Embed Size (px)
Citation preview

Review Article · Übersichtsarbeit
Forsch Komplementmed 2011;18:176–184 Published online: August 1, 2011
DOI: 10.1159/000330725
© 2011 S. Karger GmbH, Freiburg1661-4119/11/0184-0176$38.00/0
Accessible online at: www.karger.com/fok
Fax +49 761 4 52 07 [email protected]
Jann Arends, MDTumor Biology Center at Freiburg UniversityBreisacher Straße 117, 79106 Freiburg, GermanyTel. +49 761 206-1801, Fax [email protected]
Vitamin D in OncologyJann Arends
Tumor Biology Center, Freiburg University, Freiburg i.Br., Germany
KeywordsCancer · Neoplasms · Vitamin D · Mortality · Immunocompetence · Lymphoma · Palliative care
SummaryThe vitamin D system has been strongly conserved in evolution. It links sun exposure to a multitude of endo-crine messages. In most body cells the active hormone calcitriol binds intracellularly to the vitamin D receptor and regulates the expression of specific gene products. Vitamin D deficiency is epidemic affecting some 1 billion people worldwide and is mainly caused by chronically inadequate sun exposure. This deficiency is associated with harmful effects on almost all tissues including a predisposition to cancer. In cancer patients vitamin D de-ficiency is associated with a worsening of the prognosis. The active hormone calcitriol has anti-tumor activity and is being investigated as an anticancer agent. There is general agreement that exposure to sunlight should be increased while carefully avoiding UV erythema. In addi-tion, recent suggestions call for a health-promoting die-tary intake of 25–100 g (1,000–4,000 IU) of vitamin D3. While supplements of vitamin D improve musculoskele-tal symptoms, proof is still lacking that these doses con-vey a protection from cancer. Interventional studies that administer vitamin D versus placebo in patients with cancer should be a high priority because of the hypothe-sized benefits and the low risk of supplementation with vitamin D.
SchlüsselwörterKrebs · Neoplasmen · Vitamin D · Sterblichkeit · Immunkompetenz · Lymphom · Palliativpflege
ZusammenfassungDas Vitamin-D-System ist in der Evolution seit 500 Milli-onen Jahren etabliert und koppelt bei Wirbeltieren Sonnenexposition an eine Vielzahl endokriner Wirkun-gen. Das aktive Hormon Calcitriol bindet in den meisten Körperzellen intrazellulär an den Vitamin-D-Rezeptor und reguliert die Expression spezifischer Genprodukte. Niedrige Vitamin-D-Spiegel sind epidemisch und betref-fen weltweit etwa 1 Milliarde Menschen; Ursache ist vor allem eine unzureichende Sonnenexposition. Dieser Mangel führt zu Dysfunktionen diverser Gewebe und ist mit einem erhöhten Tumorrisiko assoziiert. Bei Tumor-patienten geht ein Vitamin-D-Mangel mit einer schlech-teren Erkrankungsprognose einher. Calcitriol besitzt eine antitumorale Aktivität und wird in dieser Hinsicht auf seine klinische Wirksamkeit untersucht. Aktuell werden zur Normalisierung der Vitamin-D-Versorgung allgemein eine vorsichtige Steigerung der Sonnenexpo-sition unter Vermeidung von UV-Erythemen sowie von einigen Experten eine Tagesaufnahme von 25–100 g (1000–4000 IU) Vitamin D3 empfohlen. Während eine positive Wirkung von Vitamin-D3-Supplementation auf das muskuloskeletale System akzeptiert ist, besteht noch keine Sicherheit bezüglich der Prävention von Tumorerkrankungen. Qualitativ hochwertige interven-tionelle Studien zur Wirkung von Vitamin D bei onko-logischen Patienten sollten wegen der potentiellen Vor-teile und der guten Verträglichkeit mit hoher Priorität gefördert werden.

Forsch Komplementmed 2011;18:176–184Vitamin D in Oncology 177
nuclear receptor family of transcription factors; upon acti-vation by vitamin D the VDR forms a heterodimer with the retinoid-X receptor and binds to hormone response elements on DNA resulting in expression or transrepression of specific gene products [7]. It is now recognized that most cells in the body have a vitamin D receptor as well as the capacity of pro-ducing calcitriol, which in turn is capable of regulating a wide variety of genes that have important functions in regulating cell growth and modulating immune function and cardiovas-cular health [5].
Vitamin D DeficiencyThere has been an intensive debate regarding optimal vitamin D levels in the blood. Most authors agree that 25-hydroxyvita-min D3 levels below 50 nmol/l (20 ng/ml) should be consid-ered inadequate [8, 9], but this has been challenged by others [5, 10]. Physiological arguments support a target level of 25-hydroxyvitamin D above 75 nmol/l (30 ng/ml). This is based on the observations that intestinal calcium absorption is maximized above 80 nmol/l and that parathyroid hormone concentrations in adults continue to decline and reach a nadir at vitamin D levels of 75–100 nmol/l [11]. Vitamin D intoxica-tion typically does not occur until 25-hydroxyvitamin D con-centrations are above 375 nmol/l [11]. These arguments are supported by epidemiologic data that associate vitamin D lev-els below 75 nmol/l with increased morbidity [5]. Accordingly, it has been proposed to define vitamin D insufficiency and deficiency as a 25-hydroxyvitamin D level below 75 or below 50 nmol/l, respectively (fig. 2) [5]. Inadequacy of vitamin D is epidemic. In Europe more than 40% of young adults, 8–60% of healthy elderly, and 70–100% of institutionalized elderly have 25-hydroxyvitamin D levels below 25 nmol/l during the
Introduction
During the last century the therapy of cancer has focused on increasingly tailor-made as well as personalized concepts and attempts to remove or destroy malignant tissues. The aim of curing the disease, however, is still only achieved in approxi-mately 50% of all cases [1], and the cancer rate is increasing due to our aging populations [2]. The complex processes of cancerous growth have not yet been elucidated in full detail, and there is a constant addition of new information and in-sights regarding the molecular, biological, immunological, and metabolic hallmarks of cancer, cancer progression and the formation of metastases as well as approaches to prevent or inhibit tumor growth. The vitamin D system is an exciting ex-ample of a newly appreciated biological target for influencing the inhibition of tumor growth and improving the well-being of cancer patients.
