Embed Size (px)
Citation preview

Online only Supplement
Supplemental Figures
1

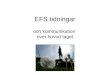
eFigure 1: Breast cancer event free survival based on pCR status among clinical trial studies only
Legend: Forest plot of the association between pCR and improved event free survival (EFS) among prospective clinical trials including HR estimate with 95% probability interval (PI), as compared to residual disease (RD). For comparison, the raw study specific HR estimates are reported.
2

eFigure 2: Overall survival based on pCR status among clinical trial studies only
Legend: Forest plot of the association between pCR and improved overall survival (OS) among prospective clinical trials including HR estimate with 95% probability interval (PI), as compared to residual disease (RD). For comparison, the raw study specific HR estimates are reported.
eFigure 3: Breast cancer event free survival based on pCR status among studies with 5 years of follow-up or greater
3

Legend: Forest plot of the association between pCR and improved event free survival (EFS) among studies with 5 or more years of follow-up, including HR estimate with 95% probability interval (PI), as compared to residual disease (RD). For comparison, the raw study specific HR estimates are reported.
eFigure 4: Breast cancer event free survival based on pCR status among breast cancer subtypes, A) triple negative, B) HER2+, and C) hormone receptor-positive
4

A.
B.
5

C.
6

Legend: Forest plot of the association between pCR and improved event free survival (EFS) among the major breast cancer subtypes, including HR estimate with 95% probability interval (PI), as compared to residual disease (RD). For comparison, the raw study specific HR estimates are reported.
7

eFigure 5: Overall survival based on pCR status among breast cancer subtypes, A) triple negative, B) HER2+, and C) hormone receptor-positive
A.
8

B.
9

C.
Legend: Forest plot of the association between pCR and improved overall survival (OS) among the major breast cancer subtypes, including HR estimate with 95% probability interval (PI), as compared to residual disease (RD). For comparison, the raw study specific HR estimates are reported.
10

eFigure 6A-D: Relationship between pCR and OS overall and among the major breast cancer subtypes
Legend: Kaplan-Meier curves depicting the relationship between pathologic complete response (pCR) and overall survival (OS) overall (A), in triple negative breast cancer (B), HER2-positive breast cancer (C), and hormone receptor-positive breast cancer (D), based on hazard ratio data from the studies. The blue line represents the pCR group and the orange line represents the residual disease group. The shaded regions represent the 95% pointwise probability interval for their respective color.
11

eFigure 7A-B: Breast cancer event free survival based on pCR among HER2+ patients receiving neoadjuvant anti-HER2 therapies (A) and those not receiving neoadjuvant anti-HER2 therapies (B) A
B
Legend: Forest plot of the association between pCR and improved event free survival (EFS) among HER2+ patients based on receipt of neoadjuvant anti-HER2 therapies, including HR estimate with 95% probability interval (PI), as compared to residual disease (RD). For comparison, the raw study specific HR estimates are reported.
12

eFigure 8A-B: Breast cancer event free survival based on pCR among HER2+ patients receiving adjuvant anti-HER2 therapies (A) and those not receiving adjuvant anti-HER2 therapies (B)A
B
Legend: Forest plot of the association between pCR and improved event free survival (EFS) among HER2+ patients based on receipt of adjuvant anti-HER2 therapies, including HR estimate with 95% probability interval (PI), as compared to residual disease (RD). For comparison, the raw study specific HR estimates are reported.
13

eFigure 9A-B: Tables for (A) greater than 90% of patients received adjuvant chemotherapy vs (B) less than 10% of patients received adjuvant chemotherapy
A
14

B
15

eFigure 10A-B: Impact of adjuvant chemotherapy on the relationship between pCR and OS
Legend: Forest plot of the association between pCR and overall survival (OS), as compared to residual disease (RD), among (A) the populations with at least 90% of patients receiving adjuvant chemotherapy and (B) the populations with at most 10% of patients receiving adjuvant chemotherapy. The hazard ratio (HR) estimate with the 95% probability interval (PI) are shown overall. For comparison, the raw study specific HR estimates are reported.
16

