Embed Size (px)
Citation preview


What About All Those Critical Lines?
Lines, catheters and drains can be accommodated, securedEVD line stationary bike

What About All Those Critical Lines?
Patient lines and drains can be accommodated
Including Femoral Lines
Mechanical ventilation and CVVH lines
Damluji, A., et al. (2013). "Safety and feasibility of femoral catheters during physical rehabilitation in the intensive care unit." J Crit Care.
Winkelman, C. (2011). "Ambulating with pulmonary artery or femoral catheters in place." Crit Care Nurse 31(5): 70-73.

Activity Intensity and Dosage
Individualized treatments based on patient prior activity, goals
PT consults for chronic patients, delirious patients, patients unable to lift full leg from mattress
Lines, catheters and drains can be accommodated, secured
PTs optimize intensity of mobility
Garzon-Serrano, J., C. Ryan, et al. (2011). "Early Mobilization in Critically Ill Patients: Patients' Mobilization Level Depends on Health Care Provider's Profession." PM R 3 (4): 307-313

When Is It Time to Stop and Rest?Patient remains unresponsive
Fatigued, pale appearance
Respiratory rate consistently > 10 bpm above baseline
Decreasing muscle recruitment
Loss of balance
Decreasing weight bearing ability
Diaphoresis

When Quality of Life Is Restored
Avoiding Post Traumatic Stress Disorder in Patients and FamiliesDavydow, D. S., J. M. Gifford, et al. (2008). "Posttraumatic stress disorder in general intensive care unit survivors: a systematic review." Gen Hosp Psychiatry 30(5): 421-434
ICU DiariesJones, C., C. Backman, et al. (2010).
"Intensive care diaries reduce new onset post traumatic stress disorder following critical illness: a randomised, controlled trial." Crit Care Med

KEY REFERENCES: Laying the Foundation for E of ABCDEF Bundle
ICU-acquired weakness and cognitive deficits: occur quickly and resolve slowly• Herridge M. N Engl J Med. 2003;348:683-93.
• De Jonghe B. Crit Care Clin. 2007;23:55-69.
• Levine S. N Engl J Med. 2008;358:1327-35.
• Herridge M. N Engl J Med. 2011;364:1293-304.
• Grosu H. Chest. 2012;142:1455-60.
• Puthucheary Z. JAMA. 2013;310:1591-600.
• Calvo-Ayala E. Chest. 2013;144:1469-80.
• Kress J. N Engl J Med. 2014;370:1626-35.
• Fan E. Am JRespir Crit Care Med. 2014;190:1437-46.
• Pandharipande P. N Engl J Med. 2013;369:1306-16.

KEY REFERENCES: Laying the Foundation for E of ABCDEF Bundle
Early progressive mobility interventions work• Thomsen G. Crit Care Med. 2008;36:1119-24.
• Schweickert W. Lancet. 2009;373:1874-82.
• Pohlman M. Crit Care Med. 2010;38:2089-94.
• Needham D. Arch Phys Med Rehabil. 2010;91:536-42.
• Morris P. Am J Med Sci. 2011;341:373-7.
• Hopkins R. Phys Ther. 2012;92:1518-23.
• Lord R. Crit Care Med. 2013;41:717-24.
• Kayambu G. Crit Care Med. 2013;41:1543-54.
• Kayambu G. Intensive Care Med. 2015;41:865-74.
• Miller M. Ann Am Thorac Soc. epub May 2015.

KEY REFERENCES: Laying the Foundation for E of ABCDEF Bundle
Safety of early progressive mobility• Damluji A. J Crit Care. 2013;535:e9-15.
• Winkelman C. Crit Care Nurse. 2011;31:70-3.
• Bailey P. Crit Care Med. 2007;35:139-45.
• Sricharoenchai T. J Crit Care. 2014;29:395-400.
• Perme C. Cardiopulm Phys Ther J. 2013;24:12-7.
• Hopkins R. Crit Care Clinics. 2007;23:81-96

KEY REFERENCES: Laying the foundation for mobility for femoral catheters
• Perme C. Cardiopulm Phys Ther J. 2013;24(2):12-17.
• Damluji A J. Crit Care. 2013 Aug;28(4):535.e9-15
• Perme C. . J Acute Care Phys Ther. 2011;2(1):32-36.
• Perme C. Am J Respir Crit Care Med. 2009;179:A1586.