Vitamin D in Oncology
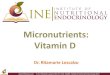
Vitamin D SystemThe vitamin D system has been conserved in evolution for more than 500 million years. While the role of vitamin D in lower life forms is not well understood, vitamin D evolved into an endocrine messenger in vertebrates which are criti-cally dependent on an adequate source of vitamin D – either from exposure to sunlight or from the diet [3]. Vitamin D3 (cholecalciferol or calciol) is synthesized in the skin from 7-dehydrocholesterol (7-DHC) by a UVB-induced photo-chemical reaction producing previtamin D which in turn rapidly isomerises to calciol. With prolonged solar exposure previtamin D forms inert metabolites or is changed back to 7-DHC (fig. 1) so that toxicity from sun exposure is not a con-cern [4]. Rich dietary sources of vitamin D include cod, beef or chicken liver, cold water fish, egg yolk, and milk. Vitamin D deficiency is often unrecognized in adults who are not ex-posed to adequate sunlight and this can exacerbate osteo-porosis and cause the painful bone disease osteomalacia [3]. More recently, vitamin D deficiency has been linked to an in-creased risk for many chronic diseases including cancer [5]. After exposure to sunlight newly formed vitamin D circulates with a half-life of around 20 h [6] before being hydroxylysed in the liver to 25-hydroxyvitamin D3 (calcidiol) (fig. 1). Bound to vitamin D-binding protein, calcidiol circulates in the blood with a half-life of some 3 weeks to 3 months [6], thus serving as a long-term inactive storage form. The biologically active form of vitamin D3 is finally produced in the kidney and many other tissues by a second highly regulated hydroxylation lead-ing to 1,25-dihydroxyvitamin D3 (calcitriol) [4]. Calcitriol interacts with its vitamin D receptor in specific effector tissues to regulate calcium metabolism and bone health [5]. It has a short half-life and is deactivated by a 24-hydroxylase. The vi-tamin D receptor (VDR) is a member of the steroid-binding
Fig. 1. Simplified flow chart of the synthesis and inactivation of vitamin D3. UVB from sunlight produces provitamin D from 7-DHC. Provitamin D converts spontaneously to vitamin D or if exposed to further sunlight reverts back to 7-DHC or is converted to other inactive compounds. Vita-min D3 is hydroxylated at position 25 by the liver to a storage form with a long half-life and finally activated in the kidneys and many other tissues by another hydroxylation at position 1 to a short-lived hormone interact-ing with the vitamin D receptor. Inactivation occurs by further hydroxyla-tion at position 24 (7-DHC = 7 dehydrocholesterol; pD3 = provitamin D3; D3 = calciol; 25OH-D3 = 25-hydroxyvitamin D; 1,25OH-D3 = 1,25-dihy-droxyvitamin D3; 1,24,25OH-D3 = 1,24,25-trihydroxyvitamin D3; VDR = vitamin D receptor; tH = half-life).

178 Forsch Komplementmed 2011;18:176–184 Arends
of vitamin D raises serum 25-hydroxyvitamin D concentra-tions by approximately 1 ng/ml, some experts have suggested a health-promoting dietary intake of up to 100 g (4,000 IU) of vitamin D per day [10] (fig. 3).
Clinical Effects of Vitamin D DeficiencyVitamin D exerts physiological effects on many tissues and organs (table 1); this includes muscle function, bone density [19], insulin sensitivity [20], immunocompetence [14], neuro-cognition, and mental health [14, 21]. Consequently, during the last years inadequate and deficient levels of vitamin D have been associated with a large number of epidemiologi-cally relevant adverse clinical outcome parameters (table 1). Several of these associations are of special importance to cancer patients since they may aggravate tumor-induced or treatment-related problems. Weakness of bones and muscles may increase cancer-associated fatigue, the risk of falling, and the risk of fractures, thus increasing morbidity and re-striction of mobility. Clinical depression may diminish the ability of coping with the subjective burden of cancer diag-nosis and progression, while vitamin D-associated con-straints on cognition may augment preexisting fatigue and opioid-induced effects on cognitive functioning. While asso-ciation of vitamin D deficiency with deficits in organ func-tion is gaining credibility, there is still only scarce evidence for beneficial effects of vitamin D supplementation [4, 8, 22–24]. This may be due to the often small supplemental doses of vitamin D used. Treatment studies addressing vita-min D-associated organ dysfunctions in cancer patients are lacking. Well conducted trials on the effects of vitamin D supplementation in vitamin D-deficient cancer patients, therefore, are eagerly awaited.
Vitamin D and Cancer IncidenceIn 1941, Apperly [25] reported that cancer mortality in North America correlated inversely with sun exposure; mortality in states with the highest solar radiation index was some 50% of that in states with the lowest index. He suggested that cancer deaths may be reduced by exposure of the skin to sunlight. In 1980, Garland and Garland [26] proposed vitamin D to be a protective factor against colon cancer. Comparing cancer mortality rates in the USA, several groups found that solar
winter season [12] and thus should be considered vitamin D deficient. It is estimated that 1 billion people worldwide have vitamin D levels below 75 nmol/l [5]. A variety of factors influ-ence the cutaneous production of vitamin D including the time of day, season, latitude, degree of skin pigmentation, sunscreen use, and aging [13]. The skin has a large capacity to produce vitamin D. Adults exposing their whole body to sun-light to cause a light pinkness of their skin 24 h later (the mini-mal erythemal dose) produce an amount that is equivalent to the ingestion of 500 g (20,000 IU) of vitamin D [14] (fig. 3). In healthy subjects living under sun-rich conditions, the meas-ured vitamin D levels in the blood usually are above 100 ng/ml and below 200 ng/ml. This appears to correspond best to the situation in our early ancestors, suggesting that evolution has effectively designed us to live in the presence of far more vitamin D than what current levels amount to today [15]. On the other hand, for subjects living above 35° Northern latitude (North Africa), vitamin D is produced in the skin only from April through September between 10 am and 3 pm; a sun-screen with protection factor of 30 reduces vitamin D produc-tion by 95%; subjects with dark skin color often require 5–10 times longer exposure to produce an adequate amount of vita-min D in their skin; and a 70-year-old person produces about 25% of the amount of vitamin D that a 20-year-old person can produce [14]. Ethnicity also influences vitamin D levels in dif-ferent populations [16]. Since sun exposure is inefficient for adequate vitamin D levels in many people and since with few exceptions there is little or no vitamin D in the food that hu-mans normally eat [15], dietary supplements have been sug-gested since the 19th century, first using cod liver oil, later ir-radiated milk, and finally synthetic vitamin D [11]. The daily requirement has been set at 5–10 g (200–400 IU) of vitamin D by the German, Austrian and Swiss Nutrition Societies (DACH) [17] (fig. 3), and at 15–20 g (600–800 IU) by the Institute of Medicine [18]. Based on the data reviewed above and on the observation that dietary intake of 100 IU (2.5 g)
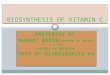
Fig. 2. Classification of 25-hydroxyvitamin D3 blood concentrations. While levels below 50 nmol/l are generally accepted as inadequate, there is an ongoing debate whether levels between 50 and 75 nmol/l should be considered adequate [9] or inadequate [10]. 70% of Central Europeans have yearly average values below 50 nmol/l [96].
Fig. 3. Suggestions for daily vitamin D requirements. A = daily dietary requirement according to DACH (5–10 g = 200–400 IU) [17] or recom-mended daily allowance according to IOM (15–20 g = 600–800 IU) [9]; B = daily dose to maintain plasma levels above 100 nmol/l and requirement according to several expert groups [6, 10, 97}; C = equivalent dose pro-duced by whole body exposure to minimal erythemal dose [14].

Forsch Komplementmed 2011;18:176–184Vitamin D in Oncology 179
oping pancreatic cancer when the total dietary vitamin D intake was above 300 IU (7.5 g) per day.
Associations between vitamin D status and colorectal or breast cancers have been reported by several groups. Gar-land et al. [44] using data of a 19-year observational study found a significant correlation between calculated dietary vitamin D and the risk of developing colorectal cancer. The same group reported for colorectal cancer a risk reduction of 50% for a daily intake of 1,000 IU of vitamin D or for blood levels above 30 ng/ml (75 nmol/l) [45, 46]. Two reviews on 17 and 29 studies, respectively, reported a protective effect of vitamin D levels against colorectal adenoma [47] and against colorectal cancer [48]. Recent data from the European EPIC study confirmed that circulating vitamin D levels in the high-est versus the lowest quintile reduced the risk of colorectal cancer by 40% [49]. While several studies report a reduction in the incidence of breast cancer in women with high com-pared to low vitamin D levels [50–55], there are negative reports from other studies [56–57]. In 579 women with inci-dental breast cancer compared to 574 matched controls, Yao et al. [55] observed lower vitamin D levels; and low levels of vitamin D were correlated with higher histological grade, negative estrogen receptor, and higher odds of having triple-negative cancer.