Supplemental Tables
eTable 1: Summary of Study Characteristics
CharacteristicStudies, No. (%)(N= 52)
Study type- Randomized trial- Non-randomized trial- Pooled- Retrospective
5 (9.6)10 (19.2)5* (9.6)32 (61.5)
Publication date, median (range), y 2013 (1999-2016)Follow-up for recurrence, median (range), mo 48 (21.3-107)Follow-up for mortality, median (range), mo 49.9 (31.2-118)Clinical tumor subtypes included in studies- All (ER+/HR+, HER2+, TNBC)- ER+/HR+ and TNBC only- HER2+ - TNBC
32 (61.5)1 (1.9)13 (25.0)6 (11.5)
Type of cytotoxic NAT- Anthracycline-based- Taxane-based- Anthracycline/taxane-based- Anthracycline-based and/or taxane-based- Anthracycline/taxane/platinum-based- Taxane/platinum-based- Taxane-based and taxane/platinum-based - Anthracycline/platinum-based- Anthracycline/platinum/taxane-based- Multiple, other
1 (1.9)4 (7.7)12 (23.1)11 (21.2)4 (7.7) 3 (5.8)1 (1.9)1 (1.9)4 (7.7)11 (21.2)
Pathologic complete response definition, No. (%)- No invasive disease in breast or nodes (ypT0/is ypN0)- No invasive or in situ disease in breast or nodes (ypT0 ypN0)
47 (90.4)5 (9.6)
Use of adjuvant cytotoxic chemotherapy- ≤ 10% of patients- ≥85% of patients
19 (36.5)9 (17.3)
17

- 10-85% of patients, or % unknown 24 (46.2)Legend: y, year; mo, month; ER+, estrogen receptor positive; HR+, hormone receptor positive; HER2, human epidermal growth factor 2; TNBC, triple negative breast cancer; ND, no data; NAT, neoadjuvant therapy.*Representing 23 total clinical trials
eTable 2: Patient and study characteristics of included manuscripts
A. Patient characteristics and receptor status
Author YearPubMed ID Median
agePost-
menopausalPre-
menopausalSubtypes included ER+/HR+ HER2+ TNBC
HER2 status known
Kuerer 1999 10080586 47 ND ND All 106 ND ND NoChollet 2002 16077072 49 204 247 All 118 ND ND NoDieras 2004 15611510 47 69 131 All 106 ND ND NoLee 2004 15585076 51 ND ND All 36 10 ND YesRing 2004 15558072 ND 109 293 All 271 ND ND NoAbrial 2005 16267618 50 324 386 All 363 ND ND NoGuarneri 2006 16505422 49 882 825 All 1163 321 317 YesHurley 2006 16549824 51 27 21 HER2 26 48 0 YesAndre 2007 17468948 50 ND ND All 327 105 159 YesEralp 2008 18581139 32 0 110 All 65 29 ND YesLiedtke 2008 18250347 49 ND ND All 645 272 255 YesAl-Tweigeri 2009 19526202 41 14 45 All 42 17 ND YesFrasci 2009 19218307 48 ND ND TNBC 0 0 74 YesChang 2010 20549829 50 ND ND All 33 30 11 YesChen 2010 20372832 49 109 116 All 119 65 53 YesJinno 2010 19854722 50 37 34 All 47 19 ND YesKim 2010 21430399 ND ND ND All 143 78 76 YesMasuda 2010 20593180 50 ND ND All 7 ND 26 SomeArun 2011 21900106 39 ND ND All (BRCA+ 197 60 77 Yes
18

enriched)Fasching 2011 22081974 53 ND ND All 307 92 121 YesWu 2011 21830158 46 ND ND All ND ND 54 YesEsserman 2012 22649152 49 115 106 All 125 67 53 YesIm 2012 22094934 43 ND ND HER2 24 53 ND YesMelichar 2012 22392196 54 ND ND All 232 89 51 YesYoo 2012 22807938 44 ND ND All 156 99 69 YesZhang 2012 22547076 47 36 66 HER2 53 102 0 YesGuarneri 2013 24013581 48 ND ND All ND ND ND YesGuiu 2013 22863283 49 ND ND All 252 101 61 YesHurley 2013 23542956 49 61 83 TNBC 0 0 144 YesKrishnan 2013 24188937 50 142 273 All 236 125 78 SomeMarme 2013 23400797 47 ND ND All 103 36 23 YesNatoli 2013 23604446 48 ND ND HER2 125 205 0 YesCortazar 2014 24529560 49 ND ND All 3702 1921 1157 Somede Azambuja 2014 25130998 50 ND ND HER2 232 455 0 YesGroheux 2014 25432784 ND ND ND TNBC 0 0 74 YesKawajiri 2014 24527070 53 ND ND All 48 15 27 YesTakada 2014 24682674 53 422 335 HER2 334 776 0 YesTanioka 2014 24742606 54 ND ND HER2 169 366 0 YesWang 2014 25041784 ND 111 198 All 216 80 47 YesAl-Tweigeri 2015 26563257 43 14 66 All 56 29 13 Yes
Bear 2015 14559892 ND ND NDHR+/HER2-, TNBC 716 0 490 Yes
Gonzalez-Angulo 2015 25584488 ND ND ND HER2 348 589 0 YesKo 2015 26357493 44 ND ND All 53 52 28 YesLiu 2015 26526577 52 60 48 HER2 58 108 0 YesMayer 2015 25205424 46 ND ND HER2 57 88 0 YesVillarreal- 2015 25698148 49 ND ND HER2 121 244 0 Yes
19