KEY REFERENCES: Laying the foundation for Nursing Progressive Mobility Program in ICU
• Dang S L Crit Care Nurs Q. 2013;36(2):163-168.
• Zomorodi M. Criti Care Res Pract. 2012;2012:964547.
• Dammeyer J. Crit Care Nurs Q. 2013;36(1):37-49.
Mobility is basic nursing care!

We Need The Entire Bundle for SuccessKey references: Laying the foundation for implementing
the entire bundle
Implementing the entire ABCDEF Bundle is crucial!• Balas M. Crit Care Med. 2013;42:1024-36.
• Bassett R. Jt Comm J Qual Patient Saf. 2015;41:62-74.
• Klompas M. Am J Respir Crit Care Med. 2015;191:292-301.
• Miller M. Ann Am Thorac Soc. 2015;12:1066-71.

Objectives
1. Understand the deficits ICU survivors face and describe the benefits of early mobility in ICU
2. Identify strategies for successful implementation of early mobilization programs in your ICU
3. Discuss potential barriers to early mobilization programs

Question to Ask During Rounds: Did the Patient Achieve his or her Maximal Mobility Activity Today?

Did the Patient Achieve his or her Maximal Mobility Activity Today?
YES!
• Mobility is everyone’s job!• RN, PT, OT, etc.
• Communicate patient’s current mobility status to all ICU team members
• Encourage patients to perform active movements if possible

Did Our Patient Achieve his or her Maximal Mobility Activity Today?
NO!
• Why not?
• Was the patient walking before admission?
• Is the patient hemodynamically stable?
• Is the patient awake?
Why Mobilize Patients in ICU?

Side Effects of Bed Rest
• Muscle strength in a healthy person can decrease 1.3% to 3% for every day spent on bedrest.1
• Effects are more profound in older people and in those with critical illness.2
• A new study suggests that 3% to 11% strength loss occurs for every day in bed in an ICU setting.3
• Age and days on bedrest are independent predictors of worsening function.
Topp R. Am J Crit Care. Clin Issues 2002.Yende S. Thorax. 2006.Fan E. Am JRespir Crit Care Med. 2014;190:1437-46.

Evidence-Based Benefits of Early Progressive Mobility
•Decrease ICU and hospital LOS
• Improve overall physical functioning
•Decrease duration of mechanical ventilation
•Decrease incidence of delirium
Bailey P. Crit Care Med. 2007;35:139-45.Morris P. Crit Care Med. 2008 Aug;36:2238-43.Schweickert W. Lancet. 2009;373:1874-82.

Early Activity is Feasible and Safe in Respiratory Failure Patients
Results:
1,449 activity events in 103 patients
• Sit on bed: 233 ( 16%)
• Sit in chair: 454 (31%)
• Ambulate: 762 (53%)
Patients with an endotracheal tube in place:
• 593 activity events
• 249 were ambulatory (42%)
There were < 1% activity-related adverse events
Bailey P. Crit Care Med. 2007;35:139-145.

Early Activity is Feasible and Safe in Respiratory Failure Patients (cont’d.)
Conclusion:
• A majority of survivors (69%) were able to ambulate >100 feet at RICU discharge
• Patients who went home ambulated farther (mean = 337 feet) than patients who went to a skilled nursing facility (Mean =293 feet)
Bailey P. Crit Care Med. 2007;35:139-145.