UVB radiation was associated with the incidence or mortality in 15 different types of cancer [27–29]. Grant [30] reported that most of these associations satisfied strict criteria of cau-sality, and he suggested to increase sun exposure and to use vitamin D3 supplementation [27]. Garland [31] analyzed 63 observational studies and reported that the majority found a protective relationship between sufficient vitamin D status and lower risk of cancer. Analyzing data from the Health Professionals Follow-Up Study, Giovannucci et al. [32] con-cluded that an increment of 25 nmol/l (10 ng/ml) in predicted vitamin D levels would reduce the cancer incidence by 17% and cancer mortality by 29%.
Ecological studies comparing sun exposure with cancer-specific mortality rates in 175 countries revealed that cancer risk increases with geographical latitude and that UVB irra-diation protects against melanoma [33], malignant lymphoma [34, 35], and cancer of the lung [36], ovaries [37], brain [38], bladder [39], prostate [40] and pancreas [41]. Since dietary calcium decreases the formation of calcitriol, the epidemio-logic association of high calcium intake and higher incidence of prostate cancer has been interpreted as indirect evidence for a protective influence of vitamin D3 on prostate cancer [42]. Analyzing data from 2 large observational studies, Skin-ner et al. [43] calculated a 40% reduction in the risk of devel-
Parameter References
Overall mortality [8, 22]Bone and muscle systems [19]
Risk of fallingBone density, risk of fracturesMuscle weakness
Lung diseaseSeverity of chronic obstructive pulmonary disease (COPD) [98, 99]Incidence of asthma [99]
Metabolic derangementsHypertension [100]Cardiovascular disease [101]Cardiovascular mortality [22, 102]Metabolic syndrome [20]Type 2 diabetes [103]
Immune responsesCytokine crosstalk, inflammatory response (increase in Th1/Th2 ratio) [14, 104]Defects in antimicrobial activity (including against Mycobacterium
tuberculosis)[14, 105, 106]
Reactivation of tuberculosis [107]Autoimmune diseases [14]Type 1 diabetes [108, 109]Rheumatoid arthritis [110]Relapse rate in multiple sclerosis [111]
Mental diseasesDepression [112]Neurocognitive defects [113]Alzheimer’s disease, dementia [14, 114]Schizophrenia [115]
Tab. 1. Non-oncologic outcomes associated with vitamin D deficiency

180 Forsch Komplementmed 2011;18:176–184 Arends
Anti-Tumor Activity of Vitamin DCalcitriol and analogues inhibit the growth of several malig-nant cell lines in vitro and in vivo [65] (table 2). This includes cancer cell lines of the prostate [66], lung [66], pancreas [67–69], liver [70], kidney [71], bladder [72], ovaries [73], as well as melanoma [74, 75], myeloma [66] and tumor-derived murine endothelial [76] cells. In addition, calcitriol has been shown to enhance the anti-tumor activity of several chemo-therapeutic agents, including cisplatin and gemcitabine [67, 72] as well as the cytotoxic effects of gamma irradiation [65, 77]. Interestingly, glucocorticoids enhance the anti-tumor effects of calcitriol [66]. The effects induced in malignant cells differ from those in non-malignant cells [72–74, 76]. The ob-served mechanisms of anti-tumor activity include anti-pro-liferative and apoptotic effects [71], inhibition of cell cycle progression [66, 71, 76], induction of p27 [66, 76], p73 [72] and p38 MAPK expression [73], and cleavage of caspases [66]. Calcitriol also exerts potent anti-inflammatory and anti-ang-iogenic effects resulting in inhibition of tumor angiogenesis, invasion, and metastasis [78]. Considering these effects, vita-min D and analogues have been proposed as chemopreven-tive and as anti-tumor agents [65, 78, 79]. Preclinical data sug-gest that high exposure to calcitriol is necessary for anti-tumor effects, and clinical data show that high doses can be adminis-tered safely [79]. Early clinical trials, however, have been negative or inconclusive [80, 81], and further well designed trials are needed to clarify the potential role of vitamin D as an anti-cancer drug [65, 79].
Prognostic Effects of Vitamin D in Human CancersVitamin D has anti-proliferative and apoptotic effects, some data suggest that vitamin D may be more strongly related to cancer progression than to incidence, and most cancer pa-tients are vitamin D deficient [29, 82, 83]. Therefore, vitamin D levels may be prognostic in cancer patients. Many breast cancer patients have very low vitamin D levels which decrease further during chemotherapy treatment [83–87]. In a cohort of 512 women with early breast cancer, only 24% had adequate vitamin D levels. Women with well-differentiated G1 cancers had significantly higher vitamin D levels than women with undifferentiated G3 tumors. During a mean follow-up of 11.6 years, 116 women had distant recurrence and 106 women died. Women with inadequate vitamin D levels below 50 nmol/l had an almost two-fold risk of distant recurrence and death compared to those with sufficient vitamin D levels [85].
Prospective examination of the association between pre- diagnostic 25-hydroxyvitamin D levels and mortality among 304 participants in the Nurses Health Study and the Health Profes-sionals Follow-Up Study diagnosed with colorectal cancer re-sulted in an improved survival with high vitamin D levels. Overall survival (OS) for participants with vitamin D levels in the highest versus the lowest quartile was improved by a factor of 2 [88]. A post-diagnosis analysis of predicted 25-hydroxy-vitamin D levels in a larger cohort (n = 1,017) of the same
While the evidence from observational studies is accumu-lating, there are few interventional studies. Most importantly, up to now no large randomized study dealing with vitamin D has been published with cancer as a pre-specified primary outcome parameter [9]. A large (n = 36,282) randomized trial of 7 years of supplemental calcium (1,000 mg) and vitamin D (400 IU = 5 g) per day did not affect the risk of breast cancer [58] or colorectal cancer [59]. The supplemental dose of vita-min D, however, was low. In a randomized study in 1,179 postmenopausal women, daily supplementation for 4 years with 1,500 mg calcium plus 1,100 IU (27.5 g) vitamin D3 resulted in a significant reduction of total cancer incidence compared to placebo [60]. Using a modeling approach, Grant et al. [61] suggested that a daily intake of 1,000 IU of vitamin D might decrease the total cancer mortality in Western Eu-rope by 14–20%. More critical reviews, however, have high-lighted the lack of good quality studies and the possibility of publication bias. Thus, Rhee et al. [62] concluded that sun-light most probably is protective against cancer but that avail-able evidence might only support a protection by vitamin D levels against colorectal but not against other cancers. Simi-larly, in a meta-analysis of 35 studies, Gandini et al. [63] con-cluded that an increase in vitamin D levels only reduces the risk of colorectal cancer but not that of breast or prostate cancer. Other critical voices have drawn attention to the fact that no cause-effect relationship has yet been established for the role of vitamin D in preventing cancer [9]. The available studies are limited by potential confounding factors asso ciated with low vitamin D levels, such as obesity (increasing vitamin D sequestration), lack of physical activity (limiting outdoor activity), skin pigmentation (affecting vitamin D synthesis), diet or supplementation practices, and social status (with effects on outdoor activity, obesity, dietary habits) [9]. These authors caution that several observational and interventional studies did not report any association of vitamin D levels or supplementation with cancer incidence and that there is some evidence for an increased risk of pancreatic cancer with very high 25-hydroxyvitamin D3 levels above 100 nmol/l [64].