GarzaZelnak 2015 25065563 49 15 12 HER2 11 27 0 YesGianni 2016 27179402 50 ND ND HER2 197 417 0 YesLi 2016 27191991 47 64 123 TNBC 0 0 186 YesShao 2016 27131315 ND ND ND TNBC 0 0 53 YesVillarreal-Garza 2016 27189008 49 ND ND All 910 430 287 YesZhang 2016 27447966 47 32 59 TNBC 0 0 91 Yes
B. Clinical staging and grade
Author Year Stage 1 Stage 2 Stage 3 T0-T1 T2 T3 T4 Node + Node -Grade 1 Grade 2 Grade 3
Kuerer 1999 0 89 283 17 87 112 144 296 76 ND ND NDChollet 2002 0 338 113 ND ND ND ND ND ND 46 156 111Dieras 2004 ND ND ND 0 125 75 0 116 84 21 86 77Lee 2004 0 10 47 0 0 29 43 42 15 ND ND NDRing 2004 ND ND ND 5 235 168 20 ND ND 31 169 179Abrial 2005 0 553 157 ND ND ND ND ND ND 84 267 182Guarneri 2006 ND ND ND ND ND ND ND ND ND 57 551 1073Hurley 2006 0 9 39 0 0 33 21 35 13 ND ND NDAndre 2007 ND ND ND 73 338 79 42 329 204 ND ND 289Eralp 2008 0 56 54 ND ND ND ND 110 0 ND ND 84Liedtke 2008 ND ND ND 170 538 161 225 713 380 ND ND NDAl-Tweigeri 2009 0 19 40 0 15 27 17 ND ND 0 28 31Frasci 2009 ND ND ND 0 35 39 0 48 26 ND ND 49Chang 2010 ND ND ND 0 14 42 17 40 32 ND ND NDChen 2010 ND ND 0 0 41 131 53 183 42 ND ND NDJinno 2010 ND ND ND 5 57 9 0 46 25 ND ND NDKim 2010 ND ND ND 34 179 35 0 243 14 ND ND NDMasuda 2010 ND ND ND 1 24 6 2 21 12 1 4 27
20

Arun 2011 14 161 123 38 173 57 45 217 89 19 107 186Fasching 2011 ND ND ND 92 372 26 61 ND ND 28 301 172Wu 2011 ND ND ND 10 132 62 45 170 80 15 92 142Esserman 2012 3 104 113 ND ND ND ND 143 78 18 96 103Im 2012 0 6 47 ND ND ND ND 53 0 ND ND NDMelichar 2012 0 182 163 ND ND ND ND 134 186 ND ND NDYoo 2012 ND ND ND ND ND ND ND 230 46 ND ND 106Zhang 2012 0 76 26 8 66 18 10 57 45 0 79 23Guarneri 2013 0 81 26 ND ND ND ND ND ND ND ND 81Guiu 2013 ND ND ND 16 198 86 37 224 121 28 168 136Hurley 2013 0 32 112 2 12 76 54 111 33 ND ND NDKrishnan 2013 0 47 368 ND ND ND ND 369 46 29 154 177Marme 2013 0 126 18 ND ND ND ND 75 75 6 61 72Natoli 2013 ND ND ND ND ND ND ND ND ND ND ND NDCortazar 2014 ND ND ND 785 7328 2493 1263 5487 6320 426 4392 3217de Azambuja 2014 ND ND ND 9 251 192 ND ND ND ND ND NDGroheux 2014 0 31 43 ND ND ND ND ND ND 0 10 63Kawajiri 2014 0 63 40 25 ND ND ND 108 20 ND ND NDTakada 2014 ND ND ND 86 476 122 91 523 252 107 184 350Tanioka 2014 16 226 124 ND ND ND ND 238 128 ND ND NDWang 2014 0 ND ND ND ND ND ND 213 96 ND ND NDAl-Tweigeri 2015 0 20 60 0 13 46 21 ND ND 0 32 48Bear 2015 ND ND ND ND ND ND ND 561 645 84 428 694Gonzalez-Angulo 2015 8 293 282 ND ND ND ND ND ND ND ND 452Ko 2015 ND ND ND 5 64 84 21 156 18 23 75 32Liu 2015 ND ND ND 14 69 18 7 67 41 4 39 65Mayer 2015 0 46 42 3 33 30 22 54 34 ND ND NDVillarreal-Garza 2015 ND ND ND 2 82 94 66 235 0 ND ND ND
21

