheral blood by leukocyte apheresis, led to differentiate into dendritic cells in culture and incubated with expanded irradiated autologous self-renewing, cancer-initiating cells (CICs).
eltrapuldencel cellules dendritiques autologues chargées avec un antigène de cellules tumorales autologues, auto-renouvellantes, proliférantes et irradiées, dans une solution de facteur de stimulation des colonies de granulocytes et de macrophages (GM-CSF). Les monocytes des patients sont recueillis par leucaphérèse à partir de sang périphérique, conduits à se différencier en cellules dendritiques par culture et incubés avec des cellules initiatrices de cancer (CICs) autologues ayant des propriétés d'auto-renouvellement.
eltrapuldencel células dendríticas autólogas cargadas con un antígeno de células tumorales autólogas, autorenovables, proliferantes e irradiadas, en una solución de factor de estimulación de colonias de granulocitos y de macrófagos (GM-CSF). Los monocitos de los pacientes se recogen por leucoféresis a partir de sangre periférica, conducidos a diferenciarse en células dendríticas para el cultivo e incubados con las células iniciadoras de cáncer (CICs) autólogas con las propiedades de autorenovación.
emapalumabum # emapalumab immunoglobulin G1-lambda1, anti-[Homo sapiens IFNG
(interferon gamma, IFN gamma)], Homo sapiens monoclonal antibody; gamma1 heavy chain (1-453) [Homo sapiens VH (IGHV3-23*01 -(IGHD) -IGHJ5*02) [8.8.16] (1-123) -IGHG1*03, Gm17,1 (CH1 (124-221), hinge (222-236), CH2 (237-346), CH3 (347-451), CHS (452-453)) (124-453)], (226-216')-disulfide with lambda1 light chain (1'-217') [Homo sapiens V-LAMBDA (IGLV6-57*01 (99.00%) -IGLJ3*02) [8.3.10] (1'-111') -IGLC2*01 (112'-217')]; dimer (232-232'':235-235'')-bisdisulfide

WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
91
émapalumab immunoglobuline G1-lambda1, anti-[Homo sapiens IFNG (interféron gamma, IFN gamma)], Homo sapiens anticorps monoclonal; chaîne lourde gamma1 (1-453) [Homo sapiens VH (IGHV3-23*01 -(IGHD) -IGHJ5*02) [8.8.16] (1-123) -IGHG1*03, Gm17,1 (CH1 (124-221), charnière (222-236), CH2 (237-346), CH3 (347-451), CHS (452-453)) (124-453)],(226-216')-disulfure avec la chaîne légère lambda1 (1'-217') [Homo sapiens V-LAMBDA (IGLV6-57*01 (99.00%) -IGLJ3*02) [8.3.10] (1'-111') -IGLC2*01 (112'-217')]; dimère (232-232'':235-235'')-bisdisulfure
emapalumab inmunoglobulina G1-lambda1, anti-[Homo sapiens IFNG (interferón gamma, IFN gamma)], Homo sapiens anticuerpo monoclonal; cadena pesada gamma1 (1-453) [Homo sapiens VH (IGHV3-23*01 -(IGHD) -IGHJ5*02) [8.8.16] (1-123) -IGHG1*03, Gm17,1 (CH1 (124-221), bisagra (222-236), CH2 (237-346), CH3 (347-451), CHS (452-453)) (124-453)], (226-216')-disulfuro con la cadena ligera lambda1 (1'-217') [Homo sapiens V-LAMBDA (IGLV6-57*01 (99.00%) -IGLJ3*02) [8.3.10] (1'-111') -IGLC2*01 (112'-217')]; dímero (232-232'':235-235'')-bisdisulfuro
ensartinibum ensartinib 6-amino-5-[(1R)-1-(2,6-dichloro-3-fluorophenyl)ethoxy]-
N-{4-[(3R,5S)-3,5-dimethylpiperazine- 1-carbonyl]phenyl}pyridazine-3-carboxamide
ensartinib 6-amino-5-[(1R)-1-(2,6-dichloro-3-fluorophényl)éthoxy]- N-{4-[(3R,5S)-3,5-diméthylpiperazine- 1-carbonyl]phényl}pyridazine-3-carboxamide
ensartinib 6-amino-5-[(1R)-1-(2,6-dicloro-3-fluorofenil)etoxi]- N-{4-[(3R,5S)-3,5-dimetilpiperazina- 1-carbonil]fenil}piridazina-3-carboxamida
Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
92
C26H27Cl2FN6O3
NN
O
HN
O
N
NH
CH3H
CH3
H
O
H2N
H
CH3
Cl
Cl
F
enzaplatovirum enzaplatovir (10aR)-1-(3-methyl-1,2-oxazole-4-carbonyl)-
10a-(6-methylpyridin-3-yl)-2,3,10,10a-tetrahydro- 1H,5H-imidazo[1,2-a]pyrrolo[1,2-d]pyrazin-5-one
enzaplatovir (10aR)-1-(3-méthyl-1,2-oxazole-4-carbonyl)- 10a-(6-méthylpyridin-3-yl)-2,3,10,10a-tétrahydro- 1H,5H-imidazo[1,2-a]pyrrolo[1,2-d]pyrazin-5-one
enzaplatovir (10aR)-1-(3-metil-1,2-oxazol-4-carbonil)- 10a-(6-metilpiridin-3-il)-2,3,10,10a-tetrahidro- 1H,5H-imidazo[1,2-a]pirrolo[1,2-d]pirazin-5-ona
C20H19N5O3
epertinibum epertinib N-{3-chloro-4-[(3-fluorophenyl)methoxy]phenyl}-6-[(1Z)-
N-{[(3R)-morpholin-3-yl]methoxy}but- 2-ynimidoyl]quinazolin-4-amine
épertinib N-{3-chloro-4-[(3-fluorophényl)méthoxy]phényl}-6-[(1Z)- N-{[(3R)-morpholin-3-yl]méthoxy}but- 2-ynimidoyl]quinazolin-4-amine
epertinib N-{3-cloro-4-[(3-fluorofenil)metoxi]fenil}-6-[(1Z)-N-{[(3R)-morfolin-3-il]metoxi}but-2-inimidoil]quinazolin-4-amina
C30H27ClFN5O3

WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
93
eptinezumabum # eptinezumab immunoglobulin G1-kappa, anti-[Homo sapiens CALCA
(calcitonin related polypeptide alpha) calcitonin gene-related peptide 1, CGRP1, 83-119 and Homo sapiens CALCB (calcitonin related polypeptide beta) calcitonin gene-related peptide 2, CGRP2, 82-118], humanized monoclonal antibody; gamma1 heavy chain (1-441) [humanized VH (Homo sapiens IGHV3-66*01 (81.40%) -(IGHD)-IGHJ3*02) [8.7.5] (1-111) -Homo sapiens IGHG1*03 (CH1 K119>A (156) (112-209), hinge (210-224), CH2 N84.4>A (291) (225-334), CH3 (335-439), CHS (440-441)) (112-441)], (214-219')-disulfide with kappa light chain (1'-219') [humanized V-KAPPA (Homo sapiens IGKV1-27*01 (86.20%) -IGKJ4*01) [8.3.13] (1'-112') -Homo sapiens IGKC*01, Km3 (113'-219')]; dimer (220-220":223-223")-bisdisulfide
eptinezumab immunoglobuline G1-kappa, anti-[Homo sapiens CALCA (polypeptide alpha apparenté à la calcitonine) peptide 1 apparenté au gène de la calcitonine, CGRP1, 83-119 et Homo sapiens CALCB (polypeptide bêta apparenté à la calcitonine) peptide 2 apparenté au gène de la calcitonine, CGRP2, 82-118], anticorps monoclonal humanisé; chaîne lourde gamma1 (1-441) [VH humanisé (Homo sapiens IGHV3-66*01 (81.40%) -(IGHD)-IGHJ3*02) [8.7.5] (1-111) -Homo sapiens IGHG1*03 (CH1 K119>A (156) (112-209), charnière (210-224), CH2 N84.4>A (291) (225-334), CH3 (335-439), CHS (440-441)) (112-441)], (214-219')-disulfure avec la chaîne légère kappa (1'-219') [V-KAPPA humanisé (Homo sapiens IGKV1-27*01 (86.20%) -IGKJ4*01) [8.3.13] (1'-112') -Homo sapiens IGKC*01, Km3 (113'-219')]; dimère (220-220":223-223")-bisdisulfure
eptinezumab inmunoglobulina G1-kappa, anti-[Homo sapiens CALCA (polipéptido alfa relacionado con la calcitonina) péptido 1 relacionado con el gen de la calcitonina, CGRP1, 83-119 y Homo sapiens CALCB (polipéptido beta relacionado con la calcitonina) péptido 2 relacionado con el gen de la calcitonina, CGRP2, 82-118], anticuerpo monoclonal humanizado; cadena pesada gamma1 (1-441) [VH humanizado (Homo sapiens IGHV3-66*01 (81.40%) -(IGHD)-IGHJ3*02) [8.7.5] (1-111) -Homo sapiens IGHG1*03 (CH1 K119>A (156) (112-209), bisagra (210-224), CH2 N84.4>A (291) (225-334), CH3 (335-439), CHS (440-441)) (112-441)], (214-219')-disulfuro con la cadena ligera kappa (1'-219') [V-KAPPA humanizado (Homo sapiens IGKV1-27*01 (86.20%) -IGKJ4*01) [8.3.13] (1'-112') -Homo sapiens IGKC*01, Km3 (113'-219')]; dímero (220-220":223-223")-bisdisulfuro
Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
94
erenumabum # erenumab immunoglobulin G2-lambda, anti-[Homo sapiens CALCRL
(calcitonin receptor like receptor, calcitonin gene-related peptide receptor, CGRPR, CGRP-R, CRLR)], Homo sapiens monoclonal antibody; gamma2 heavy chain (1-456) [Homo sapiens VH (IGHV3-30*03 (93.90%) -(IGHD) -IGHJ6*01) [8.8.23] (1-130) -IGHG2*01, G2m.. (CH1 (131-228), hinge (229-240), CH2 (241-349), CH3 (350-454), CHS (455-456)) (131-456)], (144-215')-disulfide with lambda light chain (1'-216') [Homo sapiens V-LAMBDA (IGLV1-51*01 (98.00%) -IGLJ2*01) [8.3.11] (1'-110') -IGLC1*01 (111'-216')]; dimer (232-232'':233-233'':236-236'':239-239'')-tetrakisdisulfide
érénumab immunoglobuline G2-lambda, anti-[Homo sapiens CALCRL (récepteur analogue au récepteur de la calcitonine, récepteur du peptide apparenté au gène de la calcitonine, CGRPR, CGRP-R, CRLR)], Homo sapiens anticorps monoclonal; chaîne lourde gamma2 (1-456) [Homo sapiens VH (IGHV3-30*03 (93.90%) -(IGHD) -IGHJ6*01) [8.8.23] (1-130) -IGHG2*01, G2m.. (CH1 (131-228), charnière (229-240), CH2 (241-349), CH3 (350-454), CHS (455-456)) (131-456)], (144-215')-disulfure avec la chaîne légère lambda (1'-216') [Homo sapiens V-LAMBDA (IGLV1-51*01 (98.00%) -IGLJ2*01) [8.3.11] (1'-110') -IGLC1*01 (111'-216')]; dimère (232-232'':233-233'':236-236'':239-239'')-tétrakisdisulfure
erenumab inmunoglobulina G2-lambda, anti-[Homo sapiens CALCRL (receptor análogo del receptor de la calcitonina, receptor del péptido relacionado con el gen de la calcitonina, CGRPR, CGRP-R, CRLR)], Homo sapiens anticuerpo monoclonal;

WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
95
cadena pesada gamma2 (1-456) [Homo sapiens VH
(IGHV3-30*03 (93.90%) -(IGHD) -IGHJ6*01) [8.8.23] (1-130) -IGHG2*01, G2m.. (CH1 (131-228), bisagra (229-240), CH2 (241-349), CH3 (350-454), CHS (455-456)) (131-456)], (144-215')-disulfuro con la cadena ligera lambda (1'-216') [Homo sapiens V-LAMBDA (IGLV1-51*01 (98.00%) -IGLJ2*01) [8.3.11] (1'-110') -IGLC1*01 (111'-216')]; dímero (232-232'':233-233'':236-236'':239-239'')-tetrakisdisulfuro
eretidigenum velentivecum # eretidigene velentivec Recombinant, non-replicating, lentiviral vector
w1.6_hWAS_WPREmut6 (VSV-G*) encoding the human Wiskott-Aldrich syndrome (WAS) gene under the control of its native promoter, post-transcriptionally-regulated by a modified WPRE (mut6 WPRE**) * VSV-G = vesicular stomatitis virus G envelope protein ** WPRE m6 = WPRE mut6 = mut6 = mut6 WPRE: mutated woodchuck hepatitis virus posttranscriptional regulatory element
érétidigène vélentivec vecteur lentiviral recombinant sans capacité de réplication w1.6_hWAS_WPREmut6 (VSV-G*) contenant le gène humain du syndrome de Wiskott-Aldrich sous le contrôle de son promoteur natif, régulé en post-transcription par WPRE** modifié (mut6 WPRE**) * VSV-G = glycoprotéine G du virus de la stomatite vésiculaire **WPRE m6 = WPRE mut6 = mut6 = mut6 WPRE: élément muté de régulation post-transcriptionnelle du virus de l'hépatite de la marmotte d'Amérique
Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
96
eretidigén velentivec vector lentiviral recombinante no replicativo w1.6_hWAS_WPREmut6 (VSV-G*) que contiene el gen humano del síndrome de Wiskott-Aldrich bajo el control de su promotor nativo, regulado post-transcripcionalmente por WPRE** modificado (mut6 WPRE**) * VSV-G = glicoproteína G del virus de la estomatitis vesicular **WPRE m6 = WPRE mut6 = mut6 = mut6 WPRE: elemento mutado de regulación post-transcriptionnal del virus de la hepatitis de la marmota de América
evobrutinibum evobrutinib 1-[4-({[6-amino-5-(4-phenoxyphenyl)pyrimidin-
4-yl]amino}methyl)piperidin-1-yl]prop-2-en-1-one
évobrutinib 1-[4-({[6-amino-5-(4-phénoxyphényl)pyrimidin- 4-yl]amino}méthyl)pipéridin-1-yl]prop-2-én-1-one
evobrutinib 1-[4-({[6-amino-5-(4-fenoxifenil)pirimidin- 4-il]amino}metil)piperidin-1-il]prop-2-en-1-ona
C25H27N5O2
NCH2
O
HNN
N
ONH2
fezolinetantum fezolinetant (4-fluorophenyl)[(8R)-8-methyl-3-(3-methyl-1,2,4-
thiadiazol-5-yl)-5,6-dihydro-1,2,4-triazolo[4,3-a]pyrazin-7(8H)-yl]methanone
fézolinétant (4-fluorophényl)[(8R)-8-méthyl-3-(3-méthyl-1,2,4-thiadiazol-5-yl)-5,6-dihydro-1,2,4-triazolo[4,3-a]pyrazin-7(8H)-yl]méthanone
fezolinetant (4-fluorofenil)[(8R)-8-metil-3-(3-metil-1,2,4-tiadiazol-5-il)-5,6-dihidro-1,2,4-triazolo[4,3-a]pirazin-7(8H)-il]metanona
C16H15FN6OS
flurdihydroergotaminum flurdihydroergotamine 5'α-benzyl-12'-hydroxy-2'-methyl-2-(trifluoromethyl)-(10α)-
9,10-dihydroergotaman-3',6',18-trione
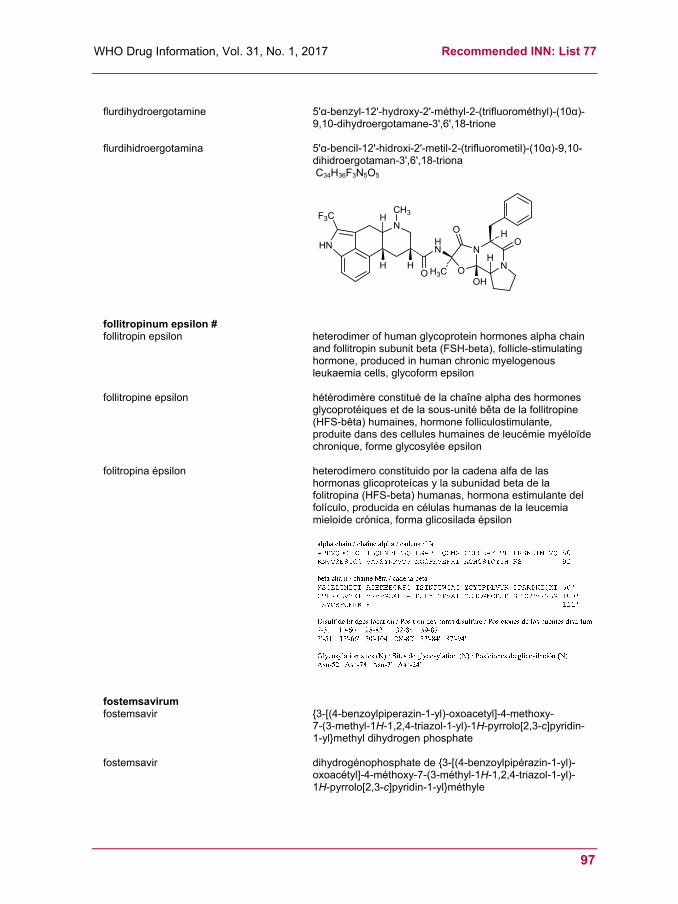
WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
97
flurdihydroergotamine 5'α-benzyl-12'-hydroxy-2'-méthyl-2-(trifluorométhyl)-(10α)-
9,10-dihydroergotamane-3',6',18-trione
flurdihidroergotamina 5'α-bencil-12'-hidroxi-2'-metil-2-(trifluorometil)-(10α)-9,10-dihidroergotaman-3',6',18-triona
C34H36F3N5O5
N
HN
H
H
CH3
HN
HO
N
NO
O
H3C
H
HO
OH
F3C
follitropinum epsilon # follitropin epsilon heterodimer of human glycoprotein hormones alpha chain
and follitropin subunit beta (FSH-beta), follicle-stimulating hormone, produced in human chronic myelogenous leukaemia cells, glycoform epsilon
follitropine epsilon hétérodimère constitué de la chaîne alpha des hormones glycoprotéiques et de la sous-unité bêta de la follitropine (HFS-bêta) humaines, hormone folliculostimulante, produite dans des cellules humaines de leucémie myéloïde chronique, forme glycosylée epsilon
folitropina épsilon heterodímero constituido por la cadena alfa de las hormonas glicoproteícas y la subunidad beta de la folitropina (HFS-beta) humanas, hormona estimulante del folículo, producida en células humanas de la leucemia mieloide crónica, forma glicosilada épsilon
fostemsavirum fostemsavir {3-[(4-benzoylpiperazin-1-yl)-oxoacetyl]-4-methoxy-
7-(3-methyl-1H-1,2,4-triazol-1-yl)-1H-pyrrolo[2,3-c]pyridin-1-yl}methyl dihydrogen phosphate
fostemsavir dihydrogénophosphate de {3-[(4-benzoylpipérazin-1-yl)-oxoacétyl]-4-méthoxy-7-(3-méthyl-1H-1,2,4-triazol-1-yl)-1H-pyrrolo[2,3-c]pyridin-1-yl}méthyle

Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
98
fostemsavir dihidrogenofosfato de {3-[(4-benzoilpiperazin-1-il)-oxoacetil]-4-metoxi-7-(3-metil-1H-1,2,4-triazol-1-il)- 1H-pirrolo[2,3-c]piridin-1-il}metilo
C25H26N7O8P
N
N
O
O
O
N
N
OCH3
N
O P
OH
OHO
N
N
H3C
fremanezumabum # fremanezumab immunoglobulin G2-kappa, anti-[Homo sapiens CALCA
(calcitonin related polypeptide alpha) calcitonin gene-related peptide 1, CGRP1, 83-119 and Homo sapiens CALCB (calcitonin related polypeptide beta) calcitonin gene-related peptide 2, CGRP2, 82-118], humanized monoclonal antibody; gamma2 heavy chain (1-448) [humanized VH (Homo sapiens IGHV3-7*01 (85.70%) -(IGHD) -IGHJ4*01) [8.10.13] (1-122) -Homo sapiens IGHG2*01, G2m..(CH1 (123-220), hinge (221-232), CH2 A115>S (331), P116>S (332) (233-341), CH3 (342-446), CHS (447-448)) (123-448)], (136-214')-disulfide with kappa light chain (1'-214') [humanized V-KAPPA (Homo sapiens IGKV3-11*01 (85.30%) -IGKJ2*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 (108'-214')]; dimer (224-224":225-225":228-228":231-231'')-tetrakisdisulfide
frémanezumab immunoglobuline G2-kappa, anti-[Homo sapiens CALCA (polypeptide alpha apparenté à la calcitonine) peptide 1 apparenté au gène de la calcitonine, CGRP1, 83-119 et Homo sapiens CALCB (polypeptide bêta apparenté à la calcitonine) peptide 2 apparenté au gène de la calcitonine, CGRP2, 82-118], anticorps monoclonal humanisé; chaîne lourde gamma2 (1-448) [VH humanisé (Homo sapiens IGHV3-7*01 (85.70%) -(IGHD) -IGHJ4*01) [8.10.13] (1-122) -Homo sapiens IGHG2*01, G2m..(CH1 (123-220), charnière (221-232), CH2 A115>S (331), P116>S (332) (233-341), CH3 (342-446), CHS (447-448)) (123-448)], (136-214')-disulfure avec la chaîne légère kappa (1'-214') [V-KAPPA humanisé (Homo sapiens IGKV3-11*01 (85.30%) -IGKJ2*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 (108'-214')]; dimère (224-224":225-225":228-228":231-231'')-tétrakisdisulfure
fremanezumab inmunoglobulina G2-kappa, anti-[Homo sapiens CALCA (polipéptido alfa relacionado con la calcitonina) péptido 1 relacionado con el gen de la calcitonina, CGRP1, 83-119 y Homo sapiens CALCB (polipéptido beta relacionado con la calcitonina) péptido 2 relacionado con el gen de la calcitonina, CGRP2, 82-118], anticuerpo monoclonal humanizado;

WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
99
cadena pesada gamma2 (1-448) [VH humanizado (Homo sapiens IGHV3-7*01 (85.70%) -(IGHD) -IGHJ4*01) [8.10.13] (1-122) -Homo sapiens IGHG2*01, G2m.. (CH1 (123-220), bisagra (221-232), CH2 A115>S (331), P116>S (332) (233-341), CH3 (342-446), CHS (447-448)) (123-448)], (136-214')-disulfuro con la cadena ligera kappa (1'-214') [V-KAPPA humanizado (Homo sapiens IGKV3-11*01 (85.30%) -IGKJ2*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 (108'-214')]; dímero (224-224":225-225":228-228":231-231'')-tetrakisdisulfuro
gemtuzumabum ozogamicinum # gemtuzumab ozogamicin immunoglobulin G4-kappa, anti-[Homo sapiens CD33
(sialic acid binding Ig-like lectin 3, SIGLEC3, SIGLEC-3, gp67, p67)], humanized monoclonal antibody conjugated to N-acetyl-gamma calicheamicin; gamma4 heavy chain (1-443) [humanized VH (Homo sapiens IGHV1-3*01 (72.90%) -(IGHD) -IGHJ5*01) [8.8.9] (1-116)), IGHG4*01 (CH1 (117-214), hinge S10>P (224) (215-226), CH2 (227-336), CH3 (337-441), CHS (442-443)) (117-443)], (130-218')-disulfide with kappa light chain (1'-218') [humanized V-KAPPA (Homo sapiens IGKV1-5*01 (81.90%) -IGKJ1*01) [10.3.9] (1'-111') -Homo sapiens IGKC*01, Km3 (112'-218')]; dimer (232-232":235-235")-bisdisulfide; conjugated, on an average of 2 or 3 lysyl (0-6), to N-acetyl-S'-des(methylsulfanyl)-S'-(4-hydrazinyl-2-methyl-4-oxobutan-2-yl)calicheamicin γ1 via a bifunctional 4-(4-acetylphenoxy)butanoyle (AcBut) linker
gemtuzumab ozogamicine immunoglobuline G4-kappa, anti-[Homo sapiens CD33 (lectine 3 de type Ig-like liant l'acide sialique, SIGLEC3, SIGLEC-3, gp67, p67)], anticorps monoclonal humanisé conjugué à la N-acétyl-gamma calichéamicine; chaîne lourde gamma4 chain (1-443) [VH humanisé (Homo sapiens IGHV1-3*01 (72.90%) -(IGHD) -IGHJ5*01) [8.8.9] (1-116)), IGHG4*01 (CH1 (117-214), charnière S10>P (224) (215-226), CH2 (227-336), CH3 (337-441),

Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
100
CHS (442-443)) (117-443)], (130-218')-disulfure avec la chaîne légère (1'-218') [V-KAPPA humanisé (Homo sapiens IGKV1-5*01 (81.90%) -IGKJ1*01) [10.3.9] (1'-111') -Homo sapiens IGKC*01, Km3 (112'-218')]; dimère (232-232":235-235")-bisdisulfure; conjugué, sur 2 ou 3 lysyl en moyenne (0-6), à la N-acétyl-S'-dés(méthylsulfanyl)-S'-(4-hydrazinyl-2-méthyl-4-oxobutan-2-yl)calichéamicine γ1 via un linker bifunctionnel 4-(4-acétylphénoxy)butanoyle (AcBut)
gemtuzumab ozogamicina inmunoglobulina G4-kappa, anti-[Homo sapiens CD33 (lectina de tipo inmunoglobulina 3 que se une al ácido siálico, SIGLEC3, SIGLEC-3, gp67, p67)], anticuerpo monoclonal humanizado conjugado con la N-acetil-gamma calicheamicina; cadena pesada gamma4 cadena (1-443) [VH humanizado (Homo sapiens IGHV1-3*01 (72.90%) -(IGHD) -IGHJ5*01) [8.8.9] (1-116)), IGHG4*01 (CH1 (117-214), bisagra S10>P (224) (215-226), CH2 (227-336), CH3 (337-441), CHS (442-443)) (117-443)], (130-218')-disulfuro con la cadena ligera (1'-218') [V-KAPPA humanizada (Homo sapiens IGKV1-5*01 (81.90%) -IGKJ1*01) [10.3.9] (1'-111') -Homo sapiens IGKC*01, Km3 (112'-218')]; dímero (232-232":235-235")-bisdisulfuro; conjugado, sobre 2 o 3 lisil por término medio (0-6), a la N-acetil-S'-des(metilsulfanil)-S'-(4-hidrazinil-2-metil-4-oxobutan- 2-il)calicheamicina γ1 mediante un enlace bifuncional 4-(4-acetilfenoxi)butanoil (AcBut)

WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
101
golodirsenum golodirsen all-P-ambo-[2',3'-azanediyl-P-(dimethylamino)-P,2',3'-
trideoxy-2',3'-seco](2'-N→5')(G-T-T-G-C-C-T-C-C-G-G-T-T-C-T-G-A-A-G-G-T-G-T-T-C) 5'-{P-[4-({2-[2-(2-hydroxyethoxy)ethoxy]ethoxy}carbonyl)piperazin-1-yl]-N,N-dimethylphosphonamidate}
golodirsen tout-P-ambo-5'-{P-[4-({2-[2-(2-hydroxy-éthoxy)éthoxy]éthoxy}carbonyl)pipérazin-1-yl]-N,N-diméthylphosphonamidate} de [2',3'-azanediyl-P-(diméthylamino)-P,2',3'-tridéoxy-2',3'-séco](2'-N→5')(G-T-T-G-C-C-T-C-C-G-G-T-T-C-T-G-A-A-G-G-T-G-T-T-C)
golodirsén todo-P-ambo-5'-{P-[4-({2-[2-(2-hidroxietoxi)etoxi]etoxi}carbonil)piperazin-1-il]-N,N-dimetilfosfonamidato} de [2',3'-azanediil-P-(dimetilamino)-P,2',3'-tridesoxi-2',3'-seco](2'-N→5')(G-T-T-G-C-C-T-C-C-G-G-T-T-C-T-G-A-A-G-G-T-G-T-T-C)
C305H481N138O112P25
hemoglobinum betafumarilum (bovinum) # hemoglobin betafumaril (bovine) S3.β92,S3.β'92-bis(2-amino-2-oxoethyl)-N6.β81,N6.β'81-[(2E)-(but-
2-enedioyl)]bovine hemoglobin (α2β2 tetramer)
hémoglobine bêtafumaril (bovine) S3.β92,S3.β'92-bis(2-amino-2-oxoéthyl)-N6.β81,N6.β'81-[(2E)-(but-2-ènedioyl)]hémoglobine bovine (tétramère α2β2)
hemoglobina betafumarilo (bovina) S3.β92,S3.β'92-bis(2-amino-2-oxoetil)-N6.β81,N6.β'81-[(2E)-(but- 2-enedioil)]hemoglobina bovina (tetrámero α2β2)

Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
102
ifabotuzumabum # ifabotuzumab immunoglobulin G1-kappa, anti-[Homo sapiens EPHA3
(ephrin receptor A3, EPH receptor A3, ephrin type-A receptor 3, tyrosine protein kinase TYR04, tyrosine-protein kinase receptor REK4, ETK, ETK1, HEK, HEK4)], humanized monoclonal antibody; gamma1 heavy chain (1-449) [humanized VH (Homo sapiens IGHV1-2*02 (91.80%) -(IGHD)-IGHJ6*01) [8.8.11] (1-118) -Homo sapiens IGHG1*03, Gm3 (CH1 (119-216), hinge (217-231), CH2 (232-341), CH3 (342-447), CHS (448-449)) (119-448)], (221-214')-disulfide with kappa light chain (1'-214') [humanized V-KAPPA (Homo sapiens IGKV1D-16*01 (91.60%) -IGKJ2*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01 (108'-214')]; dimer (227-227":230-230")-bisdisulfide
ifabotuzumab immunoglobuline G1-kappa, anti-[Homo sapiens EPHA3 (récepteur A3 d'éphrine, récepteur A3 d'EPH, récepteur 3 type-A d'éphrine, protéine tyrosine kinase TYR04, récepteur tyrosine-protéine kinase REK4, ETK, ETK1, HEK, HEK4)], anticorps monoclonal humanisé; chaîne lourde gamma1 (1-449) [VH humanisé (Homo sapiens IGHV1-2*02 (91.80%) -(IGHD)-IGHJ6*01) [8.8.11] (1-118) -Homo sapiens IGHG1*03, Gm3 (CH1 (119-216), charnière (217-231), CH2 (232-341), CH3 (342-447), CHS (448-449)) (119-448)], (221-214')-disulfure avec la chaîne légère kappa (1'-214') [V-KAPPA humanisé (Homo sapiens IGKV1D-16*01 (91.60%) -IGKJ2*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01 (108'-214')]; dimère (227-227":230-230")-bisdisulfure
ifabotuzumab inmunoglobulina G1-kappa, anti-[Homo sapiens EPHA3 (receptor A3 de efrina, receptor A3 d'EPH, receptor 3 tipo-A de efrina, tirosina protein kinasa TYR04, receptor tirosina-protein kinasa REK4, ETK, ETK1, HEK, HEK4)], anticuerpo monoclonal humanizado; cadena pesada gamma1 (1-449) [VH humanizado (Homo sapiens IGHV1-2*02 (91.80%) -(IGHD)-IGHJ6*01) [8.8.11] (1-118) -Homo sapiens IGHG1*03, Gm3 (CH1 (119-216), bisagra (217-231), CH2 (232-341), CH3 (342-447), CHS (448-449)) (119-448)], (221-214')-disulfuro con la cadena ligera kappa (1'-214') [V-KAPPA humanizado (Homo sapiens IGKV1D-16*01 (91.60%) -IGKJ2*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01 (108'-214')]; dímero (227-227":230-230")-bisdisulfuro

WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
103
Heavy chain / Chaîne lourde / Cadena pesadaQVQLVQSGAE VKKPGASVKV SCKASGYTFT GYWMNWVRQA PGQGLEWMGD 50IYPGSGNTNY DEKFQGRVTM TRDTSISTAY MELSRLRSDD TAVYYCARGG 100YYEDFDSWGQ GTTVTVSSAS TKGPSVFPLA PSSKSTSGGT AALGCLVKDY 150FPEPVTVSWN SGALTSGVHT FPAVLQSSGL YSLSSVVTVP SSSLGTQTYI 200CNVNHKPSNT KVDKRVEPKS CDKTHTCPPC PAPELLGGPS VFLFPPKPKD 250TLMISRTPEV TCVVVDVSHE DPEVKFNWYV DGVEVHNAKT KPREEQYNST 300YRVVSVLTVL HQDWLNGKEY KCKVSNKALP APIEKTISKA KGQPREPQVY 350TLPPSREEMT KNQVSLTCLV KGFYPSDIAV EWESNGQPEN NYKTTPPVLD 400SDGSFFLYSK LTVDKSRWQQ GNVFSCSVMH EALHNHYTQK SLSLSPGK 448
Light chain / Chaîne légère / Cadena ligeraDIQMTQSPSF LSASVGDRVT ITCRASQGII SYLAWYQQKP EKAPKRLIYA 50ASSLQSGVPS RFSGSGSGTE FTLTISSLQP EDFATYYCGQ YANYPYTFGQ 100GTKLEIKRTV AAPSVFIFPP SDEQLKSGTA SVVCLLNNFY PREAKVQWKV 150DNALQSGNSQ ESVTEQDSKD STYSLSSTLT LSKADYEKHK VYACEVTHQG 200LSSPVTKSFN RGEC 214 Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H (C23-C104) 22-96 145-201 262-322 368-426 22''-96'' 145''-201'' 262''-322'' 368''-426''Intra-L (C23-C104) 23'-88' 134'-194' 23'''-88''' 134'''-194''' Inter-H-L (h 5-CL 126) 221-214' 221''-214''' Inter-H-H (h 11, h 14) 227-227'' 230-230''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:298, 298''Afucosylated complex bi-antennary CHO-type glycans / glycanes de type CHO bi-antennairescomplexes afucosylés / glicanos de tipo CHO biantenarios complejos no fucosilados
ilmetropii iodidum ilmetropium iodide (1R,3r,5S)-3-{[(2RS)-2-(hydroxymethyl)-
2-phenylbutanoyl]oxy}-8,8-dimethyl- 8-azabicyclo[3.2.1]octanium iodide
iodure d'ilmétropium iodure de (1R,3r,5S)-3-{[(2RS)-2-(hydroxyméthyl)- 2-phénylbutanoyl]oxy}-8,8-diméthyl- 8-azabicyclo[3.2.1]octanium
ioduro de ilmetropio ioduro de (1R,3r,5S)-3-{[(2RS)-2-fenil- 2-(hidroximetil)butanoil]oxi}-8,8-dimetil- 8-azabiciclo[3.2.1]octanio
C20H30INO3
imlatoclaxum imlatoclax 4-(4-{[2-(4-chlorophenyl)-4,4-dimethylcyclohex-1-en-
1-yl]methyl}piperazin-1-yl)-N-(4-{[(trans-4-hydroxy- 4-methylcyclohexyl)methyl]amino}-3-nitrobenzenesulfonyl)-2-[(1H-pyrrolo[2,3-b]pyridin-5-yl)oxy]benzamide
imlatoclax 4-(4-{[2-(4-chlorophényl)-4,4-diméthylcyclohex-1-én- 1-yl]méthyl}pipérazin-1-yl)-N-(4-{[(trans-4-hydroxy- 4-méthylcyclohexyl)méthyl]amino}-3-nitrobenzenesulfonyl)-2-[(1H-pyrrolo[2,3-b]pyridin-5-yl)oxy]benzamide
imlatoclax 4-(4-{[2-(4-clorofenil)-4,4-dimetilciclohex-1-en- 1-il]metil}piperazin-1-il)-N-(4-{[(trans-4-hidroxi- 4-metilciclohexil)metil]amino}-3-nitrobencenosulfonil)- 2-[(1H-pirrolo[2,3-b]piridin-5-il)oxi]benzamida
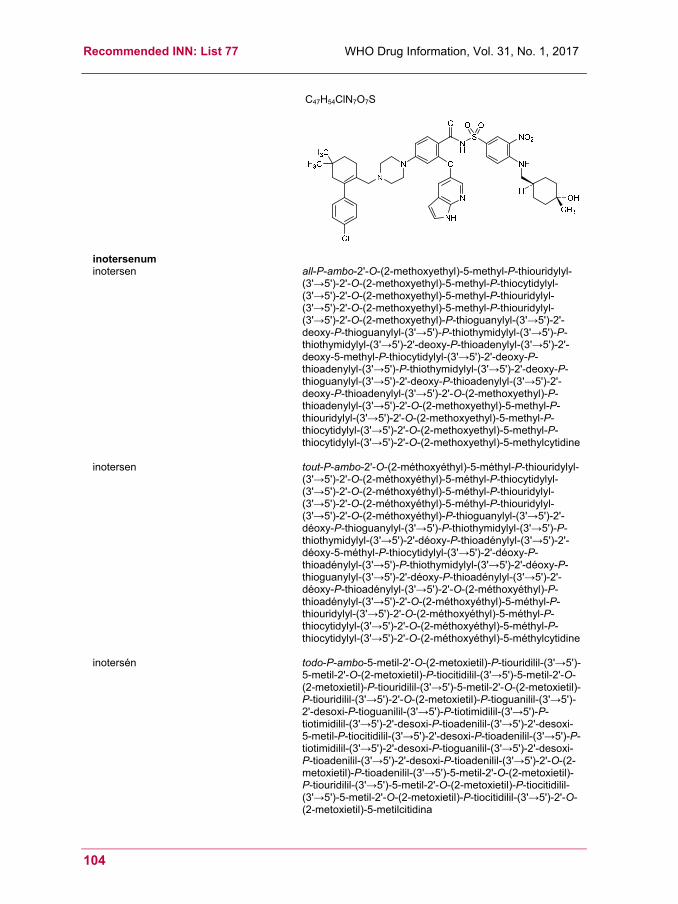
Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
104
C47H54ClN7O7S
inotersenum inotersen all-P-ambo-2'-O-(2-methoxyethyl)-5-methyl-P-thiouridylyl-
(3'→5')-2'-O-(2-methoxyethyl)-5-methyl-P-thiocytidylyl-(3'→5')-2'-O-(2-methoxyethyl)-5-methyl-P-thiouridylyl-(3'→5')-2'-O-(2-methoxyethyl)-5-methyl-P-thiouridylyl-(3'→5')-2'-O-(2-methoxyethyl)-P-thioguanylyl-(3'→5')-2'-deoxy-P-thioguanylyl-(3'→5')-P-thiothymidylyl-(3'→5')-P-thiothymidylyl-(3'→5')-2'-deoxy-P-thioadenylyl-(3'→5')-2'-deoxy-5-methyl-P-thiocytidylyl-(3'→5')-2'-deoxy-P-thioadenylyl-(3'→5')-P-thiothymidylyl-(3'→5')-2'-deoxy-P-thioguanylyl-(3'→5')-2'-deoxy-P-thioadenylyl-(3'→5')-2'-deoxy-P-thioadenylyl-(3'→5')-2'-O-(2-methoxyethyl)-P-thioadenylyl-(3'→5')-2'-O-(2-methoxyethyl)-5-methyl-P-thiouridylyl-(3'→5')-2'-O-(2-methoxyethyl)-5-methyl-P-thiocytidylyl-(3'→5')-2'-O-(2-methoxyethyl)-5-methyl-P-thiocytidylyl-(3'→5')-2'-O-(2-methoxyethyl)-5-methylcytidine
inotersen tout-P-ambo-2'-O-(2-méthoxyéthyl)-5-méthyl-P-thiouridylyl-(3'→5')-2'-O-(2-méthoxyéthyl)-5-méthyl-P-thiocytidylyl-(3'→5')-2'-O-(2-méthoxyéthyl)-5-méthyl-P-thiouridylyl-(3'→5')-2'-O-(2-méthoxyéthyl)-5-méthyl-P-thiouridylyl-(3'→5')-2'-O-(2-méthoxyéthyl)-P-thioguanylyl-(3'→5')-2'-déoxy-P-thioguanylyl-(3'→5')-P-thiothymidylyl-(3'→5')-P-thiothymidylyl-(3'→5')-2'-déoxy-P-thioadénylyl-(3'→5')-2'-déoxy-5-méthyl-P-thiocytidylyl-(3'→5')-2'-déoxy-P-thioadénylyl-(3'→5')-P-thiothymidylyl-(3'→5')-2'-déoxy-P-thioguanylyl-(3'→5')-2'-déoxy-P-thioadénylyl-(3'→5')-2'-déoxy-P-thioadénylyl-(3'→5')-2'-O-(2-méthoxyéthyl)-P-thioadénylyl-(3'→5')-2'-O-(2-méthoxyéthyl)-5-méthyl-P-thiouridylyl-(3'→5')-2'-O-(2-méthoxyéthyl)-5-méthyl-P-thiocytidylyl-(3'→5')-2'-O-(2-méthoxyéthyl)-5-méthyl-P-thiocytidylyl-(3'→5')-2'-O-(2-méthoxyéthyl)-5-méthylcytidine
inotersén todo-P-ambo-5-metil-2'-O-(2-metoxietil)-P-tiouridilil-(3'→5')-5-metil-2'-O-(2-metoxietil)-P-tiocitidilil-(3'→5')-5-metil-2'-O-(2-metoxietil)-P-tiouridilil-(3'→5')-5-metil-2'-O-(2-metoxietil)-P-tiouridilil-(3'→5')-2'-O-(2-metoxietil)-P-tioguanilil-(3'→5')-2'-desoxi-P-tioguanilil-(3'→5')-P-tiotimidilil-(3'→5')-P-tiotimidilil-(3'→5')-2'-desoxi-P-tioadenilil-(3'→5')-2'-desoxi-5-metil-P-tiocitidilil-(3'→5')-2'-desoxi-P-tioadenilil-(3'→5')-P-tiotimidilil-(3'→5')-2'-desoxi-P-tioguanilil-(3'→5')-2'-desoxi-P-tioadenilil-(3'→5')-2'-desoxi-P-tioadenilil-(3'→5')-2'-O-(2-metoxietil)-P-tioadenilil-(3'→5')-5-metil-2'-O-(2-metoxietil)-P-tiouridilil-(3'→5')-5-metil-2'-O-(2-metoxietil)-P-tiocitidilil-(3'→5')-5-metil-2'-O-(2-metoxietil)-P-tiocitidilil-(3'→5')-2'-O-(2-metoxietil)-5-metilcitidina
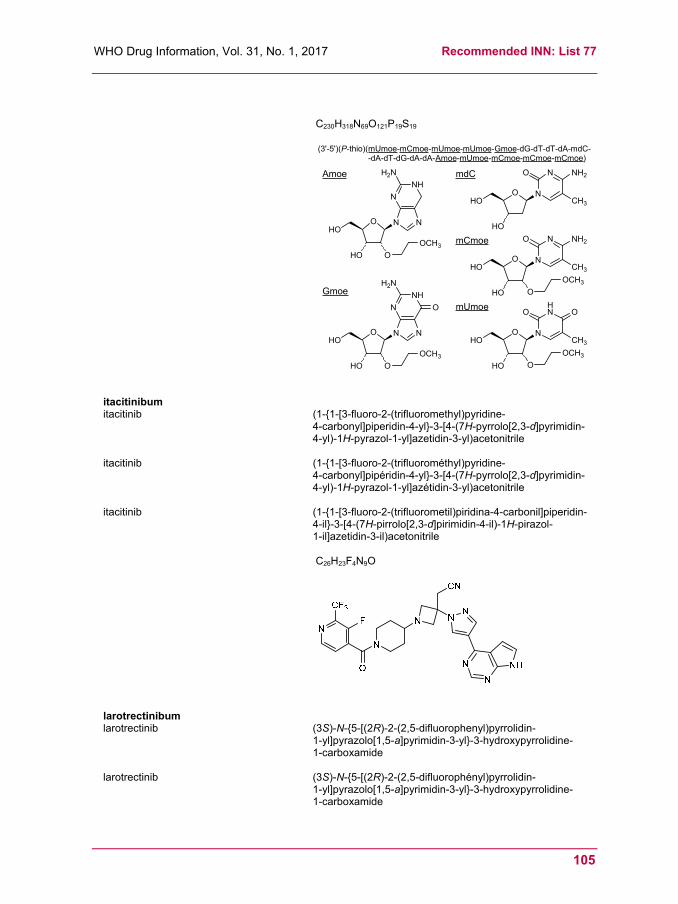
WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
105
C230H318N69O121P19S19
O
HO O
N N
NH
N O
H2N
OCH3
Gmoe
mUmoe
N
NO NH2
O
HO
CH3
N
HNO O
O
HO
CH3
mdC
(3'-5')(P-thio)(mUmoe-mCmoe-mUmoe-mUmoe-Gmoe-dG-dT-dT-dA-mdC--dA-dT-dG-dA-dA-Amoe-mUmoe-mCmoe-mCmoe-mCmoe)
O
OCH3
O
HO O
N N
NH
N
H2N
OCH3
Amoe
N
NO NH2
O
HO
CH3
mCmoe
O
OCH3
HO
HO
HO
HO
HO
itacitinibum itacitinib (1-{1-[3-fluoro-2-(trifluoromethyl)pyridine-
4-carbonyl]piperidin-4-yl}-3-[4-(7H-pyrrolo[2,3-d]pyrimidin-4-yl)-1H-pyrazol-1-yl]azetidin-3-yl)acetonitrile
itacitinib (1-{1-[3-fluoro-2-(trifluorométhyl)pyridine- 4-carbonyl]pipéridin-4-yl}-3-[4-(7H-pyrrolo[2,3-d]pyrimidin-4-yl)-1H-pyrazol-1-yl]azétidin-3-yl)acetonitrile
itacitinib (1-{1-[3-fluoro-2-(trifluorometil)piridina-4-carbonil]piperidin-4-il}-3-[4-(7H-pirrolo[2,3-d]pirimidin-4-il)-1H-pirazol- 1-il]azetidin-3-il)acetonitrile
C26H23F4N9O
larotrectinibum larotrectinib (3S)-N-{5-[(2R)-2-(2,5-difluorophenyl)pyrrolidin-
1-yl]pyrazolo[1,5-a]pyrimidin-3-yl}-3-hydroxypyrrolidine- 1-carboxamide
larotrectinib (3S)-N-{5-[(2R)-2-(2,5-difluorophényl)pyrrolidin- 1-yl]pyrazolo[1,5-a]pyrimidin-3-yl}-3-hydroxypyrrolidine- 1-carboxamide
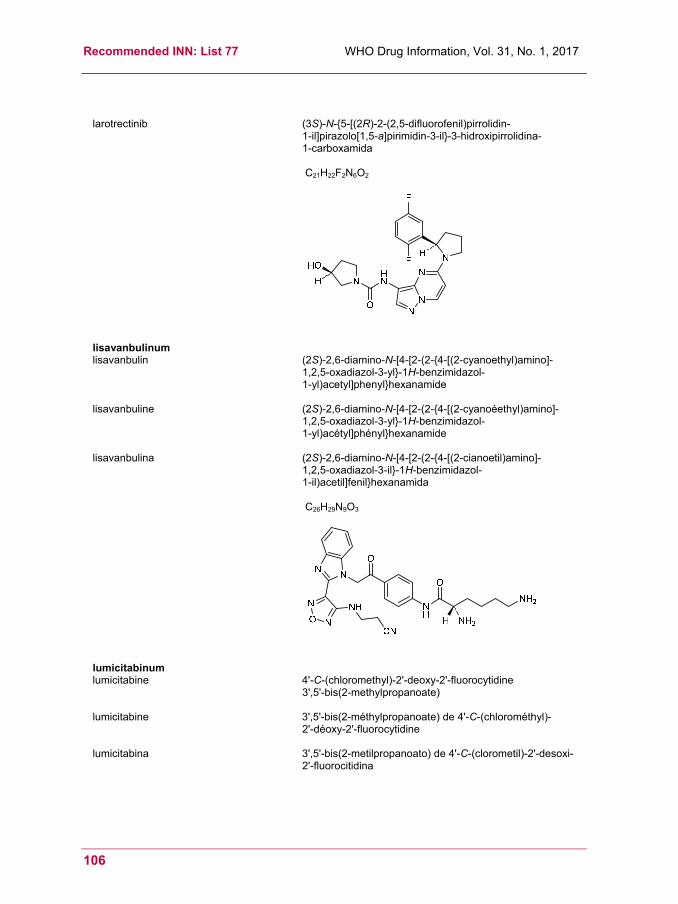
Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
106
larotrectinib (3S)-N-{5-[(2R)-2-(2,5-difluorofenil)pirrolidin- 1-il]pirazolo[1,5-a]pirimidin-3-il}-3-hidroxipirrolidina- 1-carboxamida
C21H22F2N6O2
lisavanbulinum lisavanbulin (2S)-2,6-diamino-N-[4-[2-(2-{4-[(2-cyanoethyl)amino]-
1,2,5-oxadiazol-3-yl}-1H-benzimidazol- 1-yl)acetyl]phenyl}hexanamide
lisavanbuline (2S)-2,6-diamino-N-[4-[2-(2-{4-[(2-cyanoéethyl)amino]-1,2,5-oxadiazol-3-yl}-1H-benzimidazol- 1-yl)acétyl]phényl}hexanamide
lisavanbulina (2S)-2,6-diamino-N-[4-[2-(2-{4-[(2-cianoetil)amino]- 1,2,5-oxadiazol-3-il}-1H-benzimidazol- 1-il)acetil]fenil}hexanamida
C26H29N9O3
lumicitabinum lumicitabine 4'-C-(chloromethyl)-2'-deoxy-2'-fluorocytidine
3',5'-bis(2-methylpropanoate)
lumicitabine 3',5'-bis(2-méthylpropanoate) de 4'-C-(chlorométhyl)- 2'-déoxy-2'-fluorocytidine
lumicitabina 3',5'-bis(2-metilpropanoato) de 4'-C-(clorometil)-2'-desoxi-2'-fluorocitidina
WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
107
C18H25ClFN3O6
lupartumabum # lupartumab immunoglobulin G1-lambda1, anti-[Homo sapiens LYPD3
(Ly6/PLAUR domain containing 3, GPI-anchored cell-surface protein C4.4a, C4.4A)], Homo sapiens monoclonal antibody; gamma1 heavy chain (1-446) [Homo sapiens VH (IGHV3-48*03 (92.90%) -(IGHD) -IGHJ4*01) [8.8.10](1-117) -IGHG1*01, Gm17,1 (CH1 (118-215), hinge (216-230), CH2 (231-340), CH3 (341-445), CHS K>del (446)) (118-446)], (220-216')-disulfide with lambda1 light chain (1'-217') [Homo sapiens V-LAMBDA (IGLV1-47*01 (87.90%) -IGLJ2*01) [9.3.11] (1'-111') -IGLC2*01 (112'-217')]; dimer (226-226'':229-229'')-bisdisulfide
lupartumab immunoglobuline G1-lambda1, anti-[Homo sapiens LYPD3 (protéine 3 contenant un domaine Ly6/PLAUR, protéine C4.4a GPI-ancrée à la surface cellulaire, C4.4A)], Homo sapiens anticorps monoclonal; chaîne lourde gamma1 (1-446) [Homo sapiens VH (IGHV3-48*03 (92.90%) -(IGHD) -IGHJ4*01) [8.8.10](1-117) -IGHG1*01, Gm17,1 (CH1 (118-215), charnière (216-230), CH2 (231-340), CH3 (341-445), CHS K>del (446)) (118-446)], (220-216')-disulfure avec la chaîne légère lambda1 (1'-217') [Homo sapiens V-LAMBDA (IGLV1-47*01 (87.90%) -IGLJ2*01) [9.3.11] (1'-111') -IGLC2*01 (112'-217')]; dimère (226-226'':229-229'')-bisdisulfure
lupartumab inmunoglobulina G1-lambda1, anti-[Homo sapiens LYPD3 (proteína 3 que contiene un dominio Ly6/PLAUR, proteína C4.4a GPI-anclada en la superficie celular, C4.4A)], Homo sapiens anticuerpo monoclonal; cadena pesada gamma1 (1-446) [Homo sapiens VH (IGHV3-48*03 (92.90%) -(IGHD) -IGHJ4*01) [8.8.10](1-117) -IGHG1*01, Gm17,1 (CH1 (118-215), bisagra (216-230), CH2 (231-340), CH3 (341-445), CHS K>del (446)) (118-446)], (220-216')-disulfuro con la cadena ligera lambda1 (1'-217') [Homo sapiens V-LAMBDA (IGLV1-47*01 (87.90%) -IGLJ2*01) [9.3.11] (1'-111') -IGLC2*01 (112'-217')]; dímero (226-226'':229-229'')-bisdisulfuro

Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
108
lupartumabum amadotinum # lupartumab amadotin immunoglobulin G1-lambda1, anti-[Homo sapiens LYPD3
(Ly6/PLAUR domain containing 3, GPI-anchored cell-surface protein C4.4a, C4.4A)], Homo sapiens monoclonal antibody conjugated to an auristatin W derivative; gamma1 heavy chain (1-446) [Homo sapiens VH (IGHV3-48*03 (92.90%) -(IGHD) -IGHJ4*01) [8.8.10](1-117) -IGHG1*01, Gm17,1 (CH1 (118-215), hinge (216-230), CH2 (231-340), CH3 (341-445), CHS K>del (446)) (118-446)], (220-216')-disulfide with lambda1 light chain (1'-217') [Homo sapiens V-LAMBDA (IGLV1-47*01 (87.90%) -IGLJ2*01) [9.3.11] (1'-111') -IGLC2*01 (112'-217')]; dimer (226-226'':229-229'')-bisdisulfide; S-substituted on an average of 4 reduced cysteinyl by reaction with N-demethyl-N-[4-(6-maleimidohexanohydrazido)- 4-oxobutyl]auristatin W amide
lupartumab amadotine immunoglobuline G1-lambda1, anti-[Homo sapiens LYPD3 (protéine 3 contenant un domaine Ly6/PLAUR, protéine C4.4a GPI-ancrée à la surface cellulaire, C4.4A)], Homo sapiens anticorps monoclonal conjugué à un dérivé de l'auristatine W; chaîne lourde gamma1 (1-446) [Homo sapiens VH (IGHV3-48*03 (92.90%) -(IGHD) -IGHJ4*01) [8.8.10](1-117) -IGHG1*01, Gm17,1 (CH1 (118-215), charnière (216-230), CH2 (231-340), CH3 (341-445), CHS K>del (446)) (118-446)], (220-216')-disulfure avec la chaîne légère lambda1 (1'-217') [Homo sapiens V-LAMBDA (IGLV1-47*01 (87.90%) -IGLJ2*01) [9.3.11] (1'-111') -IGLC2*01 (112'-217')]; dimère (226-226'':229-229'')-bisdisulfure; S-substitué, sur 4 cystéines réduits en moyenne, par reaction avec N-desméthyl-N-[4-(6-maléimidohexanohy-drazido)-4-oxobutyl]auristatine W amide

WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
109
lupartumab amadotina
inmunoglobulina G1-lambda1, anti-[Homo sapiens LYPD3 (proteína 3 que contiene un dominio Ly6/PLAUR, proteína C4.4a GPI-anclada a la superficie celular, C4.4A)], Homo sapiens anticuerpo monoclonal conjugado con un derivado de la auristatina W; cadena pesada gamma1 (1-446) [Homo sapiens VH (IGHV3-48*03 (92.90%) -(IGHD) -IGHJ4*01) [8.8.10](1-117) -IGHG1*01, Gm17,1 (CH1 (118-215), bisagra (216-230), CH2 (231-340), CH3 (341-445), CHS K>del (446)) (118-446)], (220-216')-disulfuro con la cadena ligera lambda1 (1'-217') [Homo sapiens V-LAMBDA (IGLV1-47*01 (87.90%) -IGLJ2*01) [9.3.11] (1'-111') -IGLC2*01 (112'-217')]; dímero (226-226'':229-229'')-bisdisulfuro; S-sustituido, en 4 grupos cisteinil reducidos por término medio, por reacción con N-desmetil-N-[4-(6-maleimidohexanohidrazido)-4-oxobutil]auristatina W amida

Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
110
lutikizumabum # lutikizumab immunoglobulin G1-kappa, anti-[Homo sapiens IL1A
(interleukin 1 alpha) and Homo sapiens IL1B (interleukin 1 beta, IL-1B, 1L1F2)], humanized monoclonal antibody, tetravalent bispecific; gamma1 heavy chain (1-577) [humanized VH anti-IL1B (Homo sapiens IGHV3-23*04 (80.60%) -(IGHD)-IGHJ4*01) [8.8.12] (1-119) -6-mer linker (120-125) -Homo sapiens VH anti-IL1A (IGHV3-30*03 (88.80%) -(IGHD)-IGHJ1*01) [8.8.15] (126-247) -Homo sapiens IGHG1*01 (CH1 (248-345), hinge (346-360), CH2 L1.3>A (364), L1.2>A (365), (361-470), CH3 (471-575), CHS (576-577)) (248-577)], (350-327')-disulfide with kappa light chain (1'-327') [humanized V-KAPPA anti-IL1B (Homo sapiens IGKV1-27*01 (82.10%) -IGKJ2*01) [6.3.9] (1'-106') -7-mer linker -Homo sapiens V-KAPPA anti-IL1A (IGKV1-12*01 (92.60%) -IGKJ4*01) [6.3.9] (114'-220') -Homo sapiens IGKC*01, Km3 (221'-327')]; dimer (356-356":359-359")-bisdisulfide
lutikizumab immunoglobuline G1-kappa, anti-[Homo sapiens IL1A (interleukine 1 alpha) et Homo sapiens IL1B (interleukine 1 bêta, IL-1B, 1L1F2)], anticorps monoclonal humanisé, tétravalent bispécifique; chaîne lourde gamma1 chaîne (1-577) [VH humanisé anti-IL1B (Homo sapiens IGHV3-23*04 (80.60%) -(IGHD)-IGHJ4*01) [8.8.12] (1-119) -6-mer linker (120-125) -Homo sapiens VH anti-IL1A (IGHV3-30*03 (88.80%) -(IGHD)-IGHJ1*01) [8.8.15] (126-247)-Homo sapiens IGHG1*01 (CH1 (248-345), charnière (346-360), CH2 L1.3>A (364), L1.2>A (365), (361-470), CH3 (471-575), CHS (576-577)) (248-577)], (350-327')-disulfure avec la chaîne légère (1'-327') [V-KAPPA humanisé anti-IL1B (Homo sapiens IGKV1-27*01 (82.10%) -IGKJ2*01) [6.3.9] (1'-106') -7-mer linker -Homo sapiens V-KAPPA anti-IL1A (IGKV1-12*01 (92.60%) -IGKJ4*01) [6.3.9] (114'-220') -Homo sapiens IGKC*01, Km3 (221'-327')]; dimère (356-356":359-359")-bisdisulfure
lutikizumab immunoglobulina G1-kappa, anti-[Homo sapiens IL1A (interleukina 1 alfa) y Homo sapiens IL1B (interleukina 1 beta, IL-1B, 1L1F2)], anticuerpo monoclonal humanizado, tetravalente biespecífico; cadena pesada gamma1 cadena (1-577) [VH humanizado anti-IL1B (Homo sapiens IGHV3-23*04 (80.60%) -(IGHD)-IGHJ4*01) [8.8.12] (1-119) -linker 6-mer (120-125) -Homo sapiens VH anti-IL1A (IGHV3-30*03 (88.80%) -(IGHD)-IGHJ1*01) [8.8.15] (126-247)-Homo sapiens IGHG1*01 (CH1 (248-345), bisagra (346-360), CH2 L1.3>A (364), L1.2>A (365), (361-470), CH3 (471-575), CHS (576-577)) (248-577)], (350-327')-disulfuro con la cadena ligera (1'-327') [V-KAPPA humanizado anti-IL1B (Homo sapiens IGKV1-27*01 (82.10%) -IGKJ2*01) [6.3.9] (1'-106') linker 7-mer -Homo sapiens V-KAPPA anti-IL1A (IGKV1-12*01 (92.60%) -IGKJ4*01) [6.3.9] (114'-220') -Homo sapiens IGKC*01, Km3 (221'-327')]; dímero (356-356":359-359")-bisdisulfuro
WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
111
miridesapum miridesap 1,1'-hexanedioyldi-D-proline
miridésap 1,1'-hexanedioyldi-D-proline
miridesap 1,1'-hexanodioildi-D-prolina
C16H24N2O6
mivebresibum mivebresib N-[4-(2,4-difluorophenoxy)-3-(6-methyl-7-oxo-6,7-dihydro-
1H-pyrrolo[2,3-c]pyridin-4-yl)phenyl]ethanesulfonamide
mivébrésib N-[4-(2,4-difluorophénoxy)-3-(6-méthyl-7-oxo-6,7-dihydro-1H-pyrrolo[2,3-c]pyridin-4-yl)phényl]éthanesulfonamide
mivebresib N-[4-(2,4-difluorofenoxi)-3-(6-metil-7-oxo-6,7-dihidro- 1H-pirrolo[2,3-c]piridin-4-il)fenil]etanosulfonamida

Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
112
C22H19F2N3O4S
N
O
F
F
NH
O
CH3
HN
S CH3
O O
nacubactamum nacubactam (1R,2S,5R)-2-[(2-aminoethoxy)carbamoyl]-7-oxo-
1,6-diazabicyclo[3.2.1]octan-6-yl hydrogen sulfate
nacubactam hydrogénosulfate de (1R,2S,5R)-2-[(2-aminoéthoxy) carbamoyl]-7-oxo-1,6-diazabicyclo[3.2.1]octan-6-yle
nacubactam hidrogenosulfato de (1R,2S,5R)-2-[(2-aminoetoxi) carbamoil]-7-oxo-1,6-diazabiciclo[3.2.1]octan-6-ilo
C9H16N4O7S
naquotinibum naquotinib 6-ethyl-3-{4-[4-(4-methylpiperazin-1-yl)piperidin-
1-yl]anilino}-5-{[(3R)-1-(prop-2-enoyl)pyrrolidin- 3-yl]oxy}pyrazine-2-carboxamide
naquotinib 6-éthyl-3-{4-[4-(4-méthylpipérazin-1-yl)pipéridin- 1-yl]anilino}-5-{[(3R)-1-(prop-2-énoyl)pyrrolidin- 3-yl]oxy}pyrazine-2-carboxamide
naquotinib 6-etil-3-{4-[4-(4-metilpiperazin-1-il)piperidin-1-il]anilino}- 5-{[(3R)-1-(prop-2-enoil)pirrolidin-3-il]oxi}pirazina- 2-carboxamida
C30H42N8O3

WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
113
navoximodum navoximod trans-4-{(1R)-2-[(5S)-6-fluoro-5H-imidazo[5,1-a]isoindol-
5-yl]-1-hydroxyethyl}cyclohexan-1-ol
navoximod trans-4-{(1R)-2-[(5S)-6-fluoro-5H-imidazo[5,1-a]isoindol- 5-yl]-1-hydroxyéthyl}cyclohexan-1-ol
navoximod trans-4-{(1R)-2-[(5S)-6-fluoro-5H-imidazo[5,1-a]isoindol- 5-il]-1-hidroxietil}ciclohexan-1-ol
C18H21FN2O2
nelatimotidum nelatimotide L-cysteinyl[human Wilms tumor protein (WT33)-(126-134)-
peptide] (1-10) and [236-L-tyrosine(M>Y)]human Wilms tumor protein (WT33)-(235-243)-peptide (1'-9'), (1-1')-disulfide
nélatimotide (1-1')-disulfure entre le L-cystéinyl-[protéine tumorale de Wilms humaine (WT33)-(126-133)-peptide] (1-10) et le [236-L-tyrosine(M>Y)]protéine tumorale de Wilms humaine (WT33)-(235-243)-peptide (1'-9')
nelatimotida (1-1')-disulfuro entre la L-cisteinil[proteína tumoral de Wilms humana (WT33)-(126-134)-péptido] (1-10) y la [236-L-tirosina(M>Y)]proteína tumoral de Wilms humana (WT33)-(235-243)-péptido (1'-9')
C106H153N27O28S4
nirogacestatum nirogacestat (2S)-2-{[(2S)-6,8-difluoro-1,2,3,4-tetrahydronaphthalen-
2-yl]amino}-N-(1-{1-[(2,2-dimethylpropyl)amino]- 2-methylpropan-2-yl}-1H-imidazol-4-yl)pentanamide
nirogacéstat (2S)-2-{[(2S)-6,8-difluoro-1,2,3,4-tétrahydronaphtalén- 2-yl]amino}-N-(1-{1-[(2,2-diméthylpropyl)amino]- 2-méthylpropan-2-yl}-1H-imidazol-4-yl)pentanamide
nirogacestat (2S)-2-{[(2S)-6,8-difluoro-1,2,3,4-tetrahidronaftalen- 2-il]amino}-N-(1-{1-[(2,2-dimetilpropil)amino]- 2-metilpropan-2-il}-1H-imidazol-4-il)pentanamida
Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
114
C27H41F2N5O
obicetrapibum obicetrapib 4-{[2-({[3,5-bis(trifluoromethyl)phenyl]methyl}[(2R,4S)-
1-(ethoxycarbonyl)-2-ethyl-6-(trifluoromethyl)- 1,2,3,4-tetrahydroquinolin-4-yl]amino)pyrimidin- 5-yl]oxy}butanoic acid
obicétrapib acide 4-{[2-({[3,5-bis(trifluorométhyl)phényl]méthyl}[(2R,4S)- 1-(éthoxycarbonyl)-2-éthyl-6-(trifluorométhyl)- 1,2,3,4-tétrahydroquinoléin-4-yl]amino)pyrimidin- 5-yl]oxy}butanoïque
obicetrapib ácido 4-{[2-({[3,5-bis(trifluorometil)fenil]metil}[(2R,4S)- 2-etil-1-(etoxicarbonil)-6-(trifluorometil)- 1,2,3,4-tetrahidroquinolein-4-il]amino)pirimidin- 5-il]oxi}butanoico
C32H31F9N4O5
ofranergenum obadenovecum # ofranergene obadenovec A recombinant non-replicating adenovirus type 5 vector
carrying a fas-chimera transgene consisting of fas and human tumour necrosis factor receptor 1 (TNFR1), under transcriptional control of a murine pre-proendothelin promoter (PPE-1-3X*) *PPE-1-3X = modified PPE-1 promoter that contains three copies of the endothelial cells (EC)-positive regulatory elements.
ofranergéne obadénovec vecteur adenoviral 5 recombinant sans capacité de réplication, contenant un transgène chimérique-fas constitué du fas et du récepteur 1 du facteur de nécrose tumorale humain (TNFR1), sous le contrôle transcriptionnel d'un promoteur pré-pro-endothéline murin (PPE-1-3X*) *PPE-1-3X = promoteur pré-pro-endothéline modifié contenant trois copies d'éléments de régulation positive provenant des cellules endothéliales
WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
115
ofranergén obadenovec vector adenoviral 5 recombinante no replicante, que contiene un transgec quimérico-fas constituido del fas y del receptor 1 del factor de necrosis tumoral humano (TNFR1), bajo el control transcripcional de un promotor pre-pro-endotelina murino (PPE-1-3X*) *PPE-1-3X = promotor pre-pro-endotelina modificado que contiene tres copias de elementos de regulación positiva que proviene de las células endoteliales
padsevonilum padsevonil (4R)-4-(2-chloro-2,2-difluoroethyl)-1-{[2-(methoxymethyl)-
6-(trifluoromethyl)imidazo[2,1-b][1,3,4]thiadiazol- 5-yl]methyl}pyrrolidin-2-one
padsévonil (4R)-4-(2-chloro-2,2-difluoroéthyl)-1-{[2-(méthoxyméthyl)-6-(trifluorométhyl)imidazo[2,1-b][1,3,4]thiadiazol- 5-yl]méthyl}pyrrolidin-2-one
padsevonil (4R)-4-(2-cloro-2,2-difluoroetil)-1-{[2-(metoximetil)- 6-(trifluorometil)imidazo[2,1-b][1,3,4]tiadiazol- 5-il]metil}pirrolidin-2-ona
C14H14ClF5N4O2S
palucorcelum palucorcel allogeneic human umbilical tissue derived cells (hUTC)
obtained by enzymatic digestion of post-partum blood-free umbilical cord tissue and ex vivo expansion. Cells secrete trophic factors and do not express markers of endothelial cells (CD31), cord blood cells (CD45), epithelial cells (E-cadherin) and fibroblasts (FSP-1).
palucorcel cellules humaines allogéniques dérivées de tissu ombilical (hUTC) obtenues par réactions enzymatiques de tissu de cordon ombilical post-partum exsangue et par expansion ex vivo. Les cellules secrètent des facteurs trophiques et n'expriment pas les marqueurs des cellules endothéliales (CD31), des cellules sanguines du cordon (CD45), des célulles épithéliales (cadhérine E) ni des fibroblastes (FSP-1).
palucorcel células humanas alogénicas derivadas de tejido umbilical (hUTC) obtenidas por reacciones enzimáticas de tejido de cordón umbilical posparto libre de sangre y por expansión ex vivo. Las células secretan los factores tróficos y no expresan los marcadores de las células endoteliales (CD31), las células sanguíneas del cordón (CD45), las células epiteliales (cadherina E) y los fibroblastos (FSP-1).
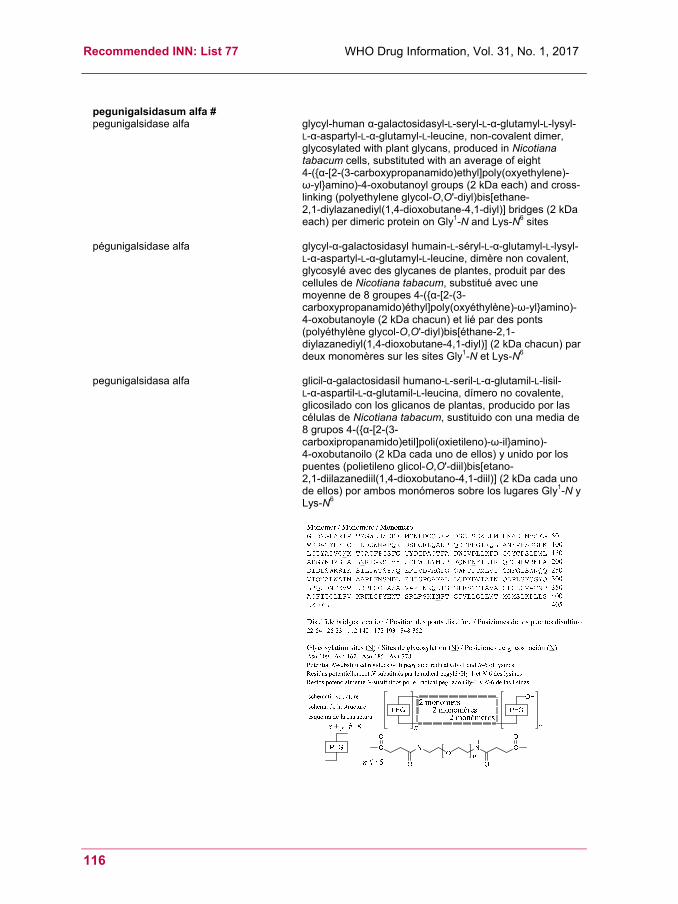
Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
116
pegunigalsidasum alfa # pegunigalsidase alfa glycyl-human α-galactosidasyl-L-seryl-L-α-glutamyl-L-lysyl-
L-α-aspartyl-L-α-glutamyl-L-leucine, non-covalent dimer, glycosylated with plant glycans, produced in Nicotiana tabacum cells, substituted with an average of eight 4-({α-[2-(3-carboxypropanamido)ethyl]poly(oxyethylene)- ω-yl}amino)-4-oxobutanoyl groups (2 kDa each) and cross-linking (polyethylene glycol-O,O'-diyl)bis[ethane- 2,1-diylazanediyl(1,4-dioxobutane-4,1-diyl)] bridges (2 kDa each) per dimeric protein on Gly1-N and Lys-N6 sites
pégunigalsidase alfa glycyl-α-galactosidasyl humain-L-séryl-L-α-glutamyl-L-lysyl-L-α-aspartyl-L-α-glutamyl-L-leucine, dimère non covalent, glycosylé avec des glycanes de plantes, produit par des cellules de Nicotiana tabacum, substitué avec une moyenne de 8 groupes 4-({α-[2-(3-carboxypropanamido)éthyl]poly(oxyéthylène)-ω-yl}amino)-4-oxobutanoyle (2 kDa chacun) et lié par des ponts (polyéthylène glycol-O,O'-diyl)bis[éthane-2,1-diylazanediyl(1,4-dioxobutane-4,1-diyl)] (2 kDa chacun) par deux monomères sur les sites Gly1-N et Lys-N6
pegunigalsidasa alfa glicil-α-galactosidasil humano-L-seril-L-α-glutamil-L-lisil-
L-α-aspartil-L-α-glutamil-L-leucina, dímero no covalente, glicosilado con los glicanos de plantas, producido por las células de Nicotiana tabacum, sustituido con una media de 8 grupos 4-({α-[2-(3-carboxipropanamido)etil]poli(oxietileno)-ω-il}amino)- 4-oxobutanoilo (2 kDa cada uno de ellos) y unido por los puentes (polietileno glicol-O,O'-diil)bis[etano- 2,1-diilazanediil(1,4-dioxobutano-4,1-diil)] (2 kDa cada uno de ellos) por ambos monómeros sobre los lugares Gly1-N y Lys-N6

WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
117
pegvorhyaluronidasum alfa # pegvorhyaluronidase alfa human hyaluronidase PH-20 (hyaluronoglucosaminidase
PH-20, sperm adhesion molecule 1, EC 3.2.1.35) precursor-(36-482)-peptide (mature (1-447)-peptide), produced in Chinese hamster ovary (CHO) cells, glycoform alfa, substituted on N6 of an average of 4 to 5 lysyl residues with 4-[ω-methoxypoly(oxyethylene)-α-yl]butanoyl groups (~30 kDa each)
pègvorhyaluronidase alfa hyaluronidase PH-20 humaine (hyaluronoglucosaminidase PH-20, molécule adhésive 1 du sperme, EC 3.2.1.35) précurseur-(36-482)-peptide (à maturité-(1-447)-peptide), produite par des cellules ovariennes de hamster chinois (CHO), forme glycosylée alfa, substituée sur les N6 de 4 à 5 résidus lysyl en moyenne par des groupes 4-[ω-méthoxypoly(oxyéthylène)-α-yl]butanoyle (~30 kDa chacun)
pegvorhialuronidasa alfa hialuronidasa PH-20 humana (hialuronoglucosaminidasa PH-20, molécula de adhesión 1 de esperma, EC 3.2.1.35) precursor-(36-482)-péptido (maduro-(1-447)-péptido), producida por células ováricas de hamster chino (CHO), forma glicosilada alfa, sustituída en N6 de 4 a 5 restos lysyl pro termino medio por grupos 4-[ω-metoxipoli(oxietileno)-α-il]butanoilo (~ 30 kDa cada uno)
pimodivirum pimodivir (2S,3S)-3-{[5-fluoro-2-(5-fluoro-1H-pyrrolo[2,3-b]pyridin-
3-yl)pyrimidin-4-yl]amino}bicyclo[2.2.2]octane-2-carboxylic acid
pimodivir acide (2S,3S)-3-{[5-fluoro-2-(5-fluoro-1H-pyrrolo[2,3-b]pyridin-3-yl)pyrimidin-4-yl]amino}bicyclo[2.2.2]octane- 2-carboxylique
pimodivir ácido (2S,3S)-3-{[5-fluoro-2-(5-fluoro-1H-pirrolo[2,3-b]piridin-3-il)pirimidin-4-il]amino}biciclo[2.2.2]octano- 2-carboxílico

Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
118
C20H19F2N5O2
poseltinibum poseltinib N-[3-({2-[4-(4-methylpiperazin-1-yl)anilino]furo[3,2-
d]pyrimidin-4-yl}oxy)phenyl]prop-2-enamide
poseltinib N-[3-({2-[4-(4-méthylpipérazin-1-yl)anilino]furo[3,2-d]pyrimidin-4-yl}oxy)phényl]prop-2-énamide
poseltinib N-[3-({2-[4-(4-metilpiperazin-1-il)anilino]furo[3,2-d]pirimidin-4-il}oxi)fenil]prop-2-enamida
C26H26N6O3
ranevetmabum # ranevetmab immunoglobulin G1-kappa, anti-[Mus musculus NGF
(nerve growth factor, nerve growth factor beta polypeptide, NGFB, beta-NGF)], caninized monoclonal antibody; gamma1 heavy chain (1-453) [caninizedVH (Rattus norvegicus IGHV5S13*01 (71.40%) -(IGHD)-IGHJ4*01) [8.7.16] (1-122) -Canis lupus familiaris IGHG1*01 (CH1 (123-219), hinge (220-233), CH2 (234-343), CH3 (344-451), CHS (452-453)) (123-453)], (137-213')-disulfide with kappa light chain (1'-217') [caninizedV-KAPPA (Rattus norvegicus IGKV12S34*01 (76.80%) -IGKJ2-3*01) [6.3.9] (1'-107') -Canis lupus familiaris IGKC*01 (108'-213') -4-mer (214'-217')]; dimer (224-224'':226-226'':232-232'')-trisdisulfide
ranévetmab immunoglobuline G2-kappa, anti-[Mus musculus NGF (facteur de croissance du nerf, facteur de croissance du nerf polypeptide bêta, NGFB, bêta-NGF)], anticorps monoclonal caninisé; chaîne lourde gamma2 (1-453) [VH caninisé (Rattus norvegicus IGHV5S13*01 (71.40%) -(IGHD)-IGHJ4*01) [8.7.16] (1-122) -Canis lupus familiaris IGHG1*01 (CH1 (123-219), charnière (220-233), CH2 (234-343), CH3 (344-451), CHS (452-453)) (123-453)], (137-213')-disulfure avec la chaîne légèrekappa (1'-217') [V-KAPPA caninisé (Rattus norvegicus IGKV12S34*01 (76.80%) -IGKJ2-3*01) [6.3.9] (1'-107') -Canis lupus familiaris IGKC*01 (108'-213') -4-mer (214'-217')]; dimère (224-224'':226-226'':232-232'')-trisdisulfure
WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
119
ranevetmab inmunoglobulina G2-kappa, anti-[Mus musculus NGF (factor de crecimiento de los nervios, factor de crecimiento de nervios polipéptido beta, NGFB, beta-NGF)], anticuerpo monoclonal caninizado; cadena pesada gamma2 (1-453) [VH caninizado (Rattus norvegicus IGHV5S13*01 (71.40%) -(IGHD)-IGHJ4*01) [8.7.16] (1-122) -Canis lupus familiaris IGHG1*01 (CH1 (123-219), bisagra (220-233), CH2 (234-343), CH3 (344-451), CHS (452-453)) (123-453)], (137-213')-disulfuro con la cadena ligerakappa (1'-217') [V-KAPPA caninizado (Rattus norvegicus IGKV12S34*01 (76.80%) -IGKJ2-3*01) [6.3.9] (1'-107') -Canis lupus familiaris IGKC*01 (108'-213') -4-mer (214'-217')]; dímero (224-224'':226-226'':232-232'')-trisdisulfuro
ravoxertinibum ravoxertinib 1-[(1S)-1-(4-chloro-3-fluorophenyl)-2-hydroxyethyl]-
4-{2-[(1-methyl-1H-pyrazol-5-yl)amino]pyrimidin- 4-yl}pyridin-2(1H)-one
ravoxertinib 1-[(1S)-1-(4-chloro-3-fluorophényl)-2-hydroxyéthyl]- 4-{2-[(1-méthyl-1H-pyrazol-5-yl)amino]pyrimidin- 4-yl}pyridin-2(1H)-one
ravoxertinib 1-[(1S)-1-(4-cloro-3-fluorofenil)-2-hidroxietil]-4-{2-[(1-metil-1H-pirazol-5-il)amino]pirimidin-4-il}piridin-2(1H)-ona

Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
120
C21H18ClFN6O2
recanaclotidum recanaclotide S1,S6:S2,S10:S5,S13-tricyclo(L-cysteinyl-L-cysteinyl-
O-phosphono-L-seryl-L-leucyl-L-cysteinyl-L-cysteinyl- L-asparaginyl-L-prolyl-L-alanyl-L-cysteinyl-L-threonylglycyl-L-cysteine)
récanaclotide S1,S6:S2,S10:S5,S13-tricyclo(L-cystéinyl-L-cystéinyl- O-phosphono-L-séryl-L-leucyl-L-cystéinyl-L-cystéinyl- L-asparaginyl-L-prolyl-L-alanyl-L-cystéinyl-L-thréonylglycyl-L-cystéine)
recanaclotida S1,S6:S2,S10:S5,S13-triciclo(L-cisteinil-L-cisteinil-O-fosfono- L-seril-L-leucil-L-cisteinil-L-cisteinil-L-asparaginil-L-prolil- L-alanil-L-cisteinil-L-treonilglicil-L-cisteína)
C45H71N14O20PS6
reltecimodum reltecimod D-alanyl-[T-cell-specific surface glycoprotein CD28-(8-15)-
peptide]-D-alanine: D-alanyl-L-seryl-L-prolyl-L-methionyl-L-leucyl-L-valyl- L-alanyl-L-tyrosyl-L-α-aspartyl-D-alanine
reltécimod D-alanyl-[(8-15)-peptide de glycoprotéine de surface CD28 spécifique des cellules T]-D-alanine: D-alanyl-L-séryl-L-prolyl-L-méthionyl-L-leucyl-L-valyl- L-alanyl-L-tyrosyl-L-α-aspartyl-D-alanine
reltecimod D-alanil-[(8-15)-péptido de glicoproteína de superfice CD28 específica de las células T]-D-alanina: D-alanil-L-seril-L-prolil-L-metionil-L-leucil-L-valil-L-alanil- L-tirosil-L-α-aspartil-D-alanina
C46H72N10O15S
WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
121
remetinostatum remetinostat methyl 4-{[8-(hydroxyamino)-8-oxooctanoyl]oxy}benzoate
rémétinostat 4-{[8-(hydroxyamino)-8-oxooctanoyl]oxy}benzoate de
méthyle
remetinostat 4-{[8-(hidroxiamino)-8-oxooctanoil]oxi}benzoato de metilo
C16H21NO6
remtolumabum # remtolumab immunoglobulin G1-kappa, anti-[Homo sapiens IL17A
(interleukin 17A, IL-17A) and Homo sapiens TNF (tumor necrosis factor (TNF) superfamily member 2, TNFSF2, TNF-alpha, TNFA)], Homo sapiens monoclonal antibody, tetravalent bispecific; gamma1 heavy chain (1-587) [Homo sapiens VH anti-TNF (IGHV3-9*01 (93.90%) -(IGHD) -IGHJ4*01) [8.8.14] (1-121) -10-mer bis(tetraglycyl-seryl) linker (122-132) -Homo sapiens VH' anti-IL17A (IGHV1-69*01 (85.70%) -(IGHD) -IGHJ6*01) [8.8.19] (132-257) -IGHG1*01, G1m17,1 (CH1 (258-355), hinge (356-370), CH2 (371-480), CH3 (481-585), CHS (586-587)) (258-587)], (360-331')-disulfide with kappa light chain (1'-331') [Homo sapiens V-KAPPA anti-TNF (IGKV1-27*01 (95.80%) -IGKJ2*01) [6.3.9] (1'-107') -Homo sapiens V-KAPPA anti-IL17A (IGKV6-21*01 (90.50%) -IGKJ3*01) [6.3.9] (118'-224') -IGKC*01, Km3 (225'-213')]; dimer (366-366'':369-369'')-bisdisulfide
remtolumab immunoglobuline G1-kappa, anti-[Homo sapiens IL17A (interleukine 17A, IL-17A) et Homo sapiens TNF (facteur de nécrose tumorale membre 2 de la superfamille du TNF, TNFSF2, TNF-alpha, TNFA)], Homo sapiens anticorps monoclonal, tétravalent bispécifique; chaîne lourde gamma1 (1-587) [Homo sapiens VH anti-TNF (IGHV3-9*01 (93.90%) -(IGHD) -IGHJ4*01) [8.8.14] (1-121) -10-mer bis(tétraglycyl-séryl) linker (122-132) -Homo sapiens VH' anti-IL17A (IGHV1-69*01 (85.70%) -(IGHD) -IGHJ6*01) [8.8.19] (132-257) -IGHG1*01, G1m17,1 (CH1 (258-355), charnière (356-370), CH2 (371-480), CH3 (481-585), CHS (586-587)) (258-587)], (360-331')-disulfure avec la chaîne légère kappa (1'-331') [Homo sapiens V-KAPPA anti-TNF (IGKV1-27*01 (95.80%) -IGKJ2*01) [6.3.9] (1'-107') -Homo sapiens V-KAPPA anti-IL17A (IGKV6-21*01 (90.50%) -IGKJ3*01) [6.3.9] (118'-224') -IGKC*01, Km3 (225'-213')]; dimère (366-366'':369-369'')-bisdisulfure
remtolumab inmunoglobulina G1-kappa, anti-[Homo sapiens IL17A (interleukina 17A, IL-17A) y Homo sapiens TNF (factor de necrosis tumoral miembro 2 de la superfamilia del TNF, TNFSF2, TNF-alfa, TNFA)], Homo sapiens anticuerpo monoclonal, tetravalente biespecífico;
Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
122
cadena pesada gamma1 (1-587) [Homo sapiens VH anti-TNF (IGHV3-9*01 (93.90%) -(IGHD) -IGHJ4*01) [8.8.14] (1-121) -10-mer bis(tetraglicil-seril) linker (122-132) -Homo sapiens VH' anti-IL17A (IGHV1-69*01 (85.70%) -(IGHD) -IGHJ6*01) [8.8.19] (132-257) -IGHG1*01, G1m17,1 (CH1 (258-355), bisagra (356-370), CH2 (371-480), CH3 (481-585), CHS (586-587)) (258-587)], (360-331')-disulfuro con la cadena ligera kappa (1'-331') [Homo sapiens V-KAPPA anti-TNF (IGKV1-27*01 (95.80%) -IGKJ2*01) [6.3.9] (1'-107') -Homo sapiens V-KAPPA anti-IL17A (IGKV6-21*01 (90.50%) -IGKJ3*01) [6.3.9] (118'-224') -IGKC*01, Km3 (225'-213')]; dímero (366-366'':369-369'')-bisdisulfuro
rogaratinibum rogaratinib 4-{[4-amino-6-(methoxymethyl)-5-(7-methoxy-5-methyl-
1-benzothiophen-2-yl)pyrrolo[2,1-f][1,2,4]triazin- 7-yl]methyl}piperazin-2-one
rogaratinib 4-{[4-amino-6-(méthoxyméthyl)-5-(7-méthoxy-5-méthyl- 1-benzothiophén-2-yl)pyrrolo[2,1-f][1,2,4]triazin- 7-yl]méthyl}pipérazin-2-one
rogaratinib 4-{[4-amino-5-(5-metil-7-metoxi-1-benzotiofen-2-il)- 6-(metoximetil)pirrolo[2,1-f][1,2,4]triazin-7-il]metil}piperazin-2-ona

WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
123
C23H26N6O3S
rosiptorum rosiptor 7-amino-17-methylidene-6,7-seco-5α-androstane-3β,6-diol
rosiptor 7-amino-17-méthylidène-6,7-séco-5α-androstane-3β,6-diol
rosiptor 7-amino-17-metilideno-6,7-seco-5α-androstano-3β,6-diol
C20H35NO2
rosmantuzumabum # rosmantuzumab immunoglobulin G1-kappa, anti-[Homo sapiens RSPO3 (R-
spondin 3, thrombospondin type I (TSP1) domain containing protein 2, THSD2)], humanized monoclonal antibody; gamma1 heavy chain (1-447) [humanized VH (Homo sapiens IGHV1-46*01 (84.50%) -(IGHD)-IGHJ4*01) [8.8.10] (1-117) -Homo sapiens IGHG1*03, (CH1 (118-215), hinge (216-230), CH2 (231-340), CH3 (341-445), CHS (446-447)) (118-447)], (220-218')-disulfide with kappa light chain (1'-218') [humanized V-KAPPA (Homo sapiens IGKV1-39*01 (83.80%) -IGKJ4*01) [10.3.9] (1'-111') -Homo sapiens IGKC*01, Km3 (112'-218')]; dimer (226-226":229-229")-bisdisulfide
rosmantuzumab immunoglobuline G1-kappa, anti-[Homo sapiens RSPO3 (R-spondine 3, protéine 2 contenant un domaine thrombospondine de type I (TSP1), THSD2)], anticorps monoclonal humanisé; chaîne lourde gamma1 (1-447) [VH humanisé (Homo sapiens IGHV1-46*01 (84.50%) -(IGHD)-IGHJ4*01) [8.8.10] (1-117) -Homo sapiens IGHG1*03, (CH1 (118-215), charnière (216-230), ), CH2 (231-340), CH3 (341-445), CHS (446-447)) (118-447)], (220-218')-disulfure avec la chaîne légère (1'-218') [V-KAPPA humanisé (Homo sapiens IGKV1-39*01 (83.80%) -IGKJ4*01) [10.3.9] (1'-111') -Homo sapiens IGKC*01, Km3 (112'-218')]; dimère (226-226":229-229")-bisdisulfure
Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
124
rosmantuzumab
inmunoglobulina G1-kappa, anti-[Homo sapiens RSPO3 (R-espondina 3, proteína 2 que contiene un dominio tromboespondina de tipo I (TSP1), THSD2)], anticuerpo monoclonal humanizado; cadena pesada gamma1 (1-447) [VH humanizado (Homo sapiens IGHV1-46*01 (84.50%) -(IGHD)-IGHJ4*01) [8.8.10] (1-117) -Homo sapiens IGHG1*03, (CH1 (118-215), bisagra (216-230), ), CH2 (231-340), CH3 (341-445), CHS (446-447)) (118-447)], (220-218')-disulfuro con la cadena ligera (1'-218') [V-KAPPA humanizado (Homo sapiens IGKV1-39*01 (83.80%) -IGKJ4*01) [10.3.9] (1'-111') -Homo sapiens IGKC*01, Km3 (112'-218')]; dímero (226-226":229-229")-bisdisulfuro
rosomidnarum rosomidnar DNA oligonucleotide sequence that is complementary to a
region upstream of the B-cell lymphoma (BCL-2) gene: 2'-deoxycytidylyl-(3'→5')-2'-deoxyadenylyl-(3'→5')-2'-deoxycytidylyl-(3'→5')-2'-deoxyguanylyl-(3'→5')-2'-deoxycytidylyl-(3'→5')-2'-deoxyadenylyl-(3'→5')-2'-deoxycytidylyl-(3'→5')-2'-deoxyguanylyl-(3'→5')-2'-deoxycytidylyl-(3'→5')-2'-deoxyguanylyl-(3'→5')-2'-deoxycytidylyl-(3'→5')-2'-deoxyadenylyl-(3'→5')-thymidylyl-(3'→5')-2'-deoxycytidylyl-(3'→5')-2'-deoxycytidylyl-(3'→5')-2'-deoxycytidylyl-(3'→5')-2'-deoxycytidylyl-(3'→5')-2'-deoxyguanylyl-(3'→5')-2'-deoxycytidylyl-(3'→5')-2'-deoxycytidylyl-(3'→5')-2'-deoxycytidylyl-(3'→5')-2'-deoxyguanylyl-(3'→5')-thymidylyl-(3'→5')-2'-deoxyguanosine
WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
125
rosomidnar
séquence oligonucléotide d'ADN complémentaire d'une région en amont du gène (BCL-2) lymphome formé de lymphocytes B: 2'-déoxycytidylyl-(3'→5')-2'-déoxyadénylyl-(3'→5')-2'-déoxycytidylyl-(3'→5')-2'-déoxyguanylyl-(3'→5')-2'-déoxycytidylyl-(3'→5')-2'-déoxyadénylyl-(3'→5')-2'-déoxycytidylyl-(3'→5')-2'-déoxyguanylyl-(3'→5')-2'-déoxycytidylyl-(3'→5')-2'-déoxyguanylyl-(3'→5')-2'-déoxycytidylyl-(3'→5')-2'-déoxyadénylyl-(3'→5')-thymidylyl-(3'→5')-2'-déoxycytidylyl-(3'→5')-2'-déoxycytidylyl-(3'→5')-2'-déoxycytidylyl-(3'→5')-2'-déoxycytidylyl-(3'→5')-2'-déoxyguanylyl-(3'→5')-2'-déoxycytidylyl-(3'→5')-2'-déoxycytidylyl-(3'→5')-2'-déoxycytidylyl-(3'→5')-2'-déoxyguanylyl-(3'→5')-thymidylyl-(3'→5')-2'-déoxyguanosine
rosomidnar secuencia de oligonucleótidos de ADN complementaria de una región ascendente del gen (BCL-2) de linfomas de células B: 2'-desoxicitidilil-(3'→5')-2'-desoxiadenilil-(3'→5')-2'-desoxicitidilil-(3'→5')-2'-desoxiguanilil-(3'→5')-2'-desoxicitidilil-(3'→5')-2'-desoxiadenilil-(3'→5')-2'-desoxicitidilil-(3'→5')-2'-desoxiguanilil-(3'→5')-2'-desoxicytidilil-(3'→5')-2'-desoxiguanilil-(3'→5')-2'-desoxicitidilil-(3'→5')-2'-desoxiadenilil-(3'→5')-timidilil-(3'→5')-2'-desoxicitidilil-(3'→5')-2'-desoxicitidilil-(3'→5')-2'-desoxicitidilil-(3'→5')-2'-desoxicitidilil-(3'→5')-2'-desoxiguanilil-(3'→5')-2'-desoxicitidilil-(3'→5')-2'-desoxicitidilil-(3'→5')-2'-desoxicitidilil-(3'→5')-2'-desoxiguanilil-(3'→5')-timidilil-(3'→5')-2'-desoxiguanosina
C227H291N88O141P23
rozanolixizumabum # rozanolixizumab immunoglobulin G4-kappa, anti-[Homo sapiens FCGRT
(Fc fragment of IgG receptor and transporter, neonatal Fc receptor, FcRn, transmembrane alpha chain of the neonatal receptor)], humanized and chimeric monoclonal antibody; gamma4 heavy chain (1-444) humanized [humanized VH (Homo sapiens IGHV3-7*01 (86.50%) -(IGHD) -IGHJ4*01) [8.8.10] (1-117)), Homo sapiens IGHG4*01 (CH1 (118-215), hinge S10>P (225) (216-227),CH2 (228-337), CH3 (338-442), CHS (443-444)) (118-444)], (131-219')-disulfide with kappa light chain chimeric (1'-219') [synthetic V-KAPPA (Homo sapiens IGKV1-9*01 (76.00%) -Homo sapiens IGKJ2*01) [11.3.9] (1'-112') -Homo sapiens IGKC*01, Km3 (113'-219')]; dimer (223-223":226-226")-bisdisulfide

Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
126
rozanolixizumab
immunoglobuline G4-kappa, anti-[Homo sapiens FCGRT (récepteur du fragment Fc des IgG et transporteur, récepteur Fc néonatal, FcRn, chaîne alpha transmembranaire du récepteur néonatal)], anticorps monoclonal humanisé et chimérique; chaîne lourde gamma4 humanisée (1-444) [VH humanisé (Homo sapiens IGHV3-7*01 (86.50%) -(IGHD) -IGHJ4*01) [8.8.10] (1-117)), Homo sapiens IGHG4*01 (CH1 (118-215), charnière S10>P (225) (216-227), CH2 (228-337), CH3 (338-442), CHS (443-444)) (118-444)], (131-219')-disulfure avec la chaîne légère kappa chimérique (1'-219') [V-KAPPA synthétique (Homo sapiensIGKV1-9*01 (76.00%) -Homo sapiens IGKJ2*01) [11.3.9] (1'-112') -Homo sapiens IGKC*01, Km3 (113'-219')]; dimère (223-223":226-226")-bisdisulfure
rozanolixizumab inmunoglobulina G4-kappa, anti-[Homo sapiens FCGRT (receptor del fragmento Fc de las IgG y transportador, receptor Fc neonatal, FcRn, cadena alfa transmembranaria del receptor neonatal)], anticuerpo monoclonal humanizado y quimérico; cadena pesada gamma4 humanizada (1-444) [VH humanizado (Homo sapiens IGHV3-7*01 (86.50%) -(IGHD) -IGHJ4*01) [8.8.10] (1-117)), Homo sapiens IGHG4*01 (CH1 (118-215), bisagra S10>P (225) (216-227), CH2 (228-337), CH3 (338-442), CHS (443-444)) (118-444)], (131-219')-disulfuro con la cadena ligera kappa quimérica (1'-219') [V-KAPPA sintético (Homo sapiensIGKV1-9*01 (76.00%) -Homo sapiens IGKJ2*01) [11.3.9] (1'-112') -Homo sapiens IGKC*01, Km3 (113'-219')]; dímero (223-223":226-226")-bisdisulfuro
WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
127
sacituzumabum # sacituzumab immunoglobulin G1-kappa, anti-[Homo sapiens TACSTD2
(tumor-associated calcium signal transducer 2, membrane component chromosome 1 surface marker 1, M1S1, gastrointestinal tumor-associated antigen GA7331, pancreatic carcinoma marker protein GA733-1, epithelial glycoprotein-1, EGP-1, trophoblast antigen-2, cell surface glycoprotein Trop-2, TROP2)], humanized monoclonal antibody; gamma1 heavy chain (1-451) [humanized VH (Homo sapiens IGHV7-4-1*02 (85.70%) -(IGHD)-IGHJ2*01) [8.8.14] (1-121) -Homo sapiens IGHG1*03, G1m3 (CH1 (122-219), hinge (220-234), CH2 (235-344), CH3 (345-449), CHS (450-451)) (122-451)], (224-214')-disulfide with kappa light chain (1'-214') [humanized V-KAPPA (Homo sapiens IGKV1-9*01 (82.20%) -IGKJ4*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 (108'-214')]; dimer (230-230":233-233")-bisdisulfide
sacituzumab immunoglobuline G1-kappa, anti-[Homo sapiens TACSTD2 (transducteur 2 de signaux calciques associé aux tumeurs, composant membranaire du chromosome 1 marqueur de surface 1, M1S1, antigène GA7331 associé aux tumeurs gastrointestinales, protéine GA733-1 marqueur de carcinomes pancréatiques, glycoprotéine épithéliale 1, EGP-1, antigène 2 du trophoblaste, glycoprotéine Trop-2 à la surface des cellules, TROP2)], anticorps monoclonal humanisé; chaîne lourde gamma1 (1-451) [VH humanisé (Homo sapiens IGHV7-4-1*02 (85.70%) -(IGHD)-IGHJ2*01) [8.8.14] (1-121) -Homo sapiens IGHG1*03, G1m3 (CH1 (122-219), charnière (220-234), CH2 (235-344), CH3 (345-449), CHS (450-451)) (122-451)], (224-214')-disulfure avec la chaîne légère kappa (1'-214') [V-KAPPA humanisé (Homo sapiens IGKV1-9*01 (82.20%) -IGKJ4*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 (108'-214')]; dimère (230-230":233-233")-bisdisulfure
sacituzumab inmunoglobulina G1-kappa, anti-[Homo sapiens TACSTD2 (transductor 2 de señales cálcicas asociado a los tumores, componente membranario del cromosoma 1 marcador de superficie 1, M1S1, antígeno GA7331 asociado a todos los tumores gastrointestinales, proteína GA733-1 marcador de carcinomas pancreáticos, glicoproteína epitelial 1, EGP-1, antígeno 2 de trofoblasto, glicoproteína Trop-2 de la superficie de las células, TROP2)], anticuerpo monoclonal humanizado; cadena pesada gamma1 (1-451) [VH humanizado (Homo sapiens IGHV7-4-1*02 (85.70%) -(IGHD)-IGHJ2*01) [8.8.14] (1-121) -Homo sapiens IGHG1*03, G1m3 (CH1 (122-219), bisagra (220-234), CH2 (235-344), CH3 (345-449), CHS (450-451)) (122-451)], (224-214')-disulfuro con la cadena ligera kappa (1'-214') [V-KAPPA humanizado (Homo sapiens IGKV1-9*01 (82.20%) -IGKJ4*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 (108'-214')]; dímero (230-230":233-233")-bisdisulfuro
Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
128
satoreotidum satoreotide S2,S7-cyclo{4-chloro-L-phenylalanyl-D-cysteinyl-4-[(4S)-2,6-
dioxo-1,3-diazinane-4-carboxamido]-L-phenylalanyl-4-(carbamoylamino)-D-phenylalanyl-L-lysyl-L-threonyl-L-cysteinyl-D-tyrosinamide}
satoréotide S2,S7-cyclo{4-chloro-L-phénylalanyl-D-cystéinyl-4-[(4S)-2,6-dioxo-1,3-diazinane-4-carboxamido]-L-phénylalanyl-4-(carbamoylamino)-D-phénylalanyl-L-lysyl-L-thréonyl-L-cystéinyl-D-tyrosinamide}
satoreotida S2,S7-ciclo{4-cloro-L-fenilalanil-D-cisteinil-4-[(4S)-2,6-dioxo-1,3-diazinano-4-carboxamido]-L-fenilalanil-4-(carbamoilamino)-D-fenilalanil-L-lisil-L-treonil-L-cisteinil-D-tirosinamida}
C58H72ClN15O14S2
seladelparum seladelpar [4-({(2R)-2-ethoxy-3-[4-
(trifluoromethyl)phenoxy]propyl}sulfanyl)- 2-methylphenoxy]acetic acid

WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
129
séladelpar acide [4-({(2R)-2-éthoxy-3-[4-(trifluorométhyl)phénoxy]propyl}sulfanyl)- 2-méthylphénoxy]acétique
seladelpar ácido [4-({(2R)-2-etoxi-3-[4-(trifluorometil)fenoxi]propil}sulfanil)-2-metilfenoxi]acético
C21H23F3O5S
seltorexantum seltorexant [(3aR,6aS)-5-(4,6-dimethylpyrimidin-
2-yl)hexahydropyrrolo[3,4-c]pyrrol-2(1H)-yl][2-fluoro- 6-(2H-1,2,3-triazol-2-yl)phenyl]methanone
seltorexant [(3aR,6aS)-5-(4,6-diméthylpyrimidin- 2-yl)hexahydropyrrolo[3,4-c]pyrrol-2(1H)-yl][2-fluoro- 6-(2H-1,2,3-triazol-2-yl)phényl]méthanone
seltorexant [(3aR,6aS)-5-(4,6-dimetilpirimidin-2-il)hexahidropirrolo[3,4-c]pirrol-2(1H)-il][2-fluoro-6-(2H-1,2,3-triazol- 2-il)fenil]metanona
C21H22FN7O
serabelisibum serabelisib [6-(2-amino-1,3-benzoxazol-5-yl)imidazo[1,2-a]pyridin-
3-yl](morpholin-4-yl)methanone
sérabélisib [6-(2-amino-1,3-benzoxazol-5-yl)imidazo[1,2-a]pyridin- 3-yl](morpholin-4-yl)méthanone
serabelisib [6-(2-amino-1,3-benzoxazol-5-il)imidazo[1,2-a]piridin- 3-il](morfolin-4-il)metanona
Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
130
C19H17N5O3
sofpironii bromidum sofpironium bromide 1-ambo-(3R)-3-{[(R)-(cyclopentyl)hydroxy(phenyl)
acetyl]oxy}-1-(2-ethoxy-2-oxoethyl)-1-methylpyrrolidinium bromide
bromure de sofpironium bromure de 1-ambo-(3R)-3-{[(R)-(cyclopentyl)hydroxyl (phényl)acétyl]oxy}-1-(2-éthoxy-2-oxoéthyl)- 1-méthylpyrrolidinium
bromuro de sofpironio bromuro de 1-ambo-(3R)-3-{[(R)-(ciclopentil)hidroxi (fenil)acetil]oxi}-1-(2-etoxi-2-oxoetil)-1-metilpirrolidinio
C22H32BrNO5
somatrogonum # somatrogon fusion protein of human choriogonadotropin subunit β (CG-
β)-(118-145)-peptide (1-28) with human somatotropin (growth hormone, GH) (29-219) and two tandem copies of human choriogonadotropin subunit β (CG-β)-(118-145)-peptide (220-247, 248-275), O-glycosylated on 12-18 serines, produced in Chinese hamster ovary (CHO) cells
somatrogon sous-unité bêta de la choriogonadotrophine humaine (CG-β)-(118-145)-peptide (1-28) protéine de fusion avec la somatropine humaine (hormone de croissance, GH) (29-219) protéine de fusion avec deux copies de la sous-unité bêta de la choriogonadotrophine humaine (CG-β)-(118-145)-peptide (1-28), 12-18 sérines sont O-glycosylées, produite par des cellules ovariennes de hamster chinois (CHO)
somatrogón subunidad beta de la coriogonadotropina humana (CG-β)-(118-145)-péptido (1-28) proteína de fusión con la somatropina humana (hormona de crecimiento, GH) (29-219) proteína de fusión con ambas copias de la subunidad beta de la coriogonadotropina humana (CG-β)-(118-145)-péptido (1-28), 12-18 serinas O-glicosiladas, producidas por las células de ovario de hamster chino (CHO)
WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
131
suptavumabum # suptavumab immunoglobulin G1-kappa, anti-[human respiratory
syncytial virus (RSV) fusion glycoprotein F], Homo sapiens monoclonal antibody; gamma1 heavy chain (1-453) [Homo sapiens VH (IGHV3-9*01 (87.90%) -(IGHD) -IGHJ6*01) [8.8.16](1-123) -IGHG1*01, G1m17,1 (CH1 (124-221), hinge (222-236), CH2 (237-346), CH3 (347-451), CHS (452-453))(124-453)], (226-214')-disulfide with kappa light chain (1'-214') [Homo sapiens V-KAPPA (IGKV3-15*01 (94.70%) -IGKJ4*01) [6.3.9] (1'-107')-IGKC*01, Km3 (108'-214')]; dimer (232-232'':235-235'')-bisdisulfide
suptavumab immunoglobuline G1-kappa, anti-[glycoprotéine de fusion F du virus respiratoire syncytial (VRS) humain], Homo sapiens anticorps monoclonal; chaîne lourde gamma1 (1-453) [Homo sapiens VH (IGHV3-9*01 (87.90%) -(IGHD) -IGHJ6*01) [8.8.16] (1-123) -IGHG1*01, G1m17,1 (CH1 (124-221), charnière (222-236), CH2 (237-346), CH3 (347-451), CHS (452-453))(124-453)], (226-214')-disulfure avec la chaîne légère kappa (1'-214') [Homo sapiens V-KAPPA (IGKV3-15*01 (94.70%) -IGKJ4*01) [6.3.9] (1'-107') -IGKC*01, Km3 (108'-214')]; dimère (232-232'':235-235'')-bisdisulfure
suptavumab inmunoglobulina G1-kappa, anti-[glicoproteína de fusión F del virus respiratorio sincitial (VRS) humano], Homo sapiens anticuerpo monoclonal; cadena pesada gamma1 (1-453) [Homo sapiens VH (IGHV3-9*01 (87.90%) -(IGHD) -IGHJ6*01) [8.8.16] (1-123) -IGHG1*01, G1m17,1 (CH1 (124-221), bisagra (222-236), CH2 (237-346), CH3 (347-451), CHS (452-453))(124-453)], (226-214')-disulfuro con la cadena ligera kappa (1'-214') [Homo sapiens V-KAPPA (IGKV3-15*01 (94.70%) -IGKJ4*01) [6.3.9] (1'-107') -IGKC*01, Km3 (108'-214')]; dímero (232-232'':235-235'')-bisdisulfuro

Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
132
telisotuzumabum # telisotuzumab immunoglobulin G1-kappa, anti-[Homo sapiens MET (met
proto-oncogene, hepatocyte growth factor (HGF) receptor, HGFR, scatter factor (SF) receptor, HGF/SF receptor, receptor tyrosine-protein kinase c-met, papillary renal cell carcinoma 2, RCCP2)], humanized monoclonal antibody; gamma1 heavy chain (1-445) [humanized VH (Homo sapiens IGHV1-2*02 (92.90%) -(IGHD)-IGHJ4*01) [8.8.11] (1-118) -Homo sapiens IGHG1*03, G1m3 (CH1 (119-216), hinge K7>del, T8>C (223), T10>del (217-229), CH2 (230-339), CH3 (340-444), CHS K>del (445)) (119-445)], (221-218')-disulfide with kappa light chain (1'-218') [humanized V-KAPPA (Homo sapiens IGKV4-1*01 (85.10%) -IGKJ4*01) [10.3.9] (1'-111') -Homo sapiens IGKC*01, Km3 (112'-218')]; dimer (223-223":225-225":228:228")-trisdisulfide
télisotuzumab immunoglobuline G1-kappa, anti-[Homo sapiens MET (proto-oncogène met, récepteur du facteur de croissance hépatocytaire, HGFR, récepteur du facteur de dispersion, récepteur de l'HGF/SF, récepteur protéine-tyrosine kinase c-Met, carcinome papillaire à cellules rénales 2, RCCP2)], anticorps monoclonal humanisé; chaîne lourde gamma1 (1-445) [VH humanisé (Homo sapiens IGHV1-2*02 (92.90%) -(IGHD)-IGHJ4*01) [8.8.11] (1-118) -Homo sapiens IGHG1*03, G1m3 (CH1 (119-216),charnière K7>del, T8>C (223), T10>del (217-229), CH2 (230-339), CH3 (340-444), CHS K>del (445)) (119-445)], (221-218')-disulfure avec la chaîne légère kappa (1'-218') [V-KAPPA humanisé (Homo sapiens IGKV4-1*01 (85.10%) -IGKJ4*01) [10.3.9] (1'-111') -Homo sapiens IGKC*01, Km3 (112'-218')]; dimère (223-223":225-225":228:228")-trisdisulfure

WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
133
telisotuzumab inmunoglobulina G1-kappa, anti-[Homo sapiens MET (proto-oncogen met, receptor del factor de crecimiento de hepatocitos, HGFR, receptor del factor de dispersión, receptor del HGF/SF, receptor proteína-tirosina kinasa c-Met, carcinoma papilar de células renales 2, RCCP2)], anticuerpo monoclonal humanizado; cadena pesada gamma1 (1-445) [VH humanizado (Homo sapiens IGHV1-2*02 (92.90%) -(IGHD)-IGHJ4*01) [8.8.11] (1-118) -Homo sapiens IGHG1*03, G1m3 (CH1 (119-216),bisagra K7>del, T8>C (223), T10>del (217-229), CH2 (230-339), CH3 (340-444), CHS K>del (445)) (119-445)], (221-218')-disulfuro con la cadena ligera kappa (1'-218') [V-KAPPA humanizado (Homo sapiens IGKV4-1*01 (85.10%) -IGKJ4*01) [10.3.9] (1'-111') -Homo sapiens IGKC*01, Km3 (112'-218')]; dímero (223-223":225-225":228:228")-trisdisulfuro
telisotuzumabum vedotinum # telisotuzumab vedotin immunoglobulin G1-kappa, anti-[Homo sapiens MET (met
proto-oncogene, hepatocyte growth factor (HGF) receptor, HGFR, scatter factor (SF) receptor, HGF/SF receptor, receptor tyrosine-protein kinase c-met, papillary renal cell carcinoma 2, RCCP2)], humanized monoclonal antibody conjugated to auristatin E; gamma1 heavy chain (1-445) [humanized VH (Homo sapiens IGHV1-2*02 (92.90%) -(IGHD)-IGHJ4*01) [8.8.11] (1-118) -Homo sapiens IGHG1*03, G1m3 (CH1 (119-216), hinge K7>del, T8>C (223), T10>del (217-229), CH2 (230-339), CH3 (340-444), CHS K>del (445)) (119-445)], (221-218')-disulfide with kappa light chain (1'-218') [humanized V-KAPPA (Homo sapiens IGKV4-1*01 (85.10%) -IGKJ4*01) [10.3.9] (1'-111') -Homo sapiens IGKC*01, Km3 (112'-218')]; dimer (223-223":225-225":228:228")-trisdisulfide; conjugated, on an average of 3 cysteinyl, to
Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
134
monomethylauristatin E (MMAE), via a cleavable maleimidocaproyl-valyl-citrullinyl-p-aminobenzyloxycarbonyl (mc-val-cit-PABC) type linker For the vedotin part, please refer to the document "INN for pharmaceutical substances: Names for radicals, groups and others"*.
télisotuzumab védotine immunoglobuline G1-kappa, anti-[Homo sapiens MET (proto-oncogène met, récepteur du facteur de croissance hépatocytaire, HGFR, récepteur du facteur de dispersion, récepteur de l'HGF/SF, récepteur protéine-tyrosine kinase c-Met, carcinome papillaire à cellules rénales 2, RCCP2)], anticorps monoclonal humanisé conjugué à l'auristatine E; chaîne lourde gamma1 (1-445) [VH humanisé (Homo sapiens IGHV1-2*02 (92.90%) -(IGHD)-IGHJ4*01) [8.8.11] (1-118) -Homo sapiens IGHG1*03, G1m3 (CH1 (119-216),charnière K7>del, T8>C (223), T10>del (217-229), CH2 (230-339), CH3 (340-444), CHS K>del (445)) (119-445)], (221-218')-disulfure avec la chaîne légère kappa (1'-218') [V-KAPPA humanisé (Homo sapiens IGKV4-1*01 (85.10%) -IGKJ4*01) [10.3.9] (1'-111') -Homo sapiens IGKC*01, Km3 (112'-218')]; dimère (223-223":225-225":228:228")-trisdisulfure; conjugué, sur 3 cystéinyl en moyenne, au monométhylauristatine E (MMAE), via un linker clivable de type maléimidocaproyl-valyl-citrullinyl- p-aminobenzyloxycarbonyl (mc-val-cit-PABC) Pour la partie védotine, veuillez-vous référer au document "INN for pharmaceutical substances: Names for radicals, groups and others"*.
telisotuzumab vedotina inmunoglobulina G1-kappa, anti-[Homo sapiens MET (protooncogén met, receptor del factor de crecimiento de los hepatocitos, HGFR, receptor del factor de dispersión, receptor del HGF/SF, receptor proteína-tirosina kinasa c-Met, carcinoma papilar de las células renales 2, RCCP2)], anticuerpo monoclonal humanizado conjugado con la auristatina E; cadena pesada gamma1 (1-445) [VH humanizado (Homo sapiens IGHV1-2*02 (92.90%) -(IGHD)-IGHJ4*01) [8.8.11] (1-118) -Homo sapiens IGHG1*03, G1m3 (CH1 (119-216),bisagra K7>del, T8>C (223), T10>del (217-229), CH2 (230-339), CH3 (340-444), CHS K>del (445)) (119-445)], (221-218')-disulfuro con la cadena ligera kappa (1'-218') [V-KAPPA humanizado (Homo sapiens IGKV4-1*01 (85.10%) -IGKJ4*01) [10.3.9] (1'-111') -Homo sapiens IGKC*01, Km3 (112'-218')]; dímero (223-223":225-225":228:228")-trisdisulfuro; conjugado, sobre una media de 3 cisteinil, a la monometilauristatina E (MMAE), mediante un enlace escindible de tipo maleimidocaproil-valil-citrulinil-p-aminobenciloxicarbonil (mc-val-cit-PABC) Para la fracción vedotina se pueden referir al documento "INN for pharmaceutical substances: Names for radicals, groups and others"*.

WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
135
tenofovirum exalidexum tenofovir exalidex 3-(hexadecyloxy)propyl hydrogen ({[(2R)-1-(6-amino-
9H-purin-9-yl)propan-2-yl]oxy}methyl)phosphonate
ténofovir exalidex ({[(2R)-1-(6-amino-9H-purin-9-yl)propan- 2-yl]oxy}méthyl)hydrogénophosphonate de 3-(hexadécyloxy)propyle
tenofovir exalidex ({[(2R)-1-(6-amino-9H-purin-9-il)propan- 2-il]oxi}metil)hidrogenofosfonato de 3-(hexadeciloxi)propilo
C28H52N5O5P
tirabrutinibum tirabrutinib 6-amino-9-[(3R)-1-(but-2-ynoyl)pyrrolidin-3-yl]-
7-(4-phenoxyphenyl)-7,9-dihydro-8H-purin-8-one
tirabrutinib 6-amino-9-[(3R)-1-(but-2-ynoyl)pyrrolidin-3-yl]- 7-(4-phénoxyphényl)-7,9-dihydro-8H-purin-8-one
tirabrutinib 6-amino-9-[(3R)-1-(but-2-inoil)pirrolidin-3-il]- 7-(4-fenoxifenil)-7,9-dihidro-8H-purin-8-ona
Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
136
C25H22N6O3
tonabacasum # tonabacase Staphylococcus aureus phage 1 (SAP-1)-derived soluble
endolysin (Staphylococcus aureus phage lysin-1, bacteriolysin SAL-1), produced in Escherichia coli
tonabacase endolysine soluble dérivée du phage 1 de Staphylococcus aureus (lysine du phage 1 de Staphylococcus aureus, bactériolysine SAL-1), produite par Escherichia coli
tonabacasa endolisina soluble derivada del fago 1 de Staphylococcus aureus (lisina del fago 1 de Staphylococcus aureus, bacteriolisina SAL-1), producida por Escherichia coli
tonogenconcelum # tonogenconcel Allogeneic primary human chondrocytes transduced with a
retroviral vector expressing human transforming growth factor-beta1 (TGF-β1). A master cell bank of primary human chondrocytes, grown from cartilage tissue obtained from the surgical excision of a polydactyly finger from a three-year-old female donor, was prepared. After transduction of cells from the master cell bank, a single clonal population was selected using limiting dilution and submitted to irradiation. Cells express TGF-β1, Type I and Type II collagen as well as Type I and Type II TGF-β1 receptors; they lack expression of gag and pol genes.
tonogenconcel Chondrocytes humains primaires allogéniques transduits par un vecteur rétroviral exprimant le facteur de croissance transformant-bêta1 (TGF-β1). Une banque de cellules primaires a été préparée à partir de tissu cartilagineux obtenu par excision chirurgicale d'un doigt surnuméraire d'un donneur âgé de 3 ans et de sexe féminin. Après transduction des cellules de la banque de cellules primaires, un seul clone a été sélectionné en utilisant une dilution limitative et en le soumettant à une irradiation. Les cellules expriment le TGF- β1, du collagène de type I et II ainsi que les récepteurs de type I et II du TGF- β1; elles sont dépourvues d'expression de gènes gag et pol.
WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
137
tonogenconcel Condrocitos humanos primarios alogénicos transducidos por un vector retroviral que expresa el factor de crecimiento transformador-bêta1 (TGF-β1). Un banco de células primarias preparado a partir de tejido cartilaginoso obtenido por escisión quirúrgica de un dedo adicional de un donante de 3 años de edad y de sexo femenino. Después de la transducción de las células del banco de células primarias, se selecciona un único clon utilizando una dilución limitante y se somete a radiación. Las células que expresan el TGF- β1, del colágeno de tipo I y II así como los receptes de tipo I y II del TGF- β1; ellas carecen de la expresión de los genes gag y pol.
tozuleristidum tozuleristide N6.27-[6-(2-{(1E,2E,4E,6E)-7-[1,1-dimethyl-3-(4-
sulfonatobutyl)-1H-benzo[e]indol-3-ium-2-yl]hepta-2,4,6-trien-1-ylidene}-1,1-dimethyl-1,2-dihydro-3H-benzo[e]indol-3-yl)hexanoyl]-[Lys15>Arg,Lys23>Arg]chlorotoxin (Leiurus quinquestriatus quinquestriatus) (Egyptian scorpion)
tozuléristide N6.27-[6-(2-{(1E,2E,4E,6E)-7-[1,1-diméthyl-3-(4-sulfonatobutyl)-1H-benzo[e]indol-3-ium-2-yl]hepta-2,4,6-trién-1-ylidène}-1,1-diméthyl-1,2-dihydro-3H-benzo[e]indol-3-yl)hexanoyl]-[Lys15>Arg,Lys23>Arg]chlorotoxine de Leiurus quinquestriatus quinquestriatus (scorpion égyptien)
tozuleristida N6.27-[6-(2-{(1E,2E,4E,6E)-7-[1,1-dimetil-3-(4-sulfonatobutil)-1H-benzo[e]indol-3-ium-2-il]hepta-2,4,6-trien-1-ilideno}-1,1-dimetil-1,2-dihidro-3H-benzo[e]indol-3-il)hexanoil]-[Lys15>Arg,Lys23>Arg]clorotoxina de Leiurus quinquestriatus quinquestriatus (escorpión egipcio)
C203H296N58O52S12
trastuzumabum duocarmazinum # trastuzumab duocarmazine immunoglobulin G1-kappa, anti-[Homo sapiens ERBB2
(epidermal growth factor receptor 2, receptor tyrosine-protein kinase erbB-2, EGFR2, HER2, HER-2, p185c-erbB2, NEU, CD340)], humanized monoclonal antibody conjugated to the pro-drug seco-duocarmycin-hydroxybenzamide-azaindole (seco-DUBA);

Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
138
gamma1 heavy chain (1-449) [humanized VH (Homo sapiens (IGHV3-66-*01 (81.60%) -(IGHD)-IGHJ6*01) [8.8.13] (1-120) -Homo sapiens IGHG1*01, G1m17, nG1m1 (CH1 (121-218), hinge (219-233),CH2 (234-343), CH3 D12>E (359), L14>M (361) (344-448), CHS K>del (449)) (121-449)], (223-214')-disulfide with kappa light chain (1'-214') [humanized V-KAPPA (Homo sapiens IGKV1-39*01 (86.30%) -IGKJ1*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 (108'-214')]; dimer (229-229":232-232")-bisdisulfide, conjugated on an average of 2 or 4 cysteines, to seco-DUBA via the cleavable linker N-[2-(2-maleimidoethoxy)ethoxycarbonyl]-L-valyl-L-citrullinyl-p-aminobenzyloxycarbonyl-N-[2-(2-hydroxyethoxy)ethyl]-N-[2-(methylamino)ethyl]carbamoyl
trastuzumab duocarmazine immunoglobuline G1-kappa, anti-[Homo sapiens ERBB2 (récepteur 2 du facteur de croissance épidermique, récepteur tyrosine-protéine kinase erbB-2, EGFR2, HER2, HER-2, p185c-erbB2, NEU, CD340)], anticorps monoclonal humanisé conjugué à la pro-drogue seco-duocarmycine-hydroxybenzamide-azaindole (seco-DUBA); chaîne lourde gamma1 (1-449) [VH humanisé (Homo sapiens (IGHV3-66-*01 (81.60%) -(IGHD)-IGHJ6*01) [8.8.13] (1-120) -Homo sapiens IGHG1*01, G1m17, nG1m1 (CH1 (121-218), charnière (219-233),CH2 (234-343), CH3 D12>E (359), L14>M (361) (344-448), CHS K>del (449)) (121-449)], (223-214')-disulfure avec la chaîne légère kappa (1'-214') [V-KAPPA humanisé (Homo sapiens IGKV1-39*01 (86.30%) -IGKJ1*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 (108'-214')]; dimère (229-229":232-232")-bisdisulfure, conjugué sur une moyenne de 2 ou 4 cystéines au séco-DUBA via le linker clivable N-[2-(2-maléimidoéthoxy)éthoxycarbonyl]-L-valyl-L-citrullinyl-p-aminobenzyloxycarbonyl-N-[2-(2-hydroxyéthoxy)éthyl]-N-[2-(méthylamino)éthyl]carbamoyle
trastuzumab duocarmazina inmunoglobulina G1-kappa, anti-[Homo sapiens ERBB2 (receptor 2 del factor de crecimiento epidérmico, receptor tirosina-proteína kinasa erbB-2, EGFR2, HER2, HER-2, p185c-erbB2, NEU, CD340)], anticuerpo monoclonal humanizado conjugado con el profármaco seco-duocarmicina-hidroxibenzamida-azaindol (seco-DUBA); cadena pesada gamma1 (1-449) [VH humanizado (Homo sapiens (IGHV3-66-*01 (81.60%) -(IGHD)-IGHJ6*01) [8.8.13] (1-120) -Homo sapiens IGHG1*01, G1m17, nG1m1 (CH1 (121-218), bisagra (219-233),CH2 (234-343), CH3 D12>E (359), L14>M (361) (344-448), CHS K>del (449)) (121-449)], (223-214')-disulfuro con la cadena ligera kappa (1'-214') [V-KAPPA humanizado (Homo sapiens IGKV1-39*01 (86.30%) -IGKJ1*01) [6.3.9] (1'-107') -Homo sapiens IGKC*01, Km3 (108'-214')]; dímero (229-229":232-232")-bisdisulfuro; conjugado en 2 o 4 cisteínas, por término medio con seco-DUBA mediante el enlace escin-dible N-[2-(2-maleimidoetoxi)etoxicarbonil]-L-valil-L-citrulinil-p-aminobenciloxicarbonil-N-[2-(2-hidroxietoxi)etil]-N-[2-(metilamino)etil]carbamoilo

WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
139
tucidinostatum tucidinostat N-(2-amino-4-fluorophenyl)-4-{[(2E)-3-(pyridin-3-yl)prop-
2-enamido]methyl}benzamide
tucidinostat N-(2-amino-4-fluorophényl)-4-{[(2E)-3-(pyridin-3-yl)prop- 2-énamido]méthyl}benzamide
tucidinostat N-(2-amino-4-fluorofenil)-4-{[(2E)-3-(piridin-3-il)prop- 2-enamido]metil}benzamida
C22H19FN4O2
upadacitinibum upadacitinib (3S,4R)-3-ethyl-4-(3H-imidazo[1,2-a]pyrrolo[2,3-e]pyrazin-
8-yl)-N-(2,2,2-trifluoroethyl)pyrrolidine-1-carboxamide

Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
140
upadacitinib (3S,4R)-3-éthyl-4-(3H-imidazo[1,2-a]pyrrolo[2,3-e]pyrazin-8-yl)-N-(2,2,2-trifluoroéthyl)pyrrolidine-1-carboxamide
upadacitinib (3S,4R)-3-etil-4-(3H-imidazo[1,2-a]pirrolo[2,3-e]pirazin- 8-il)-N-(2,2,2-trifluoroetil)pirrolidina-1-carboxamida
C17H19F3N6O
uprifosbuvirum uprifosbuvir propan-2-yl N-[(R)-{[(2R,3R,4R,5R)-4-chloro-5-(2,4-dioxo-
3,4-dihydropyrimidin-1(2H)-yl)-3-hydroxy-4-methyloxolan-2-yl]methoxy}phenoxyphosphoryl]-D-alaninate
uprifosbuvir N-[(R)-{[(2R,3R,4R,5R)-4-chloro-5-(2,4-dioxo-3,4-dihydropyrimidin-1(2H)-yl)-3-hydroxy-4-méthyloxolan- 2-yl]méthoxy}phénoxyphosphoryl]-D-alaninate de propan-2-yle
uprifosbuvir N-[(R)-{[(2R,3R,4R,5R)-4-cloro-5-(2,4-dioxo- 3,4-dihidropirimidin-1(2H)-il)-3-hidroxi-4-metiloxolan- 2-il]metoxi}fenoxifosforil]-D-alaninato de propan-2-ilo
C22H29ClN3O9P
utomilumabum # utomilumab immunoglobulin G2-lambda, anti-[Homo sapiens TNFRSF9
(tumor necrosis factor receptor (TNFR) superfamily member 9, 4-1BB, T cell antigen ILA, CD137)], Homo sapiens monoclonal antibody; gamma2 heavy chain (1-442) [Homo sapiens VH (IGHV5-10-1*04 (94.90%) -(IGHD)-IGHJ4*01) [8.8.9] (1-116) -IGHG2*01, G2m.. (CH1 (117-214), hinge (215-226), CH2 (227-335), CH3 (336-440), CHS (441-442)) (117-442)], (130-213')-disulfide with lambda light chain (1'-214') [Homo sapiens V-LAMBDA (IGLV3-1*01 (90.00%) -IGLJ7*01) [6.3.11] (1'-108') -IGLC2*01 (109'-214')]; dimer (218-218'':219-219'':222-222'':225-225'')-tetrakisdisulfide
utomilumab immunoglobuline G2-lambda, anti-[Homo sapiens TNFRSF9 (membre 9 de la superfamille des récepteurs du facteur de nécrose tumorale, 4-1BB, antigène ILA de lymphocyte T, CD137)], Homo sapiens anticorps monoclonal;

WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
141
chaîne lourde gamma2 (1-442) [Homo sapiens VH (IGHV5-10-1*04 (94.90%) -(IGHD)-IGHJ4*01) [8.8.9] (1-116) -IGHG2*01, G2m.. (CH1 (117-214), charnière (215-226), CH2 (227-335), CH3 (336-440), CHS (441-442)) (117-442)], (130-213')-disulfure avec la chaîne légère lambda (1'-214') [Homo sapiens V-LAMBDA (IGLV3-1*01 (90.00%) -IGLJ7*01) [6.3.11] (1'-108') -IGLC2*01 (109'-214')]; dimère (218-218'':219-219'':222-222'':225-225'')-tétrakisdisulfure
utomilumab inmunoglobulina G2-lambda, anti-[Homo sapiens TNFRSF9 (miembro 9 de la superfamilia de los receptores del factor de necrosis tumoral, 4-1BB, antígeno ILA de linfocito T, CD137)], Homo sapiens anticuerpo monoclonal; cadena pesada gamma2 (1-442) [Homo sapiens VH (IGHV5-10-1*04 (94.90%) -(IGHD)-IGHJ4*01) [8.8.9] (1-116) -IGHG2*01, G2m.. (CH1 (117-214), bisagra (215-226), CH2 (227-335), CH3 (336-440), CHS (441-442)) (117-442)], (130-213')-disulfuro con la cadena ligera lambda (1'-214') [Homo sapiens V-LAMBDA (IGLV3-1*01 (90.00%) -IGLJ7*01) [6.3.11] (1'-108') -IGLC2*01 (109'-214')]; dímero (218-218'':219-219'':222-222'':225-225'')-tetrakisdisulfuro
Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
142
valnivudinum valnivudine {(2R,3S,5R)-3-hydroxy-5-[2-oxo-6-(4-pentylphenyl)furo[2,3-
d]pyrimidin-3(2H)-yl]oxolan-2-yl}methyl L-valinate
valnivudine L-valinate de {(2R,3S,5R)-3-hydroxy-5-[2-oxo- 6-(4-pentylphényl)furo[2,3-d]pyrimidin-3(2H)-yl]oxolan-2-yl}methyl
valnivudina L-valinato de {(2R,3S,5R)-3-hidroxi-5-[2-oxo-6-(4-pentilfenil)furo[2,3-d]pirimidin-3(2H)-il]oxolan-2-il}metilo
C27H35N3O6
vamorolonum vamorolone 17,21-dihydroxy-16α-methylpregna-1,4,9(11)-triene-
3,20-dione
vamorolone 17,21-dihydroxy-16α-méthylprègna-1,4,9(11)-triène- 3,20-dione
vamorolona 17,21-dihidroxi-16α-metilpregna-1,4,9(11)-trieno- 3,20-diona
C22H28O4
vandefitemcelum vandefitemcel human differentiation-restricted descendents (DRCs) of
bone-marrow-derived adherent stromal cells (MASCs) isolated from adult donor. To obtain DRCs, MASCs were transiently transfected with a DNA plasmid encoding human Notch-1 intracellular domain (NICD) and expanded in growth media. The transfection does not result in permanent incorporation of the gene into the cells, but does result in changes in a number of proteins and in the methylation pattern of the DNA (there is complete loss of recombinant NICD protein and of the plasmid in the final cell population). The transfection changes the nature of the cells such that they no longer readily differentiate into bone, cartilage or adipose cells, and also results in cells altered in their ability to secrete trophic and chemotactic factors, and extracellular matrix proteins to support damaged neural cells.

WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
143
Cells are positive for mesenchymal stem cell (MSC) markers (CD29, CD90, CD105) and negative for hematopoietic markers (CD31, CD34, CD45).
vandéfitemcel descendants à différenciation restreinte (DRCs) humains de cellules stromales adhérentes dérivées de la moelle osseuse (MASCs) isolées d'un donneur adulte. Pour obtenir les DRCs, les MASCs ont été transitoirement transfectées avec un plasmide dont l'ADN code pour le domaine intracellulaire de Notch-1 humain (NICD) et ont été expansées par des moyens de croissance. La transfection ne résulte pas d'une incorporation permanente du gène dans les cellules, mais de changements dans un nombre de protéines et dans les méthylations de l'ADN (il y a une perte complète de la protéine recombinante NICD et du plasmide dans la population finale). La transfection change la nature des cellules de telle sorte qu'elles ne se différencient plus en cellules osseuses, cartilagineuses ou adipeuses et il en résulte aussi des cellules modifiées dans leur capacité à secréter des facteurs trophiques et chimiotactiques, et des protéines de la matrice extracellulaire qui supportent les cellules neuronales endommagées. Les cellules sont positives pour les marqueurs des cellules souches mésenchymateuses (CD29, CD90, CD105) et négatives pour les marqueurs hématopoïétiques (CD31, CD34, CD45).
vandefitemcel descendientes humanos de la diferenciación restrictiva (DRCs) de células estromales adherentes derivadas de la médula ósea (MASCs) aisladas de un donante adulto. Para obtener los DRCs, las MASCs se transfectan transitoriamente con un plásmido de ADN que codifica para el dominio intracelular Notch-1 humano (NICD) y se expanden en un medio de crecimiento. La transfección no resulta en una incorporación permanente del gen dentro de las células, pero sí en cambios en el número de proteínas y en el patrón de metilación del DNA (hay una pérdida completa de proteína recombinante NICD y del plásmido en la población final celular). La transfección cambia la naturaleza de las células de tal modo que no se diferencian con más facilidad en células óseas, cartilaginosas o adiposas y también resulta en células modificadas bajo la capacidad de secretar factores tróficos y quimiotácticos, y las proteínas de la matriz extracelular que soportan las células neuronales dañadas. Las células son positivas para los marcadores de las células madres mesenquimales (CD29, CD90, CD105) y negativas para los marcadores hematopoyéticos (CD31, CD34, CD45).
velagliflozinum velagliflozin 2-[(4-cyclopropylphenyl)methyl]-
4-β-D-glucopyranosylbenzonitrile
vélagliflozine 2-[(4-cyclopropylphényl)méthyl]- 4-β-D-glucopyranosylbenzonitrile
Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
144
velagliflozina 2-[(4-ciclopropilfenil)metil]-4-β-D-glucopiranosilbenzonitrilo C23H25NO5
vestronidasum alfa # vestronidase alfa human β-glucuronidase, natural Leu627>Pro variant,
homotetramer, produced in Chinese hamster ovary cells (CHO), glycoform alfa
vestronidase alfa β-glucuronidase humaine, variant naturel Leu627>Pro, homotétramère, produit dans des cellules ovariennes de hamsters chinois (CHO), glycoforme alfa
vestronidasa alfa β-glucuronidasa humana, variante natural Leu627>Pro, homotetrámero, producido en células de ovario de hamster chino (CHO), glicoforma alfa
voretigenum neparvovecum # voretigene neparvovec recombinant adeno-associated serotype 2 (rAAV-2) virus
vector that carries the RPE65 gene, encoding a retinal pigment (RPE)-specific human retinoid isomerohydrolase, containing a modified Kozak sequence at the translation start site and under the control of the cytomegalovirus (CMV) immediate early enhancer and the chicken beta-actin (CBA) promoter.
voretigène néparvovec vecteur viral adéno-associé de type 2 (rAAV-2) recombinant, contenant le gène RPE65 codant pour l'isomérohydrolase des rétinoïdes, humaine, spécifique de l'épithélium pigmentaire de la rétine, contenant une séquence de Kozak au site de démarrage de la traduction et sous le contrôle de l'activateur immédiat-précoce du cytomégalovirus et du promoteur de l'actine bêta du poulet (ABP, CBA).
WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
145
voretigén neparvovec vector viral adeno-associado de tipo 2 (rAAV-2) recombinante, que contiene el gen RPE65 que codifica para la retinoide isomerohidrolasa, humana, especifica del epitelium pigmentario de la retina, que contiene una secuencia de Kozak al sitio del comienzo de la traducción y bajo el control del activador inmediato precoz del citomegalovirus (CMV) y del promotor de la actina beta del pollo (CBA).
vorolanibum vorolanib N-[(3S)-1-(dimethylcarbamoyl)pyrrolidin-3-yl]-
5-[(Z)-(5-fluoro-2-oxo-1,2-dihydro-3H-indol- 3-ylidene)methyl]-2,4-dimethyl-1H-pyrrole-3-carboxamide
vorolanib N-[(3S)-1-(diméthylcarbamoyl)pyrrolidin-3-yl]- 5-[(Z)-(5-fluoro-2-oxo-1,2-dihydro-3H-indol- 3-ylidène)méthyl]-2,4-diméthyl-1H-pyrrole-3-carboxamide
vorolanib N-[(3S)-1-(dimetilcarbamoil)pirrolidin-3-il]-5-[(Z)-(5-fluoro- 2-oxo-1,2-dihidro-3H-indol-3-ilideno)metil]-2,4-dimetil- 1H-pirrolo-3-carboxamida
C23H26FN5O3
vunakizumabum # vunakizumab immunoglobulin G1-kappa, anti-[Homo sapiens IL17A
(interleukin 17A, IL-17A)], humanized monoclonal antibody; gamma1 heavy chain (1-453) [humanized VH (Homo sapiens IGHV1-2*02 (82.70%) -(IGHD)-IGHJ4*01) [8.8.16] (1-123) -Homo sapiens IGHG1*01, G1m17, nG1m1 (CH1 (124-221), hinge (222-236),CH2 (237-346), CH3 D12>E (362), L14>M (364) (347-451), CHS (452-453)) (124-453)], (226-213')-disulfide with kappa light chain (1'-213') [humanized V-KAPPA (Homo sapiens IGKV6-21*01 (80.00%) -IGKJ1*01) [5.3.9] (1'-106') -Homo sapiens IGKC*01, Km3 (107'-213')]; dimer (232-232":235-235")-bisdisulfide
vunakizumab immunoglobuline G1-kappa, anti-[Homo sapiens IL17A (interleukine 17A, IL-17A)], anticorps monoclonal humanisé; chaîne lourde gamma1 (1-453) [VH humanisé (Homo sapiens IGHV1-2*02 (82.70%) -(IGHD)-IGHJ4*01) [8.8.16] (1-123) -Homo sapiens IGHG1*01, G1m17, nG1m1 (CH1 (124-221), charnière (222-236),CH2 (237-346), CH3 D12>E (362), L14>M (364) (347-451), CHS (452-453)) (124-453)], (226-213')-disulfure avec la chaîne légère

Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
146
kappa (1'-213') [V-KAPPA humanisé (Homo sapiens IGKV6-21*01 (80.00%) -IGKJ1*01) [5.3.9] (1'-106') -Homo sapiens IGKC*01, Km3 (107'-213')]; dimère (232-232":235-235")-bisdisulfure
vunakizumab inmunoglobulina G1-kappa, anti-[Homo sapiens IL17A (interleukina 17A, IL-17A)], anticuerpo monoclonal humanizado; cadena pesada gamma1 (1-453) [VH humanizado (Homo sapiens IGHV1-2*02 (82.70%) -(IGHD)-IGHJ4*01) [8.8.16] (1-123) -Homo sapiens IGHG1*01, G1m17, nG1m1 (CH1 (124-221), bisagra (222-236),CH2 (237-346), CH3 D12>E (362), L14>M (364) (347-451), CHS (452-453)) (124-453)], (226-213')-disulfuro con la cadena ligera kappa (1'-213') [V-KAPPA humanizado (Homo sapiens IGKV6-21*01 (80.00%) -IGKJ1*01) [5.3.9] (1'-106') -Homo sapiens IGKC*01, Km3 (107'-213')]; dímero (232-232":235-235")-bisdisulfuro
# Electronic structure available on Mednet: http://mednet.who.int/ # Structure électronique disponible sur Mednet: http://mednet.who.int/ # Estructura electrónica disponible en Mednet: http://mednet.who.int/ * http://www.who.int/medicines/services/inn/publication/en/
WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
147
AMENDMENTS TO PREVIOUS LISTS MODIFICATIONS APPORTÉES AUX LISTES ANTÉRIEURES
MODIFICACIONES A LAS LISTAS ANTERIORES Recommended International Nonproprietary Names (Rec. INN): List 32 Dénominations communes internationales recommandées (DCI Rec.): Liste 32 Denominaciones Comunes Internacionales Recomendadas (DCI Rec.): Lista 32 (WHO Drug Information, Vol. 6, No. 3, 1992) p. 9 suprimáse insertese tacrolimus tacrólimus Recommended International Nonproprietary Names (Rec. INN): List 34 Dénominations communes internationales recommandées (DCI Rec.): Liste 34 Denominaciones Comunes Internacionales Recomendadas (DCI Rec.): Lista 34 (WHO Drug Information, Vol. 8, No. 3, 1994) p. 19 suprimáse insertese sirolimus sirólimus Recommended International Nonproprietary Names (Rec. INN): List 43 Dénominations communes internationales recommandées (DCI Rec.): Liste 43 Denominaciones Comunes Internacionales Recomendadas (DCI Rec.): Lista 43 (WHO Drug Information, Vol. 14, No. 1, 2000) p. 64 suprimáse insertese pimecrolimús pimecrólimus Recommended International Nonproprietary Names (Rec. INN): List 44 Dénominations communes internationales recommandées (DCI Rec.): Liste 44 Denominaciones Comunes Internacionales Recomendadas (DCI Rec.): Lista 44 (WHO Drug Information, Vol. 14, No. 3, 2000) p. 194 suprimáse insertese everolimus everólimus Recommended International Nonproprietary Names (Rec. INN): List 54 Dénominations communes internationales recommandées (DCI Rec.): Liste 54 Denominaciones Comunes Internacionales Recomendadas (DCI Rec.): Lista 54 (WHO Drug Information, Vol. 19, No. 3, 2005) p. 266 suprimáse insertese temsirolimus temsirólimus Recommended International Nonproprietary Names (Rec. INN): List 56 Dénominations communes internationales recommandées (DCI Rec.): Liste 56 Denominaciones Comunes Internacionales Recomendadas (DCI Rec.): Lista 56 (WHO Drug Information, Vol. 20, No. 3, 2006) p. 233 suprimáse insertese zotarolimus zotarólimus
Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
148
Recommended International Nonproprietary Names (Rec. INN): List 65 Dénominations communes internationales recommandées (DCI Rec.): Liste 65 Denominaciones Comunes Internacionales Recomendadas (DCI Rec.): Lista 65 (WHO Drug Information, Vol. 25, No. 1, 2011) p. 91 suprimáse insertese umirolimús umirólimus Recommended International Nonproprietary Names (Rec. INN): List 67 Dénominations communes internationales recommandées (DCI Rec.): Liste 67 Denominaciones Comunes Internacionales Recomendadas (DCI Rec.): Lista 67 (WHO Drug Information, Vol. 26, No. 1, 2012) p. 77 suprimáse insertese olcorolimús olcorólimus Recommended International Nonproprietary Names (Rec. INN): List 69 Dénominations communes internationales recommandées (DCI Rec.): Liste 69 Denominaciones Comunes Internacionales Recomendadas (DCI Rec.): Lista 69 (WHO Drug Information, Vol. 27, No. 1, 2013) p. 44 antithrombinum gamma # antithrombin gamma replace the structure by the following one antithrombine gamma remplacer la structure par la suivante antitrombina gamma sustitúyase la estructura por la siguiente
HGSPVDICTA KPRDIPMNPM CIYRSPEKKA TEDEGSEQKI PEATNRRVWE 50
LSKANSRFAT TFYQHLADSK NDNDNIFLSP LSISTAFAMT KLGACNDTLQ 100QLMEVFKFDT ISEKTSDQIH FFFAKLNCRL YRKANKSSKL VSANRLFGDK 150SLTFNETYQD ISELVYGAKL QPLDFKENAE QSRAAINKWV SNKTEGRITD 200VIPSEAINEL TVLVLVNTIY FKGLWKSKFS PENTRKELFY KADGESCSAS 250MMYQEGKFRY RRVAEGTQVL ELPFKGDDIT MVLILPKPEK SLAKVEKELT 300PEVLQEWLDE LEEMMLVVHM PRFRIEDGFS LKEQLQDMGL VDLFSPEKSK 350LPGIVAEGRD DLYVSDAFHK AFLEVNEEGS EAAASTAVVI AGRSLNPNRV 400TFKANRPFLV FIREVPLNTI IFMGRVANPC VK 432
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuro8-128 21-95 247-430
Glycosylation sites (N) / Sites de glycosylation (N) / Posiciones de glicosilación (N)Asn-96 Asn-135 Asn-155 Asn-192
-Man4--Gl-N4--Gl-NN-Sia3--Gal3--Gl-N2--Man6-
-Sia3--Gal3--Gl-N2--Man3-
Recommended International Nonproprietary Names (Rec. INN): List 69 Dénominations communes internationales recommandées (DCI Rec.): Liste 69 Denominaciones Comunes Internacionales Recomendadas (DCI Rec.): Lista 69 (WHO Drug Information, Vol. 27, No. 1, 2013) p. 90 suprimáse insertese ridaforolimus ridaforólimus

WHO Drug Information, Vol. 31, No. 1, 2017 Recommended INN: List 77
149
Recommended International Nonproprietary Names (Rec. INN): List 76 Dénominations communes internationales recommandées (DCI Rec.): Liste 76 Denominaciones Comunes Internacionales Recomendadas (DCI Rec.): Lista 76 (WHO Drug Information, Vol. 30, No. 3, 2016) p. 496 enoblituzumabum # enoblituzumab replace the structure by the following one énoblituzumab remplacer la structure par la suivante enoblituzumab sustitúyase la estructura por la siguiente
Heavy chain / Chaîne lourde / Cadena pesada
EVQLVESGGG LVQPGGSLRL SCAASGFTFS SFGMHWVRQA PGKGLEWVAY 50 ISSDSSAIYY ADTVKGRFTI SRDNAKNSLY LQMNSLRDED TAVYYCGRGR 100 ENIYYGSRLD YWGQGTTVTV SSASTKGPSV FPLAPSSKST SGGTAALGCL 150 VKDYFPEPVT VSWNSGALTS GVHTFPAVLQ SSGLYSLSSV VTVPSSSLGT 200 QTYICNVNHK PSNTKVDKRV EPKSCDKTHT CPPCPAPELV GGPSVFLLPP 250 KPKDTLMISR TPEVTCVVVD VSHEDPEVKF NWYVDGVEVH NAKTKPPEEQ 300 YNSTLRVVSV LTVLHQDWLN GKEYKCKVSN KALPAPIEKT ISKAKGQPRE 350 PQVYTLPPSR EEMTKNQVSL TCLVKGFYPS DIAVEWESNG QPENNYKTTP 400 LVLDSDGSFF LYSKLTVDKS RWQQGNVFSC SVMHEALHNH YTQKSLSLSP 450 GK 452
Light chain / Chaîne légère / Cadena ligeraDIQLTQSPSF LSASVGDRVT ITCKASQNVD TNVAWYQQKP GKAPKALIYS 50 ASYRYSGVPS RFSGSGSGTD FTLTISSLQP EDFATYYCQQ YNNYPFTFGQ 100 GTKLEIKRTV AAPSVFIFPP SDEQLKSGTA SVVCLLNNFY PREAKVQWKV 150 DNALQSGNSQ ESVTEQDSKD STYSLSSTLT LSKADYEKHK VYACEVTHQG 200 LSSPVTKSFN RGEC 214
Disulfide bridges location / Position des ponts disulfure / Posiciones de los puentes disulfuroIntra-H (C23-C104) 22-96 149-205 266-326 372-430 22''-96'' 149''-205'' 266''-326'' 372''-430''Intra-L (C23-C104) 23'-88' 134'-194' 23'''-88''' 134'''-194''' Inter-H-L (h 5-CL 126) 225-214' 225''-214''' Inter-H-H (h 11, h 14) 231-231'' 234-234''
N-glycosylation sites / Sites de N-glycosylation / Posiciones de N-glicosilaciónH CH2 N84.4:302, 302''Fucosylated complex bi-antennary CHO-type glycans / glycanes de type CHO bi-antennairescomplexes fucosylés / glicanos de tipo CHO biantenarios complejos fucosilados
p. 511 leniolisibum leniolisib replace the chemical name by the following one léniolisib remplacer le nom chimique par le suivant leniolisib sustitúyase el nombre químico por el siguiente
1-[(3S)-3-({6-[6-methoxy-5-(trifluoromethyl)pyridin-3-yl]-5,6,7,8-
tetrahydropyrido[4,3-d]pyrimidin-4-yl}amino)pyrrolidin-1-yl]propan- 1-one
1-[(3S)-3-({6-[6-méthoxy-5-(trifluorométhyl)pyridin-3-yl]-5,6,7,8-tétrahydropyrido[4,3-d]pyrimidin-4-yl}amino)pyrrolidin-1-yl]propan- 1-one
1-[(3S)-3-({6-[6-metoxi-5-(trifluorometil)piridin-3-il]-5,6,7,8-tetrahidropirido[4,3-d]pirimidin-4-il}amino)pirrolidin-1-il]propan-1-ona

Recommended INN: List 77 WHO Drug Information, Vol. 31, No. 1, 2017
150
Procedure and Guiding Principles / Procédure et Directives / Procedimientos y principios generales
The text of the Procedures for the Selection of Recommended International Nonproprietary Names for Pharmaceutical Substances and General Principles for Guidance in Devising International Nonproprietary Names for Pharmaceutical Substances will be reproduced in proposed INN lists only.
Les textes de la Procédure à suivre en vue du choix de dénominations communes internationales recommandées pour les substances pharmaceutiques et des Directives générales pour la formation de dénominations communes internationales applicables aux substances pharmaceutiques seront publiés seulement dans les listes des DCI proposées.
El texto de los Procedimientos de selección de denominaciones comunes internacionales recomendadas para las sustancias farmacéuticas y de los Principios generales de orientación para formar denominaciones comunes internacionales para sustancias farmacéuticas aparece solamente en las listas de DCI propuestas.