Tab. 2. Preclinical anti-tumor effects of calcitriol and analogues: suscep-tible cell types
Cell type References
Prostate cancer cells [66]Lung cancer cells [66]Pancreatic carcinoma cells [66–69]Rat ascites hepatoma cells [70]Melanoma cells [74, 75]Kidney cancer cells [71]Bladder cancer cells [72]Tumor-derived murine endothelial cells [76]Myeloma cells [66]Ovarian cancer cells [73]

Forsch Komplementmed 2011;18:176–184Vitamin D in Oncology 181
tamin D3 [95]. While waiting for the results of prospective randomized trials to determine the benefit of elevating vita-min D levels above 75 nmol/l, no general recommendation to use supplements in this situation can be made. If marginally low levels (below 75 nmol/l) are found, an effort to carefully increase UVB exposure from sunlight may be made, prefer-ably by increasing outdoor activity. UV erythema and sun-burns, however, should be avoided at all costs. Outdoor activity may combine vitamin D production with the benefits of physical exercise on strength, endurance, body composi-tion, and insulin sensitivity. A general recommendation is 15–20 min of daily sun exposure without the use of sun-screens. However, local and individual factors need to be considered, like latitude, season, time of day, as well as skin pigmentation. It is mandatory to take into consideration the increased susceptibility to skin damage by radiotherapy as well as anticancer medications (especially fluorouracil and epidermal growth factor receptor antagonists) and other drugs. The simplistic argument of whether sun exposure in-creases the risk of melanoma or protects against cancer needs to take into account the evidence suggesting protective effects of sun exposure and higher vitamin D3 levels against melanoma [33, 90]. If vitamin D levels are below 50 nmol/l, dietary advice may be given to increase the intake of fatty fish such as salmon, tuna, and mackerel (100–400 IU per serving), and possibly cheese and eggs (5–40 IU per serving). Intake of fish liver oil may be suggested (1,000 IU per tablespoon). If levels are well below the target range (e.g. <25 nmol/l), substi-tution is indicated to treat vitamin D deficiency [95]. Deficient subjects should be treated with high-strength calciferol (i.e. 100–200 g/day or 1,000 g/week) for 8–12 weeks, followed by evaluation of vitamin D status and regular vitamin D supple-ments (1,000 IU/day). If there is no response of vitamin D lev-els to supplementation, malabsorption should be considered.
Conclusion
Low vitamin D3 levels are epidemic and mainly caused by inadequate exposure to sunlight. This inadequacy has harmful
studies yielded a similar result; higher predicted 25-hydroxy-vitamin D levels were associated with a significant reduction in colorectal cancer-specific and overall mortality [89].
In a cohort of 872 patients with early melanoma, higher 25-hydroxyvitamin D3 levels were associated with lower Bres-low thickness at the time of diagnosis and with a lower risk of tumor relapse and death [90] (table 3). Drake et al. [91] com-pared vitamin D levels obtained within 120 days of diagnosis to event-free survival (EFS) and OS in 370 patients with dif-fuse large B-cell lymphoma (DLCL) and 70 patients with T-cell lymphoma (TCL). Taking the Inter national Prognostic Index (IPI) into account, inadequate 25-hydroxyvitamin D levels below 25 ng/ml (62.5 nmol/l) were associated with a worse EFS and OS in both lymphoma subgroups [91] (table 4).
Vitamin D in Supportive and Palliative CareVitamin D inadequacy is pandemic among rehabilitation pa-tients affecting male and female patients of all ages and ethnic backgrounds [92]. In 267 patients with chronic pain using opi-oids, Turner et al. [93] reported that patients with inadequate vitamin D levels below 50 nmol/l compared to those with adequate levels required a much higher average opioid equi-valent dose and longer treatment. Vitamin D deficiency causes osteopenia, exacerbates osteoporosis, causes painful osteomalacia, and aggravates proximal muscle strength and postural sway [92]. These pathologies should be considered in the differential diagnosis of patients with musculoskeletal pain, fibromyalgia, chronic fatigue syndrome or myositis, and should lead to the assessment and optimization of the vitamin D status. Vitamin D levels are low in the majority of breast cancer survivors [85–87]. This is associated with bone mineral density and may increase bone loss, joint symptoms, and fractures in postmenopausal women receiving aromatase in-hibitors for treating early breast cancer [84, 94]. Arthralgia induced by aromatase inhibitors was significantly attenuated by raising vitamin D levels above 40 ng/ml (100 nmol/l) by supplementation with vitamin D [86].
Recommendations for the Normalization of Vitamin D Levels in Cancer PatientsSince inadequate vitamin D levels are common, vitamin D status should be determined by assay of serum 25-hydroxyvi-
Tab. 3. Association of vitamin D levels and prognosis in melanoma patients [90]
n Relapse rate, %
RFS (HR)
VD-deficient (<41.3 nmol/l) 231 22VD-sufficient (>61.4 nmol/l) 260 13 0.79*
* Significantly different from 1. RFS = Relapse-free survival; HR = hazard ratio; VD = 25-hydroxyvitamin D.
Tab. 4. Association of vitamin D levels and prognosis in lymphoma patients [91]
n EFS (HR) OS (HR)
DLCL (n = 370)VD-deficient (< 24 ng/ml) 192 1.41 1.99*
TCL (n = 70)VD-deficient (< 24 ng/ml) 40 1.94* 2.38*
* Significantly different from 1. EFS = Event-free survival; OS = overall survival; HR = hazard ratio; VD = 25-hydroxyvitamin D; DLCL = diffuse large B-cell lymphoma; TCL = T-cell lymphoma.

182 Forsch Komplementmed 2011;18:176–184 Arends
without a supplement. While supplements of vitamin D im-prove musculoskeletal symptoms, proof is still lacking that these doses convey a protection from developing cancer. In-terventional studies that administer vitamin D versus placebo in patients with cancer are of high priority because of the hypothesized benefits and the low risk of dietary supplemen-tation with vitamin D.
Disclosure Statement
There is no conflict of interest.
effects on almost all tissues and is associated with a predis-position to cancer. In cancer patients, vitamin D deficiency is associated with an inferior prognosis. At the same time, the active hormone calcitriol has anti-tumor activity and is being investigated as an anticancer agent. As a general conse-quence, exposure to sunlight should be increased carefully without inducing UV erythemas. According to standard rec-ommendations, dietary or supplemental daily intake should provide at least 5–20 g, while recent suggestions recommend a much higher health promoting dietary intake of 25–100 g (1,000–4,000 IU) of vitamin D3. Since very few foods contain vitamin D, an intake above 20 g cannot usually be obtained
Literatur
1 Garcia M, Jemal A, Ward E, Center M, Hao Y, Siegel R, Thun M: Global Cancer: Facts and Fig-ures 2007. Atlanta, Georgia, American Cancer So-ciety, 2007.
2 Boyle P, Anderson BO, Andersson LC, et al.: Need for global action for cancer control. Ann Oncol 2008;19:1519–1521.
3 Holick MF: Evolution and function of vitamin D. Recent Results Cancer Res 2003;164:3–28.
4 Cranney A, Horsley T, O’Donnell S, Weiler H, Puil L, Ooi D, Atkinson S, Ward L, Moher D, Hanley D, Fang M, Yazdi F, Garritty C, Sampson M, Barrowman N, Tsertsvadze A, Mamaladze V: Effectiveness and safety of vitamin D in relation to bone health. Evid Rep Technol Assess (Full Rep) 2007;(158):1–235.