Zelnak 2015 2 21 4 ND ND ND ND 14 13 2 19 6Gianni 2016 ND ND ND ND ND ND ND 293 123 ND ND NDLi 2016 ND ND ND 4 74 99 9 149 37 ND ND NDShao 2016 ND ND ND ND ND ND ND ND ND ND ND NDVillarreal-Garza 2016 ND ND ND 33 546 557 491 1487 149 215 443 918Zhang 2016 0 31 60 5 49 29 15 70 21 ND ND ND
C. Treatment
Author Year NA regimen(s)
NA HER2-directed therapy
Adjuvant chemotherapy
% Receiving adjuvant chemotherapy
Adjuvant HER2-directed therapy BCT
Mastec-tomy
Kuerer 1999 FAC No Some ND No 103 253
Chollet 2002AVCF/M, NEM, taxotere, TNCF, or NET No Some 22.7 No 280 116
Dieras 2004Doxorubicin/paclitaxel vs. doxorubicin/cyclophosphamide No Some ND No 107 85
Lee 2004 Docetaxel/cisplatin No Yes 100 No 1 55Ring 2004 Varied No No 0 No 165 270
Abrial 2005
Median 6 cycles (1-9) of anthracycline-based (73%), anthracyline/taxane (14%), or taxane alone (13%) No Some 17 No 470 186
Guarneri 2006 Varied No No 0 No 589 1142Hurley 2006 Docetaxel/cisplatin/traztuzumab Yes Yes 100 No ND NDAndre 2007 Paclitaxel/FAC No No 0 No ND NDEralp 2008 Anthracyclines +/- taxanes No No 0 No ND NDLiedtke 2008 Many regimens No Some 34 No 365 753
22

Al-Tweigeri 2009 Doxorubicin-->cisplatin/docetaxel No No 0 No 26 33Frasci 2009 Cisplatin/epirubicin/taxol No Yes 100 NA 50 24
Chang 2010Docetaxel/carboplatin +/- traztuzumab Some Yes 100 Yes 33 41
Chen 2010 VE, PCb, CEF +/-T, CTF No Some ND No ND NDJinno 2010 XD x 4 --> FEC x 4 No No 0 No ND NDKim 2010 Adriamycin/docetaxel No Yes 100 No 39 218Masuda 2010 FEC + taxane No ND ND No ND NDArun 2011 Many regimens +/- trastuzumab Some (76.7%) No 0 No 61 256
Fasching 2011Anthracycline +/- taxane-based regimens +/- trastuzumab, CMF Some ND ND Some ND ND
Wu 2011 Taxane + adriamycin or epirubicin No No 0 No 72 177Esserman 2012 AC +/- taxane +/- trastuzumab No (excluded) Some ND No (excluded) 92 123Im 2012 Taxol/gemcitabine/trastuzumab Yes No 0 Yes 42 11Melichar 2012 AT, ddAC-T, ddAC-TH Some (5.9%) No 0 No 176 153Yoo 2012 Many regimens +/- trastuzumab Some (14.9%) Some 22.8 Some 88 179Zhang 2012 TH (taxol or taxotere) or TCH Yes Some ND Yes 16 86
Guarneri 2013ET, GET, FEC, FEC-paclitaxel, +/- anti-HER2 therapies Some ND ND Some ND ND
Guiu 2013 Many regimens +/- trastuzumab Some (17.8%) Some ND Some 163 185
Hurley 2013Anthracycline/taxane-based plus cisplatin or carboplatin No Some ND No 11 127
Krishnan 2013 FEC+/-D, AC, ET, +/- trastuzumab Some (12.1%) Some 44.4 Some 69 296Marme 2013 Epirubicin/gemcitabine/docetaxel No No 0 No ND NDNatoli 2013 Many regimens + trastuzumab Yes Some 6.8 Some 97 108Cortazar 2014 Many regimens No Some 6.71 Some ND ND
de Azambuja 2014
Lapatinib vs trastuzumab vs Lapatinib/trastuzumab --> taxol + assigned anti-HER2 agent(s) Yes Some 90 Yes ND ND
23