Early ICU Mobility Therapy in the Treatment of Acute Respiratory Failure
Morris P. Crit Care Med. 2008;36:2238-43
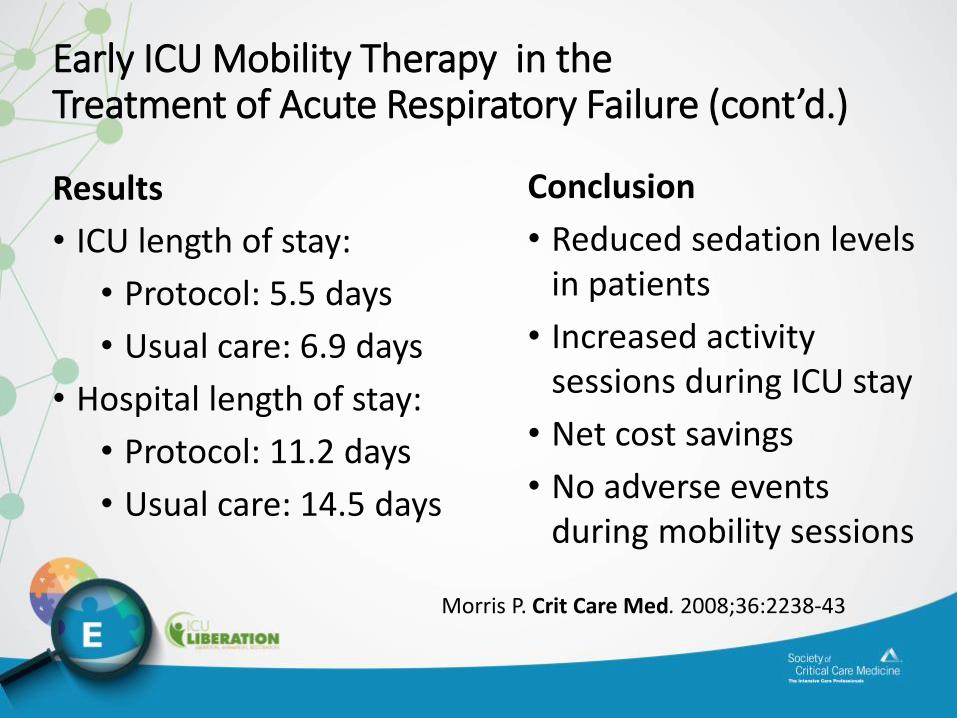
Early ICU Mobility Therapy in the Treatment of Acute Respiratory Failure (cont’d.)
Results
• ICU length of stay:
• Protocol: 5.5 days
• Usual care: 6.9 days
• Hospital length of stay:
• Protocol: 11.2 days
• Usual care: 14.5 days
Conclusion
• Reduced sedation levels in patients
• Increased activity sessions during ICU stay
• Net cost savings
• No adverse events during mobility sessions
Morris P. Crit Care Med. 2008;36:2238-43

Early Physical and Occupational Therapy in Mechanically Ventilated, Critically Ill Patients: A Randomised Controlled Trial
Results
• 104 patients on mechanical ventilation
• Intervention group: OT/PT median of 1.5 days after intubation
• Control group: OT/PT median of 7.4 days after intubation
• 1 adverse event with no harm to patient in 498 mobility sessions
Schweickert W. Lancet. 2009;373:1874-82.

Conclusion
• Intervention group had:
• Decreased days of delirium (50%) and MV
• ICU LOS reduced by 2-day median
• 59% return to independent function at hospital discharge vs. only 35% in control group
Early Physical and Occupational Therapy in Mechanically Ventilated, Critically Ill Patients: A Randomised Controlled Trial (cont’d.)
Schweickert W. Lancet. 2009;373:1874-82.