5 Holick MF: Vitamin D: evolutionary, physiological and health perspectives. Curr Drug Targets 2011; 12:4–18.
6 Hathcock JN, Shao A, Vieth R, Heaney R: Risk assessment for vitamin D. Am J Clin Nutr 2007; 85:6–18.
7 Moore DD, Kato S, Xie W, Mangelsdorf DJ, Schmidt DR, Xiao R, Kliewer SA. International Union of Pharmacology. LXII. The NR1H and NR1I receptors: constitutive androstane receptor, pregnene receptor, farnesoid receptor alpha, farnesoid receptor beta, liver receptor alpha, liver receptor beta, and vitamin D receptor. Phar-macol Rev 2006;58:742–759.
8 Zittermann A, Gummert JF, Börgermann J: Vi-tamin D deficiency and mortality. Curr Opin Clin Nutr Metab Care 2009;12:634–639.
9 Manson JE, Mayne ST, Clinton SK: Vitamin D and prevention of cancer – ready for prime time? N Engl J Med 2011;364:1385–1387.
10 Heaney RP, Holick MF: Why the IOM recommen-dations for vitamin D are deficient. J Bone Miner Res 2011;26:455–457.
11 Holick MF, Chen TC: Vitamin D deficiency: a worldwide problem with health consequences. Am J Clin Nutr 2008;87:1080S–6S.
12 McKenna MJ: Differences in vitamin D status between countries in young adults and the elderly. Am J Med 1992;93:69–77.
13 Holick MF: Vitamin D deficiency. N Engl J Med 2007;357:266–281.
14 Nimitphong H, Holick MF: Vitamin D, neurocog-nitive functioning and immunocompetence. Curr Opin Clin Nutr Metab Care 2011;14:7–14.
15 Vieth R: Vitamin D supplementation, 25-hydroxy-vitamin D concentrations, and safety. Am J Clin Nutr 1999;69:842–856.
16 Prentice A: Vitamin D deficiency: a global perspec-tive. Nutr Rev 2008;66(10 suppl 2):S153–164.
17 Deutschen Gesellschaft für Ernährung (DGE): Referenzwerte für die Nährstoffzufuhr; 1. Aufl. Neustadt, Umschau Buchverlag, 2008.
18 Ross AC, Manson JE, Abrams SA, Aloia JF, Bran-non PM, Clinton SK, Durazo-Arvizu RA, Gallagh-er JC, Gallo RL, Jones G, Kovacs CS, Mayne ST, Rosen CJ, Shapses SA: The 2011 report on dietary reference intakes for calcium and vitamin D from the Institute of Medicine: what clinicians need to know. J Clin Endocrinol Metab 2011;96:53–58.
19 Bischoff-Ferrari H, Staehelin HB. Vitamin D: Up-date bone and muscle effects. Aktuel Ernaehr Med 2010;35:18–22.
20 Lee DM, Rutter MK, O’Neill TW, Boonen S, Vanderschueren D, Bouillon R, Bartfai G, Casanueva FF, Finn JD, Forti G, Giwercman A, Han TS, Huhtaniemi IT, Kula K, Lean MEJ, Pend-leton N, Punab M, Silman AJ, Wu FCW: Vitamin D, parathyroid hormone and the metabolic syn-drome in middle-aged and older European men. Eur J Endocrinol 2009;161:947–954.
21 Humble MB: Vitamin D, light and mental health. J Photochem Photobiol B 2010;101:142–149.
22 Dobnig H, Pilz S, Scharnagl H, Renner W, Seel-horst U, Wellnitz B, Kinkeldei J, Boehm BO, Weihrauch G, Maerz W: Independent asso-ciation of low serum 25-hydroxyvitamin d and 1,25-dihydroxy vitamin d levels with all-cause and cardiovascular mortality. Arch Intern Med 2008; 168:1340–1349.
23 Pittas AG, Chung M, Trikalinos T, Mitri J, Bren-del M, Patel K, Lichtenstein AH, Lau J, Balk EM: Systematic review: vitamin D and cardiometabolic outcomes. Ann Intern Med 2010;152:307–314.
24 Pittas AG, Dawson-Hughes B: Vitamin D and dia-betes. J Steroid Biochem Mol Biol 2010;121:425–429.
25 Apperly FL: The relation of solar radiation to can-cer mortality in North America. Cancer Res 1941; 1:191–195.
26 Garland CF, Garland FC: Do sunlight and vitamin D reduce the likelihood of colon cancer? Int J Epi-demiol 1980;9:227–231.
27 Grant WB: An estimate of premature cancer mor-tality in the U.S. due to inadequate doses of solar ultraviolet-B radiation. Cancer 2002;94:1867–1875.
28 Grant WB, Garland CF: The association of solar ultraviolet B (UVB) with reducing risk of cancer: multifactorial ecologic analysis of geographic vari-ation in age-adjusted cancer mortality rates. Anti-cancer Res 2006;26:2687–2699.
29 Boscoe FP, Schymura MJ: Solar ultraviolet-B ex-posure and cancer incidence and mortality in the United States, 1993–2002. BMC Cancer 2006;6:264.
30 Grant WB: How strong is the evidence that solar ultraviolet B and vitamin D reduce the risk of cancer? An examination using Hill’s criteria for causality. Dermatoendocrinol 2009;1:17–24.
31 Garland CF, Garland FC, Gorham ED, Lipkin M, Newmark H, Mohr SB, Holick MF: The role of vitamin D in cancer prevention. Am J Public Health 2006;96:252–261.
32 Giovannucci E, Liu Y, Rimm EB, Hollis BW, Fuchs CS, Stampfer MJ, Willett WC: Prospective study of predictors of vitamin D status and cancer incidence and mortality in men. J Natl Cancer Inst 2006;98:451–459.
33 Berwick M, Armstrong BK, Ben-Porat L, Fine J, Kricker A, Eberle C, Barnhill R: Sun exposure and mortality from melanoma. J Natl Cancer Inst 2005; 97:195–199.
34 Smedby KE, Hjalgrim H, Melbye M, Torrång A, Rostgaard K, Munksgaard L, Adami J, Hansen M, Porwit-MacDonald A, Jensen BA, Roos G, Ped-ersen BB, Sundström C, Glimelius B, Adami H-O: Ultraviolet radiation exposure and risk of malignant lymphomas. J Natl Cancer Inst 2005;97:199–209.
35 Kricker A, Armstrong BK, Hughes AM, Goumas C, Smedby KE, Zheng T, Spinelli JJ, De Sanjosé S, Hartge P, Melbye M, Willett EV, Becker N, Chiu BCH, Cerhan JR, Maynadié M, Staines A, Cocco P, Boffeta P: Personal sun exposure and risk of non Hodgkin lymphoma: a pooled analysis from the In-terlymph Consortium. Int J Cancer 2008;122:144–154.
36 Mohr SB, Garland CF, Gorham ED, Grant WB, Garland FC: Could ultraviolet B irradiance and vi-tamin D be associated with lower incidence rates of lung cancer? J Epidemiol Community Health 2008; 62:69–74.
37 Garland CF, Mohr SB, Gorham ED, Grant WB, Garland FC: Role of ultraviolet B irradiance and vitamin D in prevention of ovarian cancer. Am J Prev Med 2006;31:512–514.
38 Mohr SB, Gorham ED, Garland CF, Grant WB, Garland FC: Low ultraviolet B and increased risk of brain cancer: an ecological study of 175 coun-tries. Neuroepidemiology 2010;35:281–290.
39 Mohr SB, Garland CF, Gorham ED, Grant WB, Garland FC: Ultraviolet B irradiance and incidence rates of bladder cancer in 174 countries. Am J Prev Med 2010;38:296–302.