Groheux 2014 EC-D, SIM No ND ND No 28 46Kawajiri 2014 FEC-D +/- trastuzumab Some (27.8%) No 0 Some ND ND
Takada 2014Anthracyclines +/- taxanes +/- trastuzumab Some (80%) Some 5.8 Yes 493 277
Tanioka 2014Anthracyclines +/- taxanes +/- trastuzumab Some Some 22 Some ND ND
Wang 2014 CE or ET No Some 80.9 No 21 285
Al-Tweigeri 2015FEC+cisplatin/docetaxel +/- trastuzumab Some (36.3) No 0 No 8 72
Bear 2015
Docetaxel-based (alone, + gemcitabine, +capecitabine) +/- bevacizumab -> AC No No 0 No ND ND
Gonzalez-Angulo 2015 TH-FEC Yes No 0 Some ND ND
Ko 2015AC, AT, AC-T, trastuzumab-based regimens Some (26.4%) ND ND ND 103 71
Liu 2015 Trastuzumab-based regimens Yes Some 8.3 Some 12 96Mayer 2015 TH or NH Yes Yes 100 Some 37 51
Villarreal-Garza 2015
Anthracycline/taxane-based plus trastuzumab Yes ND ND ND ND ND
Zelnak 2015Nab-paclitaxel-vinorelbine/trastuzumab Yes Some ND Yes ND ND
Gianni 2016 TH, THP, HP, TP Yes Yes 100 Yes ND ND
Li 2016PCb, docetaxel/carboplatin, CEF, VE No Yes 100 No 0 186
Shao 2016 E-CMF, D-FEC/FEC-D, ET, others No ND ND No ND NDVillarreal-Garza 2016 Many regimens ND ND ND ND 142 1494Zhang 2016 PCb vs. epirubicin/paclitaxel No Some ND No 12 75
24

Legend: NA, not applicable; ND, no data; ER+, estrogen receptor-positive; HR+, hormone receptor-positive; HER2+, human epidermal growth factor receptor 2-positive; TNBC, triple negative breast cancer; ND, no data; BCS, breast conservation surgery; FAC, 5-fluorouracil (5-FU), doxorubicin, and cyclophosphamide; AVCF/M, doxorubicin, vincristine, cyclophosphamide, fluorouracil, methotrexate; NEM, vinorelbine, epirubicin, methotrexate; TNCF, theprubicin, vinorelbine, cyclophosphamide, fluorouracil; NET, vinorelbine, epirubicin, paclitaxel; EXC, epirubicin, capecitabine, cisplatin; VE, vinorelbine plus epirubicin; PCb, paclitaxel plus carboplatin; CEF +/- T, cyclophosphamide, epirubicin, fluorouracil, +/- taxane; CTF, cyclophosphamide, pirarubicin, and fluorouracil; XD, capecitabine, docetaxel; FEC, 5-FU, epirubicin, cyclophosphamide; AC, doxorubicin/cyclophosphamide; AD, doxorubicin/docetaxel; CMF, cyclophosphamide, methotrexate, and fluorouracil; TCH, taxane, carboplatin, trastuzumab; AT, doxorubicin/paclitaxel; dd, dose-dense; AC-T, doxorubicin/cyclophosphamide, taxane; AC-TH, doxorubicin/cyclophosphamide, taxane/trastuzumab; TH, taxane/trastuzumab; ET, paclitaxel/epirubicin; GET, gemcitabine, epirubicin, docetaxel; NPLD, non-pegylated liposome-encapsulated doxorubicin; EC-D, epirubicin, cyclophosphamide, docetaxel; SIM, epirubicin, cyclophosphamide; vinorelbine/trastuzumab; THP, docetaxel/trastuzumab/pertuzumab; HP, trastuzumab/pertuzumab; TP, docetaxel/pertuzumab
Appendix
eAppendix 1: PubMed Search Strategy
(((((((((((((LBC OR LABC OR LLABC) OR (local OR localised OR localized OR locally)) AND breast neoplasms[mh])))) OR
25