STARTING AN EARLY
PROGRESSIVE MOBILITY AND
EARLY REHABILITATION PROGRAM
0 7 14 21 280
20
40
60
80
50 100
Control
Intervention
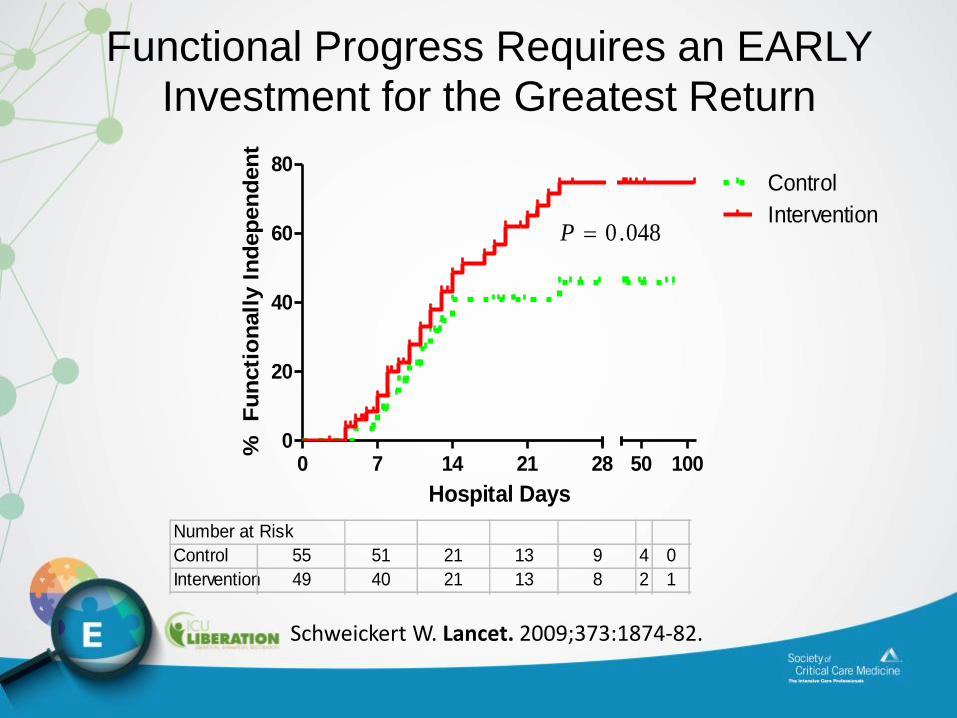
Number at Risk
Control 55 51 21 13 9 4 0
Intervention 49 40 21 13 8 2 1
048.0P
Hospital Days
%
Fu
ncti
on
all
y I
nd
ep
en
den
t
Functional Progress Requires an EARLY Investment for the Greatest Return
Schweickert W. Lancet. 2009;373:1874-82.

Education for ICU Staff
• Long-term impact for patients and families
• Benefits of early progressive mobility
• Role of all team members
• Specific processes

Keys for Successful Early Progressive Mobility and Rehabilitation Program in ICU
• Program tailored toward specific needs of each ICU
• Strong nursing mobility program with general nursing guidelines to consistently promote early mobility
• Strong physical therapy mobility program
• Specific guidelines for referral to physical and occupational therapy
• Strong interprofessional program staff commitment

• Shared vision for early mobility and mutual goals among all members of the team
• Color signs near the bed to alert staff and families about patient’s mobility status
• Patient and family educational material
• Appropriate resources
• Adequate equipment
Keys for Successful Early Progressive Mobility and Rehabilitation Program in ICU (cont’d.)

Changing Behaviors to Improve Patient Outcomes in ICU
• Greatly impacts practices at institutions
• Varies among facilities

Early Progressive Mobility in ICU
In-bed mobility
• Passive range-of-motion exercises
• Turning side to side
• Sitting on the side of the bed
• Active strengthening exercises
Out-of-bed mobility
• Standing at bedside
• Sitting on a regular chair
• Sitting on a cardiac chair
• Walking
MOBILITY IS EVERYONE’S JOB INTHE INTENSIVE CARE UNIT!

Equipment
General equipment
• Chair
• Portable cardiac monitor
• Walker
• Wheelchair
• IV poles
• Oxygen tank
• Transport ventilator
Specific rehabilitation equipment
• TheraBand
• Cuff weights
• Overhead trapeze and pulleys
• Standing frame
• Cycle ergometers
• Leg press
• Moveo table
• Video game systems

Considerations Before Mobilizing Patients in ICU• Neurologic: Level of alertness
• Cardiac: Hemodynamic stability• Vasoactive medications
• Pulmonary: Ventilation/oxygenation needs
• Risk vs. benefit
• Guidelines vs. Protocols • Fewer absolute contraindications
• Importance of interdisciplinary collaboration

Hodgson, C. et al. Critical Care Medicine 2014; 18: 658-666

Perceived Barriers to Progressive Early Mobility
• Severity of disease
• Severity of weakness
• Premorbid level of function
• ICU culture that promotes bed rest
• Nutritional state
• Sleep deprivation
• Level of delirium
• Pain
• Obesity

Absolute Contraindications to Progressive Mobility in ICU
• Patients on neuromuscular blockade• Hemodynamic instability requiring escalating dose or
multiple vasopressors• Significant oxygenation dysfunction requiring high level of
oxygen• Unstable fractures• Cerebral edema with uncontrolled intracranial pressure• Active bleeding• Intra-aortic balloon pump on femoral artery• Pacer dependent with transvenous temporary pacemaker• ECMO with femoral cannulation• Femoral arterial sheath• Open chest/open abdomen

Patient on Mechanical Ventilation AND CVVH with Femoral Catheter
Perme C. Cardiopulm Phys Ther J. 2013;24(2):12-17.Damluji A J. Crit Care. 2013 Aug;28(4):535.e9-15 Perme C. . J Acute Care Phys Ther. 2011;2(1):32-36.Perme C. Am J Respir Crit Care Med. 2009;179:A1586.