40 Hanchette CL, Schwartz GG: Geographic patterns of prostate cancer mortality. Evidence for a protec-tive effect of ultraviolet radiation. Cancer 1992;70: 2861–2869.

Forsch Komplementmed 2011;18:176–184Vitamin D in Oncology 183
41 Mohr SB, Garland CF, Gorham ED, Grant WB, Garland FC: Ultraviolet B irradiance and vitamin D status are inversely associated with incidence rates of pancreatic cancer worldwide. Pancreas 2010;39: 669–674.
42 Rodriguez C, McCullough ML, Mondul AM, Jacobs EJ, Fakhrabadi-Shokoohi D, Giovannucci EL, Thun MJ, Calle EE: Calcium, dairy products, and risk of prostate cancer in a prospective cohort of United States men. Cancer Epidemiol Biomark-ers Prev 2003;12:597–603.
43 Skinner HG, Michaud DS, Giovannucci E, Willett WC, Colditz GA, Fuchs CS: Vitamin D intake and the risk for pancreatic cancer in two cohort studies. Cancer Epidemiol Biomarkers Prev 2006;15:1688–1695.
44 Garland C, Shekelle RB, Barrett-Connor E, Criqui MH, Rossof AH, Paul O: Dietary vitamin D and calcium and risk of colorectal cancer: a 19-year prospective study in men. Lancet 1985;1:307–309.
45 Gorham ED, Garland CF, Garland FC, Grant WB, Mohr SB, Lipkin M, Newmark HL, Giovannucci E, Wei M, Holick MF: Vitamin D and prevention of colorectal cancer. J Steroid Biochem Mol Biol 2005;97:179–194.
46 Gorham ED, Garland CF, Garland FC, Grant WB, Mohr SB, Lipkin M, Newmark HL, Giovannucci E, Wei M, Holick MF: Optimal vitamin D status for colorectal cancer prevention: a quantitative meta analysis. Am J Prev Med 2007;32:210–216.
47 Wei MY, Garland CF, Gorham ED, Mohr SB, Giovannucci E: Vitamin D and prevention of colorectal adenoma: a meta-analysis. Cancer Epi-demiol Biomarkers Prev 2008;17:2958–2969.
48 Zhou G, Stoitzfus J, Swan BA: Optimizing vita-min D status to reduce colorectal cancer risk: an evidentiary review. Clin J Oncol Nurs 2009;13:E3–E17.
49 Jenab M, Bueno-de-Mesquita HB, Ferrari P, van Duijnhoven FJB, Norat T, Pischon T, Jansen EHJM, Slimani N, Byrnes G, Rinaldi S, Tjøn-neland A, Olsen A, Overvad K, Boutron-Ruault M-C, Clavel-Chapelon F, Morois S, Kaaks R, Lin-seisen J, Boeing H, Bergmann MM, Trichopoulou A, Misirli G, Trichopoulos D, Berrino F, Vineis P, Panico S, Palli D, Tumino R, Ros MM, van Gils CH, Peeters PH, Brustad M, Lund E, Tormo M-J, Ardanaz E, Rodríguez L, Sánchez M-J, Dorron-soro M, Gonzalez CA, Hallmans G, Palmqvist R, Roddam A, Key TJ, Khaw K-T, Autier P, Hainaut P, Riboli E: Association between pre-diagnostic circulating vitamin D concentration and risk of colorectal cancer in European populations:a nested case-control study. Br Med J 2010;340:b5500.
50 Garland CF, Gorham ED, Mohr SB, Grant WB, Giovannucci EL, Lipkin M, Newmark H, Holick MF, Garland FC: Vitamin D and prevention of breast cancer: pooled analysis. J Steroid Biochem Mol Biol 2007;103:708–711.
51 Rejnmark L, Tietze A, Vestergaard P, Buhl L, Lehbrink M, Heickendorff L, Mosekilde L: Re-duced prediagnostic 25-hydroxyvitamin D levels in women with breast cancer: a nested case-control study. Cancer Epidemiol Biomarkers Prev 2009;18: 2655–2660.
52 Engel P, Fagherazzi G, Boutten A, Dupré T, Mes-rine S, Boutron-Ruault M-C, Clavel-Chapelon F: Serum 25(OH) vitamin D and risk of breast can-cer: a nested case-control study from the French E3N cohort. Cancer Epidemiol Biomarkers Prev 2010;19:2341–2350.
53 Yin L, Grandi N, Raum E, Haug U, Arndt V, Bren-ner H: Meta-analysis: serum vitamin D and breast cancer risk. Eur J Cancer 2010;46:2196–2205.
54 Engel P, Fagherazzi G, Mesrine S, Boutron-Ruault M-C, Clavel-Chapelon F: Joint effects of dietary vitamin D and sun exposure on breast cancer risk: results from the French E3N cohort. Cancer Epide-miol. Biomarkers Prev 2011;20:187–198.
55 Yao S, Sucheston LE, Millen AE, Johnson CS, Trump DL, Nesline MK, Davis W, Hong C-C, McCann SE, Hwang H, Kulkarni S, Edge SB, O’Connor TL, Ambrosone CB: Pretreatment serum concentrations of 25-hydroxyvitamin D and breast cancer prognostic characteristics: a case-control and a case-series study. PLoS ONE 2011;6:e17251.
56 McCullough ML, Stevens VL, Patel R, Jacobs EJ, Bain EB, Horst RL, Gapstur SM, Thun MJ, Calle EE: Serum 25-hydroxyvitamin D concentrations and postmenopausal breast cancer risk: a nested case control study in the Cancer Prevention Study-II Nutrition Cohort. Breast Cancer Res 2009;11:R64.
57 Jacobs ET, Thomson CA, Flatt SW, Al-Delaimy WK, Hibler EA, Jones LA, Leroy EC, Newman VA, Parker BA, Rock CL, Pierce JP: Vitamin D and breast cancer recurrence in the Women’s Healthy Eating and Living (WHEL) Study. Am J Clin Nutr 2011;93:108–117.
58 Chlebowski RT, Johnson KC, Kooperberg C, Pet-tinger M, Wactawski-Wende J, Rohan T, Rossouw J, Lane D, O’Sullivan MJ, Yasmeen S, Hiatt RA, Shikany JM, Vitolins M, Khandekar J, Hubbell FA: Calcium plus vitamin D supplementation and the risk of breast cancer. J Natl Cancer Inst 2008;100: 1581–1591.
59 Wactawski-Wende J, Kotchen JM, Anderson GL, Assaf AR, Brunner RL, O’Sullivan MJ, Margolis KL, Ockene JK, Phillips L, Pottern L, Prentice RL, Robbins J, Rohan TE, Sarto GE, Sharma S, Ste-fanick ML, Van Horn L, Wallace RB, Whitlock E, Bassford T, Beresford SAA, Black HR, Bonds DE, Brzyski RG, Caan B, Chlebowski RT, Cochrane B, Garland C, Gass M, Hays J, Heiss G, Hendrix SL, Howard BV, Hsia J, Hubbell FA, Jackson RD, Johnson KC, Judd H, Kooperberg CL, Kuller LH, LaCroix AZ, Lane DS, Langer RD, Lasser NL, Lewis CE, Limacher MC, Manson JE: Calcium plus vitamin D supplementation and the risk of colorectal cancer. N Engl J Med 2006;354:684–696.
60 Lappe JM, Travers-Gustafson D, Davies KM, Reck-er RR, Heaney RP: Vitamin D and calcium sup-plementation reduces cancer risk: results of a rand-omized trial. Am J Clin Nutr 2007;85:1586–1591.