((local OR localised OR localized OR locally) AND breast AND (cancer OR tumor OR tumors OR tumour OR tumours OR malignan* OR carcinoma OR cancer OR neoplasm OR neoplasms))) AND (("1900/01/01"[PDat] : "2016/08/31"[PDat]) AND English[lang])) OR (((breast neoplasms[MeSH Terms]) AND drug therapy[MeSH Subheading]) AND (("1900/01/01"[PDat] : "2016/08/31"[PDat]) AND English[lang])) OR ((("breast neoplasm"[Title] OR "breast neoplasms"[Title] OR "breast cancer"[Title] OR "breast carcinoma"[Title] OR "breast tumor*"[Title] OR "breast tumour*"[Title])) AND (("1900/01/01"[PDat] : "2016/08/31"[PDat]) AND English[lang]))) AND ((((Neoadjuvant Therapy[mh] OR neoadjuvant OR neo-adjuvant OR "neo adjuvant" OR preoperative care[mesh] OR preoperative period[mesh] OR "pre surgical" OR pre-surgical OR presurgical OR preoperative OR pre-operative OR "pre operative"))) AND (("1900/01/01"[PDat] : "2016/08/31"[PDat]) AND English[lang]))) AND (("1900/01/01"[PDat] : "2016/08/31"[PDat]) AND English[lang])) AND (((((pathology OR pathologic OR pathologically OR pathologies) AND ((complete* AND response*) OR (complete* AND respond*) OR (complete* AND remission)))) OR pCR) OR "Survival Rate"[Mesh] OR "Treatment Outcome"[Mesh] OR "Disease-Free Survival"[Mesh] AND (("1900/01/01"[PDat] : "2016/08/31"[PDat]) AND English[lang]))) AND (("1900/01/01"[PDat] : "2016/08/31"[PDat]) AND English[lang])) NOT ((((comment[Publication Type] OR case reports[Publication Type] OR letter[Publication Type] OR editorial[Publication Type] OR news[Publication Type])) OR (comment[Title] OR case report*[Title] OR letter[Title] OR editorial[Title] OR news[Title])) AND (("1900/01/01"[PDat] : "2016/08/31"[PDat]) AND English[lang]))
eAppendix 2: Supplementary Statistical Methods
S1. Model Specification
26

A Bayesian piecewise exponential proportional hazards model with study-specific random effects was used to describe the dependence of hazard functions on pCR status in each study. For simplicity, study effects where assumed to act proportionally on the baseline hazard, as in Model A of Crowther et al. (2012). Our modeling perspective is Bayesian because i) this approach is especially suited to computationally fit flexible hierarchical models and ii) it easily allows the propagation of uncertainty from model parameters to other quantities of interests (Berchialla et al. 2009).
In more detail, the model was specified as follows. First, the time-axis was partitioned in a finite number of intervals ( τ j−1 , τ j ], j=1 ,…, m+1, according to a sequence of cut-points τ 0=0<τ1<⋯< τm< τm+1=+∞. Following Broglio et al. (2016), we considered two initial cut-points at 6 months and 12 months of follow-up, followed by a sequence of 19 others equally spaced 12 months of follow-up, for a total of m=21 cut-points. Second, the hazard function λk ,i (t ) describing the distribution of event times (OR or RFS) for the i-th subject enrolled in the k-th included study was assumed to be constant over each interval ( τ j−1 , τ j ], where
λk ,i (t )=l0 , j ⋅exp (α k+θk ⋅ pCRk ,i )
for all t∈ (τ j−1, τ j ], where:
l0 , j is the constant value of the baseline hazard in the interval ( τ j−1 , τ j ]. pCRk ,i is the pCR indicator (1 for pCR, 0 for RD) for the i-th subject in the k-th trial. θk∼N (μθ , σθ
2) is the (independent) random effect describing the effect of pCR in the k-th study. The value θk equals the log-hazard ratio measuring the association between pCR and the clinical outcome (OS or RFS) in the k-th study.
α k∼N (μα , σ α2 ) is the (independent) random effect for the k-th study; α k is the log-hazard ratio describing the effect of the k-th
study on the distribution of event times; to avoid identifiability, a study was chosen as reference and its log-hazard rate α 0 was fixed to α 0=0. Similarly as in Broglio et al. (2016), the largest study included in the analysis, i.e. the study of Cortazar et al. (2014), was chosen as reference.
In a random effect meta-analytic model, the included studies are considered a random sample from a larger hypothetical population of studies (Borenstein et al. 2010). The parameter μθ is the mean of the distribution of random effects for pCR in this hypothetical
27