Interprofessional Team in ICU
• Patient
• Physician
• Nurse
• Respiratory therapist
• Physical therapist
• Occupational therapist
• Dietitian
• Pharmacist
• Nurse assistant
• Social worker
• Case manager
• Chaplain
• Family
• Speech therapist

Different Teams Mobilizing Patientsin ICU
• Physical therapists and nurses
• Physical therapists and rehabilitation technicians
• Physical therapists and occupational therapists
Engel HJ. Crit Care Med. 2013;41(9 Suppl 1):S69-80.
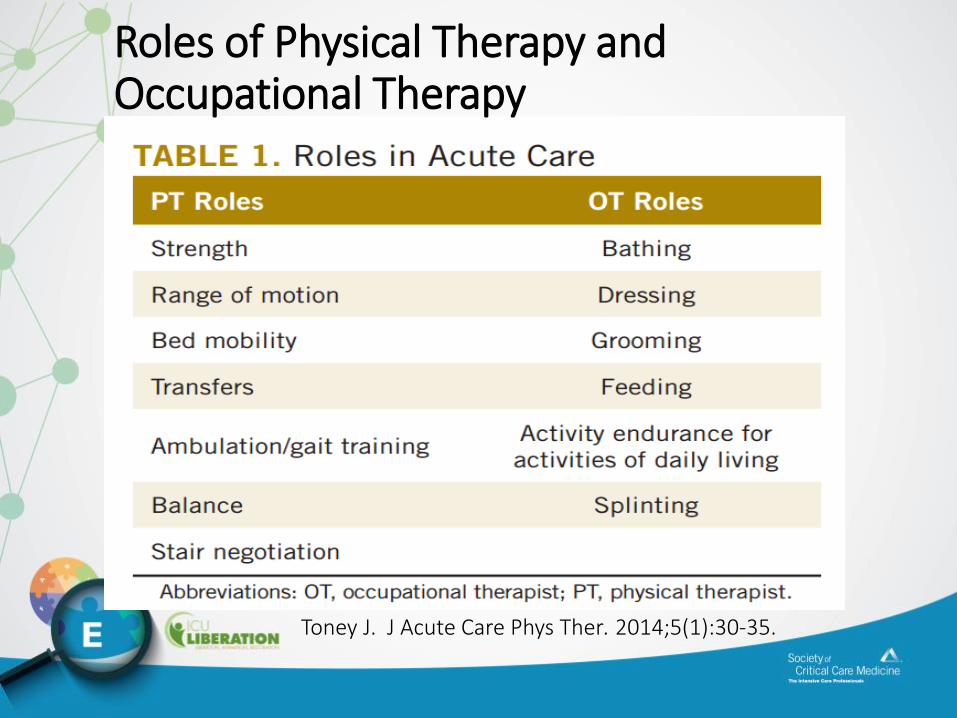
Toney J. J Acute Care Phys Ther. 2014;5(1):30-35.
Roles of Physical Therapy and Occupational Therapy

Therapeutic Interventions
Physical Therapy
• Education
• Positioning
• Exercises
• Transfers
• Walking re-education
• Chest physical therapy
Occupational Therapy
• Education
• Positioning
• Exercises
• Transfers
• ADLS
• Splints
• Cognitive training

Keys to Optimizing Therapy Interventions
• Developing individualized plans of care
• Not protocolizing
• Stepwise progression
• Reassessing frequently for changes in status

Mobility as a Vital Sign and as an Investment
Consider the patient activity tolerance on a daily basis
Gradual progression of activity with adequate rest and recovery
Delirium and altered mental Status

Patient and Family CollaborationPromote:
• Patient autonomy
• Communication strategies
• Use of ICU Diaries
• Proper sleep/wake cycle
• Ways to connect to the outside world
• Family engagement in progressive mobility

Early Progressive Mobility in ICU:It’s Worth the Effort!





