61 Grant WB, Garland CF, Gorham ED: An estimate of cancer mortality rate reductions in Europe and the US with 1,000 IU of oral vitamin D per day. Recent Results Cancer Res 2007;174:225–234.
62 Rhee H, Coebergh JW, Vries E: Sunlight, vitamin D and the prevention of cancer: a systematic re-view of epidemiological studies. Eur J Cancer Prev 2009;18:458–475.
63 Gandini S, Boniol M, Haukka J, Byrnes G, Cox B, Sneyd MJ, Mullie P, Autier P: Meta-analysis of observational studies of serum 25-hydroxyvitamin D levels and colorectal, breast and prostate cancer and colorectal adenoma. Int. J Cancer 2011;128: 1414–1424.
64 Helzlsouer KJ: Overview of the Cohort Consor-tium Vitamin D Pooling Project of Rarer Cancers. Am J Epidemiol 2010;172:4–9.
65 Ma Y, Trump DL, Johnson CS: Vitamin D in com-bination cancer treatment. J Cancer 2010;1:101–107.
66 Johnson CS, Muindi JR, Hershberger PA, Trump DL: The antitumor efficacy of calcitriol: preclinical studies. Anticancer Res 2006;26:2543–2549.
67 Yu W-D, Ma Y, Flynn G, Muindi JR, Kong R-X, Trump DL, Johnson CS: Calcitriol enhances gem-citabine anti-tumor activity in vitro and in vivo by promoting apoptosis in a human pancreatic carci-noma model system. Cell Cycle 2010;9:3022–3029.
68 Colston KW, James SY, Ofori-Kuragu EA, Binderup L, Grant AG: Vitamin D receptors and anti-proliferative effects of vitamin D derivatives in human pancreatic carcinoma cells in vivo and in vitro. Br J Cancer 1997;76:1017–1020.
69 Kawa S, Nikaido T, Aoki Y, Zhai Y, Kumagai T, Furihata K, Fujii S, Kiyosawa K: Vitamin D ana-logues up-regulate p21 and p27 during growth in-hibition of pancreatic cancer cell lines. Br J Cancer 1997;76:884–889.
70 Sato T, Takusagawa K, Asoo N, Konno K: Effect of 1 alpha-hydroxyvitamin D3 on metastasis of rat as-cites hepatoma K-231. Br J Cancer 1984;50:123–125.
71 Lambert JR, Eddy VJ, Young CD, Persons KS, Sarkar S, Kelly JA, Genova E, Lucia MS, Faller DV, Ray R: A vitamin D receptor-alkylating deriv-ative of 1 ,25-dihydroxyvitamin D3 inhibits growth of human kidney cancer cells and suppresses tumor growth. Cancer Prev Res (Phila) 2010;3:1596–1607.
72 Ma Y, Yu W-D, Trump DL, Johnson CS: 1,25D3 enhances antitumor activity of gemcitabine and cisplatin in human bladder cancer models. Cancer 2010;116:3294–3303.
73 Lange TS, Stuckey AR, Robison K, Kim KK, Singh RK, Raker CA, Brard L: Effect of a vitamin D(3) derivative (B3CD) with postulated anti-cancer activity in an ovarian cancer animal model. Invest New Drugs 2010;28:543–553.
74 Slominski AT, Kim T-K, Janjetovic Z, Tuckey RC, Bieniek R, Yue J, Li W, Chen J, Nguyen MN, Tang EKY, Miller D, Chen TC, Holick M: 20-Hydroxy-vitamin D2 is a noncalcemic analog of vitamin D with potent antiproliferative and prodifferentia-tion activities in normal and malignant cells. Am J Physiol, Cell Physiol 2011;300:C526–541.
75 Sertznig P, Seifert M, Tilgen W, Reichrath J: Ac-tivation of vitamin D receptor (VDR) and per-oxisome proliferator-activated receptor (PPAR)-signaling pathways through 1,25(OH)(2)D(3) in melanoma cell lines and other skin-derived cell lines. Dermatoendocrinology 2009;1:232–238.
76 Flynn G, Chung I, Yu W-D, Romano M, Modze- lewski RA, Johnson CS, Trump DL: Calcitriol (1,25-dihydroxycholecalciferol) selectively inhib-its proliferation of freshly isolated tumor-derived endothelial cells and induces apoptosis. Oncology 2006;70:447–457.
77 Sundaram S, Sea A, Feldman S, Strawbridge R, Hoopes PJ, Demidenko E, Binderup L, Gewirtz DA: The combination of a potent vitamin D3 ana-log, EB 1089, with ionizing radiation reduces tumor growth and induces apoptosis of MCF-7 breast tumor xenografts in nude mice. Clin Cancer Res 2003;9:2350–2356.
78 Krishnan AV, Feldman D: Molecular pathways mediating the anti-inflammatory effects of calcitri-ol: implications for prostate cancer chemopreven-tion and treatment. Endocr Relat Cancer 2010;17: R19–38.
79 Trump DL, Deeb KK, Johnson CS. Vitamin D: considerations in the continued development as an agent for cancer prevention and therapy. Cancer J 2010;16:1–9.
80 Trump DL, Potter DM, Muindi J, Brufsky A, John-son CS: Phase II trial of high-dose, intermittent calcitriol (1,25 dihydroxyvitamin D3) and dexam-ethasone in androgen-independent prostate cancer. Cancer 2006;106:2136–2142.

184 Forsch Komplementmed 2011;18:176–184 Arends
81 Jain RK, Trump DL, Egorin MJ, Fernandez M, Johnson CS, Ramanathan RK: A phase I study of the vitamin D(3) analogue ILX23–7553 adminis-tered orally to patients with advanced solid tumors. Invest New Drugs 2010; Epub ahead of print.
82 Giovannucci E, Chan AT: Role of vitamin and mineral supplementation and aspirin use in cancer survivors. J Clin Oncol 2010;28:4081–4085.
83 Santini D, Galluzzo S, Vincenzi B, Zoccoli A, Fer-raro E, Lippi C, Altomare V, Tonini G, Bertoldo F: Longitudinal evaluation of vitamin D plasma lev-els during anthracycline- and docetaxel-based ad-juvant chemotherapy in early-stage breast cancer patients. Ann Oncol 2010;21:185–186.
84 Chlebowski RT, Johnson KC, Lane D, Pettinger M, Kooperberg CL, Wactawski-Wende J, Rohan T, O’Sullivan MJ, Yasmeen S, Hiatt RA, Shikany JM, Vitolins M, Khandekar J, Hubbell FA: 25-hy-droxyvitamin D concentration, vitamin D intake and joint symptoms in postmenopausal women. Maturitas 2011;68:73–78.
85 Goodwin PJ, Ennis M, Pritchard KI, Koo J, Hood N: Prognostic effects of 25-hydroxyvitamin D levels in early breast cancer. J Clin Oncol 2009;27:3757–3763.
86 Prieto-Alhambra D, Javaid MK, Servitja S, Arden NK, Martinez-García M, Diez-Perez A, Albanell J, Tusquets I, Nogues X: Vitamin D threshold to prevent aromatase inhibitor-induced arthralgia: a prospective cohort study. Breast Cancer Res Treat 2011;125:869–878.
87 Neuhouser ML, Sorensen B, Hollis BW, Ambs A, Ulrich CM, McTiernan A, Bernstein L, Wayne S, Gilliland F, Baumgartner K, Baumgartner R, Bal-lard-Barbash R: Vitamin D insufficiency in a multi-ethnic cohort of breast cancer survivors. Am J Clin Nutr 2008;88:133–139.