population. In other words, μθ is the average log-hazard ratio measuring the effect of pCR. Similarly, the parameter μα is the mean of the distribution of random study effects and so it represents the average log-hazard ratio measuring the change in hazards between the considered study and the one chosen as reference. The variances σ θ
2 and σ α2 determine the dispersion of random effects from their mean
and so determine the heterogeneity of effects across different studies.
Proceeding in the Bayesian framework, all model parameters were assigned a prior distribution. For all parameters, we considered weakly informative distributions as done by Broglio et al. (2016) to let the data drive our inferences. Specifically, a diffuse N (0,100) prior was assigned to μθ and μα, independently. An inverse gamma prior distribution with shape parameter 1 and scale parameter 0.5 (yielding a distribution centered at 1 and with infinite variance) was instead assigned to σ θ
2 and σ α2, independently. Lastly, each l0 , j was
independently assigned a gamma prior distribution with shape parameter 0.01 and rate parameter 0.01.
S2. Model Implementation
The model described in Supplementary Section S1 was implemented in R (v. 3.5.1) using the STAN probabilistic programming language (http://mc-stan.org/) using a Poisson formulation of the likelihood function (Crowther et al. 2012). Specifically, using the RSTAN (v. 2.17.3) R library, 2000 values were sampled (via Hamiltonian Monte Carlo) from the posterior distributions of the model’s parameters, the first 1000 were discarded as burn-in, and the remaining 1000 were retained for inference. Convergence of the Monte Carlo chains was assessed by visual inspection of the trace plots (data not shown). The STAN code used to implement the analysis is attached below:
library(rstan)
modelcode <- "data { int<lower=0> K; // number of time intervals int<lower=0> N; // number of subjects int<lower=0> S; // number of studies row_vector<lower=0,upper=1>[K] ev[N]; // event indicator row_vector<lower=0>[K] pt[N]; // person time at risk
28

vector[N] pCR; // pCR values matrix<lower=0,upper=1>[N,S] study; // study indicators}parameters { vector<lower=0>[K] lambda; // baseline hazards vector[S] z_theta; // standardized study-specific pCR effect vector[S] z_alpha; // standardized study effects real mu_alpha; // mean of study-specific random effects real<lower=0> sigma2_alpha; // between-studies variance real mu_theta; // mean pCR effect real<lower=0> sigma2_theta; // between-study variance of pCR effects}transformed parameters { vector[N] linpred; // linear predictors vector[K] loglambda; // baseline hazards real<lower=0> sigma_alpha; // between-studies standard deviation vector[S] alpha; // study random effects real<lower=0> sigma_theta; // between-study standard dev. of pCR effects vector[S] theta; // study pCR random effects sigma_alpha = sqrt(sigma2_alpha); sigma_theta = sqrt(sigma2_theta); alpha = sigma_alpha*z_alpha + mu_alpha; theta = sigma_theta*z_theta + mu_theta; linpred = (study*theta) .* pCR + study*alpha; loglambda = log(lambda);}model {// log-likelihood contributionsfor(i in 1:N){ target += ev[i]*(loglambda + linpred[i]) - pt[i]*exp(loglambda + linpred[i]);}
// priorlambda ~ gamma(0.01,0.01);z_alpha ~ normal(0,1);mu_alpha ~ normal(0,10); // standard deviation=10sigma2_alpha ~ inv_gamma(2,1);z_theta ~ normal(0,1);
29