88 Ng K, Meyerhardt JA, Wu K, Feskanich D, Hollis BW, Giovannucci EL, Fuchs CS: Circulating 25-hy-droxyvitamin d levels and survival in patients with colorectal cancer. J Clin Oncol 2008;26:2984–2991.
89 Ng K, Wolpin BM, Meyerhardt JA, Wu K, Chan AT, Hollis BW, Giovannucci EL, Stampfer MJ, Willett WC, Fuchs CS: Prospective study of pre-dictors of vitamin D status and survival in patients with colorectal cancer. Br J Cancer 2009;101:916–923.
90 Newton-Bishop JA, Beswick S, Randerson-Moor J, Chang Y-M, Affleck P, Elliott F, Chan M, Leake S, Karpavicius B, Haynes S, Kukalizch K, Whitaker L, Jackson S, Gerry E, Nolan C, Bertram C, Marsden J, Elder DE, Barrett JH, Bishop DT: Serum 25-hydroxyvitamin D3 levels are associated with Breslow thickness at presentation and survival from melanoma. J Clin Oncol 2009;27:5439–5444.
91 Drake MT, Maurer MJ, Link BK, Habermann TM, Ansell SM, Micallef IN, Kelly JL, Macon WR, Nowakowski GS, Inwards DJ, Johnston PB, Singh RJ, Allmer C, Slager SL, Weiner GJ, Witzig TE, Cerhan JR: Vitamin D insufficiency and prog-nosis in non-Hodgkin’s lymphoma. J Clin Oncol 2010;28:4191–4198.
92 Shinchuk LM, Shinchuk L, Holick MF: Vitamin D and rehabilitation: improving functional out-comes. Nutr Clin Pract 2007;22:297–304.
93 Turner MK, Hooten WM, Schmidt JE, Kerk-vliet JL, Townsend CO, Bruce BK: Prevalence and clinical correlates of vitamin D inadequacy among patients with chronic pain. Pain Med 2008; 9:979–984.
94 Nogues X, Servitja S, Peña MJ, Prieto-Alhambra D, Nadal R, Mellibovsky L, Albanell J, Diez-Perez A, Tusquets I: Vitamin D deficiency and bone mineral density in postmenopausal women receiving aromatase inhibitors for early breast cancer. Maturitas 2010;66:291–297.
95 Pearce SHS, Cheetham TD: Diagnosis and man-agement of vitamin D deficiency. Br Med J 2010; 340:b5664.
96 Bayer W: Steckbrief: Vitamin D. Ernähr Med 2009;24:21–22.
97 Vieth R, Chan PC, MacFarlane GD: Efficacy and safety of vitamin D3 intake exceeding the lowest observed adverse effect level. Am J Clin Nutr 2001;73:288–294.
98 Janssens W, Bouillon R, Claes B, Carremans C, Lehouck A, Buysschaert I, Coolen J, Mathieu C, Decramer M, Lambrechts D: Vitamin D defi-ciency is highly prevalent in COPD and correlates with variants in the vitamin D-binding gene. Tho-rax 2010;65:215–220.
99 Gilbert CR, Arum SM, Smith CM: Vitamin D deficiency and chronic lung disease. Can Respir J 2009;16:75–80.
100 Rostand SG: Vitamin D, blood pressure, and Af-rican Americans: toward a unifying hypothesis. Clin J Am Soc Nephrol 2010;5:1697–1703.
101 Wang TJ, Pencina MJ, Booth SL, Jacques PF, Ingelsson E, Lanier K, Benjamin EJ, D’Agostino RB, Wolf M, Vasan RS: Vitamin D deficiency and risk of cardiovascular disease. Circulation 2008;117:503–511.
102 Wang L, Manson JE, Song Y, Sesso HD: System-atic review: vitamin D and calcium supplementa-tion in prevention of cardiovascular events. Ann Intern Med 2010;152:315–323.
103 Pittas AG, Sun Q, Manson JE, Dawson-Hughes B, Hu FB: Plasma 25-hydroxyvitamin D concen-tration and risk of incident type 2 diabetes in women. Diabetes Care 2010;33:2021–2023.
104 Timms PM, Mannan N, Hitman GA, Noonan K, Mills PG, Syndercombe-Court D, Aganna E, Price CP, Boucher BJ: Circulating MMP9, vita-min D and variation in the TIMP-1 response with VDR genotype: mechanisms for inflammatory damage in chronic disorders? Quart J Med 2002; 95:787–796.
105 Coussens A, Timms PM, Boucher BJ, Venton TR, Ashcroft AT, Skolimowska KH, Newton SM, Wilkinson KA, Davidson RN, Griffiths CJ, Wilkinson RJ, Martineau AR: 1alpha,25-dihy-droxyvitamin D3 inhibits matrix metalloprotein-ases induced by Mycobacterium tuberculosis in-fection. Immunology 2009;127:539–548.
106 Luong KVQ, Nguyen LTH: Impact of vitamin D in the treatment of tuberculosis. Am J Med Sci 2011;341:493–498
107 Sita-Lumsden A, Lapthorn G, Swaminathan R, Milburn HJ: Reactivation of tuberculosis and vi-tamin D deficiency: the contribution of diet and exposure to sunlight. Thorax 2007;62:1003–1007.
108 Takiishi T, Gysemans C, Bouillon R, Mathieu C: Vitamin D and diabetes. Endocrinol Metab Clin North Am 2010;39:419–446.
109 Mohr SB, Garland CF, Gorham ED, Garland FC: The association between ultraviolet B irradi-ance, vitamin D status and incidence rates of type 1 diabetes in 51 regions worldwide. Diabetologia 2008;51:1391–1398.
110 Wen H, Baker JF: Vitamin D, immunoregula-tion, and rheumatoid arthritis. J Clin Rheumatol 2011;17:102–107.
111 Burton JM, Kimball S, Vieth R, Bar-Or A, Dosch H-M, Cheung R, Gagne D, D’Souza C, Ursell M, O’Connor P: A phase I/II dose-escalation trial of vitamin D3 and calcium in multiple sclerosis. Neurology 2010;74:1852–1859.
112 Lee DM, Tajar A, O’Neill TW, O’Connor DB, Bartfai G, Boonen S, Bouillon R, Casanueva FF, Finn JD, Forti G, Giwercman A, Han TS, Huhtaniemi IT, Kula K, Lean ME, Punab M, Silman AJ, Vanderschueren D, Wu FC, Pend-leton N: Lower vitamin D levels are associated with depression among community-dwelling European men. J Psychopharmacol 2010; doi: 10.1177/0269881110379287..
113 Lee DM, Tajar A, Ulubaev A, Pendleton N, O’Neill TW, O’Connor DB, Bartfai G, Boonen S, Bouillon R, Casanueva FF, Finn JD, Forti G, Giwercman A, Han TS, Huhtaniemi IT, Kula K, Lean MEJ, Punab M, Silman AJ, Vanderschuer-en D, Wu FCW: Association between 25-hydrox-yvitamin D levels and cognitive performance in middle-aged and older European men. J Neurol Neurosurg Psychiatr 2009;80:722–729.
114 Pogge E: Vitamin D and Alzheimer’s disease: is there a link? Consult Pharm 2010;25:440–450.
115 McGrath JJ, Burne TH, Féron F, Mackay-Sim A, Eyles DW: Developmental vitamin D deficiency and risk of schizophrenia: a 10-year update. Schizo phr Bull 2010;36:1073–1078.