mu_theta ~ normal(0,10); // standard deviation=10sigma2_theta ~ inv_gamma(2,1);}"
cmpl_model <- stan_model(model_code = modelcode)
S3. Construction of a Single-Study Survival Curve
From the posterior samples obtained as described in Supplementary Section S2 above we estimated survival functions (with 95% pointwise probability intervals) for the pCR and the RD groups representative of an hypothetical study where the random effects are fixed to the average of their distribution. Specifically, these were obtained as follows. First, from the posterior samples of the model parameters, a corresponding posterior sample of the hazard function
λ pCR (t )=l0 , j exp ( μα+μθ ) (t ∈ ( τ j−1 , τ j ] )
for the pCR group and λRD (t )=l0 , jexp ( μα ) ( t∈ ( τ j−1 , τ j ])
for the RD group were obtained. Second, a posterior sample of the associated survival functions SpCR (t) and SRD(t) was obtained through the integral transformations
SpCR ( t )=exp¿¿
SRD ( t )=exp ¿¿
These are available in closed form given the simple structure of the piecewise exponential model. In fact, from a simple calculation it is possible to obtain that
SpCR ( t )=exp (−∑τ j−1≤ t
l0 , j ⋅exp ( μα +μθ ) ⋅min (t−τ j−1 , τ j−τ j−1 ))
30

SRD ( t )=exp(−∑τ j−1 ≤t
l0 , j ⋅exp ( μα ) ⋅min (t−τ j−1 , τ j−τ j−1 ))Lastly, the mean and 2.5% and 97.25% percentiles of the resulting posterior samples of SpCR (t) and SRD(t), over a fixed grid of values for t , were obtained, respectively yielding the posterior estimate and lower and upper 95% probability limits for the survival curves.
S4. Incremental Effect of changes in pCR on the Hazard
Figures 4A-B were created following the approach of Berry and Hudis (2015). This produces hypothetical survival curves representative of treatment effects under the assumption that the only effect of treatment is move a certain proportion of patients from the RD group to the pCR group. Assuming that i) the difference in proportion of pCR patients in the treatment arm versus the control arm is equal to Δ (0 ≤ Δ≤ 1) and ii) that, as done by Berry and Hudis (2015), the proportion of pCR patients in the control group is 50%, then these hypothetical survival curves for the treatment (T) and control (C) group are given by
ST , Δ (t )=(0.5+ Δ2 )SpCR (t )+(0.5− Δ
2 )SRD (t )
and
SC ( t )=0.5 S pCR (t )+0.5 SRD ( t ) .
The hazard ratio HR Δ measuring the effect of a treatment producing a change equal to Δ in the proportion of pCR patients across study arms is obtained as
HR Δ=−log (ST , Δ (τ m ))/τ m
−log (SC (τm ) )/τm
31

assuming an exponential distribution in both arms.
To prepare Figures 4A-B, the single-study survival curves from Supplementary Section S3 were used for SpCR (t ) and SRD ( t ). The posterior distribution of HR Δ for different fixed values of Δ was approximated from the posterior samples of SpCR ( t ) and SRD ( t ). The mean 95% probability interval of these distributions were then plotted as a function of Δ.
Bibliography
Crowther MJ, Riley RD, Staessen JA, Wang J, Gueyffier F, Lambert PC. Individual patient data meta-analysis of survival data using Poisson regression models. BMC Medical Research Methodology 12:34, 2012
Berchialla P, Baldi I, Notaro V, Barone‐Monfrin S, Bassi F, Gregori D. Flexibility of Bayesian generalized linear mixed models for oral health research. Statistics in medicine 28:3509-22, 2009.
Borenstein M, Hedges LV, Higgins JP, Rothstein HR. A basic introduction to fixed‐effect and random‐effects models for meta‐analysis. Research synthesis methods 1:97-111, 2010.
Broglio KR, Quintana M, Foster M, Olinger M, McGlothlin A, Berry SM, Boileau JF, Brezden-Masley C, Chia S, Dent S, Gelmon K. Association of pathologic complete response to neoadjuvant therapy in HER2-positive breast cancer with long-term outcomes: a meta-analysis. JAMA Oncology 2:751-60, 2016
Cortazar P, Zhang L, Untch M, et al: Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. The Lancet 384:164–172, 2014
Berry DA, Hudis CA. Neoadjuvant therapy in breast cancer as a basis for drug approval. JAMA Oncol 1:875-876, 2015.
32